DELIRIUM DR S A R A H A B D E L A T I S A S DR H I L A R Y W O L F E N D A L E S T 4
|
|
|
- Vivian Stone
- 5 years ago
- Views:
Transcription
1 DELIRIUM DR S A R A H A B D E L A T I S A S DR H I L A R Y W O L F E N D A L E S T 4
2 AIMS Define delirium Identify: Different types of delirium Risk factors Preventable causes Screening tools Management

3 Can you define delirium?
4 How many types of delirium are there? Can you name them? Which of these do we see commonly in hospital?
5 Who is most at risk?
6 What is the prevalence of delirium? Medical patients? Surgical patients? Patients in long term care?
7 Can delirium be prevented? If so, can you think of any ways?
8 How do we screen for delirium? Can you think of any screening tools?
9 How does delirium affect patients and carers? Morbidity? Mortality? Complications?
10 NICE Guidelines Prevention Diagnosis and Management
11 Definition Acute confusional state common clinical syndrome Disturbance in consciousness, cognitive function and perception Acute onset Fluctuating course Preventable and treatable Assocc. with poor outcome
12 Prevalence On medical wards 20-30% Surgical patients 10-50% In long term care <20% Poor awareness and under reporting
13 Indicators Recent (hours/days) changes or fluctuation in behaviour Reported by patient, carer or relative If indicators present a competent HP should carry out a screening test
14 Indicators Cognitive function - reduced concentration, slow responses & confusion Perception - visual /auditory hallucinations Physical function - reduced mobility, slow movements, change in appetite, sleep disturbance, restlessness agitation Social behaviour - lack of cooperation, withdrawn, alteration in communication, mood and attitude
15 Types Hyperactive heightened arousal, restlessness, agitation and aggression Hypoactive withdrawn, quiet, drowsy Mixed combination of both Delirium in Dementia difficult to recognise
16 Risk Factors Older age > 65yrs Cognitive impairment Past or present Severe illness any condition at risk of deteriorating Hip fracture
17 Outcomes Longer hospital stay Increased risk of ICU admission Increased risk of hospital acquired complications falls and pressure sores i.e Increased need for long term care Increased risk of death
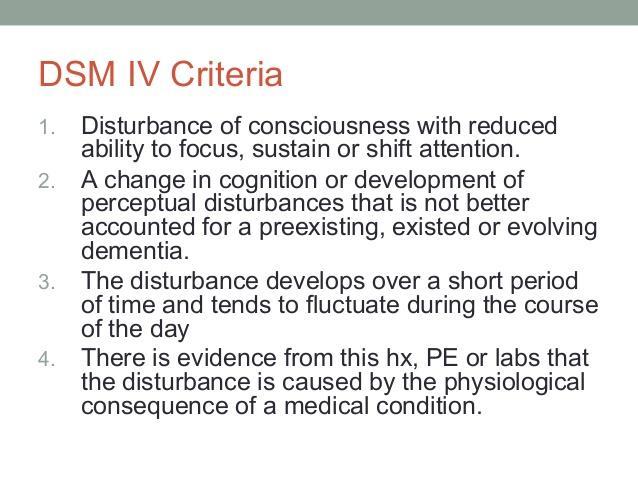
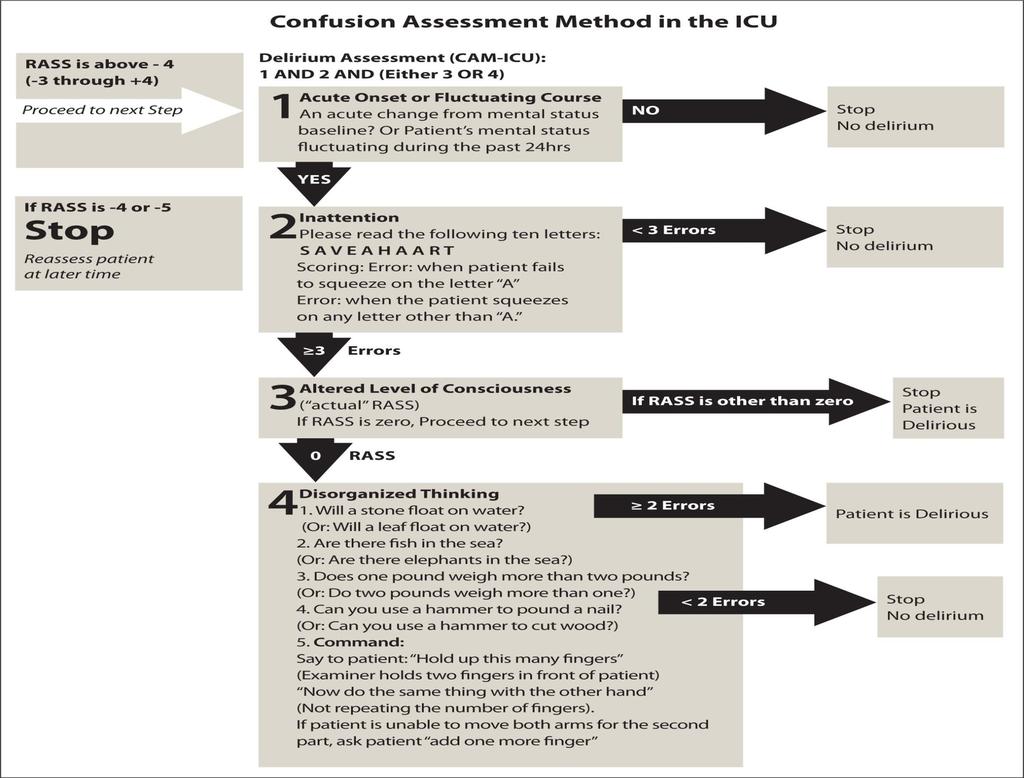
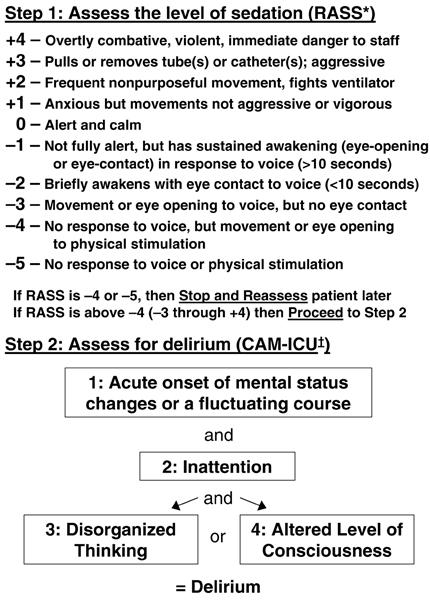
18 Diagnosis If indicators for delirium identified: Assess using Diagnositic and Statistical Manual of Mental Disorders (DSM-IV) criteria or short Confusion Assessment Method (CAM) In ICU or recovery room post-op CAM-ICU
19 Diagnosis If unclear whether delirium, dementia or delirium superimposed on dementia treat as delirium first Assessment to be carried out by trained competent HP Diagnosis of Delirium should be documented in both hospital and primary care health records.
