I. Healing of the Extraction Site. Bach Le, DDS, MD, FICD, FACD. F. Kyle Yip, MS, DDS, MD. Normal extraction physiology
|
|
|
- June Doyle
- 5 years ago
- Views:
Transcription
1 I. Healing of the Extraction Site Bach Le, DDS, MD, FICD, FACD F. Kyle Yip, MS, DDS, MD Normal extraction physiology Early histologic studies in the mid-20 th century of human and animal extraction sockets by Mangos, 1 Christopher, 2 Amler, 3, 4 and Boyne, 5 explored in detail the early and late phases of socket healing. Evian further characterized socket healing between four and 16 weeks in 1982 utilizing biopsies of sockets and core biopsies. 6 The following sequence was generally seen in healthy sockets: 1. Day 1 Clot formation 2. Day 2-7 Granulation tissue fills socket 3. Day 4-20 Connective tissue replaces granulation tissue; spindle cells, collagen fibers, and early vascularity is seen 4. Day 7 Bone formation begins with uncalcified spicules and osteoid at the socket base and periphery 5. Day 20 Mineralization begins 6. Day 40 two-thirds socket filled with immature bone, lamina dura becomes lost 7. Day Bone matures into trabecular pattern resembling alveolus 8. Day 100 Socket density comparable to surrounding bone, minimal residual osteogenic activity Socket Epithelialization Proliferation of epithelium at the periphery of the socket was noted by Amler to begin at day 4. 3 Amler and Mangos found complete fusion of the overlying epithelium around day 20-30, although some sockets were noted to remain incompletely covered at day 35. 1, 3 Amler noted that epithelialization was delayed by sloughing epithelium at edges of ragged and traumatized native epithelium, but minimal sloughing was found at the edges where clean incisions were made. 3 Dimensional Changes of the Socket and Ridge The alveolar process is comprised of both cortical and bundle bone. The term bundle bone is used because of the insertion of Sharpey s fibers from the periodontal ligament (PDL). It comprises a thin layer surrounding teeth, while the remainder of the alveolus is cortical bone. Al-Hezaimi et al. demonstrated in monkeys that the blood supply to the alveolar process surrounding teeth comes from the PDL, interdental bone, and overlying supraperiosteal vessels. 7 During tooth extraction, loss of the PDL and damage to the interdental bone and vasculature results in resorption of the bundle bone. Araujo demonstrated in dogs that the bundle bone is replaced by woven bone, resulting in significant vertical reduction of the buccal crest. 8 The outer surfaces subsequently resorb on both buccal and lingual aspects, resulting in horizontal bone loss. In single
2 extraction sites or small areas, up to 50% reduction in width may occur in the first year, with the majority occurring in the first 3 months. 9 The buccal plate resorbs at a greater degree than the lingual plate, 8 resulting in a lingual migration of the alveolar crest. In multiple extraction sockets, damage to interdental vasculature and loss of PDLs results in proportionally more width and height reduction than single sites. 10 A systematic review in 2009 of 11 papers reported a mean reduction in alveolar ridge width of 3.87 mm after tooth loss 11. II. Atraumatic Tooth Extraction Tooth extraction should involve as minimal injury as possible to the surrounding bone and soft tissue. 7, 12 Damage to the labial plate can exacerbate horizontal and vertical resorption, while damage to the interproximal bone can result in loss of papilla. Unnecessary flap elevation should be avoided to minimize devascularization of the labial plate and exacerbate labial bone loss. 12, 13 Flap elevation during tooth removal has been reported to increase bone resorption by 16%. 12 Sectioning of teeth and the judicious use of peritomes, proximators, and luxators will aid in expansion of the PDL space and tooth removal while limiting trauma to the surrounding alveolus. Once the tooth is removed, the socket should be inspected in all dimensions for integrity of the surrounding bone III. SOCKET PRESERVATION AND AUGMENTATION Adequate crestal bone and ridge thickness is a prerequisite for implant placement. 18 Alveolar bone loss after extraction may result in compromised implant position or angulation. Since buccal bone is more susceptible to resorption than other areas of the alveolar ridge, 19, 20 techniques to maintain or correct existing defects are necessary for ideal implant placement. Socket grafting for ridge preservation has been advocated to decrease the amount of bone loss following tooth extraction Socket grafting, socket augmentation, and ridge preservation also are commonly used terms to describe grafting of the socket. Controlled animal and clinical studies have demonstrated a significant reduction in bone loss after tooth extraction when socket grafting is performed. 21, This may obviate the need to undergo more invasive bone augmentation procedures, thereby shortening treatment duration. Some opponents of socket grafting claim that placing foreign material may hinder bone growth and become osseo-obtrusive Histology from these studies have demonstrated a decrease in vital bone formation with retention of graft particles up to four years after placement. Stavropoulos 34 studied xenograft compared to no graft in a guided tissue regeneration (GTR) rat model and found interference of new bone formation with xenograft. Utilizing a Teflon capsule for space maintenance, xenograft was compared to empty space. Histology at one year after grafting showed that bovine bone xenograft resulted in only 23% volume of newly formed bone compared with 88% in the empty capsule control group. Nevertheless, the presence of residual graft materials at four months after socket augmentation has not been
3 shown to affect the osseointegration of implants. 35 IV. GRAFT MATERIALS Autogenous bone Araujo 36 demonstrated histologically in a dog model that autologous bone chips in a fresh extraction socket were almost completely resorbed (2% residual non-vital bone chips) at the 3-month mark. Overall, the autologous bone chips did not stimulate or retard bone formation, but failed to prevent ridge resorption after tooth extraction. However in a human study with iliac crest bone graft, Pelegrine 37 demonstrated no statistically significant change in the amount of mineralized bone after 6-months (42% vs. 45%), but did show a reduction in ridge resorption compared to untreated controls (1.14 mm vs mm horizontal, 0.62 mm vs mm vertical). These limited studies show autogenous bone may be a viable graft material, but will require an additional surgical site and increased morbidity. Allograft Allografts also have been studied for socket preservation. Histologic analyses of sites grafted with allograft have shown adequate bone formation for implant osseointegration. 38 Mineralized human allograft has demonstrated a range from 27-68% vital new bone formation, 4-15% residual graft particles, and 38-58% non-bone connective tissue in various histologic studies taken at four to six months. 24, 30, 39, 40 This appears to demonstrate greater vital new bone formation and decreased residual graft particles compared to bovinederived bone material (xenograft) ( % vital new bone formation, 26-36% residual graft particles at eight to nine months). 23, 41 The timing of implant placement after socket grafting has had limited study. Beck and Mealey 42 compared biopsies at the 3-month and 6-month post-operative time point after ridge preservation with mineralized allograft. They demonstrated similar new bone formation (45.8% vs. 45%) and residual graft material (14.6% and 13.5%) at the 3-month and 6-month post-operative periods respectively. There is some debate between the use of mineralized and demineralized variants of allograft. Mineralized bone retains more structural integrity, while the decalfication of demineralized bone is thought to expose bone morphogenetic protein BMP and increase osteoinduction. 43, 44 Wood and Mealey 45 demonstrated at the 4-month mark after augmenting intact sockets that demineralized bone allograft had a significantly greater percentage of vital bone (38.4% vs. 24.6%) and significantly lower percentage of residual graft particles (8.8% vs. 25.4%) when compared to mineralized bone. Neither showed any significant difference in alveolar ridge changes. However, sockets with buccal wall defects or atrophic ridges may not be adequately treated using demineralized graft material due to its lack of structure. Mineralized grafts have been shown to produce comparable results to autogenous bone for augmentation in atrophic alveolar ridges, 46 and longterm structural stability. 14, 47
4 Xenograft Xenograft is bone material derived from animal sources such as bovine or porcine bone. Bovine bone matrix has been reported to preserve the alveolar ridge with adequate bone formation and enable successful implant placement. 35, 48, 49 Histologic analysis of bone retrieved nine years after sinus augmentation and implant placement revealed that bovine graft remnants persisted (16%), and newly formed bone accounted for only 46% of the biopsy specimens. 50 This persistence of graft materials is consistent with other reports taken after implant loading from six months to four years These authors noted that the bovine graft material was in intimate contact with newly formed bone, and that newly formed bone was in intimate contact with implant surfaces. While the graft material may remain, its slow resorbing qualities may aid its function in space maintenance. There were no differences in vital bone to implant contact when comparing sinus augmentations with xenograft vs. autogenous bone. 54 While certain graft materials, xenografts in particular, demonstrate very slow resorption rates, it is not conclusive whether this affects vital bone formation or if any effect is clinically significant with respect to implant success. The success of integration and initial implant survival is dependent on two aspects of bone quality; 55 the density and rigidity of bone and hence its ability to establish primary stability, and the availability of vital bone for bone-to-implant contact at the microscopic level. It has been shown that boneto-implant contact around osseointegrated implants ranges from 42% to 96%, 56 but it is unknown what absolute minimum is required for long-term success. Studies comparing autografts to xenografts with histologic analysis of bone-to-implant contact have shown similar degrees of osseointegration, and residual graft particles incorporated in direct contact with newly formed bone. 57, 58 This is consistent with systematic reviews that have demonstrated no decrease in survival rates with implants placed in GBR-treated sites 59 and augmented sinuses. 60 Alloplast The term alloplast encompasses bone substitute material that is synthetic in nature. This can include a variety of materials including but not limited to hydroxyapatite variants, bioactive glass, calcium sulfate, and collagen. Advantages for using synthetic material include eliminating the risk of disease transmission, and the avoidance of biologic materials that patients may refuse for personal or religious reasons. Clinical and histologic studies have shown that various alloplasts demonstrate improved vital bone formation and reduced residual graft material to allografts and xenografts, and are appropriate for socket grafting. 63 However, a recent systematic review 64 of randomized controlled clinical trials of various graft materials revealed that while histologic outcomes were better with alloplasts, there was no decrease in ridge dimension loss compared to sockets with no grafting. However, sockets grafted with allografts and xenografts showed significant reduction in loss of ridge dimensions. This suggests that while alloplasts demonstrate good osteoconductive properties, they may not have the structural stability needed to maintain or augment ridge dimensions. 55, 61,


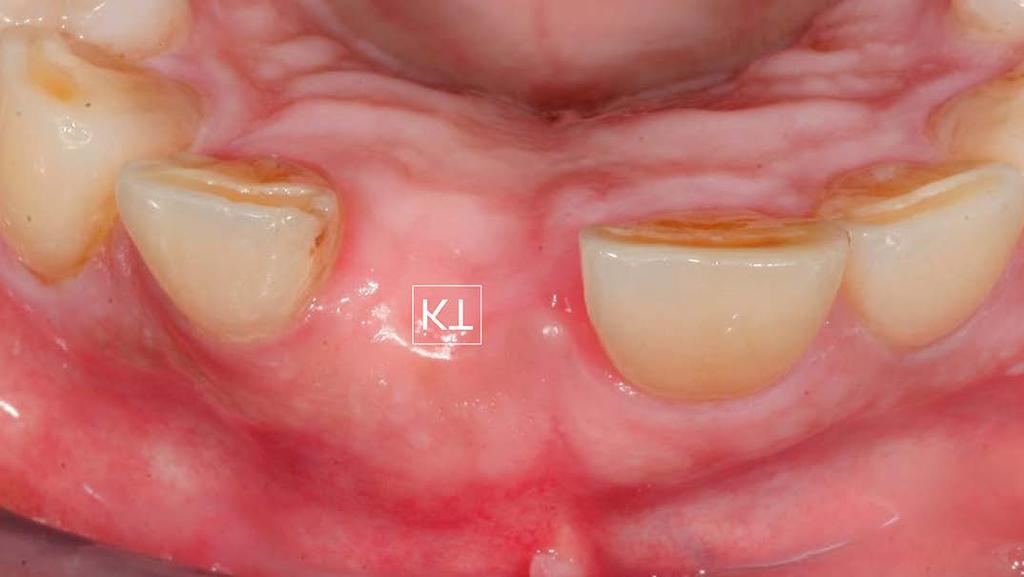
5 Particle size In selecting particulate graft material, particle size is an important consideration. In a controlled animal study, cortical allograft with particle sizes between microns produced rapid healing by direct ossification when placed into critical-sized defects, while particles larger than 300 µm healed more slowly, and those that were too small were not osseoconductive. 65 Although graft materials of different types and sizes are capable of bone formation when used for socket preservation, a thorough understanding of the material of choice and its handling properties is important for successful ridge preservation and subsequent dental implant placement. V. TECHNIQUE Sockets with intact labial walls Fig. 1A Fig. 1B


6 Fig. 1C Fig. 1D Various techniques have been described for ridge preservation after tooth extraction. One technique involves partially filling the socket with graft material and then occluding the top of the socket with a collagen plug to protect the graft. 39 No flap is elevated, and a figure-of-eight suture is utilized to help retain the collagen dressing. Other authors suggest utilizing a free gingival graft taken from the palate, 66 while others do not use any occlusive dressing. 67 Another technique involves raising a mucoperiosteal flap to secure the bone graft with a membrane. 24, 68 For socket defects with an intact labial plate and normal crest level, the senior author prefers to place a small-particle cancellous allograft without a barrier membrane. (Figure 1A-D)

7 Several recent systematic reviews have been unable to demonstrate superiority of one ridge preservation technique over another, although two 29, 72 suggested that flap elevation and membrane usage might improve results. Furthermore, although these reviews demonstrate socket grafting can minimize ridge resorption, there is no conclusive evidence that these procedures improve the ability to place implants. 70 Further study focusing on long-term esthetic outcomes of implants after socket augmentation is needed. 73 Sockets with labial wall defects Fig. 2A

8 Fig. 2B


9 Fig. 2C


10 Fig. 2D Fig. 2E Fig. 2F

11 Fig. 2G Fig. 2H


12 Fig. 2I Fig. 2J



13 Fig. 2K Fig. 2L Fig. 2M
 Teeth with periapical radiolucencies, labial fistulas, or lost as a result of trauma often have compromised labial walls.")
14 Fig. 2N Teeth with labial wall defects require socket augmentation using guided tissue regeneration with an open flap procedure to fully correct or overcorrect the alveolar ridge to achieve ideal contours. (Figure 2A-N) Teeth with periapical radiolucencies, labial fistulas, or lost as a result of trauma often have compromised labial walls. These defects can lose as much as 40%-60% of the alveolar ridge width within 1-year. 20, 74, 75 Different techniques to address labial wall defects using guided tissue regeneration have been described. Although adequate clinical documentation is still lacking, a flapless approach has been described, which involves positioning a barrier membrane within the socket and packing mineralized allograft into the socket. 68 While a flapless surgery may be technically easier to perform, this technique inherently limits bone regeneration to the confines of the socket, and likely resorbs past the confines of the original labial wall during the healing process. 17 Anatomical contours may not be achieved, necessitating further augmentation procedures. Augmentation with an open-flap approach is recommended for sockets with labial wall defects, yielding predictable peri-implant tissue, bone stability, and contour. 15, 76, 78 The senior author prefers to use the open book flap for augmentation of these defects, particularly in sites where there is loss of labial attached tissue

15 Fig. 15A (See Figure 15 A). The open book flap is developed with a crestal incision made slightly lingual to the ridge midline to preserve an adequate amount of keratinized tissue in the flap. This is followed by a distal, curvilinear, vertical incision that follows the gingival margin of the distal tooth. A wide subperiosteal reflection is made to expose 2 to 3 times the treatment area, and then the papilla is reflected on the mesial side of the edentulous site.

