Basal-Bolus Insulin Therapy. Veronica Brady, PhD, FNP-BC, BC-ADM, CDE ECHO January
|
|
|
- Thomas Mitchell
- 5 years ago
- Views:
Transcription
1 Basal-Bolus Insulin Therapy Veronica Brady, PhD, FNP-BC, BC-ADM, CDE ECHO January
2
3
4 Terminology No longer using the term diabetic. Diabetes does not define people. People with diabetes are individuals with diabetes, not diabetics. Diabetic will continue to be used related to complications, e.g., diabetic retinopathy. ADA, Diabetes Care,2016;
5 Objectives Review insulin therapy Older Newer Latest Discuss starting Insulin Discuss adjusting Insulin
6 The Case of AB (Diagnosis) AB is a 34 year old male who presents to the office with complains of worsening vison, nocturia, nightmares, and extreme thirst. MH is non-contributory SH-tonsillectomy, appendectomy FH is significant for DM in his father and paternal grandmother, CAD in father with stents at age 54, HTN in his mother SH is significant for smoking ½ ppdx20 years, occasional ETOH, +marijuana. He is single and works in a packing warehouse.
7 The Case of AB cont Vitals-weight 234#, BMI 35, BP 149/87, P89 A1c in office today 9.3% PE- HEENT-WNL Cardio-RRR Lungs-CTA Abdomen-obese LE-trace edema, ++DP pulses, Feet-+sensation to 10gram monofilament
8 The Case of AB (year 1) AB returns to your office 3 months after diagnosis. He has been to DSME classes. He states that he has attempted to change his eating habits (less fatty foods, fewer sweets, etc.) and tried to exercise (he walks a lot at work and lifts heavy boxes). He weight today is 230#, BP: 140/90 Labs: chol-204mg/dl, LDL 112mg/dL, Cr-1.3, microalb-10, TSH 2.5, A1c-8%
9 The Case of AB (year 3) It has been 3 years since diagnosis. You have seen AB in clinic every 3-4 months in the interim since his first visit. In that time you have increased his Metformin to 1gm BID, started glimiperide 4mg BID and put him on max dose of Invokana 300mg/d. He is also on a statin and an ACE. He has managed to lose 12# and keep it off. He reports mild nausea, urinary frequency and some numbness and tingling of his feet.
10 The Case of AB (year 3) Labs: chol-157mg/dl, LDL 95mg/dL, urine microalb-25, A1c-8.8% PE: unremarkable
11 "There are two times to start insulin for type 2 diabetes," "The first is any time blood sugar is significantly out of control and a patient has symptoms,. "In these cases, the need for insulin may be short-term. The second time is when type 2 diabetes has progressed over many years and the pancreas can no longer make enough insulin to respond to other diabetes medications." Alaleh Mazhari, DO Loyola University Health System

12 Insulin A peptide hormone composed of 51 amino acids secreted by pancreatic beta cells Synthesized as preproinsulin, then cleaved to proinsulin and stored in secretory granules, which is then cleaved into C-peptide and insulin in the secretory granules
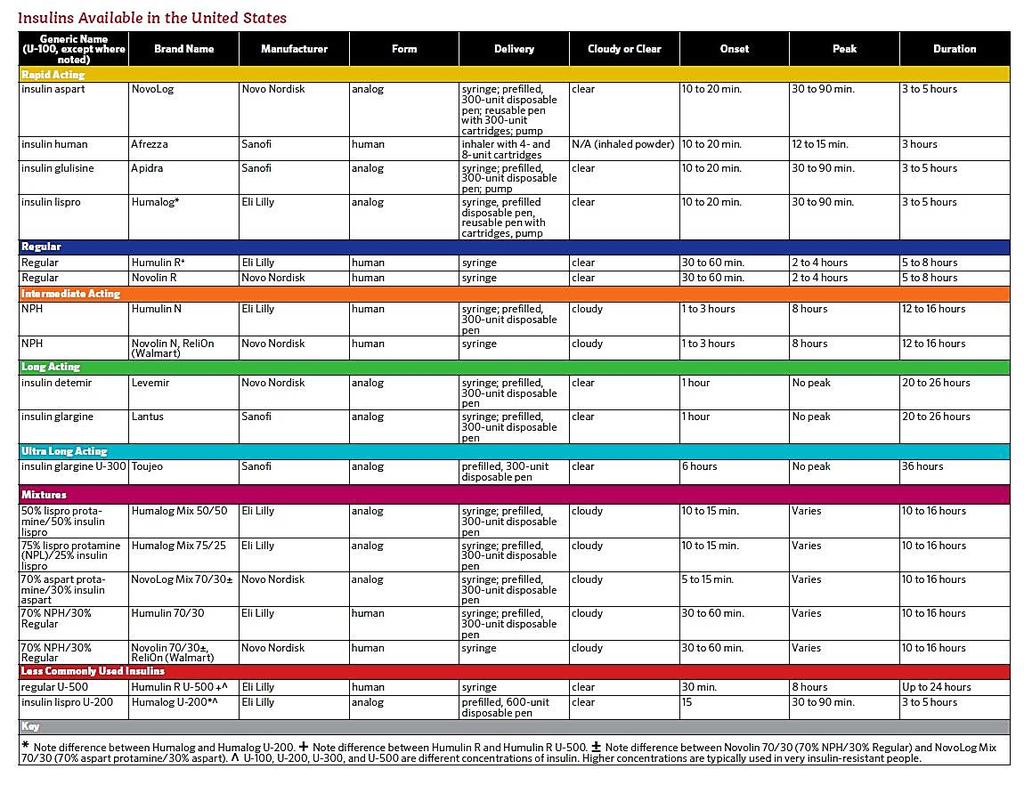
13 Rapid Acting Short Acting Intermediate Acting Long Acting Ultra Long Acting Insulins
14 What is the Best Practice for Managing Diabetes with Insulin? Anticipatory, physiologic insulin dosing prescribed as a basal/ bolus insulin regimen giving the right type of insulin, in the right amount, at the right time, to meet the insulin needs of the patient Wesorick, et al.
