Dr. Melvyn Letier Constantiaberg Mediclinic October 2016
|
|
|
- Marion Anderson
- 6 years ago
- Views:
Transcription

1 Dr. Melvyn Letier Constantiaberg Mediclinic October 2016
2 This presentation will enable you to: Understand the pathophysiology of IBS Recognize the clinical manifestations of IBS Make a confident diagnosis of IBS Be better able to treat your patients with IBS
3 IRRITABLE BOWEL SYNDROME The bowels are at one time constipated, at another lax, in the same person How the disease has two such different symptoms I do not profess to explain W Cumming, London Medical Gazette, 1849



4 Recurrent abdominal pain or discomfort for at least 3 days/month in last 3 months, associated with 2 or more of the following: Improved with defaecation Onset associated with change in stool frequency Onset associated with change in stool form Criteria fulfilled for at least 3 months, and symptom onset at least 6 months prior to diagnosis Longstreth GF Gastroent 2006

5


6 The history and physical examination, and where appropriate selected laboratory tests, should exclude alarm symptoms and signs Anaemia Fever Unexplained weight loss Persistent Diarrhoea Severe Constipation Nocturnal symptoms Coeliac disease Rectal bleeding Family history of colorectal cancer or IBD New onset symptoms > 50
7 Not Routinely Recommended May be helpful Recommended FBC, ESR, CRP Coeliac serology in D- IBS, M-IBS s-ttg Colonoscopy in patients with family history of CRC; over 50 years Serum Chemistry Thyroid functions Stool MC+S* Abdominal imaging * H2 Breath testing for lactose intolerance H2 Breath test for small bowel bacterial overgrowth Am J Gastroenterol 2009; 104; S1

8 Enhanced Perception Vagal Nuclei 5-HT Sympathetic Altered Motility Visceral Hypersensitivity Adapted from Camilleri and Choi. Aliment Pharmacol Ther. 1997;11:3.

9
 TCAs exert benefit at lower than antidepressant doses e.g. 10-20mg nocte.")
10 Have analgesic as well as mood improving effects Modes of action of TCAs and SSRIs are: endogenous endorphin release, blockade of noradrenalin reuptake, and blockade of serotonin A meta-analysis showed antidepressants more effective than placebo for pain relief and global symptoms, in a 1-3 month period. (NNT=4) TCAs exert benefit at lower than antidepressant doses e.g mg nocte. Treat initially for 3-4 weeks
11 Post-infectious IBS (PI-IBS)-odds increased six fold after acute gastroenteritis Risk factors for PI-IBS include young age, prolonged fever, anxiety and depression, longer illness duration Causes of PI-IBS thought to include malabsorption, increased lymphocytes and entero-endocrine cells, and antibiotic use
12 Alteration in faecal microflora. Small intestinal bacterial overgrowth: positive H2- breath test, response to antibiotics Food sensitivity/food allergy; carbohydrate malabsorption, gluten sensitivity. FODMAPS (fermentable oligo-, di-, and monosaccharides and polyols) enter distal small bowel and colon and undergo fermentation

13 Abdominal Pain Chronic Variable sites and intensity Triggers include food and stress Nocturnal pain is unusual
14 HMO group (Kaiser Permanente) Surgical predisposition in IBS; misdiagnosis important underlying factor Women undergoing hysterectomy for pain more likely to have IBS Increased multidisciplinary collaboration may improve diagnosis and reduce surgery Longstreth, Yao. Gastroent 2004;126
15 Surgery IBS (%) N=4587 Non IBS(%) N=84421 Cholecyst Appendicec Hysterect Back surg CABG Peptic ulcer
16 Diarrhoea Small-moderate volume loose stools; more frequent Crampy pain, relieved after stool Constipation Hard, pellet-like stools; may have normal or loose stools; less frequent Crampy pain, relieved after stool Sense of incomplete evacuation Sense of incomplete evacuation Mucus in ± 50%

17 Reproduced by kind permission of Dr K W Heaton, Reader in Medicine at the University of Bristol Norgine Ltd.

18 Often worse postprandial Worse as day goes on Increased abdominal girth, without increase in total gas content Mechanism: gas trapping in small intestine

19



20 Family Practice Gastroenterology IBS OTHER IBS OTHER 12% of GP Visits 28% of Gastro Visits
 Increased health care burden and more days off work Medical costs - + $8 billion in USA")
21 Prevalence 4 to 30% (average + 20%) Up to 75% of persons with IBS do not seek medical attention 8 15% of primary care and 20 40% of referrals to gastroenterologists Remains common in the elderly (Often misdiagnosed as symptomatic diverticulosis) Increased health care burden and more days off work Medical costs - + $8 billion in USA annually
22 The North-West University (Potchefstroom) study. The purpose of the study: To investigate the relationship of job burnout and work engagement with self-reported received treatment for health conditions (Cardiovascular condition, High cholesterol, Depression, Diabetes, Hypertension and Irritable bowel syndrome), while controlling for age, gender, smoking and alcohol use. Results: The results showed that job burnout had a positive relationship with self-reported received treatment for Depression, Diabetes, Hypertension and Irritable bowel syndrome. Reference : Leon T. de Beer1*, Jaco Pienaar1 & Sebastiaan Rothmann Jr.2 Published online 10 April 2014 in Wiley Online Library (wileyonlinelibrary.com) DOI: /smi.2576
23 Reference : Leon T. de Beer1*, Jaco Pienaar1 & Sebastiaan Rothmann Jr.2 Published online 10 April 2014 in Wiley Online Library (wileyonlinelibrary.com) DOI: /smi.2576
24 1. Why present now? 2. Establish therapeutic relationship 3. Patient education 4. Dietary modification 5. Physical activity 6. Psychosocial therapy 7. Medication 8. Alternative therapies
25 Change in symptoms e.g. medication, diet Concern about serious illness Stressors Hidden agenda e.g. disability, request for opiates or tranquillizers Psychological co-morbidity

26 Non-judgmental Establish realistic expectations Involve patient in treatment decisions Patients with established, positive physician interactions have fewer IBS related follow-up visits
27 Education helps validate patients illness experience Sets the basis for therapeutic intervention Stress the chronic, benign nature of IBS The diagnosis of IBS (well validated) is robust and unlikely to change over time IBS has no effect on lifespan

28 Take a careful dietary history Consider Lactose intolerance, trial of Lactose-free diet, FODMAP diet Reduced intake of gas forming foods in patients with increased gas Food allergy testing not recommended Gluten restriction in non- Coeliac patients may be of benefit
29 Fermentable oligo-di-monosaccharide and polyols (FODMAPs) enter distal small bowel and colon, fermented, and cause symptoms FODMAPs include Fructans, Galactans, Lactose, Fructose, Sorbitol, Xylitol and Mannitol Several studies on low FODMAPs diet have been shown to be of benefit in patients with IBS A trial of low FODMAPs diet is reasonable, provided nutritional status is monitored Gibson PR APT 2005

30 30
31 Modes of action: increased water holding in stool; gel formation to lubricate stool; bulking of stool; bile salt binding Bulking agents showed no benefit over placebo for reducing IBS global symptoms Hi-fiber foods e.g. All Bran may aggravate bloating Because of safety and placebo effect a trial of therapy is reasonable, especially in C-IBS (<30g/d)
32 Increased physical activity may help with symptoms of IBS In a Scandinavian study of 102 IBS patients, moderate to vigorous exercise 3-5 times per week showed significant benefit over non-exercising. Active Exercise Group Non-active Group Decrease in symptom score Worsening Symptoms % 23% Am J Gastroent 2011
33 Behavioral treatment e.g. Hypnotherapy, Biofeedback, Psychotherapy may be useful They reduce anxiety levels, encourage health promoting behavior, involve patients in treatment and improve pain tolerance A 2009 meta-analysis of 20 studies (n=1278) showed Psychological therapy including Antidepressants to be significantly more effective vs. control or standard of care Ford AC GUT 2009
34 Medication must be considered an ADJUNCT to IBS treatment Drug selection will vary with dominant symptoms Chronic drug use should be minimized: IBS is a lifelong condition; lack of convincing evidence of efficacy High placebo response rate in IBS
35 1. Antispasmodics 2. Antidepressants 3. Anti-diarrhoeal agents 4. Anti-constipation agents 5. Probiotics 6. Alternative therapies

