Obliterative Procedures LeFort Colpocleisis Colpectomy (Vaginectomy) April 4, 2018
|
|
|
- Byron Goodman
- 6 years ago
- Views:
Transcription
1 Obliterative Procedures LeFort Colpocleisis Colpectomy (Vaginectomy) April 4, 2018
 Vaginectomy (colpectomy)- partial")
2 Obliterative Procedures for uterovaginal prolapse Total colpocleisis Partial colpocleisis (LeFort) Vaginectomy (colpectomy)- partial /total
3 Obliterative Procedures colpocleisis 1867-Neugebauer (Germany): denudation 3x6cm anterior and posterior near introitus and suturing them together. Published LeFort (France) :narrow area of denudation followed by colpoperineoplasty 8 days later 1880-Berlin (USA) : failures - addition of perineorrhaphy Wyatt: wider dissection 1900s- sparing distal vagina/urethra to lessen urinary incontinence
4 Obliterative Procedures Indications / Candidates Advanced prolapse No desire to preserve vaginal sexual function Failed / unsatisfactory pessary trial Recurrent prolapse / Failed prior procedures Elderly (mean age 79 +/- 10) Co-morbidities Avoidance of major surgery Avoidance of the peritoneal cavity Avoidance of general anesthesia
5 Obliterative Procedures Contraindications Vaginal preservation desired for any reason
6 Obliterative Procedures for Prolapse Benefits Minimally invasive High satisfaction rates Regional anesthesia (spinal, epidural) Low complications Shorter operation time Less blood loss Low regret, improved QOL, substantial goal attainment (Hullfish, et al 2007)
7 Patient Satisfaction Low Regret High Satisfaction Body Image improved Am J Obstet Gynecol Nov;209(5):473.e1-7. doi: /j.ajog Epub 2013 May 9. Body image, regret, and satisfaction following colpocleisis. Crisp CC 1, Book NM, Smith AL, Cunkelman JA, Mishan V, Treszezamsky AD, Adams SR, Apostolis C, Lowenstein L, Pauls RN; Fellows' Pelvic Research Network, Society of Gynecologic Surgeons. Author information 1Division of Urogynecology and Pelvic Reconstructive Surgery, Department of Obstetrics and Gynecology, Good Samaritan Hospital, Cincinnati, OH. Electronic address: Catrina_Crisp@trihealth.com. Abstract OBJECTIVE: Colpocleisis is a definitive surgical treatment for prolapse resulting in vaginal obliteration. We sought to evaluate body image, regret, satisfaction, and pelvic floor symptoms following this procedure. STUDY DESIGN: This was a prospective multicenter study through the Fellows' Pelvic Research Network. All women electing colpocleisis for management of pelvic organ prolapse were screened for enrollment. The Pelvic Floor Impact Questionnaire, Pelvic Floor Distress Inventory, and the modified Body Image Scale (BIS) were completed preoperatively and 6 weeks following surgery. Additionally, the Decision Regret Scale and the Satisfaction with Decision Scale were administered at the 6-week postoperative visit. A sample size of 88 subjects was calculated to evaluate change in the BIS score. RESULTS: In all, 87 patients were analyzed. Mean age was 79 years (SD 5.8) with a mean body mass index of 27 (SD 5.3). The majority (89.3%) was Caucasian. Six weeks after surgery, significant improvements were noted in all parameters. Mean BIS scores decreased from 4.8 to 1.2 (P <.001), signifying improved body image. Indeed, the overall number of subjects with BIS scores in the normal range doubled after surgery. Pelvic Floor Distress Inventory and Pelvic Floor Impact Questionnaire scores decreased significantly (P <.001 and P <.001), suggesting a positive impact on bladder, bowel, and prolapse symptoms. Finally, low levels of regret (mean score 1.35) and concurrent high satisfaction (mean score 4.73) were documented. CONCLUSION: Colpocleisis improves body image and pelvic floor symptoms while giving patients a definitive surgical option that results in low regret and high satisfaction.
8 Bowel symptoms obstructive and incontinence symptoms improved Int Urogynecol J Apr;21(4): doi: /s z. Epub 2009 Dec 4. Effects of colpocleisis on bowel symptoms among women with severe pelvic organ prolapse. Gutman RE 1, Bradley CS, Ye W, Markland AD, Whitehead WE, Fitzgerald MP; Pelvic Floor Disorders Network. Author information 1Department of Obstetrics and Gynecology, Washington Hospital Center, Washington, DC, USA. Abstract INTRODUCTION AND HYPOTHESIS: Our objective was to evaluate bowel symptoms after colpocleisis. METHODS: This was a planned ancillary analysis of a prospective, colpocleisis cohort study of 152 women. Those with baseline and 1-year questionnaires (Colorectal-Anal Distress Inventory (CRADI) and the Colorectal-Anal Impact Questionnaire (CRAIQ)) were included. "Bothersome" CRADI symptoms (score>2("moderately", "quite a bit")) were identified. CRADI and CRAIQ scores were compared, and postoperative symptom resolution and new symptom development were measured. RESULTS: Of 121 (80%) subjects with complete data, mean age was /- 5.4 years and all had stage 3-4 prolapse. Procedures performed: partial colpocleisis (61%), total colpocleisis (39%), levator myorrhaphy (71%), and perineorrhaphy (97%). Bothersome bowel symptom(s) were present in 77% at baseline (obstructive (17-26%), incontinence (12-35%) and pain/irritation (3-34%)). All bothersome obstructive and most bothersome incontinence symptoms were less prevalent 1 year after surgery. CRADI and CRAIQ scores significantly improved. The majority of bothersome symptoms resolved (50-100%) with low rates of de novo symptoms (0-14%). CONCLUSIONS: Most bothersome bowel symptoms resolve after colpocleisis, especially obstructive and incontinence symptoms, with low rates of de novo symptoms.
9 Preoperative Considerations Elderly-Functional status General physical condition Cognitive status (Capacity for independent decision making) Social support Living situation Post op rehab, SNF Advance Directive, Living Will, Healthcare POA Obstructive uropathy? For advanced prolapse Co-morbities (74% have at least one) Cardiac Pulmonary
10 Postoperative Considerations Geriatrics Decreased renal function (fluids, NSAIDs) GI reflux (H2 blockers, PPIs) Decreased muscle mass /increased fat = increased Vd Decreased max HR (beta blockers) Post op risks increased Falls Delerium (17% gynonc pts---snf) SSI Electrolyte imbalance
11 Should hysterectomy be done at the time of colpocleisis? Current practice patterns vary in US. Routine hyst is uncommon. ( Jones et al 2017) Benefit - Prevention High risk for cancer cervix / endometrium Prevention pyometrium (rare) Hysterovaginectomy in high risk population is not associated with clinically significant difference in morbidity over vaginectomy alone 13pts vs 41 (Hoffman, et al 2003) Risk Increased operation time Increased morbidity (blood loss, hospital stay) (vonpechmann, et al 2003)
12 LeFort colpocleisis Should pre-op endometrial evaluation be performed? (asymptomatic) No consensus Based on risk factors, is often recommended (expert opinion) Cervical stenosis and elongation- (D+C in OR) Jones et al 2017 practice pattern study 68% routine eval (81% utilized TVUS endometrium)
13 Risk of occult endometrial CA is low in asymptomatic women with prolapse 2/63 (3.17%) Female Pelvic Med Reconstr Surg Mar-Apr;20(2): doi: /SPV.0b013e31829ff5b8. Unanticipated uterine pathologic finding after morcellation during robotic-assisted supracervical hysterectomy and cervicosacropexy for uterine prolapse. Hill AJ 1, Carroll AW, Matthews CA. Author information 1From the *Department of Obstetrics and Gynecology, Virginia Commonwealth University Health System, and Division of Urogynecology and Reconstructive Pelvic Surgery, University of North Carolina, Chapel Hill, NC. Abstract BACKGROUND: Identification of occult malignancy after intra-abdominal morcellation at the time of robotic-assisted supracervical hysterectomy and cervicosacropexy for uterine prolapse may lead to challenging postoperative management and leads one to question the need for preoperative evaluation. CASES: We present 2 cases of occult endometrial carcinoma after robotic-assisted supracervical hysterectomy and cervicosacropexy with intra-abdominal uterine morcellation from January 2008 to December A total of 63 patients underwent the stated surgical procedure with 2 patients (3.17%) found to have abnormal uterine pathologic finding with International Federation of Gynecology and Obstetrics grade 1 endometrial adenocarcinoma. Both cases occurred in asymptomatic postmenopausal patients without risk factors for endometrial cancer, including no history of postmenopausal bleeding or hormone replacement therapy. Owing to intraoperative uterine morcellation and cervical retention, appropriate postoperative management was controversial and problematic. Each patient was referred to gynecologic oncology. To date, both patients are without evidence of residual disease. CONCLUSION: Owing to the risk of occult uterine pathologic finding and complicated postoperative management, preoperative endometrial assessment should be considered on all postmenopausal patients undergoing intra-abdominal uterine morcellation, regardless of risk factors.
14 Should concomitant prophylactic urethral sling be placed? Individualize Dementia, UUI, elevated PVRV, +ST??? Similar rates of complications in those with and without MUS. (Catanzarite, et al 2014) Jones et al practice pattern study - MUS is common (54% required +ST, nl PVRV) Urinary retention uncommon after colpocleisis with concomitant MUS (Abbasy, et al 2009). regardless of preop PVRV, voiding improved
15 Complications UTI most common 6-35% Mortality -0.4 (Catanzarite, et al 2015)- 1.3% (Zebede, et al 2013) Return to OR with in 30 days 2.1% Complications not increased with concomitant sling, anesthesia type, or OR time Blood loss- increased with concomitant hyst Hematocolpos- Bakri balloon, Pyometria- H/S via tunnel drainage, gent irrigation
16 Adverse Events Low Mueller et al multicenter 4776 cases Age 43% >80yo 52% 60-79yo High volume centers had lower ICU admissions, lower complication rate, and shorter LOS Younger women had high ICU admissions, higher complications, and higher LOS Surgeon type- Complications higher- urol and obgyn vs urogyn ICU admissions higher- urol vs obgyn and urogyn LOS longer- urol Female Pelvic Med Reconstr Surg Jan-Feb;21(1):30-3. Colpocleisis: a safe, minimally invasive option for pelvic organ prolapse. Mueller MG 1, Ellimootil C, Abernethy MG, Mueller ER, Hohmann S, Kenton K.
17 LeFort Colpocleisis Procedure Everyone is a little different