15 Normal Insulin Secretion Basal: continuous insulin to compensate for liver glucose Bolus: surge for food 1 st phase: rapid rise in serum insulin levels inhibits glucagon release and therefore inhibits glycogenolysis 2 nd phase: to maintain normoglycemia postprandially
16 Components of Physiologic Insulin Regimen Basal insulin (detemir, glargine, NPH,degludec) Circulates between feedings Restrains glucose production, and catabolism of stored fuels Defends against ketoacidosis About 50% of daily insulin requirement Nutritional insulin (aspart, glulisine, lispro, regular) Mimics rapid secretion of insulin in response to feeding Promotes assimilation of ingested nutrients Moderates post-prandial hyperglycemia
17
18 OLDER INSULINS
19 Rapid Acting Insulin Lispro/Humalog Glulisine/Apidra Aspart/Novolog Onset: 15 minutes Peak: minutes Duration:3-5 hours
20 Short Acting Insulin Regular Onset: Peak: Duration: 1 hr 2-4 hrs 4-12 hrs
21 NPH Intermediate Acting Insulin Onset: Peak: Duration: hrs 4-12 hrs up to 24 hrs
22 Long Acting Insulin Detemir/Levemir Onset: Peak: Duration: hrs hrs up to 24 hrs Glargine/Lantus Onset: Peak: Duration: 1-2 hrs peakless 24 hrs
23 Premixed insulin at breakfast and supper
24 Combination Insulins Humulin 70/30 Novolin 70/30 Relion 70/30 Humulin 50/50 Humalog Mix 75/25 Humalog Mix 50/50 Novolog Mix % Isophane Suspension (intermediate acting insulin) 30% Regular 70% Isophane Suspension (intermediate acting insulin) 30% Regular 50% Isophane Suspension (intermediate acting insulin) 50% Regular 75% Lispro Protamine Suspension (NPL) (intermediate acting) 25% lispro 50% Lispro Protamine Suspension (NPL) (intermediate acting) 50% lispro 70% Aspart Protamine Suspension (intermediate acting) 30% aspart Vial: 28 days once in use, Pen: 10 days once in use 28 days once in use 28 days once in use Vial: 28 days once in use; Pen 10 days once in use Vial: 28 days once in use; Pen 14 days once in use

25 NEWER INSULINS
26 RAPID ACTING

27 Inhaled Insulin Stimulates glucose uptake by skeletal muscle and fat: inhibits hepatic glucose output
28 Inhaled Insulin Onset & peak duration of action Main Benefits Peak 53 minutes Duration 160 minutes Less hypoglycemia Common adverse effects Hypoglycemia, cough, throat pain or irritation Cautious Use Acute bronchospasm reported in patients with asthma and COPD using inhaled insulin Contraindications Contraindicated in patients with chronic lung disease, smoker, DKA, hypersensitivity to regular human insulin
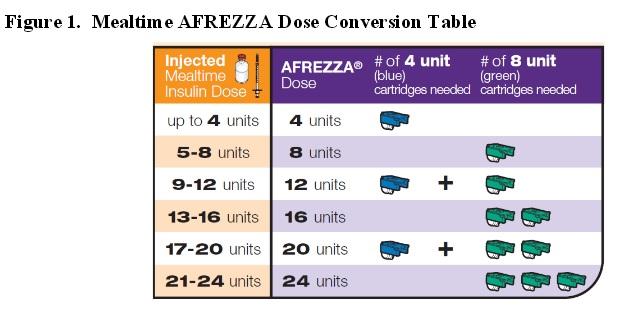
29 Afrezza

30 Afrezza Considerations: Lung function-no smoking (none within 6 months) Set doses not possible to get 3 units Amount of insulin needed for each meal Must be at room temp for 10 minutes before use

31
32 Humalog U-200 Generic Name- lispro U-200 Brand Name: Humalog U-200 Manufacturer: Eli Lilly Form: analog Delivery: pre-filled pen (600 units) Storage: in use 28 days do not refridgerate Onset: 15 minutes Peak: minutes Duration: 3-5 hours
33 INTERMEDIATE ACTING
34 U-500 pens Generic Name-regular U-500 Brand Name: Humulin R U-500 Manufacturer: Eli Lilly Form: human Delivery: 3 ml pen fill (1500 units) Storage- in use do not refrigerate 28 days Onset: 30 minutes Peak: 8 hours Duration: up to 24 hours
35 U-500 pens Considerations: Indicated for patients requiring more than 200 units of insulin/day. Administer 2-3 times a day 30 minutes before meals Do not mix with other insulins
36 U-500 Insulin Pharmacologic profile similar to NPH Useful in patients with: Obesity Immune-mediated insulin resistance Genetic abnormalities of the insulin receptor
37 U-500 Insulin Pharmacologic profile similar to NPH Useful in patients with: Obesity Immune-mediated insulin resistance Genetic abnormalities of the insulin receptor
38 LONG ACTING
39 Long-Acting Insulin Basaglar (biosimilar Lantus) Onset: Peak: Duration: 1-2 hrs peakless 24 hrs x B L D x
40 Basaglar Generic Name-glargine Brand Name: Basaglar Manufacturer: Eli Lilly Form: analog Delivery: 3 ml pen fill Storage-pen in use 28 days Onset: one hour Peak: no peak Duration: 24 hours

41 Ultra Long Acting Insulin Glargine U-300/Toujeo Onset: Peak: Duration: 6 hrs peakless 36 hrs

42 Toujeo Generic Name: glargine U-300 Brand Name: Toujeo Manufacturer: Sanofi Form: Analog Delivery: (450unit) prefilled pen Storage-pen in use good for 42 days Onset: 6 hours Peak: No peak Duration: 36 hours Maximum single injection: 80 units

43 Comparison of U-100 & U-300 insulin glargine U-100 U-300


44 Ultra Long Acting Insulin Degludec/Tresiba Onset: Peak: Duration: ½-1.5 hrs peakless 42 hrs
 Storage: in use room temperature up to 48 days Onset: one hour Peak: No peak Duration: 42 hours Maximum single dose: 160 units")
45 Tresiba Generic Name: degludec Brand Name: Tresiba Manufacturer: Novo Nordisk Form: Analog Delivery: prefilled pen u-100 (300) u-200 (600) Storage: in use room temperature up to 48 days Onset: one hour Peak: No peak Duration: 42 hours Maximum single dose: 160 units
46 WHAT S THE LATEST?
; 30-60 units/day start 30 units Max dose 60 units (60G/20 lixisenatide) One hour prior to 1 st meal Supplied in 3ml")
47 Insulin + GLP-1 Soliqua 100/33 (glargine 100/lixisenatide 33mcg per ml) Using <60units of basal or lixisenatide If <30 units/day --start with 15 units (15glargine/5mcg lixisenatide); units/day start 30 units Max dose 60 units (60G/20 lixisenatide) One hour prior to 1 st meal Supplied in 3ml prefilled pens
48 Insulin + GLP-1 Xultophy 100/3.6 (100 units degludec/3.6 mg liraglutide Using less than 50 units basal or liraglutide < 1.8 Starting dose 16 units (16 units degludec/0.58mg Max dose 50 units (50 units degludec/1.8mg liraglutide Independent of food Supplied in 3ml prefilled pens

49 Fiasp Generic Name- fast acting insulin aspart Brand Name- Fiasp Manufacturer- Novonordisk Form- analog Delivery- 3ml pre-filled pen, 10 ml vials Storage-open in use 28 days-room temperature Onset- 2.5 minutes (dose dependent) Peak- 63 minutes (dose dependent) Duration- 5-7 hours (dose dependent)
50 STARTING INSULIN & ADJUSTING INSULIN
51 Who Should be on Insulin? Type 1 diabetes at any age Uncontrolled hyperglycemia on oral agents Presentation with decompensated diabetes Pregnant women with hyperglycemia Critical illness e.g. myocardial infarction, sepsis No oral access Oral agents contraindicated e.g. NPO, renal or hepatic disease
52
53 How much insulin to start? New start: Usual starting total daily dose: units/ kg larger dose if: steroid therapy, massive obesity smaller dose if: renal failure, hepatic failure, malnourished, type 1 diabetes Half basal, half prandial/bolus ± correctional
54
55 The Case of AB (cont) 37 yo male. 222#, BMI- 33, BP 150/90, A1c 8.8% It s time for insulin What to do?
56 The Case of AB (year 10) He is now 44 years old. He has regained the weight he previously lost plus an additional 20#--254# (BMI 38). He is not checking BG often, but no feelings of lows. His A1c is 10%. He states he is taking insulin as prescribed, but BG remains elevated What to do now?
