Inter-hospital Geriatric Meeting: An older lady with low back pain: Is the new technology useful? Presenter: Dr Ma HM Supervisor: Dr Ho WS PWH
|
|
|
- Edwin Stephens
- 5 years ago
- Views:
Transcription
1 Inter-hospital Geriatric Meeting: An older lady with low back pain: Is the new technology useful? Presenter: Dr Ma HM Supervisor: Dr Ho WS PWH
2 Case History [1] 87/F, Madam Tsang Admitted to the medical unit of PWH on 14/11/10 for reduced oral intake and decrease in general condition
3 Case History [2] Presented to AED 3 days ago for LBP Recent vertebroplasty done in private X-ray L/S spine: degenerative spines and vertebral collapse Stay in AED EMW Back pain improved by physiotherapy Tramadol 50mg QID and salcitonin 200 IU nasal given for 2 weeks BP on high side: add hydrochlorothiazide 50mg daily and nifedpine SR 20mg bd Discharged on 13/11/2010
4 Case History [3] At medical ward, clarify the history of back pain from patient and relatives LBP for 3 months already Can only walk with few steps at home by holding onto the furniture No history of falls Not relieved by OTC analgesics Sometimes poor sleep at night time due to pain Bathing help from daughter, other ADL remained independent
5 Case History [4] Attended private 20 days before admission Private X-ray spine: collapse of T7 and T8 spines Vertebroplasty done on 26/10/10: 4ml bone cement injected in T8 vertebral body and 3ml cement into T7 vertebral body Back pain worsen despite operation done
6 Case History [5] PMH: HT, hyperlipidemia, minor CAD Drug history: aspirin 80mg daily, atenolol 75mg daily, famotidine 40mg bd, hydrochlorothiazide 25mg daily, nifedipine slow release 20mg bd and simvastatin 20mg nocte NKDA FU by FM clinic Social history: living with daughter, ADLI, take care of her grandchildren, prepare meals for family members, walk unaided
7 Physical examination [1] General: emaciated, BW 40kg, dehydrated Tell history but tired Conscious and orientated to TPP Mood on low side (no suicidal ideation) BP: 139/76 (No postural drop), P: 80bpm, SaO2: 99% (RA) Temp: 37.4 Chest, cardiovascular and abdominal examination unremarkable
8 Physical examination [2] A large palpable bladder Anal tone normal Localized tenderness over the mid-thoracic spine Neurology: generalized limb weakness with power grade 4/5, reflexes normal and downgoing plantar responses bilaterally Sensation over the UL and LLs intact
9 Physical examination [3] Unremarkable breast and thyroid examination No palpable cervical, axillary and inguinal lymph node MMSE 24/30 ( ) GDS 5/15
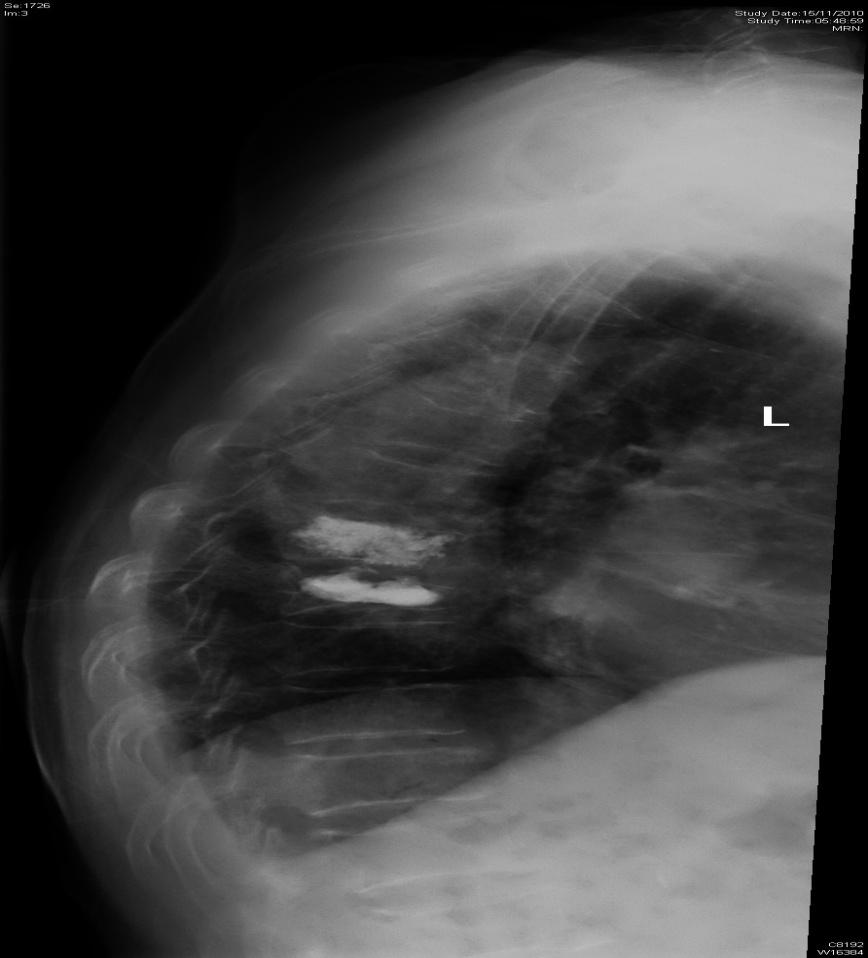
10 Investigations [1] Urine multistix: RBC and WBC +ve; nitrite -ve Post void RU 389ml CXR bilateral lungs clear X-ray T/L/S spine: loss of vertebra height T7 and T8 vertebra. The hyperdense mass in the body of T7 and T8 vertebra may represent cement from previous vertebroplasty. Disc space, end plates and pedicles were grossly intact. Degenerative changes were noted over the lumbar spines.

11
12 Investigations [2] CBC: Hb 12.6, plt 344, WCC 8.3 ESR 16, CRP 1.9 RFT: 125/3.3/11.3/82, albumin 43 LFT/CaPO4 normal, RG 7.0 Paired blood and urine tests (after giving NS for rehydration): Serum Na 129, osmolality 262 Urine Na 71, osmolality 553 TSH 0.81, random cortisol 497 LDSST adequate response
13 Problem list Hyponatremia (HCT, poor intake) Dehydration (poor oral intake after tramadol / pain) Decreased GC (hyponatremia, dehydration, tramadol) Persistent LBP (worsen despite vertebroplasty)? UTI v.s. asymptomatic bacteriuria
14 Initial Management Stop HCT and rehydrate with NS Insert urinary catheter Simplification of medication LBP Paracetamol and opioid analgesic (dologesic and tramadol) + gabapentin Salcitonin for osteoporotic LBP Refer to PT for back physiotherapy and mobilization
15 Progress [1] Hyponatremia Serum Na improved to 130 Keep urinary catheter Urine culture pending LBP Better pain control after medication titration and physiotherapy Functional status Sitting over the bedside with pair trunk control Able to walk with rolator and two assistants
16 Progress [2] Case reviewed in our geriatric team round: Patient was in low mood but GDS 5/15, plan to observe mood +/- consider anti-depressant Pain control improved and plan to step down analgesics (stop gabapentin and keep tramadol only) Consult orthopaedic team for assessment Plan to transfer to SH for mobilization after orthopaedic assessment for: Mobilization Drug titration for LBP Off urinary catheter
17 Progress [3] Developed fever ( C) on Day 7 No respiratory/abdominal/urinary symptoms Clear urine in BSB via urinary catheter Repeat physical examination similar, including thoracic spinal tenderness Urine multistix: blood large and protein +ve, WBC/nitrite both ve Previous urine culture no growth Na 126, K 3.2, Cr 50, urea 5.2, osmolality 260 CRP 14.8, WCC 6.8, Hb 11.1 Repeat CXR no consolidation
18 Progress [4] Further deterioration with mental dullness and sudden onset of bilateral paraplegia on Day 10 GCS 9/15 (E2M5V2) Responded to pain stimuli Bilateral lower limb power grade 1/5, hyporeflexia and left upgoing plantar response, no ankle clonus, anal tone preserved, upper limb power grade 3/5 bilaterally? Cord compression? Analgesics causing drowsiness (though cannot account for paraplegia) Stop tramadol Drowsiness not reversed by naloxone
19 Progress [5] Urgent MRI scan of whole spine (no contrast): Motion artefacts and suboptimal scan Cervical spine was not well visualized There was abnormal signal in the T7 and T8 vertebral bodies due to previous vertebroplasty There was also partial collapse of T8 with mild posterior bony retropulsion No significant canal stenosis or cord compression

20
21 Progress [6] Plain CT brain: Periventricular ischemia Old lacunar infarcts in bilateral basal ganglia No hemorrhage/sol
22 Progress [7] Neurologist suspected CNS infection (dullness + fever) LP attempted: first one failed and reattempt on the next day Second LP: mildly traumatic tap, OP 10cm, straw colored CSF (look like urine!) Add ceftriaxone 2g Q12H IV
23 Progress [8] CSF analysis: WCC 70 (95% lymphocytes) TP 6.05 (blood stained CSF) Glucose 0.5 HSV1 and 2, Enterovirus and VZV ve Cytology negative for malignancy but a large amount of WBC (half polymorphs and half lymphocytes)
24 Causes of her neurological deterioration (?) 1. CNS infection Fever, high CRP and urine-like CSF Iatrogenic cause (LP) Increased CSF protein/wbc and low glucose x Insidious onset (not typical of meningitis) x Apparent lesion at cord level (bilateral upward plantar + hyporeflexia LL) x CSF opening pressure not elevated x CSF urine-like but NOT cloudy / turbid as expected with high protein / WBC
25 Causes of her neurological deterioration (?) 2. Cord compression Sudden onset of paralysis + LBP Neurological findings compatible with cord compression (L1 spinal level ~ T8/9 vertebral level) Elevated CSF protein level CSF opening pressure not high (obstruction above L4/5) x Not supported by MRI finding (absence of significant cord compression)
26 Causes of her neurological deterioration (?) 3. Vertebroplasty Is the CSF finding normal for vertebroplasty??? (high protein/wcc may be due to vertebroplasty, but low glucose was unexplainable) Working diagnosis: cord compression related to vertebroplasty Empirically treated as for TB meningitis as it was the only potentially reversible factor
27 Progress [9] CRP further elevated to ~30 (mg/l) Plan to repeat MRI brain and whole spine (with contrast) on 6/12/2010 CSF MTB PCR negative Patient downhill trend and gasping Relatives agreed for comfort care Started on morphine drip Finally succumbed on 2/12/2010 Cause of death: meningitis (put on the death certificate)
