Renal failure and thrombocytopaenia? Don t forget TTP/HUS. Jonathan Wala Nephrologist
|
|
|
- Hannah Hoover
- 5 years ago
- Views:
Transcription
1 Renal failure and thrombocytopaenia? Don t forget TTP/HUS Jonathan Wala Nephrologist
2 Thrombotic microangiopathies Disorders characterized by: thrombocytopaenia microangiopathic haemolytic anaemia (MAHA) microvascular occlusion, often resulting in brain and kidney ischaemia Result from microvascular occlusion by hyaline thrombi Spectrum ranges from TTP to HUS
3 Thrombotic microangiopathies Although rare, should always be considered in any pt presenting with AKI assoc with thrombocytopaenia Therapeutic plasma infusion or exchange are effective treatment modalities 3 case reports are presented to heighten the index of suspicion regarding this catastrophic disorder and to illustrate challenges faced in its diagnosis and management
4 Case 1 44y-old lady, S.P. DOA: 13/1/2012 Presentation: Diarrhoea X 2/52 Jaundice and vomiting X 2/52 Managed for viral hepatitis Progressive dyspnoea hospitalization PMHx: unremarkable Examination: Respiratory distress Bilateral leg petechiae Jaundice Pallor PR 106/min, BP 139/79 Clear chest auscultation Alert but agitated No hepatosplenomegaly Urine output: nil
5 Case 1 Laboratory: Hb 6.7g/dL, WBC 38 X 109/L, platelet 37 X 109/L PBF: anisilopoikilocytosis with microspherocytes and few schistocytes Marked neutrophilia with left shift and toxic granulations Thrombocytopaenia INR 2.3 Urea 26.8mmol/L, creat 567umol/L, K+ 3.7mmol/L Bilirubin 184umol/L (direct 102umol/L), AST 184, ALT 36 LDH 825 U/mL CRP 266 mg/l Blood and urine culture: sterile Requested but no result: Stool culture ± E. coli typing Stool Shiga toxin assay ADAMTS13 serum levels Complement protein assays
6 Diagnosis AKI with MAHA and thrombocytopaenia: DDx: Septic AKI with DIC HUS/TTP SLE with autoimmune anaemia and thrombocytopaenia (Evans syndrome) and lupus nephritis
7 Management Haemodialysis Blood component transfusion: RBC transfusion Platelet transfusion Plasma transfusion (FFP) Antibiotic cover (empirical)
8 Hospital course of platelet count and creatinine of case HD + 4 RBCs HD + FFP HD + FFP 500 HD + 6 platelets Antibiotics Platelet count Serum creatinine (umol/l) Days after admission
9 Outcome Anuric at discharge and maintained intermittent HD Progressive recovery of renal function thereafter Stopped haemodialysis 3 weeks later Last follow-up 10 months later: creatinine 70umoL/L
10 CASE 2
11 Case 2: AK 60y-old lady, AM DOA: 16/10/2012 Type 2 diabetes on metformin Presentation: Cough X 1/52 Diarrhoea X 3/7 Dyspnoea and fever X 2/7 Examination: Sick, respiratory distress PR 128/min, BP 91/54mmHg RR 34/min, SO2 84% on room air Bilateral crepitations No hepatosplenomegaly Urine output 15mL/h after fluid resuscitation and IV Furosemide, anuric by 2 nd day
12 Case 2 Laboratory: Hb 12.5g/dL, WBC 5.7 X 109/L, platelets 34 X 109/L PBF: anisilopoikilocytosis with few schistocytes Urea 14.9mmol/L, creat 272umol/L, Na+ 123mmol/L, K+ 3.6mmol/L Bil 28umol/L, AST 56 LDH 748 U/mL Urinalysis: blood 2+, protein +, granular casts CRP 339mg/L Blood culture: Escherichia coli (MDR) Urine culture: Escherichia coli (MDR) Stool culture: no growth (sample obtained 2 days after antibiotics commenced) Requested but not available: E. coli typing Stool Shiga toxin assay Serum ADAMTS13 level Complement assays
13 Case 2 Diagnosis Septic shock from lobar pneumonia AKI with thrombocytopaenia Differential diagnosis: TTP/HUS: Shiga-toxin associated E. coli Neuraminidaseproducing Streptococcus pneumoniae Septic AKI with DIC
14 Management Septic shock: Fluid resuscitation Norepinephrine Antibiotic: Imipenem Respiratory failure: endotracheal intubation and mechanical ventilation AKI: alternate-day intermittent haemodialysis TTP/HUS: Plasma infusion with ultrafiltration across haemodialysis Therapeutic plasma exchange: Plasmapharesis with a plasma filter Duration 3h Blood flow ml/min Plasma volume exchanged: 50mL/kg = ~ 3500ml plasma = 25 units FFP Alternate days for 1 week
15 Hospital course of platelet count and creatinine of case HD Plasma transfusion 15 units HD TPE 25 units HD + TPE 20 units TPE 25 units Antibiotics 50 0 Serum creatinine (umol/l) Platelet count Days after admission
16 Outcome At discharge: Ambulant Haemodynamically stable Hb 7.0g/dL, WBC 5.8 X 109/L, platelet 196 X 109/L Creat 131umol/L, urea 7.4mmol/L, K+ 4.0mmol/L, Na+ 136mmol/L Follow up at 4 months: Creatinine umol/L: egfr 50-55mL/min
17 Case 3 68y-old lady, S.S. DOA: 25/5/2012 Comorbidity: HTN, GERD, previous PTB Presentation: Abdominal pain + 1 episode of non-bloody diarrhoea Chills Examination: Afebrile (fever later) Tender epigastrium No petechiae After admission: 3 generalized tonicclonic seizures ICU, ventilation, anticonvulsants
18 Case 3 Laboratory: Hb , WBC 7.3, platelet PBF: fragmented RBCs, burr cells Coagulation profile: normal LDH 691 U/mL Creat umol/L Urinalysis: protein 3+, blood +, granular casts CRP 8mg/L LFTs normal MRI brain: motion artifacts, cerebral atrophy
19 Case 3 Diagnosis: Thrombotic microangiopathy complicated by: DDx: Renal failure Neurological manifestations Vasculitis Sepsis with DIC SLE with lupus nephritis and neurolupus
20 Case 3 Management: Initially for sepsis: Antibiotics Acyclovir for presumed encephalitis Haemodialysis initiated Plasma transfusion: 8 units FFP Steroids: methylprednisolone Transferred for plasmapharesis on day 4
21 Course of creatinine and platelet for case 3 Daily TPE units FFP Bleeding diasthesis Alternate-day HD Candidaemia Diffuse alveolar haemorrhage Platelet count Serum creatinine umol/l Days after admission
22 Discussion 3 cases presenting with AKI, thrombocytopaenia and MAHA Consistent with thrombotic microangiopathy Major differential diagnosis: Sepsis with septic AKI and thrombocytopaenia
23 Thrombotic microangiopathy Clinico-pathological syndrome resulting from hyaline thrombi in microvasculature of various organs Presents acutely with: MAHA thrombocytopaenia variable degrees of organ dysfunction Depending on predominant distribution of lesions (CNS or kidney) 2 pathologically identical but clinically distinct syndromes: Haemolytic uraemic syndrome Thrombotic thrombocytopaenic purpura
24 Syndromes of thrombotic microangiopathy Thrombotic thrombocytopenic purpura (TTP): Abruptly devt of VWF- and platelet-rich thrombi in arterioles and capillaries of brain, heart, other organs Neurological abnormalities are common Mild renal abnormalities e.g. haematuria, proteinuria Rare: hypertension, AKI requiring dialysis Prognosis: without treatment: very high mortality rate (> 90%) plasma infusion or plasma exchange: 70 90% survival HUS: Usually in young children AKI and absent or minimal neurological involvement May be: diarrhoea associated: typical HUS no diarrhoea: atypical HUS Prognosis of typical HUS: Dialysis in 50% Benign: 90% recover fully

