Thad Wilkins, M.D., Department of Family Medicine, Georgia Health Sciences University
|
|
|
- Osborn Townsend
- 5 years ago
- Views:
Transcription
1 Diagnosis and management of upper gastrointestinal bleeding Thad Wilkins, M.D., Department of Family Medicine, Georgia Health Sciences University Naiman Khan, M.D., Department of Family Medicine, Georgia Health Sciences University Akash Nabh, M.D., Department of Medicine, Georgia Health Sciences University Robert R. Schade, M.D., Department of Medicine, Georgia Health Sciences University Author Information Thad Wilkins, M.D. Associate Professor Department of Family Medicine th Street, HB-4032 Georgia s Health Sciences University Augusta, GA Contact information Phone: twilkins@mcg.edu Abstract word count: 241 ( ) Manuscript word count: 1592 ( ) Number of references: 33 (10-35) Number of tables: 5 Number of figures: 6 1
2 Abbreviations: Upper gastrointestinal bleeding (UGIB) Nonsteroidal anti-inflammatory drug (NSAID) Odds ratio (OR) Peptic ulcer disease (PUD) Peptic ulcer bleeding (PUB) Helicobacter pylori (H. Pylori) 2
3 Abstract Upper gastrointestinal bleeding (UGIB) causes significant morbidity and mortality in the United States. Bleeding due to peptic ulcer disease is the most common cause of UGIB and is associated with NSAID use and the relatively high prevalence of H. Pylori infection. Patients with portal hypertension and cirrhosis may hemorrhage from varices. Rapid assessment and resuscitation should precede diagnostic evaluation. Two large caliber peripheral catheters or a central venous line should be inserted for intravenous access and crystalloid intravenous fluids initiated. Initial laboratory tests should include: hemoglobin, hematocrit, platelet count, prothrombin time, partial thromboplastin time, INR, creatinine, BUN, type and cross match. Blood transfusion should be administered to patients with a hemoglobin level less than 7 g/dl. Patients can be risk stratified based on clinical assessment and endoscopic findings. Early endoscopy (within 24 hours of presentation) is recommended in most patients, allowing rapid diagnosis and application of endoscopic therapies including injection with epinephrine, thermal therapy, application of clips, and banding. Endoscopic therapy results in reduced morbidity, decreased hospital stay, decreased risk of recurrent bleeding, and the need for surgery. Although administration of proton pump inhibitors does not decrease mortality, risk for rebleeding, or surgery, they downstage the severity of the bleeding lesion and reduce the need for endoscopic therapy. Despite successful endoscopic therapy, rebleeding can occur in 10-20% of patients and a second attempt at endoscopic therapy is recommended. Arteriography or surgery may be needed if there is persistent and severe bleeding. 3
4 <LH>Background In the US in 2004, non-variceal upper gastrointestinal bleeding (UGIB) resulted in 400,000 hospital admissions per year, costing more than $2 billion annually (1). UGIB is associated with increasing nonsteroidal anti-inflammatory drug (NSAID) usage and the high prevalence (64%) of Helicobacter pylori (H. Pylori) infections in patients with peptic ulcer bleeding (PUB) (2). UGIB is twice as common in men as in women and increases in prevalence with age (3). Despite advances in therapy, the in-hospital mortality from UGIB remains high (13%) and rebleeding is common (15%) (4, 5). This review article focuses on acute nonvariceal UGIB in adults although we briefly review management of variceal bleeding. <LH> Pathogenesis UGIB includes hemorrhage originating from the esophagus to the ligament of Treitz. PUB is the main cause of UGIB (61%), and in the US, duodenal ulcers are more common than gastric ulcers (6). Hospitalizations for PUB decreased by 30% from 1996 to 2006, and in 2006 the inpatient mortality from PUB was 2.7% (6). Patients with gastric ulcers (55.1%) are hospitalized more commonly than patients with duodenal ulcers (38.5%), but the mortality rate for duodenal ulcers (3.7%) is higher than that of gastric ulcers (2.1%) (6). Duodenal ulcers are more likely to erode into large vessels causing more severe bleeding. Table 1 lists common causes of UGIB. In a meta-analysis of 16 studies of 1633 participants taking NSAIDs, both H. Pylori (odds ratio (OR) (1.7)) and NSAID use (OR 4.8) increase the risk of UGIB, and this risk increases when both factors are present (OR 6.1) (7). H. Pylori adheres to the gastric epithelium and renders the underlying mucosa more vulnerable to damage by producing enzymes and toxins (8), and affecting gastrin levels and acid output. The risk of UGIB varies based on the type of NSAID (9), (Table 2). <LH> Diagnosis 4
5 Rapid assessment and resuscitation should precede the diagnostic evaluation in unstable patients with severe bleeding. Some patients may require intubation to decrease risk for aspiration. All patients with active bleeding resulting in hemodynamic instability should be admitted to an intensive care unit for resuscitation and close observation. Two large caliber peripheral catheters or a central venous line should be inserted for intravenous access and crystalloid fluids initiated. Other measures include monitoring urine output, obtaining electrocardiogram, and continuous telemetry monitoring. The physician should consider transferring a patient with significant UGIB to a tertiary medical center based on local expertise and the availability of facilities. Patients admitted primarily for UGIB have a lower mortality compared to patients admitted for other reasons who have a subsequent UGIB during their hospitalization (4, 10). See Figure 1 for an algorithmic approach to UGIB. <SH> History and physical examination Important historical information includes: presence of abdominal pain, vomiting, dysphagia, black tarry stools, bright red blood per rectum, hematemesis, and chest pain. Medication use should be elicited, especially prior use of clopidogrel, warfarin, NSAIDs, aspirin, selective serotonin reuptake inhibitors (SSRIs), or corticosteroids since treatment with these medications increase the risk for UGIB (11-13). SSRIs inhibit platelet aggregation and are associated with UGIB; the concurrent use of NSAIDs or aspirin with SSRIs further increases the risk of UGIB (13). The physician should ascertain prior history of peptic ulcer disease (PUD), prior episode of UGIB, history of cirrhosis, and alcohol or illicit drug use. The physician should also inquire about other comorbid conditions that may affect outcomes such as prior abdominal surgery, diabetes mellitus, coronary artery disease, chronic renal or liver disease, or chronic obstructive pulmonary disease. 5
6 Blood pressure and pulse rate may be normal. If bleeding is severe, patients may be hypotensive or tachycardic or may exhibit orthostatic hypotension. Physical examination should assess for tenderness, guarding, rebound, prior surgical scars, or sequela of chronic liver disease. Rectal examination should be performed and stool color assessed, e.g. for melena or bright red blood. Stool specimen should be collected for occult blood testing. Initial laboratory tests should include: hemoglobin, hematocrit, platelet count, prothrombin time, partial thromboplastin time, INR, BUN, creatinine, and type and crossmatch. Patients with active bleeding and a coagulopathy or thrombocytopenia should be considered for transfusion with fresh frozen plasma and platelets, respectively (4). Blood transfusions should be administered to patients with hemoglobin of less than 7 g/dl and hemoglobin maintained at 9 g/dl (4, 14). <SH> Nasogastric tube lavage Evaluation should focus on determining whether the bleed is from an upper or a lower gastrointestinal source. Nasogastric lavage has a low sensitivity and poor negative likelihood ratio for UGIB in patients with melena or hematochezia (15, 16). However, a positive nasogastric tube lavage that yields blood or coffee-ground like material confirms the diagnosis of UGIB and predicts that bleeding is caused by a high-risk lesion (15, 16). <SH>Risk stratification Risk stratification is based on clinical assessment and endoscopic findings. Clinical assessment includes age, presence of shock, systolic blood pressure, heart rate, and comorbid conditions. Mortality increases with increasing co-morbid conditions and age (17). Endoscopic findings include the cause of the bleeding and stigmata of recent hemorrhage, see Table 3. The 6
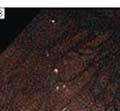
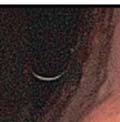
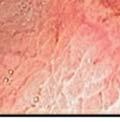
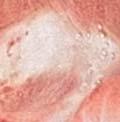
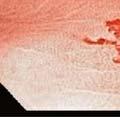
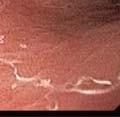
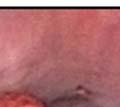
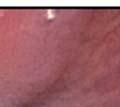
