Inflammatory Bowel Disease and the Microbiome: Clinical Progress and Questions Left Unanswered
|
|
|
- Angelina Farmer
- 6 years ago
- Views:
Transcription



1 Inflammatory Bowel Disease and the Microbiome: Clinical Progress and Questions Left Unanswered Photo Credit: Jonathan Landsman JESSICA R. ALLEGRETTI, MD, MPH DIRECTOR, FECAL MICROBIOTA TRANSPLANT PROGRAM DIVISION OF GASTROENTEROLGY BRIGHAM AND WOMEN S HOSPITAL
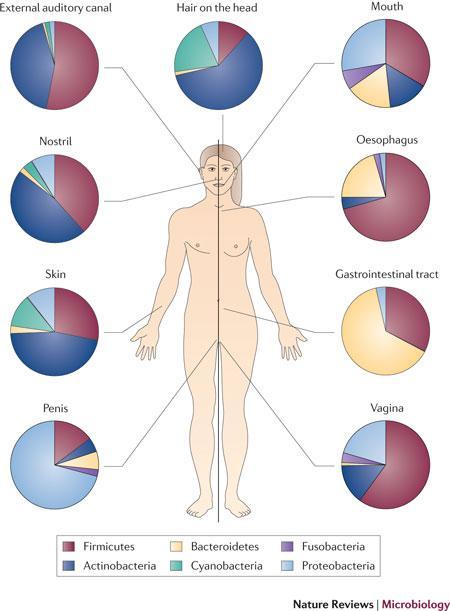
2 What is the Microbiome? Defined as the ecological community of commensal, symbiotic and pathogenic microorganisms that literally share our body space The human microbiome consists of about 100 trillion microbial cells Outnumber human cells 10:1
3
4

5

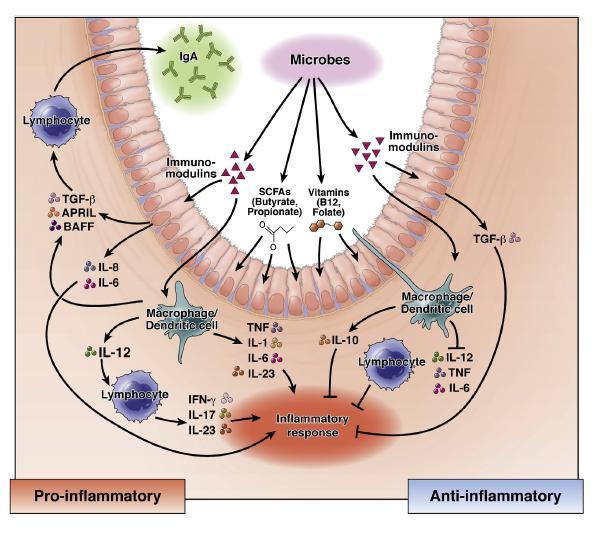
6 Dysbiosis Disrupts Health Alan W. Walker, Trevor D. Lawley. Pharmacological Research Vol 69, Issue

7 Dysbiosis in IBD
8 Kostic, et al. Gastro. 2014; 146(5):
9 Therapeutic Manipulations of the Microbiome in IBD Crohn s disease: role seems clear Diversion of fecal stream is effective Antibiotics are beneficial is subsets of CD patients Role for TPN/bowel rest Ulcerative colitis: role less clear Diversion not effective No clear role for antibiotics or TPN/bowel rest VSL #3 & E. coli Nissle 1917 effective
10 The Emergence of FMT
11 Fecal Microbiota Transplantation Instillation of minimally manipulated microbial communities from stool of a healthy donor into a patient s GI tract. FMT is distinguished from a defined consortia of microorganisms, highlighting the degree of complexity and functionality of the microbiome. Can be considered both a drug and a biologic or tissue

12 Regulations: US May use to treat C. difficile not responding to standard therapy No IND required Informed consent State it is investigational Discuss real and theoretical risks Draft guidance March 2016 Would enforce IND requirement for stool banks
13 Recurrent CDI Recurrence of symptoms after successful initial therapy for C. difficile endogenous persistence of C. difficile spores acquisition of a new strain from an exogenous source. Strains Analysis: two different serogroups in 21.5% same serogroup in 78.5% Barbut et al.
14 Recurrent CDI Recurrence is present when CDI reoccurs within 8 weeks provided the symptoms from the previous episode resolved May occurs within days
15 Recurrent CDI 15-20% of patients ( regardless of initial therapy) 2 nd recurrence: 30-45%; 3 rd recurrence: 45-60% Relapses can continue for years
16 Recurrent CDI in IBD Prevalance 2.5 to 8 times higher 10% lifetime risk of CDI Higher rates of recurrence, chronic carriage and mortality CDI can illicit flares, worsen disease severity and overall course
17 Recurrent CDI: Why does it occur? Impaired host response Altered intestinal microbiome
18 Impaired Host Response Kyne et al. N Engl J Med 2000

19 Impaired Host Response

20 Altered Intestinal Microbiome Decreased phylogenic richness Bacteroidetes and Firmicutes are reduced in patients with recurrent CDI, not in patients with just one episode Chang JY, et al. J Infect Dis 2008:197;435-8
21 Not just microbial membership but function Antibiotics disturb not only the structure of the microbiome but also the function Fermentation of SCFA Lipid metabolism Protein digestion Bile salt metabolism
22 CDI is communicated by ingestion of spores. Spores: 1 are resistant to heat and antibiotics and are able to survive outside of the colon. 2 germinate in the GI tract and become vegetative cells which can produce toxin. 3 Germination is critical to initiate CDI. 4 Bile acids are vital to the germination process. Bartlett. Ann Intern Med 2006 Ridlon et al. J Lipid Res 2006
23 The Relationship between CDI and Bile Acids In vitro primary bile acids can stimulate germination of C. difficile spores: The secondary bile acid deoxycholate can inhibit growth of the vegetative form. Antibiotic therapy may ablate critical members of the microbiota that generate inhibitory (protective) secondary bile acids. Stool extracts from antibiotic treated mice have higher concentrations of primary bile acids and form untreated mice have relatively higher secondary bile acids. The relationship between the host microbiome and bile salt metabolism is poorly defined in humans with CDI.
24 Bile Salt Analysis in Stool
25 Accuracy of Bile Salts as Predictors
26 Treatment: Recurrent CDI First recurrence: In IBD vancomycin should be used. Second recurrence :pulsed vancomycin regimen 125 mg orally four times daily for 14 days 125 mg orally twice daily for 7 days 125 mg orally once daily for 7 days 125 mg orally every other day for 7 days 125 mg orally every 3 days for 14 days *Alternative: fidaxomicin Third recurrence: Fecal Microbiota Transplantation
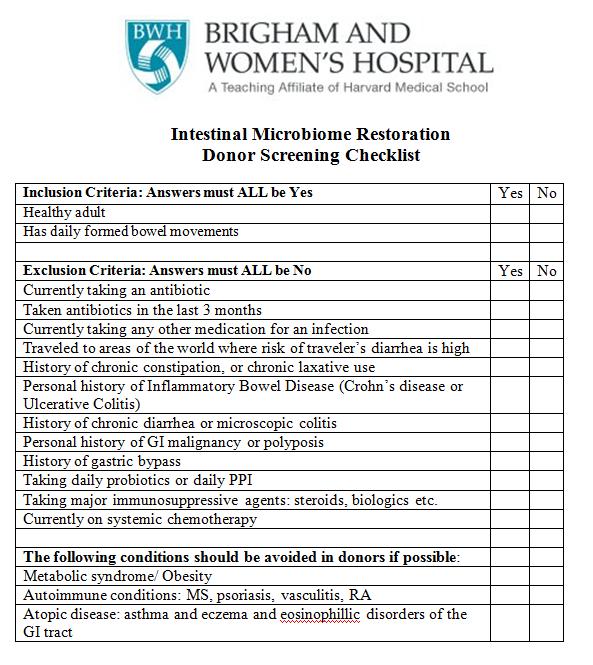
27 Fidaxomicin Trade Name: Dificid Non-systemic (minimally absorbed) Bactericidal Dose 200mg BID x 10 days
28 Non-antibiotic Therapies IVIG no RCT data, no role in severe fulminant disease 400 mg/kg once every 3 weeks for a total of 2 or 3 doses Probiotics Saccharomyces boulardii or lactobacillus species may be added during the final 2 weeks of the vancomycin taper and for at least 4 weeks thereafter (preferably 8 weeks). The efficacy of probiotics in preventing recurrent C. difficile infection is unclear

