Diabetes is a chronic disease of impaired glucose intolerance caused by absolute or relative insulin deficiency.
|
|
|
- Georgiana Rose
- 5 years ago
- Views:
Transcription
1 June 2015
2 Diabetes is a chronic disease of impaired glucose intolerance caused by absolute or relative insulin deficiency.
3 Types of Diabetes Type 1 Type 2 Gestational
4 Diabetes and Pregnancy 0.3% of pregnancies involve women with preexisting diabetes Gestational diabetes occurs in 1-14% of pregnant women. Gestational diabetes is glucose intolerance of variable severity, with onset or first recognition during the current pregnancy
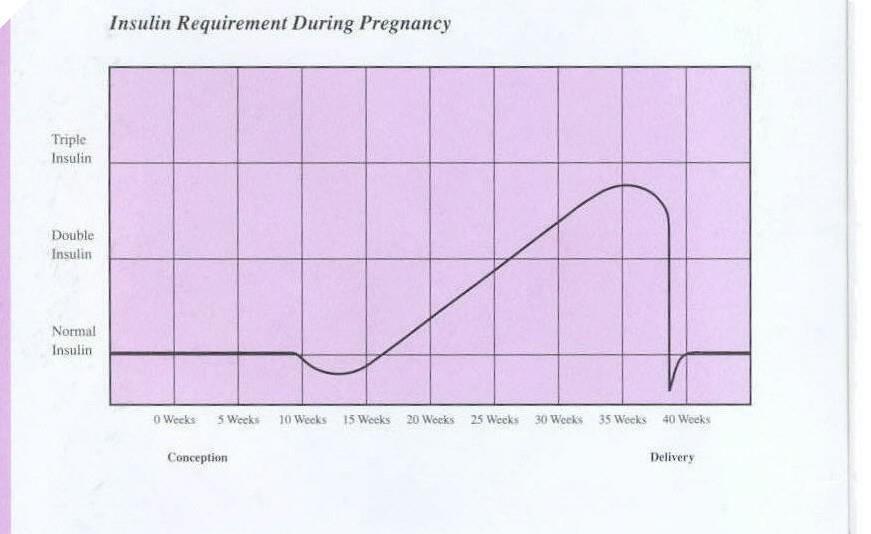
5 Normal Metabolic Changes in Pregnancy Fasting hypoglycemia (55-65 mg/dl) Postprandial hyperglycemia (enhances delivery of glucose to fetus and promotes fetal growth) Insulin resistance Hyperinsulinemia
6
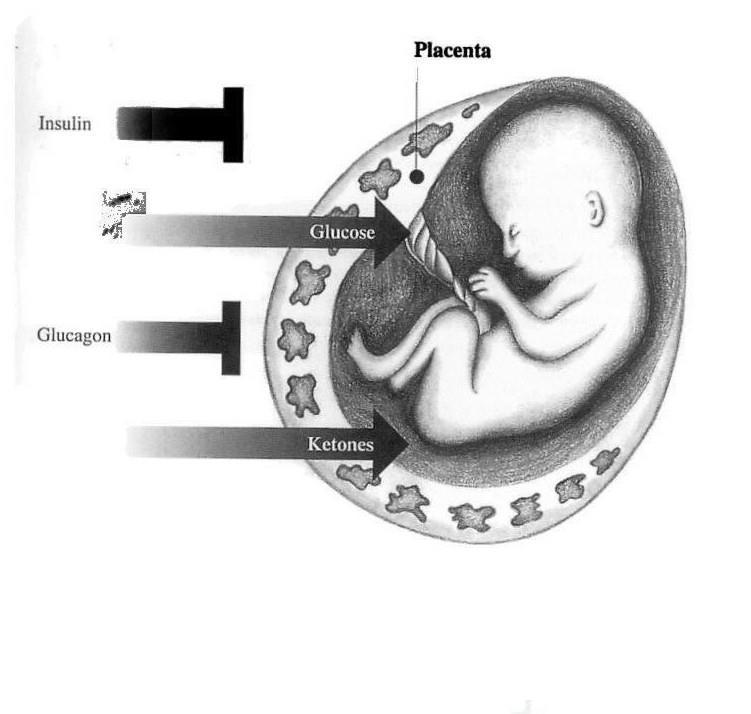
7 Diabetes & Pregnancy Glucose and ketones cross the placenta Insulin does not cross the placenta Ketones may be dangerous to the fetal nervous system and/or may signal maternal DKA
8
9 Gestational Diabetes
10 Gestational Diabetes Elevated glucoses during pregnancy that usually return to normal after delivery Caused by the placental hormone (Human Placental Lactogen) working against maternal insulin
11 GDM Risk Factors Over age 25 Family history of diabetes Overweight Personal history of gestational diabetes Previous large birthweight baby (>9#) or stillbirth PCOS African American, Hispanic, Asian or Native American
12 Diagnosis of Gestational Diabetes Risk assessment at first prenatal visit Screen in first trimester or at first prenatal visit if high risk: Personal history of GDM Marked obesity Glycosuria Strong family history of DM Previous large baby (>9#) Prior stillbirth If first trimester result is normal, rescreen at weeks
13 Diagnosis of Gestational Diabetes Screen avg risk women at weeks with 1-hour 50-gram GTT (older guidelines) ADA no glucose testing if low risk < 25 years old Normal weight before pregnancy Not in high risk ethnic group No family history of DM in first-degree relatives No history of abnormal GTT No history of poor OB outcome We recommend screening EVERYONE
14 Diagnosis of Gestational Diabetes If 1-hour GTT is > 140 mg/dl, do 3-hour 100-gram GTT Threshold >140 mg/dl identifies 80% of women with GDM Threshold >130 mg/dl identifies 90% of women with GDM
15 Diagnosis of Gestational Diabetes 3-hour GTT diagnostic criteria 2 or more values must be met or exceeded for diagnosis of GDM FBS 95 mg/dl 1-hour 180 mg/dl 2-hour 155 mg/dl 3-hour 140 mg/dl (Carpenter and Coustan)
16 If 3-hour GTT results reveal only one abnormal value, manage patient with: Meal plan Exercise Management of One Abnormal Value Then retest at weeks
17 Current GDM Diagnostic Criteria Established >40 years ago Chosen to identify women at high risk for development of diabetes after pregnancy Derived from criteria for non-pregnant adults Not designed to identify pregnancies with increased risk for adverse perinatal outcome Not based on research of outcomes for fetus/neonate/child Different standards in U.S. and rest of world Yet. we ve always done it that way, so we continue to use them.
18 New Recommendations for GDM Diagnosis First prenatal visit Measure FPG, HbA1c or random glucose on high-risk women If results indicate overt diabetes, treat as preexisting diabetes If results not diagnostic for overt diabetes FPG >92 but <126, diagnose as GDM FPG <92, test for GDM at weeks with 75-gram OGTT
19 New GDM Diagnostic Criteria 2-hour GTT Recommended by American Diabetes Association in 2010 Still not approved by ACOG Avera McKennan implemented in gram glucola 1 value met or exceeded to make GDM diagnosis FBS 1-hour 2-hour 92 mg/dl 180 mg/dl 153 mg/dl
20 Implications of New GDM Diagnostic Criteria More women will be dx with GDM, perhaps 2-3x more With current U.S. guidelines, 5-8% of women dx with GDM In HAPO trial, 16% of women met at least one of dx criteria New criteria reflect risk of perinatal harm, not mother s future risk of DM, so should lead to better neonatal outcomes Cost of screening & care

21 Treatment Goals for GDM Minimize fetal hyperinsulinemia Minimize maternal and fetal complications Baby <90 th percentile for gestational age
22 Goals for Glucose Control Gestational Diabetes Fasting 1-hour PP 2-hour PP mg/dl < 140 mg/dl <120 mg/dl Fasting glucose >105 mg/dl assoc with increased risk of intrauterine death during last 4-8 weeks gestation
23 Maternal Complications with GDM Polyhydramnios Preterm labor Infections vaginal, bladder & kidney Increased risk for type 2 diabetes (up to 60%)
24 Fetal Complications with GDM Macrosomia or IUGR Delayed lung maturation Labor and delivery trauma Hypoglycemia Hyperbilirubinemia Polycythemia Hypocalcemia Stillbirth

25 Complications for Children of Women with GDM Increased risk of Obesity Glucose intolerance Diabetes All can occur in late adolescence and young adulthood

26 Gestational Diabetes Education Obtain results of GTT from MD/CNM & review with patient If using 2 step method and 1-hour is significantly elevated, 3-hour may be deferred Consider HbA1c to determine if GDM vs. preexisting DM if 1-hour markedly high

27 Gestational Diabetes Education VISIT 1 Inform/reassure Baby will not be born with diabetes No increased risk for birth defects Nothing mother did to cause GDM Increased risk for type 2 diabetes later in life Good control is essential for a healthy outcome!
28 Gestational Diabetes Education VISIT 1 Initial education Explanation of GDM GDM risk factors Fetal complications of hyperglycemia Maternal complications of hyperglycemia Goal glucose range Importance of working with healthcare team to achieve a healthy outcome
29 Gestational Diabetes Education VISIT 1 Treatment regimen Healthy eating Exercise Glucose monitoring (QID fasting and 1-hour postprandial) Ketone testing (first thing daily) Insulin/oral agent if needed Fetal movement counting (daily)
30 Nutritional Management of Gestational Diabetes Refer to RD experienced in GDM 3 meals/3 snacks daily HS snack EVERY night Avoid juice and cereal for breakfast Limit sugar intake Focus on healthy nutrition for mom and baby Check urine ketones to assess adequacy of HS snack & total daily carb intake