7 Rockall risk scoring system uses a combination of clinical and endoscopic findings to predict the risk of rebleeding and mortality, (table 4) (18). <LH> Treatment Early upper endoscopy (within 24 hours of presentation) is recommended in most patients with UGIB as it confirms the diagnosis and allows for targeted endoscopic treatment, resulting in reduced morbidity, hospital stay, risk of recurrent bleeding, and need for surgery (4). Figures 2-6 show examples of endoscopic findings. Although prokinetic agents to evacuate the stomach are not recommended (19), gastric lavage should be considered. One of the benefits of gastric lavage is to clear the stomach of blood, increasing the success of endoscopic localization of the source of bleeding. Endoscopic therapies include injection with epinephrine, thermal application, application of clips, and banding. A Cochrane review of 18 studies of PUB including 1868 participants found that adding an additional endoscopic treatment after epinephrine injection significantly reduced rebleeding rates from 18.5% to 10% and reduced mortality from 4.7% to 2.5% (20). Low risk patients, e.g. clean ulcer base with PUB can be safely discharged on the same day as endoscopy (4). Most patients with high-risk PUB stigmata, e.g. active arterial bleeding, visible vessel, or adherent clot should be hospitalized for at least 72 hours with intravenous PPI therapy after endoscopic hemostasis since most rebleeding occurs in this time frame (4). Although a systematic review of 6 randomized controlled trials of 2223 participants found no statistically significant differences in mortality, rebleeding, or surgery between patients receiving proton pump inhibitors (PPIs) and control treatment (placebo or H 2 receptor antagonists) (21). Patients treated with PPI therapy compared to control treatment had significantly reduced stigmata of recent hemorrhage, e.g. active arterial bleeding, visible vessel, or adherent clot (37.2% compared to 46.5%, OR 0.67) and reduced need for endoscopic 7
8 therapy (8.6% compared to 11.7%, OR 0.68) (21). In a randomized controlled trial of 767 patients with PUB randomly assigned to intravenous PPI therapy or placebo, fewer patients receiving intravenous PPI therapy (5.9%) had recurrent bleeding within 72 hours than those receiving placebo (10.3%) (P= 0.026) (22). The difference in bleeding recurrence remains significant at 7 days and 30 days (P= 0.010) (22). All patients admitted with significant UGIB should be started on intravenous PPI therapy until confirmation of the cause of bleeding at endoscopy (4). Use of H 2 receptor antagonists is not recommended for patients with UGIB. <SH>Recurrent hemorrhage Rebleeding after successful endoscopic therapy occurs in 10-20% of patients. The risk of rebleeding and mortality can be calculated with a clinical decision rule (18, 23). If rebleeding occurs, a second attempt at endoscopic therapy is recommended. In patients determined to be at high-risk for rebleeding, scheduled repeat endoscopy may reduce the rebleeding rate and be cost effective (4). However, a routine second-look endoscopy the next day is not recommended (4). Arteriography with embolization usually precedes surgical therapy since both are equally effective in treating patients with persistent bleeding (24). Surgical therapy is usually recommended if therapeutic methods including endoscopy and arteriography with embolization have failed to control the bleeding or if interventional radiology expertise is not available after failed endoscopic attempt. Surgical therapy is also indicated in patients with recurrent hemorrhage or hemodynamic instability despite fluid resuscitation and blood transfusion. In patients in whom no cause of UGIB was identified, small bowel evaluation with enteroscopy or video capsule endoscopy should be considered to evaluate for a small bowel source of the bleeding. Table 5 lists advantages and disadvantages of common tests used to diagnose UGIB. <LH>Prevention 8
9 H. Pylori and NSAIDs are the major causes of PUB in the US and preventive strategies should focus on these etiologies. Smoking and alcohol use impairs ulcer healing and patients should be counseled about smoking cessation and moderation of alcohol use. A systematic review of 41 randomized controlled trials of patients on NSAIDs found that double dose H 2 receptor antagonist (RR 0.44) and PPIs (RR =0.40) significantly reduced the risk of PUB (25). In patients with a history of PUB, aspirin, clopidogrel, and NSAIDs should be avoided if possible. In patients on aspirin who develop PUB, aspirin therapy with PPI therapy should be restarted as soon as the risk for cardiovascular complication is thought to outweigh the risk of rebleeding (1). A Cochrane review of 7 studies of 578 patients concluded that eradication of H. Pylori infection in patients with PUB reduces the long-term rate of rebleeding (2.9%) compared with patients in the non-eradication group (20%) (NNT = 7) (26). In patients with PUB associated with H. Pylori eradication is essential and should be confirmed by urea breath test, stool antigen test, or the biopsy urease test. A repeat upper endoscopy in 8-12 weeks is recommended for patients with PUB secondary to gastric ulcers to assess for healing and to exclude malignancy and for patients with severe esophagitis to exclude Barrett s esophagus. <LH> Variceal hemorrhage Patients with cirrhosis should be screened with upper endoscopy to rule out varices (27). If patients have no varices on the initial endoscopy, it should be repeated in 3 years (27). Consider starting nonselective β-blockers, e.g. propranolol or nadolol in patients with varices to reduce portal pressure and decrease the risk of future hemorrhage (27). In patients with a history of varices who present with acute UGIB, upper endoscopy should be performed within 12 hours to confirm the diagnosis and to treat variceal hemorrhage (27). Endoscopic variceal ligation is the preferred endoscopic treatment for esophageal variceal hemorrhage and is superior to sclerotherapy (28). A review of 12 trials of 1241 patients found that broad-spectrum antibiotics, e.g. ceftriaxone, norfloxacin, ciprofloxacin in patients with variceal hemorrhage 9
10 reduced overall mortality (RR 0.79) and risk of rebleeding (RR 0.53) (29). A Cochrane review of 21 trials of 2588 patients found no difference in mortality or risk of rebleeding with somatostatin and its derivatives, e.g. octreotide in active variceal hemorrhage (30). Octreotide is often administered to patients with variceal hemorrhage however its use is controversial. If octreotide is used it should be initiated promptly in patients with variceal bleeding and continued for 3-5 days in conjunction with endoscopic therapy since this improves the immediate and 5 day rebleeding rates (27). Salvage treatment with transjugular intrahepatic portosystemic stentshunt procedure or surgery should be considered especially for patients with gastric varices when medical and endoscopic treatment fail to control bleeding (31). The Model for End-Stage Liver Disease score should be calculated for prognosis and as a guide to decision-making regarding liver transplant (32). 10
11 Key recommendations for practice. Key Clinical Recommendation Evidence Rating References Immediately evaluate and C (4) initiate appropriate resuscitation Transfuse patients with C (4, 14) hemoglobin level < 7.0 mg/l Perform upper C (4) endoscopy for the evaluation of upper gastrointestinal bleeding within 24 hours of presentation Low-risk patients with C (4) acute peptic ulcer bleeding based on clinical and endoscopic criteria may be discharged promptly after 11
12 endoscopy High-risk patients based C (4) on clinical and endoscopic criteria should remain hospitalized for at least 72 hours Start intravenous proton B (33) pump inhibitors at presentation until confirmation of a cause of bleeding at endoscopy Routine second-look C (34) endoscopy is not recommended 12
13 Table 1. Causes of upper gastrointestinal bleeding. Diagnosis Distinguishing features Frequency (%) Peptic ulcer disease Esophagogastric varices Gastritis and duodenitis Mallory-Weiss tears Gastrointestinal malignancy Arteriovenous malformations Esophagitis or esophageal ulcer Dieulafoy s lesion Other Prior history of aspirin or NSAID use associated with abdominal pain, food reduces pain, nocturnal symptoms, past history of peptic ulcer disease or Helicobacter pylori History of cirrhosis and portal hypertension Same as peptic ulcer disease above History of repeated retching or vomiting History of weight loss, smoking, or alcohol consumption, more common in Asians Painless bleeding in older patients (>70 years old), history of iron deficiency anemia Heartburn, indigestion, or dysphagia More common in men, painless bleeding Variable No identifiable source 8 Adapted from (3)
14 Table 2. The relative risk of upper gastrointestinal bleeding associated with use of nonsteroidal anti-inflammatory drugs (NSAIDs) NSAID Relative risk of upper gastrointestinal bleeding Ibuprofen 2.7 Diclofenac 4.0 Meloxicam 4.0 Naproxen 5.2 Indomethacin 5.3 Ketoprofen 5.7 Piroxicam 9.3 Ketorolac 14.0 Source: (9) 14
15 Table 3. The prevalence and risk of rebleeding based on the endoscopic stigmata of hemorrhage in peptic ulcer bleeding Endoscopic Prevalence (%) Rebleeding rate without Rebleeding rate with appearance endoscopic treatment (%) successful endoscopic treatment (%) Active arterial bleeding Visible vessel Adherent clot Oozing without stigmata Data not available Flat spot 10 7 Data not available Clean ulcer base 32 3 Data not available Source: (17, 35) 15
16 Table 4. Rockall risk scoring system for risk assessment after acute upper gastrointestinal bleeding Variable * Age Less than 60 years old years old Greater than 80 years old Shock Absent Tachycardia Hypotension Systolic blood >100 >100 <100 pressure (mm Hg) Heart rate <100 >100 >100 Comorbidities None None Heart failure, coronary artery disease Endoscopic diagnosis Stigmata of recent hemorrhage Mallory-Weiss tear or no lesion identified, and no stigmata of recent hemorrhage None or dark spot only All other diagnoses Malignancy of upper gastrointestinal tract Blood in upper gastrointestinal tract, adherent clot, visible or spurting vessel Renal failure, liver failure, disseminated malignancy * Score the patient on each variable and calculate the total score. The total score is used below to calculate risk of rebleeding and mortality. Risk of rebleeding and mortality based on Rockall risk score Score >8 Rebleeding (%) Mortality (%) Source: (18) 16