18 Exam under anesthesia What do I have to work with? What is behind the prolapsing vagina? Where will I encounter my blood supply, bladder, and ureters? What is the status of the urethra? What is different from the office exam?

19

20

21

22

23

24

25

26

27
28

29

30

31

32

33

34

35

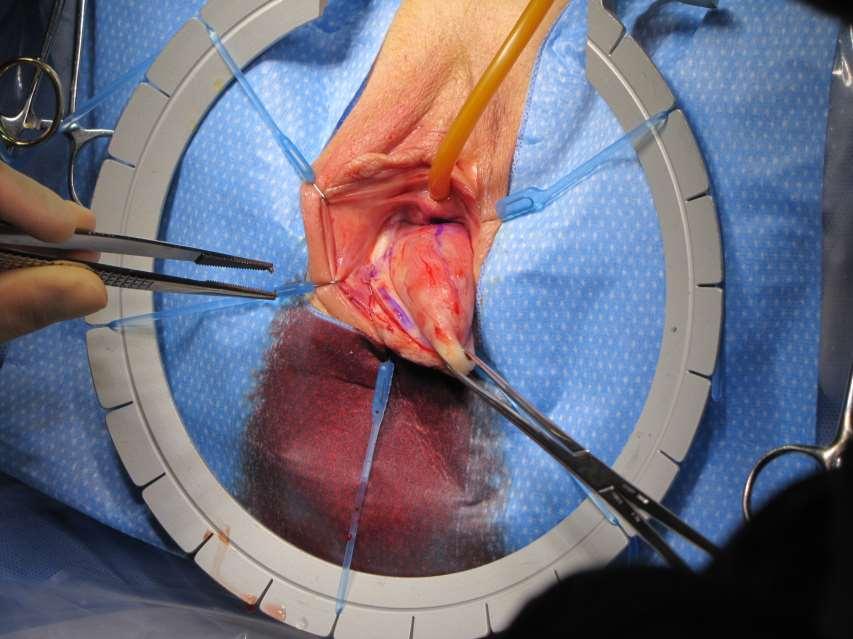
36

37

38

39

40

41

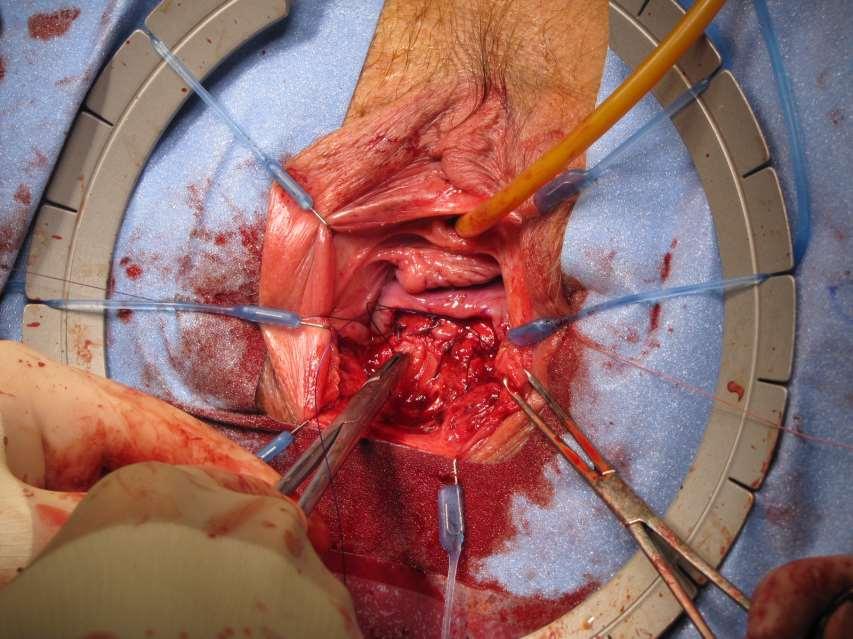
42 Lateral drainage tunnels

43


44 Anterior to posterior sutures


45

46

47
48
49 Posterior colpoperinorrhaphy High levator plication Perineoplasty Shortens the Genital Hiatus Takes tension off prior layers, reduces recurrence risk

50

51

52
53 Close epithelium Interrupted or running
54 Vaginectomy /Colpectomy Total
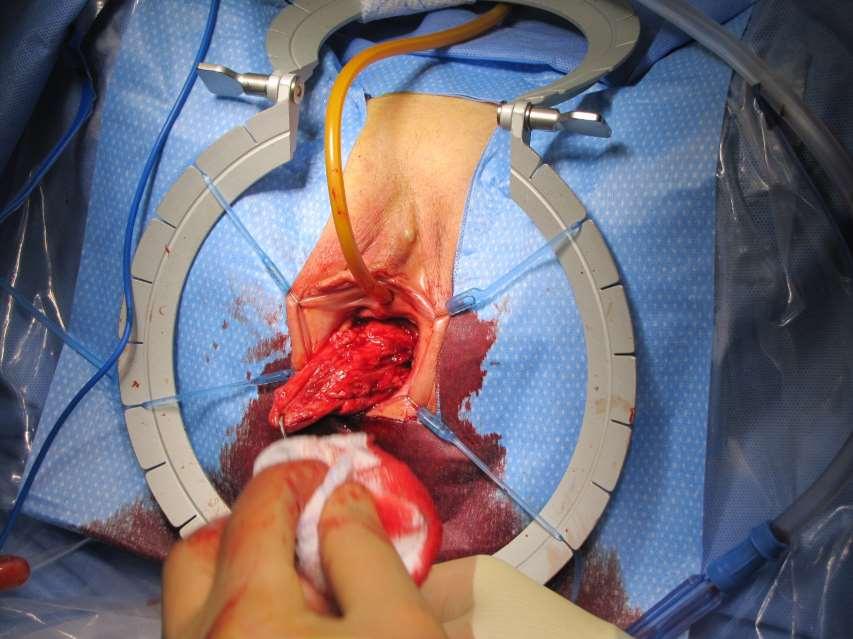
55 Colpectomy Mark out dissection limits Infiltrate Sharp mobilization or epithelium from fibromucularis Mobilize levator ani m. and perineal muscles from skin Control bleeding Suture concentric or A to P multiple layers/rows Colpoperinorrhaphy Close epithelium Cystoscopy +/- MUS

