Paula Bolton-Maggs Medical Director SHOT
|
|
|
- Esmond Davidson
- 6 years ago
- Views:
Transcription
1 Paula Bolton-Maggs Medical Director SHOT


2 Lancet April 30, 1983 The baby was transfused in March 1981 but there was reluctance by reviewers and publishers to publish rapidly NEJM: Confirmed link between transfusion and AIDS 28% of 2157 patients with AIDS had previously been transfused
3 Surveillance procedures from the collection of blood and its components to the follow up of the recipients To collect and assess information on unexpected and undesirable effects resulting from the therapeutic use of labile blood components And to prevent their occurrence or recurrence
4 Identify trends in adverse reactions and events Inform policy within transfusion services, DH, EU Target areas for improvement of practice Aid production of clinical guidelines for use of blood components Promote development of suitable education and training Identify and promote standards of practice Stimulate research and detailed audit Raise awareness of transfusion hazards and their prevention Be an early warning of new complications Improve safety of transfusion for patients
5
6 In 1990s - growing awareness of safety issues in blood transfusion especially HIV, HCV, hospital errors (McClelland BMJ 1994;308:1205) Incidence of major complications of blood transfusion was unknown Working group set up in 1994 to consider haemovigilance SHOT launched 1996 SHOT report first published for data Increasing number of reports each year Evolution of new categories reflecting reports 17 th report (2013 data) published July 2014
7 Professionally led scheme providing analysis of anonymised data by experts in each area of reporting Regular output in annual report, papers, meetings Recommendations for actions made to CMOs, DH, hospitals, professional bodies and blood services Measurable impact on patient safety Reduction in transfusion-related acute lung injury (TRALI) Reduction in ABO incompatible transfusions Reduction in bacterial contamination
8 Hospital transfusion teams Consultant haematologist Laboratory manager Transfusion practitioner On-line reporting system Categories Follow up with incident investigation Annual reports
9 The European Directive 2002/98/EC Blood Safety and Quality Regulations 2005 To set high standards of quality and safety for the collection, testing, processing, storage and distribution of human blood and blood components To reassure the public that human blood and components, which are derived from donations in one member state, meet the same requirements as those in their own country
10 UK Blood Safety and Quality Regulations (BSQR) 2005 (SI 50) Became law Nov 2005 MHRA became the competent authority
11 All serious adverse reactions same as for SHOT All serious adverse events signalling a process failure in the Quality Management System (QMS) occurring within the responsibility of the Blood Establishment or the Hospital Blood Bank, regardless of whether the component was transfused (SHOT reportable if transfused) Adverse events involving only clinical staff are not reportable to MHRA, but are reportable to SHOT, comprising the largest sub-group of SHOT reports
12 Competent Authority appointed by DH to implement new legislation and as regulator product quality and safety compliance with requirements for QMS Legal requirement to send numbers of SAEs and SARs to EU annually first year of mandatory reporting 2008 (June) May impose sanctions and demand corrective actions on individual sites not analysing trends or making recommendations
13 MHRA Medicines and Healthcare Products Regulatory Agency Competent Authority for the BSQR 2005 QMS in blood establishments and hospital blood banks Competent Authority for the Medicines Act 1968 Competent Authority for the Medical Devices Regulations 2008 STATUTORY reporting SHOT Serious Hazards of Transfusion Confidential enquiry Serious adverse reactions/events AND near misses all of which occur in BOTH a laboratory and CLINICAL environment PROFESSIONALLY MANDATED reporting
14 Decision to transfuse Prescription/request Sampling for pre-transfusion testing Laboratory testing Collection of blood from issue fridge Bedside administration Monitoring the patient
15 SHOT since 1996 set standards in EU and beyond BSQR implemented from November 2005 adverse event reporting to EU mandatory SABRE web based reporting to MHRA 2005 Web-based reporting to SHOT 2010 Initial data entered via SABRE to link case numbers
16 So what is the greatest risk of transfusion
17 SHOT Cumulative data: 17 years n=13141 Transfusion reactions which may not be preventable Possibly or probably preventable by improved practice and monitoring Adverse events due to mistakes
18 + Errors 77.6%
19 Incorrect blood component transfused Where are the mistakes made? Clinical errors Laboratory errors Copyright SHOT 2014
20 Incorrect blood component transfused Data from 220 reports 547 errors Copyright SHOT 2014
21 Incorrect blood component transfused Data from 220 reports 547 errors The common combinations of three: 78% request, prescription and administration 12% collection, prescription and administration Copyright SHOT 2014
22 Identification Documentation Communication Copyright SHOT October2014
23
24
25 Outcome of ABO incompatible red cell transfusions 66% have no adverse effect 15 deaths to 2005 BSQR 4 deaths NPSA SPN 14 Competency assessments Copyright SHOT 2014
26 Immediate and life-threatening : ABO incompatibility; anaphylaxis Hours: pulmonary complications, bacterial infections, transfusion reactions Days: Haemolytic reactions Late (months or years): viral infections; iron overload
27 Transfusion reactions may have many overlapping symptoms and signs with varying severity Fever, chills, rigor, myalgia, nausea, urticaria, itching, swelling, respiratory symptoms...etc. Advise patients to report any adverse events in 24 hrs after transfusion
28 A 56 year old man with acute myeloid leukaemia is having a platelet transfusion 5 minutes into the transfusion he feels unwell His temperature has increased to 40 o C He is sweating with severe hypotension
29 (Choose 1) 1. Allergic reaction 2. Haemolytic reaction 3. Infection in central venous line 4. Infection in platelet bag
30 ABO incompatibility Contact laboratory immediately Bacterial infection Central and peripheral blood cultures Start broad spectrum antibiotics Inform laboratory and haematologist to arrange culture of the unit Inform the Blood Service
31 Stop the transfusion, maintain IV access with saline and check the bag and patient ID Rapid medical assessment Inform the transfusion laboratory Blood culture and return blood bag to lab Renal function Monitor fluid balance (input and output) Collect first and subsequent urine samples


32 Correct patient identification is vital Patient Blood Component Sample Testing
33 Diagnosis and identification of possible need to transfuse Decision to transfuse Phlebotomy for group and crossmatch Written request to lab for blood Written prescription/order/authorisation for transfusion Laboratory testing, component selection and issue Collection from issue site Bedside checking of patient, unit ID and administration Monitoring/observing and noticing adverse event or reaction Appropriate management of adverse event or reaction
34 Transposed patient ID during phlebotomy leads to ABO incompatible transfusion Patient A, blood group O RhD negative, was transfused 2 units of A RhD positive blood during cardiac surgery On arrival in ICU he received two more group A units without apparent adverse events. Following transfusion, the patient showed evidence of haemolysis, with a fall in Hb requiring further transfusions, and rise in bilirubin to 241mmol/L within 6 days He had an extended stay in ITU.
35 Patient A and patient B were sampled at the same time in a preoperative clinic. The nurse was distracted while bleeding patient A, did not complete the process at the bedside, and so patient details were transposed when labelling the samples. Near Miss: Patient B s mislabelled sample was detected in the laboratory, because a historical group was available. Adverse event: Patient A had no historical group and the error was not detected.
