Preventing DSA-Mediated Renal Allograft Injury: Practical Strategies to Maintain Adequate Immunosuppression in Individual Patients
|
|
|
- Victor Laurence Rice
- 6 years ago
- Views:
Transcription

1 Preventing DSA-Mediated Renal Allograft Injury: Practical Strategies to Maintain Adequate Immunosuppression in Individual Patients This symposium is not part of the ATC official educational program and the session and content are not endorsed by ATC.
2 Disclosures Stanley C. Jordan, MD, FASN, has a financial interest/relationship or affiliation in the form of: Consultant for Genentech, Inc.; Hansa Medical; Novartis Pharmaceuticals Corporation; and Vitaeris Inc. Grant/Research Support from Genentech, Inc.; Hansa Medical; and Novartis Pharmaceuticals Corporation. Stanley C. Jordan, MD, FASN, does intend to discuss either non-fda-approved or investigational use with the following products/devices: therapeutic modalities to prevent/treat antibody-mediated rejection in kidney transplant recipients. Alexander Wiseman, MD, FAST, has a financial interest/relationship or affiliation in the form of: Grant/Research Support from Alexion Pharmaceuticals Inc.; Astellas; Bristol-Myers Squibb; Novartis Pharmaceuticals Corporation; Oxford Immunotec, Inc.; and Quark Pharmaceuticals, Inc. Advisory Board for Veloxis Pharmaceuticals. Alexander Wiseman, MD, FAST, does not intend to discuss any non-fda approved or investigational use of any products/devices. This CME activity is jointly provided by Medical Learning Institute, Inc. and PVI, PeerView Institute for Medical Education. This activity is supported by an educational grant from Astellas.




3 A Closer Look at DSAs as Mediators of Allograft Injury Stanley C. Jordan, MD, FASN Professor of Pediatrics & Medicine David Geffen School of Medicine at UCLA Director, Nephrology & Transplant Immunology Medical Director, Kidney Transplant Program Cedars-Sinai Medical Center Los Angeles, California

4 Patients With De Novo DSA Have Early (0-6 Months) TCMR With More Intense PTC Inflammation 1-3 TCMR PTC Score 2.0 de novo DSA 1.0 No DSA P <.05 Source: Peter Nickerson 1. Wiebe C et al. Am J Transplant. 2002;12: Gibson IW et al. Am J Transplant. 2008;8: Muczynski KA et al. J Am Soc Nephrol. 2003;14:


5 De Novo DSA Generation 1 APCs present alloantigens to T FH cells T FH cells activate Bn cells to become Bm and plasmablasts Plasmablasts evolve to plasma cells and generate DSAs 1. Archdeacon P et al. Am J Transplant. 2011;11: Source: Peter Nickerson
6 Etiology of Allograft Failure: Changing the Way We Think 1 Past Present Primarily a T-cell mediated process Insufficient control of the humoral arm of a recipient s immune system by current immunosuppressive regimens Progressively superseding the historical dogma that such allograft losses were caused by CNI toxicity and CAN 1. Loupy A et al. Nat Rev Nephrol. 2012;8:


7 Understanding the Causes of Kidney Transplant Failure: The Dominant Role of AMR and Nonadherence 1 Distribution of Histologic Diagnosis and Adherence Status Expressed as Probability Plots Conditional on Time of Biopsy Post Transplant Days Post Transplantation 1. Sellarés J et al. Am J Transplant. 2012;12:

8 Evidence for Antibody-Mediated Injury as a Major Determinant of Late Kidney Allograft Failure 1 Kaplan-Meier Analysis of the Impact of Primary or Secondary Local Diagnosis of CNI Nephrotoxicity on Kidney Allograft Survival After For-Cause Biopsy 1. Gaston RS et al. Transplantation. 2010;90:68-74.


9 Death-Censored Graft Survival by Clinical Phenotype and dndsa Status 1 1. Wiebe C et al. Am J Transplant. 2015;15:

10 dndsa Development: Impact of Adherence 1 1. Wiebe C et al. Am J Transplant. 2015;15:
11 Graft Survival in Type 1 and Type 2 AMR Patients and By IF/TA Scores (N = 80) 1 P =.047 Type 1 Type 2 P =.0007 (ci + ct <3) (ci + ct 3) 1. Haas M et al. Kidney Int. 2017;91:
 1 P =.")

12 Graft Survival in Type 1 and Type 2 AMR Patients and By DSA Scores (N = 80) 1 P =.047 Type 1 Type 2 P =.005 ΔRIS score <-2 ΔRIS score Haas M et al. Kidney Int. 2017;91:
13 dndsas Portend Poor Graft Outcomes Log rank P <.0001 Pre-existing DSA De novo DSA 0.0 Time Post AMR, Years 1. Aubert O et al. J Am Soc Nephrol Mar 2 [Epub ahead of print].

14 camr + TG Predicts Early Graft Failure 1 Kidney Graft Survival Following camr Diagnosis 1. Redfield RR et al. Hum Immunol. 2016;77:

15 Survival Probability Current Therapies Show Some Beneficial Effects 1 Kidney Graft Survival After camr Based on Treatment a P < Redfield RR et al. Hum Immunol. 2016;77:
16

17 Mechanisms of Donor-Specific Antibody-Mediated Endothelial Injury in Renal Allografts 1 1. Farkash EA, Colvin RB. Nat Rev Nephrol. 2012;8:

18 Model Linking TCMR, dndsa, and AMR With Graft Loss 1 Source: Peter Nickerson 1. Wiebe C et al. Am J Transplant. 2012;12:
 Rituximab (anti-cd20) Bortezomib")

19 De Novo DSA Treatment Options 1 tacrolimus/mmf ± prednisone IVIG ± pheresis (FDA ~SOC 1 ) Rituximab (anti-cd20) Bortezomib (proteosome inhibitor) Eculizumab (C5a inhibitor)/c1inh IdeS? IL-6/IL-6R inhibitors? 1. Archdeacon P et al. Am J Transplant. 2011;11:

20 1. Farkash EA, Colvin RB. Nat Rev Nephrol. 2012;8: Therapeutic Options for AMR 1
21 Targeting camr and TG: Can It Be Treated?
22 IL-6 and Antibody-Mediated Rejection Chronic DSA+ AMR and TG limit the function and longevity of renal allografts, accounting for the majority of graft losses in the United States This results in increased cost to the healthcare system, increased stresses on patients and their families, and reduced life expectancy on dialysis Currently, there are no good therapies for camr and TG Here, we explore the use of tocilizumab (anti-il-6r) in patients with resistant camr TG


23 Signaling Pathways for IL-6/IL-6R 1 Classical IL-6R Signaling IL-6R Trans-Signaling All other cell types 1. Adapted from: Yao X et al. Pharmacol Ther. 2014;141:

24 IL-6 Drives B-Cell Activation and Differentiation to Antibody-Producing Plasma Cells 1 IL-6 IL-6 + IL-21 Donor-specific antibodies CD4+ T FH CXCR5+ Bcl-6+ Naïve B cell IL-6 producing plasmablast Plasma cell IL-6 + IL-21 Germinal center 1. Jordan SC et al. Transplantation. 2017;101:32-44.
25 IL-6 Shapes T-Cell Immunity 1 Naïve T Cell TGF-β IL-12, IL-6 IL-4, IL-6 IL-1, IL-6 IL-21, IL-6 IL-6 T-Reg T H 1 T H 2 T H 17 T FH Fox P3 Stat-1, T-bet Stat-6 GATA-3 Stat-3, RORC Bcl6 TGF-β, IL-10 g-ifn IL-4 IL-5 & IL-13 IL-17A, IL-17F IL-21, IL-22 IL-21 Tolerance; prevents autoimmunity Autoimmunity; allograft rejection Allergy; atopic disease Cytotoxic T cells; autoimmunity; allograft rejection B cells plasma cells 1. Jordan SC et al. Transplantation. 2017;101:32-44.
26 Anti-IL-6/IL-6R Therapies Modify Inflammatory T-Cell Responses and Induce Regulatory T Cells 1 Naïve T Cell TGF-β IL-12, IL-6 IL-4, IL-6 IL-1, IL-6 IL-21, IL-6 T-Reg IL-6 T H 1 T H 2 T H 17 T FH Fox P3 Stat-1, T-bet Stat-6 GATA-3 Stat-3, RORC Bcl6 TGF-β, IL-10 g-ifn IL-4 IL-5 & IL-13 IL-17A, IL-17F IL-21, IL-22 IL-21 Tolerance; prevents autoimmunity Autoimmunity; allograft rejection Allergy; atopic disease Cytotoxic T cells; autoimmunity; allograft rejection B cells plasma cells 1. Jordan SC et al. Transplantation. 2017;101:32-44.
27






28 Anti IL-6R Inhibits Plasma Cell IgG Production and Anti HLA-A2 Antibody 1 Anti IL-6R Significantly Suppressed IgG+ Plasma Cells in the Bone Marrow and Spleens Demonstrated in an ELISpot Assay Detection of Anti HLA-A2 IgG Antibodies in Conditioned Media of BM Cell Cultures by Flow-Antibody Binding Assay Anti IL-6R Anti IL-6R BM Spleen Anti IL-6R a P <.01. b P < Kim I et al. Transplantation. 2014;98:
29




30 Tocilizumab Protocol for Desensitization Pre and Post Transplant 1 Schema for Desensitization With IVIG + TCZ Schema for Post Transplant a Days -30 and Vo AA et al. Transplantation. 2015;99:


31 DSA Patterns Before and After Transplantation 1 Course of Immunodominant DSAs Mean Immunodominant DSA Scores for TCZ-Treated and Transplanted Patients 1. Vo AA et al. Transplantation. 2015;99:
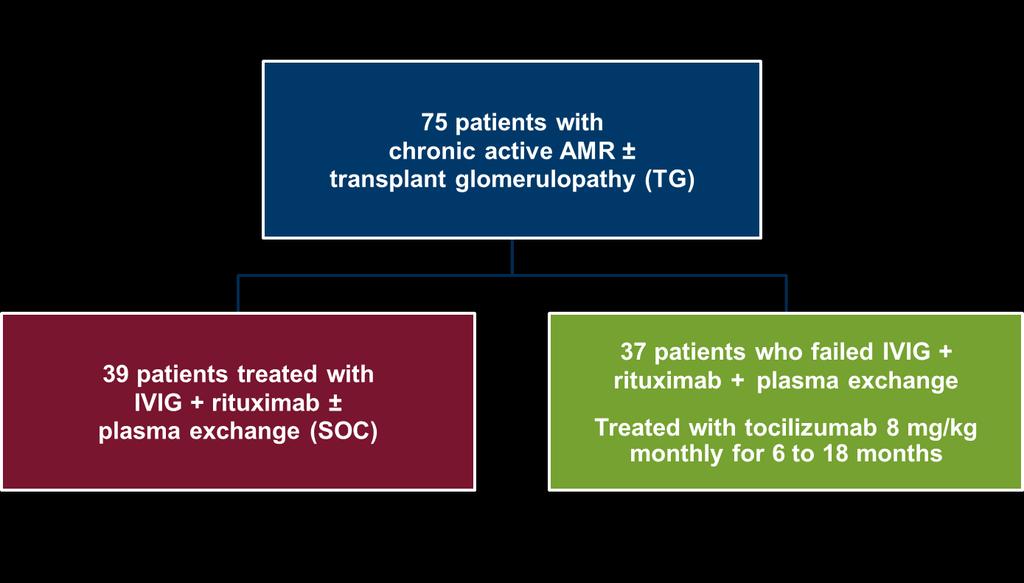

32 Tocilizumab Treatment of camr and TG: Treatment Protocol


33 Kidney Allograft and Patient Survival After Treatment With Tocilizumab for camr 1 1. Choi J et al. Am J Transplant Feb 15 [Epub ahead of print].

34 egfrs in Adult and Pediatric Patients Treated With Tocilizumab for camr 1 Time Post AMR, Months Time Post AMR, Months 1. Choi J et al. Am J Transplant Feb 15 [Epub ahead of print].

35 Allograft Phenotype Pre and Post Tocilizumab Treatment 1 g + pct Score P =.0175 IF/TA Score P = Choi J et al. Am J Transplant Feb 15 [Epub ahead of print].


