A. F. Ozer, 1 F. Keskin, 2 T. Oktenoglu, 3 T. Suzer, 3 Y. Ataker, 4 C. Gomleksiz, 5 and M. Sasani Introduction
|
|
|
- Francis Benson
- 6 years ago
- Views:
Transcription
1 Advances in Orthopedics Volume 2013, Article ID , 6 pages Clinical Study A Novel Approach to the Surgical Treatment of Lumbar Disc Herniations: Indications of Simple Discectomy and Posterior Transpedicular Dynamic Stabilization Based on Carragee Classification A. F. Ozer, 1 F. Keskin, 2 T. Oktenoglu, 3 T. Suzer, 3 Y. Ataker, 4 C. Gomleksiz, 5 and M. Sasani 3 1 Neurosurgery Department, Koç University School of Medicine, Rumelifeneri Yolu Sarıyer, Istanbul, Turkey 2 Neurosurgery Department, Necmettin Erbakan University Meram Medical Faculty Hospital, Konya, Turkey 3 Neurosurgery Department, American Hospital, Istanbul, Turkey 4 Physical Therapy and Rehabilitation Department, American Hospital, Istanbul, Turkey 5 Neurosurgery Department, Mengücek Gazi Training and Research Hospital, School of Medicine, Erzincan University, Erzincan, Turkey Correspondence should be addressed to A. F. Ozer; alifahirozer@gmail.com Received 30 January 2013; Accepted 7 March 2013 Academic Editor: Deniz Erbulut Copyright 2013 A. F. Ozer et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Surgery of lumbar disc herniation is still a problem since Mixter and Barr. Main trouble is dissatisfaction after the operation. Today there is a debate on surgical or conservative treatment despite spending great effort to provide patients with satisfaction. The main problem is segmental instability, and the minimally invasive approach via microscope or endoscope is not necessarily appropriate solution for all cases. Microsurgery or endoscopy would be appropriate for the treatment of Carragee type I and type III herniations. On the other hand in Carragee type II and type IV herniations that are prone to develop recurrent disc herniation and segmental instability, the minimal invasive techniques might be insufficient to achieve satisfactory results. The posterior transpedicular dynamic stabilization method might be a good solution to prevent or diminish the recurrent disc herniation and development of segmental instability. In this study we present our experience in the surgical treatment of disc herniations. 1. Introduction Thesurgicaltreatmentoflumbardischerniationisperformed when the conservative treatment is recalcitrant and only ten percent of all lumbar disc herniations cases are candidates to surgery [1]. The main problem with the surgery is that the lumbar pain of the patients does not necessarily relieved following surgery and even they might become worse. For this reason, there are serious anxiety and suspicion against the surgical treatment of lumbar disc herniations. This phenomenon is also valid for some spine surgeons who will perform the operation. Even on their own series of Mixter and Barr, who first performed the discectomy of lumbar disc herniations, the success and failure rates compete head to head [2]. Later Caspar and Yasargil introduced the microscope into the disc surgery and allowed minimal anatomic damage; however, no significant rise was achieved in satisfactory results [3, 4]. Carragee et al. revealed that the occurrence of disc herniation, the type of surgery, and the rates of reherniation areinacloserelationwiththedefectonposteriorannulus [5]. Lumbar disc herniation is not a separate illness but a part of a degenerative process, so the treatment should be designed in this manner. It is known that if the defect on the annulus is small, annulus has capacity to repair itself after fragmentectomy with both operative techniques: endoscopy and microdiscectomy. On the other hand, if the defect is large, problemarisesatthattime[6, 7]. In this paper, we discussed our results in the light of literature.weevaluatedtheroleofloadsharingprinciplewith
2 2 Advances in Orthopedics application of posterior transpedicular dynamic stabilization (PTDS) in lumbar disc herniation cases with large annulus defect, instead of performing radical discectomy. 2. Materials and Methods This is a prospective study held between 2008 and Totally 98 patients were included in the study who did not respond to conservative treatment and minimal invasive painprocedurethatwasappliedataminimumof6weeks. Conservative treatment includes back exercises program and medicine. Epidural steroid injection and anauloplasty with laser were also performed for some of these cases as a minimal invasive pain procedure. Five surgeons performed the operations. The patients included for the study met the following inclusion criteria: (1) the findings of neurologic examination concordant with the patient s sciatica, (2) one level lumbar disc herniation determined with MR, (3) the surgical procedure applied electively, and (4) not having a spine operation before. Additionally, the patients with infection, instability, scoliosis, and malignancy are excluded fromthestudy.thetypeoftheoperationtobeappliedwas told to all the patients and the consent of patients was taken. Before the operation, magnetic resonance imaging was done to all cases and the deformation of annulus was evaluated with MR study and under the surgical microscope in operation. Patients were divided into four groups according to the classification of Carragee et al. [5] with a slight modification. In regard to achieving low recurrence notes, we accepted annulus defect as 4 mm difference from Carragee: (i) Type I: there is no significant defect on annulus (Figure 1), (ii) Type II: annular defect > 4mm(Figure 2), (iii) Type III: annular defect < 4mm(Figure 3), (iv) Type IV: massive-large annular defect (Figure 4). The mean age of the patients was (between 16 and 80). We determined the type of surgical intervention in reference to CS based on intraoperative observation and MR study. Clinic results were evaluated with visual analog scale (VAS) and Oswestry Disability Index (ODI) in the 3rd, 12th, and 24th months after the surgery. All patients who developed severe low back pain and/or recurrence sciatica were evaluated with MR for recurrence of disc herniation Surgical Technique. The surgical interventions were applied by five surgeons using standard microsurgical techniques at the same hospital. Before the surgical intervention, a single prophylactic antibiotic was given. According to the classification of modified Carragee, only fragmentectomy was applied to the cases of Type I herniation and discectomy was not applied in the course of the operation since annular tear was not observed under the surgical microscope. Limited discectomy was applied to the patients in the other groups. While discectomy was performed through the interlaminar gapinmostofthepatients,discectomywasappliedtosome patients following laminotomy with use of high speed drill. In the course of the operation the types of disc herniation were defined with regard to MCC. In the cases with MC Type II herniation, fragmentectomy (annular tear > 4 mm), limited discectomy with excision of degenerate nucleus pulposus, and annulus repair were performed. Annulus repair is carried out with bipolar cauterization of damaged outer layers of annulus fibrosus under the surgical microscope. PTDS was applied under C-arm scopy through paravertebral muscles as per Wiltse method, Cosmic (Ulrich GmbH & Co. KG, Ulm, Germany) and Safinaz (Medikon, Ankara, Turkey) screw and rods used for PTDS.InthecaseswithMCTypeIIIherniations,limited discectomy (annular tear < 4 mm) with excision of degenerate nucleus pulposus and annulus repair were performed and PTDS was applied. In the cases with MC Type IV herniations, limited discectomy (massive annular tear) with excision of degenerate nucleus pulposus and annulus repair were performed. Then PTDS was applied. In the course of operation, annular structure and the size of the annular defect were evaluated by at least two surgeons. 3. Results Totally 13 out of 98 patients, operated with fragmentectomy, limited discectomy applied to 20 patients, and limited discectomyandptdswereappliedto65patients.thefrequent type of herniation observed in our study was MCC Type II (47.8%) and the frequency of Type I, Type III, and Type IV was 18.3%, 26.5%, and 7.4%, respectively. Intraoperative complication was not observed. In the course of followup, for patients with Type II herniation, one patient developed a screw break and in one patient we observed screw loosening. It was noticed that these two patients were morbid obese. In the postoperative 8th and 12th month, the instrumentation systems were revised. In Type IV group, in one patient screw break was observed following a severe trauma. The instrumentation system of this patient was revised in 16th postoperative month. Finally a recurrence disc herniation was observed in a patient whose body structure was above the normal standards according to her age. In two patients with Type II and one patient with Type IV, adjacent segment degeneration was monitored. On the other hand, these patients did not complain clinically; therefore an extra surgical intervention was not considered. The follow-up period of cases with Type I group, reherniation, and recurrence herniation were not recorded. In two patients with Type II group reherniation, I in two cases with Type III group reherniation, and in one case with Type IV group, and reherniation as recorded. 4. Discussion Even though it is thought that lumbar disc herniation is a separate disease; in fact, the degenerative change of the vertebrae is a part of the process. Following disc degeneration and before the loss of total disc integrity, the disc becomes clinically problematic due to improvement of painful black
.")
.")

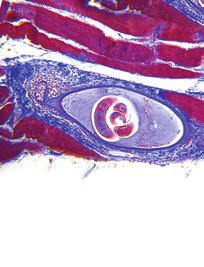
3 Advances in Orthopedics 3 Figure 1: A small extruded fragment was observed under the nerve root. Notice that there is no apparent annulus defect (Carragee Type I). Figure 2: A large extruded fragment and noncontained disc herniation compress right S1 nerve root and cauda equina. Integrity of annulus fibrosus completely destroyed (Carragee Type II). The patient was operated on due to severe neurologic deficit and PTDS was applied to the patient after L5-S1 microdiscectomy and annular repair. Figure 3: A small annulus defect (<4 mm) was observed at the left side just under the S1 nerve root. Integrity of the annulus fibrosus is preserved (Carragee Type III).

