Delirium, Depression and Dementia
|
|
|
- Philip Williams
- 6 years ago
- Views:
Transcription
1 Delirium, Depression and Dementia Martha Watson, MS, APRN, GCNS Some material included in this presentation is adapted from: NICHE (2009). Geriatric Resource Nurse Core Curriculum [Power Point presentation]. New York: Hartford Institute for Geriatric Nursing, New York University College of Nursing

2 Program Objectives Describe the difference between dementia, delirium and depression. Review simple screening tools for each that the RN can perform. Identify first interventions for each.
3 3 Prevalence in Older Adults General population Hospitalized patients Depression Delirium* Dementia Minor depressive symptoms 3-26% Minor depressive symptoms 23% 10-15% on admission 10-40% in-hospital (new onset) 43-61% of hip surgery patients 5% of 65+ adults 50% of 85+ adults 25% 31% of older adults admitted to medical intensive care units Depression + dementia 22-54% 83% of mechanically ventilated patients (all ages) Delirium + dementia 22-89% *Based on 1994 U.S. vital health statistics, complications associated with delirium occur in more than 2.3 million hospitalized older adults every year with associated Medicare costs equaling $8 billion annually.

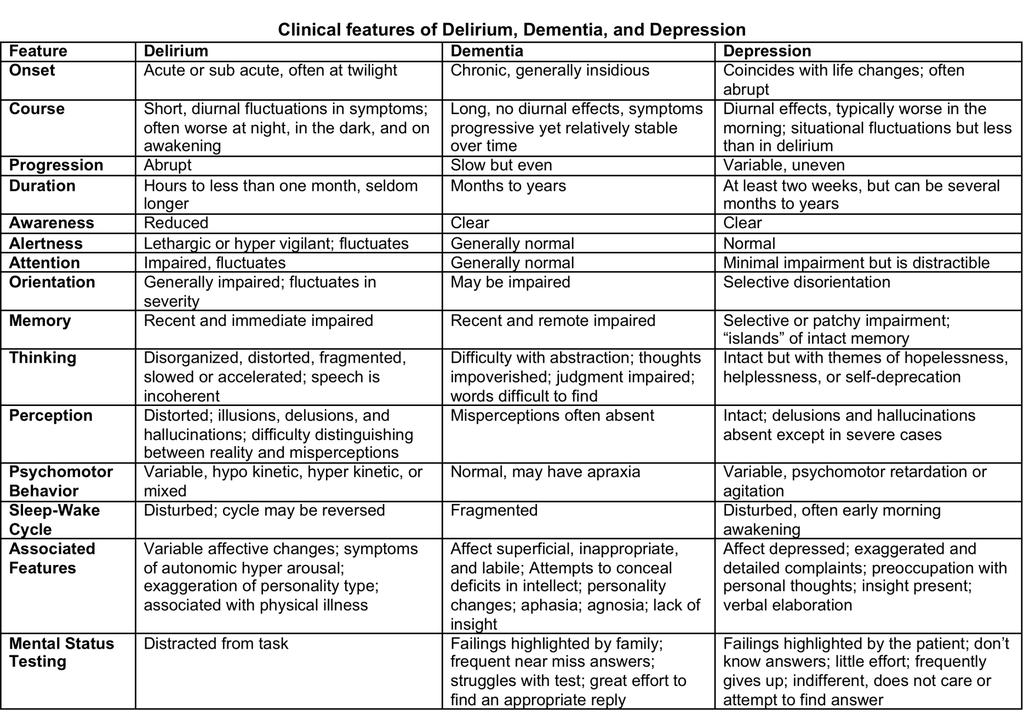
4 Delirium, Depression and Dementia What are the differences between the 3 D s? the ultra short version.
5
6 DELIRIUM
7 Delirium DSM-5 (May 2013): 1. Disturbance in attention 2. Acute fluctuation in mental status 3. Altered mental status 4. Not a result of severely reduced LOC (ie. Coma)
8 Significance of Delirium Increased healthcare Increased death rate Increased complications post op Longer hospital stays Functional decline New nursing home placement Long term cognitive decline
9 Prevalence? Prevalence varies by population being studied Delirium in the Community overall prevalence 0.4-2%. Higher rates in the Hospital setting % of hospitalized patients above age 65 Post operative Delirium 15-62% Intensive care units 70-87% 50% of our Hospital beds occupancy are in ages > 65. Delirium complication put in dollars. 6.9 billion Medicare Hosp. Exp. (2004)
10 Description of Delirium Acute confusional state, ICU psychosis Change in Mental Status Common syndrome with rapid onset (hours or days) Impaired attention Disorganized thinking Tends to change with a variable course Evidence of underlying medical condition

11 Do we do a good job of detecting delirium? Only 50% recognized by nurses Only 20% recognized by physicians
12 Persons at Risk for Delirium The risk of delirium increases with age, but it is not not, not a normal age related change Most common Dementia Male gender Advanced age Medical illness Predisposing Poor functional status Alcohol abuse Depression Dehydration Sensory impairment
 Centrally acting antihypertensives Antiparkinsonian drugs 0000_NICHE Program Development 13 3/9/2015")
13 High Risk Medications Anticholinergics (benadryl) Opioids (meperidine) Sedative hypnotics (benzodiazepines) Histamine (H2) receptor antagonists Corticosteroids (prednisone) Centrally acting antihypertensives Antiparkinsonian drugs 0000_NICHE Program Development 13 3/9/ :40:47 PM

14 Delirium Risk Factors Predisposing + Precipitating Factors Delirium
15 Types of Delirium Hyperactive Hypoactive Mixed
16 Hypoactive Delirium Most likely to be missed/not recognized 60% of all delirium cases Higher risk for DEATH Signs and symptoms Sleepy, sluggish, uninterested, withdrawn Slow speech, mumbling Laying in bed with little interaction Visual hallucinations (sensory perception not related to external event) often seen as picking in the air
17 Hypoactive Delirium Patients are Sicker on admission Have longer lengths of stay Are more likely to develop pressure ulcers as a result of immobility Are more likely to die May be diagnosed as having depression The hypoactive form is often overlooked in elderly!!! (increased lethargy, decreased activity)
18 Hyperactive Delirium Most easily recognized 30% of all delirium cases Higher fall risk Signs and symptoms Restless, irritable, combative, angry, uncooperative, easily distracted Fast or loud speech Wandering, climbing out of bed Visual hallucinations
19 Mixed Delirium Shift between hyperactive & hypoactive states May account for about 10% of all delirium cases Daily care is challenging because course of the disease is unpredictable and changing
20 Implications of Delirium Patient Family Staff Acute anxiety Barrier to communication Decreased self care Time lost Increased blood tests, x-rays, etc. Increased treatment and medications Barrier to communication Time lost Stressful Increased risk of conflict with staff Possible bereavement Barrier to communication Difficulty in assessing patient symptoms and course of illness Stressful Increased risk of conflict with family TIME!!!