36 IBS Drug Treatment Pain and Bloating IBS Anti-spasmodics Tricyclics SSRIs Constipation Laxatives Prucalopride* Lubiprostone* Linaclotide* Diarrhoea Loperamide 5HT3 Antagonists e.g. Alosetron*
37 Most widely used drugs in IBS Should be used on demand rather than on a regular basis May be useful in patients with post-prandial pain, gas, bloating and faecal urgency Agents available in SA include Mebeverine, Hyoscine, Peppermint oil, Librax Poynard T et al APT 2001
38 More effective than placebo for pain relief and global symptom improvement; NNT=4 Tricyclics effective at lower than antidepressant doses e.g. amitriptyline mg daily. Use with caution in constipated patients. Aim at 3-4 week trial of therapy given delayed onset of action SSRI treatment data less consistent than TCAs Reupert L Cochrane Database 2011
39 Use step-up approach Others Irritant Laxatives Irritant laxatives + Bulking agent Osmotic laxatives; Bulking agents
40 Administration of Bifidobacterium Infantis alleviated IBS symptoms including abdominal pain, bloating and normalized bowel movement. An abnormal IL10/IL12 ratio at baseline was normalized by feeding B. Infantis. B. Infantis changed a pro-inflammatory ratio to an antiinflammatory state i.e. Immune modulating effect A prospective placebo-controlled study found patients with diarrhoea predominant IBS taking Saccharomyces Boulardii, a probiotic yeast, had a significant reduction on the number and improvement in consistency of bowel movements. O Mahoney et al Clin Gastroenterol Hepatol 2005
41 Meta-analysis of 14 probiotic trials: Small improvement in overall IBS symptoms Effects on individual symptoms i.e. bloating, pain, flatulence conflicting evidence No adverse effects Systematic review of 18 trials: Most used combination or Lactobacilli/ Bifidobacteria Statistically significant effect over placebo wrt Global IBS symptoms, pain & flatulence but not bloating ACG guidelines give probiotics a weak recommendation due to lack of long term data Hoveyda et al Gastroenterology 2009; Moayyedi et al Gut 2010
42 Iberogast (German Herbal medication) Rifaximin (Antibiotic not available in S.A) Tranquilizers e.g. Librax Hypnotherapy Acupuncture
43 Recent studies have suggested that Rifaximin, a non-absorbable antibiotic, can be used as an effective treatment for abdominal bloating and flatulence, giving more credibility to the potential role of bacterial overgrowth in some patients with IBS. A double-blind, randomized, placebo-controlled trial compared the multi-herbal extract Iberogast versus placebo in the treatment of all three forms of irritable bowel syndrome. This multi-target phytopharmaceutical was found to be significantly superior to placebo via both an abdominal pain scale (p value = ) and an IBS symptom score (p value = 0.001) after four weeks of treatment. Enteric coated Peppermint oil capsules has been advocated for IBS symptoms in adults and children; however, results from trials have been inconsistent. Peppermint may exacerbate GORD.
44 There is a strong brain-gut component to IBS, and Cognitive therapy may improve symptoms in a proportion of patients in conjunction with Antidepressants. In a randomized controlled trial of referred patients, Cognitive behavioural therapy helped even though patients in this study did not have any psychiatric diagnoses. Gut-directed or gut-specific Hypnotherapy or self-hypnosis is one of the most promising areas of IBS treatment. Current research shows that symptom reduction/elimination from IBS hypnotherapy can last at least five years.

45

46

47

48

49

50

51

52

53

54

55

56

57
58

59

60
61 Pharmaceutical companies Financial potential (High prevalence, Affliction of affluence, Lack of effective therapy) Will these patients ever uniformly benefit from drug treatment? Animal models for functional disorders do not accurately reflect the human condition Recent phase 3 trials fundamentally flawed

62 Only 6/93 trials of IBS intervention found to be scientifically adequate in recent review Great difficulty in defining end-points in clinical trials to reflect beneficial effect on global well-being & IBS symptoms Pressure groups may have +ve or ve impact on decisions by licensing authorities and politicians

63

64 It s not life-threatening, after all, it s not cancer. You need to learn to live with it. Come back and see me if you get a new symptom, but otherwise it s just IBS. Heck I can't even find a doctor to actually diagnose me for IBS. A virus that needs to work its way out? Has this doctor never heard of the Rome 3 criteria? Don t they teach this stuff in Medical school?
65 Aim to make a positive diagnosis with Rome criteria history, examination Beware alarm symptoms: Wt loss, PR bleeding, recent change in bowel habit, etc Basic Ix: stool culture, FBC, U&E, LFT, CRP, TFT, anti ttg Ab, glucose, Ca Refer for further investigation Explanation, reassurance, dietary and lifestyle advice IBS-C IBS-D Pain/Bloating Increase dietary fibre / fluid Bulk forming laxative(s) Consider Citalopram Dietary modification Anti-diarrhoeal agents Consider Amitriptyline Reduced fibre intake Increased fluids Antispasmodics Consider TCA s/citalopram In refractory cases consider Counselling, Hypnotherapy, Biofeedback, role of Probiotics

66 IBS is a chronic medical condition characterized by abdominal pain, diarrhoea or constipation, bloating, passage of mucus and feelings of incomplete evacuation Precise etiology of IBS is unknown and therefore treatment is focused on relieving symptoms rather that curing disease A complex multifactorial disease Huge resource usage Probably grossly over investigated in many cases Targeted drug therapy difficult New therapies but modest results
67 Although many IBS patients complain of symptoms after eating, true food allergies are uncommon Specific therapies are determined by individual patient symptoms Life-style modifications and possible alternative therapies may relieve symptoms
68 Current drug therapy often provides inadequate relief of IBS symptoms, leading many patients to consider CAM therapies (Complementary and Alternative Medicine). Aloe barbadensis Miller Extract (AVH200 ) is a CAM therapy that is well tolerated, safe and has been shown to be a promising treatment option for patients with IBS.


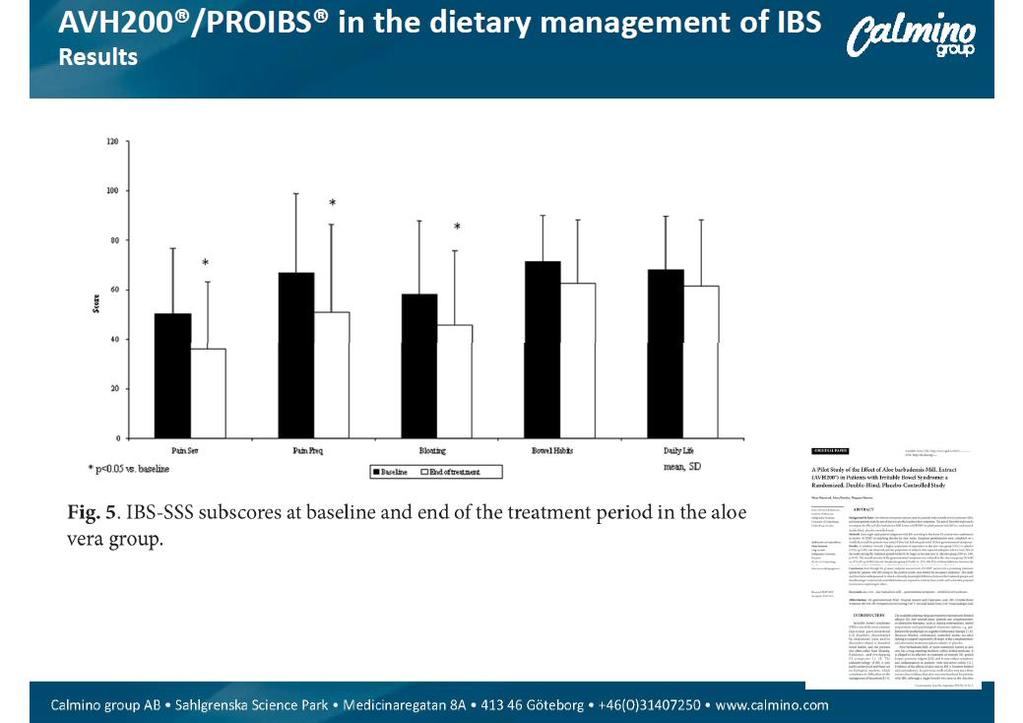
69 PROIBS which contains AVH200 has successfully completed a randomized placebo study at the Sahlgrenska University Hospital in Sweden. The results from the study showed that symptoms in adults with diagnosed IBS improved significantly when the diet was supplemented with AVH200 compared to the placebo. AVH200 was seen to reduce problems of discomfort and perceived feeling of bloating. Thus, PROIBS containing this unique extract is seen as a promising treatment adjunct for the dietary management of IBS.

