Prescription Opioids in Vermont A DISCUSSION ABOUT LAWS AND GUIDELINES MICHAEL J. KENOSH, MD
|
|
|
- Moses Collins
- 5 years ago
- Views:
Transcription
1 Prescription Opioids in Vermont A DISCUSSION ABOUT LAWS AND GUIDELINES MICHAEL J. KENOSH, MD
2 Rule(s) Governing the Prescribing of Opioids for Pain KEY rule adopted pursuant to Sections 14(e) and 11(e) of Act 75 (2013) and Sections 2(e) and 2a of Act 173 (2016). CDC guideline Areas of change with stakeholder input Area not changed despite stakeholder input
3 Rule(s) Governing the Prescribing of Opioids for Pain adopted pursuant to Act No. 75 of the Acts of the 2013 Session (8/01/15); adopted pursuant to Sections 14(e) and 11(e) of Act 75 (2013) and Sections 2(e) and 2a of Act 173 (2016). (7/01/17.) legal requirements for the appropriate use of opioids in treating pain in order to minimize opportunities for misuse, abuse, and diversion, and optimize prevention of addiction and overdose prescription limits for acute pain only apply to the first prescription written for a given course of treatment, and do not apply to refills. The prescribing limits under this rule do not apply to palliative care, or end of life care.
4 CDC Guideline chronic pain (ie, pain conditions that typically last >3 months or past the time of normal tissue healing) in outpatient settings. intended for primary care clinicians (eg, family physicians, internists, nurse practitioners, and physician assistants.) Use in other acute care settings or by other specialists is not the focus of the guideline improve communication regarding the benefits and risks of opioids, improve safety and effectiveness of pain treatment, reduce risks associated with long-term opioid therapy
5 CDC Guideline CDC updated a systematic Review sponsored by AHRQ on the effectiveness and risks of long-term opioid treatment of chronic pain Controversy about effectiveness of long-term opioids for outcomes at least 1 year later related to pain, function, and quality of life; whether findings on short-term effectiveness can be extrapolated to estimate benefits of long-term therapy for chronic pain updated review revealed that evidence on long-term opioid therapy for chronic pain outside of end-of-life care remains limited, with insufficient evidence to determine long-term benefits, although evidence suggests risk of serious harms that is dose-dependent
6 4.0 Universal Precautions Any opioid, Schedule II, III, or IV, for the first time during a course of treatment to any patient Consider Non-Opioid and Non-Pharmacological Treatment Query the Vermont Prescription Monitoring System (VPMS) Provide Patient Education and Informed Consent
7 4.0 Universal Precautions Consider and Document Non-Opioid and Non-Pharmacological Treatment Include but not limited to NSAIDs Acetaminophen Acupuncture OMT Chiropractic PT to document the consideration of alternatives for pain management is unnecessarily burdensome and will not be effective-eliminated
8 CDC Guideline In this article, we summarize benefits and harms of nonopioid therapies found in the clinical literature and harms of opioid therapy, including additional studies not included in the clinical evidence review (eg, studies not restricted to patients with chronic pain) Several nonpharmacologic and nonopioid pharmacologic treatments were found to be effective for chronic pain in studies ranging up to 6 months. For example, cognitive behavioral therapy (CBT) had small positive effects on disability and catastrophic thinking. Exercise therapy reduced pain and improved function in chronic low back pain; improved function and reduced pain in osteoarthritis of the knee and hip; and improved well-being, symptoms, and physical function in fibromyalgia. Multimodal and multidisciplinary therapies helped reduce pain and improve function more effectively than single modalities
9 4.0 Universal Precautions Query the Vermont Prescription Monitoring System (VPMS)
10 4.0 Universal Precautions Provide Patient Education and Informed Consent in-person discussion with the patient (parent, guardian, or legal representative) regarding potential side effects, risks of dependence and overdose, alternative treatments, appropriate tapering and safe storage and disposal Prior to prescribing, shall provide the patient with the Department of Health patient education sheet published on the Health Department website, or a written alternative signed informed consent Information on potential for misuse, abuse, diversion, and addiction; risks of life-threatening respiratory depression; fatal overdose from accidental exposure, especially in children; neonatal opioid withdrawal syndrome; and fatal overdose when combining with alcohol and/or other psychoactives (benzodiazepines and barbiturates)
11 4.0 Universal Precautions Provide Patient Education and Informed Consent signed informed consent with no ability to delegate before every opiate prescription for acute pain-denied
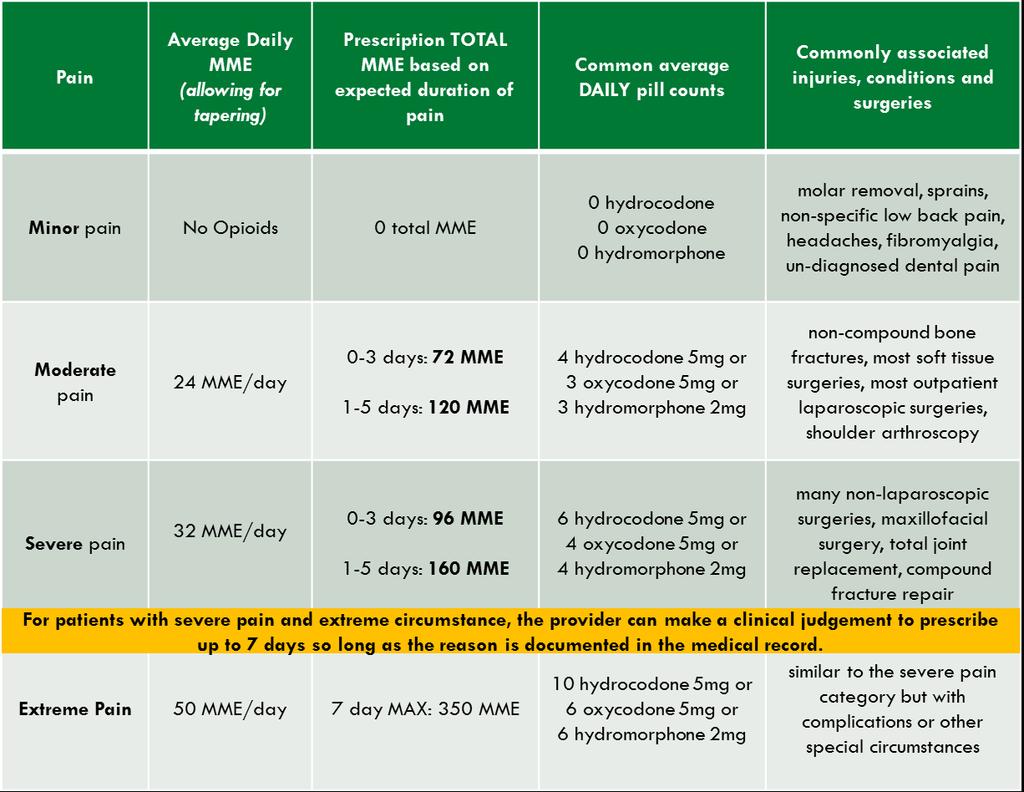
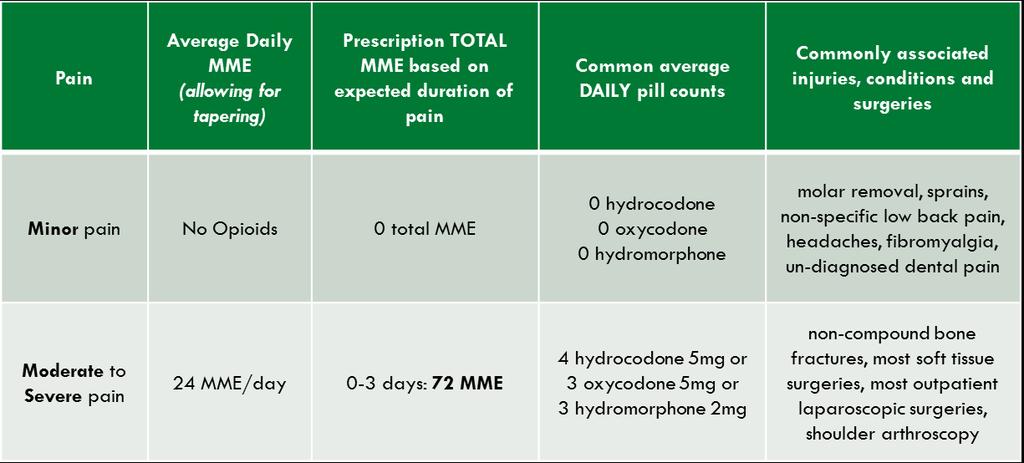
12 Prescribing Opioids for Acute Pain Framework smallest doses for the shortest periods of time limits found in Figures 1.0 and 2.0 are maximums Maximums are averages, not absolute daily limits. This may allow larger doses at the start of the prescription with smaller doses at the end as the patient tapers limits apply to patients who are opioid naïve and are receiving their first prescriptions not administered in a healthcare setting [decision making required by the rule would be too complicated to manage for medications that would be administered where there is minimal risk of diversion in a hospital] has not used opioids for more than seven consecutive days during the previous 30 days.