25 Pathogenesis of typical HUS
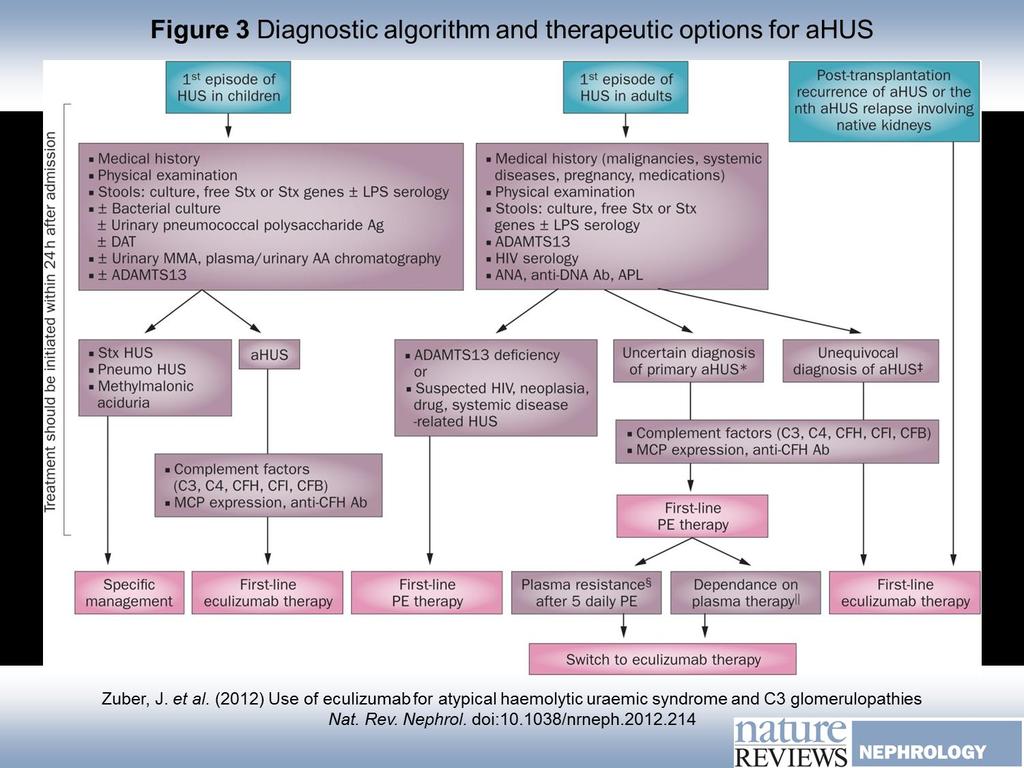
26 Pathogenesis of atypical HUS
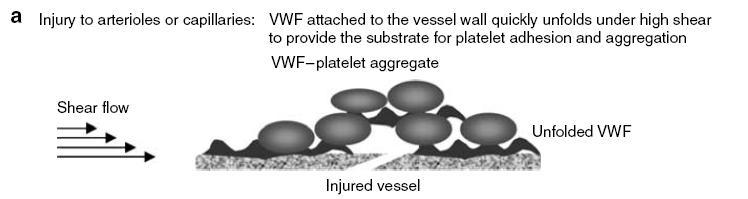
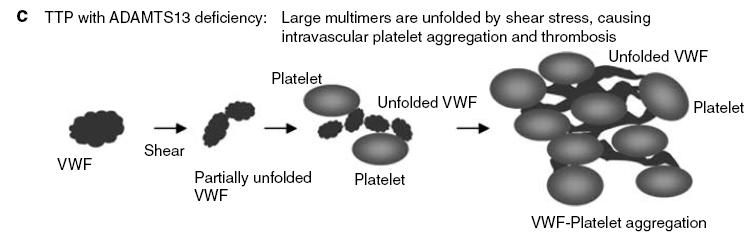
27 Pathogenesis of TTP


28 Kidney biopsies Hemolytic uremic syndrome, D+ Glomerular capillary lumina closed by thickening of capillary walls RBCs and fragmented RBCs in mesangial areas Thrombotic thrombocytopenic purpura Glomerular capillary lumina occluded by homogenous eosinophilic thrombi
29 New classification Known aetiopathogenesis: Infection-induced: Shiga and verocytotoxin (shiga-like toxin)-producing bacteria: Enterohemorrhagic Escherichia coli Shigella dysenteriae type 1 Citrobacter freundii Streptococcus pneumoniae: neuraminidase T-antigen exposure Disorders of complement regulation: Genetic Acquired ADAMTS13 deficiency Genetic disorders of ADAMTS13 Acquired ADAMTS13 deficiency: autoimmune drug induced Defective cobalamine metabolism Quinine-induced Clinical associations: etiology unknown HIV Malignancy-related: Disseminated carcinoma Chemotherapy: mitomycin, gemcitabine Ionizing radiation Transplant-related: Calcineurin inhibitors Bone marrow transplantation Pregnancy-related: Pregnancy HELLP syndrome Oral contraceptive pill SLE-related: SLE antiphospholipid antibody syndrome Others: Glomerulopathy Familial Unclassified
30
31 Challenges for us Diagnostic challenges: High-index of suspicion Laboratory deficiencies: Peripheral blood film for schistocytes Stool culture with appropriate culture media Unavailable assays: Shiga toxin ADAMTS13 activity Complement factors Treatment challenges: Confirmed typical HUS: Supportive No role for plasma therapy Atypical HUS and TTP: Benefit from plasma therapy Expensive treatment Unavailable Plenty of FFPs required = many donors required Nursing expertise (and patience) required
32 Final word Thrombotic microangiopathies are a catastrophic cause of AKI High index of suspicion needed whenever AKI is accompanied by thrombocytopaenia Appropriate lab back-up needed Plasma therapy, when required, provides good outcomes but is fraught with cost and logistical challenges
What is meant by Thrombotic Microangiopathy (TMA)?
?") What is meant by Thrombotic Microangiopathy (TMA)? Thrombotic Microangiopathy (TMA) is a group of disorders characterized by injured endothelial cells, microangiopathic hemolytic anemia (MAHA), with its
What is meant by Thrombotic Microangiopathy (TMA)? Thrombotic Microangiopathy (TMA) is a group of disorders characterized by injured endothelial cells, microangiopathic hemolytic anemia (MAHA), with its
Hemolytic uremic syndrome: Investigations and management
 Hemolytic uremic syndrome: Investigations and management SAWAI Toshihiro M.D., Ph.D. Department of Pediatrics, Shiga University of Medical Science Otsu, JAPAN AGENDA TMA; Thrombotic micro angiopathy STEC-HUS;
Hemolytic uremic syndrome: Investigations and management SAWAI Toshihiro M.D., Ph.D. Department of Pediatrics, Shiga University of Medical Science Otsu, JAPAN AGENDA TMA; Thrombotic micro angiopathy STEC-HUS;
DR V PHILIP CLINICAL HAEMATOLOGY UNIT CHRIS HANI BARAGWANATH ACADEMIC HOSPITAL
 DR V PHILIP CLINICAL HAEMATOLOGY UNIT CHRIS HANI BARAGWANATH ACADEMIC HOSPITAL Rare but fatal disease if unrecognized and untreated Incidence about 1: 1 million in the USA Female preponderance of 2:1 Part
DR V PHILIP CLINICAL HAEMATOLOGY UNIT CHRIS HANI BARAGWANATH ACADEMIC HOSPITAL Rare but fatal disease if unrecognized and untreated Incidence about 1: 1 million in the USA Female preponderance of 2:1 Part
DRUG NAME: Eculizumab Brand(s): Soliris DOSAGE FORM/ STRENGTH: 10 mg/ml (300 mg per vial)
: Soliris DOSAGE FORM/ STRENGTH: 10 mg/ml (300 mg per vial)") Preamble: A confirmed diagnosis of atypical hemolytic uremic syndrome (ahus) is required for eculizumab funding. The information below is to provide clinicians with context for how a diagnosis of ahus
Preamble: A confirmed diagnosis of atypical hemolytic uremic syndrome (ahus) is required for eculizumab funding. The information below is to provide clinicians with context for how a diagnosis of ahus
Primary causes: Complement dysregulation (50% of non-shiga toxin-producing E. coli ) Secondary causes:
 Secondary causes:") General department INTRODUCTION The hemolytic uremic syndrome (HUS): microangiopathic hemolytic anemia, thrombocytopenia, and acute kidney injury One of the main causes of acute kidney injury in children
General department INTRODUCTION The hemolytic uremic syndrome (HUS): microangiopathic hemolytic anemia, thrombocytopenia, and acute kidney injury One of the main causes of acute kidney injury in children
* Renal insufficiencies
 Thrombotic Thrombocytopenic Purpura Behzad Poopak, DCLS PhD. Tehran medical Branch Islamic Azad university bpoopak@yahoo.com Case Summary Ms. X, a 35-year year-old woman Complained of weakness, low grade
Thrombotic Thrombocytopenic Purpura Behzad Poopak, DCLS PhD. Tehran medical Branch Islamic Azad university bpoopak@yahoo.com Case Summary Ms. X, a 35-year year-old woman Complained of weakness, low grade
ISTITUTO DI RICERCHE FARMACOLOGICHE MARIO NEGRI CLINICAL RESEARCH CENTER ALDO E FOR CELE RARE DACCO DISEASES ALDO E CELE DACCO
 ISTITUTO DI RICERCHE FARMACOLOGICHE MARIO NEGRI CENTRO MARIO DI NEGRI RICERCHE INSTITUTE CLINICHE FOR PHARMACOLOGICAL PER LE MALATTIE RESEARCH RARE CLINICAL RESEARCH CENTER ALDO E FOR CELE RARE DACCO DISEASES
ISTITUTO DI RICERCHE FARMACOLOGICHE MARIO NEGRI CENTRO MARIO DI NEGRI RICERCHE INSTITUTE CLINICHE FOR PHARMACOLOGICAL PER LE MALATTIE RESEARCH RARE CLINICAL RESEARCH CENTER ALDO E FOR CELE RARE DACCO DISEASES
A 60 year old woman with altered mental status and thrombotic microangiopathy. Josh Veatch
 A 60 year old woman with altered mental status and thrombotic microangiopathy Josh Veatch Previously healthy 60 year old woman 2 3 months of fatigue following a URI, transient episodes being out of it
A 60 year old woman with altered mental status and thrombotic microangiopathy Josh Veatch Previously healthy 60 year old woman 2 3 months of fatigue following a URI, transient episodes being out of it
THROMBOTIC MICROANGIOPATHY. Jun-Ki Park 7/19/11
 THROMBOTIC MICROANGIOPATHY Jun-Ki Park 7/19/11 TMAs are microvascular occlusive disorders characterized by systemic or intrarenal aggregation of platelets, thrombocytopenia, and mechanical injury to erythrocytes.