4 4 Advances in Orthopedics Figure 4: A large annulus defect (>4 mm) was observed at the midline of posterior annulus fibrosus. Integrity of annulus is preserved (Carragee Type IV). The patient is unresponsive to the conservative treatment and PTDS was applied to the patient after L5-S1 microdiscectomy and annular repair. disc, degenerative spondylolisthesis, or lumbar disc herniation pathologies. That is why its treatment should be with the concepts by which we approach the degenerative process. Sincethebeginningofthesurgeryforthetreatmentof lumbar disc herniation, the basic aim has been to increase the rate of success of the surgical treatment. Because while in some patients even there was no recurrence or residue herniation radiologically, there is still low back and/or radicular pain and in the other group who had very successful operation, they might have several recurrences on the same level and the same side. It has been thought that the results of the surgery implemented with little anatomic damage by using surgical microscope will affect in a positive way, and some reports supported this method [3, 4]. But the issues occurring after that period. However the later reports showed that the result did not change much in reference to the classic surgery [8, 9]. For a long time period, it is believed that fibrosis is sufical area which is somewhat more in some patientsduetoanunknownreason,anditisthoughtthatthe surgical success would increase if the improvement of fibrosis is prevented and made a big bid for this subject; yet, in the meantime the segmental instability was missed out [10 12]. Following the symptomatic lumbar disc herniation surgery at the height loss on disc space, the relaxation on the facet joint capsule, and ligamentous structures were well-known alternations.afterthesurgery,theloadonthefacetjoints increases and it may lead to segmental instability [13 15]. For this reason, segmental instability and chronic lumbar pain which improve after the lumbar discectomy cause this type of treatment to which has been used for long years, become disputable [16].Onlytheremovalofnucleuspulposusisnot suitable to stop the segmental degeneration related to the rotational and translational motions [17 19]. Therefore one of the important reasons of the failure of lumbar surgery is segmental instability. Yorimitsu has been following his patients for more than ten years after the disc surgery and concludedthatthefrequencyofthechroniclumbarpainwas more in proportion to reherniation based on the height loss on disc space [16]. Segmental instability has been shown with the radiological and clinical findings. These findings may not always support each other [20, 21]. The association of lumbar disc herniation and segmental instability is declared to be 20% in the literature[22]. Kotilainen determined that 22% of the patients developed segmental instability following one level microlumbar discectomy studies and concluded that 29% of them had chronic lumbar pain [23]. Frymoyer signified that on wide based L4-5 disc hernias, there was severe lumbar pain and it is related to degenerative instability [22]. In the surgical treatment of lumbar disc herniation, it is very obvious that disc tried to be taken out; that is to say, radical discectomy does not solve the problem. Although it was realized, disc should not be completely removed. The more the existing disc structure is kept, the better the patient will become after the operation. That is to say, the theory of being respectful of the integrity became the main topic of the conversation with Spengeler who defined limited discectomy in This concept was improved more, and it is suggested by Williams that the fragment only should be removedandtheintegrityofthediscshouldbeprotected [24, 25]. Williams reported successful clinic results with minimal disc tissue taken out from the disc while they documented 4 9% recurrence rate and 90% clinic success rate [25, 26]. Afterwards, in the literature the discussions began if fragmentectomy or discectomy would be better. Wera et al. compared subtotal discectomy and sequestrectomy in the cases of herniation in Type II. They found that while intheeventsmadewithsubtotaldiscectomy,reoperation rate was 3.4%, in the events made only fragmentectomy reoperation rate was 21.2%. Consequently, they informed that in the herniation events in Type II, subtotal discectomywouldbemoresuitable[6]. Rogers compared massive discectomy with fragmentectomy in the disc herniations which are ruptured and reported that in the events of fragmentectomy the recurrence rate was 21% which is in ahighrate[27]. Mochida et al. compared the clinical and radiological results of the patients who were operated on by percutaneous nucleotomy and standard discectomy. They documented that in the younger people below 40, surgery performed by protected nucleus pulposus, there were better radiological and clinic results [28]. Thomé et al. stated that recurrence rate is higher by microdiscectomy compared to sequestrectomy [13]. Barth et al. compared the two year rates of reherniation with microdiscectomy and microscopic sequestrectomy. They observed 10.5% reherniation rate in the microdiscectomy group and 12.5% in the events of fragmentectomy and concluded that there was no significant difference between these two groups [29]. However even the results of the patients who had fragmentectomy are better;
5 Advances in Orthopedics 5 duetohighrecurrencerates,somesurgeonsdidnotgiveup performing subtotal discectomy [6, 7]. It is Carragee who emphasized that in the treatment of the lumbar disc herniation, the success is related to the defect on the posterior annulus. Carragee et al. reported in their study that for the patients of Type I group (who had small annular defect with fragment), only fragmentectomy was applied. The rate of reherniation and reoperation was 1%. In the group of Type II (fragment defect), the rate of recurrence sciatica was 27.3%, reoperation rate was high like 21.2%. In the group of Type III (fragment-contained), the rate of recurrence was 11.9% and the reoperation rate was 4.8%. In the group of Type IV (non-fragment-contained), reherniation rate was 37.5% and the rate of reoperation was 6.3%. Only fragmentectomy was applied to Type I group; the other groups were operated on by limited discectomy. Although the clinic results in Type I group were satisfactory, for the other groups, it was observed that the rates of reherniation and reoperation were rather high [5]. Therefore, the persistent pain after the operation and the recurrence is related to segmental instability and directly proportional to the integrity of defect in the posterior annulus. In this study, we applied limited discectomy or fragmentectomy to support posterior tension band; appropriate cases are required in respect to the integrity of disc material. We supported the spine with PTDS. The system shares the load appliedontospinethusdecreasestheloadontheanterior column and this might allow disc to repair itself. Despite the fact that for the patients in Type I and Type III, our approach is the same with Carragee, for patients in Type II and Type IV, we used PTDS in addition to decompression. As a result of this, we achieved better VAS and Oswestry results compared to Carragee and Wera. The rates of recurrence for Type II is 5%andinTypeIVis4%.Whenwereviewthepatientswith recurrence, it was determined that one of them had a trauma in earlier time after the operation and the rest of them were those whose height and weight standards were really high according to the standards of society. Practicallyifweexcludethepatientswhoareoverweight and had trauma, the rate of recurrence will be lower. It is a necessity that for the overweight people in reference to standards, dynamic systems should be designed restoratively. In conclusion, the concept of the stabilisation of the spine in motion has been developed lately. Therearestillmanydarkspotssuchashowmuchit keeps the motion, long term clinic results are unknown; the effectofitontheadjacentsegmentsareunknown.onthe other hand, it has an undeniable reality in its clinical success. Dynamic system technology is open to improvement and it is very certain that we will see the breakthroughs. By time, the dynamic screws, dynamic rods, and even those screws will have the flexibility of their body in the course of adaptation to the bone, will be developed. The rigid systems will leave their places to the systems which will be close to the structure of ligaments. Thus, the use of dynamic systems in the treatment of the cases with Type II and Type IV disc herniations would notbeanovertreatedapproachbutitisastepdirectedto the protection of the disc space following discectomy in more physiological conditionsç. References [1] S. S. Hu, Lumbar disc herniation section of disorders, diseases, and injuries of the spine, in Current Diagnosis and Treatment in Orthopedics, H.B.Skinner,Ed.,pp ,McGraw-Hill, New York, NY, USA, 4th edition, [2] W. J. Mixter and J. S. Barr, Rupture of intervertebral disc with involvement of spinal canal, New England Medicine, vol. 211, pp , [3] W. Caspar, A new surgical procedure for lumbar disc herniation causing less tissue damage through a microsurgical approach, Lumbar Disc Adult Hydrocephalus,vol.4,pp.74 80, [4] M. G. Yasargil, Microsurgical operation of herniated lumbar disc, Advances in Neurosurgery,vol.4,p.81,1977. [5] E. J. Carragee, M. Y. Han, P. W. Suen, and D. Kim, Clinical outcomes after lumbar discectomy for sciatica: the effects of fragment type and anular competence, Bone and Joint Surgery A,vol.85,no.1,pp ,2003. [6] G. D. Wera, C. L. Dean, U. M. Ahn et al., Reherniation and failure after lumbar discectomy: a comparison of fragment excision alone versus subtotal discectomy, Spinal Disorders and Techniques,vol.21,no.5,pp ,2008. [7] E. J. Carragee, A. O. Spinnickie, T. F. Alamin, and S. Paragioudakis, A prospective controlled study of limited Versus subtotal posterior discectomy: short-term outcomes in patients withherniatedlumbarintervertebraldiscsandlargeposterior anular defect, Spine, vol. 31,no. 6, pp , [8] Y. Katayama, Y. Matsuyama, H. Yoshihara et al., Comparison of surgical outcomes between macro discectomy and micro discectomy for lumbar disc herniation: a prospective randomized study with surgery performed by the same spine surgeon, Spinal Disorders and Techniques, vol.19,no.5,pp , [9] K. Türeyen, One-level one-sided lumbar disc surgery with and without microscopic assistance: 1-year outcome in 114 consecutive patients, neurosurgery,vol.99,no.3,pp , [10] A. F. Ozer, T. Oktenoglu, M. Sasani et al., Preserving the ligamentum flavum in lumbar discectomy: a new technique that prevents scar tissue formation in the first 6 months postsurgery, Neurosurgery, vol. 59, supplement 1, pp. S126 S133, [11] J. Brotchi, B. Pirotte, O. De Witte, and M. Levivier, Prevention of epidural fibrosis in a prospective series of 100 primary lumbosacral discectomy patients: follow-up and assessment at reoperation, Neurological Research,vol.21,supplement1,pp.S47 S50, [12] R. N. Alkalay, D. H. Kim, D. W. Urry, J. Xu, T. M. Parker, and P. A. Glazer, Prevention of postlaminectomy epidural fibrosis using bioelastic materials, Spine,vol.28,no.15,pp , [13] C. Thomé, M. Barth, J. Scharf, and P. Schmiedek, Outcome after lumbar sequestrectomy compared with microdiscectomy: a prospective randomized study, Neurosurgery, vol. 2, no. 3, pp , [14] C. Cinotti and F. Postacchini, Biomechanics, in Lumbar Disc Herniation, F. Postacchini, Ed., pp , Springer-Verlag, Wien, Austria, [15] M. Wenger, L. Mariani, A. Kalbarczyk, and U. Gröger, Longterm outcome of 104 patients after lumbar sequestrectomy according to Williams, Neurosurgery, vol.49,no.2,pp , 2001.
