SAFE PRESCRIBING: RULES AND REGULATIONS. Michelle Y. Owens, MD MS State Board of Medical Licensure June 30, 2017
|
|
|
- Shanon Tyler
- 5 years ago
- Views:
Transcription
1 SAFE PRESCRIBING: RULES AND REGULATIONS Michelle Y. Owens, MD MS State Board of Medical Licensure June 30, 2017
2 DISCLOSURES I have no financial disclosures.
3 OBJECTIVES Discuss the significance of the opiate epidemic Name 2 recommendations from the CDC guidelines on opiate prescribing Name one clinical manifestation of Neonatal Abstinence Syndrome
4 OPIATES Heroin Codeine Fentanyl Morphine Methadone Oxycodone Meperidine Hydromorphone Hydrocodone Propoxyphene Buprenorphine
5 TERMS TO KNOW: Abuse Opiate Use Disorder Dependence Tolerance Addiction Withdrawal Overdose
6 SUBSTANCE ABUSE A maladaptive pattern of substance use resulting in significant negative physical, social, interpersonal or legal consequences.
7 DEPENDENCE Physical dependence - is a physiological state of adaptation to a substance, the absence of which produces symptoms and signs of withdrawal. Psychological dependence Mentally dependent upon a substance. DSM-V definition Substance use disorder, may include physical dependence, but additional criteria are required.
8 OPIATE USE DISORDER (OUD) A problematic pattern of opioid use that causes clinically significant impairment or distress. A diagnosis is based on specific criteria such as unsuccessful efforts to cut down or control use, as well as use resulting in social problems and a failure to fulfill obligations at work, school, or home. Opioid use disorder has also been referred to as opioid abuse or dependence or opioid addiction.
9 TOLERANCE A condition in which higher doses of a drug are required to produce the same effect experienced during initial use.
10 ADDICTION Chronic relapsing brain disease characterized by compulsive drug seeking and use, despite harmful consequences. Four C s Craving Control Compulsion Consequences
11 WITHDRAWAL A constellation of symptoms and signs that a person experiences when after a period of regular use, the quantity of available substance to the brain is reduced.
12 OVERDOSE Injury to the body that happens when a drug is taken in excessive amounts. An overdose can be fatal or nonfatal.
13
14
15
16
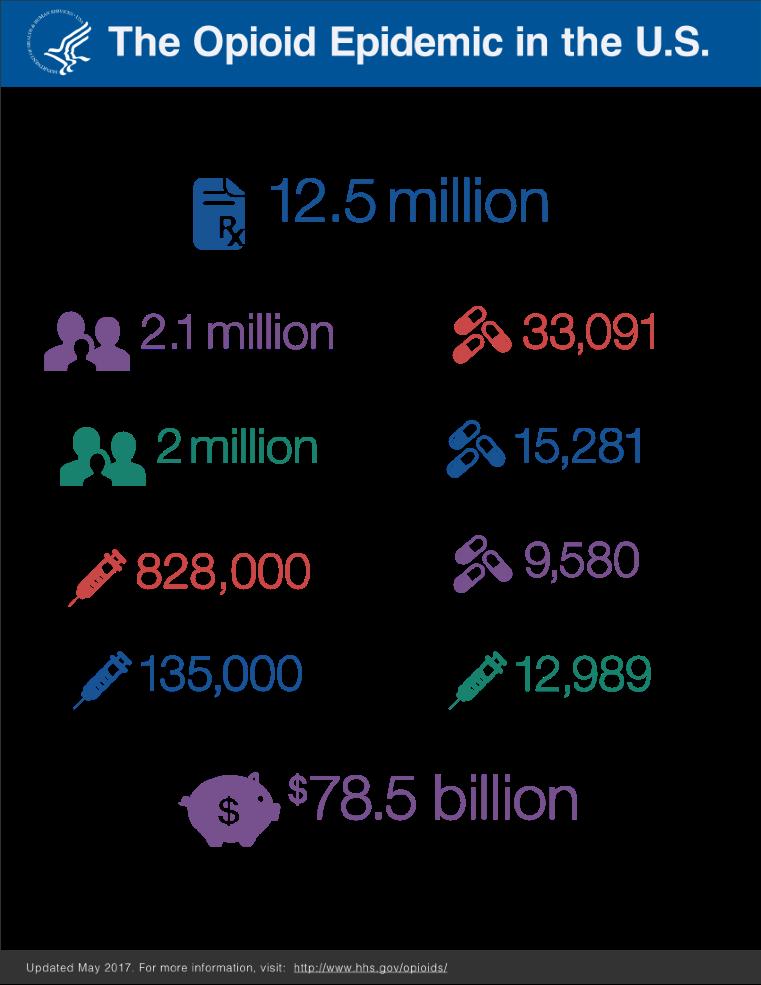
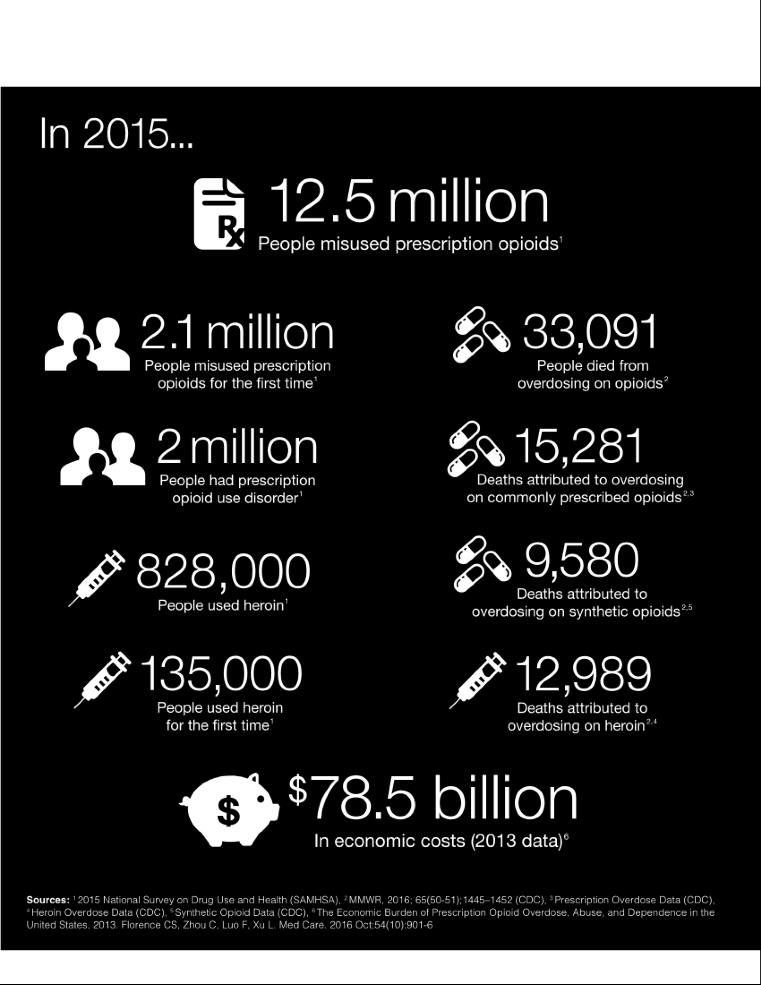
17 WOMEN AND OPIATES HIGH RISK ALERT About 18 women die every day of a prescription painkiller overdose in the US, more than 6,600 deaths in Prescription painkiller overdoses are an under-recognized and growing problem for women. The 2015 National Survey on Drug Use and Health found that 4 percent of females age 12 and older misused prescription pain relievers in the last year.
18 WOMEN AND OPIATES HIGH RISK ALERT Women are more likely than men to have chronic pain, to be prescribed prescription pain relievers, to be given higher doses, and to use them for longer time periods. Women may become dependent on prescription pain relievers more quickly than men and may experience more cravings than men. Psychological and emotional distress are risk factors for opioid misuse among women, but not among men.
19 WOMEN AND OPIATES HIGH RISK ALERT Women are more likely to be introduced to substances by a partner; men are more likely to be introduce by a peer. Rates of childhood and adult sexual abuse, risk factors for substance misuse, are higher among women than men. Women are more likely than men to have co-occurring mental health and substance use disorders.

20 WOMEN AND OPIATES: HIGH RISK ALERT
21 WHAT CAN WE DO? Recognize that women are at risk of prescription painkiller overdose. Follow guidelines for responsible prescribing, including screening and monitoring for substance abuse and mental health problems. Use prescription drug monitoring programs to identify patients who may be improperly obtaining or using prescription painkillers and other drugs.
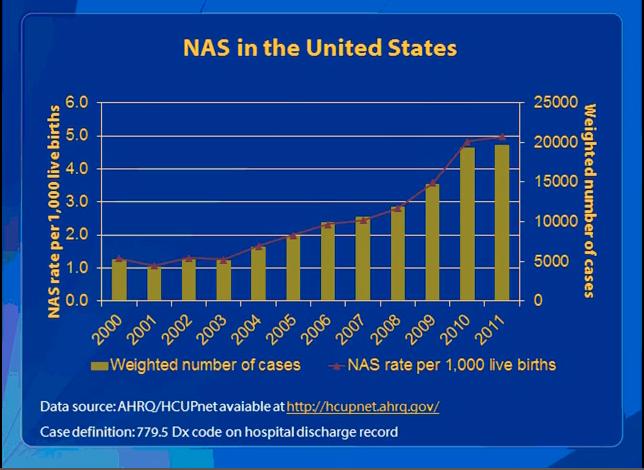
22 NEONATAL ABSTINENCE SYNDROME (NAS) Incidence 55-94% in mothers with opioid abuse National prevalence increasing (doubled in less than 10 years)
23
24
25 NEONATAL ABSTINENCE SYNDROME (NAS) Central Nervous System Seizure activity Irritability Exaggerated Moro reflex Increased muscle tone Gastrointestinal Dysfunction Vomiting Diarrhea Poor weight gain Feeding difficulties
26 NEONATAL ABSTINENCE SYNDROME (NAS) Tx: Tincture of opium Similar with methadone or buprenorphine Longer hospitalization for neonate Buprenorphine and NAS: MOTHER trial Severity of NAS (treatment dose, hospital stay, NAS score) Less with buprenorphine vs. methadone Lower concentrations in fetal circulation compared with methadone (50% less drug exposure).