31 Gestational Diabetes Education VISIT 2 Review glucoses, ketones and food records Check meter memory Schedule third visit if glucoses not in goal range after changes made in meal plan/exercise Ongoing care plan Weekly contact with Diabetes & Pregnancy Team or MD FP/OB/CNM/Perinatologist visits as directed Return for further education if insulin needed
32 Medications for Glucose Control Glyburide Stimulates pancreatic insulin secretion Several clinical studies have shown it to be safe and effective during pregnancy Does not cross the placenta Starting dose 2.5 mg daily to BID If insulin sensitive, consider 1.25 mg daily Increase in 2.5 mg increments; max dose = 20 mg daily

33 Medications for Glucose Control Insulin therapy Tailor regimen to glucose pattern Elevated FBS NPH at HS Elevated post-breakfast AM Humalog/NovoLog Elevated post-noon AM NPH Elevated post-supper PM Humalog/NovoLog All elevated NPH with Humalog/NovoLog BID Instruct on insulin administration and hypoglycemia symptoms and treatment
34 Pre-Existing Diabetes and Pregnancy




35 Pre-Pregnancy Counseling Should include all women of childbearing age Begin at the onset of puberty Divide women into two categories Planning pregnancy in next year Desire to delay/prevent pregnancy Unplanned pregnancies occur in 2/3 of women with diabetes
36 Pre-Pregnancy Counseling Optimal glucose control pre-conception HbA1c normal or < 1% above normal for 3-6 months before conception Obtain lowest HbA1c possible without undue risk of maternal hypoglycemia (ADA) Pre-meal glucoses mg/dl 1-hour PP glucoses < 140 mg/dl
37 Pre-Pregnancy Counseling Education Risk and prevention of congenital anomalies Two- to fivefold increased risk of baby with congenital anomaly Organogenesis complete by 8 weeks gestation Chronic complications can worsen with pregnancy Financial realities Personal commitment and motivation Review all aspects of diabetes self-management Early prenatal care
38 Treatment Goals for Pre-Existing Diabetes Minimize fetal hyperinsulinemia Prevent congenital anomalies Prompt detection of maternal complications Baby < 90 th percentile for gestational age
39 Maternal Complications with Preexisting Diabetes: Hypoglycemia Ketoacidosis Infections Polyhydramnios Preterm labor Hypertension Worsening of chronic complications Labor and delivery trauma
40 Maternal Chronic Complications with Pre-Existing Diabetes: Retinopathy Nephropathy Neuropathy Large vessel disease
41 Fetal Complications with Pre-Existing Diabetes Spontaneous abortion (30-60%) Related to degree of hyperglycemia at conception Congenital anomalies (6-12%) Cardiac Neural tube Skeletal Hyperbilirubinemia Hypocalcemia Polycythemia
42 Fetal Complications with Pre-Existing Diabetes Hypoglycemia Hypomagnesemia IUGR Macrosomia RDS Birth injury Stillbirth
43 Goals for Glucose Control Pre-existing Diabetes & Pregnancy Fasting Premeal 1-hour PP 2-hour PP mg/dl mg/dl < 140 mg/dl <120 mg/dl Fasting glucose >105 mg/dl assoc with increased risk of intrauterine death during last 4-8 weeks gestation
44 Pre-Existing Diabetes and Pregnancy Management Physical exam and Lab Blood pressure Dilated retinal exam Cardiovascular exam for cardiac or peripheral vascular disease HbA1c 24-hour urine for total protein and creatinine clearance Thyroid panel if type 1
45 Insulin for all type 1 and type 2 patients At least BID NPH with Humalog/NovoLog Consider Humalog/NovoLog TID and Levemir at HS for type 1 Levemir is now Pregnancy Category B Lantus is Pregnancy Category C Insulin pump follow closely by endocrinologist or perinatologist Oral agent Glyburide has been used safely and effectively in one study for type 2 DM Pre-Existing Diabetes and Pregnancy Management
 Sick")
46 Pre-Existing Diabetes and Pregnancy Education VISIT 1 Assess current knowledge, skills and practices Meal plan Exercise Insulin administration Glucose monitoring knowledge Urine ketone testing Hypoglycemia symptoms and treatment (milk is preferred treatment) Sick day management

47 Pre-Existing Diabetes and Pregnancy Education VISIT 1 Instruct on/review key topics as needed Diabetes and pregnancy Rationale for optimal control Potential maternal and fetal complications of hyperglycemia Glucose monitoring regimen Goal glucose ranges Medication regimen
48 Pre-Existing Diabetes and Pregnancy Education VISIT 1 Metabolic changes during pregnancy 1 st trimester Morning sickness Decreased or same insulin requirements 2 nd trimester Appetite increases Increased insulin requirements 3 rd trimester Increased insulin requirements until last few weeks
49 Pre-Existing Diabetes and Pregnancy Education VISIT 2 Review glucoses, ketones and food records Check meter memory Additional education as needed Ongoing care plan Weekly contact with Diabetes & Pregnancy Team or MD Ongoing insulin adjustment may require 2-3 times as much insulin as in non-pregnant state Fetal movement counting daily starting at 28 weeks FP/OB/Perinatologist visits as directed
50 Pre-Existing Diabetes and Pregnancy Monitoring Glucose testing at least QID FBS and 1-hour or 2-hour PP MD may want pre-prandial tests as well May need check to assess for nocturnal hypoglycemia Ketone testing with first AM void and if ill

51 Mom Type 1 x 8 years, induced at 39.0 wks, C/S for failure to progress/descend. Baby boy weighed 9# 0 oz., head 14 ½, chest 14. First BG via meter: 44 mg/dl. To NICU for IV.

52 Mom Type 1 x 11 years, induction of labor at 39.4 weeks. Vaginal birth, 1 st degree laceration. Baby girl, weight 7# 4 oz. First blood glucose via meter 79 mg/dl.
53 Standard of Care: Fetal Surveillance

54 Fetal Surveillance: Ultrasound First trimester 16 to 18 weeks 20 to 22 weeks Serial fetal evaluations Doppler flow studies
55 Fetal Movement Counting Initiate at ~ 28 wks gestation Fetus sensitive to O2 levels, assoc. w/ limb movement Perform approx. same time each day Record length of time to obtain ten kicks Call PCP if time lengthens considerably or has not obtained 10 kicks in 2 hours
56 Biophysical Profile (BPP) 28 weeks if insulin requiring, weeks if non-insulin requiring Variables Fetal tone, gross body movements, fetal breathing, AFV, NST

57 Scoring of BPP Scoring 2 points for each variable present, 0 if absent Score 8-10 assoc. w/good fetal outcome x 1 wk If 6, repeat or deliver
 CST, follow-up.")
58 Nonstress Test (NST) wks if insulin requiring, 36 wks if non-insulin requiring Sooner if other risk factors Interpretation: Reactive: 2 accels of 15x15 in 20 minutes Nonreactive: < 2 accels meeting criteria Reactive: weekly to 36 wks, then 2x wk If nonreactive, consider CST or BPP (-) CST, follow-up. (+) CST, amnio or deliver

59 Contraction Stress Test (CST) Also Oxytocin Challenge Test (OCT) IV pitocin per protocol until: 3 UC s of moderate intensity in 10 min. UC s last seconds Nipple stimulation occasionally used
60 CST Interpretation Negative - no late decels or significant variables Positive - late decels w/50% or > of UC s Equivocal-suspicious - intermittent late decels or significant variable decels Equivocal-hyperstimulatory - FHR decels w/uc s > than q. 2 min. or > 90 sec. Unsatisfactory - fewer than 3 UC s in 10 minutes or an uninterpretable tracing
61 Amniocentesis L/S ratio (lecithin/sphingomyelin) PG (phospholipid phosphatidylglycerol) Indicated if induction of labor prior to weeks gestation, poor dating, poor control Mature L/S ratio (2.0 or >) associated with 3% risk of RDS Presence of PG associated with RDS
62 Standard of Care: Intrapartal Management
63 Intrapartum Management Admission history Overall glucose control --- ask to see log book? Episodes of hypoglycemia, ketoacidosis What levels trigger hypoglycemia, S/S, treatment Vascular complications Fetal surveillance testing - U/S for fetal size, hydramnios? Last food intake, insulin dose
64 Intrapartum Management Non-Insulin Requiring If testing WNL, can often await spontaneous labor Blood glucose on admit and then as ordered (usually every 4-6 hours). Best practice is to use a hospital glucose meter or Lab glucose for all inpatient clinical decisions If necessary to use patient s personal meter, hospital should have a policy in place to validate the accuracy of the patient s meter
65 Intrapartum Management Non-Insulin Requiring Clear liquids in labor, IV fluids Fetal monitoring as non-diabetic May augment with pitocin, cytotec, cervidil Monitor for signs of CPD or shoulder dystocia (arrest of dilatation or arrest of descent) Monitor baby closely after birth for BG Jitteriness, irritability, lethargy, poor feedings, hypotonia, apnea, cyanosis, seizures
66 Intrapartum Management Insulin-Requiring With good control, no complications, reassuring AP testing, delivery can be planned at 39 weeks May need IV infusion w/glucose and an insulin drip Spontaneous labor: manage same as non diabetic Induction of labor: Diet and insulin as usual day before induction Withhold insulin and food day of induction IV with ~ 100cc/hr

