Iron Deficiency Anaemia but Why? Dr LAU Ching-wa Specialist in Haematology Blood Transfusion Service
|
|
|
- Silas Roberts
- 5 years ago
- Views:
Transcription
1 Iron Deficiency but Why? Dr LAU Ching-wa Specialist in Haematology Blood Transfusion Service 1
2 3 Questions 1. Is anaemia incurable in my patient? 2. Is anaemia unavoidable in my bleeding patient? 3. Is transfusion improved clinical outcomes in this particular clinical scenario? 2








3 Iron Distribution Total Body Iron ~ 50mg/kg BW 3000~ 4000mg Blood Volume ~ 75ml/kg BW 2200~ 2600mg Total Iron in RBC 1ml blood 0.5mg elemental Iron Myoglobin & Iron containing Enzymes 300~ 400mg Average Store ~10mg/kg 500~ 1000mg Total Body Iron ~ 40mg/kg BW Blood Volume ~ 65ml/kg BW Average Store 5-10mg/kg 2000~ 3000mg 1300~ 1950mg 300~ 400mg 400~ 600mg 3


 Relative Iron")
4 Iron Homeostasis Absolute Iron Deficiency 1. Inadequate Iron Absorption 2. Blood Loss (1ml blood 0.5mg elemental Iron 1g/dl Hb 200mg elemental Iron loss) Relative Iron Deficiency Fail to Mobilize Iron Store of Chronic Illness 4
5 Underdiagnosed Being Screened During First-time Blood Donation (Aged 16~65) Proportion of Chinese First Time Donor who Failed Pre-donation Hemoglobin Check (2016 & 2017) Men (Cut-off Hb < 13.0 g/dl) Women (Cut-off Hb < 11.5 g/dl) Total No. Age of Group New Donors Total Overall in Men, n (%) 1066 (5.3%) 533 (5.3%) 262 (4.9%) 248 (7.2%) 158 (8.4%) 11 (11.8%) 2281 (5.6%) Mild (Hb g/dl) 1022 (5.1%) 515 (5.1%) 256 (4.8%) 238 (6.9%) 150 (8.0%) 10 (10.8%) 2194 (5.4%) Moderate (Hb g/dl) 43 (0.2%) 18 (0.2%) 6 (0.1%) 10 (0.3%) 8 (0.4%) 1 (1.0%) 86 (0.2%) Ferritin 1ng/mL 8mg Iron Store Severe (Hb < 8.0 g/dl) 1 (0.0%) 0 (0.0%) 0 (0.0%) 0 (0.0%) 0 (0.0%) 0 (0.0%) 1 (0.0%) Total No. of New Donors Overall in Women, n (%) 3379 (12.3%) 1368 (12.1%) 1199 (13.9%) 1109 (17.1%) 284 (9.0%) 10 (8.6%) 7352 (12.8%) Mild (Hb g/dl) 1542 (5.6%) 626 (5.5%) 501 (5.8%) 422 (6.5%) 155 (4.9%) 7 (6.0%) 3254 (5.7%) Another Study of Successful First-time Donors Female: 32.4% have serum ferritin level below 30ng/ml & 19.6% have serum ferritin level below 15ng/ml (n=102). Male: 1% have serum ferritin level below 30ng/ml (n=104). Moderate (Hb g/dl) 1789 (6.5%) 723 (6.4%) 675 (7.8%) 650 (10.0%) 124 (3.9%) 3 (2.6%) 3966 (6.9%) Severe (Hb < 8.0 g/dl) 48 (0.2%) 19 (0.2%) 23 (0.3%) 37 (0.6%) 5 (0.2%) 0 (0.0%) 132 (0.2%) Overall in Both Sexes 4445 (9.3%) 1901 (8.9%) 1461 (10.5%) 1357 (13.7%) 442 (8.8%) 21 (10.1%) 9633 (9.8%) Remark: WHO Definition of in Women 12.0g/dL 5 BTS Blood Donation Cutoff for Women: 11.5g/dL
6 Projected Overall Underdiagnosed in the Society (Aged 16~65) Data projected from Proportion of Low Hb Deferral of New Blood Donors 2016 to 2017 and Population Census data in 2017 Men Women Both Sexes Age group Mild (Hb g/dl) Moderate (Hb g/dl) Severe (Hb<8.0 g/dl) Overall in Men Overall in Men % Mild (Hb g/dl) Moderate (Hb g/dl) Severe (Hb<8.0 g/dl) Overall in Women Overall in Women % Mild (Hb 11 to 11.5 Moderate for female & (Hb 8 to 11 to 12.9g/dL for male) 10.9g/dL) Severe (Hb<8 g/dl) Overall in both sexes Overall in both sexes % % % % % % % % % % % % % % % % % % % Total % % % A portion of the mild anaemia may be related to thalassemia. However, moderate and severe anaemia can seldom be explained by thalassemia. Remark: WHO Definition of in Women 12.0g/dL 6 BTS Blood Donation Cutoff for Women: 11.5g/dL
7 Indications of Blood Transfusion in % 50% 14% Blood Loss (Gynecology 4%, GIB 20%, Elective operations 13%, Emergency operations 8%, Trauma 5%) Renal Insufficiency (Hemodialysis 7%, peritoneal dialysis and non-dialysis 7%) Marrow Failure 10%, Red Cell Disorders 6%, Hematological Malignancy 10%, some Oncological conditions 10% Data from CDARDS_2016 7


8 Perpetuation of Iron Deficiency Hospital Settings: Blood Transfusion as reflex response to treat Pathological causes of Blood Loss managed Under-diagnosed Iron Deficiency in many chronic illness e.g. Chronic Renal Impairment, Chronic Heart Failure, Malignancy, Inflammatory Conditions Blood Loss due to various procedures and blood taking Insufficient treatment to minimize Blood Loss Underlying Iron Deficiency seldom received adequate treatment GP/FM/SOPD Settings: Pathological causes of Blood Loss diagnosed and treated or referred to Hospital Underlying Iron Deficiency seldom received adequate treatment Insufficient treatment to control chronic Blood Loss (physiological or pathological) Anti-platelet or oral anticoagulation therapy may increase Blood Loss Acid suppressants inhibit Iron Absorption Iron Deficiency related to: Inadequate Iron Intake Suboptimal Iron Absorption Helicobacter Pylori Infection Physiological Blood Loss Suboptimal Iron Supplement during pregnancy Blood Donation Poor Compliance to Iron Therapy 8

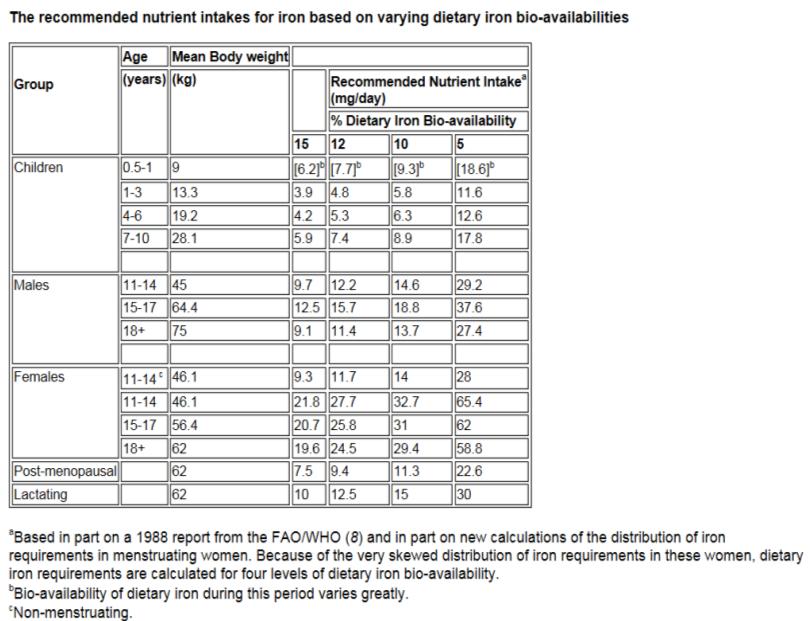
9 1. Inadequate Iron Intake >80% of the male population & >90% of the female population below the recommended nutrient intake level for iron for adult Centre for Food Safety of the Food and Environmental Hygiene Department

10 10


11 2. Food Interaction affecting Heme Iron Absorption 11


12 3. Food Interaction affecting non-heme Iron Absorption 12

13 4. Helicobacter Pylori 58.4% population is infected by H. Pylori H. Pylori diminishes Iron Absorption from diet A number of meta-analyses confirmed the role of H. pylori eradication in improving Iron Deficiency correction with appropriate Iron therapy 13
 for 1 year > 500mg Loss in Elemental")
14 5. Physiological Blood Loss in Women 1 ml Blood= 0.5mg Elemental Iron In 1g/dL Hb 200mg Loss in Elemental Iron Menorrhagia (>80ml/cycle) for 1 year > 500mg Loss in Elemental Iron / yr Each Full Term Pregnancy Consumes 900mg Elemental Iron (WHO) 14