17 Table 5. Advantages and disadvantages of various tests to assess for upper gastrointestinal bleeding. Test Advantages Disadvantages Esophagogastroduodenoscopy with endoscopic therapy Confirms diagnosis and initiates endoscopic therapy, decreases risk for rebleeding, transfusion requirements, and length of hospital stay Costs, risk of sedation, risk of aspiration, invasive test, risk of perforation Arteriography Small bowel enteroscopy Targeted therapy for ongoing hemorrhage, may prevent need for surgery Allows for precise identification of lesion in small bowel and application of endoscopic therapy, localization of lesion with tattooing if surgery is planned Invasive, expensive, requires special expertise, exposure to radiation, risk of contrast-induced nephropathy, risk of bleeding from arterial puncture site Operator-dependent, requires special equipment and expertise, may not visualize all of small bowel, expensive, risk of sedation, risk of perforation, expensive 17
18 Capsule endoscopy No sedation required, noninvasive test, allows visualization of the entire small bowel Capsule retention may occur, can miss lesions because images are not continuous, cannot perform therapeutic maneuvers 18
19 Figure 1. An algorithm for management of acute upper gastrointestinal hemorrhage. 19





















20 Figure 2. Gastric ulcer with protuberant vessel treated with heater probe. Followup endoscopy to assesss healing at 4 weeks. A. Gastric ulcer with protuberant vessel B. Gastric ulcer following treatment with heater probe C, Healing gastric ulcer (after 4 weeks) 20












21 Figure 3. Duodenal ulcer with adherent clot 21















22 Figure 4. Dieulafoy s lesion causing upper GI bleeding A. Dieulafoy s lesion causing upper GI bleeding B. Dieulafoy s lesion after application of clip 22









23 Figure 5. Mallory-Weis tear A. Mallory-Weiss tear 23









24 Figure 6. Esophageal varix causing upper GI bleeding after endoscopic ligation 24
25 REFERENCES 1. Kanwal F, Barkun A, Gralnek IM, Asch SM, Kuipers EJ, Bardou M, et al. Measuring quality of care in patients with nonvariceal upper gastrointestinal hemorrhage: development of an explicit quality indicator set. Am J Gastroenterol Aug;105(8): Sanchez Delgado J, Gene E, Suarez D, Garcia Iglesias P, Brullet E, Gallach M, et al. Has H. pylori Prevalence in Bleeding Peptic Ulcer Been Underestimated[quest] A Meta Regression. Am J Gastroenterol Longstreth GF. Epidemiology of hospitalization for acute upper gastrointestinal hemorrhage: a population based study. Am J Gastroenterol Feb;90(2): Barkun AN, Bardou M, Kuipers EJ, Sung J, Hunt RH, Martel M, et al. International consensus recommendations on the management of patients with nonvariceal upper gastrointestinal bleeding. Ann Intern Med Jan 19;152(2): van Leerdam ME, Vreeburg EM, Rauws EA, Geraedts AA, Tijssen JG, Reitsma JB, et al. Acute upper GI bleeding: did anything change? Time trend analysis of incidence and outcome of acute upper GI bleeding between 1993/1994 and Am J Gastroenterol Jul;98(7): Wang YR, Richter JE, Dempsey DT. Trends and outcomes of hospitalizations for peptic ulcer disease in the United States, 1993 to Ann Surg Jan;251(1): Huang JQ, Sridhar S, Hunt RH. Role of Helicobacter pylori infection and non steroidal antiinflammatory drugs in peptic ulcer disease: a meta analysis. Lancet Jan 5;359(9300): Pajares JM. H. pylori infection: its role in chronic gastritis, carcinoma and peptic ulcer. Hepatogastroenterology Nov Dec;42(6): Masso Gonzalez EL, Patrignani P, Tacconelli S, Garcia Rodriguez LA. Variability among nonsteroidal antiinflammatory drugs in risk of upper gastrointestinal bleeding. Arthritis Rheum Jun;62(6): Silverstein FE, Gilbert DA, Tedesco FJ, Buenger NK, Persing J. The national ASGE survey on upper gastrointestinal bleeding. II. Clinical prognostic factors. Gastrointest Endosc May;27(2): Delaney JA, Opatrny L, Brophy JM, Suissa S. Drug drug interactions between antithrombotic medications and the risk of gastrointestinal bleeding. Cmaj Aug 14;177(4): Hernandez Diaz S, Rodriguez LA. Steroids and risk of upper gastrointestinal complications. Am J Epidemiol Jun 1;153(11): Yuan Y, Tsoi K, Hunt RH. Selective serotonin reuptake inhibitors and risk of upper GI bleeding: confusion or confounding? Am J Med Sep;119(9): Hebert PC, Wells G, Blajchman MA, Marshall J, Martin C, Pagliarello G, et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. Transfusion Requirements in Critical Care Investigators, Canadian Critical Care Trials Group. N Engl J Med Feb 11;340(6): Palamidessi N, Sinert R, Falzon L, Zehtabchi S. Nasogastric aspiration and lavage in emergency department patients with hematochezia or melena without hematemesis. Acad Emerg Med Feb;17(2): Aljebreen AM, Fallone CA, Barkun AN. Nasogastric aspirate predicts high risk endoscopic lesions in patients with acute upper GI bleeding. Gastrointest Endosc Feb;59(2): Zimmerman J, Siguencia J, Tsvang E, Beeri R, Arnon R. Predictors of mortality in patients admitted to hospital for acute upper gastrointestinal hemorrhage. Scand J Gastroenterol Apr;30(4): Rockall TA, Logan RF, Devlin HB, Northfield TC. Risk assessment after acute upper gastrointestinal haemorrhage. Gut Mar;38(3):
26 19. Barkun AN, Bardou M, Martel M, Gralnek IM, Sung JJ. Prokinetics in acute upper GI bleeding: a meta analysis. Gastrointest Endosc Dec;72(6): Vergara M, Calvet X, Gisbert JP. Epinephrine injection versus epinephrine injection and a second endoscopic method in high risk bleeding ulcers. Cochrane Database Syst Rev. 2007(2):CD Sreedharan A, Martin J, Leontiadis GI, Dorward S, Howden CW, Forman D, et al. Proton pump inhibitor treatment initiated prior to endoscopic diagnosis in upper gastrointestinal bleeding. Cochrane Database Syst Rev. 2010(7):CD Sung JJ, Barkun A, Kuipers EJ, Mossner J, Jensen DM, Stuart R, et al. Intravenous esomeprazole for prevention of recurrent peptic ulcer bleeding: a randomized trial. Ann Intern Med Apr 7;150(7): Song SY, Chung JB, Moon YM, Kang JK, Park IS. Comparison of the hemostatic effect of endoscopic injection with fibrin glue and hypertonic saline epinephrine for peptic ulcer bleeding: a prospective randomized trial. Endoscopy Nov;29(9): Ripoll C, Banares R, Beceiro I, Menchen P, Catalina MV, Echenagusia A, et al. Comparison of transcatheter arterial embolization and surgery for treatment of bleeding peptic ulcer after endoscopic treatment failure. J Vasc Interv Radiol May;15(5): Rostom A, Dube C, Wells G, Tugwell P, Welch V, Jolicoeur E, et al. Prevention of NSAID induced gastroduodenal ulcers. Cochrane Database Syst Rev. 2002(4):CD Gisbert JP, Khorrami S, Carballo F, Calvet X, Gene E, Dominguez Munoz JE. H. pylori eradication therapy vs. antisecretory non eradication therapy (with or without long term maintenance antisecretory therapy) for the prevention of recurrent bleeding from peptic ulcer. Cochrane Database Syst Rev. 2004(2):CD Garcia Tsao G, Sanyal AJ, Grace ND, Carey W. Prevention and management of gastroesophageal varices and variceal hemorrhage in cirrhosis. Hepatology Sep;46(3): Laine L, Cook D. Endoscopic ligation compared with sclerotherapy for treatment of esophageal variceal bleeding. A meta analysis. Ann Intern Med Aug 15;123(4): Chavez Tapia NC, Barrientos Gutierrez T, Tellez Avila FI, Soares Weiser K, Uribe M. Antibiotic prophylaxis for cirrhotic patients with upper gastrointestinal bleeding. Cochrane Database Syst Rev. 2010(9):CD Gotzsche PC, Hrobjartsson A. Somatostatin analogues for acute bleeding oesophageal varices. Cochrane Database Syst Rev. 2008(3):CD Rossle M, Haag K, Ochs A, Sellinger M, Noldge G, Perarnau JM, et al. The transjugular intrahepatic portosystemic stent shunt procedure for variceal bleeding. N Engl J Med Jan 20;330(3): Kamath PS, Wiesner RH, Malinchoc M, Kremers W, Therneau TM, Kosberg CL, et al. A model to predict survival in patients with end stage liver disease. Hepatology Feb;33(2): Lau JY, Leung WK, Wu JC, Chan FK, Wong VW, Chiu PW, et al. Omeprazole before endoscopy in patients with gastrointestinal bleeding. N Engl J Med Apr 19;356(16): Romagnuolo J. Routine second look endoscopy: ineffective, costly and potentially misleading. Can J Gastroenterol Jun;18(6): Forrest JA, Finlayson ND, Shearman DJ. Endoscopy in gastrointestinal bleeding. Lancet Aug 17;2(7877):
ACG Clinical Guideline: Management of Patients with Ulcer Bleeding
 ACG Clinical Guideline: Management of Patients with Ulcer Bleeding Loren Laine, MD 1,2 and Dennis M. Jensen, MD 3 5 1 Section of Digestive Diseases, Yale University School of Medicine, New Haven, Connecticut,
ACG Clinical Guideline: Management of Patients with Ulcer Bleeding Loren Laine, MD 1,2 and Dennis M. Jensen, MD 3 5 1 Section of Digestive Diseases, Yale University School of Medicine, New Haven, Connecticut,
A bleeding ulcer: What can the GP do? Gastrointestinal bleeding is a relatively common. How is UGI bleeding manifested? Who is at risk?
 Focus on CME at the University of British Columbia A bleeding ulcer: What can the GP do? By Robert Enns, MD, FRCP Gastrointestinal bleeding is a relatively common disorder affecting thousands of Canadians
Focus on CME at the University of British Columbia A bleeding ulcer: What can the GP do? By Robert Enns, MD, FRCP Gastrointestinal bleeding is a relatively common disorder affecting thousands of Canadians
On-Call Upper GI Bleeding. Upper Gastrointestinal Bleeding
 On-Call Upper GI Bleeding John R Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Associate Professor of Medicine Harvard Medical School Upper Gastrointestinal Bleeding 300,000000 hospitalizations/year
On-Call Upper GI Bleeding John R Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Associate Professor of Medicine Harvard Medical School Upper Gastrointestinal Bleeding 300,000000 hospitalizations/year
Anticoagulants are a contributing factor. Other causes are Mallory-Weiss tears, AV malformations, and malignancy and aorto-enteric fistula.
