When and How to avoid Antipsychotics in Patients with Dementia and Behavioral Symptoms
|
|
|
- Samson Washington
- 5 years ago
- Views:
Transcription

1 When and How to avoid Antipsychotics in Patients with Dementia and Behavioral Symptoms Elizabeth Eckstrom, MD, MPH* Oregon Health & Science University Oregon Partnership to Improve Dementia Care *I have no disclosures
2 Today s Patients Mr. Smith has been hitting- especially when helped to the bathroom Mr. Jones is anxious, withdrawn after a hospitalization Mrs. Black is insisting she see her mother
3 Mr. Smith is having distress Mr. Smith is 84 and has had dementia for several years. He lives in a memory care facility; needs help with all his ADLs except eating. His wife lives in assisted living and spends much of the day with him. Staff notes he is becoming paranoid, and Mrs. Smith admits he has hit her several times when she tries to help him to the bathroom. He is starting to fall, and team members are having a harder time getting him up. He no longer speaks in full sentences, has become incontinent, and is spitting out his food. He has lost 10 pounds in the last several months.
4 Why is Mr. Smith aggressive? You begin to examine Mr. Smith, and notice growing agitation when you examine his stomach and legs. You ask when Mr. Smith has been aggressive, and it is with toileting and transfering. You ask if he had osteoarthritis or other pain in the past, and Mrs. Smith remembers he used to complain of his back and knees. He doesn t complain now, and he doesn t take any pills.
5 Pain in Patients with Dementia Patients with dementia often cannot express pain; they just feel distressed and may show this by hitting, refusing ADL assistance, stopping eating If we don t figure out they have pain and treat it appropriately, their distress will simply worsen
6 Upon Admission (or before the patient has dementia) Do a thorough pain history Back pain? Arthritis? Headaches? Neuropathy? Find out what works for their pain Tylenol is best for older patients Ibuprofen (caution in older adults- but safer than narcotics!) Gabapentin or other nerve choices
7 If new distress and no clear reason for possible pain, do a careful exam Ears Mouth- sores? Illfitting dentures? Broken tooth? Arms and legs (a facility missed a broken arm!) Feet and hands Urinary retention? Constipation? UTI?
8 Common Sources of Pain Degenerative joint disease Spinal stenosis Fractures Pressure ulcers Urinary retention Constipation Peripheral vascular disease Post-stroke syndrome Improper positioning Fibromyalgia Cancer Contractures Postherpetic neuralgia Dental problems Shega et al, 2007
9 Checklist of Nonverbal Pain Vocalization Grimace Bracing Rubbing Restlessness/ agitation
10 Pain Assessment in Advanced Dementia Scale Items Score Breathing independent of vocalization Negative vocalization Facial expression Body Language Normal None Smiling or inexpressive Relaxed Occasional labored breathing, brief hyperventilation Occasional moan or groan. Low level negative speech Sad, frightened, frowning Tense, distressed, pacing, fidgeting Consolability No need Reassured by voice or touch Total score Noisy, labored breathing, long hyperventilation, Cheyne-stokes Repeated troubled calling out. Loud moan/ groan. Crying Facial grimace Rigid. Fists clenched, knees pulled up, pulling pushing away, striking out Unable to console, distract, or reassure
11 If you think your patient s Try to fix it! behavior is due to pain Treat ear infection or UTI Manage constipation or urinary retention Ask the dentist to fit a new denture, bridge, etc Try non-pharmacologic strategies Up and moving/ frequent position changes Heating pad (hot water bottle) 20 min TID Gentle massage
12 If you think your patient s behavior is due to pain Acetaminophen (Tylenol) 650 mg TID SCHEDULED Increase to 1000 mg TID scheduled if they seem a little better but still room for improvement If you notice that their pain seems to be in one location (neck, back, knees) consider: Diclofenac gel (if kidney function OK) Lidoderm patch
13 If you think your patients behavior is due to pain What about NSAIDs? (Ibuprofen, Aleve, etc) NOT as safe as tylenol Stomach, kidney, heart (BP) are main concerns SAFER than narcotics Fewer fractures LESS acute kidney injury! LESS hospitalizations and deaths!» Solomon, Arch Intern Med. 2010;170(22):
14 What about NSAIDS? If your patient is not in kidney failure (egfr>30 or >45 to be extra safe), doesn t have uncontrolled CHF or HTN, and hasn t had a GI bleed, may consider an NSAID Naproxen (Aleve) 250 BID scheduled Ibuprofen (Advil, Motrin) 400 TID scheduled Check kidney function after a week or two, monitor blood pressure and edema (salt restriction usually prevents edema with NSAID use)
15 What if these aren t good enough? Fairly good evidence that pain is the issue (known spinal stenosis, arthritis, etc) Other strategies haven t fully worked Patient clearly suffering/distressed Now is the time to try low dose opioids Observe patient for times when most distressed and schedule drugs for those times (for example, 1 hr prior to ADLs or PT) If distress is around the clock, schedule drugs to cover
16 Using Opioids Start low, increase gradually Avoid morphine if poor kidney function Completely avoid methadone and tramadol Monitor closely the first few doses- dizzy, confused, etc Check kidney function after a week or so Recheck pain scales, behaviors frequently to see if it helped- DISCONTINUE the drug if your patient does not show improvement in distress
17 Using Opioids- Always SCHEDULE in dementia patients What to start with Vicodin 5/350 ½-1 tab daily- TID (watch total tylenol dosage) Oxycodone 2.5 mg once daily- QID How quickly should I increase the dose? I usually wait at least a week to do dose adjustments What if my patient has acute severe pain? Dilaudid 1-2 mg q4-6 hrs, fentanyl patch (12.5 mg)
18 Back to Mr. Smith Hitting out when care team attempts to assist with ADLs History of back and knee pain What would you like to do?
19 Back to Mr. Smith Hitting out when care team attempts to assist with ADLs History of back and knee pain What would you like to do? Daily activity, frequent position changes Heating pad TID Scheduled tylenol 650 mg TID, increase to 1000 TID if needed Diclofenac gel before ADLs and activity (up to QID)
20 Back to Mr. Smith Hitting out when care team attempts to assist with ADLs History of back and knee pain If first steps don t solve the problem, what next?
21 Back to Mr. Smith Hitting out when care team attempts to assist with ADLs History of back and knee pain If first steps don t solve the problem, what next? Try NSAID- aleve 250 mg BID in addition to tylenol or instead of tylenol (depending on whether you noticed any tylenol effectiveness)
22 Back to Mr. Smith Hitting out when care team attempts to assist with ADLs History of back and knee pain If still no response, what you would like to do?