29 Considerations Prior to Initiating Therapy for rcdi: Consider other etiologies of diarrhea: post infectious IBS, IBD flare Retesting not recommended after therapy unless moderate to severe diarrhea In patients with persistent diarrhea despite appropriate treatment with vancomycin or flagyl other causes must be considered C.difficile is rarely if ever resistant to flagyl or vancomycin
30 Fecal Transplantation: the Basics
31 Steps of FMT : The Four D s 1. Decision: is FMT indicated? 2. Donor Selection: Patient directed vs. universal Fresh or frozen 3. Delivery Modality: Enema Colonoscopy / sigmoidoscopy NG/NJ tube Capsules 4. Discharge and Follow-up
32 Step 1: Decision Patient Selection Appropriate candidates are: patients who have confirmed relapsing CDI (a history of 3 or more episodes, or 2 episodes that required hospitalization) patients with refractory disease that is unresponsive to traditional antibiotics.
33 Step 2: Donor Selection Patient Directed Source: Family or Friend Pros: Patient comfort Cons: Multiple tests Expensive Delays care Physician s time Universal Donor Pros: Routinely tested healthy individual proven donor track Minimize cost Cons Billing Food allergies
34 Donors Donors must be 18 years old Donors may be relatives or friends to the recipient Donors should be otherwise healthy and have daily formed BMs. They should not have a history of Inflammatory Bowel Disease or chronic constipation. No antibiotics within the last 3 months
35

36 Frozen vs. Fresh Stool Randomized, double blind, non-inferiority trial 232 adults with recurrent or refractory CDI Up to 2 FMT by enema Clinical 13 weeks mitt: 75% (frozen) & 70% (fresh) Per Protocol: 83.5% (frozen) & 85.1% (fresh) Lee CH, et al. JAMA 2016
37 Screening Blood: Hepatitis A (IgG and IgM) Hepatitis B (HBsAg/Ab and HBcAb) Hepatitis C Ab HIV-1/2 (Ab and viral load) Syphilis (TP-IgG) during Stool: C. difficile (by culture) Routine stool culture Giardia antigen Cryptosporidium antigen O&P Food Allergies


38 Frozen stool from a bank: OpenBiome Model 1 Clinician orders fecal preparations from a stool bank <5% pass rate 2 Stool bank provides rigorously screened, processed, frozen material 3 The clinician thaws material and performs FMT Donor Assessment 109-point clinical assessment for transmissible infectious diseases and potentially microbiome-mediated conditions E.g. IBD, IBS, depression, anxiety, age, obesity, metabolic syndrome, autoimmune diseases and others Stool testing Stool & Serological Testing - C. diff toxin PCR, Ova & Parasites, Isospora, Cyclospora, Giardia EIA; Cryptosporidium EIA; H. pylori Ag, Common enteric pathogens (e.g. Salmonella, Shigella, E. coli, Campylobacter, Vibrio, Norovirus PCR, Adenovirus EIA, Rotovirus EIA, VRE culture, Microsporidium Serological testing - HIV 1 & 2, HAV, HBV, HCV, HTLV 1 & 2, Treponema pallidum. CBC, LFTs Processing, Monitoring & Re-testing 60-day quarantine procedure Continuous requalification Processing controls Filtering & homogenization Safety aliquots Storage & shipping controls Traceability 16s rrna (microbiome) sequencing & characterization




39 Step 3: Mode of Delivery Nasogastric or nasoduodenal tube Uncomfortable Requires radiology Retention enemas Variable patient ability to tolerate Lower endoscopy Enables examination of mucosa Encapsulation Decreased procedure related risk & cost Aas et al. 2003; Rubin et al 2012; Van Nood 2013; Silverman et al. 2010; Kassam et al 2012; Lee et al 2014;

40 Cumulative evidence 87%-89% experienced clinical resolution No adverse events associated with FMT reported 93% 81% 86% 82% 91% 83% Cammarota G. J Clin Gastroenterol 2014 Kassam Z, Am J Gastroenterol 2013
41 Preparation Recipient: Standard bowel prep required Continue Abx until day before Donor: MOM the night before is ok Stool volume: gm Collected within 6 hrs of procedure Stool should not be refrigerated *Avoid food allergens
42 Stool Preparation Stool is blended with 500cc NS for 1 min until liquid Solution is passed through a strainer into an emesis basin Drawn up into 60cc syringes Solution can be instilled through the scope Full colonoscopy to the TI is performed Instillation in the TI and right colon

43



44

45

46
47 Step 4: Discharge and Follow Up Post FMT Retain slurry for 2-6 hours Imodium post-procedure Avoid future antibiotics
48
49 Fischer/Allegretti DDW 2016 What if I Need an Antibiotics Again? N= % Overall Post FMT CDI recurrence rate (63%) received antibiotics 6 (37%)did not receive antibiotics
50 If I take an antibiotic, should I take a prophylactic antibiotic or probiotic with it to prevent c.diff, and if so which ones? Recurrence Rates: with neither: 23% (4/17) with probiotic only: 21% (3/14) with anti-cdi antibiotic only: 0% (0/12) with concomitant anti-cdi antibiotic + probiotic: 20% (3/15) with concomitant anti-cdi antibiotics and/or probiotic 15%(6/41)
51 What if They Need Antibiotics Again? Reassure: recurrence rates are low post FMT Suggest the most narrow spectrum antibiotics Prophylactic Flagyl or Vancomycin not recommended - No proven benefit, possible harm

52 How Effective is FMT?
53 How Effective is FMT for recurrent CDI? Multiple systematic reviews and meta analyses: shows 90% efficacy Guol APT 2012 Sofi Scand J Gastro 2013; Kassam Am J Gastroenterol Drekonja JAMA 2015 Now, 4 randomized controlled trials VanNood Youngster Cammarota Kelly C.
54 Rates of Cure without Relapse for Recurrent Clostridium difficile Infection. Duodenal Infusion of Donor Feces for Recurrent Clostridium difficile van Nood E et al. N Engl J Med 2013;368:
55 Kassam et al. AM J Gastroenterol, 2013 Summary: 89.7%, 95% CI 84%-93%)
56 How Effective is FMT for recurrent CDI in IBD? 67 patient with IBD who underwent FMT CDI Outcomes: 79% efficacy at clearing CDI IBD Outcomes: 46.3% improved 35.8% unchanced 17.9% worsened
57
58 Safety profile in IBD Mild Adverse Events: Vomiting, diarrhea, flatulence, bloating Infection Transmission: CMV after self-administered-fmt Life-threatening Listeria infection in UC patient Disease Flare: Fevers, elevated inflammatory markers and abdominal tenderness post-fmt IBD patients on immunosuppressive therapy who underwent FMT for CDI 5/36 IBD (14%) experienced IBD flare post FMT Vermeire S. Gastroenterology 2012 Angelberger S, et al. Am J Gastroenterol 20 Hohmann E, et al. N Engl J Med 2014 Iokona C, Kelly C. et al. Am J. Gastro 2014 Surawicz C. personnel communications
59

60 Capsules: he Future of FMT Research in IBD
61 Capsules Pros avoid a procedure, anesthesia lower cost No bowel prep Cons motility large pills many pills Dose unknown
62 FMT capsules: Current Landscape A recent proof-of-concept case series suggested a version of oral FMT capsules may be effective Method: Stool suspension generated in saline Sequentially sieved & centrifuged, Resuspend pellet in saline/glycerol Size 00 capsules and frozen (-80 o C) Mean stool per capsule: 1.6g Dosing: 15 capsules on 2 consecutive days Total of 48 grams of stool If non-response, re-treated with 15 capsules on 2 consecutive days Youngster et al JAMA 2014 Results: Single course: 70% clinical cure Extended course: 90% clinical cure No serious adverse events Issues: 1 Unstable formulation aqueous attack on gelatin vehicle Propensity for degradation 2 3 Time consuming & non-scalable Arbitrary dose The minimum effective dose of capsule based FMT is unknown. Current dosing standards: 25 grams of stool in 250mls of saline for lower GI administration 12.5 grams of stool in 30mls of saline for upper GI administration.



63 Novel FMT Capsule: Microbial Emulsion Matrix 1 Highly stable at room temperature 2 Scalable process >25,000 capsules produced 3 Dosing Mean stool per capsule: 0.75g Viability Stability Mendolia, Kassam et al, ACG 2015
 referred for FMT Failed to maintain CDI cure after standard therapy Allegretti")
 between high & low dose 2. Clinical resolution of diarrhea with no CDI recurrence at 8-weeks")
64 Methods: Study Overview Open-label, cluster dose-finding study performed at two academic, quaternary care hospitals High dose: 45g Day 1 30 capsules Day 2 30 capsules Inclusion criteria Outpatient recurrent CDI (3 or more episodes) referred for FMT Failed to maintain CDI cure after standard therapy Allegretti DDW 2016 Site 1 Site 2 Key exclusion criteria Dysphagia / test capsule failure History of aspiration Severe-complicated CDI IBD Day 1 30 capsules Low dose: 22.5g Day 3 Day 7 Week 4 Week 8 Endpoints 1. Safety (grade 2+) between high & low dose 2. Clinical resolution of diarrhea with no CDI recurrence at 8-weeks
65 Results: Single FMT capsule course No adverse events attributed to FMT were observed in either group High Dose N=7 Low Dose N=10 P-value Clinical remission at 72 hours Clinical cure at 8 week 7 (100%) 8 (80%) (71%) 7 (70%) 0.33
66 Results Overall 5 patients were non-responders 3 low dose group 2 high dose group After re-treatment with high dose capsule FMT, 4/5 (80%) had resolution of symptoms 1 patient underwent successful FMT by colonoscopy Aggregate FMT capsule response rate: 16/17 (94%) Treatment algorithm: initial course of low dose capsules followed by high dose retreatment for nonresponders

