ahus: Facts, Controversies & Treatment Updates Patrick D. Brophy MD Pediatric Nephrology, Dialysis & Transplant University of Iowa
|
|
|
- Marybeth Horn
- 5 years ago
- Views:
Transcription
1 ahus: Facts, Controversies & Treatment Updates Patrick D. Brophy MD Pediatric Nephrology, Dialysis & Transplant University of Iowa
2 DISCLOSURE STATEMENT I, Patrick Brophy disclose the following relationships. Any real or apparent conflicts of interest related to the content of this presentation have been resolved. Affiliation / Financial Interest Advisor Organization Alexion International Atypical Hemolytic Uremic Syndrome Advisory Board The following presentation will not discuss unapproved or off-label, experimental or investigational use of medications.
3 Objectives Review the diagnosis of ahus What its is Genetics behind it Case presentations Diagnostic dilemmas Treatment option Old & New Homegrown perspectives
4 ahus FACTS


5 ahus? TTP HIT AMR ahus STEC HUS AKI DIC TMA ITP HELLP MAHA SIRS AI
6 A Classification of TMA (Thrombotic Microangiopathy) Typical / diarrheal Complement defects von Willebrand proteinase (ADAMSTS13) defeciency Cobalamin-C deficiency Quinine-related Post transplantation (calcineurin inhibitior related) (HUS or TTP) Atypical HUS Generally TTP TMA + multiorgan failure Abrupt TMA, exposure related De-novo renal TMA May be renal isolated Others: HIV, radiation, chemotherapy HELLP, antiphospholipid Ab syndrome, unclassified Besbas et al. Kidney International 2006
7 Typical HUS Triad of : Microangiopathic hemolytic anemia Thrombocytopenia Acute kidney injury Generally diarrhea-associated Shiga toxin produced by E coli serotype O157:H7 Shigella, Salmonella, others also Food borne disease: uncooked / unpasteurized products contaminated by animal wastes Or other infections (respiratory): Invasive S. Pneumoniae or viral infections
8 Typical HUS A severe condition: acutely 2.5% mortality, often significant morbidity Long term results (10-20 years after HUS*) 63% Complete recovery 12% Recovery with proteinuria 6% Recovery with proteinuria and HTN 16% Recovery with low GFR ± proteinuria or HTN 3% ESRD * Diarrheal or URI- related only, pediatric Spizzirri et al. Pediatric Nephrology 1996
9 Atypical HUS Clinically very severe 15% died 25% ESRD 60% major sequelae 15% renal insufficiency 1/3 recover without significant renal disease most (75%) of these had a single episode few (25%) of these had recurrent ahus (a pediatric series) Taylor et al Ped Neph 2004
10 R/O STEC HUS R/O Streptococcus pneumoniae infection R/O Thrombotic thrombocytopenia purpura R/O Other secondary causes of TMA R/O Cobalamin metabolism abnormality (i.e. methyl-malonic aciduria)) R/O Rheumatologic Disease R/O HIV R/O Pregnancy Associated TMA/HELLP Syndrome Rule in Complement Pathway Abnormality Laboratory evaluation of suspected ahus Stool or rectal swab: culture for STEC; PCR for Stx Serum: Antibody testing Blood cultures, pulmonary cultures Plasma ADAMTS13 activity ± inhibitor Blood pressure, pancreatitis, malignancy, medication Homocysteine, Methionine, urine organic acid testing Consider genetic testing for mutation in MMACHC gene Antinuclear antibody, lupus anticoagulant, anti-phospholipid antibodies HIV Serology Pregnancy test, liver enzymes. Good Clinical History C3, Factor H, Factor I, Factor B serology Anti-factor H autoantibodies MCP - surface expression on leucocytes by FACS Gene mutation analysis for CFH, CFI, CFB, C3, CFHR5, MCP and CFHR1/3 Deletion
11 Complement and Atypical HUS Since the early 1970 s alternative pathway complement activation (low C3), has been recognized in some cases of atypical HUS 1981: 1 st case of HUS with factor H deficiency described 1998: Linkage analysis in 3 families with HUS provided clear association with CFH Clin. Exp. Immunol. (1981), Kidney International (1998)


12 Atypical HUS COMPLEMENT DYSREGULATION complement components and pathways Janeway, C, et al, Immunobiology, New York: Garland Science, 2005.
13 The Alternate Complement Pathway Remuzzi, NEJM, ;17 13

14 Atypical HUS COMPLEMENT DYSREGULATION complement regulation


15 Atypical HUS COMPLEMENT DYSREGULATION pathogenesis of atypical HUS infection/inflammation increases rate of C3b formation activates complement cascade and C3a/C5a C3a/C5a attract leukocytes, producing TNF and IL-8 cytokines cause endothelial damage and exposure of extracellular matrix ECM exposure amplifies deposition of C3b and complement activation lack of normal factor H, factor I, or MCP results in unchecked activation progressive tissue damage occurs
16 Atypical HUS COMPLEMENT DYSREGULATION FH, FI, and MCP deficiency have incomplete penetrance disease modifiers or other factors may have role environmental triggers infections preceded 70% of those with FH mutation 60% of those with FI mutation 100% of cases of HUS in MCP-mutants pregnancy trigger in 4% of FH-HUS 40% of FI-HUS multiple-hits one pedigree in which atypical HUS occurred only with inheritance of ALL: MCP P131S mutation MCP promoter polymorphism dinucleotide insertion into FI gene resulted in 50% expression level of each protein Richards, A, 2007, Mol Immunol 44:
17 Atypical HUS COMPLEMENT DYSREGULATION outcomes of atypical HUS overall 50% of patients develop ESRD 25% mortality during acute illness end-stage renal disease 70% with FH-deficiency HUS develop ESRD or die >60% with FI-deficiency HUS develop ESRD 86% with MCP-deficiency HUS remain dialysis-free 70% had recurrence of HUS Richards, A, 2007, Mol Immunol 44:
18 SUMMARY Zipfel, PF, et al, 2006, Semin Thromb Hemost 32:
19 Genetic Abnormalities and Clinical Outcome in Patients with Atypical Hemolytic Uremic Syndrome Gene Protein Affected Main Effect Frequency Response to Plasma Therapy Long-term Outcome Outcome of Kidney Transplant CFH CFHR1/3 Factor H Factor HR1, R3 No binding to endothelium 20-30% 60% Remission ESRD in 70-80% 80-90% Recurrence Anti-factor H Antibodies 6% 70-80% Remission ESRD in 30-40% 20% Recurrence MCP Membrane cofactor protein No surface expression 10-15% No definitive indication for Therapy ESRD in <20% 15-20% Recurrence CFI Factor I Low level or low cofactor activity 4-10% 30-40% Remission ESRD in 60-70% 70-80% Recurrence CFB Factor B C3 Convertase stabilization 1-2% 30% Remission ESRD in 70% Recurrence in one case C3 Complement C3 Resistance to C3b inactivation 5-10% 40-50% Remission ESRD in 60% 40-50% Recurrence THBD Thrombomodulin Reduced C3b inactivation 5% 60% Remission ESRD in 60% Recurrence in one case Adapted from Remuzzi, NEJM, ;17 19
20 Atypical HUS COMPLEMENT DYSREGULATION factor H, factor I, or MCP deficiency accounts for 50% of atypical HUS FACTOR H 150kD plasma glycoprotein synthesized in liver 20 homologous units of 61 residues (short consensus repeats SCRs) N-terminal domains SCR1 SCR4 bind C3b complement decay accelerating activity located here H = three heparin binding sites tertiary structure through to be bent backwards exposes C-terminal SCR20 functions as co-factor for factor I-mediated degradation of C3b,Bb
21 Atypical HUS FACTOR H DEFICIENCY thought to account for 10-22% of atypical HUS cases reported in both familial and sporadic forms usually presents in infancy or early childhood, but may present in adulthood one study of 16 FH-deficient patients 6 with homozygous deficiency 4 had membranoproliferative glomerulonephritis 2 had atypical HUS 10 had heterozygous deficiency all developed atypical HUS homozygotes had low levels of FH, C3, FB and CH 50 heterozygotes had low to normal values some patients present with meningococcal infections acquired C3 or terminal C deficiencies some present with SLE, having combined FH and C2 deficiency Dragon-Durey, M-A, et al, 2004, J Am Soc Nephrol 15:
22 Atypical HUS FACTOR H DEFICIENCY 69 different FH mutations identified to date 3 patients have been described with atypical HUS and acquired anti-fh autoantibodies
23 Atypical HUS FACTOR I 88kD plasma serine protease synthesized in liver N-terminal heavy chain LDL-receptor domains x2 CD5 domain FIMAC domain (factor I membrane attack complex) C-terminal catalytic domain functions to directly cleave C4b or C3b to inactivate complement efficient cleavage requires co-factors (C4bp, FH, MCP)
24 Atypical HUS FACTOR I DEFICIENCY reported only in sporadic forms of atypical HUS in one study, 2 out of 76 patients with atypical HUS had FI deficiency most reported cases involve hyterozygous mutations no increased susceptibility to infection homozygous FI deficiency associated with increased infection susceptibility encapsulated organisms (meningococcus, pneumococcus, hemophilus) acquired C3 deficiency due to uncontrolled consumption variable penetrance and expressivity C3 can be low to normal Dragon-Durey, M-A, et al, 2005, Springer Semin Immun 27: Kavanagh, D, et al, 2005, J Am Soc Nephrol 16:
25 Atypical HUS FACTOR I DEFICIENCY 11 different FI mutations identified to date
26 Atypical HUS MEMBRANE COFACTOR PROTEIN (MCP = CD46) ~65 kd transmembrane glycoprotein on leukocytes, platelets, endothelial & epithelial cells, fibroblasts, kidney extracellular domain four SCR domains alternative splice sites for O-glycosylation multiple isoforms exist transmembrane domain cytoplasmic C-terminal anchor functions as cofactor for FI pathogen receptor for measles, adenovirus, HHV-6, Neisseria, and GAS
27 Atypical HUS MCP DEFICIENCY reported only in familial forms of atypical HUS both homozygous and heterozygous types seen 80% of patients are heterozygotes Fremeaux-Bacchi, V, et al, 2006, J Am Soc Nephrol 17:
28 Atypical HUS MCP DEFICIENCY 25 different MCP mutations identified to date
29 C3 Levels By Mutation Sellier-Leclerc, A.-L. et al. J Am Soc Nephrol 2007;18:
30 Complement and Atypical HUS About 50%-60% of ahus cases are associated with a mutation in a complement-related gene Protein Gene Source Location % of ahus Factor H CFH Liver circulates ~ 15-30% Factor I CFI Liver circulates ~ 5-10% Membrane Cofactor Protein MCP Widespread Membrane bound ~ 10-15% Factor B CFB Liver,? circulates <5% C3 C3 Liver,? circulates ~ 5-10% Anti-FH-Ab CFHR1/ CFHR3 Lymphocyte circulates ~ 10% Unknown ~ 40-50% Jozsi et al. Blood 2008, Frémeaux-Bacchi V et al. Blood 2008, Goicoechea de Jorge 2007, Caprioli, et al Blood 2006, Kavanagh Curr Opin Nephrol Hypertens, 2007
