Algorithm for Haematuria
|
|
|
- Bartholomew Peters
- 6 years ago
- Views:
Transcription
1 Procedure that produces the answer to a question or the solution to a problem in a finite number of steps. Algorithm for Haematuria Helen Forristal MSc (ANP) BSc (Hons) IAUN 2013

2

3

4
 Painful Painless Nephrological Urological")
5 Haematuria presence of Red Blood Cells in the urine. Distinctions Macroscopic Microscopic (Cameron 1996) Painful Painless Nephrological Urological Differential Diagnosis Initial Terminal Total

6 Haematuria There is a poor correlation between the degree of haematuria and the severity of any underlying cause. An older person with visible haematuria is more likely to have serious underlying pathology than a younger person with microscopic haematuria and no symptoms. All people with haematuria need further investigation. Diagnostic tests and algorithms used in the investigation of haematuria available at )

7 Haematuria Kidney- Trauma (Blunt Penetrating) Calculi; Tumours : Carcinoma of the Renal Parenchyma; Benign Renal Tumours, TCC Renal Pelvis Angiomyolipoma Infections: TB, Pyogenic Infections Congenital disorders: Polycystic kidney disease, Renal Cysts Bleeding Disorders: haemophilia ; leukaemia, sickle cell disease, Anticoagulation therapy Vascular causes : Renal Emboli, Renal vein thrombosis Interstitial Renal Disease Glomerularnephritis, pyelonephritis, papillary necrosis Bladder Trauma Infections-, TB, Schistomiasis, Stone disease Carcinoma - 90%, TCC, SCC, Adenocarcinoma Radiation Haemorrhagic Cystitis Exercise Induced haematuria Pharmacology - Cyclophosphamide Prostate BPH, Adenocarcinoma 90% Prostatitis Urethra and Penis Trauma Urethral and penile tumours -!% Urethritis
8 Haematuria How is haematuria diagnosed? Clinical Assessment Physical Assessment ( DRE and PV examination) Urine test strip Urinalysis for culture and sensitivity Cytology Laboratory investigations Interventional tests eg. Cystoscopy Radiology investigations
.")
9 Natasha, a 53 year old lady presented during routine follow up with a three week history of macroscopic haematuria, dysuria, frequency, hesitancy, polyuria, incomplete voids, urinary incontinence and abdominal discomfort. This was further aggravated by walking and pain was relieved by simple analgesia. Natasha was diagnosed with asthma 24 years ago but this has not been troublesome. (2 Algorithm). Presently fit, takes alcohol socially and stopped smoking 12 years ago. In 2008 she was diagnosed with a muscle invasive bladder cancer and subsequently received radical radiotherapy which was complete June 2009.
10 Clinical Assessment (1) The initial clinical evaluation should provide indications as to the Cause of haematuria Help to eliminate potential benign causes, for example vigorous exercise, menstruation and trauma. (3 Algorithm). Specific questioning regarding health history (4 Algorithm) with focused physical assessment should lead to a number of possible differential diagnoses. (5- Algorithm). Risk factors for significant disease include: Smoking history Occupational exposure to chemicals History of gross haematuria age over 40 years Urological disease Urinary tract infection Analgesic abuse Pelvic irradiation. (Grossfield et al 2001)
11 Clinical Assessment (2) Common or concerning symptoms such as: Fatigue and weakness Changes in weight Fever, chills, night sweats Pain are non specific symptoms but could be associated with some of the differential diagnoses. (4- Algorithm)
12 Physical Assessment (1) Haemodynamic status Abdominal examination: Natasha was complaining of abdominal discomfort and examination revealed suprapubic tenderness with dullness suggesting incomplete emptying of her bladder possibly indicating cystitis. Usual presentation for pyelonephritis could be the classic triad of fever, costovertebral angle pain, and nausea and/or vomiting. (Burke et al 2009). Renal colic often presents with nausea and/or vomiting with severe colicky pain in ureteral obstruction from renal stone. The kidneys were examined specifically for costovertebral angle tenderness; this was absent but if present would indicate renal infection. Right upper quadrant pain might indicate pancreatitis or cholecystitis. ( Bickley & Szilagyi 2009). Genitalia examination: The genitalia was observed and examined externally to rule out the presence of discharge which may indicate urethritis and assessment of urinary leakage noted. (Burke et al 2009) Skin examination (5 Algorithm)
13 Physical Assessment (2) As many as 50% of patients with muscle invasive bladder cancer may have occult metastasis that become clinically apparent within five years of initial diagnosis. (Steinberg et al 2010). For this reason examination of the thorax and peripheral vascular system (PVS) was conducted. (5 Algorithm) The thorax was inspected. (5 Algorithm) The Peripheral Vascular System (PVS) Regional lymphadenopathy is a risk as Natasha s initial diagnosis was muscle invasive bladder cancer Grade 2, almost 3 years ago. The horizontal and vertical group were assessed but no palpable lymph nodes were identified. All pulses were brisk (2+). ( Bickley & Szilagyi 2009). (5 Algorithm).
14 Physical Assessment (4) Natasha was asymptomatic with no bone pain normal calcium and alkaline phosphate levels; therefore a bone scan was unnecessary. (Steinberg et al 2010). (14-15 Algorithm) An FBC indicating low or borderline Hb may indicate the presence of anaemia, particularly with Bladder Cancer or Haemorrhagic Cystitis. Natasha s haemoglobin was 12g/dl (Steinberg et al 2010) (7 - Algorithm) FBC and U & E s are mandatory especially in the presence of pyrexia and /or single functioning kidney. (Guidelines for Acute Management of first presentation of Renal/Ureteric lithiasis, 2008). (7 - Algorithm). Further specific investigations are necessary to determine definite diagnosis.

15 Urinalysis
16 Lab Investigation An uncontaminated MSU sample is adequate for use in tests for haematuria. (7 - Algorithm). Transient causes that need to be excluded before establishing the presence of significant haematuria are: UTI, haematuria in association with UTI is not uncommon. UTI is most readily excluded by a negative dipstick result for both leucocytes and nitrites. (8 Algorithm). The presence of haematuria should not be attributed to anti-coagulation or antiplatelet therapy and patients should be evaluated regardless of these medications. BAUS/RA Guidelines (2008). (3 - Algorithm) The presence or absence of clotted blood is not completely helpful in determining the etiology of haemorrhagic cystitis but the presence of long stringy clots suggest upper urinary tract etiology, this can lead to acute retention of urine or near episodes. Basler & Miyamoto (2009). (11 - Algorithm) Proteinuria, elevated U & E s and / or hypertension may indicate renal disease and these patients require a nephrological assessment. (BAUS / RA Guidelines 2008) (6 - Algorithm)

17 CLINITEK Step 1 Completely immerse all reagent areas into fresh, well-mixed, uncentrifuged urine. Dip briefly and remove immediately to avoid dissolving out reagents. Step 2 While removing the strip, run the edge against the rim of the urine container to remove excess urine. Hold the strip in a horizontal position to prevent possible mixing of chemicals from adjacent reagent areas or soiling of hands with urine. Step 3 After the appropriate time, compare test areas closely with the corresponding colour chart on the bottle label or bench reader at the time specified. Hold strip close to colour blocks and match carefully. Always record the results. Step 4 For enhanced convenience and standardisation, use a CLINITEK analyser to read the reagent strip and print the results


18 Urothialisis (1)
19 Urothialisis (2) Urinary stone formation is a common disease with an increasing incidence and prevalence worldwide that appears even more pronounced in industrialised countries Most stones are formed in older patients. However, clinical observations have indicated not only a changing frequency and composition of urinary calculi but also a shift in gender and age related incidences. Rare in children. As in adults, factors implicated in the metabolic syndrome complex such as Obesity Impact of climate change Changing lifestyle Dietary choices are the more probable cause of the increasing incidence and prevalence of urothialsis. Diabetes can also be an independent risk factor for the development of kidney stones. Types of Urothialisis: Calcium containing calculi Calcium Oxalate Calcium Phosphate Uric Acid calculi Cystine Calculi
20 Urothialisis (3) Diagnostic Modalities Thin slice CT stone protocol preferably within 24 hours if acute presentation to confirm diagnosis or for planning of treatment if a stone is confirmed on KUB x-ray. KUB allows 60% visibility compared with > 95% stone identification on CT. (BAUS Section of Endourology, 2008). Cystoscopy to visualise the bladder Retrograde studies may be an additional study to visualise both ureter s to determine the positioning of the stone and feasibility of removing the stone. Blood Analysis, Serum Creatinine and Urea (Algorithm 13) Sequential course of disease condition Urolithiasis (UL) is one of the most common diseases, with approximately 750,000 cases per year in Germany. Strohmaier (2000). Although most patients have only one stone episode, 25 % of patients experience recurrent stone formation. Hesse et al (2003). UL therefore has a significant impact on QoL and socioeconomic factors. Loton et al (2004).

