PSYCHIATRIC AND PSYCHOLOGICAL ASPECTS OF CANCER
|
|
|
- Russell Tate
- 5 years ago
- Views:
Transcription
1 PSYCHIATRIC AND PSYCHOLOGICAL ASPECTS OF CANCER Prof. Dr. Mine Özkan University of Istanbul Istanbul Faculty of Medicine Department of Psychiatry Institute of Oncology Department of Psychooncology
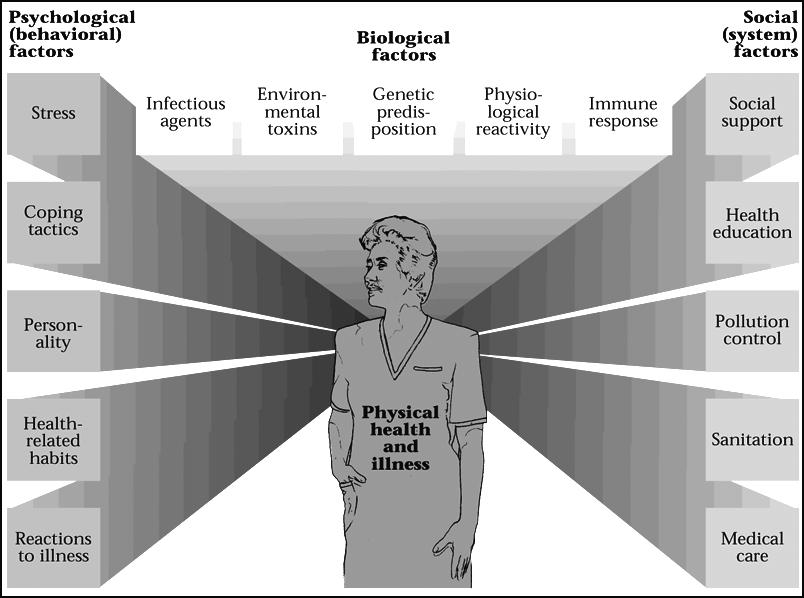
2 Biopsychosocial Model
3 Each physical illness is a crisis Medically it involves physiopathologic-organic processes For patient A biopsychosocial situation, identity and existential crisis 3
4 PSYCHO-ONCOLOGY Psycho-oncology is an area of specialization which aims to understand and to treat from prevention to bereavement, the functional aspects and psychological, emotional and quality of life issues of cancer. Psycho-oncology or psychiatric oncology investigates: 1- Psychological effects of cancer on patient, family and the medical staff. 2-The effects of psychological and behavioral factors on cancer risk and prognosis. It is also a discipline which provides psychological medicine services to cancer patients.
5 PSYCHOSOCIAL ONCOLOGY Historical Development In 1950s..Developments in chemotherapy and the onset of questioning of the quiet attitude towards cancer. In 1960s Fast developments in the diagnosis and treatment of cancer and the psychiatric research on cancer patients gains speed. In 1970s with the developments in cancer care, patients become more involved in treatment options and decisions and their quality of life expectations is heightened. Liaison psychiatry services grow faster in general hospitals and biopsychosocial perception is adopted.
6 PSYCHOSOCIAL ONCOLOGY Historical Development In 1980s psychiatric complications of cancer and its treatment strategies are better defined, discussion about medico-legal issues and euthanasia took place. In 1990s with the increase of the research on psychiatric and psychosocial research of cancer,development of psychoneuroimmunology, appearance of quality of life concept and social education and with the acceptance of psychooncology as a scientific discipline, biopsychosocial integrative approach is ultimately accepted.

7 ILLNESS AS A STRESSOR Diagnosis Pain Facing death Fear STRESS Change in family roles Decisions about treatment Decrease in physical capacity Changes in social environment Difficult treatments
8 REACTION TO CANCER DIAGNOSIS In cancer patients, emotional and behavioral reactions can be appeared. Bolund defined the process after the cancer diagnosis in 4 steps: 1) Shock 2) Reaction 3) Resistance 4) Adjustment Elisabeth Kübler Ross defined this process in 5 steps: 1) Denial 2) Anger 3) Negotiation 4) Depression 5) Acceptance 8
9 REACTION TO CANCER DIAGNOSIS First Stage Shock, denial, anger-revolt ( why me? ) Depressive mood Generally less than 1 week Second Stage Anxiety, depressive mood, appetite and sleep disturbances, attention deficit, functional disturbances Generally 1-2 weeks Third Stage: Adjustment Accepting the diagnosis validity and the evaluation of treatment options and back to normal activities. Generally 2 weeks, but it may take months 9
10 REACTION TO CANCER DIAGNOSIS FEARS OF CANCER PATIENTS Death Disability Distortion of body image Dependency Disruption in relationships, role functioning, and financial status 10
11 CANCERANDADJUSTMENT Adjustment mechanisms are defined as; Fighting spirit Helplessness and hopelessness Distressing excessive preoccupation Fatalist acceptance Avoidance and Denial
12 PSYCHOLOGICAL IMPACT High Risk Profile Patients: Passive/Helpless/Pessimistic attitude Rigid approach to new environments Demanding Highly anxious patients Low social support Time pressures being behind
13 DENIAL Denial s Function Protects patients from unbearable pain causing psychological distress or suicide Since it is a coping mechanism, an intervention such as a direct facing is not recommended Total denial may cause treatment rejection and may need intervention 13
14 GIVING BAD NEWS 1-Preparing the patient for the interview 2-Investigating patient s level of knowledge 3-Learning how much the patient wants to know. 4-Sharing the information 5-Coping with the patients emotions 6-Sharing treatment strategy and planning the forthcoming interview.
15 GIVING BAD NEWS The way of giving information is as important as the information itself The session should be held with the patient in a special setting Medical jargon should be avoided Comprehensibility, being emphatic and making eye contact is important Using open and simple expressions is important Information should be given slowly Giving support is important Including the patient into the decision making process is important Second interview should be arranged The patient should be given enough time to process the news and formulate his questions Questions should be answered honestly by maintaining hope
16 PSYCHIATRIC DISORDERS IN CANCER PATIENTS Adjustment Disorders Anxiety Disorders Depressive Syndromes Organic Brain Syndromes (delirium, dementia, neuropsychiatric side effects of chemotherapeutical agents) Personality Disorders Pain Disorder Loss of appetite, nausea and vomiting Sleep disorder Sexual dysfunction 16
17 DISTRIBUTION OF PSYCHIATRIC DISORDERS IN CANCER %0 %50 %80 %100 Normal responses to cancer, Day to day crisis, stress Adjustment disorders with depressed/ anxious symptoms Depression Delirium Anxiety Disorders Personality Disorders Major Mental Illness 17
18 ADJUSTMENT DISORDER About %21 of cancer patients have adjustment disorders Emotional or behavioral symptoms as an evidence of maladaptive reactions to stressor Adjustment to the diagnosis of cancer, its course, and treatment Malfunctioningin one or more psychosocial areas such as work, interpersonal relationships, activities of daily living is the characteristic of adjustment disorders Symptoms are not very specific and usually resolve within 6 months
19 PSYCHOLOGICAL ADJUSTMENT TO CANCER Psychological Adjustment is influenced by: 1) Medical factors : -site of tumor -stage and course of disease -prognostic factors -symptoms -pain 2) Factors related to patient: -personality -coping mechanisms -life events 3) Socio-cultural factors: -attitudes and beliefs -available social support
20 PREVELANCE OF DEPRESSION %9-20 in general population in Turkey More in women The prevalence of depression in cancer patients is reported to be in between %20-50
21 CANCER AND DEPRESSION The factors that increase depression risk in cancer patients are: Depressive disorder or alcoholism history Late stage of cancer Insufficient social support Uncontrolled pain Some drugs used during treatment
22 ASSESSING DEPRESSION IN CANCER PATIENTS Paying attention to somatic symptoms which could be caused by cancer (or treatment) is important: Poor appetite or anorexia Sleep problems, insomnia Poor concentration Loss of physical energy
23 DIAGNOSIS OF DEPRESSION IN CANCER PATIENTS Intensive and continuous depressed mood Diminished interest or pleasure in activities (also in the area of interpersonal relations) Feelings of worthlessness or excessive guilt (considering the illness as a punishment for his / her faults) Recurrent thoughts of death or suicidal ideation (not fear of death) Psychomotor retardation or agitation 23
24 DIAGNOSIS OF DEPRESSION IN CANCER PATIENTS If the patient does not participate to the treatment, does not feel good and/or has a low functioning although his physical situation does well If somatic symptoms are intensive, continuous and not proportional to physical illness, but elated to depressive mood 24
25 WHY DEPRESSION IS MORE FREQUENT? BIOLOGICAL MECHANISMS Primary or metastatic involvement of brain, existence of BOS tumor cells, related to mania or depression Chemotherapeutic agents; vinkristine, vinblastine, corticosteroids, interferon, interleukine-2, asparaginase, procarbazine, tamoxifen Cortisol, IL-6 and changes in natural killer cell activity Chronic stress and depression, activation of hypotalamic-hypophysial-adrenal axe; release of mediators that supress normal immune responses; especially in virus induced cancers, it may affect the appearence and development of the illness
26 PSYCHOSOCIAL FACTORS Stress, social relations, support, coping, personality, anxiety, depression A ENDOCRINE ACTIVATION HPA axe, autonomous activation, Other hormones. E B C CIRCADIAN RHYTHMES Sleep, activity, endocrine, Metabolic and immune rhythms F G D IMMUNE DEFENSES CTL, T cells, B cells, NK and LAK cells, macrophages. H Tumor progression (Semphton, 2003)
27 RISKS FACTORS IN MEDICALLY INDUCED DEPRESSION Unrelieved pain Other chronic illness/ disability, terminal stage Treatment side effects Metabolic (anemia, hypercalcemia ) Nutritional (deficiency of vitamin B12 or folat) Endocrine (hyper-hypotiroidism, adrenal insufficiency) Neurologic (paraneoplastic syndromes) Site of the cancer (pancreas, small cell lung, liver, head and neck, leukemia)
28 DEPRESSION IS AN APPROPRIATE REACTION TO CANCER DIAGNOSIS? Sadness and anxiety alone with the feeling of loss accompanying the cancer diagnosis are normal reactions Grief process may be diminished in days and weeks by the support of the treatment team, family and the spouse Anhedonia, treatment rejection or hopelessness and suicidal ideation which may cause social isolation should be given attention Blues sorrow is a normal reaction Depressive syndrome is never normal, the need for its treatment is certain.