70
Diagnosis and Management of Irritable Bowel Syndrome (IBS) For the Primary Care Provider
 For the Primary Care Provider") Diagnosis and Management of Irritable Bowel Syndrome (IBS) For the Primary Care Provider Elizabeth Coss, MD General Gastroenterologist Audie Murphy Veterans Hospital UT Health This presentation does not
Diagnosis and Management of Irritable Bowel Syndrome (IBS) For the Primary Care Provider Elizabeth Coss, MD General Gastroenterologist Audie Murphy Veterans Hospital UT Health This presentation does not
Irritable Bowel Syndrome. Mustafa Giaffer March 2017
 Irritable Bowel Syndrome Mustafa Giaffer March 2017 Introduction First described in 1771. 50% of patients present
Irritable Bowel Syndrome Mustafa Giaffer March 2017 Introduction First described in 1771. 50% of patients present
IBS - Definition. Chronic functional disorder of GI generally characterized by:
 IBS - Definition Chronic functional disorder of GI generally characterized by: 3500 3000 No. of Publications 2500 2000 1500 1000 Irritable Bowel syndrome Irritable Bowel Syndrome 500 0 1968-1977 1978-1987
IBS - Definition Chronic functional disorder of GI generally characterized by: 3500 3000 No. of Publications 2500 2000 1500 1000 Irritable Bowel syndrome Irritable Bowel Syndrome 500 0 1968-1977 1978-1987
Inflammatory or Irritable? (the bowel, not the speaker)
") South GP CME Edgar Centre, Dunedin August 2014 Inflammatory or Irritable? (the bowel, not the speaker) Dr Jason Hill MBChB FRACP FRCP Edin Department of Gastroenterology, Southern DHB Dunedin School Of
South GP CME Edgar Centre, Dunedin August 2014 Inflammatory or Irritable? (the bowel, not the speaker) Dr Jason Hill MBChB FRACP FRCP Edin Department of Gastroenterology, Southern DHB Dunedin School Of
Presenter. Irritable Bowel Syndrome. Objectives. Introduction. Rome Criteria. Irritable Bowel Syndrome 2/28/2018
 Presenter Irritable Bowel Syndrome Current evidence for diagnosis & management Julie Daniels DNP, CNM Assistant Professor Course Coordinator of Primary Care of Women Faculty at Frontier Nursing University
Presenter Irritable Bowel Syndrome Current evidence for diagnosis & management Julie Daniels DNP, CNM Assistant Professor Course Coordinator of Primary Care of Women Faculty at Frontier Nursing University
Advancing gastroenterology, improving patient care
 American College of Gastroenterology Advancing gastroenterology, improving patient care Note to Visitors: A fully updated ACG Systematic Review on the Management of Chronic Idiopathic Constipation and
American College of Gastroenterology Advancing gastroenterology, improving patient care Note to Visitors: A fully updated ACG Systematic Review on the Management of Chronic Idiopathic Constipation and
Irritable Bowel Syndrome (IBS)
") Irritable Bowel Syndrome (IBS) Dr Rex J Polson 17 th January 2018 Overview Description of the condition Discussion of symptoms and investigations that may be required Discussion of management and treatment
Irritable Bowel Syndrome (IBS) Dr Rex J Polson 17 th January 2018 Overview Description of the condition Discussion of symptoms and investigations that may be required Discussion of management and treatment
Irritable Bowel Syndrome Now. George M. Logan, MD Friday, May 5, :35 4:05 PM
 Irritable Bowel Syndrome Now George M. Logan, MD Friday, May 5, 2017 3:35 4:05 PM Dr. Logan indicated no potential conflict of interest to this presentation. He does not intend to discuss any unapproved/investigative
Irritable Bowel Syndrome Now George M. Logan, MD Friday, May 5, 2017 3:35 4:05 PM Dr. Logan indicated no potential conflict of interest to this presentation. He does not intend to discuss any unapproved/investigative
Irritable bowel syndrome in adults
 Irritable bowel syndrome in adults NICE provided the content for this booklet which is independent of any company or product advertised Welcome In February 2008, NICE published a clinical guideline on
Irritable bowel syndrome in adults NICE provided the content for this booklet which is independent of any company or product advertised Welcome In February 2008, NICE published a clinical guideline on
IBS Irritable Bowel syndrome Therapeutics II PHCL 430
 Salman Bin AbdulAziz University College Of Pharmacy IBS Irritable Bowel syndrome Therapeutics II PHCL 430 Email:- ahmedadel.pharmd@gmail.com Ahmed A AlAmer PharmD R.S is 32-year-old woman experiences intermittent
Salman Bin AbdulAziz University College Of Pharmacy IBS Irritable Bowel syndrome Therapeutics II PHCL 430 Email:- ahmedadel.pharmd@gmail.com Ahmed A AlAmer PharmD R.S is 32-year-old woman experiences intermittent
4) Irritable Bowel Syndrome - Dr. Shaikhani. Epidemiology. Pathophysiology. Burden. Diagnosis
 Irritable Bowel Syndrome - Dr. Shaikhani. Epidemiology. Pathophysiology. Burden. Diagnosis") 4) Irritable Bowel Syndrome - Dr. Shaikhani Epidemiology A common disorder, with a 7% prevalence. Women are 1.5 times more likely to be affected than men, most commonly between ages 20-40 years. Onset
4) Irritable Bowel Syndrome - Dr. Shaikhani Epidemiology A common disorder, with a 7% prevalence. Women are 1.5 times more likely to be affected than men, most commonly between ages 20-40 years. Onset
Primary Management of Irritable Bowel Syndrome
 Primary Management of Irritable Bowel Syndrome Jasmine Zia, MD Acting Instructor, Division of Gastroenterology Current Concepts in Drug Therapy CME Course April 23, 2015 Irritable Bowel Syndrome (IBS)
Primary Management of Irritable Bowel Syndrome Jasmine Zia, MD Acting Instructor, Division of Gastroenterology Current Concepts in Drug Therapy CME Course April 23, 2015 Irritable Bowel Syndrome (IBS)
The long-term impact of the low-fodmap diet for management of irritable bowel syndrome. Dr Miranda Lomer RD.
 The long-term impact of the low-fodmap diet for management of irritable bowel syndrome Dr Miranda Lomer RD Email: miranda.lomer@kcl.ac.uk What is IBS - ROME IV Criteria A functional bowel disorder in which
The long-term impact of the low-fodmap diet for management of irritable bowel syndrome Dr Miranda Lomer RD Email: miranda.lomer@kcl.ac.uk What is IBS - ROME IV Criteria A functional bowel disorder in which
Is one of the most common chronic disorders. causing patients to seek medical treatment.
 ILOs After this lecture you should be able to : Define IBS Identify causes and risk factors of IBS Determine the appropriate therapeutic options for IBS Is one of the most common chronic disorders causing
ILOs After this lecture you should be able to : Define IBS Identify causes and risk factors of IBS Determine the appropriate therapeutic options for IBS Is one of the most common chronic disorders causing
Clinical guideline Published: 23 February 2008 nice.org.uk/guidance/cg61
 Irritable bowel syndrome in adults: diagnosis and management Clinical guideline Published: 23 February 2008 nice.org.uk/guidance/cg61 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Irritable bowel syndrome in adults: diagnosis and management Clinical guideline Published: 23 February 2008 nice.org.uk/guidance/cg61 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Low FODMAP Dietary Approach For FGD/IBS. Our Experience. Charlotte McCamphill 19 th February 2015
 Low FODMAP Dietary Approach For FGD/IBS Our Experience Charlotte McCamphill 19 th February 2015 CONTENTS What Is IBS What are FODMAPs Service Provision Audit Results Future Work WHAT IS IBS The Rome III
Low FODMAP Dietary Approach For FGD/IBS Our Experience Charlotte McCamphill 19 th February 2015 CONTENTS What Is IBS What are FODMAPs Service Provision Audit Results Future Work WHAT IS IBS The Rome III
Evolving Therapy in Irritable Bowel Syndrome (IBS)
") Evolving Therapy in Irritable Bowel Syndrome (IBS) Dr. Syed Mohammad Arif MBBS, FCPS (Medicine), MD (Gastro) Associate Professor Department of Medicine Dhaka Medical College A good set of bowels is worth