28 Questions on the case?
29 Our questions? Is it worthwhile to do vertebroplasty in this lady? What are possible side effects / complications associated with the procedure? Do we know the normal CSF changes after spinal manipulations?
30 Vertebroplasty [1] First done by interventional radiologist in 1984 in France Osteoporosis compression fractures Vertebral fractures from benign and malignant tumours Percutaneous route under local analgesia Performed in day center Percutaneous vertebroplasty (PV): injection of bone cement under fluoroscopic guidance Mathis JM et al. Am J Neuroradiol 2004;25:840-45
31 Vertebroplasty [2] Polymethylmethacrylate (PMMA) Restore height of collapsed vertebral body
32 Kyphoplasty Balloon-assisted vertebroplasty An balloon inflates the vertebral body and pushes the end-plate apart before injecting bone cement Introduced in the early 1990s Performed by orthopaedic surgeon under general anaesthesia Mathis JM et al. Am J Neuroradiol 2004;25:840-45
33 Literature Review on the RCTs of Vertebroplasty or Kyphoplasty in the Treatment of Osteoporotic Back Pain
34 Voormolen MH et al. Am J Neuroradiol 2007;28:555-60
35 VERTOS 1 Study The first RCT to compare PV with conservative treatment P: Subacute to CHRONIC osteoporotic back pain, i.e. 6 weeks to 6 months, despite medical therapy (18 patients) I: Vertebroplasty (16 patients) C: Optimal pain medication (OPM) O: One year follow up for pain and QOL
36 VERTOS 1 Study Patient in the control arm can switch to vertebroplasty group after 2 weeks of starting treatment Mean duration of back pain: 3 months Premature termination of the study due to high switch over rate (88%) Less pain and analgesic use at 1 day and 2 weeks in the PV group
37 Buchbinder R et al. N Engl J Med 2009;361:
38 Randomized, double-blinded, controlled trial P: Back pain of no more than 12 months (ACUTE + CHRONIC) I: Vertebroplasty (35 patients) C: Sham procedure (36 patients) O: Short-term efficacy, i.e. 1 week to 6 months after procedure
39 Sham procedure: similar procedure to vertebroplasty but stopped at the step of needle puncture Pain relief occurred in both groups but no significant difference

40 Kallmes DF et al. N Engl J Med 2009;361:
41 Investigational Vertebroplasty Safety and Efficacy Trial (INVEST) Randomized, double-blinded, controlled trial P: Back pain of no more than 12 months I: Vertebroplasty (68 patients) C: Sham procedure (63 patients) O: short-term efficacy Significant improvement in back pain, functional disability and QOL at 3 day and 1 month after procedure in BOTH groups of patients WITHOUT statistically significant difference

42 Klazen CAH et al. Lancet 2010;376:
43 VERTOS II Study P: ACUTE back pain of 6 weeks or less I: Vertebroplasty (101 patients) C: Conservative treatment (101 patients) O: Pain relief Mean time from onset of pain to operation: 5.6 weeks
44 VERTOS II Study Better pain relief in the vertebroplasty group compared with the group treated conservatively from 1 day to 1 month after the procedure The differences diminished with time Vertebroplasty effective in providing control over ACUTE osteoporotic back pain Effect sustained for one year (but diminished with time)

45 Rousing R et al. Spine 2010;35:
46 P: ACUTE (<2 weeks) + SUBACUTE (2-8 weeks) back pain I: Vertebroplasty (25 patients) C: Conservative treatment (24 patients) O: Pain relief Significant pain relief immediately (24 hour) after vertebroplasty done, lasted for up to one month No difference in pain control 3 months and 12 months after the procedure done

47 Wardlaw D et al. Lancet 2009;373:
48 FREE Study P: ACUTE vertebral fractures (mean 5.6 weeks+/- 4.4) I: Balloon kyphoplasty (149 patients) C: Conservative treatment (151 patients) O: Pain relief Kyphoplasty provided better pain control than conservative treatment at 1 month after procedure done Effected lasted up to 12 months

49
50 Summary on vertebroplasty Relieving acute osteoporotic back pain May be considered if optimal medical therapy is not enough to relieve back pain Additional analgesic effects (over medical + rehabilitation treatment) seems to wean off by one year Value for beyond-acute LBP?

