Peripheral Sympathetic Nerve Dysfunction in Adolescent Japanese Girls following. Immunization with the Human Papillomavirus Vaccine
|
|
|
- Aleesha Jefferson
- 5 years ago
- Views:
Transcription
1 Peripheral Sympathetic Nerve Dysfunction in Adolescent Japanese Girls following Immunization with the Human Papillomavirus Vaccine Tomomi Kinoshita 1, Ryu-ta Abe 1, Akiyo Hineno 1, Kazuhiro Tsunekawa 2, Shunya Nakane 3, Shu-ichi Ikeda 1 1) Department of Medicine (Neurology and Rheumatology), Shinshu University School of Medicine, Matsumoto , Nagano, Japan, 2) Department of Plastic Surgery, Shinshu University School of Medicine, Matsumoto , Nagano, Japan, 3) Department of Clinical Research, Nagasaki Kawatana Medical Center, Higashisonogigun Kawata-chou, , Nagasaki, Japan Key words: human papillomavirus vaccine, complex regional pain syndrome, orthostatic hypotension, postural orthostatic tachycardia syndrome, sympathetic nerve dysfunction Correspondence to: Shu-ichi Ikeda Department of Internal Medicine (Neurology and Rheumatology), Shinshu University School of Medicine, Asahi, Matsumoto, , Japan. Tel: , Fax: ikedasi@shinshu-u.ac.jp 1
2 Abstract Objectives: To investigate the causes of neurological manifestations in girls immunized with the human papillomavirus (HPV) vaccine. Patients and methods: During the past nine months, 44 girls visited us complaining of several symptoms after HPV vaccination. Four patients with other proven disorders were excluded, and the remaining forty subjects were enrolled in this study. Results: The age at initial vaccination ranged from 11 to 17 years, and the average incubation period after the first dose of the vaccine was months. Frequent manifestations included headaches, general fatigue, coldness of the legs, limb pain and weakness. The skin temperature examined in 29 girls with limb symptoms exhibited a slight decrease in the fingers ( ) and a moderate decrease in the toes ( ). Digital plethysmograms revealed a reduced height of the waves, especially in the toes. The limb symptoms of four girls were compatible with the Japanese clinical diagnostic criteria for complex regional pain syndrome (CRPS), while those in the other 14 girls were consistent with foreign diagnostic criteria for CRPS. The Schellong test identified eight patients with orthostatic hypotension and four patients with postural orthostatic tachycardia syndrome. The girls with orthostatic intolerance and CRPS commonly experienced transient violent tremors and persistent asthenia. 2
3 Electron-microscopic examinations of the intradermal nerves showed an abnormal pathology in the unmyelinated fibers in two of the three girls examined. Conclusions: The symptoms observed in this study can be explained by abnormal peripheral sympathetic responses. The most common previous diagnosis in the studied girls was psychosomatic disease. The social problems of the study participants remained unresolved in that the severely disabled girls stopped going to school. 3
4 Introduction The immunization of adolescent girls with the human papillomavirus (HPV) vaccine was initiated to prevent uterine and cervical cancer (1, 2). The first quadrivalent vaccine (Gardasil -CSL/Merck) was approved in 2006, after which a bivalent vaccine (Cervarix -GSK) was introduced. By the end of 2011, approximately 130 million doses of Gardasil and 44 million doses of Cervarix had been distributed worldwide (according to information from the Ministry of Public Health, Labour and Welfare, Japan; see: In 2010, both vaccines were widely introduced for application in Japanese girls, and starting in April 2013, those 13 to 16 years of age were legally required to undergo vaccination. The introduction of a new vaccine invariably puts focus on its effectiveness as well as safety (3). Adverse events of HPV vaccination commonly include fever, headache and local pain at the injection site. Additionally, a relatively high incidence of chronic limb pain, frequently complicated by violent, tremulous involuntary movements, has been noted in Japanese girls following vaccination. In such cases, severe spontaneous pain affects one or more extremities and is consistently accompanied by coldness of the involved limbs, producing a marked disturbance in daily activities. This condition is thought to be a form of complex regional pain syndrome (CRPS), although this has not yet been 4
5 confirmed. CRPS is usually classified into two forms (4): CRPS-I, which occurs without known nerve injury, and CRPS-II, which includes nerve injury. CRPS-I, previously called reflex sympathetic dystrophy, is infrequently reported in individuals immunized against hepatitis B (5) and rubella (6), although a few cases of CRPS-I following HPV vaccination were recently reported from Australia (7). CRPS is characterized by persistent pain disproportionate to any inciting event and the presence of at least one sign of autonomic dysfunction (8). An abnormal sympathetic response after the initiating injury is generally considered to underlie the pathogenesis of this disorder (9). In order to clarify the cause of serious limb pain in such cases, we examined adolescent Japanese girls who visited us with a possible chief complaint of adverse events after HPV vaccination, paying special attention to the possibility of peripheral sympathetic nerve dysfunction. Patients and methods From June 21 to March 31, 2014, forty four girls visited us complaining of several symptoms after HPV vaccination, including 31 patients with a history of vaccination with Cervarix and 13 with a history of receiving Gardasil. All subjects underwent complete physical and neurological examinations and routine laboratory screening, including measurement of the serum levels of CRP and CK as well as thyroid and 5
6 adrenal gland hormones. If a patient exhibited one or both of the following findings, including hypotension and coldness of the limbs, they were evaluated with the Schellong test and a digital plethysmogram. The Schellong test was performed in conjunction with measurement of the plasma levels of catecholamines. A digital plethysmogram was recorded on the right second finger and right first toe, while checking the patient s skin temperature. In patients with limb weakness, routine motor and sensory nerve conduction studies were performed on the right ulnar and tibial nerves. i) Histopathological and ultrastructural examinations of the intradermal nerves Punch biopsies of the skin were performed. The samples were fixed in 3% glutaraldehyde in 0.1 M cacodylate buffer at a ph of 7.4, postfixed in 1% osmium tetroxide in the same buffer and embedded in epoxy resin. Sections measuring 1 m in thickness were cut, then stained with 1% toluidine blue and examined with light microscopy. Ultrathin sections were then prepared, stained with uranyl acetate and lead citrate and observed under a JEM 1400 electron microscope. ii) Detection of autoantibodies to ganglionic acetylcholine receptor antibodies (gachr) Serum was collected from each of the girls with informed consent. Serum antibodies to gachr were detected using a luciferase immunoprecipitation assay, as 6
7 described elsewhere (10, 11). This assay system can detect be used to autoantibodies against two main subunits, 3 and 4, in human AChR (12). The study protocol was approved by the local ethics committee. Results i) Clinical picture Among the 44 girls examined, four definitely diagnosed as having another disease at different hospitals were excluded, including two patients with systemic lupus erythematosus, one patient with schizophrenia and one patient with measles vaccine-related cerebellitis. The age at initial vaccination among the 40 girls examined ranged from 11 to 17years (average age: years), and the average incubation period after the first dose of vaccine was months. Clinical manifestations of the 40 girls included headaches (n=28, 70%), general fatigue (n=21, 53%), coldness of the legs (n=21, 53%), limb pain (n=20, 50%), limb weakness (n=19, 48%), difficulty in getting up (n=19, 48%), orthostatic fainting (n=17, 43%), a decreased ability to learn (n=17, 43%), arthralgia (n=17, 43%), limb tremors (n=16, 40%), gait disturbances (n=16, 40%), disturbed menstruation (n=14, 35%) and dizziness (n=12, 30%). Headaches and general fatigue were more prominent in the morning, frequently leading 7
8 to difficulty in getting up, while persistent fatigue required a long period of sleep. The most common combination of symptoms was limb coldness, pain, tremors and a gait disturbance. Less frequent but noteworthy complaints included the following: 1. polyarthralgia, primarily involving the wrist, knee and ankle joints, that lasted for several days and subsided spontaneously, although it occasionally recurred; 2. menstrual abnormalities, including amenorrhea for a few months after immunization; 3. a decreased ability to learn associated with reduced memory and concentration at school and/or while doing homework, thus resulting in a poor school record. ii) Representative case reports Case 1 (serial patient number: 37) In August 2013, an 18-year-old woman visited our hospital with complaints of continuous headaches and severe general fatigue. She had received her first dose of Cervarix the first week of August 2011, and a few days later, began to suffer from severe epigastric pain and headaches. She underwent brain magnetic resonance image (MRI) at a local hospital, which showed no abnormalities; however, her headache persisted, accompanied by psychological instability and insomnia. Since she was unable to go to school, she was referred to a mental clinic and diagnosed as being inadaptable. During the first week in October, she received the second dose of the vaccine and her 8
9 epigastric pain and headache worsened; her headache and general fatigue were more remarkable in the morning, and the administration of several types of drugs, including non-steroidal anti-inflammatory drugs (NSAIDs), failed to relieve these symptoms. The patient underwent an endoscopic examination and was given a diagnosis of superficial gastritis, possibly due to psychological stress. In mid-february, 2012, she received the third dose the of vaccine. At that time, her daily activity was severely disturbed by a difficulty in getting up, continuous heavy headaches and general fatigue. Finally, she stopped going to her regular high school and enrolled in a correspondence course at the beginning of May, She was also treated by a psychiatrist; however, her symptoms did not improve. She subsequently underwent detailed gynecological examinations due to the exacerbation of symptoms in the pre-menstrual period, the results of which showed no abnormalities. A few months prior to admission, she began to experience frequent episodes of orthostatic fainting. On a physical examination performed at our hospital, the patient was 146 cm tall and weighed 45 kg. Her pulse rate was 72 beats per minute (bpm), with a blood pressure (BP) of 98/50 mmhg in the sitting position. The findings of general physical and neurological examinations were normal, except for slight tenderness in the left occipital area. Her skin temperature was 23.0 in the right first toe and 28.0 in the right 9
10 second finger at a room temperature of 23.5, and plethysmograms of both toes and fingers disclosed a reduced height of the waves in the toes. The changes in the patient s BP and plasma level of noradrenalin on the Schellong test are presented in Figure 1. She did not exhibit orthostatic hypotension (OH), although the basal plasma level of noradrenalin was low and the increase in the plasma noradrenalin level was poor after changing positions from a supine to sitting position. These symptoms were consistent with the diagnostic criteria for orthostatic dysregulation (OD) proposed by the Japan Paediatric Society (13), including two major symptoms (A and E) and four minor symptoms (b, c, d and e). The oral administration of amezinium metilsulfate (Risumic ) (10 mg, two times per day) relieved all of the patient s symptoms, and her daily activities significantly improved. Case 2 (serial patient number: 14) In November 2013, a 15-year-old girl was referred to our hospital due to continuous headaches, limb pain and a gait disturbance. She had received her first dose of Cervarix at the end of February, 2011 and the third dose at the end of September, Her daily life had remained unchanged for a while; however, at the beginning of June, 2012 she began to complain of sharp pain in the eye balls and double vision, and, in the early morning in mid-july, she fell down after waking up due to left-sided limb 10
11 weakness. She was transferred to an emergency hospital, where her consciousness was found to be clear, and an MRI scan of the brain and routine laboratory tests were all within the normal limits. The left-sided limb weakness recovered, and she was discharged. After this event, she frequently began to skip school due to an uncertain inching pain and clumsy movement in hands, which prevented her from writing or using chopsticks (Fig. 2-A). Additionally, she became very sensitive to sound and skin stimuli, such as touch and using the shower in the bathroom, both of which easily induced a panic state, with involuntary tremulousness of the limbs, and she thus visited several hospitals, where she was given a diagnosis of a psychiatric or anxiety disorder. In early July, 2013, she developed severe anorexia, possibly due to very uncomfortable sensations in the limbs, and was hospitalized for two weeks. Although she was treated for an eating disorder, her condition did not improve, and after discharge, she remained at home. On a physical examination performed at our hospital, the patient was 150 cm tall and weighed 50 kg. Her pulse rate was 80 bpm, with a BP of 90/55 mmhg in the sitting position. Her body temperature was In general, physical findings of coldness in both legs were noted, although the neurological gross power of the limb muscles was normal. However, violent limb tremors were easily elicited whenever an examiner 11