6 6 Advances in Orthopedics [16] E. Yorimitsu, K. Chiba, Y. Toyama, and K. Hirabayashi, Longterm outcomes of standard discectomy for lumbar disc herniation: a follow-up study of more than 10 years, Spine,vol.26,no. 6, pp , [17]A.Fujiwara,K.Tamai,M.Yamatoetal., Therelationship between facet joint osteoarthritis and disc degeneration of the lumbar spine: an MRI study, European Spine Journal, vol. 8, no. 5, pp , [18] C. A. Niosi, Q. A. Zhu, D. C. Wilson, O. Keynan, D. R. Wilson, and T. R. Oxland, Biomechanical characterization of the threedimensional kinematic behaviour of the Dynesys dynamic stabilization system: an in vitro study, European Spine Journal, vol. 15, no. 6, pp , [19] A. Rohlmann, T. Zander, H. Schmidt, H. J. Wilke, and G. Bergmann, Analysis of the influence of disc degeneration on the mechanical behaviour of a lumbar motion segment using the finite element method, Biomechanics, vol. 39, no. 13, pp , [20] J.W.Frymoyer,E.N.Hanley,andJ.Howe, Acomparisonof radiographic findings in fusion and nonfusion patients ten or more years following lumbar disc surgery, Spine, vol. 4, no. 5, pp ,1979. [21] S.Sano,S.Yokokura,Y.Nagata,andSeongZeonYoung, Unstable lumbar spine without hypermobility in postlaminectomy cases: mechanism of symptoms and effect of spinal fusion with and without spinal instrumentation, Spine, vol. 15, no. 11, pp , [22] J.W.FrymoyerandD.K.Selby, Segmentalinstability:rationale for treatment, Spine, vol. 10, no. 3, pp , [23] E. Kotilainen and S. Valtonen, Clinical instability of the lumbar spine after microdiscectomy, Acta Neurochirurgica, vol. 125, no. 1 4, pp , [24] D. M. Spengler, E. A. Ouellette, M. Battie, and J. Zeh, Elective discectomy for herniation of a lumbar disc. Additional experience with an objective method, Bone and Joint Surgery A,vol.72,no.2,pp ,1990. [25] R. W. Williams, Microlumbar discectomy. A conservative surgical approach to the virgin herniated lumbar disc, Spine, vol. 3, no. 2, pp , [26] R. W. Williams, Microlumbar discectomy. A 12-year statistical review, Spine,vol.11,no.8,pp , [27] L. A. Rogers, Experience with limited versus extensive disc removal in patients undergoing microsurgical operations for ruptured lumbar discs, Neurosurgery, vol.22,no.1,pp.82 85, [28] J. Mochida, K. Nishimura, T. Nomura, E. Toh, and M. Chiba, The importance of preserving disc structure in surgical approaches to lumbar disc herniation, Spine, vol. 21, no. 13, pp , [29] M. Barth, C. Weiss, and C. Thomé, Two-year outcome after lumbar microdiscectomy versus microscopic sequestrectomypart 1: evaluation of clinical outcome, Spine, vol.33,no.3,pp , 2008.
















7 MEDIATORS of INFLAMMATION The Scientific World Journal Gastroenterology Research and Practice Diabetes Research International Endocrinology Immunology Research Disease Markers Submit your manuscripts at BioMed Research International PPAR Research Obesity Ophthalmology Evidence-Based Complementary and Alternative Medicine Stem Cells International Oncology Parkinson s Disease Computational and Mathematical Methods in Medicine AIDS Behavioural Neurology Research and Treatment Oxidative Medicine and Cellular Longevity
Minimum Two-Year Follow-Up of Cases with Recurrent Disc Herniation Treated with Microdiscectomy and Posterior Dynamic Transpedicular Stabilisation
 120 The Open Orthopaedics Journal, 2010, 4, 120-125 Open Access Minimum Two-Year Follow-Up of Cases with Recurrent Disc Herniation Treated with Microdiscectomy and Posterior Dynamic Transpedicular Stabilisation
120 The Open Orthopaedics Journal, 2010, 4, 120-125 Open Access Minimum Two-Year Follow-Up of Cases with Recurrent Disc Herniation Treated with Microdiscectomy and Posterior Dynamic Transpedicular Stabilisation
Lumbar Single-Level Dynamic Stabilization with Semi-Rigid and Full Dynamic Systems: A Retrospective Clinical and Radiological Analysis of 71 Patients
 Original Article Clinics in Orthopedic Surgery 2017;9:310-316 https://doi.org/10.4055/cios.2017.9.3.310 Lumbar Single-Level Dynamic Stabilization with Semi-Rigid and Full Dynamic Systems: A Retrospective
Original Article Clinics in Orthopedic Surgery 2017;9:310-316 https://doi.org/10.4055/cios.2017.9.3.310 Lumbar Single-Level Dynamic Stabilization with Semi-Rigid and Full Dynamic Systems: A Retrospective
Lumbar Disc Prolapse. Dr. Ahmed Salah Eldin Hassan. Professor of Neurosurgery & Consultant spinal surgeon
 Lumbar Disc Prolapse By Dr. Ahmed Salah Eldin Hassan Professor of Neurosurgery & Consultant spinal surgeon 1-What are the Functions of the Spine Structural support for upright posture Protection of Spinal
Lumbar Disc Prolapse By Dr. Ahmed Salah Eldin Hassan Professor of Neurosurgery & Consultant spinal surgeon 1-What are the Functions of the Spine Structural support for upright posture Protection of Spinal
Case Report A Rare Case of Near Complete Regression of a Large Cervical Disc Herniation without Any Intervention Demonstrated on MRI
 Case Reports in Radiology, Article ID 832765, 4 pages http://dx.doi.org/10.1155/2014/832765 Case Report A Rare Case of Near Complete Regression of a Large Cervical Disc Herniation without Any Intervention
Case Reports in Radiology, Article ID 832765, 4 pages http://dx.doi.org/10.1155/2014/832765 Case Report A Rare Case of Near Complete Regression of a Large Cervical Disc Herniation without Any Intervention
Case Report Spontaneous Regression of Herniated Lumbar Disc with New Disc Protrusion in the Adjacent Level
 Case Reports in Orthopedics Volume 2016, Article ID 1538072, 4 pages http://dx.doi.org/10.1155/2016/1538072 Case Report Spontaneous Regression of Herniated Lumbar Disc with New Disc Protrusion in the Adjacent
Case Reports in Orthopedics Volume 2016, Article ID 1538072, 4 pages http://dx.doi.org/10.1155/2016/1538072 Case Report Spontaneous Regression of Herniated Lumbar Disc with New Disc Protrusion in the Adjacent
Case Report Adjacent Lumbar Disc Herniation after Lumbar Short Spinal Fusion
 Case Reports in Orthopedics, Article ID 456940, 4 pages http://dx.doi.org/10.1155/2014/456940 Case Report Adjacent Lumbar Disc Herniation after Lumbar Short Spinal Fusion Koshi Ninomiya, Koichi Iwatsuki,
Case Reports in Orthopedics, Article ID 456940, 4 pages http://dx.doi.org/10.1155/2014/456940 Case Report Adjacent Lumbar Disc Herniation after Lumbar Short Spinal Fusion Koshi Ninomiya, Koichi Iwatsuki,
Original Date: October 2015 LUMBAR SPINAL FUSION FOR
 National Imaging Associates, Inc. Clinical guidelines Original Date: October 2015 LUMBAR SPINAL FUSION FOR Page 1 of 9 INSTABILITY AND DEGENERATIVE DISC CONDITIONS FOR CMS (MEDICARE) MEMBERS ONLY CPT4
National Imaging Associates, Inc. Clinical guidelines Original Date: October 2015 LUMBAR SPINAL FUSION FOR Page 1 of 9 INSTABILITY AND DEGENERATIVE DISC CONDITIONS FOR CMS (MEDICARE) MEMBERS ONLY CPT4
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of insertion of an annular disc implant at lumbar discectomy The tough covering of
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of insertion of an annular disc implant at lumbar discectomy The tough covering of
*Il-Nam Son, MD, Young-Hoon Kim, MD, and Kee-Yong Ha, MD
 spine clinical article J Neurosurg Spine 22:179 184, 2015 Long-term clinical outcomes and radiological findings and their correlation with each other after standard open discectomy for lumbar disc herniation
spine clinical article J Neurosurg Spine 22:179 184, 2015 Long-term clinical outcomes and radiological findings and their correlation with each other after standard open discectomy for lumbar disc herniation
Dynamic Stabilization and Sports. Low back pain is a common problem with 60-80% of the world s population suffering from
 Dynamic Stabilization and Sports Assoc. Prof. Dr. Olcay ESER Prof. Dr. Ali Fahir ÖZER Low back pain is a common problem with 60-80% of the world s population suffering from low back pain (1). Although
Dynamic Stabilization and Sports Assoc. Prof. Dr. Olcay ESER Prof. Dr. Ali Fahir ÖZER Low back pain is a common problem with 60-80% of the world s population suffering from low back pain (1). Although
Case Report A Rare Case of Progressive Palsy of the Lower Leg Caused by a Huge Lumbar Posterior Endplate Lesion after Recurrent Disc Herniation
 Case Reports in Orthopedics Volume 2016, Article ID 5963924, 4 pages http://dx.doi.org/10.1155/2016/5963924 Case Report A Rare Case of Progressive Palsy of the Lower Leg Caused by a Huge Lumbar Posterior
Case Reports in Orthopedics Volume 2016, Article ID 5963924, 4 pages http://dx.doi.org/10.1155/2016/5963924 Case Report A Rare Case of Progressive Palsy of the Lower Leg Caused by a Huge Lumbar Posterior
Recurrent Lumbar Disk Herniation With or Without Posterolateral Fusion. Ahmed Zaater, MD, Alaa Azzazi, MD, Sameh Sakr, MD, and Ahmed Elsayed, MD
 ORIGINAL ARTICLE Recurrent Lumbar Disk Herniation With or Without Posterolateral Fusion Ahmed Zaater, MD, Alaa Azzazi, MD, Sameh Sakr, MD, and Ahmed Elsayed, MD Study Design: A prospective study assessing
ORIGINAL ARTICLE Recurrent Lumbar Disk Herniation With or Without Posterolateral Fusion Ahmed Zaater, MD, Alaa Azzazi, MD, Sameh Sakr, MD, and Ahmed Elsayed, MD Study Design: A prospective study assessing
ProDisc-L Total Disc Replacement. IDE Clinical Study.
