Maternal Physiology and the Anesthetized Pregnant Patient. Kimberly Babiash, MD, MBA Oct 7, 2015
|
|
|
- Ashley White
- 6 years ago
- Views:
Transcription
1 Maternal Physiology and the Anesthetized Pregnant Patient Kimberly Babiash, MD, MBA Oct 7, 2015
2 Overview Neuraxial Anesthesia Epidurals vs spinals How they work Physiologic alterations Contraindications Patient factors Febrile patient Pre-eclampsia Anesthetic choices for Cesarean Sections Neuraxial vs General Anesthesia Physiologic alterations and why they matter Gastric emptying Airway Hemodynamic control

3 Epidural and Spinals

4 Neuraxial Anatomy


5 Neuraxial Anatomy
6 Epidurals Understanding Neuraxial Anesthesia Slow onset Long duration VOLUME dependent Better hemodynamic control Spinals Rapid onset Short duration DOSE (mass) dependent Poor hemodynamic control

7 Understanding Neuraxial anesthesia How do local anesthetics work?
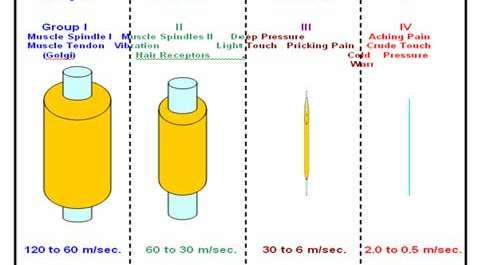
8 Understanding Neuraxial Differential Blockade Anesthesia clinical phenomenon that nerve fibers with different functions have different sensitivities to local anesthetic blockade. Length of each nerve in the thecal space Depth of the nerve fiber Distribution of Na+ and K+ channels on each nerve type

9 Understanding Neuraxial Anesthesia
10 Understanding Neuraxial Differential Blockade Anesthesia Sympathetics: most sensitive to local anesthetic agents (2-4 levels beyond motor) Pain/touch: moderately sensitive (2-3 levels beyond motor) Motor fibers: least sensitive
11 Dermatome goals Labor (T10 usually achieved with ml) Stage I = T10 L1 Stage II = S2-S4 Cesarean Section T2-S4 (higher for exteriorization of uterus) Pain sensations from pelvic organs and visceral pain fibers from other abdominal structures including the peritoneum enter spinal cord at T10-L1; however, some pelvic nerves accompany sympathetic fibers to reach the spinal cord as far as T2 Traction on uterosacral ligaments and bladder require anesthesia as low as S4 Achieved with dose of 12 mg bupivacaine
12 Why add neuraxial opioids?
13 Factors affecting block height Dose Site of injection Baricity Dextrose added for hyperbaric (sinks) Position of patient Extremes of height (minor) Lumbosacral CSF volume (interindividual variability) Explains variability in spinal with similar doses
14 Physiologic Disturbances with Neuraxial Anesthesia Cardiovascular disturbances take the cake Hyotension and bradycardia (33% and 13%) Primary Cause = Sympathectomy SNS arises from the middle of the SC in the interomedial nucleus of the lateral grey column beginning at T1 and extends to L2 (thoracolumbar outflow) Extends approx 2 dermatomes above the sensory level Venous and arterial dilation Venodilation predominates (75% of TBV) Redistributes central blood volume to splanchnics and lower extremities Vascular smooth muscle on the arterial side retains considerable tone If normal cardiac output is maintained, PVR should only decrease by 15% in the normovolemic patient
15 Physiologic Disturbances with Neuraxial Anesthesia Modulation of vasomotor tone A complex process that relies on much more than just simple augmentation or attenuation of SNS Simple thought: hypotension should lead to reflex tachycardia and vasoconstriction. But bradycardia is more commom. Shift towards vagal predominance Level of block? Cardioaccelerator fibers (t1-t4) Bezold Jarisch Reflex (a cardioinhibitory reflex) Mechano/chemosensitive receptors located in the ventricles Involved in the restorative response to reduced cardiac filling A sudden decrease in VR and PVR triggers bradycardia to preserve cardiac filling
16 Physiologic Disturbances with Neuraxial Anesthesia Respiratory Effects Decrease in Vital Capacity (IRV+ VT +ERV) due to decrease in ERV from paralysis of abdominal muscles necessary for forced expiration Nothing to do with diaphragm or phrenic nerve Therefore, expiration >inspiration Consideration for severe asthmatic High Spinal and respiratory arrest Unrelated to phrenic nerve or respiratory function Hypoperfusion of the respiratory centers of the brainstem

17 Respiratory Volumes in Pregnancy
18 Contraindications Absolute Patient refusal Obstructive intracranial hypertension Infection at the site Frank coagulopathy
19 Regional Anesthesia in the infected febrile patient Despite the apparent low risk of central nervous system infection after regional anesthesia, anesthesiologists have long considered sepsis to be a relative contraindication to the administration of spinal or epidural anesthesia. Sepsis = SIRS + suspected or documented infection There is no evidence to suggest that neuraxial anesthesia is contraindicated in chorioamnionitis alone
20 Recommendations: Serious central neuraxial infections such as arachnoiditis, meningitis, and abscess after spinal or epidural anesthesia are rare (Grade B). The decision to perform a regional anesthetic technique must be made on an individual basis considering the anesthetic alternatives, the benefits of regional anesthesia, and the risk of CNS infection (which may theoretically occur in any bacteremic patient) (Grade C). Despite conflicting results, many experts suggest that, except in the most extraordinary circumstances, central neuronal block should not be performed in patients with untreated systemic infection (Grade C). Available data suggest that patients with evidence of systemic infection may safely undergo spinal anesthesia, provided appropriate antibiotic therapy is initiated before dural puncture and the patient has shown a response to therapy, such as a decrease in fever (placement of an indwelling epidural (or intrathecal) catheter in this group of patients remains controversial) (Grade A).
21 Anesthetic Choices for Cesarean Delivery Neuraxial vs General Anesthesia (GA) Considerations GA fastest induction to delivery time GA lower APGAR scores Neuraxial is preferred to GA in most cases study done by Mancuso et al. (Spinal vs GA) 179 healthy elective Umbilical cord artery ph, Apgar score and need for assisted ventilation were evaluated and found spinal anesthesia superior to general in fetal outcome.
