Ana Catalina Macias, MD Assistant Professor, Section of Geriatrics, Department of Medicine Baylor College of Medicine Geriatric Medicine and Wound
|
|
|
- Alexandra Powell
- 5 years ago
- Views:
Transcription


1 Ana Catalina Macias, MD Assistant Professor, Section of Geriatrics, Department of Medicine Baylor College of Medicine Geriatric Medicine and Wound Care Michael E. DeBakey VA Medical Center
2 Speaker Disclosure Dr. Macias has disclosed that she has no actual or potential conflict of interest in relation to this topic.
3 Objectives By the end of this activity, the participant should be better able to: Discuss the cascade of normal wound healing. Examine the most common factors that affect wound healing. Discuss the TIME principle of wound healing. Review 4 major types of wounds.
4 Wound Healing Physiology Phases of Wound Healing Hemostasis 0 3 hours Inflammatory 0 3 days Proliferative 3 21 days Remodeling/Maturation 21 days 1.5 years Yamaguchi Y, Yoshikawa K. Cutaneous wound healing: an update. J Dermatol Oct;28(10):
5
6 Hemostasis Occurs within minutes of the initial injury unless there are underlying clotting disorders.
7 Inflammation Vasodilation increase in blood flow erythema, swelling and warmth Neutrophils phagocytize debris and micro organisms (first line of defense) Monocytes then release intracellular enzymes to further digest tissue Fibrin is broken and attracts fibroblasts and epithelial cells which are aided by local mast cells Cytokines and growth factors are released
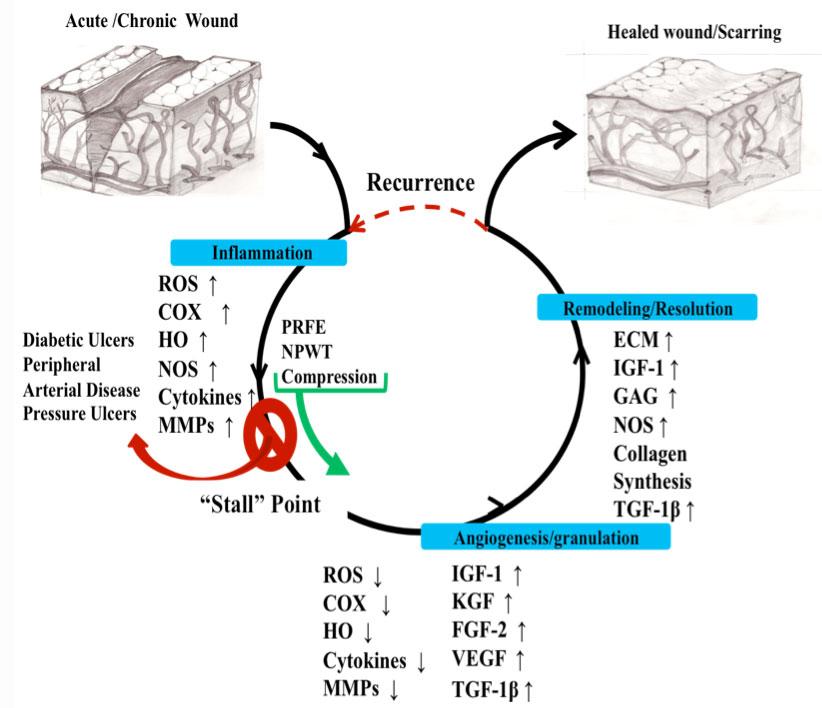
8 Inflammation Monocytes differentiate into macrophages and secrete extracellular enzymes, paving the way to resolving inflammation MMPs (Matrix metalloproteinases) Responsible for removal of devitalized tissue Repair of lost or damaged tissue Remodeling MMPs are balanced by TIMPs Tissue inhibitors of metalloproteinases Released locally by cells TIMPs bind to MMPs and deactivate them Uncontrolled MMPs cause degradation of newly formed tissue or destruction of growth factors prolonging inflammatory phase and delay in wound healing Chronic wound
9 Proliferation Characterized by angiogenesis, collagen deposition, granulation tissue formation, wound contraction and epithelialization Wound bed must fill in from the bottom up with collagen and must be maintained in an optimal environment (moisture balance) before the epithelial cells will begin to proliferate and migrate across the wound surface to close the wound. Balance between MMPs and TIMPs result in net production of new tissue.
10 Remodeling Healing process involves the remodeling and realignment of collagen Tensile strength 70 80% of what it was before the injury Main cells Fibroblasts
11 Chronic Wounds Stalled with suppressed cell division and migration Due to: High levels of inflammatory cytokines and MMPs Low levels of TIMPs and growth factors In this environment cells are senescent and unresponsive to growth factors
12 Factors Affecting Wound Healing Local Growth factors Edema Ischemia Low oxygen Infection Arterial insufficiency Venous insufficiency Neuropathy Systemic Inadequate perfusion Metabolic disease Chronic disease Nutrition Smoking Exposure to radiation
13 Wound Infection Overgrowth of Microorganisms Resultant Tissue Destruction Local symptoms Wound deterioration Erythema, edema, drainage (purulent), tenderness, warmth, induration and/or crepitus Systemic symptoms Fever, leukocytosis, confusion, tachycardia, hypotension, malaise
14 Wound Infection Prolongs the inflammatory stage Induces additional tissue destruction Delays collagen synthesis Prevents epithelialization
15 Colonization vs. Infection Colonization Bacteria in wound bed, not affecting the environment Critical Colonization Suspect bacterial burden if a clean wound shows no improvement after 14 DAYS of topical therapy Infection Invasion of the soft tissues
16 Chronic Wound Infection Wound Culture Traditional swab culture Not recommended Detects only surface bacterial colonization/contamination May not reflect the invasive organism causing infection Quantitative Wound Culture Recommended Documents bacterial burden Identifies bacteria actually invading wound tissue Tissue Biopsy, Needle Aspiration or Quantitative Swab Technique
17 Topical Antimicrobial Therapy Silver dressings Cadexomer iodine Others used just for short periods Acetic acid Hydrogen peroxide Chlorpactin Dakin s Povidone iodine
18 TIME Principle Structured approach to wound bed preparation Tissue Infection/inflammation Moisture balance Edge of wound Optimizes the management of chronic wounds Should be done with every wound assessment

19 Schultz GS, Sibbald RG, Falanga V, et al. Wound bed preparation: a systematic approach to wound management. Wound Repair Regen Mar;11 Suppl 1:S1 28.
20 T Tissue Necrotic tissue Prolongs the inflammatory phase Delays wound healing Medium for bacterial growth Debridement Facilitates visualization of wound base Transforms the chronic wound by creating an acute wound Creates a viable wound bed Autolytic, Sharp/surgical, Mechanical, Biotherapy, Enzymatic (chemical)
21 I Infection/Inflammation Biofilms Complex microbial community bacteria embedded in a protective matrix of sugars and proteins Provide protection for microorganisms embedded within them, improving tolerance to the host s immune system, antimicrobials and environmental stresses Major contributing factor to chronic inflammatory changes in the wound bed Treatment Removed by sharp debridement Antibiofilm agents silver, iodine and honey dressings
22 I Infection/Inflammation Manage bacterial load Contamination, colonization or critical colonization Treat infection Local or systemic Manage inflammation from chronic diseases Autoimmune diseases SLE, RA, Vasculitis Inflammatory conditions Inflammatory bowel disease
23 M Moisture Imbalance Excess Tissue maceration Edema of the tissue Dry Slows epithelial cell migration Eschar formation
24 E Edge of Wound Impairment of keratinocyte migration Epibole rolled or curled under wound edges Aggressive debridement
25
26 Major Types of Wounds Pressure Injury Vascular Ulcers Arterial Ulcers Venous Stasis Ulcers Neuropathic/Diabetic Foot Ulcers Others Pyoderma gangrenosum, malignancies, calciphylaxis
27 Pressure Injury Localized damage to the skin and/or underlying soft tissue usually over a bony prominence or related to a medical or other device Result of intense and/or prolonged pressure or pressure in combination with shear Tolerance of soft tissue for pressure and shear are affected by: microclimate, nutrition, perfusion, co morbidities and condition of the soft tissue
 Trochanter (9%) Ischium (4%) Knee (3%) Tibia (2%) Heel & Ankle")
28 Common Sites of Pressure Injury Occiput (<1%) Scapula (<1%) Spine (<1%) Elbow (<1%) Sacrum & Coccyx (65%) Trochanter (9%) Ischium (4%) Knee (3%) Tibia (2%) Heel & Ankle (15%)
29 Pressure Injury By 2030, 20% of the world s population will be over the age of 65 Fastest growing segment of the population Individuals over the age of 80 70% of pressure injuries occur in people over the age of 70 NPUAP (2001) Prevalence 15.1%, incidence of 7% in US hospitals U.S. Census Bureau. Population Projections Program, Population Division, U.S. Census Bureau. Washington, DC, Thomas DR. Issues and dilemmas in the prevention and treatment of pressure ulcers. J Gerontol 2001; 56A:M
30 Pressure Injury in the Elderly Frailty Malnutrition Co morbidities Immobility Dementia Halfens RJ, et al. Int J Nurs Stud 2000;37(4): Lindgren M, el al. Scand J Caring Sci 2004;18(1): Nixon J, et al. Health Technol Assess 2006;10(22):iii iv, ix x, Nixon J, et al. Int J Nurs Stud 2007;44(5): Schoonhoven L, et al. Qual Saf Health Care 2006;15(1): Anthony D, el al. Clin Rehabil 2000;14(1): Pernerger TV, et al. J Clin Epidemiol 2002; 55(5):
31 Pressure Injury How are we doing? 503,300 admissions with PI as related diagnosis (2006) Total increase of 78.9% since % increase for primary diagnosis of pressure ulcer 15% increase in total hospitalizations Compared to stays for all other conditions, hospitalizations due to pressure ulcers were: More likely discharge to nursing home More likely to result in death 72% of patients admitted with a secondary diagnosis of pressure ulcers were 65 and older Russo, C.A. (Thomson Reuters), Steiner, C. (AHRQ) and Spector, W. (AHRQ). Hospitalizations Related to Pressure Ulcers, HCUP Statistical Brief #64. December Agency for Healthcare Research and Quality, Rockville, MD. us.ahrq.gov/reports/statbriefs/sb64.pdf Pressure Ulcers in America: prevalence, incidence and implications for the future. NPUAP 2001.

