DIABETES AND PREGNANCY. CDE Exam Preparation March 22 & 27, 2018 Presented by Wendy Graham RD CDE Mentor
|
|
|
- Cecilia Harvey
- 5 years ago
- Views:
Transcription
1 DIABETES AND PREGNANCY CDE Exam Preparation March 22 & 27, 2018 Presented by Wendy Graham RD CDE Mentor
2 OBJECTIVES Describe targets for blood glucose in pregnancy Discuss the risks to baby if blood glucose is elevated Discuss Gestational Diabetes Risk Factors Screening and Diagnosis Complications Management Discuss preconception care for women with Type 1 or Type 2 diabetes Describe treatment through the pregnancy with preexisting diabetes
3 TARGET BLOOD GLUCOSE Testing Times Target Fasting < 5.3 One hour after meal < 7.8 Two hour after meal < 6.7

4 RISK TO BABY TYPE 1 OR TYPE 2 Congenital Malformation Stillbirth Macrosomia Perinatal Mortality Morbidity Hypoglycemia Jaundice Obesity in later life

5 Large for gestational age (macrosomia) Trauma Shoulder dystocia Hypoglycemia Respiratory Distress Jaundice Obesity later in life

6 Age Obesity Ethnicity PCOS Family History of Type 2 Family History of large babies (ie. >9 lbs)
 o 2 Step ( 50 g, 75g")
7 GESTATIONAL DIABETES : SCREENING AND DIAGNOSIS Two Methods in the Clinical Practice Guidelines o 1 Step ( 75 g ) o 2 Step ( 50 g, 75g )

8 GESTATIONAL DIABETES: 1 STEP 24 to 28 weeks 75 g oral glucose tolerance test Screening FBS > hr > hr > 8.5 Preferred method recommended in Waterloo Wellington

9 GESTATIONAL DIABETES: 2 STEP 24 to 28 weeks 50 g oral glucose tolerance test 1 hr pc hr > 11.0 GDM Screening Follow by 75 g glucose tolerance test FBS > hr > hr > 9.0
 Insulin Metformin")
10 Diet Blood Glucose monitoring Exercise Medication(as required) Insulin Metformin Glyburide

11 3 meals/ 3 snacks/day Bedtime snack is important B Snack L Snack D Snack Bed Control the amount of Carbohydrate at meals Adequate protein and nutrients for pregnancy Low Glycemic Index

12 GESTATIONAL DIABETES: MONITORING Diet Controlled Fasting 1 or 2 hours after each meal Using Insulin Fasting/ac meals 1 or 2 hours after meals Testing Times Target Fasting < 5.3 One hour after meal Two hour after meal < 7.8 < 6.7


13 GESTATIONAL DIABETES: COMPLICATIONS TO MOTHER Polyhydramnios Fluid retention Hypertension Preeclampsia Difficult delivery Trauma Caesarian section Infection

14 GESTATIONAL DIABETES: EXERCISE Walking after meals


15 GESTATIONAL DIABETES: MEDICATION Insulin 1st choice o No upper limit o Safe Oral Medications o Metformin o Glyburide
16 Post Partum 75 g OGTT 6 weeks 6 months Next Pregnancy Screened early in next pregnancy Risk of Type 2

17 PREGNANCY WITH PREEXISTING DIABETES
18 PRECONCEPTION CARE: TYPE 1 & TYPE 2 All women with Type 1 and Type 2 should receive education and preconception care. Optimize blood sugars Assess complications - eyes, kidneys, heart Review medications Begin folic acid supplements
19 PRECONCEPTION CARE: TYPE 1 & TYPE 2 Blood sugars A1c <7% Reduces risk of: Congenital malformations Preeclampsia Progression of retinopathy Folic acid supplements 5mg 3 months preconception up to 12 weeks Neural tube defects
20 PRECONCEPTION CARE: TYPE 1 & TYPE 2 Hyperglycemia Teratogenic to the fetus Increased birth weight Increased risk of obesity Post delivery hypoglycemia of infant Increased incidence jaundice/respiratory distress

21 PRECONCEPTION CARE: TYPE 1 & TYPE 2 Hypertension % in women with diabetes Type 1 increased risk of pre-eclampsia Type 2 chronic hypertension Teratogens: ACE/ARB Substitute with effective antihypertensives, calcium channel blockers, beta blockers eg. labatolol/aldomet


22 PRECONCEPTION CARE: TYPE 1 & TYPE 2 Hyperlipidemia Medications are teratogens Retinopathy Eye exam prior to pregnancy and in 1 st trimester and as required each trimester Retinopathy worsens during pregnancy
23 TYPE 1 1 st Trimester Insulin requirements are decreased Risk of hypoglycemia is highest Hypoglycemia unawareness Partner should be taught glucagon Risk for other autoimmune disorders hypothyroidism Risk for severe hypoglycemia in 1 st trimester especially when asleep
24 TYPE 1 2 nd Trimester o Risk of hypoglycemia until 16 weeks o Insulin requirements go up times o Frequent monitoring and insulin adjustment o Fetal monitoring 3 rd Trimester o Frequent monitoring and insulin adjustment o Fetal monitoring Ultrasound, Non stress test, kick counts