36 Identification of Rejection Phenotypes According to the Characteristics of the Dominant Donor-Specific Anti-HLA Antibody 1 1. Lefaucheur C et al. J Am Soc Nephrol. 2016;27:

37 Death-Censored Kidney Allograft Survival According to IgG idsa Subclass Status 1 1. Lefaucheur C et al. J Am Soc Nephrol. 2016;27:
38 Impact of Tocilizumab on Total IgG Anti-HLA Antibody Levels and IgG Subclass DSAs in camr Patients 1 Pre Tocilizumab Post Tocilizumab Total IgG, mg/ml 13.0 ± ± 3.0 a IgG1, μg/ml 9.5 ± ± 4.6 a IgG2, μg/ml 4.0 ± ± 1.0 a IgG3, μg/ml 1.3 ± ± 0.5 a IgG4, μg/ml 0.3 ± ± 0.2 b Anti-HLA-IgG (score) 99 ± ± 71 a DSA (score) 10.0 ± ± 6.8 a IgG3 (MFI, x1,000) 9.5 ± ± 4.4 a IgG4 (MFI, x1,000) 2.4 ± ± 1.3 a P <.05 and.05 < b P <.1 vs pre tocilizumab. 1. Shin B-H et al American Transplant Congress (ATC 2017). Abstract B75.

.")
39 Tocilizumab Induces Regulatory T Cells Post Transplant in Primate Model of Lung Transplantation 1 FL4-H Foxp3 APC FL4-H Foxp3 APC FL4-H Foxp3 APC FL4-H Foxp3 APC FL4-H Foxp3 APC FL4-H Foxp3 APC 1. Aoyama A et al American Transplant Congress (ATC 2016). Abstract 2.


40 Tocilizumab + ATG Induction Dramatically Improves Lung Allograft Survival in Incompatible Primates 1 DSA- DSA+ 1. Aoyama A et al. ATC Abstract 2.
41 Use of the Streptococcal IgG Endopeptidase (IdeS) to Eliminate Pathogenic Donor Specific Antibodies
42 Mechanism of Action of IdeS with Implications for CDC and ADCC 1 IgG scigg F(ab ) 2 & Fc IdeS IdeS Complement(+)/FcγR(+) Complement(-)/FcγR(+/-) Complement(-)/FcγR(-) CDC(+)/ADCC(+) CDC(-)/ADCC(+/-) CDC(-)/ADCC(-) 1. Jordan SC et al In press.

43 Solutions to Remove Pathogenic IgG in Patients 1 Therapeutic plasma exchange/immunoadsorption 1. Jordan SC et al In press.
44 IdeS Protocols for Desensitization: United States and Sweden 1 CXM Sweden IdeS ATGAM DD or LD treatment DSA/safety TAC + MMF + steroids 6 months United States CXM IdeS IVIG, 2 weeks post treatment Alemtuzumab, day 4 post treatment >-1 month DSA/safety 6 months IVIG/rituximab DD treatment TAC + MMF + steroids 1. Jordan SC et al In press.



45 1. Jordan SC et al In press. SDS-Page and Western Blot Analysis of Serum Pre and Post IdeS Treatment 1

46 Impact of IdeS on HLA Antibodies in Single Antigen Luminex and C1q Luminex Assay 1 1. Jordan SC et al In press.

47 Sum and Strongest DSAs Pre Transplant and 1 Month Post IdeS 1 DSA (Sum of MFI) Before Desensitization DSA (Sum of MFI) at 1 Month Post Treatment Highest DSA Before Desensitization Highest DSA at 1 Month Post Treatment 1. Jordan SC et al In press.
48 Conclusions B cells and antibodies have emerged as primary mediators of chronic allograft loss and the pre-eminent immunologic barrier to transplantation Therapies for prevention and treatment of AMR are advancing beyond traditional immunosuppressive drugs to immune modulation, primarily through induction of regulatory T cells and biologic alteration of T-effector cells and the complement system




49 Striking the Right Balance: What Can We Do to Achieve and Maintain Adequate Immunosuppression After Kidney Transplantation? Alexander Wiseman, MD, FAST Professor of Medicine, Division of Renal Diseases and Hypertension Medical Director, Kidney and Pancreas Transplant Programs University of Colorado School of Medicine Aurora, Colorado
50 The Role of Specific Immunosuppressive Agents in DSA Formation



51 OPTN/SRTR 2013 Annual Data Report: Immunosuppression in Adult Kidney Transplant Recipients 1 1. Matas AJ et al. Am J Transplant. 2015;15(suppl 2):1-34.
52 Production of dndsa is a major risk factor for acute and chronic antibody-mediated rejection and graft loss after all solid organ transplantation What do we know about the risk of individual immunosuppressive agents and their ability to prevent dndsa production?
53 Induction Therapy: A Comparison of the Risk of dndsa 1 Study N F/U, y Induction Regimen Maintenance Regimen Univariate or Multivariate Analysis (dndsa) P ratg Brokho et al 2014: Prospective, single-center study ratg or BAS TAC MMF Steroids HR = 0.16 ratg vs BAS.003 Huang et al 2012: Retrospective, single-center cohort study ratg, BAS, or none CsA or TAC MPA Steroids 7.4% ratg 40% BAS 7.1% none.030 Alemtuzumab Todeschini et al 2013: Retrospective, single-center matched control study 48 2 ALEM or ratg/bas CsA or SRL MMF Steroids to day 7 57% ALEM 12.5% ratg/bas.01 Rituximab Tydén at al 2012: Prospective, multi-center double-blind study 71 3 RITUX or placebo TAC MMF Steroids 3% RITUX 16% placebo.10 Bortezomib Ejaz et al 2013: Prospective, two-center randomized study 40 1 ratg or ratg/ritux or ratg/bort or ratg/ritux/bort TAC MMF Steroids 30% ratg 30% ratg/ritux 10% ratg/bort 30% ratg/ritux/bort NA 1. O'Leary JG et al. Transplantation. 2016;100:39-53.
54 ratg Versus Basiliximab consecutive, moderately sensitized (+DSA/-FXM) recipients of deceased donor kidney transplants from 2009 to 2011 ratg: n = 85; basiliximab: n = month follow-up Kidney Function at 12 Months Basiliximab ATG P egfr ± SD, ml/min 55 ± ± 25.9 Creatinine, mg/dl 1.4 ± ± UPC, mg/mg 0.3 ± ± DSA at 12 Months dndsa (MFI ± SD) 3,652 ± 12, ± 1, DSA (MFI ± SD) 4,060 ± 6,300 2,454 ± 4, Brokhof MM et al. Transplantation. 2014;97:
 1. Brokhof MM et al. Transplantation.")
55 ratg Versus Basiliximab (Cont d) 1 Thymoglobulin ATG (1) Basiliximab (0) 1. Brokhof MM et al. Transplantation. 2014;97:
 2.")
56 Initial Maintenance Immunosuppressive Medications: KDIGO 1 2.1: We recommend using a combination of immunosuppressive medications as maintenance therapy including a CNI and an antiproliferative agent, with or without corticosteroids (1B) 2.2: We suggest that tacrolimus be the first-line CNI used (2A) 2.3: We suggest that mycophenolate be the first-line antiproliferative agent (2B) 2.5: We recommend that if mtori are used, they should not be started until graft function is established and surgical wounds are healed (1B) 1. KDIGO Transplant Work Group. Am J Transplant. 2009;9(suppl 3):S1-S157.
57 Calcineurin Inhibitor Maintenance Therapy: A Comparison of the Risk of dndsa 1 Study Organ Type N Follow- Up Maintenance Regimen Univariate or Multivariate Analysis dndsa P Use of Therapy According to Presence/Absence of dndsa Cooper et al 2011: Retrospective, single-center cohort study Kidney or kidneypancreas y Various NA NA TAC was used in 77% of patients with dndsa and 90% of patients with no dndsa (P =.009) Huang et al 2012: Retrospective, single-center cohort study Kidney y CsA or TAC MPA Steroids 22% CsA, 4% TAC.02 Lachmann et al 2006: Prospective, single-center cohort study Kidney 1,043 >6 mo to 4 y CsA or TAC ± MMF/AZA ± Steroids 35% CsA, 20% TAC.05 Hourmant et al 2005: Prospective, single-center cohort study Kidney 1,229 5 y Various CNI was used in 93% and 95% of patients with or without dndsa, respectively (NS) 1. O'Leary JG et al. Transplantation. 2016;100:39-53.

58 CNI and DSA Formation : 244 consecutively transplanted kidney and kidney/pancreas recipients without pre transplant DSA screened for dndsa at 1, 6, 12, and 24 months and when clinically indicated DSA detected in 27% of all patients by protocol or indication screening DSA+ associated with rejection (9.5% vs 27%), lower GFR, and graft loss All patients, n (%) DSA+, n (%) DSA-, n (%) P Induction None 71 (29) 18 (28) 53 (30).73 Thymoglobulin 162 (66) 43 (66) 119 (66) IL-2RA 11 (5) 4 (6) 7 (4) Immunosuppression T/M/P 212 (87) 50 (77) 162 (90).009 S/M/P 16 (6.5) 6 (9) 10 (6) Other 16 (6.5) 9 (14) 7 (4) Tacrolimus-based therapy was associated with lower incidence of DSA formation 1. Cooper JE et al. Transplantation. 2011; 91:
59 Examples of CNI-Sparing Clinical Trials: CNI Avoidance Protocols 1 Study Comparison Groups Pts, n Ekberg et al (ELITE- Symphony) Larson et al Flechner et al (ORION) CsA-MMF-pred vs DAC- MMF-pred with: low-dose TAC; low-dose CsA; low-dose SRL TAC-MMF-pred vs SRL-MMF-pred SRL-TAC (elimination at 13 wk)-pred vs SRL-MMFpred 1 vs TAC-MMF-pred F/U, mo 1, Incidence of AR in low TAC- MMF-pred Graft Function in low TAC-MMFpred Graft Survival in low TAC-MMFpred Similar Similar Similar SRL-MFpred Similar Similar Vincenti et al (BENEFIT) belatacept (more intensive)- MMF-pred vs belatacept (less intensive)-mmf-pred vs CsA-MMF-pred belatacept (more & less intensive)- MMF-pred belatacept (more & less intensive)- MMF-pred Similar Durrbach et al (BENEFIT-EXT) belatacept (more intensive)- MMF-pred vs belatacept (less intensive)-mmf-pred vs CsA-MMF-pred (ECD) Similar belatacept (more & less intensive)- MMF-pred Similar 1. Issa N et al. Am J Nephrol. 2013;37:
60 Examples of CNI-Sparing Clinical Trials: CNI Elimination Protocols Conversion to SRL-Based Regimen 1 Study Comparison Groups Pts, n F/U, mo Incidence of AR Graft Function Graft Survival Lebranchu et al (CONCEPT) Weir et al (Spare-the- Nephron) CsA-MMF-pred vs SRL-MMF-pred CsA or TAC-MMF vs SRL-MMF Similar SRL-MMF-pred Similar Similar SRL-MMF Similar Schena et al (CONVERT) CsA or TAC-MMF or AZA-pred vs SRL-MMF-pred Similar SRL-MMF-pred for GFR >40 ml/ min/1.73 m 2 Similar 1. Issa N et al. Am J Nephrol. 2013;37:


61 Belatacept and CNI Avoidance 1-3 BENEFIT and BENEFIT-EXT trials Basiliximab/MMF/pred plus less intensive belatacept, more intensive belatacept, or CsA Acute Rejection Rates at 1 Year BENEFIT GFR: 7-Year Follow-Up P <.001 for overall treatment effect 1. Vincenti F et al. Am J Transplant ;10: Durrbach A et al. Am J Transplant. 2010;10: Vincenti F et al. New Engl J Med. 2016;374:
 Belatacept LI (n = 226) CsA (n = 215) 1.")