13 CDC Guideline KQ5: Effect of Opioid Therapy for Acute Pain on Long-term Use Opioid therapy prescribed for acute pain was associated with greater likelihood of long-term use
14 Prescribing Opioids for Acute Pain limits do not prohibit writing a second prescription (or refill prescription) for the patient if necessary Figure 1.0 for adults ages 18 years and older Figure 2.0 for children ages 0-17 years old Four categories in each figure (patient placed based on the medical judgment of the prescriber) [prescription limits that were based on categories of procedures and injuries did not allow for the necessary subjective consideration of a patient s pain]
15
16
17 CDC Calculator MME OPIOID (dose=mg/day except where noted) Codeine 0.15 Fentanyl transdermal (in mcg/hr) 2.4 CONVERSION FACTOR Hydrocodone 1 Hydromorphone 4 Methadone 1-20 mg/day mg/day mg/day mg/day 12 Oxycodone 1.5 Morphine 1 Oxymorphone 3
18 Relative Strengths Solomon, Arch Int Med 10 Morphine(MS for Morphine Sulfate)=1 Hydrocodone=1 Aspirin=1/360 MEQ Codeine, Tramadol=1/10 MEQ Oxycodone= MEQ Hydromorphone=5 MEQ Methadone=3-7.5 MEQ (high individual variation) Oxymorphone=7 MEQ Fentanyl= MEQ
19 Prescribing Opioids for Acute Pain Long-acting opioids are not indicated for acute pain; reason must be justified in the patient s medical record prior to ending care for acute pain, if not primary care provider, ensure a safe transition of care by making a reasonable effort to contact the primary care provider with any relevant clinical information concerning the patient s condition, diagnosis and treatment [a clear discharge summary that includes expectations for ongoing pain treatment shall satisfy this requirement] prior to prescribing, shall make a reasonable effort to consult with child s primary care provider
20 CDC Guideline Long-term opioid use often begins with treatment of acute pain. When opioids are used for acute pain, clinicians should prescribe the lowest effective dose of immediate-release opioids and should prescribe no greater quantity than needed for the expected duration of pain severe enough to require opioids. Three days or less will often be sufficient; more than 7days will rarely be needed Clinicians should not prescribe ER/LA opioids for the treatment of acute pain
21 Exemptions Palliative care End-of-life and hospice care Patients in skilled and intermediate care nursing facilities Pain associated with significant or severe trauma Pain associated with complex surgery (spinal surgery) Pain associated with prolonged inpatient care due to post-operative complications Medication-assisted treatment for substance use disorders Patients who are not opioid naïve Other circumstances as determined by the Commissioner of Health
22 Prescribing Opioids for Chronic Pain Schedule II, III or IV opioids for chronic pain (pain lasting longer than 90 days) prescribing for the first time during a course of treatment, the Universal Precautions in Section 4.0 apply
23 CDC Guideline KQ1: Effectiveness and Comparative Effectiveness No study of opioid therapy vs placebo, no opioid therapy, or nonopioid therapy for chronic pain evaluated long-term (>1 year) outcomes related to pain, function, or quality of life. Most placebo controlled randomized clinical trials were 6 weeks or shorter
24 CDC Guideline KQ2: Harms and Adverse Events Long-term opioid therapy was associated with problematic patterns of opioid use leading to clinically significant impairment or distress. Varying terminology has been used to reflect this pattern, including addiction (more informally), opioid abuse and opioid dependence. Such disorders are manifested by similar criteria, including unsuccessful efforts to reduce or control use and use resulting in social problems and a failure to fulfill major role obligations at work, school, or home. Different from tolerance and physical dependence
25 CDC Guideline KQ2: Harms and Adverse Events (cont) Long-term opioid therapy was associated with an increased risk of an opioid abuse or dependence diagnosis vs no opioid prescription. In primary care settings, prevalence of opioid dependence (using DSM-IV criteria) ranged from 3%to 26% Factors associated with increased risk of misuse included history of substance use disorder, younger age, major depression, and use of psychotropic medications. Opioid use was associated with a dose-dependent increased risk of fatal and nonfatal overdose. Other risks associated with opioid use included cardiovascular events, endocrinological harms, and road trauma
26 CDC Guideline-Recommendation Extensive evidence shows the possible harms of opioids (including opioid use disorder, overdose, and motor vehicle injury) Extensive evidence suggests some benefits of nonpharmacologic and nonopioid pharmacologic therapy, with less harm
27 Prescribing Opioids for Chronic Pain Screening, Evaluation, and Risk Assessment Initiating an Opioid Prescription for Chronic Pain Referrals and Consultations Reevaluation of Treatment Exemptions
28 Screening, Evaluation, and Risk Assessment conduct and document a thorough medical evaluation and physical examination document supporting diagnoses evaluate and document benefits and risks, including the risk for misuse, abuse, diversion, addiction, or overdose including 3.18 Risk Assessment for predicting a patient's likelihood of misusing or abusing opioids (SOAPP or any evidence-based screening tool ) Other examples on VDH website
29 CDC Guideline KQ4: Risk Assessment and Risk Mitigation Strategies Evidence on the accuracy of risk assessment instruments for predicting opioid abuse or misuse was inconsistent for the Opioid Risk Tool and limited for other risk assessment instruments. No study evaluated the effectiveness of risk mitigation strategies
30 Initiating an Opioid Prescription for Chronic Pain consider and document Non-opioid alternatives up to a maximum recommended by the FDA, including non-pharmacological treatments Trial use of the opioid requirements to query VPMS currently or has recently been dispensed methadone or buprenorphine or prescribed and taken any other controlled substance required by law to disclose this information signed Controlled Substance Treatment Agreement
31 CDC Guideline Clinicians should review the patient s history of controlled substance prescriptions using state prescription drug monitoring program (PDMP) data to determine whether the patient is receiving opioid dosages or dangerous combinations that put him or her at high risk for overdose Clinicians should review PDMP data when starting opioid therapy for chronic pain and periodically during opioid therapy for chronic pain, ranging from every prescription to every 3 months
32 CDC Guideline Clinicians should not dismiss patients from care based on a urine drug test result. This could have adverse consequences for patient safety, including missed opportunities to facilitate treatment for substance use disorder The use of confirmatory testing adds substantial costs and should be based on the need to detect specific opioids that cannot be identified on standard immunoassays or on the presence of unexpected urine drug test results. Clinicians should ask patients whether there might be unexpected results-discuss with Lab and patient
33 Initiating an Opioid Prescription for Chronic Pain Controlled Substance Treatment Agreement functional goals for treatment choice of dispensing pharmacy safe storage and disposal other requirements as determined by the prescriber directly observed urine drug testing and pill counts examples of informed consent and Controlled Substance Treatment Agreements will be available on VDH website
34 Initiating an Opioid Prescription for Chronic Pain For the duration of the patient s treatment Schedule and undertake periodic follow-up visits and evaluations at a frequency determined by the patient s risk factors, the medication dose and other clinical indictors stable patients reevaluated at least every 90 days write maximum daily dose or a not to exceed on script
35 CDC Guideline Determining When to Initiate or Continue Opioids for Chronic Pain Nonpharmacologic therapy and nonopioid pharmacologic therapy are preferred for chronic pain. Clinicians should consider opioid therapy only if expected benefits for both pain and function are anticipated to outweigh risks to the patient. If opioids are used, they should be combined with nonpharmacologic therapy Nonpharmacologic therapy (such as exercise therapy and CBT) should be used to reduce pain and improve function in patients with chronic pain
36 CDC Guideline Opioids should not be considered first-line or routine therapy for chronic pain outside of active cancer, palliative, and end-of-life care, given small to moderate short-term benefits, uncertain long-term benefits, and potential for serious harms This does not mean that patients should be required to sequentially fail nonpharmacologic and nonopioid pharmacologic therapy before proceeding to opioid therapy In some clinical contexts (eg, headache, fibromyalgia), expected benefits of initiating opioids are unlikely to outweigh risks regardless of previous nonpharmacologic and nonopioid pharmacologic therapies used. In other situations (eg, serious illness in a patient with poor prognosis for return to previous level of function, contraindications to other therapies, and clinician and patient agreement that the overriding goal is patient comfort) it may be appropriate
37 CDC Guideline Before starting opioid therapy for chronic pain, clinicians should establish treatment goals, including realistic goals for pain and function, and consider how opioid therapy will be discontinued if benefits do not outweigh risks Continue opioid therapy only if there is clinically meaningful improvement in pain and function that outweighs risks to patient safety. There are some clinical circumstances under which reductions in pain without improvement in physical function might be more realistic (eg, diseases with progressive functional impairment or catastrophic injuries such as spinal cord trauma) Clinically meaningful improvement has been defined as a 30% improvement in scores for both pain and function Depression, anxiety, and other psychological comorbidities should be assessed and treatment optimized
38 CDC Guideline Be explicit and realistic about expected benefits of opioids, explaining that while opioids can reduce pain during short-term use, there is no good evidence that opioids improve pain or function with long-term use and that complete relief of pain is unlikely serious adverse effects of opioids, including potentially fatal respiratory depression and development of a potentially serious lifelong opioid use disorder. Discuss effects that opioids may have on ability to safely operate a vehicle, particularly when opioids are initiated, when dosages are increased, or when other central nervous system depressants, such as benzodiazepines or alcohol, are used concurrently