16 Fig. 3A Fig. 3B (Figure 3A-B) Raising a flap for correction of the anatomical defect allows for flap release and tension-free expansion of the soft tissue matrix. Secondary bone augmentation may still be required in larger defects with multiple missing walls. Tenting screws may be used for overcorrection of the defect and support of the overlying tissue. 47 Because most bone graft procedures inherently result in secondary remodeling and resorption, 79 it is important to factor in the amount of anticipated resorption by overcorrecting the defects
17 so that the critical 2 mm threshold of labial bone is achieved in the final result.(see Figure 2E) Barrier membranes Ridge preservation may be performed with or without the use of membranes Recent systematic reviews have suggested that the use of membranes improves graft stability. 29, 72 As a socket heals, bone healing progresses at a slower rate than the overlying soft-tissue, resulting in loss of dimension. Membranes function by preventing soft-tissue ingrowth and allowing the bone matrix to mature. Non-resorbable membranes predictably prevent epithelial in-growth 1, but are more susceptible to exposure and have higher rates of infection compared to bioresorbable membranes. 85 Some studies have shown the higher exposure rate does not always equate to graft resorption. 80, 84 One randomized controlled study compared non-resorbable polytetrafluoroethylene (PTFE) membranes to resorbable collagen membranes for ridge preservation without primary closure. The authors did not find any significant difference in clinical or histologic outcomes between the two interventions. Both groups resulted in keratinized tissue covering the exposed membrane by secondary intention. 86 Barone et al., 87 in a clinical study on socket augmentation with healing by secondary intention, reported secondary soft tissue healing over grafted sockets did not compromise bone formation and soft tissue level and width of keratinized tissue were improved. (see Figure 2G-H) Other studies have demonstrated better tolerance with exposure of resorbable membranes. VI. Immediate implants Although immediate implants have been shown to integrate with high success rates similar to implants placed with a delayed approach, 17, studies have shown that implants placed into extraction sockets do not necessarily prevent alveolar ridge changes, and may often be subject to some labial gingival recession. 89, 90, 95, 96 22, 88

18 Fig. 4 (Figure 4) In a retrospective analysis of 42 single-tooth implants placed in the esthetic zone, Evans et al. 97 found a highly significant change in crown height due to marginal tissue recession of approximately 1 mm, with no difference seen between implant systems. Thin tissue biotypes showed slightly greater recession than thick-tissue biotypes. 97 Various technical advances have improved marginal bone loss and soft tissue recession after immediate implant placement. These differences are due to a number of important advances, including the introduction of platform-switch designs, immediate provisionalization, and advanced understanding of implant positioning. Platform-switching Recent short-term studies have reported diminished crestal bone loss and better peri-implant maintenance when the implant-crown margin is moved away from the outer circumference of the implant and repositioned inward, closer to the center of the implant s restorative platform This technique is now commonly known as platform-switching. 102 Platform switching has been shown to reduce marginal bone loss in a proportional manner to the abutment-implant discrepancy. 100, 103 Canullo followed 22 patients with immediate implants and provisionalization for two years, and demonstrated less facial recession and more papilla height in platform switched immediate implants compared to controls. 100 One study reported that this restorative technique allows implants to be placed closer together with less crestal bone loss. 104 As long-term documentation becomes available, utilizing the platform-switching concept may enable esthetic

19 outcomes with the placement of multiple adjacent implants. Immediate provisional restoration Immediate placement of dental implants into fresh extraction sockets with immediate delivery of a provisional restoration in the esthetic zone is a concept first reported by Wöhrle 105 in A recent systematic review by Slagter demonstrated that immediate provisionalization at the time of immediate placement in sockets with intact bony walls minimizes bone level changes to <0.5 mm without affecting survival rates. 106 Fig. 5A


20 Fig. 5B Fig. 5C


21 Fig. 5D Fig. 5E


22 Fig. 5F Fig. 5G


23 Fig. 5H Fig. 5I

24 Fig. 5J (Figure 5A-J) Block et al. 107 found no statistically significant differences in crestal or interproximal bone levels when comparing immediate or delayed implant placement with immediate provisionalization in the anterior maxilla. The authors concluded that immediate implant placement with provisionalization resulted in approximately 1 mm less facial gingival recession compared with that in the delayed group. 107 DeRouk 108 also found in a 1-year single-blind randomized study that submerged implant placement followed by delayed restoration had significantly more midfacial recession (0.75 mm additional) compared to immediate provisionalization. This is consistent with observations from previous studies that demonstrated immediate 109 and delayed 110 changes in peri-implant tissue after restoration delivery, indicating that adaptive responses to provisional contours may help maintain tissue levels. Buccal plate integrity and thickness An implant placed into an intact extraction socket, has been shown to osseointegrate and form bone as long as a stable blood clot can be maintained. 92, Fresh sockets with a thick labial plate >1 mm will respond more favorably to treatment with immediate implants with less facial recession. The flapless approach for immediate placement should be the preferred technique in these cases to reduce loss of buccal bone width and height. Thin labial plates (< 1 mm thickness) demonstrated increased labial resorption and decreased gap fill. 114 Januario et al. reported that over 50% of maxillary anterior teeth have labial plate < 0.5 mm. 115 In these cases, an open flap approach with with external grafting of the socket wall for overcorrection of ridge contours should be considered. (see Figure 2A-N) Immediate implants with buccal wall defects Controversies exist in the literature regarding the proper management of extraction sockets with a buccal plate defect. Historically, the literature does not recommend immediate implants if the buccal plate is compromised due to the increased risk of labial marginal recession. 116 However, multiple authors have
 implant placement and simultaneous augmentation of 156 sites with vertical buccal defect using a mineralized particulate allograft covered with a")
25 demonstrated predictable implant survival with simultaneous GBR of facial wall defects with immediate implant placement. 17, 77, 117 Le et al. assessed the outcome of single stage (non-submerged) implant placement and simultaneous augmentation of 156 sites with vertical buccal defect using a mineralized particulate allograft covered with a collagen membrane. 14 The vertical buccal defects were classified as small (less than 3 mm in depth), medium (3 5 mm in depth), and large (greater than 5 mm in depth). The initial vertical buccal wall defect was recorded by measuring the amount of vertical implant platform s rough surface exposure after implants were placed. Sectional CBCT scans were used at 36 months after graft healing. The site of the original vertical bone defect was evaluated for the presence of any residual vertical bone defect. The results showed the presence of bone in 100% and 79.3% of small and medium size vertical defects, respectively. Large size defects showed only partial improvement without any complete correction. Single-stage implant placement with simultaneous bone grafting to support the soft tissue margin showed promising outcomes in correcting vertical buccal wall defects of less than 3 mm. Fig. 6A

26 Fig. 6B


27 Fig. 6C Fig. 6D


28 Fig. 6E


29 Fig. 6F Fig. 6G Fig. 6H

30 Fig. 6I (Figure 6A-I) Kan studied twenty-three patients with immediate implant placement with facial wall defects and guided bone regeneration, and found that the defect morphology was highly correlated with gingival recession after one year. 17 In patients with a V-shaped defect where the interproximal boundaries of the defect were intact, only one out of 12 patients demonstrated greater than 1.5 mm recession. In U-shaped or Ultra-U-Shaped defects however, where either or both sides of interproximal bone was compromised, >1.5 mm recession was found in 43% and 100% of cases. This emphasizes the concept that graft material must have some amount of housing by native bone in order to adequately consolidate and regenerate new bone. 117 A 3-walled defect, after immediate implant placement, effectively leaves a 2-walled defect or zero or 1-walled defect. This is dependent on the condition of interproximal bone and the buccal-lingual positioning of the implant. Interestingly, Zitzmann et al. suggested that immediate or early (within 6 weeks to 6 months but after soft tissue coverage of the socket) implant placement and GBR allows for improved defect correction compared to delayed placement and GBR. 117 The authors found that more ridge resorption had occurred in the delayed group, resulting in 92% of these defects demonstrating zero or a 1-wall defect, and poorer defect correction compared to immediate and early groups. 117 In the case of apical facial wall defects, where the crestal aspect of the buccal bone is intact and sufficiently thick, the implant can be placed in a flapless manner to minimize ridge remodeling. 118 The apical dehiscence can then be addressed with a small flap through the mucosa and guided bone regeneration. 119 Biotype Patients exhibit differences in their gingival phenotypes, often termed gingival biotypes. 120 Most patients fall into two categories: slender teeth with thin gingiva and scalloped periodontium, or square teeth with thick gingiva and blunted periodontium. 120, 121


31 Fig. 7A Fig. 7B (Figure 7A-B) In a study of 100 volunteers, De Rouck et al. 121 demonstrated that approximately one-third of the patients exhibited thin biotype, which was usually associated with females. Two-thirds were thicker biotypes usually associated with males. They classified the two biotypes by using the translucency of the gingiva on probing as a marker for thickness: if the probe was visible through the facial gingival tissue, this was considered a thin biotype. 121 Much consideration has been given to the thickness of the gingiva related

32 to implant dentistry. The thinner biotype is more prone to recession and loss of interdental papilla While objective data studying esthetic outcomes with anterior implants are limited, 124 some clinicians advocate the routine use of connective tissue grafts to transform thin biotypes into thicker tissue for enhanced esthetic outcomes. 91 If an implant site exhibits a thin biotype, a connective tissue graft or bone augmentation should be considered prior to or simultaneously with implant placement. Peri-implant marginal gap (Jumping gap) When placing implants into fresh extraction sockets, a marginal defect around the implant may result, referred to as the jumping gap. Fig. 8 (Figure 8) Many practitioners have been placing bone grafts or bone substitutes into these defects, based on previous animal studies showing that a gap of more than 1 mm may lead to incomplete marginal bone formation and apical migration of the bony crest Conversely, a more recent animal study showed that defects larger than 1 mm eventually led to complete bone formation with a rough-surfaced implant, and no clinically detectable change in bone height. 112 The same authors subsequently found in a human study of 21 implants that gaps ranging from 1-3 mm healed predictably with new bone formation without the use of graft material or membrane. 92 This result was again confirmed in a split-mouth study with dogs and lingual
 implants showed a direct relationship between increasing gap size and bone")
 The authors concluded that 3 mm is the critical size for optimal buccal bone and soft tissue thickness to form.")
33 positioning of implants, with or without grafting of a 1.7 mm gap. No loss of bone height or difference was seen between groups. 111 Another prospective study in dogs 113 comparing buccal gap sizes of 1 mm, 2 mm, and 3 mm with Laser-Lok (Biohorizons) implants showed a direct relationship between increasing gap size and bone volume and soft tissue volume at 2-months. Furthermore, the authors demonstrated that a 3 mm gap was resistant to resorption at four months in comparison to the 1 mm and 2 mm groups. Fig. 9 (Figure 9) The authors concluded that 3 mm is the critical size for optimal buccal bone and soft tissue thickness to form. Tarnow, in a recent retrospective cohort study, evaluated 49 immediate implants in the esthetic zone without flap elevation, and compared groups +/- grafting of the gap and +/- provisionalization based on study casts measuring horizontal changes compared to contralateral control teeth. 129 They found that groups without grafting or provisionalization had an average of 1 mm buccal-palatal dimension change at 6 months to 4 years. Provisionalization reduced this to 0.6 mm change, and bone grafting reduced this to 0.3 mm change. A group with both provisionalization and grafting demonstrated only 0.1 mm change. These data suggested that provisionalization and grafting together most predictably maintain esthetic contours. Further comparative research in humans to determine the effect of gap size and grafting the gap on implant survival and esthetic outcomes still is needed. Implant position Dental implant therapy should be prosthetically driven and not primarily bone-driven. To this end, the implant must be accurately placed in a 3-D (mesiodistal, labiolingual, and apicocoronal) position with the goal of achieving a proper emergence profile for the final restoration. When the implant position is not accurate, the esthetic result is often compromised. Implants placed too deep apico-coronally or too labially often result in an unnaturally long restoration.
34

35

36 Fig. 10A Fig. 10B (Figure 10A-B) In addition, implant position has been shown to have a direct influence on bone and soft tissue thickness related to the implant. 76 Le et al. 130 studied the relationship between crestal labial soft tissue thickness and implant bucco-lingual angulation. The bucco-lingual angulation was recorded as cingulum, incisally, or labially-angled based on the position of the screw access hole of the provisional restoration. The implant labial bone thickness was measured at the crestal and mid-implant levels using sectional cone beam computed tomography scans. Of implants with cingulum, incisal, and labial angulations, 3.4%, 20%, and 53.3%, respectively, demonstrated crestal labial soft tissue thickness of < 2 mm. Implants with cingulum angulation had a mean crestal soft tissue thickness of 2.98 mm, while those with incisal and labial angulation had decreased mean tissue thickness of 2.24 and 1.71 mm, respectively.
. The investigators concluded that implants with labial angulations carry a higher risk of soft tissue complications when the crestal implant labial bone thickness is <2 mm.")