67 Severe CDI 14-18% 30 day all-cause mortality Surgery for refractory/complicated infection: Total abdominal colectomy with end ileostomy procedure of choice 30 day perioperative mortality 30-80% not good surgical candidates Jaber M. Am J Gastro; 2008 Schmic D. J Infect Pub Health 2014 Solomon K, et al. J Med Microbiol 2013

 cured")

68 Fischer Protocol Sequential FMT 29 patients: 10 severe & 19 severe complicated 5 toxic megacolon 59% female; mean age 65 27/29 (93%) cured Single FMT 62% 2 FMT 31% 3 FMT 7% 30 day all cause mortality 7% Fischer M. Aliment Pharm Thera 2015.
69 FMT for the Treatment of IBD
70 Cannot be performed in the US for clinical care currently IND from the FDA is required Ongoing Clinical Trials
71 Case Reports for FMT in IBD 1989: Bennet et al. self treated with fecal enemas for UC Clinical and histologic remission 2012 Systematic Review: 41 patients with IBD and CDI Reduction of symptoms (76%) disease remission (62%) Bennet JD. Lancet 1989 Borody TJ, et al. Am J Gastroenterol 2012
72 Meta-analysis 36.2% achieved clinical remission (95% CI 17.4%-60.4%) -60.5% of CD patients (95% CI 28.4%-85.6%) -64% of younger patients (95% CI 10.6%-96.4%) -22% of UC patients (95% CI 10.4%-40.8%) Colman RJ, JCC 2014

73 Randomized Controlled Trials
74 Focus Trial Double-blinded multi center RCT Included: active UC resistant to standard treatments Randomized to receive: a single FMT via colonoscopic on day 1 followed by enema 5 days/week for 8 weeks Placebo FMT via colonoscopy followed by placebo enemas Active treatment: 3 to 7 unrelated donors. Primary endpoint: steroid-free clinical remission + endoscopic response/remission
75 Results 81 patients enrolled. Steroid-free clinical remission + endoscopic response: 11 of 41 (27%) patients receiving FMT vs 3 of 40 (8%) patients receiving placebo (p = 0.02)
76



77
78 CDI Single Infusion Symptom reversal is rapid Will work in majority of patients Success: no symptoms, negative stool IBD Multiple Infusions Symptom reversal is slower and may be transient Will work in a subset of patients Success: no symptoms, normal histology
79 Ongoing Studies at BWH: Post Op Crohn s PSC Obesity
80 Patient Perspecitves


81 Patient willingness to undergo FMT Participant s self-reported disease severity and willingness to undergo FMT Adapted from C.Kelly DDW 2015 Kahn S. Inflamm Bowel Dis 2013

82 What about the patients?






83

84
85 Caution The gut microbiome contains a highly complex and dense community of microbes that include bacteria, fungi and viruses, many of which have not been fully characterized. It is a dynamic and living consortium that can change over time in ways that scientists cannot currently fully predict.
86 Safety and Ethical Concerns Acute Concerns: bacterial, viral, parasitic infections acute allergic reactions Long-term concerns is it possible that we are predisposing the recipient to the diseases the donor will develop in his/her lifetime? Animal models suggests the microbiome may play a role in the pathogenesis of several human diseases. Metabolic syndrome Heart disease Behavior
87 Conclusions FMT is an effective therapy for recurrent CDI infections in patients with and without IBD It is a therapy that shows promise for the treatment of IBD Patients and clinicians are eager for alternative therapies Safety Profile is good and risk of flares is low Long term consequences remain unclear