25 COMPLICATION TO MOTHER TYPE 1 Spontaneous abortion Hypoglycemia/ketoacidosis Polyhydramnios Infections Hypertension Pre-eclampsia Preterm labour Caesarian section Progression of complications

26 TYPE 2 Older Heavier PCOS Taking oral medications Likely to have hypertension, hyperlipidemia
27 TYPE 2 1 st Trimester o Monitoring and initiation of Insulin o Discontinuation of oral medications o ACE, ARB, statins 2 nd Trimester o Insulin requirements go increase o Frequent monitoring and insulin adjustment o Monitoring of blood pressure o Fetal monitoring 3 rd Trimester o Frequent monitoring and insulin adjustment o Fetal monitoring Ultrasound, Non stress test, kick counts

28 TYPE 1 & 2 DIABETES AND PREGNANCY Management o Monitoring 6-8 times/day o Insulin at all meals/sometimes snacks o Frequent appointments Testing Times Target Fasting < 5.3 One hour after meal < 7.8 Two hour after meal < 6.7
29 SAMPLE QUESTION # 1 Geraldine is newly-diagnosed with type 2 diabetes, A1c 8.4%. She has been started on metformin 500 mg bid and empagliflozin 25 mg. During your initial interview she shares that she and her husband are trying to have a baby. What would your 1 st concern be around this topic? a) She should lose weight before trying to conceive b) She should take a prenatal vitamin with folic acid c) She should use some type of contraception until her A1c is 7% or below d) She should not have children as they might also have diabetes
30 SAMPLE QUESTION #2 Karina has been diagnosed with gestational diabetes. Her father has type 2 diabetes and feels she is testing too often. How often should Karina be testing her blood glucose? a) Twice per day at different times b) Fasting and 1 hour after meals c) Before all meals and at bedtime d) Before and after 1 meal a day, rotating between meals.
31 SAMPLE QUESTION The recommended amount of folic acid for a woman with type 1 diabetes who is trying to conceive is: a) 1 mg b) 3 mg c) 5 mg d) 0.9mg

32 Questions Contact me at: Check out information at: waterloowellingtondiabetes.ca

33
34 Hyperglycemia Describe Diabetic Ketoacidosis (DKA) Describe Hyperglycemic Hyperosmolar State (HHS) Compare the differences in these two hyperglycemia emergencies and the appropriate treatment 34
35 DKA 35
36 Diabetic Ketoacidosis Characteristics Ketones positive Anion Gap > 12 (High) Blood Sugar > 14 (High) Bicarbonate < 15 (Low) PH < 7.3 (Low) Sodium Normal or Low Potassium Normal, Low, High Monitor every hour until fluid and acidosis is corrected (electrolytes, creatinine, osmolality, fluid balance) Pregnant women in DKA present with lower glucose levels than non-pregnant women 36
37 Diabetic Ketoacidosis Characteristics/ Symptoms Quick Less 24 hours Polyuria, polyphagia, polydipsia Kussmaul respiration Nausea and Vomiting Tachycardia Hypotension Leg cramps Abdominal pain Decreased Extracellular volume (ECFV) Weakness, weight loss Physical symptoms of dehydration 37
38 Diabetic Ketoacidosis Causes Newly Diagnosed Type 1 Insulin Omission Infection MI Trauma Flu Eating Disorders (20% recurrent) Pump Failure Thyrotoxicosis Cocaine, atypical antipsychotics, interferon 38
39 Hyperosmolar Hyperglycemic State (HHS) Characteristics Dehydration, Marked Decreased Extracellular volume Blood Sugar >33 Osmolatity > 350 PH > 7.2 Bicarb >20 Ketones +/- Can have neurologic presentation, seizures and stroke like symptoms 39