23 Back to Mr. Smith Hitting out when care team attempts to assist with ADLs History of back and knee pain If still no response, what would you like to do? Vicodin ½ tab before ADLs or BID scheduled OR Oxycodone 2.5 mg TID

24
25 Mr. Jones, age 87, has dementia and is anxious and withdrawn after a hospitalization Fred s issues Probable Alzheimer s Donepezil Fred s Meds CHF/CAD Osteoarthritis Insomnia Type 2 Diabetes BPH CRF- egfr 28 HCTZ, digoxin.25 mcg daily, metoprolol, lisinopril, ASA, simvastatin Acetaminophen, tramadol Zolpidem Metformin, glyburide Tamsulosin
26 Think about Kidney Clearance- Calculate via Cockcroft Gault Renal Clearance (ml/min) Meds to Discontinue/Adjust Dose GFR < 60 (CKD 3) GFR < (CKD 3) Dabigatran Metformin Morphine (watch for toxicity) Colchicine (dose adjust) NSAIDs GFR < 30 (CKD 4-5) Bisphosphonates HCTZ Tramadol (q 12 h, 200 mg/d max) Allopurinol ( mg/d max) Memantine
27 And Mr. Jones got discharged on Cipro for a UTI Drug Dose Considerations Ciprofloxacin 250 mg bid, 5 to 7 days Check INR Watch for delirium TMP/SMZ Nitrofurantoin (Macrobid) 80/400 mg bid, 5 to 7 days 100 mg bid, 5 to 7 days Watch kidney function; 50% if GFR < 30 Check INR; K Now considered OK if GFR < 60
28 Mr. Jones Meds Condition Alzheimer s Disease Medical Treatment Donepezil CHF/CAD Osteoarthritis Insomnia Type 2 Diabetes BPH HCTZ, Digoxin.25 mcg daily, metoprolol,, lisinopril, ASA,, simvastatin Acetaminophen,, tramadol Zolpidem Metformin, glyburide, finger sticks Tamsulosin
29 Drugs most likely to cause delirium Anticholinergics (e.g., diphenhydramine), TCAs (e.g., amitriptyline, imipramine), antipsychotics Anti-inflammatory agents, including prednisone Benzodiazepines or alcohol acute toxicity or withdrawal Cardiovascular (e.g., digitalis, antihypertensives) Diuretics Histamine blockers (e.g., cimetidine, ranitidine) Lithium Opioid analgesics Medication/Substance Withdrawal syndromes Clozapine, Paxil, alcohol are biggest offenders
30 Anticholinergic properties frequently overlooked: Elavil (amitriptyline) Cogentin (benztropine) Bentyl (dicyclomine) Ditropan (oxybutynin) Detrol (tolterodine) Benadryl (diphenhydramine) Zyprexa (olanzapine) Levsin (hyoscyamine) Flexeril (cyclobenzaprine) Atarax/Vistaril(hydroxyzine) Welbutrin/Zyban (bupropion) Antivert (meclizine) Ipratropium (atrovent) Phenergan (promethazine) Atropine Quinidine
31 What should you use instead? Nausea- suggestive evidence that ondansetron is better Sleep- No drugs are truly safe in older people Back rub, warm milk, relaxing music Rozerem may help sleep/wake cycle Trazodone mildly anticholinergic, try mg Pain- already covered GI prophylaxis: ONLY PPIs (shorted course possible) Sertraline or citalopram
32 Mr. Jones Meds Condition Alzheimer s Disease CHF/CAD Osteoarthritis Insomnia Type 2 Diabetes BPH Medical Treatment Donepezil-dose reduced metoprolol,, lisinopril, (stopped ASA,, simvastatin, HCTZ, Digoxin.25 mcg) Acetaminophen,,stopped tramadol Stopped Zolpidem Stopped Metformin, glyburide, finger sticks Stopped Tamsulosin
33 Mrs. Black is insistent Mrs. Black is 89 and has had dementia for about 10 years. Her husband continues to care for her at home, but lately has become increasingly concerned about her. She has been demanding her mother, and bursts into tears when Mr. Black tells her that her mother is dead. She has been refusing to eat, and is starting to wander at night. What do you think is going on?

34 Prevalence of Major Depressive Disorder in Alzheimer Disease Zubenko GS et al. Am J Psych 2003; 160: High prevalence rates with increasing prevalence in more severe AD.
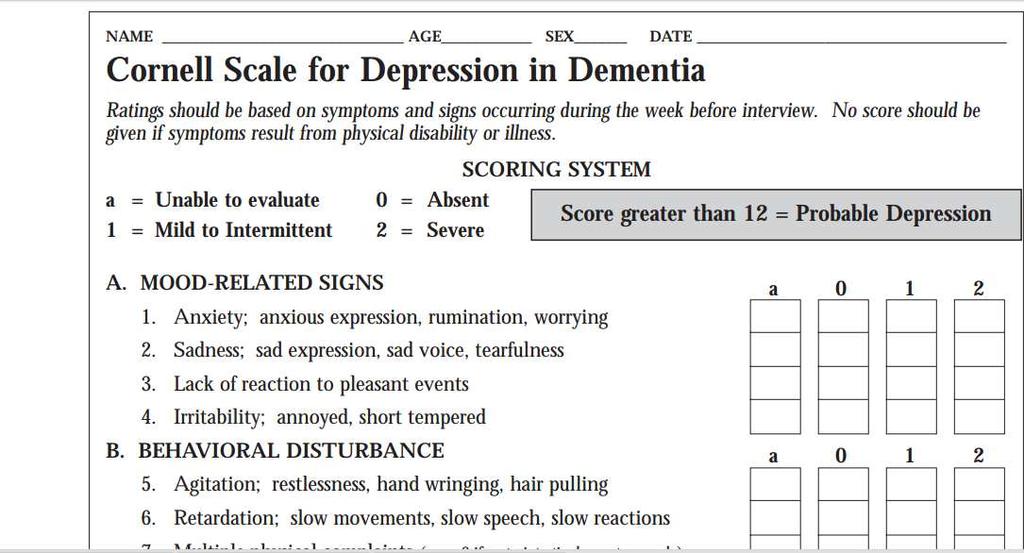
35 Depression Are there other symptoms of depression? Depressive symptoms are more common than major depression Apathy is very common Anxiety, guilt, hopelessness and suicidality can help differentiate from apathy Consider using the GDS Cornell Scale for Depression in Dementia
36
37 Depression in Dementia A number of negative trials recently- suggesting a 3 month trial of non-drug interventions and reassess Most of us who are seeing these patients and note a CHANGE in symptoms affecting quality of life and caregiver stress will initiate an SSRI Sertraline, start at 25 mg, titrate q2 weeks to 100 mg if needed Citalopram, start at 10 mg, titrate in 2 weeks to 20 mg if needed
38 Which symptoms respond best to medications? Responsive to Meds Anxiety Irritability/anger Delusions Hallucinations Insomnia Agitation/aggression Hyperactivity Dysphoria Apathy Less responsive to Meds Perseverative yelling Pacing Exit seeking Wandering Disrobing Sexual impulsivity
39 A Note on Medication SSRI s are going to require a trial of at least 2 weeks or longer Antipsychotics, trazodone should see response in a few days If your patient seems to be depressed, but is having acute distress, you may need a BRIEF course of a more rapidly acting medication to help relieve distress while the SSRI is kicking in
40 Symptomatic Approach Analgesic: restless calling out grimacing combative Mood Stabilizer impulsivity hyperactivity physical aggression irritability agitation or verbal aggression Antipsychotic Antidepressant delusions hallucinations anxiety dysphoria AChI: apathy hallucinations misperceptions confusion inattention
41 Summary When a patient with dementia is agitated, think about pain, drug side effects/ interactions, and depression as likely reasons for the agitation. NONE of these patients (or others like them) should receive antipsychotics Treating underlying etiologies is much more effective than treating symptoms with an antipsychotic!

