Mr Rab Burtun. Dr David Kim. 8:30-10:30 WS #2: Diabetes Basic 11:00-13:00 WS #9: Diabetes Basic (Repeated)
|
|
|
- Warren Marshall
- 5 years ago
- Views:
Transcription


1 Dr David Kim Endocrinologist and General Physician Waitemata DHB and Apollo Specialist Clinic Albany Auckland Mr Rab Burtun Diabetes Nurse Specialist Waitemata DHB Waitakere Hospital Auckland 8:30-10:30 WS #2: Diabetes Basic 11:00-13:00 WS #9: Diabetes Basic (Repeated)



2 Diabetes Workshop Topics Relevant in Primary Care: Basic David Kim Endocrinologist
3 Conflicts of interest Honorarium from: Sanofi Aventis Novo Nordisk
 or insulin resistance +/- deficiency (Type 2")
4 What is Diabetes? Disease characterised by impaired glucose metabolism with high blood glucose either due to insulin deficiency (Type 1 diabetes) or insulin resistance +/- deficiency (Type 2 diabetes) This high blood sugar may produce symptoms of thirst with polydipsia (increased drinking) and polyuria (increased urination) +/- weight loss and lethargy
5 What is Diabetes? Rusty Gates Insulin resistance Type 2 diabetes Not enough keys Insulin deficiency in Type 1 (+ many Type 2)

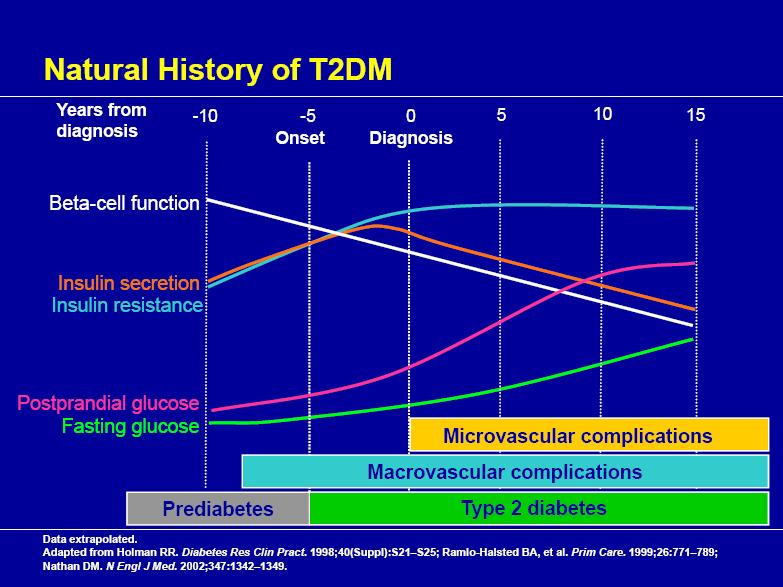
6 Type 2 Diabetes: Relevance to our practice An evolving epidemic 8% of adults in New Zealand believed to have type 2 diabetes Rate of growth slowing a little, and complication rate per patient decreasing However, prevalence of diabetes ~tripled in the last 20 years with overall burden of disease still growing

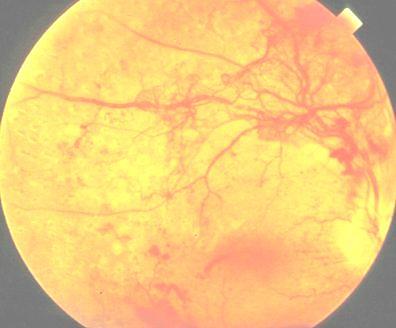





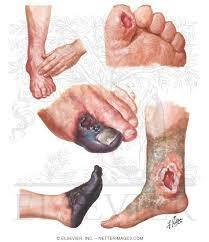
7 Why do we care about diabetes? Microvascular complications - Retinopathy - Nephropathy - Neuropathy Macrovascular complications - Coronary heart disease - Stroke - Peripheral vascular disease
8
 Lipid")
 with aim of TC <4.0-4.")
 Smoke cessation Aspirin in secondary prevention")
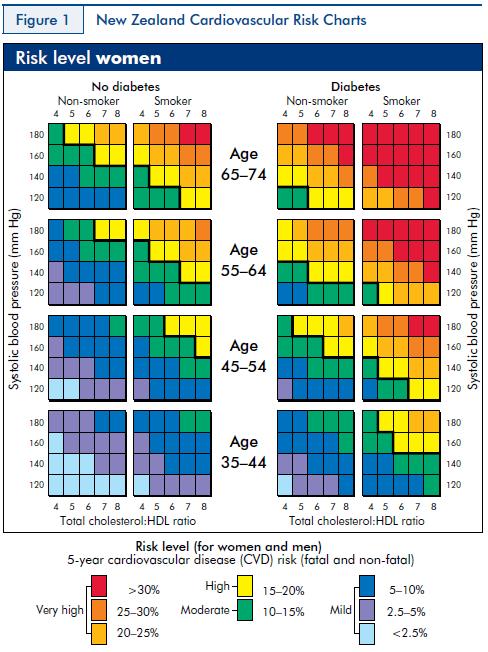
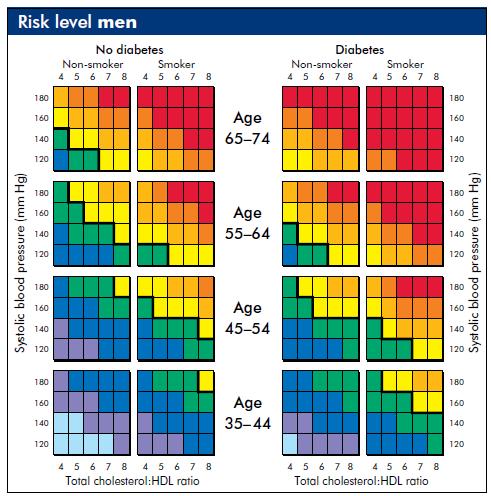
9 CVD Risk Management Summary Hypertension Rx with target blood pressure: / (ACE-i/ ARB first line) Lipid lowering Rx (i.e. Statin) in secondary prevention or high CVD risk (5 year CVD risk >15% ) with aim of TC < , LDL < (Statins) Smoke cessation Aspirin in secondary prevention or primary prevention in high CVD risk (5 year CVD risk >15% )
10 Why bother optimising HbA1c? EVERY 1% reduction in HbA 1c 1% Relative Risk N=3642 Diabetesrelated deaths Myocardial infarctions Microvascular complications Amputations or deaths from peripheral vascular disorders REDUCED RISK (P<0.0001) UKPDS=United Kingdom Prospective Diabetes Study. Data adjusted for age, sex, and ethnic group, expressed for white men aged years at diagnosis and with mean duration of diabetes of 10 years. Stratton IM et al. UKPDS 35. BMJ 2000;321:
11 Why bother optimising HbA1c? 10 YEARS AFTER UKPDS: Despite similar HbA1c between two groups post trial, benefits maintained, including CVD rates and mortality i.e. EARLY maintenance of glycaemic control matters (Legacy effect) Holman R et al, N Eng J Med 2008; 359:

12 Normal IGT Target for most acceptable in some Rx Augmentation Insulin initiation & intensification
13 Case 1: 46 y.o. overweight male with lethargy/ polyuria, otherwise well Fasting glucose 8.0mmol/L, HbA1c 58 mmol/mol Diagnosis & (glycaemic) management?
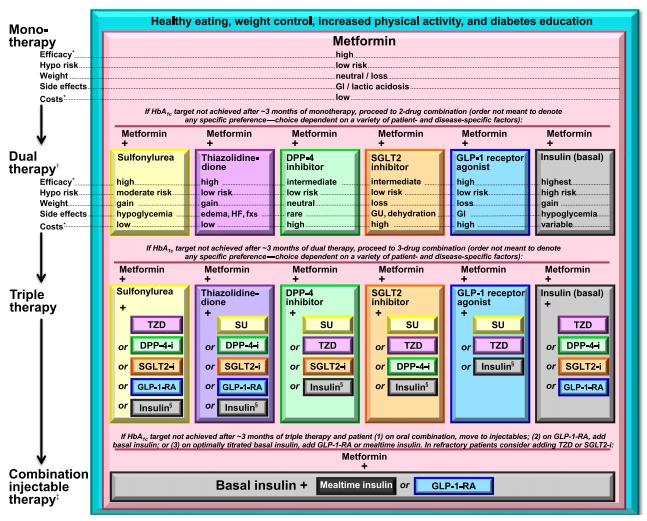
14 Metformin for all T2DM after/with lifestyle changes Pros: Weight neutral No hypoglycaemia mortality/ CVD risk May reduce cancer risk CG testing not mandatory Funded & cheap Cons: GI side-effect up to 10% Care if low egfr Care if risk of lactic acidosis e.g. critical illness/ sepsis BD/ TDS dosing
15 More on Metformin Start gently WITH FOOD (e.g. 500mg with dinner for a couple of days then 500mg BD) BD dosing as a rule, TDS dosing only for very compliant pt lunch time dose often forgotten! Titrate doses up to meet target HbA1c up to 1.5g BD (if small patient 1g BD) Dose reduction for those with egfr between (dose adjust to 850mg BD down to 500mg daily)
16 Case 2: 50 y.o. overweight male with T2DM for 4 years on metformin 1000mg mane, 1500mg nocte HbA1c now 65 mmol/mol adequate? Reasonable glycaemic target for this patient? Further glycaemic management?
17
18 Next step after Metformin - NZ version Diet & Exercise + Metformin Sulphonylurea Glipizide Gliclazide (glibenclamide) Insulin Pioglitazone or Acarbose DPP-4 inhibitor/ GLP-1 agent e.g. Sitagliptin Saxagliptin Exenatide SGLT-2 inhibitor e.g. Dapagliflozin
19 Sulphonylureas (Glipizide/ Gliclazide) Pros: Tried and true Works well with MF Funded/ cheap Cons: Hypoglyceamia, especially in elderly Weight gain? Earlier β-cell failure/ loss of effect after 5 10 years in some cases
20 Sulphonylureas Start lower dose Glipizide 2.5-5mg or Gliclazide 40-80mg 1-2 times a day Usually BD dosing with breakfast & dinner Max dose Glipizide 10mg BD/ Gliclazide 160 BD Capillary glucose testing to guide both initiation & up-titration of the regimen

21 Pioglitazone: PPAR-γ inhibitor Pros: Reduces insulin resistance HbA1c up to 10 mmol/mol Funded Once daily dosing Other favourable metabolic benefits Cons: Weight gain Ankle oedema in some Contraindicated in heart failure Osteoporosis esp. post menopausal women (# risk )
22 Pioglitazone Start at 15-30mg daily If target not achieved in 6-8 weeks, increase dose, up to 45mg daily (unless S/E) Watch out for heart failure especially in older/ those with cardiac Hx
23 Acarbose Reduces gut CHO absorption (α-glucosidase inhibitor) Minor role to play in T2DM in general Pros: Weight neutral No hypoglycaemia May reduce blood pressure & C.V. morbidity Funded Cons: G.I. side effects in many (flatulence) <5mmol/mol in HbA1c TDS or BD dosing

 GLP-1 is a gut hormone from the ileum which is reduced in type 2 diabetes.")
24 GLP-1 agents : GLP-1 analogues e.g. Exenatide (Byetta/ Bydureon) GLP-1 is a gut hormone from the ileum which is reduced in type 2 diabetes. Restoring GLP-1 levels leads to: insulin from ß cell Glucagon from α cell Gastric emptying Appetite Pros: HbA1c mmol/mol Weight loss No hypoglycaemia CVD risk reduction Cons: COST (>$250/mo) S.C. injection (BD, but possibly once weekly) Nausea (usually wears off)


25 GLP-1 agents : DPP4-inhibitors e.g. Sitagliptin (Januvia) / Saxagliptin (Onglyza) Inhibits DPP-IV enzyme that breaks down GLP-1 Pros: Once daily, oral prep. No hypoglycaemia Minimal S/E Weight neutral Cons: COST (~$100/mo) Modest efficacy HbA1c 5-10 mmol/mol

 Increased genitourinary")
26 SGLT-2 inhibitor Dapagliflozin (Forxiga) Works in the renal tubules to increase excretion of glucose in urine Pros: Once daily oral prep No hypoglycaemia Weight loss (modest) CVD risk reduction HbA1c 5-10 mmol/mol on average Cons: COST (~$100/mo) Increased genitourinary s/e
 : Acarbose GLP-1 agents: Exenatide/ DPP4-inhibitors SGLT-2 inhibitor Sulphonylureas (type 2 DM only) Insulin (both type 1 and type 2)")
27 Overview of Rx modes of action Not enough insulin Type 1 (+ many Type 2) Rusty Gates - Type 2 diabetes Diet & Exercise Metformin Pioglitazone Others for T2DM (rarely used) : Acarbose GLP-1 agents: Exenatide/ DPP4-inhibitors SGLT-2 inhibitor Sulphonylureas (type 2 DM only) Insulin (both type 1 and type 2)


28 Consider BARIATRIC SURGERY if: BMI > 35, age < 55, relatively short duration of diabetes, well motivated
29 Case 3: 55 y.o. overweight male with 9 year hx of T2DM on MF 1.5g BD, Gliclazide 160mg BD. HbA1c mmol/mol over past 6 months Why does this happen despite him seemingly adhering to treatment and lifestyle measures? What next?
30 Glycaemic control deteriorates over time UKPDS 34, Lancet 1998:352:854 65; Kahn et al (ADOPT), NEJM 2006;355:
31
32
 In type 2 diabetes start when: - Lifestyle optimised and oral agents maximised, yet high HbA1c: 60-65 mmol/mol in younger 65-70 mmol/mol in older Also consider starting in")
33 When to start insulin? (ALL type 1 diabetes) In type 2 diabetes start when: - Lifestyle optimised and oral agents maximised, yet high HbA1c: mmol/mol in younger mmol/mol in older Also consider starting in following situations: - On maximum metformin (2-3g/d) monotherapy with HbA1c >75mmol/mol (>9%) - HbA1c very high >95mmol/mol (>11%) - Uncertainty re: type 1 vs. type 2 diabetes Once insulin start is deemed necessary; JUST DO IT!