39 CDC Guideline Discuss risks to household members and other individuals if opioids are intentionally or unintentionally shared; young children are susceptible to unintentional ingestion. Discuss storage of opioids Consider whether cognitive limitations might interfere with management of opioid therapy
40 Referrals and Consultations Consider a referral to a pain specialist or substance abuse specialist not meeting the goals of treatment despite escalating doses high risk for substance misuse, abuse, diversion, addiction, or overdose as determined by history or screening reasonable grounds to believe, or confirms, misuse of opioids or other substances multiple prescribers and/or pharmacies prescribed multiple controlled substances patient request
41 Reevaluation Controlled Substance Treatment Agreements will be reviewed and documented at least yearly in medical record Specific rules relative to exceeding 90 MME/day Determine and document as part of the reevaluation: Whether to continue opioids or trial alternatives Obtain pain management, substance abuse or pharmacological consult Acknowledgement that a violation of the agreement may result in consequences
42 Reevaluation Specific rules relative to exceeding 90 MME/day in-person discussion regarding increased risk of overdose reevaluation of the effectiveness and safety of the patient's pain management plan, including an assessment of adherence potential for the use of non-opioid and nonpharmacological alternatives functional examination of the patient review of Controlled Substance Agreement and Informed Consent assessment of co-morbid conditions affected by treatment with opioids other related actions by the patient that may lead prescriber to modify pain management regimen (risk factors)
43 CDC Guideline Clinicians should use caution when prescribing opioids at any dosage, should carefully reassess evidence of individual benefits and risks when considering increasing dosage to 50 morphine milligram equivalents (MME) or more per day Clinicians should avoid increasing dosage to 90 MME or more per day or carefully justify a decision to titrate dosage to 90MME or more per day
44 CDC Guideline Clinicians should evaluate benefits and harms with patients within 1 to 4 weeks of starting opioid therapy for chronic pain or of dose escalation. Clinicians should evaluate benefits and harms of continued therapy with patients every 3 months or more frequently Clinicians should work with patients to reduce opioid dosage or to discontinue opioids when possible if clinically meaningful improvements in pain and function are not sustained Tapering: A decrease of 10% of the original dose per week is a reasonable starting point, 10% per month if have been on a long time. Rapid tapers and pregnancy may require assistance
45 CDC Guideline Clinicians should avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible. It might be safer and more practical to taper opioids first Clinicians should offer or arrange evidence-based treatment (usually medication-assisted treatment with buprenorphine or methadone in combination with behavioral therapies) for patients with opioid use disorder
46 Exemptions Chronic pain associated with cancer or cancer treatment Palliative care End-of-life and hospice care Patients in skilled and intermediate care nursing facilities Pain caused by cancer and acute pain from cancer/cancer care are not exempt from the universal precautions (checking VPMS, informed consent, providing an information sheet) nor from the prescribing limits-denied. Chronic pain may be exempt
47 Naloxone (Acute or Chronic) Co-prescribe for MME>90 or concurrent prescription for benzodiazepines Opioid-related overdose risk was dose-dependent, with higher opioid dosages associated with increased overdose risk. 1 to <20MME compared to 50 to <100MME and above Disproportionate numbers of overdose deaths associated with methadone; fatal overdose risk associated with co-prescription of opioids and benzodiazepines; and risks associated with sleepdisordered breathing, reduced renal or hepatic function, older age, pregnancy, mental health comorbidities, history of substance use disorder, and history of overdose
48 Naloxone Co-prescribe for MME>90 or concurrent prescription for benzodiazepines consider offering naloxone when prescribing opioids to patients at increased risk of overdose including patients at risk of returning to a high dose to which they are no longer tolerant (eg, patients recently released from prison)
49 Extended Release (Acute or Chronic) In addition to the above, ER hydrocodones and oxycodones not manufactured as Abuse-deterrent Opioids require conduct and document a thorough medical and physical examination diagnoses which support the use evaluate and document benefits and risks including Risk Assessment pain severe enough to require daily, around-the-clock, long-term, opioid treatment for which alternative treatment options, including nonpharmacological treatments, are ineffective, not tolerated, or are otherwise inadequate signed Informed Consent signed Controlled Substance Treatment Agreement
50 CDC Guideline KQ3: Dosing Strategies Initiation of therapy with an extended-release/longacting(er/la)opioid was associated with greater risk of nonfatal overdose than initiation with an immediate-release opioid in 1 study, with risk greatest in the first 2weeks after initiation of treatment Three studies of various ER/LA opioids found no clear differences related to pain or function
51 CDC Guideline When starting opioid therapy for chronic pain, clinicians should prescribe immediate-release opioids instead of extendedrelease/long-acting (ER/LA) opioids Clinicians should not initiate opioid treatment with ER/LA opioids and should not prescribe ER/LA opioids for intermittent use. avoiding the use of immediate-release opioids in combination with ER/LA opioids is preferable Methadone should not be the first choice for an ER/LA opioid. Avoid transdermal fentanyl
52 Extended Release Cont. query VPMS and document review of other prior controlled substances preceding ER query no less frequently than every 120 days for 40 mg or greater of hydrocodone or 30 mg or greater of oxycodone query no less frequently than as described in the Vermont Prescription Monitoring System Rule write a maximum daily dose, or a not to exceed value filled within seven (7) days of the date issued and no more than 30-day supply
53 Extended Release Periodic follow-up visits and evaluations at least every 90 days during which the following must be documented whether to continue ER need for a pain management or substance abuse consultation acknowledgement that a violation of the agreement may result in consequences
54 Additional reading port_2014.pdf uideline.pdf Rodgers J, Cunningham K, Fitzgerald K, Finnerty E. Opioid Consumption Following Outpatient Upper Extremity Surgery. J Hand Surg Am. 2012;37(4): doi: /j.jhsa
55 Additional reading Case A, Deaton A, Rising morbidity and mortality in midlife amo ng white nonhispanic Americans in the 21st century, Proceedings of the National Academy of Science s, 2015 [epub ahead of print]; 9bfb943f aedf9f4bcec9b5f9. Azevedo LF, et al. A population based study on chronic pain and the use of opioids in Portugal, P ain, 2013; 154(12): doi: /j.pain Von Korff M Opioids for chronic musculoskeletal pain: Putting pa tient safety first, Pain, 2013; 154(12):




56 VERMONT PRESCRIPTION MONITORING SYSTEM UPDATES AND TIPS October 18, 2017
57 What is VPMS? The Vermont Prescription Monitoring Program (VPMS) is a statewide electronic database of Schedule II-IV controlled substance prescriptions dispensed from Vermont-licensed pharmacies. VPMS is a clinical tool Controlled substance data collected from Vermont-licensed pharmacies includes information on the: Prescribed drug Recipient of the prescribed drug Health care provider who wrote the prescription Pharmacy that dispensed the prescription Prescriptions are required to be uploaded to the system within 24 hours or one business day Prescriptions dispensed in certain situations are not included: Emergency Departments, for treatment of pain for 48 hours or less Veterinarian offices Hubs (OTP) 57 57
58 What is new? Migration to new platform VPMS migrated to AWARxE platform on June 15 th, 2017 Rules, effective July 1 st, 2017 Includes increased query responsibilities as well as operational information Quarterly Reports Include county level metrics on prescription information Ability to query additional states Currently able to query CT, MA, ME, NH, NJ, NY, RI Increased delegate/supervisor possibilities Many/many relationship up to
59 What updates are coming? New Interface Early November Prescriber Insight Reports Fall 2017 Provide metrics on the provider s prescriptions dispensed in comparison with peers within specialty Clinical Alerts Late 2017 Patients with MME over 90, Overlapping Benzo/Opioid Rxs and/or Multiple Provider Episodes will be flagged on prescriber dashboards Annual Reports 2016 Annual Report due early 2017, 2017 Annual Report due shortly thereafter 59 59
60 How do I best use VPMS? Know when to query Remember Initial, Re-evaluation, Replacement Know the limitations of what you are seeing VT-licensed pharmacies Exact name match on bulk searches and interstate queries No hub data VPMS data is additional information it may not be complete information Provide wider queries and then narrow down Use partial name search and the minimum amount of information required in order to return the maximum results Use integrated tools Bulk Patient Upload MyRx 60 60
61 Contact VPMS Technical Support questions can be directed to: Support Desk Ticketing or Programmatic questions can be directed to the program manager, Hannah Hauser at: or (802)
Rule Governing the Prescribing of Opioids for Pain
 Rule Governing the Prescribing of Opioids for Pain 1.0 Authority This rule is adopted pursuant to Sections 14(e) and 11(e) of Act 75 (2013) and Sections 2(e) and 2a of Act 173 (2016). 2.0 Purpose This
Rule Governing the Prescribing of Opioids for Pain 1.0 Authority This rule is adopted pursuant to Sections 14(e) and 11(e) of Act 75 (2013) and Sections 2(e) and 2a of Act 173 (2016). 2.0 Purpose This
Summary of Recommendations...3. PEG: A Three-Item Scale Assessing Pain (Appendix A) Chronic Pain Flow Sheet Acute Pain Flow Sheet...