67 Intrapartum Management Insulin-Requiring Examples of insulin protocols
68 Insulin & Glucose Requirements At onset of active labor, insulin and glucose requirements may vary 6-8 grams glucose needed/hour in labor D5 solutions, 20 ml = 1 gm ( ml/hr) D10 solutions, 10 ml = 1 gm (60-80 ml/hr) Glucose goals 70 to 110 mg/dl
69 Intrapartum Management Insulin-Requiring If glucose > defined threshhold (120), initiate insulin drip 250 ml NS with 250U Humulin Regular insulin Flush tubing with 25 ml insulin solution prior to infusion Begin at 1U/hr (1 ml/hr) per infusion pump or per orders or per protocol/orders to achieve glucose goals If patient is fed, adjust rate per physician order Notify MD/CNM if patient unable to eat or emesis Policy requires 2 RN s check IV insulin dose/rate upon initiation and any rate changes
70 Insulin-Requiring risk ketoacidosis (DKA) with use of tocolytics and/or steroids Observe closely, dip urine for ketones as ordered, anticipate need for increased insulin Glucose monitoring Unit meter (not patient s meter) Lab glucose if < 60 mg/dl or > 400 mg/dl Latent labor: every 2-4 hours as ordered. Active labor: hourly once insulin drip is initiated Check for urine ketones as ordered
71 Intrapartum Management Insulin-Requiring C/S Schedule early a.m. Diet and insulin as usual day before Withhold insulin and food day of surgery IV fluids - pre-surgery hydrate with LR to avoid hyperglycemia Regional anesthetic preferred
72 Maternal Assessments Hypoglycemia (jittery, / fine motor dexterity, slowed responses) Hyperglycemia (polyuria, polydipsia, polyphagia, weakness, vision changes) Continuous fetal monitoring - observe for signs of shoulder dystocia
73 At Delivery GDM and Type 2: Discontinue insulin infusion Type 1: Adjust or stop per physician order Obtain a maternal serum glucose and cord glucose (physician order)
74 Newborn Management Monitor for hypoglycemia (jittery, lethargy, poor feeding, irritability, hypotonia, apnea, cyanosis, seizures Symptomatic newborn Check immediately If < 40 transfer to NICU for IV glucose
75 Newborn Management If initial glucose is <30 mg/dl, draw serum glucose If serum glucose is < 25 mg/dl, IV glucose If mg.dl, IV glucose
76 Newborn Management Continue to feed infant every 2-3 hours Screen glucose prior to each feed unless: 3 consecutive levels > 45 mg/dl; then check every other feed for hours If glucose is mg/dl, feed and re-check in 1 hour (if monitor reads obtain serum plasma level) If serum plasma level is 0-35 mg/dl contact physician and plan for transfer NICU

77 Standard of Care: Postpartum Management

78 Postpartum Management Gestational Diabetes No insulin required Regular diet Blood glucose monitoring If diet controlled, no BG s If insulin required, delivery day & 1st PP day or as ordered
79 Postpartum Management Pre-Existing Diabetes Insulin requirements drop after delivery, may not need insulin for hrs BGM Immediately after delivery & q. 4 hrs When eating, begin a.m. fasting & ac or pc Begin insulin or oral agent when BG levels begin to rise (> 90 mg/dl fasting, >120 mg/dl at 2 hrs postprandial) Diet Healthy eating/constant carb (consult dietitian)
 Insulin requirements may because of milk")

80 Breastfeeding Calorie intake similar to pregnancy ( intake by 300 to 500 calories/day) Insulin requirements may because of milk production Monitor for signs of hypoglycemia, especially at night most likely within 60 min. of BF may need to adjust snacks may need to evening NPH
81 Breastfeeding & Oral Agents Glucotrol & Glyburide Not reviewed by AAP A group of 5 mothers who received daily doses of glyburide (5 mg) or glucotrol (immediate-release 5 mg), neither was detectable in milk. Infant plasma glucose levels were normal. Glimepiride (Amaryl) not reviewed by AAP No data available on transfer into human milk. However, rodent studies demonstrated significant transfer and elevated plasma levels in pups. Caution is urged if used in BF humans. Observe for hypoglycemia.
82 Breastfeeding & Oral Agents Glucophage (Metformin) not reviewed by AAP Study of 7 women taking median dose 1500 mg/dl, the absolute infant dose averaged 0.04 mg/kg/day and the mean relative infant dose was 0.28%. Metformin was present in very low or undetectable concentrations in the plasma of four of the infants studied. No health problems.
83 Postpartum F.U. for Women w/gdm Healthy diet Exercise S/S hyperglycemia If mom wants to check BGs, goal FBS < 90, 2 hr PP < 120 (testing generally not required) 6 week and annual FBS 2 hour GTT with 75 gram glucose load if planning future pregnancies, otherwise FBS only Fasting < 100 mg/dl = Normal = Pre-diabetes > 126 = Diabetes
 Contraceptive")
84 Postpartum Follow Up for Women with GDM (continued) Predisposition to HTN, obesity and type 2 diabetes (67%) S/S: polydipsia, polyuria, polyphagia, blurred vision, HA, drowsiness, nausea, hyperpnea Risk of GDM with future pregnancies (30-50% reoccurrence) Contraceptive options
85 GDM: Risk of Developing Type 2 DM If woman does NOT become fit & lean after pregnancy, risk of developing Type 2 DM is ~ 10% each year, cumulative In 5 years, your risk of Type 2 DM is 50% Then, lifetime risk caps at ~ 60% If able to become lean & fit after baby is born, lifetime risk is 25% Coustan, D., Carpenter, M., O Sullivan P., & Carr, S. (1993). Gestational diabetes mellitus. Predictors of subsequent disordered glucose metabolism. American Journal of Obstetrics & Gynecology, 168,
86 PP Follow Up: Pre-Existing DM Constant carbohydrate diet or carb:insulin ratio Exercise Routine monitoring of glucoses (FBS/premeal goal mg/dl; 2 hour post-prandial < 140 mg/dl) QD if diet controlled (rotating times) BID if taking oral diabetes agent (test before meals & HS) Rotate fasting/pre-supper, next day pre-lunch/hs Wait at least 2 hrs since snack before pre-meal testing Daily BGM if BG s okay after 1 week (rotate times) QID if on insulin