31 Recommended Initial Evaluation of HUS Because infections trigger both typical and atypical HUS, initial evaluation should encompass both Testing should include C3 level as well as classic evaluation (stool culture, LDH, smear, etc.) ADAMSTS13 / auto-ab analysis if TTP not ruled out Save some plasma for later analysis
32 ahus CONTROVERSIES
33 Differentiating between ahus, TTP & STEC HUS Thrombocytopenia Platelet count <150,000 Or >25% Decrease from baseline Microangiopathic Hemolysis Schistocytes and/or Elevated LDH and/or Decreased Haptoglobin and/or Decreased Hemoglobin Neurological Symptoms Confusion/Seizures/Other abnormalities Renal Impairment Increased creatinine/decreased GFR/Abnormal UA Gastrointestinal Symptoms Diarrhea (+/-blood), N/V, gastroenteritis, Abdominal pain
34 ahus Cases 3 Cases- demonstrating the issues surrounding diagnosis and utilization of clinical criteria Case 1-45 yr old woman: Initially diagnosed with TTP but accurate diagnosis is ahus Case 2 10 yr old boy: Initially diagnosed with ahus but accurate diagnosis was TTP Case 3 12 yr old girl undergoing kidney transplant as per UI protocol Focus on clinical presentation and accurate diagnosis
35 Case 1 45 yo Admit TMA management with atypical features (normal range platelet count ). History non-bloody diarrhea. Only Medication OCP. Initial Diagnosis TTP Initially presented with foot and ankle swelling and intermittent chest tightness. Lower extremity edema since one month prior (found to have a creatinine of 3.0 and an elevated blood pressure)
36 Case 1 Systemic symptoms progressed to nausea, vomiting, occasional low-grade fever and chills. Several days later followup noted to have an creatinine of 7.7, hemoglobin 7.2, and platelet count 227. Biopsy found thrombotic microangiopathy> Complement not done Differential DIAGNOSIS: TTP vs. ahus ADAMTS13 Activity levels at 58% (Post PEX) (N >67%). APL normal. ANA reported as abnormal. Hep screen negative. Haptoglobin low. Shistocytes 1-2+ Limitation of ADAMTS13 measured post PEX its critical to utilize ADAMTS13 activity to differentiate between ahus and TTP
37 Case 1 Six PEX Treatments: Fluid replacement: 500 ml normal saline, 500 ml of 5% albumin, 3000 ml of plasma PEX initiated because of TTP diagnosis Continued Symptoms- developed irreversible renal failure now on Chronic Hemodialysis Subsequent follow up: complement levels obtained and
38 Case 1 Labs HgB Platelets Hapto LDH C3 Day PEX initiated at day ADAMTS level obtained after 1 st treatment Level 58% (N >67%)
39 Genetic Abnormalities and Clinical Outcome in Patients with Atypical Hemolytic Uremic Syndrome: Need to assess Complement in patients with TMA Gene Protein Affected Main Effect Frequency Response to Plasma Therapy Long-term Outcome Outcome of Kidney Transplant CFH CFHR1/3 Factor H Factor HR1, R3 No binding to endothelium 20-30% 60% Remission ESRD in 70-80% 80-90% Recurrence Anti-factor H Antibodies 6% 70-80% Remission ESRD in 30-40% 20% Recurrence MCP Membrane cofactor protein No surface expression 10-15% No definitive indication for Therapy ESRD in <20% 15-20% Recurrence CFI Factor I Low level or low cofactor activity 4-10% 30-40% Remission ESRD in 60-70% 70-80% Recurrence CFB Factor B C3 Convertase stabilization 1-2% 30% Remission ESRD in 70% Recurrence in one case C3 Complement C3 Resistance to C3b inactivation 5-10% 40-50% Remission ESRD in 60% 40-50% Recurrence THBD Thrombomodulin Reduced C3b inactivation 5% 60% Remission ESRD in 60% Recurrence in one case Adapted from Remuzzi, NEJM, ;17 39
40 Case 2 10 yr old male- mild fever, nausea, vomiting and some confusion (negative past history) HgB 7 mg/dl, plt 100, LDH 4715, Haptoglobin low, 8% schistocytes, Acute kidney injury creat- 1.4 mg/dl Patient referred as an ahus patient and ADAMTS13 activity level used to differentiate from TTP Complement studies- initially normal ADAMTS 13 activity level sent-given the variable presentation of ahus
41 Table 1. Successful treatment with rituximab for acute refractory thrombotic thrombocytopenic purpura related to acquired ADAMTS13 deficiency: A pediatric report and literature review. Harambat, Jerome; Lamireau, Delphine; Delmas, Yahsou; Ryman, Anne; Llanas, Brigitte; Brissaud, Olivier; MD, PhD Table 1. Course of ADAMTS13 activity and anti ADAMTS13 immunoglobulin G titer Pediatric Critical Care Medicine. 12(2):e90 e93, March DOI: /PCC.0b013e3181e89f8f ADAMTS13 to differentiate between ahus and TTP 2011The Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies. Published by Lippincott Williams & Wilkins, Inc. 3
42 Case 2 PEX Initiated with FFP replacement no initial response of hematological parameters Condition worsened and patient developed TAMOF Based on ADAMTS 13 levels (<5%) and presence of strong inhibitory antibody patient started on immunosuppression Good Response- clinical parameters began to improve: platelets, LDH etc
43 Case 3 Teenage patient- second transplant, initial diagnosis missed 28 Plasma Exchanges Platelet 144,000 mm3 to 337,000 mm3 after thirteen Exchanges over 5 weeks Hgb 5.5g/dl to 11.1 g/dl Renal Function did not recover Started on Chronic HD what else? Tx HD Eculizumab Tx RF 8 Months on Dialysis 25 Months with no renal abnormality RF PTx 15 Months on Dialysis 6/07 7/09 10/10 43?
44 Plasma Therapy- standard approach Diagnosis of HUS (Atypical Presentation) Exceptions Plasma Therapy within 24 hours of diagnosis Exchange 1.5 X plasma volume (60-75ml/kg) pr session Replace with Albumin or FFP Repeat Plasma Therapy daily X 5 days Then 5 sessions per week for 2 weeks Then 3 sessions per week for 2 weeks Withdrawal Alternate Diagnosis Complication Remission Long Term Treatment Plan 44 Aricetta, Ped Neph, (2009) 24:
45 Case 3 No mutations in CFH, CFI, CFHR5, MCP, CFB, C3 or THBD only 30-50% ahus patients have an identifiable mutation Copy Number studies (MPLA) Hybrid CFH/CFHR1 gene Fusion protein comprised of the first 18 short consensus repeats (SCRs) of CFH and the last two SCRs of CFHR1 To be continued 45

46 Venables, 2006, PLoS 3:
47 Genetic Abnormalities and Clinical Outcome in Patients with Atypical Hemolytic Uremic Syndrome Gene Protein Affected Main Effect Frequency Response to Plasma Therapy Long-term Outcome Outcome of Kidney Transplant CFH CFHR1/3 Factor H Factor HR1, R3 No binding to endothelium 20-30% 60% Remission ESRD in 70-80% 80-90% Recurrence Anti-factor H Antibodies 6% 70-80% Remission ESRD in 30-40% 20% Recurrence MCP Membrane cofactor protein No surface expression 10-15% No definitive indication for Therapy ESRD in <20% 15-20% Recurrence CFI Factor I Low level or low cofactor activity 4-10% 30-40% Remission ESRD in 60-70% 70-80% Recurrence CFB Factor B C3 Convertase stabilization 1-2% 30% Remission ESRD in 70% Recurrence in one case C3 Complement C3 Resistance to C3b inactivation 5-10% 40-50% Remission ESRD in 60% 40-50% Recurrence THBD Thrombomodulin Reduced C3b inactivation 5% 60% Remission ESRD in 60% Recurrence in one case Adapted from Remuzzi, NEJM, ;17 47
48 ahus TREATMENT
49 Gene The Genetics of Atypical Hemolytic Uremic Syndrome Role of Mutation Frequency European Cohort 1 US Cohort 2 Risk of ESRD at 3 years Risk of transplant loss within 1 year Frequency CFH MCP Mutation results in a quantitative deficiency of protein or altered binding to C3b* Mutant proteins have low C3b binding capacity and therefore decreased cofactor activity 23% 77% 71% 27% 7% 6% 0% 5% CFI Mutations induce a default of secretion of the protein or disrupt its cofactor activity altering degradation of C3b/C4b 4% 60% 67% 8% C3 Mutations interfere with binding of C3 to MCP and regulation by MCP or increased binding to CFB resulting in increased C3 convertase formation. 8% 67% 43% 2% CFB Mutated proteins binds excessively to C3b and stabilizing the C3 convertase making it resistant to decay by CFH, enhancing formation of C5b-9 1% - - 4% complexes and deposition of C3- fragments onto endothelial cell surfaces THBD Mutated proteins are less effective at moderating CFI-mediated inactivation of 5% 54% 0% 3% C3b CFHR1/3 Associated with CFH Antibodies 6% - CFHR5 Unknown Not 3% Fusion Proteins CFH Antibody Results in non-functional CFH Anti-CFH IgG bind to CFH and inhibit CFH binding to C3b and cell surfaces Reported Not Reported 3% 63% Not Reported Not Reported Unknown 52% 50% 54%


50 1. Remove abnormal proteins 2. Replace deficient proteins 3. Block terminal complement effects.
51 Plasma Therapy- standard approach Diagnosis of HUS (Atypical Presentation) Exceptions Plasma Therapy within 24 hours of diagnosis Exchange 1.5 X plasma volume (60-75ml/kg) pr session Replace with Albumin or FFP Repeat Plasma Therapy daily X 5 days Then 5 sessions per week for 2 weeks Then 3 sessions per week for 2 weeks Withdrawal Alternate Diagnosis Complication Remission Long Term Treatment Plan 51 Aricetta, Ped Neph, (2009) 24:
52 Plasmatherapy CFH Mutation CFI C3 Thrombomodulin 63% Hematologic Response 25% Hematologic Response 57% Hematologic Response 88% Hematologic Response CFH Mutation CFI C3 Thrombomodulin 63% Hematologic Response 25% Hematologic Response 57% Hematologic Response 88% Hematologic Response CFH Mutation CFI C3 Thrombomodulin 37% Death or ESRD 75% Death or ESRD 43% Death or ESRD 13% Death or ESRD CJASN, 2010;5:
53 Eculizumab Recombinant, humanized, monoclonal antibody directed against C5 specifically preventing its cleavage by the C5 convertase. Prevents the generation of the terminal complement complex C5b-9. The single most expensive drug in the world. ($409,500/yr Forbes Magazine) Nature Biotechnology 25, (2007)
54 Eculizumab and ahus N Engl J Med Jan 29;360(5):542-4 N Engl J Med May 14;360(20): N Engl J Med Jan 29;360(5):544-6 Am J Kidney Dis Apr;55(4): Pediatr Nephrol Apr;26(4): Pediatr Nephrol Apr;26(4): N Engl J Med May 6;362(18): Pediatr Nephrol Aug;26(8): Clin J Am Soc Nephrol Jun;6(6): Pediatr Nephrol Nov;26(11): Pediatr Transplant Sep;16(6):E Pediatr Nephrol Jul;27(7): Am J Transplant Jul;12(7): Pediatr Nephrol Aug 19. Pediatr Nephrol Sep 6. Am J Transplant Sep 7.