37 Fig. 11 (Figure 11) A significant association between crestal labial soft tissue thickness and implant bucco-lingual angulation was noted when implant labial bone thickness at crestal level was <2 mm (P < 0.01). The investigators concluded that implants with labial angulations carry a higher risk of soft tissue complications when the crestal implant labial bone thickness is <2 mm. Soft tissue grafting Several authors suggest concomitant connective tissue grafting to compensate for anticipated loss of labial tissue volume at the time of immediate implant placement in the maxillary anterior area. 131, 132 Grunder reported an average tissue collapse of 1.06 mm in the horizontal dimension without connective tissue augmentation, as compared to 0.34 mm gain with connective tissue grafting six months after surgery. 131 Rungcharassaeng noted an increase in tissue thickness after immediate implant placement in both grafted and non-grafted cases, but that grafted cases were significantly thicker than non-grafted cases. 132 Non-grafted cases demonstrated an increase from 1.1 mm to 1.4 mm, but grafted cases 132
38 demonstrated an increase from 1.2 mm to 2.6 mm. A minimum of 2 mm thickness is suggested to conceal zirconia, and 3 mm for all other restorative materials in the prosthesis. 133 In contrast, Le et al. 130, 134 demonstrated that proper implant positioning, angulation, and maintenance of buccal bone thickness led to facial soft tissue thickness without the need for connective tissue grafting. (Table 1) Multiple immediate implants Single-tooth implant restorations are more likely to have predictable soft tissue anatomy whereas multiple implants often have compromised soft tissue anatomy. 135 Loss of the interproximal bone and vasculature after multiple-tooth extraction results in a greater degree of bone loss and ridge remodeling than does singletooth extraction. 10 Sufficient distance must be present between implants in order to avoid inter-implant bone loss and shortened papilla height, 136 with 3 mm reported as the minimum to maintain an optimal papilla height. Although the type of implants used was not specified, some advocates of newer implant designs and surfaces have reported significantly less bone loss than older traditional implant designs. Novaes 137 demonstrated in a dog model with platform-switched implants that there was no difference between 1, 2, and 3 mm distances and papilla formation was established in all groups. If an adjacent central and lateral incisor is planned for implant-supported replacement, the lateral incisor site may be considered for substitution with a pontic. 138, 139 Soft tissue height between an implant and pontic has been reported to be as high as 5.5 mm, 140 and may allow for increased papillae height. Pontic site development has also been advocated in selected cases by using the root submergence technique 139 in order to maintain the underlying alveolar dimensions. When multiple teeth are indicated for extraction, a staged approach utilizing strategic extractions of selected teeth and fabrication of either a tooth-borne or implant-borne temporary fixed partial denture (FPD) will help to decrease bone loss and maintain the supporting bone and tissue architecture. 12, 141


39 Fig. 12A Fig. 12B


40 Fig. 12C Fig. 12D


41 Fig. 12E Fig. 12F

42 Fig. 12G

43 Fig. 12H (Figure 12A-H) In a controlled animal study, Favero et al. demonstrated that tooth extraction next to a socket into which an immediate implant is placed caused more bone loss in both bucco-lingual and mesiodistal dimensions compared with sites adjacent to a maintained tooth. 141 Socket shield technique A recent technique for alveolar ridge preservation, dubbed the socket shield technique, 142 has been proposed 139, whereby the buccal remnant of the root is intentionally retained to maintain the buccal bundle bone. Davarpanah 147 demonstrated successful implant placement and loading with implants in contact with ankylosed root fragments. Utilizing these principles, Hurzeler et al. 142, 148 placed immediate implants with an enamel matrix derivative (Emdogain) into hemi-sected roots of a dog, while maintaining a thin buccal veneer of the root. After four months, histology revealed that the alveolar crest was free of any resorptive process. The root fragment also demonstrated newly-formed cementum between areas of clinically direct contact with the implant threads. The implant body demonstrated mineralized tissue deposition and cementum between it surface and the root dentin. This concept was applied in a case study involving a central incisor with a root fracture, 142 and was subsequently adapted by Kan and Rungcharassaeng 149 with interproximal root fragments for maintenance of interproximal bone


44 Fig. 13A Fig. 13B

45 Fig. 13C (Figure 13A-C) Root fragments were maintained 1 mm coronal to the bone crest in order to maintain support of dentogingival tissue

46 Fig. 13D (Figure 13D), and implants were placed in an immediate fashion
47 Fig. 13E (Figure 13E). After implant healing and restoration, peri-implant bone and tissues were well maintained


48 Fig. 13F

49 Fig. 13G Fig. 13H Fig. 13I (Figure 13F-I). One additional retrospective study of 46 patients demonstrated 100% survival rate, with only 0.2 mm average bone loss over 2 to 5-year follow-up. One patient in their study demonstrated apical root resorption of the residual fragment, but this did not affect implant survival. Further study is needed on this
50 technique to evaluate its efficacy and utility. Immediate Molar implants Current literature suggests that immediate implant placement in molar sites demonstrates high survival rates from % While prospective, controlled clinical trials are limited, 151, 154, 160 a recent systematic review (2016) and meta-analysis of 768 implants demonstrated a cumulative survival rate of 98% with no difference between the maxilla and mandible. 158 Meta-analysis of marginal bone loss after at least 1 year was estimated to be 0.57 mm. 158 This is consistent with a previous systematic review of 1,013 immediate implants demonstrating a cumulative survival rate of 99%. 163 If sufficient primary stability is achievable, some authors also have demonstrated success with immediate occlusal loading Immediate implant placement in molar sites presents a few unique challenges. A pre-operative CBCT is critical to assess the position of the maxillary sinus for maxillary implant placement and the IA canal for mandibular implant placement. Considering molar prosthetics, a wider platform implant (5 mm) should be placed into the center of the socket for ideal axial loading and restoration. 167 Wider bodied implants also may help engage the walls of molar extraction sites and contribute lateral enforcement to primary stability. However, a recent systematic review has shown that ultra-wide implants (>6 mm) demonstrate a significantly higher failure rate (3.67 vs. 1.45%) than wide (4-6 mm) implants in molar extraction sites. 158 This suggests that an optimum implant width exists, larger than which may increase failure rates. Regardless of implant size, the molar site s multi-rooted void limits the amount of remaining bone for engagement and primary stability. To address this, some authors advocate sectioning of the crown and drilling the implant osteotomies prior to root removal in order to guide and stabilize the osteotomy position. 168 They reported a success rate of 19 out of 20 implants with one early failure and no late failures. If lateral stability is insufficient, apical bone may be engaged for primary stability if at least 5 mm of apical bone exists, but this is often precluded by the position of the sinus floor or inferior alveolar nerve. Grafting vs. non-grafting of the residual socket gaps does not appear to change implant survival or marginal bone levels. 159 Maxillary extraction sites are unique due to tri-rooted sockets that may reduce available horizontal bone, and also may be limited vertically by sinus pneumatization. A CBCT study of 95 patients demonstrated the mean distance between the sinus floor and maxillary first molar mesio-buccal, distal-buccal, and palatal root apices as mm, 0.32 mm, and -2.2 mm respectively. 169 The mean distance from the maxillary first molar furcation to sinus floor was 6.51 mm (SD=2.94 mm). Forty-six percent of patients demonstrated >5 mm apical bone and 68% of patients demonstrated >5 mm horizontal bone between root apices sufficient for implant placement. 169 If sufficient horizontal bone and a minimum of 4 mm vertical native bone exists, 170 an osteotome sinus elevation may be performed simultaneously with immediate implant placement. 152, 153, 155 With less than 4 mm native bone, a lateral window sinus elevation 171 is recommended either in a simultaneous 172 or staged approach.