27
28 DOES IT MATTER? During pregnancy, 10% (55) of women drink alcohol (4% binge, ie, had >5 alcoholic drinks on the same occasion on at least 1 day in the past 30 days), 15% (23) smoke cigarettes, and 5% (10) use an illicit substance. Substance use is as or more common than many conditions routinely screened for and assessed during prenatal care (PNC), such as cystic fibrosis, gestational diabetes, anemia, postpartum depression, or preeclampsia.
29 REGULATIONS AND PRESCRIBING
30 NEED FOR OPIOID PRESCRIBING GUIDELINES Previous opioid prescribing guidelines have been developed by several states and agencies but were inconsistent Most recent national guidelines are several years old and don t incorporate the most recent evidence Need for clear, consistent recommendations
31 CHRONIC PAIN AND PRESCRIPTION OPIOIDS 11% of Americans experience daily (chronic) pain Opioids frequently prescribed for chronic pain Primary care providers commonly treat chronic, non-cancer pain account for ~50% of opioid pain medications dispensed report concern about opioids and insufficient training
32 PURPOSE, USE, AND PRIMARY AUDIENCE Primary Care Providers Family medicine, Internal medicine Physicians, nurse practitioners, physician assistants Treating patients >18 years with chronic pain Pain longer than 3 months or past time of normal tissue healing Outpatient settings Does not include active cancer treatment, palliative care, and end-of-life care

33 OPIOID PRESCRIPTIONS AND INCREASING DEATHS

34 ROLE OF PRESCRIBING OPIOIDS AND OVERDOSE DEATHS *Death rate, 2013, National Vital Statistics System. Opioid pain reliever sales rate, 2013, DEA s Automation of Reports and Consolidated Orders System
35 GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN
36 CDC GUIDELINES 2016: ORGANIZATION OF RECOMMENDATIONS The 12 recommendations are grouped into three conceptual areas: Determining when to initiate or continue opioids for chronic pain Opioid selection, dosage, duration, follow-up, and discontinuation Assessing risk and addressing harms of opioid use CDC.gov
37 DETERMINE WHEN TO INITIATE OR CONTINUE OPIOIDS FOR CHRONIC PAIN
38 RECOMMENDATION #1 Nonpharmacologic therapy and nonopioid pharmacologic therapy are preferred for chronic pain. Clinicians should consider opioid therapy only if expected benefits for both pain and function are anticipated to outweigh risks to the patient. If opioids are used, they should be combined with nonpharmacologic therapy and nonopioid pharmacologic therapy, as appropriate. (Recommendation category A: Evidence type: 3)
39 OPIOIDS NOT FIRST-LINE OR ROUTINE THERAPY FOR CHRONIC PAIN Use nonpharmacologic therapy such as exercise or cognitive behavioral therapy (CBT) to reduce pain and improve function. Use nonopioid pharmacologic therapy (nonsteroidal antiinflammatory drugs, acetaminophen, anticonvulsants, certain antidepressants) when benefits outweigh risks, combined with nonpharmacologic therapy. When opioids used, combine with nonpharmacologic therapy and nonopioid pharmacologic therapy to provide greater benefits.
40 RECOMMENDATION #2 Before starting opioid therapy for chronic pain, clinicians should establish treatment goals with all patients, including realistic goals for pain and function, and should consider how therapy will be discontinued if benefits do not outweigh risks. Clinicians should continue opioid therapy only if there is clinically meaningful improvement in pain and function that outweighs risks to patient safety. (Recommendation category A: Evidence type: 4)
41 ESTABLISH AND MEASURE PROGRESS TOWARD GOALS Before initiating opioid therapy for chronic pain Determine how effectiveness will be evaluated. Establish treatment goals with patients. opain relief ofunction Assess progress using 3-item PEG Assessment Scale* Pain average (0-10) Interference with Enjoyment of life (0-10) Interference with General activity (0-10) *30% = clinically meaningful improvement
42 RECOMMENDATION #3 Before starting and periodically during opioid therapy, clinicians should discuss with patients known risks and realistic benefits of opioid therapy and patient and clinician responsibilities for managing therapy. (Recommendation category A: Evidence type: 3)
43 ENSURE PATIENTS ARE AWARE OF POTENTIAL BENEFITS, HARMS, AND ALTERNATIVES TO OPIOIDS Be explicit and realistic about expected benefits. Emphasize goal of improvement in pain and function. Discuss serious and common adverse effects increased risks of overdose oat higher dosages owhen opioids are taken with other drugs or alcohol periodic reassessment, PDMP and urine checks; and risks to family members and individuals in the community.
44 OPIOID SELECTION, DOSAGE, DURATION, FOLLOW-UP, AND DISCONTINUATION
45 RECOMMENDATION #4 When starting opioid therapy for chronic pain, clinicians should prescribe immediate-release opioids instead of extended-release/ long-acting (ER/LA) opioids. (Recommendation category A: Evidence type: 4)
46 CHOOSE PREDICTABLE PHARMACOKINETICS AND PHARMACODYNAMICS TO MINIMIZE OVERDOSE RISK In general, avoid the use of immediate-release opioids combined with ER/LA opioids. Methadone should not be the first choice for an ER/LA opioid. Only providers familiar with methadone s unique risk and who are prepared to educate and closely monitor their patients should consider prescribing it for pain. Only consider prescribing transdermal fentanyl if familiar with the dosing and absorption properties and prepared to educate patients about its use.
47 RECOMMENDATION #5 When opioids are started, clinicians should prescribe the lowest effective dosage. Clinicians should use caution when prescribing opioids at any dosage, should carefully reassess evidence of individual benefits and risks when increasing dosage to 50 morphine milligram equivalents (MME)/day, and should avoid increasing dosage to 90 MME/day or carefully justify a decision to titrate dosage to >90 MME/day. (Recommendation category A: Evidence type: 3)
48 START LOW AND GO SLOW Start with lowest effective dosage and increase by the smallest practical amount. If total opioid dosage >50 MME/day reassess pain, function, and treatment increase frequency of follow-up; and consider offering naloxone. Avoid increasing opioid dosages to >90 MME/day. If escalating dosage requirements discuss other pain therapies with the patient consider working with the patient to taper opioids down or off consider consulting a pain specialist.
49 IF PATIENT IS ALREADY RECEIVING A HIGH DOSAGE Offer established patients already taking >90 MME/day the opportunity to re-evaluate their continued use of high opioid dosages in light of recent evidence regarding the association of opioid dosage and overdose risk. For patients who agree to taper opioids to lower dosages, collaborate with the patient on a tapering plan.
50 RECOMMENDATION #6 Long-term opioid use often begins with treatment of acute pain. When opioids are used for acute pain, clinicians should prescribe the lowest effective dose of immediate-release opioids and should prescribe no greater quantity than needed for the expected duration of pain severe enough to require opioids. 3 days or less will often be sufficient; more than 7 days will rarely be needed. (Recommendation category A: Evidence type: 4)
51 WHEN OPIOIDS ARE NEEDED FOR ACUTE PAIN Prescribe the lowest effective dose. Prescribe amount to match the expected duration of pain severe enough to require opioids. Often < 3 days and rarely more than 7 days needed. Do not prescribe additional opioids just in case. Re-evaluate patients with severe acute pain that continues longer than the expected duration to confirm or revise the initial diagnosis and to adjust management accordingly. Do not prescribe ER/LA opioids for acute pain treatment.
52 RECOMMENDATION #7 Clinicians should evaluate benefits and harms with patients within 1 to 4 weeks of starting opioid therapy for chronic pain or of dose escalation. Clinicians should evaluate benefits and harms of continued therapy with patients every 3 months or more frequently. If benefits do not outweigh harms of continued opioid therapy, clinicians should optimize other therapies and work with patients to taper opioids to lower dosages or to taper and discontinue opioids. (Recommendation category A: Evidence type: 4)
53 FOLLOW-UP Re-evaluate patients within 1-4 weeks of starting long-term therapy or of dosage increase at least every 3 months or more frequently. At follow up, determine whether opioids continue to meet treatment goals there are common or serious adverse events or early warning signs benefits of opioids continue to outweigh risks opioid dosage can be reduced or opioids can be discontinued.