87 The ENDs! For more information, contact: Avera McKennan Diabetes Center at
88 References Kjos, S. (2013) Intrapartum and Postpartum Management of Insulin and Blood Glucose. UpToDate. American Acadamy of Pediatrics, The American College of Obstetricians and Gynecologists (2012). Guidelines for Perinatal Care, Seventh Edition.
Management of Pregestational and Gestational Diabetes Mellitus
 Background and Prevalence Management of Pregestational and Gestational Diabetes Mellitus Pregestational Diabetes - 8 million women in the US are affected, complicating 1% of all pregnancies. Type II is
Background and Prevalence Management of Pregestational and Gestational Diabetes Mellitus Pregestational Diabetes - 8 million women in the US are affected, complicating 1% of all pregnancies. Type II is
2/13/2018. Update on Gestational Diabetes. Disclosure. Objectives. I have no financial conflicts of interest.
 Update on Gestational Diabetes Lorie M. Harper, MD, MSCI Department of Obstetrics & Gynecology Division of Maternal-Fetal Medicine 2/18/2018 Disclosure I have no financial conflicts of interest. Objectives
Update on Gestational Diabetes Lorie M. Harper, MD, MSCI Department of Obstetrics & Gynecology Division of Maternal-Fetal Medicine 2/18/2018 Disclosure I have no financial conflicts of interest. Objectives
Gestational Diabetes. Gestational Diabetes:
 Gestational Diabetes Detection and Management Steven Gabbe, MD The Ohio State University Medical Center Gestational Diabetes: Detection and Management Learning Objectives: At the conclusion of this presentation,
Gestational Diabetes Detection and Management Steven Gabbe, MD The Ohio State University Medical Center Gestational Diabetes: Detection and Management Learning Objectives: At the conclusion of this presentation,
Gestational Diabetes Mellitus Dr. Fawaz Amin Saad
 Gestational Diabetes Mellitus Dr. Fawaz Amin Saad Senior Consultant OB/GYN, Al-Hayat Medical Center, Doha, Qatar DISCLOSURE OF CONFLICT OF INTEREST I am a full-time Employee at Al-Hayat Medical Center.
Gestational Diabetes Mellitus Dr. Fawaz Amin Saad Senior Consultant OB/GYN, Al-Hayat Medical Center, Doha, Qatar DISCLOSURE OF CONFLICT OF INTEREST I am a full-time Employee at Al-Hayat Medical Center.
Vishwanath Pattan Endocrinology Wyoming Medical Center
 Vishwanath Pattan Endocrinology Wyoming Medical Center Disclosure Holdings in Tandem Non for this Training Introduction In the United States, 5 to 6 percent of pregnancies almost 250,000 women are affected
Vishwanath Pattan Endocrinology Wyoming Medical Center Disclosure Holdings in Tandem Non for this Training Introduction In the United States, 5 to 6 percent of pregnancies almost 250,000 women are affected
Diabetes in Pregnancy
 Diabetes in Pregnancy Ebony Boyce Carter, MD, MPH Division of Maternal Fetal Medicine Washington University School of Medicine Disclosures I have no financial disclosures to report. Objectives Review the
Diabetes in Pregnancy Ebony Boyce Carter, MD, MPH Division of Maternal Fetal Medicine Washington University School of Medicine Disclosures I have no financial disclosures to report. Objectives Review the
Diabetes in Pregnancy. L.Sekhavat MD
 Diabetes in Pregnancy L.Sekhavat MD Diabetes in Pregnancy Gestational Diabetes Pre-gestational diabetes (overt) Insulin dependent (type1) Non-insulin dependent (type 2) Definition Gestational diabetes
Diabetes in Pregnancy L.Sekhavat MD Diabetes in Pregnancy Gestational Diabetes Pre-gestational diabetes (overt) Insulin dependent (type1) Non-insulin dependent (type 2) Definition Gestational diabetes
Gestational Diabetes. Benjamin Byers, D.O., FACOG Center for Maternal and Fetal Care Bryan Physician Network
 Gestational Diabetes Benjamin Byers, D.O., FACOG Center for Maternal and Fetal Care Bryan Physician Network Outline Definition Prevalence Risk factors complications Diagnosis Management Nonpharmacologic
Gestational Diabetes Benjamin Byers, D.O., FACOG Center for Maternal and Fetal Care Bryan Physician Network Outline Definition Prevalence Risk factors complications Diagnosis Management Nonpharmacologic
Diabetes in Pregnancy
 Diabetes in Pregnancy Susan Drummond RN MSN C-EFM Objectives 1. Describe types of diabetes and diagnosis of gestational diabetes 2. Identify a management plan for diabetes during pregnancy 3. Describe
Diabetes in Pregnancy Susan Drummond RN MSN C-EFM Objectives 1. Describe types of diabetes and diagnosis of gestational diabetes 2. Identify a management plan for diabetes during pregnancy 3. Describe
Current Trends in Diagnosis and Management of Gestational Diabetes
 Current Trends in Diagnosis and Management of Gestational Diabetes Shreela Mishra, MD Assistant Clinical Professor UCSF Fresno Medical Education Program 2/2/2019 Disclosures No disclosures 2/2/19 Objectives
Current Trends in Diagnosis and Management of Gestational Diabetes Shreela Mishra, MD Assistant Clinical Professor UCSF Fresno Medical Education Program 2/2/2019 Disclosures No disclosures 2/2/19 Objectives
Diabetes in Pregnancy
 Diabetes in Pregnancy Resident School November 5 2014 Goals Be able to screen for gestational and preexisting diabetes Be able to counsel women on the diagnosis of gestational diabetes Understand glucose
Diabetes in Pregnancy Resident School November 5 2014 Goals Be able to screen for gestational and preexisting diabetes Be able to counsel women on the diagnosis of gestational diabetes Understand glucose
Diabetes in Pregnancy
 Disclosure Diabetes in Pregnancy I have no conflicts of interest to disclose Jennifer Krupp, MD Maternal Fetal Medicine St. Marys Hospital/SSM Health Madison, WI Objectives Classification of Diabetes Classifications
Disclosure Diabetes in Pregnancy I have no conflicts of interest to disclose Jennifer Krupp, MD Maternal Fetal Medicine St. Marys Hospital/SSM Health Madison, WI Objectives Classification of Diabetes Classifications
2018 Standard of Medical Care Diabetes and Pregnancy
 2018 Standard of Medical Care Diabetes and Pregnancy 2018 Standard of Medical Care Diabetes and Pregnancy Marjorie Cypress does not have any relevant financial relationships with any commercial interests
2018 Standard of Medical Care Diabetes and Pregnancy 2018 Standard of Medical Care Diabetes and Pregnancy Marjorie Cypress does not have any relevant financial relationships with any commercial interests
APEC Guidelines Gestational Diabetes Mellitus
 Gestational diabetes mellitus (GDM) is defined as insulin resistance of variable severity with onset or first recognition during pregnancy. The prevalence of diabetes mellitus (DM) in the US is growing
Gestational diabetes mellitus (GDM) is defined as insulin resistance of variable severity with onset or first recognition during pregnancy. The prevalence of diabetes mellitus (DM) in the US is growing
Gestational Diabetes: An Update on Testing. Kimberlee A McKay, M.D. Avera Medical Group Ob/GYN
 Gestational Diabetes: An Update on Testing Kimberlee A McKay, M.D. Avera Medical Group Ob/GYN Gestational Diabetes Increased risks of: Still Birth Hydramnios Should Dystocia Prolonged Labor Preeclampsia
Gestational Diabetes: An Update on Testing Kimberlee A McKay, M.D. Avera Medical Group Ob/GYN Gestational Diabetes Increased risks of: Still Birth Hydramnios Should Dystocia Prolonged Labor Preeclampsia
CommUnityCare Women s Health Brackenridge Professional Office Building
 Guidelines for Diabetes in Pregnancy Effective Date 7/1/11 *This document does not define a standard of care, nor is it intended to dictate an exclusive course of management. There are other accepted strategies
Guidelines for Diabetes in Pregnancy Effective Date 7/1/11 *This document does not define a standard of care, nor is it intended to dictate an exclusive course of management. There are other accepted strategies
Pregnancy confers a state of insulin resistance and hyperinsulinemia that. Gestational Diabetes Mellitus MANAGEMENT REVIEW
 MANAGEMENT REVIEW Gestational Diabetes Mellitus Amanda Bird Hoffert Gilmartin, Serdar H. Ural, MD, John T. Repke, MD Division of Maternal Fetal Medicine, Department of Obstetrics and Gynecology, Penn State
MANAGEMENT REVIEW Gestational Diabetes Mellitus Amanda Bird Hoffert Gilmartin, Serdar H. Ural, MD, John T. Repke, MD Division of Maternal Fetal Medicine, Department of Obstetrics and Gynecology, Penn State
Objectives. Diabetes and Obesity in Pregnancy. In Diabetes. Diabetes in Pregnancy
 Objectives Diabetes and Obesity in Pregnancy. Health Impact for the mother and child Bresta Miranda, MD Assistant Professor of Clinical Medicine University of Miami, Miller School of Medicine Review physiologic
Objectives Diabetes and Obesity in Pregnancy. Health Impact for the mother and child Bresta Miranda, MD Assistant Professor of Clinical Medicine University of Miami, Miller School of Medicine Review physiologic
DIABETES AND PREGNANCY. CDE Exam Preparation March 22 & 27, 2018 Presented by Wendy Graham RD CDE Mentor
 DIABETES AND PREGNANCY CDE Exam Preparation March 22 & 27, 2018 Presented by Wendy Graham RD CDE Mentor OBJECTIVES Describe targets for blood glucose in pregnancy Discuss the risks to baby if blood glucose
DIABETES AND PREGNANCY CDE Exam Preparation March 22 & 27, 2018 Presented by Wendy Graham RD CDE Mentor OBJECTIVES Describe targets for blood glucose in pregnancy Discuss the risks to baby if blood glucose
Diabetes: The Effects of Maternal Diabetes on Fetal Development and Outcomes Sherrie McElvy, MD May 18, 2016