51 Recurrent back pain after vertebroplasty Lin CC et al. AJR 2010;194:
52 Cement leakage [1] Cement leakage outside vertebral body during vertebroplasty, sometimes even into the disc May result in painful new adjacent vertebral compression fracture (VCF) Usually responded to conservative treatment
53 Cement leakage [2] Retrospective review of 106 consecutive patients undergoing vertebroplasty Age: years (range) New adjacent VCF occurred in 18.9% (20/106) of patients during 24 months of follow-up (mean 38 months) Thoracolumbar junction (18), lumbar (3) and thoracic (1) Cement leakage occurred in 26 patients: 11 had new adjacent VCF Chen WJ et al. J Spinal Disord Tech 2010;23:35-39
54 CSF biochemical changes with vertebroplasty No articles could be searched for it
55 Suggestions on vertebroplasty Optimization of medications for acute osteoporotic LBP Consider referral to orthopaedic surgeon or interventional radiologist for considering vertebroplasty despite optimal medical therapy for 4 weeks Not recommended for chronic LBP Beware of possible complications, such as embolism, cement leakage, vertebral compression fracture and spinal infection
56 Novel treatment/new technology for geriatric population Selection of appropriate groups of patients, i.e. careful digestion of inclusion and exclusion criteria of studies Cautions against the possible side-effects OHAs: glitazone, gliptin NSAIDs: rofecoxib (Vioxx )
57 Discussion
Vertebral Augmentation for Compression Fractures. Scott Magnuson, MD Pain Management of North Idaho, PLLC
 Vertebral Augmentation for Compression Fractures Scott Magnuson, MD Pain Management of North Idaho, PLLC OVCFs are most common type of fragility fracture 20-25% Caucasian women and men over 50 yrs have
Vertebral Augmentation for Compression Fractures Scott Magnuson, MD Pain Management of North Idaho, PLLC OVCFs are most common type of fragility fracture 20-25% Caucasian women and men over 50 yrs have
Metastatic Spinal Disease
 Metastatic Spinal Disease Mr Neil Chiverton Consultant Spinal Surgeon, Sheffield Objectives The scale and nature of the problem NICE recommendations Surgical decision making Case illustrations Incidence
Metastatic Spinal Disease Mr Neil Chiverton Consultant Spinal Surgeon, Sheffield Objectives The scale and nature of the problem NICE recommendations Surgical decision making Case illustrations Incidence
Posterior instrumentation after a failed balloon kyphoplasty in the thoracolumbar junction: a case report
 Cumming et al. Journal of Medical Case Reports 2014, 8:189 JOURNAL OF MEDICAL CASE REPORTS CASE REPORT Open Access Posterior instrumentation after a failed balloon kyphoplasty in the thoracolumbar junction:
Cumming et al. Journal of Medical Case Reports 2014, 8:189 JOURNAL OF MEDICAL CASE REPORTS CASE REPORT Open Access Posterior instrumentation after a failed balloon kyphoplasty in the thoracolumbar junction:
Outline Vertebroplasty and Kyphoplasty: Who, What, and When
 Outline Vertebroplasty and Kyphoplasty: Who, What, and When Douglas C. Bauer, MD University of California San Francisco, USA Vertebral fracture epidemiology, consequences and diagnosis Kyphoplasty and
Outline Vertebroplasty and Kyphoplasty: Who, What, and When Douglas C. Bauer, MD University of California San Francisco, USA Vertebral fracture epidemiology, consequences and diagnosis Kyphoplasty and
Osteoporosis and Spinal Fractures
 Nader M. Hebela, MD Fellow of the American Academy of Orthopaedic Surgeons http://orthodoc.aaos.org/hebela Cleveland Clinic Abu Dhabi Cleveland Clinic Abu Dhabi Neurological Institute Al Maryah Island
Nader M. Hebela, MD Fellow of the American Academy of Orthopaedic Surgeons http://orthodoc.aaos.org/hebela Cleveland Clinic Abu Dhabi Cleveland Clinic Abu Dhabi Neurological Institute Al Maryah Island
This supplement contains the following items:
 This supplement contains the following items: 1. Original protocol, final protocol, summary of changes 2. Original statistical analysis plan, final statistical analysis plan, summary of changes Original
This supplement contains the following items: 1. Original protocol, final protocol, summary of changes 2. Original statistical analysis plan, final statistical analysis plan, summary of changes Original
Fracture REduction Evaluation (FREE) Study
 Study") Fracture REduction Evaluation (FREE) Study Efficacy and Safety of Balloon Kyphoplasty Compared with Non-surgical Care for Vertebral Compression Fracture (FREE): A Randomised Controlled Trial Wardlaw Lancet
Fracture REduction Evaluation (FREE) Study Efficacy and Safety of Balloon Kyphoplasty Compared with Non-surgical Care for Vertebral Compression Fracture (FREE): A Randomised Controlled Trial Wardlaw Lancet
Vertebral Body Augmentation
 Vertebral Body Augmentation Nitin Sekhri MD Department of Anesthesiology Department of Radiology Westchester Medical Center Maria Fareri Children's Hospital Assistant Professor of Anesthesiology New York
Vertebral Body Augmentation Nitin Sekhri MD Department of Anesthesiology Department of Radiology Westchester Medical Center Maria Fareri Children's Hospital Assistant Professor of Anesthesiology New York
Red Flags, and Clinical Presentation Mapping. Sue Greenhalgh Consultant Physiotherapist NHS Bolton
 , and Clinical Presentation Mapping Sue Greenhalgh Consultant Physiotherapist NHS Bolton Be Aware! Clinical Reasoning Recognition of serious pathology early depends on awareness, vigilance and suspicion
, and Clinical Presentation Mapping Sue Greenhalgh Consultant Physiotherapist NHS Bolton Be Aware! Clinical Reasoning Recognition of serious pathology early depends on awareness, vigilance and suspicion
Paul Allan Regional Clinical Lead - South. Lumbar Spine. Assessment & Differential Diagnosis
 Paul Allan Regional Clinical Lead - South Lumbar Spine Assessment & Differential Diagnosis Aims Refresh lumbar spine anatomy Red flags Discuss common pathologies seen in general practice Subjective and
Paul Allan Regional Clinical Lead - South Lumbar Spine Assessment & Differential Diagnosis Aims Refresh lumbar spine anatomy Red flags Discuss common pathologies seen in general practice Subjective and
YOUR SUDDEN BACK PAIN MAY BE A FRACTURE
 YOUR SUDDEN BACK PAIN MAY BE A FRACTURE Sudden-onset back pain could signal a spinal fracture. TALK WITH YOUR DOCTOR If you have tried treatments like rest and oral medication for more than a few days
YOUR SUDDEN BACK PAIN MAY BE A FRACTURE Sudden-onset back pain could signal a spinal fracture. TALK WITH YOUR DOCTOR If you have tried treatments like rest and oral medication for more than a few days
Outline. Vertebroplasty and Kyphoplasty. Epidemiology. Identifying Vertebral Fractures. Page 1
 Outline Vertebroplasty and Kyphoplasty Douglas C. Bauer, MD University of California San Francisco, USA Vertebral fracture epidemiology, consequences and diagnosis Kyphoplasty and vertebroplasty: what
Outline Vertebroplasty and Kyphoplasty Douglas C. Bauer, MD University of California San Francisco, USA Vertebral fracture epidemiology, consequences and diagnosis Kyphoplasty and vertebroplasty: what
General introduction and outlines of this thesis
 General introduction and outlines of this thesis 1 Background Since its introduction in 1984 percutaneous vertebroplasty (PV) has been progressively performed with success in mainly France and from the
General introduction and outlines of this thesis 1 Background Since its introduction in 1984 percutaneous vertebroplasty (PV) has been progressively performed with success in mainly France and from the
Departement of Neurosurgery A.O.R.N A. Cardarelli- Naples.
 Percutaneous posterior pedicle screw fixation in the treatment of thoracic, lumbar and thoraco-lumbar junction (T12-L1) traumatic and pathological spine fractures. Report of 45 cases. G. Vitale, A. Punzo,
Percutaneous posterior pedicle screw fixation in the treatment of thoracic, lumbar and thoraco-lumbar junction (T12-L1) traumatic and pathological spine fractures. Report of 45 cases. G. Vitale, A. Punzo,
Vertebroplasty Balloon kyphoplasty What has NICE said? Who can have vertebroplasty and kyphoplasty? Why has NICE said this?