 Upper GI Bleeding EMU2018 Dr. Walter Himmel MD Incidence: In non-cirrhotics, the commonest causes are peptic ulcer disease (50%) followed by erosive gastritis. In cirrhotic patients, variceal bleeding
Upper GI Bleeding EMU2018 Dr. Walter Himmel MD Incidence: In non-cirrhotics, the commonest causes are peptic ulcer disease (50%) followed by erosive gastritis. In cirrhotic patients, variceal bleeding
Improved risk assessment in upper GI bleeding
 EDITORIAL Improved risk assessment in upper GI bleeding Acute upper GI bleeding is the most common GI emergency, with a reported incidence in various epidemiological studies ranging from 50 to over 100
EDITORIAL Improved risk assessment in upper GI bleeding Acute upper GI bleeding is the most common GI emergency, with a reported incidence in various epidemiological studies ranging from 50 to over 100
Acute Upper Gastrointestinal Hemorrhage Surgical Perspective. Dr.J.H.Barnard Dept. of Surgery PAH
 Acute Upper Gastrointestinal Hemorrhage Surgical Perspective Dr.J.H.Barnard Dept. of Surgery PAH Introduction: AGH is a leading cause of admissions into ICU. Overall mortality 5-12%, but increases to 40%
Acute Upper Gastrointestinal Hemorrhage Surgical Perspective Dr.J.H.Barnard Dept. of Surgery PAH Introduction: AGH is a leading cause of admissions into ICU. Overall mortality 5-12%, but increases to 40%
Sangrado Gastrointestinal Alto Upper GI Bleeding
 Sangrado Gastrointestinal Alto Upper GI Bleeding Curso Internacional Retos Clinicos en la Gastroenterologia de Urgencias Asociacion Colombiana de Gastroenterologia 31 de Agosto, 2012 Pereira, Risaralda
Sangrado Gastrointestinal Alto Upper GI Bleeding Curso Internacional Retos Clinicos en la Gastroenterologia de Urgencias Asociacion Colombiana de Gastroenterologia 31 de Agosto, 2012 Pereira, Risaralda
James Irwin Gastroenterology Department Palmerston North Hospital. Acute Medicine Meeting Hutt Hospital. June 21, 2015
 The Management of Acute Upper Gastrointestinal Bleeding James Irwin Gastroenterology Department Palmerston North Hospital Acute Medicine Meeting Hutt Hospital June 21, 2015 Outline Common Definitions and
The Management of Acute Upper Gastrointestinal Bleeding James Irwin Gastroenterology Department Palmerston North Hospital Acute Medicine Meeting Hutt Hospital June 21, 2015 Outline Common Definitions and
GASTROINESTINAL BLEEDING. Dr.Ammar I. Abdul-Latif
 GASTROINESTINAL BLEEDING Dr.Ammar I. Abdul-Latif CLASSIFICATION OF G.I.BLEEDING GIB Appearance Acuity Site Apparent Acute Upper Obscure Chronic Lower UPPER&LOWER G.I.BLEEDING CAUSES OF UPPER G.I. BLEEDING
GASTROINESTINAL BLEEDING Dr.Ammar I. Abdul-Latif CLASSIFICATION OF G.I.BLEEDING GIB Appearance Acuity Site Apparent Acute Upper Obscure Chronic Lower UPPER&LOWER G.I.BLEEDING CAUSES OF UPPER G.I. BLEEDING
ICU Volume 14 - Issue 2 - Summer Matrix
 ICU Volume 14 - Issue 2 - Summer 2014 - Matrix Upper Gastrointestinal Bleeding Authors David Osman, MD Medical Intensive Care Unit Paris-South University Hospitals Assistance Publique-Hôpitaux de Paris
ICU Volume 14 - Issue 2 - Summer 2014 - Matrix Upper Gastrointestinal Bleeding Authors David Osman, MD Medical Intensive Care Unit Paris-South University Hospitals Assistance Publique-Hôpitaux de Paris
Upper GI Bleeding. HH Tsai MD FRCP FECG Consultant Gastroenterologist
 Upper GI Bleeding HH Tsai MD FRCP FECG Consultant Gastroenterologist Financial Disclosures I have no financial relationship with any manufacturer or supplier of any product mentioned in this talk. GI Audits:
Upper GI Bleeding HH Tsai MD FRCP FECG Consultant Gastroenterologist Financial Disclosures I have no financial relationship with any manufacturer or supplier of any product mentioned in this talk. GI Audits:
Upper Gastrointestinal Bleeding Score for Differentiating Variceal and Nonvariceal Upper Gastrointestinal Bleeding ABSTRACT
 44 Original Article Upper Gastrointestinal Bleeding Score for Differentiating Variceal and Jaroon Chasawat Varayu Prachayakul Supot Pongprasobchai ABSTRACT Background: Upper gastrointestinal bleeding (UGIB)
44 Original Article Upper Gastrointestinal Bleeding Score for Differentiating Variceal and Jaroon Chasawat Varayu Prachayakul Supot Pongprasobchai ABSTRACT Background: Upper gastrointestinal bleeding (UGIB)
Upper gastrointestinal bleeding in children. Nguyễn Diệu Vinh, MD Department of Gastroenterology
 Upper gastrointestinal bleeding in children Nguyễn Diệu Vinh, MD Department of Gastroenterology INTRODUCTION Upper gastrointestinal (UGI) bleeding : arising proximal to the ligament of Treitz in the distal
Upper gastrointestinal bleeding in children Nguyễn Diệu Vinh, MD Department of Gastroenterology INTRODUCTION Upper gastrointestinal (UGI) bleeding : arising proximal to the ligament of Treitz in the distal
UGI BLEED. Dr. KPP Abhilash Associate Professor Department of Emergency Medicine Christian Medical College, Vellore
 UGI BLEED Dr. KPP Abhilash Associate Professor Department of Emergency Medicine Christian Medical College, Vellore Outline UGI bleed: etiology and presentation Management: Non variceal / variceal bleed
UGI BLEED Dr. KPP Abhilash Associate Professor Department of Emergency Medicine Christian Medical College, Vellore Outline UGI bleed: etiology and presentation Management: Non variceal / variceal bleed
UPPER GASTROINTESTINAL BLEEDING STATE OF THE ART
 FOLIA MEDICA CRACOVIENSIA Vol. LIV, 4, 2014: 59 78 PL ISSN 0015-5616 59 Mirosław Szura 1, Artur Pasternak 1,2 UPPER GASTROINTESTINAL BLEEDING STATE OF THE ART Abstract: Upper gastrointestinal (GI) bleeding
FOLIA MEDICA CRACOVIENSIA Vol. LIV, 4, 2014: 59 78 PL ISSN 0015-5616 59 Mirosław Szura 1, Artur Pasternak 1,2 UPPER GASTROINTESTINAL BLEEDING STATE OF THE ART Abstract: Upper gastrointestinal (GI) bleeding
Review article: management of peptic ulcer bleeding the roles of proton pump inhibitors and Helicobacter pylori eradication
 Aliment Pharmacol Ther 2004; 19 (Suppl. 1): 66 70. Review article: management of peptic ulcer bleeding the roles of proton pump inhibitors and Helicobacter pylori eradication G. HOLTMANN* & C. W. HOWDEN
Aliment Pharmacol Ther 2004; 19 (Suppl. 1): 66 70. Review article: management of peptic ulcer bleeding the roles of proton pump inhibitors and Helicobacter pylori eradication G. HOLTMANN* & C. W. HOWDEN
ACUTE UPPER GASTROINTESTINAL HEMORRHAGE: PHARMACOLOGIC MANAGEMENT
 DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
Esophageal Varices Beta-Blockers or Band Ligation. Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph
 Esophageal Varices Beta-Blockers or Band Ligation Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph Esophageal Varices Beta-Blockers or Band Ligation? Risk of esophageal variceal
Esophageal Varices Beta-Blockers or Band Ligation Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph Esophageal Varices Beta-Blockers or Band Ligation? Risk of esophageal variceal
Turning off the tap: Endoscopy Blood & Guts: Transfusion and bleeding in the medical patient
 Turning off the tap: Endoscopy Blood & Guts: Transfusion and bleeding in the medical patient John Greenaway 1 Turning off the tap: Endoscopy Answer the questions Benefits and risks of endoscopy Urgency
Turning off the tap: Endoscopy Blood & Guts: Transfusion and bleeding in the medical patient John Greenaway 1 Turning off the tap: Endoscopy Answer the questions Benefits and risks of endoscopy Urgency
Emergency Surgery Board Department of General Surgery Rambam Health Care Campus
 Emergency Surgery Board Department of General Surgery Rambam Health Care Campus Surgical Complications of Peptic Ulcer Disease Bleeding Case Presentation and Review of the Literature Case Presentation
Emergency Surgery Board Department of General Surgery Rambam Health Care Campus Surgical Complications of Peptic Ulcer Disease Bleeding Case Presentation and Review of the Literature Case Presentation
Upper Gastrointestinal Bleeding and the Importance of an Early Endoscopic Study for Diagnosis: A Retrospective Study
 Case Report imedpub Journals http://www.imedpub.com/ Medical Case Reports DOI: 10.21767/2471-8041.100062 Upper Gastrointestinal Bleeding and the Importance of an Early Endoscopic Study for Diagnosis: A
Case Report imedpub Journals http://www.imedpub.com/ Medical Case Reports DOI: 10.21767/2471-8041.100062 Upper Gastrointestinal Bleeding and the Importance of an Early Endoscopic Study for Diagnosis: A
Management of acute upper gastrointestinal bleeding
 1 Department of Gastroenterology, Glasgow Royal Infirmary, Glasgow G4 OSF, UK 2 Section of Digestive Diseases, Yale School of Medicine, New Haven, and VA Connecticut Healthcare System, West Haven, Connecticut,
1 Department of Gastroenterology, Glasgow Royal Infirmary, Glasgow G4 OSF, UK 2 Section of Digestive Diseases, Yale School of Medicine, New Haven, and VA Connecticut Healthcare System, West Haven, Connecticut,
MANAGING GI BLEEDING IN A COMMUNITY HOSPITAL SETTING DR M. F. M. BRULE
 MANAGING GI BLEEDING IN A COMMUNITY HOSPITAL SETTING DR M. F. M. BRULE DISCLOSURES Presenter: Dr Michele Brule Relationships with commercial interests: None OBJECTIVES Assess the severity of GI bleeding
MANAGING GI BLEEDING IN A COMMUNITY HOSPITAL SETTING DR M. F. M. BRULE DISCLOSURES Presenter: Dr Michele Brule Relationships with commercial interests: None OBJECTIVES Assess the severity of GI bleeding
COPYRIGHTED MATERIAL. 1 Approach to the patient with gross gastrointestinal bleeding. Grace H. Elta, Mimi Takami
 1 Approach to the patient with gross gastrointestinal bleeding Grace H. Elta, Mimi Takami Gastrointestinal (GI) bleeding is a common clinical problem that requires more than 300 000 hospitalizations annually
1 Approach to the patient with gross gastrointestinal bleeding Grace H. Elta, Mimi Takami Gastrointestinal (GI) bleeding is a common clinical problem that requires more than 300 000 hospitalizations annually
Simon Everett. Consultant Gastroenterologist, SJUH, Leeds. if this is what greets you in the morning, you probably need to go see a doctor
 Simon Everett Consultant Gastroenterologist, SJUH, Leeds if this is what greets you in the morning, you probably need to go see a doctor Presentation Audit data and mortality NICE guidance Risk assessment
Simon Everett Consultant Gastroenterologist, SJUH, Leeds if this is what greets you in the morning, you probably need to go see a doctor Presentation Audit data and mortality NICE guidance Risk assessment