 Diabetes: The Effects of Maternal Diabetes on Fetal Development and Outcomes Sherrie McElvy, MD May 18, 2016 Medical Director Sweet Success Sutter Medical Center Sacramento Perinatal Associates of Sacramento
Diabetes: The Effects of Maternal Diabetes on Fetal Development and Outcomes Sherrie McElvy, MD May 18, 2016 Medical Director Sweet Success Sutter Medical Center Sacramento Perinatal Associates of Sacramento
Intrapartum and Postpartum Management of the Diabetic Mother and Infant
 Intrapartum and Postpartum Management of the Diabetic Mother and Infant Intrapartum Management Women with gestational diabetes who maintain normal glucose levels during pregnancy on diet and exercise therapy
Intrapartum and Postpartum Management of the Diabetic Mother and Infant Intrapartum Management Women with gestational diabetes who maintain normal glucose levels during pregnancy on diet and exercise therapy
The Ever-Changing Approaches to Diabetes in Pregnancy
 The Ever-Changing Approaches to Diabetes in Pregnancy Kirsten E. Salmeen, MD Assistant Professor Obstetrics, Gynecology & Reproductive Sciences Maternal-Fetal Medicine I have nothing to disclose. Approaches
The Ever-Changing Approaches to Diabetes in Pregnancy Kirsten E. Salmeen, MD Assistant Professor Obstetrics, Gynecology & Reproductive Sciences Maternal-Fetal Medicine I have nothing to disclose. Approaches
Neonatal Hypoglycemia. Presented By : Kamlah Olaimat 25\7\2010
 Neonatal Hypoglycemia Presented By : Kamlah Olaimat 25\7\2010 Definition The S.T.A.B.L.E. Program defines hypoglycemia as: Glucose delivery or availability is inadequate to meet glucose demand (Karlsen,
Neonatal Hypoglycemia Presented By : Kamlah Olaimat 25\7\2010 Definition The S.T.A.B.L.E. Program defines hypoglycemia as: Glucose delivery or availability is inadequate to meet glucose demand (Karlsen,
The New GDM Screening Guidelines. Jennifer Klinke MD, FRCPC Endocrinologist and Co director RCH Diabetes in Pregnancy Program
 The New GDM Screening Guidelines Jennifer Klinke MD, FRCPC Endocrinologist and Co director RCH Diabetes in Pregnancy Program Disclosures Current participant (RCH site) for MiTy study Metformin in women
The New GDM Screening Guidelines Jennifer Klinke MD, FRCPC Endocrinologist and Co director RCH Diabetes in Pregnancy Program Disclosures Current participant (RCH site) for MiTy study Metformin in women
Managing Gestational Diabetes. Definition of GDM
 Managing Gestational Diabetes Definition of GDM Gestational diabetes is defined as glucose intolerance of variable severity with onset or first recognition during pregnancy that excludes those with overt
Managing Gestational Diabetes Definition of GDM Gestational diabetes is defined as glucose intolerance of variable severity with onset or first recognition during pregnancy that excludes those with overt
Diabetes Related Disclosures
 Diabetes Related Disclosures Speakers Bureau Amylin Boehringer Ingelheim Eli Lilly Takeda Classification of Diabetes Diabetes Care January 2011 vol. 34 no. Supplement 1 S11-S61 Type 1 Diabetes Mellitus
Diabetes Related Disclosures Speakers Bureau Amylin Boehringer Ingelheim Eli Lilly Takeda Classification of Diabetes Diabetes Care January 2011 vol. 34 no. Supplement 1 S11-S61 Type 1 Diabetes Mellitus
A Study of Gestational Diabetes in Patients in a Tertiary Care Hospital in Hyderabad Telangana State, India
 International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 6 Number 10 (2017) pp. 2586-2590 Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2017.610.304
International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 6 Number 10 (2017) pp. 2586-2590 Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2017.610.304
Improving Outcomes in Pregnancies Complicated by Diabetes Mellitus
 Improving Outcomes in Pregnancies Complicated by Diabetes Mellitus Steven G. Gabbe, M.D. Emeritus Chief Executive Officer Professor, Obstetrics and Gynecology The Ohio State University Wexner Medical Center
Improving Outcomes in Pregnancies Complicated by Diabetes Mellitus Steven G. Gabbe, M.D. Emeritus Chief Executive Officer Professor, Obstetrics and Gynecology The Ohio State University Wexner Medical Center
Maximizing the Role of WIC Nutritionists in Prevention of DM2 among High Risk Clients ESTHER G. SCHUSTER, MS,RD,CDE
 Maximizing the Role of WIC Nutritionists in Prevention of DM2 among High Risk Clients ESTHER G. SCHUSTER, MS,RD,CDE Heavy Numbers Surgeon General report: 68% of adults in U. S. are overweight or obese
Maximizing the Role of WIC Nutritionists in Prevention of DM2 among High Risk Clients ESTHER G. SCHUSTER, MS,RD,CDE Heavy Numbers Surgeon General report: 68% of adults in U. S. are overweight or obese
Managing Diabetes Before, During, and After Pregnancy
 Managing Diabetes Before, During, and After Pregnancy This program is supported by an educational grant from Novo Nordisk Inc. It has been accredited by AADE for pharmacists, nurses, and dietitians. This
Managing Diabetes Before, During, and After Pregnancy This program is supported by an educational grant from Novo Nordisk Inc. It has been accredited by AADE for pharmacists, nurses, and dietitians. This
GESTATIONAL DIABETES TESTING AND TREAMENT
 Boston Medical Center Maternity Care Guideline: GESTATIONAL DIABETES TESTING AND TREAMENT Accepted: August 2015 Updated: December 2018 Contributors: Aviva Lee-Parritz, MD, Sara Alexanian, MD, Kari Radoff,
Boston Medical Center Maternity Care Guideline: GESTATIONAL DIABETES TESTING AND TREAMENT Accepted: August 2015 Updated: December 2018 Contributors: Aviva Lee-Parritz, MD, Sara Alexanian, MD, Kari Radoff,
during pregnancy. any degree of impaired glucose intolerance 11/19/2012 Prevalence & Diagnosis of Gestational Diabetes
 Prevalence & Diagnosis of Gestational Diabetes A.Ziaee, MD Endocrinologist Gestational diabetes mellitus (GDM); any degree of impaired glucose intolerance with onset or first recognition during pregnancy.
Prevalence & Diagnosis of Gestational Diabetes A.Ziaee, MD Endocrinologist Gestational diabetes mellitus (GDM); any degree of impaired glucose intolerance with onset or first recognition during pregnancy.
DIABETES WITH PREGNANCY
 DIABETES WITH PREGNANCY Prof. Aasem Saif MD,MRCP(UK),FRCP (Edinburgh) Maternal and Fetal Risks Diabetes in pregnancy is associated with risks to the woman and to the developing fetus. Maternal and Fetal
DIABETES WITH PREGNANCY Prof. Aasem Saif MD,MRCP(UK),FRCP (Edinburgh) Maternal and Fetal Risks Diabetes in pregnancy is associated with risks to the woman and to the developing fetus. Maternal and Fetal
Pregestational Diabetes in Pregnancy. An Update
 Pregestational Diabetes in Pregnancy An Update Disclosures D. Ware Branch, MD Nothing to disclose Questions to Be Addressed What are risks factors for adverse pregnancy outcome in pregestational diabetes?
Pregestational Diabetes in Pregnancy An Update Disclosures D. Ware Branch, MD Nothing to disclose Questions to Be Addressed What are risks factors for adverse pregnancy outcome in pregestational diabetes?
Diabetes and Pregnancy
 Diabetes and Pregnancy Eric L. Johnson, M.D. Associate Professor Department of Family and Community Medicine University of North Dakota School of Medicine And Health Sciences Assistant Medical Director
Diabetes and Pregnancy Eric L. Johnson, M.D. Associate Professor Department of Family and Community Medicine University of North Dakota School of Medicine And Health Sciences Assistant Medical Director
Management of Gestational Diabetes
 Management of Gestational Diabetes A Diabetes risk assessment should be ascertained at the First prenatal visit. Low Risk: Early blood glucose screening is NOT routinely required if most of the following
Management of Gestational Diabetes A Diabetes risk assessment should be ascertained at the First prenatal visit. Low Risk: Early blood glucose screening is NOT routinely required if most of the following
Prevention and Management of Diabetes in Pregnancy
 Prevention and Management of Diabetes in Pregnancy Sridhar Chitturi Consultant Endocrinologist Royal Darwin Hospital Outline of the talk Diabetes in Pregnancy Spectrum Diagnostic criteria Why bother about
Prevention and Management of Diabetes in Pregnancy Sridhar Chitturi Consultant Endocrinologist Royal Darwin Hospital Outline of the talk Diabetes in Pregnancy Spectrum Diagnostic criteria Why bother about
Disclosures. Diagnosis and Management of Diabetes in Pregnancy. I have nothing to disclose. Type 1. Overview GDMA1
 Diagnosis and Management of Diabetes in Pregnancy Kirsten Salmeen, MD Assistant Professor Department of Obstetrics, Gynecology & Reproductive Sciences Maternal-Fetal Medicine Disclosures I have nothing
Diagnosis and Management of Diabetes in Pregnancy Kirsten Salmeen, MD Assistant Professor Department of Obstetrics, Gynecology & Reproductive Sciences Maternal-Fetal Medicine Disclosures I have nothing
Pregestational and Gestational Diabetes
 Pregestational and Gestational Diabetes Francis S. Nuthalapaty, MD Greenville Health System University of South Carolina School of Medicine - Greenville Case History 30 year old black female presents to
Pregestational and Gestational Diabetes Francis S. Nuthalapaty, MD Greenville Health System University of South Carolina School of Medicine - Greenville Case History 30 year old black female presents to
Diabetes in obstetric patients
 Diabetes in obstetric patients Swedish Society of Obstetric Anaesthesia & Intensive Care Anita Banerjee Obstetric Physician Diabetes & Endocrinology Consultant Outline Scope of the problem Diabetes and