34 Insulins available on NZ Market


35 Lantus (insulin glargine) Sanofi Aventis Lepore M et al. Diabetes 2000;49: Lantus Data Sheet, 26 August 2010
 Sanofi")

36 Apidra (insulin glulisine) Sanofi Aventis Becker R. Clin Pharmacokinet 2008;47:7-20

37
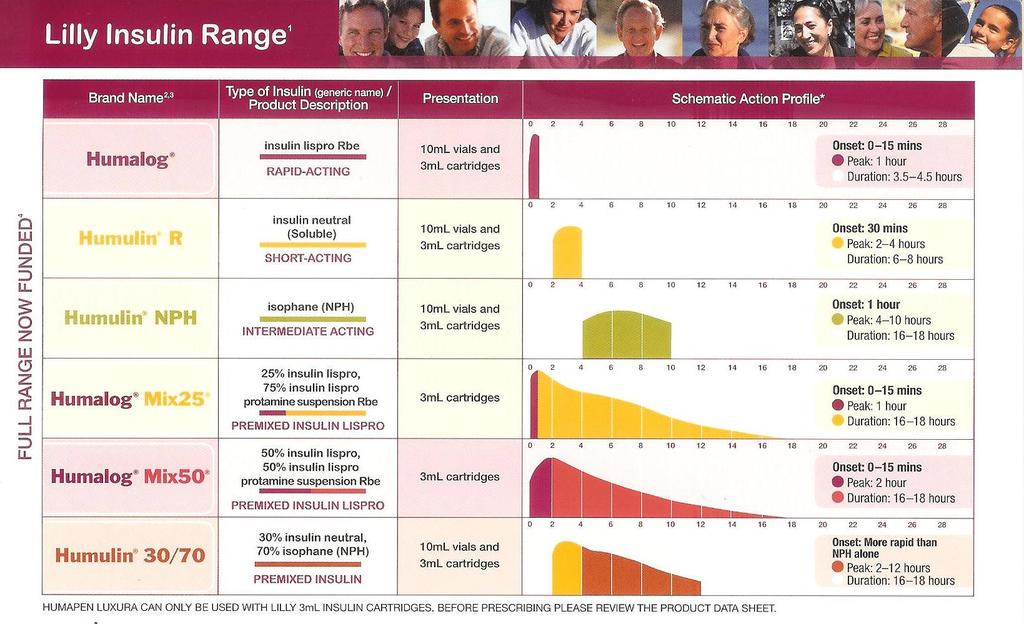
38
39 How to start? 1. Conventional approach: - Bedtime basal insulin (10 units of Protaphane/ Humulin NPH/ Glargine), titrate dose up with an aim to normalise (4-7mmol/L) fasting glucose - Particularly appropriate in those waking up with raised fasting glucose
40 How to start? More than one way to skin a cat! 2. Alternative approach: - Pre-dinner premixed insulin: e.g. 12 units of NovoMix30 or HumalogMix25 - Good for those with high post prandial glucoses, large dinners and unlikely to manage more than 2 injections a day
41 Back to Case 3 55 y.o. overweight male with 9 year hx of T2DM on MF 1.5g BD, Gliclazide 160mg BD. HbA1c mmol/mol over past 6 months What was done: Lantus (glargine) started at 10 units at night, with instructions to regularly check pre-breakfast CGs
42 Plasma glucose (mmol/l) Why start with basal insulin? Comparison of 24-hour glucose levels in untreated vs treated patients with diabetes T2DM Plasma glucose (mmol/l) 0 Meal Meal Meal 06:00 10:00 14:00 18:00 22:00 02:00 06:00 0 Time of day (hours) Adapted from Hirsch I et al. Clin Diabetes 2005; 23:

43 Patient led titration with Lantus Davies et al. Diabetes Care2005;28(6):1282-8
44 FAST SCHEDULE (PHYSICIAN-MANAGED) Increase by 2 8 units of insulin depending on fasting BGL over previous 2 3 days Mean fasting blood glucose (mmol/l) Increase in insulin dose <4 * See below No change units units units >10 8 units Adapted from Phillips PJ. Medicine Today 2007; 8(3):