42 Questions?
UCSF PAIN SUMMIT /8/15
 UCSF PAIN SUMMIT 2015 5/8/15 Case 3 Geriatric Pain Disclosure Statements UCSF PAIN SUMMIT 2015 Wendy Anderson Patrice Villars 5/8/15 Case 3 Geriatric Pain Pain Management in the Geriatric & End-of-Life
UCSF PAIN SUMMIT 2015 5/8/15 Case 3 Geriatric Pain Disclosure Statements UCSF PAIN SUMMIT 2015 Wendy Anderson Patrice Villars 5/8/15 Case 3 Geriatric Pain Pain Management in the Geriatric & End-of-Life
PAIN AND DEMENTIA: Recognition, Assessment and Management of Pain in Patients with Late-Life Dementia
 PAIN AND DEMENTIA: Recognition, Assessment and Management of Pain in Patients with Late-Life Dementia TOLU TAIWO PRESENTED AT PHC IGSI WORKSHOP #3 LACOMBE MEMORIAL CENTRE, LACOMBE MAY 25, 2018. Presenter
PAIN AND DEMENTIA: Recognition, Assessment and Management of Pain in Patients with Late-Life Dementia TOLU TAIWO PRESENTED AT PHC IGSI WORKSHOP #3 LACOMBE MEMORIAL CENTRE, LACOMBE MAY 25, 2018. Presenter
LUNCH WITH THE EXPERTS: Palliative Care for Advanced Dementia with Pain and Dementia
 LUNCH WITH THE EXPERTS: Palliative Care for Advanced Dementia with Pain and Dementia Carol Long, PhD, RN, FPCN Principal, Capstone Healthcare & Co-Director, Palliative Care for Advanced Dementia, Beatitudes
LUNCH WITH THE EXPERTS: Palliative Care for Advanced Dementia with Pain and Dementia Carol Long, PhD, RN, FPCN Principal, Capstone Healthcare & Co-Director, Palliative Care for Advanced Dementia, Beatitudes
Obstacles to appropriate and timely pain relief in the Emergency Department for people with cognitive impairment
 Obstacles to appropriate and timely pain relief in the Emergency Department for people with cognitive impairment Lynn Chenoweth Professor, Centre for Healthy Brain Ageing University of New South Wales,
Obstacles to appropriate and timely pain relief in the Emergency Department for people with cognitive impairment Lynn Chenoweth Professor, Centre for Healthy Brain Ageing University of New South Wales,
Resource: Pain Assessments
 Pain assessment is an integral part of patient care. The patient s pain should be assessed at each visit using consistent assessment tools based on the patient s ability to communicate. For all pain scales
Pain assessment is an integral part of patient care. The patient s pain should be assessed at each visit using consistent assessment tools based on the patient s ability to communicate. For all pain scales
OBJECTIVES 5NW GERIATRICS UNIT. nicheprogram.org 2016 Annual NICHE Conference Care Across the Continuum 1
 Family Education for Nonverbal Patient Pain Control Jeannette (Jeannie) Meyer, MSN, RN, CCRN CCNS, PCCN, ACHPN Clinical Nurse Specialist Palliative Care Santa Monica UCLA Medical Center Anila Ladak, RN,
Family Education for Nonverbal Patient Pain Control Jeannette (Jeannie) Meyer, MSN, RN, CCRN CCNS, PCCN, ACHPN Clinical Nurse Specialist Palliative Care Santa Monica UCLA Medical Center Anila Ladak, RN,
RMC Procedure/Guideline: P10395
 RMC Procedure/Guideline: P10395 Pain Management Department: Nursing Administration Last Review/Revision Date: 7-1-2018 Distribution Departments: 7240, 7505, 7575 Accreditation/Regulatory Standard (if applicable):
RMC Procedure/Guideline: P10395 Pain Management Department: Nursing Administration Last Review/Revision Date: 7-1-2018 Distribution Departments: 7240, 7505, 7575 Accreditation/Regulatory Standard (if applicable):
Geriatric Pain Assessment and Management. Robin Arends, DNP, CNP, FNP-BC
 + Geriatric Pain Assessment and Management Robin Arends, DNP, CNP, FNP-BC + Objectives List three reasons why elderly are less likely to report pain. List three barriers to pain management Describe two
+ Geriatric Pain Assessment and Management Robin Arends, DNP, CNP, FNP-BC + Objectives List three reasons why elderly are less likely to report pain. List three barriers to pain management Describe two
Part IV: Nursing Assistant Roles in Observing and Relieving Pain
 Part IV: Nursing Assistant Roles in Observing and Relieving Pain Objectives: Describe the roles of the NA in EOL care and pain management Define pain Describe acute and chronic pain Describe some common
Part IV: Nursing Assistant Roles in Observing and Relieving Pain Objectives: Describe the roles of the NA in EOL care and pain management Define pain Describe acute and chronic pain Describe some common
Part IV: Nursing assistant roles in observing and relieving pain. Nursing Assistant Roles in Endof-life. Nursing Assistant Roles in Pain Management
 Part IV: Nursing assistant roles in observing and relieving pain Objectives: Describe the roles of the NA in EOL care and pain management Define pain Describe acute and chronic pain Describe some common
Part IV: Nursing assistant roles in observing and relieving pain Objectives: Describe the roles of the NA in EOL care and pain management Define pain Describe acute and chronic pain Describe some common
Faces Pain Scale Hurts just. Hurts a little more. Hurts even Hurts a a little bit
 Faces Pain Scale 0 2 4 6 8 10 Hurts just Hurts even Hurts a a little bit more whole lot Very happy, no hurt Hurts a little more Hurts as much as you can imagine (don t have to be crying to feel this much
Faces Pain Scale 0 2 4 6 8 10 Hurts just Hurts even Hurts a a little bit more whole lot Very happy, no hurt Hurts a little more Hurts as much as you can imagine (don t have to be crying to feel this much
ten questions you might have about tapering (and room for your own) an informational booklet for opioid pain treatment
 an informational booklet for opioid pain treatment") ten questions you might have about tapering (and room for your own) an informational booklet for opioid pain treatment This booklet was created to help you learn about tapering. You probably have lots
ten questions you might have about tapering (and room for your own) an informational booklet for opioid pain treatment This booklet was created to help you learn about tapering. You probably have lots
GERIATRICS 101. Victoria L. Braund, MD, FACP, CMD. Director, Division of Geriatrics, NorthShore Medical Director, Symphony of Evanston
 GERIATRICS 101 Victoria L. Braund, MD, FACP, CMD Director, Division of Geriatrics, NorthShore Medical Director, Symphony of Evanston LET S REVIEW Medicare Hospice Pain mgmt. Bowel business Delirium Sleep
GERIATRICS 101 Victoria L. Braund, MD, FACP, CMD Director, Division of Geriatrics, NorthShore Medical Director, Symphony of Evanston LET S REVIEW Medicare Hospice Pain mgmt. Bowel business Delirium Sleep
Management of the Behavioral and Psychological Symptoms of Dementia (BPSD)
") Management of the Behavioral and Psychological Symptoms of Dementia (BPSD) Soheyla Mahdavian, PharmD, BCGP, TTS Associate Professor of Pharmacy Practice Florida A&M University College of Pharmacy and Pharmaceutical
Management of the Behavioral and Psychological Symptoms of Dementia (BPSD) Soheyla Mahdavian, PharmD, BCGP, TTS Associate Professor of Pharmacy Practice Florida A&M University College of Pharmacy and Pharmaceutical
Pain Assessment & Management. For General Nursing Orientation
 Pain Assessment & Management For General Nursing Orientation April 2012 Overview Definition of pain Barriers to effective pain management Types of pain Objective pain assessment Approaches to management
Pain Assessment & Management For General Nursing Orientation April 2012 Overview Definition of pain Barriers to effective pain management Types of pain Objective pain assessment Approaches to management
Foundations of Safe and Effective Pain Management
 Foundations of Safe and Effective Pain Management Evidence-based Education for Nurses, 2018 Module 1: The Multi-dimensional Nature of Pain Module 2: Pain Assessment and Documentation Module 3: Management
Foundations of Safe and Effective Pain Management Evidence-based Education for Nurses, 2018 Module 1: The Multi-dimensional Nature of Pain Module 2: Pain Assessment and Documentation Module 3: Management
A PATIENT GUIDE FOR MANAGING PAIN
 A PATIENT GUIDE FOR MANAGING PAIN PAIN MANAGEMENT Knowing the Facts Pain can be controlled. Pain is common after surgery and with many types of illnesses. Most patients with acute and chronic pain can
A PATIENT GUIDE FOR MANAGING PAIN PAIN MANAGEMENT Knowing the Facts Pain can be controlled. Pain is common after surgery and with many types of illnesses. Most patients with acute and chronic pain can
HOW WOULD I KNOW? WHAT CAN I DO?