 This leaflet has been provided to help answer some of the questions that you, or those who care for you, may have about vertebroplasty and/or balloon kyphoplasty. Vertebroplasty is a medical procedure
This leaflet has been provided to help answer some of the questions that you, or those who care for you, may have about vertebroplasty and/or balloon kyphoplasty. Vertebroplasty is a medical procedure
ISPUB.COM. Percutaneous Vertebroplasty In Osteoporotic Compression Fractures. R Chahal, S Acharya
 ISPUB.COM The Internet Journal of Spine Surgery Volume 3 Number 1 Percutaneous Vertebroplasty In Osteoporotic Compression Fractures R Chahal, S Acharya Citation R Chahal, S Acharya.. The Internet Journal
ISPUB.COM The Internet Journal of Spine Surgery Volume 3 Number 1 Percutaneous Vertebroplasty In Osteoporotic Compression Fractures R Chahal, S Acharya Citation R Chahal, S Acharya.. The Internet Journal
HIGH LEVEL - Science
 Learning Outcomes HIGH LEVEL - Science Describe the structure and function of the back and spine (8a) Outline the functional anatomy and physiology of the spinal cord and peripheral nerves (8a) Describe
Learning Outcomes HIGH LEVEL - Science Describe the structure and function of the back and spine (8a) Outline the functional anatomy and physiology of the spinal cord and peripheral nerves (8a) Describe
Kyphoplasty and Vertebroplasty
 Kyphoplasty and Vertebroplasty Policy Number: Original Effective Date: MM.06.007 01/11/2005 Line(s) of Business: Current Effective Date: HMO; PPO 02/01/2012 Section: Surgery Place(s) of Service: Inpatient;
Kyphoplasty and Vertebroplasty Policy Number: Original Effective Date: MM.06.007 01/11/2005 Line(s) of Business: Current Effective Date: HMO; PPO 02/01/2012 Section: Surgery Place(s) of Service: Inpatient;
LOTHIAN LUMBAR SPINE PATHWAYS
 LOTHIAN LUMBAR SPINE PATHWAYS Patient Completes STarT Back form Assess patient and screen for Red Flags. If present refer to Appendix 1 Establish if Neurogenic. If so refer to Appendix 2 Children under
LOTHIAN LUMBAR SPINE PATHWAYS Patient Completes STarT Back form Assess patient and screen for Red Flags. If present refer to Appendix 1 Establish if Neurogenic. If so refer to Appendix 2 Children under
Brain and Central Nervous System Cancers
 Brain and Central Nervous System Cancers NICE guidance link: https://www.nice.org.uk/guidance/ta121 Clinical presentation of brain tumours History and Examination Consider immediate referral Management
Brain and Central Nervous System Cancers NICE guidance link: https://www.nice.org.uk/guidance/ta121 Clinical presentation of brain tumours History and Examination Consider immediate referral Management
Spinal Compression Fractures
 A Patient s Guide to Spinal Compression Fractures 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet is compiled from
A Patient s Guide to Spinal Compression Fractures 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet is compiled from
Robin R. Dyer, D.O. Associate Dean for Academic Affairs Professor/Chair OMM Department Tulsa, Oklahoma. LBP Prevalence
 Robin R. Dyer, D.O. Associate Dean for Academic Affairs Professor/Chair OMM Department Tulsa, Oklahoma LBP Prevalence Approx. 80% adults sometime in their lifetime 2 nd most common pain complaint (headache
Robin R. Dyer, D.O. Associate Dean for Academic Affairs Professor/Chair OMM Department Tulsa, Oklahoma LBP Prevalence Approx. 80% adults sometime in their lifetime 2 nd most common pain complaint (headache
PERCUTANEOUS VERTEBROPLASTY AND KYPHOPLASTY
 Oxford UnitedHealthcare Oxford Clinical Policy PERCUTANEOUS VERTEBROPLASTY AND KYPHOPLASTY Policy Number: PAIN 023.3 T2 Effective Date: October 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE... 1
Oxford UnitedHealthcare Oxford Clinical Policy PERCUTANEOUS VERTEBROPLASTY AND KYPHOPLASTY Policy Number: PAIN 023.3 T2 Effective Date: October 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE... 1
Percutaneous Vertebroplasty for Treatment of Painful Osteoporotic Vertebral Compression Fractures
 Ontario Health Technology Assessment Series 2010; Vol. 10, No. 19 Percutaneous Vertebroplasty for Treatment of Painful Osteoporotic Vertebral Compression Fractures An Evidence-Based Analysis Presented
Ontario Health Technology Assessment Series 2010; Vol. 10, No. 19 Percutaneous Vertebroplasty for Treatment of Painful Osteoporotic Vertebral Compression Fractures An Evidence-Based Analysis Presented
Objectives. Comprehension of the common spine disorder
 Objectives Comprehension of the common spine disorder Disc degeneration/hernia Spinal stenosis Common spinal deformity (Spondylolisthesis, Scoliosis) Osteoporotic fracture Destructive spinal lesions Anatomy
Objectives Comprehension of the common spine disorder Disc degeneration/hernia Spinal stenosis Common spinal deformity (Spondylolisthesis, Scoliosis) Osteoporotic fracture Destructive spinal lesions Anatomy
CLINICAL GUIDELINES. Primary Care Guideline Summary Lumbar Spine Thomas J. Gilbert M.D., M.P.P. 3/17/15 revision
 CLINICAL GUIDELINES Primary Care Guideline Summary Lumbar Spine Thomas J. Gilbert M.D., M.P.P. 3/17/15 revision TRIAGE At the initial visit, a focused history and physical examination is performed to assign
CLINICAL GUIDELINES Primary Care Guideline Summary Lumbar Spine Thomas J. Gilbert M.D., M.P.P. 3/17/15 revision TRIAGE At the initial visit, a focused history and physical examination is performed to assign
A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH)
") A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH) 6565 Fannin Street Houston, TX 77030 Phone: 713-790-3333 DISCLAIMER: The information in this booklet is compiled from a variety of sources.
A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH) 6565 Fannin Street Houston, TX 77030 Phone: 713-790-3333 DISCLAIMER: The information in this booklet is compiled from a variety of sources.
Outline Vertebroplasty and Kyphoplasty: Who, What, and When
 Outline Vertebroplasty and Kyphoplasty: Who, What, and When Douglas C. Bauer, MD University of California San Francisco, USA Vertebral fracture epidemiology, consequences and diagnosis Kyphoplasty and
Outline Vertebroplasty and Kyphoplasty: Who, What, and When Douglas C. Bauer, MD University of California San Francisco, USA Vertebral fracture epidemiology, consequences and diagnosis Kyphoplasty and
Vertebroplasty/Kyphoplasty
 Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
PERCUTANEOUS BALLOON KYPHOPLASTY, RADIOFREQUENCY KYPHOPLASTY, AND MECHANICAL VERTEBRAL AUGMENTATION
 KYPHOPLASTY, AND MECHANICAL VERTEBRAL AUGMENTATION Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures,
KYPHOPLASTY, AND MECHANICAL VERTEBRAL AUGMENTATION Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures,
Percutaneous Vertebroplasty for Acute Osteoporotic Vertebral Fracture Contributes to Restoration of Ambulation
 Original Research Percutaneous Vertebroplasty for Acute Osteoporotic Vertebral Fracture Contributes to Restoration of Ambulation 1) Department of Radiology, National Center for Global Health and Medicine,
Original Research Percutaneous Vertebroplasty for Acute Osteoporotic Vertebral Fracture Contributes to Restoration of Ambulation 1) Department of Radiology, National Center for Global Health and Medicine,
Peggers Super Summaries: The Aging Spine
 Aging Spine: AGING PROCESS Osteopenia 10% of 50 year old males and 25% of 50 year females Disc dehydration Facet degeneration Soft tissue hypertrophy 2 0 deformity Leg pain worse than back pain from nerve
Aging Spine: AGING PROCESS Osteopenia 10% of 50 year old males and 25% of 50 year females Disc dehydration Facet degeneration Soft tissue hypertrophy 2 0 deformity Leg pain worse than back pain from nerve
UTERINE FIBROID EMBOLIZATION