 Chronic Pain Flow Sheet Acute Pain Flow Sheet...") Table of Contents Summary of Recommendations....3 PEG: A Three-Item Scale Assessing Pain (Appendix A)...12 Chronic Pain Flow Sheet...13 Acute Pain Flow Sheet...14 Pocket Guide: Tapering Opioids for Chronic
Table of Contents Summary of Recommendations....3 PEG: A Three-Item Scale Assessing Pain (Appendix A)...12 Chronic Pain Flow Sheet...13 Acute Pain Flow Sheet...14 Pocket Guide: Tapering Opioids for Chronic
CDC Guideline for Prescribing Opioids for Chronic Pain. Centers for Disease Control and Prevention National Center for Injury Prevention and Control
 CDC Guideline for Prescribing Opioids for Chronic Pain Centers for Disease Control and Prevention National Center for Injury Prevention and Control THE EPIDEMIC Chronic Pain and Prescription Opioids 11%
CDC Guideline for Prescribing Opioids for Chronic Pain Centers for Disease Control and Prevention National Center for Injury Prevention and Control THE EPIDEMIC Chronic Pain and Prescription Opioids 11%
HOPE. Considerations. Considerations ISING. Safe Opioid Prescribing Guidelines for ACUTE Non-Malignant Pain
 Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
Opioid Management of Chronic (Non- Cancer) Pain
 Pain") Optima Health Opioid Management of Chronic (Non- Cancer) Pain Guideline History Original Approve Date 5/08 Review/Revise Dates 11/09, 9/11, 9/13, 09/15, 9/17 Next Review Date 9/19 These Guidelines are
Optima Health Opioid Management of Chronic (Non- Cancer) Pain Guideline History Original Approve Date 5/08 Review/Revise Dates 11/09, 9/11, 9/13, 09/15, 9/17 Next Review Date 9/19 These Guidelines are
CDC Guideline for Prescribing Opioids for Chronic Pain
 National Center for Injury Prevention and Control CDC Guideline for Prescribing Opioids for Chronic Pain John Halpin, MD, MPH Medical Officer Division of Unintentional Injury Prevention Prescription Drug
National Center for Injury Prevention and Control CDC Guideline for Prescribing Opioids for Chronic Pain John Halpin, MD, MPH Medical Officer Division of Unintentional Injury Prevention Prescription Drug
New Guidelines for Prescribing Opioids for Chronic Pain
 New Guidelines for Prescribing Opioids for Chronic Pain Andrew Lowe, Pharm.D. CAPA Meeting October 6, 2016 THE EPIDEMIC Chronic Pain and Prescription Opioids 11% of Americans experience daily (chronic)
New Guidelines for Prescribing Opioids for Chronic Pain Andrew Lowe, Pharm.D. CAPA Meeting October 6, 2016 THE EPIDEMIC Chronic Pain and Prescription Opioids 11% of Americans experience daily (chronic)
Knock Out Opioid Abuse in New Jersey:
 Knock Out Opioid Abuse in New Jersey: A Resource for Safer Prescribing GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN IMPROVING PRACTICE THROUGH RECOMMENDATIONS CDC s Guideline for Prescribing Opioids
Knock Out Opioid Abuse in New Jersey: A Resource for Safer Prescribing GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN IMPROVING PRACTICE THROUGH RECOMMENDATIONS CDC s Guideline for Prescribing Opioids
SAFE PRESCRIBING: RULES AND REGULATIONS. Michelle Y. Owens, MD MS State Board of Medical Licensure June 30, 2017
 SAFE PRESCRIBING: RULES AND REGULATIONS Michelle Y. Owens, MD MS State Board of Medical Licensure June 30, 2017 DISCLOSURES I have no financial disclosures. OBJECTIVES Discuss the significance of the opiate
SAFE PRESCRIBING: RULES AND REGULATIONS Michelle Y. Owens, MD MS State Board of Medical Licensure June 30, 2017 DISCLOSURES I have no financial disclosures. OBJECTIVES Discuss the significance of the opiate
OPIOID PRESCRIBING RULES. May 17, 2017 Webinar
 OPIOID PRESCRIBING RULES May 17, 2017 Webinar Outline Introduction and Universal Precautions Dr. Levine, Commissioner, Health Department 15 Minutes Acute Pain Dr. Patti Fisher, UVMMC 20 Minutes Chronic
OPIOID PRESCRIBING RULES May 17, 2017 Webinar Outline Introduction and Universal Precautions Dr. Levine, Commissioner, Health Department 15 Minutes Acute Pain Dr. Patti Fisher, UVMMC 20 Minutes Chronic
Vermont. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile Vermont Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points of
Prescribing and Dispensing Profile Vermont Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points of
Opioid Review and MAT Clinic CDC Guidelines
 1 Opioid Review and MAT Clinic CDC Guidelines January 10, 2018 Housekeeping Use chat feature to inform everyone who s at your clinic Click chat on Zoom option bar Chat Everyone the names of those who are
1 Opioid Review and MAT Clinic CDC Guidelines January 10, 2018 Housekeeping Use chat feature to inform everyone who s at your clinic Click chat on Zoom option bar Chat Everyone the names of those who are
New Guidelines for Opioid Prescribing
 New Guidelines for Opioid Prescribing What They Mean for Elders with Chronic Pain Manu Thakral, PhD, ARNP Kaiser Permanente Washington Health Research Institute Kaiser Permanente Washington Health Research
New Guidelines for Opioid Prescribing What They Mean for Elders with Chronic Pain Manu Thakral, PhD, ARNP Kaiser Permanente Washington Health Research Institute Kaiser Permanente Washington Health Research
THE PROS & CONS OF THE CDC GUIDELINES FOR SAFE OPIOID PRESCRIBING
 THE PROS & CONS OF THE CDC GUIDELINES FOR SAFE OPIOID PRESCRIBING Ernest J Dole, PharmD, PhC, FASHP, BCPS Clinical Pharmacist University of New Mexico Hospitals And Clinical Associate Professor University
THE PROS & CONS OF THE CDC GUIDELINES FOR SAFE OPIOID PRESCRIBING Ernest J Dole, PharmD, PhC, FASHP, BCPS Clinical Pharmacist University of New Mexico Hospitals And Clinical Associate Professor University
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2018 P 4000-3 Program Opioid Overutilization Cumulative Drug Utilization Review Criteria Medication Includes all salt forms, single and
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2018 P 4000-3 Program Opioid Overutilization Cumulative Drug Utilization Review Criteria Medication Includes all salt forms, single and
Bree Collaborative AMDG Opioid Prescribing Guidelines Workgroup. Opioid Prescribing Metrics - DRAFT
 Bree Collaborative AMDG Opioid Prescribing Guidelines Workgroup Opioid Prescribing Metrics - DRAFT Definitions: Days Supply: The total of all opioid prescriptions dispensed during the calendar quarter
Bree Collaborative AMDG Opioid Prescribing Guidelines Workgroup Opioid Prescribing Metrics - DRAFT Definitions: Days Supply: The total of all opioid prescriptions dispensed during the calendar quarter
Proposed Revision to Med (i)
") Proposed Revision to Med 501.02 (i) I. Purpose This rule has been adopted to enable the Board to best protect public health and safety while providing a framework for licensees to effectively treat and
Proposed Revision to Med 501.02 (i) I. Purpose This rule has been adopted to enable the Board to best protect public health and safety while providing a framework for licensees to effectively treat and
Prescription Monitoring Program (PMP)
") 06/15/2018 FACT SHEET Implementation of Enacted Prescribing Limits and Requirements and Relevant Opioid Prescribing Laws and Rules Background: The 2016 law (Chapter 488) makes five major changes to opioid
06/15/2018 FACT SHEET Implementation of Enacted Prescribing Limits and Requirements and Relevant Opioid Prescribing Laws and Rules Background: The 2016 law (Chapter 488) makes five major changes to opioid
Standard of Practice for Prescribing Opioids (Excluding Cancer, Palliative, and End-of-Life Care)
") Standard of Practice for Prescribing Opioids (Excluding Cancer, Palliative, and End-of-Life Care) Preamble This Standard establishes the standards of practice and ethical requirements of all physicians
Standard of Practice for Prescribing Opioids (Excluding Cancer, Palliative, and End-of-Life Care) Preamble This Standard establishes the standards of practice and ethical requirements of all physicians
Readopt with amendment Med 502, effective (Document #11090), to read as follows:
, to read as follows:") Adopted Rules 11-2-16 1 Readopt with amendment Med 502, effective 5-3-16 (Document #11090), to read as follows: PART Med 502 OPIOID PRESCRIBING Med 502.01 Applicability. This part shall apply to the prescribing
Adopted Rules 11-2-16 1 Readopt with amendment Med 502, effective 5-3-16 (Document #11090), to read as follows: PART Med 502 OPIOID PRESCRIBING Med 502.01 Applicability. This part shall apply to the prescribing
Opiate Use Disorder and Opiate Overdose
 Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