 HOW WOULD I KNOW? WHAT CAN I DO? How to help someone with dementia who is in pain or distress Help! 1 Unusual behaviour may be a sign of pain or distress If you are giving care or support to somebody with
HOW WOULD I KNOW? WHAT CAN I DO? How to help someone with dementia who is in pain or distress Help! 1 Unusual behaviour may be a sign of pain or distress If you are giving care or support to somebody with
MILD PAIN Pain Scale Ratin g 1/5 ( 0-5 Scale ) or 1-3/10 ( 0-10 Scale)
 or 1-3/10 ( 0-10 Scale)") MILD PAIN Pain Scale Ratin g 1/5 ( 0-5 Scale ) or 1-3/10 ( 0-10 Scale) Complete Pain Assessment. Establish probable cause of pain when possible. Determine goal for pain relief with patient and acceptable
MILD PAIN Pain Scale Ratin g 1/5 ( 0-5 Scale ) or 1-3/10 ( 0-10 Scale) Complete Pain Assessment. Establish probable cause of pain when possible. Determine goal for pain relief with patient and acceptable
BEHAVIORAL PROBLEMS IN DEMENTIA
 BEHAVIORAL PROBLEMS IN DEMENTIA CLINICAL FEATURES Particularly as dementia progresses, psychiatric symptoms may develop that resemble discrete mental disorders such as depression or mania The course and
BEHAVIORAL PROBLEMS IN DEMENTIA CLINICAL FEATURES Particularly as dementia progresses, psychiatric symptoms may develop that resemble discrete mental disorders such as depression or mania The course and
Improving Health, Enriching Life. Pain Management. Altru HEALTH SYSTEM
 Improving Health, Enriching Life altru.org Pain Management Altru HEALTH SYSTEM There are many different causes and kinds of pain. Pain can be caused by injury, illness, sickness, disease or surgery. Treating
Improving Health, Enriching Life altru.org Pain Management Altru HEALTH SYSTEM There are many different causes and kinds of pain. Pain can be caused by injury, illness, sickness, disease or surgery. Treating
Every 67seconds, someone will develop Alzheimer's.
 We all need a purpose and responsibilities to live a healthy life. Dementia Care 101 Corrin Campbell BS, COTA/L & Michael Urban, MS, OTR/L, MBA Every 67seconds, someone will develop Alzheimer's. http://www.alz.org
We all need a purpose and responsibilities to live a healthy life. Dementia Care 101 Corrin Campbell BS, COTA/L & Michael Urban, MS, OTR/L, MBA Every 67seconds, someone will develop Alzheimer's. http://www.alz.org
Management of Behavioral Problems in Dementia
 Management of Behavioral Problems in Dementia Ghulam M. Surti, MD Clinical Assistant Professor Department of Psychiatry and Human Behavior Warren Alpert Medical School of Brown University Definition of
Management of Behavioral Problems in Dementia Ghulam M. Surti, MD Clinical Assistant Professor Department of Psychiatry and Human Behavior Warren Alpert Medical School of Brown University Definition of
Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist
 and Glutamate (NMDA) Receptor Antagonist") Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist Medication Dosage Indication for Use Aricept (donepezil) Exelon (rivastigmine) 5mg 23mg* ODT 5mg Solution
Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist Medication Dosage Indication for Use Aricept (donepezil) Exelon (rivastigmine) 5mg 23mg* ODT 5mg Solution
Understanding the impact of pain and dementia
 Understanding the impact of pain and dementia Knowing how to identify and manage the symptoms of pain in people living with dementia is an important part of a carer s role. This guide provides an overview
Understanding the impact of pain and dementia Knowing how to identify and manage the symptoms of pain in people living with dementia is an important part of a carer s role. This guide provides an overview
Cognitive enhancers PINCH ME. Anticholinergic burden BPSD. Agitation, Aggression and antipsychotics
 Cognitive enhancers PINCH ME Anticholinergic burden BPSD Agitation, Aggression and antipsychotics 2 types Cholinesterase inhibitors licensed for mild to moderate AD Donepezil Galantamine Rivastigmine also
Cognitive enhancers PINCH ME Anticholinergic burden BPSD Agitation, Aggression and antipsychotics 2 types Cholinesterase inhibitors licensed for mild to moderate AD Donepezil Galantamine Rivastigmine also
Symptom Management in the Non-Verbal Patient at the End of Life Laura Carmon, ANP-BC
 Symptom Management in the Non-Verbal Patient at the End of Life Laura Carmon, ANP-BC 2017 NPSS Asheville, NC Objectives The learner will recognize non-verbal signs and symptoms commonly seen at the EOL.
Symptom Management in the Non-Verbal Patient at the End of Life Laura Carmon, ANP-BC 2017 NPSS Asheville, NC Objectives The learner will recognize non-verbal signs and symptoms commonly seen at the EOL.
pain and dementia Some people with pain give no signs of it.
 Pain& Dementia pain and dementia Pain affects each of us differently. Some people have pain and we would never know. Some people with pain give no signs of it. Others, however, wear facial expressions
Pain& Dementia pain and dementia Pain affects each of us differently. Some people have pain and we would never know. Some people with pain give no signs of it. Others, however, wear facial expressions
BACKGROUND Measuring renal function :
 A GUIDE TO USE OF COMMON PALLIATIVE CARE DRUGS IN RENAL IMPAIRMENT These guidelines bring together information and recommendations from the Palliative Care formulary (PCF5 ) BACKGROUND Measuring renal
A GUIDE TO USE OF COMMON PALLIATIVE CARE DRUGS IN RENAL IMPAIRMENT These guidelines bring together information and recommendations from the Palliative Care formulary (PCF5 ) BACKGROUND Measuring renal
Chitra Fernando, MD March 18, 2008
 Chitra Fernando, MD March 18, 2008 Definition Statistics Risk factors Why older adults are more prone to ADE Manifestations Inappropriate medications for older adults What can be done to minimize adverse
Chitra Fernando, MD March 18, 2008 Definition Statistics Risk factors Why older adults are more prone to ADE Manifestations Inappropriate medications for older adults What can be done to minimize adverse
2/12/2016. Drugs and Dementia in the Hospice Patient. Jim Joyner, Pharm.D., C.G.P. Director of Clinical Operations Outcome Resources
 Drugs and Dementia in the Hospice Patient Jim Joyner, Pharm.D., C.G.P. Director of Clinical Operations Outcome Resources 1 Drug Therapy: Targeted at Symptoms Cognitive: Impaired abstract thinking Impaired
Drugs and Dementia in the Hospice Patient Jim Joyner, Pharm.D., C.G.P. Director of Clinical Operations Outcome Resources 1 Drug Therapy: Targeted at Symptoms Cognitive: Impaired abstract thinking Impaired
Dementia and Fall Geriatric Interprofessional Training. Wael Hamade, MD, FAAFP
 Dementia and Fall Geriatric Interprofessional Training Wael Hamade, MD, FAAFP Prevalence of Dementia Age range 65-74 5% % affected 75-84 15-25% 85 and older 36-50% 5.4 Million American have AD Dementia
Dementia and Fall Geriatric Interprofessional Training Wael Hamade, MD, FAAFP Prevalence of Dementia Age range 65-74 5% % affected 75-84 15-25% 85 and older 36-50% 5.4 Million American have AD Dementia
1/21/2016 UPDATE ON THE AMERICAN GERIATRICS SOCIETY 2015 BEERS CRITERIA DISCLOSURE OBJECTIVES AGING GOALS BEERS CRITERIA
 UPDATE ON THE AMERICAN GERIATRICS SOCIETY 2015 BEERS CRITERIA DISCLOSURE I have no financial conflict of interest to disclose. Lacey Charbonneau, Pharm.D. PGY-1 Community Practice Resident Baptist Medical
UPDATE ON THE AMERICAN GERIATRICS SOCIETY 2015 BEERS CRITERIA DISCLOSURE I have no financial conflict of interest to disclose. Lacey Charbonneau, Pharm.D. PGY-1 Community Practice Resident Baptist Medical
Geriatric Pharmacology. Kwi Bulow, M.D. Clinical Professor of Medicine Director, Academic Geriatric Resource Center