12 touched the patient s thigh or legs. Due to this severe tremulousness, the patient was unable to walk alone. Her skin temperature was 22.2 in the right first toe and 28.4 in the right second finger at a room temperature of 23.5, and plethysmograms of the toe and finger showed markedly reduced heights of the waves (Fig. 3-A). In contrast, the findings of peripheral nerve conduction studies were normal. Surface electromyograms recorded from the involved limbs indicated that the involuntary movements were not tremors, but rather myoclonus (Fig. 4 and 5). The patient s reports of persistent inching pain, sensory changes with hyperesthesia and motor dysfunction with limb weakness and tremulousness, as well as our observation of these findings, were consistent with a diagnosis of CRPS-I, according to the guidelines presented in Table 1B. On the Schellong test, her heart rate and BP changed from 78 bpm and 110/58 mmhg to 102 bpm and 67/48 mmhg, respectively, at eight minutes after standing. She was therefore diagnosed with orthostatic hypotension (OH). The intradermal nerve pathology observed in the first toe and second finger is described in a separate section. The intravenous administration of physiological saline (100 ml) and alprostadil (Liple ; 5 g) was employed to treat the leg coldness. The patient subsequently felt warmness in her limbs and the results of digital plethysmograms exhibited a normal pattern (Fig. 3-B). After discharge, she continued to receive this treatment at her neighboring hospital, 12
13 and the limb tremulousness gradually subsided. In addition, the patient again became able to walk and write (Fig. 2-B) and returned to school three months later. Case 3 (serial patient number: 2) In October 2013, a 13-year-old girl was referred to our hospital due to paroxysmal limb pain with headaches and a gait disturbance. She had a history of surgical removal of a left ovarian tumor at 10 years of age. She received her first dose of Gardasil at the end of June, 2012, and two weeks later, began to suffer from a continuous high fever (39.0~40.0 and headaches. She was evaluated at a local hospital, where no abnormal findings were detected on a routine laboratory examination, endoscopy or CT. Various NSAIDs were prescribed; however, all were ineffective in relieving the patient s symptoms. She was tentatively diagnosed as having a psychosomatic fever and stopped participating in all sport activities on campus. At the end of January, 2013, she received the third dose of the vaccine. Her high body temperature and general malaise gradually resolved; however, paroxysmal limb tremors subsequently appeared, especially while lying down, which caused the patient serious anxiety at night, resulting in insomnia. In early March, 2013, she developed severe limb pain and palpitations; the limb pain restricted her shoulder and thigh movement, sometimes accompanied by temporal paresis of the hands and legs, and the palpitations and chest discomfort were remarkably 13
14 exacerbated when the patient changed from a sitting to standing position. Both conditions resulted in difficulties in writing and walking. The patient s condition was considered to be due to psychosomatic behavior at the hospital and at school. Therefore, she stopped going to school and had stayed home since late April, On a physical examination conducted at our hospital, the patient was 155 cm tall and weighed 51 kg. Her pulse rate was 98 bpm, with a BP of 112/78 mmhg in the sitting position. Her body temperature was 37.1, and her general physical findings were normal. Neurologically, she complained of uncomfortable pain in the legs; however, manual muscle tests, objective sensory examinations and deep tendon reflex studies were all normal. No limb tremors were noted at that time. The patient was able to walk using a handrail for short distances, exhibiting a very unsteady posture that easily led to squatting. The awkward gait appeared to us to be of hysteric origin. Her skin temperature was 29.5 in the right first toe and 32.1 in the right second finger at a room temperature of 23.5, and plethysmograms of both the toes and fingers showed reduced heights of the waves in the toes. On the Schellong test, the patient s heart rate and BP changed from 91 bpm and 105/91 mmhg to 126 bpm and 98/59 mmhg, respectively, at nine minutes after standing. A cardiac scintigram obtained using 123 I-meta-iodobenzylguanidine (MIBG) revealed a reduced uptake of the isotope (Fig. 14
15 6), indicating the loss of post-ganglionic nerve terminals containing noradrenaline (14, 15). She was therefore diagnosed as having CRPS-I and postural orthostatic tachycardia syndrome (POTS) (16) and treated with the oral administration of bisoprolol fumarate (Maintate ) at a dose of 2.5 mg daily. Four months later, her gait improved, and she was able to walk with the use of stick, although she did not return to her previous school life. Case 4 (serial patient number: 24) In December 2013, a 16-year-old girl was referred to our hospital due to polyarthralgia, leg pain and weakness. She had a history of bronchial asthma and atopic dermatitis in childhood. She received the first dose of Cervarix in early October, 2011 and the third dose in early March, One month later, she noticed knee joint pain and general fatigue, with a slightly elevated body temperature. She visited a few orthopedic clinics, failing to obtain a definitive diagnosis. The arthralgia moved to other joints, and the patient began to suffer from paroxysmal limb tremulousness in autumn of that year. In early January 2013, she developed severe aching in both calves that resulted in the need for a wheelchair. She was examined at a local hospital, where positive anti-cardiolipin antibodies were detected in the serum (17 U/mL, normal 10 U/mL). Treatment with prednisolone (10 mg/day) and clopidogrel sulfate (Plavix ; 75 mg/day) was started; however, all of the patient s symptoms persisted and she stopped 15
16 going to school. On a physical examination conducted at our hospital, the patient was 157 cm tall and weighed 69 kg. Her pulse rate was 78 bpm, with a BP of mmhg in the sitting position. She exhibited reddish skin with dryness on the cheek and limbs, possibly due to atopic dermatitis. Additionally, she complained of mild tenderness without swelling in the shoulder, elbow, wrist, knee and ankle joints, and a similar degree of pain was evoked in both calves by grasping. On a neurological examination, the patient s limb power and sensations were all normal; however, she was unable to walk by herself and was thus confined to a wheelchair. Her skin temperature was 31.2 in the right first toe and 31.4 in the right second finger at a room temperature of 24.5, and plethysmograms of both the toes and fingers showed reduced heights of the waves. On the Schellong test, severe OH was induced; 10 minutes after standing, she fainted with pallor (her BP decreased from mmhg to mmhg). On laboratory tests, the serum CRP level was 0.20 mg/dl and the serum CK level was 47 IU/L. In addition, the serum titer of anti-cardiolipin antibodies was 10 U/mL (normal 10 U/mL), whereas other auto-antibodies, including rheumatoid factor and anti-double strand DNA antibodies, were undetectable. Although a needle electromyogram showed normal patterns in both the upper and lower limbs, MRI disclosed an abnormal high 16
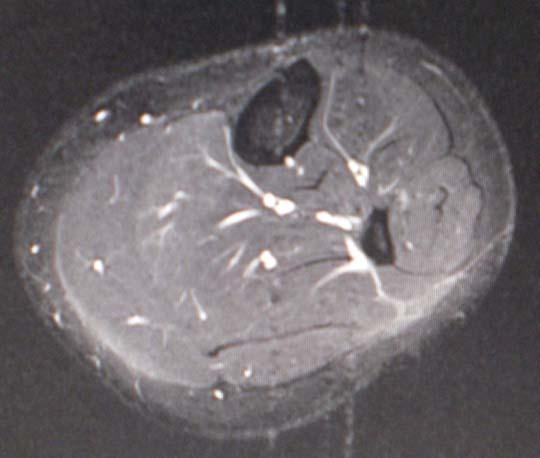
17 signal intensity in both calves (Fig. 7-A), indicating the presence of myofasciitis. Two weeks after discontinuing the dose of clopidogrel sulfate, the patient again underwent MRI of the legs and a muscle biopsy of the left gastrocnemius, which showed that the abnormal signals had disappeared (Fig. 7-B) and the histology of the muscle was normal. The intradermal nerve pathology observed in the same leg area is described in a separate section. The patient was therefore diagnosed as having CRPS-I and OH and was transferred to another hospital for gait rehabilitation. Case 5 (serial patient number: 19) In February 2014, a 15-year-old Japanese girl visited our hospital complaining of transient limb weakness and orthostatic fainting. At the beginning of May, 2010, she had received her first dose of Gardasil in a clinic in the USA since she was living there at the time. In early December, 2010, she received the third dose of the vaccine. A few days later, she felt pain in the lower limbs, especially in the left leg, leading to difficulty in walking. This symptom subsided within the following three days; however, after one month, she developed numbness and weakness in both hands that lasted for two days. Transient weakness repeatedly appeared in both the hands and legs, and the patient subsequently experienced orthostatic fainting and abdominal discomfort. She returned to Japan in April 2012 and was examined at a local hospital, where no specific findings 17
18 were noted. In addition to recurrent limb weakness, the patient newly exhibited a decreased ability to learn at school; she was unable to memorize different themes simultaneously and her understanding of textbooks was incomplete, both of which were noticed by her mother. The patient and her family were seriously worried about her symptoms. On a physical examination conducted at our hospital, the patient was 162 cm tall and weighed 47 kg. Her pulse rate was 74 bpm, with a BP of mmhg in the sitting position. Her general physical findings were normal, although a neurological examination showed slight weakness in both hands and the left leg (grip power: 18 kg in the right hand; 10 kg in the left hand). Her skin temperature was 21.8 in the right first toe and 31.1 in the right second finger at a room temperature of 27.0, and plethysmograms of both the toes and fingers showed reduced heights of the waves in the toes. The findings of peripheral nerve conduction studies of the left median and tibial nerves were normal. On the Schellong test, the patient s heart rate and BP changed from 70 bpm and 105/62 mmhg to 109 bpm and 102/52 mmhg, respectively, at seven minutes after standing. The WAIS-III disclosed the following scores: FIQ= 82, VIQ= 88, PIQ= 79, VC= 92, PO= 70, WM= 85, AS= 105. Furthermore, the patient had remarkable difficulty in quickly understanding long sentences. She was therefore 18
19 diagnosed with CRPS-I and POTS, and her slight cognitive decline was thought to be potentially related to POTS. She was treated with the oral administration of limaprost alfadex at a dose of 5 mg (Opalmon ) three times daily, and her limb symptoms disappeared. iii) Schellong test and the plasma levels of noradrenalin Twenty-one girls underwent these examinations. OH was defined as a decrease of more than 20 mmhg in systolic blood pressure and/or 5 mmhg in diastolic blood pressure within a few minutes after standing (17). POTS was defined as an increase in heart rate of more than 30 bpm within the first 10 minutes of standing or tilting the head upwards (16). Since the plasma levels of noradrenalin have been reported to increase approximately 60~120% when changing from a reclining to standing position in normal subjects (18), patients who exhibited an elevation of less than 60% within five minutes were classified as having an abnormal response in this study. OH was detected in eight patients, two of whom demonstrated orthostatic syncope during testing. POTS was noted in the four other girls. A low response in the plasma level of noradrenalin to postural change was seen in 10 girls, including four with OH and one with POTS (Table 2). iv) Skin temperature and plethysmogram of the right first toe and right second finger 19
20 The skin temperature was examined in 29 girls; the average temperature of the right second finger was , while that of the first right toe was There is no standard diagnostic criterion for diagnosing a diminished skin temperature; therefore, a value below room temperature was judged to be abnormal. The digital plethysmogram findings were evaluated according to the classification of the wave pattern, as follows (19): peripheral plateau pattern involving a reduced height of the waves in the right second finger, as detected in 12 girls, and a peripheral plateau pattern in the first right toe, as observed in 19 girls (Table 3). v) Evaluation of CRPS The diagnosis of CRPS was made based on the patient s history and clinical examination findings in reference to two different sets of diagnostic criteria: the Japanese clinical diagnostic criteria proposed by the research community in 2008 (20)(Table 1A), and the criteria used widely in foreign countries (8)(Table 1B), the recent revision of the International Association for the Study of Pain (IASP) criteria for CRPS originally described in 1999 (21). The limb symptoms were compatible with the Japanese criteria for CRPS in four girls and the foreign diagnostic criteria for CRPS in the remaining 14 girls (Table 4). Limb pain, paresis, tremulousness and gait disturbances were common manifestations in the girls diagnosed based on the revision 20
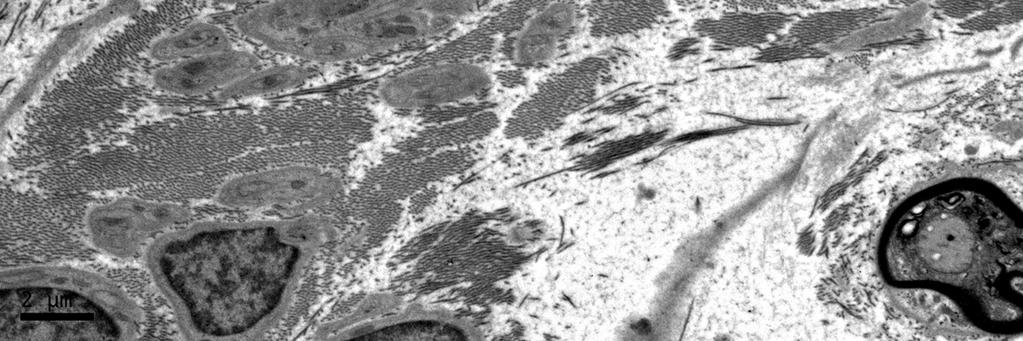
21 of the IASP criteria. Meanwhile, the girls who displayed these symptoms in addition to abnormal sweating fulfilled the Japanese criteria. vi) Skin biopsy findings Biopsies were performed in three girls, including the above Cases 2 and 4 and serial patient No. 18. The skin sample of the first toe obtained from the third girl with CRPS-I lacked any signs of pathological findings. For example, on the light microscopic examination, three small nerve fascicles were identified in one skin sample (Fig. 8-A). Some nerve fascicles were located near apocrine glands (Fig. 8-B), where sudomotor autonomic unmyelinated nerves were surmised to be present. On the electron microscopic examinations, one fascicle was found to consist of a small number of myelinated nerve fibers (most of them being less than 5 m in diameter) and a large number of unmyelinated nerve fibers. In Case 2, skin samples were harvested from the first toe and second finger. On light microscopic observation, these samples commonly displayed endoneurial edema (Fig. 8-C and D), which was more remarkable in the toe samples (Fig. 8-D). On electron microscopic observation, the finger skin contained well-preserved numbers of both myelinated and unmyelinated nerve fibers, although electron-dense coarse granular materials were seen in some axons of the unmyelinated nerve fibers (Fig. 9), reflecting degenerative changes. In the toe skin, spaces without 21
22 any structures occupied a significant portion of the endoneurium, indicating endoneurial edema (Fig. 10-A), and the number of unmyelinated nerve fibers was markedly decreased, accompanied by denervated parallel Schwann cell processes and increased collagen pockets (Fig. 10-B). Similar changes in intradermal nerves were noted in the calf skin obtained during the muscle biopsy in Case 4 (Figure 11). vii) Detection of autoantibodies to gachr All 14 girls who exhibited sympathetic dysfunction showed negative findings in these examinations. viii) Final diagnosis Our final diagnoses in the 40 girls examined are shown in Table 5. Twenty-nine girls were classified into our categorized diagnoses, while the remaining 11 were given a tentative diagnosis based on their symptoms and/or manifestations. The latter group consisted of three patients with a simple headache, three patients with polyarthritis, two patients with OD-like symptoms, one patient with lumbosacral pain, one patient with easy fatigability, chest discomfort and limb tremulousness and one patient with a fever, headache and upper limb paresthesia. Discussion 22
