Complicações Metabólicas e Ósseas da Infecção pelo HIV: Sugar and Bones
|
|
|
- Eileen Robbins
- 6 years ago
- Views:
Transcription
1 Slide 1 Complicações Metabólicas e Ósseas da Infecção pelo HIV: Sugar and Bones Todd T. Brown, MD, PhD Associate Professor of Medicine and Epidemiology Division of Endocrinology, Diabetes, & Metabolism Johns Hopkins University Baltimore, Maryland, USA
2 Slide 2 Disclosures Dr Brown has served as a consultant to Gilead, ViiV Healthcare, Merck, Abbvie, EMD-Serono, and Theratechnologies.
3 Endocrine and Metabolic Conditions are Prevalent Among HIV-infected Persons Slide 3 HIV Osteoporosis Diabetes Mellitus Dyslipidemia Hypogonadism
4 Endocrine and Metabolic Conditions are Prevalent Among HIV-infected Persons Slide 4 HIV Osteoporosis Diabetes Mellitus Dyslipidemia Hypogonadism Aging
5 Endocrine and Metabolic Conditions are Prevalent Among HIV-infected Persons Slide 5 HIV Inflammation Osteoporosis Diabetes Mellitus Dyslipidemia Hypogonadism Aging
6 Endocrine and Metabolic Conditions are Prevalent Among HIV-infected Persons Slide 6 HIV Osteoporosis Diabetes Mellitus Dyslipidemia Hypogonadism Fracture CVD Frailty Aging
7 Slide 7 Objective To know the optimal evaluation and treatment of endocrine and metabolic problems in HIV-infected patients, focusing on osteoporosis and diabetes mellitus
8 Bones Slide 8


9 Fragility Fractures in Women Slide 9 and Men over 50 years Wasnich RD, Osteoporos Int 1997;7 Suppl 3:68-72 Images from the National Osteoporosis Foundation
10 Fracture Prevalence/100 Persons Fracture Prevalence/100 Persons Fracture Prevalence in HIV-infected and non-hiv-infected Persons in MGH/Partners Healthcare System: Slide P=0.002 (overall comparison) P< (overall comparison) HIV Women Non-HIV HIV Men Non-HIV 8,525 HIV-infected 2,208,792 non HIV-infected patients Triant, JCEM,
11 Prevalence of Osteoporosis in HIVinfected Patients vs HIV-uninfected Controls: A Meta-analysis Overall prevalence of osteoporosis in HIV-infected patients 15% Study Odds ratio (95% CI) Slide 11 Amiel (2004) Brown (2004) Bruera (2003) Dolan (2004) Huang (2002) Knobel (2001) Loiseau-Peres (2002) Madeddu (2004) Tebas (2000) Teichman (2003) Yin (2005) Overall (95% CI) 5.03 (1.47,17.27) 4.26 (0.22,82.64) 4.51 (0.26,79.27) 2.11 (0.54,8.28) 3.52 (0.15,81.92) 5.13 (1.80,14.60) 4.28 (0.46,39.81) (1.80,494.92) 3.40 (0.19,61.67) (0.97,313.73) 2.37 (1.09,5.16) 3.68 (2.31,5.84) Brown, AIDS, Odds ratio 11
12 Pathophysiology and Risk Factors Slide 12 HIV Disease Factors Inflammation and Viral Proteins bone resorption bone formation Medication Factors Tenofovir (TDF) Certain PIs ART initiation ( 2-6% over 96 weeks) 12
13 Pathophysiology and Risk Factors Patient-Related Factors Low Body Weight Smoking Alcohol Use Opiate Use Hepatitis C Co-infection Physical Inactivity Hypogonadism Low Vitamin D Slide 13 13
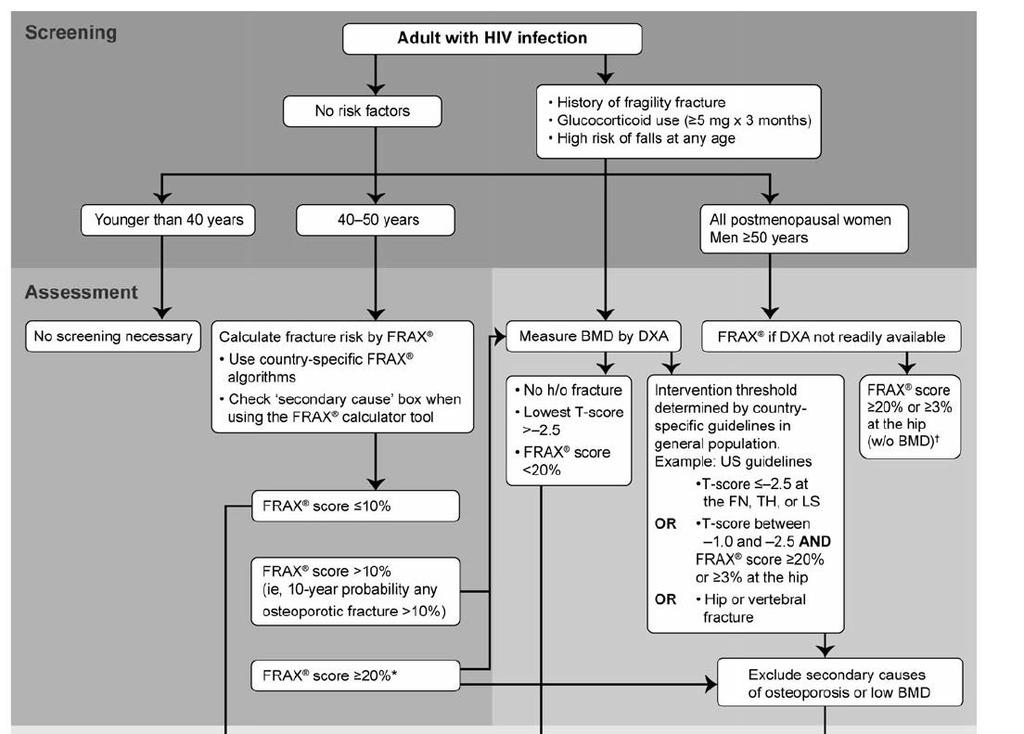
14 Slide 14 To Screen or Not to Screen. DXA DXA 14
15 Slide 15 Case Presentation: AD 62 year old white male referred to LD clinic for body fat changes HIV diagosed in 1987, nadir CD4 22, from 1997 to 2002 on d4t/3tc/idv, currently TDF/FTC/EFV Hypogonadism on transdermal testosterone COPD (60 pack-year tobacco history), multiple steroid courses No history of fracture, no height loss 15
16 Slide 16 US National Osteoporosis Foundation (NOF) Guidelines for DXA Screening Those with a fragility fracture after age 50 Women 65 yrs, Men 70 yrs Younger postmenopausal women and men years with clinical risk factors for fracture Adults with a condition (e.g., rheumatoid arthritis) or taking a medication (e.g., glucocorticoids in a daily dose 5 mg prednisone or equivalent for three months) associated with low bone mass or bone loss 16


17 Recommendations for DXA Slide 17 Screening in Brazil
18 Slide 18
19 Slide
20 Slide 20 Case Presentation: AD Dual X-ray Absorptiometry T-score L1-L4-2.2 Femoral Neck -2.2 Total Hip
21 Slide 21 Definitions Functional Definition (DXA)- WHO Definition Osteoporosis: T-score < -2.5 Osteopenia: T-score= -1.0 to -2.5 Normal: T-score > -1.0 Risk of fracture by x for each SD decrease Caveats: Z-score ( <-2.0) used in men < 50 years and premenopausal women BMD explains only about 50% of fracture risk 21