29 EFFECTS OF DEPRESSION IN CANCER PATIENTS Deterioration of the quality of life Higher levels of pain Burden for the family Longer hospital stay Reduced adherence to treatment Less efficacy of chemotherapy Shorter survival expectancy Risk of suicide
30 SUICIDE RISK IN CANCER In cancer patients, the risk of suicide is 1.5 times higher than normal population Especially in terminal phases, suicidal ideation is about %8 Desire for a faster death in cancer patients with an advanced and terminal stage disease is about %17 The desire for death is usually associated with poor physical conditions, depressive state, hopelessness, low social support
31 FACTORS AFFECTING SUICIDE RISK Psychological factors A history of depression or suicide attempt in patient or in the family Alcoholism and/or substance abuse Depression Helplessness, hopelessness, burnout Loss or grief in near past Social isolation Medical factors Uncontrolled pain Delirium with disturbed impulse control Advanced disease 31

32 TREATMENT Antidepressants TCA are potentially problematic because of anticholinergic and anti-alpha-adrenergic effects Can be useful in patients with co-morbid neuropathic pain syndromes Attention should be given to patients with a tendency for delirium and using opioids MAOI should be avoided because of drug-drug and drug-food interactions
33 Antidepressants SSRI, SNRI, mirtazapine, bupropion- most frequently because of their safety and generally favorable side effect profiles Venlafaxine, duloxetine and milnasipran are useful in pain syndromes, indicated in neuropathic pain SSRI and venlafaxine are useful for hot flashes and night sweating Be careful for the drug interactions with SSRI

34 PSYCHOSTIMULANTS Fast effect Especially for those with a limited survival time May correct cognitive problems (increase attention and concentration) Increase energy Increase the effects of analgesics and decrease opiate induced sedation Metilphenidate is especially effective for terminal patients in 48 hours
35 ANXIETY THREATS Disappearing Separation Loss of control Anxiety Conflicts Defense Mechanisms Coping Skills: Effort for being informed Sharing Taking action Denial Dependency Regression Projection Symptoms of Anxiety Discomfort Anxious waiting Physiological complaints Sleep disorder Free Anxiety Panic Disorder Psychotic Anxiety 35
36 CANCER AND ANXIETY DISORDERS Anxiety is quite often precipitated by cancer It is a subjective phenomenon difficult to assess It is about twice as common in cancer patients as in controls Often coexistent with depression Its principal component is negative affect
37 CANCER AND ANXIETY DISORDERS Main symptoms of anxiety disorders: Insomnia Excessive sensitivity Concentration deficits Impatience Panic attacks Dyspnea, heart palpitations, sweating Mouth dryness, vertigo Gastrointestinal symptoms
38 CANCER AND ANXIETY DISORDERS At the beginning, in cancer patients anxiety attacks are frequently seen during diagnosis and crisis stages. Anxiety provoking situations in these patients are: Diagnosis stage Waiting for examination results Before a new treatment Change of treatment Appearance of symptom Appearance of relapse Experiencing changes being reminiscent of the illness

39 TREATMENT Benzodiazepines SSRI Other antidepressants such as: Venlafaxine, mirtazapine, trazadone Beta-blockers Antihistaminics Neuroleptics Buspiron Combination Strategies
40 DELIRIUM IN CANCER The incidence of delirium in cancer patients is about %15-20; as a pretty high percentage In terminal patients this percentage is around %85. Direct causes Primary tumor Local invasion Metastatic invasion hematogenically or lymphatically Indirect Causes Metabolic problems Effects of treatment Infections Vascular complications Nutritional deficits 40
41 DELIRIUM IN CANCER PATIENTS Delirium is a fast and suddenly developing brain insufficiency Delirium in cancer patients is a frequently seen psychiatric situation which necessitates emergency intervention and treatment. It has high potential of causing death or dementia development. Therefore, its early detection and its fast and efficient treatment is very important.