23 In the US, the routine vaccination of girls 11 to 12 years of age using three doses of Gardasil began on June 1, 2006, and by December 31, 2008, more than 23 million Gardasil doses had been administered. During these 2.5 years, the Vaccine Adverse Event Reporting System (VAERS) received 12,424 reports of adverse events following immunization (AEFI), for a rate of 53.9 reports per 100,000 doses. A total of 772 reports (6.2% of all reports) were judged to involve serious AEFI cases, including 32 reports of death (3). The rate of reporting per 100,000 vaccine doses was 8.2 for syncope, 7.5 for local site reactions, 6.8 for dizziness, 5.0 for nausea, 4.1 for headache, 3.1 for hypersensitivity reactions, 2.6 for urticaria, 0.2 for venous thromboembolic events, autoimmune disorders and Guillain-Barré syndrome, 0.1 for anaphylaxis and death, 0.04 for transverse myelitis and pancreatitis and for motor neuron disease. A high frequency of syncope was observed immediately after injection (23). In Japan, a total of 8.75 million doses, in which Cervarix predominated, were used during the past three years (according to information obtained from the Ministry of Public Health, Labour and Welfare, Japan; see: Although similar public reports are not available in Japan, mass media largely reported that a significant number of Japanese girls suffered from severe spontaneous limb pain frequently accompanied by involuntary tremulous movements of the involved limbs 23
24 and/or gait disturbances following vaccination. Recently, a social community has been established for these girls in Tokyo, where information concerning more than 230 affected girls has been collected (antihpvvaccine@yahoo.co.jp). Such neurological manifestations have not been previously experienced at our hospital and we therefore investigated the pathogenesis of this unique disorder in this study. i) CRPS CRPS is characterized primarily by pain (with allodynia and hyperpathia), vasomotor changes, edema and a decreased range of motion (4). CRPS-I is being increasingly recognized in children and adolescents (23), with clinical features that are generally compatible with those observed in adults affected by this syndrome, including a female preponderance, with the highest incidence of disease around puberty and the lower extremities more often being involved. In this study, the diagnosis of CRPS was made based on the patient s history and clinical examination findings in reference to two different sets of diagnostic criteria: the Japanese clinical diagnostic criteria proposed by the research community (20) and the recent revision of the IASP criteria (8). The former set of criteria requires the detection of more diagnostic hallmarks. Our series of girls with chronic limb pain commonly showed a decreased skin temperature and abnormal digital plethysmogram findings, both of which indicate an impaired 24
25 vasomotor tone in the affected limbs. Among these patients, only four fulfilled the Japanese diagnostic clinical criteria for CRPS-I, while the remaining 14, who lacked signs of sweating abnormalities, skin color changes and/or trophic changes, were diagnosed with CRPS-I based on the foreign diagnostic criteria. Concerning the pathogenesis of CRPS, cold skin is thought to be the result of vasospasms caused by sympathetic denervation supersensitivity (9), and the presence of electron microscopic abnormalities in peripheral nerves supports this hypothesis. For example, the loss of small-diameter unmyelinated fibers (C-fibers) is the only finding observed in the sural nerves (24, 25), and one quantitative analysis of epidermal neurite density revealed reduced (on average by 29%) axonal densities at CRPS-affected sites in the limbs (26). Additionally, an intact population of large myelinated fibers was observed in the examined nerves in that study, explaining why the conduction velocities of neurophysiological peripheral nerves are normally preserved in the involved limbs. Among our 18 girls with a confirmed diagnosis of CRPS-I who underwent neurophysiological studies, none showed abnormal electromyography or conduction velocity findings. Our morphologic study results for the intradermal nerves obtained from affected limbs that showed endoneurial edema and selective degeneration of unmyelinated fibers coincided well with the findings mentioned above. 25
26 One important disease that must be differentiated from CRPS-I in vaccinated patients is macrophagic myofasciitis (27, 28). This disorder develops as an unusual reaction to the intramuscular injection of aluminium-containing vaccines and is characterized by common manifestations of diffuse myalgia and arthralgia, as well as elevated levels of serum CK and CRP. In our series of girls, two demonstrated myalgia and grasping pain in the calves, and MRI disclosed abnormal signals in the involved muscles. However, the serum levels of CRP and CK were normal in both girls, and it was confirmed in the present Case 4 that the calf lesions on MRI spontaneously disappeared within a short period and that the histology of the involved muscle showed no inflammation. Such muscular lesions appear to reflect transient vasogenic edema caused by neurogenic dysregulation, and the histological findings of intramuscular edema with degeneration have been previously reported in one patient with reflex sympathetic dystrophy (29). ii) Orthostatic intolerance Orthostatic intolerance can be classified into four different conditions (30), including idiopathic orthostatic hypotension (IOH) and similar conditions associated with neurological disorders. The latter group is further divided into two diverse forms: peripheral sympathetic neuropathy and central nervous system defects in the 26
27 sympathetic nerve activity. The fourth type is POTS. IOH and its related disorder, OD, are recognized to cause a variety of symptoms, such as recurrent dizziness, chronic fatigue, headaches and syncope, in school-aged children and adolescents (13). Approximately 80% of our affected girls had chronic headaches, which may have been causally related to IOH or OD in 67% of cases. Among these cases, Case 1 was the first in which all of the patient s symptoms could be attributed to OD. In addition, the patient s peripheral sympathetic nerve response based on variations in the plasma noradrenalin level during position changes was inadequate (31). POTS is a disorder of the autonomic nervous system that develops in adolescents and young people, with females being predominant. The orthostatic symptoms of POTS include lightheadedness, visual blurring or tunneling, palpitations, tremulousness and weakness, especially in the legs. Symptoms such as hyperventilation, anxiety, chest wall pain, acral coldness and pain occur less frequently (16, 32). Orthostatic stress can easily evoke intense fear or panic in some predisposed individuals (32). It is also noted that there is a considerable overlap between POTS and chronic fatigue syndrome (33), and patients with both disorders have been reported to complain of cognitive impairments, low energy and/or pronounced sleep disturbances, with the inability to complete normal educational activities or occupational duties (34). These symptoms are so severe that the 27
28 lives of the patients and their families are seriously disrupted. However, these complicated conditions are not widely recognized among physicians or pediatric specialists, and many patients are misdiagnosed as having psychiatric diseases (34). The present Cases 2 and 3, which involved orthostatic intolerance, are representative in that the patients were not adequately diagnosed and/or treated at previous institutes. For example, the visual symptoms and occurrence of transient left hemiparesis just after waking up seen in Case 2 may be caused by OH, while the chest discomfort and psychological symptoms noted in Case 3 may be produced by POTS. Additionally, the patient in Case 5, with a confirmed diagnosis of CRPS-I and POTS, exhibited slight cognitive decline, as shown on a conventional WAIS examination. Similar information regarding a decreased ability to learn was collected from 40% of the patients in our series. Concerning the causative relationship between the above sympathetic nerve-mediated manifestations and the use of HPV vaccines, our patients had three main disorders, including CRPS-I, OH and POTS. OH is well known to develop spontaneously in many adolescent girls; however, OH was accompanied by CRPS-I in the present study. The combination of both disorders is rarely seen in the normal population of adolescent Japanese girls. Another orthostatic intolerance disorder, POTS, 28
29 is classified as an attenuated form of acute autonomic neuropathy or acute pandysautonomia (35), and an autoimmune origin has been implicated in the pathogenesis of this disease. For example, viral infections very occasionally precede the onset of symptoms (16, 35), and the Mayo clinic s experience with 152 patients with POTS found that 90.5% of the patient s had a history of an antecedent viral infection (32). In addition, an interesting case of a patient who developed POTS after vaccination with Gardasil was recently reported from the US (36). In contrast, four of the present girls, including those in Cases 3 and 5, who were shown to have POTS, lacked any antecedent viral infections; therefore, a possible predisposing factor was HPV vaccination. iii) Movement disorders One initial adverse event seen in post-vaccinated Japanese girls that was also noticed by mass media was violent limb tremulousness and bizarre gait disturbances. CRPS is known to be accompanied by various neurologic manifestations, including limb paresis, incoordination, tremors, myoclonus and dystonia (37). Similarly, tremulousness and limb weakness are frequently observed in patients with POTS (38). These involuntary movements can be diminished or abolished by successful sympathetic blockade; thus, increased peripheral afferent input associated with 29
30 overactivity of the peripheral sympathetic nervous system appears to play an important role in the pathogenesis of this condition (34, 35). Denervated supersensitivity of peripheral adrenoreceptors is another candidate inducing the above abnormal movements (16, 25). The violent limb tremulousness observed in the affected girls temporally appeared in the early stage of the disease. Electromyograms recorded in our Case 2 indicated that the involuntary movements closely resembled myoclonus (39) and may be induced peripherally, since the myoclonic electromyographic discharge was not associated with any preceding electroencephalographic activity (40). Concerning gait disturbances, symptoms such as limb pain, tremulousness and weakness are thought to be responsible. The limb weakness noted in 15 of our girls was disproportionate to the patient s muscle strength on manual muscle testing and attributable to disturbed neural control of the voluntary movement system, including the pyramidal tract and peripheral somatic motor nerves. It is therefore supposed that the limb weakness was initially related to CRPS or POTS and later enhanced by psychosomatic conditions, such as severe anxiety and/or prolonged asthenia. Consequently, 13 of our 15 girls with gait disturbances discontinued their normal school lives. A decreased ability to learn and/or not attending school among post-vaccinated girls is an important social problem. 30
31 iv) Etiology It has been reported that some autoimmune neurological diseases have developed in post-vaccinated girls, including Guillain-Barré syndrome (3), acute disseminated encephalomyelitis (41) and multiple sclerosis (42, 43). Among these patients, 69 treated with Gardasil vaccination who subsequently developed Guillain-Barré syndrome were collected in the United States between 2006 and 2009 (44). The onset of symptoms was within six weeks after vaccination, and the estimated weekly rate of reporting of post- Gardasil Guillain-Barré syndrome within the first six weeks (6.6 per 10,000,000) was higher than that observed in the general population. Although CRPS is not generally accepted to be an autoimmune disorder, our patients with proven CRPS-I concomitant with OH or POTS had evidence of post-ganglionic sympathetic neuropathy, such as a decreased plasma level of noradrenalin (31), abnormal MIBG cardiac scintigram findings, as observed in the present Case 3 (14, 15), and an ultrastructural pathology of intradermal unmyelinated nerve fiber degeneration, all of which support that this condition is a form of autonomic neuropathy. Furthermore, POTS is now regarded to be an immune-mediated disorder (32). Based on the temporal relationship between immunization and the development of symptoms, we cannot deny the possibility that immunization with HPV vaccines may secondarily induce sympathetically mediated 31
32 disorders, including CRPS-I, OH and POTS. Recently, the presence of gachr antibodies in the serum has been noted to be involved in the pathogenesis of various autonomic disorders (45). Such antibodies act against neuronal acetylcholine receptors in the autonomic ganglia and are frequently found in patients with autoimmune autonomic ganglionopathy. Additionally, two rare cases of Rasmussen encephalitis with 7 AChR antibodies have been reported (46). It has also been reported that a low titer of gachr antibodies is detected in the serum in a small number of patients with POTS (32). In contrast, this autoantibody was undetectable in 14 of our girls, including four with POTS. The negative findings observed in our series of girls with autonomic symptoms indicates that the post-ganglionic peripheral sympathetic nerve lesions produced autonomic dysfunction in these cases. Finally, the above peripheral sympathetic nerve disorders have not been reported in foreign cohort studies of human HPV vaccines (47, 48) and it thus remains unclear why Japanese girls are more frequently involved. It is unlikely that the Japanese environment plays a role in the pathogenesis of this unique autonomic disorder, as the patient in our Case 5, who received vaccination in the USA, developed similar adverse reactions. Studies with large-scale investigations and experimental approaches are needed to further answer these questions. 32