15 6. Improper Iron Supplement for Pregnancy Multivitamin preparations should never be recommended as a sole therapy for iron deficient anemia, since the calcium, phosphorus and magnesium salts contained in iron-containing multivitamin pills impair absorption of elemental iron. 15

16 7. Repeated Blood Donation 1 ml Blood= 0.5mg Elemental Iron 200mg Elemental Iron loss in Each Donation N=420 16

17 Perpetuation of Iron Deficiency Hospital Settings: Blood Transfusion as reflex response to treat Pathological causes of Blood Loss managed Under-diagnosed Iron Deficiency in many chronic illness e.g. Chronic Renal Impairment, Chronic Heart Failure, Malignancy, Inflammatory Conditions Blood Loss due to various procedures and blood taking Insufficient treatment to minimize Blood Loss Underlying Iron Deficiency seldom received adequate treatment GP/FM/SOPD Settings: Pathological causes of Blood Loss diagnosed and treated or referred to Hospital Underlying Iron Deficiency seldom received adequate treatment Insufficient treatment to control chronic Blood Loss (physiological or pathological) Anti-platelet or oral anticoagulation therapy may increase Blood Loss Acid suppressants inhibit Iron Absorption Iron Deficiency related to: Inadequate Iron Intake Suboptimal Iron Absorption Helicobacter Pylori Infection Physiological Blood Loss Suboptimal Iron Supplement during pregnancy Blood Donation Poor Compliance to Iron Therapy 17
 Institution Cluster No.")
18 8. Drug Interaction affecting Iron Absorption Clinical Data Analysis & Reporting System Patient-Based Analysis Data Source in (User Defined Query: Antacids, H2 Receptor Antagonists or PPIs Drug Dispensing Date Between 01/01/2017 and 31/12/2017) Institution Cluster No. of Patient Headcount A B C D E F G Grand Total : 1,118,032 MEDICATIONS INHIBITING IRON ABSORPTION: H2 receptor blockers, antacid medications, proton pump inhibitors; tetracyclines, quinolones; ACEI; levothyroxine; levodopa, carbidopa; cholestyramine and colestipol (bile acid sequestrant) 18
 in ( Drug")
}» Drug Dispensing Date Between 01/01/2017 and 31/12/2017) Institution Cluster No.")
19 9. Anti-plaletet or oral anticoagulant may increase bleeding Clinical Data Analysis & Reporting System Patient-Based Analysis Data Source in ( «Drug{Therapeutic Classification (BNF, Principal or Secondary) in ( Drug BNF: 2.9 ANTIPLATELET DRUGS Drug BNF: ORAL ANTICOAGULANTS)}» Drug Dispensing Date Between 01/01/2017 and 31/12/2017) Institution Cluster No. of Patient Headcount A B C D E F G Grand Total : 411,804 19
20 Perpetuation of Iron Deficiency Hospital Settings: Blood Transfusion as reflex response to treat Pathological causes of Blood Loss managed Under-diagnosed Iron Deficiency in many chronic illness e.g. Chronic Renal Impairment, Chronic Heart Failure, Malignancy, Inflammatory Conditions Blood Loss due to various procedures and blood taking Insufficient treatment to minimize Blood Loss Underlying Iron Deficiency seldom received adequate treatment GP/FM/SOPD Settings: Pathological causes of Blood Loss diagnosed and treated or referred to Hospital Underlying Iron Deficiency seldom received adequate treatment Insufficient treatment to control chronic Blood Loss (physiological or pathological) Anti-platelet or oral anticoagulation therapy may increase Blood Loss Acid suppressants inhibit Iron Absorption Iron Deficiency related to: Inadequate Iron Intake Suboptimal Iron Absorption Helicobacter Pylori Infection Physiological Blood Loss Suboptimal Iron Supplement during pregnancy Blood Donation Poor Compliance to Iron Therapy 20

21 10. Gastrointestinal Blood Loss 1 ml Blood= 0.5mg Elemental Iron 1g/dL Hb 200mg Loss in Elemental Iron 21
 72 (3~105) 78 (0~106) 75 (0~105) Number of transfusion episodes 5,377 5,870 9,789 Units of RC transfused 9,179 10,262 16,558 Episodes Pre-transfusion Hb absent 97 (1.")
 1,602 (27.3%) 2,379 (24.3%) Multiple units RC given 3,230 (60.1%) 3,521 (60.0%) 5,510 (56.3%) Neither parenteral nor oral iron given 2,458 (68.2%) 2,352 (74.4%) 3,863 (68.")
22 11. GIB received Blood Transfusion in 2016: Underlying Iron Deficiency is Insufficiently Treated GI neoplasms Non-malignant Lower GIB Non-malignant Upper GIB Number of unique patients 3,604 3,161 5,612 Median age (range) 72 (3~105) 78 (0~106) 75 (0~105) Number of transfusion episodes 5,377 5,870 9,789 Units of RC transfused 9,179 10,262 16,558 Episodes Pre-transfusion Hb absent 97 (1.8%) 14 (0.2%) 17 (0.2%) Post-transfusion Hb absent 909 (16.9%) 305 (5.2%) 497 (5.1%) Pre-transfusion Hb 8 g/dl 1,423 (26.5%) 1,429 (24.3%) 2,043 (20.9%) Post transfusion Hb 10 g/dl 1,626 (30.2%) 1,602 (27.3%) 2,379 (24.3%) Multiple units RC given 3,230 (60.1%) 3,521 (60.0%) 5,510 (56.3%) Neither parenteral nor oral iron given 2,458 (68.2%) 2,352 (74.4%) 3,863 (68.8%) 1st Pillar 2nd Pillar 3 rd Pillar OPTIMIZE HEMATOPOIESIS MINIMIZE BLOOD LOSS OPTIMIZE PATIENT-SPECIFIC TOLERANCE TO ANAEMIA Neither parenteral nor oral iron in ~2/3 Post transfusion Hb 10 g/dl in 1/4 ~ 1/3 Multiple units RC given in ~2/3 Data from CDARDS
, Non-operation related Admission (2,906 Transfusion Episodes of 5,889 units RC in 2,523 Unique Patients) 1 unit RC 2 units RC 3")

23 12. Gynecology Patients received Blood Transfusion in 2016: Underlying Iron Deficiency is Insufficiently Treated Bleeding Condition is Insufficiently Managed Median Age Study Period between 01/01/2016 and 31/12/2016 Gynecology Patients Age 60 (range 11~60), Non-operation related Admission (2,906 Transfusion Episodes of 5,889 units RC in 2,523 Unique Patients) 1 unit RC 2 units RC 3 units RC 4 units RC 5 units RC >5 units RC Total Transfusion Episodes Pretransfusion Hb Posttransfusion Hb <7 Posttransfusion Hb 7~8 Posttransfusion Hb 8~9 Posttransfusion Hb 9~10 Posttransfusion Hb >10 Posttransfusion Hb missing < ~ ~ ~ Pretransfusion Hb missing Total st Pillar OPTIMIZE HEMATOPOIESIS 2nd Pillar MINIMIZE BLOOD LOSS 3 rd Pillar OPTIMIZE PATIENT-SPECIFIC TOLERANCE TO ANAEMIA 23 Data from CDARDS_2016
24 13. Treatment in Hemodialysis: Underlying Iron Deficiency is Insufficiently Treated 18.4% IV IRON 3.4% 0.2% Hemodialysis Headcount Percentage No Treatment % Transfusion Alone % EPO Alone % IV Iron Alone 8 0.2% EPO +IV Iron % EPO+Transfusion % IV Iron+ Transfusion % EPO+ IV Iron+ Transfusion % EPO 4.6% 0.4% 29.0% N= % TRANSFUSION No Treatment 15.9% 24 Data from CDARDS_2016