45 Over to you, Rab
Glucose Control drug treatments
 Glucose Control drug treatments It should be noted that glitazones are under suspicion of precipitating acute cardiac events and current recommendations contraindicate the use of glitazones in patients
Glucose Control drug treatments It should be noted that glitazones are under suspicion of precipitating acute cardiac events and current recommendations contraindicate the use of glitazones in patients
Dept of Diabetes Main Desk
 Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
TREATMENTS FOR TYPE 2 DIABETES. Susan Henry Diabetes Specialist Nurse
 TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
Insulin use in Type 2 Diabetes
 Insulin use in Type 2 Diabetes 1 Conflict of Interest I have been on advisory boards or had speaker fees from the following pharmaceutical companies: - Eli Lilly - Novo Nordisk - Sanofi Aventis - MSD -
Insulin use in Type 2 Diabetes 1 Conflict of Interest I have been on advisory boards or had speaker fees from the following pharmaceutical companies: - Eli Lilly - Novo Nordisk - Sanofi Aventis - MSD -
Guidelines to assist General Practitioners in the Management of Type 2 Diabetes. April 2010
 Guidelines to assist General Practitioners in the Management of Type 2 Diabetes April 2010 Foreword The guidelines were devised by the Diabetes Day Centre in Beaumont Hospital in consultation with a number
Guidelines to assist General Practitioners in the Management of Type 2 Diabetes April 2010 Foreword The guidelines were devised by the Diabetes Day Centre in Beaumont Hospital in consultation with a number
Drugs used in Diabetes. Dr Andrew Smith
 Drugs used in Diabetes Dr Andrew Smith Plan Introduction Insulin Sensitising Drugs: Metformin Glitazones Insulin Secretagogues: Sulphonylureas Meglitinides Others: Acarbose Incretins Amylin Analogues Damaglifozin
Drugs used in Diabetes Dr Andrew Smith Plan Introduction Insulin Sensitising Drugs: Metformin Glitazones Insulin Secretagogues: Sulphonylureas Meglitinides Others: Acarbose Incretins Amylin Analogues Damaglifozin
Insulin Initiation, titration & Insulin switch in the Primary Care-KISS
 Insulin Initiation, titration & Insulin switch in the Primary Care-KISS Rotorua GP CME 9 June 2012 Dr Kingsley Nirmalaraj FRACP Endocrinologist, BOPDHB & Suite 9, Promed House, Tenth Ave, Tauranga Linda
Insulin Initiation, titration & Insulin switch in the Primary Care-KISS Rotorua GP CME 9 June 2012 Dr Kingsley Nirmalaraj FRACP Endocrinologist, BOPDHB & Suite 9, Promed House, Tenth Ave, Tauranga Linda
Management of Type 2 Diabetes
 Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
Pharmacological Glycaemic Control in Type 2 Diabetes
 Pharmacological Glycaemic Control in Type 2 Diabetes Aim(s) and Objective(s) This guideline aims to offer advice on the pharmacological management for those who require measures beyond diet and exercise
Pharmacological Glycaemic Control in Type 2 Diabetes Aim(s) and Objective(s) This guideline aims to offer advice on the pharmacological management for those who require measures beyond diet and exercise
YOU HAVE DIABETES. Angie O Connor Community Diabetes Nurse Specialist 25th September 2013
 YOU HAVE DIABETES Angie O Connor Community Diabetes Nurse Specialist 25th September 2013 Predicated 2015 figures are already met 1 in 20 have diabetes:1in8 over 60years old Definite Diagnosis is key Early
YOU HAVE DIABETES Angie O Connor Community Diabetes Nurse Specialist 25th September 2013 Predicated 2015 figures are already met 1 in 20 have diabetes:1in8 over 60years old Definite Diagnosis is key Early
How can we improve outcomes in Type 2 diabetes?
 How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management Identify and treat all risk factors Use rational pharmacological therapy
How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management Identify and treat all risk factors Use rational pharmacological therapy
Why is Earlier and More Aggressive Treatment of T2 Diabetes Better?
 Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
Treatment Options for Diabetes: An Update
 Treatment Options for Diabetes: An Update A/Prof. Marg McGill Manager, Diabetes Centre Dr. Ted Wu Staff Specialist Endocrinologist Diabetes Centre Centre of Health Professional Education Education Provider
Treatment Options for Diabetes: An Update A/Prof. Marg McGill Manager, Diabetes Centre Dr. Ted Wu Staff Specialist Endocrinologist Diabetes Centre Centre of Health Professional Education Education Provider
Diabetes in the UK: Update on Diabetes Treatment and Care. Why is diabetes increasing? Obesity Increased waist circumference.
 Update on Diabetes Treatment and Care Tahseen A Chowdhury Consultant Diabetologist Royal London and Mile End Hospitals Diabetes prevalence (thousands) Diabetes in the UK: 1995-21 3 25 2 15 1 5 Type 1 Type
Update on Diabetes Treatment and Care Tahseen A Chowdhury Consultant Diabetologist Royal London and Mile End Hospitals Diabetes prevalence (thousands) Diabetes in the UK: 1995-21 3 25 2 15 1 5 Type 1 Type
Type 2 Diabetes: Where Do We Start with Treatment? DIABETES EDUCATION. Diabetes Mellitus: Complications and Co-Morbid Conditions
 Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
How they work and when to take them. Diabetes Medications
 How they work and when to take them Diabetes Medications BIGUANIDES Metformin Actions Slows down the release of glucose from the liver. Helps the bodies cells become more sensitive to insulin. Pros Weight
How they work and when to take them Diabetes Medications BIGUANIDES Metformin Actions Slows down the release of glucose from the liver. Helps the bodies cells become more sensitive to insulin. Pros Weight
Overview T2DM medications. Winnie Ho
 Overview T2DM medications Winnie Ho Diabetes in Australia 1.7 million Australians with diabetes, of these 85% have T2DM 2-fold excess risk CV death in patients with diabetes Risk factor for progression
Overview T2DM medications Winnie Ho Diabetes in Australia 1.7 million Australians with diabetes, of these 85% have T2DM 2-fold excess risk CV death in patients with diabetes Risk factor for progression
Navigating the New Options for the Management of Type 2 Diabetes
 Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
Volume 2; Number 14 September 2008 NICE CLINICAL GUIDELINE 66: TYPE 2 DIABETES THE MANAGEMENT OF TYPE 2 DIABETES (MAY 2008)
") Volume 2; Number 14 September 2008 NICE CLINICAL GUIDELINE 66: TYPE 2 DIABETES THE MANAGEMENT OF TYPE 2 DIABETES (MAY 2008) The purpose of this special edition of the PACE Bulletin is to summarize the
Volume 2; Number 14 September 2008 NICE CLINICAL GUIDELINE 66: TYPE 2 DIABETES THE MANAGEMENT OF TYPE 2 DIABETES (MAY 2008) The purpose of this special edition of the PACE Bulletin is to summarize the
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Proposed Health Technology Appraisal
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Proposed Health Technology Appraisal Dapagliflozin in combination therapy for the Final scope Remit/appraisal objective To appraise the clinical and
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Proposed Health Technology Appraisal Dapagliflozin in combination therapy for the Final scope Remit/appraisal objective To appraise the clinical and
Cardiovascular Management of a Patient with Diabetes
 Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