21
22 Bladder Cancer Bladder cancer is the 8 th most common malignancy in Ireland 3.5% of all malignant neoplasia 4.7% in males and 2% in females 12% of cancers are diagnosed in females between years compared to 13% in the same age range in men. Ferlay et al (2008). (10 Algorithm). Each year, approximately 331 men and 132 women are diagnosed with a bladder tumour. Incidence rates fell between 1994 and 2003 by 1.3% and 2.4% per annum in women and men respectively. Disease of older people 58% of women and 57% of men are aged over 70 at diagnosis, while only around 6-8% of cases present in those aged under 50. Bladder cancer incidence in men in Ireland is among the lowest in western Europe, while that in women is in the mid-range. However, international comparisons of bladder cancer rates are made difficult by inconsistencies in the coding and classification of these cancers. Underlying Pathological Process Almost all bladder cancers are epithelial in origin. The histological appearance of superficial bladder cancer can either represent papillary cells which include features of dysplasia or carcinoma in situ which includes features of inflammation where neutrophils are present in the epithelium and congestion causes dilatation and engorgement of the blood vessels and the epithelium becomes displaced. ( Lakhani, Dilly, Finlayson 2009).

 An MRI scan of the pelvis or CT of the Thorax Abdomen Pelvis (CTTAP) can be used to determine the presence of lymphadenopathy or extravesical")
23 Investigations for Bladder Cancer (1) Cystoscopy Flexible / Rigid - obtain biopsy samples of suspicious lesions. Attempts to include the bladder muscle in the biopsy specimen is important, this allows the pathologist to determine whether the tumour is muscle invasive. An attempt to re- resect the primary tumour should be completed known as TURBT. Steinberg et al (2010). (14 Algorithm) An MRI scan of the pelvis or CT of the Thorax Abdomen Pelvis (CTTAP) can be used to determine the presence of lymphadenopathy or extravesical disease. MRI is superior to CT in the local staging of bladder cancer. Barentz &Witjes (1998). (14 Algorithm).

24
25 Investigations for Bladder Cancer (2) Imaging of the upper urinary tract: Traditionally this was always done by means of an intravenous urogram (IVU) but more commonly done these days by contrast CT An ultrasound scan combined with an ordinary abdominal x-ray is a viable alternative to IVU or CT. The advantages of ultrasound are that it does not involve any radiation or contrast medium and that it is non-invasive. Ultrasound is also more sensitive than IVU in the detection of small tumours of the renal parenchyma. Ultrasound is less sensitive than IVU in the detection of small tumours of the drainage system of the kidney, however, the accuracy of ultrasound is dependent on the skill of the person performing the procedure. Ultrasound and IVU should be seen as complementary rather than mutually exclusive. In some patients it may be necessary to perform both tests in order to make an accurate diagnosis. If ultrasound or IVU suggests a mass in the kidney, then a CT scan is usually used as a first line investigation in haematuria. An ultrasound scan or intravenous urogram cannot rule out the presence of a bladder tumour. All patients with haematuria should undergo cystoscopy. ( Algorithm 14).

26
27 Types of Bladder Cancer Types of Tumour Because of the complex nature of development of the bladder a variety of tumours occur. Transitional Cell Carcinoma (TCC) 85% Squamous Cell Carcinoma (SCC) 5% Adenocarcinoma 2% Rhabdomyosarcoma and others 1% Causes of Bladder Cancer: There is no single cause but there are several risk factors: Smoking (bea nahthylene) Exposure to certain chemicals i.e. aniline. Exposure to petroleum products e.g. car exhaust, gas cutting equipment. Schistosomiasis (Biharzia) Analgesic abuse (Phenacetin) Chronic infection. (Algorithm 18)
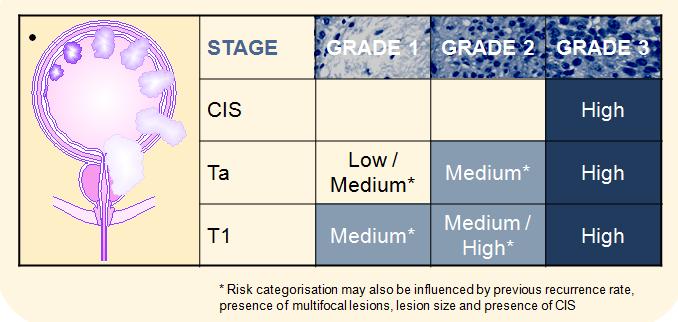
28 Bladder Cancer Sequential course of disease condition More than 70% of all newly diagnosed bladder cancers are non-muscle invasive 50-70% are Ta 20-30% are T1 10% are CIS. Approximately 5% of patients present with metastatic disease, which commonly involves the lymph nodes, lung, liver and bone. Approximately 25% of affected patients have muscle invasive disease at diagnosis. Steinberg et al (2010).

29
30 Haemorrhagic Cystitis Undergone pelvic radiation, chemotherapy or both. Matthews et al (1999). According to Chong et al (2005); Corman et al (2003); Levenback et al (1994) and Matthews et al (1999). 10% of patients who undergo pelvic irradiation 70% of patients exposed to high doses of cyclophosphamide or iphosphamide chemotherapy Matthews et al (1999). Upon examination, the patient often demonstrates suprapubic fullness and discomfort or pain to palpation, as well as costovertebral angle tenderness if the bladder obstruction is chronic. Underlying Pathological Process Characterised by inflammation of the bladder associated with haematuria. The symptoms are caused by a microscopic progressive obliterative endarteritis that leads to mucosal ischemia. The ischemic bladder mucosa then ulcerates and bleeding ensues. Neovascular ingrowth to the damaged area, then occurs causing the characteristic vascular blush on cystoscopic evaluation. The new muscles are more fragile and may leak with bladder distension, minor trauma or any mucosal irritation. Submucosal haemorrhage and overt haematuria may then begin precipitously. The histological appearance of haemorrhagic cystitis is more vascular with mucosal ulceration and haemorrhage, inflammation is present and lymphocytes are in abundance. ( Lakhani, Dilly, Finlayson 2009).
31 Diagnostic Modalities Assessed in the same way as for bladder cancer. In Natasha s case a renal ultrasound was initiated to identify any upper tract lesions. McCarville et al (2000) and Worawattanakul et al (1997). (15 Algorithm) Often, cystoscopic clot evaluation is necessary to allow inspection of the urothelium. Even in situations in which clots are initially removed with continuous bladder irrigation, an endoscopic inspection is essential in planning treatment and in preventing future episodes. Chronic inflammation is the most common finding on a bladder biopsy specimen. Basler and Miyamoto (2009). Surgical intervention other than Cystoscopy with cauterization is reserved for cases in which medical management fails. In extreme cases, when all other treatment options have failed, selective or superselective hypogastric branch artery embolization can be considered.