Re: Draft Guideline for the Use of Opioids for Chronic Pain (Docket No. CDC )
") January 13, 2016 Veronica Kennedy Acting Executive Secretary, Centers for Disease Control and Prevention National Center for Injury Prevention and Control, Centers for Disease Control and Prevention, 4770
January 13, 2016 Veronica Kennedy Acting Executive Secretary, Centers for Disease Control and Prevention National Center for Injury Prevention and Control, Centers for Disease Control and Prevention, 4770
Non Opioid Approaches to Pain and Musculoskeletal Disorders KEVIN ODONNELL, DO FLAGSTAFF BONE AND JOINT
 Non Opioid Approaches to Pain and Musculoskeletal Disorders KEVIN ODONNELL, DO FLAGSTAFF BONE AND JOINT Learning Objectives Review Opioid Crisis CDC Guidelines for opioid prescribing Discuss Alternatives
Non Opioid Approaches to Pain and Musculoskeletal Disorders KEVIN ODONNELL, DO FLAGSTAFF BONE AND JOINT Learning Objectives Review Opioid Crisis CDC Guidelines for opioid prescribing Discuss Alternatives
Opioid Prescribing Guidelines for Patients in the Emergency Department
 Opioid Prescribing Guidelines for Patients in the Emergency Department and Immediate Care Centers These guidelines are meant to assist clinicians in treating patients with acute and chronic pain in the
Opioid Prescribing Guidelines for Patients in the Emergency Department and Immediate Care Centers These guidelines are meant to assist clinicians in treating patients with acute and chronic pain in the
SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF CHRONIC NON-TERMINAL PAIN (CNTP)
") 9 SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF CHRONIC NON-TERMINAL PAIN (CNTP) SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF ACUTE PAIN NONOPIOID TREATMENTS
9 SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF CHRONIC NON-TERMINAL PAIN (CNTP) SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF ACUTE PAIN NONOPIOID TREATMENTS
Opioid Prescribing Improvement Program
 Opioid Prescribing Improvement Program Jeff Schiff, MD, MBA, Medical Director of Minnesota Health Care Programs Sarah Rinn, MPH, Opioid Prescribing Improvement Program Coordinator Agenda Opioid Prescribing
Opioid Prescribing Improvement Program Jeff Schiff, MD, MBA, Medical Director of Minnesota Health Care Programs Sarah Rinn, MPH, Opioid Prescribing Improvement Program Coordinator Agenda Opioid Prescribing
Revised 9/30/2016. Primary Care Provider Pain Management Toolkit
 Revised 9/30/2016 Primary Care Provider Pain Management Toolkit TABLE OF CONTENTS 1. INTRODUCTION Page 1 2. NON-OPIOID SERVICES &TREATMENTS FOR CHRONIC PAIN Page 2 2.1 Medical Services Page 2 2.2 Behavioral
Revised 9/30/2016 Primary Care Provider Pain Management Toolkit TABLE OF CONTENTS 1. INTRODUCTION Page 1 2. NON-OPIOID SERVICES &TREATMENTS FOR CHRONIC PAIN Page 2 2.1 Medical Services Page 2 2.2 Behavioral
Oregon Opioid Overdose Prevention Initiative
 Oregon Opioid Overdose Prevention Initiative Katrina Hedberg, MD, MPH Health Officer & State Epidemiologist Oregon Public Health Division Oregon Association of Hospitals & Health Systems February 2017
Oregon Opioid Overdose Prevention Initiative Katrina Hedberg, MD, MPH Health Officer & State Epidemiologist Oregon Public Health Division Oregon Association of Hospitals & Health Systems February 2017
Prescribing Opioids in the Opioid Epidemic. Scott Woffinden, PA-C Jason Chapman, JD
 Prescribing Opioids in the Opioid Epidemic Scott Woffinden, PA-C Jason Chapman, JD What's the Problem? http://www.zdoggmd.com/blank-script-taylor-swift-parody/ What's the Problem? CDC 115 Americans die
Prescribing Opioids in the Opioid Epidemic Scott Woffinden, PA-C Jason Chapman, JD What's the Problem? http://www.zdoggmd.com/blank-script-taylor-swift-parody/ What's the Problem? CDC 115 Americans die
OCCUPATIONAL AND PROFESSIONAL LICENSING MEDICINE AND SURGERY PRACTITIONERS MANAGEMENT OF PAIN AND OTHER CONDITIONS WITH CONTROLLED SUBSTANCES
 TITLE 16 CHAPTER 10 PART 14 OCCUPATIONAL AND PROFESSIONAL LICENSING MEDICINE AND SURGERY PRACTITIONERS MANAGEMENT OF PAIN AND OTHER CONDITIONS WITH CONTROLLED SUBSTANCES 16.10.14.1 ISSUING AGENCY: New
TITLE 16 CHAPTER 10 PART 14 OCCUPATIONAL AND PROFESSIONAL LICENSING MEDICINE AND SURGERY PRACTITIONERS MANAGEMENT OF PAIN AND OTHER CONDITIONS WITH CONTROLLED SUBSTANCES 16.10.14.1 ISSUING AGENCY: New
Prescribing drugs of dependence in general practice, Part C
 HO O Prescribing drugs of dependence in general practice, Part C Key recommendations and practice points for management of pain with opioid therapy H H HO N CH3 Acute pain Acute pain is an unpleasant sensory
HO O Prescribing drugs of dependence in general practice, Part C Key recommendations and practice points for management of pain with opioid therapy H H HO N CH3 Acute pain Acute pain is an unpleasant sensory
Management of Pain - A Comparison of Current Guidelines
 Management of Pain - A Comparison of Current Guidelines The Centers for Disease Control and Prevention (CDC) released a guideline in 2016 regarding the prescribing of opioids for chronic non-cancer pain
Management of Pain - A Comparison of Current Guidelines The Centers for Disease Control and Prevention (CDC) released a guideline in 2016 regarding the prescribing of opioids for chronic non-cancer pain
Opioid Prescribing Tips & Tricks CANDY STOCKTON, MD MAY 2018
 Opioid Prescribing Tips & Tricks CANDY STOCKTON, MD MAY 2018 Disclosures None Educational Objectives Understand CA state medical board guidelines for prescribing opioids for chronic pain Understand the
Opioid Prescribing Tips & Tricks CANDY STOCKTON, MD MAY 2018 Disclosures None Educational Objectives Understand CA state medical board guidelines for prescribing opioids for chronic pain Understand the
Oklahoma. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile Oklahoma Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Prescribing and Dispensing Profile Oklahoma Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Opioid Analgesics. Recommended starting dose for opioid-naïve patients
 Opioid Analgesics Goals: Restrict use of opioid analgesics to OHP-funded conditions with documented sustained improvement in pain and function and with routine monitoring for opioid misuse and abuse. Promote
Opioid Analgesics Goals: Restrict use of opioid analgesics to OHP-funded conditions with documented sustained improvement in pain and function and with routine monitoring for opioid misuse and abuse. Promote
Scope of the Opiate Problem 6/5/18. Chronic Pain Management and the Use of Opioid Medications: The CDC Guideline and Beyond. Overview.
 Chronic Pain Management and the Use of Opioid Medications: The CDC Guideline and Beyond David Anisman, MD Medical Director, Farmington Health Center (Primary Care) Associate Medical Director, Community
Chronic Pain Management and the Use of Opioid Medications: The CDC Guideline and Beyond David Anisman, MD Medical Director, Farmington Health Center (Primary Care) Associate Medical Director, Community
EXTENDED RELEASE OPIOID DRUGS
 RATIONALE FOR INCLUSION IN PA PROGRAM Background Hydrocodone (Hysingla ER, Vantrela ER, Zohydro ER), hydromorphone (Exalgo), morphine sulfate (Arymo ER, Avinza, Embeda, Kadian, MorphaBond, MS Contin),
RATIONALE FOR INCLUSION IN PA PROGRAM Background Hydrocodone (Hysingla ER, Vantrela ER, Zohydro ER), hydromorphone (Exalgo), morphine sulfate (Arymo ER, Avinza, Embeda, Kadian, MorphaBond, MS Contin),
Subject: Pain Management (Page 1 of 7)
") Subject: Pain Management (Page 1 of 7) Objectives: Managing pain and restoring function are basic goals in helping a patient with chronic non-cancer pain. Federal and state guidelines require that all
Subject: Pain Management (Page 1 of 7) Objectives: Managing pain and restoring function are basic goals in helping a patient with chronic non-cancer pain. Federal and state guidelines require that all
Recommendations in Opioid Prescribing Guidelines for Chronic Pain
 Recommendations in Opioid Prescribing Guidelines for Chronic Pain The use of opioids for treating chronic pain has been increasing. 1 In 2010, an estimated 20% of patients presenting to physician offices
Recommendations in Opioid Prescribing Guidelines for Chronic Pain The use of opioids for treating chronic pain has been increasing. 1 In 2010, an estimated 20% of patients presenting to physician offices
3. Has the patient had a sustained improvement in Pain or Function (e.g. PEG scale with a 30 percent response from baseline)?