22 Slide 22 Secondary Causes of Low BMD Vitamin D deficiency 25 OH Vit D Hyperparathyroidism PTH, Ca++ Subclinical Hyperthyroidism TSH Hypogonadism Males: Free Testosterone Phosphate wasting Fractional Excretion of Phosphate Idiopathic Hypercalciuria 24 hr Urinary Calcium Celiac Sprue Tissue Transglutaminase Multiple Myeloma Serum Protein Electrophoresis Mastocytosis Serum Tryptase Cushing s Syndrome 24 hr Urinary Free Cortisol
23 Secondary Causes of Low BMD Vitamin D deficiency 25 OH Vit D Phosphate wasting Fractional Excretion of Phosphate Slide 23 23
24 Slide 24 Osteomalacia Impaired bone mineralization Accompanied by weakness, fracture, pain, anorexia, and weight loss Treated with Vitamin D, Ca++, +/- phosphate, not bisphosphonates Most important differential diagnosis for low BMD 24
25 US NOF Guidelines: Who to Treat* Slide 25 Those with hip or vertebral fractures Those with BMD T-scores -2.5 at the femoral neck, total hip, or spine by DXA Those with T-score b/t -1 and -2.5 (osteopenia) at above sites AND 10- year hip fracture probability 3% or 10- year all major osteoporosis-related fracture 20% based on FRAX model *applies to post-menopausal women and men 50 years 25

26 Slide

27 Slide 27 27
28 Management Options Slide 28 General recommendations Calcium/vitamin D supplementation Smoking cessation, Alcohol reduction Weight-bearing exercise Assess fall risk (Are you worried about falling?) Strength/Balance Training Rx options Bisphosphonates Selective estrogen receptor modulator Estrogen PTH analogue
29 Considerations When Choosing Between Bisphosphonates Slide 29 Alendronate Risedronate Ibandronate Zoledronate Efficacy Cost (1 year) $350 $350 $1200 $1100 Compliance (oral)/ + (IV) + GI Side Effects Yes (20%) Yes (20%) Yes (oral)/no(iv) Osteonecrosis of the Jaw Acute Phase Reaction No Yes Yes Yes Yes No No No (oral)/yes(iv) Yes (~10%) Atrial Fibrillation???? Esophageal Cancer Atypical Femoral Fracture??? No Yes Yes Yes Yes 29
30 Would you switch him off of Slide 30 TDF? 1. Yes 2. No

31 ART Management Slide 31
32 OsteoTDF Study Switch from TDF to ABC in Osteopenia/Osteoporosis Changes in Spine and Hip BMD at Week 48 Two-centered, randomized pilot study in virologically suppressed subjects receiving TDF with osteopenia/osteoporosis. Twenty six subjects switched to ABC and 28 continued TDF. Slide 32 In this small cohort, switching from TDF to ABC resulted in increases in hip and decreases in spine BMD at week 48. Negredo E, et al. J of Antimicrob Chemother. E-published August 13, doi: /jac/dku300.
. Changes in Spine and Hip BMD at Week 48 3.0% 2.5% P <0.001 P <0.")
33 Mean % Change from BL at Week 48 TROP Study (Switch): TDF to RAL Switch from TDF to ABC in Osteopenia/Osteoporosis Changes in Spine and Hip BMD at Week 48 Slide 33 Open-label, non-randomized study comparing BMD changes at week 48 in patients with osteopenia/osteoporosis at baseline on TDF, switching to RAL with boosted PI (N=37). Changes in Spine and Hip BMD at Week % 2.5% P <0.001 P <0.001 * Left total hip In this small switch cohort, there are increases in spine and hip BMD at week 48. Bloch M, et al. HIV Medicine 2014;15:
34 Median % Change (Q1,Q3) From Baseline Change in Spine and Hip Bone Mineral Density BMD Changes From Baseline to W e ek 48 Spine Hip 6 E/C/F/TAF % p <0.001* 2 0.9% p <0.001* Weeks E/C/F/TAF n= Weeks Median percentage changes (Q1, Q3) in hip and spine BMD from baseline to Week 48 were 0.9% (-0.3, 2.7) and 1.9% (-0.3, 4.3), respectively *Two-sided Wilcoxon signed-rank test. Posniak, CROI,
35 Diabetes Slide 35
36 Slide 36 Why Care about Diabetes? Very common with rapidly increasing prevalence One of leading causes of cardiovascular disease, blindness, ESRD, amputations, hospitalizations Common in HIV-infected Populations Diabetes can be controlled, but management is complicated and requires individualization

37 Slide 37 Diabetes Prevalence in Brazil Almeida-Pititto, Diabetes, Met Syn, Obesity, 2015
38 Slide 38 Pathogenesis of Diabetes in HIV-infected Patients Antiretroviral Medication Factors Thymidine analogues, older PIs HIV Factors Residual immune activation/inflammation Host Factors Adiposity HCV Genetic Factors: Family History, Race Concomitant Medications: Corticosteroids/Aytpical Antipsychotics
39 Slide 39 Case 53 year-old African American Male, HIV+ for 20 years, on ART since 2000 HIV RNA< 50 FTC/TDF/ EFV Mild/moderate lipoatrophy of face/buttocks/thighs Mild HTN, Normal lipids, no smoking Strong family history of DM BMI 27 kg/m 2
40 Slide 40 Diabetes Screening Who? IDSA: Prior to ART, within 4-6 weeks after ART initiation, every 6-12 months thereafter