21 Risk Factors During Hospitalization Medications added Malnutrition Physical restraints used Bladder catheter and other tubes Untreated pain Infection Relocation especially to ICU It is reasonable to anticipate delirium in a hospitalized older adult
22 Recognition of Delirium

23 Simple Screening
24 Simple Screening
25 The Confusion Assessment Method (1990)
26 Early Interventions for Delirium.. Know your patient s history Be alert for risk factors Look Listen See Believe the family Believe the family Non-pharmacologic Management Control environment by reducing over stimulation, avoiding sleep deprivation, establishing routines following day and night Minimize relocation and maintain consistency of caregivers







27 Simple Interventions for Delirium Maximize Orientation Clocks and calendars Dry erase boards for staff names and scheduled activities Keep family informed Involve family members in care and routine
28 DEMENTIA

29 Dementia Clinical syndrome of cognitive defects Memory impairments and disturbance in at least one other area of cognition Gradual decline in function Gradual changes in mood and behavior
30
31 Dementia Not senility and not, not, not normal aging Syndrome of cognitive defects; many types of dementia Characterized by impaired memory, change in intellect, and personality Gradual decline in function Gradual changes in mood and behavior Most common form of dementia is Alzheimer s disease (60% of all dementias) About 25% of hospitalized older patients have dementia Dementia is a risk factor for delirium and delirium is a risk factor for dementia
32 Forms of Progressive Dementia Dementia Types % of all dementias Lesions Alzheimer s disease (AD) Vascular dementia (VaD, multi-infarct) 60% Neurofibrillary plaques and tangles 20% Multiple infarctions Single infarctions Diffuse subcortical white matter disease Hemorrhagic lesions Dementia with Lewy Bodies (DLB) Less common Lewy bodies are aggregations of alpha-synuclein in cytoplasm of neurons 0000_NICHE Program Development 32 3/9/ :40:48 PM
33 Clinical Presentation of Dementias AD VaD DLB Progressive loss of memory Deterioration in language & other cognitive functions Decline in ADLs Changes in personality & behavior Evidence of focal deficits Gait disturbance Impairments in executive function Memory not as affected as in AD Cognitive & behavioral changes in combination with features of Parkinson s disease 0000_NICHE Program Development 33 3/9/ :40:48 PM
34 Alzheimer s Disease Early Mild Moderate Noticeable deficits in demanding job situations Deficit associated with complicated tasks Deficit associated with choosing proper attire Mild cognitive decline Moderate cognitive decline Denial and withdrawal from challenging situations Moderate to severe cognitive decline Moderately severe Deficits during ADLs Severe cognitive decline with total dependence Severe Declined speech ability, loss of ability to walk, sit up, smile, hold head up Severe cognitive decline with no verbal or self care abilities 0000_NICHE Program Development 34 3/9/ :40:48 PM
35 Common Co-Morbidities Psychosis (30-50% frequency) Delusions and paranoia Hallucinations, most commonly visual Agitation (80% frequency) Aggression, combativeness, hyperactivity, wandering, hypervocalization, and disinhibition Depressive symptom (> 70% frequency)

36 Simple Screening
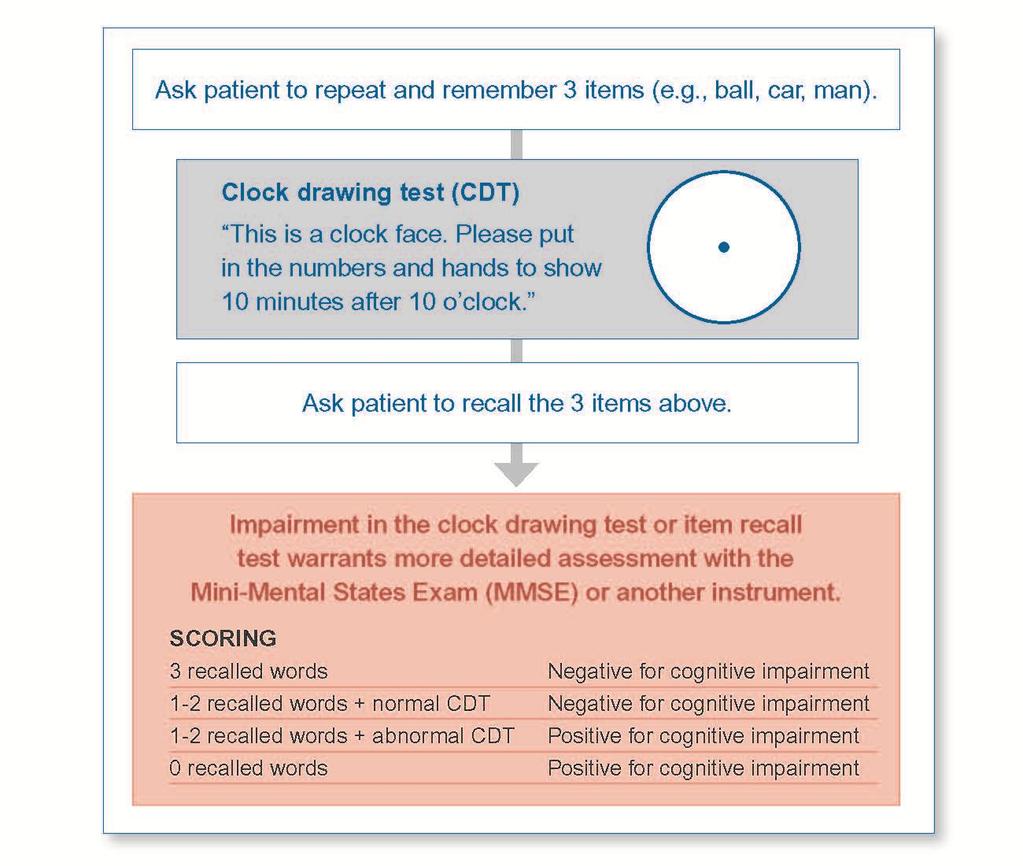
37 Mini-Cog
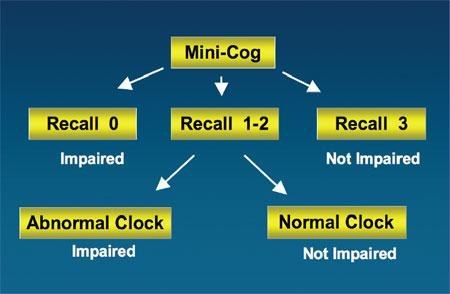
38 Mini-Cog
39 Reality of Dementia It changes everything, with time It is NOT something the individual can control It is different for every person It is NOT a mental illness It is very hard for families Information to obtain from caregiver: Best way to communicate How to deal with episodes of agitation Best way to perform ADL functions Tips on getting patient to eat Usual signs of pain Sleep habits Previous occupations and interests Situations that upset the patient and best responses to them

40 Pearls of Wisdom Patients with dementia are more likely to develop delirium Be aware of what is normal behavior Be alert for pain, nausea, fatigue Be aware of any medication changes Be alert to protein/energy malnutrition and dehydration


41 Caregiver Assessment Caregiver Burden: Fatigue Grief Changes in social relationships Depression Physical illness Death 0000_NICHE Program Development 41 3/9/ :40:48 PM
42 DEPRESSION

43 Depression 1. Depressed, sad, or irritable mood 2. Diminished pleasure in pleasurable people and activities 3. Feelings of worthlessness, self reproach, and excessive guilt 4. Difficulty thinking or diminished concentration 5. Suicidal thinking or attempts 6. Fatigue and loss of energy 7. Changes in appetite and weight 8. Disturbed sleep 9. Psychomotor agitation or retardation

44 Depression in Rhode Island cations/healthriskreports/adult s/2006depression.pdf
45 Depression Most common emotional disorder in older adults; not, not, not a normal part of aging May range from mild to severe Under diagnosed and under treated High rate of suicide among white men > 85 years Depressed mood may be not be obvious Atypical presentation: somatic complaints, anxious, irritable, pacing, constant worrying, feeling tired Symptoms may be associated with a medical illness ( CHF or lung disease)
46 Clinical Presentation Major depression (most severe) 5 out of 9 criteria present for 2 week period Change from previous functioning Minor depression (most common) Fewer than 5 criteria for 2 week period Change from previous functioning The somatic or physical symptoms of depression are often difficult to distinguish from symptoms associated with acute or chronic physical illness
47 Risk Factors/High Risk Groups Social and demographic risk factors: Female sex, Unmarried status Stressful life events, Absence of social support Current alcohol/substance abuse Functional disability Medical comorbidities Disability, older age, new medical diagnosis, and poor health status are among the most consistent of all correlates of depression among older medical patients
48 Consequences of Depression Turns up the Volume Pain and disability Delayed recovery Worsening of medical symptoms Risk of physical illness Increased healthcare use Cognitive impairment Poor nutrition Depression is present in 22-54% of the cases of dementia