25 14. Operation 1 ml Blood= 0.5mg Elemental Iron 1g/dL Hb 200mg Loss in Elemental Iron is present in up to 90% of patients in the immediate postoperative period after major surgery. 25
26 15.Obstetric Patients undergoing Cesarean Section in 2016/17: Bleeding Condition is Insufficiently Managed Hospital Code in (All Hospitals) AND Discharge Date between 01/10/2016 and 30/09/2017 AND Diagnosis Code (ICD9) in (74 CESAREAN SECTION AND REMOVAL OF FETUS) Use of IV Transamin Yes No Row Total Institution Cluster No. of Episodes No. of Episodes No. of Episodes (Admission Date) Headcounts Headcounts Headcounts A B C D E F G Grand Total : Data from CDARDS 26
27 16. Obstetric Patients with PPH in 2016/17: Bleeding Condition is Insufficiently Managed Hospital Code in (All Hospitals) AND Discharge Date between 01/10/2016 and 30/09/2017 AND Diagnosis Code (ICD9) in (666 POSTPARTUM HEMORRHAGE) Use of IV Transamin Yes No Row Total Institution Cluster No. of Episodes No. of Episodes No. of Episodes (Admission Date) Headcounts Headcounts Headcounts A B C D E F G Grand Total : Data from CDARDS 27
28 Perpetuation of Iron Deficiency Hospital Settings: Blood Transfusion as reflex response to treat Pathological causes of Blood Loss managed Under-diagnosed Iron Deficiency in many chronic illness e.g. Chronic Renal Impairment, Chronic Heart Failure, Malignancy, Inflammatory Conditions Blood Loss due to various procedures and blood taking Insufficient treatment to minimize Blood Loss Underlying Iron Deficiency seldom received adequate treatment GP/FM/SOPD Settings: Pathological causes of Blood Loss diagnosed and treated or referred to Hospital Underlying Iron Deficiency seldom received adequate treatment Insufficient treatment to control chronic Blood Loss (physiological or pathological) Anti-platelet or oral anticoagulation therapy may increase Blood Loss Acid suppressants inhibit Iron Absorption Iron Deficiency related to: Inadequate Iron Intake Suboptimal Iron Absorption Helicobacter Pylori Infection Physiological Blood Loss Suboptimal Iron Supplement during pregnancy Blood Donation Poor Compliance to Iron Therapy 28
29 Diagnosis WHO Definitions of in Adult (gm/dl) Mild Moderate Severe Pregnant women Non-pregnant women < <8 Men <8 WHO Definitions of Iron Deficiency Most global experts Definitions of Iron Deficiency <15 ng/ml <30 ng/ml Sensitivity 92% Positive predictive value 83% Ferritin 1ng/ml 8mg Iron Store 29
30 TRANSFUSION ALTERNATIVES 1. Maximizing endogenous red cell production by TRANSFUSION ALTERNATIVES 2. Minimizing endogenous red cell loss by TRANSFUSION ALTERNATIVES and good surgical and anesthetic techniques 3. Safe and appropriate use of ALLOGENEIC BLOOD TRANSFUSION to improve patient clinical outcomes, not the number 30
 Marrow Failure 10%, Red Cell Disorders 6%, Hematological Malignancy 10%, some Oncological conditions 10% Data from")
31 Clinical Scenarios in which Benefits of Transfusion out-weight the Risks 36% 50% 14% Blood Loss (Gynecology 4%, GIB 20%, Elective operations 13%, Emergency operations 8%, Trauma 5%) Renal Insufficiency (Hemodialysis 7%, peritoneal dialysis and non-dialysis 7%) Marrow Failure 10%, Red Cell Disorders 6%, Hematological Malignancy 10%, some Oncological conditions 10% Data from CDARDS_


32 Allogeneic red cell metabolized in a few weeks, the only thing left inside the patient is no more than 200mg of Elemental Iron Every Unit of Red Cell 200mg Elemental Iron