40 HHS Symptoms Dry Mouth Poor Urine Output Sleepy coma Stupor Increased BUN, Cr 40
41 HHS Causes Illness Decreased Fluid intake Drugs-glucocorticoids, thiazides, lithium and atypical antipsychotics Elderly, chronic care Following cardiac surgery 41
42 Tests Glucose Electrolytes and anion gap Creatinine Osmolality Blood gases Serum and urine ketone Beta-hydroxbutyric acid (78%) Acetoacetate (20 %) Acetone( 2%) Fluid balance Monitor Level of consciousness Precipitating factors 42
43 DKA HHS Blood Sugar > 14 >34 Ketones Positive + / - Osmolality Normal > 350 PH < 7.3 > 7.2 (normal) Anion gap increased normal Presentation Rapid Slower Characteristics Treatment Weight Loss Vomiting Abdominal pain Insulin (0.1u/kg/h) Hydration Mortality < 1 % (age 20-49) 16% (over 75) Incidence hospital admissions US Illness Dehydration Stupor Hydration Insulin % 4-9 % < 1 % 43
")
44 Treatment DKA HHS Fluid resuscitation Avoid Hypokalemia Insulin Avoid rapidly falling serum osmolality Causes Fluid resuscitation K Bicarb Electrolytes Avoid Hypokalemia Avoid rapidly falling serum osmolality Causes Insulin Concerns: Cerebral Edema if hyperosmolality is reduced quickly( only 3 mmol/kg/hr) 44
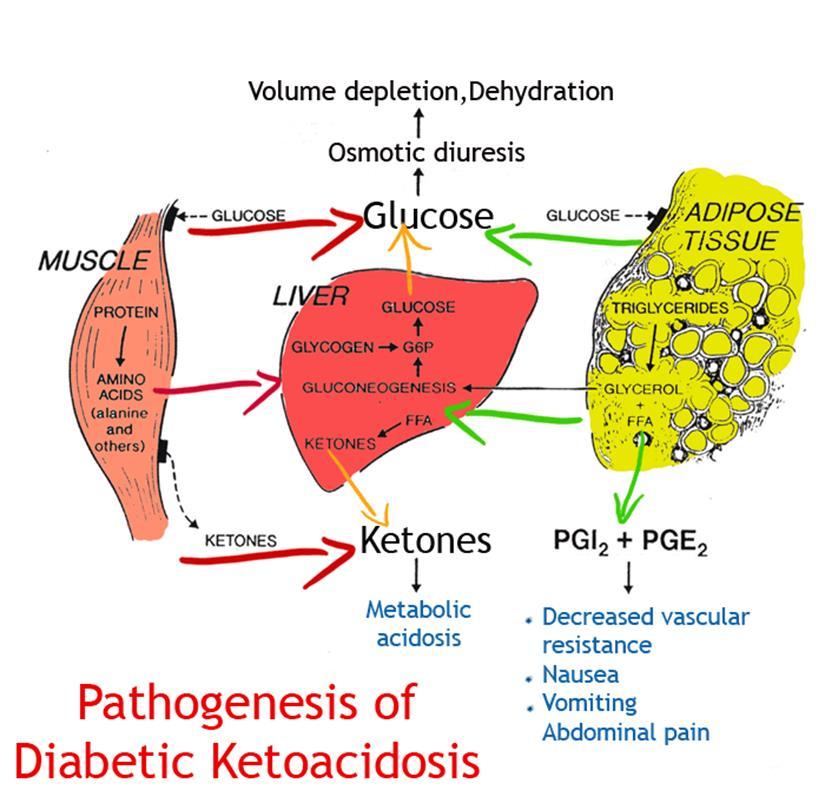
45 Increased gluconeogensis Increased glycogenolysis Decreased glucose utilization by liver, muscle, fat Ketones Acidosis Insulin Insulin Deficiency Hyperglycemia Type 1 Glucagon is increased Increased Cortisol Type 2 Increased Catecholamines Suppresses insulin release Urinary Water Loss (Na, K, Cl) Extracellular Fluid Volume depletion Wendy s attempt to simplify Diabetic Ketoacidosis 45