49 Suicide in Older Adults Higher mortality rate Highest rate of any age group White men >85 years at greatest risk Depressive symptoms, perceived health status, sleep quality, and no confidant Physical illness, functional impairment, and depression Disruption of social support, family conflict, and loneliness

50 Simple Screening
51 Simple Screening
52 Scoring Answers in bold indicate depression. Score 1 point for each bolded answer. A score > 5 points is suggestive of depression. A score 10 points is almost always indicative of depression. A score > 5 points should warrant a follow-up comprehensive assessment
53 Treatment Strategies Pharmacologic TCAs, SSRIs, SNRIs Group and Individual psychotherapy Electroconvulsive Therapy Interdisciplinary team approach
54 Nursing Strategies 1. Promote nutrition, elimination, sleep/rest patterns, physical comfort, and pain control 2. Structure and encourage daily participation in relaxation therapies and pleasant activities 3. Enhance function 4. Enhance social support 5. Maximize autonomy, personal control, self efficacy, and decision making 6. Encourage pleasant reminiscing 7. Provide emotional support and supportive listening, encourage expression of feelings, and instill hope 8. Identify and reinforce strengths and capabilities 10. Monitor and document responses to medication and other therapies 11. Promote communication 12. Educate patients and families about depression and effective management
55 REVIEW
56
57 Tools For Assessment Mini-Cog Confusion Assessment Method Geriatric Depression Scale
58 QUESTIONS? Thank you.
Depression in the Eldery Handout Package
 Depression in the Eldery Handout Package Depression in the Elderly 1 Learning Objectives Upon completion of this module, you should be able to: 1. State the prevalence and describe the consequences of
Depression in the Eldery Handout Package Depression in the Elderly 1 Learning Objectives Upon completion of this module, you should be able to: 1. State the prevalence and describe the consequences of
Delirium. Delirium is characterized by an acute onset (hours or days) and fluctuating course of deterioration in mental functioning.
 and fluctuating course of deterioration in mental functioning.") Delirium Delirium is characterized by an acute onset (hours or days) and fluctuating course of deterioration in mental functioning. DELIRIUM IS A MEDICAL EMERGENCY! Delirium: Hallmark Features Inattention-
Delirium Delirium is characterized by an acute onset (hours or days) and fluctuating course of deterioration in mental functioning. DELIRIUM IS A MEDICAL EMERGENCY! Delirium: Hallmark Features Inattention-
Delirium. Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta
 Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach
 Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach Featuring: Felice Rogers Evans BSN RN BC Ty Breiter MSN RN CNL Tampa General Hospital NICHE exemplar hospital Three time
Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach Featuring: Felice Rogers Evans BSN RN BC Ty Breiter MSN RN CNL Tampa General Hospital NICHE exemplar hospital Three time
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE
 Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
Recognition and Management of Behavioral Disturbances in Dementia
 Recognition and Management of Behavioral Disturbances in Dementia Danielle Hansen, DO, MS (Med Ed), MHSA INTRODUCTION 80% 90% of patients with dementia develop at least one behavioral disturbances or psychotic
Recognition and Management of Behavioral Disturbances in Dementia Danielle Hansen, DO, MS (Med Ed), MHSA INTRODUCTION 80% 90% of patients with dementia develop at least one behavioral disturbances or psychotic
Are All Older Adults Depressed? Common Mental Health Disorders in Older Adults
 Are All Older Adults Depressed? Common Mental Health Disorders in Older Adults Cherie Simpson, PhD, APRN, CNS-BC Myth vs Fact All old people get depressed. Depression in late life is more enduring and
Are All Older Adults Depressed? Common Mental Health Disorders in Older Adults Cherie Simpson, PhD, APRN, CNS-BC Myth vs Fact All old people get depressed. Depression in late life is more enduring and
The Person: Dementia Basics
 The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
Delirium Assessment. February 24, Susan Schumacher, MS, APRN-BC
 Delirium Assessment February 24, 2016 Susan Schumacher, MS, APRN-BC Objectives Define delirium Differentiate delirium from dementia Identify predisposing and precipitating factors leading to delirium.
Delirium Assessment February 24, 2016 Susan Schumacher, MS, APRN-BC Objectives Define delirium Differentiate delirium from dementia Identify predisposing and precipitating factors leading to delirium.
Delirium in the Elderly
 Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Dementia. Assessing Brain Damage. Mental Status Examination
 Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Delirium in Palliative care. Presentation to Volunteers 2016 David Falk
 Delirium in Palliative care Presentation to Volunteers 2016 David Falk Delirium What is delirium? Case Study - Delirium 60+ year old PQ presents to hospice very somnolent. She was admitted with her adult
Delirium in Palliative care Presentation to Volunteers 2016 David Falk Delirium What is delirium? Case Study - Delirium 60+ year old PQ presents to hospice very somnolent. She was admitted with her adult
Chapter 20 Psychosocial Nursing of the Physically Ill Client Psychosocial Assessment Interactive process that involves gathering data and evaluating
 Chapter 20 Psychosocial Nursing of the Physically Ill Client Psychosocial Assessment Interactive process that involves gathering data and evaluating the past and current level of functioning of the client
Chapter 20 Psychosocial Nursing of the Physically Ill Client Psychosocial Assessment Interactive process that involves gathering data and evaluating the past and current level of functioning of the client
Delirium. Delirium. Delirium Etiology and Pathophysiology. Fall 2018
 Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Behavioral Interventions
 Behavioral Interventions Linda K. Shumaker, R.N.-BC, MA Pennsylvania Behavioral Health and Aging Coalition Behavioral Management is the key in taking care of anyone with a Dementia! Mental Health Issues
Behavioral Interventions Linda K. Shumaker, R.N.-BC, MA Pennsylvania Behavioral Health and Aging Coalition Behavioral Management is the key in taking care of anyone with a Dementia! Mental Health Issues
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017.
 DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
ALZHEIMER S DISEASE. Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey
 ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
nicheprogram.org 16th Annual NICHE Conference Forging New Paths and Partnerships 1
 Improving Patient Outcomes in Geriatric Post-Operative Orthopedic Patients: Translating Research into Practice Tripping into The CAM Presented by: Diana LaBumbard, RN, MSN, ACNP/GNP-BC, CWOCN Denise Williams,
Improving Patient Outcomes in Geriatric Post-Operative Orthopedic Patients: Translating Research into Practice Tripping into The CAM Presented by: Diana LaBumbard, RN, MSN, ACNP/GNP-BC, CWOCN Denise Williams,
Delirium. A Plan to Reduce Use of Restraints. David Wensel DO, FAAHPM Medical Director Midland Care
 Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Delirium in the Elderly
 Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium Pilot Project
 CCU Nurses: Delirium Pilot Project Our unit has been selected to develop and implement a delirium assessment and intervention program. We are beginning Phase 1 with education and assessing for our baseline
CCU Nurses: Delirium Pilot Project Our unit has been selected to develop and implement a delirium assessment and intervention program. We are beginning Phase 1 with education and assessing for our baseline
ADRC Dementia Care Training. Module 10: Supporting People with Serious Mental Illness and Dementia: Bipolar Disorders, Dementia, and Delirium
 ADRC Dementia Care Training Module 10: Supporting People with Serious Mental Illness and Dementia: Bipolar Disorders, Dementia, and Delirium 1 Federal definition: Ages 18 and older Serious Mental Illness
ADRC Dementia Care Training Module 10: Supporting People with Serious Mental Illness and Dementia: Bipolar Disorders, Dementia, and Delirium 1 Federal definition: Ages 18 and older Serious Mental Illness
Cognitive Status. Read each question below to the patient. Score one point for each correct response.
 Diagnosis of dementia or delirium Cognitive Status Six Item Screener Read to the patient: I have a few questions I would like to ask you. First, I am going to name three objects. After I have said all
Diagnosis of dementia or delirium Cognitive Status Six Item Screener Read to the patient: I have a few questions I would like to ask you. First, I am going to name three objects. After I have said all
Addressing Difficult Behaviors in Dementia
 Addressing Difficult Behaviors in Dementia GEORGE SCHOEPHOERSTER, MD GERIATRICIAN GENEVIVE/CENTRACARE CLINIC Objectives By the end of the session, you will be able to: 1) Explain the role of pain management
Addressing Difficult Behaviors in Dementia GEORGE SCHOEPHOERSTER, MD GERIATRICIAN GENEVIVE/CENTRACARE CLINIC Objectives By the end of the session, you will be able to: 1) Explain the role of pain management
Aging and Mental Health Current Challenges in Long Term Care
 Aging and Mental Health Current Challenges in Long Term Care Stephanie Saur & Christina Pacheco Acute Care Behavioural Consultants Alzheimer Society Peel What is Mental Health? Mental health includes our
Aging and Mental Health Current Challenges in Long Term Care Stephanie Saur & Christina Pacheco Acute Care Behavioural Consultants Alzheimer Society Peel What is Mental Health? Mental health includes our
For more information about how to cite these materials visit
 Author(s): Rachel Glick, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author(s): Rachel Glick, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Test your Knowledge: Recognizing Delirium
 The Ottawa Hospital Name: Unit: Profession: RN RPN PT OT SW Other Note: Each question has only one correct answer. 1. If a patient is identified as being at high risk for developing delirium, his/her mental
The Ottawa Hospital Name: Unit: Profession: RN RPN PT OT SW Other Note: Each question has only one correct answer. 1. If a patient is identified as being at high risk for developing delirium, his/her mental
Behavioral Issues in Dementia. March 27, 2014 Dylan Wint, M.D.
 Behavioral Issues in Dementia March 27, 2014 Dylan Wint, M.D. OVERVIEW Key points Depression Definitions and detection Treatment Psychosis Definitions and detection Treatment Agitation SOME KEY POINTS
Behavioral Issues in Dementia March 27, 2014 Dylan Wint, M.D. OVERVIEW Key points Depression Definitions and detection Treatment Psychosis Definitions and detection Treatment Agitation SOME KEY POINTS
Understanding Dementia &
 Understanding Dementia & Care Options for Those Suffering with the Disease Paige Landry BSN Hospice Care Consultant SouthernCare New Beacon Hospice Objectives Understand Dementia Understand Common Problems
Understanding Dementia & Care Options for Those Suffering with the Disease Paige Landry BSN Hospice Care Consultant SouthernCare New Beacon Hospice Objectives Understand Dementia Understand Common Problems
Geriatric Alterations Associated with Neurological Conditions
 Geriatric Alterations Associated with Neurological Conditions I have no conflicts of interest. Julie Bronson The Older Adult According to the World Health Organization Africa 50-55 or 50-65 United Nations
Geriatric Alterations Associated with Neurological Conditions I have no conflicts of interest. Julie Bronson The Older Adult According to the World Health Organization Africa 50-55 or 50-65 United Nations
Delirium. Quick reference guide. Issue date: July Diagnosis, prevention and management
 Issue date: July 2010 Delirium Diagnosis, prevention and management Developed by the National Clinical Guideline Centre for Acute and Chronic Conditions About this booklet This is a quick reference guide
Issue date: July 2010 Delirium Diagnosis, prevention and management Developed by the National Clinical Guideline Centre for Acute and Chronic Conditions About this booklet This is a quick reference guide
Geriatrics and Cancer Care
 Geriatrics and Cancer Care Roger Wong, BMSc, MD, FRCPC, FACP Postgraduate Dean of Medical Education Clinical Professor, Division of Geriatric Medicine UBC Faculty of Medicine Disclosure No competing interests
Geriatrics and Cancer Care Roger Wong, BMSc, MD, FRCPC, FACP Postgraduate Dean of Medical Education Clinical Professor, Division of Geriatric Medicine UBC Faculty of Medicine Disclosure No competing interests
Session outline. Introduction to depression Assessment of depression Management of depression Follow-up Review
 Depression 1 Session outline Introduction to depression Assessment of depression Management of depression Follow-up Review 2 Activity 1: Person s story followed by group discussion Present the first person
Depression 1 Session outline Introduction to depression Assessment of depression Management of depression Follow-up Review 2 Activity 1: Person s story followed by group discussion Present the first person
Depression among Older Adults. Prevalence & Intervention Strategies
 Depression among Older Adults Prevalence & Intervention Strategies Definition Depression is a complex syndrome complex characterized by mood disturbance plus variety of cognitive, psychological, and vegetative
Depression among Older Adults Prevalence & Intervention Strategies Definition Depression is a complex syndrome complex characterized by mood disturbance plus variety of cognitive, psychological, and vegetative
Introduction to Screening/Assessment Tools for Mood & Cognition