20 Prevention For those at risk Provided by a team of HCP familiar with the patient Provide Multicomponent Intervention Package (MCIP) Assess patient within 24hrs of admission for clinical risk factors Tailor the MCIP to individual need
21 Prevention 1- Avoid room/ward changes unless absolutely necessary 2- Cognitive Impairment/disorientation- provide: Good lighting Clear Signage 24hr clock Calendar Re-orientation informing patient who they are, where they are and what you role is Facilitate visits from family and friends
22 Prevention 3- Dehydration prevent and treat, encourage oral intake and supplement with S/C and IV fluids 4- Constipation prevent and treat 5-Hypoxia assess and treat 6-Address infections investigate and treat avoid unnecessary catheterisation implement infection control procedure
23 Prevention 7- Immobility encourage to mobilise provide necessary aids early mobilisation post-op in bedbound pts encourage active range of motion exercises 8-Pain assess for non verbal signs in learning difficulties, dementia, ventilated and trachy. patients Medication review and analgesia 9-Nutrition assess status and check dentures
24 Prevention 10- Sensory impairment Resolving reversible causes ensuring visual and hearing aids available and in good working order 11- Good sleep pattern and hygiene avoid nursing/medical procedures during sleep hours schedule medication rounds to avoid sleep disturbance reduce noise
25 Treatment Identify and manage the underlying cause Effective communication, re-orientation and reassurance Involve family, friends and carers Provide a suitable environment
26 Treatment Distressed patients at risk to self and others verbal and non verbal de-escalation techniques short term use of anti-psychotics Haloperidol and Olanzepine at lowest doses titrate according to response ( less than 1 week) Anti-psychotics should be used with caution in patients with Parkinson Ds and Lewi-Body Dementia
27 Treatment If delirium does not resolve Re-evaluate the underlying cause(s) Follow up and assess for dementia
28 Diagnostic algorithm for Delirium
29
30
31
32
33
34
35 References NICE guidelines Trust guidelines Dec

36 Mrs P 82 yo lady BG of IHD, OA, CVA 2015 Lives in sheltered accommodation Admitted with a fall Found on floor by grandson Brought to ED > MAU >Med ward
37 Referral ATSP day 3 of admission Confusion Poor oral intake Poor mobility Poorly communicative Is this her new baseline? Collateral history from Grandson
38 Investigations Bloods: Raised CK and AKI 1 Mildly raised WCC and CRP CXR some basal atelectasis CTB cerebral atrophy, established (old) lacunar infarct ECG sinus rhythm, 86bpm L&S BP no significant postural drop
39 On examination A- MOA B- Good AE, sats 95% RA, RR 17 C- HS regular I+II+0, calves SNT, BP 114/76, catheter draining clear urine D- Abdo firm, non-tender, BS normal, BM 5.8 AVPU Poorly attentive, disorientated to TPP, Appeared low in mood
40 Charts Catheterised- good UO Poor oral intake BNO? not documented Not mobilising Waterlow score >10
41 Medications Amitriptyline Regular co-codamol Bendroflumethiazide Clopidogrel Ramipril Bisoprolol Solifenacin Hypromellose eye drops PRN Tramadol