36 Why did it happen? What can be learned from it? Corrective and preventive actions to reduce likelihood of recurrence
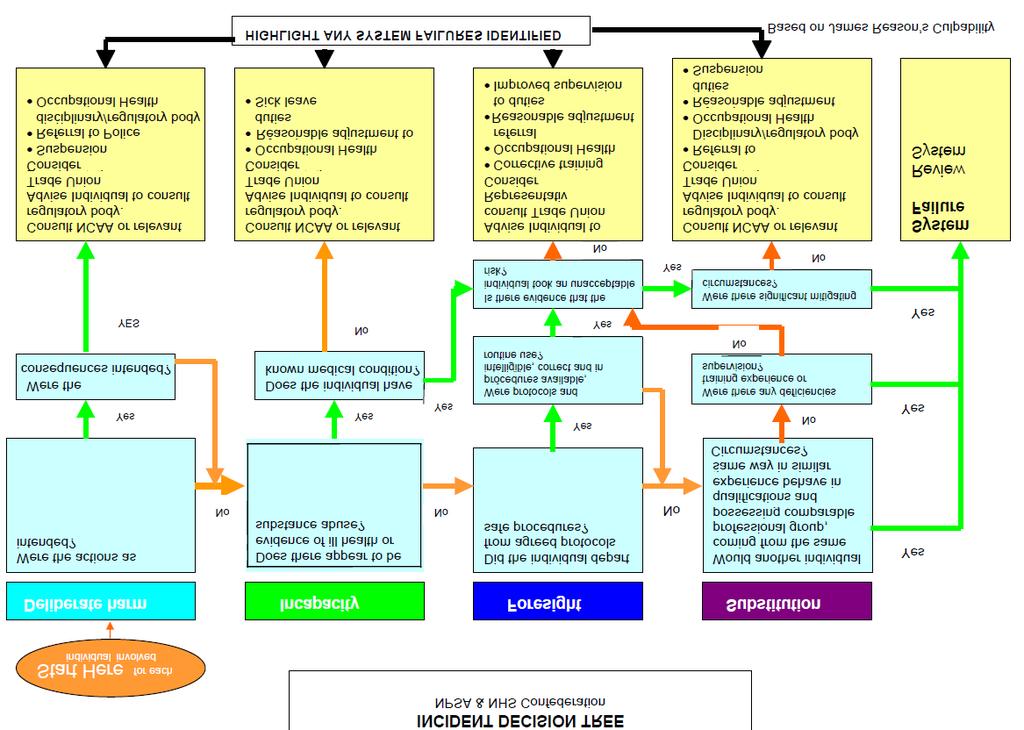
37 A child with beta thalassaemia major, blood group O, receives 3 ml of an incompatible unit of blood group A Recognised early, stopped, no harm done, but kept in hospital overnight for observation Blame culture dreadful deed, sack the nurse No-blame culture- understand the circumstances which led to this and take action to prevent recurrence
38 (James Reason, 2004)
39
40 Likelihood multiplied by the consequence gives a RISK SCORE
41 She did not intend to make this mistake but it could have resulted in death, and was very likely to happen again, so was treated as a very serious incident with a high risk score Likelihood multiplied by the consequence gives a RISK SCORE
42 The nurse was working alone in the day unit Three people needed transfusions she collected all three units at the same time She borrowed a nurse from the next ward to check all three, putting each down on a table beside the patient She was using aseptic technique to access the portacath, and the second nurse handed her the wrong unit which was not checked again at the bedside Incident recognised when next unit put up with bedside check
43 Key Root Cause: Collection of three units at the same time, and later failure to do the final bedside check immediately prior to transfusion The nurse was working alone in the day unit The staff were accepting a culture of chronic understaffing audit Three showed people solo working needed 75% transfusions of the time. Lone working she was collected also all three associated units with at a poor the record same (42%) time of correct observations during transfusion. As a result of this investigation, an addition member of She staff borrowed was employed nurse from the next ward to check all three, putting each down on a table beside the patient She was using aseptic technique to access the portacath, and the second nurse handed her the wrong unit The which layout was of the day not unit checked was reviewed again and changed at the bedside Incident recognised when next unit put up with bedside check The transfusion training of both nurses was out of date, and she forgot that collection of more than one unit at a time was against policy but also it was difficult to get away from the ward on three separate occasions while working alone So, the RCA resulted in several SOLUTIONS to improve the system
44 An elderly male patient received the first unit of FFP to correct a coagulopathy Half-way through the unit, he developed marked hypotension (from 100/60 to 50/20) and a widespread urticarial rash and shortness of breath with wheeze
45 (Choose 2) 1. Discontinue the transfusion 2. Continue the transfusion more slowly 3. Give hydrocortisone and piriton 4. Give adrenaline 5. Try a different unit
46 Allergic or anaphylactic reactions are unpredictable and usually occur early This is why all patients having blood products must be monitored Adrenaline (IM) is the treatment of choice and should be available in all areas where transfusions take place
47 Minor reactions excluded
48 Life threatening Requires immediate intervention Intramuscular adrenaline Support the airway (oxygen) Longer term: discuss with immunologist how to manage future transfusions See BCSH guidelines on acute transfusion reactions
49 An elderly woman with cirrhosis, ischaemic heart disease and a coagulopathy had an elective knee replacement She was transfused with 2 units FFP and 2 doses of platelets to cover removal of lines and epidural 30 mins after completing the transfusion she became suddenly breathless and hypoxic with signs of heart failure
50 The CXR showed bilateral shadowing and she was known to have impaired left ventricular function
51 (Choose 1) 1. TACO (transfusion-associated circulatory overload) 2. Chest infection 3. Acute myocardial infarction 4. TRALI (Transfusion-associated acute lung injury)
52 Consider TRALI or TACO Check airway and give oxygen Get expert medical assessment CXR and oxygen saturation
53 Acute dyspnoea with hypoxia and bilateral pulmonary infiltrates during or within 6h of transfusion, not due to circulatory overload or any other likely causes. Most suspected cases are complex Need expert panel assessment Serology: find anti-leucocyte antibodies in donor which react with recipient neutrophil antigens

54 Important cause of transfusion-related mortality and major morbidity Caused by HLA/HNA abs main source is donor plasma: A donor with a history of transfusion A female donor with a history of pregnancy abs in 10-15%
55 She was ventilated for 5 days and made a full recovery She was also treated with diuretics and IV fluids She was investigated for TRALI and this was confirmed by serological evidence of concordant HLA antibodies in one female donor of the apheresis platelets
56 TRALI relative risk from different components Red cells Cryo FFP Platelets TRALI cases Components issued 18,370, ,000 2,515,000 1,842,000 Risk/ component issued Relative risk compared to red cells 1:556,000 1:317,000 1:81,000 1:68 000
57 Decision to use male donors for FFP
58 TACO is much more common than TRALI and it can be difficult to confirm the cause of acute respiratory symptoms Elderly patients are particularly at risk of TACO Even small transfusions may be enough All patients need careful monitoring and appropriate investigation
59 (unsatisfactory definition) Any 4 of the following occurring within 6h of transfusion Acute respiratory distress Tachycardia Increased blood pressure Acute or worsening pulmonary oedema Evidence of positive fluid balance
60 TRALI TACO Type of component Usually plasma or platelets Any BP Often reduced Often raised Temperature Often raised Normal Echo Normal Abnormal Diuretics Worsen Improve Fluid loading Improves Worsens
61
62
63 An 83-year-old male with refractory anaemia related to CRF received 2 units of RBCs, each over approximately hours. He had continuing bradycardia during the second unit. He remained stable, but the bradycardia persisted at bpm. Within 15 minutes of the start of the 3 rd unit of RBC, he became unresponsive with no cardiac output. Resuscitation was ultimately unsuccessful. A post-mortem examination showed acute LVF, hypertensive heart disease with mitral valve prolapse and hypertensive nephropathy. TACO following RBC transfusion to elderly male with renal impairment and cardiac failure
64 May need investigation in similar way Sustained rise in temperature and/or other systemic symptoms (chills, myalgia, nausea) may indicate bacterial infection or haemolysis Management may include antihistamines, oxygen etc.
65 A woman with Hb SC was transfused 2 units of red cells after an emergency caesarian section 10 days later she presents with Hb 67g/L, fever hypoxia and pain
66 (choose 1) 1. Sickle cell crisis 2. Delayed haemolytic transfusion reaction 3. Bacterial infection 4. Pulmonary embolism
67 She underwent exchange transfusion for sickle crisis but still had symptoms The Hb dropped below pre-transfusion levels with evidence of haemolysis noted on the blood film
68 1. None (choose any that are relevant) 2. Pre and post-transfusion samples for group and antibody detection 3. Direct antiglobulin test 4. Recheck cross match 5. Eluate of pre and post-exchange samples
69 DAT positive with anti-jk a detectable in eluate on pre- and post-exchange samples Four out of six units for exchange transfusion were Jk(a+) The anti-jk a became detectable in the plasma after a couple of days
70 Delayed transfusion reactions in sickle patients may be confused with sickle crises Antibodies may only be detectable by washing them off the red cells (eluate) Sickle cell disease patients are at particular risk of alloimmunisation and missed special requirements because clinicians forget to tell the lab
71 Young woman with history of multiple transfusions admitted with Hb 78g/L Transfused 7 d earlier; raised bilirubin and creatinine on this admission Anti Fy b found now in addition to previously known anti s Two Fy(b-) s- units transfused but during 2 nd unit she had rigors and respiratory arrest
72 ITU admission for a week Investigation: new weak anti-jk a by enzyme only Both units were Jk(a+) as were 2 of the 4 transfused 7 d before Acute and delayed HTR
73 Symptoms Fever >2 o C rise or >39 o C Investigations Standard plus repeat compatibility testing, DAT, LDH and haptoglobin Blood cultures from patient Coagulation screen Do not discard unit Sustained fever: return unit to lab, repeat antibody screen and DAT NB. Standard investigations for all transfusion reactions FBC, renal and liver function, assessment of urine for haemoglobin
74 Symptoms Mucosal swelling Dyspnoea, wheeze or features of anaphylaxis Hypotension (isolated fall systolic of > 30mm resulting in level > 80mm Investigations Standard, plus IgA If <0.07g/L and no general hypogammaglobulinaemia confirm and look for IgA antibodies Standard, plus oxygen saturation/blood gases, CXR; Investigate as for fever If allergy suspected, IgA
75 Definition: sudden onset of thrombocytopenia occurring 5-12 d following red cell transfusion associated with antibodies in the patient directed against human platelet antigen systems. Commoner in women, rare (1-2 pa) Management: IVIg Women are at risk of neonatal alloimmune thrombocytopenia in future pregnancies
76
77 Category Risk per components issued Total risk of death (including probable cases) 1 in 125,000 Total risk of major morbidity 1 in 19,157 Risk of death from error 1 in 454,545 Risk of major morbidity from error 1 in 196,078 Risk of death from TACO 1 in 227,273 Risk of major morbidity from TACO 1 in 81,3000 Risk of major morbidity from ATR 1 in 36,764 Category HBV HCV HIV Risk of infected donation entering blood supply 1 in 1.3 million 1 in 28.6 million 1 in 7.1 million
78 Viral infections Identify and report Establish link with previous transfusion Counselling and management Iron overload Think of this in any chronically transfused patient and do regular assessment of iron loading May be missed in young patients undergoing cancer chemotherapy?