 Introduction to Screening/Assessment Tools for Mood & Cognition Pam Hamilton Psychogeriatric Resource Consultant for KFLA Susanne Murphy Resource Consultant, BCICC-LTC & GiiC Screening/Assessment for Delirium,
Introduction to Screening/Assessment Tools for Mood & Cognition Pam Hamilton Psychogeriatric Resource Consultant for KFLA Susanne Murphy Resource Consultant, BCICC-LTC & GiiC Screening/Assessment for Delirium,
WEBINAR SERIES: AGING IN INDIVIDUALS WITH INTELLECTUAL AND DEVELOPMENTAL DISABILITIES
 WEBINAR SERIES: AGING IN INDIVIDUALS WITH INTELLECTUAL AND DEVELOPMENTAL DISABILITIES 1 CMS Medicare-Medicaid Coordination Office (MMCO) Established by Section 2602 of the Affordable Care Act Purpose:
WEBINAR SERIES: AGING IN INDIVIDUALS WITH INTELLECTUAL AND DEVELOPMENTAL DISABILITIES 1 CMS Medicare-Medicaid Coordination Office (MMCO) Established by Section 2602 of the Affordable Care Act Purpose:
Managing Pain. in Marfan Syndrome. Traci J. Speed, MD PhD Assistant Professor, Department of Psychiatry and Behavioral Sciences
 Managing Pain in Marfan Syndrome Traci J. Speed, MD PhD Assistant Professor, Department of Psychiatry and Behavioral Sciences No financial disclosures Objectives Define pain Discuss the role of comorbid
Managing Pain in Marfan Syndrome Traci J. Speed, MD PhD Assistant Professor, Department of Psychiatry and Behavioral Sciences No financial disclosures Objectives Define pain Discuss the role of comorbid
Session outline. Introduction to dementia Assessment of dementia Management of dementia Follow-up Review
 Dementia 1 Session outline Introduction to dementia Assessment of dementia Management of dementia Follow-up Review 2 Activity 1: Person s story Present a person s story of what it feels like to live with
Dementia 1 Session outline Introduction to dementia Assessment of dementia Management of dementia Follow-up Review 2 Activity 1: Person s story Present a person s story of what it feels like to live with
Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018
 Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018 Delirium common Prolongs hospitalization Worsens dementia ( if you survive) Increased risk of institutionalization
Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018 Delirium common Prolongs hospitalization Worsens dementia ( if you survive) Increased risk of institutionalization
When is a Psychological Disorder a Disability? Dr. Leigh Ann Ford, PhD, HSP Licensed Psychologist ABVE 2017 Annual Conference. Goals for presentation
 When is a Psychological Disorder a Disability? Dr. Leigh Ann Ford, PhD, HSP Licensed Psychologist ABVE 2017 Annual Conference Goals for presentation *To review DSM-V criteria for some of the most frequently
When is a Psychological Disorder a Disability? Dr. Leigh Ann Ford, PhD, HSP Licensed Psychologist ABVE 2017 Annual Conference Goals for presentation *To review DSM-V criteria for some of the most frequently
GERIATRIC WORKFORCE ENHANCEMENT PROGRAM (GWEP) FACULTY DEVELOPMENT MASTERWORKS SERIES
 FACULTY DEVELOPMENT MASTERWORKS SERIES") UNIVERSITY OF SOUTH FLORIDA GERIATRIC WORKFORCE ENHANCEMENT PROGRAM (GWEP) FACULTY DEVELOPMENT MASTERWORKS SERIES Kathryn Hyer, PhD, MPP Principal Investigator h Providers of Continuing Education For additional
UNIVERSITY OF SOUTH FLORIDA GERIATRIC WORKFORCE ENHANCEMENT PROGRAM (GWEP) FACULTY DEVELOPMENT MASTERWORKS SERIES Kathryn Hyer, PhD, MPP Principal Investigator h Providers of Continuing Education For additional
When Behaviors Become Difficult
 When Behaviors Become Difficult Help me! Help me! Help me! A Problem-Solving Approach Philomena Poole, RN, GNP-BC Prevalence Alzheimer s Disease is the sixth leading cause of death in the US Will affect
When Behaviors Become Difficult Help me! Help me! Help me! A Problem-Solving Approach Philomena Poole, RN, GNP-BC Prevalence Alzheimer s Disease is the sixth leading cause of death in the US Will affect
Chapter 01 Introduction
 Chapter 01 Introduction Defining the Elderly There is no universally accepted age cut-off defining elderly. This reflects the fact that chronological age itself is less important than biological events
Chapter 01 Introduction Defining the Elderly There is no universally accepted age cut-off defining elderly. This reflects the fact that chronological age itself is less important than biological events
Alzheimer Disease and Related Dementias
 Alzheimer Disease and Related Dementias Defining Generic Key Terms and Concepts Mild cognitive impairment: (MCI) is a state of progressive memory loss after the age of 50 that is beyond what would be expected
Alzheimer Disease and Related Dementias Defining Generic Key Terms and Concepts Mild cognitive impairment: (MCI) is a state of progressive memory loss after the age of 50 that is beyond what would be expected
Delirium in the hospitalized patient
 Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
Strategies To Maintain Independence In The Elderly
 Strategies To Maintain Independence In The Elderly Laura Seriguchi, RN Guardian Medical Monitoring, Inc. And in the end, it s not the years in your life that count, it s the life in your years. ABRAHAM
Strategies To Maintain Independence In The Elderly Laura Seriguchi, RN Guardian Medical Monitoring, Inc. And in the end, it s not the years in your life that count, it s the life in your years. ABRAHAM
Delirium in the Emergency Department. Emergency Medicine Rounds April 14, 2015 Paul R. Vanhoutte
 Delirium in the Emergency Department Emergency Medicine Rounds April 14, 2015 Paul R. Vanhoutte Goals of Rounds: Review Definition Management An Understanding What is important is to spread confusion,
Delirium in the Emergency Department Emergency Medicine Rounds April 14, 2015 Paul R. Vanhoutte Goals of Rounds: Review Definition Management An Understanding What is important is to spread confusion,
AACN PCCN Review. Behavioral
 AACN PCCN Review Behavioral Presenter: Carol A. Rauen, RN, MS, CCNS, CCRN, PCCN, CEN Independent Clinical Nurse Specialist & Education Consultant rauen.carol104@gmail.com 0 Behavioral I. INTRODUCTION PCCN
AACN PCCN Review Behavioral Presenter: Carol A. Rauen, RN, MS, CCNS, CCRN, PCCN, CEN Independent Clinical Nurse Specialist & Education Consultant rauen.carol104@gmail.com 0 Behavioral I. INTRODUCTION PCCN
AGED SPECIFIC ASSESSMENT TOOLS. Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services
 AGED SPECIFIC ASSESSMENT TOOLS Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services Issues in assessing the Elderly Association between biological, psychological, social and cultural
AGED SPECIFIC ASSESSMENT TOOLS Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services Issues in assessing the Elderly Association between biological, psychological, social and cultural
Delirium Information for patients and relatives. Delirium is common Delirium is treatable Relatives can stay to help us
 Delirium Information for patients and relatives Delirium is common Delirium is treatable Relatives can stay to help us What is delirium? Delirium is caused by a disturbance of brain function. It is used
Delirium Information for patients and relatives Delirium is common Delirium is treatable Relatives can stay to help us What is delirium? Delirium is caused by a disturbance of brain function. It is used
Delirium A guide for caregivers
 Delirium A guide for caregivers Disclaimer This is general information developed by The Ottawa Hospital. It is not intended to replace the advice of a qualified health-care provider. Please consult your