46 Case Study Judy was brought to hospital by her husband. She has been weak and sleepy for the last 24 hours. She is now complaining of abdominal pain. What blood tests would you look at to determine if this is DKA or HHS? a) Blood Glucose, anion gap, urine ketones, bicarbonate b) Ethanol, salicylate, acetominophen c) Insulin levels, blood ketones d) Blood glucose, anion gap, blood ketones, ph, bicarbonate 46
CDE Exam Preparation Presented by Wendy Graham RD CDE May 4, 2017
 CDE Exam Preparation Presented by Wendy Graham RD CDE May 4, 2017 DKA at organ level 3 Diabetic Ketoacidosis Characteristics Ketones positive Anion Gap > 12 (High) Blood Sugar > 14 (High) Bicarbonate
CDE Exam Preparation Presented by Wendy Graham RD CDE May 4, 2017 DKA at organ level 3 Diabetic Ketoacidosis Characteristics Ketones positive Anion Gap > 12 (High) Blood Sugar > 14 (High) Bicarbonate
Diabetes in Pregnancy
 Diabetes in Pregnancy Ebony Boyce Carter, MD, MPH Division of Maternal Fetal Medicine Washington University School of Medicine Disclosures I have no financial disclosures to report. Objectives Review the
Diabetes in Pregnancy Ebony Boyce Carter, MD, MPH Division of Maternal Fetal Medicine Washington University School of Medicine Disclosures I have no financial disclosures to report. Objectives Review the
Management of Pregestational and Gestational Diabetes Mellitus
 Background and Prevalence Management of Pregestational and Gestational Diabetes Mellitus Pregestational Diabetes - 8 million women in the US are affected, complicating 1% of all pregnancies. Type II is
Background and Prevalence Management of Pregestational and Gestational Diabetes Mellitus Pregestational Diabetes - 8 million women in the US are affected, complicating 1% of all pregnancies. Type II is
Diabetic Emergencies: Ketoacidosis and the Hyperglycemic Hyperosmolar State. Adam Bursua, Pharm.D., BCPS
 Diabetic Emergencies: Ketoacidosis and the Hyperglycemic Hyperosmolar State Adam Bursua, Pharm.D., BCPS Objectives Describe the epidemiology of diabetic ketoacidosis (DKA) and the hyperglycemic hyperosmolar
Diabetic Emergencies: Ketoacidosis and the Hyperglycemic Hyperosmolar State Adam Bursua, Pharm.D., BCPS Objectives Describe the epidemiology of diabetic ketoacidosis (DKA) and the hyperglycemic hyperosmolar
Diabetes in obstetric patients
 Diabetes in obstetric patients Swedish Society of Obstetric Anaesthesia & Intensive Care Anita Banerjee Obstetric Physician Diabetes & Endocrinology Consultant Outline Scope of the problem Diabetes and
Diabetes in obstetric patients Swedish Society of Obstetric Anaesthesia & Intensive Care Anita Banerjee Obstetric Physician Diabetes & Endocrinology Consultant Outline Scope of the problem Diabetes and
2018 Standard of Medical Care Diabetes and Pregnancy
 2018 Standard of Medical Care Diabetes and Pregnancy 2018 Standard of Medical Care Diabetes and Pregnancy Marjorie Cypress does not have any relevant financial relationships with any commercial interests
2018 Standard of Medical Care Diabetes and Pregnancy 2018 Standard of Medical Care Diabetes and Pregnancy Marjorie Cypress does not have any relevant financial relationships with any commercial interests
Name: Oasis: Questions EPCP. Professional Development: Diabetes
 EPCP Professional Development: Diabetes Name: Oasis: Questions 1) Type 1 diabetes in characterized by which of the following: 1) adult onset, obesity 2) juvenile onset, lean build 3) auto-immune beta cell
EPCP Professional Development: Diabetes Name: Oasis: Questions 1) Type 1 diabetes in characterized by which of the following: 1) adult onset, obesity 2) juvenile onset, lean build 3) auto-immune beta cell
DIABETES WITH PREGNANCY
 DIABETES WITH PREGNANCY Prof. Aasem Saif MD,MRCP(UK),FRCP (Edinburgh) Maternal and Fetal Risks Diabetes in pregnancy is associated with risks to the woman and to the developing fetus. Maternal and Fetal
DIABETES WITH PREGNANCY Prof. Aasem Saif MD,MRCP(UK),FRCP (Edinburgh) Maternal and Fetal Risks Diabetes in pregnancy is associated with risks to the woman and to the developing fetus. Maternal and Fetal
Pregnancies complicated by diabetes. Marina Mickleson Nurse Practitioner Midwife CDE
 Pregnancies complicated by diabetes Marina Mickleson Nurse Practitioner Midwife CDE Two types Pre gestational Gestational diabetes Both types are on the increase Pre conception work up is imperative for
Pregnancies complicated by diabetes Marina Mickleson Nurse Practitioner Midwife CDE Two types Pre gestational Gestational diabetes Both types are on the increase Pre conception work up is imperative for
Diabetic Ketoacidosis
 Diabetic Ketoacidosis Definition: Diabetic Ketoacidosis is one of the most serious acute complications of diabetes. It s more common in young patients with type 1 diabetes mellitus. It s usually characterized
Diabetic Ketoacidosis Definition: Diabetic Ketoacidosis is one of the most serious acute complications of diabetes. It s more common in young patients with type 1 diabetes mellitus. It s usually characterized
Gestational Diabetes Mellitus Dr. Fawaz Amin Saad
 Gestational Diabetes Mellitus Dr. Fawaz Amin Saad Senior Consultant OB/GYN, Al-Hayat Medical Center, Doha, Qatar DISCLOSURE OF CONFLICT OF INTEREST I am a full-time Employee at Al-Hayat Medical Center.