56

57

58
59

60

61
62

63


64

65

66

67

68

69

70
71 Should cystoscopy be performed? YES
72 When should ureteral catheters or stents be placed? Selectively Known or suspected obstruction preop Known or suspected risk of obstruction intraop Concurrent fistula Concurrent removal of mesh
Obliterative surgery for the treatment of pelvic organ prolapse: A patient survey on
 Obliterative surgery for the treatment of pelvic organ prolapse: A patient survey on reasons for surgery selection and post-operative decision regret and satisfaction. Michelle M. Takase-Sanchez, MD Indiana
Obliterative surgery for the treatment of pelvic organ prolapse: A patient survey on reasons for surgery selection and post-operative decision regret and satisfaction. Michelle M. Takase-Sanchez, MD Indiana
International Federation of Gynecology and Obstetrics
 International Federation of Gynecology and Obstetrics COMMITTEE FOR UROGYNAECOLOGY AND PELVIC FLOOR MEMBER: TSUNG-HSIEN (CHARLES) SU, CHAIR (TAIWAN) DAVID RICHMOND, CO-CHAIR (UK) CHITTARANJAN PURANDARE,
International Federation of Gynecology and Obstetrics COMMITTEE FOR UROGYNAECOLOGY AND PELVIC FLOOR MEMBER: TSUNG-HSIEN (CHARLES) SU, CHAIR (TAIWAN) DAVID RICHMOND, CO-CHAIR (UK) CHITTARANJAN PURANDARE,
Clinical Curriculum: Urogynecology
 Updated July 201 Clinical Curriculum: Urogynecology GOAL: The primary goal of the Urogynecology rotation at the University of Alabama at Birmingham (UAB) is to train physicians to have a broad knowledge
Updated July 201 Clinical Curriculum: Urogynecology GOAL: The primary goal of the Urogynecology rotation at the University of Alabama at Birmingham (UAB) is to train physicians to have a broad knowledge
PRACTICE BULLETIN Female Pelvic Medicine & Reconstructive Surgery Volume 23, Number 4, July/August 2017
 PRACTICE BULLETIN Number 176, April 2017 (Replaces Committee Opinion Number 513, December 2011) Pelvic Organ Prolapse Pelvic organ prolapse (POP) is a common, benign condition in women. For many women
PRACTICE BULLETIN Number 176, April 2017 (Replaces Committee Opinion Number 513, December 2011) Pelvic Organ Prolapse Pelvic organ prolapse (POP) is a common, benign condition in women. For many women
Daniel K Roberts MD, PhD 2014 Annual Clinical Update
 Daniel K Roberts MD, PhD 2014 Annual Clinical Update Kevin E Miller, MD Division of Female Pelvic Medicine and Reconstructive Surgery Dept. of OBGYN University of Kansas School of Medicine- Wichita at
Daniel K Roberts MD, PhD 2014 Annual Clinical Update Kevin E Miller, MD Division of Female Pelvic Medicine and Reconstructive Surgery Dept. of OBGYN University of Kansas School of Medicine- Wichita at
Understanding Pelvic Organ Prolapse. Stephanie Pickett, MD, MS Female Pelvic Medicine and Reconstructive Surgery
 Understanding Pelvic Organ Prolapse Stephanie Pickett, MD, MS Female Pelvic Medicine and Reconstructive Surgery Disclosures None I am the daughter of a physician assistant. Objectives List types of pelvic
Understanding Pelvic Organ Prolapse Stephanie Pickett, MD, MS Female Pelvic Medicine and Reconstructive Surgery Disclosures None I am the daughter of a physician assistant. Objectives List types of pelvic
What are we talking about? Symptoms. Prolapse Risk Factors. Vaginal bulge 1 Splinting. ?? Pelvic pressure Back pain 1 Urinary complaints 2
 Options for Vaginal Prolapse What are we talking about? Michelle Y. Morrill, M.D. Director of Urogynecology The Permanente Medical Group Kaiser, San Francisco Assistant Professor, Volunteer Faculty Department
Options for Vaginal Prolapse What are we talking about? Michelle Y. Morrill, M.D. Director of Urogynecology The Permanente Medical Group Kaiser, San Francisco Assistant Professor, Volunteer Faculty Department
By:Dr:ISHRAQ MOHAMMED
 By:Dr:ISHRAQ MOHAMMED Protrusion of an organ or structure beyond its normal confines. Prolapses are classified according to their location and the organs contained within them. 1-Anterior vaginal wall
By:Dr:ISHRAQ MOHAMMED Protrusion of an organ or structure beyond its normal confines. Prolapses are classified according to their location and the organs contained within them. 1-Anterior vaginal wall
Traditional Anterior, Posterior, and Apical Compartment Repairs A Technique Based Review
 Traditional Anterior, Posterior, and Apical Compartment Repairs A Technique Based Review Sandip Vasavada, MD Center for Female Urology and Pelvic Reconstructive Surgery The Glickman Urological and Kidney
Traditional Anterior, Posterior, and Apical Compartment Repairs A Technique Based Review Sandip Vasavada, MD Center for Female Urology and Pelvic Reconstructive Surgery The Glickman Urological and Kidney
Facing Gynecologic Surgery?
 Facing Gynecologic Surgery? Domenico Vitobello, MD Domenico Vitobello is the medical director of the Gynecologic Unit at the Humanitas Clinical and Research Center since 2009. He has developed a comprehensive
Facing Gynecologic Surgery? Domenico Vitobello, MD Domenico Vitobello is the medical director of the Gynecologic Unit at the Humanitas Clinical and Research Center since 2009. He has developed a comprehensive
Gynecology Dr. Sallama Lecture 3 Genital Prolapse
 Gynecology Dr. Sallama Lecture 3 Genital Prolapse Genital(utero-vaginal )prolapse is extremely common, with an estimated 11% of women undergoing at least one operation for this condition. Definition: A
Gynecology Dr. Sallama Lecture 3 Genital Prolapse Genital(utero-vaginal )prolapse is extremely common, with an estimated 11% of women undergoing at least one operation for this condition. Definition: A
Postoperative Care for Pelvic Fistulae. Peter Jeppson, MD October 3, 2017
 Postoperative Care for Pelvic Fistulae Peter Jeppson, MD October 3, 2017 No Disclosures Rational for Postoperative Care Intraoperative injury may be managed by: Identification Closure Continuous post-operative
Postoperative Care for Pelvic Fistulae Peter Jeppson, MD October 3, 2017 No Disclosures Rational for Postoperative Care Intraoperative injury may be managed by: Identification Closure Continuous post-operative
ASYMPTOMATIC MICROSCOPIC HEMATURIA IN WOMEN JOLYN HILL, MD ASSISTANT PROFESSOR, CLINICAL UROGYNECOLOGY FEBRUARY14, 2017
 ASYMPTOMATIC MICROSCOPIC HEMATURIA IN WOMEN JOLYN HILL, MD ASSISTANT PROFESSOR, CLINICAL UROGYNECOLOGY FEBRUARY14, 2017 DISCLOSURES No financial disclosures Urogynecologist via Ob/Gyn pathway ASYMPTOMATIC
ASYMPTOMATIC MICROSCOPIC HEMATURIA IN WOMEN JOLYN HILL, MD ASSISTANT PROFESSOR, CLINICAL UROGYNECOLOGY FEBRUARY14, 2017 DISCLOSURES No financial disclosures Urogynecologist via Ob/Gyn pathway ASYMPTOMATIC
Introduction to GYN Specialties
 Outline Introduction to GYN Specialties Gynecologic Oncology* Female Pelvic Medicine and Reconstructive Surgery* Reproductive Endocrinology and Infertility* Pediatric and Adolescent Gynecology** Family
Outline Introduction to GYN Specialties Gynecologic Oncology* Female Pelvic Medicine and Reconstructive Surgery* Reproductive Endocrinology and Infertility* Pediatric and Adolescent Gynecology** Family
Stop Coping. Start Living. Talk to your doctor about pelvic organ prolapse and sacrocolpopexy
 Stop Coping. Start Living Talk to your doctor about pelvic organ prolapse and sacrocolpopexy Did you know? One in three women will suffer from a pelvic health condition in her lifetime. Four of the most
Stop Coping. Start Living Talk to your doctor about pelvic organ prolapse and sacrocolpopexy Did you know? One in three women will suffer from a pelvic health condition in her lifetime. Four of the most
Sara Schaenzer Grand Rounds January 24 th, 2018
 Sara Schaenzer Grand Rounds January 24 th, 2018 Bladder Anatomy Ureter Anatomy Areas of Injury Bladder: Posterior bladder wall above trigone Ureter Crosses beneath uterine vessels At pelvic brim when ligating
Sara Schaenzer Grand Rounds January 24 th, 2018 Bladder Anatomy Ureter Anatomy Areas of Injury Bladder: Posterior bladder wall above trigone Ureter Crosses beneath uterine vessels At pelvic brim when ligating
Interventional procedures guidance Published: 28 June 2017 nice.org.uk/guidance/ipg583