Delirium A guide for caregivers Disclaimer This is general information developed by The Ottawa Hospital. It is not intended to replace the advice of a qualified health-care provider. Please consult your
Guidelines for the Management of Behavioural and Psychological Symptoms of Dementia (BPSD) Summary document for Primary Care
 Summary document for Primary Care") Guidelines for the Management of Behavioural and Psychological Symptoms of Dementia (BPSD) Summary document for Primary Care Guidelines for the Management of Behavioural and Psychological Symptoms of Dementia
Guidelines for the Management of Behavioural and Psychological Symptoms of Dementia (BPSD) Summary document for Primary Care Guidelines for the Management of Behavioural and Psychological Symptoms of Dementia
BEHAVIORAL PROBLEMS IN DEMENTIA
 BEHAVIORAL PROBLEMS IN DEMENTIA CLINICAL FEATURES Particularly as dementia progresses, psychiatric symptoms may develop that resemble discrete mental disorders such as depression or mania The course and
BEHAVIORAL PROBLEMS IN DEMENTIA CLINICAL FEATURES Particularly as dementia progresses, psychiatric symptoms may develop that resemble discrete mental disorders such as depression or mania The course and
ALZHEIMER S DISEASE, DEMENTIA & DEPRESSION
 ALZHEIMER S DISEASE, DEMENTIA & DEPRESSION Daily Activities/Tasks As Alzheimer's disease and dementia progresses, activities like dressing, bathing, eating, and toileting may become harder to manage. Each
ALZHEIMER S DISEASE, DEMENTIA & DEPRESSION Daily Activities/Tasks As Alzheimer's disease and dementia progresses, activities like dressing, bathing, eating, and toileting may become harder to manage. Each
Mental Health Disorders Civil Commitment UNC School of Government
 Mental Health Disorders 2017 Civil Commitment UNC School of Government Edward Poa, MD, FAPA Chief of Inpatient Services, The Menninger Clinic Associate Professor, Baylor College of Medicine NC statutes
Mental Health Disorders 2017 Civil Commitment UNC School of Government Edward Poa, MD, FAPA Chief of Inpatient Services, The Menninger Clinic Associate Professor, Baylor College of Medicine NC statutes
Understanding Behaviors
 Understanding Behaviors Linda K. Shumaker, R.N.-BC, MA Pennsylvania Behavioral Health and Aging Coalition Causes of Behavioral Problems in Older Adults Psychiatric illness Regressive symptoms of psychiatric
Understanding Behaviors Linda K. Shumaker, R.N.-BC, MA Pennsylvania Behavioral Health and Aging Coalition Causes of Behavioral Problems in Older Adults Psychiatric illness Regressive symptoms of psychiatric
Delirium. A Geriatric Syndrome. Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine
 Delirium A Geriatric Syndrome Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine Introduction Common Serious Unrecognized: a medical emergency
Delirium A Geriatric Syndrome Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine Introduction Common Serious Unrecognized: a medical emergency
THE BEHAVIOURAL VITAL SIGNS (BVS) TOOL
 TOOL") DID YOU KNOW THE BEHAVIOURAL VITAL SIGNS (BVS) TOOL. Did you know that it is essential to know the target cluster(s)/symptom(s) one is treating to guide and monitor non-pharmacological approaches and pharmacological
DID YOU KNOW THE BEHAVIOURAL VITAL SIGNS (BVS) TOOL. Did you know that it is essential to know the target cluster(s)/symptom(s) one is treating to guide and monitor non-pharmacological approaches and pharmacological
Dementia and Fall Geriatric Interprofessional Training. Wael Hamade, MD, FAAFP
 Dementia and Fall Geriatric Interprofessional Training Wael Hamade, MD, FAAFP Prevalence of Dementia Age range 65-74 5% % affected 75-84 15-25% 85 and older 36-50% 5.4 Million American have AD Dementia
Dementia and Fall Geriatric Interprofessional Training Wael Hamade, MD, FAAFP Prevalence of Dementia Age range 65-74 5% % affected 75-84 15-25% 85 and older 36-50% 5.4 Million American have AD Dementia
DELIRIUM DR S A R A H A B D E L A T I S A S DR H I L A R Y W O L F E N D A L E S T 4
 DELIRIUM DR S A R A H A B D E L A T I S A S DR H I L A R Y W O L F E N D A L E S T 4 AIMS Define delirium Identify: Different types of delirium Risk factors Preventable causes Screening tools Management
DELIRIUM DR S A R A H A B D E L A T I S A S DR H I L A R Y W O L F E N D A L E S T 4 AIMS Define delirium Identify: Different types of delirium Risk factors Preventable causes Screening tools Management
Delirium Prevention: The State-of-the-Art & Implications to Improve Care in our State
 Delirium Prevention: The State-of-the-Art & Implications to Improve Care in our State Jonny Macias, MD & Michael Malone, MD Aurora Health Care/ University of Wisconsin School of Medicine & Public Health
Delirium Prevention: The State-of-the-Art & Implications to Improve Care in our State Jonny Macias, MD & Michael Malone, MD Aurora Health Care/ University of Wisconsin School of Medicine & Public Health
Mental Health Nursing: Organic Disorders. By Mary B. Knutson, RN, MS, FCP
 Mental Health Nursing: Organic Disorders By Mary B. Knutson, RN, MS, FCP A Definition of Cognition Mental process characterized by knowing, thinking, learning, and judging Cognitive disorders include delirium
Mental Health Nursing: Organic Disorders By Mary B. Knutson, RN, MS, FCP A Definition of Cognition Mental process characterized by knowing, thinking, learning, and judging Cognitive disorders include delirium
Jacinta Lucke Resident Emergency Medicine PHD Gerontology & Geriatrics
 Jacinta Lucke Resident Emergency Medicine PHD Gerontology & Geriatrics TAKE HOME MESSAGE When managing confusion in older patients: Routinely screen for impaired cognition Patients with impaired cognition
Jacinta Lucke Resident Emergency Medicine PHD Gerontology & Geriatrics TAKE HOME MESSAGE When managing confusion in older patients: Routinely screen for impaired cognition Patients with impaired cognition
Care of Patient with Delirium
 Care of Patient with Delirium Introduction Delirium is an alteration in consciousness involving confusion and other changes in cognitive ability that has a brief duration. 1 Patients specifically at risk
Care of Patient with Delirium Introduction Delirium is an alteration in consciousness involving confusion and other changes in cognitive ability that has a brief duration. 1 Patients specifically at risk
Do you know. Assessment of Delirium. What is Delirium? Which syndrome occurs more commonly in elderly populations? a. Delirium b.
 Assessment of Delirium Marianne McCarthy, PhD, GNP, PMHNP Arizona State University College of Nursing and Health Innovation What is Delirium? Delirium is a common clinical syndrome characterized by: Inattention
Assessment of Delirium Marianne McCarthy, PhD, GNP, PMHNP Arizona State University College of Nursing and Health Innovation What is Delirium? Delirium is a common clinical syndrome characterized by: Inattention
Mental Health: Subjective evaluation of overall quality of life (QOL) Happiness, life satisfaction, morale, trait effect, etc. Quality of Life (QOL)
 Happiness, life satisfaction, morale, trait effect, etc. Quality of Life (QOL)") Mental Health: Subjective evaluation of overall quality of life (QOL) Happiness, life satisfaction, morale, trait effect, etc. Quality of Life (QOL) Multidimensional concept Includes: Physical health Cognitive
Mental Health: Subjective evaluation of overall quality of life (QOL) Happiness, life satisfaction, morale, trait effect, etc. Quality of Life (QOL) Multidimensional concept Includes: Physical health Cognitive
Mental Health Issues in Nursing Homes. I m glad you asked.