Peptic ulcer bleeding remains the most common cause of hospitalization
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2009;7:311 316 Predicting Mortality in Patients With Bleeding Peptic Ulcers After Therapeutic Endoscopy PHILIP W. Y. CHIU,* ENDERS K. W. NG,* FRANCES K. Y. CHEUNG,*
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2009;7:311 316 Predicting Mortality in Patients With Bleeding Peptic Ulcers After Therapeutic Endoscopy PHILIP W. Y. CHIU,* ENDERS K. W. NG,* FRANCES K. Y. CHEUNG,*
Clinical outcome of acute nonvariceal upper gastrointestinal bleeding after hours: the role of urgent endoscopy
 ORIGINAL ARTICLE Korean J Intern Med 2016;31:470-478 Clinical outcome of acute nonvariceal upper gastrointestinal bleeding after hours: the role of urgent endoscopy Dong-Won Ahn 1,2,*, Young Soo Park 1,3,*,
ORIGINAL ARTICLE Korean J Intern Med 2016;31:470-478 Clinical outcome of acute nonvariceal upper gastrointestinal bleeding after hours: the role of urgent endoscopy Dong-Won Ahn 1,2,*, Young Soo Park 1,3,*,
Clinical and Endoscopic Features of Peptic Ulcer Bleeding in Malaysia
 Clinical and Endoscopic Features of Peptic Ulcer Bleeding in Malaysia * P Kandasami, FRCS, ** K Harjit, FRCS, *** H Hanafiah, FRCS * Department of Surgery, International Medical University, ** Department
Clinical and Endoscopic Features of Peptic Ulcer Bleeding in Malaysia * P Kandasami, FRCS, ** K Harjit, FRCS, *** H Hanafiah, FRCS * Department of Surgery, International Medical University, ** Department
Clinical Endoscopic Parameters of Upper Gastrointestinal Bleeding Hemal Shah, 1 T. P. Manohar 2
 Original Article Clinical Endoscopic Parameters of Upper Gastrointestinal Bleeding Hemal Shah, 1 T. P. Manohar 2 1 Junior Resident 2 Associate Professor,Department of Medicine, N.K.P. Salve Institute Of
Original Article Clinical Endoscopic Parameters of Upper Gastrointestinal Bleeding Hemal Shah, 1 T. P. Manohar 2 1 Junior Resident 2 Associate Professor,Department of Medicine, N.K.P. Salve Institute Of
Guidelines for the Management of Upper gastrointestinal bleeding
 Guidelines for the Management of Upper gastrointestinal bleeding By Dr. Sinan Butrus F.I.C.M.S Clinical Standards & Guidelines Kurdistan Board For Medical Specialties Upper gastrointestinal bleeding is
Guidelines for the Management of Upper gastrointestinal bleeding By Dr. Sinan Butrus F.I.C.M.S Clinical Standards & Guidelines Kurdistan Board For Medical Specialties Upper gastrointestinal bleeding is
UGI Bleeding: Impact and Outcome of Early Endoscopy at the Referral Community Hospital ABSTRACT
 Original Article Jewsuebpong T THAI J GASTROENTEROL 2008 Vol. 9 No. 2 May - Aug. 2008 67 UGI Bleeding: Impact and Outcome of Early Endoscopy at the Referral Community Hospital Jewsuebpong T ABSTRACT Background:
Original Article Jewsuebpong T THAI J GASTROENTEROL 2008 Vol. 9 No. 2 May - Aug. 2008 67 UGI Bleeding: Impact and Outcome of Early Endoscopy at the Referral Community Hospital Jewsuebpong T ABSTRACT Background:
Acute Upper Gastro Intestinal (UGI) Bleeding
 Bleeding") T Acute Upper Gastro Intestinal (UGI) Bleeding University Hospitals of Leicester NHS Trust Guidelines for Management of Acute Medical Emergencies 1. Has there been a GI bleed? There are also UHL trust
T Acute Upper Gastro Intestinal (UGI) Bleeding University Hospitals of Leicester NHS Trust Guidelines for Management of Acute Medical Emergencies 1. Has there been a GI bleed? There are also UHL trust
Upper Gastrointestinal Bleeding. December 4, 2018 & December 11, 2018 Sonia Lin
 Upper Gastrointestinal Bleeding December 4, 2018 & December 11, 2018 Sonia Lin Roadmap Evaluation of acute GIB Causes of upper GI bleeding Initial management of upper GI bleed Case 1 Case 2 Questions!
Upper Gastrointestinal Bleeding December 4, 2018 & December 11, 2018 Sonia Lin Roadmap Evaluation of acute GIB Causes of upper GI bleeding Initial management of upper GI bleed Case 1 Case 2 Questions!
Outcome of Upper Gastrointestinal Hemorrhage According to the BLEED Risk Classification: a Two-year Prospective Survey
 Bahrain Medical Bulletin, Vol. 29, No. 1, March 2007 Outcome of Upper Gastrointestinal Hemorrhage According to the BLEED Risk Classification: a Two-year Prospective Survey Javad Salimi, MD* Ahmad Salimzadeh,
Bahrain Medical Bulletin, Vol. 29, No. 1, March 2007 Outcome of Upper Gastrointestinal Hemorrhage According to the BLEED Risk Classification: a Two-year Prospective Survey Javad Salimi, MD* Ahmad Salimzadeh,
ACG Clinical Guideline: Management of Patients with Acute Lower Gastrointestinal Bleeding
 ACG Clinical Guideline: Management of Patients with Acute Lower Gastrointestinal Bleeding Lisa L. Strate, MD, MPH, FACG 1 and Ian M. Gralnek, MD, MSHS 2 1 Division of Gastroenterology, University of Washington
ACG Clinical Guideline: Management of Patients with Acute Lower Gastrointestinal Bleeding Lisa L. Strate, MD, MPH, FACG 1 and Ian M. Gralnek, MD, MSHS 2 1 Division of Gastroenterology, University of Washington
New Techniques. Incidence of Peptic Ulcer. Changing. Contents - with an emphasis on peptic ulcer bleeding. Cause of death in peptic ulcer bleeding
 Contents - with an emphasis on peptic ulcer bleeding New Techniques in Treating GI Bleeding Incidence and cause of death Acid suppression Endoscopic hemostasis Prediction of rebleeding and death Second
Contents - with an emphasis on peptic ulcer bleeding New Techniques in Treating GI Bleeding Incidence and cause of death Acid suppression Endoscopic hemostasis Prediction of rebleeding and death Second
Efficacy of dual therapy (APC & Adrenaline) in high risk peptic ulcer bleeding
 in high risk peptic ulcer bleeding") ISSN: 2347-3215 Volume 2 Number 7 (July-2014) pp. 203-208 www.ijcrar.com Efficacy of dual therapy (APC & Adrenaline) in high risk peptic ulcer bleeding Saleh Azad Bakht*, Manouchehr Khoshbaten, Kamal Bostani,
ISSN: 2347-3215 Volume 2 Number 7 (July-2014) pp. 203-208 www.ijcrar.com Efficacy of dual therapy (APC & Adrenaline) in high risk peptic ulcer bleeding Saleh Azad Bakht*, Manouchehr Khoshbaten, Kamal Bostani,
Eugenia Lauret, Jesús Herrero, Lorena Blanco, Olegario Castaño, Maria Rodriguez, Isabel Pérez, Verónica Alvarez, Adolfo Suárez, and Luis Rodrigo
 Gastroenterology Research and ractice Volume 2013, Article ID 584540, 5 pages http://dx.doi.org/10.1155/2013/584540 Clinical Study Epidemiological Clinical Features and Evolution of Gastroduodenal Ulcer
Gastroenterology Research and ractice Volume 2013, Article ID 584540, 5 pages http://dx.doi.org/10.1155/2013/584540 Clinical Study Epidemiological Clinical Features and Evolution of Gastroduodenal Ulcer
Clinical guideline Published: 13 June 2012 nice.org.uk/guidance/cg141
 Acute upper gastrointestinal bleeding in over 16s: management Clinical guideline Published: June 2012 nice.org.uk/guidance/cg141 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Acute upper gastrointestinal bleeding in over 16s: management Clinical guideline Published: June 2012 nice.org.uk/guidance/cg141 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Helicobacter pylori. Objectives. Upper Gastrointestinal Bleeding Peptic Ulcer Disease
 Upper Gastrointestinal Bleeding Peptic Ulcer Disease Pharmacotherapy Issues in Acute Management and Secondary Prevention Peter J. Zed, B.Sc., B.Sc.(Pharm), Pharm.D. Pharmacotherapeutic Specialist - Emergency
Upper Gastrointestinal Bleeding Peptic Ulcer Disease Pharmacotherapy Issues in Acute Management and Secondary Prevention Peter J. Zed, B.Sc., B.Sc.(Pharm), Pharm.D. Pharmacotherapeutic Specialist - Emergency
Gastrointestinal bleeding and life threating conditions in surgery
 CM w Bydgoszczy UMK w Toruniu Włodzimierz Gniłka Gastrointestinal bleeding and life threating conditions in surgery Gastrointestinal hemorrhage Upper GI hemorrhage proximal to the Treitz ligament (accounts
CM w Bydgoszczy UMK w Toruniu Włodzimierz Gniłka Gastrointestinal bleeding and life threating conditions in surgery Gastrointestinal hemorrhage Upper GI hemorrhage proximal to the Treitz ligament (accounts
Original Article INTRODUCTION
 Original Article Endoscopic treatment for high risk bleeding peptic ulcers: A randomized, controlled trial of epinephrine alone with epinephrine plus fresh Mahsa Khodadoostan, Mohammad Karami Horestani,
Original Article Endoscopic treatment for high risk bleeding peptic ulcers: A randomized, controlled trial of epinephrine alone with epinephrine plus fresh Mahsa Khodadoostan, Mohammad Karami Horestani,
Early Management of the Patient with Acute GI Bleeding
 Early Management of the Patient with Acute GI Bleeding Dr Sarah Hearnshaw Consultant Gastroenterologist Newcastle upon Tyne NHS Trust Go through.. Stats Transfusion / resuscitation PPIs When to call us
Early Management of the Patient with Acute GI Bleeding Dr Sarah Hearnshaw Consultant Gastroenterologist Newcastle upon Tyne NHS Trust Go through.. Stats Transfusion / resuscitation PPIs When to call us
PEPTIC ULCER DISEASE JOHN R SALTZMAN, MD. Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School
 PEPTIC ULCER DISEASE JOHN R SALTZMAN, MD Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School No disclosures Disclosures Overview Causes of peptic ulcer disease
PEPTIC ULCER DISEASE JOHN R SALTZMAN, MD Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School No disclosures Disclosures Overview Causes of peptic ulcer disease
Bleeding in the Digestive Tract
 Bleeding in the Digestive Tract National Digestive Diseases Information Clearinghouse National Institute of Diabetes and Digestive and Kidney Diseases NATIONAL INSTITUTES OF HEALTH U.S. Department of Health
Bleeding in the Digestive Tract National Digestive Diseases Information Clearinghouse National Institute of Diabetes and Digestive and Kidney Diseases NATIONAL INSTITUTES OF HEALTH U.S. Department of Health
Outline. GI-Bleeding. Initial intervention
 Internal Medicine Board Review 2016: GI-Bleeding Stephan Goebel, M.D. Assistant Professor Division of Digestive Diseases Management UGI-Bleeding (80%) Ulcers Varices others LGI-Bleeding (20%) Outline Initial
Internal Medicine Board Review 2016: GI-Bleeding Stephan Goebel, M.D. Assistant Professor Division of Digestive Diseases Management UGI-Bleeding (80%) Ulcers Varices others LGI-Bleeding (20%) Outline Initial
NICE Pathways bring together all NICE guidance, quality standards and other NICE information on a specific topic.