Gestational Diabetes Mellitus Dr. Fawaz Amin Saad Senior Consultant OB/GYN, Al-Hayat Medical Center, Doha, Qatar DISCLOSURE OF CONFLICT OF INTEREST I am a full-time Employee at Al-Hayat Medical Center.
Diabetic Ketoacidosis: When Sugar Isn t Sweet!!!
 Diabetic Ketoacidosis: When Sugar Isn t Sweet!!! W Ricks Hanna Jr MD Assistant Professor of Pediatrics University of Tennessee Health Science Center LeBonheur Children s Hospital Introduction Diabetes
Diabetic Ketoacidosis: When Sugar Isn t Sweet!!! W Ricks Hanna Jr MD Assistant Professor of Pediatrics University of Tennessee Health Science Center LeBonheur Children s Hospital Introduction Diabetes
Objectives / Learning Targets: The learner who successfully completes this course will be able to demonstrate understanding of the following concepts:
 Objectives / Learning Targets: The learner who successfully completes this course will be able to demonstrate understanding of the following concepts: Insulin s function in the body. The basics of diabetes
Objectives / Learning Targets: The learner who successfully completes this course will be able to demonstrate understanding of the following concepts: Insulin s function in the body. The basics of diabetes
The New GDM Screening Guidelines. Jennifer Klinke MD, FRCPC Endocrinologist and Co director RCH Diabetes in Pregnancy Program
 The New GDM Screening Guidelines Jennifer Klinke MD, FRCPC Endocrinologist and Co director RCH Diabetes in Pregnancy Program Disclosures Current participant (RCH site) for MiTy study Metformin in women
The New GDM Screening Guidelines Jennifer Klinke MD, FRCPC Endocrinologist and Co director RCH Diabetes in Pregnancy Program Disclosures Current participant (RCH site) for MiTy study Metformin in women
Diabetes in Pregnancy
 Disclosure Diabetes in Pregnancy I have no conflicts of interest to disclose Jennifer Krupp, MD Maternal Fetal Medicine St. Marys Hospital/SSM Health Madison, WI Objectives Classification of Diabetes Classifications
Disclosure Diabetes in Pregnancy I have no conflicts of interest to disclose Jennifer Krupp, MD Maternal Fetal Medicine St. Marys Hospital/SSM Health Madison, WI Objectives Classification of Diabetes Classifications
DKA : Diabetic Ketoacidosis & HHS: Hyperlgycemic Hyperosmolar Syndrome Protocol. Glycemic Task Force September 2014
 DKA : Diabetic Ketoacidosis & HHS: Hyperlgycemic Hyperosmolar Syndrome Protocol Glycemic Task Force September 2014 Hyperglycemic Crises: Pathophysiology DKA HHS Hyperglycemia DKA HHS Umpierrez, In Shoemaker,
DKA : Diabetic Ketoacidosis & HHS: Hyperlgycemic Hyperosmolar Syndrome Protocol Glycemic Task Force September 2014 Hyperglycemic Crises: Pathophysiology DKA HHS Hyperglycemia DKA HHS Umpierrez, In Shoemaker,
Vishwanath Pattan Endocrinology Wyoming Medical Center
 Vishwanath Pattan Endocrinology Wyoming Medical Center Disclosure Holdings in Tandem Non for this Training Introduction In the United States, 5 to 6 percent of pregnancies almost 250,000 women are affected
Vishwanath Pattan Endocrinology Wyoming Medical Center Disclosure Holdings in Tandem Non for this Training Introduction In the United States, 5 to 6 percent of pregnancies almost 250,000 women are affected
Chapter Goal. Learning Objectives 9/12/2012. Chapter 25. Diabetic Emergencies
 Chapter 25 Diabetic Emergencies Chapter Goal Use assessment findings to formulate field impression & implement treatment plan for patients with diabetic emergencies Learning Objectives Describe pathophysiology
Chapter 25 Diabetic Emergencies Chapter Goal Use assessment findings to formulate field impression & implement treatment plan for patients with diabetic emergencies Learning Objectives Describe pathophysiology
Diabetes in Pregnancy
 Diabetes in Pregnancy Susan Drummond RN MSN C-EFM Objectives 1. Describe types of diabetes and diagnosis of gestational diabetes 2. Identify a management plan for diabetes during pregnancy 3. Describe
Diabetes in Pregnancy Susan Drummond RN MSN C-EFM Objectives 1. Describe types of diabetes and diagnosis of gestational diabetes 2. Identify a management plan for diabetes during pregnancy 3. Describe
A S Y N T H E S I Z E D H A N D B O O K ON G E S T A T I O N A L D I A B E T E S
 A S Y N T H E S I Z E D H A N D B O O K ON G E S T A T I O N A L D I A B E T E S P R E F A C E Dear reader, This is a synthesized handbook conceived to serve as a tool to health personnel in the screening,
A S Y N T H E S I Z E D H A N D B O O K ON G E S T A T I O N A L D I A B E T E S P R E F A C E Dear reader, This is a synthesized handbook conceived to serve as a tool to health personnel in the screening,
Management of Gestational Diabetes
 Management of Gestational Diabetes A Diabetes risk assessment should be ascertained at the First prenatal visit. Low Risk: Early blood glucose screening is NOT routinely required if most of the following
Management of Gestational Diabetes A Diabetes risk assessment should be ascertained at the First prenatal visit. Low Risk: Early blood glucose screening is NOT routinely required if most of the following
Prevention and Management of Diabetes in Pregnancy
 Prevention and Management of Diabetes in Pregnancy Sridhar Chitturi Consultant Endocrinologist Royal Darwin Hospital Outline of the talk Diabetes in Pregnancy Spectrum Diagnostic criteria Why bother about
Prevention and Management of Diabetes in Pregnancy Sridhar Chitturi Consultant Endocrinologist Royal Darwin Hospital Outline of the talk Diabetes in Pregnancy Spectrum Diagnostic criteria Why bother about
