DIAGNOSTIC CRITERIA (ICD 10)
|
|
|
- Catherine Austin
- 5 years ago
- Views:
Transcription
1
2 DEPRESSION Depression is a major public health problem around the world Affects 1:5 older people living in the community Affects 2:5 older people living in care homes Various treatment options available, irrespective of age Morbidity and mortality increased with age as more vulnerable to consequences of self neglect Placebo effect can be significant
3 AETIOLOGY BIOPSYCHOSOCIAL FACTORS INVOLVED Painful events; past depression; family history; physical illness; medication; alcohol SOME PARTICULAR STRESSORS AS YOU AGE: RETIREMENT HAVING LESS MONEY HEALTH PROBLEMS LOSS OF PARTNER OR FRIENDS SOCIAL ISOLATION
4 IMPORTANT TO. Not dismiss depression as part of normal ageing or as understandable in context of life events Make sure that what you think is depression is not actually apathy secondary to subcortical damage or hypoactive delirium Not attribute all symptoms to depression without checking for physical health issues first comprehensive blood screen required (FBC, U&E, LFTS, TFTS, glucose, calcium,, B12 and folate, possibly Vitamin D) Check alcohol and substance abuse history (including prescribed medication)
5 DIAGNOSTIC CRITERIA (ICD 10) At least 2 weeks of sustained low mood (varying little from day to day and unresponsive to circumstances), loss of interest or enjoyment and reduced energy Reduced concentration Reduced self esteem and confidence Ideas of guilt and unworthiness Pessimistic views of the future Ideas of acts of self harm or suicide Disturbed sleep Decreased appetite
6 HOW BAD? MILD 2 of the above symptoms MODERATE At least 3 and of a level that leaves considerable difficulty in continuing with social, work or domestic activities SEVERE Over 4 of the above and individual is unable to continue with activities except to a limited extent
7 PARTICULAR PROBLEMS FOR OLDER PEOPLE Physical symptoms and depression Important to exclude physical illnesses that can cause similar symptoms thyroid problems, arthritis, heart disease, respiratory difficulties Long-term illness Depression can cause increased distress about health issues even where these are stable repeated phone calls. Confusion and memory problems Depression, worry and anxiety can all affect memory and make confusion more apparent (even on validated testing) A new sense of loneliness Living alone does not automatically cause depression, but feeling lonely for no obvious reason may be a sign of depression
8 HOW MIGHT IT PRESENT IN OLDER ADULTS? Older people tend to think more about physical illness, rather than mental disorder, so may present with repeated calls to GP, emergency services, family and resist explanations that there is nothing physically wrong.
9 CASE PRESENTATION - 67 year old retired shop assistant - c/o problems with memory and concentration - 6/12 h/o rapid decline in memory from normal baseline, together with change in personality (more apathetic and disinterested) - More irritable - Appetite reduced, sleep disturbed (EMW) - Denies feeling depressed but says he can t concentrate very well although this improves as the day goes on - Well orientated to time and place
10 HOW TO DISTINGUISH DEPRESSION FROM DEMENTIA Depression and AD can be hard to distinguish because of overlapping signs and symptoms 1 Neuropsychological deficits can be present in both but will improve with treatment of depression! Overlapping signs can include 1-3 Apathy Disturbance in concentration Loss of interest Social withdrawal Self-neglect Irritability Anxiety
11 DEPRESSION VS DEMENTIA Depression - Relatively acute onset Low mood ( + psychomotor retardation in some) Biological symptoms Diurnal variation in cognitive impairment Past or family psychiatric history
12 TREATMENT NICE GUIDELINES FOR MANAGEMENT OF DEPRESSION IN PRIMARY CARE Depends on severity of condition 20% of completed suicides occur in the elderly If the individual has severe depression, is suicidal or psychotic REFER TO SPECIALIST MENTAL HEALTH SERVICES
13 IF MILD.. Psychological, social and self-help Consider specific needs e.g. social care, bereavement counselling, social care Encourage the individual to talk about thoughts and feelings Consider referral for counselling/voluntary sector support Self-help material/information leaflets Encourage a structured day Encourage a balanced diet Reduce alcohol intake Consider problem solving/solutions focused interventions Exercise HOWEVER COCHRANE CONCLUSIONS no strong support for psychotherapeutic treatments in the management of depression in older people
14 IF MODERATE (OR MILD WITH PAST HISTORY OF DEPRESSION) Psychological/social and self help strategies as before Antidepressant trial for at least 8 weeks If a drug has worked before, usually first choice (but not TCA unless nothing else has worked before) SSRIs are standard first choice Mirtazapine if very agitated, poor sleep, poor appetite symptom profile Start at ½ dose for 2 weeks, then increase Review at 8 weeks.
15 AT 8 WEEK REVIEW Partial remission or deterioration Increase dose if partial response (within BNF limits) If no response, consider second line treatment Review diagnosis Review comorbidity Review suicidal ideation REFER TO CMHT Review presence of psychosis REFER TO CMHT Review again after another 8 weeks
16 AT 16 WEEK REVIEW If symptoms still present (after trial of 2 drug and 1 nondrug treatment) Consider if physical cause present Medication e.g. BZDP, opiates, betablockers Compliance check Alcohol useage 10% of first episode depression in older age due to cerebrovascular disease vascular depression If depression still present, refer to CMHT
17 DRUGS OF CHOICE SSRI Sertraline: start 25mg mane, increase to 50mg mane, can then increase in stages to mg daily if tolerated Citalopram : start 10mg mane, increase to 20mg mane (watch QTc) Mirtazapine Start 15mg nocte, increase to 30mg nocte and can go to 45mg nocte if tolerated
18 WATCH OUT FOR Hyponatraemia particularly SSRIs but mirtazapine too QTc prolongation citalopram Nausea and GI disturbance SSRI Increase in agitation - SSRI Excess drowsiness impaired mobility mirtazapine Altered FBC mirtazapine check if infections GI bleeds SSRIs (protect with PPI) esp if on NSAID, CEI, steroids Increased bleeding time - SSRI
19 SECOND LINE TREATMENT Change class of antidepressant e.g. from SSRI to mirtazapine Venlafaxine XL start at 37.5mg od, then increase to 75mg XL od, up to 150mg XL od (measure BP if going above this) Escitalopram Augmentation regimes E.g. SSRI or VLF +mirtazapine
20 ARE ALL ANTIDEPRESSANTS THE SAME? Effective Mirtazapine Escitalopram Venlafaxine sertraline Less effective Duloxetine Fluoxetine Fluvoxamine paroxetine BEST FOR ELDERLY
21 IF REMISSION ACHIEVED Continue at the dose that achieved remission (no reduction to a maintenance dose), for 1 episode depression : 6-9 months 2 episodes depression : 2-3 years 3 episodes or more : no reason to ever stop! HIGH RECURRENCE RATES IN FIRST EPISODE LATE LIFE DEPRESSION (61% RECURRENCE ONCE AD withdrawn)
22 STRATEGIES FOR ACHIEVING REMISSION 1. PROLONG TREATMENT (for at least 12 weeks) If no or stalled response at 12 weeks, change 2. INCREASE DOSE Push to max tolerated dose 3. SWITCH ANTIDEPRESSANTS Risky, can lose all benefits, only switch if no clear benefit on first treatment 4. COMBINE ANTIDEPRESSANTS Lots of potential combinations 5. AUGMENTATION STRATEGIES Aripiprazole; lithium; thyroxine; anticonvulsants
23 VASCULAR DEPRESSION 10% first episode depression in older adults due to cerebrovascular disease Clinical picture : Prominent apathy; anergia; anhedonia with slowness of processing Cause = subcortical vascular disease If this diagnosis is being considered, CT scan and if positive or clinically suspiciou investigate and treat as if they had TIA or other end stage cerebrovascular disease
24 POOR PROGNOSTIC INDICATORS Medical illness burden Comorbid (persistent ) anxiety Cognitive impairment White matter hyperintensities
25 ANXIETY Lots of types of anxiety disorder GAD most frequent anxiety disorder encountered in primary care Panic disorder Specific phobia PTSD OCD Dissociative states etc.etc
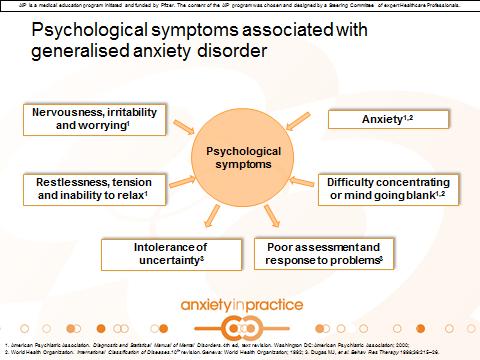
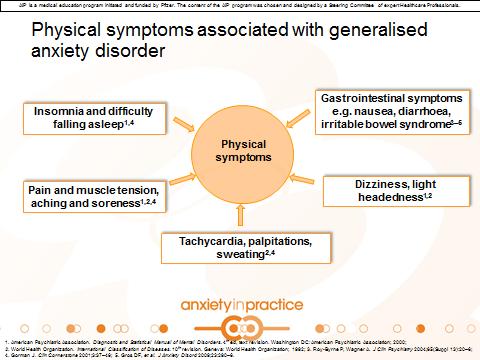
26 GENERALISED ANXIETY DISORDER ICD definition Anxiety, generalised and persistent, but not restricted to, or even strongly predominating in, any particular environmental circumstances i.e. free-floating Dominant symptoms variable but include Persistent nervousness Trembling Muscular tension Sweating Lightheadedness Palpitations Dizziness Epigastric discomfort
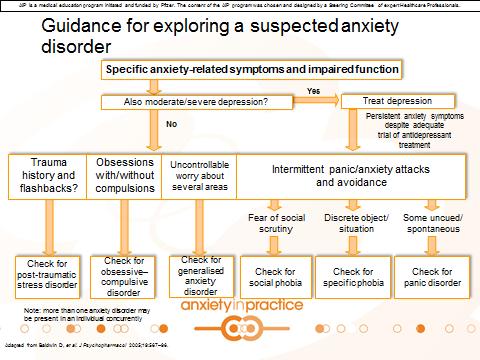
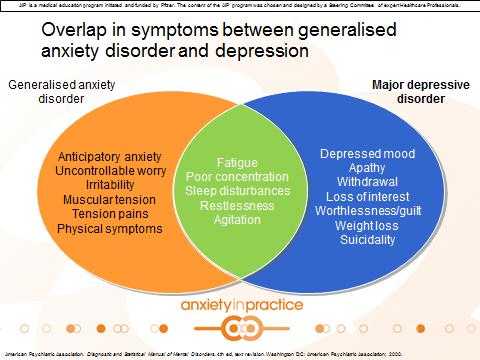
27 DIFFERENTIATING FEATURES GAD Excessive anxiety and apprehensive expectation Free-floating anxiety Many physical complaints No phobic avoidance behaviour No severe depressed mood or anhedonia No frequent panic attacks Panic disorder Spontaneous recurrent anxiety attacks occur at any time an in any setting Social phobia Avoidance, not only fear, of social or performance situations in a public setting