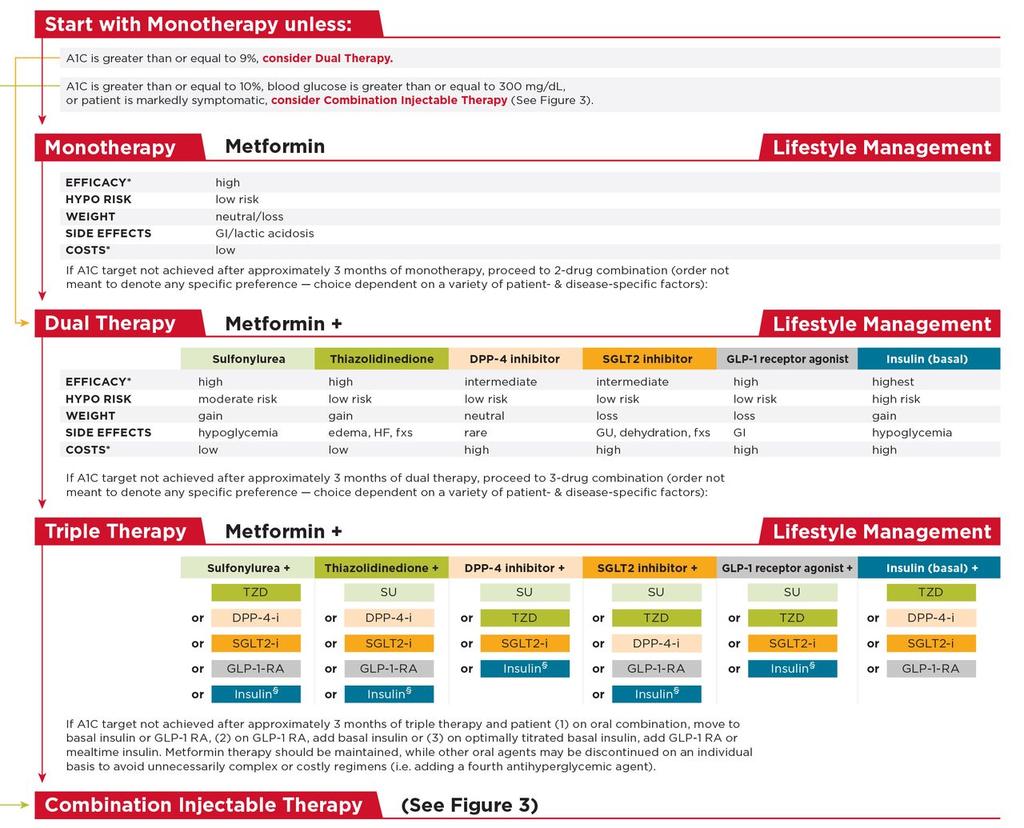
57 Pharmacological Therapy For T2DM If noninsulin monotherapy at maximal tolerated dose does not achieve or maintain the A1C target over 3 months, add a second oral agent, a GLP-1 receptor agonist, or insulin. Use a patient-centered approach to treatment. Don t delay insulin initiation in patients not achieving glycemic goals. ADA, Diabetes Care,2016; American Diabetes Association Standards of Medical Care in Diabetes. Approaches to glycemic treatment. Diabetes Care 2016; 39 (Suppl. 1): S52-S59
58 Recommendations: Older Adults Glycemic goals for some older adults might be relaxed but hyperglycemia leading to symptoms or risk of acute hyperglycemic complications should be avoided in all patients. Hypoglycemia should be avoided in older adults with diabetes. It should be screened for and managed by adjusting glycemic targets and pharmacologic interventions. American Diabetes Association Standards of Medical Care in Diabetes. Older adults. Diabetes Care 2016; 39 (Suppl. 1): S81-S85

59 Questions?
Insulin Prior Authorization with optional Quantity Limit Program Summary
 Insulin Prior Authorization with optional Quantity Limit Program Summary 1-13,16-19, 20 FDA LABELED INDICATIONS Rapid-Acting Insulins Humalog (insulin lispro) NovoLog (insulin aspart) Apidra (insulin glulisine)
Insulin Prior Authorization with optional Quantity Limit Program Summary 1-13,16-19, 20 FDA LABELED INDICATIONS Rapid-Acting Insulins Humalog (insulin lispro) NovoLog (insulin aspart) Apidra (insulin glulisine)
Objectives. Navigating New Insulins. Disclosures. Diabetes: The Stats. Normal Insulin Release Individuals without diabetes. History of Insulin 5/23/17
 Objectives Compare and contrast currently available products. Navigating New s Diana Isaacs, PharmD, BCPS, BC-ADM, CDE Clinical Pharmacy Specialist Cleveland Clinic Diabetes Center Determine the factors
Objectives Compare and contrast currently available products. Navigating New s Diana Isaacs, PharmD, BCPS, BC-ADM, CDE Clinical Pharmacy Specialist Cleveland Clinic Diabetes Center Determine the factors
8/21/2017 UNRAVELING THE CROWED INSULIN SCENE. A Practical Overview of Insulin Focusing on New Insulin Preparations
 UNRAVELING THE CROWED INSULIN SCENE A Practical Overview of Insulin Focusing on New Insulin Preparations Patricia Garnica MS, ANP-BC, CDE, CDTC North Shore University Hospital, Manhasset, N.Y. October
UNRAVELING THE CROWED INSULIN SCENE A Practical Overview of Insulin Focusing on New Insulin Preparations Patricia Garnica MS, ANP-BC, CDE, CDTC North Shore University Hospital, Manhasset, N.Y. October
Newer Insulins. Boca Raton Regional Hospital 15th Annual Internal Medicine Conference
 Newer Insulins Boca Raton Regional Hospital 15th Annual Internal Medicine Conference Luigi F. Meneghini, MD, MBA Professor of Internal Medicine, UT Southwestern Medical Center Executive Director, Global
Newer Insulins Boca Raton Regional Hospital 15th Annual Internal Medicine Conference Luigi F. Meneghini, MD, MBA Professor of Internal Medicine, UT Southwestern Medical Center Executive Director, Global
Tips and Tricks for Starting and Adjusting Insulin. MC MacSween The Moncton Hospital
 Tips and Tricks for Starting and Adjusting Insulin MC MacSween The Moncton Hospital Progression of type 2 diabetes Beta cell apoptosis Natural History of Type 2 Diabetes The Burden of Treatment Failure
Tips and Tricks for Starting and Adjusting Insulin MC MacSween The Moncton Hospital Progression of type 2 diabetes Beta cell apoptosis Natural History of Type 2 Diabetes The Burden of Treatment Failure
GLP-1 RECEPTOR AGONIST SHOULD I TRY IT? VERONICA BRADY, PHD, BC-ADM, CDE PROJECT ECHO JUNE 21, 2018
 GLP-1 RECEPTOR AGONIST SHOULD I TRY IT? VERONICA BRADY, PHD, BC-ADM, CDE PROJECT ECHO JUNE 21, 2018 SOMETHING TO CONSIDER IF YOU COULD PRESCRIBE A MEDICATION FOR YOUR PATIENT WITH DIABETES THAT: DECREASED
GLP-1 RECEPTOR AGONIST SHOULD I TRY IT? VERONICA BRADY, PHD, BC-ADM, CDE PROJECT ECHO JUNE 21, 2018 SOMETHING TO CONSIDER IF YOU COULD PRESCRIBE A MEDICATION FOR YOUR PATIENT WITH DIABETES THAT: DECREASED
8/13/2016. Insulin Basics. Rapid-Acting Insulin Analogs. Current Insulin Products and Pens. Basal Insulin Analogs. History of Insulin Therapy
 Insulin Basics Anabolic hormone involved in metabolism Following carbohydrate ingestion insulin release is stimulated Suppresses hepatic glucose production Stimulates peripheral glucose uptake Commercially-available
Insulin Basics Anabolic hormone involved in metabolism Following carbohydrate ingestion insulin release is stimulated Suppresses hepatic glucose production Stimulates peripheral glucose uptake Commercially-available
Insulin Prior Authorization Criteria For Individuals Who Purchased BlueCare/KS Solutions/EPO Products
 Insulin Prior Authorization Criteria For Individuals Who Purchased BlueCare/KS Solutions/EPO Products FDA LABELED INDICATIONS 1-13,16-21 Rapid-Acting Indication Onset Peak Duration Insulins Admelog (insulin
Insulin Prior Authorization Criteria For Individuals Who Purchased BlueCare/KS Solutions/EPO Products FDA LABELED INDICATIONS 1-13,16-21 Rapid-Acting Indication Onset Peak Duration Insulins Admelog (insulin
Learning Objectives. Are you ready for more insulin formulations?