CCRN/PCCN Review Course May 30, 2013
 A & P Review CCRN/PCCN Review Course May 30, 2013 Endocrine Anterior pituitary Growth hormone: long bone growth Thyroid stimulating hormone: growth, thyroid secretion Adrenocorticotropic hormone: growth,
A & P Review CCRN/PCCN Review Course May 30, 2013 Endocrine Anterior pituitary Growth hormone: long bone growth Thyroid stimulating hormone: growth, thyroid secretion Adrenocorticotropic hormone: growth,
AACN PCCN Review. Endocrine
 AACN PCCN Review Endocrine Presenter: Carol A. Rauen, RN, MS, CCNS, CCRN, PCCN, CEN Independent Clinical Nurse Specialist & Education Consultant rauen.carol104@gmail.com Endocrine I. INTRODUCTION Disorders
AACN PCCN Review Endocrine Presenter: Carol A. Rauen, RN, MS, CCNS, CCRN, PCCN, CEN Independent Clinical Nurse Specialist & Education Consultant rauen.carol104@gmail.com Endocrine I. INTRODUCTION Disorders
Diabetes and Pregnancy
 Diabetes and Pregnancy Dr Warren Gillibrand Deputy Director of Postgraduate Education Department of Nursing & Midwifery Department of AHP and Sports Science w.p.gillibrand@hud.ac.uk Aims of the session
Diabetes and Pregnancy Dr Warren Gillibrand Deputy Director of Postgraduate Education Department of Nursing & Midwifery Department of AHP and Sports Science w.p.gillibrand@hud.ac.uk Aims of the session
DIABETES MELLITUS. IAP UG Teaching slides
 DIABETES MELLITUS 1 DIABETES MELLITUS IN CHILDREN Introduction, Definition Classification, pathogenesis Clinical features Investigations and diagnosis Therapy and follow up Complications Carry home message
DIABETES MELLITUS 1 DIABETES MELLITUS IN CHILDREN Introduction, Definition Classification, pathogenesis Clinical features Investigations and diagnosis Therapy and follow up Complications Carry home message
Diabetes: The Effects of Maternal Diabetes on Fetal Development and Outcomes Sherrie McElvy, MD May 18, 2016
 Diabetes: The Effects of Maternal Diabetes on Fetal Development and Outcomes Sherrie McElvy, MD May 18, 2016 Medical Director Sweet Success Sutter Medical Center Sacramento Perinatal Associates of Sacramento
Diabetes: The Effects of Maternal Diabetes on Fetal Development and Outcomes Sherrie McElvy, MD May 18, 2016 Medical Director Sweet Success Sutter Medical Center Sacramento Perinatal Associates of Sacramento
Diabetic Ketoacidosis (DKA) Critical Care Guideline Two Bag System
 Critical Care Guideline Two Bag System") Critical Care Guideline Two Bag System Inclusion Criteria (Definition of DKA): Blood glucose (BG) > 200 mg/dl Acidosis (bicarbonate < 15 or blood gas ph < 7.3) Associated glycosuria, ketonuria &/or ketonemia
Critical Care Guideline Two Bag System Inclusion Criteria (Definition of DKA): Blood glucose (BG) > 200 mg/dl Acidosis (bicarbonate < 15 or blood gas ph < 7.3) Associated glycosuria, ketonuria &/or ketonemia
Hyperglycaemic Emergencies GRI EDUCATION
 Hyperglycaemic Emergencies GRI EDUCATION LEARNING OUTCOMES Develop and describe your system of blood gas interpretation and recognise common patterns of acid-base abnormality. Describe the pathophysiology
Hyperglycaemic Emergencies GRI EDUCATION LEARNING OUTCOMES Develop and describe your system of blood gas interpretation and recognise common patterns of acid-base abnormality. Describe the pathophysiology
Diabetes mellitus - diagnosis, classification and acute complications. David Karásek 3rd Department of Internal Medicine University Hospital Olomouc
 Diabetes mellitus - diagnosis, classification and acute complications David Karásek 3rd Department of Internal Medicine University Hospital Olomouc Diabetes mellitus is a group of metabolic diseases, characterized
Diabetes mellitus - diagnosis, classification and acute complications David Karásek 3rd Department of Internal Medicine University Hospital Olomouc Diabetes mellitus is a group of metabolic diseases, characterized
Metformin Hydrochloride
 Metformin Hydrochloride 500 mg, 850 mg, 500 mg LA and 750 mg LA Tablet Description Informet is a preparation of metformin hydrochloride that belongs to a biguanide class of oral antidiabetic drugs. Metformin
Metformin Hydrochloride 500 mg, 850 mg, 500 mg LA and 750 mg LA Tablet Description Informet is a preparation of metformin hydrochloride that belongs to a biguanide class of oral antidiabetic drugs. Metformin
9/11/2012. Chapter 11. Learning Objectives. Learning Objectives. Endocrine Emergencies. Differentiate type 1 and type 2 diabetes
 Chapter 11 Endocrine Emergencies Learning Objectives Differentiate type 1 and type 2 diabetes Explain roles of glucagon, glycogen, and glucose in hypoglycemia Learning Objectives Discuss following medications
Chapter 11 Endocrine Emergencies Learning Objectives Differentiate type 1 and type 2 diabetes Explain roles of glucagon, glycogen, and glucose in hypoglycemia Learning Objectives Discuss following medications
Diabetes in Pregnancy. L.Sekhavat MD
 Diabetes in Pregnancy L.Sekhavat MD Diabetes in Pregnancy Gestational Diabetes Pre-gestational diabetes (overt) Insulin dependent (type1) Non-insulin dependent (type 2) Definition Gestational diabetes
Diabetes in Pregnancy L.Sekhavat MD Diabetes in Pregnancy Gestational Diabetes Pre-gestational diabetes (overt) Insulin dependent (type1) Non-insulin dependent (type 2) Definition Gestational diabetes