42 DELIRIUM IN CANCER PATIENTS Symptoms experienced in these patients are as follows: Confusion Orientation deficits Psychomotor agitation or retardation Inability to pay attention (distractibility) Sleep-wake cycle disruption Diurnal variation Autonomic dysfunction Illusions and hallusinations Delusions

43 TREATMENT The main aim is the treatment of the underlying disorder Preventing self or environmentally injuring behaviors Close observance Arranging environmental conditions Antipsychotics Benzodiazepines
44 CANCER AND FAMILY The illness causes a crisis not only for the patient but also for his/her family Besides the cancer patient, generally families also need psychological treatment and support In the families where the relationships are balanced, emotions are easily expressed, conflicts are rare and cooperation is high, thus the patient adaptation is increased In case of unclear family roles, over controlling and strict family contexts, the adaptation of the patient becomes more difficult Denial of the possible conflicts makes the solution of these conflicts even more difficult
45 CANCER AND MEDICAL STAFF Staff working with cancer patients are under stress in every stage of the illness, especially during terminal stage Difficulties experienced by the staff are related to: The patient s situation Relations with patient and patient s family Care context Treatment conditions Their own roles and expectancies 45
46 CANCER AND MEDICAL STAFF After the death of the patient many experts experience: -Feelings of guilt -Headache -Sleep disturbances -Various psycho-physiological function deficits The team of consultation-liaison psychiatry by providing psychiatric and psychosocial care help medical staff in solving these difficulties 46
47 PSYCHOTHERAPY IN CANCER Cognitive behavioral therapy Psychodynamic therapies (supportive-expressive) Crisis intervention and short term psychotherapies Behavioral techniques Short term dynamic psychotherapy Group psychotherapy Psychosocial care and the arrangement of therapeutic context 47
48 PSYCHOLOGICAL TREATMENT The main goals : to reduce psychological anxiety and pain to establish adaptation to increase the quality of life to help in the expression of emotions to increase the life energy and coping to help in coping with the illness multidimensional crisis in a healthy way to correct existing misperceptions to correct all or nothing style behaviors and thoughts to enhance social support and communication
49 Considering the patient as a whole while treating the patient Psychological withdrawal precipitates bodily exhaustion The healthy adjustment of a patient to the new situation is related to his/her psychological health Life should be reconstructed relevant to the new physical and psychological condition and relationships maintained normally
50 The perception of the treatment team towards the patients and the illness influences patient s self perception Avoidance of stigmatic attitude towards cancer is important A positive fighting spirit should be created Our aim is to conduct a marathon together with the patient, family and multidisciplinary treatment team without being exhausted
51 From illness to life As a team, with the belief and pride that science, trust and affection are the prime values for health and happiness
52 THANK YOU
Psychosis, Mood, and Personality: A Clinical Perspective
 Psychosis, Mood, and Personality: A Clinical Perspective John R. Chamberlain, M.D. Assistant Director, Psychiatry and the Law Program Assistant Clinical Professor University of California San Francisco
Psychosis, Mood, and Personality: A Clinical Perspective John R. Chamberlain, M.D. Assistant Director, Psychiatry and the Law Program Assistant Clinical Professor University of California San Francisco
PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS. Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA
 CASE #1 PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA OBJECTIVES Epidemiology Presentation in older adults Assessment Treatment
CASE #1 PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA OBJECTIVES Epidemiology Presentation in older adults Assessment Treatment
8/22/2016. Contemporary Psychiatric-Mental Health Nursing Third Edition. Theories: Anxiety Disorders. Theories: Anxiety Disorders (cont'd)
") Contemporary Psychiatric-Mental Health Nursing Third Edition CHAPTER 18 Anxiety Disorders Theories: Anxiety Disorders Biological changes in the brain Noradrenergic system is sensitive to norepinephrine;
Contemporary Psychiatric-Mental Health Nursing Third Edition CHAPTER 18 Anxiety Disorders Theories: Anxiety Disorders Biological changes in the brain Noradrenergic system is sensitive to norepinephrine;
Caring for the Mind: Managing Depression and Anxiety. Highlights from 2017 ONS Congress
 Caring for the Mind: Managing Depression and Anxiety Highlights from 2017 ONS Congress Mood and Anxiety Disorders: Symptoms of mood disorders Non-reactive mood, worthlessness, guilt, loss of interest,
Caring for the Mind: Managing Depression and Anxiety Highlights from 2017 ONS Congress Mood and Anxiety Disorders: Symptoms of mood disorders Non-reactive mood, worthlessness, guilt, loss of interest,
Contemporary Psychiatric-Mental Health Nursing Third Edition. Theories: Anxiety Disorders. Theories: Anxiety Disorders (cont'd) 10/2/2014
 10/2/2014") Contemporary Psychiatric-Mental Health Nursing Third Edition CHAPTER 18 Anxiety Disorders Theories: Anxiety Disorders Biological changes in the brain Neurotransmitters are associated with anxiety. low
Contemporary Psychiatric-Mental Health Nursing Third Edition CHAPTER 18 Anxiety Disorders Theories: Anxiety Disorders Biological changes in the brain Neurotransmitters are associated with anxiety. low
SECTION 1. Children and Adolescents with Depressive Disorder: Summary of Findings. from the Literature and Clinical Consultation in Ontario
 SECTION 1 Children and Adolescents with Depressive Disorder: Summary of Findings from the Literature and Clinical Consultation in Ontario Children's Mental Health Ontario Children and Adolescents with
SECTION 1 Children and Adolescents with Depressive Disorder: Summary of Findings from the Literature and Clinical Consultation in Ontario Children's Mental Health Ontario Children and Adolescents with
Depression in Late Life
 Depression in Late Life Robert Madan MD FRCPC Geriatric Psychiatrist Key Learnings Robert Madan MD FRCPC Key Learnings By the end of the session, participants will be able to List the symptoms of depression
Depression in Late Life Robert Madan MD FRCPC Geriatric Psychiatrist Key Learnings Robert Madan MD FRCPC Key Learnings By the end of the session, participants will be able to List the symptoms of depression
Depression Workshop 26 January 2007
 Depression Workshop 26 January 2007 Leslie G Walker Professor of Cancer Rehabilitation Donald M Sharp Senior Lecturer in Behavioural Oncology Mary B Walker Senior Clinical and Research Nurse Specialist
Depression Workshop 26 January 2007 Leslie G Walker Professor of Cancer Rehabilitation Donald M Sharp Senior Lecturer in Behavioural Oncology Mary B Walker Senior Clinical and Research Nurse Specialist
A Basic Approach to Mood and Anxiety Disorders in the Elderly
 A Basic Approach to Mood and Anxiety Disorders in the Elderly November 1 2013 Sarah Colman MD FRCPC Clinical Fellow, Geriatric Psychiatry Mount Sinai Hospital, University of Toronto Disclosure No conflict
A Basic Approach to Mood and Anxiety Disorders in the Elderly November 1 2013 Sarah Colman MD FRCPC Clinical Fellow, Geriatric Psychiatry Mount Sinai Hospital, University of Toronto Disclosure No conflict
Depression in the Eldery Handout Package
 Depression in the Eldery Handout Package Depression in the Elderly 1 Learning Objectives Upon completion of this module, you should be able to: 1. State the prevalence and describe the consequences of
Depression in the Eldery Handout Package Depression in the Elderly 1 Learning Objectives Upon completion of this module, you should be able to: 1. State the prevalence and describe the consequences of
Guidelines MANAGEMENT OF MAJOR DEPRESSIVE DISORDER (MDD)
") MANAGEMENT OF MAJOR DEPRESSIVE DISORDER (MDD) Guidelines CH Lim, B Baizury, on behalf of Development Group Clinical Practice Guidelines Management of Major Depressive Disorder A. Introduction Major depressive
MANAGEMENT OF MAJOR DEPRESSIVE DISORDER (MDD) Guidelines CH Lim, B Baizury, on behalf of Development Group Clinical Practice Guidelines Management of Major Depressive Disorder A. Introduction Major depressive
Terry Rabinowitz, MD, DDS
 Terry Rabinowitz, MD, DDS Office: FAHC, Patrick 431 Telephone: 802-847-2112 E-mail: Terry.Rabinowitz@vtmednet.org Understand what depression is and differentiate it from the blues Learn about stress and
Terry Rabinowitz, MD, DDS Office: FAHC, Patrick 431 Telephone: 802-847-2112 E-mail: Terry.Rabinowitz@vtmednet.org Understand what depression is and differentiate it from the blues Learn about stress and
SCREENING FOR COMMON MENTAL DISORDERS DEPRESSIVE AND ANXIETY DISORDERS SUBSTANCE USE DISORDERS
 SCREENING FOR COMMON MENTAL DISORDERS DEPRESSIVE AND ANXIETY DISORDERS SUBSTANCE USE DISORDERS COMMON MENTAL DISORDERS Depressive Disorders Anxiety Disorders Substance use disorders CMD in HIV Twice as
SCREENING FOR COMMON MENTAL DISORDERS DEPRESSIVE AND ANXIETY DISORDERS SUBSTANCE USE DISORDERS COMMON MENTAL DISORDERS Depressive Disorders Anxiety Disorders Substance use disorders CMD in HIV Twice as
Depressive, Bipolar and Related Disorders
 Depressive, Bipolar and Related Disorders Robert Kelly, MD Assistant Professor of Psychiatry Weill Cornell Medical College White Plains, New York Lecture available at www.robertkelly.us Financial Conflicts