32
33 Urinary Tract Infection (1) UTI s may be referred to as cystitis or pyelonephritis Uropathogens are specific bacteria that have been clinically associated with invasion of the urinary tract. Complicated UTI s may be subdivided into four categories; Structural abnormalities, Metabolic or hormonal abnormalities, Impaired host responses and Unusual pathogens for example yeast. (12 Algorithm)
34 Urinary Tract Infections (2) Diagnostic Modalities Further tests such as Glomerular Filtration Rate (GFR), Protien Creatinine Ratio (PCR) or Albumin Creatinine Ratio (ACR) should be carried out if a urological cause has been excluded and a nephrology referral should be considered. Criteria for referral to Nephrology (21- Algorithm) The IVU is the traditional standard for upper tract urothelium imaging; however it is poor for evaluating the renal parenchyma. (Steinberg et al 2010). (16 Algorithm).
35 Urinary Tract Infections-some facts (3) Factors unfavourable to bacterial growth include a low Ph (5.5 or less, a high concentration of Urea and the presence of organic acids derived from a diet that includes fruits and protien. Sexual intercourse contributes to increased risk, as does use of a diaphragm and /or spermicide. The high urine glucose content in patients with diabetes mellitus. Rates of infection are high in postmenopausal women loss of estrogen. The prognosis for most women with cystitis and pyelonephritis is good; about 25% of women with cystitis will experience a recurrence. TB of the Kidney results from hematogenous spread but is relatively rare in developing countries. TB of the kidney does not manifest until 5-15 years after the primary infection. UTI s have been well studied in Sweden and other parts of Europe. As 1 in 5 adult women experience UTI at some point, it is an exceedingly common, clinically apparent, worldwide patient problem.
36 Criteria for Referral to Nephrology 24 hour urine collections for protein are rarely required. An approximation to the 24hour urine protein or albumen secretion is obtained by multiplying the ratio (in mg/mmol) x10. The need for a nephrology referral in this situation depends on factors other than simply the presence of haematuria. Nephrology referral is recommended if there is concurrent: Evidence of declining GFR by > 10ml/min at any stage within the previous 5 years or by > 5ml/min within the last one year; Stage four or five chronic kidney disease, that is a GFR of < 30ml/min; Significant protienuria ACR less than or equal to 30 mg/mmol or PCR of greater than or equal to 50 mg/mmol. Isolated haematuria, that is in the absence of significant protienuria with hypertension in those aged less than 40. Visible haematuria coinciding with intercurrent, usually upper respiratory tract infection. BAUS/RA Guidelines (2008)
37 Conclusion Diagnosis was confirmed as recurrent Ta G1 TCC which requires regular Cystoscopy, possible resection and serial radiological review. External beam radiotherapy has been shown to be inferior to radical Cystectomy for the treatment of bladder cancer. The overall 5 year survival after treatment with external beam radiotherapy is 20-40% compared to 90% 5-year survival after Cystectomy for organ confined disease. In Natasha s case she made an informed decision regarding definitive treatment bladder cancer and choose external beam radiotherapy, it may be that she will require a salvage Cystectomy in her future management. (Steinberg et al 2010). Devising this algorithm has lead to a logical approach to the diagnosis of frequent patient presentations encountered in my area of clinical practice. It has further assisted me to develop a valid approach in differential diagnosis for macroscopic haematuria by indicating in a structured manner, recurrent encountered decisions in the diagnostic reasoning pathway