22 Anesthetic Choices for Cesarean Delivery The relative risk of fatality during GA has increased to more than 8 times that for regional anesthesia Failed intubation incidence of failed intubation in OB patient is 1:300 whereas incidence in general population is 1:2,230 (8 fold increased risk) Increased difficulty (vascular engorgement, obesity, breast size, preeclampsia) Rapid time to desaturation Increased oxygen consumption and decreased FRC Pulmonary aspiration *see next slide Maternal awareness Neonatal depression
23 Gastric Changes in Pregnancy Decreased tone and motility progesterone possibly due to decreased levels of motility Conflicting info about delayed gastric emptying Reduced tone of the gastroesophageal junction sphincter Increased intraabdominal pressure leads to acid reflux
24 Preeclampsia and Neuraxial 1950s evidence that preeclampsia actually attenuates spinal-anesthesia hypotension 1990s clinical trials demonstrate safety of spinals in this population 3 prospective trials Less severe and less frequent hypotension and smaller doses of vasopressors Early epidural placement in laboring preeclamptic parturients is ideal Complications of GA Hypertensive crisis (common with RSI) Stroke (difficult to recognize under GA; conflict in management between RSI and deep plane of anesthesia/stable induction to maintain CBF) Difficult airway management (pharyngeal and subglottic edema along with traumatic laryngoscopy and further bleeding)
25 Preeclampsia and Neuraxial Spinal compared to GA in severe preeclampsia with nonreassuring FHT Dyer et al: 70 parturients prospectively compared Spinal greater mean neonatal umbilical artery base deficit (7.1 vs 4.7) and lower median umbilical artery ph (7.2 vs 7.23) Spinal group had higher ephedrine use (fetal ph) 1 min APGAR significantly lower in GA (but at 5 min no statistical difference) No significant intergroup differences in other markers of neonatal compromise Need for resuscitation, APGAR <7, ph <7.2, need for PPV
26 Anesthetic Choices for Cesarean Delivery GA APGAR scores are lower at 1 and 5 min Equivocal regarding differences in umbilical artery ph values Reduces the time to skin incision Greater maternal complications Epidural Increases time to skin incision Reduces the quality of anesthesia compared to spinal CSE vs epidural No difference in frequency of hypotension or 1 minute APGAR Better anesthesia Faster time to skin incision

27 Failed Epidural, Now What? Epidural anesthesia is less reliable that spinal Concern with spinal after a failed epidural High spinal from compression of intrathecal space Especially when >20 ml in epidural space less than 30 minutes before spinal Reduction in spinal dose of 20-30%
28 Anesthetic Medications Volatile anesthetics Dose dependent decrease in uterine smooth muscle contractility and blood flow Propofol Only modest at 0.5 MAC Rapidly cross placenta but quickly exhaled in neonate GABA agonist Potent myocardial depressant and inhibits sympathetic tone Distributes quickly to the vessel rich placenta Studies with barbiturates indicate optimal timing of fetal delivery 4-8 minutes post induction However, in a poorly perfused placenta, time is of the essence
29 Pre-induction Fentanyl? Peak effect 3-5 minutes Rapid placental transfer Though not associated with lower umbilical artery ph or APGAR scores after 1mcg/kg on induction
30 Nitrous? Peak effect lags the start of its administration by 50 sec Uterine contractions typically peak 30 sec after they start Reductions in pain scores seem similar to that of systemic opioids, which some authors suggest have little effect on labor pain Its use does not seem to appreciably affect the rates of maternal nausea or emesis during labor The direct respiratory depressant effect along with maternal hypocapnea may increases the rate of maternal oxygen desaturation between contractions It does NOT affect uterine contractility The effects of the fetus exposed to nitrous in utero is unknown With rising concern about the subtle long-term effects of perinatally administered anesthetics, the role of nitrous certainly demands judiciuos scrutiny

31 Thank You!
Maternal and Fetal Physiology
 Background Maternal and Fetal Physiology Anderson Lo, DO Fellow, Maternal-Fetal Medicine Wayne State University School of Medicine SEMCME Fetal Assessment Course July 20, 2018 Oxygen pathway Mother Placenta
Background Maternal and Fetal Physiology Anderson Lo, DO Fellow, Maternal-Fetal Medicine Wayne State University School of Medicine SEMCME Fetal Assessment Course July 20, 2018 Oxygen pathway Mother Placenta
Pain Management for Labour and Delivery
 Indu Singh, MD FRCPC 1 Existence of Labour Pain Pain Management for Labour and Delivery The existence of chronic pain, which often lacks an obvious outward cause, is now unquestioned Michelle Gros MD FRCPC
Indu Singh, MD FRCPC 1 Existence of Labour Pain Pain Management for Labour and Delivery The existence of chronic pain, which often lacks an obvious outward cause, is now unquestioned Michelle Gros MD FRCPC
Cardiovascular Effects of Anesthesia for Cesarean Delivery in the Cardiac Patient
 Cardiovascular Effects of Anesthesia for Cesarean Delivery in the Cardiac Patient Katherine W. Arendt, M.D. Associate Professor of Anesthesiology Mayo Clinic, Rochester, Minnesota Cardiac Problems in Pregnancy
Cardiovascular Effects of Anesthesia for Cesarean Delivery in the Cardiac Patient Katherine W. Arendt, M.D. Associate Professor of Anesthesiology Mayo Clinic, Rochester, Minnesota Cardiac Problems in Pregnancy
Epidural Analgesia in Labor - Whats s New
 Epidural Analgesia in Labor - Whats s New Wichelewski Josef 821 Selective neural blockade has many clinical applications in medicine but nowhere has its use been so well accepted than in the field of Obstetrics.
Epidural Analgesia in Labor - Whats s New Wichelewski Josef 821 Selective neural blockade has many clinical applications in medicine but nowhere has its use been so well accepted than in the field of Obstetrics.
ANESTHESIA EXAM (four week rotation)
") SPARROW HEALTH SYSTEM ANESTHESIA SERVICES ANESTHESIA EXAM (four week rotation) Circle the best answer 1. During spontaneous breathing, volatile anesthetics A. Increase tidal volume and decrease respiratory
SPARROW HEALTH SYSTEM ANESTHESIA SERVICES ANESTHESIA EXAM (four week rotation) Circle the best answer 1. During spontaneous breathing, volatile anesthetics A. Increase tidal volume and decrease respiratory
HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT.
 HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT. Donna M. Sisak, CVT, LVT, VTS (Anesthesia/Analgesia) Seattle Veterinary Specialists Kirkland, WA dsisak@svsvet.com THE ANESTHETIZED PATIENT
HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT. Donna M. Sisak, CVT, LVT, VTS (Anesthesia/Analgesia) Seattle Veterinary Specialists Kirkland, WA dsisak@svsvet.com THE ANESTHETIZED PATIENT
Post-Anesthesia Care In the ICU
 Post-Anesthesia Care In the ICU The following is based on current research and regional standards of care. At completion you will be able to identify Basic equipment needed at the bedside. Aldrete scoring
Post-Anesthesia Care In the ICU The following is based on current research and regional standards of care. At completion you will be able to identify Basic equipment needed at the bedside. Aldrete scoring
General anesthesia. No single drug capable of achieving these effects both safely and effectively.
 General anesthesia General anesthesia is essential to surgical practice, because it renders patients analgesic, amnesia, and unconscious reflexes, while causing muscle relaxation and suppression of undesirable
General anesthesia General anesthesia is essential to surgical practice, because it renders patients analgesic, amnesia, and unconscious reflexes, while causing muscle relaxation and suppression of undesirable
Introduction to Obstetric Anesthesia
 Introduction to Obstetric Anesthesia Dr A Alberts Department of Anesthesiology and Critical Care 2007 INTRODUCTION During obstetric anesthesia the anesthetist controls the following Maternal Gas exchange,
Introduction to Obstetric Anesthesia Dr A Alberts Department of Anesthesiology and Critical Care 2007 INTRODUCTION During obstetric anesthesia the anesthetist controls the following Maternal Gas exchange,
Supplemental Digital Content: Definitions Based on the International Classification of Diseases, Ninth Revision, Clinical Modification
 Supplemental Digital Content: Definitions Based on the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) Diagnose and Procedures Codes 1. ICD-9-CM definition of
Supplemental Digital Content: Definitions Based on the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) Diagnose and Procedures Codes 1. ICD-9-CM definition of
FHR Monitoring: Maternal Fetal Physiology
 FHR Monitoring: Maternal Fetal Physiology M. Sean Esplin, MD and Alexandra Eller, MD Maternal Fetal Medicine Intermountain Healthcare University of Utah Health Sciences Center Disclosures I have no financial
FHR Monitoring: Maternal Fetal Physiology M. Sean Esplin, MD and Alexandra Eller, MD Maternal Fetal Medicine Intermountain Healthcare University of Utah Health Sciences Center Disclosures I have no financial
Practice Guidelines for Obstetric Anesthesia
 Anesthesiology 2007; 106:843 63 Copyright 2007, the American Society of Anesthesiologists, Inc. Lippincott Williams & Wilkins, Inc. Practice Guidelines for Obstetric Anesthesia An Updated Report by the
Anesthesiology 2007; 106:843 63 Copyright 2007, the American Society of Anesthesiologists, Inc. Lippincott Williams & Wilkins, Inc. Practice Guidelines for Obstetric Anesthesia An Updated Report by the
Regional Anesthesia. Fatiş Altındaş Dept. of Anesthesiology
 Regional Anesthesia Fatiş Altındaş Dept. of Anesthesiology Regional anesthesia - Definition Renders a specific area of the body, e.g. foot, arm, lower extremities insensating to stimulus of surgery or
Regional Anesthesia Fatiş Altındaş Dept. of Anesthesiology Regional anesthesia - Definition Renders a specific area of the body, e.g. foot, arm, lower extremities insensating to stimulus of surgery or
Nothing to Disclose. Severe Pulmonary Hypertension
 Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Pharmacologic Pain Relief: It s Use in Labor. Linda Robinson MSN, RNC Clinical Nurse Specialist, Northwest Hospital Spring, 2016
 Pharmacologic Pain Relief: It s Use in Labor Linda Robinson MSN, RNC Clinical Nurse Specialist, Northwest Hospital Spring, 2016 Objectives Recognize common medications used in the management of labor pain
Pharmacologic Pain Relief: It s Use in Labor Linda Robinson MSN, RNC Clinical Nurse Specialist, Northwest Hospital Spring, 2016 Objectives Recognize common medications used in the management of labor pain
Spinal anesthesia without hypotension a myth or reality?