28 DIFFERENTIATING FEATURES Agoraphobia Fear of being trapped in a situation (which can be nonsocial) from which escape is difficult or embarassing, clearly avoidant phobic behaviour Specific phobia Unreasonable fear and avoidance of a specific object or situation PTSD A traumatic event is persistently re-experienced Major depressive disorder Primary symptoms are severe depressed mood and marked anhedonia
29 GAD Most frequent anxiety disorder in primary care (primary care prevalence 8.5%) Source of major morbidity Anxiety disorders associated with high use of primary care resources (reported as main reason for contact by 4.6% of people going to see primary care) High rate of disorders co-occurring with GAD
30 GAD Associated with high levels of impairment in daily function, even when compared to individuals with other chronic and disabling medical conditions In older adults increases carer burden and could lead to placement Lifetime prevalence increases with age Women almost twice as likely to have GAD than men
31 PRIMARY CARE BURDEN On average, people with GAD (with or without co-occurring major depressive disorder) have 2x as many visits to primary care as those with neither GAD or MDD Patients with GAD +/- MDD visit their primary care physician more than once every month Associated with low rates of remission (38% of patients of all ages achieved full remission over 5 years (least likely in those with poor family relationships or personality disorder) Ref: Yonkers et al
32 DIAGNOSTIC CHALLENGES Under-recognised and undertreated in approximately 2/3 of patients with the disorder Low rate of diagnosis due to : Lack of physician knowledge Lack of time Competing demands during consultation Prioritisation of physical symptoms/conditions Co-occurrence with other anxiety and depressive disorders e.g hypochondriasis, MDD 90% of patients with GAD have at least one other psychiatric diagnosis Waxing and waning of symptoms Poor description of symptoms by patient Patients typically have their symptoms for 5-10 years before appropriate diagnosis and treatment
33 ANXIETY IS OFTEN NOT THE PRIMARY COMPLAINT IN GAD (only 13% of patients with GAD presented to primary care c/o anxiety) Physical symptoms Pain Depression Insomnia
34 WHAT TO CONSIDER Does the patient suffer from normal, appropriate anxiety or excessive worry? Is there an underlying organic illness full examination and history to exclude this? Is there a co-occurring psychiatric condition? Any use of medication/substances known to cause anxiety? Multiple visits to primary care with MUS?
35
36 RESOURCES British Association of Psychopharmacology evidence based guidelines on management of anxiety disorders GAD 7 : screening tool for GAD Patient health questionnaire 2 : screens for depressed mood and anhedonia Hospital Anxiety and Depression scale : screens for anxiety and depression BUT CONFIRM DIAGNOSIS USING ICD 10 CRITERIA
37 HOW DOES GAD PRESENT? Most people present with a combination of symptoms Behavioural (reassurance seeking), psychological (nervousness, poor concentration, restlessness, muscular tension, poor problem assessment and response) and physical (sleep disturbance, IBS symptoms) Worry out of proportion to the likelihood of the event excessive and non-specific, intolerance of uncertainty Symptoms can: Wax and wane Vary between different individuals Become more persistent with age
38
39
40 COMORBID CONDITIONS 88% of individuals with GAD report co-occurring anxiety disorders, mood disorders or substance misuse disorders Social phobia/simple phobia 34% Panic disorder 22% Agoraphobia 21% Substance misuse 33%
41
42 TREATMENT AIMS Reduce psychiatric and physical symptoms Improve quality of life Achieve remission Reduce disability Prevent relapse or recurrence of co-occuring disorders Longer duration of untreated illness may be associated with worse clinical course GAD independently predicts increased risk of hypertension and coronary heart disease
43 MANAGEMENT Appropriate diagnosis essential Treatment aims Reduce psychiatric and physical symptoms Improve quality of life Reduce disability Prevent relapse or recurrence of co-occurring disorders Achieve remission
44 PRIMARY CARE MANAGEMENT PLAN Use a stepped approach (after discussion with patient and considering patient preference) Step 1 : recognition and diagnosis Step 2 : treat in primary care Step 3 : review and consider alternative treatments Step 4: review and refer to specialist mental health services (if no relief of, or an increase in, their symptoms after two trial interventions i.e. psychotherapy, self help, pharmacotherapy) Step 5 : step up to secondary mental health services
45 NON-PHARMACOLOGICAL TREATMENTS Provide information about GAD Relaxation Slowed diaphragmatic breathing, meditation, visual imagery Cognitive techniques e.g. CBT Learn to manage difficult situations and stop anxiety spiralling out of control Behavioural techniques Build up level of activity and improve self confidence
46
47
48
49 PHARMACOLOGICAL TREATMENTS
50
51 AVAILABLE PHARMACOLOGICAL TREATMENT FOR ANXIETY DISORDERS SSRI FIRST LINE Start at half starting dose for depression Titrate upwards as tolerated May see initial worsening of anxiety Response usually seen in 6 weeks (older may take longer) Treat for at least 1 year Effective treatment of GAD may present development of MDD Fluoxetine most effective, but sertraline best tolerated
52 PREGABALIN Calcium channel blocker Licensed for GAD In older adults, start low e.g. 25mg bd and increase as tolerated Don t stop abruptly as may precipitate rebound anxiety and seizures Rapid onset of effect Few drug interactions Side effects Dizziness, sedation, weight gain, discontinuation symptoms, dry mouth, increased risk of falls
53 BENZODIAZEPINES Rapid symptomatic relief BUT lots of problems in elderly Risk of dependence esp with short acting agents e.g. lorazepam Long acting agents e.g. diazepam, build up and cause ataxia and mobility problems, increase risk of falls Significant withdrawal difficulties Only recommended for short term use (4 weeks) whilst alternative treatments are started If anxiety is so severe as to consider long term use, then consider this carefully a small number of patients with very severe disabling anxiety may require long term prescription Cognitive and psychomotor impairment Not licensed for treatment of GAD in UK
54 OTHER DRUGS Mirtazapine Venlafaxine Duloxetine Beta blockers Atypical antipsychotics e.g. quetiapine, aripiprazole
55 TREATMENT FOLLOW UP Review within 2 weeks of starting treatment and every couple of weeks thereafter (may take longer than 12 weeks to see response in older adults) Has there been an improvement after 12 weeks? YES continue NO reassess and try another intervention IF NO RESPONSE AFTER AT LEAST SECOND INTERVENTION TRIED REFER TO CMHT
56 TREATMENT DURATION GAD Tends to wax and wane Reassess patient weekly during first few weeks to assess drug performance, early discontinuation associated with higher relapse rates After remission, continue treatment for at least 1 year in order to reduce risk of relapse Treatment resistance may indicate organic anxiety e.g. secondary to cerebrovascular damage to limbic system
57 PARTICULAR CONCERNS Co occurring disorders Medical Psychiatric : ssri may be effective in GAD and MDD Suicidality Potential risk factor when GAD coexists with MDD Start an antidepressant, avoid use of BZDP Insomnia Reported by 2/3 patients with GAD Discuss lifestyle choices sleep hygiene, diet, exercise Some antidepressants may help with sleep more than others e.g. mirtazapine better than SSRI Subtance abuse Patients with GAD may self medicate with alcohol or other substances
 DEPRESSION Depression is a major public health problem around the world Affects 1:5 older people living in the community Affects 2:5 older people living in care homes Various treatment options available,
DEPRESSION Depression is a major public health problem around the world Affects 1:5 older people living in the community Affects 2:5 older people living in care homes Various treatment options available,
Guidelines MANAGEMENT OF MAJOR DEPRESSIVE DISORDER (MDD)
") MANAGEMENT OF MAJOR DEPRESSIVE DISORDER (MDD) Guidelines CH Lim, B Baizury, on behalf of Development Group Clinical Practice Guidelines Management of Major Depressive Disorder A. Introduction Major depressive
MANAGEMENT OF MAJOR DEPRESSIVE DISORDER (MDD) Guidelines CH Lim, B Baizury, on behalf of Development Group Clinical Practice Guidelines Management of Major Depressive Disorder A. Introduction Major depressive
KEY MESSAGES. It is often under-recognised and 30-50% of MDD cases in primary care and medical settings are not detected.