38


39
H(a)ematuria. FX Keeley Consultant Urologist Bristol Urological Institute
ematuria. FX Keeley Consultant Urologist Bristol Urological Institute") H(a)ematuria FX Keeley Consultant Urologist Bristol Urological Institute From Philadelphia to Bristol, England Southmead Hospital, 1916 Southmead Hospital, 2013 Southmead Hospital, 2014 H(a)ematuria Blood
H(a)ematuria FX Keeley Consultant Urologist Bristol Urological Institute From Philadelphia to Bristol, England Southmead Hospital, 1916 Southmead Hospital, 2013 Southmead Hospital, 2014 H(a)ematuria Blood
MODULE 5: HEMATURIA LEARNING OBJECTIVES DEFINITION. KEY WORDS: Hematuria, Cystoscopy, Urine Cytology, UTI, bladder cancer
 MODULE 5: HEMATURIA KEY WORDS: Hematuria, Cystoscopy, Urine Cytology, UTI, bladder cancer LEARNING OBJECTIVES At the end of this clerkship, the learner will be able to: 1. Define microscopic hematuria.
MODULE 5: HEMATURIA KEY WORDS: Hematuria, Cystoscopy, Urine Cytology, UTI, bladder cancer LEARNING OBJECTIVES At the end of this clerkship, the learner will be able to: 1. Define microscopic hematuria.
Lec-8 جراحة بولية د.نعمان
 4th stage Lec-8 جراحة بولية د.نعمان 11/10/2015 بسم هللا الرحمن الرحيم Ureteric, Vesical, & urethral stones Ureteric Calculus Epidemiology like renal stones Etiology like renal stones Risk factors like
4th stage Lec-8 جراحة بولية د.نعمان 11/10/2015 بسم هللا الرحمن الرحيم Ureteric, Vesical, & urethral stones Ureteric Calculus Epidemiology like renal stones Etiology like renal stones Risk factors like
HMM 4401 Genito-urinary tract diseases
 HMM 4401 Genito-urinary tract diseases Urine production Core elements: Glomerulus, proximal and distal convoluted tube, loop of Henle, collecting tubules, ureters, bladder, sphincter, uretra, and out
HMM 4401 Genito-urinary tract diseases Urine production Core elements: Glomerulus, proximal and distal convoluted tube, loop of Henle, collecting tubules, ureters, bladder, sphincter, uretra, and out
Haematuria and Modern Bladder Cancer Treatment
 Haematuria and Modern Bladder Cancer Treatment Mr Nikhil Vasdev MBBS MRCS MCh(Urol) FRCS(Urol) RCSEng/BAUS Robotic Fellowship Accredited and Trained Consultant Urological and Robotic Surgeon Hertfordshire
Haematuria and Modern Bladder Cancer Treatment Mr Nikhil Vasdev MBBS MRCS MCh(Urol) FRCS(Urol) RCSEng/BAUS Robotic Fellowship Accredited and Trained Consultant Urological and Robotic Surgeon Hertfordshire
Bladder Cancer in Primary Care. Dr Penny Kehagioglou Consultant Clinical Oncologist
 Bladder Cancer in Primary Care Dr Penny Kehagioglou Consultant Clinical Oncologist Objectives Patient presentation in primary care Investigating bladder cancer Management of bladder cancer Differential
Bladder Cancer in Primary Care Dr Penny Kehagioglou Consultant Clinical Oncologist Objectives Patient presentation in primary care Investigating bladder cancer Management of bladder cancer Differential
Lower Urinary Tract Infection (UTI) in Males
 in Males") Lower Urinary Tract Infection (UTI) in Males Clinical presentation For patients in care homes see UTI in adults where IV Antibiotics in the community may be appropriate (under development) History and
Lower Urinary Tract Infection (UTI) in Males Clinical presentation For patients in care homes see UTI in adults where IV Antibiotics in the community may be appropriate (under development) History and
Hey Doc, there s blood in my urine Evaluation of hematuria. Christian S. Kuhr, MD FACS May 4, 2018
 Hey Doc, there s blood in my urine Evaluation of hematuria Christian S. Kuhr, MD FACS May 4, 2018 Objectives Understand the algorithm for hematuria evaluation Know the differential diagnosis for hematuria
Hey Doc, there s blood in my urine Evaluation of hematuria Christian S. Kuhr, MD FACS May 4, 2018 Objectives Understand the algorithm for hematuria evaluation Know the differential diagnosis for hematuria
BLADDER CANCER: PATIENT INFORMATION
 BLADDER CANCER: PATIENT INFORMATION The bladder is the balloon like organ located in the pelvis that stores and empties urine. Urine is produced by the kidneys, is conducted to the bladder by the ureters,
BLADDER CANCER: PATIENT INFORMATION The bladder is the balloon like organ located in the pelvis that stores and empties urine. Urine is produced by the kidneys, is conducted to the bladder by the ureters,
Urological Tumours 1 Kidney tumours 2 Bladder tumours
 Urological Tumours 1 Kidney tumours 2 Bladder tumours Tim Bracey SpR Histopathology Derriford Hospital Kidney tumours What are we going to talk about?! Anatomy of urinary tract! Types of kidney tumours!
Urological Tumours 1 Kidney tumours 2 Bladder tumours Tim Bracey SpR Histopathology Derriford Hospital Kidney tumours What are we going to talk about?! Anatomy of urinary tract! Types of kidney tumours!
Glossary of Terms Primary Urethral Cancer
 Patient Information English Glossary of Terms Primary Urethral Cancer Advanced cancer A tumour that grows into deeper layers of tissue, adjacent organs, or surrounding muscles. Anaesthesia (general, spinal,
Patient Information English Glossary of Terms Primary Urethral Cancer Advanced cancer A tumour that grows into deeper layers of tissue, adjacent organs, or surrounding muscles. Anaesthesia (general, spinal,
MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER
 10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
Alterations of Renal and Urinary Tract Function
 Alterations of Renal and Urinary Tract Function Chapter 29 Urinary Tract Obstruction Urinary tract obstruction is an interference with the flow of urine at any site along the urinary tract The obstruction
Alterations of Renal and Urinary Tract Function Chapter 29 Urinary Tract Obstruction Urinary tract obstruction is an interference with the flow of urine at any site along the urinary tract The obstruction
Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer
 Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Symptoms, Diagnosis and Classification
 Patient Information English 2 Symptoms, Diagnosis and Classification The underlined terms are listed in the glossary. Signs and symptoms Blood in the urine is the most common symptom when a bladder tumour
Patient Information English 2 Symptoms, Diagnosis and Classification The underlined terms are listed in the glossary. Signs and symptoms Blood in the urine is the most common symptom when a bladder tumour
6 UROLOGICAL CANCERS. 6.1 Key Points
 6 UROLOGICAL CANCERS 6.1 Key Points Prostate Cancer Commonest cancer in males in Scotland Approximately 99% of cases occur in men aged > 50 years About 40% of cases present in men aged < 70 years when
6 UROLOGICAL CANCERS 6.1 Key Points Prostate Cancer Commonest cancer in males in Scotland Approximately 99% of cases occur in men aged > 50 years About 40% of cases present in men aged < 70 years when
Renal tumors of adults
 Renal tumors of adults Urinary Tract Tumors 2%-3% of all cancers in adults. The most common malignant tumor of the kidney is renal cell carcinoma. Tumors of the lower urinary tract are twice as common
Renal tumors of adults Urinary Tract Tumors 2%-3% of all cancers in adults. The most common malignant tumor of the kidney is renal cell carcinoma. Tumors of the lower urinary tract are twice as common
Diagnosis and classification
 Patient Information English 2 Diagnosis and classification The underlined terms are listed in the glossary. Signs and symptoms Blood in the urine is the most common symptom when a bladder tumour is present.
Patient Information English 2 Diagnosis and classification The underlined terms are listed in the glossary. Signs and symptoms Blood in the urine is the most common symptom when a bladder tumour is present.
3.1 Investigations for Patients Presenting with Haematuria Table 1
 3.1 Investigations for Patients Presenting with Haematuria Table 1 Patients at risk of bacterial endocarditis should be given antibiotic prophylaxis as per local guidelines. Patients with heart valve replacements
3.1 Investigations for Patients Presenting with Haematuria Table 1 Patients at risk of bacterial endocarditis should be given antibiotic prophylaxis as per local guidelines. Patients with heart valve replacements
GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER
 GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER (Limited text update December 21) M. Babjuk, W. Oosterlinck, R. Sylvester, E. Kaasinen, A. Böhle, J. Palou, M. Rouprêt Eur Urol 211 Apr;59(4):584-94 Introduction
GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER (Limited text update December 21) M. Babjuk, W. Oosterlinck, R. Sylvester, E. Kaasinen, A. Böhle, J. Palou, M. Rouprêt Eur Urol 211 Apr;59(4):584-94 Introduction
Case studies. Stephen Mark Rob Walker