88 Zain Kassam MD, MPH Mark Smith, PhD Majdi Osman, MD, MPH Elaine Vo, PhD Nancy Dubois, MSN, MBA James Burgess Dan Blackler Gina Mendolia Carolyn Edelstein, MPA Kelly Ling Andrew Noh Laura Burns Deberly Kauffman Daniel Martin Karl Yoder, MPP Kelsey O Brien, MPH Clinical Advisory Board Dr. Colleen Kelly Dr. Ciaran Kelly Dr. Paul Moayyedi Dr. Anne Hayes Dr. Richard Hunt Dr. Daniel Murphy Dr. Monika Fischer Dr. Kanchana Amaratunga Dr. Paul Beck Dr. Tim O Shea Dr. Neil Stollman Dr. Michael Edmonds Joshua Korzenik, MD Walter Chan, MD, MPH Madeline Carrellas Margaret Storm Jessica Sitko Lyn Bry, MD, MPH Georg Gerber MD, MPH, PhD Eric Alm, PhD Clary Clish, PhD Thank You
C. difficile: When to Do Fecal Microbiota Transplant (FMT)
") C. difficile: When to Do Fecal Microbiota Transplant (FMT) Lawrence J. Brandt, MD, MACG Emeritus Chief, Gastroenterology Montefiore Medical Center Professor of Medicine and Surgery Albert Einstein College
C. difficile: When to Do Fecal Microbiota Transplant (FMT) Lawrence J. Brandt, MD, MACG Emeritus Chief, Gastroenterology Montefiore Medical Center Professor of Medicine and Surgery Albert Einstein College
All POOPed out: fecal microbiota transplant in C. difficile
 All POOPed out: fecal microbiota transplant in C. difficile SUSAN M. KELLIE, MD, MPH PROFESSOR OF INTERNAL MEDICINE DIVISION OF INFECTIOUS DISEASES UNIVERSITY OF NEW MEXICO SCHOOL OF MEDICINE HOSPITAL
All POOPed out: fecal microbiota transplant in C. difficile SUSAN M. KELLIE, MD, MPH PROFESSOR OF INTERNAL MEDICINE DIVISION OF INFECTIOUS DISEASES UNIVERSITY OF NEW MEXICO SCHOOL OF MEDICINE HOSPITAL
Star Articles in Review
 Star Articles in Review CDDW/CASL Meeting Toronto, February 10, 2014 Christina M. Surawicz, MD MACG Professor of Medicine Division of Gastroenterology Department of Medicine University of Washington Disclosure
Star Articles in Review CDDW/CASL Meeting Toronto, February 10, 2014 Christina M. Surawicz, MD MACG Professor of Medicine Division of Gastroenterology Department of Medicine University of Washington Disclosure
Corporate Medical Policy Fecal Microbiota Transplantation
 Corporate Medical Policy Fecal Microbiota Transplantation File Name: Origination: Last CAP Review: Next CAP Review: Last Review: Fecal_microbiota_transplantation 7/2014 11/2017 11/2018 11/2017 Description
Corporate Medical Policy Fecal Microbiota Transplantation File Name: Origination: Last CAP Review: Next CAP Review: Last Review: Fecal_microbiota_transplantation 7/2014 11/2017 11/2018 11/2017 Description
Clinical Review Criteria Fecal Microbial Transplant for Treatment of C. Difficile Infection Fecal GI Infusion Fecal Capsule (G3 OpenBiome)
") Clinical Review Criteria Fecal Microbial Transplant for Treatment of C. Difficile Infection Fecal GI Infusion Fecal Capsule (G3 OpenBiome) Criteria Codes Revision History Kaiser Foundation Health Plan
Clinical Review Criteria Fecal Microbial Transplant for Treatment of C. Difficile Infection Fecal GI Infusion Fecal Capsule (G3 OpenBiome) Criteria Codes Revision History Kaiser Foundation Health Plan
Division of GIM Lecture Series Case Presentation David A. Erickson, M.D October 9th, 2013
 Division of GIM Lecture Series Case Presentation David A. Erickson, M.D October 9th, 2013 Financial Disclosures No financial disclosures Objectives Review a case of recurrent Clostridium difficile infection
Division of GIM Lecture Series Case Presentation David A. Erickson, M.D October 9th, 2013 Financial Disclosures No financial disclosures Objectives Review a case of recurrent Clostridium difficile infection
When To Do Fecal Microbiota Transplant (FMT) For C. difficile
 For C. difficile") When To Do Fecal Microbiota Transplant (FMT) For C. difficile Lawrence J. Brandt, MD, MACG Emeritus Chief, Gastroenterology Montefiore Medical Center Professor of Medicine and Surgery Albert Einstein College
When To Do Fecal Microbiota Transplant (FMT) For C. difficile Lawrence J. Brandt, MD, MACG Emeritus Chief, Gastroenterology Montefiore Medical Center Professor of Medicine and Surgery Albert Einstein College
Fecal Microbiota Transplantation
 Protocol Fecal Microbiota Transplantation (20192) Medical Benefit Effective Date: 10/01/14 Next Review Date: 07/18 Preauthorization Yes Review Dates: 07/14, 07/15, 07/16, 07/17 Preauthorization is required.
Protocol Fecal Microbiota Transplantation (20192) Medical Benefit Effective Date: 10/01/14 Next Review Date: 07/18 Preauthorization Yes Review Dates: 07/14, 07/15, 07/16, 07/17 Preauthorization is required.
Fecal Microbiota Transplantation. Description
 Section: Medicine Effective Date: April 15, 2017 Original Policy Date: September 12, 2014 Subject: Fecal Microbiota Transplantation Page: 1 of 10 Last Review Status/Date: March 2017 Fecal Microbiota Transplantation
Section: Medicine Effective Date: April 15, 2017 Original Policy Date: September 12, 2014 Subject: Fecal Microbiota Transplantation Page: 1 of 10 Last Review Status/Date: March 2017 Fecal Microbiota Transplantation
Microbiome GI Disorders
 Microbiome GI Disorders Prof. Ram Dickman Neurogastroenterology Unit Rabin Medical Center Israel 1 Key Points Our gut microbiota Were to find them? Symbiosis or Why do we need them? Dysbiosis or when things
Microbiome GI Disorders Prof. Ram Dickman Neurogastroenterology Unit Rabin Medical Center Israel 1 Key Points Our gut microbiota Were to find them? Symbiosis or Why do we need them? Dysbiosis or when things
10/4/2014. The Microbiome vs. the Gastroenterologist. Human Microbiome. Microbiome and Host Physiology: A Delicate Balance
 The Microbiome vs. the Gastroenterologist John K. Marshall MD MSc FRCPC AGAF Division of Gastroenterology McMaster University Human Microbiome Mouth Finlay BB. Scientific American 2010;302:56-63 Microbiome
The Microbiome vs. the Gastroenterologist John K. Marshall MD MSc FRCPC AGAF Division of Gastroenterology McMaster University Human Microbiome Mouth Finlay BB. Scientific American 2010;302:56-63 Microbiome
Fecal Microbiota Transplantation (FMT): Current Concepts in Clostridium difficile and beyond
: Current Concepts in Clostridium difficile and beyond") Fecal Microbiota Transplantation (FMT): Current Concepts in Clostridium difficile and beyond Amir Patel, MD Assistant Professor of Medicine Froedtert Hospital and the Medical College of Wisconsin I have
Fecal Microbiota Transplantation (FMT): Current Concepts in Clostridium difficile and beyond Amir Patel, MD Assistant Professor of Medicine Froedtert Hospital and the Medical College of Wisconsin I have
Patient presentation
 Update: Clostridium difficile Colitis David H. Kerman, MD Assistant Professor of Clinical Medicine Director, Fellowship Program Division of Gastroenterology University of Miami Miller School of Medicine
Update: Clostridium difficile Colitis David H. Kerman, MD Assistant Professor of Clinical Medicine Director, Fellowship Program Division of Gastroenterology University of Miami Miller School of Medicine
Fecal microbiota transplantation: The When,the How and the Don t. By Dr Rola Hussein
 Fecal microbiota transplantation: The When,the How and the Don t By Dr Rola Hussein Introduction Fecal microbiota transplantation (FMT) involves administration of fecal material containing distal gut microbiota
Fecal microbiota transplantation: The When,the How and the Don t By Dr Rola Hussein Introduction Fecal microbiota transplantation (FMT) involves administration of fecal material containing distal gut microbiota
Title: Fecal microbiota transplantation in recurrent Clostridium difficile infection in a patient with concomitant inflammatory bowel disease
 Title: Fecal microbiota transplantation in recurrent Clostridium difficile infection in a patient with concomitant inflammatory bowel disease Authors: Marta Gravito-Soares, Elisa Gravito-Soares, Francisco
Title: Fecal microbiota transplantation in recurrent Clostridium difficile infection in a patient with concomitant inflammatory bowel disease Authors: Marta Gravito-Soares, Elisa Gravito-Soares, Francisco
Treatment Update on Fecal Microbiota Transplantation. Arnab Ray, MD Ochsner Clinic Foundation Gastroenterology Department
 Treatment Update on Fecal Microbiota Transplantation Arnab Ray, MD Ochsner Clinic Foundation Gastroenterology Department Disclosure I serve as a paid medical monitor for Rebiotix Objectives The scope of
Treatment Update on Fecal Microbiota Transplantation Arnab Ray, MD Ochsner Clinic Foundation Gastroenterology Department Disclosure I serve as a paid medical monitor for Rebiotix Objectives The scope of
Faecal Microbiota Transplants: The evidence and experience
 Faecal Microbiota Transplants: The evidence and experience Dr Simon Goldenberg Consultant Microbiologist and Infection Control Doctor Guy s & St Thomas NHS Foundation Trust Gut microbiota and health Level
Faecal Microbiota Transplants: The evidence and experience Dr Simon Goldenberg Consultant Microbiologist and Infection Control Doctor Guy s & St Thomas NHS Foundation Trust Gut microbiota and health Level
Fecal Microbiota Transplantation
 Fecal Microbiota Transplantation Policy Number: 2.01.92 Last Review: 7/2018 Origination: 5/2015 Next Review: 7/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for
Fecal Microbiota Transplantation Policy Number: 2.01.92 Last Review: 7/2018 Origination: 5/2015 Next Review: 7/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for
Clostridium difficile Infection (CDI) Management Guideline
 Management Guideline") Clostridium difficile Infection (CDI) Management Guideline Do not test all patients with loose or watery stools for CDI o CDI is responsible for