51 Immediate implants in localized infections Immediate implants placed into sites with localized infection such as periapical radiolucencies have shown equal survival to non-infected sites. Chrcanovic, in their systematic review, evaluated immediate placement of implants into infected sites. Although a cumulative survival was not calculated, all twenty-one human studies demonstrated over 90% survival, with the vast majority over 97%. 173 This is consistent with earlier systematic reviews demonstrating high success of immediate placement of implants into infected sites. 174 Risk Assessment Procedures with a high level of predictability will have a small number of esthetic failures defined by significant tissue recession or exposure of the abutment margin. Based on the many important factors that may affect the esthetic outcome of immediate implant treatment, we recommend a thorough risk assessment analysis when considering immediate implant as a treatment option. Fig. 14 (Figure 14) VII. SUMMARY It is reported that up to 16% of single implant restorations in the esthetic zone fail for esthetic reasons, with gingival recession and a lack of interdental papilla being the most common complications. Esthetic outcomes are predictable with a thorough understanding of bone and soft tissue physiology and implant principles. Most complications can be avoided with proper treatment planning and execution.. 1. Mangos, J.F., The healing of extraction wounds. New Zealand Dental Journal, (4). 2. Christopher, E.R., Histological study of bone healing in relation to the extraction of teeth. Northwest University Bul., (5). 3. Amler, M.H., P.L. Johnson, and I. Salman, Histological and histochemical investigation of human alveolar socket healing in undisturbed extraction wounds. J Am Dent Assoc, : p Amler, M.H., The time sequence of tissue regeneration in human extraction wounds. Oral Surg Oral Med
52 Oral Pathol, (3): p Boyne, P.J., Osseous repair of the postextraction alveolus in man. Oral Surg Oral Med Oral Pathol, (6): p Evian, C.I., et al., The osteogenic activity of bone removed from healing extraction sockets in humans. J Periodontol, (2): p Al-Hezaimi, K., et al., An extraction socket classification developed using analysis of bone type and blood supply to the buccal bone in monkeys. Int J Periodontics Restorative Dent, (4): p Araujo, M.G. and J. Lindhe, Dimensional ridge alterations following tooth extraction. An experimental study in the dog. J Clin Periodontol, (2): p Schropp, L., et al., Bone healing and soft tissue contour changes following single-tooth extraction: a clinical and radiographic 12-month prospective study. Int J Periodontics Restorative Dent, (4): p Al-Askar, M., et al., Effect of single and contiguous teeth extractions on alveolar bone remodeling: a study in dogs. Clin Implant Dent Relat Res, (4): p Van der Weijden, F., F. Dell'Acqua, and D.E. Slot, Alveolar bone dimensional changes of post-extraction sockets in humans: a systematic review. J Clin Periodontol, (12): p Fickl, S., et al., Tissue alterations after tooth extraction with and without surgical trauma: a volumetric study in the beagle dog. J Clin Periodontol, (4): p Blanco, J., et al., Biological width following immediate implant placement in the dog: flap vs. flapless surgery. Clin Oral Implants Res, (6): p Le, B.T. and A. Borzabadi-Farahani, Simultaneous implant placement and bone grafting with particulate mineralized allograft in sites with buccal wall defects, a three-year follow-up and review of literature. J Craniomaxillofac Surg, (5): p Le, B. and J. Burstein, Esthetic grafting for small volume hard and soft tissue contour defects for implant site development. Implant Dent, (2): p Park, S.H. and H.L. Wang, Management of localized buccal dehiscence defect with allografts and acellular dermal matrix. Int J Periodontics Restorative Dent, (6): p Kan, J.Y., et al., Effects of the facial osseous defect morphology on gingival dynamics after immediate tooth replacement and guided bone regeneration: 1-year results. J Oral Maxillofac Surg, (7 Suppl 1): p Spray, J.R., et al., The influence of bone thickness on facial marginal bone response: stage 1 placement
53 through stage 2 uncovering. Ann Periodontol, (1): p Fickl, S., et al., Hard tissue alterations after socket preservation: an experimental study in the beagle dog. Clin Oral Implants Res, (11): p Pietrokovski, J. and M. Massler, Alveolar ridge resorption following tooth extraction. J Prosthet Dent, (1): p Barone, A., et al., Xenograft versus extraction alone for ridge preservation after tooth removal: a clinical and histomorphometric study. J Periodontol, (8): p Lekovic, V., et al., A bone regenerative approach to alveolar ridge maintenance following tooth extraction. Report of 10 cases. J Periodontol, (6): p Artzi, Z., H. Tal, and D. Dayan, Porous bovine bone mineral in healing of human extraction sockets. Part 1: histomorphometric evaluations at 9 months. J Periodontol, (6): p Iasella, J.M., et al., Ridge preservation with freeze-dried bone allograft and a collagen membrane compared to extraction alone for implant site development: a clinical and histologic study in humans. J Periodontol, (7): p Fickl, S., et al., Dimensional changes of the alveolar ridge contour after different socket preservation techniques. J Clin Periodontol, (10): p Fickl, S., et al., Hard tissue alterations after socket preservation with additional buccal overbuilding: a study in the beagle dog. J Clin Periodontol, (10): p Fickl, S., et al., Dimensional changes of the ridge contour after socket preservation and buccal overbuilding: an animal study. J Clin Periodontol, (5): p Ten Heggeler, J.M., D.E. Slot, and G.A. Van der Weijden, Effect of socket preservation therapies following tooth extraction in non-molar regions in humans: a systematic review. Clin Oral Implants Res, (8): p Vittorini Orgeas, G., et al., Surgical techniques for alveolar socket preservation: a systematic review. Int J Oral Maxillofac Implants, (4): p Becker, W., et al., Histologic findings after implantation and evaluation of different grafting materials and titanium micro screws into extraction sockets: case reports. J Periodontol, (4): p Zitzmann, N.U., et al., Alveolar ridge augmentation with Bio-Oss: a histologic study in humans. Int J Periodontics Restorative Dent, (3): p Simion, M., P. Trisi, and A. Piattelli, GBR with an e-ptfe membrane associated with DFDBA: histologic and histochemical analysis in a human implant retrieved after 4 years of loading. Int J Periodontics
54 Restorative Dent, (4): p Araujo, M., E. Linder, and J. Lindhe, Effect of a xenograft on early bone formation in extraction sockets: an experimental study in dog. Clin Oral Implants Res, (1): p Stavropoulos, A., et al., Deproteinized bovine bone (Bio-Oss) and bioactive glass (Biogran) arrest bone formation when used as an adjunct to guided tissue regeneration (GTR): an experimental study in the rat. J Clin Periodontol, (7): p Molly, L., et al., Bone formation following implantation of bone biomaterials into extraction sites. J Periodontol, (6): p Araujo, M.G. and J. Lindhe, Socket grafting with the use of autologous bone: an experimental study in the dog. Clin Oral Implants Res, (1): p Pelegrine, A.A., et al., Clinical and histomorphometric evaluation of extraction sockets treated with an autologous bone marrow graft. Clin Oral Implants Res, (5): p Minichetti, J.C., et al., Human histologic analysis of mineralized bone allograft (Puros) placement before implant surgery. J Oral Implantol, (2): p Wang, H.L. and Y.P. Tsao, Mineralized bone allograft-plug socket augmentation: rationale and technique. Implant Dent, (1): p Fotek, P.D., R.F. Neiva, and H.L. Wang, Comparison of dermal matrix and polytetrafluoroethylene membrane for socket bone augmentation: a clinical and histologic study. J Periodontol, (5): p Ferreira, C.E., et al., Grafting the nasal cavity with 100% anorganic bovine bone: a clinical and histomorphometric pilot report. Int J Oral Maxillofac Implants, (3): p Beck, T.M. and B.L. Mealey, Histologic analysis of healing after tooth extraction with ridge preservation using mineralized human bone allograft. J Periodontol, (12): p Kolk, A., et al., Current trends and future perspectives of bone substitute materials - from space holders to innovative biomaterials. J Craniomaxillofac Surg, (8): p Urist, M.R. and B.S. Strates, Bone morphogenetic protein. J Dent Res, (6): p Wood, R.A. and B.L. Mealey, Histologic comparison of healing after tooth extraction with ridge preservation using mineralized versus demineralized freeze-dried bone allograft. J Periodontol, (3): p Beitlitum, I., Z. Artzi, and C.E. Nemcovsky, Clinical evaluation of particulate allogeneic with and without autogenous bone grafts and resorbable collagen membranes for bone augmentation of atrophic
55 alveolar ridges. Clin Oral Implants Res, (11): p Le, B., M.D. Rohrer, and H.S. Prasad, Screw "tent-pole" grafting technique for reconstruction of large vertical alveolar ridge defects using human mineralized allograft for implant site preparation. J Oral Maxillofac Surg, (2): p Sclar, A.G., Preserving alveolar ridge anatomy following tooth removal in conjunction with immediate implant placement. The Bio-Col technique. Atlas Oral Maxillofac Surg Clin North Am, (2): p Araujo, M., et al., The influence of Bio-Oss Collagen on healing of an extraction socket: an experimental study in the dog. Int J Periodontics Restorative Dent, (2): p Traini, T., et al., A histologic and histomorphometric evaluation of anorganic bovine bone retrieved 9 years after a sinus augmentation procedure. J Periodontol, (5): p Piattelli, M., et al., Bone reactions to anorganic bovine bone (Bio-Oss) used in sinus augmentation procedures: a histologic long-term report of 20 cases in humans. Int J Oral Maxillofac Implants, (6): p Scarano, A., et al., Osseointegration in a sinus augmented with bovine porous bone mineral: histological results in an implant retrieved 4 years after insertion. A case report. J Periodontol, (8): p Rosenlicht, J.L. and D.P. Tarnow, Human histologic evidence of integration of functionally loaded hydroxyapatite-coated implants placed simultaneously with sinus augmentation: a case report 2 1/2 years postplacement. J Oral Implantol, (1): p Hallman, M., L. Sennerby, and S. Lundgren, A clinical and histologic evaluation of implant integration in the posterior maxilla after sinus floor augmentation with autogenous bone, bovine hydroxyapatite, or a 20:80 mixture. Int J Oral Maxillofac Implants, (5): p Chan, H.L., et al., Alterations in bone quality after socket preservation with grafting materials: a systematic review. Int J Oral Maxillofac Implants, (3): p Degidi, M., et al., Mineralized bone-implant contact and implant stability quotient in 16 human implants retrieved after early healing periods: a histologic and histomorphometric evaluation. Int J Oral Maxillofac Implants, (1): p Berglundh, T. and J. Lindhe, Healing around implants placed in bone defects treated with Bio-Oss. An experimental study in the dog. Clin Oral Implants Res, (2): p Hockers, T., et al., The combined use of bioresorbable membranes and xenografts or autografts in the treatment of bone defects around implants. A study in beagle dogs. Clin Oral Implants Res, (6): p Clementini, M., et al., Success rate of dental implants inserted in horizontal and vertical guided bone
56 regenerated areas: a systematic review. Int J Oral Maxillofac Surg, (7): p Del Fabbro, M., S.S. Wallace, and T. Testori, Long-term implant survival in the grafted maxillary sinus: a systematic review. Int J Periodontics Restorative Dent, (6): p Collins, J.R., et al., Clinical and histological evaluation of socket grafting using different types of bone substitute in adult patients. Implant Dent, (4): p Mahesh, L., et al., Socket grafting with calcium phosphosilicate alloplast putty: a histomorphometric evaluation. Compend Contin Educ Dent, (8): p. e Kotsakis, G.A., et al., A randomized, blinded, controlled clinical study of particulate anorganic bovine bone mineral and calcium phosphosilicate putty bone substitutes for socket preservation. Int J Oral Maxillofac Implants, (1): p Jambhekar, S., F. Kernen, and A.S. Bidra, Clinical and histologic outcomes of socket grafting after flapless tooth extraction: a systematic review of randomized controlled clinical trials. J Prosthet Dent, (5): p Malinin, T.I., E.M. Carpenter, and H.T. Temple, Particulate bone allograft incorporation in regeneration of osseous defects; importance of particle sizes. Open Orthop J, : p Landsberg, C.J. and N. Bichacho, A modified surgical/prosthetic approach for optimal single implant supported crown. Part I--The socket seal surgery. Pract Periodontics Aesthet Dent, (2): p. 11-7; quiz Stambaugh, R., Aesthetic ridge and extraction site augmentation for anterior implant placement without barrier membrane. Pract Periodontics Aesthet Dent, (9): p ; quiz Elian, N., et al., A simplified socket classification and repair technique. Pract Proced Aesthet Dent, (2): p ; quiz Vignoletti, F., et al., Surgical protocols for ridge preservation after tooth extraction. A systematic review. Clin Oral Implants Res, Suppl 5: p Mardas, N., et al., Does ridge preservation following tooth extraction improve implant treatment outcomes: a systematic review: Group 4: Therapeutic concepts & methods. Clin Oral Implants Res, Suppl 11: p Horvath, A., et al., Alveolar ridge preservation. A systematic review. Clin Oral Investig, (2): p Avila-Ortiz, G., et al., Effect of alveolar ridge preservation after tooth extraction: a systematic review and meta-analysis. J Dent Res, (10): p
57 73. Chen, S.T. and D. Buser, Esthetic outcomes following immediate and early implant placement in the anterior maxilla--a systematic review. Int J Oral Maxillofac Implants, Suppl: p Schropp, L., et al., Patient experience of, and satisfaction with, delayed-immediate vs. delayed singletooth implant placement. Clin Oral Implants Res, (4): p Johnson, K., A study of the dimensional changes occurring in the maxilla following tooth extraction. Aust Dent J, (4): p Chu, S.J., et al., Flapless Postextraction Socket Implant Placement, Part 2: The Effects of Bone Grafting and Provisional Restoration on Peri-implant Soft Tissue Height and Thickness- A Retrospective Study. Int J Periodontics Restorative Dent, (6): p Sarnachiaro, G.O., et al., Immediate Implant Placement into Extraction Sockets with Labial Plate Dehiscence Defects: A Clinical Case Series. Clin Implant Dent Relat Res, Covani, U., R. Cornelini, and A. Barone, Buccal bone augmentation around immediate implants with and without flap elevation: a modified approach. Int J Oral Maxillofac Implants, (5): p Keller, E.E., D.E. Tolman, and S.E. Eckert, Maxillary antral-nasal inlay autogenous bone graft reconstruction of compromised maxilla: a 12-year retrospective study. Int J Oral Maxillofac Implants, (5): p Simion, M., et al., Guided bone regeneration using resorbable and nonresorbable membranes: a comparative histologic study in humans. Int J Oral Maxillofac Implants, (6): p Gielkens, P.F., et al., Is there evidence that barrier membranes prevent bone resorption in autologous bone grafts during the healing period? A systematic review. Int J Oral Maxillofac Implants, (3): p Llambes, F., F.J. Silvestre, and R. Caffesse, Vertical guided bone regeneration with bioabsorbable barriers. J Periodontol, (10): p Hellem, S., et al., Implant treatment in combination with lateral augmentation of the alveolar process: a 3-year prospective study. Clin Implant Dent Relat Res, (4): p Simion, M., et al., Vertical ridge augmentation by expanded-polytetrafluoroethylene membrane and a combination of intraoral autogenous bone graft and deproteinized anorganic bovine bone (Bio Oss). Clin Oral Implants Res, (5): p Murphy, K.G., Postoperative healing complications associated with Gore-Tex Periodontal Material. Part II. Effect of complications on regeneration. Int J Periodontics Restorative Dent, (6): p Arbab, H., et al., Ridge Preservation Comparing a Nonresorbable PTFE Membrane to a Resorbable Collagen Membrane: A Clinical and Histologic Study in Humans. Implant Dent, (1): p