33 GLOBAL BENCHMARK 33
ANEMIA & HEMODIALYSIS
 ANEMIA & HEMODIALYSIS The anemia of CKD is, in most patients, normocytic and normochromic, and is due primarily to reduced production of erythropoietin by the kidney and to shortened red cell survival.
ANEMIA & HEMODIALYSIS The anemia of CKD is, in most patients, normocytic and normochromic, and is due primarily to reduced production of erythropoietin by the kidney and to shortened red cell survival.
Microcytic Hypochromic Anemia An Approach to Diagnosis
 Microcytic Hypochromic Anemia An Approach to Diagnosis Decreased hemoglobin synthesis gives rise to microcytic hypochromic anemias. Hypochromic anemias are characterized by normal cellular proliferation
Microcytic Hypochromic Anemia An Approach to Diagnosis Decreased hemoglobin synthesis gives rise to microcytic hypochromic anemias. Hypochromic anemias are characterized by normal cellular proliferation
Intravenous Iron: A Good Thing Made Better? Marilyn Telen, MD Wellcome Professor of Medicine Duke University
 Intravenous Iron: A Good Thing Made Better? Marilyn Telen, MD Wellcome Professor of Medicine Duke University Use of IV Iron There are increasing data regarding safety of IV iron. IV iron is superior to
Intravenous Iron: A Good Thing Made Better? Marilyn Telen, MD Wellcome Professor of Medicine Duke University Use of IV Iron There are increasing data regarding safety of IV iron. IV iron is superior to
Hematopoiesis, The hematopoietic machinery requires a constant supply iron, vitamin B 12, and folic acid.
 Hematopoiesis, 200 billion new blood cells per day The hematopoietic machinery requires a constant supply iron, vitamin B 12, and folic acid. hematopoietic growth factors, proteins that regulate the proliferation
Hematopoiesis, 200 billion new blood cells per day The hematopoietic machinery requires a constant supply iron, vitamin B 12, and folic acid. hematopoietic growth factors, proteins that regulate the proliferation
Types of Anaemias and their Management. S. Moncrieffe, Pharm.D., MPH, Dip.Ed., RPh. PSJ CE Mandeville Hotel April 27, 2014
 Types of Anaemias and their Management S. Moncrieffe, Pharm.D., MPH, Dip.Ed., RPh. PSJ CE Mandeville Hotel April 27, 2014 Objectives At the end of the presentations participants should be able to: 1. Define
Types of Anaemias and their Management S. Moncrieffe, Pharm.D., MPH, Dip.Ed., RPh. PSJ CE Mandeville Hotel April 27, 2014 Objectives At the end of the presentations participants should be able to: 1. Define
Iron depletion in frequently donating whole blood donors. B. Mayer, H. Radtke
 Iron depletion in frequently donating whole blood donors B. Mayer, H. Radtke Iron: relevance oxygen-transporting and storage proteins hemoglobin and myoglobin iron-containing centers in many enzymes mitochondrial
Iron depletion in frequently donating whole blood donors B. Mayer, H. Radtke Iron: relevance oxygen-transporting and storage proteins hemoglobin and myoglobin iron-containing centers in many enzymes mitochondrial
Management of Anaemia reduces Red cell Transfusion in NI. Dr Susan Atkinson NI Transfusion Committee
 Management of Anaemia reduces Red cell Transfusion in NI Dr Susan Atkinson NI Transfusion Committee BBTS September 2014 Patient and Client Council Department of Health Chief Medical Officer Expert Professionals
Management of Anaemia reduces Red cell Transfusion in NI Dr Susan Atkinson NI Transfusion Committee BBTS September 2014 Patient and Client Council Department of Health Chief Medical Officer Expert Professionals
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Intermediate Outcome
 Quality ID #328 (NQF 1667): Pediatric Kidney Disease: ESRD Patients Receiving Dialysis: Hemoglobin Level < 10 g/dl National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL
Quality ID #328 (NQF 1667): Pediatric Kidney Disease: ESRD Patients Receiving Dialysis: Hemoglobin Level < 10 g/dl National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL
Efficacy and tolerability of oral Sucrosomial Iron in CKD patients with anemia. Ioannis Griveas, MD, PhD
 Efficacy and tolerability of oral Sucrosomial Iron in CKD patients with anemia Ioannis Griveas, MD, PhD Anaemia is a state in which the quality and/or quantity of circulating red blood cells are below
Efficacy and tolerability of oral Sucrosomial Iron in CKD patients with anemia Ioannis Griveas, MD, PhD Anaemia is a state in which the quality and/or quantity of circulating red blood cells are below
Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89
 Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89 Presented by Jennifer Kurkulonis 1 FOUR MAJOR TYPES OF BLOOD CELLS White blood cells
Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89 Presented by Jennifer Kurkulonis 1 FOUR MAJOR TYPES OF BLOOD CELLS White blood cells
Anemia Management in Peritoneal Dialysis Patients Pranay Kathuria, FACP, FASN
 Anemia Management in Peritoneal Dialysis Patients Pranay Kathuria, FACP, FASN Professor of Medicine Director, Division of Nephrology and Hypertension University of Oklahoma College of Medicine Definition
Anemia Management in Peritoneal Dialysis Patients Pranay Kathuria, FACP, FASN Professor of Medicine Director, Division of Nephrology and Hypertension University of Oklahoma College of Medicine Definition
Utilizing Sysmex RET He to Evaluate Anemia in Cancer Patients
 Utilizing Sysmex RET He to Evaluate Anemia in Cancer Patients Ellinor I. Peerschke, Ph.D., F.A.H.A. Vice Chair, Laboratory Medicine Chief, Hematology & Coagulation Laboratory Services Memorial Sloan Kettering
Utilizing Sysmex RET He to Evaluate Anemia in Cancer Patients Ellinor I. Peerschke, Ph.D., F.A.H.A. Vice Chair, Laboratory Medicine Chief, Hematology & Coagulation Laboratory Services Memorial Sloan Kettering
Patient Blood Management in the Netherlands: Between practice and evidence
 Patient Blood Management in the Netherlands: Between practice and evidence Marian van Kraaij MD PhD hematologist transfusion medicine specialist Department of Transfusion Medicine, Sanquin Blood Bank Radboud
Patient Blood Management in the Netherlands: Between practice and evidence Marian van Kraaij MD PhD hematologist transfusion medicine specialist Department of Transfusion Medicine, Sanquin Blood Bank Radboud
Monitoring of iron in whole blood donors at Sanquin Blood Bank
 Monitoring of iron in whole blood donors at Sanquin Blood Bank M.G.J. van Kraaij, MD PhD Hematologist Transfusion Medicine Specialist Director Dept. Donor Affairs and Transfusion Medicine Sanquin Blood
Monitoring of iron in whole blood donors at Sanquin Blood Bank M.G.J. van Kraaij, MD PhD Hematologist Transfusion Medicine Specialist Director Dept. Donor Affairs and Transfusion Medicine Sanquin Blood
GASTROINTESTINAL SYSTEM MANAGEMENT OF DYSPEPSIA
 GASTROINTESTINAL SYSTEM MANAGEMENT OF DYSPEPSIA MANAGEMENT Dyspepsia refers to a spectrum of usually intermittent upper gastrointestinal symptoms, including epigastric pain and heartburn. For the majority
GASTROINTESTINAL SYSTEM MANAGEMENT OF DYSPEPSIA MANAGEMENT Dyspepsia refers to a spectrum of usually intermittent upper gastrointestinal symptoms, including epigastric pain and heartburn. For the majority
Oral Iron Safe, Effective, and Misunderstood Duke Debates 2017
 Oral Iron Safe, Effective, and Misunderstood Duke Debates 2017 John Strouse, MD, PhD Instructor (temp) Medicine and Pediatrics Director, Adult Sickle Cell Program April 20, 2017 1 Disclosures I have no
Oral Iron Safe, Effective, and Misunderstood Duke Debates 2017 John Strouse, MD, PhD Instructor (temp) Medicine and Pediatrics Director, Adult Sickle Cell Program April 20, 2017 1 Disclosures I have no
British Society of Gastroenterology. St. Elsewhere's Hospital. National Comparative Audit of Blood Transfusion
 British Society of Gastroenterology UK Com parat ive Audit of Upper Gast roint est inal Bleeding and t he Use of Blood Transfusion Extract December 2007 St. Elsewhere's Hospital National Comparative Audit
British Society of Gastroenterology UK Com parat ive Audit of Upper Gast roint est inal Bleeding and t he Use of Blood Transfusion Extract December 2007 St. Elsewhere's Hospital National Comparative Audit
I. Definitions. V. Evaluation A. History B. Physical Exam C. Laboratory evaluation D. Bone marrow examination E. Specialty referrals
 I. Definitions II. III. Red blood cell life cycle Iron metabolism IV. Causes of anemia A. Kinetic approach 1. decreased production 2. increased destruction 3. blood loss B. Morphologic approach 1. normocytic
I. Definitions II. III. Red blood cell life cycle Iron metabolism IV. Causes of anemia A. Kinetic approach 1. decreased production 2. increased destruction 3. blood loss B. Morphologic approach 1. normocytic
Blood Transfusion Guidelines in Clinical Practice
 Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
Erythropoiesis Stimulating Agents (ESA)
") Erythropoiesis Stimulating Agents (ESA) Policy Number: Original Effective Date: MM.04.008 04/15/2007 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 06/01/2015 Section: Prescription
Erythropoiesis Stimulating Agents (ESA) Policy Number: Original Effective Date: MM.04.008 04/15/2007 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 06/01/2015 Section: Prescription
BONE MARROW PERIPHERAL BLOOD Erythrocyte
 None Disclaimer Objectives Define anemia Classify anemia according to pathogenesis & clinical significance Understand Red cell indices Relate the red cell indices with type of anemia Interpret CBC to approach