Clostridium difficile Infection (CDI) Management Guideline Do not test all patients with loose or watery stools for CDI o CDI is responsible for
Fecal microbiota transplantation: Breaking the chain of recurrent C. difficile infection
 Fecal microbiota transplantation: Breaking the chain of recurrent C. difficile infection Issue Date: June 2013 Vol. 8 No. 6 Author: Amy Marinski, MSN, RN, CCRN, CNL More than 3 million new cases of Clostridium
Fecal microbiota transplantation: Breaking the chain of recurrent C. difficile infection Issue Date: June 2013 Vol. 8 No. 6 Author: Amy Marinski, MSN, RN, CCRN, CNL More than 3 million new cases of Clostridium
Clinical Policy Bulletin: Fecal Bacteriotherapy
 Clinical Policy Bulletin: Fecal Bacteriotherapy Number: 0844 Policy Aetna considers fecal bacteriotherapy medically necessary for persons with Clostridium difficile infection, with infection confirmed
Clinical Policy Bulletin: Fecal Bacteriotherapy Number: 0844 Policy Aetna considers fecal bacteriotherapy medically necessary for persons with Clostridium difficile infection, with infection confirmed
Managing Clostridium Difficile: An Old Bug With
 932 The Red Section see related editorial on page x Managing Clostridium Difficile: An Old Bug With New Tricks Stephen M. Vindigni, MD, MPH 1,2 and Christina M. Surawicz, MD 1 Am J Gastroenterol (2018)
932 The Red Section see related editorial on page x Managing Clostridium Difficile: An Old Bug With New Tricks Stephen M. Vindigni, MD, MPH 1,2 and Christina M. Surawicz, MD 1 Am J Gastroenterol (2018)
(No Image Selected) Video Submission Confirmation: No Video Upload: Abstract Author: Investigator Commercial Products or Services: No Designed Study:
 Video Submission Confirmation: No Video Upload: Abstract Author: Investigator Commercial Products or Services: No Designed Study:") Found 3 Abstracts CONTROL ID: 1745628 TITLE: Fecal Microbiota Transplantation (FMT) for Treatment of Clostridium difficile Infection (CDI) in Immunocompromised Patients CONTACT (NAME ONLY): Colleen Kelly
Found 3 Abstracts CONTROL ID: 1745628 TITLE: Fecal Microbiota Transplantation (FMT) for Treatment of Clostridium difficile Infection (CDI) in Immunocompromised Patients CONTACT (NAME ONLY): Colleen Kelly
FECAL TRANSPLANTATION
 FECAL TRANSPLANTATION From Theory to Practice in Ridge Meadows Edward Auersperg 13 January 2016 The Human Genome How many different chromosomes do humans have? 46 chromosomes 23 pairs The Human Genome
FECAL TRANSPLANTATION From Theory to Practice in Ridge Meadows Edward Auersperg 13 January 2016 The Human Genome How many different chromosomes do humans have? 46 chromosomes 23 pairs The Human Genome
Fecal transplantation as a treatment option for recurrent Clostridium difficile infection
 Fecal transplantation as a treatment option for recurrent Clostridium difficile infection Josbert Keller Department of Gastroenterology Haga Teaching Hospital, The Hague Case: 81 yrs, CVA, recurrent UTI,
Fecal transplantation as a treatment option for recurrent Clostridium difficile infection Josbert Keller Department of Gastroenterology Haga Teaching Hospital, The Hague Case: 81 yrs, CVA, recurrent UTI,
Patient Safety Summit 2014
 Patient Safety Summit 2014 The War on C Diff Mark Mellow, MD + C Diff The Organism Gram + bacillus Anaerobic Spore forming Intestinal flora (up to 35% hospitalized patients, 3% of healthy adults) Leading
Patient Safety Summit 2014 The War on C Diff Mark Mellow, MD + C Diff The Organism Gram + bacillus Anaerobic Spore forming Intestinal flora (up to 35% hospitalized patients, 3% of healthy adults) Leading
Clostridium Difficile Infection: Applying New Treatment Guidelines and Strategies to Reduce Recurrence Rate
 Clostridium Difficile Infection: Applying New Treatment Guidelines and Strategies to Reduce Recurrence Rate Objectives Summarize the changing epidemiology and demographics of patients at risk for Clostridium
Clostridium Difficile Infection: Applying New Treatment Guidelines and Strategies to Reduce Recurrence Rate Objectives Summarize the changing epidemiology and demographics of patients at risk for Clostridium
Updates in Fecal Microbial Transplant
 Updates in Fecal Microbial Transplant Dina Kao, MD FRCPC Associate Professor, Gastroenterology University of Alberta Nikhil Pai, MD FAAP FRCPC Assistant Professor, Ped Gastroenterology McMaster University
Updates in Fecal Microbial Transplant Dina Kao, MD FRCPC Associate Professor, Gastroenterology University of Alberta Nikhil Pai, MD FAAP FRCPC Assistant Professor, Ped Gastroenterology McMaster University
Modern approach to Clostridium Difficile Infection
 Modern approach to Clostridium Difficile Infection Pseudomembranous Colitis: Principles for diagnosis and treatment Aggelos Stefos Internist, Infectious diseases Specialist Department of Medicine and Research
Modern approach to Clostridium Difficile Infection Pseudomembranous Colitis: Principles for diagnosis and treatment Aggelos Stefos Internist, Infectious diseases Specialist Department of Medicine and Research
OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA
 OMED 17 OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA 29.5 Category 1-A CME credits anticipated ACOFP / AOA s 122 nd Annual Osteopathic Medical Conference & Exposition Joint Session with ACOFP and Cleveland
OMED 17 OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA 29.5 Category 1-A CME credits anticipated ACOFP / AOA s 122 nd Annual Osteopathic Medical Conference & Exposition Joint Session with ACOFP and Cleveland
more intense treatments are needed to get rid of the infection.
 What Is Clostridium Difficile (C. Diff)? Clostridium difficile, or C. diff for short, is an infection from a bacterium that can grow in your intestines and cause bad GI symptoms. The main risk of getting
What Is Clostridium Difficile (C. Diff)? Clostridium difficile, or C. diff for short, is an infection from a bacterium that can grow in your intestines and cause bad GI symptoms. The main risk of getting
CLINICAL MEDICAL POLICY
 Policy Name: Policy Number: Responsible Department(s): CLINICAL MEDICAL POLICY Fecal Microbiota Transplant MP-066-MD-DE Medical Management Provider Notice Date: 10/15/2018; 04/15/2018 Issue Date: 11/15/2018;
Policy Name: Policy Number: Responsible Department(s): CLINICAL MEDICAL POLICY Fecal Microbiota Transplant MP-066-MD-DE Medical Management Provider Notice Date: 10/15/2018; 04/15/2018 Issue Date: 11/15/2018;
Duodenal infusion of donor feces for recurrent Clostridium difficile infection A French experience
 Duodenal infusion of donor feces for recurrent Clostridium difficile infection A French experience Benoit Guery Unité des Maladies Infectieuses CHRU - Faculté de Médecine Lille Conflicts of interest Conferences,
Duodenal infusion of donor feces for recurrent Clostridium difficile infection A French experience Benoit Guery Unité des Maladies Infectieuses CHRU - Faculté de Médecine Lille Conflicts of interest Conferences,
ENGLISH FOR PROFESSIONAL PURPOSES UNIT 3 HOW TO DEAL WITH CLOSTRIDIUM DIFFICILE
 ENGLISH FOR PROFESSIONAL PURPOSES UNIT 3 HOW TO DEAL WITH CLOSTRIDIUM DIFFICILE The diagnosis of CDI should be based on a combination of clinical and laboratory findings. A case definition for the usual
ENGLISH FOR PROFESSIONAL PURPOSES UNIT 3 HOW TO DEAL WITH CLOSTRIDIUM DIFFICILE The diagnosis of CDI should be based on a combination of clinical and laboratory findings. A case definition for the usual
Case 1. Which of the following would be next appropriate investigation/s regarding the pts diarrhoea?
 Case 1 21 yr old HIV +ve, Cd4-100 HAART naïve Profuse diarrhoea for 3/52. Stool MC&S ve Which of the following would be next appropriate investigation/s regarding the pts diarrhoea? Repeat stool MC&S Stool
Case 1 21 yr old HIV +ve, Cd4-100 HAART naïve Profuse diarrhoea for 3/52. Stool MC&S ve Which of the following would be next appropriate investigation/s regarding the pts diarrhoea? Repeat stool MC&S Stool
Gut Microbiota Transplant Pro Position. Christina Surawicz, MD, MACG Professor of Medicine University of Washington Seattle WA
 Gut Microbiota Transplant Pro Position Christina Surawicz, MD, MACG Professor of Medicine University of Washington Seattle WA My Focus Recurrent Clostridium difficile infection No uniformly successful
Gut Microbiota Transplant Pro Position Christina Surawicz, MD, MACG Professor of Medicine University of Washington Seattle WA My Focus Recurrent Clostridium difficile infection No uniformly successful
CLINICAL MEDICAL POLICY
 Policy Name: Policy Number: Responsible Department(s): CLINICAL MEDICAL POLICY Fecal Microbiota Transplant MP-066-MD-PA Medical Management Provider Notice Date: 10/15/2018; 01/15/2018 Issue Date: 11/15/2018;
Policy Name: Policy Number: Responsible Department(s): CLINICAL MEDICAL POLICY Fecal Microbiota Transplant MP-066-MD-PA Medical Management Provider Notice Date: 10/15/2018; 01/15/2018 Issue Date: 11/15/2018;
MEDICAL POLICY SUBJECT: FECAL BACTERIOTHERAPY EFFECTIVE DATE: 08/16/12 REVISED DATE: 08/15/13, 07/17/14, 07/16/15, 06/16/16, 06/15/17
 MEDICAL POLICY SUBJECT: FECAL BACTERIOTHERAPY PAGE: 1 OF: 7 If a product excludes coverage for a service, it is not covered, and medical policy criteria do not apply. If a commercial product, including
MEDICAL POLICY SUBJECT: FECAL BACTERIOTHERAPY PAGE: 1 OF: 7 If a product excludes coverage for a service, it is not covered, and medical policy criteria do not apply. If a commercial product, including