58 87. Barone, A., et al., Flap versus flapless procedure for ridge preservation in alveolar extraction sockets: a histological evaluation in a randomized clinical trial. Clin Oral Implants Res, (7): p Lekovic, V., et al., Preservation of alveolar bone in extraction sockets using bioabsorbable membranes. J Periodontol, (9): p De Rouck, T., K. Collys, and J. Cosyn, Immediate single-tooth implants in the anterior maxilla: a 1-year case cohort study on hard and soft tissue response. J Clin Periodontol, (7): p Chen, S.T., et al., Immediate implant placement postextraction without flap elevation. J Periodontol, (1): p Kan, J.Y., et al., Facial gingival tissue stability after connective tissue graft with single immediate tooth replacement in the esthetic zone: consecutive case report. J Oral Maxillofac Surg, (11 Suppl): p Botticelli, D., T. Berglundh, and J. Lindhe, Hard-tissue alterations following immediate implant placement in extraction sites. J Clin Periodontol, (10): p Covani, U., R. Cornelini, and A. Barone, Vertical crestal bone changes around implants placed into fresh extraction sockets. J Periodontol, (5): p de Sanctis, M., et al., Immediate implants at fresh extraction sockets: bone healing in four different implant systems. J Clin Periodontol, (8): p Kan, J.Y., K. Rungcharassaeng, and J. Lozada, Immediate placement and provisionalization of maxillary anterior single implants: 1-year prospective study. Int J Oral Maxillofac Implants, (1): p Kan, J.Y., et al., Periimplant tissue response following immediate provisional restoration of scalloped implants in the esthetic zone: a one-year pilot prospective multicenter study. J Prosthet Dent, (6 Suppl): p. S Evans, C.D. and S.T. Chen, Esthetic outcomes of immediate implant placements. Clin Oral Implants Res, (1): p Baggi, L., et al., The influence of implant diameter and length on stress distribution of osseointegrated implants related to crestal bone geometry: a three-dimensional finite element analysis. J Prosthet Dent, (6): p Luongo, R., et al., Hard and soft tissue responses to the platform-switching technique. Int J Periodontics Restorative Dent, (6): p Canullo, L., G. Iurlaro, and G. Iannello, Double-blind randomized controlled trial study on postextraction immediately restored implants using the switching platform concept: soft tissue response.
59 Preliminary report. Clin Oral Implants Res, (4): p Hurzeler, M., et al., Peri-implant bone level around implants with platform-switched abutments: preliminary data from a prospective study. J Oral Maxillofac Surg, (7 Suppl 1): p Lazzara, R.J. and S.S. Porter, Platform switching: a new concept in implant dentistry for controlling postrestorative crestal bone levels. Int J Periodontics Restorative Dent, (1): p Annibali, S., et al., Peri-implant marginal bone level: a systematic review and meta-analysis of studies comparing platform switching versus conventionally restored implants. J Clin Periodontol, (11): p Rodriguez-Ciurana, X., et al., The effect of interimplant distance on the height of the interimplant bone crest when using platform-switched implants. Int J Periodontics Restorative Dent, (2): p Wohrle, P.S., Single-tooth replacement in the aesthetic zone with immediate provisionalization: fourteen consecutive case reports. Pract Periodontics Aesthet Dent, (9): p ; quiz Slagter, K.W., et al., Immediate placement of dental implants in the esthetic zone: a systematic review and pooled analysis. J Periodontol, (7): p. e Block, M.S., et al., Prospective evaluation of immediate and delayed provisional single tooth restorations. J Oral Maxillofac Surg, (11 Suppl): p De Rouck, T., et al., Instant provisionalization of immediate single-tooth implants is essential to optimize esthetic treatment outcome. Clin Oral Implants Res, (6): p Gallucci, G.O., et al., Influence of immediate implant loading on peri-implant soft tissue morphology in the edentulous maxilla. Int J Oral Maxillofac Implants, (4): p Lai, H.C., et al., Evaluation of soft-tissue alteration around implant-supported single-tooth restoration in the anterior maxilla: the pink esthetic score. Clin Oral Implants Res, (6): p Favero, G., et al., Alveolar bony crest preservation at implants installed immediately after tooth extraction: an experimental study in the dog. Clin Oral Implants Res, (1): p Botticelli, D., et al., The jumping distance revisited: An experimental study in the dog. Clin Oral Implants Res, (1): p Pluemsakunthai, W., B. Le, and S. Kasugai, Effect of buccal gap distance on alveolar ridge alteration after immediate implant placement: a microcomputed tomographic and morphometric analysis in dogs. Implant Dent, (1): p Tomasi, C., et al., Bone dimensional variations at implants placed in fresh extraction sockets: a multilevel multivariate analysis. Clin Oral Implants Res, (1): p
60 115. Januario, A.L., et al., Dimension of the facial bone wall in the anterior maxilla: a cone-beam computed tomography study. Clin Oral Implants Res, (10): p Bressan, E., et al., Healing of buccal dehiscence defects at implants installed immediately into extraction sockets - an experimental study in dogs. Clin Oral Implants Res, (3): p Zitzmann, N.U., P. Scharer, and C.P. Marinello, Factors influencing the success of GBR. Smoking, timing of implant placement, implant location, bone quality and provisional restoration. J Clin Periodontol, (10): p Cosyn, J., N. Hooghe, and H. De Bruyn, A systematic review on the frequency of advanced recession following single immediate implant treatment. J Clin Periodontol, (6): p Steigmann, M. and H.L. Wang, Esthetic buccal flap for correction of buccal fenestration defects during flapless immediate implant surgery. J Periodontol, (3): p Seibert, J., & Lindhe, J., Esthetics and periodontal therapy, in Textbook of Clinical Periodontology. 1989, Munksgaard: Copenhagen, Denmark. p De Rouck, T., et al., The gingival biotype revisited: transparency of the periodontal probe through the gingival margin as a method to discriminate thin from thick gingiva. J Clin Periodontol, (5): p Hammerle, C.H., S.T. Chen, and T.G. Wilson, Jr., Consensus statements and recommended clinical procedures regarding the placement of implants in extraction sockets. Int J Oral Maxillofac Implants, Suppl: p Muller, H.P., T. Eger, and A. Schorb, Gingival dimensions after root coverage with free connective tissue grafts. J Clin Periodontol, (5): p den Hartog, L., et al., Treatment outcome of immediate, early and conventional single-tooth implants in the aesthetic zone: a systematic review to survival, bone level, soft-tissue, aesthetics and patient satisfaction. J Clin Periodontol, (12): p Carlsson, L., et al., Implant fixation improved by close fit. Cylindrical implant-bone interface studied in rabbits. Acta Orthop Scand, (3): p Caudill, R.F. and R.M. Meffert, Histologic analysis of the osseointegration of endosseous implants in simulated extraction sockets with and without e-ptfe barriers. 1. Preliminary findings. Int J Periodontics Restorative Dent, (3): p Akimoto, K., et al., Evaluation of titanium implants placed into simulated extraction sockets: a study in dogs. Int J Oral Maxillofac Implants, (3): p
61 128. Knox, R., R. Caudill, and R. Meffert, Histologic evaluation of dental endosseous implants placed in surgically created extraction defects. Int J Periodontics Restorative Dent, (5): p Tarnow, D.P., et al., Flapless postextraction socket implant placement in the esthetic zone: part 1. The effect of bone grafting and/or provisional restoration on facial-palatal ridge dimensional change-a retrospective cohort study. Int J Periodontics Restorative Dent, (3): p Le, B.T., A. Borzabadi-Farahani, and W. Pluemsakunthai, Is buccolingual angulation of maxillary anterior implants associated with the crestal labial soft tissue thickness? Int J Oral Maxillofac Surg, (7): p Grunder, U., Crestal ridge width changes when placing implants at the time of tooth extraction with and without soft tissue augmentation after a healing period of 6 months: report of 24 consecutive cases. Int J Periodontics Restorative Dent, (1): p Rungcharassaeng, K., et al., Immediate implant placement and provisionalization with and without a connective tissue graft: an analysis of facial gingival tissue thickness. Int J Periodontics Restorative Dent, (6): p Jung, R.E., et al., In vitro color changes of soft tissues caused by restorative materials. Int J Periodontics Restorative Dent, (3): p Le, B.T. and A. Borzabadi-Farahani, Labial bone thickness in area of anterior maxillary implants associated with crestal labial soft tissue thickness. Implant Dent, (5): p Belser, U.C., et al., Outcome analysis of implant restorations located in the anterior maxilla: a review of the recent literature. Int J Oral Maxillofac Implants, Suppl: p Tarnow, D., et al., Vertical distance from the crest of bone to the height of the interproximal papilla between adjacent implants. J Periodontol, (12): p Novaes, A.B., Jr., et al., The effects of interimplant distances on papilla formation and crestal resorption in implants with a morse cone connection and a platform switch: a histomorphometric study in dogs. J Periodontol, (11): p Spear, F.M., The use of implants and ovate pontics in the esthetic zone. Compend Contin Educ Dent, (2): p. 72-4, 76-80; quiz 81, Salama, M., et al., Advantages of the root submergence technique for pontic site development in esthetic implant therapy. Int J Periodontics Restorative Dent, (6): p Salama, H., et al., The interproximal height of bone: a guidepost to predictable aesthetic strategies and soft tissue contours in anterior tooth replacement. Pract Periodontics Aesthet Dent, (9): p ; quiz 1142.
62 141. Favero, G., et al., Role of teeth adjacent to implants installed immediately into extraction sockets: an experimental study in the dog. Clin Oral Implants Res, (4): p Hurzeler, M.B., et al., The socket-shield technique: a proof-of-principle report. J Clin Periodontol, (9): p Sapir, S. and J. Shapira, Decoronation for the management of an ankylosed young permanent tooth. Dent Traumatol, (1): p Cohenca, N. and A. Stabholz, Decoronation - a conservative method to treat ankylosed teeth for preservation of alveolar ridge prior to permanent prosthetic reconstruction: literature review and case presentation. Dent Traumatol, (2): p Malmgren, B., Decoronation: how, why, and when? J Calif Dent Assoc, (11): p Filippi, A., Y. Pohl, and T. von Arx, Decoronation of an ankylosed tooth for preservation of alveolar bone prior to implant placement. Dent Traumatol, (2): p Davarpanah, M. and S. Szmukler-Moncler, Unconventional implant treatment: I. Implant placement in contact with ankylosed root fragments. A series of five case reports. Clin Oral Implants Res, (8): p Baumer, D., et al., The socket-shield technique: first histological, clinical, and volumetrical observations after separation of the buccal tooth segment - a pilot study. Clin Implant Dent Relat Res, (1): p Kan, J.Y. and K. Rungcharassaeng, Proximal socket shield for interimplant papilla preservation in the esthetic zone. Int J Periodontics Restorative Dent, (1): p. e Block, M.S., Placement of implants into fresh molar sites: results of 35 cases. J Oral Maxillofac Surg, (1): p Siciliano, V.I., et al., Soft tissues healing at immediate transmucosal implants placed into molar extraction sites with buccal self-contained dehiscences. A 12-month controlled clinical trial. Clin Oral Implants Res, (5): p Fugazzotto, P.A., Implant placement at the time of maxillary molar extraction: treatment protocols and report of results. J Periodontol, (2): p Fugazzotto, P.A., Implant placement at the time of mandibular molar extraction: description of technique and preliminary results of 341 cases. J Periodontol, (4): p Cafiero, C., et al., Immediate transmucosal implant placement in molar extraction sites: a 12-month prospective multicenter cohort study. Clin Oral Implants Res, (5): p
63 155. Artzi, Z., A. Parson, and C.E. Nemcovsky, Wide-diameter implant placement and internal sinus membrane elevation in the immediate postextraction phase: clinical and radiographic observations in 12 consecutive molar sites. Int J Oral Maxillofac Implants, (2): p Wagenberg, B. and S.J. Froum, A retrospective study of 1925 consecutively placed immediate implants from 1988 to Int J Oral Maxillofac Implants, (1): p Prosper, L., et al., Five-year follow-up of wide-diameter implants placed in fresh molar extraction sockets in the mandible: immediate versus delayed loading. Int J Oral Maxillofac Implants, (3): p Ketabi, M., D. Deporter, and E.G. Atenafu, A Systematic Review of Outcomes Following Immediate Molar Implant Placement Based on Recently Published Studies. Clin Implant Dent Relat Res, Urban, T., L. Kostopoulos, and A. Wenzel, Immediate implant placement in molar regions: risk factors for early failure. Clin Oral Implants Res, (2): p Urban, T., L. Kostopoulos, and A. Wenzel, Immediate implant placement in molar regions: a 12-month prospective, randomized follow-up study. Clin Oral Implants Res, (12): p Hayacibara, R.M., et al., The success rate of immediate implant placement of mandibular molars: a clinical and radiographic retrospective evaluation between 2 and 8 years. Clin Oral Implants Res, (7): p Vandeweghe, S., et al., Surgical protocol and short-term clinical outcome of immediate placement in molar extraction sockets using a wide body implant. J Oral Maxillofac Res, (3): p. e Atieh, M.A., et al., Immediate placement or immediate restoration/loading of single implants for molar tooth replacement: a systematic review and meta-analysis. Int J Oral Maxillofac Implants, (2): p Cornelini, R., et al., Immediate restoration of single-tooth implants in mandibular molar sites: a 12- month preliminary report. Int J Oral Maxillofac Implants, (6): p Crespi, R., et al., Immediate occlusal loading of implants placed in fresh sockets after tooth extraction. Int J Oral Maxillofac Implants, (6): p Schincaglia, G.P., et al., Replacement of mandibular molars with single-unit restorations supported by wide-body implants: immediate versus delayed loading. A randomized controlled study. Int J Oral Maxillofac Implants, (3): p Shin, S.W., S.R. Bryant, and G.A. Zarb, A retrospective study on the treatment outcome of wide-bodied implants. Int J Prosthodont, (1): p Hamouda, N.I., et al., Immediate implant placement into fresh extraction socket in the mandibular
64 molar sites: a preliminary study of a modified insertion technique. Clin Implant Dent Relat Res, Suppl 1: p. e Matsuda, H., Borzabadi-Farahani, A., Le, B.T., Three-dimensional alveolar bone anatomy of the maxillary first molars: A cone beam computed tomography study. Implant Dent, In Press Calin, C., A. Petre, and S. Drafta, Osteotome-mediated sinus floor elevation: a systematic review and meta-analysis. Int J Oral Maxillofac Implants, (3): p Boyne, P.J. and R.A. James, Grafting of the maxillary sinus floor with autogenous marrow and bone. J Oral Surg, (8): p Peleg, M., et al., Sinus floor augmentation with simultaneous implant placement in the severely atrophic maxilla. J Periodontol, (12): p Chrcanovic, B.R., M.D. Martins, and A. Wennerberg, Immediate placement of implants into infected sites: a systematic review. Clin Implant Dent Relat Res, Suppl 1: p. e1-e Waasdorp, J.A., C.I. Evian, and M. Mandracchia, Immediate placement of implants into infected sites: a systematic review of the literature. J Periodontol, (6): p Figure Legends Figure 1A-D For socket defects with an intact labial plate and normal crest level, small-particle cancellous allograft can be placed without a barrier membrane. Figure 2A-N Teeth with labial wall defects require socket augmentation using guided tissue regeneration with an open flap to overcorrect the alveolar ridge to achieve ideal contours Figure 3A-B Open Book Flap Design. The open book flap design should be utilized for large defects to improve visualizationand access to the graft site. Figure 4 Labial Gingival Recession. Labial gingival recession 1 year after implant placement. Figure 5A-J Immediate implant placement with immediate provisionalization. Figure 6A-I Single-stage Implant Placement with Simultaneous Bone Grafting. Open book flap design with esthetic contour graft and non-submerged closure around healing abutment. Figure 7A-B Gingival Biotype. Most patients will fall into two categories: slender teeth with thin gingiva and scalloped periodontium or square teeth with thick gingiva and blunted periodontium. Figure 8 Peri-implant Marginal Gap (Jumping gap). Figure 9 Effect of Buccal Gap Distance on Alveolar Ridge Alteration After Immediate Implant Placement.
65 The 3 mm is the optimal gap distance among the groups examined, which drastically influences the healing of bone and soft tissue surrounding the implants. Figure 10A-B Implants placed too deep in an apicocoronal position or too labial often result is an unnaturally long restoration. Figure 11 The Relationship Between Crestal Labial Soft Tissue Thickness and Implant Bucco-lingual Angulation. Figure 12A-H Staged Approach for Extraction and Implant Restoration of Teeth #8 and #9. A, B, Before extraction. C-E, Extraction of the left central incisor with immediate implant placement and provisional restoration. F, Four months later, extraction of the right central incisor was performed with immediate implant placement and provisional restoration. G, H, Final restoration at three years follow-up with x-rays showing preserved gingival architecture. Figure 13 Socket Shield Technique. Table 1. Labial Soft Tissue Thickness and Labial Bone Thickness. Linear correlation between labial crestal soft tissue thickness and underlying bone thickness.