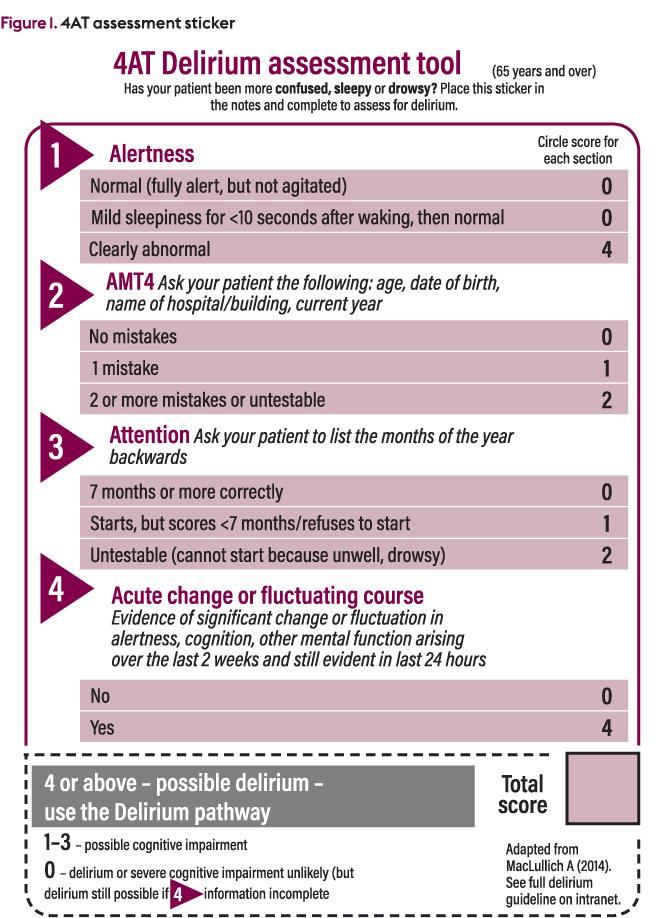
42 Screening CAM 4AT
43 Diagnosis?
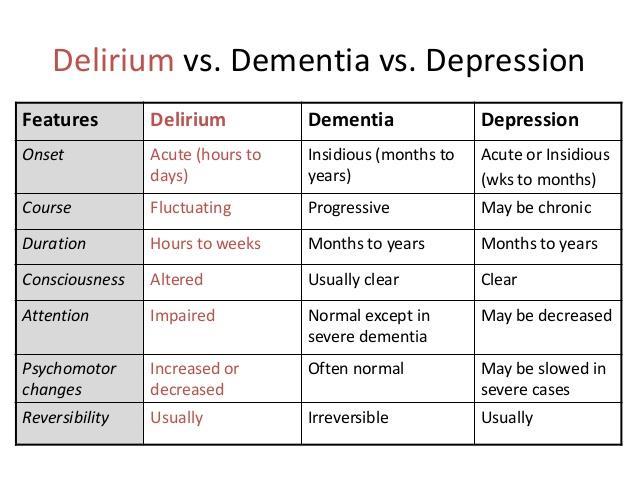
44 Diagnosis? Delirium- Hypoactive Dementia Depression
45 Risk factors
46 Risk factors Age Comorbidities
47 Causes of delirium?
48 Causes of delirium? 3 different transfers during stay Sensory impairment glasses, hearing aid Nutrition dentures Hydration Catheterised Constipated Polypharmacy Immobility walking stick
49 Management 3 different transfers during stay Avoid transfers/sleepouts Sensory impairment Ensure glasses, hearing aids, dentures available in reach and working Nutrition SLT, Dietician, regular mouthcare Hydration Assess and treat, avoid lines where possible
50 Management Catheterised TWOC asap Constipated Avoid constipating drugs, prescribe laxatives, PR exams- enemas Polypharmacy Reduce Immobility Early mobilisation, provide aids, PT/OT input
51 Management Daily assessment CAM Ongoing management of preventable causes If no improvement, re-review preventable causes +/ diagnosis Document to GP episode of delirium
52 Can you define delirium? Disturbance in consciousness, cognitive function or perception Acute onset over hours to days Fluctuating course Serious condition associated with poor outcomes Preventable and treatable
53 How many types of delirium are there? Hyperactive- heightened arousal, restless, agitated, aggressive Hypoactive- withdrawn, quiet, sleepy Mixed
54 Who is most at risk? Older people (>65 yo) People with cognitive impairment (past or present) and/or dementia Severe illness Current hip fracture
55 Prevalence Medical wards 20-30% Surgical patients 10-50% In long term care <20% Poor awareness and under reporting
56 Can delirium be prevented? YES Identify those at risk Number of modifiable risk factors Preventing delirium should improve outcomes for people at risk and have cost savings for service providers
57 How do we screen for delirium? CAM CAM-ICU DSM IV criteria 4AT
58 How does delirium affect patients and carers? More likely to: Have longer hospital stay Have dementia at 3 year f/u Have more hospital-acquired complications eg. falls and pressure sores Have to go into long term care on discharge Die
59

60
Delirium. Quick reference guide. Issue date: July Diagnosis, prevention and management
 Issue date: July 2010 Delirium Diagnosis, prevention and management Developed by the National Clinical Guideline Centre for Acute and Chronic Conditions About this booklet This is a quick reference guide
Issue date: July 2010 Delirium Diagnosis, prevention and management Developed by the National Clinical Guideline Centre for Acute and Chronic Conditions About this booklet This is a quick reference guide
Confusion in the acute setting Dr Susan Shenkin
 Confusion in the acute setting Dr Susan Shenkin Susan.Shenkin@ed.ac.uk 4 th International Conference, Society for Acute Medicine, Edinburgh 7-8 October 2010 Summary Confusion is not a diagnosis Main differentials
Confusion in the acute setting Dr Susan Shenkin Susan.Shenkin@ed.ac.uk 4 th International Conference, Society for Acute Medicine, Edinburgh 7-8 October 2010 Summary Confusion is not a diagnosis Main differentials
Delirium Assessment and the assessment of people at risk
 Assessment and the assessment of people at risk Tracey Mc Erlain Burns RGN, Dip N (lond), MBA, Chief Nurse The Rotherham NHS Foundation Trust What is delirium? Historically seen as a person who is confused/
Assessment and the assessment of people at risk Tracey Mc Erlain Burns RGN, Dip N (lond), MBA, Chief Nurse The Rotherham NHS Foundation Trust What is delirium? Historically seen as a person who is confused/
Mouth care for people with dementia. Delirium (Confusion) Understanding changes in behaviour in dementia
 Understanding changes in behaviour in dementia") Mouth care for people with dementia Delirium (Confusion) Understanding changes in behaviour in dementia 2 Dementia UK Delirium (confusion) A sudden change in a person s mental state is known as delirium.
Mouth care for people with dementia Delirium (Confusion) Understanding changes in behaviour in dementia 2 Dementia UK Delirium (confusion) A sudden change in a person s mental state is known as delirium.
Delirium Assessment and management in relation to falls risk in hospital
 Delirium Assessment and management in relation to falls risk in hospital A house call - Mrs JM 95-year-old lady Normally cognitively intact Multiple medical problems, including falls Housebound, mobile
Delirium Assessment and management in relation to falls risk in hospital A house call - Mrs JM 95-year-old lady Normally cognitively intact Multiple medical problems, including falls Housebound, mobile
Delirium. Delirium is characterized by an acute onset (hours or days) and fluctuating course of deterioration in mental functioning.
 and fluctuating course of deterioration in mental functioning.") Delirium Delirium is characterized by an acute onset (hours or days) and fluctuating course of deterioration in mental functioning. DELIRIUM IS A MEDICAL EMERGENCY! Delirium: Hallmark Features Inattention-
Delirium Delirium is characterized by an acute onset (hours or days) and fluctuating course of deterioration in mental functioning. DELIRIUM IS A MEDICAL EMERGENCY! Delirium: Hallmark Features Inattention-
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Delirium: developing and implementing a multi-component intervention
 Delirium: developing and implementing a multi-component intervention Dr. Duncan Forsyth Consultant Geriatrician Addenbrooke s Hospital Cambridge University Hospitals NHS Foundation Trust Cambridge, England
Delirium: developing and implementing a multi-component intervention Dr. Duncan Forsyth Consultant Geriatrician Addenbrooke s Hospital Cambridge University Hospitals NHS Foundation Trust Cambridge, England
Test your Knowledge: Recognizing Delirium
 The Ottawa Hospital Name: Unit: Profession: RN RPN PT OT SW Other Note: Each question has only one correct answer. 1. If a patient is identified as being at high risk for developing delirium, his/her mental
The Ottawa Hospital Name: Unit: Profession: RN RPN PT OT SW Other Note: Each question has only one correct answer. 1. If a patient is identified as being at high risk for developing delirium, his/her mental
Delirium in the Elderly
 Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium. Patient Information Leaflet
 Delirium Patient Information Leaflet Betty, a lady who had been admitted to hospital with a broken hip, had been fully independent in her own home. A few days after surgery to repair her hip she became
Delirium Patient Information Leaflet Betty, a lady who had been admitted to hospital with a broken hip, had been fully independent in her own home. A few days after surgery to repair her hip she became
Information for Patients, Relatives and Carers
 Delirium Department of Geriatric Medicine Information for Patients, Relatives and Carers This leaflet aims to describe the main symptoms of delirium and highlights those patients that are at high risk
Delirium Department of Geriatric Medicine Information for Patients, Relatives and Carers This leaflet aims to describe the main symptoms of delirium and highlights those patients that are at high risk
Delirium Information for relatives, carers and patients
 Delirium Information for relatives, carers and patients Contents Part A Introduction What is delirium? Quotes from relatives or carers showing what might happen to a patient suffering from delirium How
Delirium Information for relatives, carers and patients Contents Part A Introduction What is delirium? Quotes from relatives or carers showing what might happen to a patient suffering from delirium How
Delirium in the Elderly
 Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
DELIRIUM MODULE: CORE MEDICINE: CARE OF THE ELDERLY TARGET: FY1/2 OR CMT 1/2 (+ NURSES, HCA, OT) BACKGROUND: RELEVANT AREAS OF THE CMT CURRICULUM
 BACKGROUND: RELEVANT AREAS OF THE CMT CURRICULUM") DELIRIUM MODULE: CORE MEDICINE: CARE OF THE ELDERLY TARGET: FY1/2 OR CMT 1/2 (+ NURSES, HCA, OT) BACKGROUND: Delirium (or acute confusional state) is a common and serious clinical syndrome, which is associated
DELIRIUM MODULE: CORE MEDICINE: CARE OF THE ELDERLY TARGET: FY1/2 OR CMT 1/2 (+ NURSES, HCA, OT) BACKGROUND: Delirium (or acute confusional state) is a common and serious clinical syndrome, which is associated
Delirium. Dr. Lesley Wiesenfeld. Deputy Psychiatrist in Chief, Mount Sinai Hospital. Dr. Carole Cohen
 Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Northumbria Healthcare NHS Foundation Trust. Your guide to understanding Delirium. Issued by Department of Medicine
 Northumbria Healthcare NHS Foundation Trust Your guide to understanding Delirium Issued by Department of Medicine Purpose of this leaflet This leaflet is for patients and carers and aims to give you information
Northumbria Healthcare NHS Foundation Trust Your guide to understanding Delirium Issued by Department of Medicine Purpose of this leaflet This leaflet is for patients and carers and aims to give you information