 Geriatric Pharmacology Kwi Bulow, M.D. Clinical Professor of Medicine Director, Academic Geriatric Resource Center Silver Tsunami 2010: 40 million (13%) 2030: 72 million (20%) Baby Boomers (1946-1964)
Geriatric Pharmacology Kwi Bulow, M.D. Clinical Professor of Medicine Director, Academic Geriatric Resource Center Silver Tsunami 2010: 40 million (13%) 2030: 72 million (20%) Baby Boomers (1946-1964)
Pain In Primary Care. Dr. Chris Frank Dr. John Puxty Deanna Abbott-McNeil, GiiC Consultant Susanne Murphy, GiiC Consultant
 Pain In Primary Care Dr. Chris Frank Dr. John Puxty Deanna Abbott-McNeil, GiiC Consultant Susanne Murphy, GiiC Consultant Outline è Definition of pain è Prevalence and significance è Causes è Assessment
Pain In Primary Care Dr. Chris Frank Dr. John Puxty Deanna Abbott-McNeil, GiiC Consultant Susanne Murphy, GiiC Consultant Outline è Definition of pain è Prevalence and significance è Causes è Assessment
A Geriatrician s Perspective on Successful Aging. Ariel Green, MD, MPH Assistant Professor of Medicine
 A Geriatrician s Perspective on Successful Aging Ariel Green, MD, MPH Assistant Professor of Medicine 1 Disclosures Johns Hopkins Clinical Research Scholars Program American College of Cardiology Foundation
A Geriatrician s Perspective on Successful Aging Ariel Green, MD, MPH Assistant Professor of Medicine 1 Disclosures Johns Hopkins Clinical Research Scholars Program American College of Cardiology Foundation
APPENDIX E: HEALTHCARE PRACTITIONER- REPORTED REDUCTION OF PAIN MEDICATION
 Contents Appendix E: Healthcare Practitioner-Reported Reduction of Pain Medication... E-1 Appendix E: Healthcare Practitioner- Reported Reduction of Pain Medication Note: Word choice and spellings have
Contents Appendix E: Healthcare Practitioner-Reported Reduction of Pain Medication... E-1 Appendix E: Healthcare Practitioner- Reported Reduction of Pain Medication Note: Word choice and spellings have
Have You Ever Wondered
 Have You Ever Wondered A few facts about medication use and related falls The Number of Medications You Take & The Connection to Falls CONCERN: As you increase the number of medications that you take,
Have You Ever Wondered A few facts about medication use and related falls The Number of Medications You Take & The Connection to Falls CONCERN: As you increase the number of medications that you take,
Tips for Pain Management
 Tips for Pain Management Going for the 3 Increases: Increase in Health, Increase in Happiness & Increase in Energy Strategies for Success in Health Management By: James J. Messina, Ph.D. What are the medical
Tips for Pain Management Going for the 3 Increases: Increase in Health, Increase in Happiness & Increase in Energy Strategies for Success in Health Management By: James J. Messina, Ph.D. What are the medical
INFORMATION FOR PATIENTS. Let s Manage Pain
 INFORMATION FOR PATIENTS Let s Manage Pain 1 About this booklet Persistent pain, also called chronic pain, is pain which continues for longer than expected. Pain can affect all areas of your life. People
INFORMATION FOR PATIENTS Let s Manage Pain 1 About this booklet Persistent pain, also called chronic pain, is pain which continues for longer than expected. Pain can affect all areas of your life. People
Fall Prevention in Hospice (A pharmacologic and nonpharmacologic approach)
") Fall Prevention in Hospice (A pharmacologic and nonpharmacologic approach) Chinenye Emereole, Pharm.D. Clinical Pharmacist Hospice Pharmacy Solutions Objectives Assess and identify hospice patients who
Fall Prevention in Hospice (A pharmacologic and nonpharmacologic approach) Chinenye Emereole, Pharm.D. Clinical Pharmacist Hospice Pharmacy Solutions Objectives Assess and identify hospice patients who
BLCS 1-Clinical Overview. Dr. Chris Rauscher Clinical Lead Shared Care Polypharmacy Risk Reduction Initiative
 BLCS 1-Clinical Overview Dr. Chris Rauscher Clinical Lead Shared Care Polypharmacy Risk Reduction Initiative Fraser Health Guide To Person-Centered Medication Decisions Factors to Consider When Systematically
BLCS 1-Clinical Overview Dr. Chris Rauscher Clinical Lead Shared Care Polypharmacy Risk Reduction Initiative Fraser Health Guide To Person-Centered Medication Decisions Factors to Consider When Systematically
County Alameda Public Health Department Emergency Medical Services Division. Trial Study The Prehospital Use of Fentanyl.
 County Alameda Public Health Department Emergency Medical Services Division Trial Study The Prehospital Use of Fentanyl 18 Month Report March 24, 2009 TABLE OF CONTENTS Introduction... 1 Methods... 2 Data
County Alameda Public Health Department Emergency Medical Services Division Trial Study The Prehospital Use of Fentanyl 18 Month Report March 24, 2009 TABLE OF CONTENTS Introduction... 1 Methods... 2 Data
Treatments for Alzheimer s Disease A Quick Guide for Patients and Caregivers
 Treatments for Alzheimer s Disease A Quick Guide for Patients and Caregivers By Kelsey F. Lee, PharmD candidate 2011 Preceptor: Demetra Antimisiaris, PharmD University of Louisvlle Dept. Family Medicine
Treatments for Alzheimer s Disease A Quick Guide for Patients and Caregivers By Kelsey F. Lee, PharmD candidate 2011 Preceptor: Demetra Antimisiaris, PharmD University of Louisvlle Dept. Family Medicine
PAIN. TREATMENT TABLES Analgesics. NON-OPIOID ANALGESICS Generic Name Trade Names (Examples) Duration Initial Dose
 Duration Initial Dose") NON-OPIOID SHORT-ACTING LONG-ACTING **** O PAIN TREATMENT TABLES Analgesics NON-OPIOID ANALGESICS Generic Name Trade Names (Examples) Duration Initial Dose Tramadol 50 mg Ultram Every 4 hours 1-2 tabs,
NON-OPIOID SHORT-ACTING LONG-ACTING **** O PAIN TREATMENT TABLES Analgesics NON-OPIOID ANALGESICS Generic Name Trade Names (Examples) Duration Initial Dose Tramadol 50 mg Ultram Every 4 hours 1-2 tabs,
Pain and Ways to Manage It
 Pain and Ways to Manage It FM.850.M311.PHC (R.Jul-15) 1 Contents This page intentionally left blank. What the words mean............................. 2 Why is it important to manage your pain?............
Pain and Ways to Manage It FM.850.M311.PHC (R.Jul-15) 1 Contents This page intentionally left blank. What the words mean............................. 2 Why is it important to manage your pain?............
System Patient Care Services
 North Shore-LIJ Health System is now Northwell Health System Patient Care Services POLICY TITLE: Pain Management: Assessment and Reassessment POLICY #: PCS.1603 System Approval Date: 10/20/16 CLINICAL
North Shore-LIJ Health System is now Northwell Health System Patient Care Services POLICY TITLE: Pain Management: Assessment and Reassessment POLICY #: PCS.1603 System Approval Date: 10/20/16 CLINICAL
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE
 Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
Mental Health Issues in Nursing Homes. I m glad you asked.
 Mental Health Issues in Nursing Homes I m glad you asked. I m glad you asked Susan Wehry, M.D. Associate Professor of Psychiatry, College of Medicine, University of Vermont Consultant, State of Vermont
Mental Health Issues in Nursing Homes I m glad you asked. I m glad you asked Susan Wehry, M.D. Associate Professor of Psychiatry, College of Medicine, University of Vermont Consultant, State of Vermont
Delirium, Depression and Dementia
 Delirium, Depression and Dementia Martha Watson, MS, APRN, GCNS Some material included in this presentation is adapted from: NICHE (2009). Geriatric Resource Nurse Core Curriculum [Power Point presentation].
Delirium, Depression and Dementia Martha Watson, MS, APRN, GCNS Some material included in this presentation is adapted from: NICHE (2009). Geriatric Resource Nurse Core Curriculum [Power Point presentation].