66 Figure 14 Risk Assessment of Critical Factors Affecting Immediate Implant Success. Fig 15 A-K Extraction Management of a Tooth with Labial Wall Defect and Loss of Labial Attached Tissue using the Open Book Flap A-B Failing right maxillary lateral incisor with labial tissue loss C-D Open Book Flap incision design E- F Mineralized cancellous allograft placement with overcorrection and collagen membrane coverage G Soft tissue closure; note slight exposure of membrane left to heal by secondary intention H-I Healing at 4 months post-operative with flapless implant placement J-K Final restoration at 3 years with corresponding radiograph
Masking Buccal Plate Remodeling in the Esthetic Zone with Connective Tissue Grafts: Concepts and Techniques with Immediate Implants
 Peer-Reviewed and Indexed Annual Implant Issue Masking Buccal Plate Remodeling in the Esthetic Zone with Connective Tissue Grafts: Concepts and Techniques with Immediate Implants of Continuing Education
Peer-Reviewed and Indexed Annual Implant Issue Masking Buccal Plate Remodeling in the Esthetic Zone with Connective Tissue Grafts: Concepts and Techniques with Immediate Implants of Continuing Education
Socket preservation in the daily practice: A clinical case report
 Clinical Socket preservation in the daily practice: A clinical case report Rabih Abi Nader 1 and Carine Tabarani 2 Abstract Soft tissue contour depends on the underlying bone anatomy. Following tooth extraction,
Clinical Socket preservation in the daily practice: A clinical case report Rabih Abi Nader 1 and Carine Tabarani 2 Abstract Soft tissue contour depends on the underlying bone anatomy. Following tooth extraction,
Case Study. Case # 1 Author: Dr. Suheil Boutros (USA) 2013 Zimmer Dental, Inc. All rights reserved. 6557, Rev. 03/13.
 2013 Zimmer Dental, Inc. All rights reserved. 6557, Rev. 03/13.") Placement of a Zimmer Trabecular Metal Dental Implant with Simultaneous Ridge Augmentation and Immediate Non-Functional Loading Following Tooth Extraction and Orthodontic Treatment for Implant Site Development
Placement of a Zimmer Trabecular Metal Dental Implant with Simultaneous Ridge Augmentation and Immediate Non-Functional Loading Following Tooth Extraction and Orthodontic Treatment for Implant Site Development
BONE AUGMENTATION AND GRAFTING
 1 A Computer-Guided Bone Block Harvesting Procedure: A Proof-of-Principle Case Report and Technical Notes Effectiveness of Lateral Bone Augmentation on the Alveolar Crest Dimension: A Systematic Review
1 A Computer-Guided Bone Block Harvesting Procedure: A Proof-of-Principle Case Report and Technical Notes Effectiveness of Lateral Bone Augmentation on the Alveolar Crest Dimension: A Systematic Review
REGENERATIONTIME. A Case Report by. Ridge Augmentation and Delayed Implant Placement on an Upper Lateral Incisor
 A Case Report by Dr. Daniele Cardaropoli Ridge Augmentation and Delayed Implant Placement on an Upper Lateral Incisor The Situation An adult female patient presented with an endodontic/prosthetic failure
A Case Report by Dr. Daniele Cardaropoli Ridge Augmentation and Delayed Implant Placement on an Upper Lateral Incisor The Situation An adult female patient presented with an endodontic/prosthetic failure
Rehabilitating a Compromised Site for Restoring Form, Function and Esthetics- A Case Report
 Research & Reviews: Journal of Dental Sciences Rehabilitating a Compromised Site for Restoring Form, Function and Esthetics- A Case Report Priyanka Prakash* Division of Periodontology, Department of Dental
Research & Reviews: Journal of Dental Sciences Rehabilitating a Compromised Site for Restoring Form, Function and Esthetics- A Case Report Priyanka Prakash* Division of Periodontology, Department of Dental
Clinical Case Reports using Cytoplast GTR Barrier Membranes
 Clinical Case Reports using Cytoplast GTR Barrier Membranes Barry K. Bartee, DDS, MD The Cytoplast Technique: Extraction Site Grafting Without Primary Closure 1. 1. Preoperative view. To maximize the result
Clinical Case Reports using Cytoplast GTR Barrier Membranes Barry K. Bartee, DDS, MD The Cytoplast Technique: Extraction Site Grafting Without Primary Closure 1. 1. Preoperative view. To maximize the result
Evaluation of a Combination Allograft Material Compared to DFDBA in Alveolar Ridge Preservation. Sanju P. Jose
 Evaluation of a Combination Allograft Material Compared to DFDBA in Alveolar Ridge Preservation by Sanju P. Jose B.S., University of Maryland Baltimore County, 2008 D.D.S., University of Maryland School
Evaluation of a Combination Allograft Material Compared to DFDBA in Alveolar Ridge Preservation by Sanju P. Jose B.S., University of Maryland Baltimore County, 2008 D.D.S., University of Maryland School
Alveolar ridge preservation techniques
 Alveolar ridge preservation techniques Semmelweis University, Department of Periodontology, Budapest Dr. Windisch Péter Head of Department of Periodontology Changes of the alveolar ridge dimensions after
Alveolar ridge preservation techniques Semmelweis University, Department of Periodontology, Budapest Dr. Windisch Péter Head of Department of Periodontology Changes of the alveolar ridge dimensions after
Management of a complex case
 2 Soft- and hard-tissue reconstruction of a severely deficient site prior to implant placement: a case report Management of a complex case Younes Khosroshahy, DDS, MFDS RCS (Eng), Dip Imp Dent RCSEd, Blue
2 Soft- and hard-tissue reconstruction of a severely deficient site prior to implant placement: a case report Management of a complex case Younes Khosroshahy, DDS, MFDS RCS (Eng), Dip Imp Dent RCSEd, Blue
MANAGEMENT OF ATROPHIC ANTERIOR MAXILLA USING RIDGE SPLIT TECHNIQUE, IMMEDIATE IMPLANTATION AND TEMPORIZATION
 Case Report International Journal of Dental and Health Sciences Volume 02, Issue 06 MANAGEMENT OF ATROPHIC ANTERIOR MAXILLA USING RIDGE SPLIT TECHNIQUE, IMMEDIATE IMPLANTATION AND TEMPORIZATION Rakshith
Case Report International Journal of Dental and Health Sciences Volume 02, Issue 06 MANAGEMENT OF ATROPHIC ANTERIOR MAXILLA USING RIDGE SPLIT TECHNIQUE, IMMEDIATE IMPLANTATION AND TEMPORIZATION Rakshith
Dental Implants: A Predictable Solution for Tooth Loss. Reena Talwar, DDS PhD FRCD(C) Oral & Maxillofacial Surgeon Associate Clinical Professor
 Oral & Maxillofacial Surgeon Associate Clinical Professor") Dental Implants: A Predictable Solution for Tooth Loss Reena Talwar, DDS PhD FRCD(C) Oral & Maxillofacial Surgeon Associate Clinical Professor What are Dental Implants? Titanium posts used to replace missing
Dental Implants: A Predictable Solution for Tooth Loss Reena Talwar, DDS PhD FRCD(C) Oral & Maxillofacial Surgeon Associate Clinical Professor What are Dental Implants? Titanium posts used to replace missing
Pre op Failed endodontic treatment with sinus involvement.
 Case #1 of 10 consecutive extraction sockets grafted with Socket Graft Putty, covered with Socket Seal and sealed with Periacryl. I D # HEU This patient is a 66 year old female. Pre op Failed endodontic
Case #1 of 10 consecutive extraction sockets grafted with Socket Graft Putty, covered with Socket Seal and sealed with Periacryl. I D # HEU This patient is a 66 year old female. Pre op Failed endodontic
More than bone regeneration. A total solution.
 More than bone regeneration. A total solution. More than a dental implant company. A total solution. When it comes to treatment options, your patients want positive results both functionally and esthetically.
More than bone regeneration. A total solution. More than a dental implant company. A total solution. When it comes to treatment options, your patients want positive results both functionally and esthetically.
Contemporary Implant Dentistry
 Contemporary Implant Dentistry C H A P T ER 1 4 O F C O N T E M P OR A R Y O R A L A N D M A X I L L OFA C IA L S U R G E RY B Y : D R A R A S H K H O J A S T EH Dental implant is suitable for: completely
Contemporary Implant Dentistry C H A P T ER 1 4 O F C O N T E M P OR A R Y O R A L A N D M A X I L L OFA C IA L S U R G E RY B Y : D R A R A S H K H O J A S T EH Dental implant is suitable for: completely
CASE REPORT. CBCT-Assisted Treatment of the Failing Long Span Bridge with Staged and Immediate Load Implant Restoration
 Computer Aided Implantology Academy Newsletter - Newsletter 20 - July 2009 CASE REPORT CBCT-Assisted Treatment of the Failing Long Span Bridge with Staged and Immediate Load Implant Restoration Case Report
Computer Aided Implantology Academy Newsletter - Newsletter 20 - July 2009 CASE REPORT CBCT-Assisted Treatment of the Failing Long Span Bridge with Staged and Immediate Load Implant Restoration Case Report
Extraction with Immediate Implant Placement and Ridge Preservation in the Posterior
 Extraction with Immediate Implant Placement and Ridge Preservation in the Posterior by Timothy F. Kosinski, DDS, MAGD The following case presentation illustrates the diagnosis, planning and treatment for
Extraction with Immediate Implant Placement and Ridge Preservation in the Posterior by Timothy F. Kosinski, DDS, MAGD The following case presentation illustrates the diagnosis, planning and treatment for
Horizontal bone augmentation by means of guided bone regeneration
 Periodontology 2000, Vol. 66, 2014, 13 40 2014 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd Printed in Singapore. All rights reserved PERIODONTOLOGY 2000 Horizontal bone augmentation by means
Periodontology 2000, Vol. 66, 2014, 13 40 2014 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd Printed in Singapore. All rights reserved PERIODONTOLOGY 2000 Horizontal bone augmentation by means
Consensus Report Tissue augmentation and esthetics (Working Group 3)
") B. Klinge Thomas F. Flemmig Consensus Report Tissue augmentation and esthetics (Working Group 3) Members of working group: Matteo Chiapasco Jan-Eirik Ellingsen Ronald Jung Friedrich Neukam Isabella Rocchietta
B. Klinge Thomas F. Flemmig Consensus Report Tissue augmentation and esthetics (Working Group 3) Members of working group: Matteo Chiapasco Jan-Eirik Ellingsen Ronald Jung Friedrich Neukam Isabella Rocchietta
The Original remains unique.
 The Original remains unique. Geistlich leading regeneration 2A, 2B Geistlich is the world leader in regenerative dentistry. We transform natural biomaterials into safe and reliable treatment methods that
The Original remains unique. Geistlich leading regeneration 2A, 2B Geistlich is the world leader in regenerative dentistry. We transform natural biomaterials into safe and reliable treatment methods that
Working together as a team, the periodontist
 The Team Approach to Esthetic Immediate Implant Placement Bobby L. Butler, DDS; and Greggory Kinzer, DDS Working together as a team, the periodontist and restorative dentist can provide an increased level
The Team Approach to Esthetic Immediate Implant Placement Bobby L. Butler, DDS; and Greggory Kinzer, DDS Working together as a team, the periodontist and restorative dentist can provide an increased level
Puros Cancellous Particulate Allograft & Puros Block Allograft
 Puros Cancellous Particulate Allograft & Puros Block Allograft Puros Cancellous Particulate Allograft The Natural Choice For Healthy 1 Bone Growth. 1. Proven, Predictable Regeneration Acts as an osteoconductive
Puros Cancellous Particulate Allograft & Puros Block Allograft Puros Cancellous Particulate Allograft The Natural Choice For Healthy 1 Bone Growth. 1. Proven, Predictable Regeneration Acts as an osteoconductive
Bringing you Geistlich biocompatibility with improved application and handling benefits. Your combination for success
 Bringing you Geistlich biocompatibility with improved application and handling benefits Your combination for success Geistlich Combi-Kit Collagen: Combining ease and predictablility Geistlich Combi-Kit
Bringing you Geistlich biocompatibility with improved application and handling benefits Your combination for success Geistlich Combi-Kit Collagen: Combining ease and predictablility Geistlich Combi-Kit
MODIFIED SINGLE ROLL FLAP APPROACH FOR SIMULTANEOUS IMPLANT PLACEMENT AND GINGIVAL AUGMENTATION
 Journal of IMAB ISSN: 1312-773X https://www.journal-imab-bg.org https://doi.org/10.5272/jimab.2017233.1667 Journal of IMAB - Annual Proceeding (Scientific Papers). 2017 Jul-Sep;23(3): Case report MODIFIED
Journal of IMAB ISSN: 1312-773X https://www.journal-imab-bg.org https://doi.org/10.5272/jimab.2017233.1667 Journal of IMAB - Annual Proceeding (Scientific Papers). 2017 Jul-Sep;23(3): Case report MODIFIED
Hyun-Jae Cho, Kun-Soo Jang, Ki-Hyun Jeong, Jae-Yun Jeon, Kyung-Gyun Hwang, Chang-Joo Park
 Vol. 33 No. 1, March 2014 Peri-implant gingival tissue changes following immediate placement of maxillary anterior single implant with a collagen-coated xenograft: A 1-year follow-up result Hyun-Jae Cho,
Vol. 33 No. 1, March 2014 Peri-implant gingival tissue changes following immediate placement of maxillary anterior single implant with a collagen-coated xenograft: A 1-year follow-up result Hyun-Jae Cho,
The International Journal of Periodontics & Restorative Dentistry
 The International Journal of Periodontics & Restorative Dentistry 3 Influence of the 3-D Bone-to-Implant Relationship on Esthetics Ueli Grunder, DMD* Stefano Gracis, DMD** Matteo Capelli, DMD** There are
The International Journal of Periodontics & Restorative Dentistry 3 Influence of the 3-D Bone-to-Implant Relationship on Esthetics Ueli Grunder, DMD* Stefano Gracis, DMD** Matteo Capelli, DMD** There are
Bone Grafting for Socket Preservation
 Bone Grafting for Socket Preservation Dr. Karl R. Koerner Normal extraction facial bone loss. Excessive force. Commonly the thickness of facial bone. Hussain, A. et al. Ridge preservation comparing a nonresorbable
Bone Grafting for Socket Preservation Dr. Karl R. Koerner Normal extraction facial bone loss. Excessive force. Commonly the thickness of facial bone. Hussain, A. et al. Ridge preservation comparing a nonresorbable
Purpose: To assess the long term survival of sites treated by GTR.
 Cortellini P, Tonetti M. Long-term tooth survival following regenerative treatment of intrabony defects. J Periodontol 2004; 75:672-8. (28 Refs) Purpose: To assess the long term survival of sites treated
Cortellini P, Tonetti M. Long-term tooth survival following regenerative treatment of intrabony defects. J Periodontol 2004; 75:672-8. (28 Refs) Purpose: To assess the long term survival of sites treated
RELIABLE WHEN IT COUNTS. The unique collagenase-resistant membrane protects bone graft and supports treatment success even when exposed 4
 RELIABLE WHEN IT COUNTS 1 RELIABLE WHEN IT COUNTS RESISTANT TO EXPOSURE The unique collagenase-resistant membrane protects bone graft and supports treatment success even when exposed 4 RELIABLE BARRIER
RELIABLE WHEN IT COUNTS 1 RELIABLE WHEN IT COUNTS RESISTANT TO EXPOSURE The unique collagenase-resistant membrane protects bone graft and supports treatment success even when exposed 4 RELIABLE BARRIER
Thick vs. Thin Gingival Biotypes: A Key Determinant in Treatment Planning for Dental Implants
 r s Thick vs. Thin Gingival Biotypes: A Key Determinant in Treatment Planning for Dental Implants richard t. kao, dds, phd; mark c. fagan, ms, dds; and gregory j. conte, ms, dmd abstract During the treatment
r s Thick vs. Thin Gingival Biotypes: A Key Determinant in Treatment Planning for Dental Implants richard t. kao, dds, phd; mark c. fagan, ms, dds; and gregory j. conte, ms, dmd abstract During the treatment
Prosthetic Options in Implant Dentistry. Hakimeh Siadat, DDS, MSc Associate Professor
 Prosthetic Options in Dentistry Hakimeh Siadat, DDS, MSc Associate Professor Dental Research Center, Department of Prosthodontics & Dental s Faculty of Dentistry, Tehran University of Medical Sciences
Prosthetic Options in Dentistry Hakimeh Siadat, DDS, MSc Associate Professor Dental Research Center, Department of Prosthodontics & Dental s Faculty of Dentistry, Tehran University of Medical Sciences
Limited bone availability makes implant placement challenging
 Bone Grafting: Essential Indications and Techniques in Implant Dentistry Limited bone availability makes implant placement challenging and sometimes unpredictable. Candidates for implant therapy must have
Bone Grafting: Essential Indications and Techniques in Implant Dentistry Limited bone availability makes implant placement challenging and sometimes unpredictable. Candidates for implant therapy must have