Clostridium difficile Infection: Diagnosis and Management
 Clostridium difficile Infection: Diagnosis and Management Brian Viviano D.O. Case study 42 year old female with history of essential hypertension and COPD presents to ED complaining of 24 hours of intractable,
Clostridium difficile Infection: Diagnosis and Management Brian Viviano D.O. Case study 42 year old female with history of essential hypertension and COPD presents to ED complaining of 24 hours of intractable,
Update on Clostridium difficile infection.
 Update on Clostridium difficile infection. K. Honein Gastroenterologist, HDF Associate Professor Head of Medicine Department St Joseph University-Beirut. Introduction Gram+anaerobic bacillus responsible
Update on Clostridium difficile infection. K. Honein Gastroenterologist, HDF Associate Professor Head of Medicine Department St Joseph University-Beirut. Introduction Gram+anaerobic bacillus responsible
The good, the bad and the ugly. Our microbiome and it s effect on health and disease.
 The good, the bad and the ugly Our microbiome and it s effect on health and disease. Objectives Discuss C difficile infection including treatment options Explain process of Fecal MicrobiotaTransplantation
The good, the bad and the ugly Our microbiome and it s effect on health and disease. Objectives Discuss C difficile infection including treatment options Explain process of Fecal MicrobiotaTransplantation
9/18/2018. Clostridium Difficile: Updates on Diagnosis and Treatment. Clostridium difficile Infection (CDI) Clostridium difficile Infection (CDI)
 Clostridium difficile Infection (CDI)") Clostridium Difficile: Updates on Diagnosis and Treatment Elizabeth Hudson, DO, MPH 9/25/18 Antibiotic-associated diarrhea and colitis were well established soon after widespread use of antibiotics In
Clostridium Difficile: Updates on Diagnosis and Treatment Elizabeth Hudson, DO, MPH 9/25/18 Antibiotic-associated diarrhea and colitis were well established soon after widespread use of antibiotics In
Encapsulated oral FMT for recurrent C. difficile Infection
 Encapsulated oral FMT for recurrent C. difficile Infection Elizabeth L. Hohmann MD Infectious Disease Division Massachusetts General Hospital Harvard Medical School Boston MA DISCLOSURE Clinical Investigator
Encapsulated oral FMT for recurrent C. difficile Infection Elizabeth L. Hohmann MD Infectious Disease Division Massachusetts General Hospital Harvard Medical School Boston MA DISCLOSURE Clinical Investigator
Stony Brook Adult Clostridium difficile Management Guidelines. Discontinue all unnecessary antibiotics
 Stony Brook Adult Clostridium difficile Management Guidelines Summary: Use of the C Diff Infection (CDI) PowerPlan (Adult) Required Patient with clinical findings suggestive of Clostridium difficile infection
Stony Brook Adult Clostridium difficile Management Guidelines Summary: Use of the C Diff Infection (CDI) PowerPlan (Adult) Required Patient with clinical findings suggestive of Clostridium difficile infection
Objectives RECENT ADVANCES IN FECAL MICROBIOTA TRANSFORMATION. TRANSPLANT in Inflammatory Bowel Disease
 RECENT ADVANCES IN FECAL MICROBIOTA TRANSFORMATION TRANSPLANT in Inflammatory Bowel Disease David Suskind M.D. Professor of Pediatrics Division of Gastroenterology University of Washington Seattle Children
RECENT ADVANCES IN FECAL MICROBIOTA TRANSFORMATION TRANSPLANT in Inflammatory Bowel Disease David Suskind M.D. Professor of Pediatrics Division of Gastroenterology University of Washington Seattle Children
CLOSTRIDIUM DIFICILE. Negin N Blattman Infectious Diseases Phoenix VA Healthcare System
 CLOSTRIDIUM DIFICILE Negin N Blattman Infectious Diseases Phoenix VA Healthcare System ANTIBIOTIC ASSOCIATED DIARRHEA 1978: C diff first identified 1989-1992: Four large outbreaks in the US caused by J
CLOSTRIDIUM DIFICILE Negin N Blattman Infectious Diseases Phoenix VA Healthcare System ANTIBIOTIC ASSOCIATED DIARRHEA 1978: C diff first identified 1989-1992: Four large outbreaks in the US caused by J
The Netherlands Donor Feces Bank a. it takes stool to get better
 The Netherlands Donor Feces Bank a it takes stool to get better H.W. Verspaget Dept. of Biobanking and Dept. of Gastroenterology Leiden University Medical Center The Netherlands Fecal MicrobiotaTransplantation
The Netherlands Donor Feces Bank a it takes stool to get better H.W. Verspaget Dept. of Biobanking and Dept. of Gastroenterology Leiden University Medical Center The Netherlands Fecal MicrobiotaTransplantation
Clinically proven to quickly relieve symptoms of common gastrointestinal disorders. TERRAGASTRO - Good health starts in the gut
 Clinically proven to quickly relieve symptoms of common gastrointestinal disorders GASTROINTESTINAL DISEASE Referred to as gastrointestinal diseases, they are common disorders which affect the esophagus,
Clinically proven to quickly relieve symptoms of common gastrointestinal disorders GASTROINTESTINAL DISEASE Referred to as gastrointestinal diseases, they are common disorders which affect the esophagus,
Microbiome in You: Optimizing Gut Bacteria for Better IBD Management
 Microbiome in You: Optimizing Gut Bacteria for Better IBD Management KT Park, M.D., M.S. Assistant Professor Co-Director, Stanford Children s Inflammatory Bowel Disease Center Stanford University School
Microbiome in You: Optimizing Gut Bacteria for Better IBD Management KT Park, M.D., M.S. Assistant Professor Co-Director, Stanford Children s Inflammatory Bowel Disease Center Stanford University School
BENEFIT APPLICATION BLUE CARD/NATIONAL ACCOUNT ISSUES
 Medical Policy BCBSA Ref. Policy: 2.01.92 Last Review: 11/15/2018 Effective Date: 11/15/2018 Section: Medicine Related Policies 2.04.26 Fecal Analysis in the Diagnosis of Intestinal Dysbiosis DISCLAIMER
Medical Policy BCBSA Ref. Policy: 2.01.92 Last Review: 11/15/2018 Effective Date: 11/15/2018 Section: Medicine Related Policies 2.04.26 Fecal Analysis in the Diagnosis of Intestinal Dysbiosis DISCLAIMER
What s New for Clostridium difficile John Lynch MD MPH Harborview Medical Center University of Washington
 What s New for Clostridium difficile 2013 John Lynch MD MPH Harborview Medical Center University of Washington Pathogenic Mechanisms of Diarrhea Toxins: Preformed: S aureus, C perfringens, B cereus Formed
What s New for Clostridium difficile 2013 John Lynch MD MPH Harborview Medical Center University of Washington Pathogenic Mechanisms of Diarrhea Toxins: Preformed: S aureus, C perfringens, B cereus Formed
The Epidemiology of Clostridium difficile DANIEL SAMAN, DRPH, MPH RESEARCH SCIENTIST ESSENTIA INSTITUTE OF RURAL HEALTH
 The Epidemiology of Clostridium difficile DANIEL SAMAN, DRPH, MPH RESEARCH SCIENTIST ESSENTIA INSTITUTE OF RURAL HEALTH Some history first Clostridium difficile, a spore-forming gram-positive (i.e., thick
The Epidemiology of Clostridium difficile DANIEL SAMAN, DRPH, MPH RESEARCH SCIENTIST ESSENTIA INSTITUTE OF RURAL HEALTH Some history first Clostridium difficile, a spore-forming gram-positive (i.e., thick
DISCLOSURE Relevant relationships with commercial entities Wyeth (received advisory board & speaker honoraria) Potential for conflicts of interest wit
 Potential for conflicts of interest wit") GASTROENTERITIS DISCLOSURE Relevant relationships with commercial entities Wyeth (received advisory board & speaker honoraria) Potential for conflicts of interest within this presentation fidaxomicin (which
GASTROENTERITIS DISCLOSURE Relevant relationships with commercial entities Wyeth (received advisory board & speaker honoraria) Potential for conflicts of interest within this presentation fidaxomicin (which
! Macrolide antibacterial. Fidaxomicin (Dificid ) package labeling. Optimer Pharmaceuticals, Inc. May 2011.
 package labeling. Optimer Pharmaceuticals, Inc. May 2011.") Disclosure! I have no conflicts of interest related to this presentation Nina Naeger Murphy, Pharm.D., BCPS Clinical Pharmacy Specialist Infectious Diseases MetroHealth Medical Center Learning Objectives!
Disclosure! I have no conflicts of interest related to this presentation Nina Naeger Murphy, Pharm.D., BCPS Clinical Pharmacy Specialist Infectious Diseases MetroHealth Medical Center Learning Objectives!
Fecal microbial transplantation
 Version 09/16 Consent Form For Fecal microbial transplantation Fecal transplant is an operation in which liquid produced from a healthy human being (as per a survey questionnaire and blood and feces tests)
Version 09/16 Consent Form For Fecal microbial transplantation Fecal transplant is an operation in which liquid produced from a healthy human being (as per a survey questionnaire and blood and feces tests)
Fecal Microbiota Transplantation in C. diff. colitis Benefits and Limitations
 January 27th 2017, 8th Gastro Foundation Weekend for Fellows; Spier Hotel & Conference Centre, Stellenbosch Fecal Microbiota Transplantation in C. diff. colitis Benefits and Limitations Gerhard Rogler,
January 27th 2017, 8th Gastro Foundation Weekend for Fellows; Spier Hotel & Conference Centre, Stellenbosch Fecal Microbiota Transplantation in C. diff. colitis Benefits and Limitations Gerhard Rogler,
Nicola Petrosillo Istituto Nazionale per le Malattie Infettive Lazzaro Spallanzani, IRCCS Roma. L infezione da C difficile grave o complicata
 Nicola Petrosillo Istituto Nazionale per le Malattie Infettive Lazzaro Spallanzani, IRCCS Roma L infezione da C difficile grave o complicata Bagdasarian N et al. JAMA 2015; 313: 398-408 European Society