32 us.ahrq.gov/reports/statbriefs/sb64.jsp
33 Pressure Injury Cost Overall impact US 1.2% of total health care expenditure 2006 Cost Data Estimated cost to heal a single pressure ulcer range from $3,500 to $60,000 Legal Issues More than 17,000 lawsuits filed annually Average $250,000 per judgment Centers for Medicare and Medicaid. Fed Regist 2007 Aug 22;72(162): Bennett G et al. Age Aging. 2004;33(3): Severens JL, et al. Adv Skin Wound Care. 2002; 15(2): Bennet RG, et al. J AM Geriatric Soc. 2000; 48(1): 73 81
34 Pressure Injury Changes NPUAP changed terminology from Pressure ulcer to Pressure injury This more accurately describes pressure injuries to both intact and ulcerated skin Also, Arabic numbers are now used instead of Roman numerals The term suspected has been removed from the Deep Tissue Injury label
35 Pressure Injury Staging Staged to indicate the extent of tissue damage Only used for pressure ulcers Stage all pressure ulcers at the deepest level of damage Once a pressure ulcer is staged, it remains at that stage Reverse staging/back staging should never be used to describe the healing of a pressure ulcer
36 Pressure Injury Stage 1 Non blanchable erythema of intact skin Presence of blanchable erythema or changes in sensation, temperature, or firmness may precede visual changes. Color changes do not include purple or maroon discoloration
37 Pressure Injury Stage 1


38 Pressure Injury Stage 1
39 Pressure Injury Stage 2 Partial thickness skin loss with exposed dermis Wound bed is viable, pink or red, moist May also present as an intact or ruptured serum filled blister Adipose (fat) is not visible and deeper tissues are not visible
40 Pressure Injury Stage 2 Granulation tissue, slough and eschar are not present. Usually result from adverse microclimate and shear in the skin This stage should not be used to describe moisture associated skin damage (MASD) or traumatic wounds (skin tears, burns, abrasions
41 Pressure Injury Stage 2


42 Pressure Injury Stage 2
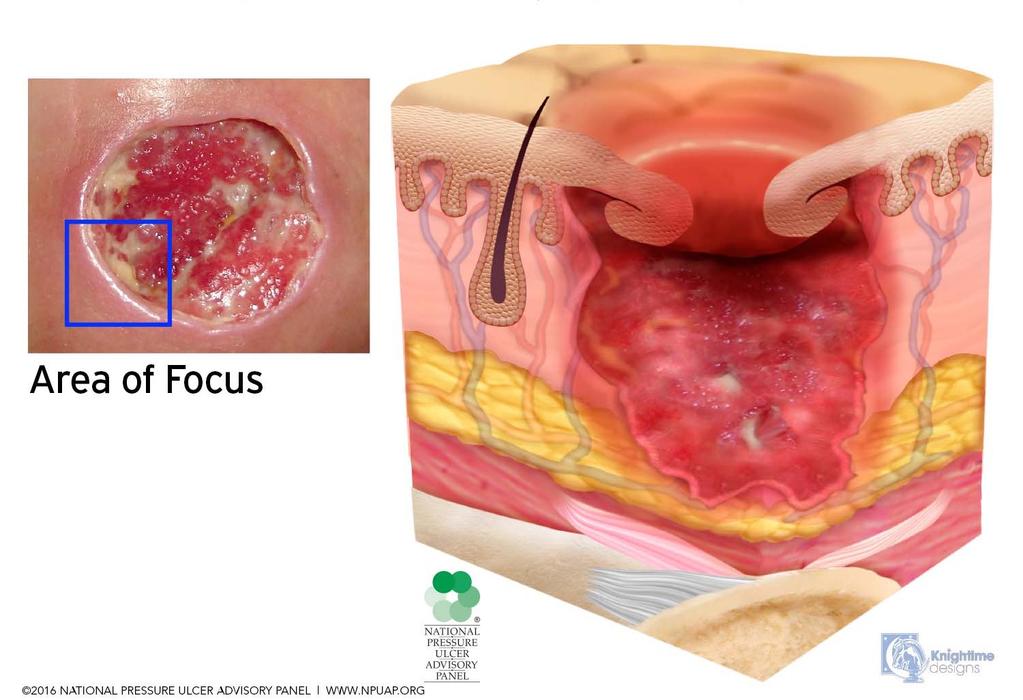
43 Pressure Injury Stage 3 Full thickness skin loss Adipose (fat) is visible in the ulcer Granulation tissue and epibole (rolled wound edges) are often present Slough and/or eschar may be visible
44 Pressure Injury Stage 3 Depth of tissue damage varies by anatomical location Areas of significant adiposity can develop deep wounds Undermining and tunneling may occur Fascia, muscle, tendon, ligament, cartilage and/or bone are not exposed If slough or eschar obscures the extent of tissue loss this is an Unstageable Pressure Injury
45 Pressure Injury Stage 3

46 Pressure Injury Stage 3
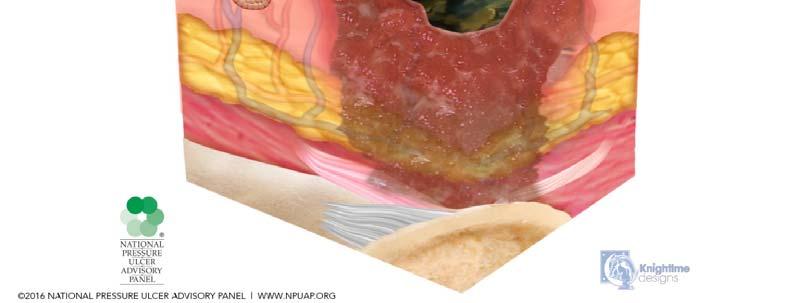
47 Pressure Injury Stage 4 Full thickness skin and tissue loss Exposed or directly palpable fascia, muscle, tendon, ligament, cartilage or bone in the ulcer Slough and/or eschar may be visible
48 Pressure Injury Stage 4 Epibole (rolled edges), undermining and/or tunneling often occur Depth varies by anatomical location If slough or eschar obscures the extent of tissue loss this is an Unstageable Pressure Injury
49 Pressure Injury Stage 4

50 Pressure Injury Stage 4
51 Unstageable Pressure Injury Full thickness skin and tissue loss in which the extent of tissue damage within the ulcer cannot be confirmed because it is obscured by slough or eschar If slough or eschar is removed, a Stage 3 or Stage 4 pressure injury will be revealed Stable eschar on the heel or ischemic limb should not be softened or removed

52 Unstageable Pressure Injury
53 Unstageable Pressure Injury

54 Unstageable Pressure Injury
55 Deep Tissue Pressure Injury Persistent non blanchable deep red, maroon or purple discoloration Pain and temperature change often precede skin color changes Discoloration may appear differently in darkly pigmented skin
56 Deep Tissue Pressure Injury Results from intense and/or prolonged pressure and shear forces at the bone muscle interface It may evolve rapidly to reveal the actual extent of tissue injury, or may resolve without tissue loss Do not use DTPI to describe vascular, traumatic, neuropathic, or dermatologic conditions
57 Deep Tissue Pressure Injury


58 Deep Tissue Pressure Injury
59 Other Definitions Medical Device Related Pressure Injury Result from the use of devices designed and applied for diagnostic or therapeutic purposes The resultant pressure injury generally conforms to the pattern or shape of the device The injury should be staged using the staging system.