 95% CI 64-100 Change in Renal Function One stage improvement 11/17 patients (65%) Less than one stage 4/17 patients (23%) Removal from dialysis 5/7")
 95% CI 60-98 TMA Interventions 0/17 patients (0%) Pediatric Patients Exposed to Eculizumab")
55 Terminal Complement Blockade Eculizumab and Atypical Hemolytic Uremic Syndrome Patients Resistant to Plasma Therapy - 26 Week Results Change in Platelet Count X 10 9 P = <.0001 TMA Event Free Status 15/17 patients (88%) 95% CI Change in Renal Function One stage improvement 11/17 patients (65%) Less than one stage 4/17 patients (23%) Removal from dialysis 5/7 patients (71%) Quality of Life Improvement EuroQol 5D: P = <0001 Patients on Chronic Plasma Therapy - 12 week Results TMA Event Free Status 13/15 patients (87%) 95% CI TMA Interventions 0/17 patients (0%) Pediatric Patients Exposed to Eculizumab - Retrospective Review of 4 Week Data Hematologic Parameters Normalization in 8/19 patients (42%) Change in Renal Function > 15ml/min/1.73m 2 improvement in 7/19 patients (78%) Removal from dialysis 4/8 patients (50%) FDA Approval September 2011
56 Liver-Kidney Transplant- Option 1 Goal: correct genetic defect Liver protein replacement strategy Initial attempts - high mortality Early failure of transplant liver 7/8 with extensive PTx have retained their liver 8th died of hepatic encephalopathy 56
57 Liver Transplant CFH, CFI, CFB and C3 20 Cases (Presse Med. 2012; 41: e115 e135) 4 procedures in 2002 All Fatal With preconditioning - 86% patient survival reported Protection against kidney transplant rejection No reports of ahus recurrence

58 Eculizumab J Am Soc Nephrol May;20(5):940-9
59 Liver Transplant PEX with FFP 4-6 hours before transfer to OR Eculizumab Intraoperative transplant immune suppression Hepatectomy Whole-liver orthotopic transplant Intra-operative FFP after liver perfusion Kidney transplant Eculizumab Heparin/ASA Am J Kidney Dis. 2011;58(1):109-
60 Impediments to Care Consideration of the diagnosis Availability of diagnostic studies Decision to PEX or Ecu acutely may be based on logistics Local Expertise Formulary concerns Hospital financial concerns
61 New Kidney + Plasma Therapy & Eculizumab Option 2 61
62 The Alternate Complement Pathway Remuzzi, NEJM, ;17 62

63 The Alternate Complement Pathway Remuzzi, NEJM, ;17 63
64 Case 3 On dialysis for 15 months Altruistic donor comes forward Rare Renal Disease Team approval Renal Transplant Protocol Approved Eculizumab and Plasma Therapy Transplant 10/07/10 Tx HD Eculizumab Tx RF 8 Months on Dialysis 25 Months with no renal abnormality RF PTx 15 Months on Dialysis? 6/07 7/09 10/10
65 Concerns Genetic Testing Efficacy Life time risk of infection Surveillance Length of Therapy Payment On going research Tx HD Eculizumab Tx RF 8 Months on Dialysis 25 Months with no renal abnormality RF PTx 15 Months on Dialysis? 6/07 7/09 10/10
66 Patient Update Creatinine 0.9, 16 months s/p transplant No bacterial infections Returned to school full time 1/13 H&H 12.2/36 3/10 6.3/18 WBC, platelets normal Borderline low C3 What else do you want to know? 66
67 Hemolytic Workup Negative Bone Marrow Biopsy Mildly hypocellular bone marrow (50-70%) showing normal granulopoiesis, normal megakaryocytes and markedly decreased erythropoiesis with maturation arrest and giant normoblasts with viral inclusions Now what do you want to know? 67
68 Parvovirus B19 found in bone marrow Cellcept discontinued 1 Unit PRBC given 3/10 2 nd Unit given 3/24 68
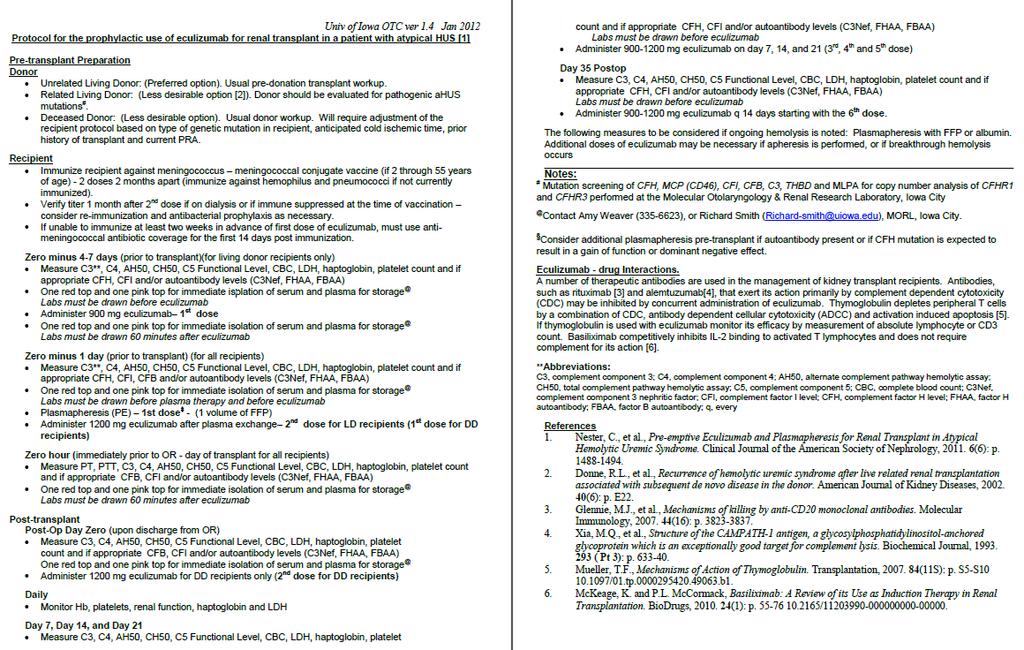
69 Pre-transplant Evaluation Donor evaluation for pathogenic ahus mutations Immunize against meningococcus (as well as hemophilus and pneumococci if not current) Verify titer if on dialysis or if immune suppressed at the time of vaccination consider reimmunization and antibacterial prophylaxis as necessary. Zero minus 1 week (prior to transplant) Measure C3*, C4, AH50, CH50, C5 Functional Level, CBC, LDH, haptoglobin, platelet count and if appropriate C3Nef, CFI and/or CFI levels. Labs must be drawn before plasma therapy and before eculizumab Plasma exchange or Infusion 1st dose - (1.5 volumes of Albumin) Administer 900 mg eculizumab 1st dose Zero minus (24-48 hours prior to transplant) Measure C3, C4, AH50, CH50, C5 Functional Level, CBC, LDH, haptoglobin, platelet count and if appropriate C3Nef, CFI and/or CFI levels. Labs must be drawn before plasma therapy and before eculizumab Plasma exchange or infusion 2 nd dose (1.5 volumes of FFP) Zero hour (0-24 hours before transplant) Administer 900mg eculizumab 2 nd dose Post-transplant Measure C3, C4, AH50, CH50, C5 Functional Level, CBC, LDH, haptoglobin, platelet count and if appropriate C3Nef, CFI and/or CFI levels. Labs must be drawn before plasma therapy and before eculizumab Administer 900mg eculizumab q7 days times two (3rd and 4 th dose) Administer 900mg eculizumab q 14 days
70 Kidney Transplant
71 Molecular Otolaryngology & Renal Research Laboratory University of Iowa Dr. Richard Smith CLIA Testing Research Testing Clinician/Patient driven IRB Mechanism 71
72 MORL (Molecular Otolaryngology & Renal Research Laboratory) Not for profit Lab Diagnostics section CLIA certified ahus testing screen all KNOWN genes for ANY possible variant. will detect novel mutations and previously reported mutations Discovery section Genetics of rare renal diseases including atypical HUS and Dense Deposit Disease (one section) New assays in development
73 Specialized Testing Adam TS 13 mutations- ELISA TTP analysis smac testing only lab in US- some with DDD and all with C3 GN- Only ~50% DDD patients successful in transplantation those seem to have smac (eculizumab)
74 ahus 260 cases processed and diagnosed in lab Large genetics repository- goal to develop more fully a complete registry Other tests recent German cases: may have complement abnormalities underlying as well EHEC may help ID those with underlying genetic predisposition




75 Characterization of an American ahus Cohort


76 Prevalence of Mutations in American Cohort


77 American ahus Patients Carrying Multiple Complement Gene Variants
78 Percentage of Mutations found in American patients Similar Overall mutations found ~50% CFH Mutations ~30% CFI ~10% THBD ~5% Increased CFB ~4% compared to ~2% (doubled) Decreased CD46 ~5% compared to ~10% - Likely due to the level of severity in our cohort (half) C3 ~2% compared to ~10% (one quarter) Important to screen all known susceptibility genes 12% of patients that were mutation positive carried more then one mutation Likely that rare variants are important in disease Thrombomodulin- unsure of the significance of the variants at this point Ethnic controls are important Summary of Results
79 University of Iowa Rare Renal Disease Clinic Research: Dr Smith and his research team a.edu/labs/morl/ Clinical- held in the Pediatric Specialty Clinics Dr. Richard Smith Dr. Carla Nester Dr. Christie Thomas Dr. Alan Reed Dr. Pat Brophy
80 Thank You Carla Nester Jeff Saland Gary Pien Brad Dixon Rare Renal team University of Iowa
Atypical Hemolytic Uremic Syndrome: When the Environment and Mutations Affect Organ Systems. A Case Report with Review of Literature
 Atypical Hemolytic Uremic Syndrome: When the Environment and Mutations Affect Organ Systems. A Case Report with Review of Literature Mouhanna Abu Ghanimeh 1, Omar Abughanimeh 1, Ayman Qasrawi 1, Abdulraheem
Atypical Hemolytic Uremic Syndrome: When the Environment and Mutations Affect Organ Systems. A Case Report with Review of Literature Mouhanna Abu Ghanimeh 1, Omar Abughanimeh 1, Ayman Qasrawi 1, Abdulraheem
M.Weitz has documented that he has no relevant financial relationships to disclose or conflict of interest to resolve.