Controlling Tissue Contours with a Prosthetically Driven Approach to Implant Dentistry
 Controlling Tissue Contours with a Prosthetically Driven Approach to Implant Dentistry Go online for in-depth content by Timothy F. Kosinski, DDS, MAGD With continual improvements in the design and production
Controlling Tissue Contours with a Prosthetically Driven Approach to Implant Dentistry Go online for in-depth content by Timothy F. Kosinski, DDS, MAGD With continual improvements in the design and production
Case Report. RapidSorb Rapid Resorbable Fixation System. Ridge augmentation in a one-step surgical protocol.
 Case Report RapidSorb Rapid Resorbable Fixation System. Ridge augmentation in a one-step surgical protocol. RapidSorb Rapid Resorbable Fixation System. Ridge augmentation in a one-step surgical protocol.
Case Report RapidSorb Rapid Resorbable Fixation System. Ridge augmentation in a one-step surgical protocol. RapidSorb Rapid Resorbable Fixation System. Ridge augmentation in a one-step surgical protocol.
The International Journal of Periodontics & Restorative Dentistry
 The International Journal of Periodontics & Restorative Dentistry 67 Efficacy Evaluation of a New Buccal Bone Plate Preservation Technique: A Pilot Study Federico Brugnami, DDS* Alfonso Caiazzo, DDS**
The International Journal of Periodontics & Restorative Dentistry 67 Efficacy Evaluation of a New Buccal Bone Plate Preservation Technique: A Pilot Study Federico Brugnami, DDS* Alfonso Caiazzo, DDS**
Immediate Implant Placement:
 Immediate Implant Placement: Parameters Influencing Tissue Remodeling Bernard Touati, DDS and Mario Groisman, DDS In esthetic implant therapy, the patient s objective is to obtain an imperceptible, natural-looking
Immediate Implant Placement: Parameters Influencing Tissue Remodeling Bernard Touati, DDS and Mario Groisman, DDS In esthetic implant therapy, the patient s objective is to obtain an imperceptible, natural-looking
Periimplant Regeneration Fenestration
 Indication Sheet PIR Periimplant Regeneration Fenestration Treatment concept of Dr. Jean-Pierre Gardella (surgeon) and Dr. Christian Richelme (prosthodontist), Marseille, France > Filling of a peri-implant
Indication Sheet PIR Periimplant Regeneration Fenestration Treatment concept of Dr. Jean-Pierre Gardella (surgeon) and Dr. Christian Richelme (prosthodontist), Marseille, France > Filling of a peri-implant
ANATOMY OF THE PERIODONTIUM. Dr. Fatin Awartani
 ANATOMY OF THE PERIODONTIUM Part II Cementum and Alveolar bone Associate Professor Periodontal division King Saud university Cementum Calcified mesenchymal tissue that forms the outer covering of the anatomic
ANATOMY OF THE PERIODONTIUM Part II Cementum and Alveolar bone Associate Professor Periodontal division King Saud university Cementum Calcified mesenchymal tissue that forms the outer covering of the anatomic
( ) 2009;28(2):89-94
 2009;28(2):89-94") ( ) 2009;28(2):89-94 Osseointegration is important in the functional aspect, however, esthetics is also important, especially in the maxillary anterior region. An adequate surgical technique is necessary
( ) 2009;28(2):89-94 Osseointegration is important in the functional aspect, however, esthetics is also important, especially in the maxillary anterior region. An adequate surgical technique is necessary
Surgical reconstruction of lost papilla around implant with a modified technique: A case report
 Journal of Periodontology & Implant Dentistry Case Report Surgical reconstruction of lost papilla around implant with a modified technique: A case report Mahdi Faraji* Andre Van Zyl University of Pretoria,
Journal of Periodontology & Implant Dentistry Case Report Surgical reconstruction of lost papilla around implant with a modified technique: A case report Mahdi Faraji* Andre Van Zyl University of Pretoria,
Periimplant Regeneration Fenestration
 Indication Sheet PIR-1 Periimplant Regeneration Fenestration Treatment concept of Dr. Jean-Pierre Gardella (surgeon) and Dr. Christian Richelme (prosthodontist), Marseille, France > Filling of a peri-implant
Indication Sheet PIR-1 Periimplant Regeneration Fenestration Treatment concept of Dr. Jean-Pierre Gardella (surgeon) and Dr. Christian Richelme (prosthodontist), Marseille, France > Filling of a peri-implant
Patient s Presenting Complaint V.C. presented with discomfort and mobility from the crowned maxillary left central incisor tooth. Fig 1.
 Patient s Presenting Complaint V.C. presented with discomfort and mobility from the crowned maxillary left central incisor tooth. Fig 1. A longitudinal root fracture was suspected and confirmed when the
Patient s Presenting Complaint V.C. presented with discomfort and mobility from the crowned maxillary left central incisor tooth. Fig 1. A longitudinal root fracture was suspected and confirmed when the
Immediate implant placement in the Title central incisor region: a case repo. Journal Journal of prosthodontic research,
 Immediate implant placement in the Title central incisor region: a case repo Author(s) Sekine, H; Taguchi, T; Yamagami, M; Alternative Takanashi, T; Furuya, K Journal Journal of prosthodontic research,
Immediate implant placement in the Title central incisor region: a case repo Author(s) Sekine, H; Taguchi, T; Yamagami, M; Alternative Takanashi, T; Furuya, K Journal Journal of prosthodontic research,
Labial and lingual/palatal bone thickness of maxillary and mandibular anteriors in human cadavers in Koreans
 Research Article J Periodontal Implant Sci 2011;41:60-66 doi: 10.5051/jpis.2011.41.2.60 Labial and lingual/palatal bone thickness of maxillary and mandibular anteriors in human cadavers in Koreans Ji Young
Research Article J Periodontal Implant Sci 2011;41:60-66 doi: 10.5051/jpis.2011.41.2.60 Labial and lingual/palatal bone thickness of maxillary and mandibular anteriors in human cadavers in Koreans Ji Young
Peri-implant Augmentation
 Indication Sheet PIR3 Peri-implant Augmentation Early implantation with simultaneous GBR for contour augmentation using the technique by Prof. Daniel Buser and Prof. Urs Belser, University of Berne, Switzerland
Indication Sheet PIR3 Peri-implant Augmentation Early implantation with simultaneous GBR for contour augmentation using the technique by Prof. Daniel Buser and Prof. Urs Belser, University of Berne, Switzerland
Socket Treatment. Procedure Guide
 Socket Treatment Procedure Guide www.implantdirect.com 888.649.6425 Extraction Healing and Ridge Resorption The Why Working with patients to educate them on the benefits of bone maintenance post extraction
Socket Treatment Procedure Guide www.implantdirect.com 888.649.6425 Extraction Healing and Ridge Resorption The Why Working with patients to educate them on the benefits of bone maintenance post extraction
SOCKET PRESERVATION AND TECHNIQUES AN EVALUATION OF THE LITERATURE
 SOCKET PRESERVATION AND TECHNIQUES AN EVALUATION OF THE LITERATURE Raghav Khandelwal, DMD Highland General Hospital Assistant Program Director: Ben Shimel, DDS Program Director/Chair: Chan Park, DDS,MD
SOCKET PRESERVATION AND TECHNIQUES AN EVALUATION OF THE LITERATURE Raghav Khandelwal, DMD Highland General Hospital Assistant Program Director: Ben Shimel, DDS Program Director/Chair: Chan Park, DDS,MD
SOCKET WHETHER TO PRESERVE IT NOW OR TO CREATE LATER? - A CASE REPORT
 MAVEN CASE REPORT SOCKET WHETHER TO PRESERVE IT NOW OR TO CREATE LATER? - A CASE REPORT Dr. Parthasarathi Biswas 1, Dr. Debajyoti Mondal 1, Dr. B Praveena Devi 1, Dr. Indrasri Das 2, Dr. Somen Bagchi 3,
MAVEN CASE REPORT SOCKET WHETHER TO PRESERVE IT NOW OR TO CREATE LATER? - A CASE REPORT Dr. Parthasarathi Biswas 1, Dr. Debajyoti Mondal 1, Dr. B Praveena Devi 1, Dr. Indrasri Das 2, Dr. Somen Bagchi 3,
Flapless, Immediate Implantation & Immediate Loading with Socket Preservation in the Esthetic Area Using the Alpha-Bio Tec's NeO Implants
 Flapless Surgery Case Study 48 Flapless, Immediate Implantation & Immediate Loading with Socket Preservation in the Esthetic Area Using the Alpha-Bio Tec's NeO Implants Dr. Gadi Schneider DMD, Specialist
Flapless Surgery Case Study 48 Flapless, Immediate Implantation & Immediate Loading with Socket Preservation in the Esthetic Area Using the Alpha-Bio Tec's NeO Implants Dr. Gadi Schneider DMD, Specialist
A new approach with an in-situ self-hardening grafting material
 74 Bone grafting with simultaneous early implant placement A new approach with an in-situ self-hardening grafting material MINAS LEVENTIS 1,2, PHD; PETER FAIRBAIRN 1,3, BDS; ORESTIS VASILIADIS 2,4, DDS
74 Bone grafting with simultaneous early implant placement A new approach with an in-situ self-hardening grafting material MINAS LEVENTIS 1,2, PHD; PETER FAIRBAIRN 1,3, BDS; ORESTIS VASILIADIS 2,4, DDS
Vertical and Horizontal Augmentation Using Guided Bone Regeneration. Ph.D. Thesis. Dr. med. dent. et univ. Istvan Urban
 Vertical and Horizontal Augmentation Using Guided Bone Regeneration Ph.D. Thesis Dr. med. dent. et univ. Istvan Urban Supervisor: Prof. Dr. Katalin Nagy, DDS, PhD Faculty of Dentistry, University of Szeged
Vertical and Horizontal Augmentation Using Guided Bone Regeneration Ph.D. Thesis Dr. med. dent. et univ. Istvan Urban Supervisor: Prof. Dr. Katalin Nagy, DDS, PhD Faculty of Dentistry, University of Szeged
Evaluation of different grafting materials in three-wall intra-bony defects around dental implants in beagle dogs
 Current Applied Physics 5 (2005) 507 511 www.elsevier.com/locate/cap Evaluation of different grafting materials in three-wall intra-bony defects around dental implants in beagle dogs Ui-Won Jung a, Hee-Il
Current Applied Physics 5 (2005) 507 511 www.elsevier.com/locate/cap Evaluation of different grafting materials in three-wall intra-bony defects around dental implants in beagle dogs Ui-Won Jung a, Hee-Il
Utilizing Digital Treatment Planning and Guided Surgery in Conjunction with Narrow Body Implants. by Timothy F. Kosinski, DDS, MAGD
 Utilizing Digital Treatment Planning and Guided Surgery in Conjunction with Narrow Body Implants by Timothy F. Kosinski, DDS, MAGD Implant dentistry is undergoing some amazing transformations. With the
Utilizing Digital Treatment Planning and Guided Surgery in Conjunction with Narrow Body Implants by Timothy F. Kosinski, DDS, MAGD Implant dentistry is undergoing some amazing transformations. With the
Replacement of a congenitally missing lateral incisor in the maxillary anterior aesthetic zone using a narrow diameter implant: A case report
 C A S E R E P O R T Replacement of a congenitally missing lateral incisor in the maxillary anterior aesthetic zone using a narrow diameter implant: A case report Rhoodie Garrana 1 and Govindrau Mohangi
C A S E R E P O R T Replacement of a congenitally missing lateral incisor in the maxillary anterior aesthetic zone using a narrow diameter implant: A case report Rhoodie Garrana 1 and Govindrau Mohangi
Ridge Split Procedure
 Ridge Split Procedure in the Atrophic Maxilla Udatta Kher B.D.S., M.D.S. Loss of teeth causes extensive resorption of the alveolar ridge. In the maxilla the resorption pattern occurs towards the midline,
Ridge Split Procedure in the Atrophic Maxilla Udatta Kher B.D.S., M.D.S. Loss of teeth causes extensive resorption of the alveolar ridge. In the maxilla the resorption pattern occurs towards the midline,
Puros Cancellous Particulate Allograft & Puros Block Allograft
 Puros Cancellous Particulate Allograft & Puros Block Allograft Puros Cancellous Particulate Allograft The Natural Choice For Healthy 1 Bone Growth. 1. Proven, Predictable Regeneration Acts as an osteoconductive
Puros Cancellous Particulate Allograft & Puros Block Allograft Puros Cancellous Particulate Allograft The Natural Choice For Healthy 1 Bone Growth. 1. Proven, Predictable Regeneration Acts as an osteoconductive
The Use of Alpha-Bio Tec's Narrow NeO Implants with Cone Connection for Restoration of Limited Width Ridges
 Case Study 48 The Use of Alpha-Bio Tec's Narrow NeO Implants with Cone Connection for Restoration of Limited Width Ridges Dr. Amir Gazmawe DMD, Specialist in Prosthodontics, Israel Dr. Amir Gazmawe graduated
Case Study 48 The Use of Alpha-Bio Tec's Narrow NeO Implants with Cone Connection for Restoration of Limited Width Ridges Dr. Amir Gazmawe DMD, Specialist in Prosthodontics, Israel Dr. Amir Gazmawe graduated
Extraction Defect: Assessment, Classification and Management
 International Extraction Journal Defect: of Clinical Assessment, Implant Dentistry, Classification January-April and Management 2009;1(1):1-11 Extraction Defect: Assessment, Classification and Management
International Extraction Journal Defect: of Clinical Assessment, Implant Dentistry, Classification January-April and Management 2009;1(1):1-11 Extraction Defect: Assessment, Classification and Management
The Essential Choice. With the Benefits of Biologic Predictability
 The Essential Choice With the Benefits of Biologic Predictability Documented, Reliable, Experienced is the essential choice for your daily regenerative needs. Throughout our long history and dedication
The Essential Choice With the Benefits of Biologic Predictability Documented, Reliable, Experienced is the essential choice for your daily regenerative needs. Throughout our long history and dedication
Dental Implant Treatment Planning and Restorative Considerations
 Dental Implant Treatment Planning and Restorative Considerations Aldo Leopardi, BDS, DDS, MS Practice Limited to Implant, Fixed and Removable Prosthodontics Greenwood Village, Colorado www.knowledgefactoryco.com
Dental Implant Treatment Planning and Restorative Considerations Aldo Leopardi, BDS, DDS, MS Practice Limited to Implant, Fixed and Removable Prosthodontics Greenwood Village, Colorado www.knowledgefactoryco.com
Cytoflex Barrier Membrane Clinical Evaluation
 Cytoflex Barrier Membrane Clinical Evaluation Historical Background Guided tissue regeneration is a well established concept in the repair of oral bone defects. The exclusion of soft tissue epithelial
Cytoflex Barrier Membrane Clinical Evaluation Historical Background Guided tissue regeneration is a well established concept in the repair of oral bone defects. The exclusion of soft tissue epithelial
Multi-Modality Anterior Extraction Site Grafting Increased Predictability for Aesthetics Michael Tischler, DDS
 Page 1 of 5 Issue Date: March 2003, Posted On: 8/1/2005 Multi-Modality Anterior Extraction Site Grafting Increased Predictability for Aesthetics Michael Tischler, DDS The extraction of teeth creates a
Page 1 of 5 Issue Date: March 2003, Posted On: 8/1/2005 Multi-Modality Anterior Extraction Site Grafting Increased Predictability for Aesthetics Michael Tischler, DDS The extraction of teeth creates a
Surgery All at Once : Socket preservation and immediate placement of an implant in an infected site in the anterior region a Case Report
 Surgery All at Once : Socket preservation and immediate placement of an implant in an infected site in the anterior region a Case Report W.P. van der Schoor*, A.R.M. van der Schoor Tooth extraction followed
Surgery All at Once : Socket preservation and immediate placement of an implant in an infected site in the anterior region a Case Report W.P. van der Schoor*, A.R.M. van der Schoor Tooth extraction followed
Ridge Augmentation. Selection of Applicable Abstracts and Posters. Using Titanium-Reinforced PTFE Membranes
 Ridge Augmentation Selection of Applicable Abstracts and Posters Using Titanium-Reinforced PTFE Membranes Gultekin BA, Cansiz E, Borahan MO. Clinical and 3-Dimensional Radiographic Evaluation of Autogenous
Ridge Augmentation Selection of Applicable Abstracts and Posters Using Titanium-Reinforced PTFE Membranes Gultekin BA, Cansiz E, Borahan MO. Clinical and 3-Dimensional Radiographic Evaluation of Autogenous
Surgical Therapy. Tuesday, April 2, 13. Alessan"o Geminiani, DDS, MS
 Surgical Therapy Alessan"o Geminiani, DDS, MS Periodontal Flap: a surgical procedure in which incisions are made in the gingiva or mucosa to allow for separation of the epithelium and connective tissues
Surgical Therapy Alessan"o Geminiani, DDS, MS Periodontal Flap: a surgical procedure in which incisions are made in the gingiva or mucosa to allow for separation of the epithelium and connective tissues
Clinical Case Reports using Cytoplast GTR Barrier Membranes