 ProDisc-L Total Disc Replacement. IDE Clinical Study. A multi-center, prospective, randomized clinical trial. Instruments and implants approved by the AO Foundation Table of Contents Indications, Contraindications
ProDisc-L Total Disc Replacement. IDE Clinical Study. A multi-center, prospective, randomized clinical trial. Instruments and implants approved by the AO Foundation Table of Contents Indications, Contraindications
Patient Selection and Lumbar Operative Interventions
 Patient Selection and Lumbar Operative Interventions John C France MD Professor of Orthopaedic & Neurosurgery West Virginia University Low back pain is a symptom not a diagnosis Epidemiology of LBP General
Patient Selection and Lumbar Operative Interventions John C France MD Professor of Orthopaedic & Neurosurgery West Virginia University Low back pain is a symptom not a diagnosis Epidemiology of LBP General
Physician Reference Manual
 Nucleotome Physician Reference Manual Automated Percutaneous Lumbar Discectomy 900487-001-00, Page 1 Nucleotome Automated Percutaneous Lumbar Discectomy (APLD) Table of Contents Section 1 I. Description
Nucleotome Physician Reference Manual Automated Percutaneous Lumbar Discectomy 900487-001-00, Page 1 Nucleotome Automated Percutaneous Lumbar Discectomy (APLD) Table of Contents Section 1 I. Description
Long-term Follow-up Results of Percutaneous Endoscopic Lumbar Discectomy. Sang Soo Eun, MD, Sang Ho Lee, MD, PhD, and Luigi Andrew Sabal, MD
 Pain Physician 2016; 19:E1161-E1166 ISSN 2150-1149 Retrospective Evaluation Long-term Follow-up Results of Percutaneous Endoscopic Lumbar Discectomy Sang Soo Eun, MD, Sang Ho Lee, MD, PhD, and Luigi Andrew
Pain Physician 2016; 19:E1161-E1166 ISSN 2150-1149 Retrospective Evaluation Long-term Follow-up Results of Percutaneous Endoscopic Lumbar Discectomy Sang Soo Eun, MD, Sang Ho Lee, MD, PhD, and Luigi Andrew
Comprehension of the common spine disorder.
 Objectives Comprehension of the common spine disorder. Disc degeneration/hernia. Spinal stenosis. Common spinal deformity (Spondylolisthesis, Scoliosis). Osteoporotic fracture. Anatomy Anatomy Anatomy
Objectives Comprehension of the common spine disorder. Disc degeneration/hernia. Spinal stenosis. Common spinal deformity (Spondylolisthesis, Scoliosis). Osteoporotic fracture. Anatomy Anatomy Anatomy
Huan-Chieh Chen, 1 Chih-Hsun Lee, 1 Li Wei, 1 Tai-Ngar Lui, 1 and Tien-Jen Lin 1,2. 1. Introduction
 Neurology Research International Volume 2015, Article ID 791943, 5 pages http://dx.doi.org/10.1155/2015/791943 Clinical Study Comparison of Percutaneous Endoscopic Lumbar Discectomy and Open Lumbar Surgery
Neurology Research International Volume 2015, Article ID 791943, 5 pages http://dx.doi.org/10.1155/2015/791943 Clinical Study Comparison of Percutaneous Endoscopic Lumbar Discectomy and Open Lumbar Surgery
ProDisc-L Total Disc Replacement. IDE Clinical Study
 Total Disc Replacement IDE Clinical Study Study Design TDR vs. circumferential fusion: Multi-center, prospective, randomized trial 17 centers, 292 patients 162 patients 80 fusion patients 50 non-randomized
Total Disc Replacement IDE Clinical Study Study Design TDR vs. circumferential fusion: Multi-center, prospective, randomized trial 17 centers, 292 patients 162 patients 80 fusion patients 50 non-randomized
Spinal canal stenosis Degenerative diseases F 06
 What is spinal canal stenosis? The condition known as spinal canal stenosis is a narrowing (stenosis) of the spinal canal that in most cases develops due to the degenerative (wear-induced) deformation
What is spinal canal stenosis? The condition known as spinal canal stenosis is a narrowing (stenosis) of the spinal canal that in most cases develops due to the degenerative (wear-induced) deformation
Int J Clin Exp Med 2018;11(2): /ISSN: /IJCEM Yi Yang, Hao Liu, Yueming Song, Tao Li
: /ISSN: /IJCEM Yi Yang, Hao Liu, Yueming Song, Tao Li") Int J Clin Exp Med 2018;11(2):1278-1284 www.ijcem.com /ISSN:1940-5901/IJCEM0063093 Case Report Dislocation and screws pull-out after application of an Isobar TTL dynamic stabilisation system at L2/3 in
Int J Clin Exp Med 2018;11(2):1278-1284 www.ijcem.com /ISSN:1940-5901/IJCEM0063093 Case Report Dislocation and screws pull-out after application of an Isobar TTL dynamic stabilisation system at L2/3 in
A PROSPECTIVE STUDY OF INCIDENTAL DURAL TEARS IN MICROENDOSCOPIC LUMBAR DECOMPRESSION SURGERY: INCIDENCE AND OUTCOMES
 A PROSPECTIVE STUDY OF INCIDENTAL DURAL TEARS IN MICROENDOSCOPIC LUMBAR DECOMPRESSION SURGERY: INCIDENCE AND OUTCOMES Takahiro Tsutsumimoto, Mutsuki Yui, Masashi Uehara, Hiroki Ohba, Hiroshi Ohta, Hidemi
A PROSPECTIVE STUDY OF INCIDENTAL DURAL TEARS IN MICROENDOSCOPIC LUMBAR DECOMPRESSION SURGERY: INCIDENCE AND OUTCOMES Takahiro Tsutsumimoto, Mutsuki Yui, Masashi Uehara, Hiroki Ohba, Hiroshi Ohta, Hidemi
BARRICAID PROSTHESIS for Partial Anulus Replacement. Optimizing discectomy outcomes in high-risk patients. Prevent Reherniation. Preserve Disc.