60 Other Definitions Mucosal Membrane Pressure Injury Found on mucous membranes with a history of a medical device in use at the location of the injury Due to the anatomy of the tissue these ulcers cannot be staged
61 Pressure Injury Treatment Treatments: Wound Debridement if appropriate Appropriate dressing and frequency of change Main Remove pressure
62 Venous Insufficiency Ulcers Result from disorders of the deep venous system 1% of the population 3.5% of persons >65 Recurrence rate 70% Venous ulcers account for 90% of all chronic wounds on the lower leg
63 Venous Insufficiency Ulcers Predisposing factors: Thrombophlebitis Deep Vein Thrombosis (DVT) Prior pregnancy Leg trauma Cardiac disease Poor nutrition Absence of/or poor calf muscle pumps
64 Venous Insufficiency Ulcers Most are located in the medial aspect of leg superior to medial malleolus Granulation tissue usually present Irregular wound margins Exudation varies Degree of pain varies greatly from painless to extremely painful


65 Venous Insufficiency Ulcers
66 Venous Insufficiency Ulcers Assessment Edema Hemosiderin deposits Pulses present Ankle flaring Lipodermatosclerosis subcutaneous tissue fibrosis Dermatitis Scarring from previous ulcer
67 Venous Insufficiency Ulcers Treatments: Wound Debridement if appropriate Appropriate dressing and frequency of change depending on exudate Compression Leg elevation
68 Venous Insufficiency Ulcers Treatments: Exercise Weight loss Appropriate nutrition Consider use of adjunctive therapies Lymphedema pump
69 Compression Goal Reduce venous hypertension and improve venous return Necessary for healing ABI must be >0.8 to apply compression Explain to patient that compression therapy is lifelong Consider if patient will be able to apply them
70 Compression Different types Graded elastic compressive stockings Paste gauze boots Layered bandaging Adjustable layered compression garments Garments should be changed every 6 9 months if worn daily Noncompliance is the primary cause of compression therapy failure
71 Compression Contraindications Severe PVD Uncontrolled CHF Cutaneous infection Pulmonary edema Active DVT (OK once anticoagulation initiated)
72 Arterial Insufficiency Ulcers Impairment of arterial blood flow leading to tissue ischemia, necrosis or ulceration Most common disorder associated with compromised wound healing
73 Arterial Insufficiency Ulcers Risk Factors: Peripheral Vascular Disease (PVD) Diabetes Mellitus Hypertension Advanced age Smoking
74 Arterial Insufficiency Ulcers Most are located in the distal toes, heel, pretibial area Painful Pale wound bed lacking granulation, may be necrotic Minimal drainage desiccated and dry Appearance punched out Peri wound skin pale


75 Arterial Insufficiency Ulcers
76 Arterial Insufficiency Ulcers Assessment: Weak/absent pulses, Cool feet Pain and Claudication Dependent rubor Elevation pallor Absence of leg hair Skin shiny, dry, pale Thickened nails
77 Arterial Insufficiency Ulcers Treatments: Maximize blood flow and tissue perfusion Surgical revascularization Angioplasty Pharmacotherapy agents Lifestyle changes Judicious debridement
78 Neuropathic Ulcers Annual incidence 1% to 6.84% Lifetime risk 15% to 25% Associated with amputations 14% to 24% Death 5% to 13% of cases After an amputation 50% risk of contralateral amputations within 2 years Boulton AJ, Kirsner, RS, Vileikyte L. N Engl J Med. 2004; 351 (1): Boulton AJ, et al. Lancet. 2005;366(9498): Sanders LF. J Am Podiatric Med Assoc. 1994;84(7):
79 Neuropathic Ulcers Hospital admissions in diabetic patients related to foot ulcers is 6% to 25% Diabetic foot ulcers are a contributing factor in >85% of all diabetes related lower extremity amputations Relative 5 year mortality rates of for patients with neuropathic and ischemic diabetic foot ulcers were 45% and 55% respectively Apelqvist J, Larson J. Diabetes Metab Res Rev. 2000;16:S75 83 Pecoraro RE, Reiber GE, Burgess EM. Diabetes Care. 1990;13(5):
80 Neuropathic Ulcers Predisposing factors: Noncompliance with diabetes management/uncontrolled Peripheral vascular disease Peripheral neuropathy Motor leads to excessive callus build up and Charcot joint Sensory Diminished or absent sensation to pain, temperature and position. Loss of protective sensation Autonomic reduced or absent sweating, dry skin Cuts or trauma can go unnoticed
81 Neuropathic Ulcers Systemic factors: Uncontrolled hyperglycemia Duration of diabetes Peripheral vascular disease Visual impairment Older age Local factors: Peripheral neuropathy Structural foot deformity Trauma Improperly fitted shoes History of prior ulcer Pressure Limited joint mobility
82 Neuropathic Ulcers Painless Even wound margins with propensity to form callous Deep wound bed Granular tissue


83 Neuropathic Ulcers
84 Neuropathic Ulcers Wagner Classification System 0 No open lesions; may have deformity or cellulitis 1 Superficial diabetic ulcer (partial or full thickness) 2 Ulcer extension to ligament, tendon, joint capsule, or deep fascia without abscess or osteomyelitis 3 Deep ulcer with abscess, osteomyelitis, or joint sepsis 4 Gangrene localized to portion of forefoot or heel 5 Extensive gangrenous involvement of the entire foot Adapted from Wagner FW Jr. The Diabetic Foot. Orthopedics 1987;10:
85 Neuropathic Ulcers Assessment: Neuropathy Diminished or no sensation in foot Arterial evaluation Foot deformities
86 Neuropathic Ulcers Treatment Wound Debridement necrotic tissue and hyperkeratotic rim Appropriate dressing and frequency of change Control serum glucose levels Offloading and Orthotics Monitor for infection
87 Take Home Points The basic principles of wound healing apply to almost all types of wounds Accurate assessment of each type of wound is needed Refer to a wound care specialist when the wound is complicated or not healing
88 Thank You!
89 In what phase of wound healing are most chronic wounds likely stalled? 1. Proliferative phase 2. Hemostasis phase 3. Inflammatory phase 4. Remodeling/Maturation phase
90 Which is the most common pressure injury site? 1. Shoulder 2. Heel 3. Elbow 4. Sacrum
91 After wound is healed, the skin tensile strength is % of what it was before the injury % % % %
92 Noncompliance is the primary cause of compression therapy failure. 1. True 2. False
Wound Care for the Primary Care Physician
 Saturday General Session Wound Care for the Primary Care Physician Ana Catalina Macias, MD Assistant Professor of Medicine, Geriatrics Section Baylor College of Medicine Houston, Texas Educational Objectives
Saturday General Session Wound Care for the Primary Care Physician Ana Catalina Macias, MD Assistant Professor of Medicine, Geriatrics Section Baylor College of Medicine Houston, Texas Educational Objectives
Pressure Injury Staging Update 2016
 Pressure Injury Staging Update 2016 A Review of the New Changes for Pressure Injury Documentation and Staging Jeanne Terefenko, BSN, RN, CWOCN Ext. 5855 Pressure Ulcer Staging Updates: In April, 2016,
Pressure Injury Staging Update 2016 A Review of the New Changes for Pressure Injury Documentation and Staging Jeanne Terefenko, BSN, RN, CWOCN Ext. 5855 Pressure Ulcer Staging Updates: In April, 2016,
Treat the whole patient, not just the hole in the patient! 3/21/2017 CAN YOU CONNECT THE DOTS?? PHILOSOPHY OBJECTIVES
 CAN YOU CONNECT THE DOTS?? Boone Hospital Wound Healing Center Kimberly Jamison, MD, FACP, FAPWCA, PCWC Kim Mitchell, RN, BSN OBJECTIVES Describe the basic concepts of chronic wound care to ensure an optimal
CAN YOU CONNECT THE DOTS?? Boone Hospital Wound Healing Center Kimberly Jamison, MD, FACP, FAPWCA, PCWC Kim Mitchell, RN, BSN OBJECTIVES Describe the basic concepts of chronic wound care to ensure an optimal
New Strategies to Improve Assessment, Documentation and Prevention of Pressure Injuries
 New Strategies to Improve Assessment, Documentation and Prevention of Pressure Injuries Janet Cuddigan, PhD, RN, CWCN, FAAN Professor, UNMC College of Nursing Omaha, NE Focus of this Presentation New developments
New Strategies to Improve Assessment, Documentation and Prevention of Pressure Injuries Janet Cuddigan, PhD, RN, CWCN, FAAN Professor, UNMC College of Nursing Omaha, NE Focus of this Presentation New developments
Pressure Injury Definition and Stages
 Program Objective Pressure Injury Definition and Stages Identify the changes to the 2016 NPUAP staging system Changes to the Staging System in 2016 2 Anatomy of the Skin Anatomy of the Skin Largest organ
Program Objective Pressure Injury Definition and Stages Identify the changes to the 2016 NPUAP staging system Changes to the Staging System in 2016 2 Anatomy of the Skin Anatomy of the Skin Largest organ
Recognizing Pressure Injury
 Recognizing Pressure Injury Karen Zulkowski, DNS, RN Hawaii Recorded on March 8, 2017 1 A Little About Myself Executive editor of the Journal of the World Council of Enterostomal Therapists (JWCET) and
Recognizing Pressure Injury Karen Zulkowski, DNS, RN Hawaii Recorded on March 8, 2017 1 A Little About Myself Executive editor of the Journal of the World Council of Enterostomal Therapists (JWCET) and
Teaming Together to Understand Pressure Injuries / (Ulcers): NPUAP Terminology and Staging Clarification
: NPUAP Terminology and Staging Clarification") Teaming Together to Understand Pressure Injuries / (Ulcers): NPUAP Terminology and Staging Clarification We encourage you to share this information with your staff and colleagues by facilitating clinician
Teaming Together to Understand Pressure Injuries / (Ulcers): NPUAP Terminology and Staging Clarification We encourage you to share this information with your staff and colleagues by facilitating clinician