Nicola Petrosillo Istituto Nazionale per le Malattie Infettive Lazzaro Spallanzani, IRCCS Roma L infezione da C difficile grave o complicata Bagdasarian N et al. JAMA 2015; 313: 398-408 European Society
Fecal Microbiota Transplantation
 Fecal Microbiota Transplantation CDDW Small Group Session March 5, 2017 (11:50-12:30) Nikhil Pai, MD FAAP FRCPC Assistant Professor, Division of Pediatric GI & Nutrition McMaster Children s Hospital, McMaster
Fecal Microbiota Transplantation CDDW Small Group Session March 5, 2017 (11:50-12:30) Nikhil Pai, MD FAAP FRCPC Assistant Professor, Division of Pediatric GI & Nutrition McMaster Children s Hospital, McMaster
Pennington Feb 19, 2015
 Trust your gut Pennington Feb 19, 2015 Crohn s Disease -an autoimmune disorder that causes inflammation of the intestinal tract along with unpredictable, often incapacitating episodes of abdominal pain
Trust your gut Pennington Feb 19, 2015 Crohn s Disease -an autoimmune disorder that causes inflammation of the intestinal tract along with unpredictable, often incapacitating episodes of abdominal pain
Is FMT the answer? Challenging Cases in CDI. Ted Steiner, M.D. April 1, 2016
 Is FMT the answer? Challenging Cases in CDI Ted Steiner, M.D. April 1, 2016 CONFLICT OF INTEREST DISCLOSURE SLIDE In the past 2 years I have been an employee of: In the past 2 years I have been a consultant
Is FMT the answer? Challenging Cases in CDI Ted Steiner, M.D. April 1, 2016 CONFLICT OF INTEREST DISCLOSURE SLIDE In the past 2 years I have been an employee of: In the past 2 years I have been a consultant
FMT Capsule G3 Clinical Primer
 FMT Capsule G3 Clinical Primer 1 FMT CAPSULE G3 CLINICAL CHECKLIST 5 CLINICAL CONTEXT 5 Formulation 6 Clinical Evidence 8 Dosing and Delivery 10 Material Handling 11 QUALITY ASSURANCE AND SAFETY REPORTING
FMT Capsule G3 Clinical Primer 1 FMT CAPSULE G3 CLINICAL CHECKLIST 5 CLINICAL CONTEXT 5 Formulation 6 Clinical Evidence 8 Dosing and Delivery 10 Material Handling 11 QUALITY ASSURANCE AND SAFETY REPORTING
Original Article YH FANG, J CHEN, JD YU, YY LUO, JG LOU. Key words. Introduction
 HK J Paediatr (new series) 2017;22:199-203 Original Article The Preliminary Investigation of Faecal Microbiota Transplantation for Paediatric Recurrent Chronic Bowel Diseases and Literature Review YH FANG,
HK J Paediatr (new series) 2017;22:199-203 Original Article The Preliminary Investigation of Faecal Microbiota Transplantation for Paediatric Recurrent Chronic Bowel Diseases and Literature Review YH FANG,
-2002: Rectal blood loss, UC? (no definite diagnosis) rectal mesalazine. -June 2008: Recurrence of rectal blood loss and urgency
 rectal mesalazine. -June 2008: Recurrence of rectal blood loss and urgency") SD, male 40 yrs. old. (680718M467.) -2002: Rectal blood loss, UC? (no definite diagnosis) rectal mesalazine -June 2008: Recurrence of rectal blood loss and urgency Total colonoscopy: ulcerative rectitis,
SD, male 40 yrs. old. (680718M467.) -2002: Rectal blood loss, UC? (no definite diagnosis) rectal mesalazine -June 2008: Recurrence of rectal blood loss and urgency Total colonoscopy: ulcerative rectitis,
Labeled Uses: Treatment of Clostiridum Difficile associated diarrhea (CDAD)
") Brand Name: Dificid Generic Name: fidaxomicin Manufacturer 1,2,3,4,5 : Optimer Pharmaceuticals, Inc. Drug Class 1,2,3,4,5 : Macrolide Antibiotic Uses 1,2,3,4,5 : Labeled Uses: Treatment of Clostiridum
Brand Name: Dificid Generic Name: fidaxomicin Manufacturer 1,2,3,4,5 : Optimer Pharmaceuticals, Inc. Drug Class 1,2,3,4,5 : Macrolide Antibiotic Uses 1,2,3,4,5 : Labeled Uses: Treatment of Clostiridum
Updates to pharmacological management in the prevention of recurrent Clostridium difficile
 Updates to pharmacological management in the prevention of recurrent Clostridium difficile Julia Shlensky, PharmD PGY2 Internal Medicine Resident September 12, 2017 2017 MFMER slide-1 Clinical Impact Increasing
Updates to pharmacological management in the prevention of recurrent Clostridium difficile Julia Shlensky, PharmD PGY2 Internal Medicine Resident September 12, 2017 2017 MFMER slide-1 Clinical Impact Increasing
Initial Experience of Faecal Microbiota Transplantation for the Treatment of Clostridium difficile Infection in Hong Kong
 HA Convention 2018 Initial Experience of Faecal Microbiota Transplantation for the Treatment of Clostridium difficile Infection in Hong Kong Rashid NS Lui MBChB (CUHK), MRCP (UK), FHKCP Division of Gastroenterology
HA Convention 2018 Initial Experience of Faecal Microbiota Transplantation for the Treatment of Clostridium difficile Infection in Hong Kong Rashid NS Lui MBChB (CUHK), MRCP (UK), FHKCP Division of Gastroenterology
Clinical Infectious Diseases Advance Access published December 7, 2012
 Clinical Infectious Diseases Advance Access published December 7, 2012 1 Physician Attitudes Towards the Use of Fecal Transplantation for Recurrent Clostridium Difficile Infection in a Large Metropolitan
Clinical Infectious Diseases Advance Access published December 7, 2012 1 Physician Attitudes Towards the Use of Fecal Transplantation for Recurrent Clostridium Difficile Infection in a Large Metropolitan
The Potential For Microbiome Modification In Critical Illness. Deborah Cook
 The Potential For Microbiome Modification In Critical Illness Deborah Cook To review Objectives The microbiome & concepts about its modification during critical illness Interventions Predisposition to
The Potential For Microbiome Modification In Critical Illness Deborah Cook To review Objectives The microbiome & concepts about its modification during critical illness Interventions Predisposition to
Clinical Primer: Position Statement for Fecal Microbiota Transplantation Administration for Recurrent Clostridium difficile Infection
 Clinical Primer: Position Statement for Fecal Microbiota Transplantation Administration for Recurrent Clostridium difficile Infection Zain Kassam MD, MPH, FRCPC Chief Medical Officer, OpenBiome Disclaimer
Clinical Primer: Position Statement for Fecal Microbiota Transplantation Administration for Recurrent Clostridium difficile Infection Zain Kassam MD, MPH, FRCPC Chief Medical Officer, OpenBiome Disclaimer
Responders as percent of overall members in each category: Region: New England 50 (57% of 87 members) 46 (57% of 81 members) 21 (55% of 38 members)
 46 (57% of 81 members) 21 (55% of 38 members)") Infectious Diseases Society of America Emerging Infections Network Report for Query: Recurrent C. difficile Infections (CDI) Overall response rate: 621/1212 (51.2%) physicians responded from 09/26/12 to
Infectious Diseases Society of America Emerging Infections Network Report for Query: Recurrent C. difficile Infections (CDI) Overall response rate: 621/1212 (51.2%) physicians responded from 09/26/12 to
ACP Aaron Fieker, D.O
 ACP 2016 Aaron Fieker, D.O Colorectal cancer (CRC) Update on screening strategies and tools Irritable Bowel Syndrome (IBS) New therapeutic options C-difficile Updates on treating recurrent disease CRC
ACP 2016 Aaron Fieker, D.O Colorectal cancer (CRC) Update on screening strategies and tools Irritable Bowel Syndrome (IBS) New therapeutic options C-difficile Updates on treating recurrent disease CRC
Management of the Hospitalized IBD Patient. Drew DuPont MD
 Management of the Hospitalized IBD Patient Drew DuPont MD Ulcerative Colitis: Indications for Admission Severe ulcerative colitis Frequent loose bloody stools ( 6 per day) Severe cramps Systemic toxicity:
Management of the Hospitalized IBD Patient Drew DuPont MD Ulcerative Colitis: Indications for Admission Severe ulcerative colitis Frequent loose bloody stools ( 6 per day) Severe cramps Systemic toxicity:
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Update on C. difficile: Diagnosis and Therapy Including Fecal Transplant
 Update on C. difficile: Diagnosis and Therapy Including Fecal Transplant Colleen R. Kelly, MD Clinical Assistant Professor of Medicine Brown University Warren Alpert School of Medicine Rhode Island Chapter,
Update on C. difficile: Diagnosis and Therapy Including Fecal Transplant Colleen R. Kelly, MD Clinical Assistant Professor of Medicine Brown University Warren Alpert School of Medicine Rhode Island Chapter,
EDUCATIONAL COMMENTARY CLOSTRIDIUM DIFFICILE UPDATE
 EDUCATIONAL COMMENTARY CLOSTRIDIUM DIFFICILE UPDATE Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits click
EDUCATIONAL COMMENTARY CLOSTRIDIUM DIFFICILE UPDATE Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits click
OpenBiome Quality Metrics
 OpenBiome Quality Metrics Donor Assessment Stool Collection & Production Controls Quality Assurance Purpose This section summarizes the assays and process controls that OpenBiome has developed to ensure
OpenBiome Quality Metrics Donor Assessment Stool Collection & Production Controls Quality Assurance Purpose This section summarizes the assays and process controls that OpenBiome has developed to ensure
Gut bugs and health. Patrick Bateson
 Gut bugs and health Patrick Bateson Characteristic odour of kin group is produced by inherited bacterial flora degrading fats secreted by anal glands An increasing number of people in developed countries
Gut bugs and health Patrick Bateson Characteristic odour of kin group is produced by inherited bacterial flora degrading fats secreted by anal glands An increasing number of people in developed countries
Clostridium Difficile colitismore
 Clostridium Difficile colitismore virulent than ever ECHO- February 18, 2016 Charles Krasner, M.D. UNR School of Medicine Sierra NV Veterans Affairs Hospital Growing problem of pseudomembranous colitis