Evolving Therapy in Irritable Bowel Syndrome (IBS) Dr. Syed Mohammad Arif MBBS, FCPS (Medicine), MD (Gastro) Associate Professor Department of Medicine Dhaka Medical College A good set of bowels is worth
 Disorders in which symptoms cannot be explained by the presence of structural or tissue abnormalities Irritable bowel syndrome Functional heartburn Functional dyspepsia Functional constipation Functional
Disorders in which symptoms cannot be explained by the presence of structural or tissue abnormalities Irritable bowel syndrome Functional heartburn Functional dyspepsia Functional constipation Functional
Irritable Bowel Syndrome
 Irritable Bowel Syndrome A Simple Tool for Identification and Dietary Management Dr Adrian Gilliland, GP and Clinical Advisor Primary Care, Capital and Coast DHB. Dr Rees Cameron, Gastroenterologist, Capital
Irritable Bowel Syndrome A Simple Tool for Identification and Dietary Management Dr Adrian Gilliland, GP and Clinical Advisor Primary Care, Capital and Coast DHB. Dr Rees Cameron, Gastroenterologist, Capital
Bowel cancer risk in the under 50s. Greg Rubin Professor of General Practice and Primary Care
 Bowel cancer risk in the under 50s Greg Rubin Professor of General Practice and Primary Care Prevalence of GI problems in the consulting population Thompson et al, Gut 2000 Number of patients % of patients
Bowel cancer risk in the under 50s Greg Rubin Professor of General Practice and Primary Care Prevalence of GI problems in the consulting population Thompson et al, Gut 2000 Number of patients % of patients
Xifaxan, Lotronex and Viberzi Prior Authorization and Quantity Limit Program Summary
 Xifaxan, Lotronex and Viberzi Prior Authorization and Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1,2 Lotronex (alosetron) a Indication For women with severe diarrheapredominant irritable
Xifaxan, Lotronex and Viberzi Prior Authorization and Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1,2 Lotronex (alosetron) a Indication For women with severe diarrheapredominant irritable
Management of Functional Bowel Disorders
 Management of Functional Bowel Disorders Amy Foxx-Orenstein, DO, FACG, FACP Professor of Medicine Mayo Clinic Tucson Osteopathic Medical Foundation May 1, 2016 Objectives Review epidemiology and pathophysiology
Management of Functional Bowel Disorders Amy Foxx-Orenstein, DO, FACG, FACP Professor of Medicine Mayo Clinic Tucson Osteopathic Medical Foundation May 1, 2016 Objectives Review epidemiology and pathophysiology
David Leff, DO. April 13, Disclosure. I have the following financial relationships to disclosure:
 David Leff, DO AOMA 94 th Annual Convention April 13, 2016 Disclosure I have the following financial relationships to disclosure: Speaker s Bureau: Allergan Labs, Takeda Pharmaceutical, Valeant Pharmaceutical
David Leff, DO AOMA 94 th Annual Convention April 13, 2016 Disclosure I have the following financial relationships to disclosure: Speaker s Bureau: Allergan Labs, Takeda Pharmaceutical, Valeant Pharmaceutical
The Leeds Teaching Hospitals NHS Trust Irritable Bowel Syndrome
 n The Leeds Teaching Hospitals NHS Trust Irritable Bowel Syndrome Information for patients Irritable bowel syndrome (IBS) is a common, long term condition of the digestive system (gut). It causes episodes
n The Leeds Teaching Hospitals NHS Trust Irritable Bowel Syndrome Information for patients Irritable bowel syndrome (IBS) is a common, long term condition of the digestive system (gut). It causes episodes
Why does my stomach hurt? Exploring irritable bowel syndrome
 Why does my stomach hurt? Exploring irritable bowel syndrome By Flavio M. Habal, MD, PhD, FRCPC Case In this article: 1. What is IBS? A 45-year-old female is referred to your office with recurrent 2. How
Why does my stomach hurt? Exploring irritable bowel syndrome By Flavio M. Habal, MD, PhD, FRCPC Case In this article: 1. What is IBS? A 45-year-old female is referred to your office with recurrent 2. How
IBS. Dan Carter, M.D. Institute of Gastroenterology Sheba medical center
 IBS Dan Carter, M.D. Institute of Gastroenterology Sheba medical center Epidemiology Irritable bowel syndrome is a common functional gastrointestinal disorder that manifests as abdominal pain or discomfort
IBS Dan Carter, M.D. Institute of Gastroenterology Sheba medical center Epidemiology Irritable bowel syndrome is a common functional gastrointestinal disorder that manifests as abdominal pain or discomfort
National Institute for Health and Care Excellence Surveillance programme
 National Institute for Health and Care Excellence Surveillance programme Surveillance proposal consultation document Irritable bowel syndrome NICE guideline CG61 8-year surveillance review Background information
National Institute for Health and Care Excellence Surveillance programme Surveillance proposal consultation document Irritable bowel syndrome NICE guideline CG61 8-year surveillance review Background information
Appendix A: Summary of evidence from surveillance
 Appendix A: Summary of evidence from surveillance 8-year surveillance (2016) Irritable bowel syndrome in adults (2008) NICE guideline CG61 Summary of evidence from surveillance... 1 Research recommendations...
Appendix A: Summary of evidence from surveillance 8-year surveillance (2016) Irritable bowel syndrome in adults (2008) NICE guideline CG61 Summary of evidence from surveillance... 1 Research recommendations...
William D. Chey, MD Professor of Medicine University of Michigan
 Evidence-based Treatment Strategies for IBS William D. Chey, MD Professor of Medicine University of Michigan Rome III criteria for IBS Recurrent abdominal pain or discomfort at least 3 days / month in
Evidence-based Treatment Strategies for IBS William D. Chey, MD Professor of Medicine University of Michigan Rome III criteria for IBS Recurrent abdominal pain or discomfort at least 3 days / month in
IBS-D: The Role of Pathophysiology in Assessment and Treatment ReachMD Page 1 of 7
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Irritable Bowel Syndrome (IBS) Information Leaflet THE DIGESTIVE SYSTEM
 Information Leaflet THE DIGESTIVE SYSTEM") THE DIGESTIVE SYSTEM http://healthfavo.com/digestive-system-for-kids.html This factsheet is about Irritable Bowel Syndrome (IBS) Irritable Bowel Syndrome (IBS) consists of a number of symptoms. The most
THE DIGESTIVE SYSTEM http://healthfavo.com/digestive-system-for-kids.html This factsheet is about Irritable Bowel Syndrome (IBS) Irritable Bowel Syndrome (IBS) consists of a number of symptoms. The most
Irritable Bowel Syndrome. Paul Sheykhzadeh, DO, FACG Digestive Health Associates Reno, NV NAPNA Symposium March 5, 2016
 Irritable Bowel Syndrome Paul Sheykhzadeh, DO, FACG Digestive Health Associates Reno, NV NAPNA Symposium March 5, 2016 Definition of Irritable Bowel Syndrome (IBS) Rome III Criteria Recurrent abdominal
Irritable Bowel Syndrome Paul Sheykhzadeh, DO, FACG Digestive Health Associates Reno, NV NAPNA Symposium March 5, 2016 Definition of Irritable Bowel Syndrome (IBS) Rome III Criteria Recurrent abdominal
Functional Dyspepsia
 Functional Dyspepsia American College of Gastroenterology Boston Massachusetts, June 2015 Brian E. Lacy, PhD, MD, FACG Professor of Medicine Geisel School of Medicine at Dartmouth Chief, Section of Gastroenterology
Functional Dyspepsia American College of Gastroenterology Boston Massachusetts, June 2015 Brian E. Lacy, PhD, MD, FACG Professor of Medicine Geisel School of Medicine at Dartmouth Chief, Section of Gastroenterology
IRRITABLE BOWEL SYNDROME
 DR. PHILIP K. BLUSTEIN M.D. F.R.C.P.(C) 415 14 TH ST. NW. CALGARY AB T2N2A1 PHONE (403) 270-9555 FAX (403) 270-7479 IRRITABLE BOWEL SYNDROME DEFINITION: *FUNCTIONAL GASTROINTESTINAL DISORDER CHARACTERIZED