2 Pressure Ulcer or Pressure Injury? (Do you have skin in the game?)
") Pressure Ulcer or Pressure Injury? (Do you have skin in the game?) Ann Rambusch, MSN, HCS D, HCS O, RN June 28, 2016 1 Pressure Ulcer or Pressure Injury? (Do you have skin in the game?) Understanding NPUAP
Pressure Ulcer or Pressure Injury? (Do you have skin in the game?) Ann Rambusch, MSN, HCS D, HCS O, RN June 28, 2016 1 Pressure Ulcer or Pressure Injury? (Do you have skin in the game?) Understanding NPUAP
Wound Jeopardy: Name That Wound Session 142 Saturday, September 10 th 2011
 Initial Wound Care Consult History Physical Examination Detailed examination of the wound Photographs Cultures Procedures TCOM ABI Debridement Management Decisions A Detailed History and Physical (wound)
Initial Wound Care Consult History Physical Examination Detailed examination of the wound Photographs Cultures Procedures TCOM ABI Debridement Management Decisions A Detailed History and Physical (wound)
Bed Sores No More! Pressure Injuries Risk Factors and Updated Staging Methodology. Nicolle Samuels, MSPT, CLT-LANA, CWS, CKTP
 Bed Sores No More! Pressure Injuries Risk Factors and Updated Staging Methodology Nicolle Samuels, MSPT, CLT-LANA, CWS, CKTP Objectives Understand updated definitions as well as staging and classification
Bed Sores No More! Pressure Injuries Risk Factors and Updated Staging Methodology Nicolle Samuels, MSPT, CLT-LANA, CWS, CKTP Objectives Understand updated definitions as well as staging and classification
Acute and Chronic WOUND ASSESSMENT. Wound Assessment OBJECTIVES ITEMS TO CONSIDER
 WOUND ASSESSMENT Acute and Chronic OBJECTIVES Discuss classification systems and testing methods for pressure ulcers, venous, arterial and diabetic wounds List at least five items to be assessed and documented
WOUND ASSESSMENT Acute and Chronic OBJECTIVES Discuss classification systems and testing methods for pressure ulcers, venous, arterial and diabetic wounds List at least five items to be assessed and documented
Advanced Clinical Solutions. Pressure Ulcer. Carilex Medical Group 1
 Advanced Clinical Solutions Pressure Ulcer Carilex Medical Group 1 Advanced Clinical Solutions Contents About Pressure Ulcer! 2 Stages of Pressure Ulcer! 5 Reference! 7 Carilex Medical Group 1 About Pressure
Advanced Clinical Solutions Pressure Ulcer Carilex Medical Group 1 Advanced Clinical Solutions Contents About Pressure Ulcer! 2 Stages of Pressure Ulcer! 5 Reference! 7 Carilex Medical Group 1 About Pressure
Diabetic Foot Ulcers. Alex Khan APRN ACNS-BC MSN CWCN CFCN WCN-C. Advanced Practice Nurse / Adult Clinical Nurse Specialist
 Diabetic Foot Ulcers Alex Khan APRN ACNS-BC MSN CWCN CFCN WCN-C Advanced Practice Nurse / Adult Clinical Nurse Specialist Organization of Wound Care Nurses www.woundcarenurses.org Objectives Identify Diabetic/Neuropathic
Diabetic Foot Ulcers Alex Khan APRN ACNS-BC MSN CWCN CFCN WCN-C Advanced Practice Nurse / Adult Clinical Nurse Specialist Organization of Wound Care Nurses www.woundcarenurses.org Objectives Identify Diabetic/Neuropathic
Venous. Arterial. Neuropathic (e.g. diabetic foot ulcer) Describe Wound Types & Stages of. Pressure Ulcers. Identify Phases of Healing & Wound Care
 Describe Wound Types & Stages of. Pressure Ulcers. Identify Phases of Healing & Wound Care") A dressing the situation at hand Describe Wound Types & Stages of Pressure Ulcers Identify Phases of Healing & Wound Care Goals Clarify Referral Protocol Lacerations- The goal is nearest to complete approximation
A dressing the situation at hand Describe Wound Types & Stages of Pressure Ulcers Identify Phases of Healing & Wound Care Goals Clarify Referral Protocol Lacerations- The goal is nearest to complete approximation
Wound Classification. Overview
 Overview Jeffrey A. Niezgoda, MD FACHM, MAPWCA, CHWS Review of Initial Wound Care Consultation Rational for Classification Wound Appearance Wound Etiology Management Algorithms Initial Wound Care Consult
Overview Jeffrey A. Niezgoda, MD FACHM, MAPWCA, CHWS Review of Initial Wound Care Consultation Rational for Classification Wound Appearance Wound Etiology Management Algorithms Initial Wound Care Consult
Pressure Ulcer Staging. Staging of Wounds are based on the deepest level of tissue damage
 Pressure Ulcer Staging Staging of Wounds are based on the deepest level of tissue damage Pressure Ulcer Staging New Pressure Ulcer Staging Stage I Stage II Stage III Stage IV Unstageable Suspected Deep
Pressure Ulcer Staging Staging of Wounds are based on the deepest level of tissue damage Pressure Ulcer Staging New Pressure Ulcer Staging Stage I Stage II Stage III Stage IV Unstageable Suspected Deep
SECTION M: SKIN CONDITIONS. M0210: Unhealed Pressure Ulcer(s) Item Rationale
 Item Rationale") SECTION M: SKIN CONDITIONS Intent: The items in this section of the April 1, 2014 release of the LTCH CARE Data Set Version 2.01 document the presence, appearance, and change of pressure ulcers. If warranted
SECTION M: SKIN CONDITIONS Intent: The items in this section of the April 1, 2014 release of the LTCH CARE Data Set Version 2.01 document the presence, appearance, and change of pressure ulcers. If warranted
Definitions and criteria
 Several disciplines are involved in the management of diabetic foot disease and having a common vocabulary is essential for clear communication. Thus, based on a review of the literature, the IWGDF has
Several disciplines are involved in the management of diabetic foot disease and having a common vocabulary is essential for clear communication. Thus, based on a review of the literature, the IWGDF has
Wound Care Program for Nursing Assistants-
 Wound Care Program for Nursing Assistants- Wound Cleansing,Types & Presentation Elizabeth DeFeo, RN, WCC, OMS, CWOCN Wound, Ostomy, & Continence Specialist ldefeo@cornerstonevna.org Outline/Agenda At completion
Wound Care Program for Nursing Assistants- Wound Cleansing,Types & Presentation Elizabeth DeFeo, RN, WCC, OMS, CWOCN Wound, Ostomy, & Continence Specialist ldefeo@cornerstonevna.org Outline/Agenda At completion
Pressure Ulcer Staging and Documentation. Carolyn Watts MSN, RN, CWON Vanderbilt Medical Center
 Pressure Ulcer Staging and Documentation Carolyn Watts MSN, RN, CWON Vanderbilt Medical Center Overview of the Pressure Ulcer Problem Scope Over 1 million cases each year, 1 in 4 patients Cost In acute
Pressure Ulcer Staging and Documentation Carolyn Watts MSN, RN, CWON Vanderbilt Medical Center Overview of the Pressure Ulcer Problem Scope Over 1 million cases each year, 1 in 4 patients Cost In acute
ULCERS 1/12/ million diabetics in the US (2012) Reamputation Rate 26.7% at 1 year 48.3% at 3 years 60.7% at 5 years
 Reamputation Rate 26.7% at 1 year 48.3% at 3 years 60.7% at 5 years") Jay Christensen D.P.M Advanced Foot and Ankle of Wisconsin 2-4% of the population at any given time will have ulcers 0.06-0.20% of the total population Average age of patients 70 years increased as more
Jay Christensen D.P.M Advanced Foot and Ankle of Wisconsin 2-4% of the population at any given time will have ulcers 0.06-0.20% of the total population Average age of patients 70 years increased as more
Venous Insufficiency Ulcers. Patient Assessment: Superficial varicosities. Evidence of healed ulcers. Dermatitis. Normal ABI.
 Venous Insufficiency Ulcers Patient Assessment: Superficial varicosities Evidence of healed ulcers Dermatitis Normal ABI Edema Eczematous skin changes 1. Scaling 2. Pruritus 3. Erythema 4. Vesicles Lipodermatosclerosis
Venous Insufficiency Ulcers Patient Assessment: Superficial varicosities Evidence of healed ulcers Dermatitis Normal ABI Edema Eczematous skin changes 1. Scaling 2. Pruritus 3. Erythema 4. Vesicles Lipodermatosclerosis
The Importance of Skin Examination. following Spinal Cord Injury
 The Importance of Skin Examination following Spinal Cord Injury An individual who sustains a spinal cord injury (SCI) has a lifetime of increased susceptibility to skin problems, including pressure ulcers
The Importance of Skin Examination following Spinal Cord Injury An individual who sustains a spinal cord injury (SCI) has a lifetime of increased susceptibility to skin problems, including pressure ulcers
Uncovering the Pressure Ulcer Coverup Rhonda Kistler RN MS CWON Wound Care Concepts Gentell
 Uncovering the Pressure Ulcer Coverup Rhonda Kistler RN MS CWON Wound Care Concepts Gentell Objectives Identify the stages of pressure ulcer according to the depth of tissue destruction. Discuss the differences
Uncovering the Pressure Ulcer Coverup Rhonda Kistler RN MS CWON Wound Care Concepts Gentell Objectives Identify the stages of pressure ulcer according to the depth of tissue destruction. Discuss the differences
Wound, Ostomy and Continence Nurses Society s Guidance on OASIS-D Integumentary Items: Best Practice for Clinicians
 Wound, Ostomy and Continence Nurses Society s Guidance on OASIS-D Integumentary Items: Best Practice for Clinicians Table of Contents Table of Contents... 2 Acknowledgments... 3 Introduction... 4 Purpose...
Wound, Ostomy and Continence Nurses Society s Guidance on OASIS-D Integumentary Items: Best Practice for Clinicians Table of Contents Table of Contents... 2 Acknowledgments... 3 Introduction... 4 Purpose...