?") Pharmacy Prior Authorization AETA BETTER HEALTH KETUCK Opioids Long-Acting and Short-Acting (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
Pharmacy Prior Authorization AETA BETTER HEALTH KETUCK Opioids Long-Acting and Short-Acting (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
Full details and resource documents available:
 Clinical & Regulatory News by Pharmerica Urinary Tract Infection (UTI) Second Most Common Cause of Hospital Readmission within 30 days UTIs are prevalent and account for up to 22% of infections in LTC,
Clinical & Regulatory News by Pharmerica Urinary Tract Infection (UTI) Second Most Common Cause of Hospital Readmission within 30 days UTIs are prevalent and account for up to 22% of infections in LTC,
Prior Authorization Guideline
 Guideline GL-35952 Opioid Quantity Limit Overrides Formulary OptumRx Formulary Note: Approval Date 7/10/2017 Revision Date 7/10/2017 Technician Note: P&T Approval Date: 2/16/2010; P&T Revision Date: 7/12/2011
Guideline GL-35952 Opioid Quantity Limit Overrides Formulary OptumRx Formulary Note: Approval Date 7/10/2017 Revision Date 7/10/2017 Technician Note: P&T Approval Date: 2/16/2010; P&T Revision Date: 7/12/2011
Clinical and Contextual Evidence Reviews
 Clinical and Contextual Evidence Reviews Roger Chou, MD Professor of Medicine Oregon Health & Science University Director, Pacific Northwest Evidence-based Practice Center Purpose Summarize methods for
Clinical and Contextual Evidence Reviews Roger Chou, MD Professor of Medicine Oregon Health & Science University Director, Pacific Northwest Evidence-based Practice Center Purpose Summarize methods for
The STOP Measure. Safe and Transparent Opioid Prescribing to Promote Patient Safety and Reduced Risk of Opioid Misuse FEBRUARY 2018
 The STOP Measure Safe and Transparent Opioid Prescribing to Promote Patient Safety and Reduced Risk of Opioid Misuse FEBRUARY 2018 AHIP s Safe, Transparent Opioid Prescribing (STOP) Initiative Methodology
The STOP Measure Safe and Transparent Opioid Prescribing to Promote Patient Safety and Reduced Risk of Opioid Misuse FEBRUARY 2018 AHIP s Safe, Transparent Opioid Prescribing (STOP) Initiative Methodology
Utah. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile Utah Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points of view
Prescribing and Dispensing Profile Utah Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points of view
Safe Prescribing of Drugs with Potential for Misuse/Diversion
 College of Physicians and Surgeons of British Columbia Safe Prescribing of Drugs with Potential for Misuse/Diversion Preamble This document establishes both professional standards as well as guidelines
College of Physicians and Surgeons of British Columbia Safe Prescribing of Drugs with Potential for Misuse/Diversion Preamble This document establishes both professional standards as well as guidelines
Clinical Policy: Opioid Analgesics Reference Number: CP.PMN.97 Effective Date: Last Review Date: 02.19
 Clinical Policy: Reference Number: CP.PMN.97 Effective Date: 02.11 Last Review Date: 02.19 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important regulatory
Clinical Policy: Reference Number: CP.PMN.97 Effective Date: 02.11 Last Review Date: 02.19 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important regulatory
April 26, New Mexico Board of Pharmacy Prescription Monitoring Program (PMP) New Mexico Board of Pharmacy Prescription Monitoring Program (PMP)
 New Mexico Board of Pharmacy Prescription Monitoring Program (PMP)") New Mexico Board of Pharmacy Prescription Monitoring Program (PMP) New Mexico Nurse Practitioner Council New Mexico Board of Pharmacy Prescription Monitoring Program (PMP) Peter Ryba, PharmD PMP Director
New Mexico Board of Pharmacy Prescription Monitoring Program (PMP) New Mexico Nurse Practitioner Council New Mexico Board of Pharmacy Prescription Monitoring Program (PMP) Peter Ryba, PharmD PMP Director
Mandatory PDMP Use PDMP Use STATE Prescriber Dispenser Conditions, if applicable
 Arizona Amends worker s compensation statute to require physicians to request PMP information within two (2) business days of writing or dispensing prescriptions for at least a 30 day supply of an opioid
Arizona Amends worker s compensation statute to require physicians to request PMP information within two (2) business days of writing or dispensing prescriptions for at least a 30 day supply of an opioid
OPIOID IR COMBO DRUGS. Oxycodone-acetaminophen, Oxycodone-aspirin, Oxycodone-ibuprofen, Tramadolacetaminophen
 RATIONALE FOR INCLUSION IN PA PROGRAM Background Apadaz (benzhydrocodone-acetaminophen), codeine-acetaminophen, dihydrocodeine-caffeineacetaminophen, hydrocodone-acetaminophen, hydrocodone-ibuprofen, oxycodoneacetaminophen,
RATIONALE FOR INCLUSION IN PA PROGRAM Background Apadaz (benzhydrocodone-acetaminophen), codeine-acetaminophen, dihydrocodeine-caffeineacetaminophen, hydrocodone-acetaminophen, hydrocodone-ibuprofen, oxycodoneacetaminophen,
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: Reference Number: HIM.PA.139 Effective Date: 12.01.17 Last Review Date: 02.18 Line of Business: Health Insurance Marketplace Revision Log See Important Reminder at the end of this policy
Clinical Policy: Reference Number: HIM.PA.139 Effective Date: 12.01.17 Last Review Date: 02.18 Line of Business: Health Insurance Marketplace Revision Log See Important Reminder at the end of this policy
Welcome - we will begin the webinar shortly Please read the participation tips below:
 Welcome - we will begin the webinar shortly Please read the participation tips below: All guest phones have been muted: Background noises, conversations, white noise etc., can be disruptive to a webinar.
Welcome - we will begin the webinar shortly Please read the participation tips below: All guest phones have been muted: Background noises, conversations, white noise etc., can be disruptive to a webinar.
Tennessee. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile Tennessee Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Prescribing and Dispensing Profile Tennessee Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
MOA: Practice Managers Program. Presented by: Kimber Debelak, CMC, CMOM, CMIS. May 17, zpain Management. & New Opioid Laws
 MOA: Practice Managers Program Presented by: Kimber Debelak, CMC, CMOM, CMIS May 17, 2018 Pain Management & New Opioid Laws Objectives and Educational Statement Objectives To understand the need for new
MOA: Practice Managers Program Presented by: Kimber Debelak, CMC, CMOM, CMIS May 17, 2018 Pain Management & New Opioid Laws Objectives and Educational Statement Objectives To understand the need for new
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: Opioid Analgesics Reference Number: HIM.PA.139 Effective Date: 12.01.17 Last Review Date: 11.17 Line of Business: Health Insurance Marketplace Revision Log See Important Reminder at the
Clinical Policy: Opioid Analgesics Reference Number: HIM.PA.139 Effective Date: 12.01.17 Last Review Date: 11.17 Line of Business: Health Insurance Marketplace Revision Log See Important Reminder at the
Long-Acting Opioid Analgesics
 Market DC Long-Acting Opioid Analgesics Override(s) Prior Authorization Step Therapy Quantity Limit Approval Duration Initial request: 3 months Maintenance Therapy: Additional prior authorization required
Market DC Long-Acting Opioid Analgesics Override(s) Prior Authorization Step Therapy Quantity Limit Approval Duration Initial request: 3 months Maintenance Therapy: Additional prior authorization required
Long-Acting Opioid Analgesics
 Market DC Long-Acting Opioid Analgesics Override(s) Prior Authorization Step Therapy Quantity Limit Approval Duration Initial request: 3 months Maintenance Therapy: Additional prior authorization required
Market DC Long-Acting Opioid Analgesics Override(s) Prior Authorization Step Therapy Quantity Limit Approval Duration Initial request: 3 months Maintenance Therapy: Additional prior authorization required
Mandatory PDMP Use PDMP Use STATE Prescriber Dispenser Conditions, if applicable
 Arizona Amends worker s compensation statute to require physicians to request PMP information within two (2) business days of writing or dispensing prescriptions for at least a 30 day supply of an opioid
Arizona Amends worker s compensation statute to require physicians to request PMP information within two (2) business days of writing or dispensing prescriptions for at least a 30 day supply of an opioid
Treatment of Pain in an Emergent Setting
 Updated: October 22, 2018 Prescribing Guidelines for Pennsylvania Treatment of Pain in an Emergent Setting Opioids, including heroin and fentanyl, contribute to thousands of overdose deaths in Pennsylvania
Updated: October 22, 2018 Prescribing Guidelines for Pennsylvania Treatment of Pain in an Emergent Setting Opioids, including heroin and fentanyl, contribute to thousands of overdose deaths in Pennsylvania
2. Is this request for a preferred medication? Y N
 Pharmacy Prior Authorization AETA BETTER HEALTH EW JERSE (MEDICAID) Opioids Long-Acting and Short-Acting (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
Pharmacy Prior Authorization AETA BETTER HEALTH EW JERSE (MEDICAID) Opioids Long-Acting and Short-Acting (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
California. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile California Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Prescribing and Dispensing Profile California Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Appropriate Prescribing of Opioids for Chronic Non Cancer Pain
 Appropriate Prescribing of Opioids for Chronic Non Cancer Pain Dr. Cheri Olson La Crosse Mayo Family Medicine Residency Assistant Professor of Family Medicine, Mayo Graduate School of Medicine Disclosure
Appropriate Prescribing of Opioids for Chronic Non Cancer Pain Dr. Cheri Olson La Crosse Mayo Family Medicine Residency Assistant Professor of Family Medicine, Mayo Graduate School of Medicine Disclosure
PROPOSED DUR CRITERIA FOR MANAGING OPIOID USE AND MINIMIZING RISK OF OVERDOSE
 BACKGROUND PROPOSED DUR CRITERIA FOR MANAGING OPIOID USE AND MINIMIZING RISK OF OVERDOSE In March, 2016, the CDC released the final version of their Guidelines for Prescribing Opioids for Chronic Pain.