 BARRICAID PROSTHESIS for Partial Anulus Replacement Optimizing discectomy outcomes in high-risk patients Prevent Reherniation. Preserve Disc. Today s standard discectomy is performed in such manner that
BARRICAID PROSTHESIS for Partial Anulus Replacement Optimizing discectomy outcomes in high-risk patients Prevent Reherniation. Preserve Disc. Today s standard discectomy is performed in such manner that
Waveflex elastic fixation and discectomy annulus in repair and reconstruction of spinal stability in patients with lumbar disc herniation
 19 44 20151022 Chinese Journal of Tissue Engineering Research October 22, 2015 Vol.19, No.44 Waveflex ( 221009) 1 Waveflex 2 3 Waveflex Waveflex (XZB201311) Waveflex Waveflex 38 18 Waveflex 20 (JOA)Oswestry
19 44 20151022 Chinese Journal of Tissue Engineering Research October 22, 2015 Vol.19, No.44 Waveflex ( 221009) 1 Waveflex 2 3 Waveflex Waveflex (XZB201311) Waveflex Waveflex 38 18 Waveflex 20 (JOA)Oswestry
POSTERIOR CERVICAL FUSION
 AN INTRODUCTION TO PCF POSTERIOR CERVICAL FUSION This booklet provides general information on the Posterior Cervical Fusion (PCF) surgical procedure for you to discuss with your physician. It is not meant
AN INTRODUCTION TO PCF POSTERIOR CERVICAL FUSION This booklet provides general information on the Posterior Cervical Fusion (PCF) surgical procedure for you to discuss with your physician. It is not meant
Byung-Joon Shin. Soonchunhyang University College of Medicine, Seoul, Korea
 Asian Spine Journal Asian Spine Review Journal Article Asian Spine J 2014;8(2):211-215 http://dx.doi.org/10.4184/asj.2014.8.2.211 Recurrent disc 211 Risk Factors for Recurrent Lumbar Disc Herniations Byung-Joon
Asian Spine Journal Asian Spine Review Journal Article Asian Spine J 2014;8(2):211-215 http://dx.doi.org/10.4184/asj.2014.8.2.211 Recurrent disc 211 Risk Factors for Recurrent Lumbar Disc Herniations Byung-Joon
ACDF. Anterior Cervical Discectomy and Fusion. An introduction to
 An introduction to ACDF Anterior Cervical Discectomy and Fusion This booklet provides general information on ACDF. It is not meant to replace any personal conversations that you might wish to have with
An introduction to ACDF Anterior Cervical Discectomy and Fusion This booklet provides general information on ACDF. It is not meant to replace any personal conversations that you might wish to have with
Microdiscectomy for the Treatment of Lumbar Disc Herniation: An Evaluation of Reoperations and Long-Term Outcomes
 Original Research 77 Microdiscectomy for the Treatment of Lumbar Disc Herniation: An Evaluation of Reoperations and Long-Term Outcomes Alexander Aichmair 1 Jerry Y. Du 1 Jennifer Shue 1 Gisberto Evangelisti
Original Research 77 Microdiscectomy for the Treatment of Lumbar Disc Herniation: An Evaluation of Reoperations and Long-Term Outcomes Alexander Aichmair 1 Jerry Y. Du 1 Jennifer Shue 1 Gisberto Evangelisti
Artificial intervertebral disc
 The University of Toledo The University of Toledo Digital Repository Master s and Doctoral Projects Artificial intervertebral disc Vikas Ghai Medical University of Ohio Follow this and additional works
The University of Toledo The University of Toledo Digital Repository Master s and Doctoral Projects Artificial intervertebral disc Vikas Ghai Medical University of Ohio Follow this and additional works
Lumbar Laminotomy DEFINING APPROPRIATE COVERAGE POSITIONS NASS COVERAGE POLICY RECOMMENDATIONS TASKFORCE
 NASS COVERAGE POLICY RECOMMENDATIONS Lumbar Laminotomy DEFINING APPROPRIATE COVERAGE POSITIONS North American Spine Society 7075 Veterans Blvd. Burr Ridge, IL 60527 TASKFORCE Introduction North American
NASS COVERAGE POLICY RECOMMENDATIONS Lumbar Laminotomy DEFINING APPROPRIATE COVERAGE POSITIONS North American Spine Society 7075 Veterans Blvd. Burr Ridge, IL 60527 TASKFORCE Introduction North American
Original Article Sequestrectomy versus microdiscectomy in the treatment of lumbar disc herniation: a meta-analysis
 Int J Clin Exp Med 2015;8(5):7261-7269 www.ijcem.com /ISSN:1940-5901/IJCEM0004641 Original Article Sequestrectomy versus microdiscectomy in the treatment of lumbar disc herniation: a meta-analysis Teng
Int J Clin Exp Med 2015;8(5):7261-7269 www.ijcem.com /ISSN:1940-5901/IJCEM0004641 Original Article Sequestrectomy versus microdiscectomy in the treatment of lumbar disc herniation: a meta-analysis Teng
Cervical intervertebral disc disease Degenerative diseases F 04
 Cervical intervertebral disc disease Degenerative diseases F 04 How is a herniated cervical intervertebral disc treated? Conservative treatment is generally sufficient for mild symptoms not complicated
Cervical intervertebral disc disease Degenerative diseases F 04 How is a herniated cervical intervertebral disc treated? Conservative treatment is generally sufficient for mild symptoms not complicated
LASE Efficacy and Safety More Effective Less Costly
 LASE Efficacy and Safety More Effective Less Costly Table of Contents Overview: A Product and a Technique for Percutaneous Lumbar Discectomy of Contained Herniations Discussion: A Product and a Technique
LASE Efficacy and Safety More Effective Less Costly Table of Contents Overview: A Product and a Technique for Percutaneous Lumbar Discectomy of Contained Herniations Discussion: A Product and a Technique
SPORT Lumbar Intervertebral Disk Herniation and Back Pain
 SPORT Lumbar Intervertebral Disk Herniation and Back Pain Does Treatment, Location, or Morphology Matter? Adam M. Pearson, MD, MS,* Emily A. Blood, MS,* John W. Frymoyer, MD,* Harry Herkowitz, MD, William
SPORT Lumbar Intervertebral Disk Herniation and Back Pain Does Treatment, Location, or Morphology Matter? Adam M. Pearson, MD, MS,* Emily A. Blood, MS,* John W. Frymoyer, MD,* Harry Herkowitz, MD, William
SpineFAQs. Neck Pain Diagnosis and Treatment
 SpineFAQs Neck Pain Diagnosis and Treatment Neck pain is a common reason people visit their doctor. Neck pain typically doesn't start from a single injury. Instead, the problem usually develops over time
SpineFAQs Neck Pain Diagnosis and Treatment Neck pain is a common reason people visit their doctor. Neck pain typically doesn't start from a single injury. Instead, the problem usually develops over time
Quality of Life. Quality of Motion. A Patient s Guide to. Artificial Lumbar Disc Replacement
 Quality of Life. Quality of Motion. A Patient s Guide to Artificial Lumbar Disc Replacement Each year, hundreds of thousands of adults are diagnosed with Lumbar Disc Degeneration, a lower spine condition
Quality of Life. Quality of Motion. A Patient s Guide to Artificial Lumbar Disc Replacement Each year, hundreds of thousands of adults are diagnosed with Lumbar Disc Degeneration, a lower spine condition
Herniated Disk in the Lower Back
 Herniated Disk in the Lower Back This article is also available in Spanish: Hernia de disco en la columna lumbar (topic.cfm?topic=a00730). Sometimes called a slipped or ruptured disk, a herniated disk
Herniated Disk in the Lower Back This article is also available in Spanish: Hernia de disco en la columna lumbar (topic.cfm?topic=a00730). Sometimes called a slipped or ruptured disk, a herniated disk
Patient Information ACDF. Anterior Cervical Discectomy and Fusion
 Patient Information ACDF Anterior Cervical Discectomy and Fusion Table of Contents Anatomy of the Spine...2-3 General Conditions of the Cervical Spine...4 5 What is an ACDF?...6 How is an ACDF performed?...7
Patient Information ACDF Anterior Cervical Discectomy and Fusion Table of Contents Anatomy of the Spine...2-3 General Conditions of the Cervical Spine...4 5 What is an ACDF?...6 How is an ACDF performed?...7
Back Pain Policies Summary
 Back Pain Policies Summary These policies are part of the wider project, Reviewing local health policies, which is reviewing and updating more than 100 policies, of which back pain are part of. This review
Back Pain Policies Summary These policies are part of the wider project, Reviewing local health policies, which is reviewing and updating more than 100 policies, of which back pain are part of. This review
Case Report Intra-Articular Entrapment of the Medial Epicondyle following a Traumatic Fracture Dislocation of the Elbow in an Adult
 Hindawi Case Reports in Orthopedics Volume 2018, Article ID 5401634, 6 pages https://doi.org/10.1155/2018/5401634 Case Report Intra-Articular Entrapment of the Medial Epicondyle following a Traumatic Fracture
Hindawi Case Reports in Orthopedics Volume 2018, Article ID 5401634, 6 pages https://doi.org/10.1155/2018/5401634 Case Report Intra-Articular Entrapment of the Medial Epicondyle following a Traumatic Fracture
Kinematic Cervical Spine Magnetic Resonance Imaging in Low-Impact Trauma Assessment
 Kinematic Cervical Spine Magnetic Resonance Imaging in Low-Impact Trauma Assessment 1 Seminars in Ultrasound, CT, and MRI June 2009; Volume 30; Number 3; pp. 168-173 Vincenzo Giuliano, MD, Antonio Pinto,
Kinematic Cervical Spine Magnetic Resonance Imaging in Low-Impact Trauma Assessment 1 Seminars in Ultrasound, CT, and MRI June 2009; Volume 30; Number 3; pp. 168-173 Vincenzo Giuliano, MD, Antonio Pinto,
Degenerative Disease of the Spine
 Degenerative Disease of the Spine Introduction: I. Anatomy Talk Overview II. Overview of Disease Processes: A. Spondylosis B. Intervertebral Disc Disease III. Diagnosis IV. Therapy Introduction: Myelopathy
Degenerative Disease of the Spine Introduction: I. Anatomy Talk Overview II. Overview of Disease Processes: A. Spondylosis B. Intervertebral Disc Disease III. Diagnosis IV. Therapy Introduction: Myelopathy
RETROLISTHESIS. Retrolisthesis. is found mainly in the cervical spine and lumbar region but can also be often seen in the thoracic spine
 RETROLISTHESIS A retrolisthesis is a posterior displacement of one vertebral body with respect to adjacent vertebrae Typically a vertebra is to be in retrolisthesis position when it translates backward
RETROLISTHESIS A retrolisthesis is a posterior displacement of one vertebral body with respect to adjacent vertebrae Typically a vertebra is to be in retrolisthesis position when it translates backward
Objectives. Comprehension of the common spine disorder
 Objectives Comprehension of the common spine disorder Disc degeneration/hernia Spinal stenosis Common spinal deformity (Spondylolisthesis, Scoliosis) Osteoporotic fracture Destructive spinal lesions Anatomy
Objectives Comprehension of the common spine disorder Disc degeneration/hernia Spinal stenosis Common spinal deformity (Spondylolisthesis, Scoliosis) Osteoporotic fracture Destructive spinal lesions Anatomy
A Patient s Guide to Artificial Cervical Disc Replacement
 A Patient s Guide to Artificial Cervical Disc Replacement Each year, hundreds of thousands of adults are diagnosed with Cervical Disc Degeneration, an upper spine condition that can cause pain and numbness
A Patient s Guide to Artificial Cervical Disc Replacement Each year, hundreds of thousands of adults are diagnosed with Cervical Disc Degeneration, an upper spine condition that can cause pain and numbness
Lumbar disc reherniation after transforaminal lumbar endoscopic discectomy
 Original Article Page 1 of 5 Lumbar disc reherniation after transforaminal lumbar endoscopic discectomy Thomas A. Kosztowski, David Choi, Jared Fridley, Michael Galgano, Ziya Gokaslan, Adetokunbo Oyelese,
Original Article Page 1 of 5 Lumbar disc reherniation after transforaminal lumbar endoscopic discectomy Thomas A. Kosztowski, David Choi, Jared Fridley, Michael Galgano, Ziya Gokaslan, Adetokunbo Oyelese,
Corporate Medical Policy
 Corporate Medical Policy Image-Guided Minimally Invasive Decompression (IG-MLD) for File Name: Origination: Last CAP Review: Next CAP Review: Last Review: image-guided_minimally_invasive_decompression_for_spinal_stenosis
Corporate Medical Policy Image-Guided Minimally Invasive Decompression (IG-MLD) for File Name: Origination: Last CAP Review: Next CAP Review: Last Review: image-guided_minimally_invasive_decompression_for_spinal_stenosis
Case Report Reverse Segond Fracture Associated with Anteromedial Tibial Rim and Tibial Attachment of Anterior Cruciate Ligament Avulsion Fractures
 Hindawi Case Reports in Orthopedics Volume 2017, Article ID 9637153, 4 pages https://doi.org/10.1155/2017/9637153 Case Report Reverse Segond Fracture Associated with Anteromedial Tibial Rim and Tibial
Hindawi Case Reports in Orthopedics Volume 2017, Article ID 9637153, 4 pages https://doi.org/10.1155/2017/9637153 Case Report Reverse Segond Fracture Associated with Anteromedial Tibial Rim and Tibial
The main causes of cervical radiculopathy include degeneration, disc herniation, and spinal instability.