 KEY MESSAGES Major depressive disorder (MDD) is a significant mental health problem that disrupts a person s mood and affects his psychosocial and occupational functioning. It is often under-recognised
KEY MESSAGES Major depressive disorder (MDD) is a significant mental health problem that disrupts a person s mood and affects his psychosocial and occupational functioning. It is often under-recognised
Depression in Late Life
 Depression in Late Life Robert Madan MD FRCPC Geriatric Psychiatrist Key Learnings Robert Madan MD FRCPC Key Learnings By the end of the session, participants will be able to List the symptoms of depression
Depression in Late Life Robert Madan MD FRCPC Geriatric Psychiatrist Key Learnings Robert Madan MD FRCPC Key Learnings By the end of the session, participants will be able to List the symptoms of depression
Appendix 4B - Guidance for the use of Pharmacological Agents for the Treatment of Depression in Adults (18 years and over)
") Appendix 4B - Guidance for the use of Pharmacological Agents for the Treatment of Depression in Adults (18 years and over) Introduction / Background Treatment comes after diagnosis Diagnosis is based on
Appendix 4B - Guidance for the use of Pharmacological Agents for the Treatment of Depression in Adults (18 years and over) Introduction / Background Treatment comes after diagnosis Diagnosis is based on
A Basic Approach to Mood and Anxiety Disorders in the Elderly
 A Basic Approach to Mood and Anxiety Disorders in the Elderly November 1 2013 Sarah Colman MD FRCPC Clinical Fellow, Geriatric Psychiatry Mount Sinai Hospital, University of Toronto Disclosure No conflict
A Basic Approach to Mood and Anxiety Disorders in the Elderly November 1 2013 Sarah Colman MD FRCPC Clinical Fellow, Geriatric Psychiatry Mount Sinai Hospital, University of Toronto Disclosure No conflict
Pharmacological Treatment of Anxiety & Depressive Disorders
 Pharmacological Treatment of Anxiety & Depressive Disorders Dr Gary Jackson (MB BCh FRCPsych) Consultant Psychiatrist The Priory Hospital Chelmsford Wellesley Hospital Southend-on-Sea Medical Secretary:
Pharmacological Treatment of Anxiety & Depressive Disorders Dr Gary Jackson (MB BCh FRCPsych) Consultant Psychiatrist The Priory Hospital Chelmsford Wellesley Hospital Southend-on-Sea Medical Secretary:
Medication for Anxiety and Depression. PJ Cowen Department of Psychiatry, University of Oxford
 Medication for Anxiety and Depression PJ Cowen Department of Psychiatry, University of Oxford Topics Medication for anxiety disorders Medication for first line depression treatment Medication for resistant
Medication for Anxiety and Depression PJ Cowen Department of Psychiatry, University of Oxford Topics Medication for anxiety disorders Medication for first line depression treatment Medication for resistant
Reducing the Anxiety of Pediatric Anxiety Part 2: Treatment
 Reducing the Anxiety of Pediatric Anxiety Part 2: Treatment Lisa Lloyd Giles, MD Medical Director, Behavioral Consultation, Crisis, and Community Services Primary Children s Hospital Associate Professor,
Reducing the Anxiety of Pediatric Anxiety Part 2: Treatment Lisa Lloyd Giles, MD Medical Director, Behavioral Consultation, Crisis, and Community Services Primary Children s Hospital Associate Professor,
Anxiety Disorders. Dr Simon Christopherson Dr Alison Macrae
 Anxiety Disorders Dr Simon Christopherson Dr Alison Macrae 1 What is anxiety? Universal fight or flight experience Nerves / fearfulness can boost performance Worries keep you alert & prevent you missing
Anxiety Disorders Dr Simon Christopherson Dr Alison Macrae 1 What is anxiety? Universal fight or flight experience Nerves / fearfulness can boost performance Worries keep you alert & prevent you missing
How to Manage Anxiety
 How to Manage Anxiety Dr Tony Fernando Psychological Medicine University of Auckland Auckland District Health Board www.insomniaspecialist.co.nz www.calm.auckland.ac.nz Topics How to diagnose How to manage
How to Manage Anxiety Dr Tony Fernando Psychological Medicine University of Auckland Auckland District Health Board www.insomniaspecialist.co.nz www.calm.auckland.ac.nz Topics How to diagnose How to manage
Treatment of Anxiety (without benzos)
") Treatment of Anxiety (without benzos) Alison C. Lynch MD MS Clinical Professor Departments of Psychiatry and Family Medicine University of Iowa Health Care None Disclosures Overview/objectives Review common
Treatment of Anxiety (without benzos) Alison C. Lynch MD MS Clinical Professor Departments of Psychiatry and Family Medicine University of Iowa Health Care None Disclosures Overview/objectives Review common
Mental illness A Broad Overview. Dr H Pathmanandam March 2017
 Mental illness A Broad Overview Dr H Pathmanandam March 2017 Introduction Mental disorders are common in primary and secondary care Many are not recognised and not treated Some receive unnecessary or inappropriate
Mental illness A Broad Overview Dr H Pathmanandam March 2017 Introduction Mental disorders are common in primary and secondary care Many are not recognised and not treated Some receive unnecessary or inappropriate
SCREENING FOR COMMON MENTAL DISORDERS DEPRESSIVE AND ANXIETY DISORDERS SUBSTANCE USE DISORDERS
 SCREENING FOR COMMON MENTAL DISORDERS DEPRESSIVE AND ANXIETY DISORDERS SUBSTANCE USE DISORDERS COMMON MENTAL DISORDERS Depressive Disorders Anxiety Disorders Substance use disorders CMD in HIV Twice as
SCREENING FOR COMMON MENTAL DISORDERS DEPRESSIVE AND ANXIETY DISORDERS SUBSTANCE USE DISORDERS COMMON MENTAL DISORDERS Depressive Disorders Anxiety Disorders Substance use disorders CMD in HIV Twice as
Anxiety Disorders: First aid and when to refer on
 Anxiety Disorders: First aid and when to refer on Presenter: Dr Roger Singh, Consultant Psychiatrist, ABT service, Hillingdon Educational resources from NICE, 2011 NICE clinical guideline 113 What is anxiety?
Anxiety Disorders: First aid and when to refer on Presenter: Dr Roger Singh, Consultant Psychiatrist, ABT service, Hillingdon Educational resources from NICE, 2011 NICE clinical guideline 113 What is anxiety?