 Mental Health Issues in Nursing Homes I m glad you asked. I m glad you asked Susan Wehry, M.D. Associate Professor of Psychiatry, College of Medicine, University of Vermont Consultant, State of Vermont
Mental Health Issues in Nursing Homes I m glad you asked. I m glad you asked Susan Wehry, M.D. Associate Professor of Psychiatry, College of Medicine, University of Vermont Consultant, State of Vermont
Primary Care: Referring to Psychiatry
 Primary Care: Referring to Psychiatry Carol Capitano, PhD, APRN-BC Assistant Professor, Clinical Educator University of New Mexico College of Nursing University of New Mexico Psychiatric Center Objectives
Primary Care: Referring to Psychiatry Carol Capitano, PhD, APRN-BC Assistant Professor, Clinical Educator University of New Mexico College of Nursing University of New Mexico Psychiatric Center Objectives
In-Service Education. workbook 3. by Hartman Publishing, Inc. second edition
 In-Service Education workbook 3 second edition by Hartman Publishing, Inc. Alzheimer s Disease Dignity Diabetes Restraints and Restraint Alternatives Abuse and Neglect Death and Dying Managing Stress Perf
In-Service Education workbook 3 second edition by Hartman Publishing, Inc. Alzheimer s Disease Dignity Diabetes Restraints and Restraint Alternatives Abuse and Neglect Death and Dying Managing Stress Perf
7/3/2013 ABNORMAL PSYCHOLOGY SEVENTH EDITION CHAPTER FOURTEEN CHAPTER OUTLINE. Dementia, Delirium, and Amnestic Disorders. Oltmanns and Emery
 ABNORMAL PSYCHOLOGY SEVENTH EDITION Oltmanns and Emery PowerPoint Presentations Prepared by: Ashlea R. Smith, Ph.D. This multimedia and its contents are protected under copyright law. The following are
ABNORMAL PSYCHOLOGY SEVENTH EDITION Oltmanns and Emery PowerPoint Presentations Prepared by: Ashlea R. Smith, Ph.D. This multimedia and its contents are protected under copyright law. The following are
MOOD (AFFECTIVE) DISORDERS and ANXIETY DISORDERS
 DISORDERS and ANXIETY DISORDERS") MOOD (AFFECTIVE) DISORDERS and ANXIETY DISORDERS Shelley Klipp AS91 Spring 2010 TIP 42 Pages 226-231 and 369-379 DSM IV-TR APA 2000 Co-Occurring Substance Abuse and Mental Disorders by John Smith Types
MOOD (AFFECTIVE) DISORDERS and ANXIETY DISORDERS Shelley Klipp AS91 Spring 2010 TIP 42 Pages 226-231 and 369-379 DSM IV-TR APA 2000 Co-Occurring Substance Abuse and Mental Disorders by John Smith Types
Understanding Mental Illness A Review of the Disorders
 Understanding Mental Illness A Review of the Disorders Objectives Define and describe mental illness To be able to recognize signs, symptoms, and behaviors of the major categories of mental illness Recognition
Understanding Mental Illness A Review of the Disorders Objectives Define and describe mental illness To be able to recognize signs, symptoms, and behaviors of the major categories of mental illness Recognition
9/24/2012. Amer M Burhan, MBChB, FRCP(C)
") Depression and Dementia Amer M Burhan MBChB, FRCPC Head of CAMH Memory Clinic, Toronto Geriatric Neuropsychiatrist Assistant Prof Psychiatry at U of T Objectives Discuss the prevalence and impact of depression
Depression and Dementia Amer M Burhan MBChB, FRCPC Head of CAMH Memory Clinic, Toronto Geriatric Neuropsychiatrist Assistant Prof Psychiatry at U of T Objectives Discuss the prevalence and impact of depression
Communication with Cognitively Impaired Clients For CNAs
 Communication with Cognitively Impaired Clients For CNAs This course has been awarded one (1.0) contact hour. This course expires on August 31, 2017. Copyright 2005 by RN.com. All Rights Reserved. Reproduction
Communication with Cognitively Impaired Clients For CNAs This course has been awarded one (1.0) contact hour. This course expires on August 31, 2017. Copyright 2005 by RN.com. All Rights Reserved. Reproduction
Delirium. Dr. John Puxty
 Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
Table to Demonstrate a method of working through Triggered CAPs.
 CAP Problem Goals Triggers Guidelines Physical Activities increase hours of exercises Reports less than 2 hours Personal choice Promotion and physical activity activity in last 3 days Instrumental Activities
CAP Problem Goals Triggers Guidelines Physical Activities increase hours of exercises Reports less than 2 hours Personal choice Promotion and physical activity activity in last 3 days Instrumental Activities
Introduction to Dementia: Complications
 Introduction to Dementia: Complications Created in March 2005 Duration: about 15 minutes Axel Juan, MD The Geriatrics Institute axel.juan@med.va.gov 305-575-3388 Credits Principal medical contributor:
Introduction to Dementia: Complications Created in March 2005 Duration: about 15 minutes Axel Juan, MD The Geriatrics Institute axel.juan@med.va.gov 305-575-3388 Credits Principal medical contributor:
Delirium. Assessment and Management
 Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
DELIRIUM. Approach and Management
 DELIRIUM Approach and Management By Dr. K.S. Jacob, Professor of Psychiatry and Dr. Anju Kuruvilla, Professor of Psychiatry, Christian Medical College, Vellore. Based on a chapter in the book Psychiatric
DELIRIUM Approach and Management By Dr. K.S. Jacob, Professor of Psychiatry and Dr. Anju Kuruvilla, Professor of Psychiatry, Christian Medical College, Vellore. Based on a chapter in the book Psychiatric
Contemporary Psychiatric-Mental Health Nursing Third Edition. Introduction. Introduction 9/10/ % of US suffers from Mood Disorders
 Contemporary Psychiatric-Mental Health Nursing Third Edition CHAPTER 17 Mood Disorders Introduction 12% of US suffers from Mood Disorders MD are a group of psychiatric DO characterized by physical, emotional
Contemporary Psychiatric-Mental Health Nursing Third Edition CHAPTER 17 Mood Disorders Introduction 12% of US suffers from Mood Disorders MD are a group of psychiatric DO characterized by physical, emotional
Chapter 15: Late Life and Psychological Disorders
 \ Chapter 15: Late Life and Psychological Disorders 1. Ageism refers to a. the physical deterioration that accompanies old age. b. the intellectual deterioration that frequently occurs as a person ages.
\ Chapter 15: Late Life and Psychological Disorders 1. Ageism refers to a. the physical deterioration that accompanies old age. b. the intellectual deterioration that frequently occurs as a person ages.
CAREGIVER SUMMIT. The PD You Can't See: Dealing with Non-Motor Symptoms. Kaitlyn Roland, PhD. Sponsored by:
 CAREGIVER SUMMIT The PD You Can't See: Dealing with Non-Motor Symptoms Kaitlyn Roland, PhD Sponsored by: Cognition VS Dementia Memory Executive Function Attention Bradyphrenia Visuospatial Language Hallucinations
CAREGIVER SUMMIT The PD You Can't See: Dealing with Non-Motor Symptoms Kaitlyn Roland, PhD Sponsored by: Cognition VS Dementia Memory Executive Function Attention Bradyphrenia Visuospatial Language Hallucinations
Palliative Approach to the Person with Advanced Dementia
 Mid North Coast Rural Palliative Care Project Link Nurse Education 2004 Palliative Approach to the Person with Advanced Dementia Anne Sneesby CNC - ACAT To care for the dying is a very human opportunity
Mid North Coast Rural Palliative Care Project Link Nurse Education 2004 Palliative Approach to the Person with Advanced Dementia Anne Sneesby CNC - ACAT To care for the dying is a very human opportunity
Handout 3: Mood Disorders
 Handout 3: Mood Disorders Mood disorders are called affective (emotional) disorders. There are two categories of mood disorders: Depressive Disorders Bipolar Affective Disorders Depressive Disorders Minor
Handout 3: Mood Disorders Mood disorders are called affective (emotional) disorders. There are two categories of mood disorders: Depressive Disorders Bipolar Affective Disorders Depressive Disorders Minor
Every 67seconds, someone will develop Alzheimer's.