THROMBOTIC MICROANGIOPATHY Jun-Ki Park 7/19/11 TMAs are microvascular occlusive disorders characterized by systemic or intrarenal aggregation of platelets, thrombocytopenia, and mechanical injury to erythrocytes.
Dr. E.SUDHA (Fellow in Pediatric Nephrology) DEPT OF PEDIATRIC NEPHROLOGY & DIALYSIS Dr.MEHTA CHILDRENS HOSPITAL
 DEPT OF PEDIATRIC NEPHROLOGY & DIALYSIS Dr.MEHTA CHILDRENS HOSPITAL") Dr. E.SUDHA (Fellow in Pediatric Nephrology) DEPT OF PEDIATRIC NEPHROLOGY & DIALYSIS Dr.MEHTA CHILDRENS HOSPITAL CASE HISTORY 4 yrs old previously well boy Born to 2 nd degree consanguinity Fever x 5 days
Dr. E.SUDHA (Fellow in Pediatric Nephrology) DEPT OF PEDIATRIC NEPHROLOGY & DIALYSIS Dr.MEHTA CHILDRENS HOSPITAL CASE HISTORY 4 yrs old previously well boy Born to 2 nd degree consanguinity Fever x 5 days
Things to never miss in the office. Brett Houston MD FRCPC (PYG-5, hematology) Leonard Minuk MD FRCPC
 Leonard Minuk MD FRCPC") Things to never miss in the office Brett Houston MD FRCPC (PYG-5, hematology) Leonard Minuk MD FRCPC Presenter Disclosure Faculty / Speaker s name: Brett Houston / Leonard Minuk Relationships with commercial
Things to never miss in the office Brett Houston MD FRCPC (PYG-5, hematology) Leonard Minuk MD FRCPC Presenter Disclosure Faculty / Speaker s name: Brett Houston / Leonard Minuk Relationships with commercial
Atypical Hemolytic Uremic Syndrome: When the Environment and Mutations Affect Organ Systems. A Case Report with Review of Literature
 Atypical Hemolytic Uremic Syndrome: When the Environment and Mutations Affect Organ Systems. A Case Report with Review of Literature Mouhanna Abu Ghanimeh 1, Omar Abughanimeh 1, Ayman Qasrawi 1, Abdulraheem
Atypical Hemolytic Uremic Syndrome: When the Environment and Mutations Affect Organ Systems. A Case Report with Review of Literature Mouhanna Abu Ghanimeh 1, Omar Abughanimeh 1, Ayman Qasrawi 1, Abdulraheem
Year 2004 Paper one: Questions supplied by Megan
 QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
A 23 year old Caucasian male presented with shortness of breath, hypertension, bloody sputum, and a history of drug abuse (confirmed by urinalysis).
.") A 23 year old Caucasian male presented with shortness of breath, hypertension, bloody sputum, and a history of drug abuse (confirmed by urinalysis). He was found to have severe kidney injury requiring
A 23 year old Caucasian male presented with shortness of breath, hypertension, bloody sputum, and a history of drug abuse (confirmed by urinalysis). He was found to have severe kidney injury requiring
R. Coward has documented that he has received cooperative grants from Takeda and Novo Nordisk
 R. Coward has documented that he has received cooperative grants from Takeda and Novo Nordisk Advances in our understanding of the pathogenesis of glomerular thrombotic microangiopathy Lindsay Keir Richard
R. Coward has documented that he has received cooperative grants from Takeda and Novo Nordisk Advances in our understanding of the pathogenesis of glomerular thrombotic microangiopathy Lindsay Keir Richard
Approccio morfologico alle microangiopatie trombotiche
 Approccio morfologico alle microangiopatie trombotiche Gina Zini Polo Oncologia e Ematologia Policlinico A. Gemelli Università Cattolica S. Cuore - Roma 1 Thrombotic microangiopathies Occlusive microangiopathic
Approccio morfologico alle microangiopatie trombotiche Gina Zini Polo Oncologia e Ematologia Policlinico A. Gemelli Università Cattolica S. Cuore - Roma 1 Thrombotic microangiopathies Occlusive microangiopathic
Thrombotic Microangiopathies (TMA) / TTP/HUS/αHUS Pathology & Molecular. Genetics
 / TTP/HUS/αHUS Pathology & Molecular. Genetics") Thrombotic Microangiopathies (TMA) / TTP/HUS/αHUS Pathology & Molecular Genetics Helen Liapis, M.D. Senior Consultant Arkana Labs Professor of Pathology & Immunology. retired Washington University School
Thrombotic Microangiopathies (TMA) / TTP/HUS/αHUS Pathology & Molecular Genetics Helen Liapis, M.D. Senior Consultant Arkana Labs Professor of Pathology & Immunology. retired Washington University School
PLASMA EXCHANGE J MANION NEPEAN HOSPITAL
 PLASMA EXCHANGE J MANION NEPEAN HOSPITAL PLASMA The fluid portion of blood Normally approx 5% body weight or 3.5L in 70kg male Clots on standing unless anticoagulated Common plasma proteins are albumin,
PLASMA EXCHANGE J MANION NEPEAN HOSPITAL PLASMA The fluid portion of blood Normally approx 5% body weight or 3.5L in 70kg male Clots on standing unless anticoagulated Common plasma proteins are albumin,
Non-immune acquired haemolytic anaemias. Dr.Maysem
 Non-immune acquired haemolytic anaemias Dr.Maysem Causes of Non-immune acquired haemolytic anaemias. Infections Infections can cause haemolysis in a variety of ways: -They may precipitate an acute haemolytic
Non-immune acquired haemolytic anaemias Dr.Maysem Causes of Non-immune acquired haemolytic anaemias. Infections Infections can cause haemolysis in a variety of ways: -They may precipitate an acute haemolytic
RaDaR Inclusion and Exclusion Criteria. Diagnosis Inclusion Criteria Exclusion Criteria. Alport Syndrome definite or probable
 Alport Syndrome and Type IV collagenopathies APRT Deficiency Alport Syndrome definite or probable Alport carrier definite or probable Thin basement membrane nephropathy APRT Deficiency confirmed Abolished
Alport Syndrome and Type IV collagenopathies APRT Deficiency Alport Syndrome definite or probable Alport carrier definite or probable Thin basement membrane nephropathy APRT Deficiency confirmed Abolished
Thrombotic Microangiopathies
 Thrombotic Microangiopathies ASH/San Antonio Breast Cancer Symposium Review James N. George March 14, 2015 Thrombotic Microangiopathies (TMA): Everything you need to know from 5 patient stories Thrombotic
Thrombotic Microangiopathies ASH/San Antonio Breast Cancer Symposium Review James N. George March 14, 2015 Thrombotic Microangiopathies (TMA): Everything you need to know from 5 patient stories Thrombotic
Thrombotic Thrombocytopenic Purpura and the Role of ADAMTS-13
 Thrombotic Thrombocytopenic Purpura and the Role of ADAMTS-13 Mark Cunningham,MD Director, Hematology Laboratory Department of Pathology University of Kansas Medical Center College of American Pathologists
Thrombotic Thrombocytopenic Purpura and the Role of ADAMTS-13 Mark Cunningham,MD Director, Hematology Laboratory Department of Pathology University of Kansas Medical Center College of American Pathologists
Let`s go for the diagnosis! Yazeed Toukan, MD Pediatric Pulmonary Institute, Ruth Rappaport Children`s Hospital July 2016
 Let`s go for the diagnosis! Yazeed Toukan, MD Pediatric Pulmonary Institute, Ruth Rappaport Children`s Hospital July 2016 Case report 20 months old girl Israeli Arab Muslim family, consanguineous marriage