DR. PHILIP K. BLUSTEIN M.D. F.R.C.P.(C) 415 14 TH ST. NW. CALGARY AB T2N2A1 PHONE (403) 270-9555 FAX (403) 270-7479 IRRITABLE BOWEL SYNDROME DEFINITION: *FUNCTIONAL GASTROINTESTINAL DISORDER CHARACTERIZED
Treat primary. symptoms. Offer general lifestyle advice. Manage IBS according to the dominant symptom. Follow up. Symptoms do not improve
 Treat primary symptoms Background information for clinicians Offer general lifestyle advice Background information for patients Manage IBS according to the dominant symptom Provenance Psychological symptoms
Treat primary symptoms Background information for clinicians Offer general lifestyle advice Background information for patients Manage IBS according to the dominant symptom Provenance Psychological symptoms
Irritable Bowel Disease. Dr. Alexandra Ilnyckyj MD
 Irritable Bowel Disease Dr. Alexandra Ilnyckyj MD Exactly what is IBS? Common condition affecting mostly women Symptoms are variable but they reflect altered gut movement (motility) and sensation Commonly
Irritable Bowel Disease Dr. Alexandra Ilnyckyj MD Exactly what is IBS? Common condition affecting mostly women Symptoms are variable but they reflect altered gut movement (motility) and sensation Commonly
Irritable bowel syndrome in adults
 Irritable bowel syndrome in adults Diagnosis and management of irritable bowel syndrome in primary care Issued: February 2008 NICE clinical guideline 61 guidance.nice.org.uk/cg61 NICE has accredited the
Irritable bowel syndrome in adults Diagnosis and management of irritable bowel syndrome in primary care Issued: February 2008 NICE clinical guideline 61 guidance.nice.org.uk/cg61 NICE has accredited the
5 Things to Know About Irritable Bowel Syndrome
 5 Things to Know About Irritable Bowel Syndrome Mike Kolber MD, CCFP, MSc PEIP 2017 Faculty/Presenter Disclosure Presenter: Mike Kolber Relationships that may introduce potential bias and/or conflict of
5 Things to Know About Irritable Bowel Syndrome Mike Kolber MD, CCFP, MSc PEIP 2017 Faculty/Presenter Disclosure Presenter: Mike Kolber Relationships that may introduce potential bias and/or conflict of
What is Irritable Bowel Syndrome (IBS)?
?") What is Irritable Bowel Syndrome (IBS)? Irritable bowel syndrome (IBS) is a health issue found in your intestines (gut). IBS can cause symptoms such as: Belly pain. Cramping. Gas. Bloating (or swelling)
What is Irritable Bowel Syndrome (IBS)? Irritable bowel syndrome (IBS) is a health issue found in your intestines (gut). IBS can cause symptoms such as: Belly pain. Cramping. Gas. Bloating (or swelling)
Dr Melanie Lockett. BSc MBBS MD FRCP Consultant Physician and Gastroenterologist
 Dr Melanie Lockett BSc MBBS MD FRCP Consultant Physician and Gastroenterologist Background & definitions Differential diagnoses NICE guidance 2008 Newer drugs FODMAPs Faecal calprotectin Common IBS mimics
Dr Melanie Lockett BSc MBBS MD FRCP Consultant Physician and Gastroenterologist Background & definitions Differential diagnoses NICE guidance 2008 Newer drugs FODMAPs Faecal calprotectin Common IBS mimics
Irritable Bowel Syndrome
 Irritable Bowel Syndrome Irritable bowel syndrome (IBS) has a variety of symptoms, most commonly cramping, abdominal pain, bloating, constipation, and diarrhea. Symptoms can vary from person to person,
Irritable Bowel Syndrome Irritable bowel syndrome (IBS) has a variety of symptoms, most commonly cramping, abdominal pain, bloating, constipation, and diarrhea. Symptoms can vary from person to person,
Microbiome GI Disorders
 Microbiome GI Disorders Prof. Ram Dickman Neurogastroenterology Unit Rabin Medical Center Israel 1 Key Points Our gut microbiota Were to find them? Symbiosis or Why do we need them? Dysbiosis or when things
Microbiome GI Disorders Prof. Ram Dickman Neurogastroenterology Unit Rabin Medical Center Israel 1 Key Points Our gut microbiota Were to find them? Symbiosis or Why do we need them? Dysbiosis or when things
William D. Chey, MD, FACG. Page 1 of ACG Midwest Regional Postgraduate Course Copyright 2016 American College of Gastroenterology
 Dietary and Other Non-pharmacological Management of IBS William D. Chey, MD, FACG Nostrant Professor of Medicine Director GI Nutrition Program University of Michigan Peter Loftus, May 2, 2016 Page 1 of
Dietary and Other Non-pharmacological Management of IBS William D. Chey, MD, FACG Nostrant Professor of Medicine Director GI Nutrition Program University of Michigan Peter Loftus, May 2, 2016 Page 1 of
Current and Emerging Pharmacological Treatments in Irritable Bowel Syndrome
 Current and Emerging Pharmacological Treatments in Irritable Bowel Syndrome Anthony Lembo, M.D. Associate Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School What is the general
Current and Emerging Pharmacological Treatments in Irritable Bowel Syndrome Anthony Lembo, M.D. Associate Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School What is the general
ROME IV CRITERIA FOR IBS
 PRACTICAL CONSIDERATIONS IN THE MANAGEMENT OF IBS BRENDA HORWITZ MD PROFESSOR OF CLINICAL MEDICINE LEWIS KATZ SCHOOL OF MEDICINE AND TEMPLE UNIVERSITY HEALTH SCIENCES CENTER OR THINGS I ALWAYS WANTED TO
PRACTICAL CONSIDERATIONS IN THE MANAGEMENT OF IBS BRENDA HORWITZ MD PROFESSOR OF CLINICAL MEDICINE LEWIS KATZ SCHOOL OF MEDICINE AND TEMPLE UNIVERSITY HEALTH SCIENCES CENTER OR THINGS I ALWAYS WANTED TO
NEL RISPETTO DELLE NUOVE DISPOSIZIONI IN MATERIA DI ECM, A SEGUITO DELL ATTUAZIONE DELL ACCORDO STATO-REGIONI DEL 5/11/09 E SUCCESSIVE
 NOME E NUMERO DEL PROVIDER: I&C SRL - 5387 ECM N : 180726 TITOLO: XVII CONGRESSO NAZIONALE GISMAD SEDE: MILANO, HOTEL NHOW DATA: 09-10/03/2017 NEL RISPETTO DELLE NUOVE DISPOSIZIONI IN MATERIA DI ECM, A
NOME E NUMERO DEL PROVIDER: I&C SRL - 5387 ECM N : 180726 TITOLO: XVII CONGRESSO NAZIONALE GISMAD SEDE: MILANO, HOTEL NHOW DATA: 09-10/03/2017 NEL RISPETTO DELLE NUOVE DISPOSIZIONI IN MATERIA DI ECM, A
Do Probiotics Provide Adequate Relief From Overall Symptoms, Including Abdominal Pain and Bloating, in Adults With Irritable Bowel Syndrome?
 Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 2015 Do Probiotics Provide Adequate Relief
Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 2015 Do Probiotics Provide Adequate Relief
PELVIC PAIN : Gastroenterological Conditions
 PELVIC PAIN : Gastroenterological Conditions Departman Tarih Prof. A. Melih OZEL, MD Department of Gastroenterology Anadolu Medical Center Hospital Gebze Kocaeli - TURKEY Presentation plan 15 min. Introduction
PELVIC PAIN : Gastroenterological Conditions Departman Tarih Prof. A. Melih OZEL, MD Department of Gastroenterology Anadolu Medical Center Hospital Gebze Kocaeli - TURKEY Presentation plan 15 min. Introduction
SESSION 5 2:30pm 3:45pm
 SESSION 5 2:3pm 3:45pm Optimizing the Diagnosis, Treatment, and Management of Irritable Bowel Syndrome SPEAKERS Richard J. Saad, MD, MS Spencer Dorn, MD, MPH, MHA Presenter Disclosure Information The following
SESSION 5 2:3pm 3:45pm Optimizing the Diagnosis, Treatment, and Management of Irritable Bowel Syndrome SPEAKERS Richard J. Saad, MD, MS Spencer Dorn, MD, MPH, MHA Presenter Disclosure Information The following
Hompes Method. Practitioner Training Level II. Lesson Eight Part 1C SIBO Protocols
 Hompes Method Practitioner Training Level II Lesson Eight Part 1C SIBO Protocols Health for the People Ltd not for reuse without expressed permission Hompes Method is a trading name of Health For The People
Hompes Method Practitioner Training Level II Lesson Eight Part 1C SIBO Protocols Health for the People Ltd not for reuse without expressed permission Hompes Method is a trading name of Health For The People
The Use of Antidepressants in the Treatment of Irritable Bowel Syndrome and Other Functional GI Disorders What are functional GI disorders?
 The Use of Antidepressants in the Treatment of Irritable Bowel Syndrome and Other Functional GI Disorders Christine B. Dalton, PA-C Douglas A. Drossman, MD and Kellie Bunn, PA-C What are functional GI