54 TAPERING OPIOIDS Work with patients to taper opioids down or off when no sustained clinically meaningful improvement in pain and function opioid dosages >50 MME/day without evidence of benefit concurrent benzodiazepines that can t be tapered off patients request dosage reduction or discontinuation patients experience overdose, other serious adverse events, warning signs. Taper slowly enough to minimize opioid withdrawal A decrease of 10% per week is a reasonable starting point Access appropriate expertise for tapering during pregnancy Optimize nonopioid pain management and psychosocial support
55 ASSESSING RISK AND ADDRESSING HARMS OF OPIOID USE
56 RECOMMENDATION #8 Before starting and periodically during continuation of opioid therapy, clinicians should evaluate risk factors for opioid-related harms. Clinicians should incorporate into the management plan strategies to mitigate risk, including considering offering naloxone when factors that increase risk for opioid overdose, such as history of overdose, history of substance use disorder, higher opioid dosages (>50 MME/day), or concurrent benzodiazepine use, are present. (Recommendation category A: Evidence type: 4)
57 CERTAIN FACTORS INCREASE RISKS FOR OPIOID- ASSOCIATED HARMS Avoid prescribing opioids to patients with moderate or severe sleepdisordered breathing when possible. During pregnancy, carefully weigh risks and benefits with patients. Use additional caution with renal or hepatic insufficiency, aged >65 years. Ensure treatment for depression is optimized. Consider offering naloxone when patients have a history of overdose have a history of substance use disorder are taking central nervous system depressants with opioids are on higher dosages of opioids (> 50 MME/day).
58 RECOMMENDATION #9 Clinicians should review the patient s history of controlled substance prescriptions using state PDMP data to determine whether the patient is receiving opioid dosages or dangerous combinations that put him/her at high risk for overdose Clinicians should review PDMP data when starting opioid therapy for chronic pain and periodically during opioid therapy for chronic pain, ranging from every prescription to every 3 months. (Recommendation category A: Evidence type: 4)
59 IF PRESCRIPTIONS FROM MULTIPLE SOURCES, HIGH DOSAGES, OR DANGEROUS COMBINATIONS Discuss safety concerns with patient (and any other prescribers they may have), including increased risk for overdose. For patients receiving high total opioid dosages, consider tapering to a safer dosage, consider offering naloxone. Consider opioid use disorder and discuss concerns with your patient. If you suspect your patient might be sharing or selling opioids and not taking them, consider urine drug testing to assist in determining whether opioids can be discontinued without causing withdrawal. Do not dismiss patients from care use the opportunity to provide potentially lifesaving information and interventions.
60 RECOMMENDATION #10 When prescribing opioids for chronic pain, clinicians should use urine drug testing before starting opioid therapy and consider urine drug testing at least annually to assess for prescribed medications as well as other controlled prescription drugs and illicit drugs. (Recommendation category B: Evidence type: 4)
61 USE UDT TO ASSESS FOR PRESCRIBED OPIOIDS AND OTHER DRUGS THAT INCREASE RISK Be familiar with urine drug testing panels and how to interpret results. Don t test for substances that wouldn t affect patient management. Before ordering urine drug testing explain to patients that testing is intended to improve their safety explain expected results; and ask patients whether there might be unexpected results. Discuss unexpected results with local lab and patients. Verify unexpected, unexplained results using specific test. Do not dismiss patients from care based on a urine drug test result.
62 RECOMMENDATION #11 Clinicians should avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible. (Recommendation category A: Evidence type: 3)
63 AVOID CONCURRENT OPIOIDS AND BENZODIAZEPINES WHENEVER POSSIBLE Taper benzodiazepines gradually. Offer evidence-based psychotherapies for anxiety. cognitive behavioral therapy specific anti-depressants approved for anxiety other non-benzodiazepine medications approved for anxiety Coordinate care with mental health professionals.
64 RECOMMENDATION #12 Clinicians should offer or arrange evidence-based treatment (usually medication-assisted treatment with buprenorphine or methadone in combination with behavioral therapies) for patients with opioid use disorder. (Recommendation category A: Evidence type: 2)
65 IF YOU SUSPECT OPIOID USE DISORDER (OUD) Discuss with your patient and provide an opportunity to disclose concerns. Assess for OUD using DSM-5 criteria. If present, offer or arrange MAT. Buprenorphine through an office-based buprenorphine treatment provider or an opioid treatment program specialist Methadone maintenance therapy from an opioid treatment program specialist Oral or long-acting injectable formulations of naltrexone (for highly motivated non-pregnant adults) Consider obtaining a waiver to prescribe buprenorphine for OUD (see
66 TOOLS AND RESOURCES
67
68 BURNOUT
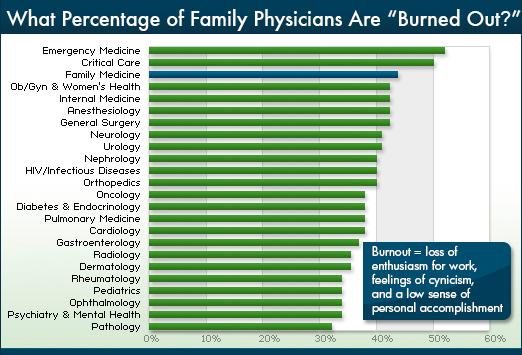
69 BURNOUT STATISTICS Over 54% of physicians affected >400,000 people All specialties Effects all levels of the medical hierarchy (students, residents, and attendings)
70
71
72
73
74 SIGNS OF BURNOUT: Depleted enthusiasm Social isolation Emotional volatility Patient depersonalization Chemical stimulation Change in sleeping habits Diminished physical activity
75
76 CHALLENGES Physicians do not reliably self-assess their own distress (Dyrbye 2013) How we deal with stress Intellectualize Minimize Intensify
77 HIGH-RISK CHARACTERISTICS Hectic schedule Strong achievement orientation The inability to say no.
78
79 FALLOUT FROM BURNOUT Decreased patient satisfaction Increased job turnover and reduced hours Increased medical errors Increased malpractice risk Increased potential for patient harm
80 OTHER MANIFESTATIONS Disruptive behavior Motor vehicle accidents and near-misses Depression Substance use disorders Suicide

81 BURNOUT AND PHYSICIAN SUICIDE
82 BURNOUT AND PHYSICIAN SUICIDE Highest suicide rate of any profession. More than twice as likely to commit suicide than non-physicians. More attempts and higher success rates than the general population. Males : 40% higher Females: 130% higher
83 BURNOUT AND PHYSICIAN SUICIDE Suicide is the 2 nd most common cause of death in medical students. 50% of students met criteria for burnout over the past year. 11% met criteria for suicidal ideation in the past year. Dyrbye et al, Annals Int Med 2008
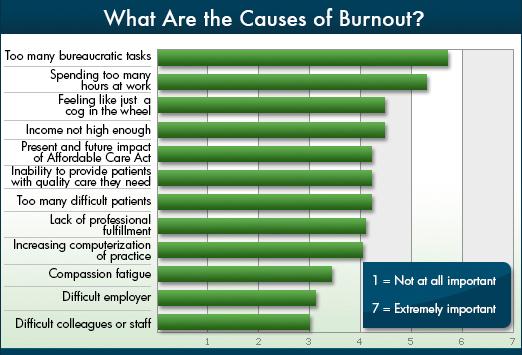
84 KEY DRIVERS: Excessive workload Inefficient work environment, inadequate support Loss of autonomy/flexibility/control Loss of meaning in work Problems with work-life integration and balance
85 REMEDIES: WHAT DOES THE LITERATURE SAY? Making choices (work/life balance) Stress management techniques Spiritual nurturing Positive life philosophy Self-care Strive for meaning in work
86
87
88 ONE OF THE MYSTERIES OF ILLNESS IS THAT NO ONE CAN BE HEALED BY ANYONE WHOSE EMPTINESS IS GREATER THAN THEIR OWN. Mark Nepo
89
90 THANK YOU!
CDC Guideline for Prescribing Opioids for Chronic Pain. Centers for Disease Control and Prevention National Center for Injury Prevention and Control
 CDC Guideline for Prescribing Opioids for Chronic Pain Centers for Disease Control and Prevention National Center for Injury Prevention and Control THE EPIDEMIC Chronic Pain and Prescription Opioids 11%
CDC Guideline for Prescribing Opioids for Chronic Pain Centers for Disease Control and Prevention National Center for Injury Prevention and Control THE EPIDEMIC Chronic Pain and Prescription Opioids 11%
New Guidelines for Prescribing Opioids for Chronic Pain
 New Guidelines for Prescribing Opioids for Chronic Pain Andrew Lowe, Pharm.D. CAPA Meeting October 6, 2016 THE EPIDEMIC Chronic Pain and Prescription Opioids 11% of Americans experience daily (chronic)
New Guidelines for Prescribing Opioids for Chronic Pain Andrew Lowe, Pharm.D. CAPA Meeting October 6, 2016 THE EPIDEMIC Chronic Pain and Prescription Opioids 11% of Americans experience daily (chronic)
New Guidelines for Opioid Prescribing
 New Guidelines for Opioid Prescribing What They Mean for Elders with Chronic Pain Manu Thakral, PhD, ARNP Kaiser Permanente Washington Health Research Institute Kaiser Permanente Washington Health Research
New Guidelines for Opioid Prescribing What They Mean for Elders with Chronic Pain Manu Thakral, PhD, ARNP Kaiser Permanente Washington Health Research Institute Kaiser Permanente Washington Health Research
Non Opioid Approaches to Pain and Musculoskeletal Disorders KEVIN ODONNELL, DO FLAGSTAFF BONE AND JOINT
 Non Opioid Approaches to Pain and Musculoskeletal Disorders KEVIN ODONNELL, DO FLAGSTAFF BONE AND JOINT Learning Objectives Review Opioid Crisis CDC Guidelines for opioid prescribing Discuss Alternatives
Non Opioid Approaches to Pain and Musculoskeletal Disorders KEVIN ODONNELL, DO FLAGSTAFF BONE AND JOINT Learning Objectives Review Opioid Crisis CDC Guidelines for opioid prescribing Discuss Alternatives
Summary of Recommendations...3. PEG: A Three-Item Scale Assessing Pain (Appendix A) Chronic Pain Flow Sheet Acute Pain Flow Sheet...