 Sacrocolpopexy using mesh to repair vaginal vault prolapse Interventional procedures guidance Published: 28 June 2017 nice.org.uk/guidance/ipg583 Your responsibility This guidance represents the view of
Sacrocolpopexy using mesh to repair vaginal vault prolapse Interventional procedures guidance Published: 28 June 2017 nice.org.uk/guidance/ipg583 Your responsibility This guidance represents the view of
Two-thirds of the almost one-half million
 Minimally Invasive Surgery New data and the guidance of our professional societies are bringing us closer to clarity in understanding the superiority of minimally invasive techniques of hysterectomy Amy
Minimally Invasive Surgery New data and the guidance of our professional societies are bringing us closer to clarity in understanding the superiority of minimally invasive techniques of hysterectomy Amy
Urogynecology ICD-9 to ICD-10 Crosswalks
 1100 Wayne Ave, Suite 825 Silver Spring, MD 20910 301.273.0570 Fax 301.273.0778 info@augs.org www.augs.org Urogynecology ICD-9 to ICD-10 Crosswalks ICD 9 ICD 9 Description ICD 10 Code ICD 10 Description
1100 Wayne Ave, Suite 825 Silver Spring, MD 20910 301.273.0570 Fax 301.273.0778 info@augs.org www.augs.org Urogynecology ICD-9 to ICD-10 Crosswalks ICD 9 ICD 9 Description ICD 10 Code ICD 10 Description
Subjective and objective results 1 year after robotic sacrocolpopexy using a lightweight Y-mesh
 DOI 10.1007/s00192-013-2265-x ORIGINAL ARTICLE Subjective and objective results 1 year after robotic sacrocolpopexy using a lightweight Y-mesh Patrick J. Culligan & Emil Gurshumov & Christa Lewis & Jennifer
DOI 10.1007/s00192-013-2265-x ORIGINAL ARTICLE Subjective and objective results 1 year after robotic sacrocolpopexy using a lightweight Y-mesh Patrick J. Culligan & Emil Gurshumov & Christa Lewis & Jennifer
Subspecialty Procedural Volume Guidelines
 Subspecialty Review Committee for Obstetrics and Gynecology In response to requests from program directors, and in an effort to be transparent, the Review Committee for Obstetrics and Gynecology has elected
Subspecialty Review Committee for Obstetrics and Gynecology In response to requests from program directors, and in an effort to be transparent, the Review Committee for Obstetrics and Gynecology has elected
Posterior Deep Endometriosis. What is the best approach? Posterior Deep Endometriosis. Should we perform a routine excision of the vagina??
 Posterior Deep Endometriosis What is the best approach? Dept Gyn Obst Polyclinique Hotel Dieu CHU Clermont Ferrand France Posterior Deep Endometriosis Organs involved - Peritoneum - Uterine cervix -Rectum
Posterior Deep Endometriosis What is the best approach? Dept Gyn Obst Polyclinique Hotel Dieu CHU Clermont Ferrand France Posterior Deep Endometriosis Organs involved - Peritoneum - Uterine cervix -Rectum
Le Forts partial colpocleisis: a review of one surgeons experience
 Gynecol Surg (2004) 1:15 19 DOI 10.1007/s10397-004-0006-3 ORIGINAL ARTICLE Amanda J. O Leary Sanjay K. Vyas Le Forts partial colpocleisis: a review of one surgeons experience Published online: 13 February
Gynecol Surg (2004) 1:15 19 DOI 10.1007/s10397-004-0006-3 ORIGINAL ARTICLE Amanda J. O Leary Sanjay K. Vyas Le Forts partial colpocleisis: a review of one surgeons experience Published online: 13 February
Hysterectomy. What is a hysterectomy? Why is hysterectomy done? Are there alternatives to hysterectomy?
 301.681.3400 OBGYNCWC.COM What is a hysterectomy? Hysterectomy Hysterectomy is surgery to remove the uterus. It is a very common type of surgery for women in the United States. Removing your uterus means
301.681.3400 OBGYNCWC.COM What is a hysterectomy? Hysterectomy Hysterectomy is surgery to remove the uterus. It is a very common type of surgery for women in the United States. Removing your uterus means
Avoiding Mesh Disasters: Tips and Tricks for Success and Handling Complications
 Avoiding Mesh Disasters: Tips and Tricks for Success and Handling Complications Karyn S. Eilber, M.D. Cedars-Sinai FPMRS Associate Professor, Cedars-Sinai Dept of Surgery Associate Director, Urology Residency
Avoiding Mesh Disasters: Tips and Tricks for Success and Handling Complications Karyn S. Eilber, M.D. Cedars-Sinai FPMRS Associate Professor, Cedars-Sinai Dept of Surgery Associate Director, Urology Residency
OUTCOMES OF ROBOTIC, LAPAROSCOPIC AND OPEN ABDOMINAL HYSTERECTOMY FOR BENING CONDITIONS IN OBESE PATIENTS
 OUTCOMES OF ROBOTIC, LAPAROSCOPIC AND OPEN ABDOMINAL HYSTERECTOMY FOR BENING CONDITIONS IN OBESE PATIENTS Omer L. Tapisiz, Tufan Oge, Ibrahim Alanbay, Mostafa Borahay, Gokhan S. Kilic Department of Obstetrics
OUTCOMES OF ROBOTIC, LAPAROSCOPIC AND OPEN ABDOMINAL HYSTERECTOMY FOR BENING CONDITIONS IN OBESE PATIENTS Omer L. Tapisiz, Tufan Oge, Ibrahim Alanbay, Mostafa Borahay, Gokhan S. Kilic Department of Obstetrics
Female Pelvic Medicine & Reconstructive Surgery
 Female Pelvic Medicine & Reconstructive Surgery APPLICATION FOR NEW FELLOWSHIP Name of Institution: McGill University Location: Royal Victoria Hospital (Glen Site), St Mary s Hospital Centre Type of Fellowship:
Female Pelvic Medicine & Reconstructive Surgery APPLICATION FOR NEW FELLOWSHIP Name of Institution: McGill University Location: Royal Victoria Hospital (Glen Site), St Mary s Hospital Centre Type of Fellowship:
Motility Disorders. Pelvic Floor. Colorectal Center for Functional Bowel Disorders (N = 701) January 2010 November 2011
 January 2010 November 2011") Motility Disorders Pelvic Floor Colorectal Center for Functional Bowel Disorders (N = 71) January 21 November 211 New Patients 35 3 25 2 15 1 5 Constipation Fecal Incontinence Rectal Prolapse Digestive-Genital
Motility Disorders Pelvic Floor Colorectal Center for Functional Bowel Disorders (N = 71) January 21 November 211 New Patients 35 3 25 2 15 1 5 Constipation Fecal Incontinence Rectal Prolapse Digestive-Genital
Anatomical and Functional Results of Pelvic Organ Prolapse Mesh Repair: A Prospective Study of 105 Cases
 International Journal of Clinical Urology 2018; 2(1): 20-24 http://www.sciencepublishinggroup.com/j/ijcu doi: 10.11648/j.ijcu.20180201.14 Anatomical and Functional Results of Pelvic Organ Prolapse Mesh
International Journal of Clinical Urology 2018; 2(1): 20-24 http://www.sciencepublishinggroup.com/j/ijcu doi: 10.11648/j.ijcu.20180201.14 Anatomical and Functional Results of Pelvic Organ Prolapse Mesh
Index. Cyclical pelvic pain, 37 Cystocele, 22, 23, 25, 48, 51, 52, 54, 56, 124, 148, 160
 A Abdominal approach, 141 Abdominal hernia s surgery, 123, 124 Abdominal sacrocolpopexy (ASC), 116, 117 Abnormal uterine bleeding, 96 Anterior compartment repair, 101, 102 Apical compartment repair, 96
A Abdominal approach, 141 Abdominal hernia s surgery, 123, 124 Abdominal sacrocolpopexy (ASC), 116, 117 Abnormal uterine bleeding, 96 Anterior compartment repair, 101, 102 Apical compartment repair, 96
Review Colpocleisis revisited
 The Obstetrician & Gynaecologist 10.1576/toag.10.3.133.27414 www.rcog.org.uk/togonline Colpocleisis revisited Authors Pallavi M Latthe / Kamakshi Karri / AS Arunkalaivanan Key content: Colpocleisis is
The Obstetrician & Gynaecologist 10.1576/toag.10.3.133.27414 www.rcog.org.uk/togonline Colpocleisis revisited Authors Pallavi M Latthe / Kamakshi Karri / AS Arunkalaivanan Key content: Colpocleisis is
Ina S. Irabon, MD, FPOGS, FPSRM, FPSGE Obstetrics and Gynecology Reproductive Endocrinology and Infertility Laparoscopy and Hysteroscopy
 Ina S. Irabon, MD, FPOGS, FPSRM, FPSGE Obstetrics and Gynecology Reproductive Endocrinology and Infertility Laparoscopy and Hysteroscopy Comprehensive Gynecology 7 th edition, 2017 (Lobo RA, Gershenson
Ina S. Irabon, MD, FPOGS, FPSRM, FPSGE Obstetrics and Gynecology Reproductive Endocrinology and Infertility Laparoscopy and Hysteroscopy Comprehensive Gynecology 7 th edition, 2017 (Lobo RA, Gershenson
Pelvic Prolapse. A Patient Guide to Pelvic Floor Reconstruction
 Pelvic Prolapse A Patient Guide to Pelvic Floor Reconstruction Pelvic Prolapse When an organ becomes displaced, or slips down in the body, it is referred to as a prolapse. Your physician has diagnosed
Pelvic Prolapse A Patient Guide to Pelvic Floor Reconstruction Pelvic Prolapse When an organ becomes displaced, or slips down in the body, it is referred to as a prolapse. Your physician has diagnosed