Let`s go for the diagnosis! Yazeed Toukan, MD Pediatric Pulmonary Institute, Ruth Rappaport Children`s Hospital July 2016 Case report 20 months old girl Israeli Arab Muslim family, consanguineous marriage
Beyond Plasma Exchange: Targeted Therapy for Thrombotic Thrombocytopenic Purpura
 Beyond Plasma Exchange: Targeted Therapy for Thrombotic Thrombocytopenic Purpura Kristen Knoph, PharmD, BCPS PGY2 Pharmacotherapy Resident Pharmacy Grand Rounds April 25, 2017 2016 MFMER slide-1 Objectives
Beyond Plasma Exchange: Targeted Therapy for Thrombotic Thrombocytopenic Purpura Kristen Knoph, PharmD, BCPS PGY2 Pharmacotherapy Resident Pharmacy Grand Rounds April 25, 2017 2016 MFMER slide-1 Objectives
CRRT Fundamentals Pre-Test. AKI & CRRT 2017 Practice Based Learning in CRRT
 CRRT Fundamentals Pre-Test AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling at home. He
CRRT Fundamentals Pre-Test AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling at home. He
Haemolytic uraemic syndrome the story of a whodunit
 Haemolytic uraemic syndrome the story of a whodunit Paul Warwicker Lancashire Teaching Hospitals NHS Trust RCP Kidney for the General Physician Conference Nov 17 Renal thrombotic microangiopathy (TMA)
Haemolytic uraemic syndrome the story of a whodunit Paul Warwicker Lancashire Teaching Hospitals NHS Trust RCP Kidney for the General Physician Conference Nov 17 Renal thrombotic microangiopathy (TMA)
Symposium. Acute Kidney Injury with Thrombocytopenia. Lalitha A V*, Suryanarayana G**, Sumithra S***
 Symposium Acute Kidney Injury with Thrombocytopenia 10.21304/2018.0502.00372 Lalitha A V*, Suryanarayana G**, Sumithra S*** *Associate Professor, Head,PICU **, Fellow in PICU, *** Assistant Professor,
Symposium Acute Kidney Injury with Thrombocytopenia 10.21304/2018.0502.00372 Lalitha A V*, Suryanarayana G**, Sumithra S*** *Associate Professor, Head,PICU **, Fellow in PICU, *** Assistant Professor,
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Lapeyraque A-L, Malina M, Fremeaux-Bacchi V, et al. Eculizumab
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Lapeyraque A-L, Malina M, Fremeaux-Bacchi V, et al. Eculizumab
Haematological Emergencies (Part 1) Ray Mun Koo Haematology Advanced Trainee Canberra Hospital
 Ray Mun Koo Haematology Advanced Trainee Canberra Hospital") Haematological Emergencies (Part 1) Ray Mun Koo Haematology Advanced Trainee Canberra Hospital Case Number 1 43 year old male presenting with fevers, abdominal distension and weight gain over 2 weeks.
Haematological Emergencies (Part 1) Ray Mun Koo Haematology Advanced Trainee Canberra Hospital Case Number 1 43 year old male presenting with fevers, abdominal distension and weight gain over 2 weeks.
Putting the Pieces Together. Anne Longtine MD Internal Medicine Residency, Maine Medical Center Maine ACP Annual Meeting Clinical Vignette 9/16/2017
 Putting the Pieces Together Anne Longtine MD Internal Medicine Residency, Maine Medical Center Maine ACP Annual Meeting Clinical Vignette 9/16/2017 One Week Ago: Outpatient Clinic 64 y/o female presenting
Putting the Pieces Together Anne Longtine MD Internal Medicine Residency, Maine Medical Center Maine ACP Annual Meeting Clinical Vignette 9/16/2017 One Week Ago: Outpatient Clinic 64 y/o female presenting
Transfusion-Related Acute Lung Injury (TRALI) and Strategies for Prevention. Khalid Abdulla Sharif, MD, MRCP (UK)*
 and Strategies for Prevention. Khalid Abdulla Sharif, MD, MRCP (UK)*") Bahrain Medical Bulletin, Vol. 29, No.4, December 2007 Transfusion-Related Acute Lung Injury (TRALI) and Strategies for Prevention Khalid Abdulla Sharif, MD, MRCP (UK)* Background: Transfusion-Related
Bahrain Medical Bulletin, Vol. 29, No.4, December 2007 Transfusion-Related Acute Lung Injury (TRALI) and Strategies for Prevention Khalid Abdulla Sharif, MD, MRCP (UK)* Background: Transfusion-Related
Blood is serious business
 Transfusion at RCH BLOOD TRANSFUSION Anthea Greenway Dept of Clinical Haematology >10000 fresh blood products per year Supports craniofacial and cardiac surgery Support bone marrow, liver transplant and
Transfusion at RCH BLOOD TRANSFUSION Anthea Greenway Dept of Clinical Haematology >10000 fresh blood products per year Supports craniofacial and cardiac surgery Support bone marrow, liver transplant and
Maresce Bizaare AWACC 2013
 Maresce Bizaare AWACC 2013 Cytopaenias in HIV Most common complication of HIV Anaemia is most common cytopaenia ITP occurs in 30%, may be first manifestation of HIV Laboratory approach to cytopaenia FBC,
Maresce Bizaare AWACC 2013 Cytopaenias in HIV Most common complication of HIV Anaemia is most common cytopaenia ITP occurs in 30%, may be first manifestation of HIV Laboratory approach to cytopaenia FBC,
Some renal vascular disorders
 Some renal vascular disorders Introduction Nearly all diseases of the kidney involve the renal blood vessels secondarily We will discuss: -Hypertension (arterionephrosclerosis in benign HTN & hyperplastic
Some renal vascular disorders Introduction Nearly all diseases of the kidney involve the renal blood vessels secondarily We will discuss: -Hypertension (arterionephrosclerosis in benign HTN & hyperplastic
Effect of under filling tube
 Effect of under filling tube 2 What constitutes underfilling? A 4.5ml vacutainer collection tube should contain at least 4ml of blood Less than that could give falsely prolonged clotting times ALSO be
Effect of under filling tube 2 What constitutes underfilling? A 4.5ml vacutainer collection tube should contain at least 4ml of blood Less than that could give falsely prolonged clotting times ALSO be
1. INSTRUCTIONS 2. DEFINITION OF HUS
 CQ_IBK_aHUS_01 / version 25/11/09 European Paediatric Research Group for HUS and related disorders Case questionnaire for diarrhoea negative/vtec (STEC) negative cases acute phase 1. INSTRUCTIONS Please
CQ_IBK_aHUS_01 / version 25/11/09 European Paediatric Research Group for HUS and related disorders Case questionnaire for diarrhoea negative/vtec (STEC) negative cases acute phase 1. INSTRUCTIONS Please
Heme (Bleeding and Coagulopathies) in the ICU
 in the ICU") Heme (Bleeding and Coagulopathies) in the ICU General Topics To Discuss Transfusions DIC Thrombocytopenia Liver and renal disease related bleeding Lack of evidence in managing critical illness related
Heme (Bleeding and Coagulopathies) in the ICU General Topics To Discuss Transfusions DIC Thrombocytopenia Liver and renal disease related bleeding Lack of evidence in managing critical illness related
Bleeding and Thrombotic Disorders. Kristine Krafts, M.D.