 INTERVENTIONAL RADIOLOGY PROTOCOLS UTERINE FIBROID EMBOLIZATION Interventional Radiology Tower Health Medical Group offers the option to treat uterine fibroids with fibroid embolization (UFE), an alternative
INTERVENTIONAL RADIOLOGY PROTOCOLS UTERINE FIBROID EMBOLIZATION Interventional Radiology Tower Health Medical Group offers the option to treat uterine fibroids with fibroid embolization (UFE), an alternative
DELIRIUM DR S A R A H A B D E L A T I S A S DR H I L A R Y W O L F E N D A L E S T 4
 DELIRIUM DR S A R A H A B D E L A T I S A S DR H I L A R Y W O L F E N D A L E S T 4 AIMS Define delirium Identify: Different types of delirium Risk factors Preventable causes Screening tools Management
DELIRIUM DR S A R A H A B D E L A T I S A S DR H I L A R Y W O L F E N D A L E S T 4 AIMS Define delirium Identify: Different types of delirium Risk factors Preventable causes Screening tools Management
Practical Management Of Osteoporosis
 Practical Management Of Osteoporosis CONFERENCE 2012 Education Centre, Bournemouth.19 November The following companies have given funding towards the cost of this meeting but have no input into the agenda
Practical Management Of Osteoporosis CONFERENCE 2012 Education Centre, Bournemouth.19 November The following companies have given funding towards the cost of this meeting but have no input into the agenda
Cement augmentation in spinal tumors: a systematic review comparing vertebroplasty and kyphoplasty
 35 35 43 Cement augmentation in spinal tumors: a systematic review comparing vertebroplasty and kyphoplasty Authors Josh E Schroeder¹, Erika Ecker², Andrea C Skelly², Leon Kaplan¹ Institutions ¹ Orthopedic
35 35 43 Cement augmentation in spinal tumors: a systematic review comparing vertebroplasty and kyphoplasty Authors Josh E Schroeder¹, Erika Ecker², Andrea C Skelly², Leon Kaplan¹ Institutions ¹ Orthopedic
외래에서흔히접하는 요통환자의진단과치료 울산의대서울아산병원가정의학과 R3 전승엽
 외래에서흔히접하는 요통환자의진단과치료 울산의대서울아산병원가정의학과 R3 전승엽 Index Introduction Etiology & Type Assessment History taking & Physical examination Red flag sign Imaging Common disorder Management Reference Introduction Pain
외래에서흔히접하는 요통환자의진단과치료 울산의대서울아산병원가정의학과 R3 전승엽 Index Introduction Etiology & Type Assessment History taking & Physical examination Red flag sign Imaging Common disorder Management Reference Introduction Pain
A RARE NEUROLOGICAL PRESENTATION OF SLE. Dr Yoganand M N Dr Prithvi P Nayak
 A RARE NEUROLOGICAL PRESENTATION OF SLE Dr Jayachandra Dr Yoganand M N Dr Prithvi P Nayak Presenter: Dr Shambhavi K R CHIEF COMPLAINTS A 30 year old lady hailing from Nepal presented to OPD with complaints
A RARE NEUROLOGICAL PRESENTATION OF SLE Dr Jayachandra Dr Yoganand M N Dr Prithvi P Nayak Presenter: Dr Shambhavi K R CHIEF COMPLAINTS A 30 year old lady hailing from Nepal presented to OPD with complaints
Percutaneous Vertebroplasty and Sacroplasty
 Percutaneous Vertebroplasty and Sacroplasty Policy Number: 6.01.25 Last Review: 11/2017 Origination: 2/2001 Next Review: 11/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide
Percutaneous Vertebroplasty and Sacroplasty Policy Number: 6.01.25 Last Review: 11/2017 Origination: 2/2001 Next Review: 11/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide
Guide to Percutaneous
 Guide to Percutaneous Ve r t e b r o p l a s t y Synergie Ingénierie Médicale S.A.R.L. Z.A. de L Angle - 19370 Chamberet - France rd@synimed.com Guide to Percutaneous Vertebroplasty Notice This guide is
Guide to Percutaneous Ve r t e b r o p l a s t y Synergie Ingénierie Médicale S.A.R.L. Z.A. de L Angle - 19370 Chamberet - France rd@synimed.com Guide to Percutaneous Vertebroplasty Notice This guide is
Vertebroplasty. Radiology Department. Patient information leaflet
 Vertebroplasty Radiology Department Patient information leaflet This leaflet informs you about the procedure known as a vertebroplasty. It explains what is involved and the possible risks. The benefits
Vertebroplasty Radiology Department Patient information leaflet This leaflet informs you about the procedure known as a vertebroplasty. It explains what is involved and the possible risks. The benefits
University of Jordan. Professor Freih Abuhassan -
 Freih Odeh Abu Hassan F.R.C.S.(Eng.), F.R.C.S.(Tr.& Orth.). Professor of Orthopedics University of Jordan 1 A. Sacroiliitis History Trauma is very common Repetitive LS motion--lumbar rotation or axial
Freih Odeh Abu Hassan F.R.C.S.(Eng.), F.R.C.S.(Tr.& Orth.). Professor of Orthopedics University of Jordan 1 A. Sacroiliitis History Trauma is very common Repetitive LS motion--lumbar rotation or axial
Upper back pain and blood in urine
 Upper back pain and blood in urine Search 27-2-2018 For about 6 weeks I have been experiencing mid back pain when I wake up in the morning. The pain is so bad, I cannot go back to sleep, and NO position.
Upper back pain and blood in urine Search 27-2-2018 For about 6 weeks I have been experiencing mid back pain when I wake up in the morning. The pain is so bad, I cannot go back to sleep, and NO position.
Suspecting Tumors, or Could it be cancer?
 Suspecting Tumors, or Could it be cancer? Donna E. Reece, M.D. Princess Margaret Cancer Centre University Health Network Toronto, ON CANADA 07 February 2018 Background Low back pain is common However,
Suspecting Tumors, or Could it be cancer? Donna E. Reece, M.D. Princess Margaret Cancer Centre University Health Network Toronto, ON CANADA 07 February 2018 Background Low back pain is common However,
Outcomes of Balloon Kyphoplasty and Its Use in Pathological Vertebral Compression Fractures; a Single Centre Experience
 The Open Cancer Journal, 2012, 5, 3-6 3 Open Access Outcomes of Balloon Kyphoplasty and Its Use in Pathological Vertebral Compression Fractures; a Single Centre Experience Joseph Merola*, Thirayan Muthu
The Open Cancer Journal, 2012, 5, 3-6 3 Open Access Outcomes of Balloon Kyphoplasty and Its Use in Pathological Vertebral Compression Fractures; a Single Centre Experience Joseph Merola*, Thirayan Muthu
Current Spine Procedures
 SPINE BOOT CAMP: WHAT YOU DON T KNOW MAY COST YOU! David Abraham, M.D. The Reading Neck and Spine Center Reading, PA Current Spine Procedures Epidural/Transforaminal Injections Lumbar Procedures Laminectomy
SPINE BOOT CAMP: WHAT YOU DON T KNOW MAY COST YOU! David Abraham, M.D. The Reading Neck and Spine Center Reading, PA Current Spine Procedures Epidural/Transforaminal Injections Lumbar Procedures Laminectomy
VERTEBRAL COLUMN ANATOMY IN CNS COURSE
 VERTEBRAL COLUMN ANATOMY IN CNS COURSE Vertebral body Sections of the spine Atlas (C1) Axis (C2) What type of joint is formed between atlas and axis? Pivot joint What name is given to a fracture of both
VERTEBRAL COLUMN ANATOMY IN CNS COURSE Vertebral body Sections of the spine Atlas (C1) Axis (C2) What type of joint is formed between atlas and axis? Pivot joint What name is given to a fracture of both
A Structural Service Plan: Towards Better and Safer Spine Surgeries. Department of Orthopaedics & Traumatology Tuen Mun Hospital
 A Structural Service Plan: Towards Better and Safer Spine Surgeries Department of Orthopaedics & Traumatology Tuen Mun Hospital Cheung KK Wong CY Chan Andrew Tse Alfred Chow YY Department of Orthopaedics
A Structural Service Plan: Towards Better and Safer Spine Surgeries Department of Orthopaedics & Traumatology Tuen Mun Hospital Cheung KK Wong CY Chan Andrew Tse Alfred Chow YY Department of Orthopaedics
Vertebroplasty & Kyphoplasty
 Scan for mobile link. Vertebroplasty & Kyphoplasty Vertebroplasty and kyphoplasty are procedures used to treat painful vertebral compression fractures in the spinal column, which are a common result of
Scan for mobile link. Vertebroplasty & Kyphoplasty Vertebroplasty and kyphoplasty are procedures used to treat painful vertebral compression fractures in the spinal column, which are a common result of
FUNCTIONAL OUTCOMES OF TRAUMATIC PARAPLEGIA PATIENTS: DOES SURGERY IMPROVE THE QUALITY OF LIFE?