 M.Weitz has documented that he has no relevant financial relationships to disclose or conflict of interest to resolve. Prophylactic eculizumab prior to kidney transplantation for atypical hemolytic uremic
M.Weitz has documented that he has no relevant financial relationships to disclose or conflict of interest to resolve. Prophylactic eculizumab prior to kidney transplantation for atypical hemolytic uremic
Recent advances in pathogenesis & treatment of ahus
 Recent advances in pathogenesis & treatment of ahus Miquel Blasco Pelicano Nephrology and Kidney Transplant Unit Hospital Clínic, Barcelona Atypical Hemolytic Uremic Syndrome (ahus) Ultra-rare disease:
Recent advances in pathogenesis & treatment of ahus Miquel Blasco Pelicano Nephrology and Kidney Transplant Unit Hospital Clínic, Barcelona Atypical Hemolytic Uremic Syndrome (ahus) Ultra-rare disease:
Hemolytic uremic syndrome: Investigations and management
 Hemolytic uremic syndrome: Investigations and management SAWAI Toshihiro M.D., Ph.D. Department of Pediatrics, Shiga University of Medical Science Otsu, JAPAN AGENDA TMA; Thrombotic micro angiopathy STEC-HUS;
Hemolytic uremic syndrome: Investigations and management SAWAI Toshihiro M.D., Ph.D. Department of Pediatrics, Shiga University of Medical Science Otsu, JAPAN AGENDA TMA; Thrombotic micro angiopathy STEC-HUS;
Hemolytic uremic syndrome
 Hemolytic uremic syndrome Doyeun Oh Department of Internal Medicine CHA University School of Medicine Disclosures for Doyeun Oh Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau
Hemolytic uremic syndrome Doyeun Oh Department of Internal Medicine CHA University School of Medicine Disclosures for Doyeun Oh Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau
Risk factors of chronic renal failure after atypical Hemolytic Uremic Syndrome under plasmatherapy
 Risk factors of chronic renal failure after atypical Hemolytic Uremic Syndrome under plasmatherapy Professeur Eric Rondeau Urgences néphrologiques et Transplantation rénale Hôpital Tenon, Paris WWA SFH
Risk factors of chronic renal failure after atypical Hemolytic Uremic Syndrome under plasmatherapy Professeur Eric Rondeau Urgences néphrologiques et Transplantation rénale Hôpital Tenon, Paris WWA SFH
TMA CASE STUDY. Pamela Harmon, RN & Keturah Tomlin, RN Toronto General Hospital Apheresis Unit
 TMA CASE STUDY Pamela Harmon, RN & Keturah Tomlin, RN Toronto General Hospital Apheresis Unit Cumulative fraction of patients free of events ahus is a catastrophic disease that can result in sudden & progressive
TMA CASE STUDY Pamela Harmon, RN & Keturah Tomlin, RN Toronto General Hospital Apheresis Unit Cumulative fraction of patients free of events ahus is a catastrophic disease that can result in sudden & progressive
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Lapeyraque A-L, Malina M, Fremeaux-Bacchi V, et al. Eculizumab
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Lapeyraque A-L, Malina M, Fremeaux-Bacchi V, et al. Eculizumab
R. Coward has documented that he has received cooperative grants from Takeda and Novo Nordisk
 R. Coward has documented that he has received cooperative grants from Takeda and Novo Nordisk Advances in our understanding of the pathogenesis of glomerular thrombotic microangiopathy Lindsay Keir Richard
R. Coward has documented that he has received cooperative grants from Takeda and Novo Nordisk Advances in our understanding of the pathogenesis of glomerular thrombotic microangiopathy Lindsay Keir Richard
Beyond Plasma Exchange: Targeted Therapy for Thrombotic Thrombocytopenic Purpura
 Beyond Plasma Exchange: Targeted Therapy for Thrombotic Thrombocytopenic Purpura Kristen Knoph, PharmD, BCPS PGY2 Pharmacotherapy Resident Pharmacy Grand Rounds April 25, 2017 2016 MFMER slide-1 Objectives
Beyond Plasma Exchange: Targeted Therapy for Thrombotic Thrombocytopenic Purpura Kristen Knoph, PharmD, BCPS PGY2 Pharmacotherapy Resident Pharmacy Grand Rounds April 25, 2017 2016 MFMER slide-1 Objectives
Dr. E.SUDHA (Fellow in Pediatric Nephrology) DEPT OF PEDIATRIC NEPHROLOGY & DIALYSIS Dr.MEHTA CHILDRENS HOSPITAL
 DEPT OF PEDIATRIC NEPHROLOGY & DIALYSIS Dr.MEHTA CHILDRENS HOSPITAL") Dr. E.SUDHA (Fellow in Pediatric Nephrology) DEPT OF PEDIATRIC NEPHROLOGY & DIALYSIS Dr.MEHTA CHILDRENS HOSPITAL CASE HISTORY 4 yrs old previously well boy Born to 2 nd degree consanguinity Fever x 5 days
Dr. E.SUDHA (Fellow in Pediatric Nephrology) DEPT OF PEDIATRIC NEPHROLOGY & DIALYSIS Dr.MEHTA CHILDRENS HOSPITAL CASE HISTORY 4 yrs old previously well boy Born to 2 nd degree consanguinity Fever x 5 days
New insights in thrombotic microangiopathies : TTP and ahus
 New insights in thrombotic microangiopathies : TTP and ahus Dr Catherine LAMBERT Hematology Cliniques universitaires Saint-Luc Catherine.lambert@uclouvain.be New insights in thrombotic microangiopathies
New insights in thrombotic microangiopathies : TTP and ahus Dr Catherine LAMBERT Hematology Cliniques universitaires Saint-Luc Catherine.lambert@uclouvain.be New insights in thrombotic microangiopathies
DRUG NAME: Eculizumab Brand(s): Soliris DOSAGE FORM/ STRENGTH: 10 mg/ml (300 mg per vial)
: Soliris DOSAGE FORM/ STRENGTH: 10 mg/ml (300 mg per vial)") Preamble: A confirmed diagnosis of atypical hemolytic uremic syndrome (ahus) is required for eculizumab funding. The information below is to provide clinicians with context for how a diagnosis of ahus
Preamble: A confirmed diagnosis of atypical hemolytic uremic syndrome (ahus) is required for eculizumab funding. The information below is to provide clinicians with context for how a diagnosis of ahus
Introduction to pathogenesis and treatment of thrombotic microangiopathies (TMA)
") Introduction to pathogenesis and treatment of thrombotic microangiopathies (TMA) JM.Campistol, Nephrology and Renal Transplant Department, Hospital Clinic, University of Barcelona, Barcelona, Spain. jmcampis@clinic.cat
Introduction to pathogenesis and treatment of thrombotic microangiopathies (TMA) JM.Campistol, Nephrology and Renal Transplant Department, Hospital Clinic, University of Barcelona, Barcelona, Spain. jmcampis@clinic.cat
What is meant by Thrombotic Microangiopathy (TMA)?
?") What is meant by Thrombotic Microangiopathy (TMA)? Thrombotic Microangiopathy (TMA) is a group of disorders characterized by injured endothelial cells, microangiopathic hemolytic anemia (MAHA), with its
What is meant by Thrombotic Microangiopathy (TMA)? Thrombotic Microangiopathy (TMA) is a group of disorders characterized by injured endothelial cells, microangiopathic hemolytic anemia (MAHA), with its
Safety and Efficacy of Eculizumab in Pediatric Patients With ahus, With or Without Baseline Dialysis
 SP281 Safety and Efficacy of Eculizumab in Pediatric Patients With ahus, With or Without Baseline Johan Vande Walle, 1 Larry A. Greenbaum, 2 Camille L. Bedrosian, 3 Masayo Ogawa, 3 John F. Kincaid, 3 Chantal
SP281 Safety and Efficacy of Eculizumab in Pediatric Patients With ahus, With or Without Baseline Johan Vande Walle, 1 Larry A. Greenbaum, 2 Camille L. Bedrosian, 3 Masayo Ogawa, 3 John F. Kincaid, 3 Chantal
Thrombotic Microangiopathies (TMA) / TTP/HUS/αHUS Pathology & Molecular. Genetics
 / TTP/HUS/αHUS Pathology & Molecular. Genetics") Thrombotic Microangiopathies (TMA) / TTP/HUS/αHUS Pathology & Molecular Genetics Helen Liapis, M.D. Senior Consultant Arkana Labs Professor of Pathology & Immunology. retired Washington University School
Thrombotic Microangiopathies (TMA) / TTP/HUS/αHUS Pathology & Molecular Genetics Helen Liapis, M.D. Senior Consultant Arkana Labs Professor of Pathology & Immunology. retired Washington University School
ahus A PATIENT S GUIDE To learn more about ahus, visit Copyright 2011, Alexion Pharmaceuticals, Inc. All rights reserved.