 Spinal anesthesia without hypotension a myth or reality? Peter Poredoš, MD, PhD, DESA peter.poredos@kclj.si University Medical Centre Ljubljana, Slovenia Department for Anesthesiology and Intensive Care
Spinal anesthesia without hypotension a myth or reality? Peter Poredoš, MD, PhD, DESA peter.poredos@kclj.si University Medical Centre Ljubljana, Slovenia Department for Anesthesiology and Intensive Care
PAAQS Reference Guide
 Q. 1 Patient's Date of Birth (DOB) *Required Enter patient's date of birth PAAQS Reference Guide Q. 2 Starting Anesthesiologist *Required Record the anesthesiologist that started the case Q. 3 Reporting
Q. 1 Patient's Date of Birth (DOB) *Required Enter patient's date of birth PAAQS Reference Guide Q. 2 Starting Anesthesiologist *Required Record the anesthesiologist that started the case Q. 3 Reporting
Pharmacologic Pain Relief: It s Use in Labor
 Pharmacologic Pain Relief: It s Use in Labor Linda Robinson MSN, RNC Clinical Nurse Specialist, Northwest Hospital Fall, 2016 Objectives Recognize common medications used in the management of labor pain
Pharmacologic Pain Relief: It s Use in Labor Linda Robinson MSN, RNC Clinical Nurse Specialist, Northwest Hospital Fall, 2016 Objectives Recognize common medications used in the management of labor pain
EQUIPMENT: Nitrous Oxygen Delivery System:
 Policy: Nitrous Oxide Use in the Intrapartum and Immediate Postpartum Period for Obstetrical Patients in the Family Birth Place Approvers: CEO. CNO, Medical Staff President, Anesthesia Chair, OB Medical
Policy: Nitrous Oxide Use in the Intrapartum and Immediate Postpartum Period for Obstetrical Patients in the Family Birth Place Approvers: CEO. CNO, Medical Staff President, Anesthesia Chair, OB Medical
MD (Anaesthesiology) Title (Plan of Thesis) (Session )
 Title (Plan of Thesis) (Session )") S.No. 1. COMPARATIVE STUDY OF CENTRAL VENOUS CANNULATION USING ULTRASOUND GUIDANCE VERSUS LANDMARK TECHNIQUE IN PAEDIATRIC CARDIAC PATIENT. 2. TO EVALUATE THE ABILITY OF SVV OBTAINED BY VIGILEO-FLO TRAC
S.No. 1. COMPARATIVE STUDY OF CENTRAL VENOUS CANNULATION USING ULTRASOUND GUIDANCE VERSUS LANDMARK TECHNIQUE IN PAEDIATRIC CARDIAC PATIENT. 2. TO EVALUATE THE ABILITY OF SVV OBTAINED BY VIGILEO-FLO TRAC
Regional Anaesthesia for Caesarean Section
 Regional Anaesthesia for Caesarean Section "The Best Recipe" Warwick D. Ngan Kee Dept of Anaesthesia & Intensive Care The Chinese University of Hong Kong What I will not do. Magic recipes One shoe to fit
Regional Anaesthesia for Caesarean Section "The Best Recipe" Warwick D. Ngan Kee Dept of Anaesthesia & Intensive Care The Chinese University of Hong Kong What I will not do. Magic recipes One shoe to fit
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 14 Practical Anesthesia Key Points 2 14.1 General Anesthesia Have a clear plan before starting anesthesia Never use an unfamiliar anesthetic technique in an emergency
Surgical Care at the District Hospital 1 14 Practical Anesthesia Key Points 2 14.1 General Anesthesia Have a clear plan before starting anesthesia Never use an unfamiliar anesthetic technique in an emergency
What s new in obstetric anesthesia?
 SAOA 2013 - SPRING MEETING BERN What s new in obstetric anesthesia? PD Dr. Med Georges Savoldelli Médecin Adjoint Unité d anesthésiologie gynéco-obstétricale Service d Anesthésiologie, HUG An objectively
SAOA 2013 - SPRING MEETING BERN What s new in obstetric anesthesia? PD Dr. Med Georges Savoldelli Médecin Adjoint Unité d anesthésiologie gynéco-obstétricale Service d Anesthésiologie, HUG An objectively
Combined spinalepidural. epidural analgesia in labour (review) By Neda Taghizadeh
 By Neda Taghizadeh") Combined spinalepidural versus epidural analgesia in labour (review) By Neda Taghizadeh Cochrane review Cochrane collaboration was founded in 1993 and is named after Archie Cochrane (1909-1988), British
Combined spinalepidural versus epidural analgesia in labour (review) By Neda Taghizadeh Cochrane review Cochrane collaboration was founded in 1993 and is named after Archie Cochrane (1909-1988), British
Case Report A Rare Case of C2 Sensory Blockade with Preserved Phrenic Nerve Function in an Obstetric Patient
 Case Reports in Anesthesiology Volume 2016, Article ID 3064373, 4 pages http://dx.doi.org/10.1155/2016/3064373 Case Report A Rare Case of C2 Sensory Blockade with Preserved Phrenic Nerve Function in an
Case Reports in Anesthesiology Volume 2016, Article ID 3064373, 4 pages http://dx.doi.org/10.1155/2016/3064373 Case Report A Rare Case of C2 Sensory Blockade with Preserved Phrenic Nerve Function in an
Anesthesia Final Exam
 Anesthesia Final Exam 1) For a patient who is chronically taking the following medications, which two should be withheld on the day of surgery? a) Lasix b) Metoprolol c) Glucophage d) Theodur 2) A 51 year
Anesthesia Final Exam 1) For a patient who is chronically taking the following medications, which two should be withheld on the day of surgery? a) Lasix b) Metoprolol c) Glucophage d) Theodur 2) A 51 year
The Role of the Anaesthesiologist in the Perioperative Management of Preeclampsia. RA Dyer Interlaken 2017
 The Role of the Anaesthesiologist in the Perioperative Management of Preeclampsia RA Dyer Interlaken 2017 6 In preeclampsia - Understanding of pathophysiology Assessment of disease severity Prediction
The Role of the Anaesthesiologist in the Perioperative Management of Preeclampsia RA Dyer Interlaken 2017 6 In preeclampsia - Understanding of pathophysiology Assessment of disease severity Prediction
General Anesthesia. Mohamed A. Yaseen
 General Anesthesia Mohamed A. Yaseen M.S,c Surgery Before Anesthesia General Anesthesia ( GA ) Drug induced absence of perception of all sensation allowing surgery or other painful procedure to be carried
General Anesthesia Mohamed A. Yaseen M.S,c Surgery Before Anesthesia General Anesthesia ( GA ) Drug induced absence of perception of all sensation allowing surgery or other painful procedure to be carried
REGIONAL/LOCAL ANESTHESIA and OBESITY
 REGIONAL/LOCAL ANESTHESIA and OBESITY Jay B. Brodsky, MD Stanford University School of Medicine Jbrodsky@stanford.edu Potential Advantages Regional compared to General Anesthesia Minimal intra-operative
REGIONAL/LOCAL ANESTHESIA and OBESITY Jay B. Brodsky, MD Stanford University School of Medicine Jbrodsky@stanford.edu Potential Advantages Regional compared to General Anesthesia Minimal intra-operative
Why would epidural analgesia cause these symptoms? How would increasing the blood volume change venous pressure (VP)?