Delirium. Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta
 Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Delirium Information for patients and relatives. Delirium is common Delirium is treatable Relatives can stay to help us
 Delirium Information for patients and relatives Delirium is common Delirium is treatable Relatives can stay to help us What is delirium? Delirium is caused by a disturbance of brain function. It is used
Delirium Information for patients and relatives Delirium is common Delirium is treatable Relatives can stay to help us What is delirium? Delirium is caused by a disturbance of brain function. It is used
Delirium in the hospitalized patient
 Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
How to prevent delirium in nursing home. Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium
 How to prevent delirium in nursing home Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium 1 CONFLICT OF INTEREST DISCLOSURE I have no potential conflict of interest to report 2 Outline 1. Introduction
How to prevent delirium in nursing home Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium 1 CONFLICT OF INTEREST DISCLOSURE I have no potential conflict of interest to report 2 Outline 1. Introduction
10/2/2014. Disclosure. Is Playing NICE Enough? AMP 2014 Annual Meeting. Learning Objectives
 Is Playing NICE Enough? Implementing a Delirium Identification and Prevention Protocol Throughout a Hospital System October 11, 2014 Thomas W. Heinrich, MD, FAPM Professor of Psychiatry and Family Medicine
Is Playing NICE Enough? Implementing a Delirium Identification and Prevention Protocol Throughout a Hospital System October 11, 2014 Thomas W. Heinrich, MD, FAPM Professor of Psychiatry and Family Medicine
Delirium. Dr. John Puxty
 Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
AGED SPECIFIC ASSESSMENT TOOLS. Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services
 AGED SPECIFIC ASSESSMENT TOOLS Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services Issues in assessing the Elderly Association between biological, psychological, social and cultural
AGED SPECIFIC ASSESSMENT TOOLS Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services Issues in assessing the Elderly Association between biological, psychological, social and cultural
Delirium in Hospital Care
 Delirium in Hospital Care Dr John Puxty 1 Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors,
Delirium in Hospital Care Dr John Puxty 1 Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors,
Workshop cases answers
 Workshop cases answers BPSD Workshop: case histories Case 1: Mrs DM Scenario This is an 83 year old lady diagnosed with multi infarct dementia in 2008. Lives with husband and the couple are supported by
Workshop cases answers BPSD Workshop: case histories Case 1: Mrs DM Scenario This is an 83 year old lady diagnosed with multi infarct dementia in 2008. Lives with husband and the couple are supported by
Improving the quality of care of patients with delirium
 Improving the quality of care of patients with delirium Alasdair MacLullich MRCP(UK), PhD Professor of Geriatric Medicine University of Edinburgh Scotland How are we doing now? We are doing badly. Difficult
Improving the quality of care of patients with delirium Alasdair MacLullich MRCP(UK), PhD Professor of Geriatric Medicine University of Edinburgh Scotland How are we doing now? We are doing badly. Difficult
Geriatrics and Cancer Care
 Geriatrics and Cancer Care Roger Wong, BMSc, MD, FRCPC, FACP Postgraduate Dean of Medical Education Clinical Professor, Division of Geriatric Medicine UBC Faculty of Medicine Disclosure No competing interests
Geriatrics and Cancer Care Roger Wong, BMSc, MD, FRCPC, FACP Postgraduate Dean of Medical Education Clinical Professor, Division of Geriatric Medicine UBC Faculty of Medicine Disclosure No competing interests
Strategies to minimize delirium for hip fracture patients
 Strategies to minimize delirium for hip fracture patients Stephen L Kates, M.D. Professor and Chairman Department Date of Orthopaedic Surgery Delirium incidence Up to 61% of hip fracture patients get delirium
Strategies to minimize delirium for hip fracture patients Stephen L Kates, M.D. Professor and Chairman Department Date of Orthopaedic Surgery Delirium incidence Up to 61% of hip fracture patients get delirium
THINK DELIRIUM. Improving the care for older people Delirium toolkit
 THINK DELIRIUM Improving the care Delirium toolkit Healthcare Improvement Scotland 2014 The contents of this document may be copied or reproduced for use within NHSScotland, or for educational, personal
THINK DELIRIUM Improving the care Delirium toolkit Healthcare Improvement Scotland 2014 The contents of this document may be copied or reproduced for use within NHSScotland, or for educational, personal
Delirium. Delirium. Delirium Etiology and Pathophysiology. Fall 2018
 Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
DELIRIUM GUIDELINES. 1 of 19. Author Lead Director. Dementia Steering Group Dr Rachel Holt, Consultant Physician, Elderly Medicine
 DELIRIUM GUIDELINES Author Lead Director Electronic File Reference Version Number 3.0 Date of Publication on MY intranet November 2015 Date Due for Revision November 2017 Dementia Steering Group Dr Rachel
DELIRIUM GUIDELINES Author Lead Director Electronic File Reference Version Number 3.0 Date of Publication on MY intranet November 2015 Date Due for Revision November 2017 Dementia Steering Group Dr Rachel
POST STROKE DELIRIUM. Dr Janet Ballantyne
 POST STROKE DELIRIUM Dr Janet Ballantyne Delirium de: away from/off lira: ridge between ploughed farrows/tracks off the tracks Acute confusional state Acute brain syndrome Acute brain failure Metabolic
POST STROKE DELIRIUM Dr Janet Ballantyne Delirium de: away from/off lira: ridge between ploughed farrows/tracks off the tracks Acute confusional state Acute brain syndrome Acute brain failure Metabolic
Guideline for the Identification and Management of Delirium (Including use of the THINK DELIRIUM Support Tool)
") Guideline for the Identification and Management of Delirium (Including use of the THINK DELIRIUM Support Tool) B27/2009 1. Introduction 1.1 Delirium is a common problem which occurs in about 15-20 out
Guideline for the Identification and Management of Delirium (Including use of the THINK DELIRIUM Support Tool) B27/2009 1. Introduction 1.1 Delirium is a common problem which occurs in about 15-20 out
Critical Care Pharmacological Management of Delirium
 Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach
 Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach Featuring: Felice Rogers Evans BSN RN BC Ty Breiter MSN RN CNL Tampa General Hospital NICHE exemplar hospital Three time
Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach Featuring: Felice Rogers Evans BSN RN BC Ty Breiter MSN RN CNL Tampa General Hospital NICHE exemplar hospital Three time
CARE HOME STAGE 2 - MULTIFACTORIAL FALLS RISK ASSESSMENT AND MANAGEMENT PLAN
 CARE HOME STAGE 2 - MULTIFACTORIAL FALLS RISK ASSESSMENT AND MANAGEMENT PLAN FIRST NAME: DATE OF BIRTH: NHS NO: CARE HOME: ROOM NO: LAST NAME: Assessment to be completed on all residents aged 65 or older
CARE HOME STAGE 2 - MULTIFACTORIAL FALLS RISK ASSESSMENT AND MANAGEMENT PLAN FIRST NAME: DATE OF BIRTH: NHS NO: CARE HOME: ROOM NO: LAST NAME: Assessment to be completed on all residents aged 65 or older
Delirium. Approach. Symptom Update Masterclass:
 Symptom Update Masterclass: Delirium Jason Boland Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine Wolfson Centre for Palliative Care Research Hull York Medical School University
Symptom Update Masterclass: Delirium Jason Boland Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine Wolfson Centre for Palliative Care Research Hull York Medical School University
GUIDELINES FOR DIAGNOSIS, PREVENTION AND TREATMENT OF DELIRIUM IN THE INPATIENT SETTING
 GUIDELINES FOR DIAGNOSIS, PREVENTION AND TREATMENT OF DELIRIUM IN THE INPATIENT SETTING Policy Details NHFT document reference MMG033 Version Final Date Ratified May 2016 Ratified by Medicines Management
GUIDELINES FOR DIAGNOSIS, PREVENTION AND TREATMENT OF DELIRIUM IN THE INPATIENT SETTING Policy Details NHFT document reference MMG033 Version Final Date Ratified May 2016 Ratified by Medicines Management
DELIRIUM Information for relatives and carers Page
 South London and Maudsley NHS Foundation Trust DELIRIUM Information for relatives and carers Page Delirium "After her hip operation, my mother became very confused and aggressive. She kept pulling out
South London and Maudsley NHS Foundation Trust DELIRIUM Information for relatives and carers Page Delirium "After her hip operation, my mother became very confused and aggressive. She kept pulling out
Delirium, Depression and Dementia
 Delirium, Depression and Dementia Martha Watson, MS, APRN, GCNS Some material included in this presentation is adapted from: NICHE (2009). Geriatric Resource Nurse Core Curriculum [Power Point presentation].