Type 2 Diabetes. Stopping Smoking. Consider referral to smoking cessation. Consider referring for weight management advice.
 Type 2 Diabetes Stopping Smoking Consider referral to smoking cessation BMI > 25 kg m² Set a weight loss target of a 5-10% reduction Consider referring for weight management advice Control BP to
Type 2 Diabetes Stopping Smoking Consider referral to smoking cessation BMI > 25 kg m² Set a weight loss target of a 5-10% reduction Consider referring for weight management advice Control BP to
Liraglutide (Victoza) in combination with basal insulin for type 2 diabetes
 in combination with basal insulin for type 2 diabetes") Liraglutide (Victoza) in combination with basal insulin for type 2 diabetes May 2011 This technology summary is based on information available at the time of research and a limited literature search. It
Liraglutide (Victoza) in combination with basal insulin for type 2 diabetes May 2011 This technology summary is based on information available at the time of research and a limited literature search. It
Insulin Initiation and titration in the Primary Care-KISS Rotorua GP CME Meeting June 2011
 Insulin Initiation and titration in the Primary Care-KISS Rotorua GP CME Meeting June 2011 Dr Kingsley Nirmalaraj FRACP Endocrinologist BOPDHB Workshop goal To make participants comfortable in the timely
Insulin Initiation and titration in the Primary Care-KISS Rotorua GP CME Meeting June 2011 Dr Kingsley Nirmalaraj FRACP Endocrinologist BOPDHB Workshop goal To make participants comfortable in the timely
MANAGEMENT OF TYPE 2 DIABETES
 MANAGEMENT OF TYPE 2 DIABETES 3 Month trial of lifestyle changes. Refer to DESMOND structured education programme. Set glycaemic target HbA1c < 7.0% (53mmol/mol) or individualised If HbA1c > 53mmol/mol
MANAGEMENT OF TYPE 2 DIABETES 3 Month trial of lifestyle changes. Refer to DESMOND structured education programme. Set glycaemic target HbA1c < 7.0% (53mmol/mol) or individualised If HbA1c > 53mmol/mol
Dr Tahseen A. Chowdhury Royal London Hospital. New Guidelines in Diabetes: NICE or Nasty?
 Dr Tahseen A. Chowdhury Royal London Hospital New Guidelines in Diabetes: NICE or Nasty? I have no conflicts of interest I do not undertake talks / advisory bodies / research for any pharma company Consultant
Dr Tahseen A. Chowdhury Royal London Hospital New Guidelines in Diabetes: NICE or Nasty? I have no conflicts of interest I do not undertake talks / advisory bodies / research for any pharma company Consultant
GLP-1 Receptor Agonists and SGLT-2 Inhibitors. Debbie Hicks
 GLP-1 Receptor Agonists and SGLT-2 Inhibitors Debbie Hicks Prescribing and Adverse Event reporting information is available at this meeting from the AstraZeneca representative The views expressed by the
GLP-1 Receptor Agonists and SGLT-2 Inhibitors Debbie Hicks Prescribing and Adverse Event reporting information is available at this meeting from the AstraZeneca representative The views expressed by the
GLP-1 agonists. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
Alia Gilani Health Inequalities Pharmacist
 Alia Gilani Health Inequalities Pharmacist THE SOUTH ASIAN HEALTH FOUNDATION (U.K.) (Registered Charity No. 1073178) 1. Case Study 2. Factors influencing prescribing 3. Special Considerations 4. Prescribing
Alia Gilani Health Inequalities Pharmacist THE SOUTH ASIAN HEALTH FOUNDATION (U.K.) (Registered Charity No. 1073178) 1. Case Study 2. Factors influencing prescribing 3. Special Considerations 4. Prescribing
Antihyperglycemic Agents in Diabetes. Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014
 Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Type 2 Diabetes Mellitus hypoglycaemic agents
 Type 2 Diabetes Mellitus hypoglycaemic agents Name Metformin Drug Name (eg brand name) Metformin (Diaformin Diabex) Cost / PBS per 28d mth $10.24 (1.5g dly) 1000mg+500mg / $4.44+$5.80 Concerns? Lactic
Type 2 Diabetes Mellitus hypoglycaemic agents Name Metformin Drug Name (eg brand name) Metformin (Diaformin Diabex) Cost / PBS per 28d mth $10.24 (1.5g dly) 1000mg+500mg / $4.44+$5.80 Concerns? Lactic
PERIOPERATIVE DIABETES GUIDELINE
 PERIOPERATIVE DIABETES GUIDELINE This Guideline does not replace the need for the application of clinical judgment in respect to each individual patient. Background Diabetes mellitus is estimated to affect
PERIOPERATIVE DIABETES GUIDELINE This Guideline does not replace the need for the application of clinical judgment in respect to each individual patient. Background Diabetes mellitus is estimated to affect
CURRENT ISSUES IN DIABETES MANAGEMENT. Screening for Diabetes Advantages of HbA1c as a Diagnostic Test. Diagnosis of Diabetes 2013
 CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening for Diabetes 2013 BMI
CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening for Diabetes 2013 BMI
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES
 ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
Oral Agents. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
Dr A Pokrajac MD MSc MRCP Consultant
 Dr A Pokrajac MD MSc MRCP Consultant Onset at 5-15 years of T1DM Can be present at diagnosis of T2DM Detect in regular MA/Cr screening (2X first urine sample, no UTI, no other causes) Contributing Factors
Dr A Pokrajac MD MSc MRCP Consultant Onset at 5-15 years of T1DM Can be present at diagnosis of T2DM Detect in regular MA/Cr screening (2X first urine sample, no UTI, no other causes) Contributing Factors
Information for Patients
 Information for Patients Guidance for Diabetic Persons having an OGD or Bronchoscopy This guidance is provided to assist with your preparation for your endoscopic procedure. If you feel unclear about how
Information for Patients Guidance for Diabetic Persons having an OGD or Bronchoscopy This guidance is provided to assist with your preparation for your endoscopic procedure. If you feel unclear about how
Management of Diabetes Mellitus: A Primary Care Perspective. Screening for Diabetes Advantages of HbA1c as a Diagnostic Test
 Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
3. Cardiovascular Disease?
 Swiss recommendations 2016 Swiss Society of Endocrinology and Diabetology 1. Deficiency? Basal Premixed- Basal + GLP-1 RA (Xultophy ) or Basal Bolus 2. egfr < 30 ml/min? 3. Cardiovascular Disease? 4. Heart
Swiss recommendations 2016 Swiss Society of Endocrinology and Diabetology 1. Deficiency? Basal Premixed- Basal + GLP-1 RA (Xultophy ) or Basal Bolus 2. egfr < 30 ml/min? 3. Cardiovascular Disease? 4. Heart
Wayne Gravois, MD August 6, 2017
 Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
Management of Diabetes
 Management of Diabetes Mellitus: Which Drugs for Which Patients? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu Disclosure No relevant financial relationships
Management of Diabetes Mellitus: Which Drugs for Which Patients? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu Disclosure No relevant financial relationships
667FM.5.1 MANAGEMENT OF TYPE 2 DIABETES: BLOOD-GLUCOSE-LOWERING THERAPY
 667FM.5.1 MANAGEMENT OF TYPE 2 DIABETES: BLOOD-GLUCOSE-LOWERING THERAPY Contents Introduction... 1 Patient Education for People with Type 2 Diabetes... 2 Dietary Advice for People with Type 2 Diabetes...
667FM.5.1 MANAGEMENT OF TYPE 2 DIABETES: BLOOD-GLUCOSE-LOWERING THERAPY Contents Introduction... 1 Patient Education for People with Type 2 Diabetes... 2 Dietary Advice for People with Type 2 Diabetes...
TYPE 2 DIABETES CRITERIA FOR REFERRAL TO LEVEL 2 OOHS