Depression & Anxiety in Adolescents
 Depression & Anxiety in Adolescents Objectives 1) Review diagnosis of anxiety and depression in adolescents 2) Provide overview of evidence-based treatment options 3) Increase provider comfort level with
Depression & Anxiety in Adolescents Objectives 1) Review diagnosis of anxiety and depression in adolescents 2) Provide overview of evidence-based treatment options 3) Increase provider comfort level with
Bipolar and Affective Disorders. Harleen Johal
 + Bipolar and Affective Disorders Harleen Johal hkj1g11@soton.ac.uk + Affective (mood) disorders n Depression n Bipolar disorder n Anxiety n Treatment + Depression: Definition n Pervasiveand persistent
+ Bipolar and Affective Disorders Harleen Johal hkj1g11@soton.ac.uk + Affective (mood) disorders n Depression n Bipolar disorder n Anxiety n Treatment + Depression: Definition n Pervasiveand persistent
Mental Health Pathway
 Mental Health Pathway Triggers for Mental Health Pathway Information for professionals Consider mainstream Mental Health Services (Green light Toolkit) Clinical Interface Protocol Clinical Assessment Information
Mental Health Pathway Triggers for Mental Health Pathway Information for professionals Consider mainstream Mental Health Services (Green light Toolkit) Clinical Interface Protocol Clinical Assessment Information
PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS. Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA
 CASE #1 PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA OBJECTIVES Epidemiology Presentation in older adults Assessment Treatment
CASE #1 PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA OBJECTIVES Epidemiology Presentation in older adults Assessment Treatment
Major Depressive Disorder (MDD) in Children under Age 6
 in Children under Age 6") in Children under Age 6 Level 0 Comprehensive assessment. Refer to Principles of Practice on page 6. Level 1 Psychotherapeutic intervention (e.g., dyadic therapy) for 6 to 9 months; assessment of parent/guardian
in Children under Age 6 Level 0 Comprehensive assessment. Refer to Principles of Practice on page 6. Level 1 Psychotherapeutic intervention (e.g., dyadic therapy) for 6 to 9 months; assessment of parent/guardian
WORKPLACE. Dr. ONG BENG KEAT Consultant Psychiatrist Psychological Medicine Clinic LohGuanLye Specialists Centre, Penang
 STRESS @ WORKPLACE Dr. ONG BENG KEAT Consultant Psychiatrist Psychological Medicine Clinic LohGuanLye Specialists Centre, Penang Outline Introduction: What is stress? Sources of stress Stress and productivity
STRESS @ WORKPLACE Dr. ONG BENG KEAT Consultant Psychiatrist Psychological Medicine Clinic LohGuanLye Specialists Centre, Penang Outline Introduction: What is stress? Sources of stress Stress and productivity
Adult Depression - Clinical Practice Guideline
 1 Adult Depression - Clinical Practice Guideline 05/2018 Diagnosis and Screening Diagnostic criteria o Please refer to Attachment A Screening o The United States Preventative Services Task Force (USPSTF)
1 Adult Depression - Clinical Practice Guideline 05/2018 Diagnosis and Screening Diagnostic criteria o Please refer to Attachment A Screening o The United States Preventative Services Task Force (USPSTF)
Antidepressant Treatment of Depression
 Antidepressant Treatment of Depression PLEASE REFER TO INTEGRATED CARE PATHWAY FOR INFORMATION RELATING TO THE OVERALL MANAGEMENT OF DEPRESSION SSRI s are first choice agents because they are as effective
Antidepressant Treatment of Depression PLEASE REFER TO INTEGRATED CARE PATHWAY FOR INFORMATION RELATING TO THE OVERALL MANAGEMENT OF DEPRESSION SSRI s are first choice agents because they are as effective
MEDICATION ALGORITHM FOR ANXIETY DISORDERS
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences MEDICATION ALGORITHM FOR ANXIETY DISORDERS RYAN KIMMEL, MD MEDICAL DIRECTOR HOSPITAL PSYCHIATRY UNIVERSITY OF WASHINGTON
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences MEDICATION ALGORITHM FOR ANXIETY DISORDERS RYAN KIMMEL, MD MEDICAL DIRECTOR HOSPITAL PSYCHIATRY UNIVERSITY OF WASHINGTON
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 Step 3: GAD with marked functional impairment or that has not improved after step 2 interventionsentions bring together everything NICE says on a topic in an interactive flowchart. are interactive and
Step 3: GAD with marked functional impairment or that has not improved after step 2 interventionsentions bring together everything NICE says on a topic in an interactive flowchart. are interactive and
Non-A, non-b=hcv; IFN/RBV; DSM-5/Ham-D, OLT; SSRI, P450
 James A. Bourgeois, O.D., M.D. Vice Chair Clinical Affairs and Director, CL Service University of California San Francisco Non-A, non-b=hcv; IFN/RBV; DSM-5/Ham-D, OLT; SSRI, P450 Localize! Sequence! 1
James A. Bourgeois, O.D., M.D. Vice Chair Clinical Affairs and Director, CL Service University of California San Francisco Non-A, non-b=hcv; IFN/RBV; DSM-5/Ham-D, OLT; SSRI, P450 Localize! Sequence! 1
PSYCHIATRIC MANAGEMENT IN PRIMARY CARE. Dr Fayyaz Khan MBBS, MRCPsych, MSc Consultant Psychiatrist (Locum) Mersey Care NHS Trust
 Mersey Care NHS Trust") PSYCHIATRIC MANAGEMENT IN PRIMARY CARE Dr Fayyaz Khan MBBS, MRCPsych, MSc Consultant Psychiatrist (Locum) Mersey Care NHS Trust Areas to cover Mood Disorders Anxiety Disorders Miscellaneous Conditions
PSYCHIATRIC MANAGEMENT IN PRIMARY CARE Dr Fayyaz Khan MBBS, MRCPsych, MSc Consultant Psychiatrist (Locum) Mersey Care NHS Trust Areas to cover Mood Disorders Anxiety Disorders Miscellaneous Conditions
Management Of Depression And Anxiety
 Management Of Depression And Anxiety CME Financial Disclosure Statement I, or an immediate family member including spouse/partner, have at present and/or have had within the last 12 months, or anticipate
Management Of Depression And Anxiety CME Financial Disclosure Statement I, or an immediate family member including spouse/partner, have at present and/or have had within the last 12 months, or anticipate
Doncaster Improving Access to Psychological Therapies (IAPT) Nurse Target September 2018 Dennis Convery
 Nurse Target September 2018 Dennis Convery") Doncaster Improving Access to Psychological Therapies (IAPT) Nurse Target September 2018 Dennis Convery Aims of the session To introduce the role and function of Doncaster IAPT (improving access to psychological
Doncaster Improving Access to Psychological Therapies (IAPT) Nurse Target September 2018 Dennis Convery Aims of the session To introduce the role and function of Doncaster IAPT (improving access to psychological
Document Title Pharmacological Management of Generalised Anxiety Disorder
 Document Title Pharmacological Management of Generalised Anxiety Disorder Document Description Document Type Policy Service Application Trust Wide Version 1.1 Policy Reference no. POL 201 Lead Author(s)
Document Title Pharmacological Management of Generalised Anxiety Disorder Document Description Document Type Policy Service Application Trust Wide Version 1.1 Policy Reference no. POL 201 Lead Author(s)
This initial discovery led to the creation of two classes of first generation antidepressants:
 Antidepressants - TCAs, MAOIs, SSRIs & SNRIs First generation antidepressants TCAs and MAOIs The discovery of antidepressants could be described as a lucky accident. During the 1950s, while carrying out
Antidepressants - TCAs, MAOIs, SSRIs & SNRIs First generation antidepressants TCAs and MAOIs The discovery of antidepressants could be described as a lucky accident. During the 1950s, while carrying out
Disclosure Information
 Disclosure Information I have no financial relationships to disclose. I will discuss the off label use of several depression and anxiety medications in pediatric population Pediatric Depression & Anxiety
Disclosure Information I have no financial relationships to disclose. I will discuss the off label use of several depression and anxiety medications in pediatric population Pediatric Depression & Anxiety
Antidepressant Medication Therapy in Primary Care July 25, 2013
 New York State Collaborative Care Initiative Antidepressant Medication Therapy in Primary Care July 25, 2013 http://uwaims.org Presenter Building on 25 years of Research and Practice in Integrated Mental
New York State Collaborative Care Initiative Antidepressant Medication Therapy in Primary Care July 25, 2013 http://uwaims.org Presenter Building on 25 years of Research and Practice in Integrated Mental
Presentation is Being Recorded
 Integrated Care for Depression & Anxiety Psychotropic Medication Management for Primary Care Providers Los Angeles County Department of Mental Health September 20, 2011 Presentation is Being Recorded Please
Integrated Care for Depression & Anxiety Psychotropic Medication Management for Primary Care Providers Los Angeles County Department of Mental Health September 20, 2011 Presentation is Being Recorded Please
Depression: selective serotonin reuptake inhibitors
 Depression: selective serotonin reuptake inhibitors Selective serotonin reuptake inhibitors (SSRIs) are considered first-line treatment for the majority of patients with depression. citalopram and fluoxetine
Depression: selective serotonin reuptake inhibitors Selective serotonin reuptake inhibitors (SSRIs) are considered first-line treatment for the majority of patients with depression. citalopram and fluoxetine
Pharmaceutical Interventions. Collaborative Model of Mental Health Care for Older Iowans Des Moines May 18, 2007
 Pharmaceutical Interventions Collaborative Model of Mental Health Care for Older Iowans Des Moines May 18, 2007 Outline Overview Overview of initial workup and decisions in elderly depressed individual
Pharmaceutical Interventions Collaborative Model of Mental Health Care for Older Iowans Des Moines May 18, 2007 Outline Overview Overview of initial workup and decisions in elderly depressed individual
Depression in adults: treatment and management
 1 2 3 4 Depression in adults: treatment and management 5 6 7 8 Appendix V3: recommendations that have been deleted of changed from 2009 guideline Depression in adults: Appendix V3 1 of 22 1 Recommendations
1 2 3 4 Depression in adults: treatment and management 5 6 7 8 Appendix V3: recommendations that have been deleted of changed from 2009 guideline Depression in adults: Appendix V3 1 of 22 1 Recommendations
Recognizing Depression and Restoring Mood and Well- Being in the Older Patient
 Recognizing Depression and Restoring Mood and Well- Being in the Older Patient Andreea L. Seritan, MD UC Davis Mini Medical School February 22, 2014 Objectives Review late life depression symptoms Review
Recognizing Depression and Restoring Mood and Well- Being in the Older Patient Andreea L. Seritan, MD UC Davis Mini Medical School February 22, 2014 Objectives Review late life depression symptoms Review
Some newer, investigational approaches to treating refractory major depression are being used.