CURRENT CONCEPTS IN PRESSURE INJURY PREVENTION AND CARE
 CURRENT CONCEPTS IN PRESSURE INJURY PREVENTION AND CARE JOIE WHITNEY, PHD, RN, CWCN, FAAN PROFESSOR BIOBEHAVIORAL NURSING AND HEALTH SYSTEMS UNIVERSITY OF WASHINGTON HARBORVIEW ENDOWED PROFESSOR IN CRITICAL
CURRENT CONCEPTS IN PRESSURE INJURY PREVENTION AND CARE JOIE WHITNEY, PHD, RN, CWCN, FAAN PROFESSOR BIOBEHAVIORAL NURSING AND HEALTH SYSTEMS UNIVERSITY OF WASHINGTON HARBORVIEW ENDOWED PROFESSOR IN CRITICAL
Team-Centered Wound Care: Making Your Wound Care Safe and Simple Again
 Team-Centered Wound Care: Making Your Wound Care Safe and Simple Again October 4 th, 2017 Ryan P. Dirks PA-C Founder and CEO Road to success Detailed Wound Assessment/Risk Assessment External Support Individualized
Team-Centered Wound Care: Making Your Wound Care Safe and Simple Again October 4 th, 2017 Ryan P. Dirks PA-C Founder and CEO Road to success Detailed Wound Assessment/Risk Assessment External Support Individualized
Hemostasis Inflammatory Phase Proliferative/rebuilding Phase Maturation Phase
 The presenters are staff members of the CHI Health St. Elizabeth Burn and Wound Center. Many of the products discussed are used in our current practice but we have no conflict of interest to disclose.
The presenters are staff members of the CHI Health St. Elizabeth Burn and Wound Center. Many of the products discussed are used in our current practice but we have no conflict of interest to disclose.
Wound Management. E. Foy White-Chu, MD, CWSP
 Wound Management E. Foy White-Chu, MD, CWSP E. Foy White-Chu, MD, CWSP Assistant Professor, OHSU Wound Medical Director, VAPORHCS List the Four Principles of Wound Bed Preparation Determine safe debridement
Wound Management E. Foy White-Chu, MD, CWSP E. Foy White-Chu, MD, CWSP Assistant Professor, OHSU Wound Medical Director, VAPORHCS List the Four Principles of Wound Bed Preparation Determine safe debridement
WOUND MANAGEMENT. A Clinical Perspective. Furqan Alex Khan, APRN ACNS-BC MSN
 WOUND MANAGEMENT A Clinical Perspective Furqan Alex Khan, APRN ACNS-BC MSN alexkhan@prohealthcare.us Ket Harris Davis, APRN FNP-C DNP keturahnp@keturah-hms.com. Objectives Understand types of wounds Discuss
WOUND MANAGEMENT A Clinical Perspective Furqan Alex Khan, APRN ACNS-BC MSN alexkhan@prohealthcare.us Ket Harris Davis, APRN FNP-C DNP keturahnp@keturah-hms.com. Objectives Understand types of wounds Discuss
Address: Left Leg. other: Nails: thick yellow brittle fungus abnormal thick yellow brittle fungus abnormal
 South West Regional Wound Care Toolkit: Interdisciplinary Lower Leg Assessment Form Instructions for use: Competent/ Proficient/ Expert level HCP to complete if lower leg ulcer present or risk of ulcer
South West Regional Wound Care Toolkit: Interdisciplinary Lower Leg Assessment Form Instructions for use: Competent/ Proficient/ Expert level HCP to complete if lower leg ulcer present or risk of ulcer
If both a standardized, validated screening tool and an evaluation of clinical factors are utilized, select Response 2.
 (M1300) Pressure Ulcer Assessment: Was this patient assessed for Risk of Developing Pressure Ulcers? 0 - No assessment conducted [Go to M1306 ] 1 - Yes, based on an evaluation of clinical factors (for
(M1300) Pressure Ulcer Assessment: Was this patient assessed for Risk of Developing Pressure Ulcers? 0 - No assessment conducted [Go to M1306 ] 1 - Yes, based on an evaluation of clinical factors (for
Critically Assessing Pressure Injuries
 Critically Assessing Injuries Copyright 2016 Gordian Medical, Inc. dba American Medical Technologies. LeadingAge Indiana presents FACULTY PAMELA SCARBOROUGH PT, DPT, CDE, CWS DIRECTOR OF PUBLIC POLICY
Critically Assessing Injuries Copyright 2016 Gordian Medical, Inc. dba American Medical Technologies. LeadingAge Indiana presents FACULTY PAMELA SCARBOROUGH PT, DPT, CDE, CWS DIRECTOR OF PUBLIC POLICY
Pressure Ulcers ecourse
 Pressure Ulcers ecourse Knowledge Checkup Module 2 Handout College of Licensed Practical Nurses of Alberta (Canada) CLPNA.com and StudywithCLPNA.com CLPNA Pressure Ulcers ecourse Knowledge Checkup Module
Pressure Ulcers ecourse Knowledge Checkup Module 2 Handout College of Licensed Practical Nurses of Alberta (Canada) CLPNA.com and StudywithCLPNA.com CLPNA Pressure Ulcers ecourse Knowledge Checkup Module
C A R O L S I E M M S N, R N, B C, G N P M U S I N C L A I R S C H O O L O F N U R S I N G Q I P M O WHAT S IN A NAME?
 M D S A N D P R E S S U R E U L C E R S C A R O L S I E M M S N, R N, B C, G N P M U S I N C L A I R S C H O O L O F N U R S I N G Q I P M O WHAT S IN A NAME? 1777: decubitus is the oldest term used 1942
M D S A N D P R E S S U R E U L C E R S C A R O L S I E M M S N, R N, B C, G N P M U S I N C L A I R S C H O O L O F N U R S I N G Q I P M O WHAT S IN A NAME? 1777: decubitus is the oldest term used 1942
Negative Pressure Wound Therapy
 Origination: 6/29/04 Revised: 8/24/16 Annual Review: 11/10/16 Purpose: To provide Negative Pressure Wound Therapy (wound care treatment) guidelines for the Medical Department staff to reference when making
Origination: 6/29/04 Revised: 8/24/16 Annual Review: 11/10/16 Purpose: To provide Negative Pressure Wound Therapy (wound care treatment) guidelines for the Medical Department staff to reference when making
Objectives. Major Changes to Section M. MDS 3.0 Section M Pressure Ulcers. Risk assessment Introduction of NPUAP guidelines
 MDS 3.0 Section M Pressure Ulcers Moderator: Barbara Baylis Sr. VP of Clinical and Residential Services, Kindred Healthcare Presenter: Glenda Mack, Sr. Director of Clinical Operations, Peoplefirst Rehabilitation
MDS 3.0 Section M Pressure Ulcers Moderator: Barbara Baylis Sr. VP of Clinical and Residential Services, Kindred Healthcare Presenter: Glenda Mack, Sr. Director of Clinical Operations, Peoplefirst Rehabilitation
Successful Wound Management Strategies : An Introduction. Alex Khan, APRN ACNS-BC. Organization of Wound Care Nurses
 Successful Wound Management Strategies : An Introduction Alex Khan, APRN ACNS-BC Organization of Wound Care Nurses www.woundcarenurses.org Goals & Objectives The role and importance of wound care management
Successful Wound Management Strategies : An Introduction Alex Khan, APRN ACNS-BC Organization of Wound Care Nurses www.woundcarenurses.org Goals & Objectives The role and importance of wound care management
Skin Integrity and Wound Care
 Skin Integrity and Wound Care By Dr. Amer Hasanien & Dr. Ali Saleh Skin Integrity and Wound Care Skin integrity: the presence of normal Skin & Uninterrupted skin layers by wounds. Factors affecting appearance
Skin Integrity and Wound Care By Dr. Amer Hasanien & Dr. Ali Saleh Skin Integrity and Wound Care Skin integrity: the presence of normal Skin & Uninterrupted skin layers by wounds. Factors affecting appearance
Frequently Asked Questions about Pressure Injury Staging. February 20, 2018, 1 to 2 pm ET
 Frequently Asked Questions about Pressure February 20, 2018, 1 to 2 pm ET Scott Bolhack, MD, MBA, CMD, CWSP, FACP, FAAP Janet Cuddigan. PhD, RN, CWCN, FAAN Joyce A. Pittman, PhD, ANP-BC, FNP-BC, CWOCN
Frequently Asked Questions about Pressure February 20, 2018, 1 to 2 pm ET Scott Bolhack, MD, MBA, CMD, CWSP, FACP, FAAP Janet Cuddigan. PhD, RN, CWCN, FAAN Joyce A. Pittman, PhD, ANP-BC, FNP-BC, CWOCN
Consider the possibility of pressure ulcer development
 Douglas Fronzaglia II, DO, MS LECOM Institute for Successful Aging LECOM Institute for Advanced Wound Care and Hyperbaric Medicine Consider the possibility of pressure ulcer development 1 Identify ulcer
Douglas Fronzaglia II, DO, MS LECOM Institute for Successful Aging LECOM Institute for Advanced Wound Care and Hyperbaric Medicine Consider the possibility of pressure ulcer development 1 Identify ulcer
Person s Name: ID Number: Date:
 South West Regional Wound Care Program Person s Name: ID Number: Interdisciplinary Diabetic/Neuropathic Foot Assessment Form MEDICAL HISTORY: Question Year diabetes diagnosed: Characteristics of onset
South West Regional Wound Care Program Person s Name: ID Number: Interdisciplinary Diabetic/Neuropathic Foot Assessment Form MEDICAL HISTORY: Question Year diabetes diagnosed: Characteristics of onset
WHY WOUNDS FAIL TO HEAL SIMPLIFIED
 WHY WOUNDS FAIL TO HEAL SIMPLIFIED 10 Some of the common signs of failure to heal with possible causes and some interventions WHY WOUNDS FAIL TO HEAL There must be adequate supplies of nutrients and oxygen
WHY WOUNDS FAIL TO HEAL SIMPLIFIED 10 Some of the common signs of failure to heal with possible causes and some interventions WHY WOUNDS FAIL TO HEAL There must be adequate supplies of nutrients and oxygen
(Words Pressure Wound Video Series and Part II appear on screen with the SCIRE logo at the top right corner.)