Depressive, Bipolar and Related Disorders Robert Kelly, MD Assistant Professor of Psychiatry Weill Cornell Medical College White Plains, New York Lecture available at www.robertkelly.us Financial Conflicts
Managing Pain. in Marfan Syndrome. Traci J. Speed, MD PhD Assistant Professor, Department of Psychiatry and Behavioral Sciences
 Managing Pain in Marfan Syndrome Traci J. Speed, MD PhD Assistant Professor, Department of Psychiatry and Behavioral Sciences No financial disclosures Objectives Define pain Discuss the role of comorbid
Managing Pain in Marfan Syndrome Traci J. Speed, MD PhD Assistant Professor, Department of Psychiatry and Behavioral Sciences No financial disclosures Objectives Define pain Discuss the role of comorbid
Mental Health Nursing: Anxiety Disorders. By Mary B. Knutson, RN, MS, FCP
 Mental Health Nursing: Anxiety Disorders By Mary B. Knutson, RN, MS, FCP A Definition of Anxiety Diffuse apprehension that is vague in nature and associated with feelings of uncertainty and helplessness
Mental Health Nursing: Anxiety Disorders By Mary B. Knutson, RN, MS, FCP A Definition of Anxiety Diffuse apprehension that is vague in nature and associated with feelings of uncertainty and helplessness
Depressive and Bipolar Disorders
 Depressive and Bipolar Disorders Symptoms Associated with Depressive and Bipolar Disorders Characteristics of mood symptoms Affects a person s well being, school, work, or social functioning Continues
Depressive and Bipolar Disorders Symptoms Associated with Depressive and Bipolar Disorders Characteristics of mood symptoms Affects a person s well being, school, work, or social functioning Continues
Depression: Assessment and Treatment For Older Adults
 Tool on Depression: Assessment and Treatment For Older Adults Based on: National Guidelines for Seniors Mental Health: the Assessment and Treatment of Depression Available on line: www.ccsmh.ca www.nicenet.ca
Tool on Depression: Assessment and Treatment For Older Adults Based on: National Guidelines for Seniors Mental Health: the Assessment and Treatment of Depression Available on line: www.ccsmh.ca www.nicenet.ca
Depression in the Medically Ill
 Mayo School of Continuous Professional Development Psychiatry in Medical Settings February 9 th, 2017 Depression in the Medically Ill David Katzelnick, M.D. Professor of Psychiatry, Mayo Clinic College
Mayo School of Continuous Professional Development Psychiatry in Medical Settings February 9 th, 2017 Depression in the Medically Ill David Katzelnick, M.D. Professor of Psychiatry, Mayo Clinic College
March 29, 2017 Debra K. Smith, Ph.D. St. Charles Hospital Port Jefferson, New York
 Traumatic Brain Injury: Management of Psychological and Behavioral Sequelae March 29, 2017 Debra K. Smith, Ph.D. St. Charles Hospital Port Jefferson, New York The Functional Impact of
Traumatic Brain Injury: Management of Psychological and Behavioral Sequelae March 29, 2017 Debra K. Smith, Ph.D. St. Charles Hospital Port Jefferson, New York The Functional Impact of
Are All Older Adults Depressed? Common Mental Health Disorders in Older Adults
 Are All Older Adults Depressed? Common Mental Health Disorders in Older Adults Cherie Simpson, PhD, APRN, CNS-BC Myth vs Fact All old people get depressed. Depression in late life is more enduring and
Are All Older Adults Depressed? Common Mental Health Disorders in Older Adults Cherie Simpson, PhD, APRN, CNS-BC Myth vs Fact All old people get depressed. Depression in late life is more enduring and
Depression and Anxiety
 Depression and Anxiety ANN HACKMAN, M.D. ASSOCIATE PROFESSOR, UNIVERSITY OF MARYLAND SCHOOL OF MEDICINE DEPARTMENT OF PSYCHIATRY Feelings of depression and anxiety vs. diagnosis Everyone feels down sometimes
Depression and Anxiety ANN HACKMAN, M.D. ASSOCIATE PROFESSOR, UNIVERSITY OF MARYLAND SCHOOL OF MEDICINE DEPARTMENT OF PSYCHIATRY Feelings of depression and anxiety vs. diagnosis Everyone feels down sometimes
Geriatric Depression; Not a Normal Part of Growing Older. Cherie Warriner, LCSW
 1 Geriatric Depression; Not a Normal Part of Growing Older Cherie Warriner, LCSW What is Depression? While it is normal to feel sad or blue on occasion, these feelings are often transient. Depression is
1 Geriatric Depression; Not a Normal Part of Growing Older Cherie Warriner, LCSW What is Depression? While it is normal to feel sad or blue on occasion, these feelings are often transient. Depression is
Chapter 7 - Mood Disorders
 Chapter 7 - Mood Disorders I. DEPRESSION A. Description Symptoms: 5+ constant over 2 weeks - sadness/depressed mood - guilt/remorse/worthlessness - suicidal thoughts - anhedonia (lack of pleasure) - fatigue/lethargy
Chapter 7 - Mood Disorders I. DEPRESSION A. Description Symptoms: 5+ constant over 2 weeks - sadness/depressed mood - guilt/remorse/worthlessness - suicidal thoughts - anhedonia (lack of pleasure) - fatigue/lethargy
KEY MESSAGES. It is often under-recognised and 30-50% of MDD cases in primary care and medical settings are not detected.
 KEY MESSAGES Major depressive disorder (MDD) is a significant mental health problem that disrupts a person s mood and affects his psychosocial and occupational functioning. It is often under-recognised
KEY MESSAGES Major depressive disorder (MDD) is a significant mental health problem that disrupts a person s mood and affects his psychosocial and occupational functioning. It is often under-recognised
AN OVERVIEW OF ANXIETY
 AN OVERVIEW OF ANXIETY Fear and anxiety are a normal part of life. Normal anxiety keeps us alert. Intervention is required when fear and anxiety becomes overwhelming intruding on a persons quality of life.
AN OVERVIEW OF ANXIETY Fear and anxiety are a normal part of life. Normal anxiety keeps us alert. Intervention is required when fear and anxiety becomes overwhelming intruding on a persons quality of life.
Symptoms Duration Impact on functioning
 Dr. Lori Triano- Antidormi Dr. Jane Storrie OPA Annual Conference February 21, 2015 Symptoms Duration Impact on functioning Numbness, shock, disbelief, denial Sadness Apathy, lack of interest, enthusiasm
Dr. Lori Triano- Antidormi Dr. Jane Storrie OPA Annual Conference February 21, 2015 Symptoms Duration Impact on functioning Numbness, shock, disbelief, denial Sadness Apathy, lack of interest, enthusiasm
Depression major depressive disorder. Some terms: Major Depressive Disorder: Major Depressive Disorder:
 Depression major depressive disorder Oldest recognized disorder: melancholia It is a positive and active anguish, a sort of psychical neuralgia wholly unknown to normal life. - William James "I am now
Depression major depressive disorder Oldest recognized disorder: melancholia It is a positive and active anguish, a sort of psychical neuralgia wholly unknown to normal life. - William James "I am now
Drugs for Emotional and Mood Disorders Chapter 16
 Drugs for Emotional and Mood Disorders Chapter 16 NCLEX-RN Review Question 1 Choices Please note Question #1 at the end of Ch 16 pg 202 & Key pg 805 answer is #4 1. Psychomotor symptoms 2. Tachycardia,
Drugs for Emotional and Mood Disorders Chapter 16 NCLEX-RN Review Question 1 Choices Please note Question #1 at the end of Ch 16 pg 202 & Key pg 805 answer is #4 1. Psychomotor symptoms 2. Tachycardia,
Contemporary Psychiatric-Mental Health Nursing. Theories: Anxiety Disorders. Theories: Anxiety Disorders - continued
 Contemporary Psychiatric-Mental Health Nursing Chapter 18 Anxiety and Dissociative Disorders Theories: Anxiety Disorders Biological changes in the brain Noradrenergic system is sensitive to norepinephrine;
Contemporary Psychiatric-Mental Health Nursing Chapter 18 Anxiety and Dissociative Disorders Theories: Anxiety Disorders Biological changes in the brain Noradrenergic system is sensitive to norepinephrine;
Mood Disorders Workshop Dr Andrew Howie / Dr Tony Fernando Psychological Medicine Faculty of Medical and Health Sciences University of Auckland
 Mood Disorders Workshop 2010 Dr Andrew Howie / Dr Tony Fernando Psychological Medicine Faculty of Medical and Health Sciences University of Auckland Goals To learn about the clinical presentation of mood
Mood Disorders Workshop 2010 Dr Andrew Howie / Dr Tony Fernando Psychological Medicine Faculty of Medical and Health Sciences University of Auckland Goals To learn about the clinical presentation of mood
Emotional Adaptation after Cancer
 Emotional Adaptation after Cancer Jesse Fann, MD, MPH Department of Psychiatry & Behavioral Sci, UW Clinical Research Division, FHCRC Director, Psychiatry & Psychology Service, SCCA Outline Fear of Recurrence
Emotional Adaptation after Cancer Jesse Fann, MD, MPH Department of Psychiatry & Behavioral Sci, UW Clinical Research Division, FHCRC Director, Psychiatry & Psychology Service, SCCA Outline Fear of Recurrence
PSYCHOSOCIAL EVALUATION AND TREATMENT IN CHRONIC RESPIRATORY DISEASES
 PSYCHOSOCIAL EVALUATION AND TREATMENT IN CHRONIC RESPIRATORY DISEASES Prof Behcet Coşar M.D. Gazi Uni. School of Med. Psychiatry Dep Consultation Liaison Psychiatry Unit HUMAN Bio Psycho Social 11/6/2009
PSYCHOSOCIAL EVALUATION AND TREATMENT IN CHRONIC RESPIRATORY DISEASES Prof Behcet Coşar M.D. Gazi Uni. School of Med. Psychiatry Dep Consultation Liaison Psychiatry Unit HUMAN Bio Psycho Social 11/6/2009
Partners in Care Quick Reference Cards
 Partners in Care Quick Reference Cards Supported by the Agency for Healthcare Research and Quality MR-1198/8-AHRQ R This project was funded by the Agency for Healthcare Research and Quality (AHRQ), formerly
Partners in Care Quick Reference Cards Supported by the Agency for Healthcare Research and Quality MR-1198/8-AHRQ R This project was funded by the Agency for Healthcare Research and Quality (AHRQ), formerly
GOALS FOR THE PSCYHIATRY CLERKSHIP
 GOALS FOR THE PSCYHIATRY CLERKSHIP GOALS - The aim of the core psychiatry clerkship is to expose students to patients with mental illness and to prepare them to provide psychiatric care at a basic level.