?") CASE 12 A 25-year-old pregnant woman is in labor at the hospital. She has no medical problems and has had no complications with this pregnancy. She is in the active phase of labor, feeling intense contractions,
CASE 12 A 25-year-old pregnant woman is in labor at the hospital. She has no medical problems and has had no complications with this pregnancy. She is in the active phase of labor, feeling intense contractions,
Pre-eclampsia: key issues. Robin Russell Nuffield Department of Anaesthetics John Radcliffe Hospital Oxford
 Robin Russell Nuffield Department of Anaesthetics John Radcliffe Hospital Oxford Antenatal Issues Labour Analgesia Anaesthesia for Delivery High Dependency Care Hypertension systolic >140 mmhg or diastolic
Robin Russell Nuffield Department of Anaesthetics John Radcliffe Hospital Oxford Antenatal Issues Labour Analgesia Anaesthesia for Delivery High Dependency Care Hypertension systolic >140 mmhg or diastolic
Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit
 Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit * Patient s name and age * Surgical procedure and type of anesthetic including drugs used * Other intraoperative
Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit * Patient s name and age * Surgical procedure and type of anesthetic including drugs used * Other intraoperative
Milestone Guide. CBD Anesthesia
 Table of Contents Department of Anesthesiology Foundations 1 Airway 1 Pharmacology 1 Physiology 1 Common Uncomplicated Anesthetics Practice 2 Obstetrics 2 Pain 2 Core 3 Perioperative Medicine 3 Complex
Table of Contents Department of Anesthesiology Foundations 1 Airway 1 Pharmacology 1 Physiology 1 Common Uncomplicated Anesthetics Practice 2 Obstetrics 2 Pain 2 Core 3 Perioperative Medicine 3 Complex
Chapter 25. General Anesthetics
 Chapter 25 1. Introduction General anesthetics: 1. Analgesia 2. Amnesia 3. Loss of consciousness 4. Inhibition of sensory and autonomic reflexes 5. Skeletal muscle relaxation An ideal anesthetic: 1. A
Chapter 25 1. Introduction General anesthetics: 1. Analgesia 2. Amnesia 3. Loss of consciousness 4. Inhibition of sensory and autonomic reflexes 5. Skeletal muscle relaxation An ideal anesthetic: 1. A
NON-OPIOID ANALGESIA & THE IMPLICATIONS OF ANESTHETIC DRUGS IN THE PERI-ANESTHETIC ARENA AMANDA AFFLECK CRNA
 NON-OPIOID ANALGESIA & THE IMPLICATIONS OF ANESTHETIC DRUGS IN THE PERI-ANESTHETIC ARENA AMANDA AFFLECK CRNA OR, ANESTHESIA, WHY DO THEY DO THAT? OUTLINE Neurotransmission of pain Arachidonic Acid pathway
NON-OPIOID ANALGESIA & THE IMPLICATIONS OF ANESTHETIC DRUGS IN THE PERI-ANESTHETIC ARENA AMANDA AFFLECK CRNA OR, ANESTHESIA, WHY DO THEY DO THAT? OUTLINE Neurotransmission of pain Arachidonic Acid pathway
Obstetric Analgesia & Anesthesia
 Obstetric Analgesia & Anesthesia Bernadette Balestrieri-Martinez RNC-OB, MSN, CNS, C-EFM Perinatal Clinical Nurse Specialist - Sharp HealthCare Objectives Describe the physiology of labor and factors effecting
Obstetric Analgesia & Anesthesia Bernadette Balestrieri-Martinez RNC-OB, MSN, CNS, C-EFM Perinatal Clinical Nurse Specialist - Sharp HealthCare Objectives Describe the physiology of labor and factors effecting
Obstetrical Anesthesia. Safe Pain Relief for Childbirth
 Obstetrical Anesthesia Safe Pain Relief for Childbirth Introduction Pain relief (analgesia) for labor and delivery is now safer than ever. In the United States approximately two-thirds of all women receive
Obstetrical Anesthesia Safe Pain Relief for Childbirth Introduction Pain relief (analgesia) for labor and delivery is now safer than ever. In the United States approximately two-thirds of all women receive
Suggested items to be included in obstetric anaesthesia records
 Suggested items to be included in obstetric anaesthesia records This list is intended as a guide to what fields could be included in an anaesthesia record used in obstetric practice. It is merely a suggested
Suggested items to be included in obstetric anaesthesia records This list is intended as a guide to what fields could be included in an anaesthesia record used in obstetric practice. It is merely a suggested
ASA Closed Claims Project: Regional Anesthesia Claims 1990 or later Lorri A. Lee MD Department of Anesthesiology University of Washington, Seattle, WA
 ASA Closed Claims Project: Regional Anesthesia Claims 1990 or later Lorri A. Lee MD Department of Anesthesiology, Seattle, WA OVERVIEW 1. Closed Claims Project 2. Peripheral Nerve Blocks 3. Neuraxial Claims
ASA Closed Claims Project: Regional Anesthesia Claims 1990 or later Lorri A. Lee MD Department of Anesthesiology, Seattle, WA OVERVIEW 1. Closed Claims Project 2. Peripheral Nerve Blocks 3. Neuraxial Claims
Core Safety Profile. Pharmaceutical form(s)/strength: 5mg/ml and 25 mg/ml, Solution for injection, IM/IV FI/H/PSUR/0010/002 Date of FAR:
/strength: 5mg/ml and 25 mg/ml, Solution for injection, IM/IV FI/H/PSUR/0010/002 Date of FAR:") Core Safety Profile Active substance: Esketamine Pharmaceutical form(s)/strength: 5mg/ml and 25 mg/ml, Solution for injection, IM/IV P-RMS: FI/H/PSUR/0010/002 Date of FAR: 29.05.2012 4.3 Contraindications
Core Safety Profile Active substance: Esketamine Pharmaceutical form(s)/strength: 5mg/ml and 25 mg/ml, Solution for injection, IM/IV P-RMS: FI/H/PSUR/0010/002 Date of FAR: 29.05.2012 4.3 Contraindications
Department of Intensive Care Medicine UNDERSTANDING CIRCULATORY FAILURE IN SEPSIS
 Department of Intensive Care Medicine UNDERSTANDING CIRCULATORY FAILURE IN SEPSIS UNDERSTANDING CIRCULATORY FAILURE IN SEPSIS a mismatch between tissue perfusion and metabolic demands the heart, the vasculature
Department of Intensive Care Medicine UNDERSTANDING CIRCULATORY FAILURE IN SEPSIS UNDERSTANDING CIRCULATORY FAILURE IN SEPSIS a mismatch between tissue perfusion and metabolic demands the heart, the vasculature
Intraspinal (Neuraxial) Analgesia Community Nurses Competency Test
 Analgesia Community Nurses Competency Test") Intraspinal (Neuraxial) Analgesia Community Nurses Competency Test 1 Intraspinal (Neuraxial) Analgesia for Community Nurses Competency Test 1) Name the two major classifications of pain. i. ii. 2) Neuropathic
Intraspinal (Neuraxial) Analgesia Community Nurses Competency Test 1 Intraspinal (Neuraxial) Analgesia for Community Nurses Competency Test 1) Name the two major classifications of pain. i. ii. 2) Neuropathic