41 Slide 41 Caveats for the use of HgbA1c for diagnosis For conditions with abnormal red cell turnover.., the diagnosis of diabetes must employ glucose criteria exclusively ADA Clinical Practice Recommendations, 2016
42 Glucose (mg/dl) Slide 42 HbA1c Underestimates Glycemia in HIV-infected Persons HIV (n=100) Control (n=200) mmol/l Kim, Diabetes Care, 2009 HBA1C (%)
43 Slide 43 How? Fasting Glucose Diabetes Screening in HIVinfected Persons If mmol/l ( mg/dl), consider 75 g OGTT Avoid A1c for screening (particularly in those on ABC, low CD4, PIs, high MCV)
44 Case 53 year-old African American Male, HIV+ for 20 years, on ART since 2000 VL< 50 FTC/TDF/ EFV Mild/moderate lipoatrophy of face/buttocks/thighs Mild HTN, Normal lipids, no smoking Strong family history of DM BMI 27 kg/m 2 Fasting Glucose 8.05 mmol/l (145 mg/dl) (confirmed) A1c 6.8% Slide 44
45 Slide 45 After DM is diagnosed, what should be the next steps? Lifestyle Modification First-line Drug Combination Therapy
46 Cumulative Incidence of Diabetes (%) Lifestyle Modifications for Slide 46 Prediabetes Diabetes Prevention Program: 150 minutes/week of exercise and caloric restriction goal: 7% weight loss 58% diabetes incidence Lifestyle Placebo Year 4.5 Knowler WC, et al. N Engl J Med. 2002;346:

47 Slide 47 Effect of Cutting 500 cal/day over 8 weeks in Obese Persons Effect on Weight Effect on Inflammation Hermana, Endocrine, 2009
48 Slide 48 After DM is diagnosed, what should be the next steps? Lifestyle Modification First-line Drug Combination Therapy


49 Slide 49 Metformin: THE First Line Drug
50 Slide 50 Metformin: Pros and Cons Pros A1c ~1% Long Track Record No Hypoglycemia No Weight Gain? CVD benefit Cons GI side effects Lactic Acidosis (rare) Contraindications: CKD (Scr>1.4 in women, 1.5 men) Hypoxia Decompensated Liver Disease Severe CHF Alcohol Abuse Past H/O Lactic Acidosis? Worsening Lipoatrophy

51 Slide 51 After DM is diagnosed, what should be the next steps? Lifestyle Modification First-line Drug Combination Therapy
52 Slide 52 What drug to add next? Sulfonylureas Glitazones (Pioglitazone) Insulin GLP-1 Analogues DPP-IV Inhibitors SGLT-2 Inhibitors Incretins
53 Slide 53 Sulfonylureas: Pros and Cons Pros A1c ~1% Long Track Record Microvascular Events Cost* ($7/month) Cons Weight Gain Hypoglycemia High Failure Rate *lowest price for average dose 30 day fill at goodrx.com
54 Slide 54 Pioglitazone: Pros and Cons Pros A1c ~1% No Hypoglycemia? CVD benefit HDL, TGs Liver Fat? Inflammation Low Failure Rate Modest effect on lipoatrophy Cons Weight Gain Fluid Retention/CHF Macular Edema Osteoporosis/Fracture Bladder Cancer (~ g)
55 Slide 55 Insulin: Pros and Cons Pros A1c: Unlimited Microvascular events Cons Hypoglycemia Weight Gain? Mitogenic effects Injectable
56 Slide 56 Starting Insulin in Type 2 DM Start with bedtime glargine, detemir, or NPH (10-15 units, increase by 2-3 units q 3 days until fasting is < 6.6 mmol/l (120 mg/dl)) Add prandial insulin if not at goal. Recommended as first line if A1c >9%, severe liver disease/kidney disease, hypertriglyceridemia


57 Slide 57 GLP-1 Effects in Humans: Understanding the Glucoregulatory Role of Incretins GLP-1 secreted upon the ingestion food Promotes satiety and reduces appetite Alpha cells: Postprandial glucagon secretion Beta cells: Enhances glucosedependent insulin secretion Liver: Glucagon reduces hepatic glucose output Stomach: Helps regulate gastric emptying Adapted from Flint A, et al. J Clin Invest. 1998;101: ; Adapted from Larsson H, et al. Acta Physiol Scand. 1997;160: ; Adapted from Nauck MA, et al. Diabetologia. 1996;39: ; Adapted from Drucker DJ. Diabetes. 1998;47:
58 Slide 58 Incretins GLP-1 Analogues exenetide (Byetta) liraglutide (Victoza) Exenetide LAR (Bydureon) dulagltide (Trulicity) albiglutide (Tanzeum) Lixisenatide (Lyxumia) DPP-IV Inhibitors sitagliptin (Januvia) saxagliptin (Onglyza) vildagliptin (Galvus) linagliptin (Trajenta) alogliptin
59 Slide 59 GLP-1 Analogues: Pros and Cons Pros A1c ~1% No Hypoglycemia Weight Loss? Inflammation? CVD benefit Cons GI Side Effects? Pancreatitis/ Pancreatic Cancer Risk
60 DPP-IV Inhibitors: Pros and Slide 60 Cons Pros No hypoglycemia Weight Neutral? Inflammation Cons A1c ~0.5% GI Side Effects? Pancreatitis/ Pancreatic Cancer Risk Hypersensitivity reaction No CVD benefit Heart Failure
 Lowers BP No hypoglycemia urinary tract infections/candidiasis Polyuria/dehydration DKA risk?")