33 Acknowledgement We are most grateful to Ms. Misuzu Kurashina at our department for her assistance, Miss Sakiko Ishihara at the Department of Rehabilitation in our hospital for conducting the WAIS examination. This work was supported by a grant from the Neuroimmunological Disease Division, Ministry of Public Health, Labour and Welfare, Japan and a Health and Labour Science Research Grant on Intractable Diseases (Pathogenesis and Diagnostic Accuracy of Neuropathic Pain, to S.I.) from the Ministry of Public Health, Labour and Welfare, Japan. 33
34 References 1. The future II study group. Quadrivalent vaccine against human papillomavirus to prevent high-grade cervical lesions. N Engl J Med 2007;356: Jeurissen S, Makar A. Epidemiological and economic impact of human papillomavirus vaccines. Int J Gynelogical Cancer 2009;19: Slade BA, Leidel L, Vellozzi C, Woo EJ, Hua W, Sutherland A, Izurieta HS, Ball R, Miller N, Braun MM, Markowitz LE, Iskander J. Postlicensure safety surveillance for quadrivalent human papillomavirus recombinant vaccine. JAMA 2009;302: Stanton-Hicks M, Jänig W, Hassenbusch S, Haddox JD, Boas R, Wilson P. Reflex sympathetic dystrophy: changing concepts and taxonomy. Pain 1995;63: Jastaniah WA, Dobson S, Lugsdin JG, et al. Complex regional pain syndrome after hepatitis B vaccine. J Pediatr 2003;143: Genc H, Karagoz A, Saracoglu M, et al. Complex regional pain syndrome type-i 34
35 after rubella vaccine. Eur J Pain 2005;9: Richards S, Chalkiadis G, Lakshman R, Buttery JP, Crawford NW. Complex regional pain syndrome following immunisation. Arch Dis Child 2012;97: Harden RN, Bruehl S, Stanton-Hicks M, et al. Proposed new diagnostic criteria for complex regional pain syndrome. Pain Med 2007;8: Kurvers HAJM, Jacobs MJHM, Beuk RJ, et al. Reflex sympathetic dystrophy: evolution of microcirculatory disturbance in time. Pain 1995;60: Burbelo et al. Antibody Profiling by Luciferase Immunoprecipitation Systems (LIPS). J. Vis. Exp. 32; e1549: Higuchi O, Hamuro J, Motomura M, Yamanashi Y. Autoantibodies to low-density lipoprotein receptor-related protein 4 in myasthenia gravis. Ann Neurol 2011;69: Skok MV, Voitenko LP, Voitenko SV, et al. Alpha subunit composition of nicotinic acetylcholine receptors in the rat autonomic ganglia neurons as determined with subunit-specific anti-alpha ( ) peptide antibodies. Neuroscience 1999;93: Tanaka H, Fujita Y, Takenaka Y, et al. Japanese clinical guidelines for juvenile orthostatic dysregulation version 1. Pediatr Int 2009;
36 14. Orimo S, Ozawa E, Nakade S, Sugimoto T, Mizusawa H. 123 I-meta-iodobenzylguanidine scintigraphy in Parkinson s disease. J Neurol Neurosurg Psychiatry 1999;67: Orirmo S, Amino T, Itoh Y, et al. Cardiac sympathetic denervation precedes neuronal loss in the sympathetic ganglia in Lewy body disease. Acta Neuropathol 2005;109: Low PA, Opfer-Gehrking TL, Textor SC, et al. Postural tachycardia syndrome (POTS). Neurology 1995;45 (suppl 5):S19-S American autonomic society. Consensus statement on the definition of orthostatic hypotension, pure autonomic failure and multiple system atrophy. Clin Auton Res 1996;6: Ziegler MG, Lake CR, Kopin IJ. The sympathetic-nervous-system defect in primary orthostatic hypotension. N Engl J Med 1977;296: S. Okubo. Digital plethysmogram. In: Kanai s Manual of Clinical Laboratory Medicine. 31 st ed. Kanai Eds. Kanahara Publisher, Tokyo, 1998: (in Japanese). 20. M. Shibata. Japanese diagnostic hallmark for CRPS. In: CRPS (complex regional pain syndrome). Mashimo T, Shibata M Eds. Medical publisher division of Shinkou 36
37 Koueki Co., Tokyo, 2009:68 (in Japanese) 21. Bruehl S, Harden RN, Galer BS, et al. Extensive validation of IASP diagnostic criteria for Complex Regional Pain Syndrome and proposed research diagnostic criteria. Pain 1999;81: Mosnaim AD, Abiola R, Wolf ME, Perlmuter LC. Etiology and risk factors for developing orthostatic hypotension. Am J Therap 2010;17: Wilder RT. Management of pediatric patients with complex regional pain syndrome. Clin J Pain 2006;22: Ochoa JL, Yarnitsky D. The triple cold syndrome. Cold hyperalgesia, cold hypoaesthesia and cold skin in peripheral nerve disease. Brain 1994;117: Van der Laan L, ter Laak HJ, Gabreëls-Festen A, Gabreëls F, Goris RJA. Complex regional pain syndrome type I (RSD). Pathology of skeletal muscle and paripheral nerve. Neurology 1998;51: Oaklander AL, Rissmiller JG, Gelman LB, Zheng L, Chang Y, Gott R. Evidence of focal small-fiber axonal degeneration in complex regional pain syndrome-i (reflex sympathetic dystrophy). Pain 2006;120: Gherardi RK, Coquet M, Bélec L, et al. Macrophagic myofasciitis: a reaction to intramuscular injections of aluminium-containing vaccines [abstract]. J Neurol 37
38 1999; 246 Suppl 1: I/ Authier F-J, Cherin P, Creange A, et al. Central nervous system disease in patients with macrophagic myofasciitis. Brain 2001;124: Kirsch K. Das Sudeck-Syndrom als Fernstorung (Kliniek und Histologie). Z Orthop 1966;116: Polinsky RJ, Ebert MH, Weise V. Pharmacologic distinction of different orthostatic hypotension syndrome. Neurology 1981;31: Suzuki T, Higa S, Sakoda S, et al. Orthostatic hypotension in familial amyloid polyneuropathy: treatment with DL-threo-3, 4-dihydroxyphenylserine. Neurology 1981;31: Thieben MJ, Sandroni P, Sletten DM, et al. Postural orthostatic tachycardia syndrome: the Mayo clinic experience. Mayo Clin Proc 2007;82: Stewart JM. Autonomic nervous system dysfunction in adolescents with postural orthostatic tachycardia syndrome and chronic fatigue syndrome is characterized by attenuated vagal baroreflex and potentiated sympathetic vasomotion. Pediatr Res 2000;48: Karas B, Grubb BP, Boeth K, Kip K. The postural orthostatic tachycardia syndrome: a potentially treatable cause of chronic fatigue, exercise intolerance, and 38
39 cognitive impairment in adolescents. PACE 2000;23: Schondorf R, Low PA. Idiopathic postural orthostatic tachycardia syndrome: an attenuated form of acute pandysautonomia?. Neurology 1993;43: Blitshteyn S. Postural tachycardia syndrome after vaccination with Gardasil. Eur J Neurol 2010;17:e Schwartzman RJ, Kerrigan J. The movement disorder of reflex sympathetic dystrophy. Neurology 1990;40: Jankovic J. Post-traumatic movement disorders: central and peripheral mechanisms. Neurology 1994;44: Shibasaki H, Motomura S, Yamashita Y, Shii H, Kuroiwa Y. Periodic synchronous discharge and myoclonus in Creutzfeldt-Jakob disease: diagnostic application of jerked locked averaging method. Ann Neurol 1981;9: Shibasaki H, Sakai T, Nishimura H, et al. Involuntary movements in chorea-acanthocytosis: acomparison with Huntington s chrorea. Ann Neurol 1982;12: Wildemann B, Jarius S, Hartmann M, Regula JU, Hametner C. Acute disseminated encephalomyelitis following vaccination against human papilloma virus. Neurology 2009;72:
40 42. Sutton I, Lahoria R, Tan IL, Clouston P, Barnett MH. CNS demyelination and quadrivalent HPV vaccination. Mult Scler 2009;15: Chang J, Campagnolo, Vollmer TL, Bomprezzi R. Demyelinating disease and polyvalent human papilloma virus vaccination. J Neurol Neurosurg Psychiatry 2011;82: Souayah N, Michas-Martin PA, Nasar A, et al. Guillain-Barré syndrome after Gardasil vaccination: data from vaccine adverse event reporting system Vaccine 2011;29: Vernino S, Lindstrom J, Hopkins S, et al. Characterization of ganglionic acetylcholine receptor autoantibodies. J Neuroimmunol 2008;197: Watson R, Jepson JE, Bermudez I, et al. Alpha 7-acetylcholine receptor antibodies in two patients with Rasmussen encephalitis. Neurology 2005;65: Gasparini R, Bonanni P, Levi M, et al. Safety and tolerability of bivalent HPV vaccine. An Italian post-licensure study. Hum Vaccin 2011;7 (Suppl): Arnheim-Dahiström L, Pasternak B, Svanström H, Hviid A. Autoimmune, neurological, and venous thromboembolitic adverse events after immunization of adolescent girls with quadrivalent human papillomavirus vaccine in Denmark and Sweden: cohort study. BJM 2013;347:f5906 doi: /bmj.f
41 49. Glycogen. In: A Textbook of HISTOLOGY 9 th edition. Bloom W, Fawcett DW Eds. WB Saunders, Philadelphia 1968:53. Figure legends Figure 1. Changes in blood pressure and the plasma level of noradrenalin on the Schellong test in Case 1. OH was not detected; however, the basal plasma level of noradrenalin was below the normal range, and the increase in the plasma concentration of noradrenalin during positional changes (57% increase at five minutes after standing) was low. Figure 2. Impaired writing of letters in Case 2. A: On admission, the patient s writing was poor due to hand tremulousness. The irregular lines are noteworthy. B: After treatment, the patient s writing improved considerably. Permission for presentation of these images was obtained from the girl and her parents. Figure 3. Digital plethysmograms in Case 2. A&B: On admission, C&D: After intravenous injection of Liple. On admission, digital plethysmograms showed a peripheral plateau pattern, with the height of wave for the toe 41
42 being very low. After treatment, the pattern of waves normalized, and the skin temperature of the toe dramatically increased. ST is an abbreviation for skin temperature. Figure 4. Figure. Surface electromyograms of the involved right upper and lower limbs in Case 2. Repetitive bursts appear at irregular intervals and the muscle contractions are not synchronous with each other, indicating that the involuntary movement is a myoclonic jerk. Figure 5. Polygraph (EEG and EMG) in Case 2. The myoclonic EMG discharge of the left biceps muscle is not associated with any particular EEG activity. EEG is an abbreviation for electroencephalogram and EMG is an abbreviation for electromyogram. Figure 6. MIBG cardiac scintigram showing a decreased uptake of the isotope in both the early and delayed phases. A: The early phase was photographed 15 minutes after isotope injection: the heart to mediastinum (H/M) ratio is B: The delayed phase was photographed at two hours: the H/M ratio was Framed or circled areas are targets for counting the radioactivity of the isotope. 42
43 Figure 7. MRI findings of the calf muscles in Case 4. A: On admission, both gastrocnemius muscles showed high-signal lesions on flair-weighted images with gadolinium enhancement. B: Two weeks later, the lesions were undetectable on the same type of images. Figure 8. Light-microscopic findings of epon-embedded skin tissues stained with 1% toluidine blue. A and B: Findings for the first toe skin in patient No. 18, who was diagnosed with CRPS-I. The patient s symptoms were not severe and she was able to walk without difficulty. A: Two small nerve fascicles (indicated by arrows) are identified in the dermis. Original magnification x120. B: One nerve fascicle (indicated by an arrow) located the near apocrine glands appears normal. This fascicle was surmised to contain a sudomotor unmyelinated autonomic nerve. Original magnification x280. C&D: Findings in Case 2 showing serious limb symptoms of CRPS-I. C: One nerve fascicle in the skin of the second finger showing slight subperineurial edema (indicated by arrows). Original magnification x500. D: One nerve fascicle in the second finger s skin showing more prominent subperineurial and endoneurial edema (indicated by arrows). Original magnification x500. Figure 9. Electron-microscopic findings of the intradermal nerves in the second finger 43
44 in Case 2. A: The number of myelinated and unmyelinated nerves was preserved, although some unmyelinated nerve axons (indicated by arrows) contained electron-dense coarse granular materials, possibly indicating degeneration. B shows an enlarged image of the unmyelinated axon indicated by the arrow b. Coarse granular structures with a diameter ranging from 200 to 500 Å. Their morphology coincided with that of glycogen granules (49). Original magnification A x7,500, B x 20,000. Figure 10. Electron-microscopic findings of the intradermal nerves in the first toe of in Case 2. A is a low-magnification image of one fascicle with extensive structure-less space in the endoneurium, indicating edema. B is a high-magnification image of the framed area in A: Denervated Schwann cell s cytoplasmic processes are surrounded by proliferating bundles of collagen fibers (indicated by arrows). Both findings indicate severe degeneration of the nerve fascicle. Original magnification A x7,500, B x 1,800. Figure 11. Electron-microscopic findings of the intradermal nerves in the calf in Case 4. A shows a few unmyelinated nerve axons (indicated by arrows) containing electron-dense coarse granular materials. B reveals denervated Schwann cell cytoplasmic processes. Both findings closely resemble those seen in Figures 8 and 9. 44
45 Original magnification A x12,000, B x 20,
46 Table 1A. Japanese diagnostic hallmark for CRPS A. Disease history must contain more than 2 in the following subjective symptoms 1. Trophic change in skin, nail or hair 2. Decreased range of joint motion 3. Persistent aching pain or shooting pain and/or hyperpathy 4. Sweating changes 5. Oedema B. Must display at least two at time of evaluation in the following objective findings 1. Trophic change in skin, nail or hair 2. Decreased range of joint motion 3. Allodynia or hyperalgesia in pin-pricking 4. Sweating changes 5. Oedema Table 1B. Proposed clinical diagnostic criterion for CRPS 1. Continuing pain which is disproportionate to any inciting event 2. Must report at least one symptom in three of the four following categories Sensory: reports of hyperaesthesia and/or allodynia Vasomotor: reports of temperature asymmetry and/or skin colour changes and/or skin colour asymmetry Sudomotor/oedema: reports of oedema and/or sweating changes and/or sweating asymmetry Motor/trophic: reports of decreased range of motion and/or motor dysfunction (weakness, tremor, dystonia) and/or trophic changes (hair, nail, skin) 3. Must display at least one sign at time of evaluation in two or more of the following categories Sensory: evidence of hyperaesthesia and/or allodynia Vasomotor: evidence of temperature asymmetry and/or skin colour changes and/or skin colour asymmetry Sudomotor/oedema: evidence of oedema and/or sweating changes and/or sweating asymmetry Motor/trophic: evidence of decreased range of motion and/or motor dysfunction (weakness, tremor, dystonia) and/or trophic changes (hair, nail, skin) 4. There is no other diagnosis that better explains the signs and symptoms 1
47 Table.2 Results of Schellong test including the changes of plasma noradrenaline level. NA at Increasing Maximum change Diagnosis Patient Age supine positionrate of NA decreased SBP increased HR No. OH POTS (ng/m ) (%) mmhg /min Abbreviations: NA: noradrenaline, SBP: systolic blood pressure, HR: heart rate, OH: orthostatic hypotension, POTS: postual orthostatic tachycardia.normal plasma level of NA at supine position is ng/ml. Increasing rate of plasma NA after standing is more than 60% of basal level after 5 minutes.