PRESCRIBING IN THE ELDERLY. CARE HOME PHARMACY TEAM Bhavini Shah, Eleesha Pentiah & Puja Vyas
 PRESCRIBING IN THE ELDERLY CARE HOME PHARMACY TEAM Bhavini Shah, Eleesha Pentiah & Puja Vyas LEARNING OUTCOMES Medicines Optimisation The effects of aging on health and medicines. Polypharmacy Acute Kidney
PRESCRIBING IN THE ELDERLY CARE HOME PHARMACY TEAM Bhavini Shah, Eleesha Pentiah & Puja Vyas LEARNING OUTCOMES Medicines Optimisation The effects of aging on health and medicines. Polypharmacy Acute Kidney
Managing Pain in the Elderly
 Managing Pain in the Elderly MILES BELGRADE, MD COMPREHENSIVE PAIN CENTER MINNEAPOLIS VA The Pain Deck is Stacked Against the Elderly Osteoporosis Fractures 1 Zoster & PHN Trigeminal Neuralgia Verne 81-year-old
Managing Pain in the Elderly MILES BELGRADE, MD COMPREHENSIVE PAIN CENTER MINNEAPOLIS VA The Pain Deck is Stacked Against the Elderly Osteoporosis Fractures 1 Zoster & PHN Trigeminal Neuralgia Verne 81-year-old
Medication Use in Older Adults
 Medication Use in Older Adults F. Michael Gloth, III, MD, AGSF, FACP, CMD Clinical Professor Department of Geriatrics, Florida State University College of Medicine Associate Professor of Medicine Division
Medication Use in Older Adults F. Michael Gloth, III, MD, AGSF, FACP, CMD Clinical Professor Department of Geriatrics, Florida State University College of Medicine Associate Professor of Medicine Division
Palliative Care. And Pain Management
 Palliative Care And Pain Management Revised: bw/september 2010 Palliative Care Symptom management is a primary goal of palliative care. Pain is one of the most feared symptoms experienced by patients.
Palliative Care And Pain Management Revised: bw/september 2010 Palliative Care Symptom management is a primary goal of palliative care. Pain is one of the most feared symptoms experienced by patients.
Residents Who Don t Sleep
 Residents Who Don t Sleep Case study........................................... An 86 yr. old woman has diagnoses of Alzheimer s disease, congestive heart failure, constipation, depression, hypertension
Residents Who Don t Sleep Case study........................................... An 86 yr. old woman has diagnoses of Alzheimer s disease, congestive heart failure, constipation, depression, hypertension
Dementia. T. Caprio Pain & Dementia October Pain Assessment and Management with Dementia. NPA Conference 1. Mild Cognitive Impairment
 Pain Assessment and Management with Dementia Thomas Caprio, MD, MPH, MSHPE, CMD, HMDC, FACP, AGSF, FAAHPM Associate Professor of Medicine, Dentistry, Nursing, & Public Health Sciences Director, Finger
Pain Assessment and Management with Dementia Thomas Caprio, MD, MPH, MSHPE, CMD, HMDC, FACP, AGSF, FAAHPM Associate Professor of Medicine, Dentistry, Nursing, & Public Health Sciences Director, Finger
PAIN MANAGEMENT Help me HELP ME!!
 PAIN MANAGEMENT Help me HELP ME!! RECOGNIZING AND IDENTIFYING PAIN Trust what the resident says Recognize other words to describe pain Implement the appropriate interventions to relieve their pain WHAT
PAIN MANAGEMENT Help me HELP ME!! RECOGNIZING AND IDENTIFYING PAIN Trust what the resident says Recognize other words to describe pain Implement the appropriate interventions to relieve their pain WHAT
Annual Pain Competency
 Annual Pain Competency 2016 Revised for RBMC Please call Professional Development at X4196 or X5947 if you have any questions The learner will be able to: Objectives Explain pain scales & appropriate use
Annual Pain Competency 2016 Revised for RBMC Please call Professional Development at X4196 or X5947 if you have any questions The learner will be able to: Objectives Explain pain scales & appropriate use
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017.
 DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
Appendix Surgery. (Appendectomy) Your surgery and recovery at home. This booklet belongs to: Royal Columbian Hospital Eagle Ridge Hospital
 Your surgery and recovery at home. This booklet belongs to: Royal Columbian Hospital Eagle Ridge Hospital") Appendix Surgery (Appendectomy) Royal Columbian Hospital Eagle Ridge Hospital Your surgery and recovery at home This booklet belongs to: We also give you Preparing for Your Surgery booklet. Read both booklets
Appendix Surgery (Appendectomy) Royal Columbian Hospital Eagle Ridge Hospital Your surgery and recovery at home This booklet belongs to: We also give you Preparing for Your Surgery booklet. Read both booklets
Delirium Information for patients and relatives. Delirium is common Delirium is treatable Relatives can stay to help us
 Delirium Information for patients and relatives Delirium is common Delirium is treatable Relatives can stay to help us What is delirium? Delirium is caused by a disturbance of brain function. It is used
Delirium Information for patients and relatives Delirium is common Delirium is treatable Relatives can stay to help us What is delirium? Delirium is caused by a disturbance of brain function. It is used
Caring for a Patient or Family Member with Alzheimer s Disease or Related Dementia
 Caring for a Patient or Family Member with Alzheimer s Disease or Related Dementia Tiffany D. Long, MS4 UNC School of Medicine MD Candidate Class of 2018 Disclaimers A portion of this project is/was supported
Caring for a Patient or Family Member with Alzheimer s Disease or Related Dementia Tiffany D. Long, MS4 UNC School of Medicine MD Candidate Class of 2018 Disclaimers A portion of this project is/was supported
COMMON DRUG RELATED PROBLEMS SEEN IN PACE AND MECHANISMS TO MITIGATE RISK
 COMMON DRUG RELATED PROBLEMS SEEN IN PACE AND MECHANISMS TO MITIGATE RISK Robert L Alesiani, PharmD, CGP Chief Pharmacotherapy Officer CareKinesis, Inc. (a Tabula Rasa Healthcare Company) 2 3 4 5 Pharmacogenomics
COMMON DRUG RELATED PROBLEMS SEEN IN PACE AND MECHANISMS TO MITIGATE RISK Robert L Alesiani, PharmD, CGP Chief Pharmacotherapy Officer CareKinesis, Inc. (a Tabula Rasa Healthcare Company) 2 3 4 5 Pharmacogenomics
Repetitive Vocalizations
 Repetitive Vocalizations Case study........................................... A 77 year old woman developed a variety of behaviours after a diagnosis of Pott s Puffy Tumor (frontal lobe) in April 2015.
Repetitive Vocalizations Case study........................................... A 77 year old woman developed a variety of behaviours after a diagnosis of Pott s Puffy Tumor (frontal lobe) in April 2015.