GOALS FOR THE PSCYHIATRY CLERKSHIP GOALS - The aim of the core psychiatry clerkship is to expose students to patients with mental illness and to prepare them to provide psychiatric care at a basic level.
4. Definition, clinical diagnosis and diagnostic criteria
 4. Definition, clinical diagnosis and diagnostic criteria 4.1. Definition Major depression is a mood disorder consisting of a set of symptoms, which include a predominance of the affective type (pathological
4. Definition, clinical diagnosis and diagnostic criteria 4.1. Definition Major depression is a mood disorder consisting of a set of symptoms, which include a predominance of the affective type (pathological
Definition. Objectives. PTSD: The Unrecognized Symptom Jorge I. Ramirez, MD, FAAHPM Caroline Schauer, RN, BSN, CHPN
 PTSD: The Unrecognized Symptom Jorge I. Ramirez, MD, FAAHPM Caroline Schauer, RN, BSN, CHPN VISN 23 Hospice and Palliative Care Objectives Describe Post Traumatic Stress Disorder (PTSD) and the population
PTSD: The Unrecognized Symptom Jorge I. Ramirez, MD, FAAHPM Caroline Schauer, RN, BSN, CHPN VISN 23 Hospice and Palliative Care Objectives Describe Post Traumatic Stress Disorder (PTSD) and the population
Primary Care: Referring to Psychiatry
 Primary Care: Referring to Psychiatry Carol Capitano, PhD, APRN-BC Assistant Professor, Clinical Educator University of New Mexico College of Nursing University of New Mexico Psychiatric Center Objectives
Primary Care: Referring to Psychiatry Carol Capitano, PhD, APRN-BC Assistant Professor, Clinical Educator University of New Mexico College of Nursing University of New Mexico Psychiatric Center Objectives
Bipolar and Affective Disorders. Harleen Johal
 + Bipolar and Affective Disorders Harleen Johal hkj1g11@soton.ac.uk + Affective (mood) disorders n Depression n Bipolar disorder n Anxiety n Treatment + Depression: Definition n Pervasiveand persistent
+ Bipolar and Affective Disorders Harleen Johal hkj1g11@soton.ac.uk + Affective (mood) disorders n Depression n Bipolar disorder n Anxiety n Treatment + Depression: Definition n Pervasiveand persistent
Affective Disorders.
 Affective Disorders http://www.bristol.ac.uk/medicalschool/hippocrates/psychethics/ Affective Disorders Depression Mania / Hypomania Bipolar mood disorder Recurrent depression Persistent mood disorders
Affective Disorders http://www.bristol.ac.uk/medicalschool/hippocrates/psychethics/ Affective Disorders Depression Mania / Hypomania Bipolar mood disorder Recurrent depression Persistent mood disorders
Depression, Anxiety, and the Adolescent Athlete: Introduction to Identification and Treatment
 Depression, Anxiety, and the Adolescent Athlete: Introduction to Identification and Treatment Jamie E. Pardini, PhD Sports Medicine and Concussion Specialists Banner University Medical Center-Phoenix University
Depression, Anxiety, and the Adolescent Athlete: Introduction to Identification and Treatment Jamie E. Pardini, PhD Sports Medicine and Concussion Specialists Banner University Medical Center-Phoenix University
depression and anxiety in later life clinical challenges and creative research
 2 nd Annual MARC Symposium Critical Themes in Ageing Melbourne, 10 th August 2018 depression and anxiety in later life clinical challenges and creative research Nicola T Lautenschlager, MD, FRANZCP Professor
2 nd Annual MARC Symposium Critical Themes in Ageing Melbourne, 10 th August 2018 depression and anxiety in later life clinical challenges and creative research Nicola T Lautenschlager, MD, FRANZCP Professor
Contemporary Psychiatric-Mental Health Nursing Third Edition. Introduction. Introduction 9/10/ % of US suffers from Mood Disorders
 Contemporary Psychiatric-Mental Health Nursing Third Edition CHAPTER 17 Mood Disorders Introduction 12% of US suffers from Mood Disorders MD are a group of psychiatric DO characterized by physical, emotional
Contemporary Psychiatric-Mental Health Nursing Third Edition CHAPTER 17 Mood Disorders Introduction 12% of US suffers from Mood Disorders MD are a group of psychiatric DO characterized by physical, emotional
Interprofessional Webinar Series
 Interprofessional Webinar Series Management of Depression and Anxiety in Advanced Illness E. Alessandra Strada, PhD, MSCP, FT Director of Integrative Medicine and Bereavement Services MJHS Institute for
Interprofessional Webinar Series Management of Depression and Anxiety in Advanced Illness E. Alessandra Strada, PhD, MSCP, FT Director of Integrative Medicine and Bereavement Services MJHS Institute for
Part 2: Pain and Symptom Management Depression
 Guidelines & Protocols Advisory Committee Part 2: Pain and Symptom Management Depression Effective Date: February 22, 2017 Key Recommendations Before diagnosing and treating major depressive disorder,
Guidelines & Protocols Advisory Committee Part 2: Pain and Symptom Management Depression Effective Date: February 22, 2017 Key Recommendations Before diagnosing and treating major depressive disorder,
9/24/2012. Amer M Burhan, MBChB, FRCP(C)
") Depression and Dementia Amer M Burhan MBChB, FRCPC Head of CAMH Memory Clinic, Toronto Geriatric Neuropsychiatrist Assistant Prof Psychiatry at U of T Objectives Discuss the prevalence and impact of depression
Depression and Dementia Amer M Burhan MBChB, FRCPC Head of CAMH Memory Clinic, Toronto Geriatric Neuropsychiatrist Assistant Prof Psychiatry at U of T Objectives Discuss the prevalence and impact of depression
Some newer, investigational approaches to treating refractory major depression are being used.
 CREATED EXCLUSIVELY FOR FINANCIAL PROFESSIONALS Rx FOR SUCCESS Depression and Anxiety Disorders Mood and anxiety disorders are common, and the mortality risk is due primarily to suicide, cardiovascular
CREATED EXCLUSIVELY FOR FINANCIAL PROFESSIONALS Rx FOR SUCCESS Depression and Anxiety Disorders Mood and anxiety disorders are common, and the mortality risk is due primarily to suicide, cardiovascular
controls past MDD current MDD
 인제대학교서울백병원김원 * decreased appetite * decreased sleep * psychomotor agitaion * poor concentraion * psychomotor retardation * anhedonia depressed mood * low energy * guilt suicidal ideation * < 0.05 * total
인제대학교서울백병원김원 * decreased appetite * decreased sleep * psychomotor agitaion * poor concentraion * psychomotor retardation * anhedonia depressed mood * low energy * guilt suicidal ideation * < 0.05 * total
When is a Psychological Disorder a Disability? Dr. Leigh Ann Ford, PhD, HSP Licensed Psychologist ABVE 2017 Annual Conference. Goals for presentation
 When is a Psychological Disorder a Disability? Dr. Leigh Ann Ford, PhD, HSP Licensed Psychologist ABVE 2017 Annual Conference Goals for presentation *To review DSM-V criteria for some of the most frequently
When is a Psychological Disorder a Disability? Dr. Leigh Ann Ford, PhD, HSP Licensed Psychologist ABVE 2017 Annual Conference Goals for presentation *To review DSM-V criteria for some of the most frequently
INDIVIDUALS ARE COPING ALL THE TIME.