Diabetes in obstetric patients Swedish Society of Obstetric Anaesthesia & Intensive Care Anita Banerjee Obstetric Physician Diabetes & Endocrinology Consultant Outline Scope of the problem Diabetes and
Gestational Diabetes: Long Term Metabolic Consequences. Outline 5/27/2014
 Gestational Diabetes: Long Term Metabolic Consequences Gladys (Sandy) Ramos, MD Associate Clinical Professor Maternal Fetal Medicine Outline Population rates of obesity and T2DM Obesity and metabolic syndrome
Gestational Diabetes: Long Term Metabolic Consequences Gladys (Sandy) Ramos, MD Associate Clinical Professor Maternal Fetal Medicine Outline Population rates of obesity and T2DM Obesity and metabolic syndrome
Gestational Diabetes in Resouce. Prof Satyan Rajbhandari (RAJ)
") Gestational Diabetes in Resouce Limited Area Prof Satyan Rajbhandari (RAJ) Case History RP, 26F Nepali girl settled in the UK Primi Gravida BMI: 23 FH of type 2 DM 75 gm Glucose OGTT in week 25 0 Min
Gestational Diabetes in Resouce Limited Area Prof Satyan Rajbhandari (RAJ) Case History RP, 26F Nepali girl settled in the UK Primi Gravida BMI: 23 FH of type 2 DM 75 gm Glucose OGTT in week 25 0 Min
Hypoglycemia. Objectives. Glucose Metabolism
 Hypoglycemia Instructor: Janet Mendis, MSN, RNC-NIC, CNS Outline: Janet Mendis, MSN, RNC-NIC, CNS Summer Morgan, MSN, RNC-NIC, CPNP UC San Diego Health System Objectives State the blood glucose level at
Hypoglycemia Instructor: Janet Mendis, MSN, RNC-NIC, CNS Outline: Janet Mendis, MSN, RNC-NIC, CNS Summer Morgan, MSN, RNC-NIC, CPNP UC San Diego Health System Objectives State the blood glucose level at
Diabetes and Pregnancy
 Diabetes and Pregnancy Dr Warren Gillibrand Deputy Director of Postgraduate Education Department of Nursing & Midwifery Department of AHP and Sports Science w.p.gillibrand@hud.ac.uk Aims of the session
Diabetes and Pregnancy Dr Warren Gillibrand Deputy Director of Postgraduate Education Department of Nursing & Midwifery Department of AHP and Sports Science w.p.gillibrand@hud.ac.uk Aims of the session
GESTATIONAL DIABETES for GP Obstetric Shared Care Accreditation Seminar. Simon Kane March 2016
 GESTATIONAL DIABETES for GP Obstetric Shared Care Accreditation Seminar Simon Kane March 2016 Objectives History and definitions Definition and Australian data Pathophysiology and prevalence Rationale
GESTATIONAL DIABETES for GP Obstetric Shared Care Accreditation Seminar Simon Kane March 2016 Objectives History and definitions Definition and Australian data Pathophysiology and prevalence Rationale
10/9/2017 OBJECTIVES DIABETES REVIEW
 OBJECTIVES MECHANICAL MADNESS: TECHNOLOGY, DIABETES AND PREGNANCY ALYSON BLUM, PHARMD, CDE CLINICAL PHARMACIST IN OBSTETRICS SACRED HEART MEDICAL CENTER, CENTER FOR MATERNAL FETAL MEDICINE WASHINGTON STATE
OBJECTIVES MECHANICAL MADNESS: TECHNOLOGY, DIABETES AND PREGNANCY ALYSON BLUM, PHARMD, CDE CLINICAL PHARMACIST IN OBSTETRICS SACRED HEART MEDICAL CENTER, CENTER FOR MATERNAL FETAL MEDICINE WASHINGTON STATE
Peripartum and Postpartum Management of Diabetes
 Peripartum and Postpartum Management of Diabetes General Principles Glucose goal ~ 100 mg/dl (70-110 mg/dl) Labor is EXERCISE with increased metabolic demands. Insulin requirements decrease however the
Peripartum and Postpartum Management of Diabetes General Principles Glucose goal ~ 100 mg/dl (70-110 mg/dl) Labor is EXERCISE with increased metabolic demands. Insulin requirements decrease however the
Diagnosis and Management of Gestational Diabetes Mellitus. Prof. Dr Md Faizul Islam Chowdhury Professor of Medicine, Department of Medicine, DMCH.
 Diagnosis and Management of Gestational Diabetes Mellitus Prof. Dr Md Faizul Islam Chowdhury Professor of Medicine, Department of Medicine, DMCH. Gestational Diabetes Mellitus I, the Fetus I, the fetus
Diagnosis and Management of Gestational Diabetes Mellitus Prof. Dr Md Faizul Islam Chowdhury Professor of Medicine, Department of Medicine, DMCH. Gestational Diabetes Mellitus I, the Fetus I, the fetus
A S Y N T H E S I Z E D H A N D B O O K ON G E S T A T I O N A L D I A B E T E S
 A S Y N T H E S I Z E D H A N D B O O K ON G E S T A T I O N A L D I A B E T E S P R E F A C E Dear reader, This is a synthesized handbook conceived to serve as a tool to health personnel in the screening,
A S Y N T H E S I Z E D H A N D B O O K ON G E S T A T I O N A L D I A B E T E S P R E F A C E Dear reader, This is a synthesized handbook conceived to serve as a tool to health personnel in the screening,
MANAGEMENT OF DIABETES IN PREGNANCY
 MANAGEMENT OF DIABETES IN PREGNANCY Ministry of Health Malaysia Malaysian Endocrine & Metabolic Society Perinatal Society of Malaysia Family Medicine Specialists Association of Malaysia Academy of Medicine
MANAGEMENT OF DIABETES IN PREGNANCY Ministry of Health Malaysia Malaysian Endocrine & Metabolic Society Perinatal Society of Malaysia Family Medicine Specialists Association of Malaysia Academy of Medicine
Diabetes in Pregnancy
 JSAFOG Diabetes in Pregnancy CONTEMPORARY REVIEW ARTICLE Diabetes in Pregnancy Neeta Deshpande Consultant, Diabetologist and Bariatric Physician, Belgaum Diabetes Center, Belgaum, Karnataka, India Correspondence:
JSAFOG Diabetes in Pregnancy CONTEMPORARY REVIEW ARTICLE Diabetes in Pregnancy Neeta Deshpande Consultant, Diabetologist and Bariatric Physician, Belgaum Diabetes Center, Belgaum, Karnataka, India Correspondence:
Significant economic burden Conservative because focus on near-term medical costs, omitting increased long-term risks Insulin Resistance
 What s New in Gestational Diabetes? Diane Reader RD, CDE International Diabetes Center Park Nicollet Health Services Minneapolis, MN GDM Statistics What s New? Proposed Changes to Diagnostic Criteria Treatment
What s New in Gestational Diabetes? Diane Reader RD, CDE International Diabetes Center Park Nicollet Health Services Minneapolis, MN GDM Statistics What s New? Proposed Changes to Diagnostic Criteria Treatment
Reminder: NPIC/QAS CME/CEU Program
 V.12.2 Special Report: Perinatal Complications associated with Gestational and Pregestational Diabetes I. Introduction Diabetes mellitus is a metabolic disease characterized by chronic hyperglycemia and
V.12.2 Special Report: Perinatal Complications associated with Gestational and Pregestational Diabetes I. Introduction Diabetes mellitus is a metabolic disease characterized by chronic hyperglycemia and
CASES: DIABETES AND PREGNANCY
 CASE 1: Visit 1: Ms. Sunny Disposition is a 32 yo G2P1001 who is approximately 15 weeks here for her first prenatal visit. She has already had an US but records not yet received. Pmhx: Unremarkable, no
CASE 1: Visit 1: Ms. Sunny Disposition is a 32 yo G2P1001 who is approximately 15 weeks here for her first prenatal visit. She has already had an US but records not yet received. Pmhx: Unremarkable, no
CASES: DIABETES AND PREGNANCY
 CASE 1: Visit 1: Ms. Sunny Disposition is a 32 yo G2P1001 who is approximately 15 weeks here for her first prenatal visit. She has already had an US but records not yet received. Pmhx: Unremarkable, no
CASE 1: Visit 1: Ms. Sunny Disposition is a 32 yo G2P1001 who is approximately 15 weeks here for her first prenatal visit. She has already had an US but records not yet received. Pmhx: Unremarkable, no
Objectives. Diabetes in Pregnancy: A Growing Dilemma. Diabetes in the US 10/6/2015. Disclosure. The presenter has no conflicts to disclose
 Diabetes in Pregnancy: A Growing Dilemma Kathy O Connell, MN RN Perinatal Clinical Nurse Specialist University of Washington Medical Center Seattle, WA koconnll@uw.edu Objectives Describe pathophysiologic
Diabetes in Pregnancy: A Growing Dilemma Kathy O Connell, MN RN Perinatal Clinical Nurse Specialist University of Washington Medical Center Seattle, WA koconnll@uw.edu Objectives Describe pathophysiologic
Diabetes in Pregnancy: Detection, Intervention, Prevention. Diabetes in Pregnancy: Outline. Diabetes in Pregnancy
 Diabetes in Pregnancy: Detection, Intervention, Prevention Michael Shannon, MD Chair, Providence Endocrinology/Diabetes CAT Diabetes in Pregnancy: Outline Prevalence, Pathophysiology and Complications
Diabetes in Pregnancy: Detection, Intervention, Prevention Michael Shannon, MD Chair, Providence Endocrinology/Diabetes CAT Diabetes in Pregnancy: Outline Prevalence, Pathophysiology and Complications
Diabetes in Pregnancy Registrar Induction. Dr Anna Dover August 31 st 2015
 Diabetes in Pregnancy Registrar Induction Dr Anna Dover August 31 st 2015 Outline Joint Antenatal Diabetes Service Pre-existing diabetes Pre-conception, antenatal management Gestational Diabetes Screening,
Diabetes in Pregnancy Registrar Induction Dr Anna Dover August 31 st 2015 Outline Joint Antenatal Diabetes Service Pre-existing diabetes Pre-conception, antenatal management Gestational Diabetes Screening,
It s Never Too Early To Prevent Diabetes: The Lasting Impact of Gestational Diabetes on Mothers and Children
 It s Never Too Early To Prevent Diabetes: The Lasting Impact of Gestational Diabetes on Mothers and Children Robert Ratner, M.D., F.A.C.P. Vice President for Scientific Affairs, Medstar Research Institute
It s Never Too Early To Prevent Diabetes: The Lasting Impact of Gestational Diabetes on Mothers and Children Robert Ratner, M.D., F.A.C.P. Vice President for Scientific Affairs, Medstar Research Institute
Diabetes & Pregnancy: Management Guide
 Diabetes & Pregnancy: Management Guide This program is supported by an educational grant from Novo Nordisk Inc. Inc Diabetes & Pregnancy: Management Guide is supported by an educational grant from Novo