 Case studies Stephen Mark Rob Walker Case 1 31 yr old woman with 3 rd UTI. E coli Frequency and dysuria Asymptomatic after treatment Recurrent UTI Lower tract symptoms Coliforms Asymptomatic after treatment
Case studies Stephen Mark Rob Walker Case 1 31 yr old woman with 3 rd UTI. E coli Frequency and dysuria Asymptomatic after treatment Recurrent UTI Lower tract symptoms Coliforms Asymptomatic after treatment
Dr. Aso Urinary Symptoms
 Haematuria The presence of blood in the urine (haematuria) is always abnormal and may be the only indication of pathology in the urinary tract. False positive stick tests and the discolored urine caused
Haematuria The presence of blood in the urine (haematuria) is always abnormal and may be the only indication of pathology in the urinary tract. False positive stick tests and the discolored urine caused
Vaginal intraepithelial neoplasia
 Vaginal intraepithelial neoplasia The terminology and pathology of VAIN are analogous to those of CIN (VAIN I-III). The main difference is that vaginal epithelium does not normally have crypts, so the
Vaginal intraepithelial neoplasia The terminology and pathology of VAIN are analogous to those of CIN (VAIN I-III). The main difference is that vaginal epithelium does not normally have crypts, so the
Bladder Cancer Guidelines
 Bladder Cancer Guidelines Agreed by Urology CSG: October 2011 Review Date: September 2013 Bladder Cancer 1. Referral Guidelines The following patients should be considered as potentially having bladder
Bladder Cancer Guidelines Agreed by Urology CSG: October 2011 Review Date: September 2013 Bladder Cancer 1. Referral Guidelines The following patients should be considered as potentially having bladder
Definition Prostate cancer
 Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
An Undergraduate Syllabus for Urology. Produced on behalf of the British Association of Urological Surgeons. March 2012
 An Undergraduate Syllabus for Urology Produced on behalf of the British Association of Urological Surgeons March 2012 Authors H Hashim, P Jones, KJ O Flynn, I Pearce, J Royle, M Shaw, AM Sinclair Correspondence
An Undergraduate Syllabus for Urology Produced on behalf of the British Association of Urological Surgeons March 2012 Authors H Hashim, P Jones, KJ O Flynn, I Pearce, J Royle, M Shaw, AM Sinclair Correspondence
Cervical cancer presentation
 Carcinoma of the cervix: Carcinoma of the cervix is the second commonest cancer among women worldwide, with only breast cancer occurring more commonly. Worldwide, cervical cancer accounts for about 500,000
Carcinoma of the cervix: Carcinoma of the cervix is the second commonest cancer among women worldwide, with only breast cancer occurring more commonly. Worldwide, cervical cancer accounts for about 500,000
Information for Patients. Primary urethral cancer. English
 Information for Patients Primary urethral cancer English Table of contents What is primary urethral cancer?... 3 Risk factors... 3 Symptoms... 4 Diagnosis... 4 Clinical examination... 4 Urinary cytology...
Information for Patients Primary urethral cancer English Table of contents What is primary urethral cancer?... 3 Risk factors... 3 Symptoms... 4 Diagnosis... 4 Clinical examination... 4 Urinary cytology...
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER
 MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
Nursing Care for Children with Genitourinary Dysfunction I
 Nursing Care for Children with Genitourinary Dysfunction I 1 Assessment of renal function Clinical manifestations Laboratory tests Urinalysis Urine culture and sensitivity Renal/bladder ultrasound Testicular
Nursing Care for Children with Genitourinary Dysfunction I 1 Assessment of renal function Clinical manifestations Laboratory tests Urinalysis Urine culture and sensitivity Renal/bladder ultrasound Testicular
M E D I C A L T E R M I N O L O G Y
 URINARY SYSTEM M E D I C A L T E R M I N O L O G Y Is the organ system which produces, stores and eliminates waste. Is responsible for waste excretion in the form of urine Fluid Intake Is necessary in
URINARY SYSTEM M E D I C A L T E R M I N O L O G Y Is the organ system which produces, stores and eliminates waste. Is responsible for waste excretion in the form of urine Fluid Intake Is necessary in
AUCKLAND REGIONAL UROLOGY GUIDELINES AND REFERRAL RECOMMENDATIONS
 AUCKLAND REGIONAL UROLOGY GUIDELINES AND REFERRAL RECOMMENDATIONS This document outlines the urological conditions currently funded at Auckland District Health Board (ADHB), Counties Manukau District Health
AUCKLAND REGIONAL UROLOGY GUIDELINES AND REFERRAL RECOMMENDATIONS This document outlines the urological conditions currently funded at Auckland District Health Board (ADHB), Counties Manukau District Health
BLADDER CANCER CONTENT CREATED BY. Learn more at
 BLADDER CANCER CONTENT CREATED BY Learn more at www.health.harvard.edu TALK TO YOUR DOCTOR Table of Contents WHAT IS BLADDER CANCER? 4 TYPES OF BLADDER CANCER 5 GRADING AND STAGING 8 TREATMENT OVERVIEW
BLADDER CANCER CONTENT CREATED BY Learn more at www.health.harvard.edu TALK TO YOUR DOCTOR Table of Contents WHAT IS BLADDER CANCER? 4 TYPES OF BLADDER CANCER 5 GRADING AND STAGING 8 TREATMENT OVERVIEW
Bladder Cancer Early Detection, Diagnosis, and Staging
 Bladder Cancer Early Detection, Diagnosis, and Staging Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms that can be
Bladder Cancer Early Detection, Diagnosis, and Staging Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms that can be
URINARY SYSTEM. Lecturer Dr.Firdous M.Jaafar Department of anatomy/histology section Lecture 3
 URINARY SYSTEM Lecturer Dr.Firdous M.Jaafar Department of anatomy/histology section Lecture 3 Objectives 1- Describe the structure of the urinary bladder, 2- Describe the structure of the ureters, bladder,
URINARY SYSTEM Lecturer Dr.Firdous M.Jaafar Department of anatomy/histology section Lecture 3 Objectives 1- Describe the structure of the urinary bladder, 2- Describe the structure of the ureters, bladder,
Diagnostic approach and microorganism resistance pattern in UTI Yeva Rosana, Anis Karuniawati, Yulia Rosa, Budiman Bela
 Diagnostic approach and microorganism resistance pattern in UTI Yeva Rosana, Anis Karuniawati, Yulia Rosa, Budiman Bela Microbiology Department Medical Faculty, University of Indonesia Urinary Tract Infection
Diagnostic approach and microorganism resistance pattern in UTI Yeva Rosana, Anis Karuniawati, Yulia Rosa, Budiman Bela Microbiology Department Medical Faculty, University of Indonesia Urinary Tract Infection
5/26/16: CT scan of the abdomen showed a multinodular liver disease highly suspicious for metastasis and hydronephrosis of the right kidney.
 Bladder Case Scenario 1 History 5/23/16: A 52-year-old male, smoker was admitted to our hospital with a 3-month history of right pelvic pain, multiple episodes of gross hematuria, dysuria, and extreme
Bladder Case Scenario 1 History 5/23/16: A 52-year-old male, smoker was admitted to our hospital with a 3-month history of right pelvic pain, multiple episodes of gross hematuria, dysuria, and extreme
Bladder Cancer Canada November 21st, Bladder Cancer 2018: A brighter light at the end of the cystoscope
 Bladder Cancer Canada November 21st, 2018 Bladder Cancer 2018: A brighter light at the end of the cystoscope Chris Morash MD FRCSC Associate Professor, University of Ottawa Head, Urological Oncology Bladder
Bladder Cancer Canada November 21st, 2018 Bladder Cancer 2018: A brighter light at the end of the cystoscope Chris Morash MD FRCSC Associate Professor, University of Ottawa Head, Urological Oncology Bladder
Hydronephrosis. What is hydronephrosis?
 What is hydronephrosis? Hydronephrosis Hydronephrosis describes the situation where the urine collecting system of the kidney is dilated. This may be a normal variant or it may be due to an underlying
What is hydronephrosis? Hydronephrosis Hydronephrosis describes the situation where the urine collecting system of the kidney is dilated. This may be a normal variant or it may be due to an underlying
Bladder cancer - suspected
 Background information Information resources for patients and carers Updates to this care map Bladder cancer - clinical presentation History Examination Consider differential diagnoses Clinical indications
Background information Information resources for patients and carers Updates to this care map Bladder cancer - clinical presentation History Examination Consider differential diagnoses Clinical indications
Primary Squamous Cell Carcinoma Of Kidney - A Case Report And Review Of Literature.
 ISPUB.COM The Internet Journal of Nephrology Volume 6 Number 1 Primary Squamous Cell Carcinoma Of Kidney - A Case Report And Review Of Literature. P Kaur, A Chauhan, G Singh, S Kataria, R Kalra Citation