79 ADU IBCT PTP ATR HTR 1 Inappropriate and 5 delayed transfusions 1 ABO incompatible transfusion 1 Post-transfusion purpura 2 Acute transfusion reactions 3 Haemolytic transfusion reactions TRALI 2Transfusion-related acute lung injury TACO 20 Transfusion-associated circulatory overload (n=39) Unclassifiable 3-2 infants with necrotising enterocolitis and 1 adult after IVIg TA-GvHD 1 transfusion-associated graft versus host disease
80 Fludarabine introduced for CLL induces profound lymphopenia TA-GvHD cases reported in 1993, 1994, 1996 Guidelines for irradiated blood components 1996 (latest update 2010) B cell diseases are not an indication on their own for irradiated products

81 Omission of irradiation in 999 patients at risk Many cases missed in patients who have received fludarabine Leucodepletion is protective
82 Patient group Number Treatment with purine analogues 178 Hodgkin lymphoma 68 Haemopoietic stem cell transplants 44 Others 99
83 Reasons for failure to provide irradiated components Haematology clinical staff forget/fail to inform the transfusion laboratory Need for irradiation overlooked when patient is admitted to a different specialty or hospital Need for irradiation is forgotten when historical (e.g. HD, fludarabine many years before) Immune deficiency not recognised (CVID, Di George syndrome) Overlooked in infants needing later top-up transfusion after intrauterine or exchange transfusion
84
85
86 UK Transfusion Laboratory Collaborative 2009 BCSH Guidelines
87 NPSA SPN14 Right patient, right blood competency assessment NPSA SPN11 Patient identification Wristbands SPN 24 NPSA RRR 17 Transfusion in an emergency Better blood transfusion initiatives DH circulars Working group set up to discuss national strategy for haemovigilance SHOT launched Start of NPSA NBTC National comparative audit programme UKTLC Figure 1
88 A programme of clinical audits looking at use and administration of blood and blood components in England and N Wales Funded by the NHSBT Started 2003, in collaboration with the clinical standards unit of the RCP
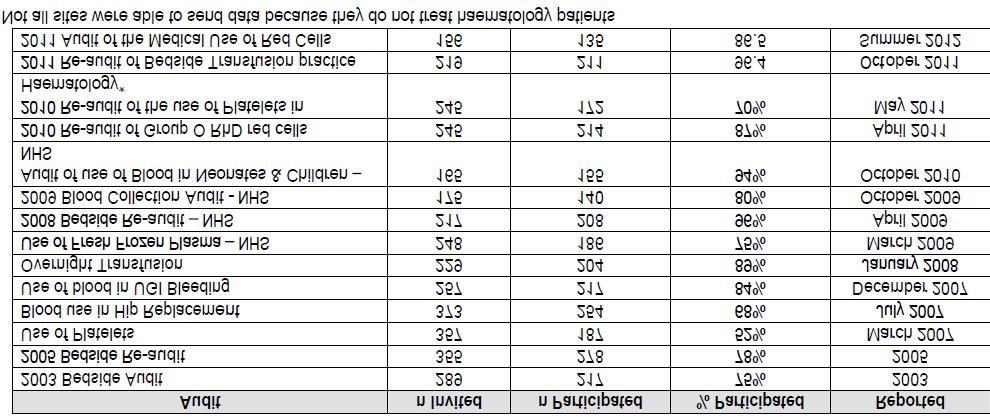
89
90 Identification Documentation Communication
91 Further information available: Educational resources Category definitions Annual Reports (including key to abbreviations)
92 Hazel Tinegate and the transfusion task force of the BCSH for ATR guidelines Hospitals for reporting cases to SHOT SHOT experts and incident specialists
Have you ever managed patients who have experienced an adverse reaction to transfusion?
 Have you ever managed patients who have experienced an adverse reaction to transfusion? A. Yes, often B. Yes, occasionally C. No A. 1 in 30 units? B. 1 in 100? C. 1 in 1000? D. 1 in 10,000? SHOT collects
Have you ever managed patients who have experienced an adverse reaction to transfusion? A. Yes, often B. Yes, occasionally C. No A. 1 in 30 units? B. 1 in 100? C. 1 in 1000? D. 1 in 10,000? SHOT collects
Definitions of Current SHOT Categories & What to Report
 Definitions of Current SHOT Categories & What to Report Revised March 2011 1 ADVERSE EVENTS TERM DEFINITION WHAT TO REPORT IBCT - Wrong Blood Transfused (Incorrect Blood Component Transfused) Where a patient
Definitions of Current SHOT Categories & What to Report Revised March 2011 1 ADVERSE EVENTS TERM DEFINITION WHAT TO REPORT IBCT - Wrong Blood Transfused (Incorrect Blood Component Transfused) Where a patient
Haemovigilance: Acute transfusion reactions. Paula Bolton-Maggs Medical Director Serious Hazards of Transfusion
 Haemovigilance: Acute transfusion reactions Paula Bolton-Maggs Medical Director Serious Hazards of Transfusion SHOT Cumulative data: 18 years n=14822 Deaths related to transfusion reported in 2015 Total
Haemovigilance: Acute transfusion reactions Paula Bolton-Maggs Medical Director Serious Hazards of Transfusion SHOT Cumulative data: 18 years n=14822 Deaths related to transfusion reported in 2015 Total
Transfusion reactions. Jim Taylor Haematology SpR Sheffield
 Transfusion reactions Jim Taylor Haematology SpR Sheffield Pre questions 1. Platelet transfusions are more prone to bacterial contamination compared to red cells. T/F 2. Common causes of an acute transfusion
Transfusion reactions Jim Taylor Haematology SpR Sheffield Pre questions 1. Platelet transfusions are more prone to bacterial contamination compared to red cells. T/F 2. Common causes of an acute transfusion
Pulmonary complications in the Elderly. Paula Bolton-Maggs Medical Director
 Pulmonary complications in the Elderly Paula Bolton-Maggs Medical Director What does SHOT do? Serious Hazards of Transfusion Collect data on serious adverse reactions and events related to transfusion
Pulmonary complications in the Elderly Paula Bolton-Maggs Medical Director What does SHOT do? Serious Hazards of Transfusion Collect data on serious adverse reactions and events related to transfusion
Julie Ball SHOT Clinical Incidents Specialist
 Julie Ball SHOT Clinical Incidents Specialist Surveillance procedures from the collection of blood and its components to the follow up of the recipients To collect and assess information on unexpected
Julie Ball SHOT Clinical Incidents Specialist Surveillance procedures from the collection of blood and its components to the follow up of the recipients To collect and assess information on unexpected
Revised November 2012
 Revised November 2012 1 ADVERSE EVENTS IBCT - Wrong Blood Transfused (Incorrect Blood Component Transfused) IBCT- SRNM (Specific Requirements Not Met) Where a patient was transfused with a blood component
Revised November 2012 1 ADVERSE EVENTS IBCT - Wrong Blood Transfused (Incorrect Blood Component Transfused) IBCT- SRNM (Specific Requirements Not Met) Where a patient was transfused with a blood component
BMS Education Day 28 th January and 4th February 2013
 BMS Education Day 28 th January and 4th February 2013 Category of Reaction 24 hours from the transfusion = DELAYED Infectious Bacterial contamination Viral HIV,
BMS Education Day 28 th January and 4th February 2013 Category of Reaction 24 hours from the transfusion = DELAYED Infectious Bacterial contamination Viral HIV,
Boot Camp Transfusion Reactions
 Boot Camp Transfusion Reactions Dr. Kristine Roland Regional Medical Lead for Transfusion Medicine, VCH Objectives By the end of this session, you should be able to: Describe in common language the potential
Boot Camp Transfusion Reactions Dr. Kristine Roland Regional Medical Lead for Transfusion Medicine, VCH Objectives By the end of this session, you should be able to: Describe in common language the potential
Acute Transfusion Reactions (Allergic, Hypotensive and Severe Febrile) (ATR) n=296 11
 (ATR) n=296 11") REACTIONS IN PATIENTS: Serious adverse reactions including EU definition ANNUAL SHOT REPORT 2015 Acute Transfusion Reactions (Allergic, Hypotensive and Severe Febrile) (ATR) n=296 11 Authors: Janet Birchall,
REACTIONS IN PATIENTS: Serious adverse reactions including EU definition ANNUAL SHOT REPORT 2015 Acute Transfusion Reactions (Allergic, Hypotensive and Severe Febrile) (ATR) n=296 11 Authors: Janet Birchall,
Blood is serious business
 Transfusion at RCH BLOOD TRANSFUSION Anthea Greenway Dept of Clinical Haematology >10000 fresh blood products per year Supports craniofacial and cardiac surgery Support bone marrow, liver transplant and
Transfusion at RCH BLOOD TRANSFUSION Anthea Greenway Dept of Clinical Haematology >10000 fresh blood products per year Supports craniofacial and cardiac surgery Support bone marrow, liver transplant and
Transfusion Reactions. Directed by M-azad March 2012
 Transfusion Reactions Directed by M-azad March 2012 Transfusion Reactions are Adverse reactions associated with the transfusion of blood and its components Transfusion reactions Non-threatening to fatal
Transfusion Reactions Directed by M-azad March 2012 Transfusion Reactions are Adverse reactions associated with the transfusion of blood and its components Transfusion reactions Non-threatening to fatal
Transfusion Reactions. Megan Rowley and Peter Struik
 Transfusion Reactions Megan Rowley and Peter Struik BMS Education Day 28 th January and 4th February 2013 This presentation provides realistic case studies which have been designed with audience participation
Transfusion Reactions Megan Rowley and Peter Struik BMS Education Day 28 th January and 4th February 2013 This presentation provides realistic case studies which have been designed with audience participation