 Are you ready for more insulin formulations? Shara Elrod, PharmD, BCACP, BCGP Learning Objectives Review pharmacology and dosing of new insulin formulations Compare and contrast new insulin formulations
Are you ready for more insulin formulations? Shara Elrod, PharmD, BCACP, BCGP Learning Objectives Review pharmacology and dosing of new insulin formulations Compare and contrast new insulin formulations
Update on New Basal Insulins and Combinations: Starting, Titrating and Adding to Therapy
 Update on New Basal Insulins and Combinations: Starting, Titrating and Adding to Therapy Jerry Meece, BPharm, CDE, FACA, FAADE Director of Clinical Services Plaza Pharmacy and Wellness Center Gainesville,
Update on New Basal Insulins and Combinations: Starting, Titrating and Adding to Therapy Jerry Meece, BPharm, CDE, FACA, FAADE Director of Clinical Services Plaza Pharmacy and Wellness Center Gainesville,
Insulin Prior Authorization Criteria For Individuals who Purchased BlueCare / KS Solutions products
 Insulin Prior Authorization Criteria For Individuals who Purchased BlueCare / KS Solutions products FDA LABELED INDICATIONS 1-13,16-20 Rapid-Acting Indication Onset Peak Duration Insulins Fiasp (insulin
Insulin Prior Authorization Criteria For Individuals who Purchased BlueCare / KS Solutions products FDA LABELED INDICATIONS 1-13,16-20 Rapid-Acting Indication Onset Peak Duration Insulins Fiasp (insulin
INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE
 INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE OBJECTIVES DESCRIBE INSULIN, INCLUDING WHERE IT COMES FROM AND WHAT IT DOES STATE THAT
INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE OBJECTIVES DESCRIBE INSULIN, INCLUDING WHERE IT COMES FROM AND WHAT IT DOES STATE THAT
Drug Use Criteria: Exogenous Insulin Products
 Texas Vendor Program Use Criteria: Exogenous Products Publication History 1. Developed June 2017. Notes: Information on indications for use or diagnosis is assumed to be unavailable. All criteria may be
Texas Vendor Program Use Criteria: Exogenous Products Publication History 1. Developed June 2017. Notes: Information on indications for use or diagnosis is assumed to be unavailable. All criteria may be
Comprehensive Diabetes Treatment
 Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018
 Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
Converting lantus to humalog 75 25
 P ford residence southampton, ny Converting lantus to humalog 75 25 This page includes the following topics and synonyms: Insulin Dosing in Type 2 Diabetes, Insulin Dosing in Type II Diabetes. Thiazide
P ford residence southampton, ny Converting lantus to humalog 75 25 This page includes the following topics and synonyms: Insulin Dosing in Type 2 Diabetes, Insulin Dosing in Type II Diabetes. Thiazide
INSULIN 101: When, How and What
 INSULIN 101: When, How and What Alice YY Cheng @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
INSULIN 101: When, How and What Alice YY Cheng @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Mixed Insulins Pick Me
 Mixed Insulins Pick Me Alvin Goo, PharmD Clinical Associate Professor University of Washington School of Pharmacy and Department of Family Medicine Objectives Critically evaluate the evidence comparing
Mixed Insulins Pick Me Alvin Goo, PharmD Clinical Associate Professor University of Washington School of Pharmacy and Department of Family Medicine Objectives Critically evaluate the evidence comparing
Objectives. Recognize all available medical treatment options for diabetes. Individualize treatment and glycemic target based on patient factors
 No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
INSULIN INITIATION AND INTENSIFICATION WITH A FOCUS ON HYPOGLYCEMIA REDUCTION
 INSULIN INITIATION AND INTENSIFICATION WITH A FOCUS ON HYPOGLYCEMIA REDUCTION Jaiwant Rangi, MD, FACE Nov 10 th 2018 DISCLOSURES Speaker Novo Nordisk Sanofi-Aventis Boheringer Ingleheim Merck Abbvie Abbott
INSULIN INITIATION AND INTENSIFICATION WITH A FOCUS ON HYPOGLYCEMIA REDUCTION Jaiwant Rangi, MD, FACE Nov 10 th 2018 DISCLOSURES Speaker Novo Nordisk Sanofi-Aventis Boheringer Ingleheim Merck Abbvie Abbott
What the Pill Looks Like. How it Works. Slows carbohydrate absorption. Reduces amount of sugar made by the liver. Increases release of insulin
 Diabetes s Oral s - Pills These are some of the pills that are currently available in Canada to treat diabetes. Each medication has benefits and side effects you should be aware of. Your diabetes team
Diabetes s Oral s - Pills These are some of the pills that are currently available in Canada to treat diabetes. Each medication has benefits and side effects you should be aware of. Your diabetes team
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
Initiating Injectable Therapy in Type 2 Diabetes
 Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Update on Therapies for Type 2 Diabetes: Angela D. Mazza, DO July 31, 2015
 Update on Therapies for Type 2 Diabetes: 2015 Angela D. Mazza, DO July 31, 2015 Objectives To present the newer available therapies for the management of T2D To discuss the advantages and disadvantages
Update on Therapies for Type 2 Diabetes: 2015 Angela D. Mazza, DO July 31, 2015 Objectives To present the newer available therapies for the management of T2D To discuss the advantages and disadvantages
Insulin Basics. Bryan Primary Care Conference May 21, 2016 Shannon Wakeley MD Complete Endocrinology
 Insulin Basics Bryan Primary Care Conference May 21, 2016 Shannon Wakeley MD Complete Endocrinology Disclosures Speakers Bureau for Sanofi, Astra Zeneca, Janssen, Boehringer-Ingelheim Objectives Discuss
Insulin Basics Bryan Primary Care Conference May 21, 2016 Shannon Wakeley MD Complete Endocrinology Disclosures Speakers Bureau for Sanofi, Astra Zeneca, Janssen, Boehringer-Ingelheim Objectives Discuss
Management of Diabetes New Concepts New Devices New Medications. Richard J. Comi, MD Professor of Medicine Geisel School of Medicine at Dartmouth
 Management of Diabetes New Concepts New Devices New Medications Richard J. Comi, MD Professor of Medicine Geisel School of Medicine at Dartmouth Objectives: At the end of this lecture, the learner will
Management of Diabetes New Concepts New Devices New Medications Richard J. Comi, MD Professor of Medicine Geisel School of Medicine at Dartmouth Objectives: At the end of this lecture, the learner will
Disclosure 1/16/2017. Michael R. Brennan D.O., M.S., F.A.C.E Director Beaumont Endocrine Center Chief of Endocrine Beaumont Grosse Pointe 1/16/2017 2
 Therapy For Diabetes Michigan Association of Osteopathic Family Physicians Mid-Winter Family Medicine Update Shanty Creek Resort, MI January 19-22nd 2017 Michael R. Brennan D.O., M.S., F.A.C.E Director
Therapy For Diabetes Michigan Association of Osteopathic Family Physicians Mid-Winter Family Medicine Update Shanty Creek Resort, MI January 19-22nd 2017 Michael R. Brennan D.O., M.S., F.A.C.E Director
Diabetes in Pregnancy
 Diabetes in Pregnancy Ebony Boyce Carter, MD, MPH Division of Maternal Fetal Medicine Washington University School of Medicine Disclosures I have no financial disclosures to report. Objectives Review the
Diabetes in Pregnancy Ebony Boyce Carter, MD, MPH Division of Maternal Fetal Medicine Washington University School of Medicine Disclosures I have no financial disclosures to report. Objectives Review the
Soliqua (insulin glargine and lixisenatide), Xultophy (insulin degludec and liraglutide)
, Xultophy (insulin degludec and liraglutide)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.48 Subject: Insulin GLP-1 Combinations Page: 1 of 5 Last Review Date: September 15, 2017 Insulin GLP-1
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.48 Subject: Insulin GLP-1 Combinations Page: 1 of 5 Last Review Date: September 15, 2017 Insulin GLP-1
Lantus levemir conversion
 Lantus levemir conversion Search Learn about starting insulin-naïve patients with type 2 diabetes on Levemir. Read Important Safety & Prescribing Info on the HCP Website. Lantus and Levemir have a variety
Lantus levemir conversion Search Learn about starting insulin-naïve patients with type 2 diabetes on Levemir. Read Important Safety & Prescribing Info on the HCP Website. Lantus and Levemir have a variety
Let s not sugarcoat it! Update on Pharmacologic Management of Type II DM
 Let s not sugarcoat it! Update on Pharmacologic Management of Type II DM Gregory Castelli, PharmD, BCPS, BC-ADM Clinical Pharmacist UPMC St. Margaret Objectives By the end of this presentation, participants
Let s not sugarcoat it! Update on Pharmacologic Management of Type II DM Gregory Castelli, PharmD, BCPS, BC-ADM Clinical Pharmacist UPMC St. Margaret Objectives By the end of this presentation, participants
Diabetes Head to Toe May 31, 2017
 Innovations in Insulin Joanne Reid RN CDE jmreid@gbhs.on.ca Danielle Benedict RPh Outline Setting the stage Insulin as pancreas replacement therapy Commonly used insulins New insulins Case Studies Dosing
Innovations in Insulin Joanne Reid RN CDE jmreid@gbhs.on.ca Danielle Benedict RPh Outline Setting the stage Insulin as pancreas replacement therapy Commonly used insulins New insulins Case Studies Dosing
New Therapies for Diabetes Management: Hope or Headache?