ISPUB.COM The Internet Journal of Nephrology Volume 6 Number 1 Primary Squamous Cell Carcinoma Of Kidney - A Case Report And Review Of Literature. P Kaur, A Chauhan, G Singh, S Kataria, R Kalra Citation
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 1/22/2011 Radiology Quiz of the Week # 4 Page 1 CLINICAL PRESENTATION AND RADIOLOGY QUIZ
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 1/22/2011 Radiology Quiz of the Week # 4 Page 1 CLINICAL PRESENTATION AND RADIOLOGY QUIZ
Update on Haematuria and Bladder Cancer
 Update on Haematuria and Bladder Cancer Hugh Mostafid FRCS(urol) FEBU Consultant Urologist, Royal Surrey County Hospital and Honorary Senior Lecturer, University of Surrey Guildford None Declarations Recent
Update on Haematuria and Bladder Cancer Hugh Mostafid FRCS(urol) FEBU Consultant Urologist, Royal Surrey County Hospital and Honorary Senior Lecturer, University of Surrey Guildford None Declarations Recent
Dr P Sigwadi 30 May 2012
 Dr P Sigwadi 30 May 2012 Introduction Haematuria Positive blood on urine dipstick 5 red blood cells/ microliter of urine Prevalence Gross haematuria ( macroscopic) 0.13 % Microscopic- 1.5% Haematuria +
Dr P Sigwadi 30 May 2012 Introduction Haematuria Positive blood on urine dipstick 5 red blood cells/ microliter of urine Prevalence Gross haematuria ( macroscopic) 0.13 % Microscopic- 1.5% Haematuria +
SHABNAM TEHRANI M.D., MPH ASSISTANT PROFESSOR OF INFECTIOUS DISEASESE &TROPICAL MEDICINE RESEARCH CENTER, SHAHID BEHESHTI UNIVERSITY OF MEDICAL
 URINARY TRACT INFECTION SHABNAM TEHRANI M.D., MPH ASSISTANT PROFESSOR OF INFECTIOUS DISEASESE &TROPICAL MEDICINE RESEARCH CENTER, SHAHID BEHESHTI UNIVERSITY OF MEDICAL SCIENCES Definition inflammatory
URINARY TRACT INFECTION SHABNAM TEHRANI M.D., MPH ASSISTANT PROFESSOR OF INFECTIOUS DISEASESE &TROPICAL MEDICINE RESEARCH CENTER, SHAHID BEHESHTI UNIVERSITY OF MEDICAL SCIENCES Definition inflammatory
Cystitis cystica is a rare chronic reactive inflammatory
 JOURNAL OF ENDOUROLOGY CASE REPORTS Volume 3.1, 2017 Mary Ann Liebert, Inc. Pp. 34 38 DOI: 10.1089/cren.2017.0010 Case Report Cystitis Cystica as a Large Solitary Bladder Cyst Stephanie Potts, MBChB and
JOURNAL OF ENDOUROLOGY CASE REPORTS Volume 3.1, 2017 Mary Ann Liebert, Inc. Pp. 34 38 DOI: 10.1089/cren.2017.0010 Case Report Cystitis Cystica as a Large Solitary Bladder Cyst Stephanie Potts, MBChB and
Urogynaecology. Colm McAlinden
 Urogynaecology Colm McAlinden Definitions Urinary incontinence compliant of any involuntary leakage of urine with many different causes Two main types: Stress Urge Definitions Nocturia: More than a single
Urogynaecology Colm McAlinden Definitions Urinary incontinence compliant of any involuntary leakage of urine with many different causes Two main types: Stress Urge Definitions Nocturia: More than a single
Renal Disease. Please refer to the assignment page Three online modules TBLs
 Renal Disease Please refer to the assignment page Three online modules TBLs 1 Renal Embryology 2 Lab Tests UA CBC Enzymes Creatinine Creatinine clearance Ammonia Abs C Bx 3 BUN Creatinine Creatinine Clearance
Renal Disease Please refer to the assignment page Three online modules TBLs 1 Renal Embryology 2 Lab Tests UA CBC Enzymes Creatinine Creatinine clearance Ammonia Abs C Bx 3 BUN Creatinine Creatinine Clearance
The Royal Marsden. MDT case study. Mr Alan Thompson Consultant Urological Surgeon The Royal Marsden
 MDT case study Mr Alan Thompson Consultant Urological Surgeon The Royal Marsden 2 The Royal Marsden Case history 56 year old lady from Bangladesh with 5 children Rarely seen her GP over the last 10 years
MDT case study Mr Alan Thompson Consultant Urological Surgeon The Royal Marsden 2 The Royal Marsden Case history 56 year old lady from Bangladesh with 5 children Rarely seen her GP over the last 10 years
Upper Tract Tcc. Mohan Arianayagam FRACS (Urology)
") Upper Tract Tcc Mohan Arianayagam FRACS (Urology) Epidemiology Peak incidence 75 to 79 years 2x more common in men 7% of all renal tumours 5% of all urothelial tumours Synchronous bilateral is rare ~ 1.6%
Upper Tract Tcc Mohan Arianayagam FRACS (Urology) Epidemiology Peak incidence 75 to 79 years 2x more common in men 7% of all renal tumours 5% of all urothelial tumours Synchronous bilateral is rare ~ 1.6%
The pathology of bladder cancer
 1 The pathology of bladder cancer Charles Jameson Introduction Carcinoma of the bladder is the seventh most common cancer worldwide [1]. It comprises 3.2% of all cancers, with an estimated 260 000 new
1 The pathology of bladder cancer Charles Jameson Introduction Carcinoma of the bladder is the seventh most common cancer worldwide [1]. It comprises 3.2% of all cancers, with an estimated 260 000 new
Carcinoma of the Urinary Bladder Histopathology
 Carcinoma of the Urinary Bladder Histopathology Reporting Proforma (Radical & Partial Cystectomy, Cystoprostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Carcinoma of the Urinary Bladder Histopathology Reporting Proforma (Radical & Partial Cystectomy, Cystoprostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
REFERRAL GUIDELINES: UROLOGY
 All patients referred to specialist clinics are assigned to a priority category based on their clinical need and related psychosocial factors. The examples given are indicative only and the clinician reviewing
All patients referred to specialist clinics are assigned to a priority category based on their clinical need and related psychosocial factors. The examples given are indicative only and the clinician reviewing
Urology An introduction to cut up DR J R GOEPEL
 Urology An introduction to cut up DR J R GOEPEL Overview Principles Individual organs Small pieces Partial resections Whole organs Data recording and data sets Principles You are working for the patient
Urology An introduction to cut up DR J R GOEPEL Overview Principles Individual organs Small pieces Partial resections Whole organs Data recording and data sets Principles You are working for the patient
Case studies: LUTS. Case 1 history. Case 1 - questions. Case 1 - outcome. Case 2 - history. Case 1 learning point 14/07/2015 DR JON REES
 Case 1 history Case studies: LUTS DR JON REES A 49 year old male comes to see you he has had gradual deterioration of his flow over the last few years- he saw a colleague of yours 6 weeks ago who recorded
Case 1 history Case studies: LUTS DR JON REES A 49 year old male comes to see you he has had gradual deterioration of his flow over the last few years- he saw a colleague of yours 6 weeks ago who recorded
UROLOGY TOPICS FOR SENIOR CLERKSHIP HEMATURIA
 UROLOGY TOPICS FOR SENIOR CLERKSHIP HEMATURIA Blood in urine is an important presenting symptom for many diseases of the urinary tract as well as for systemic disorders. Degree of hematuria has poor correlation
UROLOGY TOPICS FOR SENIOR CLERKSHIP HEMATURIA Blood in urine is an important presenting symptom for many diseases of the urinary tract as well as for systemic disorders. Degree of hematuria has poor correlation
Information for Patients. Bladder Cancer. English
 Information for Patients Bladder Cancer English Table of contents What is the function of the bladder?... 3 What is bladder cancer?... 3 What causes bladder cancer?... 3 Stages of the disease... 3 Risk
Information for Patients Bladder Cancer English Table of contents What is the function of the bladder?... 3 What is bladder cancer?... 3 What causes bladder cancer?... 3 Stages of the disease... 3 Risk
Find Medical Solutions to Your Problems HYDRONEPHROSIS. (Distension of Renal Calyces & Pelvis)
") HYDRONEPHROSIS (Distension of Renal Calyces & Pelvis) Hydronephrosis is the distension of the renal calyces and pelvis due to accumulation of the urine as a result of the obstruction to the outflow of
HYDRONEPHROSIS (Distension of Renal Calyces & Pelvis) Hydronephrosis is the distension of the renal calyces and pelvis due to accumulation of the urine as a result of the obstruction to the outflow of
Mini-Invasive Treatment in Urological Diseases Dott. Alberto Saita Responsabile Endourologia Istituto Clinico Humanitas - Rozzano
 Dipartimento di Urologia Direttore Prof. Giorgio Guazzoni Mini-Invasive Treatment in Urological Diseases Dott. Alberto Saita Responsabile Endourologia Istituto Clinico Humanitas - Rozzano alberto.saita@humanitas.it
Dipartimento di Urologia Direttore Prof. Giorgio Guazzoni Mini-Invasive Treatment in Urological Diseases Dott. Alberto Saita Responsabile Endourologia Istituto Clinico Humanitas - Rozzano alberto.saita@humanitas.it
Staging and Grading Last Updated Friday, 14 November 2008