Geri-PARDY! (2015 Beers Criteria) Pharmacology Edition
 Pharmacology Edition") Geri-PARDY! Pharmacology Edition (2015 Beers Criteria) Aurelio Muyot, MD, AGSF, FACP Assistant Professor College of Osteopathic Medicine Touro University Nevada Objectives Review the 2015 Beers Criteria
Geri-PARDY! Pharmacology Edition (2015 Beers Criteria) Aurelio Muyot, MD, AGSF, FACP Assistant Professor College of Osteopathic Medicine Touro University Nevada Objectives Review the 2015 Beers Criteria
Anthony J. Caprio, MD, CMD, AGSF 1
 Objectives 1) Discuss the dangers of polypharmacy 2) Review potentially inappropriate medications for older adults Doc, I think I am taking too many medications! 3) Develop strategies for prioritizing
Objectives 1) Discuss the dangers of polypharmacy 2) Review potentially inappropriate medications for older adults Doc, I think I am taking too many medications! 3) Develop strategies for prioritizing
Recognition and Management of Behavioral Disturbances in Dementia
 Recognition and Management of Behavioral Disturbances in Dementia Danielle Hansen, DO, MS (Med Ed), MHSA INTRODUCTION 80% 90% of patients with dementia develop at least one behavioral disturbances or psychotic
Recognition and Management of Behavioral Disturbances in Dementia Danielle Hansen, DO, MS (Med Ed), MHSA INTRODUCTION 80% 90% of patients with dementia develop at least one behavioral disturbances or psychotic
Appendix 4B - Guidance for the use of Pharmacological Agents for the Treatment of Depression in Adults (18 years and over)
") Appendix 4B - Guidance for the use of Pharmacological Agents for the Treatment of Depression in Adults (18 years and over) Introduction / Background Treatment comes after diagnosis Diagnosis is based on
Appendix 4B - Guidance for the use of Pharmacological Agents for the Treatment of Depression in Adults (18 years and over) Introduction / Background Treatment comes after diagnosis Diagnosis is based on
Pain and the MGH Promise
 Pain is an unpleasant sensory & emotional experience associated with actual or potential tissue damage or described in terms of such damage Our promise to patients we will always: Work as a team to evaluate,
Pain is an unpleasant sensory & emotional experience associated with actual or potential tissue damage or described in terms of such damage Our promise to patients we will always: Work as a team to evaluate,
Mucky Meds: A (practical) approach the nightmare med list. Michelle Gibson, MD, CCFP (COE), FCFP and Erin Beattie, MD, CCFP
 approach the nightmare med list. Michelle Gibson, MD, CCFP (COE), FCFP and Erin Beattie, MD, CCFP") Mucky Meds: A (practical) approach the nightmare med list Michelle Gibson, MD, CCFP (COE), FCFP and Erin Beattie, MD, CCFP Faculty/Presenter Disclosure Faculty: Michelle Gibson Relationships with financial
Mucky Meds: A (practical) approach the nightmare med list Michelle Gibson, MD, CCFP (COE), FCFP and Erin Beattie, MD, CCFP Faculty/Presenter Disclosure Faculty: Michelle Gibson Relationships with financial
Delirium. Assessment and Management
 Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
ANTI-DEPRESSANT MEDICATIONS
 ANTI-DEPRESSANT MEDICATIONS This information is not intended to be a substitute for medical advice. It s purpose is solely informative. If your client or yourself are taking antidepressants, do not change
ANTI-DEPRESSANT MEDICATIONS This information is not intended to be a substitute for medical advice. It s purpose is solely informative. If your client or yourself are taking antidepressants, do not change
Black holes taped on floor Redirection Music and activities Yellow straps across the door Remind other residents to use call bell when she comes in
 Intrusive Wandering Case study........................................... A 97 year old woman with dementia lives in a mixed 23 bed LTC unit. She is independently mobile in her wheelchair and goes in and
Intrusive Wandering Case study........................................... A 97 year old woman with dementia lives in a mixed 23 bed LTC unit. She is independently mobile in her wheelchair and goes in and
Pain Management Management in Hepatic Hepatic and and Renal Dysfunction
 Pain Management in Hepatic and Renal Dysfunction Review the pharmacologic basis for medications used in pain management Identify pain medications which hshould ldbe avoided in patients with hepatic dysfunction
Pain Management in Hepatic and Renal Dysfunction Review the pharmacologic basis for medications used in pain management Identify pain medications which hshould ldbe avoided in patients with hepatic dysfunction
Behavioral Issues in Dementia. March 27, 2014 Dylan Wint, M.D.
 Behavioral Issues in Dementia March 27, 2014 Dylan Wint, M.D. OVERVIEW Key points Depression Definitions and detection Treatment Psychosis Definitions and detection Treatment Agitation SOME KEY POINTS
Behavioral Issues in Dementia March 27, 2014 Dylan Wint, M.D. OVERVIEW Key points Depression Definitions and detection Treatment Psychosis Definitions and detection Treatment Agitation SOME KEY POINTS
Elizabeth McManamy, RPh Pharmacist Quality Monitor Jennifer Wills, BSN, RN Nurse Manager DADS Quality Monitoring Program
 Elizabeth McManamy, RPh Pharmacist Quality Monitor Jennifer Wills, BSN, RN Nurse Manager DADS Quality Monitoring Program Objectives 1.Summarize the pharmacology of the antipsychotic drug class 2.Describe
Elizabeth McManamy, RPh Pharmacist Quality Monitor Jennifer Wills, BSN, RN Nurse Manager DADS Quality Monitoring Program Objectives 1.Summarize the pharmacology of the antipsychotic drug class 2.Describe
OPIOIDS: THE GOOD, THE BAD, AND EVERYTHING IN-BETWEEN
 OPIOIDS: THE GOOD, THE BAD, AND EVERYTHING IN-BETWEEN ANTOINETTE BROWN, RPH LAUREL RAMER, 2019 PHARMD CANDIDATE 2018 WYOMING CONFERENCE ON AGING LARAMIE, WY OCTOBER 3, 2018 OBJECTIVES 1. Understand the
OPIOIDS: THE GOOD, THE BAD, AND EVERYTHING IN-BETWEEN ANTOINETTE BROWN, RPH LAUREL RAMER, 2019 PHARMD CANDIDATE 2018 WYOMING CONFERENCE ON AGING LARAMIE, WY OCTOBER 3, 2018 OBJECTIVES 1. Understand the
Pain: You Can Get Help
 National Institute on Aging AgePage Pain: You Can Get Help Phyllis loves playing with her grandchildren, working in the garden, and going to bingo games twice a week. But, at age 76, the constant knee
National Institute on Aging AgePage Pain: You Can Get Help Phyllis loves playing with her grandchildren, working in the garden, and going to bingo games twice a week. But, at age 76, the constant knee
Record keeping. Contents: Dementia handbook for carers Essex
 Dementia handbook for carers Essex Record keeping Contents: Contacts Appointment record Questions and concerns Summary sheet for medical care professionals Medication record (renewing prescriptions) Pain
Dementia handbook for carers Essex Record keeping Contents: Contacts Appointment record Questions and concerns Summary sheet for medical care professionals Medication record (renewing prescriptions) Pain
May 2015 Clinical Nurse Educator Arohanui Hospice
 May 2015 Clinical Nurse Educator Arohanui Hospice End of Life Care, what s on top? Feedback from last session (Physiology of Dying) Volunteer to present at August meeting Presentation: Breaking Bad News
May 2015 Clinical Nurse Educator Arohanui Hospice End of Life Care, what s on top? Feedback from last session (Physiology of Dying) Volunteer to present at August meeting Presentation: Breaking Bad News
Session outline. Introduction to dementia Assessment of dementia Management of dementia Follow-up Review
 Dementia 1 Session outline Introduction to dementia Assessment of dementia Management of dementia Follow-up Review 2 Activity 1: Person s story Present a person s story of what it feels like to live with
Dementia 1 Session outline Introduction to dementia Assessment of dementia Management of dementia Follow-up Review 2 Activity 1: Person s story Present a person s story of what it feels like to live with
Challenging Patients Curriculum Instructor Guide
 Challenging Patients Curriculum Instructor Guide The Patient with Chronic Pain Goals: A PGY-2 resident will be able to evaluate and develop a treatment plan for a geriatric patient with several co-morbidities
Challenging Patients Curriculum Instructor Guide The Patient with Chronic Pain Goals: A PGY-2 resident will be able to evaluate and develop a treatment plan for a geriatric patient with several co-morbidities
Coach on Call. Thank you for your interest in How to Prevent and Treat Aches and Pains. I hope you find this tip sheet helpful.