I have no financial disclosures
 Athina Sikavitsas DO Children's Emergency Services University of Michigan Discuss DKA Presentation Assessment Treatment I have no financial disclosures 1 6 Y/O male presents with vomiting and abdominal
Athina Sikavitsas DO Children's Emergency Services University of Michigan Discuss DKA Presentation Assessment Treatment I have no financial disclosures 1 6 Y/O male presents with vomiting and abdominal
CommUnityCare Women s Health Brackenridge Professional Office Building
 Guidelines for Diabetes in Pregnancy Effective Date 7/1/11 *This document does not define a standard of care, nor is it intended to dictate an exclusive course of management. There are other accepted strategies
Guidelines for Diabetes in Pregnancy Effective Date 7/1/11 *This document does not define a standard of care, nor is it intended to dictate an exclusive course of management. There are other accepted strategies
Hypoglycemia, Sick Days/DKA and Hospitalization
 Hypoglycemia, Sick Days/DKA and Hospitalization General survival skills for your client with diabetes at home and in Hospital Diabetes Canada guidelines for your client with diabetes while they are in
Hypoglycemia, Sick Days/DKA and Hospitalization General survival skills for your client with diabetes at home and in Hospital Diabetes Canada guidelines for your client with diabetes while they are in
DIABETIC KETOACIDOSIS (DKA) K E M I A D E Y E R I, P G Y - 1
 K E M I A D E Y E R I, P G Y - 1") DIABETIC KETOACIDOSIS (DKA) K E M I A D E Y E R I, P G Y - 1 QUESTION # 1 7 year old boy comes to the ER with a 2 week history of abdominal pain and weight loss. Further history reveals polyuria and polydipsia,
DIABETIC KETOACIDOSIS (DKA) K E M I A D E Y E R I, P G Y - 1 QUESTION # 1 7 year old boy comes to the ER with a 2 week history of abdominal pain and weight loss. Further history reveals polyuria and polydipsia,
Multiple c hoice q uestions
 Multiple c hoice q uestions Chapter 1 1. The pathogenesis of hyperglycemia in diabetic ketoacidosis includes all the following mechanisms except for: a. Increased glycogenolysis in the liver b. Increased
Multiple c hoice q uestions Chapter 1 1. The pathogenesis of hyperglycemia in diabetic ketoacidosis includes all the following mechanisms except for: a. Increased glycogenolysis in the liver b. Increased
Diabetic Emergencies. Chapter 15
 Diabetic Emergencies Chapter 15 Diabetes- is a disorder of glucose metabolism or difficulty metabolizing carbohydrates, fats and proteins Full name is diabetes mellitus which refers to the presence of
Diabetic Emergencies Chapter 15 Diabetes- is a disorder of glucose metabolism or difficulty metabolizing carbohydrates, fats and proteins Full name is diabetes mellitus which refers to the presence of
diabetes in adults Metabolic complications of
 Metabolic complications of diabetes in adults Dimitri MARGETIS MD ICU St ANTOINE PARIS Definition Diabetic acidoketosis Serious complication in type I diabetes : Hyperglycemia Metabolic acidosis Acidic
Metabolic complications of diabetes in adults Dimitri MARGETIS MD ICU St ANTOINE PARIS Definition Diabetic acidoketosis Serious complication in type I diabetes : Hyperglycemia Metabolic acidosis Acidic
Diabetes in Pregnancy Registrar Induction. Dr Anna Dover August 31 st 2015
 Diabetes in Pregnancy Registrar Induction Dr Anna Dover August 31 st 2015 Outline Joint Antenatal Diabetes Service Pre-existing diabetes Pre-conception, antenatal management Gestational Diabetes Screening,
Diabetes in Pregnancy Registrar Induction Dr Anna Dover August 31 st 2015 Outline Joint Antenatal Diabetes Service Pre-existing diabetes Pre-conception, antenatal management Gestational Diabetes Screening,
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
Objectives. Why is blood glucose important? Hypoglycaemia. Hyperglycaemia. Acute Diabetes Emergencies (DKA,HONK)
") Acute Diabetes Emergencies Ross Buchan, DSN North Glasgow September 2017 Objectives Why is blood glucose important? Hypoglycaemia Hyperglycaemia Acute Diabetes Emergencies (DKA,HONK) Importance of Blood
Acute Diabetes Emergencies Ross Buchan, DSN North Glasgow September 2017 Objectives Why is blood glucose important? Hypoglycaemia Hyperglycaemia Acute Diabetes Emergencies (DKA,HONK) Importance of Blood
Cardiac Pathophysiology
 Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
Diagnosis and Management of Gestational Diabetes Mellitus. Prof. Dr Md Faizul Islam Chowdhury Professor of Medicine, Department of Medicine, DMCH.
 Diagnosis and Management of Gestational Diabetes Mellitus Prof. Dr Md Faizul Islam Chowdhury Professor of Medicine, Department of Medicine, DMCH. Gestational Diabetes Mellitus I, the Fetus I, the fetus
Diagnosis and Management of Gestational Diabetes Mellitus Prof. Dr Md Faizul Islam Chowdhury Professor of Medicine, Department of Medicine, DMCH. Gestational Diabetes Mellitus I, the Fetus I, the fetus
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: Endocrine Revised: 11/2013
 Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: Endocrine Revised: 11/2013 Endocrine system includes 8 major glands. 1. Pituitary (master gland)
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: Endocrine Revised: 11/2013 Endocrine system includes 8 major glands. 1. Pituitary (master gland)
Diabetes Mellitus (DM) Chronic metabolic disorder with a predisposition of hyperglycaemia (increased blood glucose).