48 Table.3 Evaluation results of skin temperature and digital plethysmogram Patient Skin temprature ( o C) Digital plethysmogram No. 2nd finger 1st toe 2nd finger 1st toe normal normal normal normal normal normal normal normal normal normal n.e. n.e normal normal normal normal normal normal normal normal normal normal normal normal normal n.e: not examined. : decreased height of waves.the room at examination of skin temperature was kept at
49 Table.4 Summary of clinical picture in 29 girls showing obvious sympathetic nerve dysfunction. Patient Type of Initial Over CRPS CRPS Age Headache Limb pain Limb Limb Gait Decreased Hyperpathy No. vaccine symptom paresis tremulousnes disturbance skin sweating (Japan) (IASP) OD OH POTS 1 13 G Fatigue + + n.e G Fever G Headache * C Hyperventilation * G Headache C Headache n.e G Headache, nausia, fever C Pain in eye ball, double vision * C Fever C Headache C Limb pain G Limb pain and weakness C Limb pain + + n.e C Limb pain C Fatigue C Limb weakness C Arthralgia C Arthralgia C Fatigue, difficulty in getting up C Arthralgia Limb pain and weakness, C parethesia C Nausea G Fatigue, limb parethesia C Headache C Fever, gait disturbance C Abdominal pain C Difficulty in getting up n.e C Syncope n.e C Abdominal pain Total number Abbreviations: G: Gardasil, C: Cerverix, CRPS: complex regional pain syndrome, IASP: international association for the study of pain., OD: orthostatic dysregulation, OH: orthostatic hypotension, POTS: postual orthostatic tachycardia, n.e.: not examined, *: limb tremulousness that could be observed at our examinations. Decreased skin temperature in 1st toe is defined as lower level than examination room temperature kept at
50 Table 5. The final diagnosis of 40 girls examined Diagnosis No. CRPS-1 alone 5 CRPS-1+OH 5 CRPS-1+OD 5 CRPS-1+POTS 3 OH alone 3 OD alone 7 POTS alone 1 Others 11 1
51 BP mmhg 140 noradrenaline ng/ml spine standing 5 min min min blood pressure noradrenaline 0.5 0
52 A B


53 Right second finger Right first toe noise A ST: 28.4 B ST: 22.2 C ST: 31.8 D ST: 29.5

54 lt. Bi lt. Tri lt. WF lt. WE lt. Quad lt. Ham lt. TA lt. Gast rt. Bi rt. Tri rt. WF rt. WE rt. Quad rt. Ham rt. TA rt. Gast 1 sec 150 V

55 EEG lt. Bi rt. Bi lt. Quad rt. Quad 1 sec 150 V


56



57 A B

58 A B C D




59 B 0.5ȝm A * 2 ȝm


60 A 10 ȝm B 2 ȝm



61 A B
Peripheral Sympathetic Nerve Dysfunction in Adolescent Japanese Girls Following Immunization with the Human Papillomavirus Vaccine
 ORIGINAL ARTICLE Peripheral Sympathetic Nerve Dysfunction in Adolescent Japanese Girls Following Immunization with the Human Papillomavirus Vaccine Tomomi Kinoshita 1, Ryu-ta Abe 1, Akiyo Hineno 1, Kazuhiro
ORIGINAL ARTICLE Peripheral Sympathetic Nerve Dysfunction in Adolescent Japanese Girls Following Immunization with the Human Papillomavirus Vaccine Tomomi Kinoshita 1, Ryu-ta Abe 1, Akiyo Hineno 1, Kazuhiro
POSTURAL ORTHOSTATIC TACHYCARDIA SYNDROME (POTS) IT S NOT THAT SIMPLE
 IT S NOT THAT SIMPLE") POSTURAL ORTHOSTATIC TACHYCARDIA SYNDROME (POTS) IT S NOT THAT SIMPLE POTS Irritable heart syndrome. Soldier s heart. Effort syndrome. Vasoregulatory asthenia. Neurocirculatory asthenia. Anxiety neurosis.
POSTURAL ORTHOSTATIC TACHYCARDIA SYNDROME (POTS) IT S NOT THAT SIMPLE POTS Irritable heart syndrome. Soldier s heart. Effort syndrome. Vasoregulatory asthenia. Neurocirculatory asthenia. Anxiety neurosis.
Findings from the 2015 HRS Expert Consensus Document on Postural Tachycardia Syndrome (POTS) and Inappropriate Sinus Tachycardia (IST)
 and Inappropriate Sinus Tachycardia (IST)") Findings from the 2015 HRS Expert Consensus Document on Postural Tachycardia Syndrome (POTS) and Inappropriate Sinus Tachycardia (IST) Ahmad Hersi, MBBS, MSc, FRCPC Professor of Cardiac Sciences Consultant
Findings from the 2015 HRS Expert Consensus Document on Postural Tachycardia Syndrome (POTS) and Inappropriate Sinus Tachycardia (IST) Ahmad Hersi, MBBS, MSc, FRCPC Professor of Cardiac Sciences Consultant
Guide to the use of nerve conduction studies (NCS) & electromyography (EMG) for non-neurologists
 & electromyography (EMG) for non-neurologists") Guide to the use of nerve conduction studies (NCS) & electromyography (EMG) for non-neurologists What is NCS/EMG? NCS examines the conduction properties of sensory and motor peripheral nerves. For both
Guide to the use of nerve conduction studies (NCS) & electromyography (EMG) for non-neurologists What is NCS/EMG? NCS examines the conduction properties of sensory and motor peripheral nerves. For both
INTRODUCTION POTS is: Poorly understood Rarely considered SIGNIFICANT morbidity Appropriate initial diagnosis & care will expedite management of POTS
 Learning objectives At the end of this presentation the learner should: Define POTS & identify the various etiologies of POTS Be able to differentiate POTS from other causes of orthostatic intolerance
Learning objectives At the end of this presentation the learner should: Define POTS & identify the various etiologies of POTS Be able to differentiate POTS from other causes of orthostatic intolerance
AUTOIMMUNE DISORDERS IN THE ACUTE SETTING
 AUTOIMMUNE DISORDERS IN THE ACUTE SETTING Diagnosis and Treatment Goals Aimee Borazanci, MD BNI Neuroimmunology Objectives Give an update on the causes for admission, clinical features, and outcomes of
AUTOIMMUNE DISORDERS IN THE ACUTE SETTING Diagnosis and Treatment Goals Aimee Borazanci, MD BNI Neuroimmunology Objectives Give an update on the causes for admission, clinical features, and outcomes of
Tension-Type Headache
 Chronic Headache Tension-Type Headache Its mechanism and treatment JMAJ 47(3): 130 134, 2004 Manabu SAKUTA Chief Professor, First Internal Medicine (Neurology), Kyorin University Abstract: Tension-type
Chronic Headache Tension-Type Headache Its mechanism and treatment JMAJ 47(3): 130 134, 2004 Manabu SAKUTA Chief Professor, First Internal Medicine (Neurology), Kyorin University Abstract: Tension-type
British Journal of Rheumatology 1991; 30:
 British Journal of Rheumatology 1991; 30:468-470 CASE REPORT CARPAL TUNNEL SYNDROME COMPLICATED BY REFLEX SYMPATHETIC DYSTROPHY SYNDROME BY M.-A. FITZCHARLES AND J.M. ESDAILE Rheumatic Disease Unit, McGill
British Journal of Rheumatology 1991; 30:468-470 CASE REPORT CARPAL TUNNEL SYNDROME COMPLICATED BY REFLEX SYMPATHETIC DYSTROPHY SYNDROME BY M.-A. FITZCHARLES AND J.M. ESDAILE Rheumatic Disease Unit, McGill
CASE-BASED SMALL GROUP DISCUSSION MHD II SESSION VI
 MHD II, Session VI, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD II SESSION VI Wednesday, MARCH 26, 2014 STUDENT COPY MHD II, Session VI, Student Copy Page 2 CASE 1 History: A 57-year-old
MHD II, Session VI, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD II SESSION VI Wednesday, MARCH 26, 2014 STUDENT COPY MHD II, Session VI, Student Copy Page 2 CASE 1 History: A 57-year-old
A Patient s Guide to Pain Management: Complex Regional Pain Syndrome
 A Patient s Guide to Pain Management: Complex Regional Pain Syndrome Suite 11-13/14/15 Mount Elizabeth Medical Center 3 Mount Elizabeth Singapore, 228510 Phone: (65) 6738 2628 Fax: (65) 6738 2629 DISCLAIMER:
A Patient s Guide to Pain Management: Complex Regional Pain Syndrome Suite 11-13/14/15 Mount Elizabeth Medical Center 3 Mount Elizabeth Singapore, 228510 Phone: (65) 6738 2628 Fax: (65) 6738 2629 DISCLAIMER:
Clinical Studies 129
 Clinical Studies 129 Syncope in migraine. The population-based CAMERA study Roland D. Thijs, 1* Mark C. Kruit, 2* Mark A. van Buchem, 2 Michel D. Ferrari, 1 Lenore J. Launer, 3,4 and J. Gert van Dijk
Clinical Studies 129 Syncope in migraine. The population-based CAMERA study Roland D. Thijs, 1* Mark C. Kruit, 2* Mark A. van Buchem, 2 Michel D. Ferrari, 1 Lenore J. Launer, 3,4 and J. Gert van Dijk
Biology 3201 Nervous System # 7: Nervous System Disorders
 Biology 3201 Nervous System # 7: Nervous System Disorders Alzheimer's Disease first identified by German physician, Alois Alzheimer, in 1906 most common neurodegenerative disease two thirds of cases of
Biology 3201 Nervous System # 7: Nervous System Disorders Alzheimer's Disease first identified by German physician, Alois Alzheimer, in 1906 most common neurodegenerative disease two thirds of cases of
A Patient s Guide to Pain Management: Complex Regional Pain Syndrome
 A Patient s Guide to Pain Management: Complex Regional Pain Syndrome 950 Breckinridge Lane Suite 220 Louisville, KY 40223 Phone: 502.708.2940 DISCLAIMER: The information in this booklet is compiled from
A Patient s Guide to Pain Management: Complex Regional Pain Syndrome 950 Breckinridge Lane Suite 220 Louisville, KY 40223 Phone: 502.708.2940 DISCLAIMER: The information in this booklet is compiled from
BRAIN STEM CASE HISTORIES CASE HISTORY VII
 463 Brain stem Case history BRAIN STEM CASE HISTORIES CASE HISTORY VII A 60 year old man with hypertension wakes one morning with trouble walking. He is feeling dizzy and is sick to his stomach. His wife
463 Brain stem Case history BRAIN STEM CASE HISTORIES CASE HISTORY VII A 60 year old man with hypertension wakes one morning with trouble walking. He is feeling dizzy and is sick to his stomach. His wife
8/26/2014. Faculty/Presenter Disclosure. Complex Regional Pain Syndrome (CRPS): State of the Art review. Disclosure of Commercial Support
: State of the Art review. Disclosure of Commercial Support") Faculty/Presenter Disclosure Complex Regional Pain Syndrome (CRPS): State of the Art review Angela Mailis Gagnon MD, MSc, FRCPC(PhysMed) Director, Comprehensive Pain Program/UHN and Senior Investigator
Faculty/Presenter Disclosure Complex Regional Pain Syndrome (CRPS): State of the Art review Angela Mailis Gagnon MD, MSc, FRCPC(PhysMed) Director, Comprehensive Pain Program/UHN and Senior Investigator
:{ic0fp'16. Geriatric Medicine: Blood Pressure Monitoring in the Elderly. Terrie Ginsberg, DO, FACOI
 :{ic0fp'16 ACOFP 53 rd Annual Convention & Scientific Seminars Geriatric Medicine: Blood Pressure Monitoring in the Elderly Terrie Ginsberg, DO, FACOI Blood Pressure Management in the Elderly Terrie B.
:{ic0fp'16 ACOFP 53 rd Annual Convention & Scientific Seminars Geriatric Medicine: Blood Pressure Monitoring in the Elderly Terrie Ginsberg, DO, FACOI Blood Pressure Management in the Elderly Terrie B.
Cervical Cancer Prevention in Japan: Troubling Times
 PCC Melbourne 2015 Cervical Cancer Prevention in Japan: Troubling Times Sharon J. B. Hanley Department of Women s Health Medicine, Hokkaido University, Sapporo, Japan Declaration (Based on ICMJE guidelines)
PCC Melbourne 2015 Cervical Cancer Prevention in Japan: Troubling Times Sharon J. B. Hanley Department of Women s Health Medicine, Hokkaido University, Sapporo, Japan Declaration (Based on ICMJE guidelines)
Medical History Questionnaire
 Date Medical History Questionnaire Name DOB Reason for visit When did symptoms first appear Is the condition getting worse? Please rate your pain 0 1 2 3 4 5 6 7 8 9 10 No Pain Extreme Pain Please circle
Date Medical History Questionnaire Name DOB Reason for visit When did symptoms first appear Is the condition getting worse? Please rate your pain 0 1 2 3 4 5 6 7 8 9 10 No Pain Extreme Pain Please circle
Various Types of Pain Defined
 Various Types of Pain Defined Pain: The International Association for the Study of Pain describes pain as, An unpleasant sensory and emotional experience associated with actual or potential tissue damage,
Various Types of Pain Defined Pain: The International Association for the Study of Pain describes pain as, An unpleasant sensory and emotional experience associated with actual or potential tissue damage,
A CASE OF GIANT AXONAL NEUROPATHY HEMANANTH T SECOND YEAR POST GRADUATE IN PAEDIATRICS INSTITUTE OF SOCIAL PAEDIATRICS GOVERNMENT STANLEY HOSPITAL
 A CASE OF GIANT AXONAL NEUROPATHY HEMANANTH T SECOND YEAR POST GRADUATE IN PAEDIATRICS INSTITUTE OF SOCIAL PAEDIATRICS GOVERNMENT STANLEY HOSPITAL CASE HISTORY Nine year old male child Second born Born
A CASE OF GIANT AXONAL NEUROPATHY HEMANANTH T SECOND YEAR POST GRADUATE IN PAEDIATRICS INSTITUTE OF SOCIAL PAEDIATRICS GOVERNMENT STANLEY HOSPITAL CASE HISTORY Nine year old male child Second born Born
The Internist s Approach to Neuropathy
 The Internist s Approach to Neuropathy VOLKAN GRANIT, MD, MSC ASSISTANT PROFESSOR OF NEUROLOGY NEUROMUSCU LAR DIVISION UNIVERSITY OF MIAMI, MILLER SCHOOL OF MEDICINE RELEVANT DECLARATIONS Financial disclosures:
The Internist s Approach to Neuropathy VOLKAN GRANIT, MD, MSC ASSISTANT PROFESSOR OF NEUROLOGY NEUROMUSCU LAR DIVISION UNIVERSITY OF MIAMI, MILLER SCHOOL OF MEDICINE RELEVANT DECLARATIONS Financial disclosures:
Središnja medicinska knjižnica
 Središnja medicinska knjižnica Adamec I., Klepac N., Milivojević I., Radić B., Habek M. (2012) Sick sinus syndrome and orthostatic hypotension in Parkinson's disease. Acta Neurologica Belgica, 112 (3).