Posterior Deep Endometriosis. What is the best approach? Dept Gyn Obst CHU Clermont Ferrand France
 Posterior Deep Endometriosis What is the best approach? Dept Gyn Obst CHU Clermont Ferrand France Posterior Deep Endometriosis Organs involved - Peritoneum - Uterine cervix - Rectum - Vagina Should we
Posterior Deep Endometriosis What is the best approach? Dept Gyn Obst CHU Clermont Ferrand France Posterior Deep Endometriosis Organs involved - Peritoneum - Uterine cervix - Rectum - Vagina Should we
URINARY DIVERSIONS. Winter 2016 Dr P. O Malley
 URINARY DIVERSIONS Winter 2016 Dr P. O Malley OVERVIEW Who gets diversions? What s involved with cystectomy? What are the different types of diversions? What are the problems with various diversions? How
URINARY DIVERSIONS Winter 2016 Dr P. O Malley OVERVIEW Who gets diversions? What s involved with cystectomy? What are the different types of diversions? What are the problems with various diversions? How
Clinical Study Initial Experience with Robotic Retropubic Urethropexy Compared to Open Retropubic Urethropexy
 Obstetrics and Gynecology International Volume 2013, Article ID 315680, 5 pages http://dx.doi.org/10.1155/2013/315680 Clinical Study Initial Experience with Retropubic Urethropexy Compared to Open Retropubic
Obstetrics and Gynecology International Volume 2013, Article ID 315680, 5 pages http://dx.doi.org/10.1155/2013/315680 Clinical Study Initial Experience with Retropubic Urethropexy Compared to Open Retropubic
2/25/2013. Speaker Disclosure. Learning Objectives. Ob/Gyn Conference Series: Urinary and Fecal Incontinence After Vaginal Childbirth
 Ob/Gyn Conference Series: Urinary and Fecal Incontinence After Vaginal Childbirth Jaime Sepulveda-Toro MD FACS FACOG Female Pelvic Medicine and Reconstructive Pelvic Surgery South Miami Hospital Speaker
Ob/Gyn Conference Series: Urinary and Fecal Incontinence After Vaginal Childbirth Jaime Sepulveda-Toro MD FACS FACOG Female Pelvic Medicine and Reconstructive Pelvic Surgery South Miami Hospital Speaker
John Laughlin 4 th year Cardiff University Medical Student
 John Laughlin 4 th year Cardiff University Medical Student Prolapse/incontinence You need to know: Pelvic floor anatomy in relation to uterovaginal support and continence The classification of uterovaginal
John Laughlin 4 th year Cardiff University Medical Student Prolapse/incontinence You need to know: Pelvic floor anatomy in relation to uterovaginal support and continence The classification of uterovaginal
Robotic-Assisted Surgery in Urogynecology: Beyond Sacrocolpopexy
 Robotic-Assisted Surgery in Urogynecology: Beyond Sacrocolpopexy Marie Fidela R. Paraiso, M.D. Professor of Surgery Section Head, Urogynecology and Reconstructive Pelvic Surgery Cleveland, OH Disclosures
Robotic-Assisted Surgery in Urogynecology: Beyond Sacrocolpopexy Marie Fidela R. Paraiso, M.D. Professor of Surgery Section Head, Urogynecology and Reconstructive Pelvic Surgery Cleveland, OH Disclosures
ROBOTIC MESH SACROCOLPOPEXY
 ROBOTIC MESH SACROCOLPOPEXY Philippe E. Zimmern, MD, FACS Professor of Urology Mesh sacrocolpopexy Background First described in 1962 by Lane Until then, treatment options were: Pessary Colpocleisis Vaginal
ROBOTIC MESH SACROCOLPOPEXY Philippe E. Zimmern, MD, FACS Professor of Urology Mesh sacrocolpopexy Background First described in 1962 by Lane Until then, treatment options were: Pessary Colpocleisis Vaginal
COMPARISON OF LOCAL ANESTHESIA AND CONSCIOUS SEDATION WITH SPINAL ANESTHESIA IN VAGINAL RECONSTRUCTIVE SURGERIES
 Original Article COMPARISON OF LOCAL ANESTHESIA AND CONSCIOUS SEDATION WITH SPINAL ANESTHESIA IN VAGINAL RECONSTRUCTIVE SURGERIES Atashkhoyi Simin 1, Fardiazar Zahra 2 ABSTRACT Objective: There are some
Original Article COMPARISON OF LOCAL ANESTHESIA AND CONSCIOUS SEDATION WITH SPINAL ANESTHESIA IN VAGINAL RECONSTRUCTIVE SURGERIES Atashkhoyi Simin 1, Fardiazar Zahra 2 ABSTRACT Objective: There are some
Posterior intravaginal slingplasty for vault and uterovaginal prolapse: an initial experience
 Gynecol Surg (2006) 3: 88 92 DOI 10.1007/s10397-005-0168-7 ORIGINAL ARTICLE R. Oliver. C. Dasgupta. A. Coker Posterior intravaginal slingplasty for vault and uterovaginal prolapse: an initial experience
Gynecol Surg (2006) 3: 88 92 DOI 10.1007/s10397-005-0168-7 ORIGINAL ARTICLE R. Oliver. C. Dasgupta. A. Coker Posterior intravaginal slingplasty for vault and uterovaginal prolapse: an initial experience
INTERNATIONAL UROGYNAECOLOGICAL ASSOCIATION (IUGA) JOINT REPORT ON THE TERMINOLOGY FOR SURGICAL PROCEDURES TO
 JOINT REPORT ON THE TERMINOLOGY FOR SURGICAL PROCEDURES TO") AN AMERICAN UROGYNECOLOGIC SOCIETY (AUGS) / INTERNATIONAL UROGYNAECOLOGICAL ASSOCIATION (IUGA) JOINT REPORT ON THE TERMINOLOGY FOR SURGICAL PROCEDURES TO TREAT PELVIC ORGAN PROLAPSE NEED FOR A WORKING
AN AMERICAN UROGYNECOLOGIC SOCIETY (AUGS) / INTERNATIONAL UROGYNAECOLOGICAL ASSOCIATION (IUGA) JOINT REPORT ON THE TERMINOLOGY FOR SURGICAL PROCEDURES TO TREAT PELVIC ORGAN PROLAPSE NEED FOR A WORKING
HYSTERECTOMY FOR BENIGN CONDITIONS
 HYSTERECTOMY FOR BENIGN CONDITIONS UnitedHealthcare Oxford Clinical Policy Policy Number: SURGERY 104.7 T2 Effective Date: April 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE... 1 CONDITIONS OF COVERAGE...
HYSTERECTOMY FOR BENIGN CONDITIONS UnitedHealthcare Oxford Clinical Policy Policy Number: SURGERY 104.7 T2 Effective Date: April 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE... 1 CONDITIONS OF COVERAGE...
Hysterectomy Fact versus fiction. Richard Dover Specialist Gynaecologist
 Hysterectomy Fact versus fiction Richard Dover Specialist Gynaecologist Disclaimer Disclaimer Hysterectomy An update? Myths busted? HYSTERECTOMY Retro-chic! HMB Important cause of morbidity Affects
Hysterectomy Fact versus fiction Richard Dover Specialist Gynaecologist Disclaimer Disclaimer Hysterectomy An update? Myths busted? HYSTERECTOMY Retro-chic! HMB Important cause of morbidity Affects
PRE-OPERATIVE URODYNAMIC
 PRE-OPERATIVE URODYNAMIC STUDIES: IS THERE VALUE IN PREDICTING POST-OPERATIVE STRESS URINARY INCONTINENCE IN WOMEN UNDERGOING PROLAPSE SURGERY? Dr K Janse van Rensburg Dr JA van Rensburg INTRODUCTION POP
PRE-OPERATIVE URODYNAMIC STUDIES: IS THERE VALUE IN PREDICTING POST-OPERATIVE STRESS URINARY INCONTINENCE IN WOMEN UNDERGOING PROLAPSE SURGERY? Dr K Janse van Rensburg Dr JA van Rensburg INTRODUCTION POP
CHAU KHAC TU M.D., Ph.D.
 CHAU KHAC TU M.D., Ph.D. Hue Central Hospital Vietnam LAPAROSCOPIC PROMONTOFIXATION FOR THE GENITAL PROLAPSE TREATMENT Chau Khac Tu MD.PhD. Hue central hospital CONTENT 3 1 INTRODUCTION 2 OBJECTIVE AND
CHAU KHAC TU M.D., Ph.D. Hue Central Hospital Vietnam LAPAROSCOPIC PROMONTOFIXATION FOR THE GENITAL PROLAPSE TREATMENT Chau Khac Tu MD.PhD. Hue central hospital CONTENT 3 1 INTRODUCTION 2 OBJECTIVE AND
ENDOMETRIOSIS When and how to implement treatment
 ENDOMETRIOSIS When and how to implement treatment Francisco Carmona Hospital Clínic ENDOMETRIOSIS TREATMENT It depends on the severity of symptoms the patient's desire for pregnancy the extent of disease
ENDOMETRIOSIS When and how to implement treatment Francisco Carmona Hospital Clínic ENDOMETRIOSIS TREATMENT It depends on the severity of symptoms the patient's desire for pregnancy the extent of disease
Urethrolysis; When, Why & How. M Karram Professor of Ob/Gyn & Urology University of Cincinnati
 Urethrolysis; When, Why & How M Karram Professor of Ob/Gyn & Urology University of Cincinnati Anatomy Urethra may be fixed to the pubic bone with dense scar tissue Goal of urethrolysis is to completely
Urethrolysis; When, Why & How M Karram Professor of Ob/Gyn & Urology University of Cincinnati Anatomy Urethra may be fixed to the pubic bone with dense scar tissue Goal of urethrolysis is to completely
LAPAROSCOPIC REPAIR OF PELVIC FLOOR
 LAPAROSCOPIC REPAIR OF PELVIC FLOOR Dr. R. K. Mishra Elements comprising the Pelvis Bones Ilium, ischium and pubis fusion Ligaments Muscles Obturator internis muscle Arcus tendineus levator ani or white