62 Belatacept: dndsa Development 1,2 Belatacept MI (n = 219) Belatacept LI (n = 226) CsA (n = 215) 1. Vincenti F et al. New Engl J Med. 2016;374: Durrbach A et al. Am J Transplant. 2016;16:
63 mtor Inhibitor Maintenance Therapy: A Comparison of the Risk of dndsa 1 Study Organ Type N Time From Transplant to Switch F/U Maintenance Regimen Univariate or Multivariate Analysis (dndsa) P Kaneku et al 2013: Retrospective, single-center cohort study Liver y SRL (n = 119) or no SRL (n = 630) at 1 y ± MMF/AZA ± CsA/TAC ± Steroids OR = 0.66 SRL vs no SRL.36 Early switch (<1 y) to mtor inhibitor Liefeldt et al 2012: Prospective, single-center randomized study Kidney to 4 mo Median 3.5 y CsA or CsA converted to EVR (months 3-4.5) MPA Steroids HR = 2.67 EVR vs CsA.04 Late switch (>1 y) to mtor inhibitor Croze et al 2014: Retrospective, single-center cohort study Kidney 270 Mean, 1.3 y Mean 3.8 y TAC switched to SRL ± Steroids to month 3 HR = 2.4 SRL vs TAC.04 Ruiz San Millán et al 2014: Retrospective, single-center cohort study Kidney 35 Median 69 mo (range 3-375) 2 y CNI switched to mtor inhibitor ± MMF/AZA ± steroids 8.6% mtor inhibitor; 0% controls (n = 10) NS Perbos et al 2014: Retrospective, single-center case control study Various 131 Mean 73 mo 1 y CNI switched to EVR ± CNI or CNI ± MMF (controls) 6.7% EVR; 11.1% controls O'Leary JG et al. Transplantation. 2016;100:39-53.
64 Cumulative Incidence of DSA CNI Conversion and dndsa Formation: Cyclosporine Versus Everolimus 1 From two randomly controlled trials, at 3 to 4.5 months post transplant, 127 patients randomized to continue CsA or converted to EVR 7/65 (10.8%) on CsA developed DSA (median: 991 days) 14/61 (23.0%) on EVR developed DSA (median: 551 days; P =.048) EVR CsA Time After Transplantation, Months 1. Liefeldt L et al. Am J Transplant. 2012;12:

65 Antiproliferative Agent and dndsa (Tacrolimus Maintenance): MPA Versus mtor Inhibitor 1 Retrospective case-control study 66 patients treated with TAC/mTOR inhibitor/prednisone (SRL = 30, EVR = 36) vs 132 patients treated with TAC/MPA/prednisone No difference in rates of DSA formation or clinical outcomes Years Post Transplant 1. Mithani Z et al. Exp Clin Transplantation [Epub ahead of print].
66 Clinical Outcomes at 1 y (N = 198) MRI Within 1 y DSA De Novo Donor-Specific Antibody Formation and Clinical Outcomes 1 mtor Inhibitor Group (N = 66) Mycophenolate Group (N = 132) Within 1 mo 11 (16.7%) 13 (9.8%).18 Within 6 mo 17 (25.8%) 20 (15.2%).07 Within 1 y 19 (28.8%) 29 (22.0%).27 Overall 20 (30.3%) 37 (28.0%).73 <1,000 7 (36.8%) 8 (27.6%).66 P 1,000 to <3,000 8 (42.1%) 13 (44.8%) 3,000 to <5,000 1 (5.3%) 5 (17.2%) 5,000 3 (15.8%) 3 (10.3%) TAC trough mean (SD) 5.4 (2.5%) 6.5 (2.8%).020 Mean GFR (SD) 56.8 (17.9%) 55.5 (16.9%).62 Mean imputed GFR (SD) 55.9 (19.1%) 51.9 (21.3%).20 Proteinuria median (IQR) 0.1 (0.1%-0.3%) 0.1 (0%-0.2%).20 Acute rejection, no. (%) 1. Mithani Z et al. Exp Clin Transplantation [Epub ahead of print]. 6 (9.1%) (1 AMR, 2 cellular, 3 mixed) 15 (11.4%) (1 AMR, 5 cellular, 5 clinical, 2 mixed, 2 NA).64
67 Antimetabolite or Purine Synthesis Inhibitor Maintenance Therapy: Comparison of the Risk of dndsa 1 Study Organ Type N Follow- Up Maintenance Regimen Univariate or Multivariate Analysis dndsa P Use of Therapy According to Presence/Absence of dndsa Del Bollo et al 2014: Retrospective, singlecenter cohort study Liver 232 Median 36.5 mo Various NA NA MMF was used in 90% of pts with dndsa vs 71% of pts with no dndsa (P =.04) Kaneku et al 2013: Retrospective, singlecenter cohort study Liver y MMF or none/aza ± CsA/TAC ± Sirolimus ± Steroids OR = 1.00 MMF vs no MMF.99 Lachmann et al 2006: Prospective, singlecenter cohort study Kidney 1,043 >6 mo to 4 y MMF or AZA or no antimetabolite CsA or TAC ± Steroids 39% AZA 26% MMF 19% none.37 Piazza et al 2006: Retrospective, singlecenter cohort study Kidney 449 Not stated MMF or AZA CsA Steroids 8% MMF 23% AZA <.0001 Hourmant et al 2005: Prospective, singlecenter cohort study Kidney 1,229 5 y Various NA NA MMF was used in 43%, 31%, and 53% of pts with no antibodies, dndsa or non-dsa (P <.02) AZA was used in 31%, 43% and 23% of pts with no antibodies, dndsa or non-dsa (P <.02) 1. O'Leary JG et al. Transplantation. 2016;100:39-53.
68 Steroid Maintenance Therapy: A Comparison of the Risk of dndsa 1 Study Organ Type N Follow-Up Maintenance Regimen Univariate or Multivariate Analysis dndsa P Use of Therapy According to Presence/Absence of dndsa Del Bollo et al 2014: Retrospective, singlecenter cohort study Liver 232 Median 36.5 mo Various NA NA Steroids used in 19% of pts with dndsa and 44% of pts with no dndsa (P =.02) Kaneku et al 2013: Retrospective, singlecenter cohort study Liver y Steroids or no steroids ± CsA/TAC ± MMF/AZA ± Sirolimus OR = 0.67 steroids vs no steroids.23 Hoshino et al 2012: Prospective, singlecenter cohort study Kidney 72 1 y Clonal depletion Steroids ± CNI, MMF, or sirolimus ARR = 0.92 per 2.5 mg/day in steroid dose.03 Delgado et al 2009: Prospective, singlecenter, double-blind randomized study Kidney 37 5 y TAC MMF Steroid withdrawal at day 7 (n = 21) or standard steroids (n = 16) 0% steroid withdrawal; 6.3% standard steroids.43 Lachmann et al 2006: Prospective, singlecenter cohort study Kidney 1,043 >6 mo to 4 y Steroids or no steroids CsA or TAC ± MMF/AZA 27% steroids; 33% no steroids.44 Hourmant et al 2005: Prospective, singlecenter cohort study Kidney 1,229 5 y Various NA NA Steroids used in 22%, 40% & 43% of pts with no antibodies, dndsa or non-dsa (NS) 1. O'Leary JG et al. Transplantation. 2016;100:39-53.
69 Dosing Considerations: What Are the Limitations?

70 The Symphony Trial: Defining Today s Gold Standard 1 12-month randomized, open-label multicenter trial (N = 1,645) Four arms (all receive basiliximab induction, MMF/prednisone) CsA 150 ng/ml to 300 ng/ml x 3 months, then 100 ng/ml to 200 ng/ml CsA 50 ng/ml to 100 ng/ml TAC 3 ng/ml to 7 ng/ml SRL 4 ng/ml to 8 ng/ml a P<0.05 vs SRL low and vs CSA standard 1. Ekberg H et al. N Engl J Med. 2007;357:
 12")

71 Symphony and CNI Minimization 1 Drug Trough Tacrolimus (4-7) 12 months months Ekberg H et al. Am J Transplant. 2009;9:

72 Lower Mean Tacrolimus Troughs Increase Risk of dndsas in the First Year of Kidney Transplant Scott Davis, MD, Jane Gralla, PhD, Suhong Tong, MS, Patrick Klem, PharmD, Alexander Wiseman, MD, James Cooper, MD
73 Patient Flowchart 1 Included N = 884 Excluded n = 341 Excluded n = 341 Pretransplant DSA (n = 268) Liver-Kidney (n = 14) DSA/TAC Data (n = 59) Pretransplant DSA (n = 268) Liver-Kidney (n = 14) DSA/TAC Data (n = 59) Patients n = 543 Total TAC levels: 11,859 Mean Mean number #TAC TAC level: level: dndsa- (-) n = 425 (78.3%) dndsa+ n = 118 (21.7%) 1. Davis S et al. ATC Abstract 5.

74 Survival to DSA by Mean TAC Troughs (ng/ml) % 72.6% 1. Davis S et al. ATC Abstract 5.
75 Odds Ratios for Mean TAC Trough Ranges (ng/ml) Compared With >8 ng/ml By 12 Months 1 Adjusted for HLA mismatches, age, sex, ethnicity, donor type, induction, and DGF P < P = P = to 7.9 vs >8 4 to 5.9 vs >8 0 to 3.9 vs >8 n = 305 n = 130 n = 95 n = 130 n = 13 n = Davis S et al. ATC Abstract 5.


76 Time to dndsa by Mean TAC 1 Week to 12 Months 1 Months Post Transplant 1. Davis S et al. ATC Abstract 5.
77 Tacrolimus Intrapatient Variability and the Evolution of Acute and Chronic Histologic Lesions 1 TAC intrapatient variability (IPV) analyzed from months 6 to 12 after transplantation in a cohort of 220 renal recipients for whom paired protocol biopsies at 3 months and 2 years were available CV (%) = (SD/mean TAC concentration) x 100 Example: TAC troughs from five measures are 4.9, 7.0, 9.3, 4.1, and 8.1 Mean = 6.68 Standard deviation = 2.17 CV (%) = 2.17/6.68 x 100 = 32.4% TAC Concentration Variability From Months 6 to 12 After Transplantation Variable Number of available TAC concentrations (mean ± SD) Mean TAC concentration ± SD (ng/ml) Outpatient 5.3 ± ± 1.6 TAC CV (%) Mean ± SD 19.7 ± 10.1 Median 18.4 Range (min to max) 1.2 to Vanhove T et al. Am J Transplant Mar 25 [Epub ahead of print].
78 Predictors of Chronic Histologic Scores in Multivariate Regression 1 Histologic Parameter at 2 y Predictor(s) Odds Ratio 95% CI P ci 2 at month Borderline/subclinical acute rejection at month ci 2 Donor age, years CV tertile High Middle Low Ref ct 2 at month Borderline or subclinical acute rejection at month ct 2 Donor age, years CV tertile High Middle Low Ref Vanhove T et al. Am J Transplant Mar 25 [Epub ahead of print].
79 Predictors of Chronic Histologic Scores in Multivariate Regression (Cont d) 1 Histologic Parameter at 2 y Predictor(s) Odds Ratio 95% CI P cv 2 Donor age, years cg 2 None ah 2 None Donor age, years De novo ah CV tertile High Middle Low Ref Mean TAC trough, ng/ml Vanhove T et al. Am J Transplant Mar 25 [Epub ahead of print].

80 Change in Chronicity Score Between Month 3 and Year 2, By IPV Tertile 1 P =.023 P =.880 Conclusion High IPV is related to accelerated progression of chronic histologic lesions before any evidence of renal dysfunction Cutoff: <14.4% <22.1% >22.1% IPV Tertile Mean CV: 9.8% 18.3% 31.1% TAC trough: Vanhove T et al. Am J Transplant Mar 25 [Epub ahead of print].
 1. Sapir-Pichhadze R et al. Kidney Int.")
81 Use of Drug-Level Monitoring (IPV) to Assess Under-Immunosuppression/Adherence patients measured TAC variability while on stable dose; median follow-up: 3.72 years Composite endpoint: late allograft rejection, TG, or graft loss (including death) 1. Sapir-Pichhadze R et al. Kidney Int. 2014;85:
82 Does Time-Varying Exposure to TAC Increase Risk of Long-Term Adverse Outcomes in Adult KTRs? 1 Relative Hazard of Primary Composite Endpoint and Secondary Composite Endpoint by TacSD Threshold TacSD Threshold HR (95% CI) for Primary Composite Endpoint P HR (95% CI) for Secondary Composite Endpoint P >1.5 vs (0.75, 2.37) (0.60, 2.51).58 >2 vs (0.89, 2.54) (0.73, 2.86).29 >2.5 vs (1.04, 3.25) (0.96, 4.12).06 >3 vs (1.42, 4.62) < (1.30, 5.89).01 Conclusion Increased time-dependent TacSD may be an independent risk factor for adverse kidney transplant outcomes; TacSD may serve as a monitoring tool to identify high-risk patients 1. Sapir-Pichhadze R et al. Kidney Int ;85:


83 Impact of Within-Patient Variability in TAC Blood Levels on Kidney Graft Loss 1 Analysis of 310 deceased-donor adult renal transplants performed from 1998 to 2013 Death-Censored Graft Survival Curve Multivariate Cox Regression Analysis for DCGL HR 95% CI P Patients with CV <30% CV >30% Patients with CV >30% GFR, per 1 ml/ min per 1.73 m <.001 Proteinuria, per 1 g < Rodrigo E et al. Transplantation. 2016;100:
84 Risk Factors for dndsa Development 1 dndsa (n = 271) dndsa+ (n = 39) P dndsa (n = 271) dndsa+ (n = 39) P Recipient's age 51 ± ± Recipient s sex (male) Cold ischemia time, h 71.2% 64.1% ± ± Transplant number 1.3 ± ± Transplant number >1 20.3% 38.5%.011 Peak PRA 4.8 ± ± Mismatches 3.8 ± ± Thymoglobulin 2.6% 7.7%.091 Basiliximab 25.1% 23.1%.785 Steroid withdrawal 55.0% 46.2%.299 DGF 23.3% 25.0%.817 Acute rejection 20.4% 35.9% year GFR, ml/min per 1.73 m 2 50 ± ± year 24-h proteinuria, g 0.8 ± ± CV >30% 35.4% 51.3% Rodrigo E et al. Transplantation. 2016;100:

85 dndsa Development: Impact on Graft Survival 1 Death-Censored Graft Survival Curve 1. Rodrigo E et al. Transplantation. 2016;100:

86 dndsa Development dndsa Detection According to Coefficient of Variation 1 Log rank P =.007 CV >30% CV <30% Conclusion Tacrolimus level variability is a strong risk factor for dndsa development and DCGL; variability should be added to the current monitoring of kidney transplant recipients because of its relationship with adherence and to graft outcome 1. Rodrigo E et al. Transplantation. 2016;100:
 Median duration of BK viremia: 140 days (IQR 40 to 393 days) Neither the presence nor the duration of BK viremia had a deleterious effect on")
87 Persistent BK Viremia Does Not Increase Intermediate- Term Graft Loss But Is Associated With dndsa kidney or kidney pancreas transplant recipients; median: 3 years follow-up 132 (17%) recipients developed BK viremia (IS dose reduction) Median duration of BK viremia: 140 days (IQR 40 to 393 days) Neither the presence nor the duration of BK viremia had a deleterious effect on patient or graft survival Persistent BK viremia was associated with an increased risk of developing dndsa, particularly class II DSA (HR 2.55 [95% CI, ]) 1. Sawinski D et al. J Am Soc Nephrol. 2015;26:
88 TAC and CsA both require careful management to ensure sufficient dosing for therapeutic effectiveness, while avoiding toxicity Routine monitoring of drug levels can be employed to balance efficacy while limiting side effects
89 Optimizing Immunosuppression in Clinical Practice

90 TAC Conc, ng/ml TAC Conc, ng/ml TAC Conc, ng/ml AUC 0-24, ng/h/ml AUC 0-24, ng/h/ml Minimizing Variability in CNI Exposure: Impact of Once-Daily Dosing 1 Tacrolimus Blood Concentration Time Profile of Representative Subject From Each Dosing Regimen Correlation Between Tacrolimus Concentration and AUC Twice-Daily Dosing Conclusion C24, ng/ml Once-Daily Dosing Tacrolimus given once daily in the morning, at 85% of the twice-daily dose, provides safe and equivalent drug exposure to twice-daily dosing; this convenient dosing schedule may help to increase compliance and lower costs C24, ng/ml 1. Hardinger KL et al. Am J Transplant. 2004;4:
91 Comparison of the Main Characteristics of the Two Clinically Available Once-Daily Formulations of TAC 1 Abbreviation (Trade Name) Formulation Strengths Conversion Ratio From IR-TAC Recommended C min AUC 0-24 Starting Dose a Correlation ER-TAC (Astagraf XL) Once daily Capsules in 0.5, 1, 3, and 5 mg 1 to mg/kg/day r LCP-TAC (Envarsus XR) Once daily, MeltDose Tablets in 0.75, 1, and 4 mg 1 to 0.7 (0.85 for blacks) 0.17 mg/kg/day r a According to Summary of Medical Product Characteristics of both drugs. 1. Piotti G et al. J Nephrol. 2017;30:53-61.

92 Evaluating the Pharmacokinetics of Once-Daily TAC 1 From January 2009 to January 2010, switch from IR-TAC to ER-TAC in 130 stable RTRs Conclusion Conversion from IR-TAC to once-daily ER-TAC appears to be safe and convenient up to 2 years after conversion in some recipients 1. Tran D et al. Exp Clin Transplant. 2014;12:
 Post Transplantation Renal Function Mean Daily Tacrolimus")

93 Evaluating the Pharmacokinetics of Once-Daily TAC (Cont d) 1 Comparison of PK and pathology for IR-TAC and ER-TAC in living kidney transplantation: prospective trial (N = 102 consecutive adult patients) Post Transplantation Renal Function Mean Daily Tacrolimus Dose Mean Daily Trough Level Time Post Transplantation, d Time Post Transplantation, d Time Post Transplantation, d Conclusion Clinical efficacy, safety, and PK profile of ER-TAC are same as those of IR-TAC 1. Tsuchiya T et al. Transplantation. 2013;96:
, 14, and 21")

94 Conversion From IR-TAC to LCP-TAC: Phase 2 Trial 1 Adult stable kidney transplant patients on IR-TAC capsules were converted to once-daily TAC tablets (LCP-TAC); patients continued on once-daily LCP-TAC for days 8 to 21; trough levels were to be maintained between 5 ng/ml and 15 ng/ml; 24-hour pharmacokinetic assessments were done on days 7 (baseline pre-switch), 14, and 21 Conclusions Stable kidney transplant patients can be safely converted from IR- TAC to LCP-TAC The greater bioavailability of LCP-TAC allows for once-daily dosing and similar (AUC) exposure at a dose ~30% less than the total daily dose of IR- TAC LCP-TAC displays flatter kinetics characterized by significantly lower peak-trough fluctuations 1. Gaber AO et al. Transplantation. 2013;96:

95 Long-Term Outcomes With ER-TAC, IR-TAC, and Twice-Daily CsA subjects receiving de novo kidney transplants were randomized to one of three treatment arms: once-daily ER-TAC, twice-daily IR-TAC, or twice-daily CsA All subjects received basiliximab induction, MMF, and CsA No differences in patient or graft survival between groups at 3 years 1. Silva H et al. Transplantation. 2014; 97:636.


96 LCP-TAC Versus IR-TAC in De Novo Kidney Transplants: Phase 3 Double-Blind RCT kidney transplant recipients randomized to LCP-TAC versus twice-daily IR-TAC egfr equivalent between groups throughout 2 years 1. Budde K et al. Am J Transplant. 2014;14:
97 A Steady-State Head-to-Head Pharmacokinetic Comparison of All FK-506 (TAC) Formulations (ASTCOFF): Study Design 1 An open-label, prospective, randomized, two-arm, three-period crossover study Sequence 1 IR-TAC LCP-TAC ER-TAC Randomized Sequence 2 IR-TAC ER-TAC LCP-TAC Day PK PK PK 1. Tremblay S et al. Am J Transplant. 2017;17:


98 ASTCOFF: Mean Whole Blood Concentrations of Tacrolimus 1 1. Tremblay S et al. Am J Transplant. 2017;17:
99 Pharmacokinetic Parameters in ASTCOFF: Observed Results 1,a Observed PK Parameter LCP-TAC ER-TAC IR-TAC TDD, md/day 4.9 ± ± ± 2.9 Median, IQR 4.8 ( ) 6.0 ( ) 6.0 ( ) AUC 0-24, h*ng/ml ± ± ± 50.8 C max, ng/ml 13.9 ± ± ± 5.5 C min, ng/ml 6.8 ± ± ± 1.7 T max, h 5.9 (1.5, 14.0) 1.9 (0.9, 5.9) 1.5 (0.9, 20.0) Fluctuation, % 83.6 ± (51.7) ± (48.4) ± (53.1) a Parameter AUC 0 24, C max, C min : Presented arithmetic mean ± SD; Parameter TDD: Presented arithmetic mean ± SD; T max : Presented median (min, max). 1. Tremblay S et al. Am J Transplant. 2017;17:
100 Pharmacokinetic Parameters in ASTCOFF: Comparisons 1,a Observed PK Parameter LCP-TAC vs IR-TAC (%) ER-TAC vs IR-TAC (%) LCP-TAC vs ER-TAC (%) TDD, md/day Median, IQR AUC 0-24, h*ng/ml (107.9, 127.0) P = (85.8, 101.0) P = (114.1, 138.5) P <.001 C max, ng/ml 94.7 (85.8, 104.4) P = (83.2, 101.3) P = (92.4, 115.0) P =.638 C min, ng/ml (97.6, 117.2) P = (75.7, 90.9) P = (117.4, 141.6) P <.001 T max, h 3.0 (1.6, 4.4) P < (-0.4, 0.5) P = (1.9, 4.0) P <.001 Fluctuation, % (-48.4, -9.6) P = (-13.1, 25.7) P = (-53.4, -17.3) P <.001 a Parameter AUC 0 24, C max, C min : Presented RGM in percent (90% CI) derived from ANCOVA models that included fixed effects of treatment, sequence, period (LCP-TAC vs ER TAC analyses), and random effect of subjects (sequence). P was from two sample t test. 1. Tremblay S et al. Am J Transplant. 2017;17:

101 ASTCOFF: Group Mean Daily Tacrolimus Trough Levels 1 Group Mean Daily TAC Trough Level (ng/ml) Determined by the Dried Blood Samples in Each Period Conclusions Results from this comparative PK study of all three innovator TAC formulations, conducted in stable renal transplant recipients, demonstrate that there are significant PK differences between LCP-TAC and both IR-TAC and ER-TAC and that formulations are not interchangeable with LCP-TAC 1. Tremblay S et al. Am J Transplant. 2017;17: LCP-TAC
102 Astagraf XL to Understand the Impact of Immunosuppression on De Novo DSA Development and Chronic Immune Activation in Kidney Transplantation (ASTOUND) 1 Primary outcome: combined incidence of DSA or immune activation (peripheral blood molecular profiling) at 1 and 2 years post transplant HLA-mismatched first kidney transplant, PRA 50%, no DSA Astagraf XL TAC C 0 6 ng/ml Induction, a MMF/pred maintenance (N = 550) TAC (Prograf and generics) TAC C 0 6 ng/ml a Per center protocol Accessed April 12, 2017.
103 Take-Home Points Both the type and the degree of immunosuppression contribute to the risk of DSA formation The current standard of care (TAC-based immunosuppression) is susceptible to intrapatient variability that is clinically meaningful Novel monitoring tools, TAC CV, and newer formulations (once-daily preparations) may mitigate these risks A hypothesis to be proven: Incorporation of higher-level monitoring and long-acting CNI preparations may reduce DSA/immune activation and improve long-term graft survival