 bring together all NICE guidance, quality standards and other NICE information on a specific topic. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published.
bring together all NICE guidance, quality standards and other NICE information on a specific topic. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published.
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #10 Acute GI Bleeds
 McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #10 Acute GI Bleeds Gastrointestinal bleeding is a very common problem in emergency medicine. Between
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #10 Acute GI Bleeds Gastrointestinal bleeding is a very common problem in emergency medicine. Between
Definitive Surgical Treatment When Endoscopy Fails. Erik Peltz D.O. Resident Debate February 26 th 2007 University of Colorado Dept.
 Nonvariceal Gastrointestinal Hemorrhage: Definitive Surgical Treatment When Endoscopy Fails Erik Peltz D.O. Resident Debate February 26 th 2007 University of Colorado Dept. Surgery Non-Variceal Upper GI
Nonvariceal Gastrointestinal Hemorrhage: Definitive Surgical Treatment When Endoscopy Fails Erik Peltz D.O. Resident Debate February 26 th 2007 University of Colorado Dept. Surgery Non-Variceal Upper GI
Lower GI bleeding Management DR EHSANI PROFESSOR IN GASTROENTEROLOGY AND HEPATOLOGY
 Lower GI bleeding Management DR EHSANI PROFESSOR IN GASTROENTEROLOGY AND HEPATOLOGY 15 FEB 2018 Sources Sources Sources Initial evaluation History Physical examination Laboratory evaluation Obtained at
Lower GI bleeding Management DR EHSANI PROFESSOR IN GASTROENTEROLOGY AND HEPATOLOGY 15 FEB 2018 Sources Sources Sources Initial evaluation History Physical examination Laboratory evaluation Obtained at
Emergency Surgery Course Graz, March UPPER GI BLEEDING. Carlos Mesquita Coimbra
 UPPER GI BLEEDING Carlos Mesquita Coimbra Aim Causes Management Problem Above angle of Treitz Common emergency 1-2/1000 pts 10% rebleeed 1% angioembolization 20% over 60
UPPER GI BLEEDING Carlos Mesquita Coimbra Aim Causes Management Problem Above angle of Treitz Common emergency 1-2/1000 pts 10% rebleeed 1% angioembolization 20% over 60
Complicated issues in GI bleeding for internists? Nonthalee Pausawasdi, M.D. Faculty of Medicine Siriraj Hospital
 Complicated issues in GI bleeding for internists? Nonthalee Pausawasdi, M.D. Faculty of Medicine Siriraj Hospital Complicated issues in GI bleeding; Survey results from internists Optimal resuscitation
Complicated issues in GI bleeding for internists? Nonthalee Pausawasdi, M.D. Faculty of Medicine Siriraj Hospital Complicated issues in GI bleeding; Survey results from internists Optimal resuscitation
Predictive factors of mortality within 30 days in patients with nonvariceal upper gastrointestinal bleeding
 ORIGINAL ARTICLE Korean J Intern Med 2016;31:54-64 Predictive factors of mortality within 30 days in patients with nonvariceal upper gastrointestinal bleeding Yoo Jin Lee 1,*, Bo Ram Min 1,*, Eun Soo Kim
ORIGINAL ARTICLE Korean J Intern Med 2016;31:54-64 Predictive factors of mortality within 30 days in patients with nonvariceal upper gastrointestinal bleeding Yoo Jin Lee 1,*, Bo Ram Min 1,*, Eun Soo Kim
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Gastrointestinal bleeding: the management of acute upper gastrointestinal bleeding 1.1 Short title Acute upper GI bleeding
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Gastrointestinal bleeding: the management of acute upper gastrointestinal bleeding 1.1 Short title Acute upper GI bleeding
British Society of Gastroenterology. St. Elsewhere's Hospital. National Comparative Audit of Blood Transfusion
 British Society of Gastroenterology UK Com parat ive Audit of Upper Gast roint est inal Bleeding and t he Use of Blood Transfusion Extract December 2007 St. Elsewhere's Hospital National Comparative Audit
British Society of Gastroenterology UK Com parat ive Audit of Upper Gast roint est inal Bleeding and t he Use of Blood Transfusion Extract December 2007 St. Elsewhere's Hospital National Comparative Audit
When to Scope in Lower GI Bleeding: It Must Be Done Now. Lisa L. Strate, MD, MPH Assistant Professor of Medicine University of Washington, Seattle, WA
 When to Scope in Lower GI Bleeding: It Must Be Done Now Lisa L. Strate, MD, MPH Assistant Professor of Medicine University of Washington, Seattle, WA Outline Epidemiology Overview of available tests Urgent
When to Scope in Lower GI Bleeding: It Must Be Done Now Lisa L. Strate, MD, MPH Assistant Professor of Medicine University of Washington, Seattle, WA Outline Epidemiology Overview of available tests Urgent
Comparison of the Effectiveness of Interventional Endoscopy in Bleeding Peptic Ulcer Disease according to the Timing of Endoscopy
 Gut and Liver, Vol. 3, No. 4, December 2009, pp. 266-270 original article Comparison of the Effectiveness of Interventional Endoscopy in Bleeding Peptic Ulcer Disease according to the Timing of Endoscopy
Gut and Liver, Vol. 3, No. 4, December 2009, pp. 266-270 original article Comparison of the Effectiveness of Interventional Endoscopy in Bleeding Peptic Ulcer Disease according to the Timing of Endoscopy
Hydrogen Peroxide Improves the Visibility of Ulcer Bases in Acute Non-variceal Upper Gastrointestinal Bleeding: A Single-Center Prospective Study
 Dig Dis Sci (2009) 54:2427 2433 DOI 10.1007/s10620-009-0948-4 ORIGINAL ARTICLE Hydrogen Peroxide Improves the Visibility of Ulcer Bases in Acute Non-variceal Upper Gastrointestinal Bleeding: A Single-Center
Dig Dis Sci (2009) 54:2427 2433 DOI 10.1007/s10620-009-0948-4 ORIGINAL ARTICLE Hydrogen Peroxide Improves the Visibility of Ulcer Bases in Acute Non-variceal Upper Gastrointestinal Bleeding: A Single-Center
Blood and guts.. Haemodynamics / resuscitation. Haemodynamics / resuscitation. Blood and guts. Dr Jonathan Hoare
 Blood and guts. Dr Jonathan Hoare Consultant St Mary s Hospital Dr Jonathan Hoare Consultant St Mary s Hospital, Paddington Blood and guts.. Presentation Initial assessment and management risk stratification
Blood and guts. Dr Jonathan Hoare Consultant St Mary s Hospital Dr Jonathan Hoare Consultant St Mary s Hospital, Paddington Blood and guts.. Presentation Initial assessment and management risk stratification
Predictors for the need for endoscopic therapy in patients with presumed acute upper gastrointestinal
 ORIGINAL ARTICLE Korean J Intern Med 2019;34:288-295 Predictors for the need for endoscopic therapy in patients with presumed acute upper gastrointestinal bleeding Su Sun Kim, Kyung Up Kim, Sung Jun Kim,
ORIGINAL ARTICLE Korean J Intern Med 2019;34:288-295 Predictors for the need for endoscopic therapy in patients with presumed acute upper gastrointestinal bleeding Su Sun Kim, Kyung Up Kim, Sung Jun Kim,
Evidence-Base Management of Esophageal and Gastric Varices
 Evidence-Base Management of Esophageal and Gastric Varices Rino Alvani Gani Hepatobiliary Division Department of Internal Medicine Faculty of Medicine Universitas Indonesia Cipto Mangunkusumo National
Evidence-Base Management of Esophageal and Gastric Varices Rino Alvani Gani Hepatobiliary Division Department of Internal Medicine Faculty of Medicine Universitas Indonesia Cipto Mangunkusumo National
Aetiology Of Upper Gastrointestinal Bleeding In North- Eastern Nigeria: A Retrospective Endoscopic Study
 ISPUB.COM The Internet Journal of Third World Medicine Volume 8 Number 2 Aetiology Of Upper Gastrointestinal Bleeding In North- Eastern Nigeria: A Retrospective Endoscopic S Mustapha, N Ajayi, A Shehu
ISPUB.COM The Internet Journal of Third World Medicine Volume 8 Number 2 Aetiology Of Upper Gastrointestinal Bleeding In North- Eastern Nigeria: A Retrospective Endoscopic S Mustapha, N Ajayi, A Shehu
ACG & AASLD Joint Clinical Guideline: Prevention and Management of Gastroesophageal Varices and Variceal Hemorrhage in Cirrhosis
 ACG & AASLD Joint Clinical Guideline: Prevention and Management of Gastroesophageal Varices and Variceal Hemorrhage in Cirrhosis Guadalupe Garcia-Tsao, M.D., 1 Arun J. Sanyal, M.D., 2 Norman D. Grace,
ACG & AASLD Joint Clinical Guideline: Prevention and Management of Gastroesophageal Varices and Variceal Hemorrhage in Cirrhosis Guadalupe Garcia-Tsao, M.D., 1 Arun J. Sanyal, M.D., 2 Norman D. Grace,
Gastrointestinal Hemorrhage
 Gastrointestinal Hemorrhage Quality Measures Length of Stay RCC Costs per Case Mortality Rate Eligible Readmission Within 30 Days. Critical Event(s) Evaluation Phase/Acute Phase Baseline pain assessment
Gastrointestinal Hemorrhage Quality Measures Length of Stay RCC Costs per Case Mortality Rate Eligible Readmission Within 30 Days. Critical Event(s) Evaluation Phase/Acute Phase Baseline pain assessment
35 Practical Approach to Blood Vomiting
 C H A P T E R 35 Practical Approach to Blood Vomiting Jatinder K Mokta INTRODUCTION Hematemesis is defined as vomiting of blood, which is indicative of bleeding from the esophagus, stomach, or duodenum.