") (Words Pressure Wound Video Series and Part II appear on screen with the SCIRE logo at the top right corner.) (Fades to next slide titled Pressure Ulcer Staging. *Video contains Graphic Imagery is noted
(Words Pressure Wound Video Series and Part II appear on screen with the SCIRE logo at the top right corner.) (Fades to next slide titled Pressure Ulcer Staging. *Video contains Graphic Imagery is noted
Wound Care Assessment in the Home Care Setting
 Wound Care Assessment in the Home Care Setting Lynn Peterson, RN, BSN, CWOCN Technical Service Specialist 3M Health Care Wednesday, May 14, 2008 Objectives Describe essential elements of a wound assessment
Wound Care Assessment in the Home Care Setting Lynn Peterson, RN, BSN, CWOCN Technical Service Specialist 3M Health Care Wednesday, May 14, 2008 Objectives Describe essential elements of a wound assessment
Pressure Ulcer. Patient information leaflet. Category I. Category II. Category III. Category IV. Unstageable. Deep Tissue Injury
 Pressure Ulcers Patient information leaflet Pressure Ulcer Category I Category II Category III Category IV Unstageable Deep Tissue Injury Introduction This leaflet is about pressure ulcers and includes
Pressure Ulcers Patient information leaflet Pressure Ulcer Category I Category II Category III Category IV Unstageable Deep Tissue Injury Introduction This leaflet is about pressure ulcers and includes
Bacterial Burden (Bioburden) The metabolic load imposed by bacteria in tissue.
 The metabolic load imposed by bacteria in tissue.") Glossary Ankle Brachial Index (ABI) Is a numerical figure which indicates a quantifiable pressure index. The pressure index is determined by means of Doppler Ultra Sound. The ABI is obtained by dividing
Glossary Ankle Brachial Index (ABI) Is a numerical figure which indicates a quantifiable pressure index. The pressure index is determined by means of Doppler Ultra Sound. The ABI is obtained by dividing
Wound Care per HHVNA Wound Product Formulary
 Venous Ulcers ABI of 0.9-1.2 = normal blood flow An ABI MUST be obtained prior to inititiation of compression therapy. Compression is the Gold Standard of care to promote wound of venous ulcers. Elevation
Venous Ulcers ABI of 0.9-1.2 = normal blood flow An ABI MUST be obtained prior to inititiation of compression therapy. Compression is the Gold Standard of care to promote wound of venous ulcers. Elevation
Diabetic Foot Ulcer Treatment and Prevention
 Diabetic Foot Ulcer Treatment and Prevention Alexander Reyzelman DPM, FACFAS Associate Professor California School of Podiatric Medicine at Samuel Merritt University Diabetic Foot Ulcers One of the most
Diabetic Foot Ulcer Treatment and Prevention Alexander Reyzelman DPM, FACFAS Associate Professor California School of Podiatric Medicine at Samuel Merritt University Diabetic Foot Ulcers One of the most
Assisted Living Resident Assessment (To be used when yes is indicated for skin issues under Section 5 of Assisted Living Resident Assessment)
") Skin Assessment Current open skin areas: Yes No Current pressure ulcer: Yes No A. Stage 1 Ulcers Report based on highest stage of existing ulcers at its worst; do not reverse stage. Number of existing
Skin Assessment Current open skin areas: Yes No Current pressure ulcer: Yes No A. Stage 1 Ulcers Report based on highest stage of existing ulcers at its worst; do not reverse stage. Number of existing
Venous Leg Ulcers. Care for Patients in All Settings
 Venous Leg Ulcers Care for Patients in All Settings Summary This quality standard focuses on care for people who have developed or are at risk of developing a venous leg ulcer. The scope of the standard
Venous Leg Ulcers Care for Patients in All Settings Summary This quality standard focuses on care for people who have developed or are at risk of developing a venous leg ulcer. The scope of the standard
CRRN Review Course 2017 Skin and Wound Management. Presented by: Jenifer Stevenson BSN, CRRN, CNML
 CRRN Review Course 2017 Skin and Wound Management Presented by: Jenifer Stevenson BSN, CRRN, CNML Disclosure The presenter for this presentation has disclosed no conflict of interest related to this topic.
CRRN Review Course 2017 Skin and Wound Management Presented by: Jenifer Stevenson BSN, CRRN, CNML Disclosure The presenter for this presentation has disclosed no conflict of interest related to this topic.
Leg ulcer assessment and management
 Leg ulceration The views expressed in this presentation are solely those of the presenter and do not necessarily represent the views of Smith & Nephew. Smith & Nephew does not guarantee the accuracy or
Leg ulceration The views expressed in this presentation are solely those of the presenter and do not necessarily represent the views of Smith & Nephew. Smith & Nephew does not guarantee the accuracy or
Wound Care Evaluation by Kris Dalseg MS PT CWS CLT
 Wound Care Evaluation by Kris Dalseg MS PT CWS CLT This document is intended to describe a standard wound care evaluation for healthcare practitioners. In healthcare, all aspects of our treatment have
Wound Care Evaluation by Kris Dalseg MS PT CWS CLT This document is intended to describe a standard wound care evaluation for healthcare practitioners. In healthcare, all aspects of our treatment have
Diabetic Foot Ulcers. Care for Patients in All Settings
 Diabetic Foot Ulcers Care for Patients in All Settings Summary This quality standard focuses on care for people who have developed or are at risk of developing a diabetic foot ulcer. The scope of the standard
Diabetic Foot Ulcers Care for Patients in All Settings Summary This quality standard focuses on care for people who have developed or are at risk of developing a diabetic foot ulcer. The scope of the standard
Determining Wound Diagnosis and Documentation Tips Job Aid
 Determining Wound Diagnosis and Job Aid 1 Coding Is this a traumatic injury from an accident? 800 Codes - Injury Section of the Coding Manual Code by specific site of injury. Only use for accidents or
Determining Wound Diagnosis and Job Aid 1 Coding Is this a traumatic injury from an accident? 800 Codes - Injury Section of the Coding Manual Code by specific site of injury. Only use for accidents or
SAMPLE. Home Health Reference Tool For Nurses
 Home Health Reference Tool For Nurses Foundation Management Services, Inc. 2010. All rights reserved. Unauthorized reproduction is strictly prohibited. (10/09) Table of Contents 2 Page Medicare Eligibility
Home Health Reference Tool For Nurses Foundation Management Services, Inc. 2010. All rights reserved. Unauthorized reproduction is strictly prohibited. (10/09) Table of Contents 2 Page Medicare Eligibility
o Venous edema o Stasis ulcers o Varicose veins (not including spider veins) o Lipodermatosclerosis
 o Lipodermatosclerosis") Wound Care Equipment and Supply Benefits to Change for Texas Medicaid July 1, 2018 Effective for dates of service on or after July 1, 2018, wound care equipment and supply benefits will change for Texas
Wound Care Equipment and Supply Benefits to Change for Texas Medicaid July 1, 2018 Effective for dates of service on or after July 1, 2018, wound care equipment and supply benefits will change for Texas
Appropriate Dressing Selection For Treating Wounds
 Appropriate Dressing Selection For Treating Wounds Criteria to Consider for an IDEAL DRESSING Exudate Management Be able to provide for moist wound healing by absorbing exudate or adding moisture Secure
Appropriate Dressing Selection For Treating Wounds Criteria to Consider for an IDEAL DRESSING Exudate Management Be able to provide for moist wound healing by absorbing exudate or adding moisture Secure
Pressure Injury Complications: Diagnostic Dilemmas
 Pressure Injury Complications: Diagnostic Dilemmas Aimée D. Garcia, MD, CWS, FACCWS Associate Professor, Department of Medicine, Geriatrics Section Baylor College of Medicine Medical Director, Wound Clinic
Pressure Injury Complications: Diagnostic Dilemmas Aimée D. Garcia, MD, CWS, FACCWS Associate Professor, Department of Medicine, Geriatrics Section Baylor College of Medicine Medical Director, Wound Clinic
Your guide to wound debridement and assessment. Michelle Greenwood. Lorraine Grothier. Lead Nurse, Tissue Viability, Walsall Healthcare NHS Trust
 Your guide to wound debridement and assessment Michelle Greenwood Lead Nurse, Tissue Viability, Walsall Healthcare NHS Trust Lorraine Grothier Clinical Nurse Specialist, Tissue Viability, Central Essex
Your guide to wound debridement and assessment Michelle Greenwood Lead Nurse, Tissue Viability, Walsall Healthcare NHS Trust Lorraine Grothier Clinical Nurse Specialist, Tissue Viability, Central Essex
VASCULAR WOUNDS PATHOPHYSIOLOGY AND MANAGEMENT
 VASCULAR WOUNDS PATHOPHYSIOLOGY AND MANAGEMENT Lucy Stopher, A/CNS Vascular Surgery ...it is best to think of a wound not as a disease, but rather as a manifestation of disease. Joe McCulloch In order
VASCULAR WOUNDS PATHOPHYSIOLOGY AND MANAGEMENT Lucy Stopher, A/CNS Vascular Surgery ...it is best to think of a wound not as a disease, but rather as a manifestation of disease. Joe McCulloch In order
Arterial & Venous Ulcers. A Comprehensive Review Assessment & Management
 Arterial & Venous Ulcers A Comprehensive Review Assessment & Management 1 Objectives Understand Arterial & Venous disease Understand the etiology of lower extremities ulcers Understand assessment of lower
Arterial & Venous Ulcers A Comprehensive Review Assessment & Management 1 Objectives Understand Arterial & Venous disease Understand the etiology of lower extremities ulcers Understand assessment of lower
Case 1. July 14, th week wound gel 3 cm x 2.5 cm = 7.5 cm². May 25, st wound gel on 290 days PI treatment 4 cm x 2.4 cm = 9.