 We all need a purpose and responsibilities to live a healthy life. Dementia Care 101 Corrin Campbell BS, COTA/L & Michael Urban, MS, OTR/L, MBA Every 67seconds, someone will develop Alzheimer's. http://www.alz.org
We all need a purpose and responsibilities to live a healthy life. Dementia Care 101 Corrin Campbell BS, COTA/L & Michael Urban, MS, OTR/L, MBA Every 67seconds, someone will develop Alzheimer's. http://www.alz.org
HDSA Annual Convention June 2013 Behavior Issues: Irritability and Depression Peg Nopoulos, M.D.
 HDSA Annual Convention June 2013 Behavior Issues: Irritability and Depression Peg Nopoulos, M.D. Professor of Psychiatry, Neurology, and Pediatrics University of Iowa, Iowa City, Iowa The information provided
HDSA Annual Convention June 2013 Behavior Issues: Irritability and Depression Peg Nopoulos, M.D. Professor of Psychiatry, Neurology, and Pediatrics University of Iowa, Iowa City, Iowa The information provided
Depression in Older Adults. Key Issues
 Depression in Older Adults Key Issues Depression and Older Adults: Key Issues is an overview of important information that you should know about depression in older adults. Depression is one of the most
Depression in Older Adults Key Issues Depression and Older Adults: Key Issues is an overview of important information that you should know about depression in older adults. Depression is one of the most
Recognizing and Managing the Emotional Aspects of Parkinson s. Pamela R. Palmentera, LCSW Coordinator & Clinical Social Worker
 Recognizing and Managing the Emotional Aspects of Parkinson s Pamela R. Palmentera, LCSW Coordinator & Clinical Social Worker Sensory information from the one hemisphere crosses over to the other side
Recognizing and Managing the Emotional Aspects of Parkinson s Pamela R. Palmentera, LCSW Coordinator & Clinical Social Worker Sensory information from the one hemisphere crosses over to the other side
Understanding Dementia
 Dementia Handbook for Carers Essex Understanding Dementia What is dementia? 1 Summary of dementia symptoms 4 Medication and treatment 5 1 Dementia is the name for several conditions that lead to the progressive
Dementia Handbook for Carers Essex Understanding Dementia What is dementia? 1 Summary of dementia symptoms 4 Medication and treatment 5 1 Dementia is the name for several conditions that lead to the progressive
Management of Behavioral Symptoms in Dementia. Brenda Jordan, MS, ARNP, BC- PCM Dartmouth-Hitchcock Kendal
 Management of Behavioral Symptoms in Dementia Brenda Jordan, MS, ARNP, BC- PCM Dartmouth-Hitchcock Kendal Behavioral Symptoms Common & troubling At least one will occur in 61-92% of those with any dementia
Management of Behavioral Symptoms in Dementia Brenda Jordan, MS, ARNP, BC- PCM Dartmouth-Hitchcock Kendal Behavioral Symptoms Common & troubling At least one will occur in 61-92% of those with any dementia
Dementia. Aetiology, pathophysiology and the role of neuropsychological testing. Dr Sheng Ling Low Geriatrician
 Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Major Depression Major Depression
 Contemporary Psychiatric-Mental Health Nursing Third Edition CHAPTER 17 Mood Disorders Major Depression Major Depression Characterized by a change in several aspects of a person s life and emotional state
Contemporary Psychiatric-Mental Health Nursing Third Edition CHAPTER 17 Mood Disorders Major Depression Major Depression Characterized by a change in several aspects of a person s life and emotional state
Delirium in Hospital Care
 Delirium in Hospital Care Dr John Puxty 1 Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors,
Delirium in Hospital Care Dr John Puxty 1 Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors,
Dementia and Delirium
 Dementia and Delirium LPT Gondar Mental Health Group www.le.ac.uk Dementia and Delirium WTINP Chapter 4.6 Introduction - areas to be covered Delirium Definition and causes Clinical features Management
Dementia and Delirium LPT Gondar Mental Health Group www.le.ac.uk Dementia and Delirium WTINP Chapter 4.6 Introduction - areas to be covered Delirium Definition and causes Clinical features Management
If you have dementia, you may have some or all of the following symptoms.
 About Dementia Dementia may be caused by a number of illnesses that affect the brain. Dementia typically leads to memory loss, inability to do everyday things, difficulty in communication, confusion, frustration,
About Dementia Dementia may be caused by a number of illnesses that affect the brain. Dementia typically leads to memory loss, inability to do everyday things, difficulty in communication, confusion, frustration,
Dementia: How to explain the diagnosis to patients and relatives
 GPHot Topics (April 2017): Dementia: How to explain the diagnosis to patients and relatives mohammad somauroo Consultant Physician with specialist interest in Community Geriatrics Royal Liverpool and Broadgreen
GPHot Topics (April 2017): Dementia: How to explain the diagnosis to patients and relatives mohammad somauroo Consultant Physician with specialist interest in Community Geriatrics Royal Liverpool and Broadgreen
Delirium After Cardiac Surgery
 Patient & Family Guide 2016 Delirium After Cardiac Surgery www.nshealth.ca Delirium After Cardiac Surgery Delirium is a common complication after cardiac surgery. This can be stressful for you and your
Patient & Family Guide 2016 Delirium After Cardiac Surgery www.nshealth.ca Delirium After Cardiac Surgery Delirium is a common complication after cardiac surgery. This can be stressful for you and your
10 Facts We All Need to Know About Dementia (MNCD) in Old Age
 in Old Age") 10 Facts We All Need to Know About Dementia (MNCD) in Old Age DUNCAN ROBERTSON FRCP (LOND & EDIN) FRCPC MEDICAL ADVISOR TO ADVANCING DEMENTIA DIAGNOSIS AND MANAGEMENT IN ALBERTA AND PRIMARY HEALTH CARE
10 Facts We All Need to Know About Dementia (MNCD) in Old Age DUNCAN ROBERTSON FRCP (LOND & EDIN) FRCPC MEDICAL ADVISOR TO ADVANCING DEMENTIA DIAGNOSIS AND MANAGEMENT IN ALBERTA AND PRIMARY HEALTH CARE
We Will Discuss. Dementia and Alzheimer s Disease Basics. Dementia. Developmental Disabilities and Dementia: A Behavior Management Guide
 10/18/2013 1 Dayna Thompson M.S., LMHC Alzheimer s Educator Developmental Disabilities and Dementia: A Behavior Management Guide Alzheimer s Resource Service IU Health Bloomington-Community Health 812-353-9299
10/18/2013 1 Dayna Thompson M.S., LMHC Alzheimer s Educator Developmental Disabilities and Dementia: A Behavior Management Guide Alzheimer s Resource Service IU Health Bloomington-Community Health 812-353-9299