BACKGROUND PROPOSED DUR CRITERIA FOR MANAGING OPIOID USE AND MINIMIZING RISK OF OVERDOSE In March, 2016, the CDC released the final version of their Guidelines for Prescribing Opioids for Chronic Pain.
The Wisconsin Prescription Drug Monitoring Program. WI PDMP Timeline. PDMP Overview. What is a PDMP? PDMPs Across the Nation. Wisconsin.
 The Wisconsin Prescription Drug Monitoring Program Wisconsin Nurses Association Jail Health Care Conference May 21, 2018 WI PDMP Timeline PDMP Overview January 2013 WI PDMP operational April 2017 WI epdmp
The Wisconsin Prescription Drug Monitoring Program Wisconsin Nurses Association Jail Health Care Conference May 21, 2018 WI PDMP Timeline PDMP Overview January 2013 WI PDMP operational April 2017 WI epdmp
Prepublication Requirements
 Issued Prepublication Requirements The Joint Commission has approved the following revisions for prepublication. While revised requirements are published in the semiannual updates to the print manuals
Issued Prepublication Requirements The Joint Commission has approved the following revisions for prepublication. While revised requirements are published in the semiannual updates to the print manuals
As part of the Opioid Analgesic REMS, all opioid analgesic companies must provide the following:
 Introduction FDA s Opioid Analgesic REMS Education Blueprint for Health Care Providers Involved in the Treatment and Monitoring of Patients with Pain (January 2018) Background In July 2012, FDA approved
Introduction FDA s Opioid Analgesic REMS Education Blueprint for Health Care Providers Involved in the Treatment and Monitoring of Patients with Pain (January 2018) Background In July 2012, FDA approved
Cigna Drug and Biologic Coverage Policy
 Cigna Drug and Biologic Coverage Policy Subject Opioid Therapy Table of Contents Coverage Policy... 1 General Background... 4 Coding/Billing Information... 7 References... 7 Effective Date..1/1/2018 Next
Cigna Drug and Biologic Coverage Policy Subject Opioid Therapy Table of Contents Coverage Policy... 1 General Background... 4 Coding/Billing Information... 7 References... 7 Effective Date..1/1/2018 Next
The Oregon Opioid Initiative. State Pain & Opioid Conference Prescription Drug Monitoring May 2018 Lisa Millet, Public Health Division
 The Oregon Opioid Initiative State Pain & Opioid Conference Prescription Drug Monitoring May 2018 Lisa Millet, Public Health Division Disclosure No disclosures 2 Learning Objectives Learner will be able
The Oregon Opioid Initiative State Pain & Opioid Conference Prescription Drug Monitoring May 2018 Lisa Millet, Public Health Division Disclosure No disclosures 2 Learning Objectives Learner will be able
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: Reference Number: LA.PPA.12 Effective Date: 02/11 Last Review Date: 01/18 Line of Business: Medicaid Coding Implications Revision Log See Important Reminder at the end of this policy for
Clinical Policy: Reference Number: LA.PPA.12 Effective Date: 02/11 Last Review Date: 01/18 Line of Business: Medicaid Coding Implications Revision Log See Important Reminder at the end of this policy for
CLINICAL POLICY DEPARTMENT: Medical
 IMPTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough review and consideration of currently available generally
IMPTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough review and consideration of currently available generally
Managed Care Pushes for Safer Opioid Oversight
 Page 1 of 6 Clinical AUGUST 11, 2017 Managed Care Pushes for Safer Opioid Oversight High-risk pain Rx eyed Denver Health systems haven t escaped the nation s ongoing opioid crisis, as evidenced by surging
Page 1 of 6 Clinical AUGUST 11, 2017 Managed Care Pushes for Safer Opioid Oversight High-risk pain Rx eyed Denver Health systems haven t escaped the nation s ongoing opioid crisis, as evidenced by surging
Section I. Short-acting opioid Prior Authorization Criteria
 Request for Prior Authorization for Opioid analgesics Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 Requests for opioid analgesics may be subject to prior authorization
Request for Prior Authorization for Opioid analgesics Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 Requests for opioid analgesics may be subject to prior authorization
Pain Management and Opioid Treatment Services
 Pain Management and Opioid Treatment Services Davis, CA (530) 753-4300; Voice mail: (916) 715-5856 davidmeelee@gmail.com www.changecompanies.net www.trainforchange.net www.tipsntopics.com www.asamcriteria.org
Pain Management and Opioid Treatment Services Davis, CA (530) 753-4300; Voice mail: (916) 715-5856 davidmeelee@gmail.com www.changecompanies.net www.trainforchange.net www.tipsntopics.com www.asamcriteria.org
AETNA BETTER HEALTH Prior Authorization guideline for Narcotic Analgesic Utilization
 AETNA BETTER HEALTH Prior Authorization guideline for Narcotic Analgesic Utilization Policy applies to all formulary and non-formulary schedules II V opioid narcotics, including tramadol and codeine, as
AETNA BETTER HEALTH Prior Authorization guideline for Narcotic Analgesic Utilization Policy applies to all formulary and non-formulary schedules II V opioid narcotics, including tramadol and codeine, as
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2099-5 Program Prior Authorization/Medical Necessity Buprenorphine Products (Pain Indications) Medication Belbuca (buprenorphine
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2099-5 Program Prior Authorization/Medical Necessity Buprenorphine Products (Pain Indications) Medication Belbuca (buprenorphine
Clinical Policy: Opioid Analgesics Reference Number: CP.PMN.97 Effective Date: Last Review Date: 02.18
 Clinical Policy: Reference Number: CP.PMN.97 Effective Date: 02.11 Last Review Date: 02.18 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important regulatory
Clinical Policy: Reference Number: CP.PMN.97 Effective Date: 02.11 Last Review Date: 02.18 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important regulatory
Clinical Policy: Opioid Analgesics Reference Number: OH.PHAR.PPA.13 Effective Date: 10/2017 Last Review Date: 6/2018 Line of Business: Medicaid
 Clinical Policy: Reference Number: OH.PHAR.PPA.13 Effective Date: 10/2017 Last Review Date: 6/2018 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: Reference Number: OH.PHAR.PPA.13 Effective Date: 10/2017 Last Review Date: 6/2018 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important
Fact Sheet. Zohydro ER (hydrocodone bitartrate) Extended-Release Capsules, CII
 Extended-Release Capsules, CII") Zohydro ER (hydrocodone bitartrate) Extended-Release Capsules, CII Fact Sheet Zohydro ER (hydrocodone bitartrate) Extended-Release Capsule, CII, is a long-acting (extendedrelease) type of pain medication
Zohydro ER (hydrocodone bitartrate) Extended-Release Capsules, CII Fact Sheet Zohydro ER (hydrocodone bitartrate) Extended-Release Capsule, CII, is a long-acting (extendedrelease) type of pain medication
Rhode Island. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile Rhode Island Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Prescribing and Dispensing Profile Rhode Island Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: Reference Number: CP.CPA.259 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important regulatory
Clinical Policy: Reference Number: CP.CPA.259 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important regulatory
Missouri Guidelines for the Use of Controlled Substances for the Treatment of Pain
 Substances for the Treatment of Pain Effective January 2007, the Board of Healing Arts appointed a Task Force to review the current statutes, rules and guidelines regarding the treatment of pain. This
Substances for the Treatment of Pain Effective January 2007, the Board of Healing Arts appointed a Task Force to review the current statutes, rules and guidelines regarding the treatment of pain. This
WHAT YOU NEED TO KNOW TO ABOUT AB 474
 WHAT YOU NEED TO KNOW TO ABOUT AB 474 PRESENTED BY: NEVADA STATE BOARD OF OSTEOPATHIC MEDICINE 2275 Corporate Circle, Suite 210 Henderson, NV 89074 702-732-2147 Fax 702-732-2079 Web Site: www.bom.nv.gov
WHAT YOU NEED TO KNOW TO ABOUT AB 474 PRESENTED BY: NEVADA STATE BOARD OF OSTEOPATHIC MEDICINE 2275 Corporate Circle, Suite 210 Henderson, NV 89074 702-732-2147 Fax 702-732-2079 Web Site: www.bom.nv.gov