 Chronic Pain Flow Sheet Acute Pain Flow Sheet...") Table of Contents Summary of Recommendations....3 PEG: A Three-Item Scale Assessing Pain (Appendix A)...12 Chronic Pain Flow Sheet...13 Acute Pain Flow Sheet...14 Pocket Guide: Tapering Opioids for Chronic
Table of Contents Summary of Recommendations....3 PEG: A Three-Item Scale Assessing Pain (Appendix A)...12 Chronic Pain Flow Sheet...13 Acute Pain Flow Sheet...14 Pocket Guide: Tapering Opioids for Chronic
THE PROS & CONS OF THE CDC GUIDELINES FOR SAFE OPIOID PRESCRIBING
 THE PROS & CONS OF THE CDC GUIDELINES FOR SAFE OPIOID PRESCRIBING Ernest J Dole, PharmD, PhC, FASHP, BCPS Clinical Pharmacist University of New Mexico Hospitals And Clinical Associate Professor University
THE PROS & CONS OF THE CDC GUIDELINES FOR SAFE OPIOID PRESCRIBING Ernest J Dole, PharmD, PhC, FASHP, BCPS Clinical Pharmacist University of New Mexico Hospitals And Clinical Associate Professor University
CDC Guideline for Prescribing Opioids for Chronic Pain
 National Center for Injury Prevention and Control CDC Guideline for Prescribing Opioids for Chronic Pain John Halpin, MD, MPH Medical Officer Division of Unintentional Injury Prevention Prescription Drug
National Center for Injury Prevention and Control CDC Guideline for Prescribing Opioids for Chronic Pain John Halpin, MD, MPH Medical Officer Division of Unintentional Injury Prevention Prescription Drug
Knock Out Opioid Abuse in New Jersey:
 Knock Out Opioid Abuse in New Jersey: A Resource for Safer Prescribing GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN IMPROVING PRACTICE THROUGH RECOMMENDATIONS CDC s Guideline for Prescribing Opioids
Knock Out Opioid Abuse in New Jersey: A Resource for Safer Prescribing GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN IMPROVING PRACTICE THROUGH RECOMMENDATIONS CDC s Guideline for Prescribing Opioids
Opiate Use Disorder and Opiate Overdose
 Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
Opioid Review and MAT Clinic CDC Guidelines
 1 Opioid Review and MAT Clinic CDC Guidelines January 10, 2018 Housekeeping Use chat feature to inform everyone who s at your clinic Click chat on Zoom option bar Chat Everyone the names of those who are
1 Opioid Review and MAT Clinic CDC Guidelines January 10, 2018 Housekeeping Use chat feature to inform everyone who s at your clinic Click chat on Zoom option bar Chat Everyone the names of those who are
HOPE. Considerations. Considerations ISING. Safe Opioid Prescribing Guidelines for ACUTE Non-Malignant Pain
 Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
Prescribing Opioids in the Opioid Epidemic. Scott Woffinden, PA-C Jason Chapman, JD
 Prescribing Opioids in the Opioid Epidemic Scott Woffinden, PA-C Jason Chapman, JD What's the Problem? http://www.zdoggmd.com/blank-script-taylor-swift-parody/ What's the Problem? CDC 115 Americans die
Prescribing Opioids in the Opioid Epidemic Scott Woffinden, PA-C Jason Chapman, JD What's the Problem? http://www.zdoggmd.com/blank-script-taylor-swift-parody/ What's the Problem? CDC 115 Americans die
Prescribing drugs of dependence in general practice, Part C
 HO O Prescribing drugs of dependence in general practice, Part C Key recommendations and practice points for management of pain with opioid therapy H H HO N CH3 Acute pain Acute pain is an unpleasant sensory
HO O Prescribing drugs of dependence in general practice, Part C Key recommendations and practice points for management of pain with opioid therapy H H HO N CH3 Acute pain Acute pain is an unpleasant sensory
Revised 9/30/2016. Primary Care Provider Pain Management Toolkit
 Revised 9/30/2016 Primary Care Provider Pain Management Toolkit TABLE OF CONTENTS 1. INTRODUCTION Page 1 2. NON-OPIOID SERVICES &TREATMENTS FOR CHRONIC PAIN Page 2 2.1 Medical Services Page 2 2.2 Behavioral
Revised 9/30/2016 Primary Care Provider Pain Management Toolkit TABLE OF CONTENTS 1. INTRODUCTION Page 1 2. NON-OPIOID SERVICES &TREATMENTS FOR CHRONIC PAIN Page 2 2.1 Medical Services Page 2 2.2 Behavioral
Opioid Management of Chronic (Non- Cancer) Pain
 Pain") Optima Health Opioid Management of Chronic (Non- Cancer) Pain Guideline History Original Approve Date 5/08 Review/Revise Dates 11/09, 9/11, 9/13, 09/15, 9/17 Next Review Date 9/19 These Guidelines are
Optima Health Opioid Management of Chronic (Non- Cancer) Pain Guideline History Original Approve Date 5/08 Review/Revise Dates 11/09, 9/11, 9/13, 09/15, 9/17 Next Review Date 9/19 These Guidelines are
Rule Governing the Prescribing of Opioids for Pain
 Rule Governing the Prescribing of Opioids for Pain 1.0 Authority This rule is adopted pursuant to Sections 14(e) and 11(e) of Act 75 (2013) and Sections 2(e) and 2a of Act 173 (2016). 2.0 Purpose This
Rule Governing the Prescribing of Opioids for Pain 1.0 Authority This rule is adopted pursuant to Sections 14(e) and 11(e) of Act 75 (2013) and Sections 2(e) and 2a of Act 173 (2016). 2.0 Purpose This
Full details and resource documents available:
 Clinical & Regulatory News by Pharmerica Urinary Tract Infection (UTI) Second Most Common Cause of Hospital Readmission within 30 days UTIs are prevalent and account for up to 22% of infections in LTC,
Clinical & Regulatory News by Pharmerica Urinary Tract Infection (UTI) Second Most Common Cause of Hospital Readmission within 30 days UTIs are prevalent and account for up to 22% of infections in LTC,
Re: Draft Guideline for the Use of Opioids for Chronic Pain (Docket No. CDC )
") January 13, 2016 Veronica Kennedy Acting Executive Secretary, Centers for Disease Control and Prevention National Center for Injury Prevention and Control, Centers for Disease Control and Prevention, 4770
January 13, 2016 Veronica Kennedy Acting Executive Secretary, Centers for Disease Control and Prevention National Center for Injury Prevention and Control, Centers for Disease Control and Prevention, 4770
Recommendations in Opioid Prescribing Guidelines for Chronic Pain
 Recommendations in Opioid Prescribing Guidelines for Chronic Pain The use of opioids for treating chronic pain has been increasing. 1 In 2010, an estimated 20% of patients presenting to physician offices
Recommendations in Opioid Prescribing Guidelines for Chronic Pain The use of opioids for treating chronic pain has been increasing. 1 In 2010, an estimated 20% of patients presenting to physician offices
Standard of Practice for Prescribing Opioids (Excluding Cancer, Palliative, and End-of-Life Care)
") Standard of Practice for Prescribing Opioids (Excluding Cancer, Palliative, and End-of-Life Care) Preamble This Standard establishes the standards of practice and ethical requirements of all physicians
Standard of Practice for Prescribing Opioids (Excluding Cancer, Palliative, and End-of-Life Care) Preamble This Standard establishes the standards of practice and ethical requirements of all physicians
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2018 P 4000-3 Program Opioid Overutilization Cumulative Drug Utilization Review Criteria Medication Includes all salt forms, single and
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2018 P 4000-3 Program Opioid Overutilization Cumulative Drug Utilization Review Criteria Medication Includes all salt forms, single and
SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF CHRONIC NON-TERMINAL PAIN (CNTP)
") 9 SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF CHRONIC NON-TERMINAL PAIN (CNTP) SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF ACUTE PAIN NONOPIOID TREATMENTS
9 SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF CHRONIC NON-TERMINAL PAIN (CNTP) SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF ACUTE PAIN NONOPIOID TREATMENTS
Management of Pain - A Comparison of Current Guidelines
 Management of Pain - A Comparison of Current Guidelines The Centers for Disease Control and Prevention (CDC) released a guideline in 2016 regarding the prescribing of opioids for chronic non-cancer pain
Management of Pain - A Comparison of Current Guidelines The Centers for Disease Control and Prevention (CDC) released a guideline in 2016 regarding the prescribing of opioids for chronic non-cancer pain
Scope of the Opiate Problem 6/5/18. Chronic Pain Management and the Use of Opioid Medications: The CDC Guideline and Beyond. Overview.