104 Please remember to complete and submit your Post-Test and Evaluation for CME credit. Missed anything? Visit us at: Download slides and Practice Aids Watch for the ondemand version of this symposium Join the conversation on Thank you and good afternoon.
Literature Review: Transplantation July 2010-June 2011
 Literature Review: Transplantation July 2010-June 2011 James Cooper, MD Assistant Professor, Kidney and Pancreas Transplant Program, Renal Division, UC Denver Kidney Transplant Top 10 List: July Kidney
Literature Review: Transplantation July 2010-June 2011 James Cooper, MD Assistant Professor, Kidney and Pancreas Transplant Program, Renal Division, UC Denver Kidney Transplant Top 10 List: July Kidney
Current Trends in Kidney Transplantation: The Role of Nonadherence
 Current Trends in Kidney Transplantation: The Role of Nonadherence Donald E. Hricik, MD Professor of Medicine Case Western Reserve University Chief of the Division of Nephrology and Hypertension Medical
Current Trends in Kidney Transplantation: The Role of Nonadherence Donald E. Hricik, MD Professor of Medicine Case Western Reserve University Chief of the Division of Nephrology and Hypertension Medical
Steroid Minimization: Great Idea or Silly Move?
 Steroid Minimization: Great Idea or Silly Move? Disclosures I have financial relationship(s) within the last 12 months relevant to my presentation with: Astellas Grants ** Bristol Myers Squibb Grants,
Steroid Minimization: Great Idea or Silly Move? Disclosures I have financial relationship(s) within the last 12 months relevant to my presentation with: Astellas Grants ** Bristol Myers Squibb Grants,
Desensitization in Kidney Transplant. James Cooper, MD Assistant Professor, Kidney and Pancreas Transplant Program, Renal Division, UC Denver
 Desensitization in Kidney Transplant James Cooper, MD Assistant Professor, Kidney and Pancreas Transplant Program, Renal Division, UC Denver Organ Shortage Currently there are >90,000 patients on the kidney
Desensitization in Kidney Transplant James Cooper, MD Assistant Professor, Kidney and Pancreas Transplant Program, Renal Division, UC Denver Organ Shortage Currently there are >90,000 patients on the kidney
Literature Review Transplantation
 Literature Review 2010- Transplantation Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney and Pancreas Transplant Programs University of
Literature Review 2010- Transplantation Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney and Pancreas Transplant Programs University of
Controversies in Renal Transplantation. The Controversial Questions. Patrick M. Klem, PharmD, BCPS University of Colorado Hospital
 Controversies in Renal Transplantation Patrick M. Klem, PharmD, BCPS University of Colorado Hospital The Controversial Questions Are newer immunosuppressants improving patient outcomes? Are corticosteroids
Controversies in Renal Transplantation Patrick M. Klem, PharmD, BCPS University of Colorado Hospital The Controversial Questions Are newer immunosuppressants improving patient outcomes? Are corticosteroids
DSA Positive and then To biopsy or not?
 DSA Positive and then To biopsy or not? Banff SCT 2017 29 March 2017 Peter Nickerson, MD, FRCPC, FCAHS Flynn Family Chair in Renal Transplantation Professor of Internal Medicine and Immunology Relevant
DSA Positive and then To biopsy or not? Banff SCT 2017 29 March 2017 Peter Nickerson, MD, FRCPC, FCAHS Flynn Family Chair in Renal Transplantation Professor of Internal Medicine and Immunology Relevant
James E. Cooper, M.D. Assistant Professor, University of Colorado at Denver Division of Renal Disease and Hypertension, Kidney and PancreasTransplant
 James E. Cooper, M.D. Assistant Professor, University of Colorado at Denver Division of Renal Disease and Hypertension, Kidney and PancreasTransplant Program Has no real or apparent conflicts of interest
James E. Cooper, M.D. Assistant Professor, University of Colorado at Denver Division of Renal Disease and Hypertension, Kidney and PancreasTransplant Program Has no real or apparent conflicts of interest
SELECTED ABSTRACTS. All (n) % 3-year GS 88% 82% 86% 85% 88% 80% % 3-year DC-GS 95% 87% 94% 89% 96% 80%
 % 3-year GS 88% 82% 86% 85% 88% 80% % 3-year DC-GS 95% 87% 94% 89% 96% 80%") SELECTED ABSTRACTS The following are summaries of selected posters presented at the American Transplant Congress on May 5 9, 2007, in San Humar A, Gillingham KJ, Payne WD, et al. Review of >1000 kidney
SELECTED ABSTRACTS The following are summaries of selected posters presented at the American Transplant Congress on May 5 9, 2007, in San Humar A, Gillingham KJ, Payne WD, et al. Review of >1000 kidney
Risk Factors in Long Term Immunosuppressive Use and Advagraf. Daniel Serón Nephrology department Hospital Universitari Vall d Hebron
 Risk Factors in Long Term Immunosuppressive Use and Advagraf Daniel Serón Nephrology department Hospital Universitari Vall d Hebron Progressive well defined diseases ABMR GN Polyoma Non-specific Findings
Risk Factors in Long Term Immunosuppressive Use and Advagraf Daniel Serón Nephrology department Hospital Universitari Vall d Hebron Progressive well defined diseases ABMR GN Polyoma Non-specific Findings
The new Banff vision of the role of HLA antibodies in organ transplantation: Improving diagnostic system and design of clinical trials
 The new Banff vision of the role of HLA antibodies in organ transplantation: Improving diagnostic system and design of clinical trials Carmen Lefaucheur 1 2 Banff 2015: Integration of HLA-Ab for improving
The new Banff vision of the role of HLA antibodies in organ transplantation: Improving diagnostic system and design of clinical trials Carmen Lefaucheur 1 2 Banff 2015: Integration of HLA-Ab for improving
Overview of New Approaches to Immunosuppression in Renal Transplantation
 Overview of New Approaches to Immunosuppression in Renal Transplantation Ron Shapiro, M.D. Professor of Surgery Surgical Director, Kidney/Pancreas Transplant Program Recanati/Miller Transplantation Institute
Overview of New Approaches to Immunosuppression in Renal Transplantation Ron Shapiro, M.D. Professor of Surgery Surgical Director, Kidney/Pancreas Transplant Program Recanati/Miller Transplantation Institute
Recognition and Treatment of Chronic Allograft Dysfunction
 Recognition and Treatment of Chronic Allograft Dysfunction Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney and Pancreas Transplant Programs
Recognition and Treatment of Chronic Allograft Dysfunction Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney and Pancreas Transplant Programs
OBJECTIVES. Phases of Transplantation and Immunosuppression
 Transplant and Immunosuppression: Texas Transplant Center April 29, 2017 Regina L. Ramirez, Pharm.D., BCPS PGY1 Pharmacy Residency Program Director Clinical Practice Specialist Solid Organ Transplant and
Transplant and Immunosuppression: Texas Transplant Center April 29, 2017 Regina L. Ramirez, Pharm.D., BCPS PGY1 Pharmacy Residency Program Director Clinical Practice Specialist Solid Organ Transplant and
Donor-derived Cell-free DNA Improves DSA-informed Diagnosis of ABMR in Kidney Transplant Patients
 Donor-derived Cell-free DNA Improves DSA-informed Diagnosis of ABMR in Kidney Transplant Patients Stanley C. Jordan, MD Director, Division of Nephrology Medical Director, Kidney Transplant Program Medical
Donor-derived Cell-free DNA Improves DSA-informed Diagnosis of ABMR in Kidney Transplant Patients Stanley C. Jordan, MD Director, Division of Nephrology Medical Director, Kidney Transplant Program Medical
Treatment of Chronic Antibody Mediated Rejection
 Treatment of Chronic Antibody Mediated Rejection Robert A. Montgomery MD, DPhil Professor of Surgery Director of the NYU Langone Transplant Institute Disclosures: Served on Advisory Boards for Genentech
Treatment of Chronic Antibody Mediated Rejection Robert A. Montgomery MD, DPhil Professor of Surgery Director of the NYU Langone Transplant Institute Disclosures: Served on Advisory Boards for Genentech
Tolerance Induction in Transplantation
 Tolerance Induction in Transplantation Reza F. Saidi, MD, FACS, FICS Assistant Professor of Surgery Division of Organ Transplantation Department of Surgery University of Massachusetts Medical School Percent
Tolerance Induction in Transplantation Reza F. Saidi, MD, FACS, FICS Assistant Professor of Surgery Division of Organ Transplantation Department of Surgery University of Massachusetts Medical School Percent
What is the Best Induction Immunosuppression Regimen in Kidney Transplantation? Richard Borrows: Queen Elizabeth Hospital Birmingham
 What is the Best Induction Immunosuppression Regimen in Kidney Transplantation? Richard Borrows: Queen Elizabeth Hospital Birmingham SYMPHONY Study Ekberg et al. NEJM 2008 Excluded: DCD kidneys; CIT>30hours;
What is the Best Induction Immunosuppression Regimen in Kidney Transplantation? Richard Borrows: Queen Elizabeth Hospital Birmingham SYMPHONY Study Ekberg et al. NEJM 2008 Excluded: DCD kidneys; CIT>30hours;
Transplantation: Year in Review
 Transplantation: Year in Review Alexander Wiseman, MD Medical Director, Kidney and Pancreas Transplant Program Associate Professor, Division of Renal Diseases and Hypertension University of Colorado Outline:
Transplantation: Year in Review Alexander Wiseman, MD Medical Director, Kidney and Pancreas Transplant Program Associate Professor, Division of Renal Diseases and Hypertension University of Colorado Outline:
Management of Rejection
 Management of Rejection I have no disclosures Disclosures (relevant or otherwise) Deborah B Adey, MD Professor of Medicine University of California, San Francisco Kidney and Pancreas Transplant Center
Management of Rejection I have no disclosures Disclosures (relevant or otherwise) Deborah B Adey, MD Professor of Medicine University of California, San Francisco Kidney and Pancreas Transplant Center
Update on Transplant Glomerulopathy
 Update on Transplant Glomerulopathy Miklos Z Molnar, MD, PhD, FEBTM, FERA, FASN Associate Professor of Medicine Division of Nephrology, Department of Medicine University of Tennessee Health Science Center
Update on Transplant Glomerulopathy Miklos Z Molnar, MD, PhD, FEBTM, FERA, FASN Associate Professor of Medicine Division of Nephrology, Department of Medicine University of Tennessee Health Science Center
Better than Google- Click on Immunosuppression Renal Transplant. David Landsberg Oct
 Better than Google- Click on Immunosuppression Renal Transplant David Landsberg Oct 3 2008 OUTLINE History of Immunosuppression Trends in Immunosupression FK vs CYA Steroid Minimization CNI Avoidance Sirolimus
Better than Google- Click on Immunosuppression Renal Transplant David Landsberg Oct 3 2008 OUTLINE History of Immunosuppression Trends in Immunosupression FK vs CYA Steroid Minimization CNI Avoidance Sirolimus
Victims of success: Do we still need clinical trials? Robert S. Gaston, MD CTI Clinical Trials and Consulting University of Alabama at Birmingham
 Victims of success: Do we still need clinical trials? Robert S. Gaston, MD CTI Clinical Trials and Consulting University of Alabama at Birmingham Disclosure Employee: CTI Clinical Trials and Consulting
Victims of success: Do we still need clinical trials? Robert S. Gaston, MD CTI Clinical Trials and Consulting University of Alabama at Birmingham Disclosure Employee: CTI Clinical Trials and Consulting
HLA Part II: My Patient Has DSA, Now What?
 2017 CST-Astellas Canadian Transplant Fellows Symposium HLA Part II: My Patient Has DSA, Now What? James Lan, MD, FRCPC, D(ABHI) Dr. Lan completed his nephrology training at the University of British Columbia.
2017 CST-Astellas Canadian Transplant Fellows Symposium HLA Part II: My Patient Has DSA, Now What? James Lan, MD, FRCPC, D(ABHI) Dr. Lan completed his nephrology training at the University of British Columbia.
Innovation In Transplantation:
 Innovation In Transplantation: Improving outcomes Thomas C. Pearson Department of Surgery Emory Transplant Center CHOA Symposium October 22, 2016 Disclosures Belatacept preclinical and clinical trial were