LAPAROSCOPIC REPAIR OF PELVIC FLOOR Dr. R. K. Mishra Elements comprising the Pelvis Bones Ilium, ischium and pubis fusion Ligaments Muscles Obturator internis muscle Arcus tendineus levator ani or white
Introduction/Learning Objectives. Incontinence: Natural History. Course Outline 10/14/2016. Urinary Incontinence: Conservative Measures
 Management of Urinary Complications after Prostatectomy Course Faculty: Introduction/Learning Objectives Jaspreet S. Sandhu, MD Associate Attending Urologist Department of Surgery/Urology Memorial Sloan
Management of Urinary Complications after Prostatectomy Course Faculty: Introduction/Learning Objectives Jaspreet S. Sandhu, MD Associate Attending Urologist Department of Surgery/Urology Memorial Sloan
HYSTERECTOMY FOR BENIGN CONDITIONS
 UnitedHealthcare Commercial Medical Policy HYSTERECTOMY FOR BENIGN CONDITIONS Policy Number: 2018T0572G Effective Date: September 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE... 1 BENEFIT CONSIDERATIONS...
UnitedHealthcare Commercial Medical Policy HYSTERECTOMY FOR BENIGN CONDITIONS Policy Number: 2018T0572G Effective Date: September 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE... 1 BENEFIT CONSIDERATIONS...
Cervical Cancer 3/25/2019. Abnormal vaginal bleeding
 Cervical Cancer Abnormal vaginal bleeding Postcoital, intermenstrual or postmenopausal Vaginal discharge Pelvic pain or pressure Asymptomatic In most patients who are not sexually active due to symptoms
Cervical Cancer Abnormal vaginal bleeding Postcoital, intermenstrual or postmenopausal Vaginal discharge Pelvic pain or pressure Asymptomatic In most patients who are not sexually active due to symptoms
Long-Term Effectiveness of Uterosacral Colpopexy and Minimally Invasive Sacral Colpopexy for Treatment of Pelvic Organ Prolapse
 ORIGINAL ARTICLE Long-Term Effectiveness of Uterosacral Colpopexy and Minimally Invasive Sacral Colpopexy for Treatment of Pelvic Organ Prolapse Cecile A. Unger, MD, MPH, Matthew D. Barber, MD, MHS, Mark
ORIGINAL ARTICLE Long-Term Effectiveness of Uterosacral Colpopexy and Minimally Invasive Sacral Colpopexy for Treatment of Pelvic Organ Prolapse Cecile A. Unger, MD, MPH, Matthew D. Barber, MD, MHS, Mark
DENOMINATOR: All patients undergoing anterior or apical pelvic organ prolapse (POP) surgery
 surgery") Quality ID #428: Pelvic Organ Prolapse: Preoperative Assessment of Occult Stress Urinary Incontinence National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY
Quality ID #428: Pelvic Organ Prolapse: Preoperative Assessment of Occult Stress Urinary Incontinence National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY
Le fort s operation for prolapse uterus: A forgotten procedure
 2017; 1(2): 52-56 ISSN (P): 2522-6614 ISSN (E): 2522-6622 Gynaecology Journal www.gynaecologyjournal.com 2017; 1(2): 52-56 Received: 12-09-2017 Accepted: 13-10-2017 Dr. Jasmine Lall 3 rd Year Resident,
2017; 1(2): 52-56 ISSN (P): 2522-6614 ISSN (E): 2522-6622 Gynaecology Journal www.gynaecologyjournal.com 2017; 1(2): 52-56 Received: 12-09-2017 Accepted: 13-10-2017 Dr. Jasmine Lall 3 rd Year Resident,
AGENDA. 8:00 AM 8:30 AM Pelvic Anatomy of the Lower Urinary Tract and the Anatomy and Physiology of Continence/Incontinence Mickey M.
 Thursday, June 12, 2014 Juniper Ballroom 1: Exhibits AGENDA 6:30 AM 8:00 AM Breakfast and Exhibits EVALUATION AND MANAGEMENT OF LOWER URINARY TRACT SYMPTOMS 8:00 AM 8:30 AM Pelvic Anatomy of the Lower
Thursday, June 12, 2014 Juniper Ballroom 1: Exhibits AGENDA 6:30 AM 8:00 AM Breakfast and Exhibits EVALUATION AND MANAGEMENT OF LOWER URINARY TRACT SYMPTOMS 8:00 AM 8:30 AM Pelvic Anatomy of the Lower
Case Based Urology Learning Program
 Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 19 CBULP 2011 044 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 19 CBULP 2011 044 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
Vaginal intraepithelial neoplasia
 Vaginal intraepithelial neoplasia The terminology and pathology of VAIN are analogous to those of CIN (VAIN I-III). The main difference is that vaginal epithelium does not normally have crypts, so the
Vaginal intraepithelial neoplasia The terminology and pathology of VAIN are analogous to those of CIN (VAIN I-III). The main difference is that vaginal epithelium does not normally have crypts, so the
Total vs Subtotal Hysterectomy
 Total vs Subtotal Hysterectomy AN UNSOLVED PROBLEM? G Centini, E Zupi, A Wattiez 153 patient with 15 years of follow-up The Timeline The first successful hysterectomy (Subtotal)! First Laparoscopic Hysterectomy!
Total vs Subtotal Hysterectomy AN UNSOLVED PROBLEM? G Centini, E Zupi, A Wattiez 153 patient with 15 years of follow-up The Timeline The first successful hysterectomy (Subtotal)! First Laparoscopic Hysterectomy!
PL Narducci Department of Obstetrics and Gynecology General Hospital San Giovanni Battista Foligno, ITALY
 NESA DAYS 2018 New European Surgical Academy Perugia, April 19-21, 2018 EXCELLENCE IN FEMALE SURGERY PROLAPSE RECONSTRUCTIVE SURGERY IN SEXUALLY ACTIVE WOMEN LAPAROSCOPIC ANTERIOR ABDOMINAL WALL COLPOPEXY
NESA DAYS 2018 New European Surgical Academy Perugia, April 19-21, 2018 EXCELLENCE IN FEMALE SURGERY PROLAPSE RECONSTRUCTIVE SURGERY IN SEXUALLY ACTIVE WOMEN LAPAROSCOPIC ANTERIOR ABDOMINAL WALL COLPOPEXY
I-STOP TOMS Transobturator Male Sling
 I-STOP TOMS Transobturator Male Sling The CL Medical I-STOP TOMS sling for male stress urinary incontinence was developed in France where it is widely used and is the market leader. It is constructed with
I-STOP TOMS Transobturator Male Sling The CL Medical I-STOP TOMS sling for male stress urinary incontinence was developed in France where it is widely used and is the market leader. It is constructed with
JMSCR Volume 03 Issue 03 Page March 2015
 www.jmscr.igmpublication.org Impact Factor 3.79 ISSN (e)-2347-176x Quality of Life among Patients after Vaginal Hysterectomy and Pelvic Floor Repair Operation ABSTRACT Authors S Lovereen 1, F A Suchi 2,
www.jmscr.igmpublication.org Impact Factor 3.79 ISSN (e)-2347-176x Quality of Life among Patients after Vaginal Hysterectomy and Pelvic Floor Repair Operation ABSTRACT Authors S Lovereen 1, F A Suchi 2,
Surgical repair of vaginal wall prolapse using mesh
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Surgical repair of vaginal wall prolapse using mesh Vaginal wall prolapse happens when the normal support
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Surgical repair of vaginal wall prolapse using mesh Vaginal wall prolapse happens when the normal support
improved with an MIS approach. This clinical benefit for American women has been demonstrated with Level I evidence. Hysterectomy is one of the most
 Statement of the Society of Gynecologic Oncology to the Food and Drug Administration s Obstetrics and Gynecology Medical Devices Advisory Committee Concerning Safety of Laparoscopic Power Morcellation
Statement of the Society of Gynecologic Oncology to the Food and Drug Administration s Obstetrics and Gynecology Medical Devices Advisory Committee Concerning Safety of Laparoscopic Power Morcellation
Dr John Short. Obstetrician and Gynaecologist Christchurch Women s Hospital Oxford Women's Health Christchurch
 Dr John Short Obstetrician and Gynaecologist Christchurch Women s Hospital Oxford Women's Health Christchurch 16:30-17:30 WS #125: Everything GPs Should Know About Gynaecologists 17:35-18:30 WS #135: Everything
Dr John Short Obstetrician and Gynaecologist Christchurch Women s Hospital Oxford Women's Health Christchurch 16:30-17:30 WS #125: Everything GPs Should Know About Gynaecologists 17:35-18:30 WS #135: Everything
Options for Vaginal Prolapse. What is prolapse? What is prolapse? Disclosures 10/23/2013. Michelle Y. Morrill, M.D. None
 Options for Vaginal Prolapse Disclosures None Michelle Y. Morrill, M.D. Director of Urogynecology Kaiser, San Francisco Assistant Professor, Volunteer Faculty Department of Ob/Gyn, UCSF What is prolapse?
Options for Vaginal Prolapse Disclosures None Michelle Y. Morrill, M.D. Director of Urogynecology Kaiser, San Francisco Assistant Professor, Volunteer Faculty Department of Ob/Gyn, UCSF What is prolapse?
Karanvir Virk M.D. Minimally Invasive & Pelvic Reconstructive Surgery 01/28/2015