 2.5% Sodium Hyaluronate Wound Gel Study Cases Case 1 Patient with Lower Leg Ulcer Not Responding to Compression This patient was a 50-year old male patient with nonhealing right lower leg since January
2.5% Sodium Hyaluronate Wound Gel Study Cases Case 1 Patient with Lower Leg Ulcer Not Responding to Compression This patient was a 50-year old male patient with nonhealing right lower leg since January
PRESSURE ULCERS SIMPLIFIED
 10 PRESSURE ULCERS SIMPLIFIED This leaflet is intended to give you information and answers to some question you may have around pressure ulcers PRESSURE ULCERS SIMPLIFIED Pressure ulcer development has
10 PRESSURE ULCERS SIMPLIFIED This leaflet is intended to give you information and answers to some question you may have around pressure ulcers PRESSURE ULCERS SIMPLIFIED Pressure ulcer development has
Topical Oxygen Wound Therapy (MEDICAID)
") Topical Oxygen Wound Therapy (MEDICAID) Last Review Date: September 8, 2017 Number: MG.MM.DM.15C8v2 Medical Guideline Disclaimer Property of EmblemHealth. All rights reserved. The treating physician or
Topical Oxygen Wound Therapy (MEDICAID) Last Review Date: September 8, 2017 Number: MG.MM.DM.15C8v2 Medical Guideline Disclaimer Property of EmblemHealth. All rights reserved. The treating physician or
Lower Extremity Wound Evaluation and Treatment
 Lower Extremity Wound Evaluation and Treatment Boni-Jo Silbernagel, DPM Describe effective lower extremity wound evaluation and treatment. Discuss changes in theories of treatment in wound care and implications
Lower Extremity Wound Evaluation and Treatment Boni-Jo Silbernagel, DPM Describe effective lower extremity wound evaluation and treatment. Discuss changes in theories of treatment in wound care and implications
Will it heal? How to assess the probability of wound healing
 Will it heal? How to assess the probability of wound healing Richard F. Neville, M.D. Professor of Surgery Chief, Division of Vascular Surgery George Washington University Limb center case 69 yr old male
Will it heal? How to assess the probability of wound healing Richard F. Neville, M.D. Professor of Surgery Chief, Division of Vascular Surgery George Washington University Limb center case 69 yr old male
Ann Leland, APRN, CNP, DNP Instructor, college of surgery
 Ann Leland, APRN, CNP, DNP Instructor, college of surgery leland.ann@mayo.edu 2015 MFMER 3543652-1 Pressure ulcers Mayo School of Continuous Professional Development 2nd Annual Inpatient Medicine for NPs
Ann Leland, APRN, CNP, DNP Instructor, college of surgery leland.ann@mayo.edu 2015 MFMER 3543652-1 Pressure ulcers Mayo School of Continuous Professional Development 2nd Annual Inpatient Medicine for NPs
Surgical Wounds & Incisions
 Surgical Wounds & Incisions A Comprehensive Review Assessment & Management Alex Khan APRN ACNS-BC MSN CWCN CFCN WCN-C Advanced Practice Nurse / Adult Clinical Nurse Specialist www.woundcarenurses.org 1
Surgical Wounds & Incisions A Comprehensive Review Assessment & Management Alex Khan APRN ACNS-BC MSN CWCN CFCN WCN-C Advanced Practice Nurse / Adult Clinical Nurse Specialist www.woundcarenurses.org 1
VASCULAR DISEASE: THREE THINGS YOU SHOULD KNOW JAMES A.M. SMITH, D.O. KANSAS VASCULAR MEDICINE, P.A. WICHITA, KANSAS
 VASCULAR DISEASE: THREE THINGS YOU SHOULD KNOW JAMES A.M. SMITH, D.O. KANSAS VASCULAR MEDICINE, P.A. WICHITA, KANSAS KANSAS ASSOCIATION OF OSTEOPATHIC MEDICINE ANNUAL CME CONVENTION APRIL 13, 2018 THREE
VASCULAR DISEASE: THREE THINGS YOU SHOULD KNOW JAMES A.M. SMITH, D.O. KANSAS VASCULAR MEDICINE, P.A. WICHITA, KANSAS KANSAS ASSOCIATION OF OSTEOPATHIC MEDICINE ANNUAL CME CONVENTION APRIL 13, 2018 THREE
Spinal Cord Injury Info Sheet An information series produced by the Spinal Cord Program at GF Strong Rehab Centre.
 Spinal Cord Injury Info Sheet An information series produced by the Spinal Cord Program at GF Strong Rehab Centre. What does skin do? 1. It protects you. 2. It provides sensory information. 3. It helps
Spinal Cord Injury Info Sheet An information series produced by the Spinal Cord Program at GF Strong Rehab Centre. What does skin do? 1. It protects you. 2. It provides sensory information. 3. It helps
Coding and Documenting Pressure Injuries and Chronic Ulcers. September 21, 2016
 Coding and Documenting Pressure Injuries and Chronic Ulcers Laurie M. Johnson, MS, RHIA, FAHIMA AHIMA Approved ICD-10-CM/PCS Trainer Director of HIM Consulting Services Panacea Healthcare Solutions, Sandy
Coding and Documenting Pressure Injuries and Chronic Ulcers Laurie M. Johnson, MS, RHIA, FAHIMA AHIMA Approved ICD-10-CM/PCS Trainer Director of HIM Consulting Services Panacea Healthcare Solutions, Sandy
Wound, Ostomy and Continence Nursing Certification Board (WOCNCB) Certified Foot Care Nurse (CFCN) Detailed Content Outline
 Certified Foot Care Nurse (CFCN) Detailed Content Outline") Wound, Ostomy and Continence Nursing Certification Board (WOCNCB) Certified Foot Care Nurse (CFCN) Detailed Content Outline Description Domain I: Assessment and Care Planning 010000 40 Task 1: Obtain focused
Wound, Ostomy and Continence Nursing Certification Board (WOCNCB) Certified Foot Care Nurse (CFCN) Detailed Content Outline Description Domain I: Assessment and Care Planning 010000 40 Task 1: Obtain focused
E-learning module: Stages of pressure injuries. Disclaimer
 E-learning module: Stages of pressure injuries 1 Disclaimer Classification of pressure injuries The International Pressure Injury Category System (2009) was developed by:! the National Pressure Ulcer Advisory
E-learning module: Stages of pressure injuries 1 Disclaimer Classification of pressure injuries The International Pressure Injury Category System (2009) was developed by:! the National Pressure Ulcer Advisory
Topical antimicrobials (antiseptics) Iodine, Silver, Honey
 Iodine, Silver, Honey") Topical antimicrobials (antiseptics) Iodine, Silver, Honey Iodine Honey Silver Enzymatic debridement Proteolytic enzyme, also called Proteinase Proteinase breaks the long chainlike molecules of proteins
Topical antimicrobials (antiseptics) Iodine, Silver, Honey Iodine Honey Silver Enzymatic debridement Proteolytic enzyme, also called Proteinase Proteinase breaks the long chainlike molecules of proteins
PRESSURE ULCER INJURY
 PRESSURE ULCER INJURY Background Epidemiology Cost Definition Classification Etiology Risk assessment Skin assessment on admission Prevention Wound healing assessment Management and treatment BACKGROUND
PRESSURE ULCER INJURY Background Epidemiology Cost Definition Classification Etiology Risk assessment Skin assessment on admission Prevention Wound healing assessment Management and treatment BACKGROUND
ד"ר בוריס פונצ' קי PRESSURE ULCERS
 ד"ר בוריס פונצ' קי 25.12.2013 PRESSURE ULCERS International EPUAP-NPUAP Pressure Ulcer Definition: (European Pressure Ulcer Advisory Panel and National Pressure Ulcer Advisory Panel, 2010).. is localized
ד"ר בוריס פונצ' קי 25.12.2013 PRESSURE ULCERS International EPUAP-NPUAP Pressure Ulcer Definition: (European Pressure Ulcer Advisory Panel and National Pressure Ulcer Advisory Panel, 2010).. is localized
Debbie Theriot, MN, APRN, CWCN Ochsner Health Systems New Orleans, LA
 Debbie Theriot, MN, APRN, CWCN Ochsner Health Systems New Orleans, LA Full patient history Initiating event and wound duration Previous treatments and their outcomes Diabetes control and prior complications
Debbie Theriot, MN, APRN, CWCN Ochsner Health Systems New Orleans, LA Full patient history Initiating event and wound duration Previous treatments and their outcomes Diabetes control and prior complications
Diabetic/Neuropathic Foot Ulcer Assessment Guide South West Regional Wound Care Program Last Updated April 7,
 Developed in collaboration with the Wound Care Champions, Wound Care Specialists, Enterostomal Nurses, and South West Regional Wound Care Program (SWRWCP) members from Long Term Care Homes, Hospitals,
Developed in collaboration with the Wound Care Champions, Wound Care Specialists, Enterostomal Nurses, and South West Regional Wound Care Program (SWRWCP) members from Long Term Care Homes, Hospitals,
The Risk. Background / Bias. Integrating Wound Care into a Limb Preservation Initiative 4/24/2009
 Stimulating Wound Granulation: Advances in NPWT and other Measures (Wound Bed Preparation) Charles Andersen MD, FACS, FAPWCA Clinical Prof of Surgery UW, USUHS Chief Vascular/Endovascular/ Limb Preservation
Stimulating Wound Granulation: Advances in NPWT and other Measures (Wound Bed Preparation) Charles Andersen MD, FACS, FAPWCA Clinical Prof of Surgery UW, USUHS Chief Vascular/Endovascular/ Limb Preservation