 New Therapies for Diabetes Management: Hope or Headache? Elizabeth Stephens, MD, FACP PMG- Endocrinology Elizabeth.Stephens@providence.org November 2018 Disclosures None 1 Objectives Discussion of 3 rd
New Therapies for Diabetes Management: Hope or Headache? Elizabeth Stephens, MD, FACP PMG- Endocrinology Elizabeth.Stephens@providence.org November 2018 Disclosures None 1 Objectives Discussion of 3 rd
Type 2 Diabetes Mellitus Insulin Therapy 2012
 Type 2 Diabetes Mellitus Therapy 2012 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Preparations Onset Peak Duration
Type 2 Diabetes Mellitus Therapy 2012 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Preparations Onset Peak Duration
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Jessica Conklin, PharmD, PhC, BCACP, CDE, AAHIP Associate Professor, UNM College of Phar macy jeconklin@salud.unm.edu Luis Gonzales, PharmD, PhC UNM
What s New in Type 2 Diabetes? 2018 Diabetes Updates Jessica Conklin, PharmD, PhC, BCACP, CDE, AAHIP Associate Professor, UNM College of Phar macy jeconklin@salud.unm.edu Luis Gonzales, PharmD, PhC UNM
The York Diabetes Care Model
 This Session The York Diabetes Care Model The annual review what s it for and how to do it How to make the diagnosis of diabetes and who to test Categorisation of diabetes at diagnosis Basics of Insulin
This Session The York Diabetes Care Model The annual review what s it for and how to do it How to make the diagnosis of diabetes and who to test Categorisation of diabetes at diagnosis Basics of Insulin
INSULIN OVERVIEW. Type Brand Name Onset Peak Duration Role in glucose management Page Rapid-Acting lispro min. 3-5 hrs min.
 INSULIN OVERVIEW Type Brand Name Onset Peak Duration Role in glucose management Page Rapid-Acting lispro Humalog 15-30 min 30-90 min 3-5 hrs aspart glulisine Short-Acting Regular insulin NovoLog Apidra
INSULIN OVERVIEW Type Brand Name Onset Peak Duration Role in glucose management Page Rapid-Acting lispro Humalog 15-30 min 30-90 min 3-5 hrs aspart glulisine Short-Acting Regular insulin NovoLog Apidra
Individualizing Care for Patients with Type 2 Diabetes
 Individualizing Care for Patients with Type 2 Diabetes Disclosures Speaker: AstraZeneca, Novo Nordisk, BI/Lilly, Valeritas, Takeda Advisor: Tandem Diabetes, Sanofi Objectives Develop individualized approaches
Individualizing Care for Patients with Type 2 Diabetes Disclosures Speaker: AstraZeneca, Novo Nordisk, BI/Lilly, Valeritas, Takeda Advisor: Tandem Diabetes, Sanofi Objectives Develop individualized approaches
Initiation and Titration of Insulin in Diabetes Mellitus Type 2
 Initiation and Titration of Insulin in Diabetes Mellitus Type 2 Greg Doelle MD, MS April 6, 2016 Disclosure I have no actual or potential conflicts of interest in relation to the content of this lecture.
Initiation and Titration of Insulin in Diabetes Mellitus Type 2 Greg Doelle MD, MS April 6, 2016 Disclosure I have no actual or potential conflicts of interest in relation to the content of this lecture.
Antihyperglycemic Agents in Diabetes. Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014
 Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Insulin Management and Advancing Practice of the Registered Dietitian Nutritionist (RDN) in Diabetes Care
 in Diabetes Care") Insulin Management and Advancing Practice of the Registered Dietitian Nutritionist (RDN) in Diabetes Care Patricia Davidson, DCN, RDN, CDE, LDN, FAND West Chester University of Pennsylvania West Chester,
Insulin Management and Advancing Practice of the Registered Dietitian Nutritionist (RDN) in Diabetes Care Patricia Davidson, DCN, RDN, CDE, LDN, FAND West Chester University of Pennsylvania West Chester,
These Aren t Your Average Rookies: A Primer on New and Emerging Insulins. Alissa R. Segal, Pharm.D, CDE, CDTC, FCCP
 These Aren t Your Average Rookies: A Primer on New and Emerging Insulins Alissa R. Segal, Pharm.D, CDE, CDTC, FCCP Disclosures Eli Lilly & Company: Advisory board member Boehringer Ingelheim: Advisory
These Aren t Your Average Rookies: A Primer on New and Emerging Insulins Alissa R. Segal, Pharm.D, CDE, CDTC, FCCP Disclosures Eli Lilly & Company: Advisory board member Boehringer Ingelheim: Advisory
5/16/2018. Insulin Update: New and Emerging Insulins. Disclosures to Participants. Learning Objectives
 Insulin Update: New and Emerging Insulins Joshua J. Neumiller, PharmD, CDE, FASCP Vice Chair & Associate Professor, Department of Pharmacotherapy Washington State University Spokane, WA Disclosures to
Insulin Update: New and Emerging Insulins Joshua J. Neumiller, PharmD, CDE, FASCP Vice Chair & Associate Professor, Department of Pharmacotherapy Washington State University Spokane, WA Disclosures to
In-Hospital Management of Diabetes. Dr Benjamin Schiff Assistant Professor McGill University
 In-Hospital Management of Diabetes Dr Benjamin Schiff Assistant Professor McGill University No conflict of interest to declare CLINICAL SCENARIO 62 y/o male with hx of DM 2, COPD, and HT is admitted with
In-Hospital Management of Diabetes Dr Benjamin Schiff Assistant Professor McGill University No conflict of interest to declare CLINICAL SCENARIO 62 y/o male with hx of DM 2, COPD, and HT is admitted with
Degludec lantus conversion
 Degludec lantus conversion Search embarazadas con elevado riesgo de enfermedad tiroidea usando la. There are various possible causes of a high blood sugar level in the morning: The Dawn Phenomenon which
Degludec lantus conversion Search embarazadas con elevado riesgo de enfermedad tiroidea usando la. There are various possible causes of a high blood sugar level in the morning: The Dawn Phenomenon which
Nph insulin conversion to lantus
 Nph insulin conversion to lantus Search 26-2-2003 RESPONSE FROM AVENTIS. We appreciate the opportunity to respond to Dr. Grajower s request for information regarding Lantus ( insulin glargine [rdna origin.
Nph insulin conversion to lantus Search 26-2-2003 RESPONSE FROM AVENTIS. We appreciate the opportunity to respond to Dr. Grajower s request for information regarding Lantus ( insulin glargine [rdna origin.