Središnja medicinska knjižnica Adamec I., Klepac N., Milivojević I., Radić B., Habek M. (2012) Sick sinus syndrome and orthostatic hypotension in Parkinson's disease. Acta Neurologica Belgica, 112 (3).
Evolution of a concept: Apraxia/higher level gait disorder. ataxia v. apraxia gait = limb apraxia. low, middle, high gait disturbance levels
 Case #1 81-year-old woman Gait Imbalance: Two Unusual Cases in Older Patients February 2008: 3 years of gradually progressive gait imbalance no vertigo, dizziness or paresthesias etiology unclear on examination
Case #1 81-year-old woman Gait Imbalance: Two Unusual Cases in Older Patients February 2008: 3 years of gradually progressive gait imbalance no vertigo, dizziness or paresthesias etiology unclear on examination
Questions and answers about HPV. Facts about the virus and the vaccine
 Questions and answers about HPV Facts about the virus and the vaccine About the introduction of the human papillomavirus (HPV) vaccine Which countries have introduced the HPV vaccine? Over 100 countries
Questions and answers about HPV Facts about the virus and the vaccine About the introduction of the human papillomavirus (HPV) vaccine Which countries have introduced the HPV vaccine? Over 100 countries
NEUROPATHY IN PERIPHERAL VASCULAR DISEASE 1
 267 616.833-02:616.13-005 NEUROPATHY IN PERIPHERAL VASCULAR DISEASE 1 Its Bearing on Diabetic Neuropathy BY E. C. HUTCHINSON AND L. A. LIVERSKDGE (From the Department of Neurology, Manchester Royal Infirmary)
267 616.833-02:616.13-005 NEUROPATHY IN PERIPHERAL VASCULAR DISEASE 1 Its Bearing on Diabetic Neuropathy BY E. C. HUTCHINSON AND L. A. LIVERSKDGE (From the Department of Neurology, Manchester Royal Infirmary)
Insulin Neuritis: an old, but still an unfamiliar and mysterious condition
 Insulin Neuritis: an old, but still an unfamiliar and mysterious condition Authors: Yun Tae Hwang 1, Gerard Davies 1 1. Department of Neurology, Royal Free Hospital, United Kingdom Corresponding author:
Insulin Neuritis: an old, but still an unfamiliar and mysterious condition Authors: Yun Tae Hwang 1, Gerard Davies 1 1. Department of Neurology, Royal Free Hospital, United Kingdom Corresponding author:
American Board of Physical Medicine & Rehabilitation. Part I Curriculum & Weights
 American Board of Physical Medicine & Rehabilitation Part I Curriculum & Weights Neurologic Disorders 30% Stroke Spinal Cord Injury Traumatic Brain Injury Neuropathies a) Mononeuropathies b) Polyneuropathies
American Board of Physical Medicine & Rehabilitation Part I Curriculum & Weights Neurologic Disorders 30% Stroke Spinal Cord Injury Traumatic Brain Injury Neuropathies a) Mononeuropathies b) Polyneuropathies
Case Series Drug Analysis Print Name: Vaxigrip, Fluarix, Inflexal V og Influenzacvaccine 01Sep Oct2014
 - 16Oct2014 Report Run Date: 20-Oct-2014 Data Lock Date: 16-Oct-2014 19:00:06 Earliest Reaction Date: 28-Oct-2009 MedDRA Version: MedDRA 17.0 Vaxigrip, Fluarix, Inflexal V og Influenzacvaccine : Alle cases
- 16Oct2014 Report Run Date: 20-Oct-2014 Data Lock Date: 16-Oct-2014 19:00:06 Earliest Reaction Date: 28-Oct-2009 MedDRA Version: MedDRA 17.0 Vaxigrip, Fluarix, Inflexal V og Influenzacvaccine : Alle cases
Questionnaire for Lipedema Patients
 Questionnaire for Lipedema Patients Name Date of diagnosis Date Name of physician making diagnosis Do you also have lymphedema? What areas of the body are affected? Outside of thighs Inner thighs Knees
Questionnaire for Lipedema Patients Name Date of diagnosis Date Name of physician making diagnosis Do you also have lymphedema? What areas of the body are affected? Outside of thighs Inner thighs Knees
9 Complex Regional Pain Syndrome: The Anatomy Of A Controversy
 9 Complex Regional Pain Syndrome: The Anatomy Of A Controversy Samuel D. Hodge, Jr., Esquire Jack E. Hubbard, PhD, MD Q. What do a blood draw, a rear-end collision, a gunshot wound, carpal tunnel syndrome,
9 Complex Regional Pain Syndrome: The Anatomy Of A Controversy Samuel D. Hodge, Jr., Esquire Jack E. Hubbard, PhD, MD Q. What do a blood draw, a rear-end collision, a gunshot wound, carpal tunnel syndrome,
X-Plain Muscles Reference Summary
 X-Plain Reference Summary Introduction are very important elements of the human body. They account for about half of a person s weight. Understanding how muscles work and how they can be injured is necessary
X-Plain Reference Summary Introduction are very important elements of the human body. They account for about half of a person s weight. Understanding how muscles work and how they can be injured is necessary
Adverse events following immunisation (AEFI) with 2010/2011 seasonal influenza vaccines
 with 2010/2011 seasonal influenza vaccines") Adverse events following immunisation (AEFI) with 00/0 seasonal influenza vaccines Netherlands Pharmacovigilance Centre Lareb 8 juli 0 Goudsbloemvallei 7 57 MH s-hertogenbosch www.lareb.nl info@lareb.nl
Adverse events following immunisation (AEFI) with 00/0 seasonal influenza vaccines Netherlands Pharmacovigilance Centre Lareb 8 juli 0 Goudsbloemvallei 7 57 MH s-hertogenbosch www.lareb.nl info@lareb.nl
Movement Disorders. Psychology 372 Physiological Psychology. Background. Myasthenia Gravis. Many Types
 Background Movement Disorders Psychology 372 Physiological Psychology Steven E. Meier, Ph.D. Listen to the audio lecture while viewing these slides Early Studies Found some patients with progressive weakness
Background Movement Disorders Psychology 372 Physiological Psychology Steven E. Meier, Ph.D. Listen to the audio lecture while viewing these slides Early Studies Found some patients with progressive weakness
Section Editor Howard I Hurtig, MD
 1 of 5 9/29/2013 6:56 PM Official reprint from UpToDate www.uptodate.com 2013 UpToDate The content on the UpToDate website is not intended nor recommended as a substitute for medical advice, diagnosis,
1 of 5 9/29/2013 6:56 PM Official reprint from UpToDate www.uptodate.com 2013 UpToDate The content on the UpToDate website is not intended nor recommended as a substitute for medical advice, diagnosis,
Corporate Medical Policy
 Corporate Medical Policy Intravenous Anesthetics for the Treatment of Chronic Pain File Name: Origination: Last CAP Review: Next CAP Review: Last Review: intravenous_anesthetics_for_the_treatment_of_chronic_pain
Corporate Medical Policy Intravenous Anesthetics for the Treatment of Chronic Pain File Name: Origination: Last CAP Review: Next CAP Review: Last Review: intravenous_anesthetics_for_the_treatment_of_chronic_pain
Peripheral neuropathies, neuromuscular junction disorders, & CNS myelin diseases
 Peripheral neuropathies, neuromuscular junction disorders, & CNS myelin diseases Peripheral neuropathies according to which part affected Axonal Demyelinating with axonal sparing Many times: mixed features
Peripheral neuropathies, neuromuscular junction disorders, & CNS myelin diseases Peripheral neuropathies according to which part affected Axonal Demyelinating with axonal sparing Many times: mixed features
BACK AND NECK PAIN QUESTIONNAIRE
 Neurological Surgery and Spine Surgery, S.C. 1 Westbrook Corporate Center, Suite 800 Westchester, Illinois 60154 BACK AND NECK PAIN QUESTIONNAIRE Please PRINT all information CLEARLY and answer all questions
Neurological Surgery and Spine Surgery, S.C. 1 Westbrook Corporate Center, Suite 800 Westchester, Illinois 60154 BACK AND NECK PAIN QUESTIONNAIRE Please PRINT all information CLEARLY and answer all questions
e) None of the above e) None of the above
 None of the above e) None of the above") Neurology 1) For the management of an acute delirium acquired in the hospital, which one of the following options would be least appropriate? a) Treating the underlying cause b) Promptly increasing antibiotic
Neurology 1) For the management of an acute delirium acquired in the hospital, which one of the following options would be least appropriate? a) Treating the underlying cause b) Promptly increasing antibiotic
Joint Statement 2018 for the Victims of HPV Vaccines
 Joint Statement 2018 for the Victims of HPV Vaccines On behalf of the victims of HPV vaccine damage in the UK, Spain, Ireland, Colombia and Japan, an international symposium; "The Current Status of Worldwide
Joint Statement 2018 for the Victims of HPV Vaccines On behalf of the victims of HPV vaccine damage in the UK, Spain, Ireland, Colombia and Japan, an international symposium; "The Current Status of Worldwide
MUSCULOSKELETAL AND NEUROLOGICAL DISORDERS
 MUSCULOSKELETAL AND NEUROLOGICAL DISORDERS There are a wide variety of Neurologic and Musculoskeletal disorders which can impact driving safety. Impairment may be the result of altered muscular, skeletal,
MUSCULOSKELETAL AND NEUROLOGICAL DISORDERS There are a wide variety of Neurologic and Musculoskeletal disorders which can impact driving safety. Impairment may be the result of altered muscular, skeletal,
What could be reffered to as dizziness by the patient?
 What could be reffered to as dizziness by the patient? Rotational vertigo Sense of instability Ataxia of gait Disturbance of vision Loss of contact with surroundings Nausea Loss of memory Loss of confidence
What could be reffered to as dizziness by the patient? Rotational vertigo Sense of instability Ataxia of gait Disturbance of vision Loss of contact with surroundings Nausea Loss of memory Loss of confidence
Power Line to your Line to your Circuit Line to the station neighborhood house breaker living room. Outlet lamp Lamp with socket, Light bulb
 IMC 606 Neuroscience and Behavior Module Dr. Margaret Paroski Analysis of Sensory Lesions You walk into your living room and turn on the lamp. But no light comes on. What would you do? You would probably
IMC 606 Neuroscience and Behavior Module Dr. Margaret Paroski Analysis of Sensory Lesions You walk into your living room and turn on the lamp. But no light comes on. What would you do? You would probably
COPYRIGHT 2012 THE TRANSVERSE MYELITIS ASSOCIATION. ALL RIGHTS RESERVED
 The Transverse Myelitis Association...advocating for those with acute disseminated encephalomyelitis, neuromyelitis optica, optic neuritis and transverse myelitis ACUTE DISSEMINATED ENCEPHALOMYELITIS (ADEM)
The Transverse Myelitis Association...advocating for those with acute disseminated encephalomyelitis, neuromyelitis optica, optic neuritis and transverse myelitis ACUTE DISSEMINATED ENCEPHALOMYELITIS (ADEM)
November 16-18, 2017 Hotel Monteleone New Orleans, LA. Provided by
 November 16-18, 2017 Hotel Monteleone New Orleans, LA Provided by Diabetic Neuropathy: A Global and Growing Problem John D. England, MD Louisiana State University Health Sciences Center School of Medicine
November 16-18, 2017 Hotel Monteleone New Orleans, LA Provided by Diabetic Neuropathy: A Global and Growing Problem John D. England, MD Louisiana State University Health Sciences Center School of Medicine
Mr. LBP: Case Presentation
 CLINICAL CASES Case: Mr. LBP Mr. LBP: Case Presentation Mr. LBP is a 35-year-old male He fell down while participating in a recreational sports activity He subsequently developed low back pain Upon arrival
CLINICAL CASES Case: Mr. LBP Mr. LBP: Case Presentation Mr. LBP is a 35-year-old male He fell down while participating in a recreational sports activity He subsequently developed low back pain Upon arrival
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST The Management of Syncope remains a challenge: Clues from the History Richard Sutton, DSc Emeritus Professor of Cardiology Imperial College, St Mary s Hospital, London,
DECLARATION OF CONFLICT OF INTEREST The Management of Syncope remains a challenge: Clues from the History Richard Sutton, DSc Emeritus Professor of Cardiology Imperial College, St Mary s Hospital, London,
Central nervous system
 Central nervous system By Dr. Mohsen Dashti Clinical Medicine & Pathology 316 7 th Lecture Lecture outline Review of structure & function. Symptoms, signs & tests. Specific diseases. Review of structure
Central nervous system By Dr. Mohsen Dashti Clinical Medicine & Pathology 316 7 th Lecture Lecture outline Review of structure & function. Symptoms, signs & tests. Specific diseases. Review of structure
Slide 1. Slide 2. Slide 3. Intro to Physical Therapy for Neuromuscular Conditions. PT Evaluation. PT Evaluation
 Slide 1 Intro to Physical Therapy for Neuromuscular Conditions PTA 103 Introduction to Clinical Practice 2 Slide 2 Mental status: consciousness, attention, orientation, cognition Communication: speech
Slide 1 Intro to Physical Therapy for Neuromuscular Conditions PTA 103 Introduction to Clinical Practice 2 Slide 2 Mental status: consciousness, attention, orientation, cognition Communication: speech
Multiple choice questions: ANSWERS
 Multiple choice questions: ANSWERS Chapter 1. Redefining Parkinson s disease 1. Common non-motor features that precede the motor findings in Parkinson s disease (PD) include all of the following except?