 TYPE 2 DIABETES CRITERIA FOR REFERRAL TO LEVEL 2 OOHS The aim of the Diabetes level 2 service is to provide a high quality service for safe initiation and optimization of injectable therapy within GP networks.
TYPE 2 DIABETES CRITERIA FOR REFERRAL TO LEVEL 2 OOHS The aim of the Diabetes level 2 service is to provide a high quality service for safe initiation and optimization of injectable therapy within GP networks.
What the Pill Looks Like. How it Works. Slows carbohydrate absorption. Reduces amount of sugar made by the liver. Increases release of insulin
 Diabetes s Oral s - Pills These are some of the pills that are currently available in Canada to treat diabetes. Each medication has benefits and side effects you should be aware of. Your diabetes team
Diabetes s Oral s - Pills These are some of the pills that are currently available in Canada to treat diabetes. Each medication has benefits and side effects you should be aware of. Your diabetes team
Oral Treatments for Type 2 Diabetes. Prescribing Support Pharmacist
 Oral Treatments for Type 2 Diabetes Prescribing Support Pharmacist Learning Outcomes Familiar with classes of oral hypoglycaemic agents (OHAs) used in controlling blood glucose levels When to use each
Oral Treatments for Type 2 Diabetes Prescribing Support Pharmacist Learning Outcomes Familiar with classes of oral hypoglycaemic agents (OHAs) used in controlling blood glucose levels When to use each
Should Psychiatrists be diagnosing (and treating) metabolic syndrome
 metabolic syndrome") Should Psychiatrists be diagnosing (and treating) metabolic syndrome David Hopkins Clinical Director, Diabetes King s College Hospital, London Diabetes prevalence (thousands) Diabetes in the UK: 1995-2010
Should Psychiatrists be diagnosing (and treating) metabolic syndrome David Hopkins Clinical Director, Diabetes King s College Hospital, London Diabetes prevalence (thousands) Diabetes in the UK: 1995-2010
Comprehensive Diabetes Treatment
 Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Drug Therapy for Diabetes Mellitus. Adj A/Prof Daniel Chew Dept of Endocrinology 8 th July 2017
 Drug Therapy for Diabetes Mellitus Adj A/Prof Daniel Chew Dept of Endocrinology 8 th July 2017 Diabetes Subtypes Optimal Treatment Ominous Octet DeFronzo. DIABETES, VOL. 58, APRIL 2009 Schematic Overview
Drug Therapy for Diabetes Mellitus Adj A/Prof Daniel Chew Dept of Endocrinology 8 th July 2017 Diabetes Subtypes Optimal Treatment Ominous Octet DeFronzo. DIABETES, VOL. 58, APRIL 2009 Schematic Overview
DIABETES INDICATIONS FOR INSULIN
 DIABETES INDICATIONS FOR INSULIN 1 Introduce the likely need for insulin in the future early on as part of patient education Emphasise that it is the pancreas that fails not the patient Assess if greater
DIABETES INDICATIONS FOR INSULIN 1 Introduce the likely need for insulin in the future early on as part of patient education Emphasise that it is the pancreas that fails not the patient Assess if greater
Objectives. Recognize all available medical treatment options for diabetes. Individualize treatment and glycemic target based on patient factors
 No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
NEW DIABETES CARE MEDICATIONS
 NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
Practical Diabetes. Nic Crook. (and don t use so many charts) Kuirau Specialists 1239 Ranolf Street Rotorua. Rotorua Hospital Private Bag 3023 Rotorua
 Kuirau Specialists 1239 Ranolf Street Rotorua. Rotorua Hospital Private Bag 3023 Rotorua") Practical Diabetes (and don t use so many charts) Nic Crook Rotorua Hospital Private Bag 3023 Rotorua Kuirau Specialists 1239 Ranolf Street Rotorua Worldwide rates of diabetes mellitus: predictions 80
Practical Diabetes (and don t use so many charts) Nic Crook Rotorua Hospital Private Bag 3023 Rotorua Kuirau Specialists 1239 Ranolf Street Rotorua Worldwide rates of diabetes mellitus: predictions 80
INSULIN THERAPY. Rungnapa Laortanakul, MD Maharat Nakhon Ratchasima hospital
 INSULIN THERAPY Rungnapa Laortanakul, MD Maharat Nakhon Ratchasima hospital 3 Sep. 2013 Case Somsak is a 64-year-old man was diagnosed with T2DM, HT, and dyslipidemia 9 years ago. No history of hypoglycemia
INSULIN THERAPY Rungnapa Laortanakul, MD Maharat Nakhon Ratchasima hospital 3 Sep. 2013 Case Somsak is a 64-year-old man was diagnosed with T2DM, HT, and dyslipidemia 9 years ago. No history of hypoglycemia
Metformin should be considered in all patients with type 2 diabetes unless contra-indicated
 November 2001 N P S National Prescribing Service Limited PPR fifteen Prescribing Practice Review PPR Managing type 2 diabetes For General Practice Key messages Metformin should be considered in all patients
November 2001 N P S National Prescribing Service Limited PPR fifteen Prescribing Practice Review PPR Managing type 2 diabetes For General Practice Key messages Metformin should be considered in all patients
Fasted and Consented but Blood Glucose 18mmol/L or How to Manage Diabetes in the Peri-Operative Period
 Fasted and Consented but Blood Glucose 18mmol/L or How to Manage Diabetes in the Peri-Operative Period Dr Ketan Dhatariya MBBS MSc MD MS FRCP Consultant in Diabetes and Endocrinology Norfolk and Norwich
Fasted and Consented but Blood Glucose 18mmol/L or How to Manage Diabetes in the Peri-Operative Period Dr Ketan Dhatariya MBBS MSc MD MS FRCP Consultant in Diabetes and Endocrinology Norfolk and Norwich
Management of Diabetes Mellitus: A Primary Care Perspective
 Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Initiating Injectables in Type 2 Diabetes. Tara Kadis Team Leader Diabetes Nurse Specialist York Teaching Hospital
 Initiating Injectables in Type 2 Diabetes Tara Kadis Team Leader Diabetes Nurse Specialist York Teaching Hospital Increasing levels in delivery of diabetes care Complex Care support 3 3.1 People with diabetes
Initiating Injectables in Type 2 Diabetes Tara Kadis Team Leader Diabetes Nurse Specialist York Teaching Hospital Increasing levels in delivery of diabetes care Complex Care support 3 3.1 People with diabetes
INSULIN 101: When, How and What
 INSULIN 101: When, How and What Alice YY Cheng @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
INSULIN 101: When, How and What Alice YY Cheng @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Medical therapy advances London/Manchester RCP February/June 2016
 Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Inpatient Diabetes 20/01/2015. What should I do? Hyperglycaemia why does it matter? Why are the BSLs unstable? BSL parameters
 Hyperglycaemia why does it matter? Inpatient Diabetes Angela Sheu Endocrine Registrar St George Hospital Hyperglycaemia at admission is a predictor of mortality May be part of stress response (eg post
Hyperglycaemia why does it matter? Inpatient Diabetes Angela Sheu Endocrine Registrar St George Hospital Hyperglycaemia at admission is a predictor of mortality May be part of stress response (eg post
Diabetes Treatment Update
 Diabetes Treatment Update Timothy C. Evans, MD PhD FACP University of Washington Department of Medicine Disclosure: Dr. Evans has no significant financial interest in any of the products or manufacturers
Diabetes Treatment Update Timothy C. Evans, MD PhD FACP University of Washington Department of Medicine Disclosure: Dr. Evans has no significant financial interest in any of the products or manufacturers
Professor Rudy Bilous James Cook University Hospital
 Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes
 Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Oral and Injectable Non-insulin Antihyperglycemic Agents
 Appendix 5: Diabetes Education and Medical Management in Adults with Diabetes Oral and Injectable Non-insulin s This directive will be implemented by RPhs, RNs or RDs who have been deemed authorized implementers.
Appendix 5: Diabetes Education and Medical Management in Adults with Diabetes Oral and Injectable Non-insulin s This directive will be implemented by RPhs, RNs or RDs who have been deemed authorized implementers.
In-Hospital Management of Diabetes. Dr Benjamin Schiff Assistant Professor McGill University
 In-Hospital Management of Diabetes Dr Benjamin Schiff Assistant Professor McGill University No conflict of interest to declare CLINICAL SCENARIO 62 y/o male with hx of DM 2, COPD, and HT is admitted with
In-Hospital Management of Diabetes Dr Benjamin Schiff Assistant Professor McGill University No conflict of interest to declare CLINICAL SCENARIO 62 y/o male with hx of DM 2, COPD, and HT is admitted with
Individualizing Care for Patients with Type 2 Diabetes
 Individualizing Care for Patients with Type 2 Diabetes Disclosures Speaker: AstraZeneca, Novo Nordisk, BI/Lilly, Valeritas, Takeda Advisor: Tandem Diabetes, Sanofi Objectives Develop individualized approaches
Individualizing Care for Patients with Type 2 Diabetes Disclosures Speaker: AstraZeneca, Novo Nordisk, BI/Lilly, Valeritas, Takeda Advisor: Tandem Diabetes, Sanofi Objectives Develop individualized approaches
Case study: Lean adult with no complications, newly diagnosed with type 2 diabetes
 Case study: Lean adult with no complications, newly diagnosed with type 2 diabetes Authored by Clifford Bailey and James LaSalle on behalf of the Global Partnership for Effective Diabetes Management. The
Case study: Lean adult with no complications, newly diagnosed with type 2 diabetes Authored by Clifford Bailey and James LaSalle on behalf of the Global Partnership for Effective Diabetes Management. The
SIMPLICITY IN T2DM MANAGEMENT WITH DPP4 INHIBITORS: SPECIAL POPULATION
 SIMPLICITY IN T2DM MANAGEMENT WITH DPP4 INHIBITORS: SPECIAL POPULATION DR ROSE ZHAO-WEI TING ( 丁昭慧醫生 ) MBBS (HK), MRCP (UK), FHKCP, FHKAM (MEDICINE) Specialist in Endocrinology, Diabetes and Metabolism
SIMPLICITY IN T2DM MANAGEMENT WITH DPP4 INHIBITORS: SPECIAL POPULATION DR ROSE ZHAO-WEI TING ( 丁昭慧醫生 ) MBBS (HK), MRCP (UK), FHKCP, FHKAM (MEDICINE) Specialist in Endocrinology, Diabetes and Metabolism
What s New in Diabetes Treatment. Disclosures
 What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
Newer Drugs in the Management of Type 2 Diabetes Mellitus
 Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable?
 Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
DIABETES. overview of pharmacologic agents used in the management of. Overview 4/3/2014 OBJECTIVES. Injectable Agents
 overview of pharmacologic agents used in the management of DIABETES Kyle Roberts, Pharm.D. PGY-1 Pharmacy Resident Saint Alphonsus RMC 1. List the different classes of diabetes medications, including the
overview of pharmacologic agents used in the management of DIABETES Kyle Roberts, Pharm.D. PGY-1 Pharmacy Resident Saint Alphonsus RMC 1. List the different classes of diabetes medications, including the
STEP 3: Add or Substitute with one of
 Prescribing of Hypoglycaemic Agents for Adult Patients with Type 2 Diabetes: Sunderland Refer to DESMOND Structured Education classes to promote Increased Physical Activity, Weight Loss and Calories Reduction
Prescribing of Hypoglycaemic Agents for Adult Patients with Type 2 Diabetes: Sunderland Refer to DESMOND Structured Education classes to promote Increased Physical Activity, Weight Loss and Calories Reduction
Diabetes Mellitus. Intended Learning Objectives:
 Intended Learning Objectives: Diabetes Mellitus 1. Compare and contrast the differences between the drug therapy recommendations of several of the latest and leading diabetes guidelines. 2. Assess the
Intended Learning Objectives: Diabetes Mellitus 1. Compare and contrast the differences between the drug therapy recommendations of several of the latest and leading diabetes guidelines. 2. Assess the
Management of Type 2 Diabetes. Why Do We Bother to Achieve Good Control in DM2. Insulin Secretion. The Importance of BP and Glucose Control
 Insulin Secretion Management of Type 2 Diabetes DG van Zyl Why Do We Bother to Achieve Good Control in DM2 % reduction 0-5 -10-15 -20-25 -30-35 -40 The Importance of BP and Glucose Control Effects of tight
Insulin Secretion Management of Type 2 Diabetes DG van Zyl Why Do We Bother to Achieve Good Control in DM2 % reduction 0-5 -10-15 -20-25 -30-35 -40 The Importance of BP and Glucose Control Effects of tight
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications
 Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Intensification of Diabetic Therapy. Case studies
 Intensification of Diabetic Therapy Case studies Patient #1 1 st visit: 64 year old male, H/O prediabetes, lost weight 280 lbs. to 240 lbs. ER for dental abscess, glucose >300 A1C 11.4%, no diabetic medication,
Intensification of Diabetic Therapy Case studies Patient #1 1 st visit: 64 year old male, H/O prediabetes, lost weight 280 lbs. to 240 lbs. ER for dental abscess, glucose >300 A1C 11.4%, no diabetic medication,
Diabetes, Type 2 Management
 CLINICAL GUIDELINE Diabetes, Type 2 Management A guideline is intended to assist healthcare professionals in the choice of disease-specific treatments. Clinical judgement should be exercised on the applicability
CLINICAL GUIDELINE Diabetes, Type 2 Management A guideline is intended to assist healthcare professionals in the choice of disease-specific treatments. Clinical judgement should be exercised on the applicability
OBJECTIVES 4/7/2014. Diabetes Update Overview of the Diabetes Epidemic in the United States. ISHP Annual Spring Meeting
 Diabetes Update 2014 ISHP Annual Spring Meeting Hayley Miller MD April 13, 2014 OBJECTIVES Review diabetes guidelines. Understand diabetes management targets. Discuss current therapeutic strategies. Overview
Diabetes Update 2014 ISHP Annual Spring Meeting Hayley Miller MD April 13, 2014 OBJECTIVES Review diabetes guidelines. Understand diabetes management targets. Discuss current therapeutic strategies. Overview
The Death of Sulfonylureas? A Review of New Diabetes Medications
 The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
Mae Sheikh-Ali, M.D. Assistant Professor of Medicine Division of Endocrinology University of Florida College of Medicine- Jacksonville
 Mae Sheikh-Ali, M.D. Assistant Professor of Medicine Division of Endocrinology University of Florida College of Medicine- Jacksonville Pathogenesis of Diabetes Mellitus (DM) Criteria for the diagnosis
Mae Sheikh-Ali, M.D. Assistant Professor of Medicine Division of Endocrinology University of Florida College of Medicine- Jacksonville Pathogenesis of Diabetes Mellitus (DM) Criteria for the diagnosis
FARXIGA (dapagliflozin) Jardiance (empagliflozin) tablets. Synjardy (empagliflozin and metformin hydrochloride) tablets. GLUCOPHAGE* (metformin)
 Jardiance (empagliflozin) tablets. Synjardy (empagliflozin and metformin hydrochloride) tablets. GLUCOPHAGE* (metformin)") Type 2 Medications Drug Class How It Works Brand and Generic Names Manufacturers Usual Starting Dose The kidneys filter sugar and either absorb it back into your body for energy or remove it through your