 CREATED EXCLUSIVELY FOR FINANCIAL PROFESSIONALS Rx FOR SUCCESS Depression and Anxiety Disorders Mood and anxiety disorders are common, and the mortality risk is due primarily to suicide, cardiovascular
CREATED EXCLUSIVELY FOR FINANCIAL PROFESSIONALS Rx FOR SUCCESS Depression and Anxiety Disorders Mood and anxiety disorders are common, and the mortality risk is due primarily to suicide, cardiovascular
Medication management of anxiety & depression. Dr Katie Simpson GP Mental health lead East Berks CCG
 Medication management of anxiety & depression Dr Katie impson GP Mental health lead East Berks CCG NICE guidelines for Anxiety tepped Care RIs and NRIs in Anxiety disorders RI ertraline Citalopram Fluoxetine
Medication management of anxiety & depression Dr Katie impson GP Mental health lead East Berks CCG NICE guidelines for Anxiety tepped Care RIs and NRIs in Anxiety disorders RI ertraline Citalopram Fluoxetine
ANXIETY: FAST FACTS AND SKILLS FOR THE PRIMARY CARE PHYSICIAN
 UW PACC Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences ANXIETY: FAST FACTS AND SKILLS FOR THE PRIMARY CARE PHYSICIAN RYAN KIMMEL, MD MEDICAL DIRECTOR HOSPITAL
UW PACC Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences ANXIETY: FAST FACTS AND SKILLS FOR THE PRIMARY CARE PHYSICIAN RYAN KIMMEL, MD MEDICAL DIRECTOR HOSPITAL
Guidance on the use of Antidepressants for the Treatment of Unipolar Depression and Anxiety Spectrum Disorders in adults (Version 3 October 2014)
") Guidance on the use of Antidepressants for the Treatment of Unipolar Depression and Anxiety Spectrum Disorders in adults (Version 3 October 2014) Date of Preparation: September 2014 Date for next full
Guidance on the use of Antidepressants for the Treatment of Unipolar Depression and Anxiety Spectrum Disorders in adults (Version 3 October 2014) Date of Preparation: September 2014 Date for next full
9/20/2011. Integrated Care for Depression & Anxiety: Psychotropic Medication Management for PCPs. Presentation is Being Recorded
 Integrated Care for Depression & Anxiety Psychotropic Medication Management for Primary Care Providers Los Angeles County Department of Mental Health September 20, 2011 Presentation is Being Recorded Please
Integrated Care for Depression & Anxiety Psychotropic Medication Management for Primary Care Providers Los Angeles County Department of Mental Health September 20, 2011 Presentation is Being Recorded Please
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Scope for Partial Update
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Scope for Partial Update 1 Guideline title Anxiety: management of generalised anxiety disorder in adults in primary, secondary and community care (update)
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Scope for Partial Update 1 Guideline title Anxiety: management of generalised anxiety disorder in adults in primary, secondary and community care (update)
Anxiety Disorders. Fear & Anxiety. Anxiety Disorder? 26/5/2014. J. H. Atkinson, M.D. Fear. Anxiety. An anxiety disorder is present when
 Anxiety s J. H. Atkinson, M.D. HIV Neurobehavioral Research Center University of California, San Diego Department of Psychiatry & Veterans Affairs Healthcare System, San Diego Materials courtesy of Dr.
Anxiety s J. H. Atkinson, M.D. HIV Neurobehavioral Research Center University of California, San Diego Department of Psychiatry & Veterans Affairs Healthcare System, San Diego Materials courtesy of Dr.
ANXIETY DISORDERS IN THE ELDERLY IMPACT OF LATE-LIFE ANXIETY CHANGES IN DSM-5 THE COSTS 6/4/2015 LATE-LIFE ANXIETY TOPICS TO BE COVERED
 LATE-LIFE ANXIETY TOPICS TO BE COVERED ANXIETY DISORDERS IN THE ELDERLY Dr. Lisa Talbert Classes of Anxiety Disorders Diagnosis Comorbidities Pharmacologic Management Psychological Management LATE LIFE
LATE-LIFE ANXIETY TOPICS TO BE COVERED ANXIETY DISORDERS IN THE ELDERLY Dr. Lisa Talbert Classes of Anxiety Disorders Diagnosis Comorbidities Pharmacologic Management Psychological Management LATE LIFE
GREATER MANCHESTER INTERFACE PRESCRIBING GROUP
 GREATER MANCHESTER INTERFACE PRESCRIBING GROUP On behalf of the GREATER MANCHESTER MEDICINES MANAGEMENT GROUP SHARED CARE GUIDELINE FOR THE PRESCRIBING OF SELECTIVE SEROTONIN REUPTAKE INHIBITORS (SSRIs)
GREATER MANCHESTER INTERFACE PRESCRIBING GROUP On behalf of the GREATER MANCHESTER MEDICINES MANAGEMENT GROUP SHARED CARE GUIDELINE FOR THE PRESCRIBING OF SELECTIVE SEROTONIN REUPTAKE INHIBITORS (SSRIs)
Treatment Options for Bipolar Disorder Contents
 Keeping Your Balance Treatment Options for Bipolar Disorder Contents Medication Treatment for Bipolar Disorder 2 Page Medication Record 5 Psychosocial Treatments for Bipolar Disorder 6 Module Summary 8
Keeping Your Balance Treatment Options for Bipolar Disorder Contents Medication Treatment for Bipolar Disorder 2 Page Medication Record 5 Psychosocial Treatments for Bipolar Disorder 6 Module Summary 8
Partners in Care Quick Reference Cards
 Partners in Care Quick Reference Cards Supported by the Agency for Healthcare Research and Quality MR-1198/8-AHRQ R This project was funded by the Agency for Healthcare Research and Quality (AHRQ), formerly
Partners in Care Quick Reference Cards Supported by the Agency for Healthcare Research and Quality MR-1198/8-AHRQ R This project was funded by the Agency for Healthcare Research and Quality (AHRQ), formerly
Depression Workshop 26 January 2007
 Depression Workshop 26 January 2007 Leslie G Walker Professor of Cancer Rehabilitation Donald M Sharp Senior Lecturer in Behavioural Oncology Mary B Walker Senior Clinical and Research Nurse Specialist
Depression Workshop 26 January 2007 Leslie G Walker Professor of Cancer Rehabilitation Donald M Sharp Senior Lecturer in Behavioural Oncology Mary B Walker Senior Clinical and Research Nurse Specialist
Anxiety Disorders.