61 Slide 61 Sodium Glucose Co-transporter 2 Inhibition: The gliflozins Insulin-independent reduction in glucose dapaglifozin canagliflozin empagliflozin 0.5-1% A1c reductions Weight loss (~2kg) Lowers BP No hypoglycemia urinary tract infections/candidiasis Polyuria/dehydration DKA risk? CVD benefit (empagliflozin, NEJM, 2015)
62 Slide 62 What drug to add next? Sulfonylureas Glitazones (Pioglitazone) Insulin GLP-1 Analogues Incretins DPP-IV Inhibitors SGLT-2 Inhibitors
63 Questions How should I diagnose diabetes in the HIVinfected patient? After the diagnosis is made, what should be the next steps? What should be the glycemic target? What else should I be doing to prevent complications? Slide 63
64 Slide 64 What should be the glycemic target? < 7%

65 UKPDS: MI and Microvascular Endpoints Associated With Increasing HbA 1c Slide 65
66 Meta-Analysis of Glycemic Slide 66 Control and CVD in Diabetes 10% Risk Reduction for CVD No Benefit on CVD Mortality 2-fold Increase Risk of Severe Hypoglycemia with Intensive Control Kelly, Annals of Int Med, 2009
67 Slide 67 Previous Tight DM Control and CVD: The Legacy Effect 10 Year Follow-Up: UKPDS Study Blood Sugar Control in Follow-up Risk of MI over 10 years of Follow-up Holman, NEJM, 2008
68 Slide 68 A1c Goal < 7% Individualization is Key: Tighter Control (A1c %): Younger, Healthier Looser Control (A1c %+): Older, Hypoglycemia Prone, Co-morbidities
69 What else should I be doing to prevent Slide 69 complications?: Microvascular Retinopathy: Yearly ophthalmologic exams Nephropathy: BP Control Spot Urine Microalbumin every 6-12 months ACE-I/ARB with microalbuminuria or HTN Lipid Control Neuropathy: Foot exams every 6-12 months Instruction in foot care Podiatry if evidence of neuropathy
70 What else should I be doing to prevent Slide 70 complications?: Macrovascular Attention to all CV risk factors A: Anti-platelet therapy B: Blood pressure C: Cholesterol D: Diabetes/Glucose Management S: Smoking Cessation Steno-2 Trial (Gaede, NEJM, 2003): CV Events by 50% with intensive control of all CV Risk Factors
71 Slide 71 Conclusions Osteoporosis DXA screening in HIVinfected patients in men > 50 yrs and postmenopausal women Treatment guidelines should follow those established for the general population Remember secondary causes Consider switches of TDF in those at higher risk Diabetes Regular DM screening Avoid A1c for diagnosis Lifestyle changes are critical Metformin first Individualize 2 nd and 3 rd line-drugs Goal < 7% in most, but should be individualized Multiprong approach to prevent complications
Diabetes Risk Assessment and Treatment
 Diabetes Risk Assessment and Treatment Todd T. Brown, MD, PhD Professor of Medicine and Epidemiology Division of Endocrinology, Diabetes, & Metabolism Johns Hopkins University Baltimore, Maryland, USA
Diabetes Risk Assessment and Treatment Todd T. Brown, MD, PhD Professor of Medicine and Epidemiology Division of Endocrinology, Diabetes, & Metabolism Johns Hopkins University Baltimore, Maryland, USA
Type 2 Diabetes: Where Do We Start with Treatment? DIABETES EDUCATION. Diabetes Mellitus: Complications and Co-Morbid Conditions
 Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
HIV and Bone Disease: Through Thick and Thin! Pablo Tebas, MD
 HIV and Bone Disease: Through Thick and Thin! Pablo Tebas, MD April 30 th, 2016 Disclosures I serve in an adjudication panel in a VZV vaccine study (Glaxo) I consult for Merck My research is supported
HIV and Bone Disease: Through Thick and Thin! Pablo Tebas, MD April 30 th, 2016 Disclosures I serve in an adjudication panel in a VZV vaccine study (Glaxo) I consult for Merck My research is supported
Chief of Endocrinology East Orange General Hospital
 Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
HIV and Metabolic Cases
 HIV and Metabolic Cases Amita Gupta MD, MHS Associate Professor of Medicine & International Health Deputy Director Johns Hopkins Center for Clinical Global Health Disclosures None Receive grant funding
HIV and Metabolic Cases Amita Gupta MD, MHS Associate Professor of Medicine & International Health Deputy Director Johns Hopkins Center for Clinical Global Health Disclosures None Receive grant funding
Management of Type 2 Diabetes
 Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
Wayne Gravois, MD August 6, 2017
 Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
The Death of Sulfonylureas? A Review of New Diabetes Medications
 The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
TYP 2 DIABETES. Marc Donath
 TYP 2 DIABETES Marc Donath Treatment of Typ 2 Diabetes GLP-1 Anti-IL-1β Insulin sulfonylureas Metformin UCP-1 IL-1β Sport SGLT2i Bariatric surgery Cardiomyocytes Control Glucose Dyntar et al. Diabetes
TYP 2 DIABETES Marc Donath Treatment of Typ 2 Diabetes GLP-1 Anti-IL-1β Insulin sulfonylureas Metformin UCP-1 IL-1β Sport SGLT2i Bariatric surgery Cardiomyocytes Control Glucose Dyntar et al. Diabetes
Update Diabetes Therapie. Marc Y Donath
 Update Diabetes Therapie Marc Y Donath Recent CV outcome studies in Diabetes N Engl J Med. 2015 373:2117-28 (Empa-Reg outcome study) N Engl J Med. 2016 June 13 (LEADER trial) N Engl J Med. 2017 June 12
Update Diabetes Therapie Marc Y Donath Recent CV outcome studies in Diabetes N Engl J Med. 2015 373:2117-28 (Empa-Reg outcome study) N Engl J Med. 2016 June 13 (LEADER trial) N Engl J Med. 2017 June 12
Prevalence of Comorbidities among HIV-positive patients in Taiwan
 Prevalence of Comorbidities among HIV-positive patients in Taiwan Chien-Ching Hung, MD, PhD Department of Internal Medicine National Taiwan University Hospital, Taipei, Taiwan % of participants Comorbidity
Prevalence of Comorbidities among HIV-positive patients in Taiwan Chien-Ching Hung, MD, PhD Department of Internal Medicine National Taiwan University Hospital, Taipei, Taiwan % of participants Comorbidity
Diabetes Mellitus II CPG
 1 Diabetes Mellitus II CPG Candidates for Screening Integrated Complex Care Patients: Check Yearly Prediabetes: Check Yearly No Diabetes Mellitus (DM) Risk Factors: Check at Age 45, Repeat Every 3 Years
1 Diabetes Mellitus II CPG Candidates for Screening Integrated Complex Care Patients: Check Yearly Prediabetes: Check Yearly No Diabetes Mellitus (DM) Risk Factors: Check at Age 45, Repeat Every 3 Years
A Practical Approach to the Use of Diabetes Medications
 A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
NEW DIABETES CARE MEDICATIONS
 NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