 Chronic Pain Management and the Use of Opioid Medications: The CDC Guideline and Beyond David Anisman, MD Medical Director, Farmington Health Center (Primary Care) Associate Medical Director, Community
Chronic Pain Management and the Use of Opioid Medications: The CDC Guideline and Beyond David Anisman, MD Medical Director, Farmington Health Center (Primary Care) Associate Medical Director, Community
Prescription Opioids in Vermont A DISCUSSION ABOUT LAWS AND GUIDELINES MICHAEL J. KENOSH, MD
 Prescription Opioids in Vermont A DISCUSSION ABOUT LAWS AND GUIDELINES MICHAEL J. KENOSH, MD Rule(s) Governing the Prescribing of Opioids for Pain KEY rule adopted pursuant to Sections 14(e) and 11(e)
Prescription Opioids in Vermont A DISCUSSION ABOUT LAWS AND GUIDELINES MICHAEL J. KENOSH, MD Rule(s) Governing the Prescribing of Opioids for Pain KEY rule adopted pursuant to Sections 14(e) and 11(e)
Bree Collaborative AMDG Opioid Prescribing Guidelines Workgroup. Opioid Prescribing Metrics - DRAFT
 Bree Collaborative AMDG Opioid Prescribing Guidelines Workgroup Opioid Prescribing Metrics - DRAFT Definitions: Days Supply: The total of all opioid prescriptions dispensed during the calendar quarter
Bree Collaborative AMDG Opioid Prescribing Guidelines Workgroup Opioid Prescribing Metrics - DRAFT Definitions: Days Supply: The total of all opioid prescriptions dispensed during the calendar quarter
Ken Roy, MD, FASAM. The Opioid Epidemic and Addiction Involving the Use of Opioids. Tulane & LSU Department of Psychiatry
 Ken Roy, MD, FASAM The Opioid Epidemic and Addiction Involving the Use of Opioids Addiction Recovery Resources, Inc. Tulane & LSU Department of Psychiatry www.arrno.com kenroymd@cox.net CDC Guidelines
Ken Roy, MD, FASAM The Opioid Epidemic and Addiction Involving the Use of Opioids Addiction Recovery Resources, Inc. Tulane & LSU Department of Psychiatry www.arrno.com kenroymd@cox.net CDC Guidelines
MOA: Practice Managers Program. Presented by: Kimber Debelak, CMC, CMOM, CMIS. May 17, zpain Management. & New Opioid Laws
 MOA: Practice Managers Program Presented by: Kimber Debelak, CMC, CMOM, CMIS May 17, 2018 Pain Management & New Opioid Laws Objectives and Educational Statement Objectives To understand the need for new
MOA: Practice Managers Program Presented by: Kimber Debelak, CMC, CMOM, CMIS May 17, 2018 Pain Management & New Opioid Laws Objectives and Educational Statement Objectives To understand the need for new
2/21/2018. What are Opioids?
 Opioid Crisis: South Carolina Responds Carolyn Bogdon, MSN, FNP-BC Coordinator for Emergency Department Medication Assisted Treatment Program Medical University of South Carolina Opioid Crisis: A Mounting
Opioid Crisis: South Carolina Responds Carolyn Bogdon, MSN, FNP-BC Coordinator for Emergency Department Medication Assisted Treatment Program Medical University of South Carolina Opioid Crisis: A Mounting
(Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines)
") Buprenorphine Initiation and Maintenance in Pregnancy (Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines) Assessment The diagnosis of OUD should be confirmed by DSM-5
Buprenorphine Initiation and Maintenance in Pregnancy (Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines) Assessment The diagnosis of OUD should be confirmed by DSM-5
Brief History of Methadone Maintenance Treatment
 METHADONE Brief History of Methadone Maintenance Treatment Methadone maintenance treatment was on the cusp of the social revolution in the sixties. Doctors and public health workers had concluded what
METHADONE Brief History of Methadone Maintenance Treatment Methadone maintenance treatment was on the cusp of the social revolution in the sixties. Doctors and public health workers had concluded what
Proposed Revision to Med (i)
") Proposed Revision to Med 501.02 (i) I. Purpose This rule has been adopted to enable the Board to best protect public health and safety while providing a framework for licensees to effectively treat and
Proposed Revision to Med 501.02 (i) I. Purpose This rule has been adopted to enable the Board to best protect public health and safety while providing a framework for licensees to effectively treat and
Pain Management and Opioid Treatment Services
 Pain Management and Opioid Treatment Services Davis, CA (530) 753-4300; Voice mail: (916) 715-5856 davidmeelee@gmail.com www.changecompanies.net www.trainforchange.net www.tipsntopics.com www.asamcriteria.org
Pain Management and Opioid Treatment Services Davis, CA (530) 753-4300; Voice mail: (916) 715-5856 davidmeelee@gmail.com www.changecompanies.net www.trainforchange.net www.tipsntopics.com www.asamcriteria.org
Opioid Analgesics: Responsible Prescribing in the Midst of an Epidemic
 Opioid Analgesics: Responsible Prescribing in the Midst of an Epidemic Lucas Buffaloe, MD Associate Professor of Clinical Family and Community Medicine University of Missouri Health Care Goals for today
Opioid Analgesics: Responsible Prescribing in the Midst of an Epidemic Lucas Buffaloe, MD Associate Professor of Clinical Family and Community Medicine University of Missouri Health Care Goals for today
Linking Opioid Treatment in Primary Care. Roxanne Lewin M.D.
 Roxanne Lewin M.D. The Facts Fewer than 10 percent of individuals with an alcohol use disorder and only about 20 percent of individuals with an opioid use disorder receive specialty treatment. Many individuals
Roxanne Lewin M.D. The Facts Fewer than 10 percent of individuals with an alcohol use disorder and only about 20 percent of individuals with an opioid use disorder receive specialty treatment. Many individuals
The STOP Measure. Safe and Transparent Opioid Prescribing to Promote Patient Safety and Reduced Risk of Opioid Misuse FEBRUARY 2018
 The STOP Measure Safe and Transparent Opioid Prescribing to Promote Patient Safety and Reduced Risk of Opioid Misuse FEBRUARY 2018 AHIP s Safe, Transparent Opioid Prescribing (STOP) Initiative Methodology
The STOP Measure Safe and Transparent Opioid Prescribing to Promote Patient Safety and Reduced Risk of Opioid Misuse FEBRUARY 2018 AHIP s Safe, Transparent Opioid Prescribing (STOP) Initiative Methodology
Mark Edlund, MD, PhD RTI International. Photo courtesy of The Herb Museum, Vancouver, BC
 Opioid Use Disorders and Their Treatment Mark Edlund, MD, PhD RTI International Photo courtesy of The Herb Museum, Vancouver, BC Acknowledgements Funded by NIDA R01 DA022560-01 NIDA R01 DA034627 NIDA R01
Opioid Use Disorders and Their Treatment Mark Edlund, MD, PhD RTI International Photo courtesy of The Herb Museum, Vancouver, BC Acknowledgements Funded by NIDA R01 DA022560-01 NIDA R01 DA034627 NIDA R01
Appropriate Prescribing of Opioids for Chronic Non Cancer Pain
 Appropriate Prescribing of Opioids for Chronic Non Cancer Pain Dr. Cheri Olson La Crosse Mayo Family Medicine Residency Assistant Professor of Family Medicine, Mayo Graduate School of Medicine Disclosure
Appropriate Prescribing of Opioids for Chronic Non Cancer Pain Dr. Cheri Olson La Crosse Mayo Family Medicine Residency Assistant Professor of Family Medicine, Mayo Graduate School of Medicine Disclosure
SUBOXONE Film, SUBOXONE Tablets, and SUBUTEX Tablets. Risk Evaluation and Mitigation Strategy (REMS) Program
 Program") SUBOXONE Film, SUBOXONE Tablets, and SUBUTEX Tablets Risk Evaluation and Mitigation Strategy (REMS) Program Office-Based Buprenorphine Therapy for Opioid Dependence: Important Information for Prescribers
SUBOXONE Film, SUBOXONE Tablets, and SUBUTEX Tablets Risk Evaluation and Mitigation Strategy (REMS) Program Office-Based Buprenorphine Therapy for Opioid Dependence: Important Information for Prescribers
Medication Assisted Treatment. Karen Drexler, MD National Mental Health Program Director-Substance Use Disorders Department of Veterans Affairs
 Medication Assisted Treatment Karen Drexler, MD National Mental Health Program Director-Substance Use Disorders Department of Veterans Affairs Disclosures Employed by the Department of Veterans Affairs
Medication Assisted Treatment Karen Drexler, MD National Mental Health Program Director-Substance Use Disorders Department of Veterans Affairs Disclosures Employed by the Department of Veterans Affairs
The Prescription Review Program and College Expectations. Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP Dip. ABAM
 The Prescription Review Program and College Expectations Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP Dip. ABAM April 28, 2017 Disclosure Relationship with commercial interests: None Professional roles: Addictions
The Prescription Review Program and College Expectations Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP Dip. ABAM April 28, 2017 Disclosure Relationship with commercial interests: None Professional roles: Addictions
2. Is this request for a preferred medication? Y N
 Pharmacy Prior Authorization AETA BETTER HEALTH EW JERSE (MEDICAID) Opioids Long-Acting and Short-Acting (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
Pharmacy Prior Authorization AETA BETTER HEALTH EW JERSE (MEDICAID) Opioids Long-Acting and Short-Acting (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
3. Has the patient had a sustained improvement in Pain or Function (e.g. PEG scale with a 30 percent response from baseline)?