None Disclaimer Objectives Define anemia Classify anemia according to pathogenesis & clinical significance Understand Red cell indices Relate the red cell indices with type of anemia Interpret CBC to approach
DR. SHAMSUL AZAHARI ZAINAL BADARI DEPARTMENT OF RESOURCES MANAGEMENT AND CONSUMER STUDIES FACULTY OF HUMAN ECOLOGY UPM
 DR. SHAMSUL AZAHARI ZAINAL BADARI DEPARTMENT OF RESOURCES MANAGEMENT AND CONSUMER STUDIES FACULTY OF HUMAN ECOLOGY UPM Mineral nutrients are inorganic elements found in food which the body cannot synthesis.
DR. SHAMSUL AZAHARI ZAINAL BADARI DEPARTMENT OF RESOURCES MANAGEMENT AND CONSUMER STUDIES FACULTY OF HUMAN ECOLOGY UPM Mineral nutrients are inorganic elements found in food which the body cannot synthesis.
Drugs Used in Anemia
 Drugs Used in Anemia Drugs of Anemia Anemia is defined as a below-normal plasma hemoglobin concentration resulting from: a decreased number of circulating red blood cells or an abnormally low total hemoglobin
Drugs Used in Anemia Drugs of Anemia Anemia is defined as a below-normal plasma hemoglobin concentration resulting from: a decreased number of circulating red blood cells or an abnormally low total hemoglobin
Comment on European Renal Best Practice Position Statement on Anaemia Management in Chronic Kidney Disease.
 Comment on European Renal Best Practice Position Statement on Anaemia Management in Chronic Kidney Disease. Goldsmith D, Blackman A, Gabbay F, June 2013 Kidney Disease: Improving Global Outcomes (KDIGO)
Comment on European Renal Best Practice Position Statement on Anaemia Management in Chronic Kidney Disease. Goldsmith D, Blackman A, Gabbay F, June 2013 Kidney Disease: Improving Global Outcomes (KDIGO)
Alister Jones Patient Blood Management Practitioner NHS Blood and Transplant
 Alister Jones Patient Blood Management Practitioner NHS Blood and Transplant All medical RCC transfusions (but only 1 in 3 haematology or oncology cases) in 3 x one week periods Medical specialties include:
Alister Jones Patient Blood Management Practitioner NHS Blood and Transplant All medical RCC transfusions (but only 1 in 3 haematology or oncology cases) in 3 x one week periods Medical specialties include:
INTERELATIONSHIP BETWEEN IDA AND VITAMIN D DEFICIENCY IS NOW ESTABLISHED
 INTERELATIONSHIP BETWEEN IDA AND VITAMIN D DEFICIENCY IS NOW ESTABLISHED Rationale for Combining Iron & Vit-D Vit D deficiency and Iron deficiency Anaemia the two most menacing disorders - are inter-related
INTERELATIONSHIP BETWEEN IDA AND VITAMIN D DEFICIENCY IS NOW ESTABLISHED Rationale for Combining Iron & Vit-D Vit D deficiency and Iron deficiency Anaemia the two most menacing disorders - are inter-related
Anemia 1: Fourth year Medical Students/ October/21/ 2015/ Abdallah Abbadi.MD.FRCP Professor
 Anemia 1: Fourth year Medical Students/ October/21/ 2015/ Abdallah Abbadi.MD.FRCP Professor Email: abdalla.awidi@gmail.com Main Hematological diseases A- Benign Hematology 1- Anemias 2- Bleeding disorders
Anemia 1: Fourth year Medical Students/ October/21/ 2015/ Abdallah Abbadi.MD.FRCP Professor Email: abdalla.awidi@gmail.com Main Hematological diseases A- Benign Hematology 1- Anemias 2- Bleeding disorders
WELCOME. Evaluation Summary
 WELCOME Evaluation Summary 489 delegates from 40 countries Delegate s specialty 239 respondents Delegate s professional activity 208 respondents Overall Evaluation This symposium was helpful for your clinical
WELCOME Evaluation Summary 489 delegates from 40 countries Delegate s specialty 239 respondents Delegate s professional activity 208 respondents Overall Evaluation This symposium was helpful for your clinical
GASTROINTESTINAL AND ANTIEMETIC DRUGS. Submitted by: Shaema M. Ali
 GASTROINTESTINAL AND ANTIEMETIC DRUGS Submitted by: Shaema M. Ali GASTROINTESTINAL AND ANTIEMETIC DRUGS by: Shaema M. Ali There are four common medical conditions involving the GI system 1) peptic ulcers
GASTROINTESTINAL AND ANTIEMETIC DRUGS Submitted by: Shaema M. Ali GASTROINTESTINAL AND ANTIEMETIC DRUGS by: Shaema M. Ali There are four common medical conditions involving the GI system 1) peptic ulcers
Epogen / Procrit. Epogen / Procrit (epoetin alfa) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.10.06 Section: Prescription Drugs Effective Date: April1, 2014 Subject: Epogen / Procrit Page: 1 of 7
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.10.06 Section: Prescription Drugs Effective Date: April1, 2014 Subject: Epogen / Procrit Page: 1 of 7
Chapter 06 Lecture Outline. See separate PowerPoint slides for all figures and tables preinserted into PowerPoint without notes.
 Chapter 06 Lecture Outline See separate PowerPoint slides for all figures and tables preinserted into PowerPoint without notes. Copyright 2016 McGraw-Hill Education. 2012 Pearson Permission Education,
Chapter 06 Lecture Outline See separate PowerPoint slides for all figures and tables preinserted into PowerPoint without notes. Copyright 2016 McGraw-Hill Education. 2012 Pearson Permission Education,
Preoperative anemia Common, consequential and correctable in non-emergent surgery By Kathrine Frey, MD
 Preoperative anemia Common, consequential and correctable in non-emergent surgery By Kathrine Frey, MD Preoperative anemia is common, especially in patients undergoing nonemergent high-blood-loss surgical
Preoperative anemia Common, consequential and correctable in non-emergent surgery By Kathrine Frey, MD Preoperative anemia is common, especially in patients undergoing nonemergent high-blood-loss surgical
Management of anemia in CKD
 Management of anemia in CKD Pierre Cochat, MD PhD Professor of Pediatrics Chair, Pediatrics & Pediatric Surgery Department Head, Center for Rare Renal Diseases Néphrogones Hospices Civils de Lyon & University
Management of anemia in CKD Pierre Cochat, MD PhD Professor of Pediatrics Chair, Pediatrics & Pediatric Surgery Department Head, Center for Rare Renal Diseases Néphrogones Hospices Civils de Lyon & University
MANAGEMENT OF DYSPEPSIA AND GASTRO-OESOPHAGEAL REFLUX DISEASE (GORD)
") DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT OF DYSPEPSIA AND GASTRO-OESOPHAGEAL REFLUX DISEASE (GORD) Routine endoscopic investigation of patients of any age, presenting with dyspepsia
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT OF DYSPEPSIA AND GASTRO-OESOPHAGEAL REFLUX DISEASE (GORD) Routine endoscopic investigation of patients of any age, presenting with dyspepsia
Peri-Surgical Anemia and the TAVR Patient
 Peri-Surgical Anemia and the TAVR Patient Kathrine P Frey, MD Fairview Southdale Hospital Director of Blood and Pre-Operative Anemia Management April, 2015 MIDWEST VALVE SYMPOSIUM, April 2015 Credentials
Peri-Surgical Anemia and the TAVR Patient Kathrine P Frey, MD Fairview Southdale Hospital Director of Blood and Pre-Operative Anemia Management April, 2015 MIDWEST VALVE SYMPOSIUM, April 2015 Credentials
RAPID REFERRAL ANEMIA CLINICS
 RAPID REFERRAL ANEMIA CLINICS REDUCING INAPPROPRIATE TRANSFUSION AND OPTIMIZING PATIENT CARE ALAN TINMOUTH ORBCON APRIL 11, 2018 www.ohri.ca Affiliated with Affilié à OBJECTIVES 1. Review rationale for
RAPID REFERRAL ANEMIA CLINICS REDUCING INAPPROPRIATE TRANSFUSION AND OPTIMIZING PATIENT CARE ALAN TINMOUTH ORBCON APRIL 11, 2018 www.ohri.ca Affiliated with Affilié à OBJECTIVES 1. Review rationale for
Anemia in the elderly. Nattiya Teawtrakul MD., PhD
 Anemia in the elderly Nattiya Teawtrakul MD., PhD Contents Definition of anemia in the elderly The impact of anemia in the elderly Etiology of anemia in the elderly Management of anemia in the elderly
Anemia in the elderly Nattiya Teawtrakul MD., PhD Contents Definition of anemia in the elderly The impact of anemia in the elderly Etiology of anemia in the elderly Management of anemia in the elderly
Iron deficiency anemia:
 بسم هللا الرمحن الرحمي Before we start: Dr. Malik suggested for the third immunity lecture to be a continuation for the hematology pharmacology. And he will discuss the drugs for treating leukemia and
بسم هللا الرمحن الرحمي Before we start: Dr. Malik suggested for the third immunity lecture to be a continuation for the hematology pharmacology. And he will discuss the drugs for treating leukemia and
Medication Prior Authorization Form
 Procrit, Aranesp and (Epoetin Alfa) Policy Number: 1043 Policy History Approve Date: 12/11/2015 Effective Date: 12/11/2015 Preauthorization All Plans Benefit plans vary in coverage and some plans may not
Procrit, Aranesp and (Epoetin Alfa) Policy Number: 1043 Policy History Approve Date: 12/11/2015 Effective Date: 12/11/2015 Preauthorization All Plans Benefit plans vary in coverage and some plans may not
3. Does the patient meet ALL of the following requirements? Y N
 Pharmacy Prior Authorization AETA BETTER HEALTH FLORIDA Procrit - Retacrit (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign
Pharmacy Prior Authorization AETA BETTER HEALTH FLORIDA Procrit - Retacrit (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign
Patient Blood Management Are you providing this? Jeannie Callum, BA, MD, FRCPC Associate Professor, University of Toronto
 Patient Blood Management Are you providing this? Jeannie Callum, BA, MD, FRCPC Associate Professor, University of Toronto Disclosures Relevant relationships with commercial entities: Octapharma, CSL Behring
Patient Blood Management Are you providing this? Jeannie Callum, BA, MD, FRCPC Associate Professor, University of Toronto Disclosures Relevant relationships with commercial entities: Octapharma, CSL Behring
Table 1 Baseline characteristics of 60 hemodialysis patients with atrial fibrillation and warfarin use