New Treatments for Type 2 diabetes. Nandini Seevaratnam April 2016 Rushcliffe Patient Forum
 New Treatments for Type 2 diabetes Nandini Seevaratnam April 2016 Rushcliffe Patient Forum Overview Growing population of Type 2 diabetes Basic science on what goes wrong Current treatments Why there is
New Treatments for Type 2 diabetes Nandini Seevaratnam April 2016 Rushcliffe Patient Forum Overview Growing population of Type 2 diabetes Basic science on what goes wrong Current treatments Why there is
Management of Diabetes
 Management of Diabetes Mellitus: Which Drugs for Which Patients? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu Disclosure No relevant financial relationships
Management of Diabetes Mellitus: Which Drugs for Which Patients? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu Disclosure No relevant financial relationships
Diabetes Treatment Update
 Diabetes Treatment Update Timothy C. Evans, MD PhD FACP University of Washington Department of Medicine Disclosure: Dr. Evans has no significant financial interest in any of the products or manufacturers
Diabetes Treatment Update Timothy C. Evans, MD PhD FACP University of Washington Department of Medicine Disclosure: Dr. Evans has no significant financial interest in any of the products or manufacturers
Navigating the New Options for the Management of Type 2 Diabetes
 Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
New and Emerging Therapies for Type 2 DM
 Dale Clayton MHSc, MD, FRCPC Dalhousie University/Capital Health April 28, 2011 New and Emerging Therapies for Type 2 DM The science of today, is the technology of tomorrow. Edward Teller American Physicist
Dale Clayton MHSc, MD, FRCPC Dalhousie University/Capital Health April 28, 2011 New and Emerging Therapies for Type 2 DM The science of today, is the technology of tomorrow. Edward Teller American Physicist
Individualizing Type 2 Diabetes Management. Cynthia Gerstenlauer, ANP-BC, GCNS-BC, CDE, CCD
 Individualizing Type 2 Diabetes Management Cynthia Gerstenlauer, ANP-BC, GCNS-BC, CDE, CCD Harsh Statistics 30.3 million (9.4% of population) in US had DM in 2015 The percent of population with DM increases
Individualizing Type 2 Diabetes Management Cynthia Gerstenlauer, ANP-BC, GCNS-BC, CDE, CCD Harsh Statistics 30.3 million (9.4% of population) in US had DM in 2015 The percent of population with DM increases
Should Psychiatrists be diagnosing (and treating) metabolic syndrome
 metabolic syndrome") Should Psychiatrists be diagnosing (and treating) metabolic syndrome David Hopkins Clinical Director, Diabetes King s College Hospital, London Diabetes prevalence (thousands) Diabetes in the UK: 1995-2010
Should Psychiatrists be diagnosing (and treating) metabolic syndrome David Hopkins Clinical Director, Diabetes King s College Hospital, London Diabetes prevalence (thousands) Diabetes in the UK: 1995-2010
CURRENT ISSUES IN DIABETES MANAGEMENT. Screening for Diabetes Advantages of HbA1c as a Diagnostic Test. Diagnosis of Diabetes 2013
 CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening for Diabetes 2013 BMI
CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening for Diabetes 2013 BMI
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS
 IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
6/1/2018. Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE
 Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE 1 2 3 Sulfonylureas Glipizide Glyburide Glimeperide 4 Metformin Gold
Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE 1 2 3 Sulfonylureas Glipizide Glyburide Glimeperide 4 Metformin Gold
Newer Drugs in the Management of Type 2 Diabetes Mellitus
 Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Disclosure. Learning Objectives. Case. Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare
 Disclosure Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare Spring Therapeutics Update 2011 CSHP BC Branch Anar Dossa BScPharm Pharm D CDE April 20, 2011
Disclosure Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare Spring Therapeutics Update 2011 CSHP BC Branch Anar Dossa BScPharm Pharm D CDE April 20, 2011
Diabetes Mellitus: Implications of New Clinical Trials and New Medications
 Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Professor Rudy Bilous James Cook University Hospital
 Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Management of Diabetes Mellitus: A Primary Care Perspective. Screening for Diabetes Advantages of HbA1c as a Diagnostic Test
 Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Management of Diabetes Mellitus: A Primary Care Perspective
 Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable?
 Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes
 Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes Obesity (BMI 30 kg/m 2 ) 1994 2000 2009 No Data 26.0% Diabetes 1994 2000 2009
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes Obesity (BMI 30 kg/m 2 ) 1994 2000 2009 No Data 26.0% Diabetes 1994 2000 2009
CURRENT CONTROVERSIES IN DIABETES CARE
 CURRENT CONTROVERSIES IN DIABETES CARE Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Diabetes Mellitus: U.S. Impact
CURRENT CONTROVERSIES IN DIABETES CARE Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Diabetes Mellitus: U.S. Impact
Diabesity. Metabolic dysfunction that ranges from mild blood glucose imbalance to full fledged Type 2 DM Signs
 Diabesity Metabolic dysfunction that ranges from mild blood glucose imbalance to full fledged Type 2 DM Signs Abdominal obesity Low HDL, high LDL, and high triglycerides HTN High blood glucose (F>100l,
Diabesity Metabolic dysfunction that ranges from mild blood glucose imbalance to full fledged Type 2 DM Signs Abdominal obesity Low HDL, high LDL, and high triglycerides HTN High blood glucose (F>100l,
Cardiovascular Management of a Patient with Diabetes
 Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
Management of Type 2 Diabetes Mellitus. Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism
 Management of Type 2 Diabetes Mellitus Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism Disclosures Working for Intermountain Healthcare Some of the views represented are the opinion of ABIM-certified
Management of Type 2 Diabetes Mellitus Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism Disclosures Working for Intermountain Healthcare Some of the views represented are the opinion of ABIM-certified
Type 2 Diabetes Novel Therapies and Difficult Cases