Delirium, Depression and Dementia Martha Watson, MS, APRN, GCNS Some material included in this presentation is adapted from: NICHE (2009). Geriatric Resource Nurse Core Curriculum [Power Point presentation].
Delirium in the ICU: Prevention and Treatment. Delirium Defined Officially. Delirium: Really Defined. S. Andrew Josephson, MD
 Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
The Person: Dementia Basics
 The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
Palliative Care. Barry Lunny Registrar in Palliative Medicine
 Symptom Management in Palliative Care Delirium and Pain Barry Lunny Registrar in Palliative Medicine Delirium outline What delirium is and why it is important How to recognise it What to do about it Delirium
Symptom Management in Palliative Care Delirium and Pain Barry Lunny Registrar in Palliative Medicine Delirium outline What delirium is and why it is important How to recognise it What to do about it Delirium
Geriatric Grand Rounds
 Geriatric Grand Rounds Prevalence and Risk Factors of Delirium in Older Patients Admitted to a Community Based Acute Care Hospital Tuesday, October 27, 2009 12:00 noon Dr. Bill Black Auditorium Glenrose
Geriatric Grand Rounds Prevalence and Risk Factors of Delirium in Older Patients Admitted to a Community Based Acute Care Hospital Tuesday, October 27, 2009 12:00 noon Dr. Bill Black Auditorium Glenrose
Delirium. Information for patients, relatives and carers. Nursing and Patient Experience. Royal Surrey County Hospital. Patient information leaflet
 Patient information leaflet Royal Surrey County Hospital NHS Foundation Trust Delirium Information for patients, relatives and carers Nursing and Patient Experience What is delirium? Delirium is a word
Patient information leaflet Royal Surrey County Hospital NHS Foundation Trust Delirium Information for patients, relatives and carers Nursing and Patient Experience What is delirium? Delirium is a word
Falls Prevention Best Practice
 Falls Prevention Best Practice Prepared by Denise Tomassini Falls Prevention A case study : Mr Tony Topples ISLHD Clinical Quality Manager Clinical Governance Unit November 2011 Falls Prevention Best Practice
Falls Prevention Best Practice Prepared by Denise Tomassini Falls Prevention A case study : Mr Tony Topples ISLHD Clinical Quality Manager Clinical Governance Unit November 2011 Falls Prevention Best Practice
Community Pharmacy Dementia Audit
 Community Pharmacy Dementia Audit Introduction To comply with the NHS contractual requirements associated with the Clinical Governance Essential Service, pharmacy contractors must perform an annual practice
Community Pharmacy Dementia Audit Introduction To comply with the NHS contractual requirements associated with the Clinical Governance Essential Service, pharmacy contractors must perform an annual practice
DELIRIUM. Sabitha Rajan, MD, MSc, FHM Scott &White Healthcare Texas A&M Health Science Center School of Medicine
 DELIRIUM Sabitha Rajan, MD, MSc, FHM Scott &White Healthcare Texas A&M Health Science Center School of Medicine Disclosure Milliman Care Guidelines - Editor Objectives Define delirium Epidemiology Diagnose
DELIRIUM Sabitha Rajan, MD, MSc, FHM Scott &White Healthcare Texas A&M Health Science Center School of Medicine Disclosure Milliman Care Guidelines - Editor Objectives Define delirium Epidemiology Diagnose
DELIRIUM. Approach and Management
 DELIRIUM Approach and Management By Dr. K.S. Jacob, Professor of Psychiatry and Dr. Anju Kuruvilla, Professor of Psychiatry, Christian Medical College, Vellore. Based on a chapter in the book Psychiatric
DELIRIUM Approach and Management By Dr. K.S. Jacob, Professor of Psychiatry and Dr. Anju Kuruvilla, Professor of Psychiatry, Christian Medical College, Vellore. Based on a chapter in the book Psychiatric
The Agitated. Older Patient: old. What To Do? Michelle Gibson, MD, CCFP Presented at Brockville General Hospital Rounds, May 2003
 Focus on CME at Queen s University Focus on CME at Queen s University The Agitated The Older Patient: What To Do? Michelle Gibson, MD, CCFP Presented at Brockville General Hospital Rounds, May 2003 Both
Focus on CME at Queen s University Focus on CME at Queen s University The Agitated The Older Patient: What To Do? Michelle Gibson, MD, CCFP Presented at Brockville General Hospital Rounds, May 2003 Both
Do you know. Assessment of Delirium. What is Delirium? Which syndrome occurs more commonly in elderly populations? a. Delirium b.
 Assessment of Delirium Marianne McCarthy, PhD, GNP, PMHNP Arizona State University College of Nursing and Health Innovation What is Delirium? Delirium is a common clinical syndrome characterized by: Inattention
Assessment of Delirium Marianne McCarthy, PhD, GNP, PMHNP Arizona State University College of Nursing and Health Innovation What is Delirium? Delirium is a common clinical syndrome characterized by: Inattention
Delirium and Falls. Julia Poole CNC Aged Care RNSH
 Delirium and Falls Julia Poole CNC Aged Care RNSH Falls Risk Screening Tool Ontario STRATIFY NORTHERN SYDNEY CENTRAL COAST HEALTH Falls Risk Screening - Ontario STRATIFY Please read instructions for use
Delirium and Falls Julia Poole CNC Aged Care RNSH Falls Risk Screening Tool Ontario STRATIFY NORTHERN SYDNEY CENTRAL COAST HEALTH Falls Risk Screening - Ontario STRATIFY Please read instructions for use
Delirium Assessment. February 24, Susan Schumacher, MS, APRN-BC
 Delirium Assessment February 24, 2016 Susan Schumacher, MS, APRN-BC Objectives Define delirium Differentiate delirium from dementia Identify predisposing and precipitating factors leading to delirium.