C H A P T E R 35 Practical Approach to Blood Vomiting Jatinder K Mokta INTRODUCTION Hematemesis is defined as vomiting of blood, which is indicative of bleeding from the esophagus, stomach, or duodenum.
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: helicobacter_pylori_testing 01/01/2019 N/A 01/01/2020 01/01/2019 Policy Effective April 1, 2019 Description
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: helicobacter_pylori_testing 01/01/2019 N/A 01/01/2020 01/01/2019 Policy Effective April 1, 2019 Description
Emergency - Upper gastrointestinal haemorrhage
 Emergency - Upper gastrointestinal haemorrhage Definitions in upper gastrointestinal (UGI) haemorrhage UGI haemorrhage: bleeding that arises proximal to the ligament of Treitz i.e. from the oesophagus,
Emergency - Upper gastrointestinal haemorrhage Definitions in upper gastrointestinal (UGI) haemorrhage UGI haemorrhage: bleeding that arises proximal to the ligament of Treitz i.e. from the oesophagus,
Research Article Outcome of Holiday and Nonholiday Admission Patients with Acute Peptic Ulcer Bleeding: A Real-World Report from Southern Taiwan
 BioMed Research International, Article ID 906531, 6 pages http://dx.doi.org/10.1155/2014/906531 Research Article Outcome of Holiday and Nonholiday Admission Patients with Acute Peptic Ulcer Bleeding: A
BioMed Research International, Article ID 906531, 6 pages http://dx.doi.org/10.1155/2014/906531 Research Article Outcome of Holiday and Nonholiday Admission Patients with Acute Peptic Ulcer Bleeding: A
Michele Bettinelli RN CCRN Lahey Health and Medical Center
 Michele Bettinelli RN CCRN Lahey Health and Medical Center Differentiate the types of varices Identify glue preparations utilized when treating gastric varices Review the process of glue administration
Michele Bettinelli RN CCRN Lahey Health and Medical Center Differentiate the types of varices Identify glue preparations utilized when treating gastric varices Review the process of glue administration
Rockall risk score in predicting 30 days non-variceal upper gastrointestinal rebleeding in a Malaysian population
 ORIGINAL ARTICLE Rockall risk score in predicting 30 days non-variceal upper gastrointestinal rebleeding in a Malaysian population Henry Tan Chor Lip, MD 1,2, Heah Hsin Tak, MMed Surg 1, Tan Jih Huei,
ORIGINAL ARTICLE Rockall risk score in predicting 30 days non-variceal upper gastrointestinal rebleeding in a Malaysian population Henry Tan Chor Lip, MD 1,2, Heah Hsin Tak, MMed Surg 1, Tan Jih Huei,
Abdominal Pain in a Young Aviator
 Abdominal Pain in a Young Aviator Calen N. Wherry, MD, MPH Maj, USAF, MC, FS Peter A. Baldwin, MD, MBA, MPH Capt, USAF, MC, FS USAF School of Aerospace Medicine WPAFB, OH RAM 2013 Distribution A: Approved
Abdominal Pain in a Young Aviator Calen N. Wherry, MD, MPH Maj, USAF, MC, FS Peter A. Baldwin, MD, MBA, MPH Capt, USAF, MC, FS USAF School of Aerospace Medicine WPAFB, OH RAM 2013 Distribution A: Approved
Upper Gastrointestinal Bleeding Among Saudis: Etiology And Prevalence The Riyadh Central Hospital Experience
 Upper Gastrointestinal Bleeding Among Saudis: Etiology And Prevalence The Riyadh Central Hospital Experience Mohammed Al-Mofarreh, Facharzt; Yisa M. Fakunle, MD, FRCP (London); Mohammed Al-Moagel, Facharzt
Upper Gastrointestinal Bleeding Among Saudis: Etiology And Prevalence The Riyadh Central Hospital Experience Mohammed Al-Mofarreh, Facharzt; Yisa M. Fakunle, MD, FRCP (London); Mohammed Al-Moagel, Facharzt
Changes in the Clinical Outcomes of Variceal Bleeding in Cirrhotic Patients: A 10-Year Experience in Gangwon Province, South Korea
 Gut and Liver, Vol. 6, No. 4, October 2012, pp. 476481 ORiginal Article Changes in the Clinical Outcomes of Variceal Bleeding in Cirrhotic Patients: A 10Year Experience in Gangwon Province, South Korea
Gut and Liver, Vol. 6, No. 4, October 2012, pp. 476481 ORiginal Article Changes in the Clinical Outcomes of Variceal Bleeding in Cirrhotic Patients: A 10Year Experience in Gangwon Province, South Korea
Guideline for the Management of Upper Gastrointestinal Bleeding in Children
 Guideline for the Management of Upper Gastrointestinal Bleeding in Children 1. Introduction Upper gastrointestinal (UGI) bleeding in children poses a challenge to paediatricians and paediatric surgeons.
Guideline for the Management of Upper Gastrointestinal Bleeding in Children 1. Introduction Upper gastrointestinal (UGI) bleeding in children poses a challenge to paediatricians and paediatric surgeons.
Scottish Medicines Consortium
 Scottish Medicines Consortium esomeprazole, 40mg vial of powder for solution for intravenous injection or infusion (Nexium I.V. ) No. (578/09) AstraZeneca 09 October 2009 The Scottish Medicines Consortium
Scottish Medicines Consortium esomeprazole, 40mg vial of powder for solution for intravenous injection or infusion (Nexium I.V. ) No. (578/09) AstraZeneca 09 October 2009 The Scottish Medicines Consortium
Effect of oral omeprazole in reducing re-bleeding in bleeding peptic ulcers: a prospective, double-blind, randomized, clinical trial
 Aliment Pharmacol Ther 2003; 17: 211 216. doi: 10.1046/j.0269-2813.2003.01416.x Effect of oral omeprazole in reducing re-bleeding in bleeding peptic ulcers: a prospective, double-blind, randomized, clinical
Aliment Pharmacol Ther 2003; 17: 211 216. doi: 10.1046/j.0269-2813.2003.01416.x Effect of oral omeprazole in reducing re-bleeding in bleeding peptic ulcers: a prospective, double-blind, randomized, clinical
Proton pump inhibitor treatment initiated prior to endoscopic diagnosis in upper gastrointestinal bleeding (Review)
") Proton pump inhibitor treatment initiated prior to endoscopic diagnosis in upper gastrointestinal bleeding (Review) Sreedharan A, Martin J, Leontiadis GI, Dorward S, Howden CW, Forman D, Moayyedi P This
Proton pump inhibitor treatment initiated prior to endoscopic diagnosis in upper gastrointestinal bleeding (Review) Sreedharan A, Martin J, Leontiadis GI, Dorward S, Howden CW, Forman D, Moayyedi P This
Endoclips vs large or small-volume epinephrine in peptic ulcer recurrent bleeding
 Online Submissions: http://www.wjgnet.com/1007-9327office wjg@wjgnet.com doi:10.3748/wjg.v18.i18.2219 World J Gastroenterol 2012 May 14; 18(18): 2219-2224 ISSN 1007-9327 (print) ISSN 2219-2840 (online)
Online Submissions: http://www.wjgnet.com/1007-9327office wjg@wjgnet.com doi:10.3748/wjg.v18.i18.2219 World J Gastroenterol 2012 May 14; 18(18): 2219-2224 ISSN 1007-9327 (print) ISSN 2219-2840 (online)
Perforated peptic ulcer
 Perforated peptic ulcer - Despite the widespread use of gastric anti-secretory agents and eradication therapy, the incidence of perforated peptic ulcer has changed little, age limits increase NSAIDs elderly
Perforated peptic ulcer - Despite the widespread use of gastric anti-secretory agents and eradication therapy, the incidence of perforated peptic ulcer has changed little, age limits increase NSAIDs elderly
Review of the endoscopic and medical management of non-variceal Upper Gastro-intestinal Bleeding
 Article ID: WMC005455 ISSN 2046-1690 Review of the endoscopic and medical management of non-variceal Upper Gastro-intestinal Bleeding Peer review status: No Corresponding Author: Dr. Mohammad Fawad Khattak,
Article ID: WMC005455 ISSN 2046-1690 Review of the endoscopic and medical management of non-variceal Upper Gastro-intestinal Bleeding Peer review status: No Corresponding Author: Dr. Mohammad Fawad Khattak,
Continuation of Low-Dose Aspirin Therapy with Either PR or PO Administration in Patients with Peptic Ulcer Bleeding
 Continuation of Low-Dose Aspirin Therapy with Either PR or PO Administration in Patients with Peptic Ulcer Bleeding IRB Protocol Lucian Iancovici February 4, 2010 A. Study Design and Purpose Aspirin has
Continuation of Low-Dose Aspirin Therapy with Either PR or PO Administration in Patients with Peptic Ulcer Bleeding IRB Protocol Lucian Iancovici February 4, 2010 A. Study Design and Purpose Aspirin has
WASSIM ABI JAOUDE, MD SUNY DOWNSTATE MEDICAL CENTER MAY 20 TH, 2010 MANAGEMENT OF ACUTE UPPER GI BLEEDING
 WASSIM ABI JAOUDE, MD SUNY DOWNSTATE MEDICAL CENTER MAY 20 TH, 2010 MANAGEMENT OF ACUTE UPPER GI BLEEDING CASE PRESENTATION 74 YO female JEHOVAH S WITNESS admitted for CHEST PAIN to telemetry on 4/26/2010