The Use of Antidepressants in the Treatment of Irritable Bowel Syndrome and Other Functional GI Disorders Christine B. Dalton, PA-C Douglas A. Drossman, MD and Kellie Bunn, PA-C What are functional GI
Gut microbiota in IBS and its modification by diet: probiotics, prebiotics and low FODMAP diet
 Gut microbiota in IBS and its modification by diet: probiotics, prebiotics and low FODMAP diet Kevin Whelan PhD RD FBDA Professor of Dietetics Department of Nutritional Sciences King s College London Nutritional
Gut microbiota in IBS and its modification by diet: probiotics, prebiotics and low FODMAP diet Kevin Whelan PhD RD FBDA Professor of Dietetics Department of Nutritional Sciences King s College London Nutritional
Disclosures. Objectives. Pre-Test Question 1. Pre-Test Question 2. Pre-Test Question 3 9/23/2016
 Disclosures Beating the Bowel Blues: An Update on the Treatment of Irritable Bowel Syndrome Matthew Nelson, PharmDBCPS, Roosevelt University College of Pharmacy Matthew Nelson declares no conflicts of
Disclosures Beating the Bowel Blues: An Update on the Treatment of Irritable Bowel Syndrome Matthew Nelson, PharmDBCPS, Roosevelt University College of Pharmacy Matthew Nelson declares no conflicts of
CHAPTER 11 Functional Gastrointestinal Disorders (FGID) Mr. Ashok Kumar Dept of Pharmacy Practice SRM College of Pharmacy SRM University
 Mr. Ashok Kumar Dept of Pharmacy Practice SRM College of Pharmacy SRM University") CHAPTER 11 Functional Gastrointestinal Disorders (FGID) Mr. Ashok Kumar Dept of Pharmacy Practice SRM College of Pharmacy SRM University 1 Definition of FGID Chronic and recurrent symptoms of the gastrointestinal
CHAPTER 11 Functional Gastrointestinal Disorders (FGID) Mr. Ashok Kumar Dept of Pharmacy Practice SRM College of Pharmacy SRM University 1 Definition of FGID Chronic and recurrent symptoms of the gastrointestinal
Tana's Habitat - Vim and Vigor - They Don t Call Them High Bars For Nothin
 http://www.tanashabitat.com/vim/0404151of6.asp Do you have a tummy ache that ver seems to go away? Do you wish your gu would just calm down and let you live your life? If so, you re not alo. You may suffer
http://www.tanashabitat.com/vim/0404151of6.asp Do you have a tummy ache that ver seems to go away? Do you wish your gu would just calm down and let you live your life? If so, you re not alo. You may suffer
The effect of fluoxetine in patients with pain and constipation-predominant irritable bowel syndrome: a double-blind randomized-controlled study
 Aliment Pharmacol Ther 2005; 22: 381 385. doi: 10.1111/j.1365-2036.2005.02566.x The effect of fluoxetine in patients with pain and constipation-predominant irritable bowel syndrome: a double-blind randomized-controlled
Aliment Pharmacol Ther 2005; 22: 381 385. doi: 10.1111/j.1365-2036.2005.02566.x The effect of fluoxetine in patients with pain and constipation-predominant irritable bowel syndrome: a double-blind randomized-controlled
Rome III Criteria for IBS. Irritable Bowel Syndrome: What s the Latest? IBS: What s the Latest? Distinguishing IBS-C from CC
 Rome III Criteria for IBS Irritable Bowel Syndrome: What s the Latest? Tim Burke, DO Pacific Digestive Associates Clackamas, OR Recurrent abdominal pain or discomfort at least 3 days/month in the last
Rome III Criteria for IBS Irritable Bowel Syndrome: What s the Latest? Tim Burke, DO Pacific Digestive Associates Clackamas, OR Recurrent abdominal pain or discomfort at least 3 days/month in the last
Clinically proven to quickly relieve symptoms of common gastrointestinal disorders. TERRAGASTRO - Good health starts in the gut
 Clinically proven to quickly relieve symptoms of common gastrointestinal disorders GASTROINTESTINAL DISEASE Referred to as gastrointestinal diseases, they are common disorders which affect the esophagus,
Clinically proven to quickly relieve symptoms of common gastrointestinal disorders GASTROINTESTINAL DISEASE Referred to as gastrointestinal diseases, they are common disorders which affect the esophagus,
Objectives. Pain Types Brief Review. Referred Pain. Chronic/Recurrent Abdominal Pain 1/12/2017. I have no conflicts of interest to disclose
 Joshua D Noe, MD Associate Professor of Pediatric Gastroenterology Hepatology and Nutrition Medical College of Wisconsin I have no conflicts of interest to disclose Objectives Differentiate functional
Joshua D Noe, MD Associate Professor of Pediatric Gastroenterology Hepatology and Nutrition Medical College of Wisconsin I have no conflicts of interest to disclose Objectives Differentiate functional
Food Choices and Alternative Techniques in Management of IBS: Fad Versus Evidence
 Food Choices and Alternative Techniques in Management of IBS: Fad Versus Evidence Maria Vazquez Roque, MD, MSc Assistant Professor Gastroenterology and Hepatology 2010 MFMER slide-1 Objectives Gluten-free
Food Choices and Alternative Techniques in Management of IBS: Fad Versus Evidence Maria Vazquez Roque, MD, MSc Assistant Professor Gastroenterology and Hepatology 2010 MFMER slide-1 Objectives Gluten-free
Understanding & Alleviating Constipation. Living (Well!) with Gastroparesis Program Warm-Up Class
 with Gastroparesis Program Warm-Up Class") Understanding & Alleviating Constipation Living (Well!) with Gastroparesis Program Warm-Up Class Please Remember The information presented is for educational purposes only and is in no way intended as
Understanding & Alleviating Constipation Living (Well!) with Gastroparesis Program Warm-Up Class Please Remember The information presented is for educational purposes only and is in no way intended as
FUNCTIONAL DISORDERS TREATMENT ADVANCES. Dr. Adriana Lazarescu MD FRCPC Director GI Motility Lab, Edmonton Associate Professor University of Alberta
 FUNCTIONAL DISORDERS TREATMENT ADVANCES Dr. Adriana Lazarescu MD FRCPC Director GI Motility Lab, Edmonton Associate Professor University of Alberta Name: Dr. Adriana Lazarescu Conflict of Interest Disclosure
FUNCTIONAL DISORDERS TREATMENT ADVANCES Dr. Adriana Lazarescu MD FRCPC Director GI Motility Lab, Edmonton Associate Professor University of Alberta Name: Dr. Adriana Lazarescu Conflict of Interest Disclosure
IRRITABLE BOWEL SYNDROME
 IRRITABLE BOWEL SYNDROME CONTENT CREATED BY Learn more at www.health.harvard.edu TALK WITH YOUR DOCTOR Table of Contents Here are some questions to ask your doctor. WHAT IS IRRITABLE BOWEL SYNDROME? 4
IRRITABLE BOWEL SYNDROME CONTENT CREATED BY Learn more at www.health.harvard.edu TALK WITH YOUR DOCTOR Table of Contents Here are some questions to ask your doctor. WHAT IS IRRITABLE BOWEL SYNDROME? 4
The relationship between FODMAP intake and acute gastrointestinal symptoms in adults with IBS A novel analysis using the FAST Diary
 The relationship between FODMAP intake and acute gastrointestinal symptoms in adults with IBS A novel analysis using the FAST Diary Macintosh A 1, Wright-McNaughton M 1, Frampton C 2, Skidmore P 1, Gearry
The relationship between FODMAP intake and acute gastrointestinal symptoms in adults with IBS A novel analysis using the FAST Diary Macintosh A 1, Wright-McNaughton M 1, Frampton C 2, Skidmore P 1, Gearry
What s the Latest? Rome III Criteria for IBS
 Irritable Bowel lsyndrome: What s the Latest? American College of Gastroenterology Las Vegas, January 2014 Bi Brian E. Lacy, Ph.D., PhD M.D., MD FACG Professor of Medicine Geisel School of Medicine at
Irritable Bowel lsyndrome: What s the Latest? American College of Gastroenterology Las Vegas, January 2014 Bi Brian E. Lacy, Ph.D., PhD M.D., MD FACG Professor of Medicine Geisel School of Medicine at
Irritable Bowel Syndrome
 68 TH ANNUAL MCGILL REFRESHER COURSE FOR FAMILY PHYSICIANS 2017 Irritable Bowel Syndrome Gad Friedman, MDCM, FRCPC Jewish General Hospital DISCLOSURES I have no disclosures LEARNING OBJECTIVES 1. Review