Delirium Assessment February 24, 2016 Susan Schumacher, MS, APRN-BC Objectives Define delirium Differentiate delirium from dementia Identify predisposing and precipitating factors leading to delirium.
Tool 4a Multifactorial Falls Risk Screen (MFRS) and falls care plan (includes an osteoporosis risk screen)
 and falls care plan (includes an osteoporosis risk screen)") Tool 4a Multifactorial Falls Risk Screen (MFRS) and falls care plan (includes an osteoporosis risk screen) Name of resident: DOB: Room no.: Name of assessor: Date of assessment: Record all falls risks
Tool 4a Multifactorial Falls Risk Screen (MFRS) and falls care plan (includes an osteoporosis risk screen) Name of resident: DOB: Room no.: Name of assessor: Date of assessment: Record all falls risks
Delirium in Palliative care. Presentation to Volunteers 2016 David Falk
 Delirium in Palliative care Presentation to Volunteers 2016 David Falk Delirium What is delirium? Case Study - Delirium 60+ year old PQ presents to hospice very somnolent. She was admitted with her adult
Delirium in Palliative care Presentation to Volunteers 2016 David Falk Delirium What is delirium? Case Study - Delirium 60+ year old PQ presents to hospice very somnolent. She was admitted with her adult
BRAIN. Tumor byproducts. Autonomic nerves. Somatic nerves. Host immune cells. Cytokines
 Patient s Problems Pain (80%) Fatigue (90%) Weight Loss (80%) Lack of Appetite (80%) Nausea, Vomiting (90%) Anxiety (25%) Shortness of Breath (50%) Confusion-Agitation (80%) Tumor Mass Tumor Function Somatic
Patient s Problems Pain (80%) Fatigue (90%) Weight Loss (80%) Lack of Appetite (80%) Nausea, Vomiting (90%) Anxiety (25%) Shortness of Breath (50%) Confusion-Agitation (80%) Tumor Mass Tumor Function Somatic
Multifactorial falls risk assessment and management tool (includes an osteoporosis risk screen)
") Multifactorial falls risk assessment and management tool (includes an osteoporosis risk screen) Name of resident: DOB: Room no.: Name of assessor: Date of assessment: Record all risks and actions in the
Multifactorial falls risk assessment and management tool (includes an osteoporosis risk screen) Name of resident: DOB: Room no.: Name of assessor: Date of assessment: Record all risks and actions in the
SECTION 7: BECOMING CONFUSED AFTER AN OPERATION
 Risks associated with your anaesthetic SECTION 7: BECOMING CONFUSED AFTER AN OPERATION Anaesthesia and surgery are intended to give you relief from an illness or from pain and disability. However, these
Risks associated with your anaesthetic SECTION 7: BECOMING CONFUSED AFTER AN OPERATION Anaesthesia and surgery are intended to give you relief from an illness or from pain and disability. However, these
LEEDS TEACHING HOSPITALS TRUST
 LEEDS TEACHING HOSPITALS TRUST TITLE Clinical Guideline for the Diagnosis and Management of Delirium in adults. Guideline Detail Publication date: (to be completed by LHP staff) Next Review date: Status:
LEEDS TEACHING HOSPITALS TRUST TITLE Clinical Guideline for the Diagnosis and Management of Delirium in adults. Guideline Detail Publication date: (to be completed by LHP staff) Next Review date: Status:
Care of Patient with Delirium
 Care of Patient with Delirium Introduction Delirium is an alteration in consciousness involving confusion and other changes in cognitive ability that has a brief duration. 1 Patients specifically at risk
Care of Patient with Delirium Introduction Delirium is an alteration in consciousness involving confusion and other changes in cognitive ability that has a brief duration. 1 Patients specifically at risk
North Wales Critical Care Network
 North Wales Critical Care Network SEDATION GUIDELINES FOR ADULTS IN CRITICAL CARE Approved 6.9.12 1 Sedation guidelines for intensive care Betsi Cadwaladr University Health Board (Adapted from guidelines
North Wales Critical Care Network SEDATION GUIDELINES FOR ADULTS IN CRITICAL CARE Approved 6.9.12 1 Sedation guidelines for intensive care Betsi Cadwaladr University Health Board (Adapted from guidelines
The last days of life in hospital and at home
 The last days of life in hospital and at home Beaumont Multi-disciplinary Palliative Care Study Day 28/9/2017 Dr Sarah McLean Consultant in Palliative Medicine St Francis Hospice Beaumont Hospital Overview
The last days of life in hospital and at home Beaumont Multi-disciplinary Palliative Care Study Day 28/9/2017 Dr Sarah McLean Consultant in Palliative Medicine St Francis Hospice Beaumont Hospital Overview
Addressing Difficult Behaviors in Dementia
 Addressing Difficult Behaviors in Dementia GEORGE SCHOEPHOERSTER, MD GERIATRICIAN GENEVIVE/CENTRACARE CLINIC Objectives By the end of the session, you will be able to: 1) Explain the role of pain management
Addressing Difficult Behaviors in Dementia GEORGE SCHOEPHOERSTER, MD GERIATRICIAN GENEVIVE/CENTRACARE CLINIC Objectives By the end of the session, you will be able to: 1) Explain the role of pain management
Delirium in the Elderly
 Delirium in the Elderly Jeffrey M. Burock, MD Division Director/ Psychiatry / Miriam Hospital Clinical Assistant Professor Warren Alpert School Of Medicine Learning Objectives Identify the symptoms of
Delirium in the Elderly Jeffrey M. Burock, MD Division Director/ Psychiatry / Miriam Hospital Clinical Assistant Professor Warren Alpert School Of Medicine Learning Objectives Identify the symptoms of
FOR RESIDENTIAL FACILITIES
 AGED CASP 1a - APMHS REFERRAL ACASP 1a AGED PERSONS MENTAL HEALTH SERVICE REFERRAL FOR RESIDENTIAL FACILITIES Surname:. Rapid UR:. Given names:... D.O.B.:. Sex: Address: Phone:.. Medicare Number:. Date
AGED CASP 1a - APMHS REFERRAL ACASP 1a AGED PERSONS MENTAL HEALTH SERVICE REFERRAL FOR RESIDENTIAL FACILITIES Surname:. Rapid UR:. Given names:... D.O.B.:. Sex: Address: Phone:.. Medicare Number:. Date
PSYCHOTROPIC SOLUTIONS
 PSYCHOTROPIC SOLUTIONS A proactive approach to antipsychotic medication management A Quality Use of Medicines initiative by Choice Aged Care Copyright 2018 Key Senate Committee Recommendations: All RACF
PSYCHOTROPIC SOLUTIONS A proactive approach to antipsychotic medication management A Quality Use of Medicines initiative by Choice Aged Care Copyright 2018 Key Senate Committee Recommendations: All RACF
BGS Autumn Delirium: Recognition, prevention, management
 Delirium: Recognition, prevention, management Dr Tizzy Teale Senior Clinical Lecturer and Honorary Consultant Geriatrician University of Leeds and Bradford Teaching Hospitals NHS Trust How common is delirium?