 It was great to talk with you. Thank you for your interest in. I hope you find this tip sheet helpful. Please give me a call if you have more questions about this or other topics. As your UPMC Health Plan
It was great to talk with you. Thank you for your interest in. I hope you find this tip sheet helpful. Please give me a call if you have more questions about this or other topics. As your UPMC Health Plan
Katee Kindler, PharmD, BCACP
 Speaker Introduction Katee Kindler, PharmD, BCACP Current Practice: Clinical Pharmacy Specialist Ambulatory Care, St. Vincent Indianapolis Assistant Professor of Pharmacy Practice, Manchester University,
Speaker Introduction Katee Kindler, PharmD, BCACP Current Practice: Clinical Pharmacy Specialist Ambulatory Care, St. Vincent Indianapolis Assistant Professor of Pharmacy Practice, Manchester University,
Pain Control After Surgery. Patient Information
 Pain Control After Surgery Patient Information What is Pain? Pain is an uncomfortable feeling that tells you something may be wrong in your body. Pain is your body s way of sending a warning to your brain.
Pain Control After Surgery Patient Information What is Pain? Pain is an uncomfortable feeling that tells you something may be wrong in your body. Pain is your body s way of sending a warning to your brain.
Management of Delirium in Hospice Patients
 Presentation Objectives Management of Delirium in Hospice Patients Lynn Williams, BSPharm Clinical Pharmacist Hospice Pharmacy Solutions Identify the clinical features of delirium Understand the underlying
Presentation Objectives Management of Delirium in Hospice Patients Lynn Williams, BSPharm Clinical Pharmacist Hospice Pharmacy Solutions Identify the clinical features of delirium Understand the underlying
CONCERNED ABOUT TAKING OPIOIDS AFTER SURGERY?
 CONCERNED ABOUT TAKING OPIOIDS AFTER SURGERY? ASK YOUR DOCTOR ABOUT EXPAREL FOR LONG-LASTING, NON-OPIOID PAIN RELIEF. VISIT EXPAREL.com/patient FOR MORE INFORMATION. YOU HAVE A SAY IN HOW YOUR PAIN IS
CONCERNED ABOUT TAKING OPIOIDS AFTER SURGERY? ASK YOUR DOCTOR ABOUT EXPAREL FOR LONG-LASTING, NON-OPIOID PAIN RELIEF. VISIT EXPAREL.com/patient FOR MORE INFORMATION. YOU HAVE A SAY IN HOW YOUR PAIN IS
Treatment of Anxiety (without benzos)
") Treatment of Anxiety (without benzos) Alison C. Lynch MD MS Clinical Professor Departments of Psychiatry and Family Medicine University of Iowa Health Care None Disclosures Overview/objectives Review common
Treatment of Anxiety (without benzos) Alison C. Lynch MD MS Clinical Professor Departments of Psychiatry and Family Medicine University of Iowa Health Care None Disclosures Overview/objectives Review common
Medication Reviews within Care Homes. Catherine Armstrong
 Medication Reviews within Care Homes Catherine Armstrong What is a Medication Review? A structured, critical examination of a patient s medicines with the objective of reaching an agreement with the patient
Medication Reviews within Care Homes Catherine Armstrong What is a Medication Review? A structured, critical examination of a patient s medicines with the objective of reaching an agreement with the patient
The Use of Antidepressants in the Treatment of Irritable Bowel Syndrome and Other Functional GI Disorders What are functional GI disorders?
 The Use of Antidepressants in the Treatment of Irritable Bowel Syndrome and Other Functional GI Disorders Christine B. Dalton, PA-C Douglas A. Drossman, MD and Kellie Bunn, PA-C What are functional GI
The Use of Antidepressants in the Treatment of Irritable Bowel Syndrome and Other Functional GI Disorders Christine B. Dalton, PA-C Douglas A. Drossman, MD and Kellie Bunn, PA-C What are functional GI
Poisoning Deaths vs. Motor Vehicle Related Injury Deaths, MA Residents ( )
") Source: National Vital Statistics Poisoning Deaths vs. Motor Vehicle Related Injury Deaths, MA Residents (1997 2008) The source of the data is: Registry of Vital Records and Statistics, MA Department of
Source: National Vital Statistics Poisoning Deaths vs. Motor Vehicle Related Injury Deaths, MA Residents (1997 2008) The source of the data is: Registry of Vital Records and Statistics, MA Department of
Updates to CMS SOM rules on Psychosocial Issues, Deficiency Categorization, and Psychotropic Medication Use
 Updates to CMS SOM rules on Psychosocial Issues, Deficiency Categorization, and Psychotropic Medication Use Stephen Eide R. Ph Oni Kinberg LCSW, MSSW Updates to the SOM On March 25, 2016 CMS sent out updates
Updates to CMS SOM rules on Psychosocial Issues, Deficiency Categorization, and Psychotropic Medication Use Stephen Eide R. Ph Oni Kinberg LCSW, MSSW Updates to the SOM On March 25, 2016 CMS sent out updates
MODULE 7: COMMON CONDITIONS AND SOME OF THE DRUGS USED TO TREAT THEM
 MODULE 7: COMMON CONDITIONS AND SOME OF THE DRUGS USED TO TREAT THEM 6.1: The Heart & Blood Circulation The heart is a muscular organ about the size of a fist, located just behind and slightly left of
MODULE 7: COMMON CONDITIONS AND SOME OF THE DRUGS USED TO TREAT THEM 6.1: The Heart & Blood Circulation The heart is a muscular organ about the size of a fist, located just behind and slightly left of
Source: National Vital Statistics
 Summarize the basics of how to wean patients off of opiates and who is at risk of withdrawal. Review the signs and symptoms of withdrawal from chronic opioids. Summarize how providers can use medications
Summarize the basics of how to wean patients off of opiates and who is at risk of withdrawal. Review the signs and symptoms of withdrawal from chronic opioids. Summarize how providers can use medications
Pain Management in Older Adults. Mary Shelkey, PhD, ARNP
 Pain Management in Older Adults Mary Shelkey, PhD, ARNP Cause of Death/ Demographic and Social Trends Early 1900s Current Medicine's Focus Comfort Cure Cause of Death Infectious Diseases/ Communicable
Pain Management in Older Adults Mary Shelkey, PhD, ARNP Cause of Death/ Demographic and Social Trends Early 1900s Current Medicine's Focus Comfort Cure Cause of Death Infectious Diseases/ Communicable
PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS. Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA
 CASE #1 PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA OBJECTIVES Epidemiology Presentation in older adults Assessment Treatment
CASE #1 PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA OBJECTIVES Epidemiology Presentation in older adults Assessment Treatment
Disclosures. Management of Chronic, Non- Terminal Pain. Learning Objectives. Outline. Drug Schedules. Applicable State Laws
 Disclosures Management of Chronic, Non- Terminal Pain No financial disclosures or conflicts of interest to report Michael A. Smith, PharmD, BCPS Clinical Assistant Professor, University of Michigan College
Disclosures Management of Chronic, Non- Terminal Pain No financial disclosures or conflicts of interest to report Michael A. Smith, PharmD, BCPS Clinical Assistant Professor, University of Michigan College
Venlafaxine hydrochloride extended-release and other antidepressant medicines may cause serious side effects, including:
 Medication Guide VENLAFAXINE XR (venlafaxine hydrochloride) (Extended-Release Capsules) Read the Medication Guide that comes with venlafaxine hydrochloride extended-release before you start taking it and
Medication Guide VENLAFAXINE XR (venlafaxine hydrochloride) (Extended-Release Capsules) Read the Medication Guide that comes with venlafaxine hydrochloride extended-release before you start taking it and
Your guide to recovery. Treating concussions
 Your guide to recovery Treating concussions About concussions A concussion is a condition, usually caused when a blow to the head or body causes the brain to move rapidly within the skull, that can temporarily
Your guide to recovery Treating concussions About concussions A concussion is a condition, usually caused when a blow to the head or body causes the brain to move rapidly within the skull, that can temporarily
MODULE III Challenging Behaviors
 Mental Health Ombudsman Training Manual Advocacy and the Adult Home Resident MODULE III Challenging Behaviors S WEHRY 2004 Objectives: Part One Describe principles of communication Describe behavior as
Mental Health Ombudsman Training Manual Advocacy and the Adult Home Resident MODULE III Challenging Behaviors S WEHRY 2004 Objectives: Part One Describe principles of communication Describe behavior as