DEBRIDEMENT. Professor Donald G. MacLellan Executive Director Health Education & Management Innovations
 DEBRIDEMENT Professor Donald G. MacLellan Executive Director Health Education & Management Innovations DEBRIDEMENT Principles - CSD Methods of Debridement Biopsy options PRINCIPLES OF WOUND MANAGEMENT
DEBRIDEMENT Professor Donald G. MacLellan Executive Director Health Education & Management Innovations DEBRIDEMENT Principles - CSD Methods of Debridement Biopsy options PRINCIPLES OF WOUND MANAGEMENT
Oregon Health Care Association Presents. F686: Updates on Regulations for Pressure Ulcer/Injury Prevention and Care
 Oregon Health Care Association Presents F686: Updates on Regulations for Pressure Ulcer/Injury Prevention and Care FACULTY: PAMELA SCARBOROUGH PT, DPT, MS, CWS, CEEAA DIRECTOR OF PUBLIC POLICY & EDUCATION
Oregon Health Care Association Presents F686: Updates on Regulations for Pressure Ulcer/Injury Prevention and Care FACULTY: PAMELA SCARBOROUGH PT, DPT, MS, CWS, CEEAA DIRECTOR OF PUBLIC POLICY & EDUCATION
Wound Healing Basic Concept
 Department of Orthopaedic & Traumatology The Chinese University of Hong Kong Wound Healing Basic Concept Dr TSE Lung Fung ( 謝龍峰醫生 ) MBChB(CUHK),FRCS(Edin),FRCSEd(Orth),FHKCOS,FHKAM(Ortho) Tissue Damage
Department of Orthopaedic & Traumatology The Chinese University of Hong Kong Wound Healing Basic Concept Dr TSE Lung Fung ( 謝龍峰醫生 ) MBChB(CUHK),FRCS(Edin),FRCSEd(Orth),FHKCOS,FHKAM(Ortho) Tissue Damage
RN Cathy Hammond. Specialist Wound Management Service at Nurse Maude Christchurch
 RN Cathy Hammond Specialist Wound Management Service at Nurse Maude Christchurch 14:00-14:55 WS #141: Wound Infection - What You Need to Know 15:05-16:00 WS #153: Wound Infection - What You Need to Know
RN Cathy Hammond Specialist Wound Management Service at Nurse Maude Christchurch 14:00-14:55 WS #141: Wound Infection - What You Need to Know 15:05-16:00 WS #153: Wound Infection - What You Need to Know
Hyperbarics in Diabetic Wound Care. Aurel Mihai, MD & Brian Kline, MD
 Hyperbarics in Diabetic Wound Care Aurel Mihai, MD & Brian Kline, MD Presentation Outline The Scope of the Problem Important Definitions Standard Wound Care Hyperbaric Oxygen as an Adjunct Diabetic Foot
Hyperbarics in Diabetic Wound Care Aurel Mihai, MD & Brian Kline, MD Presentation Outline The Scope of the Problem Important Definitions Standard Wound Care Hyperbaric Oxygen as an Adjunct Diabetic Foot
OASIS NP August 2011: Special Training. OASIS-C Integument Assessment. Rhonda Will, RN, BS, COS-C, HCS-D Assistant Director OASIS Competency Institute
 OASIS NP August 211: Special Training OASIS-C Integument Assessment Rhonda Will, RN, BS, COS-C, HCS-D Assistant Director OASIS Competency Institute 243 King Street, Suite 246 Northampton, MA 16 413-584-53
OASIS NP August 211: Special Training OASIS-C Integument Assessment Rhonda Will, RN, BS, COS-C, HCS-D Assistant Director OASIS Competency Institute 243 King Street, Suite 246 Northampton, MA 16 413-584-53
Advanced Wound Care. Cut Shape Innovate
 Advanced Wound Care Cut Shape Innovate Vacutex incorporates a patented three layer construction of poly-cotton elements that promotes an accelerated capillary action on wound interfaces. Effectively lifting,
Advanced Wound Care Cut Shape Innovate Vacutex incorporates a patented three layer construction of poly-cotton elements that promotes an accelerated capillary action on wound interfaces. Effectively lifting,
Part 4: OASIS C2 Accuracy
 Part 4: OASIS C2 Accuracy Presented by: Sharon Molinari, RN, HCS D, HCS O For: HealthCare Synergy 1 M2020/M2030 General Rules o If a patient does not have the requisite knowledge of a drug s dose and administration
Part 4: OASIS C2 Accuracy Presented by: Sharon Molinari, RN, HCS D, HCS O For: HealthCare Synergy 1 M2020/M2030 General Rules o If a patient does not have the requisite knowledge of a drug s dose and administration
How Wounds Heal: A Guide for the Wound-care Novice
 C L I N I C A L P R A C T I C E How Wounds Heal: A Guide for the Wound-care Novice BY Christine Pearson Christine Pearson, RN, IIWCC, is a wound clinician for Vancouver Coastal Health and has worked in
C L I N I C A L P R A C T I C E How Wounds Heal: A Guide for the Wound-care Novice BY Christine Pearson Christine Pearson, RN, IIWCC, is a wound clinician for Vancouver Coastal Health and has worked in
Durable Medical Equipment Providers
 August 2009 Provider Bulletin Number 974 Durable Medical Equipment Providers Vacuum Assisted Wound Closure Therapy Negative pressure wound therapy (NPWT) must be requested and supplied by an enrolled durable
August 2009 Provider Bulletin Number 974 Durable Medical Equipment Providers Vacuum Assisted Wound Closure Therapy Negative pressure wound therapy (NPWT) must be requested and supplied by an enrolled durable
Introduction. Epidemiology Pathophysiology Classification Treatment
 Diabetic Foot Introduction Epidemiology Pathophysiology Classification Treatment Epidemiology DM largest cause of neuropathy in N.A. 1 million DM patients in Canada Half don t know Foot ulcerations is
Diabetic Foot Introduction Epidemiology Pathophysiology Classification Treatment Epidemiology DM largest cause of neuropathy in N.A. 1 million DM patients in Canada Half don t know Foot ulcerations is
Regenerative Tissue Matrix in Treatment of Wounds
 Regenerative Tissue Matrix in Treatment of Wounds Learning Objectives Differentiate between reparative and regenerative healing Review surgical techniques for applying a regenerative tissue scaffold to
Regenerative Tissue Matrix in Treatment of Wounds Learning Objectives Differentiate between reparative and regenerative healing Review surgical techniques for applying a regenerative tissue scaffold to
Disclosures for Tarik Alam. Wound Bed Preparation. Wound Prognosis. Session Objectives. Debridement 4/26/2015
 Disclosures for Tarik Alam Challenges in Managing Bioburden and Devitalized Tissue Tarik Alam RN, BScN, ET, MClSc(WH) Enterostomal Therapy Nurse tarikalam@hotmail.com Clinical Affairs Manager for Hollister
Disclosures for Tarik Alam Challenges in Managing Bioburden and Devitalized Tissue Tarik Alam RN, BScN, ET, MClSc(WH) Enterostomal Therapy Nurse tarikalam@hotmail.com Clinical Affairs Manager for Hollister
SKIN INTEGRITY & WOUND CARE
 SKIN INTEGRITY & WOUND CARE Chapter 34 1 skin integrity: intact skin refers to the presence of normal skin layer uninterrupted by wound 2 WOUNDS DISRUPTION IN THE INTEGRITY OF BODY TISSUE CLASSIFIED AS:
SKIN INTEGRITY & WOUND CARE Chapter 34 1 skin integrity: intact skin refers to the presence of normal skin layer uninterrupted by wound 2 WOUNDS DISRUPTION IN THE INTEGRITY OF BODY TISSUE CLASSIFIED AS:
10/29/2018. Objectives. Why Are Pressure Injuries Important?
 Pressure Injuries Genevieve Tatco-Villamayor, APRN, MSN, FNP-C, CWON, PHN 1 Copyright 2017 Kaiser Foundation Health Plan, Inc. Objectives 1. Pressure Injuries (PI s) why are they important 2. Identify
Pressure Injuries Genevieve Tatco-Villamayor, APRN, MSN, FNP-C, CWON, PHN 1 Copyright 2017 Kaiser Foundation Health Plan, Inc. Objectives 1. Pressure Injuries (PI s) why are they important 2. Identify
Lower Extremity Venous Disease (LEVD)
") Lower Extremity Venous Disease (LEVD) Lower Extremity Venous Disease (LEVD) Wounds Etiology Lower extremity venous leg ulcers are caused by chronic venous hypertension. Failure of valves in the veins or
Lower Extremity Venous Disease (LEVD) Lower Extremity Venous Disease (LEVD) Wounds Etiology Lower extremity venous leg ulcers are caused by chronic venous hypertension. Failure of valves in the veins or
The Triangle of Wound Assessment
 The Triangle of Wound Assessment A simple and holistic framework for wound management CPWSC_TOWA_Brochure_210x210_2018.indd 1 10/01/2018 15.13 ? We asked healthcare professionals around the world about
The Triangle of Wound Assessment A simple and holistic framework for wound management CPWSC_TOWA_Brochure_210x210_2018.indd 1 10/01/2018 15.13 ? We asked healthcare professionals around the world about
Slide 1. Slide 2 Disclosures. Slide 3 Objectives. Karen Rogge Miller, RN, BS, WCC Wound and Ostomy Clinician
 Slide 1 Karen Rogge Miller, RN, BS, WCC Wound and Ostomy Clinician Slide 2 Disclosures Wound and Ostomy RN at St. Vincent Healthcare and Billings Clinic, Billings, MT Former employee of KCI, a division
Slide 1 Karen Rogge Miller, RN, BS, WCC Wound and Ostomy Clinician Slide 2 Disclosures Wound and Ostomy RN at St. Vincent Healthcare and Billings Clinic, Billings, MT Former employee of KCI, a division