Innovation In Transplantation: Improving outcomes Thomas C. Pearson Department of Surgery Emory Transplant Center CHOA Symposium October 22, 2016 Disclosures Belatacept preclinical and clinical trial were
BK virus infection in renal transplant recipients: single centre experience. Dr Wong Lok Yan Ivy
 BK virus infection in renal transplant recipients: single centre experience Dr Wong Lok Yan Ivy Background BK virus nephropathy (BKVN) has emerged as an important cause of renal graft dysfunction in recent
BK virus infection in renal transplant recipients: single centre experience Dr Wong Lok Yan Ivy Background BK virus nephropathy (BKVN) has emerged as an important cause of renal graft dysfunction in recent
Considering the early proactive switch from a CNI to an mtor-inhibitor (Case: Male, age 34) Josep M. Campistol
 Josep M. Campistol") Considering the early proactive switch from a CNI to an mtor-inhibitor (Case: Male, age 34) Josep M. Campistol Patient details Name DOB ESRD Other history Mr. B.I.B. 12 January 1975 (34yo) Membranous GN
Considering the early proactive switch from a CNI to an mtor-inhibitor (Case: Male, age 34) Josep M. Campistol Patient details Name DOB ESRD Other history Mr. B.I.B. 12 January 1975 (34yo) Membranous GN
American Journal of Transplantation 2009; 9 (Suppl 3): S1 S157 Wiley Periodicals Inc.
: S1 S157 Wiley Periodicals Inc.") American Journal of Transplantation 2009; 9 (Suppl 3): S1 S157 Wiley Periodicals Inc. 2009 The Authors Journal compilation 2009 The American Society of Transplantation and the American Society of Transplant
American Journal of Transplantation 2009; 9 (Suppl 3): S1 S157 Wiley Periodicals Inc. 2009 The Authors Journal compilation 2009 The American Society of Transplantation and the American Society of Transplant
HLA and Non-HLA Antibodies in Transplantation and their Management
 HLA and Non-HLA Antibodies in Transplantation and their Management Luca Dello Strologo October 29 th, 2016 Hystory I 1960 donor specific antibodies (DSA): first suggestion for a possible role in deteriorating
HLA and Non-HLA Antibodies in Transplantation and their Management Luca Dello Strologo October 29 th, 2016 Hystory I 1960 donor specific antibodies (DSA): first suggestion for a possible role in deteriorating
Strategies for Desensitization
 Strategies for Desensitization Olwyn Johnston MB, MRCPI, MD, MHSc BC Nephrology Day October 8 th 2010 Pre-transplant crossmatch (CMX) with donor lymphocytes has been standard of practice Positive CDC CXM
Strategies for Desensitization Olwyn Johnston MB, MRCPI, MD, MHSc BC Nephrology Day October 8 th 2010 Pre-transplant crossmatch (CMX) with donor lymphocytes has been standard of practice Positive CDC CXM
3/6/2017. Prevention of Complement Activation and Antibody Development: Results from the Duet Trial
 Prevention of Complement Activation and Antibody Development: Results from the Duet Trial Jignesh Patel MD PhD FACC FRCP Medical Director, Heart Transplant Cedars-Sinai Heart Institute Disclosures Name:
Prevention of Complement Activation and Antibody Development: Results from the Duet Trial Jignesh Patel MD PhD FACC FRCP Medical Director, Heart Transplant Cedars-Sinai Heart Institute Disclosures Name:
Belatacept: An Update of Ongoing Clinical Trials
 Belatacept: An Update of Ongoing Clinical Trials Michael D. Rizzari, MD University of Wisconsin Madison School of Medicine and Public Health, Madison, Wisconsin Abstract Belatacept is a fusion protein
Belatacept: An Update of Ongoing Clinical Trials Michael D. Rizzari, MD University of Wisconsin Madison School of Medicine and Public Health, Madison, Wisconsin Abstract Belatacept is a fusion protein
Efficacy and Safety of Thymoglobulin and Basiliximab in Kidney Transplant Patients at High Risk for Acute Rejection and Delayed Graft Function
 ArtIcle Efficacy and Safety of Thymoglobulin and Basiliximab in Kidney Transplant Patients at High Risk for Acute Rejection and Delayed Graft Function Guodong Chen, 1 Jingli Gu, 2 Jiang Qiu, 1 Changxi
ArtIcle Efficacy and Safety of Thymoglobulin and Basiliximab in Kidney Transplant Patients at High Risk for Acute Rejection and Delayed Graft Function Guodong Chen, 1 Jingli Gu, 2 Jiang Qiu, 1 Changxi
Intruduction PSI MODE OF ACTION AND PHARMACOKINETICS
 Multidisciplinary Insights on Clinical Guidance for the Use of Proliferation Signal Inhibitors in Heart Transplantation Andreas Zuckermann, MD et al. Department of Cardio-Thoracic Surgery, Medical University
Multidisciplinary Insights on Clinical Guidance for the Use of Proliferation Signal Inhibitors in Heart Transplantation Andreas Zuckermann, MD et al. Department of Cardio-Thoracic Surgery, Medical University
Case Report Beneficial Effect of Conversion to Belatacept in Kidney-Transplant Patients with a Low Glomerular-Filtration Rate
 Case Reports in Transplantation, Article ID 190516, 4 pages http://dx.doi.org/10.1155/2014/190516 Case Report Beneficial Effect of Conversion to Belatacept in Kidney-Transplant Patients with a Low Glomerular-Filtration
Case Reports in Transplantation, Article ID 190516, 4 pages http://dx.doi.org/10.1155/2014/190516 Case Report Beneficial Effect of Conversion to Belatacept in Kidney-Transplant Patients with a Low Glomerular-Filtration
Supporting a Pediatric Investigational Plan for Everolimus - Defining the extrapolation plan
 Supporting a Pediatric Investigational Plan for Everolimus - Defining the extrapolation plan Thomas Dumortier, Mick Looby Novartis Pharma AG, Basel, Switzerland EMA public workshop on extrapolation of
Supporting a Pediatric Investigational Plan for Everolimus - Defining the extrapolation plan Thomas Dumortier, Mick Looby Novartis Pharma AG, Basel, Switzerland EMA public workshop on extrapolation of
Should red cells be matched for transfusions to patients listed for renal transplantation?
 Should red cells be matched for transfusions to patients listed for renal transplantation? Dr M.Willicombe Imperial College Renal and Transplant Centre, Hammersmith Hospital Should red cells be matched
Should red cells be matched for transfusions to patients listed for renal transplantation? Dr M.Willicombe Imperial College Renal and Transplant Centre, Hammersmith Hospital Should red cells be matched
Immunopathology of T cell mediated rejection
 Immunopathology of T cell mediated rejection Ibrahim Batal MD Columbia University College of Physicians & Surgeons New York, NY, USA Overview Pathophysiology and grading of TCMR TCMR is still a significant
Immunopathology of T cell mediated rejection Ibrahim Batal MD Columbia University College of Physicians & Surgeons New York, NY, USA Overview Pathophysiology and grading of TCMR TCMR is still a significant
Why Do We Need New Immunosuppressive Agents
 Why Do We Need New Immunosuppressive Agents 1 Reducing acute rejection rates has not transplanted into better long-term graft survival Incidence of early acute rejection episodes by era Relative risk for
Why Do We Need New Immunosuppressive Agents 1 Reducing acute rejection rates has not transplanted into better long-term graft survival Incidence of early acute rejection episodes by era Relative risk for
OUT OF DATE. Choice of calcineurin inhibitors in adult renal transplantation: Effects on transplant outcomes
 nep_734.fm Page 88 Friday, January 26, 2007 6:47 PM Blackwell Publishing AsiaMelbourne, AustraliaNEPNephrology1320-5358 2006 The Author; Journal compilation 2006 Asian Pacific Society of Nephrology? 200712S18897MiscellaneousCalcineurin
nep_734.fm Page 88 Friday, January 26, 2007 6:47 PM Blackwell Publishing AsiaMelbourne, AustraliaNEPNephrology1320-5358 2006 The Author; Journal compilation 2006 Asian Pacific Society of Nephrology? 200712S18897MiscellaneousCalcineurin
Transplantation in highly sensitised patients treated with intravenous immunoglobulin and Rituximab
 ORIGINAL ARTICLE Advance Access publication 1 February 2010 Transplantation in highly sensitised patients treated with intravenous immunoglobulin and Rituximab Ana Carina Ferreira 1, Sandra Brum 1, Vasco
ORIGINAL ARTICLE Advance Access publication 1 February 2010 Transplantation in highly sensitised patients treated with intravenous immunoglobulin and Rituximab Ana Carina Ferreira 1, Sandra Brum 1, Vasco
Donor-Specific HLA Antibodies in a Cohort Comparing Everolimus With Cyclosporine After Kidney Transplantation
 American Journal of Transplantation 2012; 12: 1192 1198 Wiley Periodicals Inc. C Copyright 2012 The American Society of Transplantation and the American Society of Transplant Surgeons doi: 10.1111/j.1600-6143.2011.03961.x
American Journal of Transplantation 2012; 12: 1192 1198 Wiley Periodicals Inc. C Copyright 2012 The American Society of Transplantation and the American Society of Transplant Surgeons doi: 10.1111/j.1600-6143.2011.03961.x
Update on Transplant Glomerulopathy
 Update on Transplant Glomerulopathy Miklos Z Molnar, MD, PhD, FEBTM, FERA, FASN Associate Professor of Medicine Methodist University Hospital, Transplant Institute Division of Transplantation, Department
Update on Transplant Glomerulopathy Miklos Z Molnar, MD, PhD, FEBTM, FERA, FASN Associate Professor of Medicine Methodist University Hospital, Transplant Institute Division of Transplantation, Department
Liver Transplant Immunosuppression
 Liver Transplant Immunosuppression Michael Daily, MD, MS, FACS Surgical Director, Kidney and Pancreas Transplantation University of Kentucky Medical Center Disclosures No financial disclosures I will be
Liver Transplant Immunosuppression Michael Daily, MD, MS, FACS Surgical Director, Kidney and Pancreas Transplantation University of Kentucky Medical Center Disclosures No financial disclosures I will be
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 30 November 2011
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 30 November 2011 NULOJIX 250 mg, powder for concentrate for solution for infusion B/1 (CIP code: 580 415-7) B/2 (CIP
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 30 November 2011 NULOJIX 250 mg, powder for concentrate for solution for infusion B/1 (CIP code: 580 415-7) B/2 (CIP
Utility of protocol kidney biopsies for de novo donor- specific antibodies
 Received: 6 June 2017 Revised: 24 July 2017 Accepted: 29 July 2017 DOI: 10.1111/ajt.14466 BRIEF COMMUNICATION Utility of protocol kidney biopsies for de novo donor- specific antibodies Sandesh Parajuli
Received: 6 June 2017 Revised: 24 July 2017 Accepted: 29 July 2017 DOI: 10.1111/ajt.14466 BRIEF COMMUNICATION Utility of protocol kidney biopsies for de novo donor- specific antibodies Sandesh Parajuli
Clinical Study Different Impact of Pretransplant Anti-HLA Antibodies Detected by Luminex in Highly Sensitized Renal Transplanted Patients
 BioMed Research International Volume 2013, Article ID 738404, 5 pages http://dx.doi.org/10.1155/2013/738404 Clinical Study Different Impact of Pretransplant Anti-HLA Antibodies Detected by Luminex in Highly
BioMed Research International Volume 2013, Article ID 738404, 5 pages http://dx.doi.org/10.1155/2013/738404 Clinical Study Different Impact of Pretransplant Anti-HLA Antibodies Detected by Luminex in Highly
Alemtuzumab-based induction treatment versus basiliximab based induction treatment in kidney transplantation (the 3C Study): a randomised trial
: a randomised trial") Alemtuzumab-based induction treatment versus basiliximab based induction treatment in kidney transplantation (the 3C Study): a randomised trial Journal club Feb 2014 Background and Rationale Despite substantial
Alemtuzumab-based induction treatment versus basiliximab based induction treatment in kidney transplantation (the 3C Study): a randomised trial Journal club Feb 2014 Background and Rationale Despite substantial
Transfusion support in Transplantation
 Transfusion support in Transplantation Patricia Campbell University of Alberta Hospitals University of Alberta Objectives UofA transplant programs What we do and why? HLA and ABO incompatible transplants
Transfusion support in Transplantation Patricia Campbell University of Alberta Hospitals University of Alberta Objectives UofA transplant programs What we do and why? HLA and ABO incompatible transplants
APHERESIS FOR DESENSITIZATION OF NON-RENAL TRANSPLANTS