 Anxiety Disorders Shamim Nejad, MD Medical Director, Psycho-Oncology Services Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@swedish.org Disclosures Neither I nor my spouse/partner
Anxiety Disorders Shamim Nejad, MD Medical Director, Psycho-Oncology Services Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@swedish.org Disclosures Neither I nor my spouse/partner
MOOD (AFFECTIVE) DISORDERS and ANXIETY DISORDERS
 DISORDERS and ANXIETY DISORDERS") MOOD (AFFECTIVE) DISORDERS and ANXIETY DISORDERS Shelley Klipp AS91 Spring 2010 TIP 42 Pages 226-231 and 369-379 DSM IV-TR APA 2000 Co-Occurring Substance Abuse and Mental Disorders by John Smith Types
MOOD (AFFECTIVE) DISORDERS and ANXIETY DISORDERS Shelley Klipp AS91 Spring 2010 TIP 42 Pages 226-231 and 369-379 DSM IV-TR APA 2000 Co-Occurring Substance Abuse and Mental Disorders by John Smith Types
Family Medicine Forum November 10, 2017 Montreal., Quebec. Jon Davine, CCFP, FRCP(C) Associate Professor, McMaster University
 Associate Professor, McMaster University") APPROACH TO DEPRESSION IN PRIMARY CARE Family Medicine Forum November 10, 2017 Montreal., Quebec. Jon Davine, CCFP, FRCP(C) Associate Professor, McMaster University DISCLOSURE Speaker/Presenter Disclosure
APPROACH TO DEPRESSION IN PRIMARY CARE Family Medicine Forum November 10, 2017 Montreal., Quebec. Jon Davine, CCFP, FRCP(C) Associate Professor, McMaster University DISCLOSURE Speaker/Presenter Disclosure
MANAGEMENT OF VISCERAL PAIN
 MANAGEMENT OF VISCERAL PAIN William D. Chey, MD, FACG Professor of Medicine University of Michigan 52 year old female with abdominal pain 5 year history of persistent right sided burning/sharp abdominal
MANAGEMENT OF VISCERAL PAIN William D. Chey, MD, FACG Professor of Medicine University of Michigan 52 year old female with abdominal pain 5 year history of persistent right sided burning/sharp abdominal
Depression and Anxiety. What is Depression? What is Depression? By Christopher Okiishi, MD Spring Not just being sad A syndrome of symptoms
 Depression and Anxiety By Christopher Okiishi, MD Spring 2016 What is Depression? Not just being sad A syndrome of symptoms Depressed mood Sleep disturbance Decreased interest in usual activities (anhedonia)
Depression and Anxiety By Christopher Okiishi, MD Spring 2016 What is Depression? Not just being sad A syndrome of symptoms Depressed mood Sleep disturbance Decreased interest in usual activities (anhedonia)
Psychiatry curbside: Answers to a primary care doctor s top mental health questions
 Psychiatry curbside: Answers to a primary care doctor s top mental health questions April 27, 2018 Laurel Ralston, DO Psychiatrist, Taussig Cancer Institute Objectives Review current diagnostic and prescribing
Psychiatry curbside: Answers to a primary care doctor s top mental health questions April 27, 2018 Laurel Ralston, DO Psychiatrist, Taussig Cancer Institute Objectives Review current diagnostic and prescribing
Short Clinical Guidelines: General Anxiety Disorder (GAD)
") Definition is one of the most prevalent psychiatric disorders seen in the primary care office and is characterized by excessive anxiety and worry about a number of events that cause clinically significant
Definition is one of the most prevalent psychiatric disorders seen in the primary care office and is characterized by excessive anxiety and worry about a number of events that cause clinically significant
Major Depressive Disorder (MDD) in Children under Age 6
 in Children under Age 6") in Children under Age 6 Level 0 Comprehensive assessment. Refer to Principles of Practice on page 5. Level 1 Psychotherapeutic intervention (e.g., dyadic therapy) for 6 to 9 months; assessment of parent/guardian
in Children under Age 6 Level 0 Comprehensive assessment. Refer to Principles of Practice on page 5. Level 1 Psychotherapeutic intervention (e.g., dyadic therapy) for 6 to 9 months; assessment of parent/guardian
Introduction to Drug Treatment
 Introduction to Drug Treatment LPT Gondar Mental Health Group www.le.ac.uk Introduction to Psychiatric Drugs Drugs and Neurotransmitters 5 Classes of Psychotropic medications Mechanism of action Clinical
Introduction to Drug Treatment LPT Gondar Mental Health Group www.le.ac.uk Introduction to Psychiatric Drugs Drugs and Neurotransmitters 5 Classes of Psychotropic medications Mechanism of action Clinical
depression and anxiety in later life clinical challenges and creative research
 2 nd Annual MARC Symposium Critical Themes in Ageing Melbourne, 10 th August 2018 depression and anxiety in later life clinical challenges and creative research Nicola T Lautenschlager, MD, FRANZCP Professor
2 nd Annual MARC Symposium Critical Themes in Ageing Melbourne, 10 th August 2018 depression and anxiety in later life clinical challenges and creative research Nicola T Lautenschlager, MD, FRANZCP Professor
ANXIETY DISORDERS IN DSM5
 ANXIETY DISORDERS IN DSM5 Dr Robin Lawrence robinlawrence@mac.com 117a & 96 Harley St 02074860506 PLAN FOR THIS EVENING Diagnostic Systems ICD10 & DSM5 compared A Philosophical Perspective Historic Perspective
ANXIETY DISORDERS IN DSM5 Dr Robin Lawrence robinlawrence@mac.com 117a & 96 Harley St 02074860506 PLAN FOR THIS EVENING Diagnostic Systems ICD10 & DSM5 compared A Philosophical Perspective Historic Perspective
Treating Anxiety Disorders. Adil Virani, BSc (Pharm), Pharm D, FCSHP
, Pharm D, FCSHP") Treating Anxiety Disorders Adil Virani, BSc (Pharm), Pharm D, FCSHP Outline! Michelle s Case! Types of anxiety disorders! Goals of therapy! Treatment options and guidelines! Pharmacological options! Benzodiazepines
Treating Anxiety Disorders Adil Virani, BSc (Pharm), Pharm D, FCSHP Outline! Michelle s Case! Types of anxiety disorders! Goals of therapy! Treatment options and guidelines! Pharmacological options! Benzodiazepines
A N I N T R O D U C T I O N T O S T R E S S, A N X I E T Y A N D D E P R E S S I O N F O R M A N A G E R S K A T H C H E E R
 A N I N T R O D U C T I O N T O S T R E S S, A N X I E T Y A N D D E P R E S S I O N F O R M A N A G E R S K A T H C H E E R Learning Outcomes Mental health facts and figures Greater understanding of stress,
A N I N T R O D U C T I O N T O S T R E S S, A N X I E T Y A N D D E P R E S S I O N F O R M A N A G E R S K A T H C H E E R Learning Outcomes Mental health facts and figures Greater understanding of stress,
Mood Disorders for Care Coordinators
 Mood Disorders for Care Coordinators David A Harrison, MD, PhD Assistant Professor, Dept of Psychiatry & Behavioral Sciences University of Washington School of Medicine Introduction 1 of 3 Mood disorders
Mood Disorders for Care Coordinators David A Harrison, MD, PhD Assistant Professor, Dept of Psychiatry & Behavioral Sciences University of Washington School of Medicine Introduction 1 of 3 Mood disorders
Panic disorder is a chronic and recurrent illness associated
 CLINICAL PRACTICE GUIDELINES Management of Anxiety Disorders. Panic Disorder, With or Without Agoraphobia Epidemiology Panic disorder is a chronic and recurrent illness associated with significant functional
CLINICAL PRACTICE GUIDELINES Management of Anxiety Disorders. Panic Disorder, With or Without Agoraphobia Epidemiology Panic disorder is a chronic and recurrent illness associated with significant functional
Medication Management. Dr Ajith Weeraman MBBS, MD (Psychiatry), FRANZCP Consultant Psychiatrist Epworth Clinic Camberwell 14 th March 2015
, FRANZCP Consultant Psychiatrist Epworth Clinic Camberwell 14 th March 2015") Medication Management Dr Ajith Weeraman MBBS, MD (Psychiatry), FRANZCP Consultant Psychiatrist Epworth Clinic Camberwell 14 th March 2015 1 Medication Management Objectives: 1. Principles of psycho-pharmacology
Medication Management Dr Ajith Weeraman MBBS, MD (Psychiatry), FRANZCP Consultant Psychiatrist Epworth Clinic Camberwell 14 th March 2015 1 Medication Management Objectives: 1. Principles of psycho-pharmacology
CHILD & ADOLESCENT PSYCHIATRY ALERTS, VOLUME XIV, 2012 INDEX
 A Adderall Counterfeit, 31 addiction, internet CBT, 55 ADHD Adjunctive Guanfacine, 11 Counterfeit Adderall, 31 Developmental Trajectory and Risk Factors, 5 Dopamine Transporter Alterations, 14 Extended-Release
A Adderall Counterfeit, 31 addiction, internet CBT, 55 ADHD Adjunctive Guanfacine, 11 Counterfeit Adderall, 31 Developmental Trajectory and Risk Factors, 5 Dopamine Transporter Alterations, 14 Extended-Release
Anxiety Pharmacology UNIVERSITY OF HAWAI I HILO PRE -NURSING PROGRAM
 Anxiety Pharmacology UNIVERSITY OF HAWAI I HILO PRE NURSING PROGRAM NURS 203 GENERAL PHARMACOLOGY DANITA NARCISO PHARM D Learning Objectives Understand the normal processing of fear vs fear processing
Anxiety Pharmacology UNIVERSITY OF HAWAI I HILO PRE NURSING PROGRAM NURS 203 GENERAL PHARMACOLOGY DANITA NARCISO PHARM D Learning Objectives Understand the normal processing of fear vs fear processing
Affective Disorders.