Insulin Initiation and Intensification. Disclosure. Objectives
 Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Agenda. Indications Different insulin preparations Insulin initiation Insulin intensification
 Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
AACN PCCN Review. Endocrine
 AACN PCCN Review Endocrine Presenter: Carol A. Rauen, RN, MS, CCNS, CCRN, PCCN, CEN Independent Clinical Nurse Specialist & Education Consultant rauen.carol104@gmail.com Endocrine I. INTRODUCTION Disorders
AACN PCCN Review Endocrine Presenter: Carol A. Rauen, RN, MS, CCNS, CCRN, PCCN, CEN Independent Clinical Nurse Specialist & Education Consultant rauen.carol104@gmail.com Endocrine I. INTRODUCTION Disorders
Diabetes Mellitus II CPG
 1 Diabetes Mellitus II CPG Candidates for Screening Integrated Complex Care Patients: Check Yearly Prediabetes: Check Yearly No Diabetes Mellitus (DM) Risk Factors: Check at Age 45, Repeat Every 3 Years
1 Diabetes Mellitus II CPG Candidates for Screening Integrated Complex Care Patients: Check Yearly Prediabetes: Check Yearly No Diabetes Mellitus (DM) Risk Factors: Check at Age 45, Repeat Every 3 Years
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Pharmacology Updates. Quang T Nguyen, FACP, FACE, FTOS 11/18/17
 Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Update on Insulin-based Agents for T2D
 Update on Insulin-based Agents for T2D Injectable Therapies for Type 2 Diabetes Mellitus (T2DM) and Obesity This presentation will: Describe established and newly available insulin therapies for treatment
Update on Insulin-based Agents for T2D Injectable Therapies for Type 2 Diabetes Mellitus (T2DM) and Obesity This presentation will: Describe established and newly available insulin therapies for treatment
I. General Considerations
 1 2 3 I. General Considerations A. Type I ( Juvenile Onset or IDDM) IDDM results from autoimmune destruction of beta cells inability to secrete insulin --> ketone formation --> DKA 4 Diabetic Ketoacidosis
1 2 3 I. General Considerations A. Type I ( Juvenile Onset or IDDM) IDDM results from autoimmune destruction of beta cells inability to secrete insulin --> ketone formation --> DKA 4 Diabetic Ketoacidosis
Pediatric Diabetes Update Fran R. Cogen, MD, CDE Professor of Pediatrics Director, Diabetes Services
 1.19.18 Pediatric Diabetes Update Fran R. Cogen, MD, CDE Professor of Pediatrics Director, Diabetes Services DISCLOSURES 1. No financial incentives 2. Volunteer Positions 1. National Certification Board
1.19.18 Pediatric Diabetes Update Fran R. Cogen, MD, CDE Professor of Pediatrics Director, Diabetes Services DISCLOSURES 1. No financial incentives 2. Volunteer Positions 1. National Certification Board
STEP THERAPY CRITERIA
 CATEGORY DRUG CLASS BRAND NAME (generic) STEP THERAPY CRITERIA AMYLIN ANALOG: SYMLIN/SYMLINPEN (pramlintide acetate) ANTIDIABETIC AGENTS GLUCAGON-LIKE PEPTIDE-1 RECEPTOR AGONIST (GLP-1): ADLYXIN (lixisenatide)
CATEGORY DRUG CLASS BRAND NAME (generic) STEP THERAPY CRITERIA AMYLIN ANALOG: SYMLIN/SYMLINPEN (pramlintide acetate) ANTIDIABETIC AGENTS GLUCAGON-LIKE PEPTIDE-1 RECEPTOR AGONIST (GLP-1): ADLYXIN (lixisenatide)
The New Age of Insulin: Exploring the Latest Trends in Insulin Therapy. The New Age of Insulin: Exploring the Latest Trends in Insulin Therapy
 The New Age of Insulin: Exploring the Latest Trends in Insulin Therapy Susan Cornell, PharmD, CDE, FAPhA, FAADE Associate Director of Experiential Education Associate Professor of Pharmacy Practice Midwestern
The New Age of Insulin: Exploring the Latest Trends in Insulin Therapy Susan Cornell, PharmD, CDE, FAPhA, FAADE Associate Director of Experiential Education Associate Professor of Pharmacy Practice Midwestern
Lantus to levemir conversion
 Lantus to levemir conversion The Borg System is 100 % Lantus to levemir conversion 16-6-2005 Ask the Expert on... Lantus Conversion. Karen Shapiro, PharmD, BCPS. Disclosures. June 16, 2005. Question. Would
Lantus to levemir conversion The Borg System is 100 % Lantus to levemir conversion 16-6-2005 Ask the Expert on... Lantus Conversion. Karen Shapiro, PharmD, BCPS. Disclosures. June 16, 2005. Question. Would
Drug Effectiveness Review Project Summary Report Long acting Insulins
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Objectives 2/13/2013. Figuring out the dose. Sub Optimal Glycemic Control: Moving to the Appropriate Treatment
 Sub Optimal Glycemic Control: Moving to the Appropriate Treatment Judy Thomas, MSN, FNP-BC Holt and Walton, Rheumatology and Endocrinology Objectives Upon completion of this session you will be better
Sub Optimal Glycemic Control: Moving to the Appropriate Treatment Judy Thomas, MSN, FNP-BC Holt and Walton, Rheumatology and Endocrinology Objectives Upon completion of this session you will be better
Update on Insulin-based Agents for T2D. Harry Jiménez MD, FACE
 Update on Insulin-based Agents for T2D Harry Jiménez MD, FACE Harry Jiménez MD, FACE Has received honorarium as Speaker and/or Consultant for the following pharmaceutical companies: Eli Lilly Merck Boehringer
Update on Insulin-based Agents for T2D Harry Jiménez MD, FACE Harry Jiménez MD, FACE Has received honorarium as Speaker and/or Consultant for the following pharmaceutical companies: Eli Lilly Merck Boehringer
Management: How Can We Do Better? Lori B. Sweeney, MD 2018 Virginia ACP Clinical Update March 17, 2018
 Management: How Can We Do Better? Lori B. Sweeney, MD 2018 Virginia ACP Clinical Update March 17, 2018 Disclosures I have no Objectives Use a case-based format to discuss diabetes management pearls Discuss
Management: How Can We Do Better? Lori B. Sweeney, MD 2018 Virginia ACP Clinical Update March 17, 2018 Disclosures I have no Objectives Use a case-based format to discuss diabetes management pearls Discuss
Diabetes Meds Update Disclaimer and Important Info. Objectives. Page 1. Copyright , Diabetes Education Services
 Diabetes Meds Update 2016 Beverly Dyck Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Disclaimer and Important Info This content is for educational purposes only. Please see Package
Diabetes Meds Update 2016 Beverly Dyck Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Disclaimer and Important Info This content is for educational purposes only. Please see Package
Objectives. How Medicine Works to Control Blood Sugar Levels. What Happens When We Eat? What is diabetes? High Blood Glucose (Hyperglycemia)
") How Medicine Works to Control Blood Sugar Levels Stacie Petersen, RN, CDE Objectives Define Diabetes List how medications work (ominous octet) Identify side effects of medications for diabetes What is
How Medicine Works to Control Blood Sugar Levels Stacie Petersen, RN, CDE Objectives Define Diabetes List how medications work (ominous octet) Identify side effects of medications for diabetes What is
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery
 Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
Reviewing Diabetes Guidelines. Newsletter compiled by Danny Jaek, Pharm.D. Candidate
 Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
GLUCAGON LIKE PEPTIDE (GLP) 1 AGONISTS FOR THE TREATMENT OF TYPE 2 DIABETES, WEIGHT CONTROL AND CARDIOVASCULAR PROTECTION.