 SpineFAQs Cervical Radiculopathy Neck pain has many causes. Mechanical neck pain comes from injury or inflammation in the soft tissues of the neck. This is much different and less concerning than symptoms
SpineFAQs Cervical Radiculopathy Neck pain has many causes. Mechanical neck pain comes from injury or inflammation in the soft tissues of the neck. This is much different and less concerning than symptoms
DEGENERATIVE SPINAL DISEASE PRABIN SHRESTHA ANISH M SINGH B&B HOSPITAL
 SPINAL CHAPTER, NESON DEGENERATIVE SPINAL DISEASE PRABIN SHRESTHA ANISH M SINGH B&B HOSPITAL INTRODUCTION DEGENERATIVE SPINAL DISEASE Gradual loss of normal structure and function of spine with time Also
SPINAL CHAPTER, NESON DEGENERATIVE SPINAL DISEASE PRABIN SHRESTHA ANISH M SINGH B&B HOSPITAL INTRODUCTION DEGENERATIVE SPINAL DISEASE Gradual loss of normal structure and function of spine with time Also
Research Article Relationship between Pain and Medial Meniscal Extrusion in Knee Osteoarthritis
 Advances in Orthopedics Volume 2015, Article ID 210972, 4 pages http://dx.doi.org/10.1155/2015/210972 Research Article Relationship between Pain and Medial Meniscal Extrusion in Knee Osteoarthritis Hiroaki
Advances in Orthopedics Volume 2015, Article ID 210972, 4 pages http://dx.doi.org/10.1155/2015/210972 Research Article Relationship between Pain and Medial Meniscal Extrusion in Knee Osteoarthritis Hiroaki
Kanji Mori, Kazuya Nishizawa, Akira Nakamura, and Shinji Imai. 1. Introduction. 2. Case Presentation
 Case Reports in Orthopedics Volume 2015, Article ID 301858, 4 pages http://dx.doi.org/10.1155/2015/301858 Case Report Atraumatic Occult Odontoid Fracture in Patients with Osteoporosis-Associated Thoracic
Case Reports in Orthopedics Volume 2015, Article ID 301858, 4 pages http://dx.doi.org/10.1155/2015/301858 Case Report Atraumatic Occult Odontoid Fracture in Patients with Osteoporosis-Associated Thoracic
REFERENCE DOCTOR Percutaneous Endoscopic Discectomy Transforaminal / Interlaminar. Hyeun Sung Kim, MD, PhD,
 Percutaneous Endoscopic Discectomy Transforaminal / Interlaminar Medical College of Chosun University, Gwangju, South Korea (1994) / Board of Neurosurgery (1999) MEMBERSHIPS & PROFESSIONAL SOCIETIES Korean
Percutaneous Endoscopic Discectomy Transforaminal / Interlaminar Medical College of Chosun University, Gwangju, South Korea (1994) / Board of Neurosurgery (1999) MEMBERSHIPS & PROFESSIONAL SOCIETIES Korean
Case Report Double-Layered Lateral Meniscus Accompanied by Meniscocapsular Separation
 Case Reports in Orthopedics Volume 2015, Article ID 357463, 5 pages http://dx.doi.org/10.1155/2015/357463 Case Report Double-Layered Lateral Meniscus Accompanied by Meniscocapsular Separation Aki Fukuda,
Case Reports in Orthopedics Volume 2015, Article ID 357463, 5 pages http://dx.doi.org/10.1155/2015/357463 Case Report Double-Layered Lateral Meniscus Accompanied by Meniscocapsular Separation Aki Fukuda,
Medical Policy Original Effective Date: Revised Date: Page 1 of 11
 Page 1 of 11 Content Disclaimer Description Coverage Determination Clinical Indications Lumbar Spine Surgery Lumbar Spine Surgery Description Indication Coding Lumbar Spinal Fusion (single level)surgery
Page 1 of 11 Content Disclaimer Description Coverage Determination Clinical Indications Lumbar Spine Surgery Lumbar Spine Surgery Description Indication Coding Lumbar Spinal Fusion (single level)surgery
Clinical Study Skipping Posterior Dynamic Transpedicular Stabilization for Distant Segment Degenerative Disease
 Advances in Orthopedics Volume 2012, Article ID 496817, 7 pages doi:10.1155/2012/496817 Clinical Study Skipping Posterior Dynamic Transpedicular Stabilization for Distant Segment Degenerative Disease Bilgehan
Advances in Orthopedics Volume 2012, Article ID 496817, 7 pages doi:10.1155/2012/496817 Clinical Study Skipping Posterior Dynamic Transpedicular Stabilization for Distant Segment Degenerative Disease Bilgehan
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of percutaneous coblation of the intervertebral disc for low back pain and sciatica
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of percutaneous coblation of the intervertebral disc for low back pain and sciatica
Lumbar disc herniation
 Lumbar disc herniation Thomas Kishen Spine Surgeon Sparsh Hospital for Advanced Surgeries Bangalore Symptoms and Signs Radicular Pain in the distribution of the involved nerve Neurological deficit motor,
Lumbar disc herniation Thomas Kishen Spine Surgeon Sparsh Hospital for Advanced Surgeries Bangalore Symptoms and Signs Radicular Pain in the distribution of the involved nerve Neurological deficit motor,
The Role of Surgery in the Treatment of Low Back Pain and Radiculopathy. Christian Etter, MD, Spine Surgeon Zürich, Switzerland
 The Role of Surgery in the Treatment of Low Back Pain and Radiculopathy Christian Etter, MD, Spine Surgeon Zürich, Switzerland WW Fusion Volume by Disorder 2004E % Tumor/Trauma 11% Deformity 15% Degeneration
The Role of Surgery in the Treatment of Low Back Pain and Radiculopathy Christian Etter, MD, Spine Surgeon Zürich, Switzerland WW Fusion Volume by Disorder 2004E % Tumor/Trauma 11% Deformity 15% Degeneration
GECO 2010 LES-ARCS FRANCE LP-ESP II Elastic Spine PAD2 FH-ORTHOPEDICS
 GECO 2010 LES-ARCS FRANCE LP-ESP II Elastic Spine PAD2 FH-ORTHOPEDICS First results with 100 implanted LP-ESP after one year Klinikum Leer Departement of Spinal Surgery Germany Dr. med. Hamid Afshar Klinikum
GECO 2010 LES-ARCS FRANCE LP-ESP II Elastic Spine PAD2 FH-ORTHOPEDICS First results with 100 implanted LP-ESP after one year Klinikum Leer Departement of Spinal Surgery Germany Dr. med. Hamid Afshar Klinikum
DEGENERATIVE SPONDYLOLISTHESIS
 AN INTRODUCTION TO DEGENERATIVE SPONDYLOLISTHESIS This booklet is designed to inform you about lumbar degenerative spondylolisthesis. It is not meant to replace any personal conversations that you might
AN INTRODUCTION TO DEGENERATIVE SPONDYLOLISTHESIS This booklet is designed to inform you about lumbar degenerative spondylolisthesis. It is not meant to replace any personal conversations that you might
Index 377 Index A Alajouanine, T. H., 6 Ancient medicine, management of back and leg pain, 1 3 Anesthesia, microendoscopic discectomy, 364, 365 minima
 Index 377 Index A Alajouanine, T. H., 6 Ancient medicine, management of back and leg pain, 1 3 Anesthesia, microendoscopic discectomy, 364, 365 minimally invasive lumbar surgery, 75, 76 percutaneous transpedicular
Index 377 Index A Alajouanine, T. H., 6 Ancient medicine, management of back and leg pain, 1 3 Anesthesia, microendoscopic discectomy, 364, 365 minimally invasive lumbar surgery, 75, 76 percutaneous transpedicular
This procedure lacks scientific evidence of effectiveness, and is not covered.