Diabetes & Pregnancy: Management Guide This program is supported by an educational grant from Novo Nordisk Inc. Inc Diabetes & Pregnancy: Management Guide is supported by an educational grant from Novo
Obstetrics and Gynaecology
 Purpose Pregnancy is associated with changes to insulin sensitivity which can lead to elevated maternal blood glucose levels (BGLs). When elevated BGLs are first diagnosed during pregnancy the mother has
Purpose Pregnancy is associated with changes to insulin sensitivity which can lead to elevated maternal blood glucose levels (BGLs). When elevated BGLs are first diagnosed during pregnancy the mother has
Effect of Various Degrees of Maternal Hyperglycemia on Fetal Outcome
 ORIGINAL ARTICLE Effect of Various Degrees of Maternal Hyperglycemia on Fetal Outcome ABSTRACT Shagufta Tahir, Shaheen Zafar, Savita Thontia Objective Study design Place & Duration of study Methodology
ORIGINAL ARTICLE Effect of Various Degrees of Maternal Hyperglycemia on Fetal Outcome ABSTRACT Shagufta Tahir, Shaheen Zafar, Savita Thontia Objective Study design Place & Duration of study Methodology
Screening for diabetes
 Screening for diabetes Peggy Odegard, Pharm.D, BCPS, CDE What are your risks? 1 Diabetes Mellitus A problem with glucose regulation type 1= pancreas cannot produce insulin so total insulin deficiency,
Screening for diabetes Peggy Odegard, Pharm.D, BCPS, CDE What are your risks? 1 Diabetes Mellitus A problem with glucose regulation type 1= pancreas cannot produce insulin so total insulin deficiency,
Diabetes in pregnancy
 Diabetes in pregnancy Bipin Sethi Department of Endocrinology Care Hospitals Hyderabad, India Declared no potential conflict of interest Diabetes in pregnancy Bipin Kumar Sethi Department of Endocrinology,
Diabetes in pregnancy Bipin Sethi Department of Endocrinology Care Hospitals Hyderabad, India Declared no potential conflict of interest Diabetes in pregnancy Bipin Kumar Sethi Department of Endocrinology,
Why is my Blood Sugar Too High?
 What is Gestational Diabetes? Gestational diabetes is a type of diabetes which can occur during pregnancy and usually goes away after the baby is delivered. Gestational means in pregnancy and Diabetes
What is Gestational Diabetes? Gestational diabetes is a type of diabetes which can occur during pregnancy and usually goes away after the baby is delivered. Gestational means in pregnancy and Diabetes
Current Approaches to Caring for the Woman with Diabetes During Pregnancy
 CONTINUING EDUCATION Current Approaches to Caring for the Woman with Diabetes During Pregnancy Julie Daley, RN, MS, CDE Director, Diabetes in Pregnancy Program Women & Infants Hospital of Rhode Island
CONTINUING EDUCATION Current Approaches to Caring for the Woman with Diabetes During Pregnancy Julie Daley, RN, MS, CDE Director, Diabetes in Pregnancy Program Women & Infants Hospital of Rhode Island
Pregnancies complicated by diabetes. Marina Mickleson Nurse Practitioner Midwife CDE
 Pregnancies complicated by diabetes Marina Mickleson Nurse Practitioner Midwife CDE Two types Pre gestational Gestational diabetes Both types are on the increase Pre conception work up is imperative for
Pregnancies complicated by diabetes Marina Mickleson Nurse Practitioner Midwife CDE Two types Pre gestational Gestational diabetes Both types are on the increase Pre conception work up is imperative for
Screening and Diagnosis of Diabetes Mellitus in Taiwan
 Screening and Diagnosis of Diabetes Mellitus in Taiwan Hung-Yuan Li, MD, MMSc, PhD Attending Physician, Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan Associate Professor,
Screening and Diagnosis of Diabetes Mellitus in Taiwan Hung-Yuan Li, MD, MMSc, PhD Attending Physician, Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan Associate Professor,
Diabetes in pregnancy
 Issue date: March 2008 Diabetes in pregnancy Management of diabetes and its complications from pre-conception to the postnatal period Developed by the National Collaborating Centre for Women s and Children
Issue date: March 2008 Diabetes in pregnancy Management of diabetes and its complications from pre-conception to the postnatal period Developed by the National Collaborating Centre for Women s and Children
The GDM Network presents. Diagnosing and Screening for Gestational Diabetes: Still a Controversy? Still a Challenge? June 18, :30-3:00 PM
 The GDM Network presents Diagnosing and Screening for Gestational Diabetes: Still a Controversy? Still a Challenge? June 18, 2013 1:30-3:00 PM Speakers include: Robert Silver, MD, NIH GDM Panelist Neil
The GDM Network presents Diagnosing and Screening for Gestational Diabetes: Still a Controversy? Still a Challenge? June 18, 2013 1:30-3:00 PM Speakers include: Robert Silver, MD, NIH GDM Panelist Neil
Janice Lazear, DNP, FNP-C, CDE DIAGNOSIS AND CLASSIFICATION OF DIABETES
 Janice Lazear, DNP, FNP-C, CDE DIAGNOSIS AND CLASSIFICATION OF DIABETES Objectives u At conclusion of the lecture the participant will be able to: 1. Differentiate between the classifications of diabetes
Janice Lazear, DNP, FNP-C, CDE DIAGNOSIS AND CLASSIFICATION OF DIABETES Objectives u At conclusion of the lecture the participant will be able to: 1. Differentiate between the classifications of diabetes
Diagnosis of gestational diabetes mellitus: comparison between National Diabetes Data Group and Carpenter Coustan criteria
 Asian Biomedicine Vol. 8 No. 4 August 2014; 505-509 Brief communication (Original) DOI: 10.5372/1905-7415.0804.320 Diagnosis of gestational diabetes mellitus: comparison between National Diabetes Data
Asian Biomedicine Vol. 8 No. 4 August 2014; 505-509 Brief communication (Original) DOI: 10.5372/1905-7415.0804.320 Diagnosis of gestational diabetes mellitus: comparison between National Diabetes Data
NICE guideline Published: 25 February 2015 nice.org.uk/guidance/ng3
 Diabetes in pregnancy: management from preconception to the postnatal period NICE guideline Published: 25 February 2015 nice.org.uk/guidance/ng3 NICE 2017. All rights reserved. Subject to Notice of rights
Diabetes in pregnancy: management from preconception to the postnatal period NICE guideline Published: 25 February 2015 nice.org.uk/guidance/ng3 NICE 2017. All rights reserved. Subject to Notice of rights
A CLINICAL STUDY OF GESTATIONAL DIABETES MELLITUS IN A TEACHING HOSPITAL IN KERALA Baiju Sam Jacob 1, Girija Devi K 2, V.
 A CLINICAL STUDY OF GESTATIONAL DIABETES MELLITUS IN A TEACHING HOSPITAL IN KERALA Baiju Sam Jacob 1, Girija Devi K 2, V. Baby Paul 3 HOW TO CITE THIS ARTICLE: Baiju Sam Jacob, Girija Devi K, V. Baby Paul.
A CLINICAL STUDY OF GESTATIONAL DIABETES MELLITUS IN A TEACHING HOSPITAL IN KERALA Baiju Sam Jacob 1, Girija Devi K 2, V. Baby Paul 3 HOW TO CITE THIS ARTICLE: Baiju Sam Jacob, Girija Devi K, V. Baby Paul.
AACN PCCN Review. Endocrine
 AACN PCCN Review Endocrine Presenter: Carol A. Rauen, RN, MS, CCNS, CCRN, PCCN, CEN Independent Clinical Nurse Specialist & Education Consultant rauen.carol104@gmail.com Endocrine I. INTRODUCTION Disorders
AACN PCCN Review Endocrine Presenter: Carol A. Rauen, RN, MS, CCNS, CCRN, PCCN, CEN Independent Clinical Nurse Specialist & Education Consultant rauen.carol104@gmail.com Endocrine I. INTRODUCTION Disorders
Diabetes: Definition Pathophysiology Treatment Goals. By Scott Magee, MD, FACE
 Diabetes: Definition Pathophysiology Treatment Goals By Scott Magee, MD, FACE Disclosures No disclosures to report Definition of Diabetes Mellitus Diabetes Mellitus comprises a group of disorders characterized
Diabetes: Definition Pathophysiology Treatment Goals By Scott Magee, MD, FACE Disclosures No disclosures to report Definition of Diabetes Mellitus Diabetes Mellitus comprises a group of disorders characterized
Maternal and Fetal Complications in Diabetes Pregnancy
 Maternal and Fetal Complications in Diabetes Pregnancy Helen R Murphy Professor of Medicine (Diabetes & Antenatal Care), UEA Professor of Women s Health, Kings College London hm386@medschl.cam.ac.uk 1
Maternal and Fetal Complications in Diabetes Pregnancy Helen R Murphy Professor of Medicine (Diabetes & Antenatal Care), UEA Professor of Women s Health, Kings College London hm386@medschl.cam.ac.uk 1
Pregnancy and Diabetes
 Pregnancy and Diabetes Aim(s) and objective(s) This guideline aims to highlight the importance of maintaining good glycaemic control in women of childbearing age contemplating pregnancy, during pregnancy
Pregnancy and Diabetes Aim(s) and objective(s) This guideline aims to highlight the importance of maintaining good glycaemic control in women of childbearing age contemplating pregnancy, during pregnancy
Screening & Management of Diabetes in Pregnancy: What s New?
 Screening & Management of Diabetes in Pregnancy: What s New? Jerrie S. Refuerzo, M.D. Associate Professor Division of Maternal Fetal medicine Department of Obstetrics, Gynecology and Reproductive Sciences
Screening & Management of Diabetes in Pregnancy: What s New? Jerrie S. Refuerzo, M.D. Associate Professor Division of Maternal Fetal medicine Department of Obstetrics, Gynecology and Reproductive Sciences
Diabetes in Pregnancy Dr. Hana
 Diabetes in Pregnancy Dr. Hana Introduction Diabetes occurs in 2 5% of all UK pregnancies and its prevalence is rising. Forty years ago the majority of women with diabetes attending an antenatal clinic
Diabetes in Pregnancy Dr. Hana Introduction Diabetes occurs in 2 5% of all UK pregnancies and its prevalence is rising. Forty years ago the majority of women with diabetes attending an antenatal clinic
Gestational Diabetes Mellitus