 1 AGONISTS FOR THE TREATMENT OF TYPE 2 DIABETES, WEIGHT CONTROL AND CARDIOVASCULAR PROTECTION.") GLUCAGON LIKE PEPTIDE (GLP) 1 AGONISTS FOR THE TREATMENT OF TYPE 2 DIABETES, WEIGHT CONTROL AND CARDIOVASCULAR PROTECTION. Patricia Garnica MS, ANP-BC, CDE, CDTC Inpatient Diabetes Nurse Practitioner North
GLUCAGON LIKE PEPTIDE (GLP) 1 AGONISTS FOR THE TREATMENT OF TYPE 2 DIABETES, WEIGHT CONTROL AND CARDIOVASCULAR PROTECTION. Patricia Garnica MS, ANP-BC, CDE, CDTC Inpatient Diabetes Nurse Practitioner North
GLP-1 receptor agonists for type 2 diabetes currently available in the U.S.
 GLP-1 receptor agonists for type 2 diabetes currently available in the U.S. GLP-1 agonists are a class of antidiabetic agents that mimic the actions of the glucagon-like peptide. GLP-1 is one of several
GLP-1 receptor agonists for type 2 diabetes currently available in the U.S. GLP-1 agonists are a class of antidiabetic agents that mimic the actions of the glucagon-like peptide. GLP-1 is one of several
Clinical Practice Guidelines
 Clinical Practice Guidelines Diabetes Objective The purpose is to guide the appropriate diagnosis and management of Diabetes. This guideline is designed to assist the clinician by providing a framework
Clinical Practice Guidelines Diabetes Objective The purpose is to guide the appropriate diagnosis and management of Diabetes. This guideline is designed to assist the clinician by providing a framework
New Drug Evaluation: Insulin degludec/aspart, subcutaneous injection
 New Drug Evaluation: Insulin degludec/aspart, subcutaneous injection Date of Review: March 2016 End Date of Literature Search: November 11, 2015 Generic Name: Insulin degludec and insulin aspart Brand
New Drug Evaluation: Insulin degludec/aspart, subcutaneous injection Date of Review: March 2016 End Date of Literature Search: November 11, 2015 Generic Name: Insulin degludec and insulin aspart Brand
Clinical Cases in Diabetes Management. Joseph Cook D.O.
 Clinical Cases in Diabetes Management Joseph Cook D.O. Objectives State the prevalence of Diabetes Mellitus in Ohio State the percentage of diabetic patients in the U.S. treated by Primary Care Physicians
Clinical Cases in Diabetes Management Joseph Cook D.O. Objectives State the prevalence of Diabetes Mellitus in Ohio State the percentage of diabetic patients in the U.S. treated by Primary Care Physicians
Diabetes Related Disclosures
 Diabetes Related Disclosures Speakers Bureau Amylin Boehringer Ingelheim Eli Lilly Takeda Classification of Diabetes Diabetes Care January 2011 vol. 34 no. Supplement 1 S11-S61 Type 1 Diabetes Mellitus
Diabetes Related Disclosures Speakers Bureau Amylin Boehringer Ingelheim Eli Lilly Takeda Classification of Diabetes Diabetes Care January 2011 vol. 34 no. Supplement 1 S11-S61 Type 1 Diabetes Mellitus
Type I Type II Insulin Resistance
 Insulin An aqueous hormonal solution made in the pancreas. Affects metabolism by allowing glucose to leave the blood and enter the body cells, preventing hyperglycemia. It is measured in units, e.g. 100
Insulin An aqueous hormonal solution made in the pancreas. Affects metabolism by allowing glucose to leave the blood and enter the body cells, preventing hyperglycemia. It is measured in units, e.g. 100
Medications for Diabetes
 Medications for Diabetes Sweet, but not too sweet Colette Raymond, Pharm D June 15, 2011 Learning Objectives At the end of this presentation you should be able to: Understand the prevalence and types of
Medications for Diabetes Sweet, but not too sweet Colette Raymond, Pharm D June 15, 2011 Learning Objectives At the end of this presentation you should be able to: Understand the prevalence and types of
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Afrezza Page 1 of 7 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Afrezza (human insulin) Prime Therapeutics will review Prior Authorization requests Prior Authorization
Afrezza Page 1 of 7 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Afrezza (human insulin) Prime Therapeutics will review Prior Authorization requests Prior Authorization
UKPDS: Over Time, Need for Exogenous Insulin Increases
 UKPDS: Over Time, Need for Exogenous Insulin Increases Patients Requiring Additional Insulin (%) 60 40 20 Oral agents By 6 Chlorpropamide years, Glyburide more than 50% of UKPDS patients required insulin
UKPDS: Over Time, Need for Exogenous Insulin Increases Patients Requiring Additional Insulin (%) 60 40 20 Oral agents By 6 Chlorpropamide years, Glyburide more than 50% of UKPDS patients required insulin
Images have been removed from the PowerPoint slides in this handout due to copyright restrictions. Insulins. Rapid Short Intermediate Long Mix
 Diabetes Medications Diabetes Medications Type 1 Insulin is needed Type 2 Oral Diabetes Medications Or Oral Diabetes Medications plus Insulin Or Insulin Alone Diabetes Medications Secretagogues Glipizide
Diabetes Medications Diabetes Medications Type 1 Insulin is needed Type 2 Oral Diabetes Medications Or Oral Diabetes Medications plus Insulin Or Insulin Alone Diabetes Medications Secretagogues Glipizide
Xultophy 100/3.6. (insulin degludec, liraglutide) New Product Slideshow
 New Product Slideshow") Xultophy 100/3.6 (insulin degludec, liraglutide) New Product Slideshow Introduction Brand name: Xultophy Generic name: Insulin degludec, liraglutide Pharmacological class: Human insulin analog + glucagon-like
Xultophy 100/3.6 (insulin degludec, liraglutide) New Product Slideshow Introduction Brand name: Xultophy Generic name: Insulin degludec, liraglutide Pharmacological class: Human insulin analog + glucagon-like
Learning Objectives. Perioperative SWEET Success
 Perioperative SWEET Success PERIOPERATIVE SWEET SUCCESS PRESENTED BY: KENDRA MARTIN, RN, BSN, CDE JENNIFER SIMPSON, RN, BC-ADM, MSN, CNS Disclosure to Participants Notice of Requirements For Successful
Perioperative SWEET Success PERIOPERATIVE SWEET SUCCESS PRESENTED BY: KENDRA MARTIN, RN, BSN, CDE JENNIFER SIMPSON, RN, BC-ADM, MSN, CNS Disclosure to Participants Notice of Requirements For Successful
Incredible Incretins Abby Frye, PharmD, BCACP
 Incredible Incretins Abby Frye, PharmD, BCACP Objectives & Disclosures Review the pathophysiology of T2DM and the impact of the incretin system Describe the defining characteristics of the available glucagonlike
Incredible Incretins Abby Frye, PharmD, BCACP Objectives & Disclosures Review the pathophysiology of T2DM and the impact of the incretin system Describe the defining characteristics of the available glucagonlike
The Many Faces of T2DM in Long-term Care Facilities
 The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
Starting and Helping People with Type 2 Diabetes on Insulin
 Starting and Helping People with Type 2 Diabetes on Insulin Elaine Cooke, BSc(Pharm), RPh, CDE Pharmacist and Certified Diabetes Educator Maple Ridge, BC Objectives After attending this session, participants
Starting and Helping People with Type 2 Diabetes on Insulin Elaine Cooke, BSc(Pharm), RPh, CDE Pharmacist and Certified Diabetes Educator Maple Ridge, BC Objectives After attending this session, participants
Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM
 Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM Disclosures Jennifer D Souza has no conflicts of interest to disclose. 2 When Basal Insulin Is Not Enough Learning
Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM Disclosures Jennifer D Souza has no conflicts of interest to disclose. 2 When Basal Insulin Is Not Enough Learning