 Affective Disorders http://www.bristol.ac.uk/medicalschool/hippocrates/psychethics/ Affective Disorders Depression Mania / Hypomania Bipolar mood disorder Recurrent depression Persistent mood disorders
Affective Disorders http://www.bristol.ac.uk/medicalschool/hippocrates/psychethics/ Affective Disorders Depression Mania / Hypomania Bipolar mood disorder Recurrent depression Persistent mood disorders
Managing Anxiety Disorder in Primary Care
 Saturday General Session Managing Anxiety Disorder in Primary Care Chris Ticknor, MD Private Practice, Psychiatry Adjunct Professor of Psychiatry UT Health Science Center at San Antonio San Antonio, Texas
Saturday General Session Managing Anxiety Disorder in Primary Care Chris Ticknor, MD Private Practice, Psychiatry Adjunct Professor of Psychiatry UT Health Science Center at San Antonio San Antonio, Texas
Clinical Guideline / Formulary Document Pharmacy Department Medicines Management Services
 Clinical Guideline / Formulary Document Pharmacy Department Medicines Management Services ANXIETY DISORDERS This guideline covers a range of anxiety disorders, including generalised anxiety disorder, social
Clinical Guideline / Formulary Document Pharmacy Department Medicines Management Services ANXIETY DISORDERS This guideline covers a range of anxiety disorders, including generalised anxiety disorder, social
Understanding Psychiatry & Mental Illness
 Understanding Psychiatry & Steve Ellen Mental Illness MB, BS. M.Med. MD. FRANZCP Head, Consultation, Liaison & Emergency Psychiatry, Alfred Health. Associate Professor, Monash Alfred Psychiatry Research
Understanding Psychiatry & Steve Ellen Mental Illness MB, BS. M.Med. MD. FRANZCP Head, Consultation, Liaison & Emergency Psychiatry, Alfred Health. Associate Professor, Monash Alfred Psychiatry Research
Volume 4; Number 5 May 2010
 Volume 4; Number 5 May 2010 CLINICAL GUIDELINES FOR ANTIDEPRESSANT USE IN PRIMARY AND SECONDARY CARE Lincolnshire Partnership Foundation Trust in conjunction with Lincolnshire PACEF have recently updated
Volume 4; Number 5 May 2010 CLINICAL GUIDELINES FOR ANTIDEPRESSANT USE IN PRIMARY AND SECONDARY CARE Lincolnshire Partnership Foundation Trust in conjunction with Lincolnshire PACEF have recently updated
The legally binding text is the original French version TRANSPARENCY COMMITTEE. Opinion. 1 October 2008
 The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 1 October 2008 EFFEXOR SR 37.5 mg prolonged-release capsule B/30 (CIP: 346 563-3) EFFEXOR SR 75 mg prolonged-release
The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 1 October 2008 EFFEXOR SR 37.5 mg prolonged-release capsule B/30 (CIP: 346 563-3) EFFEXOR SR 75 mg prolonged-release
Cognitive enhancers PINCH ME. Anticholinergic burden BPSD. Agitation, Aggression and antipsychotics
 Cognitive enhancers PINCH ME Anticholinergic burden BPSD Agitation, Aggression and antipsychotics 2 types Cholinesterase inhibitors licensed for mild to moderate AD Donepezil Galantamine Rivastigmine also
Cognitive enhancers PINCH ME Anticholinergic burden BPSD Agitation, Aggression and antipsychotics 2 types Cholinesterase inhibitors licensed for mild to moderate AD Donepezil Galantamine Rivastigmine also
Guidance on the use of Antidepressants for the Treatment of Unipolar Depression and Anxiety Spectrum Disorders in adults (Version 4.
 Guidance on the use of Antidepressants for the Treatment of Unipolar Depression and Anxiety Spectrum Disorders in adults (Version 4.1 December 2018) Date of Preparation: January 2018 (with addition of
Guidance on the use of Antidepressants for the Treatment of Unipolar Depression and Anxiety Spectrum Disorders in adults (Version 4.1 December 2018) Date of Preparation: January 2018 (with addition of
Recommendation 1: Diagnosis of Generalized Anxiety Disorder (IΙΙ-2)
") Final GAD RECOMMENDATIONS & EVIDENCE Recommendation 1: Diagnosis of Generalized Anxiety Disorder (IΙΙ-2) It is recommended for general practitioners and other Primary Health Care doctors to consider the
Final GAD RECOMMENDATIONS & EVIDENCE Recommendation 1: Diagnosis of Generalized Anxiety Disorder (IΙΙ-2) It is recommended for general practitioners and other Primary Health Care doctors to consider the
Anxiety Disorders- OCD. Peter Giacobbe MD FRCPC L. Ravindran MD FRCPC
 Anxiety Disorders- OCD Peter Giacobbe MD FRCPC L. Ravindran MD FRCPC Anxiety Disorders - Epidemiology Anxiety disorders are the most common class of mental disorders Estimated lifetime prevalence rates
Anxiety Disorders- OCD Peter Giacobbe MD FRCPC L. Ravindran MD FRCPC Anxiety Disorders - Epidemiology Anxiety disorders are the most common class of mental disorders Estimated lifetime prevalence rates
Depression: management of depression in primary and secondary care
 Issue date: December 2004, with amendments April 2007 Quick reference guide (amended) Depression: management of depression in primary and secondary care Amendment of recommendations concerning venlafaxine:
Issue date: December 2004, with amendments April 2007 Quick reference guide (amended) Depression: management of depression in primary and secondary care Amendment of recommendations concerning venlafaxine:
Clinical guideline Published: 28 October 2009 nice.org.uk/guidance/cg90
 Depression in adults: recognition and management Clinical guideline Published: 28 October 2009 nice.org.uk/guidance/cg90 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Depression in adults: recognition and management Clinical guideline Published: 28 October 2009 nice.org.uk/guidance/cg90 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
IPAP PTSD Algorithm -- Addenda
 www.ipap.org/ptsd General Principles IPAP PTSD Algorithm -- Addenda I. Initial and repeated evaluations A. PTSD is common and often goes undiagnosed. Given the high prevalence of exposure to trauma (including
www.ipap.org/ptsd General Principles IPAP PTSD Algorithm -- Addenda I. Initial and repeated evaluations A. PTSD is common and often goes undiagnosed. Given the high prevalence of exposure to trauma (including
BRIEF SUMMARY CONTENT
 Page 1 of 17 Brief Summary GUIDELINE TITLE Depression. The treatment and management of depression in adults. BIBLIOGRAPHIC SOURCE(S) National Collaborating Centre for Mental Health. Depression. The treatment
Page 1 of 17 Brief Summary GUIDELINE TITLE Depression. The treatment and management of depression in adults. BIBLIOGRAPHIC SOURCE(S) National Collaborating Centre for Mental Health. Depression. The treatment
The pharmacological management of anxiety disorders
 Stephen Bleakley MRPharmS, MCMHP Review in association with The pharmacological management of anxiety disorders Progress in Neurology and Psychiatry is running a series of articles on the major psychiatric
Stephen Bleakley MRPharmS, MCMHP Review in association with The pharmacological management of anxiety disorders Progress in Neurology and Psychiatry is running a series of articles on the major psychiatric
WHEN AND HOW TO USE BENZODIAZEPINES IN TREATING ANXIETY: AM I WITHHOLDING TREATMENT IF I DON'T USE BENZODIAZEPINES?
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences WHEN AND HOW TO USE BENZODIAZEPINES IN TREATING ANXIETY: AM I WITHHOLDING TREATMENT IF I DON'T USE BENZODIAZEPINES?