 APHERESIS FOR DESENSITIZATION OF NON-RENAL TRANSPLANTS GOW AREPALLY, MD MEDICAL DIRECTOR DUKE THERAPEUTIC APHERESIS SERVICE ASSOCIATE PROFESSOR, MEDICINE AMERICAN SOCIETY FOR APHERESIS MAY 25 TH 2013 OVERVIEW
APHERESIS FOR DESENSITIZATION OF NON-RENAL TRANSPLANTS GOW AREPALLY, MD MEDICAL DIRECTOR DUKE THERAPEUTIC APHERESIS SERVICE ASSOCIATE PROFESSOR, MEDICINE AMERICAN SOCIETY FOR APHERESIS MAY 25 TH 2013 OVERVIEW
For Immediate Release Contacts: Jenny Keeney Astellas US LLC (847)
") For Immediate Release Contacts: Jenny Keeney Astellas US LLC (847) 317-5405 Lauren McDonnell GolinHarris (312) 729-4233 ASTELLAS RECEIVES FDA APPROVAL FOR USE OF PROGRAF (TACROLIMUS) IN CONJUNCTION WITH
For Immediate Release Contacts: Jenny Keeney Astellas US LLC (847) 317-5405 Lauren McDonnell GolinHarris (312) 729-4233 ASTELLAS RECEIVES FDA APPROVAL FOR USE OF PROGRAF (TACROLIMUS) IN CONJUNCTION WITH
This study is currently recruiting participants.
 A Two Part, Phase 1/2, Safety, PK and PD Study of TOL101, an Anti-TCR Monoclonal Antibody for Prophylaxis of Acute Organ Rejection in Patients Receiving Renal Transplantation This study is currently recruiting
A Two Part, Phase 1/2, Safety, PK and PD Study of TOL101, an Anti-TCR Monoclonal Antibody for Prophylaxis of Acute Organ Rejection in Patients Receiving Renal Transplantation This study is currently recruiting
clevelandclinic.org/transplant
 carolyn spiotta Pancreas/Kidney Transplant Recipient I feel so fortunate and thankful that I have received a second chance at life. Carolyn Spiotta, 44, Pittsburgh. Carolyn needed a new pancreas and kidney
carolyn spiotta Pancreas/Kidney Transplant Recipient I feel so fortunate and thankful that I have received a second chance at life. Carolyn Spiotta, 44, Pittsburgh. Carolyn needed a new pancreas and kidney
Immunosuppression is now manageable in the
 EVOLVING STRATEGIES FOR IMMUNOSUPPRESSION IN RENAL TRANSPLANTATION: A REVIEW OF RECENT CLINICAL TRIALS* Stephen J. Tomlanovich, MD, Thomas C. Pearson, MD, DPhil, and Lorenzo Gallon, MD ABSTRACT When using
EVOLVING STRATEGIES FOR IMMUNOSUPPRESSION IN RENAL TRANSPLANTATION: A REVIEW OF RECENT CLINICAL TRIALS* Stephen J. Tomlanovich, MD, Thomas C. Pearson, MD, DPhil, and Lorenzo Gallon, MD ABSTRACT When using
Long-term prognosis of BK virus-associated nephropathy in kidney transplant recipients
 Original Article Kidney Res Clin Pract 37:167-173, 2018(2) pissn: 2211-9132 eissn: 2211-9140 https://doi.org/10.23876/j.krcp.2018.37.2.167 KIDNEY RESEARCH AND CLINICAL PRACTICE Long-term prognosis of BK
Original Article Kidney Res Clin Pract 37:167-173, 2018(2) pissn: 2211-9132 eissn: 2211-9140 https://doi.org/10.23876/j.krcp.2018.37.2.167 KIDNEY RESEARCH AND CLINICAL PRACTICE Long-term prognosis of BK
How to improve long term outcome after liver transplantation?
 How to improve long term outcome after liver transplantation? François Durand Hepatology & Liver Intensive Care University Paris Diderot INSERM U1149 Hôpital Beaujon, Clichy PHC 2018 www.aphc.info Long
How to improve long term outcome after liver transplantation? François Durand Hepatology & Liver Intensive Care University Paris Diderot INSERM U1149 Hôpital Beaujon, Clichy PHC 2018 www.aphc.info Long
Belatacept: An Opportunity to Personalize Immunosuppression? Andrew Adams MD/PhD Emory Transplant Center
 Belatacept: An Opportunity to Personalize Immunosuppression? Andrew Adams MD/PhD Emory Transplant Center Disclosure Research Funding from BMS. Learning Objectives -Define belatacept-resistant rejection
Belatacept: An Opportunity to Personalize Immunosuppression? Andrew Adams MD/PhD Emory Transplant Center Disclosure Research Funding from BMS. Learning Objectives -Define belatacept-resistant rejection
3/6/2017. Treatment of Detected Antibodies. I have financial relationship(s) with: Thoratec/St. Jude/Abbott Consultant CareDx Consultant/Speaker
 with: Thoratec/St. Jude/Abbott Consultant CareDx Consultant/Speaker") Treatment of Detected Antibodies Sean Pinney, MD Director, Advanced Heart Failure & Transplantation Mount Sinai Hospital New York, NY Sean Pinney, MD Associate Professor of Medicine Icahn School of Medicine
Treatment of Detected Antibodies Sean Pinney, MD Director, Advanced Heart Failure & Transplantation Mount Sinai Hospital New York, NY Sean Pinney, MD Associate Professor of Medicine Icahn School of Medicine
Practical considerations for the use of mtor inhibitors
 Diekmann and Campistol Transplantation Research 2015, 4(Suppl 1):5 DOI 10.1186/s13737-015-0029-5 TRANSPLANTATION RESEARCH REVIEW Practical considerations for the use of mtor inhibitors Fritz Diekmann 1,2*
Diekmann and Campistol Transplantation Research 2015, 4(Suppl 1):5 DOI 10.1186/s13737-015-0029-5 TRANSPLANTATION RESEARCH REVIEW Practical considerations for the use of mtor inhibitors Fritz Diekmann 1,2*
Effects of Tacrolimus Pharmacokinetic Variability on Acute Rejection and Long-Term Graft Function after Kidney Transplantation
 : Journal of Student Solutions to Pharmacy Challenges Volume 1 Issue 1 Article 4 2017 Effects of Tacrolimus Pharmacokinetic Variability on Acute Rejection and Long-Term Graft Function after Kidney Transplantation
: Journal of Student Solutions to Pharmacy Challenges Volume 1 Issue 1 Article 4 2017 Effects of Tacrolimus Pharmacokinetic Variability on Acute Rejection and Long-Term Graft Function after Kidney Transplantation
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Lefaucheur C, Loupy A, Vernerey D, et al. Antibody-mediated
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Lefaucheur C, Loupy A, Vernerey D, et al. Antibody-mediated
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/1887/29755 holds various files of this Leiden University dissertation. Author: Moes, Dirk Jan Alie Roelof Title: Optimizing immunosuppression with mtor inhibitors
Cover Page The handle http://hdl.handle.net/1887/29755 holds various files of this Leiden University dissertation. Author: Moes, Dirk Jan Alie Roelof Title: Optimizing immunosuppression with mtor inhibitors
Pleiotropic effects of mtor inhibitors : cardiovascular and cancer. Dr Paolo Malvezzi Clinique de Néphrologie CHU Grenoble
 Pleiotropic effects of mtor inhibitors : cardiovascular and cancer Dr Paolo Malvezzi Clinique de Néphrologie CHU Grenoble Tehran August 2016 Why this topic? Since last year very little news in the immunosuppressive
Pleiotropic effects of mtor inhibitors : cardiovascular and cancer Dr Paolo Malvezzi Clinique de Néphrologie CHU Grenoble Tehran August 2016 Why this topic? Since last year very little news in the immunosuppressive
Reduced graft function (with or without dialysis) vs immediate graft function a comparison of long-term renal allograft survival
 vs immediate graft function a comparison of long-term renal allograft survival") Nephrol Dial Transplant (2006) 21: 2270 2274 doi:10.1093/ndt/gfl103 Advance Access publication 22 May 2006 Original Article Reduced graft function (with or without dialysis) vs immediate graft function
Nephrol Dial Transplant (2006) 21: 2270 2274 doi:10.1093/ndt/gfl103 Advance Access publication 22 May 2006 Original Article Reduced graft function (with or without dialysis) vs immediate graft function
Long-term complications after kidney transplantation. Adnan Sharif
 Long-term complications after kidney transplantation Adnan Sharif RA guidelines (2011) KDIGO guidelines (2009) Long-term complications after kidney transplantation ATC 2013 abstracts Outline Patient/Graft
Long-term complications after kidney transplantation Adnan Sharif RA guidelines (2011) KDIGO guidelines (2009) Long-term complications after kidney transplantation ATC 2013 abstracts Outline Patient/Graft
Le migliori strategie immunosoppressive per il paziente con re-trapianto Prof. Maurizio Salvadori FIRENZE
 Le migliori strategie immunosoppressive per il paziente con re-trapianto Prof. Maurizio Salvadori FIRENZE Best Therapy for Kidney Re- Transplantation? PREVENTION!!!! Registries CTS OPTN UNOS USRDS SRTR
Le migliori strategie immunosoppressive per il paziente con re-trapianto Prof. Maurizio Salvadori FIRENZE Best Therapy for Kidney Re- Transplantation? PREVENTION!!!! Registries CTS OPTN UNOS USRDS SRTR
Le Rejet Humoral Chronique en 2010: Histoire naturelle et problématiques
 Le Rejet Humoral Chronique en 2010: Histoire naturelle et problématiques CAMR in 2010: natural history and perspectives Alexandre Loupy 1 Introduction 2 CAMR: the missing link 3 Natural history of CAMR
Le Rejet Humoral Chronique en 2010: Histoire naturelle et problématiques CAMR in 2010: natural history and perspectives Alexandre Loupy 1 Introduction 2 CAMR: the missing link 3 Natural history of CAMR
Posttransplant Human Leukocyte Antigen Antibodies in Stable Kidney Transplant Recipients
 Trends in Transplant. 2014;8:3-9 Gregor Bartel, Georg A. Böhmig: Alloantibodies and Graft Function Posttransplant Human Leukocyte Antigen Antibodies in Stable Kidney Transplant Recipients Gregor Bartel
Trends in Transplant. 2014;8:3-9 Gregor Bartel, Georg A. Böhmig: Alloantibodies and Graft Function Posttransplant Human Leukocyte Antigen Antibodies in Stable Kidney Transplant Recipients Gregor Bartel
Diagnosis and Management of Acute and Chronic Humoral Rejection. Lars Pape
 Diagnosis and Management of Acute and Chronic Humoral Rejection Lars Pape Immunosuppression Acute rejection Chronic rejection Side effects Infections Nephrotoxicity Adult population Nearly all late rejection-related
Diagnosis and Management of Acute and Chronic Humoral Rejection Lars Pape Immunosuppression Acute rejection Chronic rejection Side effects Infections Nephrotoxicity Adult population Nearly all late rejection-related
Pulmonary AMR Therapeutic Options & Strategies: The Old and the New. Ramsey Hachem, MD March 28, 2017
 Pulmonary AMR Therapeutic Options & Strategies: The Old and the New Ramsey Hachem, MD March 28, 2017 Disclosures Ramsey Hachem I have no financial relations with any relevant commercial interests I will
Pulmonary AMR Therapeutic Options & Strategies: The Old and the New Ramsey Hachem, MD March 28, 2017 Disclosures Ramsey Hachem I have no financial relations with any relevant commercial interests I will
Precision Medicine and not Individualized Therapy is Required for Successful Novel Drug Development
 Precision Medicine and not Individualized Therapy is Required for Successful Novel Drug Development 1 Disclosures F Vincenti University of California San Francisco, San Francisco, United States I have
Precision Medicine and not Individualized Therapy is Required for Successful Novel Drug Development 1 Disclosures F Vincenti University of California San Francisco, San Francisco, United States I have
Serum samples from recipients were obtained within 48 hours before transplantation. Pre-transplant
 SDC, Patients and Methods Complement-dependent lymphocytotoxic crossmatch test () Serum samples from recipients were obtained within 48 hours before transplantation. Pre-transplant donor-specific CXM was
SDC, Patients and Methods Complement-dependent lymphocytotoxic crossmatch test () Serum samples from recipients were obtained within 48 hours before transplantation. Pre-transplant donor-specific CXM was
Post-Transplant Monitoring for the Development of Anti-Donor HLA Antibodies
 Post-Transplant Monitoring for the Development of Anti-Donor HLA Antibodies Lorita M Rebellato, Ph.D., D (ABHI) Associate Professor Department of Pathology The Brody School of Medicine at ECU Scientific
Post-Transplant Monitoring for the Development of Anti-Donor HLA Antibodies Lorita M Rebellato, Ph.D., D (ABHI) Associate Professor Department of Pathology The Brody School of Medicine at ECU Scientific
2017 BANFF-SCT Joint Scientific Meeting. Personalized Medicine in Liver Transplantation
 2017 BANFF-SCT Joint Scientific Meeting Personalized Medicine in Liver Transplantation Miquel Navasa Liver Transplant Unit. Hospital Clínic. Barcelona. Barcelona, March 2017 Disclosures Consultant for
2017 BANFF-SCT Joint Scientific Meeting Personalized Medicine in Liver Transplantation Miquel Navasa Liver Transplant Unit. Hospital Clínic. Barcelona. Barcelona, March 2017 Disclosures Consultant for