 Table 1 Baseline characteristics of 60 hemodialysis patients with atrial fibrillation and warfarin use Baseline characteristics Users (n = 28) Non-users (n = 32) P value Age (years) 67.8 (9.4) 68.4 (8.5)
Table 1 Baseline characteristics of 60 hemodialysis patients with atrial fibrillation and warfarin use Baseline characteristics Users (n = 28) Non-users (n = 32) P value Age (years) 67.8 (9.4) 68.4 (8.5)
Anemia 1: Fourth year Medical Students/ Feb/22/ Abdallah Awidi Abbadi.MD.FRCP.FRCPath Professor
 Anemia 1: Fourth year Medical Students/ Feb/22/ 2018 Abdallah Awidi Abbadi.MD.FRCP.FRCPath Professor Email: abdalla.awidi@gmail.com Kidney EPO O2 Sensor Blood vessel Definition: Anemia is operationally
Anemia 1: Fourth year Medical Students/ Feb/22/ 2018 Abdallah Awidi Abbadi.MD.FRCP.FRCPath Professor Email: abdalla.awidi@gmail.com Kidney EPO O2 Sensor Blood vessel Definition: Anemia is operationally
What You Need to Know About Blood Transfusion. Elianna Saidenberg May 2014
 What You Need to Know About Blood Transfusion Elianna Saidenberg May 2014 Objectives Why your doctor might order transfusion therapy Where does the blood come from The beginning of your transfusion Consent
What You Need to Know About Blood Transfusion Elianna Saidenberg May 2014 Objectives Why your doctor might order transfusion therapy Where does the blood come from The beginning of your transfusion Consent
Management of Dyspepsia
 MPharm Programme Management of Dyspepsia Slide 1 of 28 Learning Objectives Understand the principles and wider implications underpinning evidence based therapeutics in the key clinical specialities Objectively
MPharm Programme Management of Dyspepsia Slide 1 of 28 Learning Objectives Understand the principles and wider implications underpinning evidence based therapeutics in the key clinical specialities Objectively
ISTITUTO DI RICERCHE FARMACOLOGICHE MARIO NEGRI CLINICAL RESEARCH CENTER ALDO E FOR CELE RARE DACCO DISEASES ALDO E CELE DACCO
 ISTITUTO DI RICERCHE FARMACOLOGICHE MARIO NEGRI CENTRO MARIO DI NEGRI RICERCHE INSTITUTE CLINICHE FOR PHARMACOLOGICAL PER LE MALATTIE RESEARCH RARE CLINICAL RESEARCH CENTER ALDO E FOR CELE RARE DACCO DISEASES
ISTITUTO DI RICERCHE FARMACOLOGICHE MARIO NEGRI CENTRO MARIO DI NEGRI RICERCHE INSTITUTE CLINICHE FOR PHARMACOLOGICAL PER LE MALATTIE RESEARCH RARE CLINICAL RESEARCH CENTER ALDO E FOR CELE RARE DACCO DISEASES
Managing peri-operative anaemiathe Papworth way. Dr Andrew A Klein Royal Papworth Hospital Cambridge UK
 Managing peri-operative anaemiathe Papworth way Dr Andrew A Klein Royal Papworth Hospital Cambridge UK Conflicts of interest: Unrestricted educational grants/honoraria from CSL Behring, Brightwake Ltd,
Managing peri-operative anaemiathe Papworth way Dr Andrew A Klein Royal Papworth Hospital Cambridge UK Conflicts of interest: Unrestricted educational grants/honoraria from CSL Behring, Brightwake Ltd,
RED CELL DISTRIBUTION WIDTH
 RED CELL DISTRIBUTION WIDTH A NEW MARKER OF EXERCISE INTOLERANCE IN PATIENTS WITH CHRONIC HEART FAILURE Emeline Van Craenenbroeck, Paul Beckers, Nadine Possemiers, Christiaan Vrints, Viviane Conraads Cardiology
RED CELL DISTRIBUTION WIDTH A NEW MARKER OF EXERCISE INTOLERANCE IN PATIENTS WITH CHRONIC HEART FAILURE Emeline Van Craenenbroeck, Paul Beckers, Nadine Possemiers, Christiaan Vrints, Viviane Conraads Cardiology
Safety and effectiveness of intravenous iron sucrose versus oral iron for correction of preoperative anemia in women with menorrhagia
 Scientific Journal of Medical Science (2013) 2(9) 182-186 ISSN 2322-5025 doi: 10.14196/sjms.v2.i9.924 Contents lists available at Sjournals Journal homepage: www.sjournals.com Original article Safety and
Scientific Journal of Medical Science (2013) 2(9) 182-186 ISSN 2322-5025 doi: 10.14196/sjms.v2.i9.924 Contents lists available at Sjournals Journal homepage: www.sjournals.com Original article Safety and
THE PREVENTION OF IRON DEFICIENCY IN BLOOD DONORS: THE ITALIAN APPROACH. Dott.ssa U. La Rocca Rome, 28 March 2019
 THE PREVENTION O IRON DEICIENCY IN BLOOD DONORS: THE ITALIAN APPROACH Dott.ssa U. La Rocca Rome, 28 March 2019 MAIN CAUSES O ABSOLUTE IRON DEICIENCY/IRON DEICIENCY ANEMIA IRON DEICIENCY ANEMIA AECTS >1.2
THE PREVENTION O IRON DEICIENCY IN BLOOD DONORS: THE ITALIAN APPROACH Dott.ssa U. La Rocca Rome, 28 March 2019 MAIN CAUSES O ABSOLUTE IRON DEICIENCY/IRON DEICIENCY ANEMIA IRON DEICIENCY ANEMIA AECTS >1.2
Tranexamic acid and Iron in Haematology. Andy King-Venables Transfusion Practitioner Hinchingbrooke Hospital
 Tranexamic acid and Iron in Haematology Andy King-Venables Transfusion Practitioner Hinchingbrooke Hospital Why consider an alternative? Can t we just give blood? Why consider an alternative? Can t we
Tranexamic acid and Iron in Haematology Andy King-Venables Transfusion Practitioner Hinchingbrooke Hospital Why consider an alternative? Can t we just give blood? Why consider an alternative? Can t we
Approach to a pale child
 Approach to a pale child Dr. Dafalla Ahmed Babiker Jazan university objectives Definition of anemia Classification and causes Important points in history and physical examination Investigations. Definition
Approach to a pale child Dr. Dafalla Ahmed Babiker Jazan university objectives Definition of anemia Classification and causes Important points in history and physical examination Investigations. Definition
Hydroxyurea (Hydroxycarbamide) - Guidelines for treating children with Sickle Cell Disease
 - Guidelines for treating children with Sickle Cell Disease") Hydroxyurea (Hydroxycarbamide) - Guidelines for treating children with Sickle Cell Disease Patient selection The benefits of hydroxycarbamide should be discussed with all parents/carers of children with
Hydroxyurea (Hydroxycarbamide) - Guidelines for treating children with Sickle Cell Disease Patient selection The benefits of hydroxycarbamide should be discussed with all parents/carers of children with
Iron Status in Chronic Renal Failure with Anemia
 Chattagram Maa-O-Shishu Hospital Medical College Journal DOI: 10.11566/cmosh.2013.1201.12 Original Article Iron Status in Chronic Renal Failure with Anemia Shaheda Khanam 1 * Noorzahan Begum 2 AMM Ehteshamul
Chattagram Maa-O-Shishu Hospital Medical College Journal DOI: 10.11566/cmosh.2013.1201.12 Original Article Iron Status in Chronic Renal Failure with Anemia Shaheda Khanam 1 * Noorzahan Begum 2 AMM Ehteshamul
Myelodysplasia/Myeloproliferative Neoplasms (MDS/MPN) Post-HCT Data
 Post-HCT Data") Instructions for Myelodysplasia/Myeloproliferative Neoplasms (MDS/MPN) Post-HCT Data (Form 2114) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the Myelodysplasia/Myeloproliferative
Instructions for Myelodysplasia/Myeloproliferative Neoplasms (MDS/MPN) Post-HCT Data (Form 2114) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the Myelodysplasia/Myeloproliferative
Transfusions in Sickle Cell Disease: How, When and Why
 Transfusions in Sickle Cell Disease: How, When and Why James R. Eckman, MD Professor Emeritus of Hematology and Medical Oncology Emory University School of Medicine This work is supported by the Centers
Transfusions in Sickle Cell Disease: How, When and Why James R. Eckman, MD Professor Emeritus of Hematology and Medical Oncology Emory University School of Medicine This work is supported by the Centers
Dependance on chronic transfusion
 Dependance on chronic transfusion Pr Saliou Diop Hematology Blood transfusion Dakar- Sénégal diop@cnts-dakar.sn Introduction Chronic transfusion: Regular use of blood transfusion in patients with chronic
Dependance on chronic transfusion Pr Saliou Diop Hematology Blood transfusion Dakar- Sénégal diop@cnts-dakar.sn Introduction Chronic transfusion: Regular use of blood transfusion in patients with chronic
ESM Table 2 Data extraction form and key data from included studies
 ESM Table 2 Data extraction form and key data from included studies Author, year and title Behan, 2006 [21] Cessation of menstruation improves the correlation of FPG to hemoglobin A 1c in Caucasian women
ESM Table 2 Data extraction form and key data from included studies Author, year and title Behan, 2006 [21] Cessation of menstruation improves the correlation of FPG to hemoglobin A 1c in Caucasian women
AETNA BETTER HEALTH Prior Authorization guideline for Erythropoiesis Stimulating Agents (ESA)
") AETNA BETTER HEALTH Prior Authorization guideline for Erythropoiesis Stimulating Agents (ESA) Drugs Covered Procrit Epogen Aranesp Authorization guidelines For patients who meet all of the following: Does
AETNA BETTER HEALTH Prior Authorization guideline for Erythropoiesis Stimulating Agents (ESA) Drugs Covered Procrit Epogen Aranesp Authorization guidelines For patients who meet all of the following: Does
NUTRITIONAL CARE IN ANEMIA
 االله الرحمن الرحيم بسم NUTRITIONAL CARE IN ANEMIA Nutrition Departement Faculty of Medicine University of North Sumatera Definition Deficit of circulating RBC associated with diminished oxygen-carrying
االله الرحمن الرحيم بسم NUTRITIONAL CARE IN ANEMIA Nutrition Departement Faculty of Medicine University of North Sumatera Definition Deficit of circulating RBC associated with diminished oxygen-carrying
Blood. Biol 105 Lecture 14 Chapter 11
 Blood Biol 105 Lecture 14 Chapter 11 Outline I. Overview of blood II. Functions of blood III. Composition of blood IV. Composition of plasma V. Composition of formed elements VI. Platelets VII. White blood
Blood Biol 105 Lecture 14 Chapter 11 Outline I. Overview of blood II. Functions of blood III. Composition of blood IV. Composition of plasma V. Composition of formed elements VI. Platelets VII. White blood