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences WHEN AND HOW TO USE BENZODIAZEPINES IN TREATING ANXIETY: AM I WITHHOLDING TREATMENT IF I DON'T USE BENZODIAZEPINES?
DEMENTIA AND MEDICATION
 DEMENTIA AND MEDICATION Dr. Siobhan Ni Bhriain, MRCP, MRCPsych. Clinical Director, Tallaght and SJH MHS, Consultant Old Age Psychiatrist, Chair, DSIDC Steering Committee. SUMMARY OF TODAY S TALK Dementia-definition,
DEMENTIA AND MEDICATION Dr. Siobhan Ni Bhriain, MRCP, MRCPsych. Clinical Director, Tallaght and SJH MHS, Consultant Old Age Psychiatrist, Chair, DSIDC Steering Committee. SUMMARY OF TODAY S TALK Dementia-definition,
Anxiolytics and anxiety disorders. MUDr. Vítězslav Pálenský Dept. of Psychiatry, Masaryk University, Brno
 Anxiolytics and anxiety disorders MUDr. Vítězslav Pálenský Dept. of Psychiatry, Masaryk University, Brno Anxiety disorders 1. Panic disorders and agoraphobia 2. Specific phobia and social phobia 3. Obsessive
Anxiolytics and anxiety disorders MUDr. Vítězslav Pálenský Dept. of Psychiatry, Masaryk University, Brno Anxiety disorders 1. Panic disorders and agoraphobia 2. Specific phobia and social phobia 3. Obsessive
Guilt Suicidality. Depression Co-Occurs with Medical Illness The rate of major depression among those with medical illness is significant.
 1-800-PSYCH If you are obsessive-compulsive, dial 1 repeatedly If you are paranoid-delusional, dial 2 and wait, your call is being traced If you are schizophrenic, a little voice will tell you what number
1-800-PSYCH If you are obsessive-compulsive, dial 1 repeatedly If you are paranoid-delusional, dial 2 and wait, your call is being traced If you are schizophrenic, a little voice will tell you what number
Psycho-social care in critically ill patients. Panate Pukrittayakamee
 Psycho-social care in critically ill patients Panate Pukrittayakamee Outline Delirium Depression Anxiety Delirium Neurotransmission of delirium (Trzepacz PT, 2008) Diagnosis of delirium Disturbance in
Psycho-social care in critically ill patients Panate Pukrittayakamee Outline Delirium Depression Anxiety Delirium Neurotransmission of delirium (Trzepacz PT, 2008) Diagnosis of delirium Disturbance in
Guidelines for the Management of Behavioural and Psychological Symptoms of Dementia (BPSD) Summary document for Primary Care
 Summary document for Primary Care") Guidelines for the Management of Behavioural and Psychological Symptoms of Dementia (BPSD) Summary document for Primary Care Guidelines for the Management of Behavioural and Psychological Symptoms of Dementia
Guidelines for the Management of Behavioural and Psychological Symptoms of Dementia (BPSD) Summary document for Primary Care Guidelines for the Management of Behavioural and Psychological Symptoms of Dementia
Major Depression and Anxiety in Adolescents and Adults
 Major Depression and Anxiety in Adolescents and Adults Miggie Greenberg, M.D. Associate Professor of Psychiatry St. Louis University School of Medicine greenbml@slu.edu *NO DISCLOSURES* OBJECTIVES * Recognize
Major Depression and Anxiety in Adolescents and Adults Miggie Greenberg, M.D. Associate Professor of Psychiatry St. Louis University School of Medicine greenbml@slu.edu *NO DISCLOSURES* OBJECTIVES * Recognize
For: NEON Primary Healthcare Providers By: Michelle Romero, DO June 2013
 For: NEON Primary Healthcare Providers By: Michelle Romero, DO June 2013 This power point is only a guideline for recommendations in the treatment of psychiatric disorders. This is not comprehensive. Please
For: NEON Primary Healthcare Providers By: Michelle Romero, DO June 2013 This power point is only a guideline for recommendations in the treatment of psychiatric disorders. This is not comprehensive. Please
Mentoring Session: Participant Cases
 Handout for the Neuroscience Education Institute (NEI) online activity: Mentoring Session: Participant Cases The Case: 55-year-old patient with depression and anxiety The Question: What to do when antidepressants
Handout for the Neuroscience Education Institute (NEI) online activity: Mentoring Session: Participant Cases The Case: 55-year-old patient with depression and anxiety The Question: What to do when antidepressants
9/24/2012. Amer M Burhan, MBChB, FRCP(C)
") Depression and Dementia Amer M Burhan MBChB, FRCPC Head of CAMH Memory Clinic, Toronto Geriatric Neuropsychiatrist Assistant Prof Psychiatry at U of T Objectives Discuss the prevalence and impact of depression
Depression and Dementia Amer M Burhan MBChB, FRCPC Head of CAMH Memory Clinic, Toronto Geriatric Neuropsychiatrist Assistant Prof Psychiatry at U of T Objectives Discuss the prevalence and impact of depression
Treating Pain and Depression
 Treating Pain and Depression Without Getting Depressed Joseph P, Arpaia, MD www.jparpaiamd.com More than 50% of patients with chronic pain also have clinically significant depression. Interestingly that
Treating Pain and Depression Without Getting Depressed Joseph P, Arpaia, MD www.jparpaiamd.com More than 50% of patients with chronic pain also have clinically significant depression. Interestingly that
Contemporary Psychiatric-Mental Health Nursing Third Edition. Theories: Anxiety Disorders. Theories: Anxiety Disorders (cont'd) 10/2/2014
 10/2/2014") Contemporary Psychiatric-Mental Health Nursing Third Edition CHAPTER 18 Anxiety Disorders Theories: Anxiety Disorders Biological changes in the brain Neurotransmitters are associated with anxiety. low
Contemporary Psychiatric-Mental Health Nursing Third Edition CHAPTER 18 Anxiety Disorders Theories: Anxiety Disorders Biological changes in the brain Neurotransmitters are associated with anxiety. low
Objectives. Objectives. A practice review. 02-Nov-16 MAJOR DEPRESSIVE DISORDER: NEW DEVELOPMENTS AND PRACTICAL IMPLICATIONS
 MAJOR DEPRESSIVE DISORDER: NEW DEVELOPMENTS AND PRACTICAL IMPLICATIONS Jon-Paul Khoo What is treatment resistance really? Database review 328 consecutive non-remitted MDD patients referred for private
MAJOR DEPRESSIVE DISORDER: NEW DEVELOPMENTS AND PRACTICAL IMPLICATIONS Jon-Paul Khoo What is treatment resistance really? Database review 328 consecutive non-remitted MDD patients referred for private
Clinical guideline Published: 28 October 2009 nice.org.uk/guidance/cg90
 Depression in adults: recognition and management Clinical guideline Published: 28 October 2009 nice.org.uk/guidance/cg90 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Depression in adults: recognition and management Clinical guideline Published: 28 October 2009 nice.org.uk/guidance/cg90 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Children s Hospital Of Wisconsin
 Children s Hospital Of Wisconsin Co-Management Guidelines To support collaborative care, we have developed guidelines for our community providers to utilize when referring to, and managing patients with,
Children s Hospital Of Wisconsin Co-Management Guidelines To support collaborative care, we have developed guidelines for our community providers to utilize when referring to, and managing patients with,
Carra Powell, Pharm.D. Candidate What is Generalized Anxiety Disorder (GAD)? ü Signs and Symptoms. ü Causes. ü Statistics and Diagnosis
? ü Signs and Symptoms. ü Causes. ü Statistics and Diagnosis") Carra Powell, Pharm.D. Candidate 2019 Pharm Phacts: Generalized Anxiety Disorder December 2018 What is Generalized Anxiety Disorder (GAD)? While occasional anxiety is common before stressful events, it
Carra Powell, Pharm.D. Candidate 2019 Pharm Phacts: Generalized Anxiety Disorder December 2018 What is Generalized Anxiety Disorder (GAD)? While occasional anxiety is common before stressful events, it
FROM MEDICATION TO MINDFULNESS: NEW INSIGHTS INTO THE WORLD OF ANXIETY
 13 th Pearl Leibovitch Clinical Day November 18th, 2014 Mounir H. Samy, MD, FRCP(C) Associate Professor of Psychiatry McGill University (ret.) FROM MEDICATION TO MINDFULNESS: NEW INSIGHTS INTO THE WORLD
13 th Pearl Leibovitch Clinical Day November 18th, 2014 Mounir H. Samy, MD, FRCP(C) Associate Professor of Psychiatry McGill University (ret.) FROM MEDICATION TO MINDFULNESS: NEW INSIGHTS INTO THE WORLD