 Type 2 Diabetes Novel Therapies and Difficult Cases Matt Dowell, DO Type 2 Diabetes - An Epidemic Is Here 1 Age-Adjusted Prevalence of Diagnosed Diabetes Among US Adults 2005 Missing data
Type 2 Diabetes Novel Therapies and Difficult Cases Matt Dowell, DO Type 2 Diabetes - An Epidemic Is Here 1 Age-Adjusted Prevalence of Diagnosed Diabetes Among US Adults 2005 Missing data
Overview T2DM medications. Winnie Ho
 Overview T2DM medications Winnie Ho Diabetes in Australia 1.7 million Australians with diabetes, of these 85% have T2DM 2-fold excess risk CV death in patients with diabetes Risk factor for progression
Overview T2DM medications Winnie Ho Diabetes in Australia 1.7 million Australians with diabetes, of these 85% have T2DM 2-fold excess risk CV death in patients with diabetes Risk factor for progression
TREATMENTS FOR TYPE 2 DIABETES. Susan Henry Diabetes Specialist Nurse
 TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
What s New in Diabetes Treatment. Disclosures
 What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
Side Effects of: GLP-1 agonists DPP-4 inhibitors SGLT-2 inhibitors. Bryce Fukunaga PharmD April 25, 2018
 Side Effects of: GLP-1 agonists DPP-4 inhibitors SGLT-2 inhibitors Bryce Fukunaga PharmD April 25, 2018 Objectives For each drug class: Identify the overall place in therapy Explain the mechanism of action
Side Effects of: GLP-1 agonists DPP-4 inhibitors SGLT-2 inhibitors Bryce Fukunaga PharmD April 25, 2018 Objectives For each drug class: Identify the overall place in therapy Explain the mechanism of action
Vipul Lakhani, MD Oregon Medical Group Endocrinology
 Vipul Lakhani, MD Oregon Medical Group Endocrinology Disclosures None Objectives Be able to diagnose diabetes and assess control Be able to identify appropriate classes of medications for diabetes treatment
Vipul Lakhani, MD Oregon Medical Group Endocrinology Disclosures None Objectives Be able to diagnose diabetes and assess control Be able to identify appropriate classes of medications for diabetes treatment
GLP-1 agonists. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
Multiple Small Feedings of the Mind: Diabetes. Sonja K Fredrickson, MD, BC-ADM March 7, 2014
 Multiple Small Feedings of the Mind: Diabetes Sonja K Fredrickson, MD, BC-ADM March 7, 2014 Question 1: Setting A1c Goals Describe the evidence based approach to determining the target HgbA1c in different
Multiple Small Feedings of the Mind: Diabetes Sonja K Fredrickson, MD, BC-ADM March 7, 2014 Question 1: Setting A1c Goals Describe the evidence based approach to determining the target HgbA1c in different
INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES
 INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES ARSHNA SANGHRAJKA DIABETES SPECIALIST PRESCRIBING PHARMACIST OBJECTIVES EXPLORE THE TYPES OF INSULIN AND INJECTABLE DIABETES TREATMENTS AND DEVICES AVAILABLE
INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES ARSHNA SANGHRAJKA DIABETES SPECIALIST PRESCRIBING PHARMACIST OBJECTIVES EXPLORE THE TYPES OF INSULIN AND INJECTABLE DIABETES TREATMENTS AND DEVICES AVAILABLE
Treatment Options for Diabetes: An Update
 Treatment Options for Diabetes: An Update A/Prof. Marg McGill Manager, Diabetes Centre Dr. Ted Wu Staff Specialist Endocrinologist Diabetes Centre Centre of Health Professional Education Education Provider
Treatment Options for Diabetes: An Update A/Prof. Marg McGill Manager, Diabetes Centre Dr. Ted Wu Staff Specialist Endocrinologist Diabetes Centre Centre of Health Professional Education Education Provider
Pathogenesis of Type 2 Diabetes
 9/23/215 Multiple, Complex Pathophysiological Abnmalities in T2DM incretin effect gut carbohydrate delivery & absption pancreatic insulin secretion pancreatic glucagon secretion HYPERGLYCEMIA? Pathogenesis
9/23/215 Multiple, Complex Pathophysiological Abnmalities in T2DM incretin effect gut carbohydrate delivery & absption pancreatic insulin secretion pancreatic glucagon secretion HYPERGLYCEMIA? Pathogenesis
Osteoporosis Screening and Treatment in Type 2 Diabetes
 Osteoporosis Screening and Treatment in Type 2 Diabetes Ann Schwartz, PhD! Dept. of Epidemiology and Biostatistics! University of California San Francisco! October 2011! Presenter Disclosure Information
Osteoporosis Screening and Treatment in Type 2 Diabetes Ann Schwartz, PhD! Dept. of Epidemiology and Biostatistics! University of California San Francisco! October 2011! Presenter Disclosure Information
What s the Goal? Individualizing Glycemic Targets. Matthew Freeby M.D. December 3 rd, 2016
 What s the Goal? Individualizing Glycemic Targets Matthew Freeby M.D. December 3 rd, 2016 Diabetes Mellitus: Complications and Co-Morbid Conditions Retinopathy Between 2005-2008, 28.5% of patients with
What s the Goal? Individualizing Glycemic Targets Matthew Freeby M.D. December 3 rd, 2016 Diabetes Mellitus: Complications and Co-Morbid Conditions Retinopathy Between 2005-2008, 28.5% of patients with
Diabetes 2016: Strategies for achieving optimal diabetes control
 PHASE Safety Net Community Benefit Diabetes 2016: Strategies for achieving optimal diabetes control Presented by: Lisa Gilliam, MD, PhD Clinical Leader Diabetes Program Kaiser Permanente Northern California
PHASE Safety Net Community Benefit Diabetes 2016: Strategies for achieving optimal diabetes control Presented by: Lisa Gilliam, MD, PhD Clinical Leader Diabetes Program Kaiser Permanente Northern California
DIABETES. Mary Bruskewitz APNP, MS, BC-ADM Clinical Nurse Specialist Diabetes. November 2013
 DIABETES Mary Bruskewitz APNP, MS, BC-ADM Clinical Nurse Specialist Diabetes November 2013 mbruskewitz@outlook.com Objectives Part 1 Overview of Endocrine Physiology Pathophysiology of Diabetes Diabetes
DIABETES Mary Bruskewitz APNP, MS, BC-ADM Clinical Nurse Specialist Diabetes November 2013 mbruskewitz@outlook.com Objectives Part 1 Overview of Endocrine Physiology Pathophysiology of Diabetes Diabetes
Newer and Expensive treatment of diabetes. Endocrinology Visiting Associate Professor Institute of Medicine TUTH
 Newer and Expensive treatment of diabetes Jyoti Bhattarai MD Endocrinology Visiting Associate Professor Institute of Medicine TUTH Four out of every five people with diabetes now live in developing countries.
Newer and Expensive treatment of diabetes Jyoti Bhattarai MD Endocrinology Visiting Associate Professor Institute of Medicine TUTH Four out of every five people with diabetes now live in developing countries.