Clostridium Difficile colitismore virulent than ever ECHO- February 18, 2016 Charles Krasner, M.D. UNR School of Medicine Sierra NV Veterans Affairs Hospital Growing problem of pseudomembranous colitis
Clostridium difficile CRISTINA BAKER, MD, MPH INFECTIOUS DISEASE PARK NICOLLET/HEALTH PARTNERS 11/9/2018
 Clostridium difficile CRISTINA BAKER, MD, MPH INFECTIOUS DISEASE PARK NICOLLET/HEALTH PARTNERS 11/9/2018 Disclosures None Objectives Highlight important changes in the management of Clostridium difficile
Clostridium difficile CRISTINA BAKER, MD, MPH INFECTIOUS DISEASE PARK NICOLLET/HEALTH PARTNERS 11/9/2018 Disclosures None Objectives Highlight important changes in the management of Clostridium difficile
Fecal Microbiota Transplantation for Severe sepsis and Diarrhea : a Case Report
 Fecal Microbiota Transplantation for Severe sepsis and Diarrhea : a Case Report Qiurong Li Institute of General Surgery, Jinling Hospital Nanjing Univeristy Gut Microbiota 100 trillion cells 10-fold of
Fecal Microbiota Transplantation for Severe sepsis and Diarrhea : a Case Report Qiurong Li Institute of General Surgery, Jinling Hospital Nanjing Univeristy Gut Microbiota 100 trillion cells 10-fold of
Long-Term Care Updates
 Long-Term Care Updates April 2018 By Austin Smith, PharmD Candidate and Lindsay Slowiczek, PharmD is the most common healthcare-acquired infection (HAI) in the United States. 1,2 A 2014 prevalence survey
Long-Term Care Updates April 2018 By Austin Smith, PharmD Candidate and Lindsay Slowiczek, PharmD is the most common healthcare-acquired infection (HAI) in the United States. 1,2 A 2014 prevalence survey
Clostridium Difficile Associated Disease. Edmund Krasinski, Jr., D.O., F.A.C.G. Southwest Conference on Medicine 2011
 Clostridium Difficile Associated Disease Edmund Krasinski, Jr., D.O., F.A.C.G. Southwest Conference on Medicine 2011 Introduction Which of the following is more common in community hospitals in the Southeast
Clostridium Difficile Associated Disease Edmund Krasinski, Jr., D.O., F.A.C.G. Southwest Conference on Medicine 2011 Introduction Which of the following is more common in community hospitals in the Southeast
Treating and Preventing. C. difficile Infections A Review of the Research for Adults
 Treating and Preventing C. difficile Infections A Review of the Research for Adults e Is This Information Right for Me? This information is right for you if: Your health care professional has said that
Treating and Preventing C. difficile Infections A Review of the Research for Adults e Is This Information Right for Me? This information is right for you if: Your health care professional has said that
ACG Clinical Guideline: Diagnosis, Treatment, and Prevention of Clostridium difficile Infections
 ACG Clinical Guideline: Diagnosis, Treatment, and Prevention of Clostridium difficile Infections Christina M. Surawicz, MD 1, Lawrence J. Brandt, MD 2, David G. Binion, MD 3, Ashwin N. Ananthakrishnan,
ACG Clinical Guideline: Diagnosis, Treatment, and Prevention of Clostridium difficile Infections Christina M. Surawicz, MD 1, Lawrence J. Brandt, MD 2, David G. Binion, MD 3, Ashwin N. Ananthakrishnan,
Understanding probiotics and health
 Understanding probiotics and health Gemma Laws MSc Student Microbiology and Immunology Department The gut microbiota The name given to the total microbial population living in our intestine Bacteria, fungi,
Understanding probiotics and health Gemma Laws MSc Student Microbiology and Immunology Department The gut microbiota The name given to the total microbial population living in our intestine Bacteria, fungi,
What Are Probiotics? PROBIOTICS
 PROBIOTICS What Are Probiotics? Probiotics are living, microscopic (very small) organisms that can help your gut health. Most often, probiotics are bacteria, but they may also be other organisms, such
PROBIOTICS What Are Probiotics? Probiotics are living, microscopic (very small) organisms that can help your gut health. Most often, probiotics are bacteria, but they may also be other organisms, such
Gut Microbiome Essentials
 CORE COMPONENTS I: Gut Microbiome Essentials 2016 Tom Fabian, PhD Module Outline 1. Microbiome overview: getting a sense of the microbiome, research, what we know 2. Bacteria: features, functions, communities
CORE COMPONENTS I: Gut Microbiome Essentials 2016 Tom Fabian, PhD Module Outline 1. Microbiome overview: getting a sense of the microbiome, research, what we know 2. Bacteria: features, functions, communities
2/3/2011. Adhesion of Bifidobacterium lactis HN019 to human intestinal
 PROBIOTICS LEARNING THE WHY AND WHEN PROBIOTICS DEFINITION live micro-organisms organisms that are beneficial to the host organism WHO: Live organisms which, when administered in adequate amounts, confer
PROBIOTICS LEARNING THE WHY AND WHEN PROBIOTICS DEFINITION live micro-organisms organisms that are beneficial to the host organism WHO: Live organisms which, when administered in adequate amounts, confer
Probiotics for Primary Prevention of Clostridium difficile Infection
 Probiotics for Primary Prevention of Clostridium difficile Infection Objectives Review risk factors for Clostridium difficile infection (CDI) Describe guideline recommendations for CDI prevention Discuss
Probiotics for Primary Prevention of Clostridium difficile Infection Objectives Review risk factors for Clostridium difficile infection (CDI) Describe guideline recommendations for CDI prevention Discuss
Does Fecal Microbiota Transplantation Cause Clinical Remission in Patients with Ulcerative Colitis?
 Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 12-2017 Does Fecal Microbiota Transplantation
Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 12-2017 Does Fecal Microbiota Transplantation
Updated Clostridium difficile Treatment Guidelines
 Updated Clostridium difficile Treatment Guidelines Arielle Arnold, PharmD, BCPS Clinical Pharmacist Saint Alphonsus Regional Medical Center September 29 th, 2018 Disclosures Nothing to disclose Learning
Updated Clostridium difficile Treatment Guidelines Arielle Arnold, PharmD, BCPS Clinical Pharmacist Saint Alphonsus Regional Medical Center September 29 th, 2018 Disclosures Nothing to disclose Learning
Gut Microbiota and IBD. Vahedi. H M.D Associate Professor of Medicine DDRI
 Gut Microbiota and IBD Vahedi. H M.D Associate Professor of Medicine DDRI 1393.3.1 2 GUT MICROBIOTA 100 Trillion Microbes - 10 times more than cells in our body Collective weight of about 1kg in human
Gut Microbiota and IBD Vahedi. H M.D Associate Professor of Medicine DDRI 1393.3.1 2 GUT MICROBIOTA 100 Trillion Microbes - 10 times more than cells in our body Collective weight of about 1kg in human
SMT19969: A Selective Therapy for C. difficile Infection
 SMT19969: A Selective Therapy for C. difficile Infection One Bug, One Drug 25 th September 2012 SMT19969: A Selective Therapy for CDI SMT19969 is a novel antibiotic for the specific treatment of Clostridium
SMT19969: A Selective Therapy for C. difficile Infection One Bug, One Drug 25 th September 2012 SMT19969: A Selective Therapy for CDI SMT19969 is a novel antibiotic for the specific treatment of Clostridium
Long-Term Care Updates
 Long-Term Care Updates April 2017 Bezlotoxumab to Prevent Recurrent Infection By Amy Wilson, PharmD and Zara Risoldi Cochrane, PharmD, MS, FASCP Introduction The Gram-positive bacteria is a common cause
Long-Term Care Updates April 2017 Bezlotoxumab to Prevent Recurrent Infection By Amy Wilson, PharmD and Zara Risoldi Cochrane, PharmD, MS, FASCP Introduction The Gram-positive bacteria is a common cause
PROBIOTICS: WHO S WHO AND WHAT S WHAT IN THE GUT PROBIOTICS: WHAT ARE THEY, AND HOW DO THEY WORK? Karen Jensen, (Retired ND)
") PROBIOTICS: WHO S WHO AND WHAT S WHAT IN THE GUT Karen Jensen, (Retired ND) Today many people are aware of the benefits of maintaining a healthy gut. As a result, probiotic use is becoming ever more popular.
PROBIOTICS: WHO S WHO AND WHAT S WHAT IN THE GUT Karen Jensen, (Retired ND) Today many people are aware of the benefits of maintaining a healthy gut. As a result, probiotic use is becoming ever more popular.
PEDIATRIC INFLAMMATORY BOWEL DISEASE
 PEDIATRIC INFLAMMATORY BOWEL DISEASE Alexis Rodriguez, MD Pediatric Gastroenterology Advocate Children s Hospital Disclosers Abbott Nutrition - Speaker Inflammatory Bowel Disease Chronic inflammatory disease
PEDIATRIC INFLAMMATORY BOWEL DISEASE Alexis Rodriguez, MD Pediatric Gastroenterology Advocate Children s Hospital Disclosers Abbott Nutrition - Speaker Inflammatory Bowel Disease Chronic inflammatory disease
Clostridium difficile: Can you smell the new updates?
 Clostridium difficile: Can you smell the new updates? Sunish Shah, Pharm.D. PGY-2 Infectious Disease Pharmacy Resident Yale-New Haven Hospital sshah1741@mail.usciences.edu Learning objectives Recognize
Clostridium difficile: Can you smell the new updates? Sunish Shah, Pharm.D. PGY-2 Infectious Disease Pharmacy Resident Yale-New Haven Hospital sshah1741@mail.usciences.edu Learning objectives Recognize
Clostridiodes Difficile Colitis: Update on Guidelines. Jade Le, MD Texas Health Physicians Group No disclosures April 6, 2018
 Clostridiodes Difficile Colitis: Update on Guidelines Jade Le, MD Texas Health Physicians Group No disclosures April 6, 2018 Outline Overview of CDI Diagnosis of C Difficile- updates Infection Prevention
Clostridiodes Difficile Colitis: Update on Guidelines Jade Le, MD Texas Health Physicians Group No disclosures April 6, 2018 Outline Overview of CDI Diagnosis of C Difficile- updates Infection Prevention