68 TH ANNUAL MCGILL REFRESHER COURSE FOR FAMILY PHYSICIANS 2017 Irritable Bowel Syndrome Gad Friedman, MDCM, FRCPC Jewish General Hospital DISCLOSURES I have no disclosures LEARNING OBJECTIVES 1. Review
The York Faecal Calprotectin Care Pathway for use in primary care. James Turvill
 The York Faecal Calprotectin Care Pathway for use in primary care James Turvill NICE guidance: dg11 Faecal calprotectin (FC) testing as an option in adults with recent onset of lower gastrointestinal symptoms
The York Faecal Calprotectin Care Pathway for use in primary care James Turvill NICE guidance: dg11 Faecal calprotectin (FC) testing as an option in adults with recent onset of lower gastrointestinal symptoms
IBS CLOSED REFERRAL STATUS: Dear Dr.,
 Name: PHN/ULI: DOB: RHRN: RefMD: Dr. RefMD Fax: RefDate: Date Today: CONFIRMATION: TRIAGE CATEGORY: REFERRAL STATUS: Dear Dr., Referral Received Enhanced Primary Care Pathway CLOSED IBS The clinical and
Name: PHN/ULI: DOB: RHRN: RefMD: Dr. RefMD Fax: RefDate: Date Today: CONFIRMATION: TRIAGE CATEGORY: REFERRAL STATUS: Dear Dr., Referral Received Enhanced Primary Care Pathway CLOSED IBS The clinical and
IBS current status Peter Laszlo Lakatos
 IBS current status Peter Laszlo Lakatos Semmelweis University 1st Department of Medicine Functional gastrointestinal disorders Chronic or fluctuating functional gastrointestinal symptoms that can not be
IBS current status Peter Laszlo Lakatos Semmelweis University 1st Department of Medicine Functional gastrointestinal disorders Chronic or fluctuating functional gastrointestinal symptoms that can not be
IBS-D: What to Do When Typical Treatment Methods Fail
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Melbourne GI & Endoscopy
 1 Melbourne GI & Endoscopy Multi-disciplinary care for your patients Gastroenterology Hepatobiliary & upper gastrointestinal surgery Colorectal surgery Oncology Perioperative care One contact & one address
1 Melbourne GI & Endoscopy Multi-disciplinary care for your patients Gastroenterology Hepatobiliary & upper gastrointestinal surgery Colorectal surgery Oncology Perioperative care One contact & one address
Diagnosis and Treatment of Irritable Bowel Syndrome
 Special Issue Diagnosis and Treatment of Irritable Bowel Syndrome Myung Gyu Choi, M.D. Department of Internal Medicine The Catholic University of Korea, College of Medicine Kangnam St. Mary's Hospital
Special Issue Diagnosis and Treatment of Irritable Bowel Syndrome Myung Gyu Choi, M.D. Department of Internal Medicine The Catholic University of Korea, College of Medicine Kangnam St. Mary's Hospital
The Role of Food in the Functional Gastrointestinal Disorders
 The Role of Food in the Functional Gastrointestinal Disorders H. Vahedi, MD. Gastroentrologist Associate professor of medicine DDRI 92.4.27 vahedi@ams.ac.ir Disorder Sub-category A. Oesophageal disorders
The Role of Food in the Functional Gastrointestinal Disorders H. Vahedi, MD. Gastroentrologist Associate professor of medicine DDRI 92.4.27 vahedi@ams.ac.ir Disorder Sub-category A. Oesophageal disorders
Pharmacotherapy for IBS
 Pharmacotherapy for IBS Brooks D. Cash, M.D., FACG Chief, Gastroenterology Professor of Medicine University of South Alabama Director, GI Physiology, USA Medical Center Mobile, AL Disclosures I have served
Pharmacotherapy for IBS Brooks D. Cash, M.D., FACG Chief, Gastroenterology Professor of Medicine University of South Alabama Director, GI Physiology, USA Medical Center Mobile, AL Disclosures I have served
IBS and Functional GI Disorders (FGIDs)
") Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/gi-insights/ibs-and-functional-gi-disorders-fgids/7424/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/gi-insights/ibs-and-functional-gi-disorders-fgids/7424/
Spectrum of Diverticular Disease. Outline
 Spectrum of Disease ACG Postgraduate Course January 24, 2015 Lisa Strate, MD, MPH Associate Professor of Medicine University of Washington, Seattle, WA Outline Traditional theories and updated perspectives
Spectrum of Disease ACG Postgraduate Course January 24, 2015 Lisa Strate, MD, MPH Associate Professor of Medicine University of Washington, Seattle, WA Outline Traditional theories and updated perspectives
An Evidence-based Approach to Dietary Treatment of Irritable Bowel Syndrome
 An Evidence-based Approach to Dietary Treatment of Irritable Bowel Syndrome American College of Gastroenterology August 2014, Indianapolis Brian E. Lacy, Ph.D., M.D. Professor of Medicine, Geisel School
An Evidence-based Approach to Dietary Treatment of Irritable Bowel Syndrome American College of Gastroenterology August 2014, Indianapolis Brian E. Lacy, Ph.D., M.D. Professor of Medicine, Geisel School
Chronic Abdominal Pain. Dr. Robert B. Smith Tupelo Digestive Health Specialists August 26, 2016
 Chronic Abdominal Pain Dr. Robert B. Smith Tupelo Digestive Health Specialists August 26, 2016 Disclosures Speaker Bureau for Allergan Pharmaceuticals Abdominal Pain - Definitions Acute occurring for several
Chronic Abdominal Pain Dr. Robert B. Smith Tupelo Digestive Health Specialists August 26, 2016 Disclosures Speaker Bureau for Allergan Pharmaceuticals Abdominal Pain - Definitions Acute occurring for several
Refractory IBS-D: An Evidence-Based Approach to Therapy
 Refractory IBS-D: An Evidence-Based Approach to Therapy Darren M. Brenner, MD, AGAF Associate Professor of Medicine and Surgery Director, Northwestern Neurogastromotility, Functional, and Integrated Bowel
Refractory IBS-D: An Evidence-Based Approach to Therapy Darren M. Brenner, MD, AGAF Associate Professor of Medicine and Surgery Director, Northwestern Neurogastromotility, Functional, and Integrated Bowel
FODMAPs: Major role in food sensitivities
 : Major role in food sensitivities Jessica Biesiekierski Post-doctoral Research Fellow Translational Research Center for Gastrointestinal Disorders KU Leuven, Belgium Role of food in GI symptoms? Abdominal
: Major role in food sensitivities Jessica Biesiekierski Post-doctoral Research Fellow Translational Research Center for Gastrointestinal Disorders KU Leuven, Belgium Role of food in GI symptoms? Abdominal
PELVIC PAIN : Gastroenterological Conditions
 PELVIC PAIN : Gastroenterological Conditions Departman Tarih Prof. A. Melih OZEL, MD Department of Gastroenterology Anadolu Medical Center Hospital Gebze Kocaeli - TURKEY Presentation plan 15 min. Introduction
PELVIC PAIN : Gastroenterological Conditions Departman Tarih Prof. A. Melih OZEL, MD Department of Gastroenterology Anadolu Medical Center Hospital Gebze Kocaeli - TURKEY Presentation plan 15 min. Introduction
Irritable bowel syndrome (IBS) is a chronic, potentially disabling
 is a chronic, potentially disabling") Evidence-Based Management of Irritable Bowel Syndrome With Diarrhea Mark Pimentel, MD Irritable bowel syndrome (IBS) is a chronic, potentially disabling disorder of the gastrointestinal (GI) tract with
Evidence-Based Management of Irritable Bowel Syndrome With Diarrhea Mark Pimentel, MD Irritable bowel syndrome (IBS) is a chronic, potentially disabling disorder of the gastrointestinal (GI) tract with
State of the Art: Management of Irritable Bowel Syndrome
 ACG/FGS Annual Spring Symposium March 16-18, 2018 Bonita Springs, FL State of the Art: Management of Irritable Bowel Syndrome William D. Chey, MD Professor of Medicine University of Michigan IBS: Rome
ACG/FGS Annual Spring Symposium March 16-18, 2018 Bonita Springs, FL State of the Art: Management of Irritable Bowel Syndrome William D. Chey, MD Professor of Medicine University of Michigan IBS: Rome
Canadian Association of Gastroenterology Clinical Practice Guideline for the Management of Irritable Bowel Syndrome (IBS)
") Journal of the Canadian Association of Gastroenterology, 2019, XX(X), 1 24 doi: 10.1093/jcag/gwy071 Original Article Original Article Canadian Association of Gastroenterology Clinical Practice Guideline