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications
 Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
GLP-1-based therapies in the management of type 2 diabetes
 GLP-1-based therapies in the management of type 2 diabetes Makbul Aman Mansyur Division Endocrine & Metabolism Department of Internal Medicine Faculty of Medicine Hasanuddin University/ RSUP Dr. Wahidin
GLP-1-based therapies in the management of type 2 diabetes Makbul Aman Mansyur Division Endocrine & Metabolism Department of Internal Medicine Faculty of Medicine Hasanuddin University/ RSUP Dr. Wahidin
Comorbidities: a moving area. Paul De Munter ARC Leuven BREACH
 Comorbidities: a moving area Paul De Munter ARC Leuven BREACH 27-11-2015 Contents Introduction Comorbidities Cardiovascular disease and lipids Diabetes mellitus Hepatitis C Frailty Conclusion Introduction
Comorbidities: a moving area Paul De Munter ARC Leuven BREACH 27-11-2015 Contents Introduction Comorbidities Cardiovascular disease and lipids Diabetes mellitus Hepatitis C Frailty Conclusion Introduction
Clinical Practice Guidelines
 Clinical Practice Guidelines Diabetes Objective The purpose is to guide the appropriate diagnosis and management of Diabetes. This guideline is designed to assist the clinician by providing a framework
Clinical Practice Guidelines Diabetes Objective The purpose is to guide the appropriate diagnosis and management of Diabetes. This guideline is designed to assist the clinician by providing a framework
Osteoporosis/Fracture Prevention
 Osteoporosis/Fracture Prevention NATIONAL GUIDELINE SUMMARY This guideline was developed using an evidence-based methodology by the KP National Osteoporosis/Fracture Prevention Guideline Development Team
Osteoporosis/Fracture Prevention NATIONAL GUIDELINE SUMMARY This guideline was developed using an evidence-based methodology by the KP National Osteoporosis/Fracture Prevention Guideline Development Team
OSTEOPOROSIS: PREVENTION AND MANAGEMENT
 OSTEOPOROSIS: OVERVIEW OSTEOPOROSIS: PREVENTION AND MANAGEMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Key Risk factors Screening and Monitoring
OSTEOPOROSIS: OVERVIEW OSTEOPOROSIS: PREVENTION AND MANAGEMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Key Risk factors Screening and Monitoring
Comprehensive Diabetes Treatment
 Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Type 2 Diabetes Mellitus 2011
 2011 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetes Mellitus Diagnosis 2011 Diabetes Mellitus Fasting Glucose
2011 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetes Mellitus Diagnosis 2011 Diabetes Mellitus Fasting Glucose
What s New in Diabetes Medications. Jena Torpin, PharmD
 What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
NEW DEVELOPMENTS IN OSTEOPOROSIS: SCREENING, PREVENTION AND TREATMENT
 NEW DEVELOPMENTS IN OSTEOPOROSIS: SCREENING, PREVENTION AND TREATMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF OSTEOPOROSIS: OVERVIEW Definitions Risk factors
NEW DEVELOPMENTS IN OSTEOPOROSIS: SCREENING, PREVENTION AND TREATMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF OSTEOPOROSIS: OVERVIEW Definitions Risk factors
Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE. CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010
 Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE Robert R. Henry, MD Authors and Disclosures CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010 Introduction Type 2 diabetes
Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE Robert R. Henry, MD Authors and Disclosures CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010 Introduction Type 2 diabetes
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes
 Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
DIABETES UPDATE 2018
 DIABETES UPDATE 2018 Jerome V. Tolbert, M.D., Ph.D. Assistant Professor of Medicine Icahn School of Medicine at Mt. Sinai Division of Endocrinology and Bone Diseases 317 East 17 th Street New York, New
DIABETES UPDATE 2018 Jerome V. Tolbert, M.D., Ph.D. Assistant Professor of Medicine Icahn School of Medicine at Mt. Sinai Division of Endocrinology and Bone Diseases 317 East 17 th Street New York, New
CASE 1 WHY IS IT IMPORTANT TO TREAT? FACTS CONCERNS
 4:30-5:15pm Ask the Expert: Osteoporosis SPEAKERS Silvina Levis, MD OSTEOPOROSIS - FACTS 1:3 older women and 1:5 older men will have a fragility fracture after age 50 After 3 years of treatment, depending
4:30-5:15pm Ask the Expert: Osteoporosis SPEAKERS Silvina Levis, MD OSTEOPOROSIS - FACTS 1:3 older women and 1:5 older men will have a fragility fracture after age 50 After 3 years of treatment, depending
CURRENT ISSUES IN DIABETES MANAGEMENT
 CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening for Diabetes 2011 BMI
CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening for Diabetes 2011 BMI
Osteoporosis/Fracture Prevention Clinician Guide SEPTEMBER 2017
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Osteoporosis/Fracture Prevention Clinician Guide SEPTEMBER 2017 Introduction This Clinician Guide was developed to assist Primary Care physicians
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Osteoporosis/Fracture Prevention Clinician Guide SEPTEMBER 2017 Introduction This Clinician Guide was developed to assist Primary Care physicians
Medical therapy advances London/Manchester RCP February/June 2016
 Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Bone: To DEXA or not to DEXA. Michael Yin, MD MS Associate Professor of Medicine Columbia University Medical Center
 Bone: To DEXA or not to DEXA Michael Yin, MD MS Associate Professor of Medicine Columbia University Medical Center Learning Objectives Upon completion of this presentation, learners should be better able
Bone: To DEXA or not to DEXA Michael Yin, MD MS Associate Professor of Medicine Columbia University Medical Center Learning Objectives Upon completion of this presentation, learners should be better able
Mr Rab Burtun. Dr David Kim. 8:30-10:30 WS #2: Diabetes Basic 11:00-13:00 WS #9: Diabetes Basic (Repeated)
") Dr David Kim Endocrinologist and General Physician Waitemata DHB and Apollo Specialist Clinic Albany Auckland Mr Rab Burtun Diabetes Nurse Specialist Waitemata DHB Waitakere Hospital Auckland 8:30-10:30
Dr David Kim Endocrinologist and General Physician Waitemata DHB and Apollo Specialist Clinic Albany Auckland Mr Rab Burtun Diabetes Nurse Specialist Waitemata DHB Waitakere Hospital Auckland 8:30-10:30
Objectives. Kidney Complications With Diabetes. Case 10/21/2015
 Objectives Kidney Complications With Diabetes Brian Boerner, MD Diabetes, Endocrinology, and Metabolism University of Nebraska Medical Center Review screening for, and management of, albuminuria Review
Objectives Kidney Complications With Diabetes Brian Boerner, MD Diabetes, Endocrinology, and Metabolism University of Nebraska Medical Center Review screening for, and management of, albuminuria Review
Diabetes Meds Update Disclaimer and Important Info. Objectives. Page 1. Copyright , Diabetes Education Services
 Diabetes Meds Update 2016 Beverly Dyck Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Disclaimer and Important Info This content is for educational purposes only. Please see Package
Diabetes Meds Update 2016 Beverly Dyck Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Disclaimer and Important Info This content is for educational purposes only. Please see Package
Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Oral Agents. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
GLP-1 (glucagon-like peptide-1) Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary
 Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary") OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
Diabetes Mellitus case studies. Jana Vinklerová
 Diabetes Mellitus case studies Jana Vinklerová Definition of diabetes (metabolic disorder) Chronically raised blood glucose (hyperglycaemia) Insulin/Glucagon Insulin is responsible for lowering glucose
Diabetes Mellitus case studies Jana Vinklerová Definition of diabetes (metabolic disorder) Chronically raised blood glucose (hyperglycaemia) Insulin/Glucagon Insulin is responsible for lowering glucose
Current and Emerging Strategies for Osteoporosis
 Current and Emerging Strategies for Osteoporosis I have nothing to disclose. Anne Schafer, MD Assistant Professor of Medicine Division of Endocrinology & Metabolism December 12, 2014 Outline Osteoporosis
Current and Emerging Strategies for Osteoporosis I have nothing to disclose. Anne Schafer, MD Assistant Professor of Medicine Division of Endocrinology & Metabolism December 12, 2014 Outline Osteoporosis
TREATMENT OF DIABETES AFTER METFORMIN GREGG GERETY, MD ALBANY MEDICAL COLLEGE, DIVISION OF COMMUNITY ENDOCRINOLOGY JULY 14, 2017
 TREATMENT OF DIABETES AFTER METFORMIN GREGG GERETY, MD ALBANY MEDICAL COLLEGE, DIVISION OF COMMUNITY ENDOCRINOLOGY JULY 14, 2017 Outline Review treatment algorithms from ADA/ EASD & ACE/AACE. Review positive
TREATMENT OF DIABETES AFTER METFORMIN GREGG GERETY, MD ALBANY MEDICAL COLLEGE, DIVISION OF COMMUNITY ENDOCRINOLOGY JULY 14, 2017 Outline Review treatment algorithms from ADA/ EASD & ACE/AACE. Review positive
Update on Therapies for Type 2 Diabetes: Angela D. Mazza, DO July 31, 2015
 Update on Therapies for Type 2 Diabetes: 2015 Angela D. Mazza, DO July 31, 2015 Objectives To present the newer available therapies for the management of T2D To discuss the advantages and disadvantages
Update on Therapies for Type 2 Diabetes: 2015 Angela D. Mazza, DO July 31, 2015 Objectives To present the newer available therapies for the management of T2D To discuss the advantages and disadvantages
Dr Tahseen A. Chowdhury Royal London Hospital. New Guidelines in Diabetes: NICE or Nasty?