Mary Berg, M.D. Medical Director, Transfusion Services Associate Professor of Pathology University of Colorado Hospital
 Transfusion Reactions/Complications Mary Berg, M.D. Medical Director, Transfusion Services Associate Professor of Pathology University of Colorado Hospital Acute Transfusion Reactions Can be seen with
Transfusion Reactions/Complications Mary Berg, M.D. Medical Director, Transfusion Services Associate Professor of Pathology University of Colorado Hospital Acute Transfusion Reactions Can be seen with
Chapter 13 ADVERSE TRANSFUSION EVENTS
 Chapter 13 ADVERSE TRANSFUSION EVENTS PRACTICE POINTS The most common severe reaction is ABO incompatibility caused by mis-identification or mis-labelling of the blood component, patient or pre-transfusion
Chapter 13 ADVERSE TRANSFUSION EVENTS PRACTICE POINTS The most common severe reaction is ABO incompatibility caused by mis-identification or mis-labelling of the blood component, patient or pre-transfusion
INVESTIGATION OF ADVERSE TRANSFUSION REACTIONS TABLE OF RECOMMENDED TESTS. Type of Reaction Presentation Recommended Tests Follow-up Tests
 Minor Allergic (Urticarial) Urticaria, pruritis, flushing, rash If skin reaction only and mild hives/ rash
Minor Allergic (Urticarial) Urticaria, pruritis, flushing, rash If skin reaction only and mild hives/ rash
Blood Transfusion. Dr William Dooley
 Blood Transfusion Dr William Dooley Plan Cases Blood groups / Indications Procedure Monitoring / Reactions Cases For following cases: - Would you give them a blood transfusion? - How many units you would
Blood Transfusion Dr William Dooley Plan Cases Blood groups / Indications Procedure Monitoring / Reactions Cases For following cases: - Would you give them a blood transfusion? - How many units you would
Transfusion Reactions
 Transfusion Reactions From A to T Provincial Blood Coordinating Program Daphne Osborne MN PANC (C) RN We want you to know Definition Appropriate actions Classification Complete case studies Transfusion
Transfusion Reactions From A to T Provincial Blood Coordinating Program Daphne Osborne MN PANC (C) RN We want you to know Definition Appropriate actions Classification Complete case studies Transfusion
Specific Requirements
 Specific Requirements AIMS Specific requirements your patients have for transfusion and how this is managed Classify which patients require: Irradiated components CMV negative components Washed components
Specific Requirements AIMS Specific requirements your patients have for transfusion and how this is managed Classify which patients require: Irradiated components CMV negative components Washed components
Approach to a patient with suspected blood transfusion reaction. Raju Vaddepally, MD
 Approach to a patient with suspected blood transfusion reaction Raju Vaddepally, MD Goals Detection of Acute Transfusion Reactions (ATR) Clinical and Laboratory Evaluation of ATR Management of individual
Approach to a patient with suspected blood transfusion reaction Raju Vaddepally, MD Goals Detection of Acute Transfusion Reactions (ATR) Clinical and Laboratory Evaluation of ATR Management of individual
Blood Transfusion. Dr Will Dooley
 Blood Transfusion Dr Will Dooley Plan Cases OSCE practice scenario Blood groups Monitoring / Reactions Miss Irene Bleede, 23yo Asymptomatic, healthy woman with menorrhagia Hb 78 g/l, MCV 73fl Would you
Blood Transfusion Dr Will Dooley Plan Cases OSCE practice scenario Blood groups Monitoring / Reactions Miss Irene Bleede, 23yo Asymptomatic, healthy woman with menorrhagia Hb 78 g/l, MCV 73fl Would you
Fifty ways to fail your patient. Haemolytic transfusion reactions
 Fifty ways to fail your patient Haemolytic transfusion reactions Nearly Fifty ways to fail your patient Haemolytic transfusion reactions Acute haemolytic transfusion reaction (AHTR): definition Fever and
Fifty ways to fail your patient Haemolytic transfusion reactions Nearly Fifty ways to fail your patient Haemolytic transfusion reactions Acute haemolytic transfusion reaction (AHTR): definition Fever and
Transfusion Challenges. - Transfusion Reactions - Do they need platelets? Dr. Eoghan Molloy Haem SpR 2016
 Transfusion Challenges - Transfusion Reactions - Do they need platelets? Dr. Eoghan Molloy Haem SpR 2016 Guidance on Transfusion Hospital transfusion guidelines and procedures Irish Blood Transfusion Service
Transfusion Challenges - Transfusion Reactions - Do they need platelets? Dr. Eoghan Molloy Haem SpR 2016 Guidance on Transfusion Hospital transfusion guidelines and procedures Irish Blood Transfusion Service
TRANSFUSION SAFETY 101 ARE YOU SMARTER THAN A BLOOD BANKER?
 TRANSFUSION SAFETY 101 ARE YOU SMARTER THAN A BLOOD BANKER? 1. Fatal blood transfusion reactions are most likely the result of: a. Circulatory overload b. ABO incompatible blood due to patient identification
TRANSFUSION SAFETY 101 ARE YOU SMARTER THAN A BLOOD BANKER? 1. Fatal blood transfusion reactions are most likely the result of: a. Circulatory overload b. ABO incompatible blood due to patient identification
Blood/Blood Component Utilization and Administration Annual Compliance Education
 Blood/Blood Component Utilization and Administration Annual Compliance Education This course contains annual compliance education necessary to meet compliance and regulatory requirements. Instructions:
Blood/Blood Component Utilization and Administration Annual Compliance Education This course contains annual compliance education necessary to meet compliance and regulatory requirements. Instructions:
BLOOD TRANSFUSION. Dr Lumka Ntabeni
 BLOOD TRANSFUSION Dr Lumka Ntabeni Blood transfusion definition SAFE transfer of BLOOD COMPONENTS from a DONOR to a RECEPIENT CONTENT Brief history of blood transfusion How is safety guaranteed? How do
BLOOD TRANSFUSION Dr Lumka Ntabeni Blood transfusion definition SAFE transfer of BLOOD COMPONENTS from a DONOR to a RECEPIENT CONTENT Brief history of blood transfusion How is safety guaranteed? How do
TRANSFUSION REACTIONS
 14 TRANSFUSION REACTIONS 14.1 INTRODUCTION Transfusion of blood and blood products are reported to cause reactions during or after procedure specially in patients who receive multiple transfusions. These
14 TRANSFUSION REACTIONS 14.1 INTRODUCTION Transfusion of blood and blood products are reported to cause reactions during or after procedure specially in patients who receive multiple transfusions. These
Transfusion Medicine Potpourri. BUMC - Phoenix Internal Medicine Residents September 29, 2015
 Transfusion Medicine Potpourri BUMC - Phoenix Internal Medicine Residents September 29, 2015 Clinical case A 24 year old female with sickle cell anemia has just moved to the area and presents as a new
Transfusion Medicine Potpourri BUMC - Phoenix Internal Medicine Residents September 29, 2015 Clinical case A 24 year old female with sickle cell anemia has just moved to the area and presents as a new
Transfusion Errors in Transplant Recipients. Paula Bolton-Maggs Alison Watt Debbi Poles Serious Hazards of Transfusion
 Transfusion Errors in Transplant Recipients Paula Bolton-Maggs Alison Watt Debbi Poles Serious Hazards of Transfusion BBTS September 2016 Transfusion risks in transplantation Patients receiving transplants,
Transfusion Errors in Transplant Recipients Paula Bolton-Maggs Alison Watt Debbi Poles Serious Hazards of Transfusion BBTS September 2016 Transfusion risks in transplantation Patients receiving transplants,
Transfusion-Related Acute Lung Injury (TRALI) and Strategies for Prevention. Khalid Abdulla Sharif, MD, MRCP (UK)*
 and Strategies for Prevention. Khalid Abdulla Sharif, MD, MRCP (UK)*") Bahrain Medical Bulletin, Vol. 29, No.4, December 2007 Transfusion-Related Acute Lung Injury (TRALI) and Strategies for Prevention Khalid Abdulla Sharif, MD, MRCP (UK)* Background: Transfusion-Related
Bahrain Medical Bulletin, Vol. 29, No.4, December 2007 Transfusion-Related Acute Lung Injury (TRALI) and Strategies for Prevention Khalid Abdulla Sharif, MD, MRCP (UK)* Background: Transfusion-Related
Supporting solid organ transplants: Challenges for Blood Transfusion Labs
 Supporting solid organ transplants: Challenges for Blood Transfusion Labs Dora Foukaneli Consultant in Haematology and Transfusion Medicine NHSBT Cambridge and Addenbrooke s Hospital Addenbrooke s Blood
Supporting solid organ transplants: Challenges for Blood Transfusion Labs Dora Foukaneli Consultant in Haematology and Transfusion Medicine NHSBT Cambridge and Addenbrooke s Hospital Addenbrooke s Blood
2/2/2011. Blood Components and Transfusions. Why Blood Transfusion?