 Coping Strategies INDIVIDUALS ARE COPING ALL THE TIME. COPING (CONTENDING) Coping: Is the behavior that protects us from becoming psychologically and physiologically disorganized. Usually incorporates
Coping Strategies INDIVIDUALS ARE COPING ALL THE TIME. COPING (CONTENDING) Coping: Is the behavior that protects us from becoming psychologically and physiologically disorganized. Usually incorporates
Jonathan Haverkampf BIPOLAR DISORDR BIPOLAR DISORDER. Dr. Jonathan Haverkampf, M.D.
 BIPOLAR DISORDER Dr., M.D. Abstract - Bipolar disorder is a condition affecting an individual s affective states (mood). The different flavors of bipolar disorder have in common that there are alterations
BIPOLAR DISORDER Dr., M.D. Abstract - Bipolar disorder is a condition affecting an individual s affective states (mood). The different flavors of bipolar disorder have in common that there are alterations
DEMOGRAPHICS. Old Age for DD. Dual Diagnosis: Mental Illness & Developmental Disabilities. Peggy A. Szwabo, Ph.D. 314/647/4488
 Dual Diagnosis: Mental Illness & Developmental Disabilities Peggy A. Szwabo, Ph.D. 314/647/4488 pszwabo@sbcglobal.net DEMOGRAPHICS 10-15% of DD are 65+ 40-70% mental disorder 40% not in formal delivery
Dual Diagnosis: Mental Illness & Developmental Disabilities Peggy A. Szwabo, Ph.D. 314/647/4488 pszwabo@sbcglobal.net DEMOGRAPHICS 10-15% of DD are 65+ 40-70% mental disorder 40% not in formal delivery
VA/DoD Clinical Practice Guideline for Management of Post Traumatic Stress. Core Module
 VA/DoD Clinical Practice Guideline for Management of Post Traumatic Stress Core Module Module A Acute Stress Continue Treatment for ASD Treatment for ACUTE Stress Disorder Module B PTSD Continue Treatment
VA/DoD Clinical Practice Guideline for Management of Post Traumatic Stress Core Module Module A Acute Stress Continue Treatment for ASD Treatment for ACUTE Stress Disorder Module B PTSD Continue Treatment
Chapter 2 Lecture. Health: The Basics Tenth Edition. Promoting and Preserving Your Psychological Health
 Chapter 2 Lecture Health: The Basics Tenth Edition Promoting and Preserving Your Psychological Health OBJECTIVES Define each of the four components of psychological health, and identify the basic traits
Chapter 2 Lecture Health: The Basics Tenth Edition Promoting and Preserving Your Psychological Health OBJECTIVES Define each of the four components of psychological health, and identify the basic traits
Clinical Education Initiative INTRODUCTION TO HIV PSYCHIATRY. Speaker: Hansel Arroyo, MD
 Clinical Education Initiative Support@ceitraining.org INTRODUCTION TO HIV PSYCHIATRY Speaker: Hansel Arroyo, MD 3/1/2017 Introduction to HIV Psychiatry [video transcript] 00:00:07 - So we're gonna be talking
Clinical Education Initiative Support@ceitraining.org INTRODUCTION TO HIV PSYCHIATRY Speaker: Hansel Arroyo, MD 3/1/2017 Introduction to HIV Psychiatry [video transcript] 00:00:07 - So we're gonna be talking
Mental Health Rotation Educational Goals & Objectives
 Mental Health Rotation Educational Goals & Objectives Mental illness is prevalent in the general population and is commonly seen and treated in the office of the primary care provider. Educational experiences
Mental Health Rotation Educational Goals & Objectives Mental illness is prevalent in the general population and is commonly seen and treated in the office of the primary care provider. Educational experiences
Depression among Older Adults. Prevalence & Intervention Strategies
 Depression among Older Adults Prevalence & Intervention Strategies Definition Depression is a complex syndrome complex characterized by mood disturbance plus variety of cognitive, psychological, and vegetative
Depression among Older Adults Prevalence & Intervention Strategies Definition Depression is a complex syndrome complex characterized by mood disturbance plus variety of cognitive, psychological, and vegetative
A new Anatomy of Melancholy: rethinking depression and resilience
 A new Anatomy of Melancholy: rethinking depression and resilience Prof Declan McLoughlin Dept of Psychiatry & Trinity College Institute of Neuroscience Trinity College Dublin St Patrick s University Hospital
A new Anatomy of Melancholy: rethinking depression and resilience Prof Declan McLoughlin Dept of Psychiatry & Trinity College Institute of Neuroscience Trinity College Dublin St Patrick s University Hospital
Introduction into Psychiatric Disorders. Dr Jon Spear- Psychiatrist
 Introduction into Psychiatric Disorders Dr Jon Spear- Psychiatrist Content Stress Major depressive disorder Adjustment disorder Generalised anxiety disorder Post traumatic stress disorder Borderline personality
Introduction into Psychiatric Disorders Dr Jon Spear- Psychiatrist Content Stress Major depressive disorder Adjustment disorder Generalised anxiety disorder Post traumatic stress disorder Borderline personality
MATCP When the Severity of Symptoms Interferes with Progress
 MATCP 2017 When the Severity of Symptoms Interferes with Progress 1 Overview Stages of Change, or Readiness for Change Changing Behavior Medication Adherence Disruptive Behaviors Level of Care Tools including
MATCP 2017 When the Severity of Symptoms Interferes with Progress 1 Overview Stages of Change, or Readiness for Change Changing Behavior Medication Adherence Disruptive Behaviors Level of Care Tools including
Depression. Content. Depression is common. Depression Facts. Depression kills. Depression attacks young people
 Content Depression Dr. Anna Lam Associate Consultant Department of Psychiatry, Queen Mary Hospital Honorary Clinical Assistant Professor Li Ka Shing Faculty of Medicine, The University of Hong Kong 1.
Content Depression Dr. Anna Lam Associate Consultant Department of Psychiatry, Queen Mary Hospital Honorary Clinical Assistant Professor Li Ka Shing Faculty of Medicine, The University of Hong Kong 1.
Psychosocial Problems In Reproductive Health Of Elders
 Psychosocial Problems In Reproductive Health Of Elders Dr. Sonia Oveisi Maternity and Child Health Assistant Professor of Qazvin University of Medical Science 6/2/2014 1 Goals 1. Definition 2. Epidemiology
Psychosocial Problems In Reproductive Health Of Elders Dr. Sonia Oveisi Maternity and Child Health Assistant Professor of Qazvin University of Medical Science 6/2/2014 1 Goals 1. Definition 2. Epidemiology
Pharmaceutical Interventions. Collaborative Model of Mental Health Care for Older Iowans Des Moines May 18, 2007
 Pharmaceutical Interventions Collaborative Model of Mental Health Care for Older Iowans Des Moines May 18, 2007 Outline Overview Overview of initial workup and decisions in elderly depressed individual
Pharmaceutical Interventions Collaborative Model of Mental Health Care for Older Iowans Des Moines May 18, 2007 Outline Overview Overview of initial workup and decisions in elderly depressed individual
Chapter 20 Psychosocial Nursing of the Physically Ill Client Psychosocial Assessment Interactive process that involves gathering data and evaluating
 Chapter 20 Psychosocial Nursing of the Physically Ill Client Psychosocial Assessment Interactive process that involves gathering data and evaluating the past and current level of functioning of the client
Chapter 20 Psychosocial Nursing of the Physically Ill Client Psychosocial Assessment Interactive process that involves gathering data and evaluating the past and current level of functioning of the client
Depression. There are several forms of depression (depressive disorders). Major depressive disorder and dysthymic disorder are the most common.