 Dr Tahseen A. Chowdhury Royal London Hospital New Guidelines in Diabetes: NICE or Nasty? I have no conflicts of interest I do not undertake talks / advisory bodies / research for any pharma company Consultant
Dr Tahseen A. Chowdhury Royal London Hospital New Guidelines in Diabetes: NICE or Nasty? I have no conflicts of interest I do not undertake talks / advisory bodies / research for any pharma company Consultant
John J. Wolf, DO Family Medicine
 John J. Wolf, DO Family Medicine Objectives: 1. Review incidence & Risk of Osteoporosis 2.Review indications for testing 3.Review current pharmacologic & Non pharmacologic Tx options 4.Understand & Utilize
John J. Wolf, DO Family Medicine Objectives: 1. Review incidence & Risk of Osteoporosis 2.Review indications for testing 3.Review current pharmacologic & Non pharmacologic Tx options 4.Understand & Utilize
Drug Class Review Newer Diabetes Medications and Combinations
 Drug Class Review Newer Diabetes Medications and Combinations Final Update 2 Report July 2016 The purpose reports is to make available information regarding the comparative clinical effectiveness and harms
Drug Class Review Newer Diabetes Medications and Combinations Final Update 2 Report July 2016 The purpose reports is to make available information regarding the comparative clinical effectiveness and harms
Diabetes Mellitus: A Cardiovascular Disease
 Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
The Diabetes Link to Heart Disease
 The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
Dept of Diabetes Main Desk
 Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
Advanced Practice Education Associates. Endocrine
 Advanced Practice Education Associates Endocrine Overview Diabetes Thyroid Disease 162 Copyright 2016 Advanced Practice Education Associates DIABETES MELLITUS What is the BMI cut point for screening adults
Advanced Practice Education Associates Endocrine Overview Diabetes Thyroid Disease 162 Copyright 2016 Advanced Practice Education Associates DIABETES MELLITUS What is the BMI cut point for screening adults
Diagnosis and Treatment of Osteoporosis: What s New and Controversial in ? What s New in Osteoporosis
 Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018-19? What s New in Osteoporosis The crisis in treatment and compliance Douglas C. Bauer, MD Professor of Medicine and Epidemiology
Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018-19? What s New in Osteoporosis The crisis in treatment and compliance Douglas C. Bauer, MD Professor of Medicine and Epidemiology
Non-insulin treatment in Type 1 DM Sang Yong Kim
 Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Alia Gilani Health Inequalities Pharmacist
 Alia Gilani Health Inequalities Pharmacist THE SOUTH ASIAN HEALTH FOUNDATION (U.K.) (Registered Charity No. 1073178) 1. Case Study 2. Factors influencing prescribing 3. Special Considerations 4. Prescribing
Alia Gilani Health Inequalities Pharmacist THE SOUTH ASIAN HEALTH FOUNDATION (U.K.) (Registered Charity No. 1073178) 1. Case Study 2. Factors influencing prescribing 3. Special Considerations 4. Prescribing
Bone Densitometry Pathway
 Bone Densitometry Pathway The goal of the Bone Densitometry pathway is to manage our diagnosed osteopenic and osteoporotic patients, educate and monitor the patient population at risk for bone density
Bone Densitometry Pathway The goal of the Bone Densitometry pathway is to manage our diagnosed osteopenic and osteoporotic patients, educate and monitor the patient population at risk for bone density
New Drugs for Diabetes
 NEW DRUGS FOR DIABETES Which Ones, For Which Patients? Disclosure Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu No relevant financial relationships
NEW DRUGS FOR DIABETES Which Ones, For Which Patients? Disclosure Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu No relevant financial relationships
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Page 1. Current and Emerging Strategies What s New in Osteoporosis. Osteoporosis. What is Osteoporosis? Traditional Risk Factors for Fracture
 Current and Emerging Strategies for Osteoporosis What s New in Osteoporosis Risk stratification Douglas C. Bauer, MD University of California, San Francisco Under recognition and poor compliance New potential
Current and Emerging Strategies for Osteoporosis What s New in Osteoporosis Risk stratification Douglas C. Bauer, MD University of California, San Francisco Under recognition and poor compliance New potential
Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol
 Agonists Drug Class Prior Authorization Protocol") Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Diabetes Management in CAD Patients. Stuart R. Chipkin, MD Research Professor School of Public Health and Health Sciences University of Massachusetts
 Diabetes Management in CAD Patients Stuart R. Chipkin, MD Research Professor School of Public Health and Health Sciences University of Massachusetts Disclosure Stuart R. Chipkin, MD, FACE Nothing to disclose
Diabetes Management in CAD Patients Stuart R. Chipkin, MD Research Professor School of Public Health and Health Sciences University of Massachusetts Disclosure Stuart R. Chipkin, MD, FACE Nothing to disclose
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES
 ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
Practical Diabetes. Nic Crook. (and don t use so many charts) Kuirau Specialists 1239 Ranolf Street Rotorua. Rotorua Hospital Private Bag 3023 Rotorua
 Kuirau Specialists 1239 Ranolf Street Rotorua. Rotorua Hospital Private Bag 3023 Rotorua") Practical Diabetes (and don t use so many charts) Nic Crook Rotorua Hospital Private Bag 3023 Rotorua Kuirau Specialists 1239 Ranolf Street Rotorua Worldwide rates of diabetes mellitus: predictions 80
Practical Diabetes (and don t use so many charts) Nic Crook Rotorua Hospital Private Bag 3023 Rotorua Kuirau Specialists 1239 Ranolf Street Rotorua Worldwide rates of diabetes mellitus: predictions 80
Page 1. Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018? What s New in Osteoporosis
 Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018? Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco What s
Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018? Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco What s