 Blood Components and Transfusions Describe blood components Identify nursing responsibilities r/t blood transfusion Discuss factors r/t blood transfusion including blood typing, Rh factor, and cross matching
Blood Components and Transfusions Describe blood components Identify nursing responsibilities r/t blood transfusion Discuss factors r/t blood transfusion including blood typing, Rh factor, and cross matching
Crossmatching and Issuing Blood Components; Indications and Effects.
 Crossmatching and Issuing Blood Components; Indications and Effects. Alison Muir Blood Transfusion, Blood Sciences, Newcastle Trust Topics Covered Taking the blood sample ABO Group Antibody Screening Compatibility
Crossmatching and Issuing Blood Components; Indications and Effects. Alison Muir Blood Transfusion, Blood Sciences, Newcastle Trust Topics Covered Taking the blood sample ABO Group Antibody Screening Compatibility
TACO CASE STUDIES RTC JUNE Kerry Dowling Blood Transfusion Laboratory Manager Jonathan Ricks Blood Transfusion Nurse Practitioner
 TACO CASE STUDIES RTC JUNE 2017 Kerry Dowling Blood Transfusion Laboratory Manager Jonathan Ricks Blood Transfusion Nurse Practitioner RISK FACTORS - TACO Age over 70 years although also seen in younger
TACO CASE STUDIES RTC JUNE 2017 Kerry Dowling Blood Transfusion Laboratory Manager Jonathan Ricks Blood Transfusion Nurse Practitioner RISK FACTORS - TACO Age over 70 years although also seen in younger
Transfusion Reactions. Objectives. 1) Identify a transfusion reaction 25/02/16. Dr Matthew Horan. 1) Identify a transfusion reaction
 Identify a transfusion reaction 25/02/16. Dr Matthew Horan. 1) Identify a transfusion reaction") Transfusion Reactions 25/02/16 Dr Matthew Horan Objectives 1) Identify a transfusion reaction 2) Treat a transfusion reaction 3) Report a transfusion reaction 1) Identify a transfusion reaction Could this
Transfusion Reactions 25/02/16 Dr Matthew Horan Objectives 1) Identify a transfusion reaction 2) Treat a transfusion reaction 3) Report a transfusion reaction 1) Identify a transfusion reaction Could this
All institutions that transfuse blood components and products should implement national and local policies and written procedures for:
 5.0 GENERAL GUIDE TO GOOD TRANSFUSION PRACTICE Blood and the various components prepared or manufactured from it are biologic (in the case of blood cells, living human tissues) products intended for use
5.0 GENERAL GUIDE TO GOOD TRANSFUSION PRACTICE Blood and the various components prepared or manufactured from it are biologic (in the case of blood cells, living human tissues) products intended for use
Administration of blood components. Tina Parker - Transfusion Practitioner
 . Administration of blood components Tina Parker - Transfusion Practitioner Red Cells Each unit contains 250-350mls Preserved with glucose and Mannitol to keep the correct tension Lasts 35 days from midnight
. Administration of blood components Tina Parker - Transfusion Practitioner Red Cells Each unit contains 250-350mls Preserved with glucose and Mannitol to keep the correct tension Lasts 35 days from midnight
Dr Rock LEUNG Transfusion Safety Officer Queen Mary Hospital, Hong Kong West Cluster
 Dr Rock LEUNG Transfusion Safety Officer Queen Mary Hospital, Hong Kong West Cluster HOSPITAL TRANSFUSION SERVICE IN HK Single supplier for the territory: HK Red Cross Blood Transfusion Service Public
Dr Rock LEUNG Transfusion Safety Officer Queen Mary Hospital, Hong Kong West Cluster HOSPITAL TRANSFUSION SERVICE IN HK Single supplier for the territory: HK Red Cross Blood Transfusion Service Public
Alister Jones Patient Blood Management Practitioner NHS Blood and Transplant. Lab Matters study day Oake Manor, Taunton, 8 th July 2015
 Alister Jones Patient Blood Management Practitioner NHS Blood and Transplant Lab Matters study day Oake Manor, Taunton, 8 th July 2015 NPSA Rapid Response Report 2010 Transfusion of blood and blood components
Alister Jones Patient Blood Management Practitioner NHS Blood and Transplant Lab Matters study day Oake Manor, Taunton, 8 th July 2015 NPSA Rapid Response Report 2010 Transfusion of blood and blood components
Blood Transfusion Reactions
 Blood Transfusion Reactions Introduction Many individuals require blood components and blood products. As per the BC Transfusion Medicine Advisory Group (BCTMAG), a blood component is at therapeutic component
Blood Transfusion Reactions Introduction Many individuals require blood components and blood products. As per the BC Transfusion Medicine Advisory Group (BCTMAG), a blood component is at therapeutic component
Transfusion reactions illustrated
 Transfusion reactions illustrated Chapter 1 Transfusion practice 1 Procedure of transfusion practice In general, transfusion-associated incidents occur due to multiple errors, most of which occur in the
Transfusion reactions illustrated Chapter 1 Transfusion practice 1 Procedure of transfusion practice In general, transfusion-associated incidents occur due to multiple errors, most of which occur in the
Non-Medical Authorisation Course
 Non-Medical Authorisation Course November 2017 Authorising, Prescribing & Sampling Janice Smith Matron Transfusion Specialist Aims of this session To discuss and understand: Authorising blood / blood components
Non-Medical Authorisation Course November 2017 Authorising, Prescribing & Sampling Janice Smith Matron Transfusion Specialist Aims of this session To discuss and understand: Authorising blood / blood components
Haemovigilance Report 2013
 Haemovigilance Report 213 Haemovigilance Report 213 Privacy Statement This report does not identify or attempt to identify individual patients, clinicians or healthcare institutions, and every reasonable
Haemovigilance Report 213 Haemovigilance Report 213 Privacy Statement This report does not identify or attempt to identify individual patients, clinicians or healthcare institutions, and every reasonable
25/10/2017. Clinical Relevance of the HLA System in Blood Transfusion. Outline of talk. Major Histocompatibility Complex
 Clinical Relevance of the HLA System in Blood Transfusion Dr Colin J Brown PhD FRCPath. October 2017 Outline of talk HLA genes, structure and function HLA and immune complications of transfusion TA-GVHD
Clinical Relevance of the HLA System in Blood Transfusion Dr Colin J Brown PhD FRCPath. October 2017 Outline of talk HLA genes, structure and function HLA and immune complications of transfusion TA-GVHD
SICKLE CELL AWARENESS. The Sickle Cell Society has produced the following information leaflets available at sicklecellsociety.org
 sickle cell disease in the UK Sickle cell disease (SCD) affects around 15,000 people in the UK People with Sickle Cell Disease have Sickle haemoglobin (HbS) which can make red blood cells rigid and sickle-shaped
sickle cell disease in the UK Sickle cell disease (SCD) affects around 15,000 people in the UK People with Sickle Cell Disease have Sickle haemoglobin (HbS) which can make red blood cells rigid and sickle-shaped
COMPLICATIONS OF BLOOD TRANSFUSIONS. :Prepared by Dr. Nawal Mogales & Dr. Mohammed Aqlan
 COMPLICATIONS OF BLOOD TRANSFUSIONS :Prepared by Dr. Nawal Mogales & Dr. Mohammed Aqlan COMPLICATIONS OF TRANSFUSIONS Transfusion reaction may result from either : A. Immune transfusion reaction. B. Non
COMPLICATIONS OF BLOOD TRANSFUSIONS :Prepared by Dr. Nawal Mogales & Dr. Mohammed Aqlan COMPLICATIONS OF TRANSFUSIONS Transfusion reaction may result from either : A. Immune transfusion reaction. B. Non
Prevention of TACO what Haemovigilance data tell us
 Prevention of TACO what Haemovigilance data tell us Swisstransfusion, Genève 6. Septembre 03 Markus Jutzi, Morven Rüesch Clinical Reviewer Haemovigilance, Swissmedic Swissmedic Schweizerisches Heilmittelinstitut
Prevention of TACO what Haemovigilance data tell us Swisstransfusion, Genève 6. Septembre 03 Markus Jutzi, Morven Rüesch Clinical Reviewer Haemovigilance, Swissmedic Swissmedic Schweizerisches Heilmittelinstitut
What You Need to Know About Blood Transfusion. Elianna Saidenberg May 2014
 What You Need to Know About Blood Transfusion Elianna Saidenberg May 2014 Objectives Why your doctor might order transfusion therapy Where does the blood come from The beginning of your transfusion Consent
What You Need to Know About Blood Transfusion Elianna Saidenberg May 2014 Objectives Why your doctor might order transfusion therapy Where does the blood come from The beginning of your transfusion Consent
Why the Hospital Transfusion laboratory may challenge the use of O D negative blood in an emergency.