 Gestational Diabetes Mellitus Should GPs keep a register of everyone with GDM? Ross Lawrenson Waikato Clinical School University of Auckland Definition of GDM GDM is defined as carbohydrate intolerance
Gestational Diabetes Mellitus Should GPs keep a register of everyone with GDM? Ross Lawrenson Waikato Clinical School University of Auckland Definition of GDM GDM is defined as carbohydrate intolerance
Diabetes in pregnancy & its management Begum R
 The ORION Medical Journal 2008 Jan;29:524-527 Diabetes in pregnancy & its management Begum R Introduction Diabetes mellitus is the most common medical complication of pregnancy and it carries a significant
The ORION Medical Journal 2008 Jan;29:524-527 Diabetes in pregnancy & its management Begum R Introduction Diabetes mellitus is the most common medical complication of pregnancy and it carries a significant
associated with serious complications, but reduce occurrences with preventive measures
 Wk 9. Management of Clients with Diabetes Mellitus 1. Diabetes Mellitus body s inability to metabolize carbohydrates, fats, proteins hyperglycemia associated with serious complications, but reduce occurrences
Wk 9. Management of Clients with Diabetes Mellitus 1. Diabetes Mellitus body s inability to metabolize carbohydrates, fats, proteins hyperglycemia associated with serious complications, but reduce occurrences
ELEVATED BLOOD GLUCOSE RECOMMENDATION GUIDELINES THAT PRODUCE POSITIVE MATERNAL AND PERINATAL OUTCOMES AT THE UNIVERSITY OF KANSAS OBSTETRICS CLINIC
 ELEVATED BLOOD GLUCOSE RECOMMENDATION GUIDELINES THAT PRODUCE POSITIVE MATERNAL AND PERINATAL OUTCOMES AT THE UNIVERSITY OF KANSAS OBSTETRICS CLINIC By Erin M. Plumberg, RD,LD Submitted to the graduate
ELEVATED BLOOD GLUCOSE RECOMMENDATION GUIDELINES THAT PRODUCE POSITIVE MATERNAL AND PERINATAL OUTCOMES AT THE UNIVERSITY OF KANSAS OBSTETRICS CLINIC By Erin M. Plumberg, RD,LD Submitted to the graduate
Neurodevelopmental Risk?
 Normal Newborn During transitional hypoglycemia normal newborns have an enhanced ketogenic response to fasting. Newborn brains have enhanced capability to use ketone bodies for fuel Allows newborns to
Normal Newborn During transitional hypoglycemia normal newborns have an enhanced ketogenic response to fasting. Newborn brains have enhanced capability to use ketone bodies for fuel Allows newborns to
Highlighting the Differences between Preexisting Type 1 and Type 2 Diabetes in Pregnancy and Gestational Diabetes
 Highlighting the Differences between Preexisting Type 1 and Type 2 Diabetes in Pregnancy and Gestational Diabetes Elizabeth (Libby) Downs Quiroga, MS, RD, CDE Tandem Diabetes Care Clinical Specialist Grand
Highlighting the Differences between Preexisting Type 1 and Type 2 Diabetes in Pregnancy and Gestational Diabetes Elizabeth (Libby) Downs Quiroga, MS, RD, CDE Tandem Diabetes Care Clinical Specialist Grand
Are Novel Lifestyle Approaches to Management of Type 2 Diabetes Applicable to Prevention and Treatment of Women with Gestational Diabetes Mellitus?
 Open Access Journal Volume: 1.1 Global Diabetes Open Access Journal Are Novel Lifestyle Approaches to Management of Type 2 Diabetes Applicable to Prevention and Treatment of Women with Gestational Diabetes
Open Access Journal Volume: 1.1 Global Diabetes Open Access Journal Are Novel Lifestyle Approaches to Management of Type 2 Diabetes Applicable to Prevention and Treatment of Women with Gestational Diabetes
Guideline for the Management of Diabetes in Pregnancy
 Guideline for the Management of Diabetes in Pregnancy INITIATED BY: Directorate of Obstetrics, Gynaecology & Sexual Health APPROVED BY: Integrated Business, Obstetrics, Gynaecology, Sexual Health & Patient
Guideline for the Management of Diabetes in Pregnancy INITIATED BY: Directorate of Obstetrics, Gynaecology & Sexual Health APPROVED BY: Integrated Business, Obstetrics, Gynaecology, Sexual Health & Patient
Diabetes in Pregnancy Registrar Induction Programme. Dr Anna Dover August 29 th 2016
 Diabetes in Pregnancy Registrar Induction Programme Dr Anna Dover August 29 th 2016 Diabetes in pregnancy Why it matters What our service looks like How we diagnose and manage GDM Patients with pre-existing
Diabetes in Pregnancy Registrar Induction Programme Dr Anna Dover August 29 th 2016 Diabetes in pregnancy Why it matters What our service looks like How we diagnose and manage GDM Patients with pre-existing
SARASOTA MEMORIAL HOSPITAL
 SARASOTA MEMORIAL HOSPITAL TITLE: NURSING PROCEDURE CARE OF THE INTRAPARTUM PATIENT RECEIVING CONTINUOUS INTRAVENOUS INSULIN ADMINISTRATION (obs25) DATE: REVIEWED: PAGES: 9/93 12/17 1 of 5 PS1094 ISSUED
SARASOTA MEMORIAL HOSPITAL TITLE: NURSING PROCEDURE CARE OF THE INTRAPARTUM PATIENT RECEIVING CONTINUOUS INTRAVENOUS INSULIN ADMINISTRATION (obs25) DATE: REVIEWED: PAGES: 9/93 12/17 1 of 5 PS1094 ISSUED
DIABETES MELLITUS. IAP UG Teaching slides
 DIABETES MELLITUS 1 DIABETES MELLITUS IN CHILDREN Introduction, Definition Classification, pathogenesis Clinical features Investigations and diagnosis Therapy and follow up Complications Carry home message
DIABETES MELLITUS 1 DIABETES MELLITUS IN CHILDREN Introduction, Definition Classification, pathogenesis Clinical features Investigations and diagnosis Therapy and follow up Complications Carry home message
Objectives. Medical Complications of Pregnancy. Potential Conflicts: None. Common Complicating Medical Conditions that Precede Pregnancy
 Medical Complications of Potential Conflicts: None Ellen W. Seely, M.D. Director of Clinical Research Endocrine-Hypertension Division Brigham and Women s Hospital Professor of Medicine Harvard Medical
Medical Complications of Potential Conflicts: None Ellen W. Seely, M.D. Director of Clinical Research Endocrine-Hypertension Division Brigham and Women s Hospital Professor of Medicine Harvard Medical
Maternal Child Health and Chronic Disease
 Maternal Child Health and Chronic Disease The Odd Couple or A Marriage Made in Heaven? AMCHP Women and Perinatal Health Information Series July 17, 2008 Joan Ware, MSPH, RN, Consultant, Women s s Health
Maternal Child Health and Chronic Disease The Odd Couple or A Marriage Made in Heaven? AMCHP Women and Perinatal Health Information Series July 17, 2008 Joan Ware, MSPH, RN, Consultant, Women s s Health
Neonatal Hypoglycemia
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Neonatal Hypoglycemia. These podcasts are designed to give medical students an overview of key topics in pediatrics.
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Neonatal Hypoglycemia. These podcasts are designed to give medical students an overview of key topics in pediatrics.
The Nurse s Guide to Understanding Gestational Diabetes
 The Nurse s Guide to Understanding Gestational Diabetes 1 Contact Hours Copyright 2013 by RN.com. All Rights Reserved. Reproduction and distribution of these materials is prohibited without anrn.com content
The Nurse s Guide to Understanding Gestational Diabetes 1 Contact Hours Copyright 2013 by RN.com. All Rights Reserved. Reproduction and distribution of these materials is prohibited without anrn.com content
Diabetes Mellitus (DM) - Dr Hiren Patt
 - Dr Hiren Patt") Diabetes Mellitus (DM) - Dr Hiren Patt What is DM? FPG 2-Hour PG on OGTT Diabetes Mellitus Diabetes Mellitus 126 mg/dl 100 mg/dl Impaired Fasting Glucose 200 mg/dl 140 mg/dl Impaired Glucose Tolerance
Diabetes Mellitus (DM) - Dr Hiren Patt What is DM? FPG 2-Hour PG on OGTT Diabetes Mellitus Diabetes Mellitus 126 mg/dl 100 mg/dl Impaired Fasting Glucose 200 mg/dl 140 mg/dl Impaired Glucose Tolerance
National Aboriginal Diabetes Association. Gestational Diabetes (developed by Sarah Smith, 4 th yr Nursing, University of Manitoba)
") National Aboriginal Diabetes Association Gestational Diabetes (developed by Sarah Smith, 4 th yr Nursing, University of Manitoba) Who we are NADA is a not-for-profit members-led organization established
National Aboriginal Diabetes Association Gestational Diabetes (developed by Sarah Smith, 4 th yr Nursing, University of Manitoba) Who we are NADA is a not-for-profit members-led organization established
Data from birth certificates in the United
 Chapter 36 Pregnancy in Preexisting Diabetes Thomas A. Buchanan, M.D. SUMMARY Data from birth certificates in the United States indicate that maternal diabetes complicates 2%-3% of all pregnancies, but
Chapter 36 Pregnancy in Preexisting Diabetes Thomas A. Buchanan, M.D. SUMMARY Data from birth certificates in the United States indicate that maternal diabetes complicates 2%-3% of all pregnancies, but
Management of MDR TB in special situations. Dr Sarabjit Chadha The Union
 Management of MDR TB in special situations Dr Sarabjit Chadha The Union MDR TB in special situations Pregnancy Breastfeeding Contraception Renal Insufficiency Diabetes Pregnancy and TB Pregnancy is not
Management of MDR TB in special situations Dr Sarabjit Chadha The Union MDR TB in special situations Pregnancy Breastfeeding Contraception Renal Insufficiency Diabetes Pregnancy and TB Pregnancy is not
GDM. Literature Review. GESTATIONAL DIABETES MELLITUS: A review for midwives AUTHORS BACKGROUND CONTRIBUTORS TABLE OF CONTENTS
 GDM Literature Review GESTATIONAL DIABETES MELLITUS: A review for midwives AUTHORS Sophia Kehler, BA; Tasha MacDonald, RM, MHSc; Anna Meuser, MPH CONTRIBUTORS Clinical Practice Guideline Committee (2015):
GDM Literature Review GESTATIONAL DIABETES MELLITUS: A review for midwives AUTHORS Sophia Kehler, BA; Tasha MacDonald, RM, MHSc; Anna Meuser, MPH CONTRIBUTORS Clinical Practice Guideline Committee (2015):