GUIDELINE PHYSIOLOGY OF BIRTH ASPHYXIA
 GUIDELINE PHYSIOLOGY OF BIRTH ASPHYXIA The newborn is not an adult, nor a child. In people of all ages, death can occur from a failure of breathing and / or circulation. The interventions required to aid
GUIDELINE PHYSIOLOGY OF BIRTH ASPHYXIA The newborn is not an adult, nor a child. In people of all ages, death can occur from a failure of breathing and / or circulation. The interventions required to aid
Comparision of Intravenous Bolus Phenylephrine and Ephedrine for Prevention of Post Spinal Hypotension in Cesarean Sections
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 14, Issue 7 Ver. II (July. 2015), PP 99-103 www.iosrjournals.org Comparision of Intravenous Bolus Phenylephrine
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 14, Issue 7 Ver. II (July. 2015), PP 99-103 www.iosrjournals.org Comparision of Intravenous Bolus Phenylephrine
Cardiovascular Responses to Exercise
 CARDIOVASCULAR PHYSIOLOGY 69 Case 13 Cardiovascular Responses to Exercise Cassandra Farias is a 34-year-old dietician at an academic medical center. She believes in the importance of a healthy lifestyle
CARDIOVASCULAR PHYSIOLOGY 69 Case 13 Cardiovascular Responses to Exercise Cassandra Farias is a 34-year-old dietician at an academic medical center. She believes in the importance of a healthy lifestyle
Neonatal Resuscitation. Dustin Coyle, M.D. Anesthesiology
 Neonatal Resuscitation Dustin Coyle, M.D. Anesthesiology Recognize complications Maternal-fetal factors Maternal DM PIH Chronic HTN Previous stillbirth Rh sensitization Infection Substance abuse/certain
Neonatal Resuscitation Dustin Coyle, M.D. Anesthesiology Recognize complications Maternal-fetal factors Maternal DM PIH Chronic HTN Previous stillbirth Rh sensitization Infection Substance abuse/certain
General Anesthesia. My goal in general anesthesia is to stop all of these in the picture above (motor reflexes, pain and autonomic reflexes).
.") General Anesthesia General anesthesia is essential to surgical practice, because it renders patients analgesic, amnesia and unconscious reflexes, while causing muscle relaxation and suppression of undesirable
General Anesthesia General anesthesia is essential to surgical practice, because it renders patients analgesic, amnesia and unconscious reflexes, while causing muscle relaxation and suppression of undesirable
Remifentanil PCA In Labor
 Remifentanil PCA In { Jennifer Lucero, MD Clinical Instructor UCSF Department of Anesthesia Remifentanil PCA in Discuss the Pharmokinectics of Remifentanil Review literature on the use of Remifentanil
Remifentanil PCA In { Jennifer Lucero, MD Clinical Instructor UCSF Department of Anesthesia Remifentanil PCA in Discuss the Pharmokinectics of Remifentanil Review literature on the use of Remifentanil
Core Safety Profile. Date of FAR:
 Core Safety Profile Active substance: Levobupivicaine Pharmaceutical form(s)/strength: Solution for injection, concentrate for solution for infusion, 2,5 mg/ml, 5 mg/ml, 7,5 mg/ml, 0,625 mg/ml, 1,25 mg/ml
Core Safety Profile Active substance: Levobupivicaine Pharmaceutical form(s)/strength: Solution for injection, concentrate for solution for infusion, 2,5 mg/ml, 5 mg/ml, 7,5 mg/ml, 0,625 mg/ml, 1,25 mg/ml
Drugs used in obstetrics
 Drugs used in obstetrics Drugs used in obstetrics Drugs may be used to modify uterine contractions. These include oxytocic drugs used to stimulate uterine contractions both in induction of labour and to
Drugs used in obstetrics Drugs used in obstetrics Drugs may be used to modify uterine contractions. These include oxytocic drugs used to stimulate uterine contractions both in induction of labour and to
Perioperative Pain Management
 Perioperative Pain Management Overview and Update As defined by the Anesthesiologist's Task Force on Acute Pain Management are from the practice guidelines from the American Society of Anesthesiologists
Perioperative Pain Management Overview and Update As defined by the Anesthesiologist's Task Force on Acute Pain Management are from the practice guidelines from the American Society of Anesthesiologists
Effects of IV Ondansetron during spinal anaesthesia with Ropivacaine and Fentanyl
 Original article Effects of IV Ondansetron during spinal anaesthesia with Ropivacaine and Fentanyl 1Dr Bipul Deka, 2 Dr Bharat Talukdar, 3 Dr. Amal Kumar Laha, 4 Dr. Rupak Bhattacharjee 1Assistant Professor,
Original article Effects of IV Ondansetron during spinal anaesthesia with Ropivacaine and Fentanyl 1Dr Bipul Deka, 2 Dr Bharat Talukdar, 3 Dr. Amal Kumar Laha, 4 Dr. Rupak Bhattacharjee 1Assistant Professor,
Methamphetamine Abuse During Pregnancy
 Methamphetamine Abuse During Pregnancy Robert Davis, MD / r.w.davismd@gmail.com ❶ Statistics ❷ Pregnancy Concerns ❸ Postpartum Concerns ❹ Basic Science ❺ Best Practice Guidelines ❻ Withdrawal ❼ Recovery
Methamphetamine Abuse During Pregnancy Robert Davis, MD / r.w.davismd@gmail.com ❶ Statistics ❷ Pregnancy Concerns ❸ Postpartum Concerns ❹ Basic Science ❺ Best Practice Guidelines ❻ Withdrawal ❼ Recovery
Chapter 19. Media Directory. Topical (Surface) Anesthesia. Spinal Anesthesia. Nerve-Block Anesthesia. Infiltration (Field-Block) Anesthesia
 Anesthesia. Spinal Anesthesia. Nerve-Block Anesthesia. Infiltration (Field-Block) Anesthesia") Chapter 19 Drugs for Local and General Anesthesia Slide 18 Media Directory Lidocaine Animation Upper Saddle River, New Jersey 07458 All rights reserved. Topical (Surface) Anesthesia Creams, sprays, suppositories
Chapter 19 Drugs for Local and General Anesthesia Slide 18 Media Directory Lidocaine Animation Upper Saddle River, New Jersey 07458 All rights reserved. Topical (Surface) Anesthesia Creams, sprays, suppositories
Chapters 9 & 10. Cardiorespiratory System. Cardiovascular Adjustments to Exercise. Cardiovascular Adjustments to Exercise. Nervous System Components
 Cardiorespiratory System Chapters 9 & 10 Cardiorespiratory Control Pulmonary ventilation Gas exchange Left heart Arterial system Tissues Right heart Lungs Pulmonary ventilation Cardiovascular Regulation-
Cardiorespiratory System Chapters 9 & 10 Cardiorespiratory Control Pulmonary ventilation Gas exchange Left heart Arterial system Tissues Right heart Lungs Pulmonary ventilation Cardiovascular Regulation-