 Bleeding and Thrombotic Disorders Kristine Krafts, M.D. Bleeding and Thrombotic Disorders Bleeding disorders von Willebrand disease Hemophilia A and B DIC TTP/HUS ITP Thrombotic disorders Factor V Leiden
Bleeding and Thrombotic Disorders Kristine Krafts, M.D. Bleeding and Thrombotic Disorders Bleeding disorders von Willebrand disease Hemophilia A and B DIC TTP/HUS ITP Thrombotic disorders Factor V Leiden
When the story begin, it was last year
 When the story begin, it was last year Mr. Ho, YC 58/ M Ex smoker PMH : HT, hyperlipidaemia Med: adalat retard, lopid and losartan Presented to POH on 17 th Feb., 2016 High fever and URTI symptom On admission
When the story begin, it was last year Mr. Ho, YC 58/ M Ex smoker PMH : HT, hyperlipidaemia Med: adalat retard, lopid and losartan Presented to POH on 17 th Feb., 2016 High fever and URTI symptom On admission
Keeping track of your numbers
 Keeping track of your numbers If you have relapsed or refractory multiple myeloma, keeping track of your numbers can help you take an active role in your care. It s also one way you and your doctor can
Keeping track of your numbers If you have relapsed or refractory multiple myeloma, keeping track of your numbers can help you take an active role in your care. It s also one way you and your doctor can
HEME 10 Bleeding Disorders
 HEME 10 Bleeding Disorders When injury occurs, three mechanisms occur Blood vessels Primary hemostasis Secondary hemostasis Diseases of the blood vessels Platelet disorders Thrombocytopenia Functional
HEME 10 Bleeding Disorders When injury occurs, three mechanisms occur Blood vessels Primary hemostasis Secondary hemostasis Diseases of the blood vessels Platelet disorders Thrombocytopenia Functional
Clinical Study Eculizumab Therapy Leads to Rapid Resolution of Thrombocytopenia in Atypical Hemolytic Uremic Syndrome
 Hindawi Publishing Corporation Advances in Hematology Volume 214, Article ID 295323, 7 pages http://dx.doi.org/1.1155/214/295323 Clinical Study Therapy Leads to Rapid Resolution of Thrombocytopenia in
Hindawi Publishing Corporation Advances in Hematology Volume 214, Article ID 295323, 7 pages http://dx.doi.org/1.1155/214/295323 Clinical Study Therapy Leads to Rapid Resolution of Thrombocytopenia in
Case report 24 th Summer School of Internal Medicine 2015
 Case report 24 th Summer School of Internal Medicine 2015 Goldmannová D., Horák P., Skácelová M. IIIrd Internal Clinic - endocrinology, diabetology, rheumatology, nephrology University hospital Olomouc,
Case report 24 th Summer School of Internal Medicine 2015 Goldmannová D., Horák P., Skácelová M. IIIrd Internal Clinic - endocrinology, diabetology, rheumatology, nephrology University hospital Olomouc,
UNUSUAL PRESENTATIONS OF SYSTEMIC LUPUS ERYTHEMATOSUS
 UNUSUAL PRESENTATIONS OF SYSTEMIC LUPUS ERYTHEMATOSUS Presenter- Dr. Meghana B S Prof Dr. NAGARAJA B S Prof Dr. NIRMALA A C Dr. SIVARANJANI H Dr. B C PRAKASH Dr. MUMTAZ ALI KHAN A 60 year old lady, k/c/o
UNUSUAL PRESENTATIONS OF SYSTEMIC LUPUS ERYTHEMATOSUS Presenter- Dr. Meghana B S Prof Dr. NAGARAJA B S Prof Dr. NIRMALA A C Dr. SIVARANJANI H Dr. B C PRAKASH Dr. MUMTAZ ALI KHAN A 60 year old lady, k/c/o
A TRICKY PROBLEM. Presenter-Dr Lakshmi PK
 A TRICKY PROBLEM Presenter-Dr Lakshmi PK Patient particulars 33 years old Male Resident of Andhra Pradesh Occupation-soldier Chief compliants Headache- 03 days Headache-global,throbbing type Associated
A TRICKY PROBLEM Presenter-Dr Lakshmi PK Patient particulars 33 years old Male Resident of Andhra Pradesh Occupation-soldier Chief compliants Headache- 03 days Headache-global,throbbing type Associated
RaDaR Inclusion and Exclusion Criteria. Diagnosis Inclusion Criteria Exclusion Criteria. Alport Syndrome definite or probable
 Alport Syndrome and Type IV collagenopathies APRT Deficiency Alport Syndrome definite or probable Alport carrier definite or probable Thin basement membrane nephropathy APRT Deficiency confirmed Abolished
Alport Syndrome and Type IV collagenopathies APRT Deficiency Alport Syndrome definite or probable Alport carrier definite or probable Thin basement membrane nephropathy APRT Deficiency confirmed Abolished
BREAK 11:10-11:
 1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
TMA in HUS and TTP: new insights
 TMA in HUS and TTP: new insights Daan Dierickx University Hospitals Leuven, Department of Hematology, Belgium 20th Annual Meeting Belgian Society on Thrombosis and Haemostatis Antwerpen, 22 th November
TMA in HUS and TTP: new insights Daan Dierickx University Hospitals Leuven, Department of Hematology, Belgium 20th Annual Meeting Belgian Society on Thrombosis and Haemostatis Antwerpen, 22 th November
KIDNEY FAILURE. What causes kidney failure People who are most at risk for kidney failure usually have one or more of the following causes:
 KIDNEY FAILURE Your kidneys are a pair of organs located toward your lower back. One kidney is on each side of your spine. They filter your blood and remove toxins from your body. Your kidneys send toxins
KIDNEY FAILURE Your kidneys are a pair of organs located toward your lower back. One kidney is on each side of your spine. They filter your blood and remove toxins from your body. Your kidneys send toxins
Department of Clinical Haematology. Diagnosis and management of thrombotic thrombocytopenic purpura (TTP): Summary
: Summary") Diagnosis and management of thrombotic thrombocytopenic purpura (TTP): Summary Suspected TTP Investigations Further Investigations Blood Products URGENT treatment Suspect TTP if MAHA and thrombocytopenia
Diagnosis and management of thrombotic thrombocytopenic purpura (TTP): Summary Suspected TTP Investigations Further Investigations Blood Products URGENT treatment Suspect TTP if MAHA and thrombocytopenia
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT. J. H. Helderman,MD,FACP,FAST
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
Anemia (3).ms4.25.Oct.15 Hemolytic Anemia. Abdallah Abbadi
.ms4.25.Oct.15 Hemolytic Anemia. Abdallah Abbadi") Anemia (3).ms4.25.Oct.15 Hemolytic Anemia Abdallah Abbadi Case 3 24 yr old female presented with anemia syndrome and jaundice. She was found to have splenomegaly. Hb 8, wbc 12k, Plt 212k, retics 12%, LDH
Anemia (3).ms4.25.Oct.15 Hemolytic Anemia Abdallah Abbadi Case 3 24 yr old female presented with anemia syndrome and jaundice. She was found to have splenomegaly. Hb 8, wbc 12k, Plt 212k, retics 12%, LDH
INVESTIGATION OF ADVERSE TRANSFUSION REACTIONS TABLE OF RECOMMENDED TESTS. Type of Reaction Presentation Recommended Tests Follow-up Tests
 Minor Allergic (Urticarial) Urticaria, pruritis, flushing, rash If skin reaction only and mild hives/ rash
Minor Allergic (Urticarial) Urticaria, pruritis, flushing, rash If skin reaction only and mild hives/ rash
Risk factors of chronic renal failure after atypical Hemolytic Uremic Syndrome under plasmatherapy
 Risk factors of chronic renal failure after atypical Hemolytic Uremic Syndrome under plasmatherapy Professeur Eric Rondeau Urgences néphrologiques et Transplantation rénale Hôpital Tenon, Paris WWA SFH