 To learn more about ahus, visit www.ahussource.com ahus A PATIENT S GUIDE Copyright 2011, Alexion Pharmaceuticals, Inc. All rights reserved. SOL 1169 BECOME EMPOWERED By learning more and taking control
To learn more about ahus, visit www.ahussource.com ahus A PATIENT S GUIDE Copyright 2011, Alexion Pharmaceuticals, Inc. All rights reserved. SOL 1169 BECOME EMPOWERED By learning more and taking control
TMA in HUS and TTP: new insights
 TMA in HUS and TTP: new insights Daan Dierickx University Hospitals Leuven, Department of Hematology, Belgium 20th Annual Meeting Belgian Society on Thrombosis and Haemostatis Antwerpen, 22 th November
TMA in HUS and TTP: new insights Daan Dierickx University Hospitals Leuven, Department of Hematology, Belgium 20th Annual Meeting Belgian Society on Thrombosis and Haemostatis Antwerpen, 22 th November
Soliris (eculizumab) DRUG.00050
 DRUG.00050") Market DC Soliris (eculizumab) DRUG.00050 Override(s) Prior Authorization Approval Duration 1 year Medications Soliris (eculizumab) APPROVAL CRITERIA Paroxysmal Nocturnal Hemoglobinuria I. Initiation of
Market DC Soliris (eculizumab) DRUG.00050 Override(s) Prior Authorization Approval Duration 1 year Medications Soliris (eculizumab) APPROVAL CRITERIA Paroxysmal Nocturnal Hemoglobinuria I. Initiation of
Spectrum of complement-mediated thrombotic microangiopathies after kidney transplantation
 Spectrum of complement-mediated thrombotic microangiopathies after kidney transplantation Marius Miglinas Vilnius university hospital: Nephrology center, Center of Rare Kidney Diseases Vilnius university
Spectrum of complement-mediated thrombotic microangiopathies after kidney transplantation Marius Miglinas Vilnius university hospital: Nephrology center, Center of Rare Kidney Diseases Vilnius university
1. INSTRUCTIONS 2. DEFINITION OF HUS
 CQ_IBK_aHUS_01 / version 25/11/09 European Paediatric Research Group for HUS and related disorders Case questionnaire for diarrhoea negative/vtec (STEC) negative cases acute phase 1. INSTRUCTIONS Please
CQ_IBK_aHUS_01 / version 25/11/09 European Paediatric Research Group for HUS and related disorders Case questionnaire for diarrhoea negative/vtec (STEC) negative cases acute phase 1. INSTRUCTIONS Please
Thrombotic Microangiopathy (TMA) The Clinical Facets of TMA
 The Clinical Facets of TMA") International Consensus on Management Atypical Hemolytic Uremic Syndrome in Children Loirat C. et al. Pediatr Nephrol 31: 15-39, 2016 Ruth A. McDonald, MD Professor and Vice Chair Clinical Affairs Department
International Consensus on Management Atypical Hemolytic Uremic Syndrome in Children Loirat C. et al. Pediatr Nephrol 31: 15-39, 2016 Ruth A. McDonald, MD Professor and Vice Chair Clinical Affairs Department
Hemolytic Uremic Syndrome
 Hemolytic Uremic Syndrome Francesco Emma Division of Nephrology and Dialysis Bambino Gesù Children s Hospital, IRCCS Rome, Italy Hemolytic Uremic Syndrome (HUS) microangiopathic hemolytic anemia thrombocytopenia
Hemolytic Uremic Syndrome Francesco Emma Division of Nephrology and Dialysis Bambino Gesù Children s Hospital, IRCCS Rome, Italy Hemolytic Uremic Syndrome (HUS) microangiopathic hemolytic anemia thrombocytopenia
C3 Glomerulopathy. Jun-Ki Park
 C3 Glomerulopathy Jun-Ki Park 03.08.11 For the last 30 years classification MPGN is based on glomerular findings by light microscopy with further specification on EM and staining for Ig and complement
C3 Glomerulopathy Jun-Ki Park 03.08.11 For the last 30 years classification MPGN is based on glomerular findings by light microscopy with further specification on EM and staining for Ig and complement
Safety and Efficacy of Eculizumab in Pediatric Patients With ahus, With or Without Baseline Dialysis
 SA-PO546 Safety and Efficacy of Eculizumab in Pediatric Patients With ahus, With or Without Baseline Johan Vande Walle, 1 Larry A. Greenbaum, 2 Camille L. Bedrosian, 3 Masayo Ogawa, 3 John F. Kincaid,
SA-PO546 Safety and Efficacy of Eculizumab in Pediatric Patients With ahus, With or Without Baseline Johan Vande Walle, 1 Larry A. Greenbaum, 2 Camille L. Bedrosian, 3 Masayo Ogawa, 3 John F. Kincaid,
THROMBOTIC MICROANGIOPATHY. Jun-Ki Park 7/19/11
 THROMBOTIC MICROANGIOPATHY Jun-Ki Park 7/19/11 TMAs are microvascular occlusive disorders characterized by systemic or intrarenal aggregation of platelets, thrombocytopenia, and mechanical injury to erythrocytes.
THROMBOTIC MICROANGIOPATHY Jun-Ki Park 7/19/11 TMAs are microvascular occlusive disorders characterized by systemic or intrarenal aggregation of platelets, thrombocytopenia, and mechanical injury to erythrocytes.
Atypical hemolytic uremic syndrome. Diana Karpman Department of Pediatrics Lund University
 Atypical hemolytic uremic syndrome Diana Karpman Department of Pediatrics Lund University Image courtesy of Dr. Sabine Leh, Haukeland University Hospital, Bergen Norway Hemolytic Uremic Syndrome Non-immune
Atypical hemolytic uremic syndrome Diana Karpman Department of Pediatrics Lund University Image courtesy of Dr. Sabine Leh, Haukeland University Hospital, Bergen Norway Hemolytic Uremic Syndrome Non-immune
Acquired Drivers of Disaese ahus and autoantibodies: their role in disease and their impact on patient management
 Acquired Drivers of Disaese ahus and autoantibodies: their role in disease and their impact on patient management Veronique Fremeaux-Bacchi Cordeliers Research Center and Européen Georges Pompidou Hospital,
Acquired Drivers of Disaese ahus and autoantibodies: their role in disease and their impact on patient management Veronique Fremeaux-Bacchi Cordeliers Research Center and Européen Georges Pompidou Hospital,
Clinical Study Eculizumab Therapy Leads to Rapid Resolution of Thrombocytopenia in Atypical Hemolytic Uremic Syndrome
 Hindawi Publishing Corporation Advances in Hematology Volume 214, Article ID 295323, 7 pages http://dx.doi.org/1.1155/214/295323 Clinical Study Therapy Leads to Rapid Resolution of Thrombocytopenia in
Hindawi Publishing Corporation Advances in Hematology Volume 214, Article ID 295323, 7 pages http://dx.doi.org/1.1155/214/295323 Clinical Study Therapy Leads to Rapid Resolution of Thrombocytopenia in
A 60 year old woman with altered mental status and thrombotic microangiopathy. Josh Veatch
 A 60 year old woman with altered mental status and thrombotic microangiopathy Josh Veatch Previously healthy 60 year old woman 2 3 months of fatigue following a URI, transient episodes being out of it
A 60 year old woman with altered mental status and thrombotic microangiopathy Josh Veatch Previously healthy 60 year old woman 2 3 months of fatigue following a URI, transient episodes being out of it
HUS and TTP Testing. Kenneth D. Friedman, M.D. Director, Hemostasis Reference Lab BloodCenter of Wisconsin, Milwaukee WI
 HUS and TTP Testing Kenneth D. Friedman, M.D. Director, Hemostasis Reference Lab BloodCenter of Wisconsin, Milwaukee WI Disclosures Relevant Financial Relationships Consultant: Ablynx, Bayer, CSL Behring,
HUS and TTP Testing Kenneth D. Friedman, M.D. Director, Hemostasis Reference Lab BloodCenter of Wisconsin, Milwaukee WI Disclosures Relevant Financial Relationships Consultant: Ablynx, Bayer, CSL Behring,
Specialised Services Policy: CP98 Eculizumab for Atypical Haemolytic Uraemic Syndrome (ahus)
") Specialised Services Policy: CP98 Eculizumab for Atypical Haemolytic Uraemic Syndrome (ahus) Document Author: Assistant Director for Evidence, Evaluation and Effectiveness Executive Lead: Medical Director
Specialised Services Policy: CP98 Eculizumab for Atypical Haemolytic Uraemic Syndrome (ahus) Document Author: Assistant Director for Evidence, Evaluation and Effectiveness Executive Lead: Medical Director
When a patient presents with TMA, identify the underlying cause for the appropriate diagnosis... IS IT TTP OR IS IT ahus?
 When a patient presents with TMA, identify the underlying cause for the appropriate diagnosis... IS IT TTP OR IS IT ahus? ADAMTS13 activity >5% RULES OUT a diagnosis of severe ADAMTS13 deficiency (TTP)
When a patient presents with TMA, identify the underlying cause for the appropriate diagnosis... IS IT TTP OR IS IT ahus? ADAMTS13 activity >5% RULES OUT a diagnosis of severe ADAMTS13 deficiency (TTP)
Thrombotic Thrombocytopenic Purpura and the Role of ADAMTS-13
 Thrombotic Thrombocytopenic Purpura and the Role of ADAMTS-13 Mark Cunningham,MD Director, Hematology Laboratory Department of Pathology University of Kansas Medical Center College of American Pathologists
Thrombotic Thrombocytopenic Purpura and the Role of ADAMTS-13 Mark Cunningham,MD Director, Hematology Laboratory Department of Pathology University of Kansas Medical Center College of American Pathologists
A Rational Approach to Evaluation of Thrombotic Microangiopathy
 A Rational Approach to Evaluation of Thrombotic Microangiopathy An Algorithmic Approach C. Christopher Hook, MD for the Complement Alternative Pathway Thrombotic Micro- Angiopathy (CAP-TMA) Disease-Oriented
A Rational Approach to Evaluation of Thrombotic Microangiopathy An Algorithmic Approach C. Christopher Hook, MD for the Complement Alternative Pathway Thrombotic Micro- Angiopathy (CAP-TMA) Disease-Oriented
DR V PHILIP CLINICAL HAEMATOLOGY UNIT CHRIS HANI BARAGWANATH ACADEMIC HOSPITAL
 DR V PHILIP CLINICAL HAEMATOLOGY UNIT CHRIS HANI BARAGWANATH ACADEMIC HOSPITAL Rare but fatal disease if unrecognized and untreated Incidence about 1: 1 million in the USA Female preponderance of 2:1 Part
DR V PHILIP CLINICAL HAEMATOLOGY UNIT CHRIS HANI BARAGWANATH ACADEMIC HOSPITAL Rare but fatal disease if unrecognized and untreated Incidence about 1: 1 million in the USA Female preponderance of 2:1 Part
Microangiopatia trombotica (MAT) e Sindrome emolitico-uremica atipica (SEUa): Basi patogenetiche, inquadramento diagnostico e principi del
 e Sindrome emolitico-uremica atipica (SEUa): Basi patogenetiche, inquadramento diagnostico e principi del") Microangiopatia trombotica (MAT) e Sindrome emolitico-uremica atipica (SEUa): Basi patogenetiche, inquadramento diagnostico e principi del trattamento Vincenzo Montinaro U.O. Nefrologia Azienda Ospedaliera
Microangiopatia trombotica (MAT) e Sindrome emolitico-uremica atipica (SEUa): Basi patogenetiche, inquadramento diagnostico e principi del trattamento Vincenzo Montinaro U.O. Nefrologia Azienda Ospedaliera
Soliris (eculizumab) Inhibits TMA and Improves Renal Function in Pediatric and Adult Patients with atypical Hemolytic Uremic Syndrome (ahus)
 Inhibits TMA and Improves Renal Function in Pediatric and Adult Patients with atypical Hemolytic Uremic Syndrome (ahus)") Soliris (eculizumab) Inhibits TMA and Improves Renal Function in Pediatric and Adult Patients with atypical Hemolytic Uremic Syndrome (ahus) New Data from the Largest Prospective Trial of Adult Patients
Soliris (eculizumab) Inhibits TMA and Improves Renal Function in Pediatric and Adult Patients with atypical Hemolytic Uremic Syndrome (ahus) New Data from the Largest Prospective Trial of Adult Patients
C3 Glomerulonephritis versus C3 Glomerulopathies?