?") Pharmacy Prior Authorization AETA BETTER HEALTH KETUCK Opioids Long-Acting and Short-Acting (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
Pharmacy Prior Authorization AETA BETTER HEALTH KETUCK Opioids Long-Acting and Short-Acting (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
Tapering Opioids Best Practices*
 Tapering Opioids Best Practices* Chuck Hofmann, MD, MACP 5 th Annual EOCCO Office Staff and Provider Summit September 28, 2017 Disclosure No Conflicts of Interest to report Learning Objectives Understand
Tapering Opioids Best Practices* Chuck Hofmann, MD, MACP 5 th Annual EOCCO Office Staff and Provider Summit September 28, 2017 Disclosure No Conflicts of Interest to report Learning Objectives Understand
Safe Prescribing of Drugs with Potential for Misuse/Diversion
 College of Physicians and Surgeons of British Columbia Safe Prescribing of Drugs with Potential for Misuse/Diversion Preamble This document establishes both professional standards as well as guidelines
College of Physicians and Surgeons of British Columbia Safe Prescribing of Drugs with Potential for Misuse/Diversion Preamble This document establishes both professional standards as well as guidelines
Talking with your doctor
 SUBOXONE (buprenorphine and naloxone) Sublingual Film (CIII) Talking with your doctor Opioid dependence can be treated. Talking with your healthcare team keeps them aware of your situation so they may
SUBOXONE (buprenorphine and naloxone) Sublingual Film (CIII) Talking with your doctor Opioid dependence can be treated. Talking with your healthcare team keeps them aware of your situation so they may
Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center
 Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center Data from the National Vital Statistics System Mortality The age-adjusted rate of drug overdose deaths in the United States
Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center Data from the National Vital Statistics System Mortality The age-adjusted rate of drug overdose deaths in the United States
Subject: Pain Management (Page 1 of 7)
") Subject: Pain Management (Page 1 of 7) Objectives: Managing pain and restoring function are basic goals in helping a patient with chronic non-cancer pain. Federal and state guidelines require that all
Subject: Pain Management (Page 1 of 7) Objectives: Managing pain and restoring function are basic goals in helping a patient with chronic non-cancer pain. Federal and state guidelines require that all
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
An overview of Medication Assisted Treatment (MAT) and acute pain management on MAT
 and acute pain management on MAT") An overview of Medication Assisted Treatment (MAT) and acute pain management on MAT Goals of Discussion Recognize opioid use disorder (OUD) Discuss the pharmacology of medication assisted treatments (MAT)
An overview of Medication Assisted Treatment (MAT) and acute pain management on MAT Goals of Discussion Recognize opioid use disorder (OUD) Discuss the pharmacology of medication assisted treatments (MAT)
Methadone Maintenance 101
 Methadone Maintenance 101 OTP/DAILY DOSING CLINICS - ANDREW PUTNEY MD Conflicts of Interest - Employed by Acadia HealthCare 1 Why Methadone? At adequate doses methadone decreases opioid withdrawal symptoms
Methadone Maintenance 101 OTP/DAILY DOSING CLINICS - ANDREW PUTNEY MD Conflicts of Interest - Employed by Acadia HealthCare 1 Why Methadone? At adequate doses methadone decreases opioid withdrawal symptoms
Patient and Family Agreement on Opioids
 Patient and Family Agreement on Opioids We care about our patients and are committed to their recovery and wellness. We offer our patients medications and options for various services to keep them from
Patient and Family Agreement on Opioids We care about our patients and are committed to their recovery and wellness. We offer our patients medications and options for various services to keep them from
Who is Behind the Opioid Epidemic?
 Safe and Effective Management of Pain and Addiction CARL CHRISTENSEN, MD PHD MEDICAL DIRECTOR, DAWN FARM CLINICAL ASSOCIATE PROFESSOR, WSU SCHOOL OF MEDICINE WWW.CHRISTENSENRECOVERY.COM Tonight s Talk:
Safe and Effective Management of Pain and Addiction CARL CHRISTENSEN, MD PHD MEDICAL DIRECTOR, DAWN FARM CLINICAL ASSOCIATE PROFESSOR, WSU SCHOOL OF MEDICINE WWW.CHRISTENSENRECOVERY.COM Tonight s Talk:
Beyond Birth: A Comprehensive Recovery Center serving parenting women
 Beyond Birth: A Comprehensive Recovery Center serving parenting women Session Objectives Highlight Plan of Safe Care Introduce the Beyond Birth Comprehensive Recovery Center Describe Levels of Care The
Beyond Birth: A Comprehensive Recovery Center serving parenting women Session Objectives Highlight Plan of Safe Care Introduce the Beyond Birth Comprehensive Recovery Center Describe Levels of Care The
The CARA & Buprenorphine Prescribing for APNs & PAs
 The CARA & Buprenorphine Prescribing for APNs & PAs William J. Lorman, JD, PhD, MSN, PMHNP-BC, CARN-AP FIAAN Assistant Clinical Professor, Drexel University, Philadelphia, PA V. P. & Chief Clinical Officer,
The CARA & Buprenorphine Prescribing for APNs & PAs William J. Lorman, JD, PhD, MSN, PMHNP-BC, CARN-AP FIAAN Assistant Clinical Professor, Drexel University, Philadelphia, PA V. P. & Chief Clinical Officer,
MANAGING PAIN IN PATIENTS WITH SUBSTANCE USE DISORDER Melissa B. Weimer, DO, MCR Chief of Behavioral Health & Addiction Medicine St.
 MANAGING PAIN IN PATIENTS WITH SUBSTANCE USE DISORDER Melissa B. Weimer, DO, MCR Chief of Behavioral Health & Addiction Medicine St. Peter s Health Partners, Albany, NY Assistant Professor of Medicine,
MANAGING PAIN IN PATIENTS WITH SUBSTANCE USE DISORDER Melissa B. Weimer, DO, MCR Chief of Behavioral Health & Addiction Medicine St. Peter s Health Partners, Albany, NY Assistant Professor of Medicine,
ten questions you might have about tapering (and room for your own) an informational booklet for opioid pain treatment
 an informational booklet for opioid pain treatment") ten questions you might have about tapering (and room for your own) an informational booklet for opioid pain treatment This booklet was created to help you learn about tapering. You probably have lots
ten questions you might have about tapering (and room for your own) an informational booklet for opioid pain treatment This booklet was created to help you learn about tapering. You probably have lots
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: Opioid Analgesics Reference Number: HIM.PA.139 Effective Date: 12.01.17 Last Review Date: 11.17 Line of Business: Health Insurance Marketplace Revision Log See Important Reminder at the
Clinical Policy: Opioid Analgesics Reference Number: HIM.PA.139 Effective Date: 12.01.17 Last Review Date: 11.17 Line of Business: Health Insurance Marketplace Revision Log See Important Reminder at the
Medication Assisted Treatment. MAT Opioid dependence/addiction Opioid treatment programs OTP Regulation of OTP Office Based Treatment
 Medication Assisted Treatment MAT Opioid dependence/addiction Opioid treatment programs OTP Regulation of OTP Office Based Treatment Opioid Drugs Opium Morphine Heroin Codeine Oxycodone Roxycodone Oxycontin
Medication Assisted Treatment MAT Opioid dependence/addiction Opioid treatment programs OTP Regulation of OTP Office Based Treatment Opioid Drugs Opium Morphine Heroin Codeine Oxycodone Roxycodone Oxycontin
Disclosures. Objectives 2/5/2018. Women and opioid use disorder: Optimizing care during pregnancy and beyond
 Women and opioid use disorder: Optimizing care during pregnancy and beyond Susanne Astrab Fogger, DNP, PMHNP-BC, CARN-AP, FAANP Ashley L. Hodges, PhD, CRNP, WHNP-BC Disclosures Dr. Fogger has nothing to
Women and opioid use disorder: Optimizing care during pregnancy and beyond Susanne Astrab Fogger, DNP, PMHNP-BC, CARN-AP, FAANP Ashley L. Hodges, PhD, CRNP, WHNP-BC Disclosures Dr. Fogger has nothing to
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: Reference Number: HIM.PA.139 Effective Date: 12.01.17 Last Review Date: 02.18 Line of Business: Health Insurance Marketplace Revision Log See Important Reminder at the end of this policy