Risk factors of chronic renal failure after atypical Hemolytic Uremic Syndrome under plasmatherapy Professeur Eric Rondeau Urgences néphrologiques et Transplantation rénale Hôpital Tenon, Paris WWA SFH
Dr. Rai Muhammad Asghar Associate Professor Head of Pediatric Department Rawalpindi Medical College
 Dr. Rai Muhammad Asghar Associate Professor Head of Pediatric Department Rawalpindi Medical College AN APPROACH TO BLEEDING DISORDERS NORMAL HEMOSTASIS After injury, 3 processes halt bleeding Vasoconstriction
Dr. Rai Muhammad Asghar Associate Professor Head of Pediatric Department Rawalpindi Medical College AN APPROACH TO BLEEDING DISORDERS NORMAL HEMOSTASIS After injury, 3 processes halt bleeding Vasoconstriction
THE KIDNEY AND SLE LUPUS NEPHRITIS
 THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
AUTOIMMUNE DISORDERS IN THE ACUTE SETTING
 AUTOIMMUNE DISORDERS IN THE ACUTE SETTING Diagnosis and Treatment Goals Aimee Borazanci, MD BNI Neuroimmunology Objectives Give an update on the causes for admission, clinical features, and outcomes of
AUTOIMMUNE DISORDERS IN THE ACUTE SETTING Diagnosis and Treatment Goals Aimee Borazanci, MD BNI Neuroimmunology Objectives Give an update on the causes for admission, clinical features, and outcomes of
Hemolytic Uremic Syndrome Epidemiological and Clinical Facts
 THE HEMOLYTIC IRAQI POSTGRADUATE UREMIC MEDICAL SYNDROME JOURNAL Hemolytic Uremic Syndrome Epidemiological and Clinical Facts Najla Ibrahiem Ayoub, Ahmed Hameed Mohammed, Jinan Soaod Orabi, Asaad Abdullah
THE HEMOLYTIC IRAQI POSTGRADUATE UREMIC MEDICAL SYNDROME JOURNAL Hemolytic Uremic Syndrome Epidemiological and Clinical Facts Najla Ibrahiem Ayoub, Ahmed Hameed Mohammed, Jinan Soaod Orabi, Asaad Abdullah
Definition : Stages : ( RIFLE vs. AKIN ) Causes and classification : Pre-renal Renal Post- renal Clinical manifestations and Complication Management
 Causes and classification : Pre-renal Renal Post- renal Clinical manifestations and Complication Management") AKI Definition : Stages : ( RIFLE vs. AKIN ) Causes and classification : Pre-renal Renal Post- renal Clinical manifestations and Complication Management and indications for RRT Etiology prerenal causes
AKI Definition : Stages : ( RIFLE vs. AKIN ) Causes and classification : Pre-renal Renal Post- renal Clinical manifestations and Complication Management and indications for RRT Etiology prerenal causes
Pediatric GU Dysfunction
 Pediatric GU Dysfunction Assessment of pediatric renal function Signs and symptoms Laboratory tests Radiological tests Nursing considerations Psychosocial and developmental considerations GU Disorders
Pediatric GU Dysfunction Assessment of pediatric renal function Signs and symptoms Laboratory tests Radiological tests Nursing considerations Psychosocial and developmental considerations GU Disorders
Transfusion Challenges. - Transfusion Reactions - Do they need platelets? Dr. Eoghan Molloy Haem SpR 2016
 Transfusion Challenges - Transfusion Reactions - Do they need platelets? Dr. Eoghan Molloy Haem SpR 2016 Guidance on Transfusion Hospital transfusion guidelines and procedures Irish Blood Transfusion Service
Transfusion Challenges - Transfusion Reactions - Do they need platelets? Dr. Eoghan Molloy Haem SpR 2016 Guidance on Transfusion Hospital transfusion guidelines and procedures Irish Blood Transfusion Service
Specialised Services Policy: CP98 Eculizumab for Atypical Haemolytic Uraemic Syndrome (ahus)
") Specialised Services Policy: CP98 Eculizumab for Atypical Haemolytic Uraemic Syndrome (ahus) Document Author: Assistant Director for Evidence, Evaluation and Effectiveness Executive Lead: Medical Director
Specialised Services Policy: CP98 Eculizumab for Atypical Haemolytic Uraemic Syndrome (ahus) Document Author: Assistant Director for Evidence, Evaluation and Effectiveness Executive Lead: Medical Director
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT
 PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
BBTS Advanced Clinical and laboratory case studies. Therese Callaghan
 BBTS 2017 Advanced Clinical and laboratory case studies Therese Callaghan Disclaimer Nothing to disclose A 52 year old man with history of paranoid schizophrenia presents to A&E with history of abdominal
BBTS 2017 Advanced Clinical and laboratory case studies Therese Callaghan Disclaimer Nothing to disclose A 52 year old man with history of paranoid schizophrenia presents to A&E with history of abdominal
ACUTE KIDNEY INJURY A PRIMER FOR PRIMARY CARE PHYSICIANS. Myriam Farah, MD, FRCPC
 ACUTE KIDNEY INJURY A PRIMER FOR PRIMARY CARE PHYSICIANS Myriam Farah, MD, FRCPC Clinical Assistant Professor Division of Nephrology, University of British Columbia November 2016 1. How to recognize acute
ACUTE KIDNEY INJURY A PRIMER FOR PRIMARY CARE PHYSICIANS Myriam Farah, MD, FRCPC Clinical Assistant Professor Division of Nephrology, University of British Columbia November 2016 1. How to recognize acute
CRRT Fundamentals Pre- and Post- Test. AKI & CRRT Conference 2018
 CRRT Fundamentals Pre- and Post- Test AKI & CRRT Conference 2018 Question 1 Which ONE of the following statements regarding solute clearance in CRRT is MOST correct? A. Convective and diffusive solute
CRRT Fundamentals Pre- and Post- Test AKI & CRRT Conference 2018 Question 1 Which ONE of the following statements regarding solute clearance in CRRT is MOST correct? A. Convective and diffusive solute
Thrombotic Thrombocytopenic
 The Treatment of TTP and the Prevention of Relapses GERALD APPEL, MD Professor of Clinical Medicine Columbia University College of Physicians and Surgeons NY-Presbyterian Hospital New York, New York Thrombotic
The Treatment of TTP and the Prevention of Relapses GERALD APPEL, MD Professor of Clinical Medicine Columbia University College of Physicians and Surgeons NY-Presbyterian Hospital New York, New York Thrombotic
Anemia (3).ms Hemolytic Anemia. Abdallah Abbadi Feras Fararjeh
.ms Hemolytic Anemia. Abdallah Abbadi Feras Fararjeh") Anemia (3).ms4.26.2.18 Hemolytic Anemia Abdallah Abbadi Feras Fararjeh Case 3 24 yr old female presented with anemia syndrome and jaundice. She was found to have splenomegaly. Hb 8, wbc 12k, Plt 212k,
Anemia (3).ms4.26.2.18 Hemolytic Anemia Abdallah Abbadi Feras Fararjeh Case 3 24 yr old female presented with anemia syndrome and jaundice. She was found to have splenomegaly. Hb 8, wbc 12k, Plt 212k,
Diabetes, Obesity and Heavy Proteinuria
 Diabetes, Obesity and Heavy Proteinuria Clinical Case 41 yo Black woman with heavy proteinuria History 2014: noted to have proteinuria on routine lab testing (1.1g/g). 1+ edema. Blood pressure has been
Diabetes, Obesity and Heavy Proteinuria Clinical Case 41 yo Black woman with heavy proteinuria History 2014: noted to have proteinuria on routine lab testing (1.1g/g). 1+ edema. Blood pressure has been
Management of Rejection