Introduction of a New Concept of Pain Management during Labor and a Novel Technique for Pain Free Labor
 Open Journal of Anesthesiology, 2012, 2, 79-83 http://dx.doi.org/10.4236/ojanes.2012.23019 Published Online July 2012 (http://www.scirp.org/journal/ojanes) 1 Introduction of a New Concept of Pain Management
Open Journal of Anesthesiology, 2012, 2, 79-83 http://dx.doi.org/10.4236/ojanes.2012.23019 Published Online July 2012 (http://www.scirp.org/journal/ojanes) 1 Introduction of a New Concept of Pain Management
NEUROMUSCULAR BLOCKING AGENTS
 NEUROMUSCULAR BLOCKING AGENTS Edward JN Ishac, Ph.D. Associate Professor, Pharmacology and Toxicology Smith 742, 828-2127, Email: eishac@vcu.edu Learning Objectives: 1. Understand the physiology of the
NEUROMUSCULAR BLOCKING AGENTS Edward JN Ishac, Ph.D. Associate Professor, Pharmacology and Toxicology Smith 742, 828-2127, Email: eishac@vcu.edu Learning Objectives: 1. Understand the physiology of the
Cerebral hemisphere. Parietal Frontal Occipital Temporal
 Cerebral hemisphere Sulcus / Fissure Central Precental gyrus Postcentral gyrus Lateral (cerebral) Parieto-occipital Cerebral cortex Frontal lobe Parietal lobe Temporal lobe Insula Amygdala Hippocampus
Cerebral hemisphere Sulcus / Fissure Central Precental gyrus Postcentral gyrus Lateral (cerebral) Parieto-occipital Cerebral cortex Frontal lobe Parietal lobe Temporal lobe Insula Amygdala Hippocampus
Labor Epidural: Local Anesthetics and Beyond
 Goals: Labor Epidural: Local Anesthetics and Beyond Pedram Aleshi MD The Changing Practice of Anesthesia September 2012 Review Concept of MLAC Local anesthetic efficacy Local anesthetic sparing effects:
Goals: Labor Epidural: Local Anesthetics and Beyond Pedram Aleshi MD The Changing Practice of Anesthesia September 2012 Review Concept of MLAC Local anesthetic efficacy Local anesthetic sparing effects:
Local anaesthetics. Dr JM Dippenaar
 Local anaesthetics Dr JM Dippenaar Chemical structure Lipophilic phenol ring + Amide/Ester bridge + Hydrophilic chain Local anesthetic drugs Amides Esters Lignocaine Cocaine Bupivacaine PABA esters Ropivacaine
Local anaesthetics Dr JM Dippenaar Chemical structure Lipophilic phenol ring + Amide/Ester bridge + Hydrophilic chain Local anesthetic drugs Amides Esters Lignocaine Cocaine Bupivacaine PABA esters Ropivacaine
ParasymPathetic Nervous system. Done by : Zaid Al-Ghnaneem
 ParasymPathetic Nervous system Done by : Zaid Al-Ghnaneem In this lecture we are going to discuss Parasympathetic, in the last lecture we took sympathetic and one of the objectives of last lecture was
ParasymPathetic Nervous system Done by : Zaid Al-Ghnaneem In this lecture we are going to discuss Parasympathetic, in the last lecture we took sympathetic and one of the objectives of last lecture was
Hemodynamic Changes in Obstetric Anesthesia. Sonia Vaida PANA, Hershey, April 2009
 Hemodynamic Changes in Obstetric Anesthesia Sonia Vaida PANA, Hershey, April 2009 Pregnancy is a normal healthy condition and is simultaneously the most common altered physiologic state to which human
Hemodynamic Changes in Obstetric Anesthesia Sonia Vaida PANA, Hershey, April 2009 Pregnancy is a normal healthy condition and is simultaneously the most common altered physiologic state to which human
Dr Kelly Jones Anesthesiologist at Northwest Orthopedics
 Dr Kelly Jones Anesthesiologist at Northwest Orthopedics Decrease narcotic use in the immediate post operative period. Better Pain Control Less side effects then General Anesthesia Sedation Post operative
Dr Kelly Jones Anesthesiologist at Northwest Orthopedics Decrease narcotic use in the immediate post operative period. Better Pain Control Less side effects then General Anesthesia Sedation Post operative
Figure removed due to copyright restrictions.
 Harvard-MIT Division of Health Sciences and Technology HST.071: Human Reproductive Biology Course Director: Professor Henry Klapholz IN SUMMARY HST 071 An Example of a Fetal Heart Rate Tracing Figure removed
Harvard-MIT Division of Health Sciences and Technology HST.071: Human Reproductive Biology Course Director: Professor Henry Klapholz IN SUMMARY HST 071 An Example of a Fetal Heart Rate Tracing Figure removed
PERIPARTUM CARDIOMYOPATHY
 PERIPARTUM CARDIOMYOPATHY Dr.T.Venkatachalam. Professor of Anaesthesiology Madras Medical College, Chennai Peripartum cardiomyopathy is defined as the onset of acute heart failure without demonstrable
PERIPARTUM CARDIOMYOPATHY Dr.T.Venkatachalam. Professor of Anaesthesiology Madras Medical College, Chennai Peripartum cardiomyopathy is defined as the onset of acute heart failure without demonstrable
Frederic J., Gerges MD. Ghassan E. Kanazi MD., Sama, I. Jabbour-Khoury MD. Review article from Journal of clinical anesthesia 2006.
 Frederic J., Gerges MD. Ghassan E. Kanazi MD., Sama, I. Jabbour-Khoury MD. Review article from Journal of clinical anesthesia 2006 Introduction Laparoscopic surgery started in the mid 1950s. In recent
Frederic J., Gerges MD. Ghassan E. Kanazi MD., Sama, I. Jabbour-Khoury MD. Review article from Journal of clinical anesthesia 2006 Introduction Laparoscopic surgery started in the mid 1950s. In recent
May 2013 Anesthetics SLOs Page 1 of 5
 May 2013 Anesthetics SLOs Page 1 of 5 1. A client is having a scalp laceration sutured and is to be given Lidocaine that contains Epinephrine. The nurse knows that this combination is desgined to: A. Cause
May 2013 Anesthetics SLOs Page 1 of 5 1. A client is having a scalp laceration sutured and is to be given Lidocaine that contains Epinephrine. The nurse knows that this combination is desgined to: A. Cause
10. Thick deposits of lipids on the walls of blood vessels, called, can lead to serious circulatory issues. A. aneurysm B. atherosclerosis C.
 Heart Student: 1. carry blood away from the heart. A. Arteries B. Veins C. Capillaries 2. What is the leading cause of heart attack and stroke in North America? A. alcohol B. smoking C. arteriosclerosis
Heart Student: 1. carry blood away from the heart. A. Arteries B. Veins C. Capillaries 2. What is the leading cause of heart attack and stroke in North America? A. alcohol B. smoking C. arteriosclerosis
Purpose: The goal of epidural anesthesia is to reduce or eliminate pain in the laboring patient.