Delirium: Recognition, prevention, management Dr Tizzy Teale Senior Clinical Lecturer and Honorary Consultant Geriatrician University of Leeds and Bradford Teaching Hospitals NHS Trust How common is delirium?
Appendix 1: Service self-assessment
 Appendix 1: Service self-assessment Frailty Screening Are we delivering high-quality care for frail older people? We are assessing for frailty in people aged 65+ at every entry into the service using a
Appendix 1: Service self-assessment Frailty Screening Are we delivering high-quality care for frail older people? We are assessing for frailty in people aged 65+ at every entry into the service using a
5 older patients become delirious every minute
 Management of Delirium: Nonpharmacologic and Pharmacologic Approaches Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley
Management of Delirium: Nonpharmacologic and Pharmacologic Approaches Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley
Assessment and early identification
 The Right Care: creating dementia friendly hospitals Assessment and early identification Good practice for better care 1 Assessment and early identification Section 1 Self assessment statements from National
The Right Care: creating dementia friendly hospitals Assessment and early identification Good practice for better care 1 Assessment and early identification Section 1 Self assessment statements from National
Critical Care Pharmacological Management of Delirium
 Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Delirium and Dementia. Summary
 Delirium and Dementia Paul Kettl, M.D., M.H.A. Summary DELIRIUM Acute brain failure Identify cause (meds, infection) Treat sx Poor prognostic sign DEMENTIA Chronic brain failure AD most common cause Often
Delirium and Dementia Paul Kettl, M.D., M.H.A. Summary DELIRIUM Acute brain failure Identify cause (meds, infection) Treat sx Poor prognostic sign DEMENTIA Chronic brain failure AD most common cause Often
Palliative Care and Delirium. Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care
 Palliative Care and Delirium Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care Disclosures I have no personal or professional financial relationships
Palliative Care and Delirium Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care Disclosures I have no personal or professional financial relationships
Dementia NICE Guidelines Update. Key points for primary care - NICE guideline (June 2018 update ) 26 September 2018
 26 September 2018") Dementia NICE Guidelines Update Key points for primary care - NICE guideline (June 2018 update ) 26 September 2018 How NICE guidelines are reviewed Multidisciplinary guideline committee established Review
Dementia NICE Guidelines Update Key points for primary care - NICE guideline (June 2018 update ) 26 September 2018 How NICE guidelines are reviewed Multidisciplinary guideline committee established Review
Sedation and Delirium Questions
 Sedation and Delirium Questions TLC Curriculum William J. Ehlenbach, MD MSc Assistant Professor of Medicine Pulmonary & Critical Care Medicine Question 1 Deep sedation in ventilated critically patients
Sedation and Delirium Questions TLC Curriculum William J. Ehlenbach, MD MSc Assistant Professor of Medicine Pulmonary & Critical Care Medicine Question 1 Deep sedation in ventilated critically patients
UHSM ED Pathway ELDERLY FALL / COLLAPSE
 UHSM ED Pathway ELDERLY FALL / COLLAPSE Patient name / Pathway for patients who require assessment in ED after a fall or collapse Note: - It can be used if the patient has also sustained a minor head injury
UHSM ED Pathway ELDERLY FALL / COLLAPSE Patient name / Pathway for patients who require assessment in ED after a fall or collapse Note: - It can be used if the patient has also sustained a minor head injury
Delirium in the Emergency Department. Emergency Medicine Rounds April 14, 2015 Paul R. Vanhoutte
 Delirium in the Emergency Department Emergency Medicine Rounds April 14, 2015 Paul R. Vanhoutte Goals of Rounds: Review Definition Management An Understanding What is important is to spread confusion,
Delirium in the Emergency Department Emergency Medicine Rounds April 14, 2015 Paul R. Vanhoutte Goals of Rounds: Review Definition Management An Understanding What is important is to spread confusion,
Think Delirium. Dr Linda Wolff Scotland
 Think Delirium Dr Linda Wolff Scotland Delirium Management Pathway Scottish Delirium Association: Linda Wolff and Brian McGurn Health Improvement Scotland: Michelle Millar and Karen Goudie Outline Patrick
Think Delirium Dr Linda Wolff Scotland Delirium Management Pathway Scottish Delirium Association: Linda Wolff and Brian McGurn Health Improvement Scotland: Michelle Millar and Karen Goudie Outline Patrick
Delirium in Older Persons
 Objectives Delirium in Older Persons ELITE 2018 Liza Isabel Genao, MD Division of Geriatrics Describe rate, cost, complications of delirium Effectively diagnose the syndrome Describe multicomponent model
Objectives Delirium in Older Persons ELITE 2018 Liza Isabel Genao, MD Division of Geriatrics Describe rate, cost, complications of delirium Effectively diagnose the syndrome Describe multicomponent model
Delirium: Information for Patients and Families
 health information Delirium: Information for Patients and Families 605837 Alberta Health Services, (2016/11) Resources Delirium in the Older Person Family Guide: search delirium at viha.ca Go to myhealth.alberta.ca
health information Delirium: Information for Patients and Families 605837 Alberta Health Services, (2016/11) Resources Delirium in the Older Person Family Guide: search delirium at viha.ca Go to myhealth.alberta.ca
SCE Revision Course Geriatric Medicine & Other
 SCE Revision Course Geriatric Medicine & Other Geriatric Medicine: what the curriculum says you should know Physiology of ageing Atypical presentations: the Geriatric Giants Falls and fragility fractures
SCE Revision Course Geriatric Medicine & Other Geriatric Medicine: what the curriculum says you should know Physiology of ageing Atypical presentations: the Geriatric Giants Falls and fragility fractures
Delirium Pilot Project
 CCU Nurses: Delirium Pilot Project Our unit has been selected to develop and implement a delirium assessment and intervention program. We are beginning Phase 1 with education and assessing for our baseline
CCU Nurses: Delirium Pilot Project Our unit has been selected to develop and implement a delirium assessment and intervention program. We are beginning Phase 1 with education and assessing for our baseline
Delirium Avoid it Recognize it Find the cause of it
 Delirium Delirium is acute cognitive dysfunction. It has a 20% - 30 day mortality (usually because of underlying conditions). It is associated with increased lengths of hospital stay, increased disability,
Delirium Delirium is acute cognitive dysfunction. It has a 20% - 30 day mortality (usually because of underlying conditions). It is associated with increased lengths of hospital stay, increased disability,
Delirium Screening: The next nurse sensitive indicator?