 Management of Rejection I have no disclosures Disclosures (relevant or otherwise) Deborah B Adey, MD Professor of Medicine University of California, San Francisco Kidney and Pancreas Transplant Center
Management of Rejection I have no disclosures Disclosures (relevant or otherwise) Deborah B Adey, MD Professor of Medicine University of California, San Francisco Kidney and Pancreas Transplant Center
Renal Disease. Please refer to the assignment page Three online modules TBLs
 Renal Disease Please refer to the assignment page Three online modules TBLs 1 Renal Embryology 2 Lab Tests UA CBC Enzymes Creatinine Creatinine clearance Ammonia Abs C Bx 3 BUN Creatinine Creatinine Clearance
Renal Disease Please refer to the assignment page Three online modules TBLs 1 Renal Embryology 2 Lab Tests UA CBC Enzymes Creatinine Creatinine clearance Ammonia Abs C Bx 3 BUN Creatinine Creatinine Clearance
DIABETES MELLITUS. Kidney in systemic diseases. Slower the progression: Pathology: Patients with diabetes mellitus are prone to other renal diseases:
 Kidney in systemic diseases Dr. Badri Paudel The kidneys may be directly involved in a number of multisystem diseases or secondarily affected by diseases of other organs. Involvement may be at a prerenal,
Kidney in systemic diseases Dr. Badri Paudel The kidneys may be directly involved in a number of multisystem diseases or secondarily affected by diseases of other organs. Involvement may be at a prerenal,
Paolo Gresele Dipartimento di Medicina, Sezione di Medicina Interna e Cardiovascolare, Università di Perugia
 Le sindromi trombotiche microangiopatiche: il ruolo del laboratorio Paolo Gresele Dipartimento di Medicina, Sezione di Medicina Interna e Cardiovascolare, Università di Perugia Microangiopatie trombotiche:
Le sindromi trombotiche microangiopatiche: il ruolo del laboratorio Paolo Gresele Dipartimento di Medicina, Sezione di Medicina Interna e Cardiovascolare, Università di Perugia Microangiopatie trombotiche:
Guideline on the clinical management of Henoch Schonlein Purpura (HSP)
") Guideline on the clinical management of Henoch Schonlein Purpura (HSP) Purpose To ensure a standardised approach in the management of children with HSP in southern Derbyshire. Scope The scope of this guideline
Guideline on the clinical management of Henoch Schonlein Purpura (HSP) Purpose To ensure a standardised approach in the management of children with HSP in southern Derbyshire. Scope The scope of this guideline
CRRT Fundamentals Pre- and Post- Test Answers. AKI & CRRT 2017 Practice Based Learning in CRRT
 CRRT Fundamentals Pre- and Post- Test Answers AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling
CRRT Fundamentals Pre- and Post- Test Answers AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling
New insights in thrombotic microangiopathies : TTP and ahus
 New insights in thrombotic microangiopathies : TTP and ahus Dr Catherine LAMBERT Hematology Cliniques universitaires Saint-Luc Catherine.lambert@uclouvain.be New insights in thrombotic microangiopathies
New insights in thrombotic microangiopathies : TTP and ahus Dr Catherine LAMBERT Hematology Cliniques universitaires Saint-Luc Catherine.lambert@uclouvain.be New insights in thrombotic microangiopathies
Systemic examination
 PROLONGED FEVER IN AN ADOLESCENT BOY Dr.Praveena Lionel, DNB PG, Dr.Kannan (HOD) Railway Hospital, Perambur History 11 yrs old adolescent boy was admitted with c/o Fever -1 wk Myalgia -1 wk Arthralgia
PROLONGED FEVER IN AN ADOLESCENT BOY Dr.Praveena Lionel, DNB PG, Dr.Kannan (HOD) Railway Hospital, Perambur History 11 yrs old adolescent boy was admitted with c/o Fever -1 wk Myalgia -1 wk Arthralgia
Most Common Hemostasis Consults: Thrombocytopenia
 Most Common Hemostasis Consults: Thrombocytopenia Cindy Neunert, MS MSCS Assistant Professor, Pediatrics CUMC Columbia University TSHNA Meeting, April 15, 2016 Financial Disclosures No relevant financial
Most Common Hemostasis Consults: Thrombocytopenia Cindy Neunert, MS MSCS Assistant Professor, Pediatrics CUMC Columbia University TSHNA Meeting, April 15, 2016 Financial Disclosures No relevant financial
Thrombotic microangiopathies and antineoplastic agents
 Thrombotic microangiopathies and antineoplastic agents Paul Coppo paul.coppo@aphp.fr Service d Hématologie - Hôpital Saint-Antoine AP-HP et Université Pierre & Marie Curie Centre de Référence des Microangiopathies
Thrombotic microangiopathies and antineoplastic agents Paul Coppo paul.coppo@aphp.fr Service d Hématologie - Hôpital Saint-Antoine AP-HP et Université Pierre & Marie Curie Centre de Référence des Microangiopathies
Assessing thrombocytopenia in the intensive care unit: The past, present, and future
 Assessing thrombocytopenia in the intensive care unit: The past, present, and future Ryan Zarychanski MD MSc FRCPC Sections of Critical Care and of Hematology, University of Manitoba Disclosures FINANCIAL
Assessing thrombocytopenia in the intensive care unit: The past, present, and future Ryan Zarychanski MD MSc FRCPC Sections of Critical Care and of Hematology, University of Manitoba Disclosures FINANCIAL
Nephrology. 3 rd Year Revision Session 06/05/17 Cathal Hannan
 Nephrology 3 rd Year Revision Session 06/05/17 Cathal Hannan Aims Acute Kidney Injury-recognition and management Sample OSCE Station Clinically relevant renal physiology Aetiology of Chronic Kidney Disease
Nephrology 3 rd Year Revision Session 06/05/17 Cathal Hannan Aims Acute Kidney Injury-recognition and management Sample OSCE Station Clinically relevant renal physiology Aetiology of Chronic Kidney Disease
Cytopaenias in HIV. Dr Maresce Bizaare Specialist Physician Clinical Haematology Fellow IALCH
 Cytopaenias in HIV Dr Maresce Bizaare Specialist Physician Clinical Haematology Fellow IALCH Introduction Cytopaenias in HIV are common Anaemias multifactorial causes Thrombocytopaenias may be the first
Cytopaenias in HIV Dr Maresce Bizaare Specialist Physician Clinical Haematology Fellow IALCH Introduction Cytopaenias in HIV are common Anaemias multifactorial causes Thrombocytopaenias may be the first
A 36 year old previously healthy female develops fever and ruising
 Renal vascular diseases CPC G.A. Appel MD M.B. Stokes MD Case 1 A 36 year old previously healthy female develops fever and bruising. She goes to her LMD and CBC shows plats 15 K, Hct 28%, normal PT and
Renal vascular diseases CPC G.A. Appel MD M.B. Stokes MD Case 1 A 36 year old previously healthy female develops fever and bruising. She goes to her LMD and CBC shows plats 15 K, Hct 28%, normal PT and
LAMA SHATAT TTP, ITP, DIC
 TTP, ITP, DIC Reduction in platelet number (thrombocytopenia) constitutes an important cause of generalized bleeding. A count less than 100,000 platelets/μl is generally considered to constitute thrombocytopenia.
TTP, ITP, DIC Reduction in platelet number (thrombocytopenia) constitutes an important cause of generalized bleeding. A count less than 100,000 platelets/μl is generally considered to constitute thrombocytopenia.