 Karanvir Virk M.D. Minimally Invasive & Pelvic Reconstructive Surgery 01/28/2015 Disclosures I have none Objectives Identify the basic Anatomy and causes of Pelvic Organ Prolapse Examine office diagnosis
Karanvir Virk M.D. Minimally Invasive & Pelvic Reconstructive Surgery 01/28/2015 Disclosures I have none Objectives Identify the basic Anatomy and causes of Pelvic Organ Prolapse Examine office diagnosis
We welcome comments and corrections which will be used to improve the system annually.
 ACGME Case Log Instructions: Female Pelvic Medicine and Reconstructive Surgery (FPMRS) Review Committees for Obstetrics and Gynecology, and Urology Updated July 2013 BACKGROUND The ACGME Case Log System
ACGME Case Log Instructions: Female Pelvic Medicine and Reconstructive Surgery (FPMRS) Review Committees for Obstetrics and Gynecology, and Urology Updated July 2013 BACKGROUND The ACGME Case Log System
What is endometrial cancer?
 Uterine cancer What is endometrial cancer? Endometrial cancer is the growth of abnormal cells in the lining of the uterus. The lining is called the endometrium. Endometrial cancer usually occurs in women
Uterine cancer What is endometrial cancer? Endometrial cancer is the growth of abnormal cells in the lining of the uterus. The lining is called the endometrium. Endometrial cancer usually occurs in women
Ralph & Berryl Goldman Fellowship in Neuro urology, voiding dysfunction and bladder reconstruction
 Ralph & Berryl Goldman Fellowship in Neuro urology, voiding dysfunction and bladder reconstruction Length of fellowship: A 1 year Fellowship: This fellowship has been designed for Urology or Gynecology
Ralph & Berryl Goldman Fellowship in Neuro urology, voiding dysfunction and bladder reconstruction Length of fellowship: A 1 year Fellowship: This fellowship has been designed for Urology or Gynecology
Michael G. Kelly, MD Gynecologic Oncologist University of Colorado Cancer Center
 Michael G. Kelly, MD Gynecologic Oncologist University of Colorado Cancer Center 50 yo healthy postmenopausal female with BMI = 35 with screening PAP smear = AGUS. What is the next step? (1) Colposcopy
Michael G. Kelly, MD Gynecologic Oncologist University of Colorado Cancer Center 50 yo healthy postmenopausal female with BMI = 35 with screening PAP smear = AGUS. What is the next step? (1) Colposcopy
Operative Approach to Stress Incontinence. Goals of presentation. Preoperative evaluation: Urodynamic Testing? Michelle Y. Morrill, M.D.
 Operative Approach to Stress Incontinence Goals of presentation Michelle Y. Morrill, M.D. Director of Urogynecology The Permanente Medical Group Kaiser, San Francisco Review preoperative care & evaluation
Operative Approach to Stress Incontinence Goals of presentation Michelle Y. Morrill, M.D. Director of Urogynecology The Permanente Medical Group Kaiser, San Francisco Review preoperative care & evaluation
Laparoscopic Sacrocolpopexy with & without the Robot: Tips and Tricks for success and avoidance / management of complications
 Laparoscopic Sacrocolpopexy with & without the Robot: Tips and Tricks for success and avoidance / management of complications Course Faculty: Patrick Culligan, MD Peter Rosenblatt, MD What is a Sacrocolpopexy?
Laparoscopic Sacrocolpopexy with & without the Robot: Tips and Tricks for success and avoidance / management of complications Course Faculty: Patrick Culligan, MD Peter Rosenblatt, MD What is a Sacrocolpopexy?
TURP Complications & Treatments. G. Testa
 TURP Complications & Treatments G. Testa Statistics Operative mortality 0.2 per cent Most common cause of death was sepsis which occurred >1 month after surgery 77% of patients had significant pre-existing
TURP Complications & Treatments G. Testa Statistics Operative mortality 0.2 per cent Most common cause of death was sepsis which occurred >1 month after surgery 77% of patients had significant pre-existing
Pelvic Floor Disorders Following Hysterectomy for Benign Conditions of Uterus and Endometrial Carcinoma - A Long-term Follow-up Study
 Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/527 Pelvic Floor Disorders Following Hysterectomy for Benign Conditions of Uterus and Endometrial Carcinoma - A Long-term
Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/527 Pelvic Floor Disorders Following Hysterectomy for Benign Conditions of Uterus and Endometrial Carcinoma - A Long-term
Efficacy and Adverse Effects of Monarc Versus Tension-free Vaginal Tape Obturator: a Retrospective One-year Follow-up Study
 Efficacy and Adverse Effects of Monarc Versus Tension-free Vaginal Tape Obturator: a Retrospective One-year Follow-up Study Yvonne KY CHENG MBChB, MRCOG William WK TO MBBS, M Phil, FRCOG, FHKAM (O&G) HX
Efficacy and Adverse Effects of Monarc Versus Tension-free Vaginal Tape Obturator: a Retrospective One-year Follow-up Study Yvonne KY CHENG MBChB, MRCOG William WK TO MBBS, M Phil, FRCOG, FHKAM (O&G) HX
Content. Terminology Anatomy Aetiology Presentation Classification Management
 Prolapse Content Terminology Anatomy Aetiology Presentation Classification Management Terminology Prolapse Descent of pelvic organs into the vagina Cystocele ant. vaginal wall involving bladder Uterine
Prolapse Content Terminology Anatomy Aetiology Presentation Classification Management Terminology Prolapse Descent of pelvic organs into the vagina Cystocele ant. vaginal wall involving bladder Uterine
Hysterectomy : A Clinicopathologic Correlation
 Bahrain Medical Bulletin, Vol. 28, No.2, June 2006 Hysterectomy : A Clinicopathologic Correlation Layla S Abdullah, FRCPC* Objective : To study the most common pathologies identified in hysterectomy specimens
Bahrain Medical Bulletin, Vol. 28, No.2, June 2006 Hysterectomy : A Clinicopathologic Correlation Layla S Abdullah, FRCPC* Objective : To study the most common pathologies identified in hysterectomy specimens
Kathleen C. Kobashi, MD, FACS Head, Section of Urology and Renal Transplantation Virginia Mason Medical Center, Seattle, WA
 Kathleen C. Kobashi, MD, FACS Head, Section of Urology and Renal Transplantation Virginia Mason Medical Center, Seattle, WA Disclosures Advisory Board and/or Speaker Allergan Medtronic Astellas AUA Guidelines
Kathleen C. Kobashi, MD, FACS Head, Section of Urology and Renal Transplantation Virginia Mason Medical Center, Seattle, WA Disclosures Advisory Board and/or Speaker Allergan Medtronic Astellas AUA Guidelines
CHEMO-RADIOTHERAPY FOR BLADDER CANCER. Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre
 CHEMO-RADIOTHERAPY FOR BLADDER CANCER Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre AIMS Muscle invasive disease Current Gold-Standard Rationale behind Chemo-Radiotherapy
CHEMO-RADIOTHERAPY FOR BLADDER CANCER Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre AIMS Muscle invasive disease Current Gold-Standard Rationale behind Chemo-Radiotherapy
9/24/2015. Pelvic Floor Disorders. Agenda. What is the Pelvic Floor? Pelvic Floor Problems
 Management of Pelvic Floor Disorders Doctor, I don t want THAT mesh! Agenda What are pelvic floor disorders (PFDs)? What are the treatment options? Expectant. Conservative. Surgical. How and when are grafts
Management of Pelvic Floor Disorders Doctor, I don t want THAT mesh! Agenda What are pelvic floor disorders (PFDs)? What are the treatment options? Expectant. Conservative. Surgical. How and when are grafts
11 th Dynasty- Egyptian mummies : Queen Henhenit circa 2050 BC wife of King Mentuhotep II VVF 550 BC- Ancient Egyptian documents (papyri)
") February 2019 11 th Dynasty- Egyptian mummies : Queen Henhenit circa 2050 BC wife of King Mentuhotep II VVF 550 BC- Ancient Egyptian documents (papyri) Prescription for a woman whose urine is in an irksome
February 2019 11 th Dynasty- Egyptian mummies : Queen Henhenit circa 2050 BC wife of King Mentuhotep II VVF 550 BC- Ancient Egyptian documents (papyri) Prescription for a woman whose urine is in an irksome
Ben Herbert Alex Wojtowicz
 Ben Herbert Alex Wojtowicz 54 year old female presenting with: Dragging sensation Urinary incontinence Some faecal incontinence HPC Since May 14 had noticed a mass protruding from the vagina when going