 FUNCTIONAL OUTCOMES OF TRAUMATIC PARAPLEGIA PATIENTS: DOES SURGERY IMPROVE THE QUALITY OF LIFE? Original Article Orthopaedics R S Bajoria 1, Mahendra Panwar 2, Anand Rao 3, Sameer Gupta 4 1 - Associate
FUNCTIONAL OUTCOMES OF TRAUMATIC PARAPLEGIA PATIENTS: DOES SURGERY IMPROVE THE QUALITY OF LIFE? Original Article Orthopaedics R S Bajoria 1, Mahendra Panwar 2, Anand Rao 3, Sameer Gupta 4 1 - Associate
Kyphoplasty and Vertebroplasty
 Kyphoplasty and Vertebroplasty Policy Number: Original Effective Date: MM.06.007 01/11/2005 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 09/01/2018 Section: Surgery Place(s)
Kyphoplasty and Vertebroplasty Policy Number: Original Effective Date: MM.06.007 01/11/2005 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 09/01/2018 Section: Surgery Place(s)
Indications for Kyphoplasty and Vertebroplasty
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Managing Bone Pain in Metastatic Disease. Rachel Schacht PA-C Medical Oncology and Hematology Associates Presented on 11/2/2018
 Managing Bone Pain in Metastatic Disease Rachel Schacht PA-C Medical Oncology and Hematology Associates Presented on 11/2/2018 None Disclosures Managing Bone Pain in Metastatic Disease This lecture will
Managing Bone Pain in Metastatic Disease Rachel Schacht PA-C Medical Oncology and Hematology Associates Presented on 11/2/2018 None Disclosures Managing Bone Pain in Metastatic Disease This lecture will
Anterior Cervical Discectomy and Fusion Surgery
 Disclaimer This movie is an educational resource only and should not be used to manage orthopaedic health. All decisions about the management of orthopaedic conditions must be made in conjunction with
Disclaimer This movie is an educational resource only and should not be used to manage orthopaedic health. All decisions about the management of orthopaedic conditions must be made in conjunction with
Percutaneous Vertebroplasty-Induced Adjacent Vertebral Compression Fracture. Ki Seong Eom, MD, PhD, and Tae Young Kim, MD, PhD
 Pain Physician 2012; 15:E527-E532 ISSN 2150-1149 Case Report Percutaneous Vertebroplasty-Induced Adjacent Vertebral Compression Fracture Ki Seong Eom, MD, PhD, and Tae Young Kim, MD, PhD From: Department
Pain Physician 2012; 15:E527-E532 ISSN 2150-1149 Case Report Percutaneous Vertebroplasty-Induced Adjacent Vertebral Compression Fracture Ki Seong Eom, MD, PhD, and Tae Young Kim, MD, PhD From: Department
Management of the complications of myeloma and side-effects of treatment Christine Morris Clinical Nurse Specialist in Myeloma Royal Derby Hospital
 Management of the complications of myeloma and side-effects of treatment Christine Morris Clinical Nurse Specialist in Myeloma Royal Derby Hospital Common problems in myeloma Myeloma-related complications/symptoms
Management of the complications of myeloma and side-effects of treatment Christine Morris Clinical Nurse Specialist in Myeloma Royal Derby Hospital Common problems in myeloma Myeloma-related complications/symptoms
Control. Control Through VISCOSITY Control Through DELIVERY Control Through SIMPLICITY
 Control. Now that s CONFIDENCE. Control Through VISCOSITY Control Through DELIVERY Control Through SIMPLICITY Control throughviscosity Controlled Fill Cement Interdigitation Low viscosity cement Trabecular
Control. Now that s CONFIDENCE. Control Through VISCOSITY Control Through DELIVERY Control Through SIMPLICITY Control throughviscosity Controlled Fill Cement Interdigitation Low viscosity cement Trabecular
Hailee Gibson, CCPA Neurosurgery Physician Assistant. Windsor Neurosurgery & Spine Associates. Windsor Regional Hospital Ouellette Campus
 Hailee Gibson, CCPA Neurosurgery Physician Assistant Windsor Neurosurgery & Spine Associates Windsor Regional Hospital Ouellette Campus Disclosures I have no disclosures Learning Objectives Provide information
Hailee Gibson, CCPA Neurosurgery Physician Assistant Windsor Neurosurgery & Spine Associates Windsor Regional Hospital Ouellette Campus Disclosures I have no disclosures Learning Objectives Provide information
Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2
 Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2 Case 79 yo M with hx of T3N0 colon cancer diagnosed in 2008 metastatic liver disease s/p liver segmentectomy 2009
Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2 Case 79 yo M with hx of T3N0 colon cancer diagnosed in 2008 metastatic liver disease s/p liver segmentectomy 2009
CNS Infections. Philip Gothard Consultant in Infectious Diseases Hospital for Tropical Diseases, London. Hammersmith Acute Medicine 2011
 CNS Infections Philip Gothard Consultant in Infectious Diseases Hospital for Tropical Diseases, London Hammersmith Acute Medicine 2011 Case 1 HISTORY 27y man Unwell 3 days Fever Headache Photophobia Previously
CNS Infections Philip Gothard Consultant in Infectious Diseases Hospital for Tropical Diseases, London Hammersmith Acute Medicine 2011 Case 1 HISTORY 27y man Unwell 3 days Fever Headache Photophobia Previously
Objectives. Identify and differentiate appropriate surgical cases. Good Surgical Outcomes
 ECHO February 5 th, 2015 Surgical Selection for Low Back Pain Objectives Identify and differentiate appropriate surgical cases Disclosures Medical director for UHN Rehabilitations Solution Back and Neck
ECHO February 5 th, 2015 Surgical Selection for Low Back Pain Objectives Identify and differentiate appropriate surgical cases Disclosures Medical director for UHN Rehabilitations Solution Back and Neck
Gillian Wooldridge, DO Houston Methodist Willowbrook Hospital Primary Care Sports Medicine Fellowship May 3, 2018
 Gillian Wooldridge, DO Houston Methodist Willowbrook Hospital Primary Care Sports Medicine Fellowship May 3, 2018 Disclosures Neither I nor any family members have financial disclosures Special thanks
Gillian Wooldridge, DO Houston Methodist Willowbrook Hospital Primary Care Sports Medicine Fellowship May 3, 2018 Disclosures Neither I nor any family members have financial disclosures Special thanks
The current situation is that vertebroplasty is used in three situations in this country.
 24 September 2009 Dr Brian Richards Executive Manager Health Technology and Medical Services Group Medical Benefits Division Dr Peter McCombe Level 9 Watkins Medical Centre 225 Wickham Terrace Brisbane
24 September 2009 Dr Brian Richards Executive Manager Health Technology and Medical Services Group Medical Benefits Division Dr Peter McCombe Level 9 Watkins Medical Centre 225 Wickham Terrace Brisbane
Spinal Trauma. General Rehabilitation of Patient with Spinal Trauma. Common Spinal Injuries. Important Anatomical Structures at each Vertebral Level
 Asian Association for Dynamic Osteosynthesis Workshop on Management of Spinal Trauma 22 April 2007 (Sunday) Orthopaedic Learning Centre, PWH, Shatin, Hong Kong General Rehabilitation of Patient with Spinal
Asian Association for Dynamic Osteosynthesis Workshop on Management of Spinal Trauma 22 April 2007 (Sunday) Orthopaedic Learning Centre, PWH, Shatin, Hong Kong General Rehabilitation of Patient with Spinal
LUMBAR SPINE CASE 3. Property of VOMPTI, LLC. For Use of Participants Only. No Use or Reproduction Without Consent 1. L4-5, 5-S1 disc, facet (somatic)
") LUMBAR SPINE CASE 3 A.J. Lievre, PT, DPT, OCS, CMPT Aaron Hartstein, PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Richmond 2018-2019 L4-5, 5-S1 disc, facet (somatic) L5/S1 Radiculopathy
LUMBAR SPINE CASE 3 A.J. Lievre, PT, DPT, OCS, CMPT Aaron Hartstein, PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Richmond 2018-2019 L4-5, 5-S1 disc, facet (somatic) L5/S1 Radiculopathy
Vertebral puncture reduces vertebral fracture-associated pain-do osteoplastic procedures qualify as successful placebo interventions?