 Why the Hospital Transfusion laboratory may challenge the use of O D negative blood in an emergency. Carly Lattimore Blood Bank Team Manager Chesterfield Royal Hospital Why the laboratory may challenge
Why the Hospital Transfusion laboratory may challenge the use of O D negative blood in an emergency. Carly Lattimore Blood Bank Team Manager Chesterfield Royal Hospital Why the laboratory may challenge
CrackCast Episode 7 Blood and Blood Components
 CrackCast Episode 7 Blood and Blood Components Episode Overview: 1) Describe the 3 categories of blood antigens 2) Who is the universal donor and why? 3) Define massive transfusion 4) List 5 physiologic
CrackCast Episode 7 Blood and Blood Components Episode Overview: 1) Describe the 3 categories of blood antigens 2) Who is the universal donor and why? 3) Define massive transfusion 4) List 5 physiologic
Essential Transfusion. Medical Students
 Essential Transfusion Medical Students Aim is to ensure that the student has knowledge of an acceptable and safe level for the authorisation of blood and blood components, and the management of a suspected
Essential Transfusion Medical Students Aim is to ensure that the student has knowledge of an acceptable and safe level for the authorisation of blood and blood components, and the management of a suspected
Information for patients with Sickle Cell Disease who may need a blood transfusion. Patient information
 Information for patients with Sickle Cell Disease who may need a blood transfusion Patient information This information leaflet answers some of the questions you may have about having a blood transfusion
Information for patients with Sickle Cell Disease who may need a blood transfusion Patient information This information leaflet answers some of the questions you may have about having a blood transfusion
Alister Jones Patient Blood Management Practitioner NHS Blood and Transplant
 Alister Jones Patient Blood Management Practitioner NHS Blood and Transplant All medical RCC transfusions (but only 1 in 3 haematology or oncology cases) in 3 x one week periods Medical specialties include:
Alister Jones Patient Blood Management Practitioner NHS Blood and Transplant All medical RCC transfusions (but only 1 in 3 haematology or oncology cases) in 3 x one week periods Medical specialties include:
EUROPEAN COMMISSION DIRECTORATE GENERAL FOR HEALTH AND FOOD SAFETY
 Ref. Ares(2016)5909621-13/10/2016 EUROPEAN COMMISSION DIRECTORATE GENERAL FOR HEALTH AND FOOD SAFETY Directorate B - Health systems, medical products and innovation B4 Medical products: quality, safety
Ref. Ares(2016)5909621-13/10/2016 EUROPEAN COMMISSION DIRECTORATE GENERAL FOR HEALTH AND FOOD SAFETY Directorate B - Health systems, medical products and innovation B4 Medical products: quality, safety
Transfusion 2004: Current Practice Standards. Kay Elliott, MT (ASCP) SBB SWMC Transfusion Service
 SBB SWMC Transfusion Service") Transfusion 2004: Current Practice Standards Kay Elliott, MT (ASCP) SBB SWMC Transfusion Service Massive Transfusion Protocol (MTP) When should it be activated? Massive bleeding i.e. loss of one blood
Transfusion 2004: Current Practice Standards Kay Elliott, MT (ASCP) SBB SWMC Transfusion Service Massive Transfusion Protocol (MTP) When should it be activated? Massive bleeding i.e. loss of one blood
Elements for a Public Summary
 VI.2 VI.2.1 Elements for a Public Summary Overview of disease epidemiology Nanogam is intended to be used for the treatment of diseases in patients who are suffering from a shortage of immunoglobulins
VI.2 VI.2.1 Elements for a Public Summary Overview of disease epidemiology Nanogam is intended to be used for the treatment of diseases in patients who are suffering from a shortage of immunoglobulins
Olive J Sturtevant, MHP, MT(ASCP)SBB/SLS, CQA Director, Cellular Therapy Quality Assurance Dana Farber Cancer Institute
SBB/SLS, CQA Director, Cellular Therapy Quality Assurance Dana Farber Cancer Institute") Adverse Events associated with Cell Therapy Products Olive J Sturtevant, MHP, MT(ASCP)SBB/SLS, CQA Director, Cellular Therapy Quality Assurance Dana Farber Cancer Institute 2 Objectives Review the types
Adverse Events associated with Cell Therapy Products Olive J Sturtevant, MHP, MT(ASCP)SBB/SLS, CQA Director, Cellular Therapy Quality Assurance Dana Farber Cancer Institute 2 Objectives Review the types
In The Name Of GOD ADVERSE REACTIONS OF TRANSFUSION
 In The Name Of GOD The 7 th international and 12 th national congress on quality improvement in clinical laboratories ADVERSE REACTIONS OF TRANSFUSION By Mehdi Allahbakhshian, PhD, Hematology and Blood
In The Name Of GOD The 7 th international and 12 th national congress on quality improvement in clinical laboratories ADVERSE REACTIONS OF TRANSFUSION By Mehdi Allahbakhshian, PhD, Hematology and Blood
ALL Blood Transfusion samples must be hand-written in accordance with the Trust's Blood Administration Protocol
 Blood Transfusion Routine Investigations ALL Blood Transfusion samples must be hand-written in accordance with the Trust's Blood Administration Protocol Full Group & Screen 2ml EDTA Can be stored at 2-8C
Blood Transfusion Routine Investigations ALL Blood Transfusion samples must be hand-written in accordance with the Trust's Blood Administration Protocol Full Group & Screen 2ml EDTA Can be stored at 2-8C
For more information about how to cite these materials visit
 Author(s): Robertson Davenport, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author(s): Robertson Davenport, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
REPORT OF TRANSFUSION ADVERSE REACTION TO BLOOD CENTERS
 REPORT OF TRANSFUSION ADVERSE REACTION TO BLOOD CENTERS INSTRUCTIONS: Send the form to ALL blood centers that provided blood components to this patient. Timely reporting is important, so that, if appropriate,
REPORT OF TRANSFUSION ADVERSE REACTION TO BLOOD CENTERS INSTRUCTIONS: Send the form to ALL blood centers that provided blood components to this patient. Timely reporting is important, so that, if appropriate,
Transfusion Reactions:
 Transfusion Reactions: Melissa R. George, D.O., F.C.A.P. Medical Director, Transfusion Medicine & Apheresis Penn State Milton S. Hershey Medical Center Office: HG069, Phone: 717-531-4627 E-mail: mgeorge5@hmc.psu.edu
Transfusion Reactions: Melissa R. George, D.O., F.C.A.P. Medical Director, Transfusion Medicine & Apheresis Penn State Milton S. Hershey Medical Center Office: HG069, Phone: 717-531-4627 E-mail: mgeorge5@hmc.psu.edu
EUROPEAN COMMISSION HEALTH AND FOOD SAFETY DIRECTORATE-GENERAL
 Ref. Ares(2015)2319265-03/06/2015 EUROPEAN COMMISSION HEALTH AND FOOD SAFETY DIRECTORATE-GENERAL Directorate D - Health systems and products D4 Substances of Human Origin and Tobacco Control Brussels,
Ref. Ares(2015)2319265-03/06/2015 EUROPEAN COMMISSION HEALTH AND FOOD SAFETY DIRECTORATE-GENERAL Directorate D - Health systems and products D4 Substances of Human Origin and Tobacco Control Brussels,
Transfusion in Sickle Cell Disease What the guidelines [are likely to] say. Dr Bernard Davis Whittington Hospital, London
![Transfusion in Sickle Cell Disease What the guidelines [are likely to] say. Dr Bernard Davis Whittington Hospital, London](/thumbs/85/91702350.jpg "Transfusion in Sickle Cell Disease What the guidelines [are likely to] say. Dr Bernard Davis Whittington Hospital, London") Transfusion in Sickle Cell Disease What the guidelines [are likely to] say Dr Bernard Davis Whittington Hospital, London Background to BCSH Guideline Rationale Current guidance in disparate publications
Transfusion in Sickle Cell Disease What the guidelines [are likely to] say Dr Bernard Davis Whittington Hospital, London Background to BCSH Guideline Rationale Current guidance in disparate publications
Clinical Relevance of the HLA System in Blood Transfusion. Dr Colin J Brown PhD FRCPath. October 2017
 Clinical Relevance of the HLA System in Blood Transfusion Dr Colin J Brown PhD FRCPath. October 2017 Outline of talk HLA genes, structure and function HLA and immune complications of transfusion TA-GVHD
Clinical Relevance of the HLA System in Blood Transfusion Dr Colin J Brown PhD FRCPath. October 2017 Outline of talk HLA genes, structure and function HLA and immune complications of transfusion TA-GVHD
Jo Shorthouse. With thanks to Dr Kate Pendry. Consultant Haematologist Central Manchester Hospitals. and. Clinical Director for PBM NHSBT
 Jo Shorthouse With thanks to Dr Kate Pendry Consultant Haematologist Central Manchester Hospitals and Clinical Director for PBM NHSBT What is Patient Blood Management? Why is Patient Blood Management important?