. Major depressive disorder and dysthymic disorder are the most common.") Depression Depression is a state of low mood and aversion to activity that can affect a person's thoughts, behavior, feelings and sense of well-being. People with depressed mood can feel sad, anxious,
Depression Depression is a state of low mood and aversion to activity that can affect a person's thoughts, behavior, feelings and sense of well-being. People with depressed mood can feel sad, anxious,
A Comparison between Anxious-Depressive Disorders of Stroke and Multiple Sclerosis Patients, Evaluated with Specific Twin Scales
 A Comparison between Anxious-Depressive Disorders of Stroke and Multiple Sclerosis Patients, Evaluated with Specific Twin Scales The Post Stroke Depression Rating Scale The examiner must choose for each
A Comparison between Anxious-Depressive Disorders of Stroke and Multiple Sclerosis Patients, Evaluated with Specific Twin Scales The Post Stroke Depression Rating Scale The examiner must choose for each
Brief Notes on the Mental Health of Children and Adolescents
 Brief Notes on the Mental Health of Children and Adolescents The future of our country depends on the mental health and strength of our young people. However, many children have mental health problems
Brief Notes on the Mental Health of Children and Adolescents The future of our country depends on the mental health and strength of our young people. However, many children have mental health problems
MENTAL HEALTH DISEASE CLASSIFICATIONS
 MENTAL HEALTH DISEASE CLASSIFICATIONS DIAGNOSIS OF MENTAL DISORDERS DSM-IV-TR Published by APA ( 2000 ) Multiaxial system 5 categories called axes Facilitate holistic assessment for care Is a great resource
MENTAL HEALTH DISEASE CLASSIFICATIONS DIAGNOSIS OF MENTAL DISORDERS DSM-IV-TR Published by APA ( 2000 ) Multiaxial system 5 categories called axes Facilitate holistic assessment for care Is a great resource
DIAGNOSTIC CRITERIA (ICD 10)
") DEPRESSION Depression is a major public health problem around the world Affects 1:5 older people living in the community Affects 2:5 older people living in care homes Various treatment options available,
DEPRESSION Depression is a major public health problem around the world Affects 1:5 older people living in the community Affects 2:5 older people living in care homes Various treatment options available,
Mental Health Counseling for mood, aging, and coping with life transitions and chronic illness.
 Mental Health Counseling for mood, aging, and coping with life transitions and chronic illness. Silver Linings for Seniors Silver Linings for Seniors, Inc. offers on-site confidential Mental Health Counseling
Mental Health Counseling for mood, aging, and coping with life transitions and chronic illness. Silver Linings for Seniors Silver Linings for Seniors, Inc. offers on-site confidential Mental Health Counseling
Reducing the Anxiety of Pediatric Anxiety Part 2: Treatment
 Reducing the Anxiety of Pediatric Anxiety Part 2: Treatment Lisa Lloyd Giles, MD Medical Director, Behavioral Consultation, Crisis, and Community Services Primary Children s Hospital Associate Professor,
Reducing the Anxiety of Pediatric Anxiety Part 2: Treatment Lisa Lloyd Giles, MD Medical Director, Behavioral Consultation, Crisis, and Community Services Primary Children s Hospital Associate Professor,
Chapter 6 Mood Disorders and Suicide An Overview of Mood Disorders
 Page 1 Extremes in Normal Mood Chapter 6 Mood Disorders and Suicide An Overview of Mood Disorders Nature of depression Nature of mania and hypomania Types of DSM-IV Depressive Disorders Major depressive
Page 1 Extremes in Normal Mood Chapter 6 Mood Disorders and Suicide An Overview of Mood Disorders Nature of depression Nature of mania and hypomania Types of DSM-IV Depressive Disorders Major depressive
Hospice and Palliative Medicine
 Hospice and Palliative Medicine Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the
Hospice and Palliative Medicine Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the
Recognizing Depression and Restoring Mood and Well- Being in the Older Patient
 Recognizing Depression and Restoring Mood and Well- Being in the Older Patient Andreea L. Seritan, MD UC Davis Mini Medical School February 22, 2014 Objectives Review late life depression symptoms Review
Recognizing Depression and Restoring Mood and Well- Being in the Older Patient Andreea L. Seritan, MD UC Davis Mini Medical School February 22, 2014 Objectives Review late life depression symptoms Review
 DEPRESSION Depression is a major public health problem around the world Affects 1:5 older people living in the community Affects 2:5 older people living in care homes Various treatment options available,
DEPRESSION Depression is a major public health problem around the world Affects 1:5 older people living in the community Affects 2:5 older people living in care homes Various treatment options available,
Mood, Emotions and MS
 Mood, Emotions and MS Catherine Condon Clinical Neuropsychologist Integrated Psychology Living Well with MS Living a full and meaning-filled life Social connection Valued activity Healthy exercise Healthy
Mood, Emotions and MS Catherine Condon Clinical Neuropsychologist Integrated Psychology Living Well with MS Living a full and meaning-filled life Social connection Valued activity Healthy exercise Healthy
Major Depression Major Depression
 Contemporary Psychiatric-Mental Health Nursing Third Edition CHAPTER 17 Mood Disorders Major Depression Major Depression Characterized by a change in several aspects of a person s life and emotional state
Contemporary Psychiatric-Mental Health Nursing Third Edition CHAPTER 17 Mood Disorders Major Depression Major Depression Characterized by a change in several aspects of a person s life and emotional state
Other significant mental health complaints
 Other significant mental health complaints 2 Session outline Introduction to other significant mental health complaints Assessment of other significant mental health complaints Management of other significant
Other significant mental health complaints 2 Session outline Introduction to other significant mental health complaints Assessment of other significant mental health complaints Management of other significant
Depression. Depression. What is it all about? Social and economic burden of depression
 Social and economic burden of depression Depression What is it all about? By Dr CHAN Kwok Ling Senior Medical Officer Kwai Chung Hospital 23.8.2005 1 Depression is common in the community Manic depressive
Social and economic burden of depression Depression What is it all about? By Dr CHAN Kwok Ling Senior Medical Officer Kwai Chung Hospital 23.8.2005 1 Depression is common in the community Manic depressive
GERIATRIC WORKFORCE ENHANCEMENT PROGRAM (GWEP) FACULTY DEVELOPMENT MASTERWORKS SERIES
 FACULTY DEVELOPMENT MASTERWORKS SERIES") UNIVERSITY OF SOUTH FLORIDA GERIATRIC WORKFORCE ENHANCEMENT PROGRAM (GWEP) FACULTY DEVELOPMENT MASTERWORKS SERIES Kathryn Hyer, PhD, MPP Principal Investigator h Providers of Continuing Education For additional
UNIVERSITY OF SOUTH FLORIDA GERIATRIC WORKFORCE ENHANCEMENT PROGRAM (GWEP) FACULTY DEVELOPMENT MASTERWORKS SERIES Kathryn Hyer, PhD, MPP Principal Investigator h Providers of Continuing Education For additional
HealthyPlace s Introductory Guide to Bipolar Disorder. By Natasha Tracy
 HealthyPlace s Introductory Guide to Bipolar Disorder By Natasha Tracy 1 Index Introduction Chapter One Bipolar Disorder Basics Chapter Two Bipolar Disorder Diagnosis Chapter Three Treatment of Bipolar
HealthyPlace s Introductory Guide to Bipolar Disorder By Natasha Tracy 1 Index Introduction Chapter One Bipolar Disorder Basics Chapter Two Bipolar Disorder Diagnosis Chapter Three Treatment of Bipolar
The Suffering in patients with Metastatic Breast Cancer
 The Suffering in patients with Metastatic Breast Cancer Jayoung Ahn, RN, MSN, KOAPN ASAN Medical Center Contents I. Background II. The suffering experienced by women with MBC Associated symptoms of metastasis
The Suffering in patients with Metastatic Breast Cancer Jayoung Ahn, RN, MSN, KOAPN ASAN Medical Center Contents I. Background II. The suffering experienced by women with MBC Associated symptoms of metastasis
HEADS UP ON MENTAL HEALTH CONCERNS IN CHILDREN WITH DEVELOPMENTAL DISABILITIES. CORNELIO G. BANAAG, JR. M.D. Psychiatrist
 HEADS UP ON MENTAL HEALTH CONCERNS IN CHILDREN WITH DEVELOPMENTAL DISABILITIES CORNELIO G. BANAAG, JR. M.D. Psychiatrist MENTAL HEALTH WHO: Health is more than the absence of illness Emotional well being