Clinical Policy: Reference Number: HIM.PA.139 Effective Date: 12.01.17 Last Review Date: 02.18 Line of Business: Health Insurance Marketplace Revision Log See Important Reminder at the end of this policy
Treatment of Pain in an Emergent Setting
 Updated: October 22, 2018 Prescribing Guidelines for Pennsylvania Treatment of Pain in an Emergent Setting Opioids, including heroin and fentanyl, contribute to thousands of overdose deaths in Pennsylvania
Updated: October 22, 2018 Prescribing Guidelines for Pennsylvania Treatment of Pain in an Emergent Setting Opioids, including heroin and fentanyl, contribute to thousands of overdose deaths in Pennsylvania
MAT in the Corrections Setting
 MEDICATION ASSISTED TREATMENT AND CORRECTIONS Frank Filippelli, DO, PhD September 2017 MAT in the Corrections Setting Who Does This Affect? What is MAT and What is the Evidence of Efficacy? Emphasis on
MEDICATION ASSISTED TREATMENT AND CORRECTIONS Frank Filippelli, DO, PhD September 2017 MAT in the Corrections Setting Who Does This Affect? What is MAT and What is the Evidence of Efficacy? Emphasis on
EXTENDED RELEASE OPIOID DRUGS
 RATIONALE FOR INCLUSION IN PA PROGRAM Background Hydrocodone (Hysingla ER, Vantrela ER, Zohydro ER), hydromorphone (Exalgo), morphine sulfate (Arymo ER, Avinza, Embeda, Kadian, MorphaBond, MS Contin),
RATIONALE FOR INCLUSION IN PA PROGRAM Background Hydrocodone (Hysingla ER, Vantrela ER, Zohydro ER), hydromorphone (Exalgo), morphine sulfate (Arymo ER, Avinza, Embeda, Kadian, MorphaBond, MS Contin),
OPIOID CRISIS: A PERSPECTIVE. Karl J. Haake, MD
 OPIOID CRISIS: A PERSPECTIVE Karl J. Haake, MD LEARNING OBJECTIVES Summarize the history behind the opioid epidemic in America Identify the issues surrounding the the treatment of chronic pain Demonstrate
OPIOID CRISIS: A PERSPECTIVE Karl J. Haake, MD LEARNING OBJECTIVES Summarize the history behind the opioid epidemic in America Identify the issues surrounding the the treatment of chronic pain Demonstrate
Prescription Opioid Addiction
 CSAM-SCAM Fundamentals Prescription Opioid Addiction Presentation provided by Meldon Kahan, MD Family & Community Medicine University of Toronto Conflict of interest statement I received funds from Rickett
CSAM-SCAM Fundamentals Prescription Opioid Addiction Presentation provided by Meldon Kahan, MD Family & Community Medicine University of Toronto Conflict of interest statement I received funds from Rickett
Opioid Prescribing Guidelines for Patients in the Emergency Department
 Opioid Prescribing Guidelines for Patients in the Emergency Department and Immediate Care Centers These guidelines are meant to assist clinicians in treating patients with acute and chronic pain in the
Opioid Prescribing Guidelines for Patients in the Emergency Department and Immediate Care Centers These guidelines are meant to assist clinicians in treating patients with acute and chronic pain in the
Pain, Opioids, & Substance Use Disorders
 Pain, Opioids, & Substance Use Disorders Kenny Jackson, PharmD, CPE Professor & Senior Associate Dean for Academic Affairs College of Pharmacy Larkin University Miami, Florida Editor-in-Chief Journal of
Pain, Opioids, & Substance Use Disorders Kenny Jackson, PharmD, CPE Professor & Senior Associate Dean for Academic Affairs College of Pharmacy Larkin University Miami, Florida Editor-in-Chief Journal of
Our Opioid Epidemic. The Opioid Mortality Crisis Continues 3/2/2017 STEPHEN R. BELL, DO
 Our Opioid Epidemic STEPHEN R. BELL, DO GOVERNOR S TASK FORCE ON PRESCRIPTION DRUG AND OPIOID ABUSE MICHIGAN STATE COMMISSION ON OPIOID AND PRESCRIPTION DRUG ABUSE CHAIR, MOA PRESIDENTIAL TASK FORCE ON
Our Opioid Epidemic STEPHEN R. BELL, DO GOVERNOR S TASK FORCE ON PRESCRIPTION DRUG AND OPIOID ABUSE MICHIGAN STATE COMMISSION ON OPIOID AND PRESCRIPTION DRUG ABUSE CHAIR, MOA PRESIDENTIAL TASK FORCE ON
NBPDP Drug Utilization Review Process Update
 Bulletin # 802 December 1, 2010 NBPDP Drug Utilization Review Process Update The New Brunswick Prescription Drug Program (NBPDP) employs a Drug Utilization Review (DUR) process which identifies, investigates
Bulletin # 802 December 1, 2010 NBPDP Drug Utilization Review Process Update The New Brunswick Prescription Drug Program (NBPDP) employs a Drug Utilization Review (DUR) process which identifies, investigates
Opioid Addiction: An Emerging Epidemic
 Opioid Addiction: An Emerging Epidemic Kevin L. Kraemer, MD, MSc Professor of Medicine and Clinical & Translational Science Chief, Section of Treatment, Research, and Education in Addiction Medicine (STREAM)
Opioid Addiction: An Emerging Epidemic Kevin L. Kraemer, MD, MSc Professor of Medicine and Clinical & Translational Science Chief, Section of Treatment, Research, and Education in Addiction Medicine (STREAM)
Best Practices in Prescribing Benzodiazepines. Michael Carlisle, DO Medical Director University Hospitals Geauga Medical Center
 Best Practices in Prescribing Benzodiazepines Michael Carlisle, DO Medical Director University Hospitals Geauga Medical Center Objectives To review current practice guidelines in benzodiazepine prescribing
Best Practices in Prescribing Benzodiazepines Michael Carlisle, DO Medical Director University Hospitals Geauga Medical Center Objectives To review current practice guidelines in benzodiazepine prescribing
You Asked for It! CE. Rational Opioid Use: Continuous Learning after the CDC Guideline
 You Asked for It! CE AN ONGOING CE PROGRAM of the University of Connecticut School of Pharmacy EDUCATIONAL OBJECTIVES After participating in this activity pharmacists will be able to: Discuss the continuing
You Asked for It! CE AN ONGOING CE PROGRAM of the University of Connecticut School of Pharmacy EDUCATIONAL OBJECTIVES After participating in this activity pharmacists will be able to: Discuss the continuing
Interdisciplinary Management of Opioid Use Disorder in Rural Primary Care Settings
 Interdisciplinary Management of Opioid Use Disorder in Rural Primary Care Settings BRIAN GARVEY, MD, MPH REBECCA CANTONE, MD OREGON HEALTH & SCIENCE UNIVERSITY SCAPPOOSE RURAL HEALTH CENTER Disclosures
Interdisciplinary Management of Opioid Use Disorder in Rural Primary Care Settings BRIAN GARVEY, MD, MPH REBECCA CANTONE, MD OREGON HEALTH & SCIENCE UNIVERSITY SCAPPOOSE RURAL HEALTH CENTER Disclosures
OCCUPATIONAL AND PROFESSIONAL LICENSING MEDICINE AND SURGERY PRACTITIONERS MANAGEMENT OF PAIN AND OTHER CONDITIONS WITH CONTROLLED SUBSTANCES
 TITLE 16 CHAPTER 10 PART 14 OCCUPATIONAL AND PROFESSIONAL LICENSING MEDICINE AND SURGERY PRACTITIONERS MANAGEMENT OF PAIN AND OTHER CONDITIONS WITH CONTROLLED SUBSTANCES 16.10.14.1 ISSUING AGENCY: New
TITLE 16 CHAPTER 10 PART 14 OCCUPATIONAL AND PROFESSIONAL LICENSING MEDICINE AND SURGERY PRACTITIONERS MANAGEMENT OF PAIN AND OTHER CONDITIONS WITH CONTROLLED SUBSTANCES 16.10.14.1 ISSUING AGENCY: New
PROPOSED DUR CRITERIA FOR MANAGING OPIOID USE AND MINIMIZING RISK OF OVERDOSE
 BACKGROUND PROPOSED DUR CRITERIA FOR MANAGING OPIOID USE AND MINIMIZING RISK OF OVERDOSE In March, 2016, the CDC released the final version of their Guidelines for Prescribing Opioids for Chronic Pain.
BACKGROUND PROPOSED DUR CRITERIA FOR MANAGING OPIOID USE AND MINIMIZING RISK OF OVERDOSE In March, 2016, the CDC released the final version of their Guidelines for Prescribing Opioids for Chronic Pain.
Recognizing Narcotic Abuse and Addiction and Helping Those With It
 Recognizing Narcotic Abuse and Addiction and Helping Those With It Michael McNett, MD Medical Director for Chronic Pain Member, WI Med Society Opioid Subcommittee Ancient History 1995: OxyContin approved
Recognizing Narcotic Abuse and Addiction and Helping Those With It Michael McNett, MD Medical Director for Chronic Pain Member, WI Med Society Opioid Subcommittee Ancient History 1995: OxyContin approved
Addressing the Opioid Crisis Workgroup: Treatment and Overdose Prevention
 The Accountable Community for Health of King County Addressing the Opioid Crisis Workgroup: Treatment and Overdose Prevention May 7, 2018 1 Opiate Treatment & Overdose Prevention Project Goal Immediate:
The Accountable Community for Health of King County Addressing the Opioid Crisis Workgroup: Treatment and Overdose Prevention May 7, 2018 1 Opiate Treatment & Overdose Prevention Project Goal Immediate:
The Population is Abusing Drugs, but are Drugs Abusing Insurance?