 Clinical Case Reports using Cytoplast GTR Barrier Membranes S I M P L E P R E D I C TA B L E P R A C T I C A L C L I N I C A L E D U C A T I O N 4620 71st Street Lubbock, Texas 79424 888.796.1923 www.osteogenics.com
Clinical Case Reports using Cytoplast GTR Barrier Membranes S I M P L E P R E D I C TA B L E P R A C T I C A L C L I N I C A L E D U C A T I O N 4620 71st Street Lubbock, Texas 79424 888.796.1923 www.osteogenics.com
Maryland AGD AE and Socket Grafting 2015
 The Goodacre Study 5 year retrospective study looked at Crown & Bridge Caries Single crowns 1% FPD abutments 17% Periodontal Involvement Single crowns
The Goodacre Study 5 year retrospective study looked at Crown & Bridge Caries Single crowns 1% FPD abutments 17% Periodontal Involvement Single crowns
Practical Advanced Periodontal Surgery
 Practical Advanced Periodontal Surgery Serge Dibart Blackwell Munksgaard Chapter 8 Papillary Construction After Dental Implant Therapy Peyman Shahidi, DOS, MScD, Serge Dibart, DMD, and Yun Po Zhang, PhD,
Practical Advanced Periodontal Surgery Serge Dibart Blackwell Munksgaard Chapter 8 Papillary Construction After Dental Implant Therapy Peyman Shahidi, DOS, MScD, Serge Dibart, DMD, and Yun Po Zhang, PhD,
PROSPECTIVE, COMPARATIVE VOLUMETRIC ASSESSMENT OF ALVEOLAR RIDGE PRESERVATION UTILIZING DIFFERENT BONE GRAFTING MATERIALS. David Paul Semeniuk
 PROSPECTIVE, COMPARATIVE VOLUMETRIC ASSESSMENT OF ALVEOLAR RIDGE PRESERVATION UTILIZING DIFFERENT BONE GRAFTING MATERIALS David Paul Semeniuk A thesis submitted to the faculty at the University of North
PROSPECTIVE, COMPARATIVE VOLUMETRIC ASSESSMENT OF ALVEOLAR RIDGE PRESERVATION UTILIZING DIFFERENT BONE GRAFTING MATERIALS David Paul Semeniuk A thesis submitted to the faculty at the University of North
The Essential Choice. With the Benefits of Biologic Predictability
 The Essential Choice With the Benefits of Biologic Predictability Documented, Reliable, Experienced is the essential choice for your daily regenerative needs. Throughout our long history and dedication
The Essential Choice With the Benefits of Biologic Predictability Documented, Reliable, Experienced is the essential choice for your daily regenerative needs. Throughout our long history and dedication
Periodontal Disease. Radiology of Periodontal Disease. Periodontal Disease. The Role of Radiology in Assessment of Periodontal Disease
 Radiology of Periodontal Disease Steven R. Singer, DDS srs2@columbia.edu 212.305.5674 Periodontal Disease! Includes several disorders of the periodontium! Gingivitis! Marginal Periodontitis! Localized
Radiology of Periodontal Disease Steven R. Singer, DDS srs2@columbia.edu 212.305.5674 Periodontal Disease! Includes several disorders of the periodontium! Gingivitis! Marginal Periodontitis! Localized
Creating emergence profiles in immediate implant dentistry
 Creating emergence profiles in immediate implant dentistry AUTHORS Dr. Daniel Capitán Maraver Dr. Manuel Fuentes Ortiz Visiting lecturers in the Master s Degree in Clinical Practice in Implantology and
Creating emergence profiles in immediate implant dentistry AUTHORS Dr. Daniel Capitán Maraver Dr. Manuel Fuentes Ortiz Visiting lecturers in the Master s Degree in Clinical Practice in Implantology and
The Socket Shield Technique A case Report
 The Socket Shield Technique A case Report Haseeb H. Al-Dary Private Practice, Amman Jordan dary_haseeb@yahoo.com ABSTRACT In the aim of achieving an optimal esthetic result, implant dentistry has become
The Socket Shield Technique A case Report Haseeb H. Al-Dary Private Practice, Amman Jordan dary_haseeb@yahoo.com ABSTRACT In the aim of achieving an optimal esthetic result, implant dentistry has become
The anatomic limitations of the. Implant Installation With Simultaneous Ridge Augmentation. Report of Three Cases Jun-Beom Park, DDS, MSD, PhD*
 CASE REPORT Implant Installation With Simultaneous Ridge Augmentation. Report of Three Cases Jun-Beom Park, DDS, MSD, PhD* The anatomic limitations of the residual alveolar bone may cause problems for
CASE REPORT Implant Installation With Simultaneous Ridge Augmentation. Report of Three Cases Jun-Beom Park, DDS, MSD, PhD* The anatomic limitations of the residual alveolar bone may cause problems for
Planning for esthetics Part II: adjacent implant restorations
 C L I N I C A L Planning for esthetics Part II: adjacent implant restorations William C Martin, 1 Emma Lewis, 2 Dean Morton 3 1 DMD, MS, Associate Professor & Clinical Director, Center for Implant Dentistry,
C L I N I C A L Planning for esthetics Part II: adjacent implant restorations William C Martin, 1 Emma Lewis, 2 Dean Morton 3 1 DMD, MS, Associate Professor & Clinical Director, Center for Implant Dentistry,
Conventional immediate implant placement and immediate placement with socket-shield technique Which is better
 International Journal of Clinical Medicine Research 2014; 1(5): 176-180 Published online December 30, 2014 (http://www.aascit.org/journal/ijcmr) ISSN: 2375-3838 Conventional immediate implant placement
International Journal of Clinical Medicine Research 2014; 1(5): 176-180 Published online December 30, 2014 (http://www.aascit.org/journal/ijcmr) ISSN: 2375-3838 Conventional immediate implant placement
The Sandwich Bone Augmentation Technique. Jia-Hui Fu* and Hom-Lay Wang*
 CASE REPORT The Sandwich Bone Augmentation Technique Jia-Hui Fu* and Hom-Lay Wang* Introduction: Horizontal ridge width reduction after tooth extraction is a common clinical scenario. As such, when implant-supported
CASE REPORT The Sandwich Bone Augmentation Technique Jia-Hui Fu* and Hom-Lay Wang* Introduction: Horizontal ridge width reduction after tooth extraction is a common clinical scenario. As such, when implant-supported
Bone Grafting and Immediate Implant Placement in the Anterior
 Bone Grafting and Immediate Implant Placement in the Anterior by Timothy F. Kosinski, DDS, MAGD Whether a consequence of periodontal disease, caries or trauma to the root, losing an anterior tooth is psychologically
Bone Grafting and Immediate Implant Placement in the Anterior by Timothy F. Kosinski, DDS, MAGD Whether a consequence of periodontal disease, caries or trauma to the root, losing an anterior tooth is psychologically
Socket preservation using deproteinized horsederived
 Research Article J Periodontal Implant Sci 2010;40:227-231 doi: 10.5051/jpis.2010.40.5.227 Socket preservation using deproteinized horsederived bone mineral Jang-Yeol Park, Ki-Tae Koo, Tae-Il Kim, Yang-Jo
Research Article J Periodontal Implant Sci 2010;40:227-231 doi: 10.5051/jpis.2010.40.5.227 Socket preservation using deproteinized horsederived bone mineral Jang-Yeol Park, Ki-Tae Koo, Tae-Il Kim, Yang-Jo
Immediate Implant Placement Along With Guided Bone Regeneration In Mandibular Anterior Region A Case Report.
 IMMEDIATE IMPLANT PLACEMENT ALONG WITH GUIDED BONE REGENERATION IN MANDIBULAR ANTERIOR REGION A CASE REPORT. Dr.C.P.Dhivakar 1, Dr.T.Saravanan 2, Dr.A.Aniz 3 1) Department of Periodontics, Karpaga Vinayaga
IMMEDIATE IMPLANT PLACEMENT ALONG WITH GUIDED BONE REGENERATION IN MANDIBULAR ANTERIOR REGION A CASE REPORT. Dr.C.P.Dhivakar 1, Dr.T.Saravanan 2, Dr.A.Aniz 3 1) Department of Periodontics, Karpaga Vinayaga
Alveolar Ridge Augmentation with Titanium Mesh and Particulate Allograft A Case Report
 Alveolar Ridge Augmentation with Titanium Mesh and Particulate Allograft A Case Report Dr. Pratibha Borasi, Dr. Praneeta Kamble Department of Periodontics, Nair Hospital Dental College, Mumbai, Maharashtra,
Alveolar Ridge Augmentation with Titanium Mesh and Particulate Allograft A Case Report Dr. Pratibha Borasi, Dr. Praneeta Kamble Department of Periodontics, Nair Hospital Dental College, Mumbai, Maharashtra,
Immediate implants at fresh extraction sockets: from myth to reality
 Periodontology 2000, Vol. 66, 2014, 132 152 2014 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd Printed in Singapore. All rights reserved PERIODONTOLOGY 2000 Immediate implants at fresh extraction
Periodontology 2000, Vol. 66, 2014, 132 152 2014 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd Printed in Singapore. All rights reserved PERIODONTOLOGY 2000 Immediate implants at fresh extraction
Clinical Success. with the Proven. Clinical Success. with the Proven Bone Substitute Products
 Clinical Success with the Proven Bone Substitute Products Clinical Success with the Proven Bone Geistlich Bio-Oss Substitute Geistlich Bio-Oss Collagen Geistlich Bio-Oss Pen Documented More than 1,000
Clinical Success with the Proven Bone Substitute Products Clinical Success with the Proven Bone Geistlich Bio-Oss Substitute Geistlich Bio-Oss Collagen Geistlich Bio-Oss Pen Documented More than 1,000
Implant Site Development Part I
 REVIEW ARTICLE Implant Site Development Part I 1 Umang Nayar, 2 Shankar Iyer IJCID Implant Site Development Part I 1 Consultant, Dental Surgeon and Periodontist at Max Health Care, New Delhi, Professor
REVIEW ARTICLE Implant Site Development Part I 1 Umang Nayar, 2 Shankar Iyer IJCID Implant Site Development Part I 1 Consultant, Dental Surgeon and Periodontist at Max Health Care, New Delhi, Professor
Contemporary Periodontal Surgery
 Contemporary Periodontal Surgery Chris van Kesteren, D.D.S. CPCC Dental Hygiene Program October 18, 2011 Surgical Management of Periodontitis Periodontal Plastic Surgery Soft tissue and esthetics Dental
Contemporary Periodontal Surgery Chris van Kesteren, D.D.S. CPCC Dental Hygiene Program October 18, 2011 Surgical Management of Periodontitis Periodontal Plastic Surgery Soft tissue and esthetics Dental
Dental Implant Placement in the Maxillary Anterior Region: Guidelines for Aesthetic Success Michael Tischler, DDS
 Page 1 of 10 Issue Date: March 2005, Posted On: 5/2/2005 Dental Implant Placement in the Maxillary Anterior Region: Guidelines for Aesthetic Success Michael Tischler, DDS Figure 1. A 43-year-old female
Page 1 of 10 Issue Date: March 2005, Posted On: 5/2/2005 Dental Implant Placement in the Maxillary Anterior Region: Guidelines for Aesthetic Success Michael Tischler, DDS Figure 1. A 43-year-old female
TOPICS. T O P I C S Day 2. Introduction Surgical challenges to treat esthetic implant failures Treatment options & case reports Conclusions
 T O P I C S Day 2 Implant placement post extraction with simultaneous contour augmentation using GBR: When immediate, when early, when late? CAD-CAM technology and zirconia: new opportunities for esthetic
T O P I C S Day 2 Implant placement post extraction with simultaneous contour augmentation using GBR: When immediate, when early, when late? CAD-CAM technology and zirconia: new opportunities for esthetic
Then and Now. Implant Therapy:
 Implant Therapy: Then and Now by Timothy F. Kosinski, DDS, MAGD Implant dentistry has come a long way since blade and subperiostal implants were widely used. Improvements in implant design and site preparation
Implant Therapy: Then and Now by Timothy F. Kosinski, DDS, MAGD Implant dentistry has come a long way since blade and subperiostal implants were widely used. Improvements in implant design and site preparation
Dental implants certainly have
 CLINICAL Facial Wall Defect Grafting Techniques in Preparation for a Dental Implant by Timothy Kosinski, DDS, MAGD Dental implants certainly have become a popular method of restoring missing teeth. The
CLINICAL Facial Wall Defect Grafting Techniques in Preparation for a Dental Implant by Timothy Kosinski, DDS, MAGD Dental implants certainly have become a popular method of restoring missing teeth. The
Guided surgery as a way to simplify surgical implant treatment in complex cases
 52 STARGET 1 I 12 StraUMaNN CareS r ry vincenzo MiriSOLA Di TOrreSANTO AND LUCA COrDArO Guided surgery as a way to simplify surgical implant treatment in complex cases Background A 41-year-old woman with
52 STARGET 1 I 12 StraUMaNN CareS r ry vincenzo MiriSOLA Di TOrreSANTO AND LUCA COrDArO Guided surgery as a way to simplify surgical implant treatment in complex cases Background A 41-year-old woman with
We Want to Keep You Smiling. Bone Regeneration with Geistlich Bio-Oss and Geistlich Bio-Gide
 We Want to Keep You Smiling Bone Regeneration with Geistlich Bio-Oss and Geistlich Bio-Gide Strong Bone for a Healthier Smile Strong and healthy teeth provide a feeling of well-being, self-confidence and
We Want to Keep You Smiling Bone Regeneration with Geistlich Bio-Oss and Geistlich Bio-Gide Strong Bone for a Healthier Smile Strong and healthy teeth provide a feeling of well-being, self-confidence and
Immediate implant placement in a single staged
 Bone and Crescent Shaped Free Gingival Grafting for Anterior Immediate Implant Placement: Technique and Case Report Han et al Thomas Han, DDS, MS 1 2 Abstract Immediate implant placement in a single staged
Bone and Crescent Shaped Free Gingival Grafting for Anterior Immediate Implant Placement: Technique and Case Report Han et al Thomas Han, DDS, MS 1 2 Abstract Immediate implant placement in a single staged
Rehabilitation of atrophic partially edentulous mandible using ridge split technique and implant supported removable prosthesis
 CASE REPORT Rehabilitation of atrophic partially edentulous mandible using ridge split technique and implant supported removable prosthesis Dr Ashish Yadav 1, Dr Aratee Gupta 2, Dr Archana Singh 3, 1,3-
CASE REPORT Rehabilitation of atrophic partially edentulous mandible using ridge split technique and implant supported removable prosthesis Dr Ashish Yadav 1, Dr Aratee Gupta 2, Dr Archana Singh 3, 1,3-
Several extraction socket classifications have been
 Case Report Type 3 ReceSSion DefeCTS Clinical Management of Type 3 Recession Defects With Immediate Implant and Provisional Restoration Therapy: A Case Report Dennis P. Tarnow, DDS; and Stephen J. Chu,
Case Report Type 3 ReceSSion DefeCTS Clinical Management of Type 3 Recession Defects With Immediate Implant and Provisional Restoration Therapy: A Case Report Dennis P. Tarnow, DDS; and Stephen J. Chu,
Clinical cases by Dr. Fernando Rojas-Vizcaya. botiss. dental bone & tissue regeneration. biomaterials. strictly biologic
 Clinical cases by Dr. Fernando Rojas-Vizcaya dental bone & tissue regeneration botiss biomaterials strictly biologic botiss BTR system: BONE biologic potential bovine block & granules: pure bone mineral
Clinical cases by Dr. Fernando Rojas-Vizcaya dental bone & tissue regeneration botiss biomaterials strictly biologic botiss BTR system: BONE biologic potential bovine block & granules: pure bone mineral
FRACTURES AND LUXATIONS OF PERMANENT TEETH
 FRACTURES AND LUXATIONS OF PERMANENT TEETH 1. Treatment guidelines and alveolar bone Followup Procedures INFRACTION Clinical findings Radiographic findings Treatment Follow-Up Favorable Outcome Unfavorable
FRACTURES AND LUXATIONS OF PERMANENT TEETH 1. Treatment guidelines and alveolar bone Followup Procedures INFRACTION Clinical findings Radiographic findings Treatment Follow-Up Favorable Outcome Unfavorable
Extraction socket preservation using β tricalcium phosphate bone graft plug and platelet rich fibrin membrane A case series
 2014; 1(1): 39-43 ISSN Print: 2394-7489 ISSN Online: 2394-7497 IJADS 2014; 1(1): 39-43 2014 IJADS www.oraljournal.com Received: 02-01-2015 Accepted: 07-02-2015 Shantipriya Reddy Prof and Head, department
2014; 1(1): 39-43 ISSN Print: 2394-7489 ISSN Online: 2394-7497 IJADS 2014; 1(1): 39-43 2014 IJADS www.oraljournal.com Received: 02-01-2015 Accepted: 07-02-2015 Shantipriya Reddy Prof and Head, department
Esthetic Crown Lengthening for Upper Anterior Teeth: Indications and Surgical Techniques
 I J Pre Clin Dent Res 2014;1(2):49-53 April-June All rights reserved International Journal of Preventive & Clinical Dental Research Esthetic Crown Lengthening for Upper Anterior Teeth: Indications and
I J Pre Clin Dent Res 2014;1(2):49-53 April-June All rights reserved International Journal of Preventive & Clinical Dental Research Esthetic Crown Lengthening for Upper Anterior Teeth: Indications and
Esthetic management of multiple missing anterior teeth A Case report
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861. Volume 13, Issue 1 Ver. II (Jan. 2014), PP 97-101 Esthetic management of multiple missing anterior teeth A
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861. Volume 13, Issue 1 Ver. II (Jan. 2014), PP 97-101 Esthetic management of multiple missing anterior teeth A