 Vertebral puncture reduces vertebral fracture-associated pain-do osteoplastic procedures qualify as successful placebo interventions? Objective: The results of three randomized sham-controlled trials investigating
Vertebral puncture reduces vertebral fracture-associated pain-do osteoplastic procedures qualify as successful placebo interventions? Objective: The results of three randomized sham-controlled trials investigating
CT-guided percutaneous pedicle screw fixation followed by cementoplasty in the treatment of metastatic spinal disease
 CT-guided percutaneous pedicle screw fixation followed by cementoplasty in the treatment of metastatic spinal disease Claudio Pusceddu Dpt of Interventional Radiology Oncological Hospital AOBrotzu Cagliari
CT-guided percutaneous pedicle screw fixation followed by cementoplasty in the treatment of metastatic spinal disease Claudio Pusceddu Dpt of Interventional Radiology Oncological Hospital AOBrotzu Cagliari
Recognition & Treatment of Malignant Spinal Cord Compression Study Day
 Recognition & Treatment of Malignant Spinal Cord Compression Study Day 11 th May 2017 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk Clinical
Recognition & Treatment of Malignant Spinal Cord Compression Study Day 11 th May 2017 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk Clinical
A.J. Lievre, PT, DPT, OCS, CMPT Aaron Hartstein, PT, DPT, OCS, FAAOMPT
 LUMBAR SPINE CASE #3 A.J. Lievre, PT, DPT, OCS, CMPT Aaron Hartstein, PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 L4-5, 5-S1 disc, facet (somatic) L5/S1 Radiculopathy
LUMBAR SPINE CASE #3 A.J. Lievre, PT, DPT, OCS, CMPT Aaron Hartstein, PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 L4-5, 5-S1 disc, facet (somatic) L5/S1 Radiculopathy
Management of complications and side-effects of myeloma. Jackie Quinn Myeloma CNS Belfast Trust
 Management of complications and side-effects of myeloma Jackie Quinn Myeloma CNS Belfast Trust Common problems in myeloma Myeloma-related complications/symptoms Treatment-related side-effects Myeloma bone
Management of complications and side-effects of myeloma Jackie Quinn Myeloma CNS Belfast Trust Common problems in myeloma Myeloma-related complications/symptoms Treatment-related side-effects Myeloma bone
Kyphoplasty and Vertebroplasty
 Kyphoplasty and Vertebroplasty Policy Number: Original Effective Date: MM.06.007 01/11/2005 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 06/27/2014 Section: Surgery Place(s)
Kyphoplasty and Vertebroplasty Policy Number: Original Effective Date: MM.06.007 01/11/2005 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 06/27/2014 Section: Surgery Place(s)
Pulmonary Cement Embolism in a Multiple Myeloma Patient Following Vertebroplasty: A Case Report
 Cronicon OPEN ACCESS Pulmonary Cement Embolism in a Multiple Myeloma Patient Following Vertebroplasty: A Case Report Alpaslan Senkoylu 1 *, Erdem Aktas 2, Murat Songur 3 and Elif Aktas 4 1 Gazi University
Cronicon OPEN ACCESS Pulmonary Cement Embolism in a Multiple Myeloma Patient Following Vertebroplasty: A Case Report Alpaslan Senkoylu 1 *, Erdem Aktas 2, Murat Songur 3 and Elif Aktas 4 1 Gazi University
MSCC CARE PATHWAYS & CASE STUDIES. By Michael Balloch Spine CNS
 MSCC CARE PATHWAYS & CASE STUDIES By Michael Balloch Spine CNS Aims To be familiar with the routes of MSCC prentaion How the guidelines work in practice Routes of presentation Generic intervention Managing
MSCC CARE PATHWAYS & CASE STUDIES By Michael Balloch Spine CNS Aims To be familiar with the routes of MSCC prentaion How the guidelines work in practice Routes of presentation Generic intervention Managing
Collection of abstracts
 Pre-op Post-op NOT FOR SALE IN THE US Collection of abstracts Vertebral anatomical restoration before fixation as a new method to treat vertebral compression fractures. David NORIEGA Stryker Spine International
Pre-op Post-op NOT FOR SALE IN THE US Collection of abstracts Vertebral anatomical restoration before fixation as a new method to treat vertebral compression fractures. David NORIEGA Stryker Spine International
Do you experience pain or numbness in your lower back when standing upright?
 is this you? Do you experience pain or numbness in your lower back when standing upright? Do you experience pain, numbness, or tingling in your legs or buttocks when you walk? Is your discomfort relieved
is this you? Do you experience pain or numbness in your lower back when standing upright? Do you experience pain, numbness, or tingling in your legs or buttocks when you walk? Is your discomfort relieved
CPT 2015: Save Your Practice By Shaping Up Your Spinal Procedure Reporting
 2015 Physician Coding Survival Guide CHAPTER 10: NEUROSURGERY CPT 2015: Save Your Practice By Shaping Up Your Spinal Procedure Reporting Sacroplasty codes will now be inclusive of imaging guidance. You
2015 Physician Coding Survival Guide CHAPTER 10: NEUROSURGERY CPT 2015: Save Your Practice By Shaping Up Your Spinal Procedure Reporting Sacroplasty codes will now be inclusive of imaging guidance. You
Assessment of limping child (beware the child who does not weight bear at all):
:") Department of Paediatrics Clinical Guideline Acutely Limping Child and Septic Arthritis Assessment of limping child (beware the child who does not weight bear at all): History Careful history of any significant
Department of Paediatrics Clinical Guideline Acutely Limping Child and Septic Arthritis Assessment of limping child (beware the child who does not weight bear at all): History Careful history of any significant
Vertebral body augmentation with cement such as vertebroplasty
 Case Report Stentoplasty (Cemented kyphoplasty with Stent) Under Biplane Digital Subtraction Angiography (Biplane DSA) Buranakarl T, MD email : tayard.bu@bgh.co.th Tayard Buranakarl, MD 1 Kanoknard Jaisanuk,
Case Report Stentoplasty (Cemented kyphoplasty with Stent) Under Biplane Digital Subtraction Angiography (Biplane DSA) Buranakarl T, MD email : tayard.bu@bgh.co.th Tayard Buranakarl, MD 1 Kanoknard Jaisanuk,
Medicine. The Incidence of New Vertebral Fractures Following Vertebral Augmentation. A Meta-Analysis of Randomized Controlled Trials
 Medicine SYSTEMATIC REVIEW AND META-ANALYSIS The Incidence of New Vertebral Fractures Following Vertebral Augmentation A Meta-Analysis of Randomized led Trials Weixing Xie, MSc, Daxiang Jin, MD, Chao Wan,
Medicine SYSTEMATIC REVIEW AND META-ANALYSIS The Incidence of New Vertebral Fractures Following Vertebral Augmentation A Meta-Analysis of Randomized led Trials Weixing Xie, MSc, Daxiang Jin, MD, Chao Wan,
DEGENERATIVE SPINAL DISEASE PRABIN SHRESTHA ANISH M SINGH B&B HOSPITAL
 SPINAL CHAPTER, NESON DEGENERATIVE SPINAL DISEASE PRABIN SHRESTHA ANISH M SINGH B&B HOSPITAL INTRODUCTION DEGENERATIVE SPINAL DISEASE Gradual loss of normal structure and function of spine with time Also
SPINAL CHAPTER, NESON DEGENERATIVE SPINAL DISEASE PRABIN SHRESTHA ANISH M SINGH B&B HOSPITAL INTRODUCTION DEGENERATIVE SPINAL DISEASE Gradual loss of normal structure and function of spine with time Also
The in-hospital management of COPD-exacerbation includes three core processes:
 Appendix 1A. Process flow for in-hospital management of COPDexacerbation The in-hospital management of COPD-exacerbation includes three core processes: 1. Diagnostic assessment 2. Pharmacological management
Appendix 1A. Process flow for in-hospital management of COPDexacerbation The in-hospital management of COPD-exacerbation includes three core processes: 1. Diagnostic assessment 2. Pharmacological management
Service: Imaging. Vertebroplasty. Exceptional healthcare, personally delivered
 Service: Imaging Exceptional healthcare, personally delivered Your Doctor has requested that you have a vertebroplasty. We hope the following information will answer some of the questions you may have
Service: Imaging Exceptional healthcare, personally delivered Your Doctor has requested that you have a vertebroplasty. We hope the following information will answer some of the questions you may have
Surgery. Conus medullaris and Cauda Equina Syndromes. Anatomy. See online here
 Surgery Conus medullaris and Cauda Equina Syndromes See online here Conus medullaris and cauda equina syndromes are spinal cord injuries that involve injury to the lumbosacral segment of the spinal cord.
Surgery Conus medullaris and Cauda Equina Syndromes See online here Conus medullaris and cauda equina syndromes are spinal cord injuries that involve injury to the lumbosacral segment of the spinal cord.