WASSIM ABI JAOUDE, MD SUNY DOWNSTATE MEDICAL CENTER MAY 20 TH, 2010 MANAGEMENT OF ACUTE UPPER GI BLEEDING CASE PRESENTATION 74 YO female JEHOVAH S WITNESS admitted for CHEST PAIN to telemetry on 4/26/2010
Internet Journal of Medical Update
 Internet Journal of Medical Update. 2017 July;12(2):4-9. doi: 10.4314/ijmu.v12i2.2 Internet Journal of Medical Update Journal home page: http://www.akspublication.com/ijmu Original Work A clinical study
Internet Journal of Medical Update. 2017 July;12(2):4-9. doi: 10.4314/ijmu.v12i2.2 Internet Journal of Medical Update Journal home page: http://www.akspublication.com/ijmu Original Work A clinical study
Nothing to disclose. Annually ~ 300,000 hospitalizations and ~ 20,000 deaths in US*
 Gastrointestinal Bleeding Disclosures Nothing to disclose Bennie Ray Upchurch III, MD, FACP, FASGE Clinical Associate Professor of Medicine Division of Gastroenterology, Hepatology & Nutrition The Ohio
Gastrointestinal Bleeding Disclosures Nothing to disclose Bennie Ray Upchurch III, MD, FACP, FASGE Clinical Associate Professor of Medicine Division of Gastroenterology, Hepatology & Nutrition The Ohio
Application of Forrest Classifiction in the Risk Assessment and Prediction of Rebleeding in Patients with Bleeding Peptic Ulcer in Ado-Ekiti, Nigeria
 American Journal of Medicine and Medical Sciences 214, 4(4): 18-113 DOI: 1.5923/j.ajmms.21444.2 Application of Forrest Classifiction in the Risk Assessment and Prediction of Rebleeding in Patients with
American Journal of Medicine and Medical Sciences 214, 4(4): 18-113 DOI: 1.5923/j.ajmms.21444.2 Application of Forrest Classifiction in the Risk Assessment and Prediction of Rebleeding in Patients with
Early Management of the Patient with Acute GI Bleeding
 Early Management of the Patient with Acute GI Bleeding Dr Sarah Hearnshaw Consultant Gastroenterologist Newcastle upon Tyne NHS Trust Go through.. Transfusion / resuscitation Anticoagulants new and old..
Early Management of the Patient with Acute GI Bleeding Dr Sarah Hearnshaw Consultant Gastroenterologist Newcastle upon Tyne NHS Trust Go through.. Transfusion / resuscitation Anticoagulants new and old..
Review Article The Acute Management of Nonvariceal Upper Gastrointestinal Bleeding
 Ulcers Volume 2012, Article ID 361425, 8 pages doi:10.1155/2012/361425 Review Article The Acute Management of Nonvariceal Upper Gastrointestinal Bleeding Hisham AL Dhahab and Alan Barkun Department of
Ulcers Volume 2012, Article ID 361425, 8 pages doi:10.1155/2012/361425 Review Article The Acute Management of Nonvariceal Upper Gastrointestinal Bleeding Hisham AL Dhahab and Alan Barkun Department of
CrackCast Episode 30 GI Bleeding
 CrackCast Episode 30 GI Bleeding Episode overview: 1) List 5 causes of UGIB in adults and pediatrics 2) List 5 causes of LGIB in adults and pediatrics 3) Describe your management approach for severe UGIB
CrackCast Episode 30 GI Bleeding Episode overview: 1) List 5 causes of UGIB in adults and pediatrics 2) List 5 causes of LGIB in adults and pediatrics 3) Describe your management approach for severe UGIB
The Role of Endoscopy in the Diagnosis and Management of Upper Gastrointestinal Bleeding.
 Original Article ISSN (O):2395-2822; ISSN (P):2395-2814 The Role of Endoscopy in the Diagnosis and Management of Upper Gastrointestinal Bleeding. Faroze A. Khan 1, M. H. Raza 2, Vikrant 1 1 Senior Resident,
Original Article ISSN (O):2395-2822; ISSN (P):2395-2814 The Role of Endoscopy in the Diagnosis and Management of Upper Gastrointestinal Bleeding. Faroze A. Khan 1, M. H. Raza 2, Vikrant 1 1 Senior Resident,
Peptic ulcer bleeding patients with Rockall scores 6 are at risk of long-term ulcer rebleeding: A 3.5-year prospective longitudinal study
 bs_bs_banner doi:10.1111/jgh.13822 GASTROENTEROLOGY Peptic ulcer bleeding patients with Rockall scores 6 are at risk of long-term ulcer rebleeding: A 3.5-year prospective longitudinal study Er-Hsiang Yang,*,,1
bs_bs_banner doi:10.1111/jgh.13822 GASTROENTEROLOGY Peptic ulcer bleeding patients with Rockall scores 6 are at risk of long-term ulcer rebleeding: A 3.5-year prospective longitudinal study Er-Hsiang Yang,*,,1
Proton pump inhibitor treatment initiated prior to endoscopic diagnosis in upper gastrointestinal bleeding (Review)
") Proton pump inhibitor treatment initiated prior to endoscopic diagnosis in upper gastrointestinal bleeding (Review) Sreedharan A, Martin J, Leontiadis GI, Dorward S, Howden CW, Forman D, Moayyedi P This
Proton pump inhibitor treatment initiated prior to endoscopic diagnosis in upper gastrointestinal bleeding (Review) Sreedharan A, Martin J, Leontiadis GI, Dorward S, Howden CW, Forman D, Moayyedi P This
Management for non-variceal upper gastrointestinal bleeding in elderly patients: the experience of a tertiary university hospital
 Original Article on Endoscopic Therapy Page 1 of 7 Management for non-variceal upper gastrointestinal bleeding in elderly patients: the experience of a tertiary university hospital Koichiro Kawaguchi,
Original Article on Endoscopic Therapy Page 1 of 7 Management for non-variceal upper gastrointestinal bleeding in elderly patients: the experience of a tertiary university hospital Koichiro Kawaguchi,
Lei Gu 1, Fei Xu 2,3 and Jie Yuan 1*
 Gu et al. BMC Gastroenterology (2018) 18:98 https://doi.org/10.1186/s12876-018-0828-5 RESEARCH ARTICLE Open Access Comparison of AIMS65, Glasgow Blatchford and Rockall scoring approaches in predicting
Gu et al. BMC Gastroenterology (2018) 18:98 https://doi.org/10.1186/s12876-018-0828-5 RESEARCH ARTICLE Open Access Comparison of AIMS65, Glasgow Blatchford and Rockall scoring approaches in predicting
Approach to upper gastrointestinal bleeding
 Approach to upper gastrointestinal bleeding Upper GI bleeding is the most common complication of peptic ulceration and portal hypertension. S R Thomson, ChM, FRCS (Edin&Eng) Professor and Head of Department,
Approach to upper gastrointestinal bleeding Upper GI bleeding is the most common complication of peptic ulceration and portal hypertension. S R Thomson, ChM, FRCS (Edin&Eng) Professor and Head of Department,
Management of non-variceal Upper G.I Bleed
 Article ID: WMC005456 ISSN 2046-1690 Management of non-variceal Upper G.I Bleed Peer review status: No Corresponding Author: Dr. Mohammad Fawad Khattak, Doctor, Walsall Manor Hospital - United Kingdom
Article ID: WMC005456 ISSN 2046-1690 Management of non-variceal Upper G.I Bleed Peer review status: No Corresponding Author: Dr. Mohammad Fawad Khattak, Doctor, Walsall Manor Hospital - United Kingdom
Assessment of short term prognosis in patients with upper gastrointestinal bleeding
 Medical Communication Biosci. Biotech. Res. Comm. 10(3): 341-345 (2017) Assessment of short term prognosis in patients with upper gastrointestinal bleeding Saeid Hashemieh (MD) 1, Ramtin Moradi (MD) 2,
Medical Communication Biosci. Biotech. Res. Comm. 10(3): 341-345 (2017) Assessment of short term prognosis in patients with upper gastrointestinal bleeding Saeid Hashemieh (MD) 1, Ramtin Moradi (MD) 2,
Chapter 14: Training in Radiology. DDSEP Chapter 1: Question 12
 DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
EGD Data Collection Form
 Sociodemographic Information Type Zip Code Gender Height (in inches) Race Ethnicity Inpatient Outpatient Male Female Birth Date Weight (in pounds) American Indian (Native American) or Alaska Native Asian
Sociodemographic Information Type Zip Code Gender Height (in inches) Race Ethnicity Inpatient Outpatient Male Female Birth Date Weight (in pounds) American Indian (Native American) or Alaska Native Asian
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Oakland K, Jairath V, Uberoi R, et al. Derivation
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Oakland K, Jairath V, Uberoi R, et al. Derivation
A cute upper gastrointestinal haemorrhage is
 399 BEST PRACTICE Management of haematemesis and melaena K Palmer... Acute upper gastrointestinal bleeding is a common medical emergency which carries hospital mortality in excess of 10%. The most important
399 BEST PRACTICE Management of haematemesis and melaena K Palmer... Acute upper gastrointestinal bleeding is a common medical emergency which carries hospital mortality in excess of 10%. The most important