 Washington University School of Medicine Digital Commons@Becker Kidneycentric Kidneycentric 2016 C3 Glomerulonephritis versus C3 Glomerulopathies? T. Keefe Davis Washington University School of Medicine
Washington University School of Medicine Digital Commons@Becker Kidneycentric Kidneycentric 2016 C3 Glomerulonephritis versus C3 Glomerulopathies? T. Keefe Davis Washington University School of Medicine
* Renal insufficiencies
 Thrombotic Thrombocytopenic Purpura Behzad Poopak, DCLS PhD. Tehran medical Branch Islamic Azad university bpoopak@yahoo.com Case Summary Ms. X, a 35-year year-old woman Complained of weakness, low grade
Thrombotic Thrombocytopenic Purpura Behzad Poopak, DCLS PhD. Tehran medical Branch Islamic Azad university bpoopak@yahoo.com Case Summary Ms. X, a 35-year year-old woman Complained of weakness, low grade
w ahus pathology is linked to dysregulation of the alternative complement pathway.
 ahus - Pathogenesis, Etiology, and Clinical Advances Craig B. Langman MD The Isaac A Abt MD Professor of Kidney Diseases Feinberg School of Medicine, Northwestern University Head, Kidney Diseases The Ann
ahus - Pathogenesis, Etiology, and Clinical Advances Craig B. Langman MD The Isaac A Abt MD Professor of Kidney Diseases Feinberg School of Medicine, Northwestern University Head, Kidney Diseases The Ann
Not So Benign Hematology Aplastic anemia, Paroxysmal Nocturnal Hemoglobinuria, atypical Hemolytic Uremic Syndrome, Thrombotic Thrombocytopenic Purpura
 Not So Benign Hematology Aplastic anemia, Paroxysmal Nocturnal Hemoglobinuria, atypical Hemolytic Uremic Syndrome, Thrombotic Thrombocytopenic Purpura Robert A. Brodsky, MD Johns Hopkins Family Professor
Not So Benign Hematology Aplastic anemia, Paroxysmal Nocturnal Hemoglobinuria, atypical Hemolytic Uremic Syndrome, Thrombotic Thrombocytopenic Purpura Robert A. Brodsky, MD Johns Hopkins Family Professor
Let`s go for the diagnosis! Yazeed Toukan, MD Pediatric Pulmonary Institute, Ruth Rappaport Children`s Hospital July 2016
 Let`s go for the diagnosis! Yazeed Toukan, MD Pediatric Pulmonary Institute, Ruth Rappaport Children`s Hospital July 2016 Case report 20 months old girl Israeli Arab Muslim family, consanguineous marriage
Let`s go for the diagnosis! Yazeed Toukan, MD Pediatric Pulmonary Institute, Ruth Rappaport Children`s Hospital July 2016 Case report 20 months old girl Israeli Arab Muslim family, consanguineous marriage
PREGNANCY ASSOCIATED THROMBOTIC THROMBOCYTOPENIC PURPURA AND ACUTE KIDNEY INJURY
 VII, 2013, 2 33 A, PREGNANCY ASSOCIATED THROMBOTIC THROMBOCYTOPENIC PURPURA AND ACUTE KIDNEY INJURY M. Lubomirova Clinic of Nephrology, University Hospital Aleksandrovska So a : ( ), /HELLP, (AFLP) (TTP)
VII, 2013, 2 33 A, PREGNANCY ASSOCIATED THROMBOTIC THROMBOCYTOPENIC PURPURA AND ACUTE KIDNEY INJURY M. Lubomirova Clinic of Nephrology, University Hospital Aleksandrovska So a : ( ), /HELLP, (AFLP) (TTP)
ahus: recent insights and management
 ahus: recent insights and management Steven Van Laecke MD, PhD Renal Division, Ghent University Hospital, Belgium 13 th BANTAO Sarajevo October 8 2017 The complement is everywhere I could benefit from
ahus: recent insights and management Steven Van Laecke MD, PhD Renal Division, Ghent University Hospital, Belgium 13 th BANTAO Sarajevo October 8 2017 The complement is everywhere I could benefit from
A 23 year old Caucasian male presented with shortness of breath, hypertension, bloody sputum, and a history of drug abuse (confirmed by urinalysis).
.") A 23 year old Caucasian male presented with shortness of breath, hypertension, bloody sputum, and a history of drug abuse (confirmed by urinalysis). He was found to have severe kidney injury requiring
A 23 year old Caucasian male presented with shortness of breath, hypertension, bloody sputum, and a history of drug abuse (confirmed by urinalysis). He was found to have severe kidney injury requiring
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Soliris (eculizumab) Page 1 of 11 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Soliris (eculizumab) Prime Therapeutics will review Prior Authorization requests
Soliris (eculizumab) Page 1 of 11 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Soliris (eculizumab) Prime Therapeutics will review Prior Authorization requests
ISTITUTO DI RICERCHE FARMACOLOGICHE MARIO NEGRI CLINICAL RESEARCH CENTER ALDO E FOR CELE RARE DACCO DISEASES ALDO E CELE DACCO
 ISTITUTO DI RICERCHE FARMACOLOGICHE MARIO NEGRI CENTRO MARIO DI NEGRI RICERCHE INSTITUTE CLINICHE FOR PHARMACOLOGICAL PER LE MALATTIE RESEARCH RARE CLINICAL RESEARCH CENTER ALDO E FOR CELE RARE DACCO DISEASES
ISTITUTO DI RICERCHE FARMACOLOGICHE MARIO NEGRI CENTRO MARIO DI NEGRI RICERCHE INSTITUTE CLINICHE FOR PHARMACOLOGICAL PER LE MALATTIE RESEARCH RARE CLINICAL RESEARCH CENTER ALDO E FOR CELE RARE DACCO DISEASES
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: eculizumab_soliris 8/2014 4/2018 4/2019 4/2018 Description of Procedure or Service Paroxysmal nocturnal hemoglobinuria
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: eculizumab_soliris 8/2014 4/2018 4/2019 4/2018 Description of Procedure or Service Paroxysmal nocturnal hemoglobinuria
Novel aspects of atypical haemolytic uraemic syndrome and the role of eculizumab
 Nephrol Dial Transplant (2014) 29: iv131 iv141 doi: 10.1093/ndt/gfu235 Full Review Novel aspects of atypical haemolytic uraemic syndrome and the role of eculizumab Jacobien C. Verhave 1, Jack F.M. Wetzels
Nephrol Dial Transplant (2014) 29: iv131 iv141 doi: 10.1093/ndt/gfu235 Full Review Novel aspects of atypical haemolytic uraemic syndrome and the role of eculizumab Jacobien C. Verhave 1, Jack F.M. Wetzels
Pathology of Complement Mediated Renal Disease
 Pathology of Complement Mediated Renal Disease Mariam Priya Alexander, MD Associate Professor of Pathology GN Symposium Hong Kong Society of Nephrology July 8 th, 2017 2017 MFMER slide-1 The complement
Pathology of Complement Mediated Renal Disease Mariam Priya Alexander, MD Associate Professor of Pathology GN Symposium Hong Kong Society of Nephrology July 8 th, 2017 2017 MFMER slide-1 The complement
Soliris and You. Your Guide To Living With ahus. INDICATION & IMPORTANT SAFETY INFORMATION FOR SOLIRIS (eculizumab)
") INDICATION & IMPORTANT SAFETY INFORMATION FOR SOLIRIS (eculizumab) INDICATION What is SOLIRIS? SOLIRIS is a prescription medicine called a monoclonal antibody. SOLIRIS is used to treat: adults and children
INDICATION & IMPORTANT SAFETY INFORMATION FOR SOLIRIS (eculizumab) INDICATION What is SOLIRIS? SOLIRIS is a prescription medicine called a monoclonal antibody. SOLIRIS is used to treat: adults and children
Primary causes: Complement dysregulation (50% of non-shiga toxin-producing E. coli ) Secondary causes:
 Secondary causes:") General department INTRODUCTION The hemolytic uremic syndrome (HUS): microangiopathic hemolytic anemia, thrombocytopenia, and acute kidney injury One of the main causes of acute kidney injury in children
General department INTRODUCTION The hemolytic uremic syndrome (HUS): microangiopathic hemolytic anemia, thrombocytopenia, and acute kidney injury One of the main causes of acute kidney injury in children
Soliris Medical Policy Prior Authorization Program Summary
 Soliris Medical Policy Prior Authorization Program Summary Precertification/Prior Authorization may be required under certain plans. Please verify each member s benefits. OBJECTIVE The intent of the Soliris
Soliris Medical Policy Prior Authorization Program Summary Precertification/Prior Authorization may be required under certain plans. Please verify each member s benefits. OBJECTIVE The intent of the Soliris
Not So Benign Hematology. Robert A. Brodsky, MD Johns Hopkins Family Professor of Medicine and Oncology Division Chief Hematology
 Not So Benign Hematology Robert A. Brodsky, MD Johns Hopkins Family Professor of Medicine and Oncology Division Chief Hematology Disclosures Dr. Brodsky serves as a Scientific Advisory Board member to:
Not So Benign Hematology Robert A. Brodsky, MD Johns Hopkins Family Professor of Medicine and Oncology Division Chief Hematology Disclosures Dr. Brodsky serves as a Scientific Advisory Board member to:
Introduction. Arif Asif 1 Ali Nayer 2 Christian S. Haas 3
 J Nephrol (2017) 30:347 362 DOI 10.1007/s40620-016-0357-7 REVIEW Atypical hemolytic uremic syndrome in the setting of complement-amplifying conditions: case reports and a review of the evidence for treatment
J Nephrol (2017) 30:347 362 DOI 10.1007/s40620-016-0357-7 REVIEW Atypical hemolytic uremic syndrome in the setting of complement-amplifying conditions: case reports and a review of the evidence for treatment
Thrombotic Thrombocytopenic
 The Treatment of TTP and the Prevention of Relapses GERALD APPEL, MD Professor of Clinical Medicine Columbia University College of Physicians and Surgeons NY-Presbyterian Hospital New York, New York Thrombotic
The Treatment of TTP and the Prevention of Relapses GERALD APPEL, MD Professor of Clinical Medicine Columbia University College of Physicians and Surgeons NY-Presbyterian Hospital New York, New York Thrombotic
Accepted Manuscript. No more thrombotic thrombocytopenic purpura/hemolytic uremic syndrome please. Yeong-Hau H. Lien MD, PhD S (18)
") Accepted Manuscript No more thrombotic thrombocytopenic purpura/hemolytic uremic syndrome please Yeong-Hau H. Lien MD, PhD PII: S0002-9343(18)30965-3 DOI: https://doi.org/10.1016/j.amjmed.2018.10.009 Reference:
Accepted Manuscript No more thrombotic thrombocytopenic purpura/hemolytic uremic syndrome please Yeong-Hau H. Lien MD, PhD PII: S0002-9343(18)30965-3 DOI: https://doi.org/10.1016/j.amjmed.2018.10.009 Reference:
Haemolytic uraemic syndrome the story of a whodunit
 Haemolytic uraemic syndrome the story of a whodunit Paul Warwicker Lancashire Teaching Hospitals NHS Trust RCP Kidney for the General Physician Conference Nov 17 Renal thrombotic microangiopathy (TMA)