 Image licensed from Shutterstock The Population is Abusing Drugs, but are Drugs Abusing Insurance? 01/30/2018 Gina C. Guzman, MD, DBIM, FALU, FLMI, VP and Chief Medical Director Tim Morant, FSA, MAAA,
Image licensed from Shutterstock The Population is Abusing Drugs, but are Drugs Abusing Insurance? 01/30/2018 Gina C. Guzman, MD, DBIM, FALU, FLMI, VP and Chief Medical Director Tim Morant, FSA, MAAA,
Long-Acting Opioid. Policy Number: Last Review: 12/2017 Origination: 09/2013 Next Review: 09/2018
 Long-Acting Opioid Policy Number: 5.02.519 Last Review: 12/2017 Origination: 09/2013 Next Review: 09/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for long-acting
Long-Acting Opioid Policy Number: 5.02.519 Last Review: 12/2017 Origination: 09/2013 Next Review: 09/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for long-acting
Opioid Prescribing Tips & Tricks CANDY STOCKTON, MD MAY 2018
 Opioid Prescribing Tips & Tricks CANDY STOCKTON, MD MAY 2018 Disclosures None Educational Objectives Understand CA state medical board guidelines for prescribing opioids for chronic pain Understand the
Opioid Prescribing Tips & Tricks CANDY STOCKTON, MD MAY 2018 Disclosures None Educational Objectives Understand CA state medical board guidelines for prescribing opioids for chronic pain Understand the
INFORMED CONSENT FOR OPIOID TREATMENT FOR NON-CANCER/CANCER PAIN Texas Pain and Regenerative Medicine
 INFORMED CONSENT FOR OPIOID TREATMENT FOR NON-CANCER/CANCER PAIN Texas Pain and Regenerative Medicine The purpose of this agreement is to give you information about the medications you will be taking for
INFORMED CONSENT FOR OPIOID TREATMENT FOR NON-CANCER/CANCER PAIN Texas Pain and Regenerative Medicine The purpose of this agreement is to give you information about the medications you will be taking for
THA Medication Safety Summit. Wesley Geminn, PharmD, BCPP
 THA Medication Safety Summit Wesley Geminn, PharmD, BCPP Current Trends: Overdose Deaths in 2017 72,000 Or 197 per day 8 per hour National Opioid Overdose Statistics https://www.drugabuse.gov/related-topics/trendsstatistics/overdose-death-rates
THA Medication Safety Summit Wesley Geminn, PharmD, BCPP Current Trends: Overdose Deaths in 2017 72,000 Or 197 per day 8 per hour National Opioid Overdose Statistics https://www.drugabuse.gov/related-topics/trendsstatistics/overdose-death-rates
Didactic Series. Opioid Dependence and HIV Care. Theo Katsivas, MD MAS, AAHIVS Associate Clinical Professor Owen Clinic, UCSD 10/25/2018
 Didactic Series Opioid Dependence and HIV Care Theo Katsivas, MD MAS, AAHIVS Associate Clinical Professor Owen Clinic, UCSD 10/25/2018 Physicians: This activity has been planned and implemented in accordance
Didactic Series Opioid Dependence and HIV Care Theo Katsivas, MD MAS, AAHIVS Associate Clinical Professor Owen Clinic, UCSD 10/25/2018 Physicians: This activity has been planned and implemented in accordance
Buprenorphine as a Treatment Option for Opioid Use Disorder
 Buprenorphine as a Treatment Option for Opioid Use Disorder Joji Suzuki, MD Assistant Professor of Psychiatry Harvard Medical School Director, Division of Addiction Psychiatry Brigham and Women s Hospital
Buprenorphine as a Treatment Option for Opioid Use Disorder Joji Suzuki, MD Assistant Professor of Psychiatry Harvard Medical School Director, Division of Addiction Psychiatry Brigham and Women s Hospital
Risk Reduction Strategies in Pain Management
 Risk Reduction Strategies in Pain Management Melissa J. Durham, PharmD, MACM, BCACP, DAAPM Assistant Professor of Clinical Pharmacy USC School of Pharmacy Clinical Pharmacist, The USC Pain Center Learning
Risk Reduction Strategies in Pain Management Melissa J. Durham, PharmD, MACM, BCACP, DAAPM Assistant Professor of Clinical Pharmacy USC School of Pharmacy Clinical Pharmacist, The USC Pain Center Learning
Medication Assisted Treatment. Nicole Gastala, MD
 Medication Assisted Treatment Nicole Gastala, MD Objectives Training Goals: To enhance the understanding of the participants in use of medication assisted therapy To increase the knowledge of participants
Medication Assisted Treatment Nicole Gastala, MD Objectives Training Goals: To enhance the understanding of the participants in use of medication assisted therapy To increase the knowledge of participants
The Role of the PDMP: Foundational Knowledge and Best Practices
 The Role of the PDMP: Foundational Knowledge and Best Practices Brent I. Fox, PharmD, PhD Health Outcomes Research and Policy Harrison School of Pharmacy Auburn University DISCLOSURE I, Brent Fox, have
The Role of the PDMP: Foundational Knowledge and Best Practices Brent I. Fox, PharmD, PhD Health Outcomes Research and Policy Harrison School of Pharmacy Auburn University DISCLOSURE I, Brent Fox, have
Building capacity for a CHC response to Ontario's Opioid Crisis
 Building capacity for a CHC response to Ontario's Opioid Crisis Rob Boyd Oasis Program Director Luc Cormier, RN, MScN Community Health Nurse Sandy Hill Community Health Centre #AOHC2016 @rboyd6 @SandyHillCHC
Building capacity for a CHC response to Ontario's Opioid Crisis Rob Boyd Oasis Program Director Luc Cormier, RN, MScN Community Health Nurse Sandy Hill Community Health Centre #AOHC2016 @rboyd6 @SandyHillCHC
Clinical Guidelines for the Pharmacologic Treatment of Opioid Use Disorder
 Clinical Guidelines for the Pharmacologic Treatment of Community Behavioral Health (CBH) is committed to working with our provider partners to continuously improve the quality of behavioral healthcare
Clinical Guidelines for the Pharmacologic Treatment of Community Behavioral Health (CBH) is committed to working with our provider partners to continuously improve the quality of behavioral healthcare
Product Labeling to Communicate Benefits and Risks of Treatment for Opioid Use Disorder in Pregnant Women. Hendrée E. Jones, PhD
 1 The National Academies of Sciences, Engineering and Medicine Regulatory Strategies of address prescription opioidrelated harms 4 th of November, 2016 Washington DC Product Labeling to Communicate Benefits
1 The National Academies of Sciences, Engineering and Medicine Regulatory Strategies of address prescription opioidrelated harms 4 th of November, 2016 Washington DC Product Labeling to Communicate Benefits
OPIOID IR COMBO DRUGS. Oxycodone-acetaminophen, Oxycodone-aspirin, Oxycodone-ibuprofen, Tramadolacetaminophen
 RATIONALE FOR INCLUSION IN PA PROGRAM Background Apadaz (benzhydrocodone-acetaminophen), codeine-acetaminophen, dihydrocodeine-caffeineacetaminophen, hydrocodone-acetaminophen, hydrocodone-ibuprofen, oxycodoneacetaminophen,
RATIONALE FOR INCLUSION IN PA PROGRAM Background Apadaz (benzhydrocodone-acetaminophen), codeine-acetaminophen, dihydrocodeine-caffeineacetaminophen, hydrocodone-acetaminophen, hydrocodone-ibuprofen, oxycodoneacetaminophen,
Appendix F Federation of State Medical Boards
 Appendix F Federation of State Medical Boards Model Policy Guidelines for Opioid Addiction Treatment in the Medical Office SECTION I: PREAMBLE The (name of board) recognizes that the prevalence of addiction
Appendix F Federation of State Medical Boards Model Policy Guidelines for Opioid Addiction Treatment in the Medical Office SECTION I: PREAMBLE The (name of board) recognizes that the prevalence of addiction
Physicians Health Status. Objectives. Clinical Case. Physician Suicide. Clinical Case- Continued
 Objectives Review substance use by physicians in the US Present the approach used to help impaired physicians in Virginia Review healthy approaches to physicians stress Physicians Health Status Overall
Objectives Review substance use by physicians in the US Present the approach used to help impaired physicians in Virginia Review healthy approaches to physicians stress Physicians Health Status Overall
Prescription Monitoring Program (PMP)
") 06/15/2018 FACT SHEET Implementation of Enacted Prescribing Limits and Requirements and Relevant Opioid Prescribing Laws and Rules Background: The 2016 law (Chapter 488) makes five major changes to opioid
06/15/2018 FACT SHEET Implementation of Enacted Prescribing Limits and Requirements and Relevant Opioid Prescribing Laws and Rules Background: The 2016 law (Chapter 488) makes five major changes to opioid
Wasted AN INTRODUCTION TO SUBSTANCE ABUSE
 Wasted AN INTRODUCTION TO SUBSTANCE ABUSE Dr. Brian L. Bethel Child and Family Therapist Independent Trainer and Consultant LPCC-S, LCDC III, RPT-S www.brianlbethel.com INTERPLAY COUNSELING & CONSULTING
Wasted AN INTRODUCTION TO SUBSTANCE ABUSE Dr. Brian L. Bethel Child and Family Therapist Independent Trainer and Consultant LPCC-S, LCDC III, RPT-S www.brianlbethel.com INTERPLAY COUNSELING & CONSULTING
Pharmacist perspective on the CDC guideline for prescribing opioids for chronic pain
 A ND an ongoing ce Program of THE university of connecticut school of pharmacy AND DRUG TOPICS 2 CPe CRedits EARN CE CREDIT FOR THIS ACTIVITY AT WWW.DrugTopics.com/cpE educational objectives goal: To educate
A ND an ongoing ce Program of THE university of connecticut school of pharmacy AND DRUG TOPICS 2 CPe CRedits EARN CE CREDIT FOR THIS ACTIVITY AT WWW.DrugTopics.com/cpE educational objectives goal: To educate
Prescription Opioids
 What are prescription opioids? Prescription Opioids Opioids are a class of drugs naturally found in the opium poppy plant. Some prescription opioids are made from the plant directly, and others are made
What are prescription opioids? Prescription Opioids Opioids are a class of drugs naturally found in the opium poppy plant. Some prescription opioids are made from the plant directly, and others are made
Clinical Policy: Opioid Analgesics Reference Number: CP.PMN.97 Effective Date: Last Review Date: 02.19
 Clinical Policy: Reference Number: CP.PMN.97 Effective Date: 02.11 Last Review Date: 02.19 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important regulatory
Clinical Policy: Reference Number: CP.PMN.97 Effective Date: 02.11 Last Review Date: 02.19 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important regulatory
White Paper on. Prescription Drug Abuse
 White Paper on Prescription Drug Abuse October 22, 2014 Table of Contents: I. Introduction II. Scope of the Problem III. Most Common Drugs Involved in Overdoses IV. Efforts in Tennessee V. Prescription
White Paper on Prescription Drug Abuse October 22, 2014 Table of Contents: I. Introduction II. Scope of the Problem III. Most Common Drugs Involved in Overdoses IV. Efforts in Tennessee V. Prescription