 Staging and Grading Last Updated Friday, 14 November 2008 There is a staging graph below Blood in the urine is the most common indication that something is wrong. Often one will experience pain or difficulty
Staging and Grading Last Updated Friday, 14 November 2008 There is a staging graph below Blood in the urine is the most common indication that something is wrong. Often one will experience pain or difficulty
EAU GUIDELINES ON NON-MUSCLE INVASIVE (TaT1, CIS) BLADDER CANCER
 BLADDER CANCER") EU GUIDELINES ON NON-MUSLE INVSIVE (TaT1, IS) LDDER NER (Limited text update March 2017) M. abjuk (hair), M. urger (Vice-hair), E. ompérat, P. Gontero,.H. Mostafid, J. Palou,.W.G. van Rhijn, M. Rouprêt,
EU GUIDELINES ON NON-MUSLE INVSIVE (TaT1, IS) LDDER NER (Limited text update March 2017) M. abjuk (hair), M. urger (Vice-hair), E. ompérat, P. Gontero,.H. Mostafid, J. Palou,.W.G. van Rhijn, M. Rouprêt,
Excretory urography (EU) or IVP US CT & radionuclide imaging
 or IVP US CT & radionuclide imaging") Excretory urography (EU) or IVP US CT & radionuclide imaging MRI arteriography studies requiring catherization or direct puncture of collecting system EU & to a lesser extent CT provide both functional
Excretory urography (EU) or IVP US CT & radionuclide imaging MRI arteriography studies requiring catherization or direct puncture of collecting system EU & to a lesser extent CT provide both functional
Urologic investigations
 Urologic investigations د. Laboratory studies EXAMINATION OF URINE Urinalysis: Urinalysis is one of the most important and useful urologic tests available. Reasons for inadequate urinalyses include: (1)
Urologic investigations د. Laboratory studies EXAMINATION OF URINE Urinalysis: Urinalysis is one of the most important and useful urologic tests available. Reasons for inadequate urinalyses include: (1)
Five Views of Transitional Cell Carcinoma: One Man s Journey
 September 2006 Five Views of Transitional Cell Carcinoma: One Man s Journey Amsalu Dabela, Harvard Medical School III Outline Overview: Renal Anatomy Our Patient s Story Diagnostic Imaging Studies Appearance
September 2006 Five Views of Transitional Cell Carcinoma: One Man s Journey Amsalu Dabela, Harvard Medical School III Outline Overview: Renal Anatomy Our Patient s Story Diagnostic Imaging Studies Appearance
CT Urography. Bladder. Stuart G. Silverman, M.D.
 CT Urography Stuart G. Silverman, M.D. Professor of Radiology Harvard Medical School Director, Abdominal Imaging and Intervention Brigham and Women s Hospital Bladder Boston, MA CT Urography Stuart G.
CT Urography Stuart G. Silverman, M.D. Professor of Radiology Harvard Medical School Director, Abdominal Imaging and Intervention Brigham and Women s Hospital Bladder Boston, MA CT Urography Stuart G.
Advanced Pathophysiology Unit 7: Renal-Urologic Page 1 of 6
 Advanced Pathophysiology Unit 7: Renal-Urologic Page 1 of 6 Learning Objectives for this File: 1. Understand how clinical presentation drives the diagnostic workup 2. Recognize how patient education is
Advanced Pathophysiology Unit 7: Renal-Urologic Page 1 of 6 Learning Objectives for this File: 1. Understand how clinical presentation drives the diagnostic workup 2. Recognize how patient education is
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome.
 Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
CYSTIC DISEASES of THE KIDNEY. Dr. Nisreen Abu Shahin
 CYSTIC DISEASES of THE KIDNEY Dr. Nisreen Abu Shahin 1 Types of cysts 1-Simple Cysts 2-Dialysis-associated acquired cysts 3-Autosomal Dominant (Adult) Polycystic Kidney Disease 4-Autosomal Recessive (Childhood)
CYSTIC DISEASES of THE KIDNEY Dr. Nisreen Abu Shahin 1 Types of cysts 1-Simple Cysts 2-Dialysis-associated acquired cysts 3-Autosomal Dominant (Adult) Polycystic Kidney Disease 4-Autosomal Recessive (Childhood)
MEDitorial March Bladder Cancer
 MEDitorial March 2010 Bladder Cancer Last month, my article addressed the issue of blood in the urine ( hematuria ). A concerning cause of hematuria is bladder cancer, a variably malignant tumor starting
MEDitorial March 2010 Bladder Cancer Last month, my article addressed the issue of blood in the urine ( hematuria ). A concerning cause of hematuria is bladder cancer, a variably malignant tumor starting
Bladder Cancer Knowing the Risks and Warning Signs. Part II: Warning Signs
 Bladder Cancer Knowing the Risks and Warning Signs Part II: Warning Signs May 8, 2018 Presented by: is the Director of Urologic Oncology at MedStar Washington Hospital Center and an Assistant Professor
Bladder Cancer Knowing the Risks and Warning Signs Part II: Warning Signs May 8, 2018 Presented by: is the Director of Urologic Oncology at MedStar Washington Hospital Center and an Assistant Professor
Urinary System. Dr. Thorson
 Urinary System Dr. Thorson Lesson Objectives Upon completion of this lesson, students should be able to Define and spell the terms to learn for this chapter. Describe the purpose and function of the urinary
Urinary System Dr. Thorson Lesson Objectives Upon completion of this lesson, students should be able to Define and spell the terms to learn for this chapter. Describe the purpose and function of the urinary
Prostate Case Scenario 1
 Prostate Case Scenario 1 H&P 5/12/16: A 57-year-old Hispanic male presents with frequency of micturition, urinary urgency, and hesitancy associated with a weak stream. Over the past several weeks, he has
Prostate Case Scenario 1 H&P 5/12/16: A 57-year-old Hispanic male presents with frequency of micturition, urinary urgency, and hesitancy associated with a weak stream. Over the past several weeks, he has
UNDERSTANDING BLADDER CANCER
 UNDERSTANDING BLADDER CANCER Learn About Your Treatment Options After Your Diagnosis If your doctor has told you that you have bladder cancer, you likely have many questions and concerns. Learning about
UNDERSTANDING BLADDER CANCER Learn About Your Treatment Options After Your Diagnosis If your doctor has told you that you have bladder cancer, you likely have many questions and concerns. Learning about
A patient with recurrent bladder cancer presents with the following history:
 MP/H Quiz A patient with recurrent bladder cancer presents with the following history: 9/23/06 TURB 1/12/07 TURB 4/1/07 TURB 7/12/07 TURB 11/14/07 Non-invasive papillary transitional cell carcinoma from
MP/H Quiz A patient with recurrent bladder cancer presents with the following history: 9/23/06 TURB 1/12/07 TURB 4/1/07 TURB 7/12/07 TURB 11/14/07 Non-invasive papillary transitional cell carcinoma from
Male genital tract tumors. SiCA. Division of Urology, Department of Surgery, Faculty of Medicine Siriraj Hospital.
 Male genital tract tumors Division of Urology, Department of Surgery, Faculty of Medicine Siriraj Hospital. adenocarcinoma Prostate Cancer most common male cancer in western countries more detected in
Male genital tract tumors Division of Urology, Department of Surgery, Faculty of Medicine Siriraj Hospital. adenocarcinoma Prostate Cancer most common male cancer in western countries more detected in
GUIDELINES ON RENAL CELL CANCER
 20 G. Mickisch (chairman), J. Carballido, S. Hellsten, H. Schulze, H. Mensink Eur Urol 2001;40(3):252-255 Introduction is characterised by a constant rise in incidence over the last 50 years, with a predominance
20 G. Mickisch (chairman), J. Carballido, S. Hellsten, H. Schulze, H. Mensink Eur Urol 2001;40(3):252-255 Introduction is characterised by a constant rise in incidence over the last 50 years, with a predominance
MANAGING BENIGN PROSTATIC HYPERTROPHY IN PRIMARY CARE DR GEORGE G MATHEW CONSULTANT FAMILY PHYSICIAN FELLOW IN SEXUAL & REPRODUCTIVE HEALTH
 MANAGING BENIGN PROSTATIC HYPERTROPHY IN PRIMARY CARE DR GEORGE G MATHEW CONSULTANT FAMILY PHYSICIAN FELLOW IN SEXUAL & REPRODUCTIVE HEALTH INTRODUCTION (1) Part of male sexual reproductive organ Size
MANAGING BENIGN PROSTATIC HYPERTROPHY IN PRIMARY CARE DR GEORGE G MATHEW CONSULTANT FAMILY PHYSICIAN FELLOW IN SEXUAL & REPRODUCTIVE HEALTH INTRODUCTION (1) Part of male sexual reproductive organ Size
Care of bladder cancer patients diagnosed in Northern Ireland 2010 & 2011 (Summary)
") Care of bladder cancer patients diagnosed in 2010 & 2011 (Summary) Bannon, F., Ranaghan, L., & Gavin, A. (2014). Care of bladder cancer patients diagnosed in 2010 & 2011 (Summary). N. Cancer Registry,
Care of bladder cancer patients diagnosed in 2010 & 2011 (Summary) Bannon, F., Ranaghan, L., & Gavin, A. (2014). Care of bladder cancer patients diagnosed in 2010 & 2011 (Summary). N. Cancer Registry,
Cervical Cancer 3/25/2019. Abnormal vaginal bleeding
 Cervical Cancer Abnormal vaginal bleeding Postcoital, intermenstrual or postmenopausal Vaginal discharge Pelvic pain or pressure Asymptomatic In most patients who are not sexually active due to symptoms