Haemolytic uraemic syndrome the story of a whodunit Paul Warwicker Lancashire Teaching Hospitals NHS Trust RCP Kidney for the General Physician Conference Nov 17 Renal thrombotic microangiopathy (TMA)
Guideline. Abstract. Key words
 bs_bs_banner Pediatrics International (2014) 56, 1 5 doi: 10.1111/ped.12274 Guideline Diagnostic criteria for atypical hemolytic uremic syndrome proposed by the Joint Committee of the Japanese Society
bs_bs_banner Pediatrics International (2014) 56, 1 5 doi: 10.1111/ped.12274 Guideline Diagnostic criteria for atypical hemolytic uremic syndrome proposed by the Joint Committee of the Japanese Society
Thrombotic Microangiopathies
 Thrombotic Microangiopathies ASH/San Antonio Breast Cancer Symposium Review James N. George March 14, 2015 Thrombotic Microangiopathies (TMA): Everything you need to know from 5 patient stories Thrombotic
Thrombotic Microangiopathies ASH/San Antonio Breast Cancer Symposium Review James N. George March 14, 2015 Thrombotic Microangiopathies (TMA): Everything you need to know from 5 patient stories Thrombotic
RaDaR Inclusion and Exclusion Criteria. Diagnosis Inclusion Criteria Exclusion Criteria. Alport Syndrome definite or probable
 Alport Syndrome and Type IV collagenopathies APRT Deficiency Alport Syndrome definite or probable Alport carrier definite or probable Thin basement membrane nephropathy APRT Deficiency confirmed Abolished
Alport Syndrome and Type IV collagenopathies APRT Deficiency Alport Syndrome definite or probable Alport carrier definite or probable Thin basement membrane nephropathy APRT Deficiency confirmed Abolished
Most Common Hemostasis Consults: Thrombocytopenia
 Most Common Hemostasis Consults: Thrombocytopenia Cindy Neunert, MS MSCS Assistant Professor, Pediatrics CUMC Columbia University TSHNA Meeting, April 15, 2016 Financial Disclosures No relevant financial
Most Common Hemostasis Consults: Thrombocytopenia Cindy Neunert, MS MSCS Assistant Professor, Pediatrics CUMC Columbia University TSHNA Meeting, April 15, 2016 Financial Disclosures No relevant financial
Pathogenetic mechanisms in atypical HUS
 Pathogenetic mechanisms in atypical HUS Seppo Meri University & University Hospital Helsinki, Finland Antalya, Turkey Photo: Markku Kallio 21.10.2017 HUS after eating Kebab - 22 yo female - watery diarrhea
Pathogenetic mechanisms in atypical HUS Seppo Meri University & University Hospital Helsinki, Finland Antalya, Turkey Photo: Markku Kallio 21.10.2017 HUS after eating Kebab - 22 yo female - watery diarrhea
Sacha Zeerleder, MD PhD Internist-hematologist Academic Medical Centre, Amsterdam Sanquin Research, Amsterdam
 Sacha Zeerleder, MD PhD Internist-hematologist Academic Medical Centre, Amsterdam Sanquin Research, Amsterdam Sacha Zeerleder, MD PhD Internist-hematologist Academic Medical Centre, Amsterdam Sanquin Research,
Sacha Zeerleder, MD PhD Internist-hematologist Academic Medical Centre, Amsterdam Sanquin Research, Amsterdam Sacha Zeerleder, MD PhD Internist-hematologist Academic Medical Centre, Amsterdam Sanquin Research,
Complement and the atypical hemolytic uremic syndrome in children
 Pediatr Nephrol (2008) 23:1957 1972 DOI 10.1007/s00467-008-0872-4 EDUCATIONAL REVIEW Complement and the atypical hemolytic uremic syndrome in children Chantal Loirat & Marina Noris & Véronique Fremeaux-Bacchi
Pediatr Nephrol (2008) 23:1957 1972 DOI 10.1007/s00467-008-0872-4 EDUCATIONAL REVIEW Complement and the atypical hemolytic uremic syndrome in children Chantal Loirat & Marina Noris & Véronique Fremeaux-Bacchi
Diagnosis and Treatment of Common TMAs
 Diagnosis and Treatment of Common TMAs K. Pavenski, MD FRCPC St. Michael s Hospital June 13, 2014 Disclosures I have a relevant conflict of interest - Alexion Pharmaceuticals Inc. Participated in advisory
Diagnosis and Treatment of Common TMAs K. Pavenski, MD FRCPC St. Michael s Hospital June 13, 2014 Disclosures I have a relevant conflict of interest - Alexion Pharmaceuticals Inc. Participated in advisory
HEME 10 Bleeding Disorders
 HEME 10 Bleeding Disorders When injury occurs, three mechanisms occur Blood vessels Primary hemostasis Secondary hemostasis Diseases of the blood vessels Platelet disorders Thrombocytopenia Functional
HEME 10 Bleeding Disorders When injury occurs, three mechanisms occur Blood vessels Primary hemostasis Secondary hemostasis Diseases of the blood vessels Platelet disorders Thrombocytopenia Functional
Thrombotic thrombocytopenic purpura: 2008 Update
 MEDICAL GRAND ROUNDS CME CREDIT MARK A. CROWTHER, MD Director, Division of Hematology, McMaster University, Hamilton, Ontario, Canada JAMES N. GEORGE, MD Hematology-Oncology Section, Department of Medicine,
MEDICAL GRAND ROUNDS CME CREDIT MARK A. CROWTHER, MD Director, Division of Hematology, McMaster University, Hamilton, Ontario, Canada JAMES N. GEORGE, MD Hematology-Oncology Section, Department of Medicine,
Eculizumab as Prophylactic Therapy in Atypical Hemolytic Uremic Syndrome in Adult Living-Related Kidney Transplantation
 Anti-C5 as Prophylactic Therapy in Atypical Hemolytic Uremic Syndrome in Living- Related Kidney Transplantation Authors: Miquel Blasco 1, Santiago Rodríguez de Córdoba 2, Fritz Diekmann 1, Mercedes Saiz
Anti-C5 as Prophylactic Therapy in Atypical Hemolytic Uremic Syndrome in Living- Related Kidney Transplantation Authors: Miquel Blasco 1, Santiago Rodríguez de Córdoba 2, Fritz Diekmann 1, Mercedes Saiz
Renal failure and thrombocytopaenia? Don t forget TTP/HUS. Jonathan Wala Nephrologist
 Renal failure and thrombocytopaenia? Don t forget TTP/HUS Jonathan Wala Nephrologist Thrombotic microangiopathies Disorders characterized by: thrombocytopaenia microangiopathic haemolytic anaemia (MAHA)
Renal failure and thrombocytopaenia? Don t forget TTP/HUS Jonathan Wala Nephrologist Thrombotic microangiopathies Disorders characterized by: thrombocytopaenia microangiopathic haemolytic anaemia (MAHA)
Familial DDD associated with a gain-of-function mutation in complement C3.
 Familial DDD associated with a gain-of-function mutation in complement C3. Santiago Rodríguez de Córdoba, Centro de investigaciones Biológicas, Madrid Valdés Cañedo F. and Vázquez- Martul E., Complejo
Familial DDD associated with a gain-of-function mutation in complement C3. Santiago Rodríguez de Córdoba, Centro de investigaciones Biológicas, Madrid Valdés Cañedo F. and Vázquez- Martul E., Complejo
Medical Policy. MP Eculizumab (Soliris) Related Policies None. Last Review: 01/24/2019 Effective Date: 04/25/2019 Section: Prescription Drug
 Related Policies None. Last Review: 01/24/2019 Effective Date: 04/25/2019 Section: Prescription Drug") Medical Policy Last Review: 01/24/2019 Effective Date: 04/25/2019 Section: Prescription Drug Related Policies None DISCLAIMER Our medical policies are designed for informational purposes only and are not
Medical Policy Last Review: 01/24/2019 Effective Date: 04/25/2019 Section: Prescription Drug Related Policies None DISCLAIMER Our medical policies are designed for informational purposes only and are not
Complement in vasculitis and glomerulonephritis. Andy Rees Clinical Institute of Pathology Medical University of Vienna
 Complement in vasculitis and glomerulonephritis Andy Rees Clinical Institute of Pathology Medical University of Vienna 41 st Heidelberg Nephrology Seminar March 2017 The complement system An evolutionary
Complement in vasculitis and glomerulonephritis Andy Rees Clinical Institute of Pathology Medical University of Vienna 41 st Heidelberg Nephrology Seminar March 2017 The complement system An evolutionary
THE MULTIPLE FACETS OF THROMBOTIC MICROANGIOPATHIES
 THE MULTIPLE FACETS OF THROMBOTIC MICROANGIOPATHIES Summary of Presentations from the Alexion-Sponsored Symposium, held at the 19 th EHA Congress, Milan, Italy, on 12 th June 2014 Chairperson Pier Mannuccio
THE MULTIPLE FACETS OF THROMBOTIC MICROANGIOPATHIES Summary of Presentations from the Alexion-Sponsored Symposium, held at the 19 th EHA Congress, Milan, Italy, on 12 th June 2014 Chairperson Pier Mannuccio
An international consensus approach to the management of atypical hemolytic uremic syndrome in children
 DOI 10.1007/s00467-015-3076-8 REVIEW An international consensus approach to the management of atypical hemolytic uremic syndrome in children Chantal Loirat & Fadi Fakhouri & Gema Ariceta & Nesrin Besbas
DOI 10.1007/s00467-015-3076-8 REVIEW An international consensus approach to the management of atypical hemolytic uremic syndrome in children Chantal Loirat & Fadi Fakhouri & Gema Ariceta & Nesrin Besbas
Initial management of TMA syndromes
 Initial management of TMA syndromes Elie Azoulay, Saint-Louis Hospital, Medical Intensive Care Unit Paris Diderot Sorbonne University Groupe de Recherche Respiratoire en Réanimation Onco-Hématologique
Initial management of TMA syndromes Elie Azoulay, Saint-Louis Hospital, Medical Intensive Care Unit Paris Diderot Sorbonne University Groupe de Recherche Respiratoire en Réanimation Onco-Hématologique
Thrombotic thrombocytopenic purpura: a look at the future
 Thrombotic thrombocytopenic purpura: a look at the future Andrea Artoni, MD Ph.D. Angelo Bianchi Bonomi Hemophilia and Thrombosis Center IRCCS Ca Granda Ospedale Maggiore Policlinico Milan, Italy andrea.artoni@policlinico.mi.it
Thrombotic thrombocytopenic purpura: a look at the future Andrea Artoni, MD Ph.D. Angelo Bianchi Bonomi Hemophilia and Thrombosis Center IRCCS Ca Granda Ospedale Maggiore Policlinico Milan, Italy andrea.artoni@policlinico.mi.it
A 36 year old previously healthy female develops fever and ruising
 Renal vascular diseases CPC G.A. Appel MD M.B. Stokes MD Case 1 A 36 year old previously healthy female develops fever and bruising. She goes to her LMD and CBC shows plats 15 K, Hct 28%, normal PT and