Ben Herbert Alex Wojtowicz 54 year old female presenting with: Dragging sensation Urinary incontinence Some faecal incontinence HPC Since May 14 had noticed a mass protruding from the vagina when going
Program Schedule. Update in Gynecology and Minimally Invasive Surgery 2018
 Program Schedule Update in Gynecology and Minimally Invasive Surgery 2018 Wednesday, February 7, 2018 6:00 a.m. Registration & Breakfast with Exhibitors 6:55 a.m. Welcome Announcements SESSION: Practical
Program Schedule Update in Gynecology and Minimally Invasive Surgery 2018 Wednesday, February 7, 2018 6:00 a.m. Registration & Breakfast with Exhibitors 6:55 a.m. Welcome Announcements SESSION: Practical
Considering Surgery for Pelvic Prolapse? Learn about minimally invasive da Vinci Surgery
 Considering Surgery for Pelvic Prolapse? Learn about minimally invasive da Vinci Surgery The Surgery: Pelvic Prolapse Surgery If you have pelvic prolapse symptoms, your doctor may suggest medicine or lifestyle
Considering Surgery for Pelvic Prolapse? Learn about minimally invasive da Vinci Surgery The Surgery: Pelvic Prolapse Surgery If you have pelvic prolapse symptoms, your doctor may suggest medicine or lifestyle
Prediction and prevention of stress urinary incontinence after prolapse surgery van der Ploeg, J.M.
 UvA-DARE (Digital Academic Repository) Prediction and prevention of stress urinary incontinence after prolapse surgery van der Ploeg, J.M. Link to publication Citation for published version (APA): van
UvA-DARE (Digital Academic Repository) Prediction and prevention of stress urinary incontinence after prolapse surgery van der Ploeg, J.M. Link to publication Citation for published version (APA): van
Management of Urogenital Prolapse of Women in Primary Care. Lizzie McManus MBE RGN RMN Practice nurse Womens health practitioner
 Management of Urogenital Prolapse of Women in Primary Care Lizzie McManus MBE RGN RMN Practice nurse Womens health practitioner Primary Care Womens Health Forum www.pcwhf.org.uk Useful websites RCN genital
Management of Urogenital Prolapse of Women in Primary Care Lizzie McManus MBE RGN RMN Practice nurse Womens health practitioner Primary Care Womens Health Forum www.pcwhf.org.uk Useful websites RCN genital
With our aging population, the rate of pelvic
 Original Research Short-Term Outcomes of Robotic Sacrocolpopexy Compared With Abdominal Sacrocolpopexy Elizabeth J. Geller, MD, Nazema Y. Siddiqui, MD, Jennifer M. Wu, MD, MPH, and Anthony G. Visco, MD
Original Research Short-Term Outcomes of Robotic Sacrocolpopexy Compared With Abdominal Sacrocolpopexy Elizabeth J. Geller, MD, Nazema Y. Siddiqui, MD, Jennifer M. Wu, MD, MPH, and Anthony G. Visco, MD
Breast Carcinoma The Hard Way
 Women s Health Breast Carcinoma The Hard Way C50 - Malignant neoplasm of breast C50.0 Malignant neoplasm of nipple and areola C50.01 - Malignant neoplasm of nipple and areola, female C50.011 - Malignant
Women s Health Breast Carcinoma The Hard Way C50 - Malignant neoplasm of breast C50.0 Malignant neoplasm of nipple and areola C50.01 - Malignant neoplasm of nipple and areola, female C50.011 - Malignant
MIDLAND MEMORIAL HOSPITAL Delineation of Privileges FEMALE PELVIC MEDICINE AND RECONSTRUCTIVE SURGERY (UROGYNECOLOGY)
") MIDLAND MEMORIAL HOSPITAL Delineation of Privileges FEMALE PELVIC MEDICINE AND RECONSTRUCTIVE SURGERY (UROGYNECOLOGY) Physician Name: Your home for healthcare Female Pelvic Medicine and Reconstructive
MIDLAND MEMORIAL HOSPITAL Delineation of Privileges FEMALE PELVIC MEDICINE AND RECONSTRUCTIVE SURGERY (UROGYNECOLOGY) Physician Name: Your home for healthcare Female Pelvic Medicine and Reconstructive
Voiding dysfunction after vaginal prolapse surgery: etiology, prevention and treatment Hakvoort, R.A.
 UvA-DARE (Digital Academic Repository) Voiding dysfunction after vaginal prolapse surgery: etiology, prevention and treatment Hakvoort, R.A. Link to publication Citation for published version (APA): Hakvoort,
UvA-DARE (Digital Academic Repository) Voiding dysfunction after vaginal prolapse surgery: etiology, prevention and treatment Hakvoort, R.A. Link to publication Citation for published version (APA): Hakvoort,
Elizabeth Geller, MD Mary L. Jannelli, MD Ellen C. Wells, MD
 Division of Female Pelvic Medicine and Reconstructive Surgery Department of Obstetrics and Gynecology University of North Carolina at Chapel Hill School of Medicine Program Faculty Catherine A. Matthews,
Division of Female Pelvic Medicine and Reconstructive Surgery Department of Obstetrics and Gynecology University of North Carolina at Chapel Hill School of Medicine Program Faculty Catherine A. Matthews,
Female Urology. The Results of Grade IV Cystocele Repair Using Mesh. Introduction ZARGAR MA, EMAMI M*, ZARGAR K, JAMSHIDI M
 Urology Journal UNRC/IUA Vol. 1, No. 4, 263-267 Autumn 2004 Printed in IRAN Female Urology The Results of Grade IV Cystocele Repair Using Mesh ZARGAR MA, EMAMI M*, ZARGAR K, JAMSHIDI M Department of Urology,
Urology Journal UNRC/IUA Vol. 1, No. 4, 263-267 Autumn 2004 Printed in IRAN Female Urology The Results of Grade IV Cystocele Repair Using Mesh ZARGAR MA, EMAMI M*, ZARGAR K, JAMSHIDI M Department of Urology,
EndoFast Reliant System vs. Tension- free Mesh in a Sheep Model; three arm Comparative Study Assessing the Mechanical Pullout Force of Mesh Over Time
 EndoFast Reliant System vs. Tension- free Mesh in a Sheep Model; three arm Comparative Study Assessing the Mechanical Pullout Force of Mesh Over Time Menachem Alcalay,M.D, Urogynecology unit, Sheba Medical
EndoFast Reliant System vs. Tension- free Mesh in a Sheep Model; three arm Comparative Study Assessing the Mechanical Pullout Force of Mesh Over Time Menachem Alcalay,M.D, Urogynecology unit, Sheba Medical
SciFed Journal of Public Health. Endoscopic Management of Obstetrical Uretero-Uterine Fistula. Case Report and Review of Literature
 SciFed Journal of Public Health Case Report Open Access Endoscopic Management of Obstetrical Uretero-Uterine Fistula. Case Report and Review of Literature * Yasin Idweini * Chairperson of Urology Department
SciFed Journal of Public Health Case Report Open Access Endoscopic Management of Obstetrical Uretero-Uterine Fistula. Case Report and Review of Literature * Yasin Idweini * Chairperson of Urology Department
Current status in pelvic organ prolapse surgery: an evidence based review
 Current status in pelvic organ prolapse surgery: an evidence based review Christian Falconer, MD, PhD Department of Obstetrics and Gynecology Danderyd University Hospital Stockholm, Sweden Finnish Society
Current status in pelvic organ prolapse surgery: an evidence based review Christian Falconer, MD, PhD Department of Obstetrics and Gynecology Danderyd University Hospital Stockholm, Sweden Finnish Society
Program Schedule. 3 rd Annual Collaborative Symposium: Update in Minimally Invasive Gynecologic Surgery
 Program Schedule 3 rd Annual Collaborative Symposium: Update in Minimally Invasive Gynecologic Surgery Thursday, February 5, 2015 6:45 a.m. Registration and Breakfast 7:25 a.m. Welcome / Announcements
Program Schedule 3 rd Annual Collaborative Symposium: Update in Minimally Invasive Gynecologic Surgery Thursday, February 5, 2015 6:45 a.m. Registration and Breakfast 7:25 a.m. Welcome / Announcements
New York City Development of the Geriatric Collaborative
 New York City - 2014 Development of the Geriatric Collaborative The Clinical Problem More than 50% persons age 65 years will have some surgical procedure in the remainder of his or her lifetime Outcome
New York City - 2014 Development of the Geriatric Collaborative The Clinical Problem More than 50% persons age 65 years will have some surgical procedure in the remainder of his or her lifetime Outcome
Overactive Bladder: Diagnosis and Approaches to Treatment
 Overactive Bladder: Diagnosis and Approaches to Treatment A Hidden Condition* Many Many patients self-manage by voiding frequently, reducing fluid intake, and wearing pads Nearly Nearly two-thirds thirds
Overactive Bladder: Diagnosis and Approaches to Treatment A Hidden Condition* Many Many patients self-manage by voiding frequently, reducing fluid intake, and wearing pads Nearly Nearly two-thirds thirds