Multiple choice questions: ANSWERS Chapter 1. Redefining Parkinson s disease 1. Common non-motor features that precede the motor findings in Parkinson s disease (PD) include all of the following except?
Patient Questionnaire Chronic Urticaria
 Patient Questionnaire Chronic Urticaria (Baseline) Dear Patient, Your answers to the following questions regarding the present situation of your Chronic Urticaria and its course up to now can help to better
Patient Questionnaire Chronic Urticaria (Baseline) Dear Patient, Your answers to the following questions regarding the present situation of your Chronic Urticaria and its course up to now can help to better
PERSONAL INJURY QUESTIONNAIRE
 PERSONAL INJURY QUESTIONNAIRE Name Phone ( ) Age Birth Date Sex S.S.N. Employer Address Did you report this to YOUR Car Insurance? Yes No (Circle One) Your Car Insurance Co. is Claim # Claims Adjuster
PERSONAL INJURY QUESTIONNAIRE Name Phone ( ) Age Birth Date Sex S.S.N. Employer Address Did you report this to YOUR Car Insurance? Yes No (Circle One) Your Car Insurance Co. is Claim # Claims Adjuster
Syncope By Remus Popa
 Syncope By Remus Popa A 66 years old male is brought to the ED from a restaurant where he fainted while dining out with his family. He complained of nausea and stood up to go to the restroom but immediately
Syncope By Remus Popa A 66 years old male is brought to the ED from a restaurant where he fainted while dining out with his family. He complained of nausea and stood up to go to the restroom but immediately
Dizziness, postural hypotension and postural blackouts: Two cases suggesting multiple system atrophy
 Dizziness, postural hypotension and postural blackouts: Two cases suggesting multiple system atrophy Dr Rahul Chakor, Associate Prof and Head Dept of Neurology, Dr Anand Soni, Senior Resident, T N Medical
Dizziness, postural hypotension and postural blackouts: Two cases suggesting multiple system atrophy Dr Rahul Chakor, Associate Prof and Head Dept of Neurology, Dr Anand Soni, Senior Resident, T N Medical
SECTION OF NEUROSURGERY PATIENT INFORMATION SHEET
 SECTION OF NEUROSURGERY PATIENT INFORMATION SHEET EC#: (for office use only) Patient s Name: Today s Date: Age: Date of Birth: Height: Weight: Physician you are seeing today: Marital Status: Married Work
SECTION OF NEUROSURGERY PATIENT INFORMATION SHEET EC#: (for office use only) Patient s Name: Today s Date: Age: Date of Birth: Height: Weight: Physician you are seeing today: Marital Status: Married Work
Cigna Medical Coverage Policies Musculoskeletal Regional Sympathetic Blocks
 Cigna Medical Coverage Policies Musculoskeletal Regional Sympathetic Blocks Effective January 1, 2016 Instructions for use The following coverage policy applies to health benefit plans administered by
Cigna Medical Coverage Policies Musculoskeletal Regional Sympathetic Blocks Effective January 1, 2016 Instructions for use The following coverage policy applies to health benefit plans administered by
NMH happens when there is an abnormal reflex interaction between the heart and the brain, although both are structurally normal.
 Neurally mediated hypotension: is also known as: the fainting reflex, neurocardiogenic syncope, vasodepressor syncope, the vaso-vagal reflex, and autonomic dysfunction. (Hypotension= low blood pressure,
Neurally mediated hypotension: is also known as: the fainting reflex, neurocardiogenic syncope, vasodepressor syncope, the vaso-vagal reflex, and autonomic dysfunction. (Hypotension= low blood pressure,
droxidopa (Northera )
") Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Anxiety disorders part II
 Anxiety disorders part II OBSESSIVE-COMPULSIVE DISORDER obsession a recurrent and intrusive thought, feeling, idea, or sensation compulsion a conscious, standarized, recurring pattern of behavior, such
Anxiety disorders part II OBSESSIVE-COMPULSIVE DISORDER obsession a recurrent and intrusive thought, feeling, idea, or sensation compulsion a conscious, standarized, recurring pattern of behavior, such
P1: OTA/XYZ P2: ABC c01 BLBK231-Ginsberg December 23, :43 Printer Name: Yet to Come. Part 1. The Neurological Approach COPYRIGHTED MATERIAL
 Part 1 The Neurological Approach COPYRIGHTED MATERIAL 1 2 Chapter 1 Neurological history-taking The diagnosis and management of diseases of the nervous system have been revolutionized in recent years by
Part 1 The Neurological Approach COPYRIGHTED MATERIAL 1 2 Chapter 1 Neurological history-taking The diagnosis and management of diseases of the nervous system have been revolutionized in recent years by
WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 1820/13
 WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 1820/13 BEFORE: J. P. Moore: Vice-Chair HEARING: September 18, 2013 at Kitchener Oral Post-hearing activity completed on March 20, 2014 DATE
WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 1820/13 BEFORE: J. P. Moore: Vice-Chair HEARING: September 18, 2013 at Kitchener Oral Post-hearing activity completed on March 20, 2014 DATE
Pain Syndromes after stroke
 Diagnosis and Management of Complex Regional Pain Syndrome (CRPS) after Stroke Leonard S.W. Li Honorary Clinical Professor, Department of Medicine, The University of Hong Kong Director, Neurological Rehabilitation
Diagnosis and Management of Complex Regional Pain Syndrome (CRPS) after Stroke Leonard S.W. Li Honorary Clinical Professor, Department of Medicine, The University of Hong Kong Director, Neurological Rehabilitation
Summary listing of suspected adverse reactions and events associated with use of Gardasil 01/06/ /12/2015
 1 2015-023780 2015-023788 2015-023805 2015-023819 2015-023820 2015-023821 Injection site swelling Transient immobility Abdominal pain Visual acuity reduced Chronic fatigue syndrome Mental disorder Pallor
1 2015-023780 2015-023788 2015-023805 2015-023819 2015-023820 2015-023821 Injection site swelling Transient immobility Abdominal pain Visual acuity reduced Chronic fatigue syndrome Mental disorder Pallor
IAPMR Guidelines COMPLEX REGIONAL PAIN SYNDROME
 IAPMR Guidelines COMPLEX REGIONAL PAIN SYNDROME DR.NAVITA PUROHIT, CONSULTANT AND EXPERT IN PAIN MANAGEMENT, Department of Rehabilitation Medicine, Kokilaben Dhirubhai Ambani Hospital, Mumbai CRPS is a
IAPMR Guidelines COMPLEX REGIONAL PAIN SYNDROME DR.NAVITA PUROHIT, CONSULTANT AND EXPERT IN PAIN MANAGEMENT, Department of Rehabilitation Medicine, Kokilaben Dhirubhai Ambani Hospital, Mumbai CRPS is a
Vertigo. Tunde Magyar MD, PhD
 Vertigo Tunde Magyar MD, PhD What could be reffered to as dizziness by the patient? Rotational vertigo Sense of instability Ataxia of gait Disturbance of vision Loss of contact with surroundings Nausea
Vertigo Tunde Magyar MD, PhD What could be reffered to as dizziness by the patient? Rotational vertigo Sense of instability Ataxia of gait Disturbance of vision Loss of contact with surroundings Nausea
Prof Wayne Derman MBChB,BSc (Med)(Hons) PhD, FFIMS. Pain Management in the Elite Athlete: The 2017 IOC Consensus Statement
(Hons) PhD, FFIMS. Pain Management in the Elite Athlete: The 2017 IOC Consensus Statement") Prof Wayne Derman MBChB,BSc (Med)(Hons) PhD, FFIMS Pain Management in the Elite Athlete: The 2017 IOC Consensus Statement 2 as 20 Experts published and leaders in their respective field 12 month lead in
Prof Wayne Derman MBChB,BSc (Med)(Hons) PhD, FFIMS Pain Management in the Elite Athlete: The 2017 IOC Consensus Statement 2 as 20 Experts published and leaders in their respective field 12 month lead in
Dr Ng Swee Cheng Senior Consultant Khoo Teck Puat Hospital
 Dr Ng Swee Cheng Senior Consultant Khoo Teck Puat Hospital 1. Soft Tissue Rheumatism 2. Myofascial Pain 3. Neurovascular compression Syndromes 4. Complex Regional Pain Syndromes Tendinitis, tenosynovitis
Dr Ng Swee Cheng Senior Consultant Khoo Teck Puat Hospital 1. Soft Tissue Rheumatism 2. Myofascial Pain 3. Neurovascular compression Syndromes 4. Complex Regional Pain Syndromes Tendinitis, tenosynovitis
Exercise Training for PoTS and Syncope
 B 140 120 100 80 60 40 20 0 Blood Pressure (mm Hg) Blood Pressure Heart Rate 60 degree Head Up Tilt Time 140 120 100 80 60 40 20 0 Heart Rate (beats.min -1 ) Exercise Training for PoTS and Syncope C Blood
B 140 120 100 80 60 40 20 0 Blood Pressure (mm Hg) Blood Pressure Heart Rate 60 degree Head Up Tilt Time 140 120 100 80 60 40 20 0 Heart Rate (beats.min -1 ) Exercise Training for PoTS and Syncope C Blood
Indications and Uses of Testing. Laboratory Testing of Autonomic Function. Generalized Autonomic Failure. Benign Disorders 12/30/2012.
 Indications and Uses of Testing Laboratory Testing of Autonomic Function Conditions of generalized autonomic failure Help define the degree of autonomic dysfunction and distinguish more benign from life
Indications and Uses of Testing Laboratory Testing of Autonomic Function Conditions of generalized autonomic failure Help define the degree of autonomic dysfunction and distinguish more benign from life
PART IV: NEUROPATHIC PAIN SYNDROMES JILL SINDT FEBRUARY 7, 2019
 PART IV: NEUROPATHIC PAIN SYNDROMES JILL SINDT FEBRUARY 7, 2019 NEUROPATHIC PAIN PAIN ARISING AS DIRECT CONSEQUENCE OF A LESION OR DISEASE AFFECTING THE SOMATOSENSORY SYSTEM AFFECTS 3-8% OF POPULATION
PART IV: NEUROPATHIC PAIN SYNDROMES JILL SINDT FEBRUARY 7, 2019 NEUROPATHIC PAIN PAIN ARISING AS DIRECT CONSEQUENCE OF A LESION OR DISEASE AFFECTING THE SOMATOSENSORY SYSTEM AFFECTS 3-8% OF POPULATION
UNIVERSITY HOSPITALS OF LEICESTER NHS TRUST CARDIAC INVESTIGATIONS PAEDIATRIC & CONGENITAL SYNCOPE INVESTIGATIONS/QUESTIONNAIRE PROTOCOL
 UNIVERSITY HOSPITALS OF LEICESTER NHS TRUST CARDIAC INVESTIGATIONS PAEDIATRIC & CONGENITAL SYNCOPE INVESTIGATIONS/QUESTIONNAIRE PROTOCOL Written Date: 2009 by Dr Duke, then updated by Dr Sarita Makam 12/4/2016
UNIVERSITY HOSPITALS OF LEICESTER NHS TRUST CARDIAC INVESTIGATIONS PAEDIATRIC & CONGENITAL SYNCOPE INVESTIGATIONS/QUESTIONNAIRE PROTOCOL Written Date: 2009 by Dr Duke, then updated by Dr Sarita Makam 12/4/2016
SARAH VLACH, MD TYLER HEDIN, MD JUDY GOOCH, MD
 Name: Height: Birthdate: Weight: Chief Complaint: What is the reason for your appointment? (please describe why you are here) Medications: Please list ALL medications with dosages you are currently taking,
Name: Height: Birthdate: Weight: Chief Complaint: What is the reason for your appointment? (please describe why you are here) Medications: Please list ALL medications with dosages you are currently taking,
Complex Regional Pain Syndrome Pain that won t go away. Artee Gandhi MD Medical Director Pain Management Cook Children s Hospital. What is Pain?
 Complex Regional Pain Syndrome Pain that won t go away Artee Gandhi MD Medical Director Pain Management Cook Children s Hospital What is Pain? An unpleasant sensory experience associated with real or perceived
Complex Regional Pain Syndrome Pain that won t go away Artee Gandhi MD Medical Director Pain Management Cook Children s Hospital What is Pain? An unpleasant sensory experience associated with real or perceived
CRPS for all of us. MC Chu Anaesthesia and Intensive Care, PWH. 7th November 2007
 CRPS for all of us MC Chu Anaesthesia and Intensive Care, PWH 7th November 2007 Agenda What is CRPS Physiotherapy for CRPS Other interventions for CRPS Optimizing outcome Before CRPS Reflex sympathetic
CRPS for all of us MC Chu Anaesthesia and Intensive Care, PWH 7th November 2007 Agenda What is CRPS Physiotherapy for CRPS Other interventions for CRPS Optimizing outcome Before CRPS Reflex sympathetic
Case 3. Your Diagnosis?
 Case 3 45 year-old presenting with a history of injury to the right shoulder whilst working in the freezing work. He was loading a sheep over an incline with his arm around the sheep. He felt pain in the
Case 3 45 year-old presenting with a history of injury to the right shoulder whilst working in the freezing work. He was loading a sheep over an incline with his arm around the sheep. He felt pain in the
Human Papillomavirus Immunisation Programme. Background
 Human Papillomavirus Immunisation Programme Background Recommending the use of a human papillomavirus (HPV) vaccine was first signalled in the New Zealand Cancer Control Strategy Action Plan 2005-2010.