L4-Iron Deficiency Anemia (IDA) & Biochemical Investigations
 & Biochemical Investigations") L4-Iron Deficiency Anemia (IDA) & Biochemical Investigations 1 st Year-College of Medicine Hematology Module-Biochemistry Semester II Dr. Basil OM Saleh Objectives Identify stages in development of IDA
L4-Iron Deficiency Anemia (IDA) & Biochemical Investigations 1 st Year-College of Medicine Hematology Module-Biochemistry Semester II Dr. Basil OM Saleh Objectives Identify stages in development of IDA
Policy for the use of intravenous Iron Dextran (CosmoFer )
") Policy for the use of intravenous Iron Dextran (CosmoFer ) Sharepoint Location Clinical Policies and Guidelines Sharepoint Index Directory General Policies and Guidelines Sub Area Haematology and Blood
Policy for the use of intravenous Iron Dextran (CosmoFer ) Sharepoint Location Clinical Policies and Guidelines Sharepoint Index Directory General Policies and Guidelines Sub Area Haematology and Blood
CODING KNOWLEDGE AND SKILLS ASSESSMENT Section I: Please read the following questions carefully and select the best answer.
 CODING KNOWLEDGE AND SKILLS ASSESSMENT Section I: Please read the following questions carefully and select the best answer. 1.) A coding professional may assume a cause and effect relationship between
CODING KNOWLEDGE AND SKILLS ASSESSMENT Section I: Please read the following questions carefully and select the best answer. 1.) A coding professional may assume a cause and effect relationship between
Cardiff & Vale (C&V) UHB Corporate Medicines Management Group (c MMG) SHARED CARE. Drug: MYCOPHENOLATE MOFETIL/SODIUM Protocol number: CV 15
 UHB Corporate Medicines Management Group (c MMG) SHARED CARE. Drug: MYCOPHENOLATE MOFETIL/SODIUM Protocol number: CV 15") Cardiff & Vale (C&V) UHB Corporate Medicines Management Group (c MMG) SHARED CARE Drug: MYCOPHENOLATE MOFETIL/SODIUM Protocol number: CV 15 Indication: RENAL, PANCREAS OR COMBINED RENAL PANCREAS TRANSPLANTATION
Cardiff & Vale (C&V) UHB Corporate Medicines Management Group (c MMG) SHARED CARE Drug: MYCOPHENOLATE MOFETIL/SODIUM Protocol number: CV 15 Indication: RENAL, PANCREAS OR COMBINED RENAL PANCREAS TRANSPLANTATION
CAUTION: You must refer to the intranet for the most recent version of this procedural document.
 Procedure for the use of Intravenous Iron Dextran (CosmoFer ) Sharepoint Location Sharepoint Index Directory Clinical Policies and Guidelines General Policies and Guidelines/ Haematology And blood transfusion
Procedure for the use of Intravenous Iron Dextran (CosmoFer ) Sharepoint Location Sharepoint Index Directory Clinical Policies and Guidelines General Policies and Guidelines/ Haematology And blood transfusion
Northern Treatment Advisory Group
 Northern Treatment Advisory Group Ferric Maltol (Feraccru ) for the treatment of iron deficiency Lead author: Daniel Hill Regional Drug & Therapeutics Centre (Newcastle) September 2018 2018 Summary Iron
Northern Treatment Advisory Group Ferric Maltol (Feraccru ) for the treatment of iron deficiency Lead author: Daniel Hill Regional Drug & Therapeutics Centre (Newcastle) September 2018 2018 Summary Iron
The Bleeding Jehovah s Witness: A Nightmare Scenario?
 The Bleeding Jehovah s Witness: A Nightmare Scenario? David Smith, Bristol Hospital Liaison Committee for Jehovah s Witnesses SW RTC: Bleeding in the Medical Patient - 21 February 2018 Jehovah s Witnesses
The Bleeding Jehovah s Witness: A Nightmare Scenario? David Smith, Bristol Hospital Liaison Committee for Jehovah s Witnesses SW RTC: Bleeding in the Medical Patient - 21 February 2018 Jehovah s Witnesses
IRON DEFICIENCY / ANAEMIA ANTHONY BEETON
 IRON DEFICIENCY / ANAEMIA ANTHONY BEETON HYPOXIA 1-2 mg IRON Labile iron Body iron ± 3 4 g Liver and the reticuloendothelial system and spleen (approximately 200 300 mg in adult women and 1 g in adult
IRON DEFICIENCY / ANAEMIA ANTHONY BEETON HYPOXIA 1-2 mg IRON Labile iron Body iron ± 3 4 g Liver and the reticuloendothelial system and spleen (approximately 200 300 mg in adult women and 1 g in adult
Present-on-Admission (POA) Coding
 Coding") 1 Present-on-Admission (POA) Coding Michael Pine, MD, MBA Michael Pine and Associates, Inc 2 POA and Coding Guidelines (1) Unless otherwise specified, a POA modifier must be assigned to each principal
1 Present-on-Admission (POA) Coding Michael Pine, MD, MBA Michael Pine and Associates, Inc 2 POA and Coding Guidelines (1) Unless otherwise specified, a POA modifier must be assigned to each principal
Safety Of. long-term PPI. Layli Eslami, MD Tehran, 1393
 Safety Of long-term PPI Layli Eslami, MD Tehran, 1393 n The introduction of PPIs in the late 1980s optimized the medical treatment of acidrelated disorders n In some cases such as GERD patients given the
Safety Of long-term PPI Layli Eslami, MD Tehran, 1393 n The introduction of PPIs in the late 1980s optimized the medical treatment of acidrelated disorders n In some cases such as GERD patients given the
Venous Thromboembolism. Prevention
 Venous Thromboembolism Prevention August 2010 Venous Thromboembloism Prevention 1 1 Expected Practice Assess all patients upon admission to the ICU for risk factors of venous thromboembolism (VTE) and
Venous Thromboembolism Prevention August 2010 Venous Thromboembloism Prevention 1 1 Expected Practice Assess all patients upon admission to the ICU for risk factors of venous thromboembolism (VTE) and
Cost-effectiveness of hydroxyurea in sickle cell anemia Moore R D, Charache S, Terrin M L, Barton F B, Ballas S K
 Cost-effectiveness of hydroxyurea in sickle cell anemia Moore R D, Charache S, Terrin M L, Barton F B, Ballas S K Record Status This is a critical abstract of an economic evaluation that meets the criteria
Cost-effectiveness of hydroxyurea in sickle cell anemia Moore R D, Charache S, Terrin M L, Barton F B, Ballas S K Record Status This is a critical abstract of an economic evaluation that meets the criteria
HAEMATOLOGY. Test Name Status Result Unit Reference Interval HbA1c (Glycated Haemoglobin) 5.4 % Method : HPLC Sample Type : Whole Blood EDTA
 5.4 % Method : HPLC Sample Type : Whole Blood EDTA") Institution Report Date 25-Dec-2016 05:59 PM HAEMATOLOGY HbA1c (Glycated Haemoglobin) 5.4 % 4.5-6.0 Method : HPLC Sample Type : Whole Blood EDTA REMARKS In vitro quantitative determination of HbA1c in
Institution Report Date 25-Dec-2016 05:59 PM HAEMATOLOGY HbA1c (Glycated Haemoglobin) 5.4 % 4.5-6.0 Method : HPLC Sample Type : Whole Blood EDTA REMARKS In vitro quantitative determination of HbA1c in
Disease Pathogenesis and Research Progression of Renal Anemia
 2018 3rd International Conference on Life Sciences, Medicine, and Health (ICLSMH 2018) Disease Pathogenesis and Research Progression of Renal Anemia Yingying Liu, Qi Jiang* Department of Nephrology, China-Japan
2018 3rd International Conference on Life Sciences, Medicine, and Health (ICLSMH 2018) Disease Pathogenesis and Research Progression of Renal Anemia Yingying Liu, Qi Jiang* Department of Nephrology, China-Japan
Research Article H. pylori May Not Be Associated with Iron Deficiency Anemia in Patients with Normal Gastrointestinal Tract Endoscopy Results
 Advances in Hematology, Article ID 375915, 4 pages http://dx.doi.org/10.1155/2014/375915 Research Article H. pylori May Not Be Associated with Iron Deficiency Anemia in atients with Normal Gastrointestinal
Advances in Hematology, Article ID 375915, 4 pages http://dx.doi.org/10.1155/2014/375915 Research Article H. pylori May Not Be Associated with Iron Deficiency Anemia in atients with Normal Gastrointestinal
PPIs: Good or Bad? 1. Basics of PPIs. Gastric Acid Basics. Outline. Gastric Acid Basics. Proton Pump Inhibitors (PPI)
") Outline Quick basics on Proton Pump Inhibitors (PPIs) PPIs: Good or Bad? What are potential risks of PPI therapy? How to approach your patients American Gastroenterology Association (AGA) recommendations
Outline Quick basics on Proton Pump Inhibitors (PPIs) PPIs: Good or Bad? What are potential risks of PPI therapy? How to approach your patients American Gastroenterology Association (AGA) recommendations
GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS
 CHILDREN S HOSPITALS AND CLINICS OF MINNESOTA Introduction: GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS These guidelines have been developed in conjunction with the hospital Transfusion Committee.
CHILDREN S HOSPITALS AND CLINICS OF MINNESOTA Introduction: GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS These guidelines have been developed in conjunction with the hospital Transfusion Committee.
Effective Health Care Program
 Comparative Effectiveness Review Number 83 Effective Health Care Program Biomarkers for Assessing and Managing Iron Deficiency Anemia in Late-Stage Chronic Kidney Disease Executive Summary Background Chronic
Comparative Effectiveness Review Number 83 Effective Health Care Program Biomarkers for Assessing and Managing Iron Deficiency Anemia in Late-Stage Chronic Kidney Disease Executive Summary Background Chronic
A bleeding ulcer: What can the GP do? Gastrointestinal bleeding is a relatively common. How is UGI bleeding manifested? Who is at risk?
 Focus on CME at the University of British Columbia A bleeding ulcer: What can the GP do? By Robert Enns, MD, FRCP Gastrointestinal bleeding is a relatively common disorder affecting thousands of Canadians
Focus on CME at the University of British Columbia A bleeding ulcer: What can the GP do? By Robert Enns, MD, FRCP Gastrointestinal bleeding is a relatively common disorder affecting thousands of Canadians