Type 2 Medications Drug Class How It Works Brand and Generic Names Manufacturers Usual Starting Dose The kidneys filter sugar and either absorb it back into your body for energy or remove it through your
Vipul Lakhani, MD Oregon Medical Group Endocrinology
 Vipul Lakhani, MD Oregon Medical Group Endocrinology Disclosures None Objectives Be able to diagnose diabetes and assess control Be able to identify appropriate classes of medications for diabetes treatment
Vipul Lakhani, MD Oregon Medical Group Endocrinology Disclosures None Objectives Be able to diagnose diabetes and assess control Be able to identify appropriate classes of medications for diabetes treatment
Diabetes Management: A diagnostic perspective
 Diabetes Management: A diagnostic perspective Images: http://www.engadget.com/2009/09/23/bayer-introduces-countour-usb-glucose-meter/ http://www.medtronicdiabetes.com/treatment-and-products/minimed-530g-diabetes-system-with-enlite
Diabetes Management: A diagnostic perspective Images: http://www.engadget.com/2009/09/23/bayer-introduces-countour-usb-glucose-meter/ http://www.medtronicdiabetes.com/treatment-and-products/minimed-530g-diabetes-system-with-enlite
DR HJ BODANSKY MD FRCP CONSULTANT PHYSICIAN LEEDS TEACHING HOSPITALS ASSOCIATE PROFESSOR, UNIVERSITY OF LEEDS
 DR HJ BODANSKY MD FRCP CONSULTANT PHYSICIAN LEEDS TEACHING HOSPITALS ASSOCIATE PROFESSOR, UNIVERSITY OF LEEDS DIABETETES UPDATE 2015 AIMS OF THE SEMINAR Diagnosis Investigation Management When to refer
DR HJ BODANSKY MD FRCP CONSULTANT PHYSICIAN LEEDS TEACHING HOSPITALS ASSOCIATE PROFESSOR, UNIVERSITY OF LEEDS DIABETETES UPDATE 2015 AIMS OF THE SEMINAR Diagnosis Investigation Management When to refer
Update on Pharmacological Management in Type 2 Diabetes
 Update on Pharmacological Management in Type 2 Diabetes Prof. Lotfy Hamed Abo Dahab Professor Of Internal Medicine and Cardiology Vice President of Sohag University ١ My AGENDA Targets For Glycaemic Control
Update on Pharmacological Management in Type 2 Diabetes Prof. Lotfy Hamed Abo Dahab Professor Of Internal Medicine and Cardiology Vice President of Sohag University ١ My AGENDA Targets For Glycaemic Control
Mr Gavin Hendry. Mr Rab Burtun. Prof Jim Mann. Diabetes Nurse Facilitator, Auckland. Dunedin. Human Nutrition & Medicine University of Otago, Dunedin
 Mr Rab Burtun Diabetes Nurse Facilitator, Auckland Mr Gavin Hendry Dunedin Prof Jim Mann Human Nutrition & Medicine University of Otago, Dunedin Insulin Master Class Presented by: Prof Jim Mann Gavin Hendry
Mr Rab Burtun Diabetes Nurse Facilitator, Auckland Mr Gavin Hendry Dunedin Prof Jim Mann Human Nutrition & Medicine University of Otago, Dunedin Insulin Master Class Presented by: Prof Jim Mann Gavin Hendry
Starting Insulin in General Practice
 Starting Insulin in General Practice Timothy Kenealy GP & Assoc Prof of Integrated Care, University of Auckland Auckland DHB / my version + Counties DHB version Starting Insulin surprisingly simple, safe
Starting Insulin in General Practice Timothy Kenealy GP & Assoc Prof of Integrated Care, University of Auckland Auckland DHB / my version + Counties DHB version Starting Insulin surprisingly simple, safe
Case study for CME Diabetes up-to-date management
 Case study for CME Diabetes up-to-date management Dr Ole Schmiedel, MRCP MD FRACP Physician and Endocrinologist Service Clinical Director Auckland Diabetes Centre GP referral to Auckland Diabetes Centre
Case study for CME Diabetes up-to-date management Dr Ole Schmiedel, MRCP MD FRACP Physician and Endocrinologist Service Clinical Director Auckland Diabetes Centre GP referral to Auckland Diabetes Centre
Diabetes Mellitus: Implications of New Clinical Trials and New Medications
 Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
New Treatments for Type 2 diabetes. Nandini Seevaratnam April 2016 Rushcliffe Patient Forum
 New Treatments for Type 2 diabetes Nandini Seevaratnam April 2016 Rushcliffe Patient Forum Overview Growing population of Type 2 diabetes Basic science on what goes wrong Current treatments Why there is
New Treatments for Type 2 diabetes Nandini Seevaratnam April 2016 Rushcliffe Patient Forum Overview Growing population of Type 2 diabetes Basic science on what goes wrong Current treatments Why there is
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS
 IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
Oral Treatments. SaminaAli Prescribing Support Pharmacist
 Oral Treatments for Type 2 Diabetes SaminaAli Prescribing Support Pharmacist Learning Outcomes National Guidance Familiar with classes of oral hypoglycaemic agents (OHAs) used in controlling blood glucose
Oral Treatments for Type 2 Diabetes SaminaAli Prescribing Support Pharmacist Learning Outcomes National Guidance Familiar with classes of oral hypoglycaemic agents (OHAs) used in controlling blood glucose
Table 1. Antihyperglycemic agents for use in type 2 diabetes
 Table 1. Antihyperglycemic agents for use in type 2 diabetes DRUG IN ALPHA-GLUCOSIDASE INHIBITOR: inhibits pancreatic alpha-amyle and intestinal alpha-glucoside Acarbose (Glucobay) 0.6% Negligible Not
Table 1. Antihyperglycemic agents for use in type 2 diabetes DRUG IN ALPHA-GLUCOSIDASE INHIBITOR: inhibits pancreatic alpha-amyle and intestinal alpha-glucoside Acarbose (Glucobay) 0.6% Negligible Not
Chief of Endocrinology East Orange General Hospital
 Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Arrange 3 Monthly Review Re-enforce LIFESTYLE advice and check DRUG COMPLIANCE at each visit Target HbA1c < 53mmol/mol
 Prescribing of Hypoglycaemic Agents for Adult Patients with Type 2 Diabetes: Sunderland Refer to DESMOND Structured Education classes to promote Increased Physical Activity, Weight Loss and Calories Reduction
Prescribing of Hypoglycaemic Agents for Adult Patients with Type 2 Diabetes: Sunderland Refer to DESMOND Structured Education classes to promote Increased Physical Activity, Weight Loss and Calories Reduction
Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone
 Index Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone Medication GAD glutamic acid decarboxylase GLP-1 glucagon-like peptide 1 NPH neutral
Index Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone Medication GAD glutamic acid decarboxylase GLP-1 glucagon-like peptide 1 NPH neutral
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE. Single Technology Appraisal. Canagliflozin in combination therapy for treating type 2 diabetes
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal Canagliflozin in combination therapy for Final scope Remit/appraisal objective To appraise the clinical and cost effectiveness
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal Canagliflozin in combination therapy for Final scope Remit/appraisal objective To appraise the clinical and cost effectiveness
Jennifer Loh, MD, FACE Chief of Endocrinology KP Hawaii AAMD of Medical Education, KP Hawaii
 Individualized Diabetes Treatment for the Elderly Jennifer Loh, MD, FACE Chief of Endocrinology KP Hawaii AAMD of Medical Education, KP Hawaii Extremely Relevant Baby Boomers are aging! ¼ of people age
Individualized Diabetes Treatment for the Elderly Jennifer Loh, MD, FACE Chief of Endocrinology KP Hawaii AAMD of Medical Education, KP Hawaii Extremely Relevant Baby Boomers are aging! ¼ of people age