 ARBenefits Approval: 09-21-2011 Effective Date: 01-01-2012 Revision Date: Code(s): 0275T Medical Policy Title: Minimally Invasive, Image-Guided Lumbar Decompression for Spinal Stenosis Document: ARB0186
ARBenefits Approval: 09-21-2011 Effective Date: 01-01-2012 Revision Date: Code(s): 0275T Medical Policy Title: Minimally Invasive, Image-Guided Lumbar Decompression for Spinal Stenosis Document: ARB0186
Case Report Bilateral Distal Femoral Nailing in a Rare Symmetrical Periprosthetic Knee Fracture
 Case Reports in Orthopedics, Article ID 745083, 4 pages http://dx.doi.org/10.1155/2014/745083 Case Report Bilateral Distal Femoral Nailing in a Rare Symmetrical Periprosthetic Knee Fracture Marcos Carvalho,
Case Reports in Orthopedics, Article ID 745083, 4 pages http://dx.doi.org/10.1155/2014/745083 Case Report Bilateral Distal Femoral Nailing in a Rare Symmetrical Periprosthetic Knee Fracture Marcos Carvalho,
Case Report Pediatric Transepiphyseal Seperation and Dislocation of the Femoral Head
 Case Reports in Orthopedics Volume 2013, Article ID 703850, 4 pages http://dx.doi.org/10.1155/2013/703850 Case Report Pediatric Transepiphyseal Seperation and Dislocation of the Femoral Head Mehmet Elmadag,
Case Reports in Orthopedics Volume 2013, Article ID 703850, 4 pages http://dx.doi.org/10.1155/2013/703850 Case Report Pediatric Transepiphyseal Seperation and Dislocation of the Femoral Head Mehmet Elmadag,
Cox Technic Case Report #169 published at (sent 5/9/17) 1
 1") Cox Technic Case Report #169 published at www.coxtechnic.com (sent 5/9/17) 1 Management of Lumbar Radiculopathy Associated with an Extruded L4 L5 disc and concurrent L5 S1 Spondylolytic Spondylolisthesis
Cox Technic Case Report #169 published at www.coxtechnic.com (sent 5/9/17) 1 Management of Lumbar Radiculopathy Associated with an Extruded L4 L5 disc and concurrent L5 S1 Spondylolytic Spondylolisthesis
Open Discectomy. North American Spine Society Public Education Series
 Open Discectomy North American Spine Society Public Education Series What Is Open Discectomy? Open discectomy is the most common surgical treatment for ruptured or herniated discs of the lumbar spine.
Open Discectomy North American Spine Society Public Education Series What Is Open Discectomy? Open discectomy is the most common surgical treatment for ruptured or herniated discs of the lumbar spine.
Foraminoplastic transfacet epidural endoscopic approach for removal of intraforaminal disc herniation at the L5-S1 level
 Case report Videosurgery Foraminoplastic transfacet epidural endoscopic approach for removal of intraforaminal disc herniation at the L5-S1 level Łukasz Kubaszewski 1, Jacek Kaczmarczyk 1, Andrzej Nowakowski
Case report Videosurgery Foraminoplastic transfacet epidural endoscopic approach for removal of intraforaminal disc herniation at the L5-S1 level Łukasz Kubaszewski 1, Jacek Kaczmarczyk 1, Andrzej Nowakowski
Initial Clinical Outcomes of Percutaneous Full- Endoscopic Lumbar Discectomy Using an Interlaminar Approach at the L4-L5
 Pain Physician 2017; 20:E507-E512 ISSN 2150-1149 Retrospective Evaluation Initial Clinical Outcomes of Percutaneous Full- Endoscopic Lumbar Discectomy Using an Interlaminar Approach at the L4-L5 Jun-ichiro
Pain Physician 2017; 20:E507-E512 ISSN 2150-1149 Retrospective Evaluation Initial Clinical Outcomes of Percutaneous Full- Endoscopic Lumbar Discectomy Using an Interlaminar Approach at the L4-L5 Jun-ichiro
Fusion and repeat discectomy following single level open lumbar discectomies. Survival analysis
 Fusion and repeat discectomy following single level open lumbar discectomies. Survival analysis Dr John Mortimer Mr Chris Hoffman CCDHB and TBI Health group Sciatica = Leg Dominant Pain Patients referred
Fusion and repeat discectomy following single level open lumbar discectomies. Survival analysis Dr John Mortimer Mr Chris Hoffman CCDHB and TBI Health group Sciatica = Leg Dominant Pain Patients referred
QF-78. S. Tanaka 1, T.Yokoyama 1, K.Takeuchi 1, K.Wada 2, T. Tanaka 2, S.Abrakawa 2, G.Kumagai 2, T.Asari 2, A.Ono 2, Y.
 QF-78 Patient-oriented outcomes after musclepreserving interlaminar decompression for patients with lumbar spinal canal stenosis: Multi-center study to identify risk factors for poor outcomes S. Tanaka
QF-78 Patient-oriented outcomes after musclepreserving interlaminar decompression for patients with lumbar spinal canal stenosis: Multi-center study to identify risk factors for poor outcomes S. Tanaka
Lumbar disc prolapse. Done by : Areej Al-Hadidi
 Lumbar disc prolapse Done by : Areej Al-Hadidi Anatomy of IVD IVD is composed of two components: 1. anulus fibrosus : it is the outer fibrous layer (fibrocartilage ) **It is comressible &tough 2. nucleus
Lumbar disc prolapse Done by : Areej Al-Hadidi Anatomy of IVD IVD is composed of two components: 1. anulus fibrosus : it is the outer fibrous layer (fibrocartilage ) **It is comressible &tough 2. nucleus
Posterior. Lumbar Fusion. Disclaimer. Integrated web marketing. Multimedia Health Education
 Posterior Lumbar Fusion Disclaimer This movie is an educational resource only and should not be used to make a decision on. All decisions about surgery must be made in conjunction with your surgeon or
Posterior Lumbar Fusion Disclaimer This movie is an educational resource only and should not be used to make a decision on. All decisions about surgery must be made in conjunction with your surgeon or
Case Report Successful Closed Reduction of a Lateral Elbow Dislocation
 Case Reports in Orthopedics Volume 2016, Article ID 5934281, 5 pages http://dx.doi.org/10.1155/2016/5934281 Case Report Successful Closed Reduction of a Lateral Elbow Dislocation Kenya Watanabe, Takuma
Case Reports in Orthopedics Volume 2016, Article ID 5934281, 5 pages http://dx.doi.org/10.1155/2016/5934281 Case Report Successful Closed Reduction of a Lateral Elbow Dislocation Kenya Watanabe, Takuma
Pathophysiology of lumbar disc degeneration: a review of the literature. Neurosurg Focus 13 (2): August, 2002
: August, 2002") Pathophysiology of lumbar disc degeneration: a review of the literature Neurosurg Focus 13 (2): August, 2002 MICHAEL D. MARTIN, M.D., CHRISTOPHER M. BOXELL, M.D., F.A.C.S., AND DAVID G. MALONE, M.D. FROM
Pathophysiology of lumbar disc degeneration: a review of the literature Neurosurg Focus 13 (2): August, 2002 MICHAEL D. MARTIN, M.D., CHRISTOPHER M. BOXELL, M.D., F.A.C.S., AND DAVID G. MALONE, M.D. FROM
paracentral disc herniations, especially disc extrusions and disc sequestrations, remains challenging.
 Orthopaedic Surgery SURGICAL TECHNOLOGY INTERNATIONAL XIX Transforaminal Endoscopic Lumbar Procedure for Disc Herniations: A "Between" Technique KAI-XUAN LIU, M.D, PH.D. ATLANTIC SPINAL CARE EDISON, NEW
Orthopaedic Surgery SURGICAL TECHNOLOGY INTERNATIONAL XIX Transforaminal Endoscopic Lumbar Procedure for Disc Herniations: A "Between" Technique KAI-XUAN LIU, M.D, PH.D. ATLANTIC SPINAL CARE EDISON, NEW
Original Article Management of Single Level Lumbar Degenerative Spondylolisthesis: Decompression Alone or Decompression and Fusion
 Egyptian Journal of Neurosurgery Volume 9 / No. 4 / October - December 014 51-56 Original Article Management of Single Level Lumbar Degenerative Spondylolisthesis: Decompression Alone or Decompression
Egyptian Journal of Neurosurgery Volume 9 / No. 4 / October - December 014 51-56 Original Article Management of Single Level Lumbar Degenerative Spondylolisthesis: Decompression Alone or Decompression
Erginousakis D et al. Radiology 2011;260:
 Comparative Prospective Randomized Study Comparing Conservative Treatment and Percutaneous Disk Decompression for Treatment of Intervertebral Disk Herniation Erginousakis D et al. Radiology 2011;260:487-493
Comparative Prospective Randomized Study Comparing Conservative Treatment and Percutaneous Disk Decompression for Treatment of Intervertebral Disk Herniation Erginousakis D et al. Radiology 2011;260:487-493
Departement of Neurosurgery A.O.R.N A. Cardarelli- Naples.
 Percutaneous posterior pedicle screw fixation in the treatment of thoracic, lumbar and thoraco-lumbar junction (T12-L1) traumatic and pathological spine fractures. Report of 45 cases. G. Vitale, A. Punzo,
Percutaneous posterior pedicle screw fixation in the treatment of thoracic, lumbar and thoraco-lumbar junction (T12-L1) traumatic and pathological spine fractures. Report of 45 cases. G. Vitale, A. Punzo,
ProDisc-C versus fusion with Cervios chronos prosthesis in cervical degenerative disc disease: Is there a difference at 12 months?