Jo Shorthouse With thanks to Dr Kate Pendry Consultant Haematologist Central Manchester Hospitals and Clinical Director for PBM NHSBT What is Patient Blood Management? Why is Patient Blood Management important?
Blood Transfusion Guidelines in Clinical Practice
 Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
Human Albumin Solution Infusion (HAS) - Guideline for practice
 - Guideline for practice") Human Albumin (HAS) - Guideline for practice SharePoint Location Clinical Policies and Guidelines SharePoint Index Directory General Policies and Guidelines Sub Area Haematology and Blood Transfusion Key
Human Albumin (HAS) - Guideline for practice SharePoint Location Clinical Policies and Guidelines SharePoint Index Directory General Policies and Guidelines Sub Area Haematology and Blood Transfusion Key
Febrile Non-haemolytic Transfusion Reactions. Sue Knowles Epsom and St Helier University Hospitals NHS Trust. Copyright BBTS 2008
 Febrile Nonhaemolytic Transfusion Reactions Sue Knowles Epsom and St Helier University Hospitals NHS Trust As many questions as answers Pathophysiology? Frequency following prestorage leucodepletion? How
Febrile Nonhaemolytic Transfusion Reactions Sue Knowles Epsom and St Helier University Hospitals NHS Trust As many questions as answers Pathophysiology? Frequency following prestorage leucodepletion? How
Chapter 17: Transfusion-Transmitted Infections (TTI)
") Annual SHOT Report 2014 Supplementary Information Chapter 17: Transfusion-Transmitted s (TTI) The table below is an excerpt from the full Table 17.2 which can be viewed in the main report. Case reports
Annual SHOT Report 2014 Supplementary Information Chapter 17: Transfusion-Transmitted s (TTI) The table below is an excerpt from the full Table 17.2 which can be viewed in the main report. Case reports
Red blood cell transfusion
 Red blood cell transfusion This leaflet explains more about red blood cell transfusion, including the benefits, risks and any alternatives and what you can expect when you come to hospital. If you have
Red blood cell transfusion This leaflet explains more about red blood cell transfusion, including the benefits, risks and any alternatives and what you can expect when you come to hospital. If you have
Carol Cantwell Blood Transfusion Laboratory Manager St Mary s Hospital, ICHNT
 Carol Cantwell Blood Transfusion Laboratory Manager St Mary s Hospital, ICHNT History Why is blood transfusion involved? What tests are performed in blood transfusion and why? What does a protocol look
Carol Cantwell Blood Transfusion Laboratory Manager St Mary s Hospital, ICHNT History Why is blood transfusion involved? What tests are performed in blood transfusion and why? What does a protocol look
Blood transfusion. Dr. J. Potgieter Dept. of Haematology NHLS - TAD
 Blood transfusion Dr. J. Potgieter Dept. of Haematology NHLS - TAD General Blood is collected from volunteer donors >90% is separated into individual components and plasma Donors should be: healthy, have
Blood transfusion Dr. J. Potgieter Dept. of Haematology NHLS - TAD General Blood is collected from volunteer donors >90% is separated into individual components and plasma Donors should be: healthy, have
Transfusion Associated Acute Lung Injury (TRALI)
") Transfusion Associated Acute Lung Injury (TRALI) Chris Beritela, MS, MT(ASCP)SBB Area Technical Consultant Immucor, Inc. Objectives Define Transfusion-Related Acute Lung Injury (TRALI) and the role of
Transfusion Associated Acute Lung Injury (TRALI) Chris Beritela, MS, MT(ASCP)SBB Area Technical Consultant Immucor, Inc. Objectives Define Transfusion-Related Acute Lung Injury (TRALI) and the role of
Transfusion Associated Acute Lung Injury (TRALI) Chris Beritela, MS, MT(ASCP)SBB Area Technical Consultant Immucor, Inc.
 Chris Beritela, MS, MT(ASCP)SBB Area Technical Consultant Immucor, Inc.") Transfusion Associated Acute Lung Injury (TRALI) Chris Beritela, MS, MT(ASCP)SBB Area Technical Consultant Immucor, Inc. Objectives Define Transfusion-Related Acute Lung Injury (TRALI) and the role of
Transfusion Associated Acute Lung Injury (TRALI) Chris Beritela, MS, MT(ASCP)SBB Area Technical Consultant Immucor, Inc. Objectives Define Transfusion-Related Acute Lung Injury (TRALI) and the role of
TRANSFUSION REACTION EVALUATION
 Lab Dept: Test Name: Transfusion Services TRANSFUSION REACTION EVALUATION General Information Lab Order Codes: Synonyms: CPT Codes: Test Includes: TRXR Transfusion Complication Workup; Hemolytic reaction
Lab Dept: Test Name: Transfusion Services TRANSFUSION REACTION EVALUATION General Information Lab Order Codes: Synonyms: CPT Codes: Test Includes: TRXR Transfusion Complication Workup; Hemolytic reaction
Annual SHOT Report 2016 Supplementary Information. Chapter 17: Transfusion-Transmitted Infections (TTI)
") Annual SHOT Report 2016 Supplementary Information Chapter 17: Transfusion-Transmitted s (TTI) The table below is an excerpt from the full Table 17.3 which can be viewed in the main report. Case reports
Annual SHOT Report 2016 Supplementary Information Chapter 17: Transfusion-Transmitted s (TTI) The table below is an excerpt from the full Table 17.3 which can be viewed in the main report. Case reports
MB Guideline 7. Transfusion Reaction- Identification, Management and Reporting
 MB Guideline 7 Transfusion Reaction- Identification, Management and Reporting When any unexpected or untoward sign or symptom occurs during or shortly after the transfusion of a blood component, a transfusion
MB Guideline 7 Transfusion Reaction- Identification, Management and Reporting When any unexpected or untoward sign or symptom occurs during or shortly after the transfusion of a blood component, a transfusion
Blood Components & Indications for Transfusion. Neda Kalhor
 Blood Components & Indications for Transfusion Neda Kalhor Blood products Cellular Components: Red blood cells - Leukocyte-reduced RBCs - Washed RBCs - Irradiated RBCs Platelets - Random-donor platelets
Blood Components & Indications for Transfusion Neda Kalhor Blood products Cellular Components: Red blood cells - Leukocyte-reduced RBCs - Washed RBCs - Irradiated RBCs Platelets - Random-donor platelets
A Transfusion Reaction What Do I Do Now? Judith A. Sullivan, MS, MT(ASCP)SBB, CQA(ASQ) ASCLS Region III Triennial Meeting Birmingham AL
SBB, CQA(ASQ) ASCLS Region III Triennial Meeting Birmingham AL") A Transfusion Reaction What Do I Do Now? Judith A. Sullivan, MS, MT(ASCP)SBB, CQA(ASQ) ASCLS Region III Triennial Meeting Birmingham AL This promotional educational activity is brought to you by Ortho
A Transfusion Reaction What Do I Do Now? Judith A. Sullivan, MS, MT(ASCP)SBB, CQA(ASQ) ASCLS Region III Triennial Meeting Birmingham AL This promotional educational activity is brought to you by Ortho
Blood Transfusion. What is blood transfusion? What are blood banks? When is a blood transfusion needed? Who can donate blood?