HEADS UP ON MENTAL HEALTH CONCERNS IN CHILDREN WITH DEVELOPMENTAL DISABILITIES CORNELIO G. BANAAG, JR. M.D. Psychiatrist MENTAL HEALTH WHO: Health is more than the absence of illness Emotional well being
More Than Just Moody Blaise Aguirre, MD Child and Adolescent Psychiatrist McLean Hospital Assistant Professor of Psychiatry Harvard Medical School
 More Than Just Moody Blaise Aguirre, MD Child and Adolescent Psychiatrist McLean Hospital Assistant Professor of Psychiatry Harvard Medical School Keep in Mind In the U.S., approximately 10-15% of children/adolescents
More Than Just Moody Blaise Aguirre, MD Child and Adolescent Psychiatrist McLean Hospital Assistant Professor of Psychiatry Harvard Medical School Keep in Mind In the U.S., approximately 10-15% of children/adolescents
Depression in Persons with Developmental Disabilities. Helene Silverblatt MD UNM-TEASC Team December 7, 2007
 Depression in Persons with Developmental Disabilities Helene Silverblatt MD UNM-TEASC Team December 7, 2007 The Bottom Line Indeed, the professional who is in the habit of gathering nonverbal communications
Depression in Persons with Developmental Disabilities Helene Silverblatt MD UNM-TEASC Team December 7, 2007 The Bottom Line Indeed, the professional who is in the habit of gathering nonverbal communications
Psychiatric Treatment of the Concussed Athlete
 Psychiatric Treatment of the Concussed Athlete Eastern Athletic Trainers Association January 11 th, 2015 Alexander S. Strauss, MD Centra, P.C. E-MAIL: DRSTRAUSS@ALEXSTRAUSSMD.COM Evidence Mounts Linking
Psychiatric Treatment of the Concussed Athlete Eastern Athletic Trainers Association January 11 th, 2015 Alexander S. Strauss, MD Centra, P.C. E-MAIL: DRSTRAUSS@ALEXSTRAUSSMD.COM Evidence Mounts Linking
Lecture Outline Signs and symptoms in psychiatry Adjustment Disorders Other conditions that may be a focus of clinical attention
 V Codes & Adjustment Disorders Cornelia Pinnell, Ph.D. Argosy University/Phoenix Lecture Outline Signs and symptoms in psychiatry Adjustment Disorders Other conditions that may be a focus of clinical attention
V Codes & Adjustment Disorders Cornelia Pinnell, Ph.D. Argosy University/Phoenix Lecture Outline Signs and symptoms in psychiatry Adjustment Disorders Other conditions that may be a focus of clinical attention
Mood Disorders for Care Coordinators
 Mood Disorders for Care Coordinators David A Harrison, MD, PhD Assistant Professor, Dept of Psychiatry & Behavioral Sciences University of Washington School of Medicine Introduction 1 of 3 Mood disorders
Mood Disorders for Care Coordinators David A Harrison, MD, PhD Assistant Professor, Dept of Psychiatry & Behavioral Sciences University of Washington School of Medicine Introduction 1 of 3 Mood disorders
Depression & Anxiety in Adolescents
 Depression & Anxiety in Adolescents Objectives 1) Review diagnosis of anxiety and depression in adolescents 2) Provide overview of evidence-based treatment options 3) Increase provider comfort level with
Depression & Anxiety in Adolescents Objectives 1) Review diagnosis of anxiety and depression in adolescents 2) Provide overview of evidence-based treatment options 3) Increase provider comfort level with
How to Manage Anxiety
 How to Manage Anxiety Dr Tony Fernando Psychological Medicine University of Auckland Auckland District Health Board www.insomniaspecialist.co.nz www.calm.auckland.ac.nz Topics How to diagnose How to manage
How to Manage Anxiety Dr Tony Fernando Psychological Medicine University of Auckland Auckland District Health Board www.insomniaspecialist.co.nz www.calm.auckland.ac.nz Topics How to diagnose How to manage
Department of Public Welfare PSYCHOLOGICAL IMPAIRMENT REPORT
 Department of Public Welfare PSYCHOLOGICAL IMPAIRMENT REPORT The purpose of this report is to outline the information needed to make a disability determination. This is not a required format; however,
Department of Public Welfare PSYCHOLOGICAL IMPAIRMENT REPORT The purpose of this report is to outline the information needed to make a disability determination. This is not a required format; however,
Antidepressants. Dr Malek Zihlif
 Antidepressants The optimal use of antidepressant required a clear understanding of their mechanism of action, pharmacokinetics, potential drug interaction and the deferential diagnosis of psychiatric
Antidepressants The optimal use of antidepressant required a clear understanding of their mechanism of action, pharmacokinetics, potential drug interaction and the deferential diagnosis of psychiatric
AACN PCCN Review. Behavioral
 AACN PCCN Review Behavioral Presenter: Carol A. Rauen, RN, MS, CCNS, CCRN, PCCN, CEN Independent Clinical Nurse Specialist & Education Consultant rauen.carol104@gmail.com 0 Behavioral I. INTRODUCTION PCCN
AACN PCCN Review Behavioral Presenter: Carol A. Rauen, RN, MS, CCNS, CCRN, PCCN, CEN Independent Clinical Nurse Specialist & Education Consultant rauen.carol104@gmail.com 0 Behavioral I. INTRODUCTION PCCN
Parkinson s Disease Psychosis Treatment in Long-Term Care: Clinical and Operational Considerations
 Parkinson s Disease Psychosis Treatment in Long-Term Care: Clinical and Operational Considerations Pari Deshmukh MD Triple board-certified psychiatrist (Boards of psychiatry, addiction medicine, integrative
Parkinson s Disease Psychosis Treatment in Long-Term Care: Clinical and Operational Considerations Pari Deshmukh MD Triple board-certified psychiatrist (Boards of psychiatry, addiction medicine, integrative
Condensed Clinical Practice Guideline Treatment Of Patients With Schizophrenia
 Condensed Clinical Practice Guideline Treatment Of Patients With Schizophrenia I. Key Points a. Schizophrenia is a chronic illness affecting all aspects of person s life i. Treatment Planning Goals 1.
Condensed Clinical Practice Guideline Treatment Of Patients With Schizophrenia I. Key Points a. Schizophrenia is a chronic illness affecting all aspects of person s life i. Treatment Planning Goals 1.
Treating Childhood Depression in Pediatrics. Martha U. Barnard, Ph.D. University of Kansas Medical Center Pediatrics/Behavioral Sciences
 Treating Childhood Depression in Pediatrics Martha U. Barnard, Ph.D. University of Kansas Medical Center Pediatrics/Behavioral Sciences Objectives The learner will: Describe the signs and symptoms of childhood
Treating Childhood Depression in Pediatrics Martha U. Barnard, Ph.D. University of Kansas Medical Center Pediatrics/Behavioral Sciences Objectives The learner will: Describe the signs and symptoms of childhood
Dr Steve Moss BSc MSc Phd, Consultant Research Psychologist attached to the Estia Centre, Guys Hospital, London.
 INFORMATION SHEET Psychiatric disorders in people with learning disability Dr Steve Moss BSc MSc Phd, Consultant Research Psychologist attached to the Estia Centre, Guys Hospital, London. In the whole
INFORMATION SHEET Psychiatric disorders in people with learning disability Dr Steve Moss BSc MSc Phd, Consultant Research Psychologist attached to the Estia Centre, Guys Hospital, London. In the whole
Mental illness A Broad Overview. Dr H Pathmanandam March 2017
 Mental illness A Broad Overview Dr H Pathmanandam March 2017 Introduction Mental disorders are common in primary and secondary care Many are not recognised and not treated Some receive unnecessary or inappropriate
Mental illness A Broad Overview Dr H Pathmanandam March 2017 Introduction Mental disorders are common in primary and secondary care Many are not recognised and not treated Some receive unnecessary or inappropriate
Addressing Difficult Behaviors in Dementia
 Addressing Difficult Behaviors in Dementia GEORGE SCHOEPHOERSTER, MD GERIATRICIAN GENEVIVE/CENTRACARE CLINIC Objectives By the end of the session, you will be able to: 1) Explain the role of pain management
Addressing Difficult Behaviors in Dementia GEORGE SCHOEPHOERSTER, MD GERIATRICIAN GENEVIVE/CENTRACARE CLINIC Objectives By the end of the session, you will be able to: 1) Explain the role of pain management
Understanding Psychiatry & Mental Illness
 Understanding Psychiatry & Steve Ellen Mental Illness MB, BS. M.Med. MD. FRANZCP Head, Consultation, Liaison & Emergency Psychiatry, Alfred Health. Associate Professor, Monash Alfred Psychiatry Research
Understanding Psychiatry & Steve Ellen Mental Illness MB, BS. M.Med. MD. FRANZCP Head, Consultation, Liaison & Emergency Psychiatry, Alfred Health. Associate Professor, Monash Alfred Psychiatry Research