Does the formulation of tacrolimus matter?
 Does the formulation of tacrolimus matter? This promotional meeting has been fully funded and organised by Astellas Pharma Ltd and Astellas products will be discussed. PI can be found at the end of this
Does the formulation of tacrolimus matter? This promotional meeting has been fully funded and organised by Astellas Pharma Ltd and Astellas products will be discussed. PI can be found at the end of this
PRETRANSPLANT IMMUNOLOGIC RISK ASSESMENT FOR IMMUNOSUPPRESSIVE MANAGEMENT
 PRETRANSPLANT IMMUNOLOGIC RISK ASSESMENT FOR IMMUNOSUPPRESSIVE MANAGEMENT OF KIDNEY TRANSPLANT RECIPIENTS Enver Akalin, M.D. Professor of Clinical Medicine and Surgery Albert Einstein College of Medicine
PRETRANSPLANT IMMUNOLOGIC RISK ASSESMENT FOR IMMUNOSUPPRESSIVE MANAGEMENT OF KIDNEY TRANSPLANT RECIPIENTS Enver Akalin, M.D. Professor of Clinical Medicine and Surgery Albert Einstein College of Medicine
Dix ans de transplantation rénale Fonds Boussard
 Dix ans de transplantation rénale Fonds Boussard Groupe Spiesser A.T.N. Christophe Legendre, Hôpital Necker & Université Paris Descartes, Paris Fondation Day-Solvay Actualités Néphrologiques Jean Hamburger
Dix ans de transplantation rénale Fonds Boussard Groupe Spiesser A.T.N. Christophe Legendre, Hôpital Necker & Université Paris Descartes, Paris Fondation Day-Solvay Actualités Néphrologiques Jean Hamburger
Predictors of cardiac allograft vasculopathy in pediatric heart transplant recipients
 Pediatr Transplantation 2013: 17: 436 440 2013 John Wiley & Sons A/S. Pediatric Transplantation DOI: 10.1111/petr.12095 Predictors of cardiac allograft vasculopathy in pediatric heart transplant recipients
Pediatr Transplantation 2013: 17: 436 440 2013 John Wiley & Sons A/S. Pediatric Transplantation DOI: 10.1111/petr.12095 Predictors of cardiac allograft vasculopathy in pediatric heart transplant recipients
Emerging Drug List EVEROLIMUS
 Generic (Trade Name): Manufacturer: Everolimus (Certican ) Novartis Pharmaceuticals NO. 57 MAY 2004 Indication: Current Regulatory Status: Description: Current Treatment: Cost: Evidence: For use with cyclosporine
Generic (Trade Name): Manufacturer: Everolimus (Certican ) Novartis Pharmaceuticals NO. 57 MAY 2004 Indication: Current Regulatory Status: Description: Current Treatment: Cost: Evidence: For use with cyclosporine
Kidney transplantation 2016: current status and potential challenges
 Kidney transplantation 2016: current status and potential challenges 15/12/2016 BVN-SBN : State-of-the-Art on Kidney Transplantation Patrick Peeters Ghent University Hospital, Belgium Challenges in 2016
Kidney transplantation 2016: current status and potential challenges 15/12/2016 BVN-SBN : State-of-the-Art on Kidney Transplantation Patrick Peeters Ghent University Hospital, Belgium Challenges in 2016
CKD in Other Organ Transplants
 CKD in Other Organ Transplants Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney and Pancreas Transplant Programs University of Colorado
CKD in Other Organ Transplants Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney and Pancreas Transplant Programs University of Colorado
Proteinuria and Mammalian Target of Rapamycin Inhibitors in Renal Transplantation
 Trends Fritz in Transplant. Diekmann: 2011;5:139-43 Proteinuria and Mammalian Target of Rapamycin Inhibitors in Renal Transplantation Proteinuria and Mammalian Target of Rapamycin Inhibitors in Renal Transplantation
Trends Fritz in Transplant. Diekmann: 2011;5:139-43 Proteinuria and Mammalian Target of Rapamycin Inhibitors in Renal Transplantation Proteinuria and Mammalian Target of Rapamycin Inhibitors in Renal Transplantation
Trends in immune function assay (ImmuKnow; Cylexä) results in the first year post-transplant and relationship to BK virus infection
 results in the first year post-transplant and relationship to BK virus infection") 2565 Nephrol Dial Transplant (2012) 27: 2565 2570 doi: 10.1093/ndt/gfr675 Advance Access publication 13 December 2011 Trends in immune function assay (ImmuKnow; Cylexä) results in the first year post-transplant
2565 Nephrol Dial Transplant (2012) 27: 2565 2570 doi: 10.1093/ndt/gfr675 Advance Access publication 13 December 2011 Trends in immune function assay (ImmuKnow; Cylexä) results in the first year post-transplant
Ten-year outcomes in a randomized phase II study of kidney transplant recipients administered belatacept 4-weekly or 8-weekly
 Ten-year outcomes in a randomized phase II study of kidney transplant recipients administered belatacept 4-weekly or 8-weekly F. Vincenti, University of California, San Francisco G. Blancho, University
Ten-year outcomes in a randomized phase II study of kidney transplant recipients administered belatacept 4-weekly or 8-weekly F. Vincenti, University of California, San Francisco G. Blancho, University
Kidney Allograft Fibrosis and Atrophy Early After Living Donor Transplantation
 American Journal of Transplantation 2005; 5: 1130 1136 Blackwell Munksgaard Copyright C Blackwell Munksgaard 2005 doi: 10.1111/j.1600-6143.2005.00811.x Kidney Allograft Fibrosis and Atrophy Early After
American Journal of Transplantation 2005; 5: 1130 1136 Blackwell Munksgaard Copyright C Blackwell Munksgaard 2005 doi: 10.1111/j.1600-6143.2005.00811.x Kidney Allograft Fibrosis and Atrophy Early After
BK Viral Infection and Malignancy in Renal Transplantation ~A Case History~
 BK Viral Infection and Malignancy in Renal Transplantation ~A Case History~ Mariko Toyoda, MD Department of Nephrology, Japanese Red Cross Kumamoto Hospital Statement of Disclosure The author does not
BK Viral Infection and Malignancy in Renal Transplantation ~A Case History~ Mariko Toyoda, MD Department of Nephrology, Japanese Red Cross Kumamoto Hospital Statement of Disclosure The author does not
2017 BANFF-SCT Joint Scientific Meeting. BARCELONA March 2017
 2017 BANFF-SCT Joint Scientific Meeting BARCELONA 27-31 March 2017 Adriana Zeevi PhD (D) ABHI Professor of Pathology, Surgery and Immunology Director of Histocompatibility Laboratory University of Pittsburgh
2017 BANFF-SCT Joint Scientific Meeting BARCELONA 27-31 March 2017 Adriana Zeevi PhD (D) ABHI Professor of Pathology, Surgery and Immunology Director of Histocompatibility Laboratory University of Pittsburgh
Rita R. Alloway: Consultant/member of advisory board for Veloxis Pharmaceuticals, Astellas, Sanofi, and Amgen; Speaker s bureau for Sanofi.
 Immunology/Transplantation PRN Focus Session Novel Approaches to Immunomodulation After Transplantation Activity Number: 0217-0000-15-129-L01-P, 1.50 hours of CPE credit; Activity Type: A Knowledge-Based
Immunology/Transplantation PRN Focus Session Novel Approaches to Immunomodulation After Transplantation Activity Number: 0217-0000-15-129-L01-P, 1.50 hours of CPE credit; Activity Type: A Knowledge-Based
DISCLOSURES LESS OR NONE? SAFE OR SORRY? Consulting EARLY VERSUS LATE OUTCOMES AFTER LIVER TRANSPLANTATION
 IS IT EVER SAFE TO DISCONTINUE IMMUNOSUPPRESSION AFTER PEDIATRIC LIVER TRANSPLANTATION? LESS OR NONE? SAFE OR SORRY? Sandy Feng, MD, PhD University of California San Francisco NASPGHAN Washington DC October
IS IT EVER SAFE TO DISCONTINUE IMMUNOSUPPRESSION AFTER PEDIATRIC LIVER TRANSPLANTATION? LESS OR NONE? SAFE OR SORRY? Sandy Feng, MD, PhD University of California San Francisco NASPGHAN Washington DC October
Induction of donor-specific hyporesponsiveness after renal. transplantation. Long term follow-up
 Induction of donor-specific hyporesponsiveness after renal transplantation. Long term follow-up Marc Lúcia, Oriol Bestard, Marcel la Franquesa, Josep M Cruzado, Montse Gomà, Núria Bolaños, Gema Cerezo,
Induction of donor-specific hyporesponsiveness after renal transplantation. Long term follow-up Marc Lúcia, Oriol Bestard, Marcel la Franquesa, Josep M Cruzado, Montse Gomà, Núria Bolaños, Gema Cerezo,
BK Virus (BKV) Management Guideline: July 2017
 Management Guideline: July 2017") BK Virus (BKV) Management Guideline: July 2017 BK virus has up to a 60-80% seroprevalence rate in adults due to a primary oral or respiratory exposure in childhood. In the immumocompromised renal transplant
BK Virus (BKV) Management Guideline: July 2017 BK virus has up to a 60-80% seroprevalence rate in adults due to a primary oral or respiratory exposure in childhood. In the immumocompromised renal transplant
The common premise for immunosuppressive
 therapy update Current trends in immunosuppressive therapies for renal transplant recipients The common premise for immunosuppressive therapies in kidney transplantation is to use multiple agents to work
therapy update Current trends in immunosuppressive therapies for renal transplant recipients The common premise for immunosuppressive therapies in kidney transplantation is to use multiple agents to work
Pharmacology notes Interleukin-2 receptor-blocking monoclonal antibodies: evaluation of 2 new agents
 BUMC Proceedings 1999;12:110-112 Pharmacology notes Interleukin-2 receptor-blocking monoclonal antibodies: evaluation of 2 new agents CHERYLE GURK-TURNER, RPH Department of Pharmacy Services, BUMC wo mouse/human
BUMC Proceedings 1999;12:110-112 Pharmacology notes Interleukin-2 receptor-blocking monoclonal antibodies: evaluation of 2 new agents CHERYLE GURK-TURNER, RPH Department of Pharmacy Services, BUMC wo mouse/human
Simultaneous Pancreas Kidney Transplantation:
 Simultaneous Pancreas Kidney Transplantation: What is the added advantage, and for whom? Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney
Simultaneous Pancreas Kidney Transplantation: What is the added advantage, and for whom? Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney
Statement of Disclosure
 Statement of Disclosure Mark Haas serves as a paid consultant on pathology adjudication committees for two industry-sponsored clinical trials: Shire ViroPharma Treatment of Acute ABMR AstraZeneca Treatment
Statement of Disclosure Mark Haas serves as a paid consultant on pathology adjudication committees for two industry-sponsored clinical trials: Shire ViroPharma Treatment of Acute ABMR AstraZeneca Treatment
The Banff Classification for Diagnosis of Renal Allograft Rejection: Updates from the 2017 Banff Conference
 The Banff Classification for Diagnosis of Renal Allograft Rejection: Updates from the 2017 Banff Conference Mark Haas Cedars-Sinai Medical Center Los Angeles, California, USA Statement of Disclosure Mark
The Banff Classification for Diagnosis of Renal Allograft Rejection: Updates from the 2017 Banff Conference Mark Haas Cedars-Sinai Medical Center Los Angeles, California, USA Statement of Disclosure Mark
Virtual Crossmatch in Kidney Transplantation
 Virtual Crossmatch in Kidney Transplantation Shiva Samavat Associate Professor of Nephrology Labbafinejad Hospital SBMU 2018.11.21 All transplant candidates are screened to determine the degree of humoral
Virtual Crossmatch in Kidney Transplantation Shiva Samavat Associate Professor of Nephrology Labbafinejad Hospital SBMU 2018.11.21 All transplant candidates are screened to determine the degree of humoral
The New Kidney Allocation System: What You Need to Know. Anup Patel, MD Clinical Director Renal and Pancreas Transplant Division Barnabas Health
 The New Kidney Allocation System: What You Need to Know Anup Patel, MD Clinical Director Renal and Pancreas Transplant Division Barnabas Health ~6% of patients die each year on the deceased donor waiting
The New Kidney Allocation System: What You Need to Know Anup Patel, MD Clinical Director Renal and Pancreas Transplant Division Barnabas Health ~6% of patients die each year on the deceased donor waiting
Eculizumab chez les receveurs de greffe rénal à haut risque immunologique. Mark D. Stegall Mayo Clinic, Rochester, MN
 Eculizumab chez les receveurs de greffe rénal à haut risque immunologique Mark D. Stegall Mayo Clinic, Rochester, MN Disclosure. Dr Mark Stegall. Institution : Mayo Clinic, Rochester. Research contracts
Eculizumab chez les receveurs de greffe rénal à haut risque immunologique Mark D. Stegall Mayo Clinic, Rochester, MN Disclosure. Dr Mark Stegall. Institution : Mayo Clinic, Rochester. Research contracts