Renal vascular diseases CPC G.A. Appel MD M.B. Stokes MD Case 1 A 36 year old previously healthy female develops fever and bruising. She goes to her LMD and CBC shows plats 15 K, Hct 28%, normal PT and
Thrombotic Microangiopathy and the Kidney
 CJASN epress. Published on October 17, 2017 as doi: 10.2215/CJN.00620117 Thrombotic Microangiopathy and the Kidney Vicky Brocklebank,* Katrina M. Wood, and David Kavanagh* Abstract Thrombotic microangiopathy
CJASN epress. Published on October 17, 2017 as doi: 10.2215/CJN.00620117 Thrombotic Microangiopathy and the Kidney Vicky Brocklebank,* Katrina M. Wood, and David Kavanagh* Abstract Thrombotic microangiopathy
Challenges in Renal Apheresis. Mark E. Williams MD, FACP, FASN Director, Renal Apheresis Beth Israel Deaconess Medical Center Harvard Medical School
 Challenges in Renal Apheresis Mark E. Williams MD, FACP, FASN Director, Renal Apheresis Beth Israel Deaconess Medical Center Harvard Medical School Outline Principles of Separation ASFA Guidelines Renal
Challenges in Renal Apheresis Mark E. Williams MD, FACP, FASN Director, Renal Apheresis Beth Israel Deaconess Medical Center Harvard Medical School Outline Principles of Separation ASFA Guidelines Renal
Unravelling the pathophysiology of HUS in light of recent discoveries on complement activation
 Unravelling the pathophysiology of HUS in light of recent discoveries on complement activation Marina Noris November 13, 2018 1 THROMBOTIC MICROANGIOPATHY Histology lesions: Swelling and detachment of
Unravelling the pathophysiology of HUS in light of recent discoveries on complement activation Marina Noris November 13, 2018 1 THROMBOTIC MICROANGIOPATHY Histology lesions: Swelling and detachment of
A CAREGIVER S JOURNEY
 A CAREGIVER S JOURNEY Learning about atypical hemolytic uremic syndrome (ahus) Begin your path to effective advocacy and support Caring for someone who is diagnosed with ahus can be overwhelming. You may
A CAREGIVER S JOURNEY Learning about atypical hemolytic uremic syndrome (ahus) Begin your path to effective advocacy and support Caring for someone who is diagnosed with ahus can be overwhelming. You may
Kidney disease associated with autoimmune disease
 Kidney disease associated with autoimmune disease Masaomi Nangaku Division of Nephrology and Endocrinology the University of Tokyo Graduate School of Medicine, Japan M-type Phospholipase A2 Receptor as
Kidney disease associated with autoimmune disease Masaomi Nangaku Division of Nephrology and Endocrinology the University of Tokyo Graduate School of Medicine, Japan M-type Phospholipase A2 Receptor as
Things to never miss in the office. Brett Houston MD FRCPC (PYG-5, hematology) Leonard Minuk MD FRCPC
 Leonard Minuk MD FRCPC") Things to never miss in the office Brett Houston MD FRCPC (PYG-5, hematology) Leonard Minuk MD FRCPC Presenter Disclosure Faculty / Speaker s name: Brett Houston / Leonard Minuk Relationships with commercial
Things to never miss in the office Brett Houston MD FRCPC (PYG-5, hematology) Leonard Minuk MD FRCPC Presenter Disclosure Faculty / Speaker s name: Brett Houston / Leonard Minuk Relationships with commercial
Case report 24 th Summer School of Internal Medicine 2015
 Case report 24 th Summer School of Internal Medicine 2015 Goldmannová D., Horák P., Skácelová M. IIIrd Internal Clinic - endocrinology, diabetology, rheumatology, nephrology University hospital Olomouc,
Case report 24 th Summer School of Internal Medicine 2015 Goldmannová D., Horák P., Skácelová M. IIIrd Internal Clinic - endocrinology, diabetology, rheumatology, nephrology University hospital Olomouc,
Thrombocytopenia is not mandatory to diagnose haemolytic and uremic syndrome
 Sallée et al. BMC Nephrology 2013, 14:3 RESEARCH ARTICLE Open Access Thrombocytopenia is not mandatory to diagnose haemolytic and uremic syndrome Marion Sallée 1, Khalil Ismail 1, Fadi Fakhouri 2, Henri
Sallée et al. BMC Nephrology 2013, 14:3 RESEARCH ARTICLE Open Access Thrombocytopenia is not mandatory to diagnose haemolytic and uremic syndrome Marion Sallée 1, Khalil Ismail 1, Fadi Fakhouri 2, Henri
A PATIENT S JOURNEY. Learning about atypical hemolytic uremic syndrome (ahus)
") A PATIENT S JOURNEY Learning about atypical hemolytic uremic syndrome (ahus) Begin your path to empowerment Being diagnosed with ahus can be overwhelming. You may have many questions: What is ahus? How
A PATIENT S JOURNEY Learning about atypical hemolytic uremic syndrome (ahus) Begin your path to empowerment Being diagnosed with ahus can be overwhelming. You may have many questions: What is ahus? How
From MPGN to C3G. F Fakhouri, Nantes, France. «Membranoproliferative» is a pathological feature. Mesangial expansion «Doubles contours»
 From MPGN to C3G F Fakhouri, Nantes, France Conflits d intérêt: consultant auprès d Alexion Pharmaceuticals «Membranoproliferative» is a pathological feature Mesangial expansion «Doubles contours» Immune
From MPGN to C3G F Fakhouri, Nantes, France Conflits d intérêt: consultant auprès d Alexion Pharmaceuticals «Membranoproliferative» is a pathological feature Mesangial expansion «Doubles contours» Immune
Presentation Outline. Disease Background Previous research on platelet recovery rate Goal of our study Methods Results Limitations Conclusions
 Platelet Recovery Rate at Day 5 of Therapeutic Plasma Exchange for Acquired Thrombotic Thrombocytopenic Purpura Can Aid in Identifying Risk of Disease Exacerbation Suzanne Zhou, Yara A. Park, Marian A.
Platelet Recovery Rate at Day 5 of Therapeutic Plasma Exchange for Acquired Thrombotic Thrombocytopenic Purpura Can Aid in Identifying Risk of Disease Exacerbation Suzanne Zhou, Yara A. Park, Marian A.
HEL(L)P?! when extensive laboratory diagnostics are required. Madách Krisztina
P?! when extensive laboratory diagnostics are required. Madách Krisztina") HEL(L)P?! when extensive laboratory diagnostics are required Madách Krisztina Semmelweis University Department of Anaesthesiology and Intensive Therapy Budapest Haemolysis, elevated liver enzymes, low
HEL(L)P?! when extensive laboratory diagnostics are required Madách Krisztina Semmelweis University Department of Anaesthesiology and Intensive Therapy Budapest Haemolysis, elevated liver enzymes, low
Soliris. Soliris (eculizumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.85.11 Subject: Soliris Page: 1 of 5 Last Review Date: September 20, 2018 Soliris Description Soliris
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.85.11 Subject: Soliris Page: 1 of 5 Last Review Date: September 20, 2018 Soliris Description Soliris
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT. J. H. Helderman,MD,FACP,FAST
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
Les microangiopathies thrombotiques Quoi de neuf?
 Les microangiopathies thrombotiques Quoi de neuf? Société des Sciences Vasculaires du Québec 16 Septembre 2016 Anne-Laure Lapeyraque CHU Sainte Justine, Montréal anne.laure.lapeyraque@umontreal.ca Objectifs
Les microangiopathies thrombotiques Quoi de neuf? Société des Sciences Vasculaires du Québec 16 Septembre 2016 Anne-Laure Lapeyraque CHU Sainte Justine, Montréal anne.laure.lapeyraque@umontreal.ca Objectifs
Untying the Knot of Thrombotic Thrombocytopenic Purpura and Atypical Hemolytic Uremic Syndrome
 REVIEW Untying the Knot of Thrombotic Thrombocytopenic Purpura and Atypical Hemolytic Uremic Syndrome Han-Mou Tsai, MD imah Hematology Associates, New Hyde Park, NY. ABSTRACT Patients presenting with microangiopathic
REVIEW Untying the Knot of Thrombotic Thrombocytopenic Purpura and Atypical Hemolytic Uremic Syndrome Han-Mou Tsai, MD imah Hematology Associates, New Hyde Park, NY. ABSTRACT Patients presenting with microangiopathic
PNH ahus. Dosing and Administration. For Paroxysmal Nocturnal Hemoglobinuria (PNH) and atypical Hemolytic Uremic Syndrome (ahus) patients
 and atypical Hemolytic Uremic Syndrome (ahus) patients") For Paroxysmal Nocturnal Hemoglobinuria (PNH) and atypical Hemolytic Uremic Syndrome (ahus) patients PNH ahus Dosing and Administration Soliris is indicated for the treatment of patients with paroxysmal
For Paroxysmal Nocturnal Hemoglobinuria (PNH) and atypical Hemolytic Uremic Syndrome (ahus) patients PNH ahus Dosing and Administration Soliris is indicated for the treatment of patients with paroxysmal
Eculizumab in ahus: where do we stand in Prof. Fadi Fakhouri Dept. of nephrology and immunology, CHU de Nantes.
 Eculizumab in ahus: where do we stand in 2016 Prof. Fadi Fakhouri Dept. of nephrology and immunology, CHU de Nantes. INSERM UMR S-1064 Thrombotic microangiopathy: evolving concepts ST-HUS Coagulation mediated-tma
Eculizumab in ahus: where do we stand in 2016 Prof. Fadi Fakhouri Dept. of nephrology and immunology, CHU de Nantes. INSERM UMR S-1064 Thrombotic microangiopathy: evolving concepts ST-HUS Coagulation mediated-tma
Keeping track of your numbers
 Keeping track of your numbers If you have relapsed or refractory multiple myeloma, keeping track of your numbers can help you take an active role in your care. It s also one way you and your doctor can
Keeping track of your numbers If you have relapsed or refractory multiple myeloma, keeping track of your numbers can help you take an active role in your care. It s also one way you and your doctor can
Recurrence of C3G after renal transplantation. Moglie Le Quintrec Service de Néphrologie, Hôpital Foch CRC, UMRS 1138, Equipe complement and diseases
 Recurrence of C3G after renal transplantation Moglie Le Quintrec Service de Néphrologie, Hôpital Foch CRC, UMRS 1138, Equipe complement and diseases New MPGN classification C3G MPGN I DDD C3GN IF C3 deposits
Recurrence of C3G after renal transplantation Moglie Le Quintrec Service de Néphrologie, Hôpital Foch CRC, UMRS 1138, Equipe complement and diseases New MPGN classification C3G MPGN I DDD C3GN IF C3 deposits