A Bill Regular Session, 2015 SENATE BILL 717
 Stricken language would be deleted from and underlined language would be added to present law. 0 State of Arkansas 0th General Assembly As Engrossed: S// H// A Bill Regular Session, SENATE BILL By: Senator
Stricken language would be deleted from and underlined language would be added to present law. 0 State of Arkansas 0th General Assembly As Engrossed: S// H// A Bill Regular Session, SENATE BILL By: Senator
Virginia. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile Virginia Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Prescribing and Dispensing Profile Virginia Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Opioid Use: Current Challenges & Clinical Advancements
 Opioid Use: Current Challenges & Clinical Advancements Whitney Bergquist, PharmD, MBA, BCPS Acute Care NPPA Conference February 8, 2017 2017 MFMER slide-1 No Disclosures 2017 MFMER slide-2 Objectives Summarize
Opioid Use: Current Challenges & Clinical Advancements Whitney Bergquist, PharmD, MBA, BCPS Acute Care NPPA Conference February 8, 2017 2017 MFMER slide-1 No Disclosures 2017 MFMER slide-2 Objectives Summarize
Risk Reduction Strategies in Pain Management
 Risk Reduction Strategies in Pain Management Melissa J. Durham, PharmD, MACM, BCACP, DAAPM Assistant Professor of Clinical Pharmacy USC School of Pharmacy Clinical Pharmacist, The USC Pain Center Learning
Risk Reduction Strategies in Pain Management Melissa J. Durham, PharmD, MACM, BCACP, DAAPM Assistant Professor of Clinical Pharmacy USC School of Pharmacy Clinical Pharmacist, The USC Pain Center Learning
The Wisconsin Prescription Drug Monitoring Program
 The Wisconsin Prescription Drug Monitoring Program DHS 2018 WI Opioid Forum April 12, 2018 Learning Objectives 1. How the WI epdmp supports healthcare professionals in making informed prescribing, dispensing
The Wisconsin Prescription Drug Monitoring Program DHS 2018 WI Opioid Forum April 12, 2018 Learning Objectives 1. How the WI epdmp supports healthcare professionals in making informed prescribing, dispensing
Mandatory PDMP Use PDMP Use STATE Prescriber Dispenser Conditions, if applicable
 Alaska Requires adoption of regulations that provide that a practitioner query the PDMP prior to dispensing, prescribing, or administering a Sch. II or III controlled substance; query is not required for
Alaska Requires adoption of regulations that provide that a practitioner query the PDMP prior to dispensing, prescribing, or administering a Sch. II or III controlled substance; query is not required for
Wisconsin Opioid Prescribing Guideline Draft Scope and purpose of the guideline
 Wisconsin Opioid Prescribing Guideline Draft Scope and purpose of the guideline: To help providers make informed decisions about acute and chronic pain treatment -pain lasting longer than three months
Wisconsin Opioid Prescribing Guideline Draft Scope and purpose of the guideline: To help providers make informed decisions about acute and chronic pain treatment -pain lasting longer than three months
PRE-DECISIONAL; FOR IDENTIFIED STAKEHOLDER AND PEER REVIEW ONLY 1. CDC Guideline for Prescribing Opioids for Chronic Pain, 2016
 PRE-DECISIONAL; FOR IDENTIFIED STAKEHOLDER AND PEER REVIEW ONLY 1 CDC Guideline for Prescribing Opioids for Chronic Pain, 2016 Contributing Authors: Deborah Dowell, MD, MPH, Division of Unintentional Injury
PRE-DECISIONAL; FOR IDENTIFIED STAKEHOLDER AND PEER REVIEW ONLY 1 CDC Guideline for Prescribing Opioids for Chronic Pain, 2016 Contributing Authors: Deborah Dowell, MD, MPH, Division of Unintentional Injury
The Epidemiology of Opioid Abuse Thomas Dobbs, MD, MPH 6/30/2017
 The Epidemiology of Opioid Abuse Thomas Dobbs, MD, MPH 6/30/2017 The Mississippi Drug Abuse Project, Mississippi State Department of Health Working Group Manuela Staneva, MPH, Project Epidemiologist Meg
The Epidemiology of Opioid Abuse Thomas Dobbs, MD, MPH 6/30/2017 The Mississippi Drug Abuse Project, Mississippi State Department of Health Working Group Manuela Staneva, MPH, Project Epidemiologist Meg
On December 27, 2017, the Lieutenant Governor signed into law several new requirements
 OPIOID Alert MICHIGAN OSTEOPATHIC ASSOCIATION JANUARY 2018 On December 27, 2017, the Lieutenant Governor signed into law several new requirements aimed at combating the opioid epidemic. On the following
OPIOID Alert MICHIGAN OSTEOPATHIC ASSOCIATION JANUARY 2018 On December 27, 2017, the Lieutenant Governor signed into law several new requirements aimed at combating the opioid epidemic. On the following
State, District, or Territory Criteria for Mandatory Enrol ment or Query of PDMP
 State, District, or Territory Alabama Arizona Arkansas Criteria for Mandatory Enrollment or Query of PDMP Before renewing an Alabama Controlled Substances Certificate, the applicant shall have a current
State, District, or Territory Alabama Arizona Arkansas Criteria for Mandatory Enrollment or Query of PDMP Before renewing an Alabama Controlled Substances Certificate, the applicant shall have a current
DURATION LIMIT WITH QUANTITY LIMIT AND POST LIMIT PRIOR AUTHORIZATION CRITERIA IMMEDIATE-RELEASE OPIOID ANALGESICS (BRAND AND GENERIC)*
*") Carelirst. +.V Family of health care plans cvs caremarktm DURATION LIMIT WITH QUANTITY LIMIT AND POST LIMIT PRIOR AUTHORIZATION CRITERIA DRUG CLASS generic name, dosage form IMMEDIATE-RELEASE OPIOID ANALGESICS
Carelirst. +.V Family of health care plans cvs caremarktm DURATION LIMIT WITH QUANTITY LIMIT AND POST LIMIT PRIOR AUTHORIZATION CRITERIA DRUG CLASS generic name, dosage form IMMEDIATE-RELEASE OPIOID ANALGESICS
Impact of Opioid Prescribing Rules in Post Acute and Long Term Care
 Impact of Opioid Prescribing Rules in Post Acute and Long Term Care Jessica Van Fleet-Green, MD, FAAFP, CMD Chief Medical Officer, Physicians of Southwest Washington Medical Director, ManorCare Lacey History
Impact of Opioid Prescribing Rules in Post Acute and Long Term Care Jessica Van Fleet-Green, MD, FAAFP, CMD Chief Medical Officer, Physicians of Southwest Washington Medical Director, ManorCare Lacey History
Long-Acting Opioid. Policy Number: Last Review: 12/2017 Origination: 09/2013 Next Review: 09/2018
 Long-Acting Opioid Policy Number: 5.02.519 Last Review: 12/2017 Origination: 09/2013 Next Review: 09/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for long-acting
Long-Acting Opioid Policy Number: 5.02.519 Last Review: 12/2017 Origination: 09/2013 Next Review: 09/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for long-acting
Blueprint for Prescriber Continuing Education Program
 CDER Final 10/25/11 Blueprint for Prescriber Continuing Education Program I. Introduction: Why Prescriber Education is Important Health care professionals who prescribe extended-release (ER) and long-acting
CDER Final 10/25/11 Blueprint for Prescriber Continuing Education Program I. Introduction: Why Prescriber Education is Important Health care professionals who prescribe extended-release (ER) and long-acting
CLINICAL POLICY Clinical Policy: Extended Release Opioid Analgesics
 Reference Number: AZ.CP.PMN.97 Effective Date: 02.11 Last Review Date: 02.18 Line of Business: Medicaid- AHCCCS Revision Log See Important Reminder at the end of this policy for important regulatory and
Reference Number: AZ.CP.PMN.97 Effective Date: 02.11 Last Review Date: 02.18 Line of Business: Medicaid- AHCCCS Revision Log See Important Reminder at the end of this policy for important regulatory and
Opioid Analgesic Treatment Worksheet
 Opioid Analgesic Treatment Worksheet Aetna Better Health of Louisiana Fax: 1 844 699 2889 www.aetnabetterhealth.com/louisiana/providers/pharmacy LA Legacy Fee for Service (FFS) Medicaid Fax: 1 866 797
Opioid Analgesic Treatment Worksheet Aetna Better Health of Louisiana Fax: 1 844 699 2889 www.aetnabetterhealth.com/louisiana/providers/pharmacy LA Legacy Fee for Service (FFS) Medicaid Fax: 1 866 797
Appendix F Federation of State Medical Boards
 Appendix F Federation of State Medical Boards Model Policy Guidelines for Opioid Addiction Treatment in the Medical Office SECTION I: PREAMBLE The (name of board) recognizes that the prevalence of addiction
Appendix F Federation of State Medical Boards Model Policy Guidelines for Opioid Addiction Treatment in the Medical Office SECTION I: PREAMBLE The (name of board) recognizes that the prevalence of addiction