Appendix. International coding of diseases according to ICD 10-GM Reimbursement codes per country (in alphabetical order)
") The editors thank Mrs. B. Casteels (Vice President International, Health Policy & Government Relations, Kyphon International), for her help in summarising the current international reimbursement and coding
The editors thank Mrs. B. Casteels (Vice President International, Health Policy & Government Relations, Kyphon International), for her help in summarising the current international reimbursement and coding
Do you experience pain or numbness in your lower back when standing upright?
 is this you? Do you experience pain or numbness in your lower back when standing upright? Do you experience pain, numbness, or tingling in your legs or buttocks when you walk? Is your discomfort relieved
is this you? Do you experience pain or numbness in your lower back when standing upright? Do you experience pain, numbness, or tingling in your legs or buttocks when you walk? Is your discomfort relieved
KYPHON Balloon Kyphoplasty
 KYPHON Results from a randomized controlled study comparing KYPHON to nonsurgical care for treatment of vertebral compression fractures Relief. Mobility. Quality of Life. What is? KYPHON is a minimally
KYPHON Results from a randomized controlled study comparing KYPHON to nonsurgical care for treatment of vertebral compression fractures Relief. Mobility. Quality of Life. What is? KYPHON is a minimally
Title Protocol for the management of suspected cauda equine syndrome & decompensating spinal stenosis at NDDH
 Document Control Title Protocol for the management of suspected cauda equine syndrome & decompensating spinal stenosis at NDDH Author Author s job title Consultant T&O Directorate Scheduled Care Department
Document Control Title Protocol for the management of suspected cauda equine syndrome & decompensating spinal stenosis at NDDH Author Author s job title Consultant T&O Directorate Scheduled Care Department
BRONCHOGENIC CARCINOMA CHALLENGES IN EVALUATION
 BRONCHOGENIC CARCINOMA CHALLENGES IN EVALUATION GRAND ROUND WARD 7C DATE: 25 TH MARCH 2015 PRESENTER: DR E. SAYO FACILITATOR: DR J MECHA DEMOGRAPHIC DATA NAME : CM AGE: 69 YEARS ADDRESS : KIAMBU OCCUPATION:
BRONCHOGENIC CARCINOMA CHALLENGES IN EVALUATION GRAND ROUND WARD 7C DATE: 25 TH MARCH 2015 PRESENTER: DR E. SAYO FACILITATOR: DR J MECHA DEMOGRAPHIC DATA NAME : CM AGE: 69 YEARS ADDRESS : KIAMBU OCCUPATION:
Inova. Spine Institute
 Inova Spine Institute At Inova Spine Institute, you ll find a wide range of treatment alternatives, from physical therapy and rehabilitation to pain management. For patients who require surgery, Inova
Inova Spine Institute At Inova Spine Institute, you ll find a wide range of treatment alternatives, from physical therapy and rehabilitation to pain management. For patients who require surgery, Inova
Original Article Risk factors of new symptomatic vertebral compression fractures after percutaneous vertebroplasty
 Int J Clin Exp Med 2019;12(1):949-954 www.ijcem.com /ISSN:1940-5901/IJCEM0076385 Original Article Risk factors of new symptomatic vertebral compression fractures after percutaneous vertebroplasty Zhen
Int J Clin Exp Med 2019;12(1):949-954 www.ijcem.com /ISSN:1940-5901/IJCEM0076385 Original Article Risk factors of new symptomatic vertebral compression fractures after percutaneous vertebroplasty Zhen
Value of Bone Scan Imaging in Predicting Pain Relief from Percutaneous Vertebroplasty in Osteoporotic Vertebral Fractures
 AJNR Am J Neuroradiol 21:1807 1812, November/December 2000 Value of Bone Scan Imaging in Predicting Pain Relief from Percutaneous Vertebroplasty in Osteoporotic Vertebral Fractures A. Stanley Maynard,
AJNR Am J Neuroradiol 21:1807 1812, November/December 2000 Value of Bone Scan Imaging in Predicting Pain Relief from Percutaneous Vertebroplasty in Osteoporotic Vertebral Fractures A. Stanley Maynard,
Percutaneous Vertebroplasty, Kyphoplasty, Sacroplasty, and Coccygeoplasty
 Medical Policy Manual Surgery, Policy No. 107 Percutaneous Vertebroplasty, Kyphoplasty, Sacroplasty, and Coccygeoplasty Next Review: April 2019 Last Review: April 2018 Effective: June 1, 2018 IMPORTANT
Medical Policy Manual Surgery, Policy No. 107 Percutaneous Vertebroplasty, Kyphoplasty, Sacroplasty, and Coccygeoplasty Next Review: April 2019 Last Review: April 2018 Effective: June 1, 2018 IMPORTANT
Back Pain Policies Summary
 Back Pain Policies Summary These policies are part of the wider project, Reviewing local health policies, which is reviewing and updating more than 100 policies, of which back pain are part of. This review
Back Pain Policies Summary These policies are part of the wider project, Reviewing local health policies, which is reviewing and updating more than 100 policies, of which back pain are part of. This review
Lumbar Disc Prolapse. Dr. Ahmed Salah Eldin Hassan. Professor of Neurosurgery & Consultant spinal surgeon
 Lumbar Disc Prolapse By Dr. Ahmed Salah Eldin Hassan Professor of Neurosurgery & Consultant spinal surgeon 1-What are the Functions of the Spine Structural support for upright posture Protection of Spinal
Lumbar Disc Prolapse By Dr. Ahmed Salah Eldin Hassan Professor of Neurosurgery & Consultant spinal surgeon 1-What are the Functions of the Spine Structural support for upright posture Protection of Spinal
Percutaneous vertebroplasty (PV) consists of the percutaneous
 consists of the percutaneous") ORIGINAL RESEARCH M.H.J. Voormolen W.P.T.M. Mali P.N.M. Lohle H. Fransen L.E.H. Lampmann Y. van der Graaf J.R. Juttmann X. Jansssens H.J.J. Verhaar Percutaneous Vertebroplasty Compared with Optimal Pain
ORIGINAL RESEARCH M.H.J. Voormolen W.P.T.M. Mali P.N.M. Lohle H. Fransen L.E.H. Lampmann Y. van der Graaf J.R. Juttmann X. Jansssens H.J.J. Verhaar Percutaneous Vertebroplasty Compared with Optimal Pain
REVIEW QUESTIONS ON VERTEBRAE, SPINAL CORD, SPINAL NERVES
 REVIEW QUESTIONS ON VERTEBRAE, SPINAL CORD, SPINAL NERVES 1. A 28-year-old-women presented to the hospital emergency room with intense lower back spasms in the context of coughing during an upper respiratory
REVIEW QUESTIONS ON VERTEBRAE, SPINAL CORD, SPINAL NERVES 1. A 28-year-old-women presented to the hospital emergency room with intense lower back spasms in the context of coughing during an upper respiratory
If you have a condition that compresses your nerves, causing debilitating back pain or numbness along the back of your leg.
 Below, we have provided some basic information for your benefit. Please use this information is an educational aid only. It is not intended as medical advice for individual conditions or treatments. Talk
Below, we have provided some basic information for your benefit. Please use this information is an educational aid only. It is not intended as medical advice for individual conditions or treatments. Talk
Osteoporosis, the most common metabolic. Redo Kyphoplasty with Vertebroplasty Technique: A Case Report and Review of the Literature.
 Pain Physician 2009; 12:645-649 ISSN 1533-3159 Case Report Redo Kyphoplasty with Vertebroplasty Technique: A Case Report and Review of the Literature Michael E. Frey, MD From: Virginia Commonwealth University,
Pain Physician 2009; 12:645-649 ISSN 1533-3159 Case Report Redo Kyphoplasty with Vertebroplasty Technique: A Case Report and Review of the Literature Michael E. Frey, MD From: Virginia Commonwealth University,
Name of Policy: Percutaneous Vertebroplasty, Kyphoplasty, Mechanical Vertebral Augmentation and Sacroplasty
 Name of Policy: Percutaneous Vertebroplasty, Kyphoplasty, Mechanical Vertebral Augmentation and Sacroplasty Policy #: 004 Latest Review Date: July 2014 Category: Radiology/Surgical Policy Grade: B Background/Definitions:
Name of Policy: Percutaneous Vertebroplasty, Kyphoplasty, Mechanical Vertebral Augmentation and Sacroplasty Policy #: 004 Latest Review Date: July 2014 Category: Radiology/Surgical Policy Grade: B Background/Definitions:
Comprehension of the common spine disorder.
 Objectives Comprehension of the common spine disorder. Disc degeneration/hernia. Spinal stenosis. Common spinal deformity (Spondylolisthesis, Scoliosis). Osteoporotic fracture. Anatomy Anatomy Anatomy
Objectives Comprehension of the common spine disorder. Disc degeneration/hernia. Spinal stenosis. Common spinal deformity (Spondylolisthesis, Scoliosis). Osteoporotic fracture. Anatomy Anatomy Anatomy