 Original research ProDisc-C versus fusion with Cervios chronos prosthesis in cervical degenerative disc ( ) 51 51 56 ProDisc-C versus fusion with Cervios chronos prosthesis in cervical degenerative disc
Original research ProDisc-C versus fusion with Cervios chronos prosthesis in cervical degenerative disc ( ) 51 51 56 ProDisc-C versus fusion with Cervios chronos prosthesis in cervical degenerative disc
Posterior surgical procedures are those procedures
 9 Cervical Posterior surgical procedures are those procedures that have been in use for a long time with established efficacy in the treatment of radiculopathy and myelopathy caused by pathologies including
9 Cervical Posterior surgical procedures are those procedures that have been in use for a long time with established efficacy in the treatment of radiculopathy and myelopathy caused by pathologies including
The ABC s of LUMBAR SPINE DISEASE
 The ABC s of LUMBAR SPINE DISEASE Susan O. Smith ANP-BC University of Rochester Department of Neurological Surgery Diagnosis/Imaging/Surgery of Lumbar Spine Disorders Objectives Identify the most common
The ABC s of LUMBAR SPINE DISEASE Susan O. Smith ANP-BC University of Rochester Department of Neurological Surgery Diagnosis/Imaging/Surgery of Lumbar Spine Disorders Objectives Identify the most common
Key Primary CPT Codes: Refer to pages: 7-9 Last Review Date: October 2016 Medical Coverage Guideline Number:
 National Imaging Associates, Inc. Clinical guidelines CERVICAL SPINE SURGERY: ANTERI CERVICAL DECOMPRESSION WITH FUSION CERVICAL POSTERI DECOMPRESSION WITH FUSION CERVICAL ARTIFICIAL DISC CERVICAL POSTERI
National Imaging Associates, Inc. Clinical guidelines CERVICAL SPINE SURGERY: ANTERI CERVICAL DECOMPRESSION WITH FUSION CERVICAL POSTERI DECOMPRESSION WITH FUSION CERVICAL ARTIFICIAL DISC CERVICAL POSTERI
EFSPINE CERVICAL COMBINED SET DISC PROTHESIS ORGANIZER BOX
 EFSPINE CERVICAL COMBINED SET INSTRUMENTS CERVICAL CAGE & DISC PROTHESIS ORGANIZER BOX Cervical Thoracic Thoraco - Lumbar Sacral EFSPINE CERVICAL COMBINED SET CERVICAL IMPLANTS INTRODUCTION Cervical Disc
EFSPINE CERVICAL COMBINED SET INSTRUMENTS CERVICAL CAGE & DISC PROTHESIS ORGANIZER BOX Cervical Thoracic Thoraco - Lumbar Sacral EFSPINE CERVICAL COMBINED SET CERVICAL IMPLANTS INTRODUCTION Cervical Disc
North American Spine Society Public Education Series
 Herniated Lumbar Disc North American Spine Society Public Education Series What Is a Herniated Disc? The spine is made up of a series of connected bones called vertebrae. The disc is a combination of strong
Herniated Lumbar Disc North American Spine Society Public Education Series What Is a Herniated Disc? The spine is made up of a series of connected bones called vertebrae. The disc is a combination of strong
Virginia Spine Institute - FAQs
 Virginia Spine Institute - FAQs 1. What are common causes of back pain? Back pain is one of the most common ailments known to man. Approximately 80% of the adult population will develop a significant episode
Virginia Spine Institute - FAQs 1. What are common causes of back pain? Back pain is one of the most common ailments known to man. Approximately 80% of the adult population will develop a significant episode
Am I eligible for the TOPS study? Possibly, if you suffer from one or more of the following conditions:
 Am I eligible for the TOPS study? Possibly, if you suffer from one or more of the following conditions: Radiating leg pain Greater leg / buttock pain than back pain Severe pain sets in when walking as
Am I eligible for the TOPS study? Possibly, if you suffer from one or more of the following conditions: Radiating leg pain Greater leg / buttock pain than back pain Severe pain sets in when walking as
It consist of two components: the outer, laminar fibrous container (or annulus), and the inner, semifluid mass (the nucleus pulposus).
, and the inner, semifluid mass (the nucleus pulposus).") Lumbar Spine The lumbar vertebrae are the last five vertebrae of the vertebral column. They are particularly large and heavy when compared with the vertebrae of the cervical or thoracicc spine. Their bodies
Lumbar Spine The lumbar vertebrae are the last five vertebrae of the vertebral column. They are particularly large and heavy when compared with the vertebrae of the cervical or thoracicc spine. Their bodies
Case Report Medial Radial Head Dislocation Associated with a Proximal Olecranon Fracture: A Bado Type V?
 Case Reports in Surgery, Article ID 723756, 4 pages http://dx.doi.org/10.1155/2014/723756 Case Report Medial Radial Head Dislocation Associated with a Proximal Olecranon Fracture: A Bado Type V? Neil Segaren,
Case Reports in Surgery, Article ID 723756, 4 pages http://dx.doi.org/10.1155/2014/723756 Case Report Medial Radial Head Dislocation Associated with a Proximal Olecranon Fracture: A Bado Type V? Neil Segaren,
Jessica Jameson MD Post Falls, ID
 Jessica Jameson MD Post Falls, ID Discuss the history of interventiona l pain Discuss previous tools to manage chronic pain Discuss current novel therapies to manage chronic pain and indications HISTORY
Jessica Jameson MD Post Falls, ID Discuss the history of interventiona l pain Discuss previous tools to manage chronic pain Discuss current novel therapies to manage chronic pain and indications HISTORY
Review date: February Lumbar Discectomy
 Review date: February 2019 Lumbar Discectomy Following your recent MRI scan and consultation with your spinal surgeon, you have been diagnosed as having a lumbar disc protrusion, resulting in nerve root
Review date: February 2019 Lumbar Discectomy Following your recent MRI scan and consultation with your spinal surgeon, you have been diagnosed as having a lumbar disc protrusion, resulting in nerve root
3D titanium interbody fusion cages sharx. White Paper
 3D titanium interbody fusion cages sharx (SLM selective laser melted) Goal of the study: Does the sharx intervertebral cage due to innovative material, new design, and lordotic shape solve some problems
3D titanium interbody fusion cages sharx (SLM selective laser melted) Goal of the study: Does the sharx intervertebral cage due to innovative material, new design, and lordotic shape solve some problems
Corporate Medical Policy
 Corporate Medical Policy Epidural Steroid Injections for Back Pain File Name: Origination: Last CAP Review: Next CAP Review: Last Review: epidural_steroid_injections_for_back_pain 2/2016 4/2017 4/2018
Corporate Medical Policy Epidural Steroid Injections for Back Pain File Name: Origination: Last CAP Review: Next CAP Review: Last Review: epidural_steroid_injections_for_back_pain 2/2016 4/2017 4/2018
Get back to: my life. Non-fusion treatment for lumbar spinal stenosis
 Get back to: my life Non-fusion treatment for lumbar spinal stenosis Do you have any of these symptoms? numbness, weakness or pain in the lower legs When any of these conditions occur, the spinal nerve,
Get back to: my life Non-fusion treatment for lumbar spinal stenosis Do you have any of these symptoms? numbness, weakness or pain in the lower legs When any of these conditions occur, the spinal nerve,
Case Report Synovial Cyst Mimicking an Intraspinal Sacral Mass
 , Article ID 953579, 4 pages http://dx.doi.org/10.1155/2014/953579 Case Report Synovial Cyst Mimicking an Intraspinal Sacral Mass Jason Hoover 1,2 and Stephen Pirris 3 1 The Texas Brain and Spine Institute,
, Article ID 953579, 4 pages http://dx.doi.org/10.1155/2014/953579 Case Report Synovial Cyst Mimicking an Intraspinal Sacral Mass Jason Hoover 1,2 and Stephen Pirris 3 1 The Texas Brain and Spine Institute,
NUCLEOPLASTY PERCUTANEOUS DISC DECOMPRESSION
 NUCLEOPLASTY PERCUTANEOUS DISC DECOMPRESSION ISSUE Blue Shield has received requests for coverage of nucleoplasty percutaneous disc decompression for herniated discs. The Medical Policy Committee on Quality
NUCLEOPLASTY PERCUTANEOUS DISC DECOMPRESSION ISSUE Blue Shield has received requests for coverage of nucleoplasty percutaneous disc decompression for herniated discs. The Medical Policy Committee on Quality
HERNIATED DISCS AN INTRODUCTION TO
 AN INTRODUCTION TO HERNIATED S This booklet provides general information on herniated discs. It is not meant to replace any personal conversations that you might wish to have with your physician or other
AN INTRODUCTION TO HERNIATED S This booklet provides general information on herniated discs. It is not meant to replace any personal conversations that you might wish to have with your physician or other
Surgery in cervical disc herniation: anterior cervical discectomy without fusion or with fusion
 Romanian Neurosurgery Volume XXXI Number 1 2017 January - March Article Surgery in cervical disc herniation: anterior cervical discectomy without fusion or with fusion Andrei Stefan Iencean ROMANIA DOI:
Romanian Neurosurgery Volume XXXI Number 1 2017 January - March Article Surgery in cervical disc herniation: anterior cervical discectomy without fusion or with fusion Andrei Stefan Iencean ROMANIA DOI:
2/5/2019. Facet Joint Pain. Biomechanics
 Facet Arthropathy as a Pain Source Evaluation and Management Shelby Spine Jan 31 st Feb 2 nd, 2019 Kushagra Verma MD, MS Adult and Pediatric Scoliosis And Spine Deformity Beach Orthopaedics Specialty Institute
Facet Arthropathy as a Pain Source Evaluation and Management Shelby Spine Jan 31 st Feb 2 nd, 2019 Kushagra Verma MD, MS Adult and Pediatric Scoliosis And Spine Deformity Beach Orthopaedics Specialty Institute
LUMBAR MICRODISCECTOMY: TECHNIQUE, ADVANTAGES AND OUTCOMES. SURABAYA EXPERIENCE ON 83 PATIENTS
 Lumbar Microdiscectomy: Technique, Advantages and Outcomes. Surabaya Experience on 83 Patients (Abdul Hafid Bajamal) LUMBAR MICRODISCECTOMY: TECHNIQUE, ADVANTAGES AND OUTCOMES. SURABAYA EXPERIENCE ON 83
Lumbar Microdiscectomy: Technique, Advantages and Outcomes. Surabaya Experience on 83 Patients (Abdul Hafid Bajamal) LUMBAR MICRODISCECTOMY: TECHNIQUE, ADVANTAGES AND OUTCOMES. SURABAYA EXPERIENCE ON 83