Thrombotic Microangiopathy secondary to Malignant Hypertension presenting as acute Kidney injury-a Case Report
 ISSN: 2319-7706 Volume 4 Number 12 (2015) pp. 640-644 http://www.ijcmas.com Case Study Thrombotic Microangiopathy secondary to Malignant Hypertension presenting as acute Kidney injury-a Case Report Sandeep
ISSN: 2319-7706 Volume 4 Number 12 (2015) pp. 640-644 http://www.ijcmas.com Case Study Thrombotic Microangiopathy secondary to Malignant Hypertension presenting as acute Kidney injury-a Case Report Sandeep
Clinical & Laboratory Assessment
 Clinical & Laboratory Assessment Dr Roger Pool NHLS & University of Pretoria Clinical Assessment (History) Anaemia ( haemoglobin) Dyspnoea (shortness of breath) Tiredness Angina Headache Clinical Assessment
Clinical & Laboratory Assessment Dr Roger Pool NHLS & University of Pretoria Clinical Assessment (History) Anaemia ( haemoglobin) Dyspnoea (shortness of breath) Tiredness Angina Headache Clinical Assessment
HUS and TTP Testing. Kenneth D. Friedman, M.D. Director, Hemostasis Reference Lab BloodCenter of Wisconsin, Milwaukee WI
 HUS and TTP Testing Kenneth D. Friedman, M.D. Director, Hemostasis Reference Lab BloodCenter of Wisconsin, Milwaukee WI Disclosures Relevant Financial Relationships Consultant: Ablynx, Bayer, CSL Behring,
HUS and TTP Testing Kenneth D. Friedman, M.D. Director, Hemostasis Reference Lab BloodCenter of Wisconsin, Milwaukee WI Disclosures Relevant Financial Relationships Consultant: Ablynx, Bayer, CSL Behring,
Effective Date: Approved by: Laboratory Director, Jerry Barker (electronic signature)
") 1 of 5 Policy #: 702 (PHL-702-05) Effective Date: 9/30/2004 Reviewed Date: 8/1/2016 Subject: TRANSFUSION GUIDELINES Approved by: Laboratory Director, Jerry Barker (electronic signature) Approved by: Laboratory
1 of 5 Policy #: 702 (PHL-702-05) Effective Date: 9/30/2004 Reviewed Date: 8/1/2016 Subject: TRANSFUSION GUIDELINES Approved by: Laboratory Director, Jerry Barker (electronic signature) Approved by: Laboratory
Microangiopatia trombotica (MAT) e Sindrome emolitico-uremica atipica (SEUa): Basi patogenetiche, inquadramento diagnostico e principi del
 e Sindrome emolitico-uremica atipica (SEUa): Basi patogenetiche, inquadramento diagnostico e principi del") Microangiopatia trombotica (MAT) e Sindrome emolitico-uremica atipica (SEUa): Basi patogenetiche, inquadramento diagnostico e principi del trattamento Vincenzo Montinaro U.O. Nefrologia Azienda Ospedaliera
Microangiopatia trombotica (MAT) e Sindrome emolitico-uremica atipica (SEUa): Basi patogenetiche, inquadramento diagnostico e principi del trattamento Vincenzo Montinaro U.O. Nefrologia Azienda Ospedaliera
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abdominal tumors, in children, 530 531 Alkalinization, in tumor lysis syndrome, 516 Allopurinol, in tumor lysis syndrome, 515 Anaphylaxis, drug
Note: Page numbers of article titles are in boldface type. A Abdominal tumors, in children, 530 531 Alkalinization, in tumor lysis syndrome, 516 Allopurinol, in tumor lysis syndrome, 515 Anaphylaxis, drug
There are two main causes of a low platelet count
 Thrombocytopenia Thrombocytopenia is a condition in which a person's blood has an unusually low level of platelets Platelets, also called thrombocytes, are found in a person's blood along with red blood
Thrombocytopenia Thrombocytopenia is a condition in which a person's blood has an unusually low level of platelets Platelets, also called thrombocytes, are found in a person's blood along with red blood
Blood Transfusion Guidelines in Clinical Practice
 Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
ACUTE KIDNEY INJURY AND RENAL REPLACEMENT THERAPY IN CHILDREN. Bashir Admani KPA Precongress 24/4/2018
 ACUTE KIDNEY INJURY AND RENAL REPLACEMENT THERAPY IN CHILDREN Bashir Admani KPA Precongress 24/4/2018 Case presentation SP 11month old Presenting complaint: bloody diarrhea, lethargy On exam: dehydration,
ACUTE KIDNEY INJURY AND RENAL REPLACEMENT THERAPY IN CHILDREN Bashir Admani KPA Precongress 24/4/2018 Case presentation SP 11month old Presenting complaint: bloody diarrhea, lethargy On exam: dehydration,
4100: Cellular Therapy Essential Data Follow-Up Form
 4100: Cellular Therapy Essential Data Follow-Up Form Registry Use Only Sequence Number: Date Received: Key Fields CIBMTR Center Number: Event date: Visit: 100 day 6 months 1 year 2 years >2 years, Specify:
4100: Cellular Therapy Essential Data Follow-Up Form Registry Use Only Sequence Number: Date Received: Key Fields CIBMTR Center Number: Event date: Visit: 100 day 6 months 1 year 2 years >2 years, Specify:
THERAPEUTIC PLASMA EXCHANGE
 THERAPEUTIC PLASMA EXCHANGE DIRECTORATE OF NEPHROLOGY AND TRANSPLANTATION Background and Indications Therapeutic plasma exchange (TPE) is an extracorporeal blood purification technique in which plasma
THERAPEUTIC PLASMA EXCHANGE DIRECTORATE OF NEPHROLOGY AND TRANSPLANTATION Background and Indications Therapeutic plasma exchange (TPE) is an extracorporeal blood purification technique in which plasma
Case Studies. Scleroderma Renal Crisis or Thrombotic Thrombocytopenic Purpura: Seeing Through the Masquerade. Patient 1
 Scleroderma Renal Crisis or Thrombotic Thrombocytopenic Purpura: Seeing Through the Masquerade Emily Keeler, DO, 1* Gloria Fioravanti, DO, FACP, 1 Bensson Samuel, MD, PG Dip, 1 Santo Longo, MD 2 Lab Med
Scleroderma Renal Crisis or Thrombotic Thrombocytopenic Purpura: Seeing Through the Masquerade Emily Keeler, DO, 1* Gloria Fioravanti, DO, FACP, 1 Bensson Samuel, MD, PG Dip, 1 Santo Longo, MD 2 Lab Med
Coagulation Disorders. Dr. Muhammad Shamim Assistant Professor, BMU
 Coagulation Disorders Dr. Muhammad Shamim Assistant Professor, BMU 1 Introduction Local Vs. General Hematoma & Joint bleed Coagulation Skin/Mucosal Petechiae & Purpura PLT wound / surgical bleeding Immediate
Coagulation Disorders Dr. Muhammad Shamim Assistant Professor, BMU 1 Introduction Local Vs. General Hematoma & Joint bleed Coagulation Skin/Mucosal Petechiae & Purpura PLT wound / surgical bleeding Immediate
Discussion. Case conference. Anemia. The basic evaluation of a patient newly diagnosed with anemia. Speaker : R2 趙劭倫 Supervisor : VS 林立偉
 Case conference Discussion Speaker : R2 趙劭倫 Supervisor : VS 林立偉 990123 The basic evaluation of a patient newly diagnosed with anemia Anemia CBC Reticulocyte count : reflects activity in the bone marrow
Case conference Discussion Speaker : R2 趙劭倫 Supervisor : VS 林立偉 990123 The basic evaluation of a patient newly diagnosed with anemia Anemia CBC Reticulocyte count : reflects activity in the bone marrow
A RARE NEUROLOGICAL PRESENTATION OF SLE. Dr Yoganand M N Dr Prithvi P Nayak
 A RARE NEUROLOGICAL PRESENTATION OF SLE Dr Jayachandra Dr Yoganand M N Dr Prithvi P Nayak Presenter: Dr Shambhavi K R CHIEF COMPLAINTS A 30 year old lady hailing from Nepal presented to OPD with complaints
A RARE NEUROLOGICAL PRESENTATION OF SLE Dr Jayachandra Dr Yoganand M N Dr Prithvi P Nayak Presenter: Dr Shambhavi K R CHIEF COMPLAINTS A 30 year old lady hailing from Nepal presented to OPD with complaints
Disclaimer. This is a broad survey and cannot cover all differential diagnoses or each condition in thorough detail
 Objectives Pediatric Infections: Differentiating Benign from Serious Eileen Klein, MD, MPH Rashes Infectious vs non-infectious Viral vs bacterial Respiratory and GI illnesses When do you treat When do
Objectives Pediatric Infections: Differentiating Benign from Serious Eileen Klein, MD, MPH Rashes Infectious vs non-infectious Viral vs bacterial Respiratory and GI illnesses When do you treat When do