Journal of the Canadian Association of Gastroenterology, 2019, XX(X), 1 24 doi: 10.1093/jcag/gwy071 Original Article Original Article Canadian Association of Gastroenterology Clinical Practice Guideline
Diagnosing and Managing IBS in IBD Patients. September 2012
 Diagnosing and Managing IBS in IBD Patients September 2012 Professor David S Sanders Consultant Gastroenterologist Royal Hallamshire Hospital & University of Sheffield Patient Comes to see you with GI
Diagnosing and Managing IBS in IBD Patients September 2012 Professor David S Sanders Consultant Gastroenterologist Royal Hallamshire Hospital & University of Sheffield Patient Comes to see you with GI
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Constipation: the diagnosis and management of idiopathic childhood constipation in primary and secondary care 1.1 Short title
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Constipation: the diagnosis and management of idiopathic childhood constipation in primary and secondary care 1.1 Short title
Review article: an analysis of safety profiles of treatments for diarrhoea predominant irritable bowel syndrome
 Received: 9 April 2018 First decision: 27 April 2018 Accepted: 28 July 2018 DOI: 10.1111/apt.14948 Review article: an analysis of safety profiles of treatments for diarrhoea predominant irritable bowel
Received: 9 April 2018 First decision: 27 April 2018 Accepted: 28 July 2018 DOI: 10.1111/apt.14948 Review article: an analysis of safety profiles of treatments for diarrhoea predominant irritable bowel
Tenapanor for irritable bowel syndrome with constipation
 NIHR Innovation Observatory Evidence Briefing: February 2018 Tenapanor for irritable bowel syndrome with constipation NIHRIO (HSRIC) ID: 6704 NICE ID: 9736 LAY SUMMARY Irritable bowel syndrome with constipation
NIHR Innovation Observatory Evidence Briefing: February 2018 Tenapanor for irritable bowel syndrome with constipation NIHRIO (HSRIC) ID: 6704 NICE ID: 9736 LAY SUMMARY Irritable bowel syndrome with constipation
FODMAPs: Emerging Science and Implications for Practice
 FODMAPs: Emerging Science and Implications for Practice Megan Rossi, PhD RD @DrMegan_RD @Dr_Megan www.drmeganrossi.com BDA guidelines for dietary management of IBS 1) Healthy eating and lifestyle Alcohol
FODMAPs: Emerging Science and Implications for Practice Megan Rossi, PhD RD @DrMegan_RD @Dr_Megan www.drmeganrossi.com BDA guidelines for dietary management of IBS 1) Healthy eating and lifestyle Alcohol
Irritable Bowel. Syndrome. Health Promotion Service
 The information in this leaflet is not intended to replace the knowledge or diagnosis of a qualified health practitioner. We encourage you to consult a health professional and ensure your IBS is properly
The information in this leaflet is not intended to replace the knowledge or diagnosis of a qualified health practitioner. We encourage you to consult a health professional and ensure your IBS is properly
Lower Gastrointestinal Tract KNH 406
 Lower Gastrointestinal Tract KNH 406 Lower GI Tract A&P Small Intestine Anatomy Duodenum, jejunum, ileum Maximum surface area for digestion and absorption Specialized enterocytes from stem cells of crypts
Lower Gastrointestinal Tract KNH 406 Lower GI Tract A&P Small Intestine Anatomy Duodenum, jejunum, ileum Maximum surface area for digestion and absorption Specialized enterocytes from stem cells of crypts
Clinical problems related to GI involvement in SSc
 Clinical problems related to GI involvement in SSc Incontinence Abdominal pain/distension Gastro-oesophageal Diarrhoea Weight loss/al Issues Constipation Management of incontinence Establish diagnosis
Clinical problems related to GI involvement in SSc Incontinence Abdominal pain/distension Gastro-oesophageal Diarrhoea Weight loss/al Issues Constipation Management of incontinence Establish diagnosis
Irritable Bowel Syndrome: Current and Emerging Treatment Options
 Irritable Bowel Syndrome: Current and Emerging Treatment Options Lauren Peyton, PharmD, CDE; and Joy Greene, PharmD INTRODUCTION Irritable bowel syndrome (IBS), one of the most prevalent functional gastrointestinal
Irritable Bowel Syndrome: Current and Emerging Treatment Options Lauren Peyton, PharmD, CDE; and Joy Greene, PharmD INTRODUCTION Irritable bowel syndrome (IBS), one of the most prevalent functional gastrointestinal
New Tests and Treatments for Dyspepsia and Irritable Bowel Syndrome
 New Tests and Treatments for Dyspepsia and Irritable Bowel Syndrome Soojong Hong Chae, MD Clinical Assistant Professor Digestive Diseases and Nutrition University of South Florida ROME III Functional dyspepsia
New Tests and Treatments for Dyspepsia and Irritable Bowel Syndrome Soojong Hong Chae, MD Clinical Assistant Professor Digestive Diseases and Nutrition University of South Florida ROME III Functional dyspepsia
fever a persistent unexplained change in bowel habit in somebody over 50 years of age a family history of bowel or ovarian cancer.
 If you have had these symptoms for some time, if they come and go but never completely go away, then go and see your doctor. In practice, IBS is a diagnosis of exclusion. There is no test or marker that
If you have had these symptoms for some time, if they come and go but never completely go away, then go and see your doctor. In practice, IBS is a diagnosis of exclusion. There is no test or marker that
10/1/2016. Kimberly Kearns, MS, APN, ANP-BC Mary Davitt, MS, PMHNP-BC Rachel Richardson, RD. Kimberly Kearns, APN. Mary Davitt, PMHNP.
 Kimberly Kearns, MS, APN, ANP-BC Mary Davitt, MS, PMHNP-BC Rachel Richardson, RD Kimberly Kearns, APN Speakers Bureau: Medtronic Salix Pharmaceuticals Takeda Pharmaceuticals Mary Davitt, PMHNP None Rachel
Kimberly Kearns, MS, APN, ANP-BC Mary Davitt, MS, PMHNP-BC Rachel Richardson, RD Kimberly Kearns, APN Speakers Bureau: Medtronic Salix Pharmaceuticals Takeda Pharmaceuticals Mary Davitt, PMHNP None Rachel
Irritable Bowel Syndrome
 Irritable Bowel Syndrome Dietary Management Practicalities Dearbháile O Hanlon Senior Specialist Gastroenterology Dietitian Outline Diagnosis & Red Flags Initial assessment Tips to help implement diet
Irritable Bowel Syndrome Dietary Management Practicalities Dearbháile O Hanlon Senior Specialist Gastroenterology Dietitian Outline Diagnosis & Red Flags Initial assessment Tips to help implement diet
Irritable bowel syndrome diagnosis and management: A simplified algorithm for clinical practice
 Review Article Irritable bowel syndrome diagnosis and management: A simplified algorithm for clinical practice United European Gastroenterology Journal 2017, Vol. 5(6) 773 788! Author(s) 2016 Reprints
Review Article Irritable bowel syndrome diagnosis and management: A simplified algorithm for clinical practice United European Gastroenterology Journal 2017, Vol. 5(6) 773 788! Author(s) 2016 Reprints
William Chey, MD University of Michigan Ann Arbor, MI
 Lin Chang, MD David Geffen School of Medicine at UCLA Los Angeles, CA William Chey, MD University of Michigan Ann Arbor, MI Mark Pimentel, MD Cedars-Sinai Medical Center Los Angeles, CA Accredited by Jointly
Lin Chang, MD David Geffen School of Medicine at UCLA Los Angeles, CA William Chey, MD University of Michigan Ann Arbor, MI Mark Pimentel, MD Cedars-Sinai Medical Center Los Angeles, CA Accredited by Jointly
Guidelines NICE, not NICE and the Daily Mail. Dr Andy Poullis Consultant Gastroenterologist
 Guidelines NICE, not NICE and the Daily Mail 2018 Dr Andy Poullis Consultant Gastroenterologist Coeliac IBS Gall bladder polyps PEI PPI Who to test for Coeliac persistent unexplained abdominal or gastrointestinal
Guidelines NICE, not NICE and the Daily Mail 2018 Dr Andy Poullis Consultant Gastroenterologist Coeliac IBS Gall bladder polyps PEI PPI Who to test for Coeliac persistent unexplained abdominal or gastrointestinal