Cervical Cancer Abnormal vaginal bleeding Postcoital, intermenstrual or postmenopausal Vaginal discharge Pelvic pain or pressure Asymptomatic In most patients who are not sexually active due to symptoms
PAINFUL URINATION CAUSES & NATURAL REMEDY. Dr. Bestman Anyatonwu
 LIBRACIN NATURAL MEDICINE IND. LTD PAINFUL URINATION CAUSES & NATURAL REMEDY Dr. Bestman Anyatonwu MEANING Painful urination is a broad term that describes discomfort during urination. This pain may originate
LIBRACIN NATURAL MEDICINE IND. LTD PAINFUL URINATION CAUSES & NATURAL REMEDY Dr. Bestman Anyatonwu MEANING Painful urination is a broad term that describes discomfort during urination. This pain may originate
UROLOGIC EMERGENCIES. Dr Alison Rutledge
 UROLOGIC EMERGENCIES Dr Alison Rutledge Plumbing Problems Common problems Acute urinary retention IDC insertion Haematuria Acute scrotal pain Renal colic UTIs Trauma Other bits and bobs Urinary retention
UROLOGIC EMERGENCIES Dr Alison Rutledge Plumbing Problems Common problems Acute urinary retention IDC insertion Haematuria Acute scrotal pain Renal colic UTIs Trauma Other bits and bobs Urinary retention
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Sex: 女 Age: 51 Occupation: 無 Admission date:92/07/22
 Sex: 女 Age: 51 Occupation: 無 Admission date:92/07/22 Chief complaint Unknown fever for one month Hand tremor and left huge renal tumor was noted Present illness Suffered from fever for one month, hand
Sex: 女 Age: 51 Occupation: 無 Admission date:92/07/22 Chief complaint Unknown fever for one month Hand tremor and left huge renal tumor was noted Present illness Suffered from fever for one month, hand
RATIONALE: The organs making up the urinary system consist of the kidneys, bladder, urethra, and ureters.
 Chapter 12 Section Review 12.1 1. A. Kidneys RATIONALE: The renal pelvis receives urine from the kidney, travels through the ureters on the way to the bladder, but urine is formed in the kidney. 2. C.
Chapter 12 Section Review 12.1 1. A. Kidneys RATIONALE: The renal pelvis receives urine from the kidney, travels through the ureters on the way to the bladder, but urine is formed in the kidney. 2. C.
Cystoscopy and urethroscopy
 Page 1 of 5 Cystoscopy and urethroscopy Introduction This leaflet is provided to give you information about undergoing cystoscopy and/or urethroscopy. What is a cystoscopy? A cystoscopy is a procedure
Page 1 of 5 Cystoscopy and urethroscopy Introduction This leaflet is provided to give you information about undergoing cystoscopy and/or urethroscopy. What is a cystoscopy? A cystoscopy is a procedure
PROFESSIONAL SKILLS 1 3RD YEAR SEMESTER 6 RADIOGRAPHY. THE URINARY SYSTEM Uz. Fatema shmus aldeen Tel
 PROFESSIONAL SKILLS 1 3RD YEAR SEMESTER 6 RADIOGRAPHY THE URINARY SYSTEM Uz. Fatema shmus aldeen Tel. 0925111552 Professional skills-2 THE URINARY SYSTEM The urinary system (review anatomy and physiology)
PROFESSIONAL SKILLS 1 3RD YEAR SEMESTER 6 RADIOGRAPHY THE URINARY SYSTEM Uz. Fatema shmus aldeen Tel. 0925111552 Professional skills-2 THE URINARY SYSTEM The urinary system (review anatomy and physiology)
A&P of the Urinary System
 A&P of the Urinary System Week 44 1 Objectives Identify the organs of the urinary system, from a Identify the parts of the nephron (the functional unit List the characteristics of a normal urine specimen.
A&P of the Urinary System Week 44 1 Objectives Identify the organs of the urinary system, from a Identify the parts of the nephron (the functional unit List the characteristics of a normal urine specimen.
HEALTHYSTART TRAINING MANUAL. Living well with Kidney Disease
 HEALTHYSTART TRAINING MANUAL Living well with Kidney Disease KIDNEY DISEASE CAN AFFECT ANYONE! 1 HEALTHYSTART PROGRAMME HEALTHYSTART is a lifestyle management programme to assist you to remain healthy
HEALTHYSTART TRAINING MANUAL Living well with Kidney Disease KIDNEY DISEASE CAN AFFECT ANYONE! 1 HEALTHYSTART PROGRAMME HEALTHYSTART is a lifestyle management programme to assist you to remain healthy
All about the Prostate
 MEN S HEALTH Dr Nick Pendleton January 16 th 2018 All about the Prostate 1 What does it do? Functions of the Prostate 1. Secretes Prostatic Fluid slightly alkaline fluid, 30% of volume of seminal fluid,
MEN S HEALTH Dr Nick Pendleton January 16 th 2018 All about the Prostate 1 What does it do? Functions of the Prostate 1. Secretes Prostatic Fluid slightly alkaline fluid, 30% of volume of seminal fluid,
Nephrology - the study of the kidney. Urology - branch of medicine dealing with the male and female urinary systems and the male reproductive system
 Urinary System Nephrology - the study of the kidney Urology - branch of medicine dealing with the male and female urinary systems and the male reproductive system Functions of the Urinary System 1. Regulation
Urinary System Nephrology - the study of the kidney Urology - branch of medicine dealing with the male and female urinary systems and the male reproductive system Functions of the Urinary System 1. Regulation
BACTERIAL CULTURE, URINE
 789.00-789.09 ABDOMINAL PAIN 789.60-789.69 ABDOMINAL TENDERNESS 276.2 ACIDOSIS 570 ACUTE AND SUBACUTE NECROSIS OF LIVER 580.0-580.9 ACUTE GLOMERULONEPHRITIS 780.97 ALTERED MENTAL STATUS V44.50-V44.6 ARTIFICIAL
789.00-789.09 ABDOMINAL PAIN 789.60-789.69 ABDOMINAL TENDERNESS 276.2 ACIDOSIS 570 ACUTE AND SUBACUTE NECROSIS OF LIVER 580.0-580.9 ACUTE GLOMERULONEPHRITIS 780.97 ALTERED MENTAL STATUS V44.50-V44.6 ARTIFICIAL
Prostate Gland Disorders
 Prostate Gland Disorders THE PROSTATE GLAND A male s prostate gland is located in the floor of the pelvis surrounding the urethra between the bladder and the penis. The prostate is positioned immediately
Prostate Gland Disorders THE PROSTATE GLAND A male s prostate gland is located in the floor of the pelvis surrounding the urethra between the bladder and the penis. The prostate is positioned immediately
Hong Kong College of Surgical Nursing
 Hong Kong College of Surgical Nursing Higher Surgical Nursing Training: Part B Specialty - Urological Nursing Curriculum TABLE OF CONTENTS No. Contents Page. Introduction. Aims. Learning Objectives 4.
Hong Kong College of Surgical Nursing Higher Surgical Nursing Training: Part B Specialty - Urological Nursing Curriculum TABLE OF CONTENTS No. Contents Page. Introduction. Aims. Learning Objectives 4.
CHEMO-RADIOTHERAPY FOR BLADDER CANCER. Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre
 CHEMO-RADIOTHERAPY FOR BLADDER CANCER Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre AIMS Muscle invasive disease Current Gold-Standard Rationale behind Chemo-Radiotherapy
CHEMO-RADIOTHERAPY FOR BLADDER CANCER Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre AIMS Muscle invasive disease Current Gold-Standard Rationale behind Chemo-Radiotherapy
Children s Services Medical Guideline
 See also: NICE Guidelines These local guidelines are in conjunction with NICE UTI Algorithms Renal scarring and subsequent nephropathy are important causes of later hypertension and renal failure. Early
See also: NICE Guidelines These local guidelines are in conjunction with NICE UTI Algorithms Renal scarring and subsequent nephropathy are important causes of later hypertension and renal failure. Early
Bladder Case # 1. Principal Diagnosis: Bladder Tumor, Suspect Transitional Cell Carcinoma. Secondary Diagnoses: 1. Hypertension. 2. Hyperlipidemia.
 DISCHARGE SUMMARY Bladder Case # 1 Date: 04/22/2010 Principal Diagnosis: Bladder Tumor, Suspect Transitional Cell Carcinoma. Secondary Diagnoses: 1. Hypertension. 2. Hyperlipidemia. Hospital Course: Mr.
DISCHARGE SUMMARY Bladder Case # 1 Date: 04/22/2010 Principal Diagnosis: Bladder Tumor, Suspect Transitional Cell Carcinoma. Secondary Diagnoses: 1. Hypertension. 2. Hyperlipidemia. Hospital Course: Mr.
UTI IN ELDERLY. Zeinab Naderpour
 UTI IN ELDERLY Zeinab Naderpour Urinary tract infection (UTI) is the most frequent bacterial infection in elderly populations. While urinary infection in the elderly person is usually asymptomatic, symptomatic
UTI IN ELDERLY Zeinab Naderpour Urinary tract infection (UTI) is the most frequent bacterial infection in elderly populations. While urinary infection in the elderly person is usually asymptomatic, symptomatic
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds
 Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
URINARY TRACT INFECTIONS
 URINARY TRACT INFECTIONS Learning Objectives Identify signs and symptoms that may indicate presence of UTI (both complicated and uncomplicated) List common causative organisms and risk factors for UTIs
URINARY TRACT INFECTIONS Learning Objectives Identify signs and symptoms that may indicate presence of UTI (both complicated and uncomplicated) List common causative organisms and risk factors for UTIs