 Delirium Screening: The next nurse sensitive indicator? Sharon Gunn, MSN, MA, RN, ACNS-BC, CCRN Clinical Nurse Specialist Critical Care Baylor University Medical Center Dallas, TX Objectives Recognize
Delirium Screening: The next nurse sensitive indicator? Sharon Gunn, MSN, MA, RN, ACNS-BC, CCRN Clinical Nurse Specialist Critical Care Baylor University Medical Center Dallas, TX Objectives Recognize
DELIRIUM. J. Sukanya 28.Jun.12
 DELIRIUM J. Sukanya 28.Jun.12 Outline Why? What? How? What s next? Delirium Introduction Delirium An acute decline in attention and cognition The most frequent neuropsychiatric syndrome A common, life-threatening,
DELIRIUM J. Sukanya 28.Jun.12 Outline Why? What? How? What s next? Delirium Introduction Delirium An acute decline in attention and cognition The most frequent neuropsychiatric syndrome A common, life-threatening,
Objectives. Symptom Management in the Frail Elderly Population. Disclosures. Symptom Management: Pain 12/05/2014
 Objectives Symptom Management in the Frail Elderly Population Dr. Katie Marchington, MD, CCFP Palliative Care Physician Toronto Western Hospital Kensington Hospice To reflect on why we should identify
Objectives Symptom Management in the Frail Elderly Population Dr. Katie Marchington, MD, CCFP Palliative Care Physician Toronto Western Hospital Kensington Hospice To reflect on why we should identify
Delirium. Assessment and Management
 Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Chapter 01 Introduction
 Chapter 01 Introduction Defining the Elderly There is no universally accepted age cut-off defining elderly. This reflects the fact that chronological age itself is less important than biological events
Chapter 01 Introduction Defining the Elderly There is no universally accepted age cut-off defining elderly. This reflects the fact that chronological age itself is less important than biological events
Delirium: Advanced Liaison Psychiatry 2018
 Delirium: Advanced Liaison Psychiatry 2018 Dr Tom Smith Consultant Liaison Psychiatrist Delirium reasons for referral to liaison psychiatry Can you arrange for a psychiatric admission? How do we stop this
Delirium: Advanced Liaison Psychiatry 2018 Dr Tom Smith Consultant Liaison Psychiatrist Delirium reasons for referral to liaison psychiatry Can you arrange for a psychiatric admission? How do we stop this
Fractured Neck of Femur Proforma Orthopaedic Unit. First name: Registration no: Date of birth: Age:
 Fractured Neck of Femur Proforma Orthopaedic Unit Date: Surname : ED doctor s name: Time seen: Orthopaedic admitting doctor s name: Time seen: Presenting complaint and history of fall: First name: Registration
Fractured Neck of Femur Proforma Orthopaedic Unit Date: Surname : ED doctor s name: Time seen: Orthopaedic admitting doctor s name: Time seen: Presenting complaint and history of fall: First name: Registration
Ohio/Minnesota Collaborative
 Ohio/Minnesota Collaborative Place picture here Delirium Prevention Virtual Learning Session February 24, 2016 Delirium collaboration Ohio and Minnesota HENs In December 2015, the Minnesota and Ohio HENS
Ohio/Minnesota Collaborative Place picture here Delirium Prevention Virtual Learning Session February 24, 2016 Delirium collaboration Ohio and Minnesota HENs In December 2015, the Minnesota and Ohio HENS
Confusion in Hospital Patients. Dr Nicola Lovett, Geratology Consultant OUH
 Confusion in Hospital Patients Dr Nicola Lovett, Geratology Consultant OUH I'm one of the geratology consultants working here at the John Radcliffe. This is a really wonderful opportunity for us to tell
Confusion in Hospital Patients Dr Nicola Lovett, Geratology Consultant OUH I'm one of the geratology consultants working here at the John Radcliffe. This is a really wonderful opportunity for us to tell
Managing medicines in older people. Jane Noble and Caroline Ralph
 Managing medicines in older people Jane Noble and Caroline Ralph Where? Community Hospital Care Home What? Prescribing Dispensing Administering Case 1 84 year old lady Admitted with reduced mobility Recurrent
Managing medicines in older people Jane Noble and Caroline Ralph Where? Community Hospital Care Home What? Prescribing Dispensing Administering Case 1 84 year old lady Admitted with reduced mobility Recurrent
Preventing delirium while in hospital Tips for family, whānau, and friends who are supporting an older person
 Preventing delirium while in hospital Tips for family, whānau, and friends who are supporting an older person This brochure shares some simple ways you can help our care staff to prevent delirium, recognize
Preventing delirium while in hospital Tips for family, whānau, and friends who are supporting an older person This brochure shares some simple ways you can help our care staff to prevent delirium, recognize
How to prevent delirium in the Emergency Room. Nice September 21, 2017 Steffen Schlee/ Katrin Singer
 How to prevent delirium in the Emergency Room Nice September 21, 2017 Steffen Schlee/ Katrin Singer CONFLICT OF INTEREST DISCLOSURE K. Singler and St. Schlee have no potential conflict of interest to report.
How to prevent delirium in the Emergency Room Nice September 21, 2017 Steffen Schlee/ Katrin Singer CONFLICT OF INTEREST DISCLOSURE K. Singler and St. Schlee have no potential conflict of interest to report.
Cognitive disorders. Dr S. Mashaphu Department of Psychiatry
 Cognitive disorders Dr S. Mashaphu Department of Psychiatry Delirium Syndrome characterised by: Disturbance of consciousness Impaired attention Change in cognition Develops over hours-days Fluctuates during
Cognitive disorders Dr S. Mashaphu Department of Psychiatry Delirium Syndrome characterised by: Disturbance of consciousness Impaired attention Change in cognition Develops over hours-days Fluctuates during
OVoiD delirium and improved outcomes in acute care. Introducing a model of care
 OVoiD delirium and improved outcomes in acute care. Introducing a model of care AUTHOR Anne Hoolahan MA, GradDipApSc Gerontology, GradDipHlthSc Nursing, DipTeach Clinical Nurse Consultant Dementia, Northern
OVoiD delirium and improved outcomes in acute care. Introducing a model of care AUTHOR Anne Hoolahan MA, GradDipApSc Gerontology, GradDipHlthSc Nursing, DipTeach Clinical Nurse Consultant Dementia, Northern
Improving Delirium Management: Mapping Out One Unit s Journey. Geriatrics Institute June 27, 2013
 Improving Delirium Management: Mapping Out One Unit s Journey Geriatrics Institute June 27, 2013 Rebecca Ramsden, NP Mary Ann Hamelin, CNS Susanne Loay, RN Objectives Background RNAO Best Practice Guideline
Improving Delirium Management: Mapping Out One Unit s Journey Geriatrics Institute June 27, 2013 Rebecca Ramsden, NP Mary Ann Hamelin, CNS Susanne Loay, RN Objectives Background RNAO Best Practice Guideline
Accompanied to walk Yes No Accompanied to walk Yes No Side of Fracture
 Fracture Neck Of Femur / Fast Track Criteria: Admission where femoral neck fracture is the primary diagnosis Accident & Emergency Assessment (To be completed by A/E Nurse and/or A/E doctor) Patient label
Fracture Neck Of Femur / Fast Track Criteria: Admission where femoral neck fracture is the primary diagnosis Accident & Emergency Assessment (To be completed by A/E Nurse and/or A/E doctor) Patient label