 Alaska Native Medical Center: Mother Baby Unit Subject: Epidural Anesthesia/PCEA in Laboring Patients Guideline: Epidural Anesthesia in Laboring Patients REVISION DATE: March 2013 REPLACES: L&D Epidural
Alaska Native Medical Center: Mother Baby Unit Subject: Epidural Anesthesia/PCEA in Laboring Patients Guideline: Epidural Anesthesia in Laboring Patients REVISION DATE: March 2013 REPLACES: L&D Epidural
Pharmacology: Inhalation Anesthetics
 Pharmacology: Inhalation Anesthetics This is an edited and abridged version of: Pharmacology: Inhalation Anesthetics by Jch Ko, DVM, MS, DACVA Oklahoma State University - Veterinary Medicine, February
Pharmacology: Inhalation Anesthetics This is an edited and abridged version of: Pharmacology: Inhalation Anesthetics by Jch Ko, DVM, MS, DACVA Oklahoma State University - Veterinary Medicine, February
Key Points. Angus DC: Crit Care Med 29:1303, 2001
 Sepsis Key Points Sepsis is the combination of a known or suspected infection and an accompanying systemic inflammatory response (SIRS) Severe sepsis is sepsis with acute dysfunction of one or more organ
Sepsis Key Points Sepsis is the combination of a known or suspected infection and an accompanying systemic inflammatory response (SIRS) Severe sepsis is sepsis with acute dysfunction of one or more organ
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #12 Understanding Preload and Afterload
 McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #12 Understanding Preload and Afterload Cardiac output (CO) represents the volume of blood that is delivered
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #12 Understanding Preload and Afterload Cardiac output (CO) represents the volume of blood that is delivered
Skeletal muscle. Flow increases and decreases with each muscular contraction - as a result of compression of the blood vessels by contracted muscle
 Regional blood flow Skeletal muscle Extreme increases during exercises Flow increases and decreases with each muscular contraction - as a result of compression of the blood vessels by contracted muscle
Regional blood flow Skeletal muscle Extreme increases during exercises Flow increases and decreases with each muscular contraction - as a result of compression of the blood vessels by contracted muscle
Resuscitation efforts for Mom & Baby
 Resuscitation efforts for Mom & Baby Beth Ann Clayton, CRNA, MS AmSol Obstetric Anesthesia CRNA Educator Obstetric Anesthesia Clinical Coordinator Mercy Health-Fairfield Hospital Assistant Professor, University
Resuscitation efforts for Mom & Baby Beth Ann Clayton, CRNA, MS AmSol Obstetric Anesthesia CRNA Educator Obstetric Anesthesia Clinical Coordinator Mercy Health-Fairfield Hospital Assistant Professor, University
Maternal Collapse Guideline
 Maternal Collapse Guideline Guideline Number: 664 Supersedes: Classification Clinical Version No: Date of EqIA: Approved by: Date Approved: Date made active: Review Date: 1 Obstetric Written Documentation
Maternal Collapse Guideline Guideline Number: 664 Supersedes: Classification Clinical Version No: Date of EqIA: Approved by: Date Approved: Date made active: Review Date: 1 Obstetric Written Documentation
The Spinal Cord & Spinal Nerves
 The Spinal Cord & Spinal Nerves Together with brain forms the CNS Functions spinal cord reflexes integration (summation of inhibitory and excitatory) nerve impulses highway for upward and downward travel
The Spinal Cord & Spinal Nerves Together with brain forms the CNS Functions spinal cord reflexes integration (summation of inhibitory and excitatory) nerve impulses highway for upward and downward travel
CHAPTER 3. The Human Body National Safety Council
 CHAPTER 3 The Human Body The Human Body Composed of many different organs and tissues All parts work together: To sustain life Allow activity Injury or illness impairs functions 3-3 Cranial located in
CHAPTER 3 The Human Body The Human Body Composed of many different organs and tissues All parts work together: To sustain life Allow activity Injury or illness impairs functions 3-3 Cranial located in
The Autonomic Nervous System
 The Autonomic Nervous System Responsible for control of visceral effectors and visceral reflexes: smooth muscle, glands, the heart. e.g. blood pressure, cardiac output, plasma glucose The autonomic system
The Autonomic Nervous System Responsible for control of visceral effectors and visceral reflexes: smooth muscle, glands, the heart. e.g. blood pressure, cardiac output, plasma glucose The autonomic system
Beneficial effects of the addition of intrathecal fentanyl to bupivacaine for spinal anesthesia in cesarean section
 Anesth Pain Med 2017; 12: 233-239 https://doi.org/10.17085/apm.2017.12.3.233 Clinical Research http://crossmark.crossref.org/dialog/?doi=10.17085/apm.2017.12.3.233&domain=pdf&date_stamp=2017-07-25 pissn
Anesth Pain Med 2017; 12: 233-239 https://doi.org/10.17085/apm.2017.12.3.233 Clinical Research http://crossmark.crossref.org/dialog/?doi=10.17085/apm.2017.12.3.233&domain=pdf&date_stamp=2017-07-25 pissn
Shock is defined as a state of cellular and tissue hypoxia due to : reduced oxygen delivery and/or increased oxygen consumption or inadequate oxygen
 Shock is defined as a state of cellular and tissue hypoxia due to : reduced oxygen delivery and/or increased oxygen consumption or inadequate oxygen utilization The effects of shock are initially reversible
Shock is defined as a state of cellular and tissue hypoxia due to : reduced oxygen delivery and/or increased oxygen consumption or inadequate oxygen utilization The effects of shock are initially reversible
ANESTHESIA FOR CESAREAN DELIVERY
 REVIEW ARTICLE ANESTHESIA FOR CESAREAN DELIVERY Naitik Patel Assistant Professor, Department of Anesthesia, Gujarat Adani Institute of Medical Science, Bhuj, Gujarat. ABSTRACT: Anesthetic techniques currently
REVIEW ARTICLE ANESTHESIA FOR CESAREAN DELIVERY Naitik Patel Assistant Professor, Department of Anesthesia, Gujarat Adani Institute of Medical Science, Bhuj, Gujarat. ABSTRACT: Anesthetic techniques currently
Comparative Study of Equal Doses of Intrathecal Isobaric Bupivacaine and Isobaric Ropivacaine for Lower Limb Surgeries and Perineal Surgeries
 Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/229 Comparative Study of Equal Doses of Intrathecal Isobaric Bupivacaine and Isobaric Ropivacaine for Lower Limb Surgeries
Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/229 Comparative Study of Equal Doses of Intrathecal Isobaric Bupivacaine and Isobaric Ropivacaine for Lower Limb Surgeries
General surgery. Thyroid surgery. Physiological response to pneumoperitoneum. Bowel resection
 General surgery Thyroid surgery Physiological response to pneumoperitoneum Bowel resection General surgery 3.D.9.1 James Mitchell (December 24, 2003) Thyroid surgery Preoperative Assessment Routine, plus
General surgery Thyroid surgery Physiological response to pneumoperitoneum Bowel resection General surgery 3.D.9.1 James Mitchell (December 24, 2003) Thyroid surgery Preoperative Assessment Routine, plus
Sri Lankan Journal of Anaesthesiology 17(2) : (2009)
 : (2009)") Sri Lankan Journal of Anaesthesiology 17(2) : 55-60 (2009) COMPARISON OF PROPHYLACTIC INTRAMUSCULAR EPHEDRINE WITH PRELOADING VERSUS PRELOADING ALONE IN PREVENTION OF HYPOTENSION DURING ELECTIVE CAESAREAN
Sri Lankan Journal of Anaesthesiology 17(2) : 55-60 (2009) COMPARISON OF PROPHYLACTIC INTRAMUSCULAR EPHEDRINE WITH PRELOADING VERSUS PRELOADING ALONE IN PREVENTION OF HYPOTENSION DURING ELECTIVE CAESAREAN
Unplanned cesarean section in parturients with an epidural catheter in-situ : how to obtain surgical anesthesia?