GLP-1 (glucagon-like peptide-1) Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary
 Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary") OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
Insulin Regimens: Hitting Glycemia Targets
 Insulin Regimens: Hitting Glycemia Targets Grant Kelley MD March 1 st, 2018 Faculty Disclosure: Financial relationships with commercial interests None Overview Mortality and Morbidity Insulin and Insulin
Insulin Regimens: Hitting Glycemia Targets Grant Kelley MD March 1 st, 2018 Faculty Disclosure: Financial relationships with commercial interests None Overview Mortality and Morbidity Insulin and Insulin
!"#$%&%'(!)*+'(,(&)%-!'(.#!%('"./0%(( /1#).!(&2()!(((
*+'(,(&)%-!'(.#!%('./0%(( /1#).!(&2()!(((") !"#%&%'(!)*+'(,(&)%-!'(.#!%('"./0%(( /1#).!(&2()!((( 26%5&"7%'( At the end of this presentation, participants should be able to: Evaluate the emerging role of GLP-1 Agonists for weight loss Understand
!"#%&%'(!)*+'(,(&)%-!'(.#!%('"./0%(( /1#).!(&2()!((( 26%5&"7%'( At the end of this presentation, participants should be able to: Evaluate the emerging role of GLP-1 Agonists for weight loss Understand
Inpatient Glycemic Management:
 Disclosure to Participants Conflict of Interest (COI) and Financial Relationship Disclosures: Dr. Seley attended Advisory Board Meeting: Alliance (Boehringer-Ingelheim/Lilly) Bayer Diabetes Care Sanofi
Disclosure to Participants Conflict of Interest (COI) and Financial Relationship Disclosures: Dr. Seley attended Advisory Board Meeting: Alliance (Boehringer-Ingelheim/Lilly) Bayer Diabetes Care Sanofi
Insulins: Prices, Rebates, and Other Factors Influencing Costs. May 2018
 Insulins: Prices, Rebates, and Other Factors Influencing Costs May 2018 Introduction: Types of Insulin Types of Insulin Rapid-acting: Usually taken before a meal to cover the blood glucose elevation from
Insulins: Prices, Rebates, and Other Factors Influencing Costs May 2018 Introduction: Types of Insulin Types of Insulin Rapid-acting: Usually taken before a meal to cover the blood glucose elevation from
Basal Bolus Insulin Therapy Frequently Asked Questions
 1. What is Basal Bolus Insulin Therapy (BBIT)? 2. What evidence supports the use of subcutaneous Basal Bolus Insulin Therapy? 3. Does Basal Bolus Insulin Therapy apply to all patients? 4. What s wrong
1. What is Basal Bolus Insulin Therapy (BBIT)? 2. What evidence supports the use of subcutaneous Basal Bolus Insulin Therapy? 3. Does Basal Bolus Insulin Therapy apply to all patients? 4. What s wrong
4/16/2018. Flexible Intensive Insulin Therapy (FIIT) in People with Type 2 Diabetes: A Viable Option. Disclosures. Outline. No financial disclosures
 in People with Type 2 Diabetes: A Viable Option. Disclosures. Outline. No financial disclosures") Flexible Intensive Insulin Therapy (FIIT) in People with Type Diabetes: A Viable Option Kim Bisanz, MFCS, RDN, LDN, CDE Minnesota Academy of Nutrition & Dietetics Annual Meeting April 19, 18 18 MFMER slide-1
Flexible Intensive Insulin Therapy (FIIT) in People with Type Diabetes: A Viable Option Kim Bisanz, MFCS, RDN, LDN, CDE Minnesota Academy of Nutrition & Dietetics Annual Meeting April 19, 18 18 MFMER slide-1
Intensification of Diabetic Therapy. Case studies
 Intensification of Diabetic Therapy Case studies Patient #1 1 st visit: 64 year old male, H/O prediabetes, lost weight 280 lbs. to 240 lbs. ER for dental abscess, glucose >300 A1C 11.4%, no diabetic medication,
Intensification of Diabetic Therapy Case studies Patient #1 1 st visit: 64 year old male, H/O prediabetes, lost weight 280 lbs. to 240 lbs. ER for dental abscess, glucose >300 A1C 11.4%, no diabetic medication,
Providing Stability to an Unstable Disease
 Basal Insulin Therapy Providing Stability to an Unstable Disease Thomas A. Hughes, M.D. Professor of Medicine - Retired Division of Endocrinology, Metabolism, and Diabetes University of Tennessee Health
Basal Insulin Therapy Providing Stability to an Unstable Disease Thomas A. Hughes, M.D. Professor of Medicine - Retired Division of Endocrinology, Metabolism, and Diabetes University of Tennessee Health
Adlyxin. (lixisenatide) New Product Slideshow
 New Product Slideshow") Adlyxin (lixisenatide) New Product Slideshow Introduction Brand name: Adlyxin Generic name: Lixisenatide Pharmacological class: Glucagon-like peptide-1 (GLP-1) receptor agonist Strength and Formulation:
Adlyxin (lixisenatide) New Product Slideshow Introduction Brand name: Adlyxin Generic name: Lixisenatide Pharmacological class: Glucagon-like peptide-1 (GLP-1) receptor agonist Strength and Formulation:
Diabetic Ketoacidosis
 October 2015 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Case History HPI: 24 yo man with recent 8 lb. weight loss, increased thirst and frequent
October 2015 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Case History HPI: 24 yo man with recent 8 lb. weight loss, increased thirst and frequent
Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial Treatment Protocols. Askiel Bruno, MD, MS Protocol PI
 Trial Treatment Protocols. Askiel Bruno, MD, MS Protocol PI") Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial Treatment Protocols Askiel Bruno, MD, MS Protocol PI SHINE Synopsis Acute ischemic stroke
Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial Treatment Protocols Askiel Bruno, MD, MS Protocol PI SHINE Synopsis Acute ischemic stroke
NEW DIABETES CARE MEDICATIONS
 NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
Application of the Diabetes Algorithm to a Patient
 Application of the Diabetes Algorithm to a Patient Apply knowledge gained from this activity to improve disease management and outcomes for patients with T2DM and obesity Note: The cases in this deck represent
Application of the Diabetes Algorithm to a Patient Apply knowledge gained from this activity to improve disease management and outcomes for patients with T2DM and obesity Note: The cases in this deck represent
Position Statement of ADA / EASD 2012
 Management of Hyperglycemia in Type2 Diabetes: A Patient- Centered Approach Position Statement of ADA / EASD 2012 Cause of : Type 2 diabetes Cardiovascular disorders Blindness End-stage renal failure Amputations
Management of Hyperglycemia in Type2 Diabetes: A Patient- Centered Approach Position Statement of ADA / EASD 2012 Cause of : Type 2 diabetes Cardiovascular disorders Blindness End-stage renal failure Amputations
Learning Objectives. Outline 4/3/2018. Treatment Strategies to Maximize the Value of Diabetes Medications
 Treatment Strategies to Maximize the Value of Diabetes Medications Presenters: Jennifer Toy, PharmD, BCACP and Crystal Zhou, PharmD, APh AHSCP, BCACP Learning Objectives 1. Discuss which patients may benefit
Treatment Strategies to Maximize the Value of Diabetes Medications Presenters: Jennifer Toy, PharmD, BCACP and Crystal Zhou, PharmD, APh AHSCP, BCACP Learning Objectives 1. Discuss which patients may benefit
ANGELA GINN-MEADOW RD LDN CDE
 DIABETES DRUGS & TRENDS MADE SIMPLE PHARMD TO RD ANGELA GINN-MEADOW RD LDN CDE OBJECTIVES At the end of this presentation, participants should be able to: Evaluate the emerging role of GLP-1 Agonists for
DIABETES DRUGS & TRENDS MADE SIMPLE PHARMD TO RD ANGELA GINN-MEADOW RD LDN CDE OBJECTIVES At the end of this presentation, participants should be able to: Evaluate the emerging role of GLP-1 Agonists for