Human Papillomavirus Immunisation Programme Background Recommending the use of a human papillomavirus (HPV) vaccine was first signalled in the New Zealand Cancer Control Strategy Action Plan 2005-2010.
PRODUCT CIRCULAR. GARDASIL [Quadrivalent Human Papillomavirus (Types 6, 11, 16, 18) Recombinant Vaccine]
![PRODUCT CIRCULAR. GARDASIL [Quadrivalent Human Papillomavirus (Types 6, 11, 16, 18) Recombinant Vaccine]](/thumbs/95/122763989.jpg "PRODUCT CIRCULAR. GARDASIL [Quadrivalent Human Papillomavirus (Types 6, 11, 16, 18) Recombinant Vaccine]") PRODUCT CIRCULAR [Quadrivalent Human Papillomavirus (Types 6, 11, 16, 18) Recombinant Vaccine] I. THERAPEUTIC CLASS GARDASIL is a recombinant, quadrivalent vaccine that protects against Human Papillomavirus
PRODUCT CIRCULAR [Quadrivalent Human Papillomavirus (Types 6, 11, 16, 18) Recombinant Vaccine] I. THERAPEUTIC CLASS GARDASIL is a recombinant, quadrivalent vaccine that protects against Human Papillomavirus
Comparison of Sudomotor and Sensory Nerve Testing in Painful Sensory Neuropathies
 138 Original Article Comparison of Sudomotor and Sensory Nerve Testing in Painful Sensory Neuropathies James M. Killian, MD,* Shane Smyth, MD,* Rudy Guerra, PhD, Ishan Adhikari, MD,* and Yadollah Harati,
138 Original Article Comparison of Sudomotor and Sensory Nerve Testing in Painful Sensory Neuropathies James M. Killian, MD,* Shane Smyth, MD,* Rudy Guerra, PhD, Ishan Adhikari, MD,* and Yadollah Harati,
Patient Name: Date: Address: Primary Care Physician: Online Website On TV In print On the radio
 927 W. Myrtle St. Boise, ID 83702 (208) 947-0100 NEW PATIENT INTAKE Patient Name: Date: Email Address: Primary Care Physician: How did you hear about AVT? (Please mark all that apply) Online Website On
927 W. Myrtle St. Boise, ID 83702 (208) 947-0100 NEW PATIENT INTAKE Patient Name: Date: Email Address: Primary Care Physician: How did you hear about AVT? (Please mark all that apply) Online Website On
Complex Regional Pain Syndrome: Manifestations and the Role of Neurostimulation in Its Management
 S20 Journal of Pain and Symptom Management Vol. 31 No. 4S April 2006 Special Article Complex Regional Pain Syndrome: Manifestations and the Role of Neurostimulation in Its Management Michael Stanton-Hicks
S20 Journal of Pain and Symptom Management Vol. 31 No. 4S April 2006 Special Article Complex Regional Pain Syndrome: Manifestations and the Role of Neurostimulation in Its Management Michael Stanton-Hicks
Postural Orthostatic Tachycardia Syndrome:
 Postural Orthostatic Tachycardia Syndrome: A Case Presentation Interesting Cases from the Annals of Women s Heart Care I have no financial relationships or commercial interests to disclose that are relevant
Postural Orthostatic Tachycardia Syndrome: A Case Presentation Interesting Cases from the Annals of Women s Heart Care I have no financial relationships or commercial interests to disclose that are relevant
Arm Pain, Numbness, and Tingling: Etiologies and Treatment
 Arm Pain, Numbness, and Tingling: Etiologies and Treatment Steve Fowler MD Confluence Health Department of Physiatry Education Medical School: University of Utah Residency: Mayo Clinic Work Confluence
Arm Pain, Numbness, and Tingling: Etiologies and Treatment Steve Fowler MD Confluence Health Department of Physiatry Education Medical School: University of Utah Residency: Mayo Clinic Work Confluence
CLINICAL GUIDELINES. CMM-209: Regional Sympathetic Blocks. Version Effective February 15, 2019
 CLINICAL GUIDELINES CMM-209: Regional Sympathetic Blocks Version 1.0.2019 Effective February 15, 2019 Clinical guidelines for medical necessity review of speech therapy services. CMM-209: CMM-209.1: Definitions
CLINICAL GUIDELINES CMM-209: Regional Sympathetic Blocks Version 1.0.2019 Effective February 15, 2019 Clinical guidelines for medical necessity review of speech therapy services. CMM-209: CMM-209.1: Definitions
CHIROPRACTIC ASSOCIATES CLINIC
 CHIROPRACTIC ASSOCIATES CLINIC 1127 LAKEWOOD COURT NORTH, REGINA, SK S4X 3S3 PH: (306) 924-5300 FAX: (306) 924-5252 EMAIL: cac.north@accesscomm.ca CHIROPRACTIC INITIAL HEALTH FORM PATIENT INFORMATION Last
CHIROPRACTIC ASSOCIATES CLINIC 1127 LAKEWOOD COURT NORTH, REGINA, SK S4X 3S3 PH: (306) 924-5300 FAX: (306) 924-5252 EMAIL: cac.north@accesscomm.ca CHIROPRACTIC INITIAL HEALTH FORM PATIENT INFORMATION Last
Involuntary Movements in Children and Adolescents: Is it Seizure, Tic or Something Else?
 Involuntary Movements in Children and Adolescents: Is it Seizure, Tic or Something Else? California Association of Nurse Practitioners Monterey, March 22, 2013 Julie Sprague-McRae, MS, RN, PPCNP-BC Ruth
Involuntary Movements in Children and Adolescents: Is it Seizure, Tic or Something Else? California Association of Nurse Practitioners Monterey, March 22, 2013 Julie Sprague-McRae, MS, RN, PPCNP-BC Ruth
REGIONAL SYMPATHETIC BLOCKS
 evicore healthcare. Clinical Decision Support Tool Diagnostic Strategies This tool addresses common symptoms and symptom complexes. Imaging requests for patients with atypical symptoms or clinical presentations
evicore healthcare. Clinical Decision Support Tool Diagnostic Strategies This tool addresses common symptoms and symptom complexes. Imaging requests for patients with atypical symptoms or clinical presentations
Kimberley A. Schroeder, D.O. 115 Baker Drive Tomball, TX
 Kimberley A. Schroeder, D.O. 115 Baker Drive Tomball, TX 77375 281.290.0531 www.feelwellagain.com FEMALE MEDICAL QUESTIONNAIRE (POSTMENOPAUSAL) NAME: DATE OF BIRTH: CHIEF COMPLAINT What is your primary
Kimberley A. Schroeder, D.O. 115 Baker Drive Tomball, TX 77375 281.290.0531 www.feelwellagain.com FEMALE MEDICAL QUESTIONNAIRE (POSTMENOPAUSAL) NAME: DATE OF BIRTH: CHIEF COMPLAINT What is your primary
4. A consensus definition of CFS/ME has been agreed by international experts for the purposes of research and includes the following:-
 DWP MEDICAL GUIDANCE VERSION 10 (May 2007) CHRONIC FATIGUE SYNDROME AND MYALGIC ENCEPHALOMYELITIS/ENCEPHALOPATHY What is it? (Definition) 1. The term chronic fatigue syndrome (CFS) is used to describe
DWP MEDICAL GUIDANCE VERSION 10 (May 2007) CHRONIC FATIGUE SYNDROME AND MYALGIC ENCEPHALOMYELITIS/ENCEPHALOPATHY What is it? (Definition) 1. The term chronic fatigue syndrome (CFS) is used to describe
DISORDERS OF THE NERVOUS SYSTEM
 DISORDERS OF THE NERVOUS SYSTEM Bell Work What s your reaction time? Go to this website and check it out: https://www.justpark.com/creative/reaction-timetest/ Read the following brief article and summarize
DISORDERS OF THE NERVOUS SYSTEM Bell Work What s your reaction time? Go to this website and check it out: https://www.justpark.com/creative/reaction-timetest/ Read the following brief article and summarize
Idiopathic Photosensitive Occipital Lobe Epilepsy
 Idiopathic Photosensitive Occipital Lobe Epilepsy 2 Idiopathic photosensitive occipital lobe epilepsy (IPOE) 5, 12, 73, 75, 109, 110 manifests with focal seizures of occipital lobe origin, which are elicited
Idiopathic Photosensitive Occipital Lobe Epilepsy 2 Idiopathic photosensitive occipital lobe epilepsy (IPOE) 5, 12, 73, 75, 109, 110 manifests with focal seizures of occipital lobe origin, which are elicited
Cardiovascular History Taking. Dr. Amitesh Aggarwal Assistant Professor Department of Medicine
 Cardiovascular History Taking Dr. Amitesh Aggarwal Assistant Professor Department of Medicine Overview Patient details Presenting Complaint History of Presenting Complaint Past Medical History Medications
Cardiovascular History Taking Dr. Amitesh Aggarwal Assistant Professor Department of Medicine Overview Patient details Presenting Complaint History of Presenting Complaint Past Medical History Medications
General appearance examination
 Childhood athletic participation has dramatically increased over the past twenty years. Children are being introduced to organised sports at increasingly immature stages of physical development. It is
Childhood athletic participation has dramatically increased over the past twenty years. Children are being introduced to organised sports at increasingly immature stages of physical development. It is
Introduction. What is RSD? Causes of RSD. What Makes Reflex Sympathetic Dystrophy So Complicated?
 What Makes Reflex Sympathetic Dystrophy So Complicated? Article originally appeared in inmotion Magazine: Volume 14 Issue 5 September/October 2004 Introduction Because this condition is so complex, the
What Makes Reflex Sympathetic Dystrophy So Complicated? Article originally appeared in inmotion Magazine: Volume 14 Issue 5 September/October 2004 Introduction Because this condition is so complex, the
Epilepsy DOJ Lecture Masud Seyal, M.D., Ph.D. Department of Neurology University of California, Davis
 Epilepsy DOJ Lecture - 2005 Masud Seyal, M.D., Ph.D. Department of Neurology University of California, Davis Epilepsy SEIZURE: A temporary dysfunction of the brain resulting from a self-limited abnormal
Epilepsy DOJ Lecture - 2005 Masud Seyal, M.D., Ph.D. Department of Neurology University of California, Davis Epilepsy SEIZURE: A temporary dysfunction of the brain resulting from a self-limited abnormal
Nervous system Reflexes and Senses
 Nervous system Reflexes and Senses Physiology Lab-4 Wrood Slaim, MSc Department of Pharmacology and Toxicology University of Al-Mustansyria 2017-2018 Nervous System The nervous system is the part of an
Nervous system Reflexes and Senses Physiology Lab-4 Wrood Slaim, MSc Department of Pharmacology and Toxicology University of Al-Mustansyria 2017-2018 Nervous System The nervous system is the part of an
METHODS* following surgical resection of one occipital lobe indicated absence. fields. Results with the two methods are presented.
 SENSITIVITY TO LIGHT IN A CASE OF HYSTERICAL BLINDNESS STUDIED BY REINFORCEMENT- INHIBITION AND CONDITIONING METHODS* L. H. COHEN, E. R. HILGARD, AND G. R. WENDT A previous study of sensitivity to light
SENSITIVITY TO LIGHT IN A CASE OF HYSTERICAL BLINDNESS STUDIED BY REINFORCEMENT- INHIBITION AND CONDITIONING METHODS* L. H. COHEN, E. R. HILGARD, AND G. R. WENDT A previous study of sensitivity to light
Waccamaw Chiropractic & Wellness Center
 Waccamaw Chiropractic & Wellness Center Dr. John Evans Dr. Jeff Evans 658 Wachesaw Rd. Murrells Inlet, SC 29576 www. waccamawchiropractic.com (843)357-9617 Fax (843)357-9639 DO YOU HAVE ADRENAL FATIGUE?
Waccamaw Chiropractic & Wellness Center Dr. John Evans Dr. Jeff Evans 658 Wachesaw Rd. Murrells Inlet, SC 29576 www. waccamawchiropractic.com (843)357-9617 Fax (843)357-9639 DO YOU HAVE ADRENAL FATIGUE?
Fluoroquinolone-Associated Disability (FQAD) Cases in Patients Being Treated for Uncomplicated Sinusitis, Bronchitis, and/or Urinary Tract Infection
 Cases in Patients Being Treated for Uncomplicated Sinusitis, Bronchitis, and/or Urinary Tract Infection") Joint Meeting of the Antimicrobial Drugs Advisory Committee and the Drug Safety and Risk Management Advisory Committee November 5, 2015 FDA s Adverse Event Reporting System (FAERS) Review: Fluoroquinolone-Associated
Joint Meeting of the Antimicrobial Drugs Advisory Committee and the Drug Safety and Risk Management Advisory Committee November 5, 2015 FDA s Adverse Event Reporting System (FAERS) Review: Fluoroquinolone-Associated
HASPI Medical Anatomy & Physiology 09a Lab Activity
 HASPI Medical Anatomy & Physiology 09a Lab Activity Name(s): Period: Date: http://www.fallingpixel.com/products/33817/mains/0000-malemuscular_1.jpg The Muscular System The main function of the muscular
HASPI Medical Anatomy & Physiology 09a Lab Activity Name(s): Period: Date: http://www.fallingpixel.com/products/33817/mains/0000-malemuscular_1.jpg The Muscular System The main function of the muscular
Past Medical History. Chief Complaint: Patient Name: Appointment Date: Page 1
 Appointment Date: Page 1 Chief Complaint: (Please write reason, symptoms, condition or diagnosis that prompts your appointment) Past Medical History PERSONAL SKIN HISTORY YES NO Yes - Details Melanoma
Appointment Date: Page 1 Chief Complaint: (Please write reason, symptoms, condition or diagnosis that prompts your appointment) Past Medical History PERSONAL SKIN HISTORY YES NO Yes - Details Melanoma