 (Acta Anaesth. Belg., 2013, 64, 61-74) Unplanned cesarean section in parturients with an epidural catheter in-situ : how to obtain surgical anesthesia? E. Depuydt and M. Van De Velde Abstract : Epidural
(Acta Anaesth. Belg., 2013, 64, 61-74) Unplanned cesarean section in parturients with an epidural catheter in-situ : how to obtain surgical anesthesia? E. Depuydt and M. Van De Velde Abstract : Epidural
SHOCK AETIOLOGY OF SHOCK (1) Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function
 Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function") SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
Note: At the end of the instructions, you will find a table which must be filled in to complete the exercise.
 Autonomic Nervous System Theoretical foundations and instructions for conducting practical exercises carried out during the course List of practical exercises 1. Deep (controlled) breath test 2. Cold pressor
Autonomic Nervous System Theoretical foundations and instructions for conducting practical exercises carried out during the course List of practical exercises 1. Deep (controlled) breath test 2. Cold pressor
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,500 108,000 1.7 M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,500 108,000 1.7 M Open access books available International authors and editors Downloads Our
Epidural anaesthesia and analgesia
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk Epidural anaesthesia and analgesia Author : Matthew Gurney Categories : Vets Date : June 1, 2009 Matthew Gurney discusses
Vet Times The website for the veterinary profession https://www.vettimes.co.uk Epidural anaesthesia and analgesia Author : Matthew Gurney Categories : Vets Date : June 1, 2009 Matthew Gurney discusses
Prescribing Information. Carbocaine 1% Carbocaine 2%
 Prescribing Information Carbocaine 1% 10 mg/ml, Mepivacaine Hydrochloride Injection, USP Carbocaine 2% 20 mg/ml, Mepivacaine Hydrochloride Injection, USP Local Anesthetic Pfizer Canada Inc. 17300 Trans-Canada
Prescribing Information Carbocaine 1% 10 mg/ml, Mepivacaine Hydrochloride Injection, USP Carbocaine 2% 20 mg/ml, Mepivacaine Hydrochloride Injection, USP Local Anesthetic Pfizer Canada Inc. 17300 Trans-Canada
Regional Anesthesia. procedure if required. However, many patients prefer to receive sedation either during the
 1 Regional Anesthesia Regional anaesthesia (or regional anesthesia) is anesthesia affecting only a large part of the body, such as a limb or the lower half of the body. Regional anaesthetic techniques
1 Regional Anesthesia Regional anaesthesia (or regional anesthesia) is anesthesia affecting only a large part of the body, such as a limb or the lower half of the body. Regional anaesthetic techniques
Swans and Pressors. Vanderbilt Surgery Summer School Ricky Shinall
 Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall SHOCK Hypotension SHOCK Hypotension SHOCK=Reduction of systemic tissue perfusion, resulting in decreased oxygen delivery to the tissues.
Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall SHOCK Hypotension SHOCK Hypotension SHOCK=Reduction of systemic tissue perfusion, resulting in decreased oxygen delivery to the tissues.
Swans and Pressors. Vanderbilt Surgery Summer School Ricky Shinall
 Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall Shock, Swans, Pressors in 15 minutes 4 Reasons for Shock 4 Swan numbers to know 7 Pressors =15 things to know 4 Reasons for Shock Not enough
Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall Shock, Swans, Pressors in 15 minutes 4 Reasons for Shock 4 Swan numbers to know 7 Pressors =15 things to know 4 Reasons for Shock Not enough
Sign up to receive ATOTW weekly -
 SPINAL ANAESTHETIC SPREAD ANAESTHESIA TUTORIAL OF THE WEEK 37 28 th NOVEMBER 2006 Dr Graham Hocking Consultant in Anaesthesia and Pain Medicine, John Radcliffe Hospital, Oxford, UK Email: ghocking@btinternet.com
SPINAL ANAESTHETIC SPREAD ANAESTHESIA TUTORIAL OF THE WEEK 37 28 th NOVEMBER 2006 Dr Graham Hocking Consultant in Anaesthesia and Pain Medicine, John Radcliffe Hospital, Oxford, UK Email: ghocking@btinternet.com
Pain Relief Options for Labor. Providing you with quality care, information and support
 Pain Relief Options for Labor Providing you with quality care, information and support What can I expect during my labor and delivery? As a patient in the Labor and Delivery suite at Lucile Packard Children
Pain Relief Options for Labor Providing you with quality care, information and support What can I expect during my labor and delivery? As a patient in the Labor and Delivery suite at Lucile Packard Children
Policy REVISED: 6/30/2016 3:30 PM. Applies To: ObGyn Responsible Department: ObGyn Revised: June 30, 2016
 Title: Antihypertensive Treatment for Severe Hypertension During Pregnancy Applies To: ObGyn Responsible Department: ObGyn Revised: June 30, 2016 Policy POLICY STATEMENT: Pregnant or postpartum patients
Title: Antihypertensive Treatment for Severe Hypertension During Pregnancy Applies To: ObGyn Responsible Department: ObGyn Revised: June 30, 2016 Policy POLICY STATEMENT: Pregnant or postpartum patients
ORIGINAL ARTICLE A COMPARATIVE STUDY BETWEEN 0.5% HYPERBARIC BUPIVACAINE AND 0.5% HYPERBARIC BUPIVACAINE WITH
 A COMPARATIVE STUDY BETWEEN 0.5% HYPERBARIC BUPIVACAINE AND 0.5% HYPERBARIC BUPIVACAINE WITH 25 mcg FENTANYL IN SPINAL ANAESTHESIA IN OBSTETRIC PATIENTS UNDERGOING ELECTIVE LSCS A. V. Abhinav 1, Harshavardhan
A COMPARATIVE STUDY BETWEEN 0.5% HYPERBARIC BUPIVACAINE AND 0.5% HYPERBARIC BUPIVACAINE WITH 25 mcg FENTANYL IN SPINAL ANAESTHESIA IN OBSTETRIC PATIENTS UNDERGOING ELECTIVE LSCS A. V. Abhinav 1, Harshavardhan
Chapter 13. The Spinal Cord & Spinal Nerves. Spinal Cord. Spinal Cord Protection. Meninges. Together with brain forms the CNS Functions
 Spinal Cord Chapter 13 The Spinal Cord & Spinal Nerves Together with brain forms the CNS Functions spinal cord reflexes integration (summation of inhibitory and excitatory) nerve impulses highway for upward
Spinal Cord Chapter 13 The Spinal Cord & Spinal Nerves Together with brain forms the CNS Functions spinal cord reflexes integration (summation of inhibitory and excitatory) nerve impulses highway for upward
Safety and quality of neuraxial analgesia. Ulla Sipiläinen HUCS Jorvi hospital
 Safety and quality of neuraxial analgesia Ulla Sipiläinen 6.10. 2011 HUCS Jorvi hospital Chestnut s Checklist Preparation for neuraxial labor analgesia 1.Communicate (early) with obst provider review parturient
Safety and quality of neuraxial analgesia Ulla Sipiläinen 6.10. 2011 HUCS Jorvi hospital Chestnut s Checklist Preparation for neuraxial labor analgesia 1.Communicate (early) with obst provider review parturient
THE GOOFY ANATOMIST QUIZZES
 THE GOOFY ANATOMIST QUIZZES 5. NERVES Q1. Which of the following classifications of the nervous systems is correct? A. The autonomic nervous system is composed of the brain, cranial nerves and spinal nerves.
THE GOOFY ANATOMIST QUIZZES 5. NERVES Q1. Which of the following classifications of the nervous systems is correct? A. The autonomic nervous system is composed of the brain, cranial nerves and spinal nerves.