 What is blood transfusion? A blood transfusion is a safe, common procedure in which blood is given through an intravenous (IV) line in one of the blood vessels. A blood transfusion usually takes two to
What is blood transfusion? A blood transfusion is a safe, common procedure in which blood is given through an intravenous (IV) line in one of the blood vessels. A blood transfusion usually takes two to
ISBN: Haemovigilance Report 2011
 ISBN: 978-0-620-56980-4 Haemovigilance Report 2011 South African Haemovigilance Report 2011 1 Privacy Statement This report does not identify or attempt to identify individual patients, clinicians or
ISBN: 978-0-620-56980-4 Haemovigilance Report 2011 South African Haemovigilance Report 2011 1 Privacy Statement This report does not identify or attempt to identify individual patients, clinicians or
A transfusion reaction is any adverse effect of transfusion therapy which occurs during or after administration of a blood component
 Brenda C. Barnes, Ph.D., MT(ASCP)SBB 1/2015 1 A transfusion reaction is any adverse effect of transfusion therapy which occurs during or after administration of a blood component Transfusion of any blood
Brenda C. Barnes, Ph.D., MT(ASCP)SBB 1/2015 1 A transfusion reaction is any adverse effect of transfusion therapy which occurs during or after administration of a blood component Transfusion of any blood
Learning Objectives: At the end of this exercise, the student will be able to:
 Applications in Transfusion Medicine- A CBL Exercise- Student Guide 1 Title: Applications in Transfusion Medicine A CBL Exercise Purpose: At the conclusion of this exercise, students will be able to apply
Applications in Transfusion Medicine- A CBL Exercise- Student Guide 1 Title: Applications in Transfusion Medicine A CBL Exercise Purpose: At the conclusion of this exercise, students will be able to apply
Laboratory Empowerment. Debbie Asher Adrian Ebbs Transfusion Laboratory Managers, Eastern Pathology Alliance
 Laboratory Empowerment Debbie Asher Adrian Ebbs Transfusion Laboratory Managers, Eastern Pathology Alliance Why? Electronic ICE requesting was in use for requesting red cells NBTC Indication Codes were
Laboratory Empowerment Debbie Asher Adrian Ebbs Transfusion Laboratory Managers, Eastern Pathology Alliance Why? Electronic ICE requesting was in use for requesting red cells NBTC Indication Codes were
COMPANY CORE PACKAGE INSERT CCPI (PI/CORE/ENGLISH)
") COMPANY CORE PACKAGE INSERT CCPI (PI/CORE/ENGLISH) HUMAN ALBUMIN 20 % BEHRING Rev.: 05-MAR-2008 / PEI approval 26.02.08 Supersedes previous versions Rev.: 28-NOV-2007 / Adaptation to Core SPC Rev.: 02-JAN-2007
COMPANY CORE PACKAGE INSERT CCPI (PI/CORE/ENGLISH) HUMAN ALBUMIN 20 % BEHRING Rev.: 05-MAR-2008 / PEI approval 26.02.08 Supersedes previous versions Rev.: 28-NOV-2007 / Adaptation to Core SPC Rev.: 02-JAN-2007
EDUCATIONAL COMMENTARY TRANSFUSION-RELATED ACUTE LUNG INJURY
 EDUCATIONAL COMMENTARY TRANSFUSION-RELATED ACUTE LUNG INJURY Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
EDUCATIONAL COMMENTARY TRANSFUSION-RELATED ACUTE LUNG INJURY Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
Non-Infectious Transfusion Reactions
 Non-Infectious Transfusion Reactions Transfusion Reactions ANY unfavorable consequence is considered a transfusion reaction of blood TX The risks of transfusion must be weighed against the benefits Transfusion
Non-Infectious Transfusion Reactions Transfusion Reactions ANY unfavorable consequence is considered a transfusion reaction of blood TX The risks of transfusion must be weighed against the benefits Transfusion
Thinking Twice About Transfusions: When TACOS and TRALIs Turn Treatment Into Tragedy. Megan Boysen Osborn, MD, MHPE
 Thinking Twice About Transfusions: When TACOS and TRALIs Turn Treatment Into Tragedy Megan Boysen Osborn, MD, MHPE Let s TACO bout Transfusion Reactions Megan Boysen Osborn, MD, MHPE Let s TACO bout Transfusion
Thinking Twice About Transfusions: When TACOS and TRALIs Turn Treatment Into Tragedy Megan Boysen Osborn, MD, MHPE Let s TACO bout Transfusion Reactions Megan Boysen Osborn, MD, MHPE Let s TACO bout Transfusion
WRHA Blood Conservation Service WRHA Transfusion Practice Committee. TEAM TRANSFUSION Differential Diagnosis of Adverse Events
 WRHA Blood Conservation Service WRHA Transfusion Practice Committee TEAM TRANSFUSION Differential Diagnosis of Adverse Events MANITOBA ADVERSE EVENT REPORTING SYSTEM DATA FLOW REACTION Physician orders
WRHA Blood Conservation Service WRHA Transfusion Practice Committee TEAM TRANSFUSION Differential Diagnosis of Adverse Events MANITOBA ADVERSE EVENT REPORTING SYSTEM DATA FLOW REACTION Physician orders
All you wanted to know about transfusion support for transplants
 All you wanted to know about transfusion support for transplants Dr Dora Foukaneli NHSBT and Addenbrooke s Hospital Cambridge When / why / why not? What ABO group? Do other groups matter? Transplantation
All you wanted to know about transfusion support for transplants Dr Dora Foukaneli NHSBT and Addenbrooke s Hospital Cambridge When / why / why not? What ABO group? Do other groups matter? Transplantation
GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS
 CHILDREN S HOSPITALS AND CLINICS OF MINNESOTA Introduction: GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS These guidelines have been developed in conjunction with the hospital Transfusion Committee.
CHILDREN S HOSPITALS AND CLINICS OF MINNESOTA Introduction: GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS These guidelines have been developed in conjunction with the hospital Transfusion Committee.
Management of TRALI. Handouts. Continuing Education 5/20/2015.
 Management of TRALI Christine Beritela, MS, MT(ASCP)SBB Area Technical Consultant Immucor, Inc. Massimo Mangiola, Ph.D. Director of Special Services Rhode Island Blood Center Handouts http://www.immucor.com/enus/pages/educational-program-handouts.aspx
Management of TRALI Christine Beritela, MS, MT(ASCP)SBB Area Technical Consultant Immucor, Inc. Massimo Mangiola, Ph.D. Director of Special Services Rhode Island Blood Center Handouts http://www.immucor.com/enus/pages/educational-program-handouts.aspx
LifeBridge Health Transfusion Service Sinai Hospital of Baltimore Northwest Hospital Center BQA Transfusion Criteria Version#2 POLICY NO.
 LifeBridge Health Transfusion Service Sinai Hospital of Baltimore Northwest Hospital Center BQA 1011.02 Transfusion Criteria Version#2 Department POLICY NO. PAGE NO. Blood Bank Quality Assurance Manual
LifeBridge Health Transfusion Service Sinai Hospital of Baltimore Northwest Hospital Center BQA 1011.02 Transfusion Criteria Version#2 Department POLICY NO. PAGE NO. Blood Bank Quality Assurance Manual
Clinical Transfusion Practice Guidelines for Medical Interns
 Clinical Transfusion Practice Guidelines for Medical Interns www.onlinelaege.com Foreword Blood transfusion is an important part of day to day clinical practice. Blood and blood products provide unique
Clinical Transfusion Practice Guidelines for Medical Interns www.onlinelaege.com Foreword Blood transfusion is an important part of day to day clinical practice. Blood and blood products provide unique
Blood transfusion as a management strategy for Haemoglobinopathy. Corrina McMahon Our Lady s Children s Hospital, Dublin, Ireland
 Blood transfusion as a management strategy for Haemoglobinopathy Corrina McMahon Our Lady s Children s Hospital, Dublin, Ireland Rationale for BT Sickle cell Disease Reduce the production of Hb Significant
Blood transfusion as a management strategy for Haemoglobinopathy Corrina McMahon Our Lady s Children s Hospital, Dublin, Ireland Rationale for BT Sickle cell Disease Reduce the production of Hb Significant
Transporting Patients with Blood Transfusions
 Transporting Patients with Blood Transfusions Acknowledgement This training package was created by Bronwyn Cadd - ECP and NSQHS Standards Project Clinical Lead. Please direct any questions to your CSO
Transporting Patients with Blood Transfusions Acknowledgement This training package was created by Bronwyn Cadd - ECP and NSQHS Standards Project Clinical Lead. Please direct any questions to your CSO
Essentials of Blood Group Antigens and Antibodies
 Essentials of Blood Group Antigens and Antibodies Non-Medical Authorisation of blood Components Nov 2017 East Midlands Regional Transfusion Committee Transfusion Terminology Antigens and Antibodies Antibodies
Essentials of Blood Group Antigens and Antibodies Non-Medical Authorisation of blood Components Nov 2017 East Midlands Regional Transfusion Committee Transfusion Terminology Antigens and Antibodies Antibodies
Patient Blood Management. Marisa B. Marques, MD UAB Department of Pathology November 17, 2016
 Patient Blood Management Marisa B. Marques, MD UAB Department of Pathology November 17, 2016 Learning Objectives Upon completion of the session, the participant will: 1) Differentiate between the various
Patient Blood Management Marisa B. Marques, MD UAB Department of Pathology November 17, 2016 Learning Objectives Upon completion of the session, the participant will: 1) Differentiate between the various