National Comparative Audit of red cell transfusion in Medical Patients Part Two
 National Comparative Audit of red cell transfusion in Medical Patients Part Two Dr. Kate Pendry, Project Clinical Lead John Grant-Casey, Project Manager August 2013 Part One 9216 cases from 181 sites (90%
National Comparative Audit of red cell transfusion in Medical Patients Part Two Dr. Kate Pendry, Project Clinical Lead John Grant-Casey, Project Manager August 2013 Part One 9216 cases from 181 sites (90%
LONG TERM FOLLOW-UP OF PATIENTS WITH FANCONI ANEMIA AFTER ALLOGENEIC T-CELL DEPLETED HEMATOPOITEIC STEM CELL TRANSPLANTATION FROM ALTERNATIVE DONORS
 LONG TERM FOLLOW-UP OF PATIENTS WITH FANCONI ANEMIA AFTER ALLOGENEIC T-CELL DEPLETED HEMATOPOITEIC STEM CELL TRANSPLANTATION FROM ALTERNATIVE DONORS Farid Boulad, Susan E Prockop, Praveen Anur, Danielle
LONG TERM FOLLOW-UP OF PATIENTS WITH FANCONI ANEMIA AFTER ALLOGENEIC T-CELL DEPLETED HEMATOPOITEIC STEM CELL TRANSPLANTATION FROM ALTERNATIVE DONORS Farid Boulad, Susan E Prockop, Praveen Anur, Danielle
Single unit transfusion audit PE Smith B Ferguson
 Single unit transfusion audit PE Smith B Ferguson Brief introduction Method: A retrospective audit performed in November 2015 Standards: All stable, normovolaemic adult inpatients who require transfusion
Single unit transfusion audit PE Smith B Ferguson Brief introduction Method: A retrospective audit performed in November 2015 Standards: All stable, normovolaemic adult inpatients who require transfusion
GI Pharmacology. Dr. Alia Shatanawi 5/4/2018
 GI Pharmacology Dr. Alia Shatanawi 5/4/2018 Drugs Used in Gastrointestinal Diseases Drugs used in Peptic Ulcer Diseases. Drugs Stimulating Gastrointestinal Motility &Laxatives. Antidiarrheal Agents. Drugs
GI Pharmacology Dr. Alia Shatanawi 5/4/2018 Drugs Used in Gastrointestinal Diseases Drugs used in Peptic Ulcer Diseases. Drugs Stimulating Gastrointestinal Motility &Laxatives. Antidiarrheal Agents. Drugs
Platelet Disorders. By : Saja Al-Oran
 Platelet Disorders By : Saja Al-Oran Introduction The platelet arise from the fragmentation of the cytoplasm of megakaryocyte in the bone marrow. circulate in the blood as disc-shaped anucleate particles
Platelet Disorders By : Saja Al-Oran Introduction The platelet arise from the fragmentation of the cytoplasm of megakaryocyte in the bone marrow. circulate in the blood as disc-shaped anucleate particles
BLOOD DONORS AND THALASSEMIA
 FIODS 3 rd International Seminar Lucca, 5 th October 2013 BLOOD DONORS AND THALASSEMIA Dr. Giancarlo Ferrazza, M.D. U.O.C. di Immunoematologia e Medicina Trasfusionale Policlinico Umberto I - Sapienza
FIODS 3 rd International Seminar Lucca, 5 th October 2013 BLOOD DONORS AND THALASSEMIA Dr. Giancarlo Ferrazza, M.D. U.O.C. di Immunoematologia e Medicina Trasfusionale Policlinico Umberto I - Sapienza
Acetaminophen recommendations from the Food and Drug Administration Advisory Committee
 TABLE OF CONTENTS Acetaminophen: recommendations from the FDA Advisory Committee 1 Recombinant human erythropoiesis-stimulating agents and mortality in cancer patients Hospital-acquired pneumonia: risks
TABLE OF CONTENTS Acetaminophen: recommendations from the FDA Advisory Committee 1 Recombinant human erythropoiesis-stimulating agents and mortality in cancer patients Hospital-acquired pneumonia: risks
LifeBridge Health Transfusion Service Sinai Hospital of Baltimore Northwest Hospital Center BQA Transfusion Criteria Version#2 POLICY NO.
 LifeBridge Health Transfusion Service Sinai Hospital of Baltimore Northwest Hospital Center BQA 1011.02 Transfusion Criteria Version#2 Department POLICY NO. PAGE NO. Blood Bank Quality Assurance Manual
LifeBridge Health Transfusion Service Sinai Hospital of Baltimore Northwest Hospital Center BQA 1011.02 Transfusion Criteria Version#2 Department POLICY NO. PAGE NO. Blood Bank Quality Assurance Manual
Massive Transfusion. MPQC Spring Summit April 29, Roger Belizaire MD PhD
 Massive Transfusion MPQC Spring Summit April 29, 2015 Roger Belizaire MD PhD Take home points 1. Blood is always available. Requests for massive transfusion or emergency release typically only require
Massive Transfusion MPQC Spring Summit April 29, 2015 Roger Belizaire MD PhD Take home points 1. Blood is always available. Requests for massive transfusion or emergency release typically only require
Guidelines for the Management of Dyspepsia and GORD. Gastroenterology/ Acute Adult Governance. Drugs and Therapeutics Committee
 Guidelines for the Management of Dyspepsia and GORD Document type: Version: 3.0 Author (name): Author (designation): Validated by Prescribing Dr. G. Lipscomb Date validated October 2015 Ratified by: Date
Guidelines for the Management of Dyspepsia and GORD Document type: Version: 3.0 Author (name): Author (designation): Validated by Prescribing Dr. G. Lipscomb Date validated October 2015 Ratified by: Date
2017 Repeat Audit of Red cell and Platelet Transfusion in Adult Haematology Patients
 07 Repeat Audit of Red cell and Platelet Transfusion in Adult Haematology Patients Haematology Audit July 07 The audit was conducted on adults undergoing surgery and who received a transfusion during a
07 Repeat Audit of Red cell and Platelet Transfusion in Adult Haematology Patients Haematology Audit July 07 The audit was conducted on adults undergoing surgery and who received a transfusion during a
Iron deficiency in heart failure
 Iron deficiency in heart failure Piotr Ponikowski, MD, PhD, FESC Department of Heart Diseases, Wroclaw Medical University Centre for Heart Diseases, Military Hospital, Wroclaw, Poland Objectives Importance
Iron deficiency in heart failure Piotr Ponikowski, MD, PhD, FESC Department of Heart Diseases, Wroclaw Medical University Centre for Heart Diseases, Military Hospital, Wroclaw, Poland Objectives Importance
Classification of Anaemia
 Classification of Anaemia Dr Roger Pool Department of Haematology NHLS & University of Pretoria MEASUREMENT OF HAEMATOCRIT The haematocrit ratio (Hct) is the proportion of blood made up of cells - mainly
Classification of Anaemia Dr Roger Pool Department of Haematology NHLS & University of Pretoria MEASUREMENT OF HAEMATOCRIT The haematocrit ratio (Hct) is the proportion of blood made up of cells - mainly
Management of dyspepsia and of Helicobacter pylori infection
 Management of dyspepsia and of Helicobacter pylori infection The University of Nottingham John Atherton Wolfson Digestive Diseases Centre University of Nottingham, UK Community management of dyspepsia
Management of dyspepsia and of Helicobacter pylori infection The University of Nottingham John Atherton Wolfson Digestive Diseases Centre University of Nottingham, UK Community management of dyspepsia
Intravenous Iron Requirement in Adult Hemodialysis Patients
 Intravenous Iron Requirement in Adult Hemodialysis Patients Timothy V. Nguyen, PharmD The author is a clinical pharmacy specialist with Holy Name Hospital in Teaneck, New Jersey. He is also an adjunct
Intravenous Iron Requirement in Adult Hemodialysis Patients Timothy V. Nguyen, PharmD The author is a clinical pharmacy specialist with Holy Name Hospital in Teaneck, New Jersey. He is also an adjunct
Clinician Blood Panel Results
 Page 1 of 8 Blood Panel - Markers Out of Range and Patterns (Pattern: proprietary formula using one or more Blood Markers) Blood Panel: Check for Markers that are out of Lab Range ***NOTE*** Only one supplement
Page 1 of 8 Blood Panel - Markers Out of Range and Patterns (Pattern: proprietary formula using one or more Blood Markers) Blood Panel: Check for Markers that are out of Lab Range ***NOTE*** Only one supplement
Alternatives to RBC Transfusion:
 Alternatives to RBC Transfusion: beyond Erythropoietin and David Shimabukuro, MDCM Department of Anesthesia and Perioperative Care Medical Director, 13 ICU UC SF 1 Agenda Background Erythropoietin Hemoglobin-based
Alternatives to RBC Transfusion: beyond Erythropoietin and David Shimabukuro, MDCM Department of Anesthesia and Perioperative Care Medical Director, 13 ICU UC SF 1 Agenda Background Erythropoietin Hemoglobin-based
DIABETES MELLITUS. Definition
 Definition DIABETES MELLITUS Diabetes Mellitus is absolute or relative insulin insufficiency, low insulin output from the pancreas or inresponsiveness of peripheral tissues to existing insulin Risk factor
Definition DIABETES MELLITUS Diabetes Mellitus is absolute or relative insulin insufficiency, low insulin output from the pancreas or inresponsiveness of peripheral tissues to existing insulin Risk factor
Maintenance intravenous iron therapy in pediatric hemodialysis patients Morgan H E, Gautam M, Geary D F
 Maintenance intravenous iron therapy in pediatric hemodialysis patients Morgan H E, Gautam M, Geary D F Record Status This is a critical abstract of an economic evaluation that meets the criteria for inclusion
Maintenance intravenous iron therapy in pediatric hemodialysis patients Morgan H E, Gautam M, Geary D F Record Status This is a critical abstract of an economic evaluation that meets the criteria for inclusion
Combining. and New Diagnostic. to Help Clinicians Achieve. Patient Outcomes at. per Healthcare Encounter
 Combining and New Diagnostic to Help Clinicians Achieve Patient Outcomes at per Healthcare Encounter Holly McDaniel, MD hmcdaniel@clinpath.com Holly.mcdaniel@bannerhealth.com Holly McDaniel, MD AP/CP and
Combining and New Diagnostic to Help Clinicians Achieve Patient Outcomes at per Healthcare Encounter Holly McDaniel, MD hmcdaniel@clinpath.com Holly.mcdaniel@bannerhealth.com Holly McDaniel, MD AP/CP and