 Chronic metabolic disorder with a predisposition of hyperglycaemia (increased blood glucose).") DIABETES WHAT IS DIABETES? Diabetes Mellitus (DM) Chronic metabolic disorder with a predisposition of hyperglycaemia (increased blood glucose). Diabetes Insipidus (DI) Condition in which the body has lack
DIABETES WHAT IS DIABETES? Diabetes Mellitus (DM) Chronic metabolic disorder with a predisposition of hyperglycaemia (increased blood glucose). Diabetes Insipidus (DI) Condition in which the body has lack
Highlighting the Differences between Preexisting Type 1 and Type 2 Diabetes in Pregnancy and Gestational Diabetes
 Highlighting the Differences between Preexisting Type 1 and Type 2 Diabetes in Pregnancy and Gestational Diabetes Elizabeth (Libby) Downs Quiroga, MS, RD, CDE Tandem Diabetes Care Clinical Specialist Grand
Highlighting the Differences between Preexisting Type 1 and Type 2 Diabetes in Pregnancy and Gestational Diabetes Elizabeth (Libby) Downs Quiroga, MS, RD, CDE Tandem Diabetes Care Clinical Specialist Grand
Gestational Diabetes. Gestational Diabetes:
 Gestational Diabetes Detection and Management Steven Gabbe, MD The Ohio State University Medical Center Gestational Diabetes: Detection and Management Learning Objectives: At the conclusion of this presentation,
Gestational Diabetes Detection and Management Steven Gabbe, MD The Ohio State University Medical Center Gestational Diabetes: Detection and Management Learning Objectives: At the conclusion of this presentation,
Pregestational and Gestational Diabetes
 Pregestational and Gestational Diabetes Francis S. Nuthalapaty, MD Greenville Health System University of South Carolina School of Medicine - Greenville Case History 30 year old black female presents to
Pregestational and Gestational Diabetes Francis S. Nuthalapaty, MD Greenville Health System University of South Carolina School of Medicine - Greenville Case History 30 year old black female presents to
Objectives. Why is blood glucose important? Hypoglycaemia. Hyperglycaemia. Acute Diabetes Emergencies (DKA,HONK)
") Acute Diabetes Emergencies Ross Buchan, DSN North Glasgow June 2017 Objectives Why is blood glucose important? Hypoglycaemia Hyperglycaemia Acute Diabetes Emergencies (DKA,HONK) Importance of Blood Glucose
Acute Diabetes Emergencies Ross Buchan, DSN North Glasgow June 2017 Objectives Why is blood glucose important? Hypoglycaemia Hyperglycaemia Acute Diabetes Emergencies (DKA,HONK) Importance of Blood Glucose
1/3/2008. Karen Burke Priscilla LeMone Elaine Mohn-Brown. Medical-Surgical Nursing Care, 2e Karen Burke, Priscilla LeMone, and Elaine Mohn-Brown
 Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 17 Caring for Clients with Diabetes Mellitus Diabetes Mellitus Chronic disease Not a single disorder
Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 17 Caring for Clients with Diabetes Mellitus Diabetes Mellitus Chronic disease Not a single disorder
Medical Complications of Pregnancy
 Medical Complications of Pregnancy Systems Cardiovascular Pulmonary Endocrine Gastrointestinal Urologic Neurologic Cardiovascular System Physiologic anemia 3:1 increase of plasma volume:rbc mass Treat
Medical Complications of Pregnancy Systems Cardiovascular Pulmonary Endocrine Gastrointestinal Urologic Neurologic Cardiovascular System Physiologic anemia 3:1 increase of plasma volume:rbc mass Treat
Diabetes and pregnancy. diabetes. and. pregnancy
 Diabetes and pregnancy i diabetes and pregnancy www.glucomen.co.uk Diabetes and Pregnancy Diabetes is a medical condition where there is too much sugar (glucose) in the bloodstream. Glucose is the main
Diabetes and pregnancy i diabetes and pregnancy www.glucomen.co.uk Diabetes and Pregnancy Diabetes is a medical condition where there is too much sugar (glucose) in the bloodstream. Glucose is the main
INTRAVENOUS FLUID THERAPY
 INTRAVENOUS FLUID THERAPY PRINCIPLES Postnatal physiological weight loss is approximately 5 10% in first week of life Preterm neonates have more total body water and may lose 10 15% of their weight in
INTRAVENOUS FLUID THERAPY PRINCIPLES Postnatal physiological weight loss is approximately 5 10% in first week of life Preterm neonates have more total body water and may lose 10 15% of their weight in
What is Diabetes Mellitus?
 Normal Glucose Metabolism What is Diabetes Mellitus? When the amount of glucose in the blood increases, After a meal, it triggers the release of the hormone insulin from the pancreas. Insulin stimulates
Normal Glucose Metabolism What is Diabetes Mellitus? When the amount of glucose in the blood increases, After a meal, it triggers the release of the hormone insulin from the pancreas. Insulin stimulates
1st Department of Obstetrics and Gynecology, Alexandra Maternity Hospital, National and Kapodistrian University of Athens, Athens, Greece.
 HJOG An Obstetrics and Gynecology International Journal HJOG 2019, 18 (1), 21-25 Christos Kalantzis, Kalliopi Pappa 1st Department of Obstetrics and Gynecology, Alexandra Maternity Hospital, National and
HJOG An Obstetrics and Gynecology International Journal HJOG 2019, 18 (1), 21-25 Christos Kalantzis, Kalliopi Pappa 1st Department of Obstetrics and Gynecology, Alexandra Maternity Hospital, National and
Anne Leake, PhD, APRN, BC-ADM ECHO Diabetes Learning Group 4/4/18. High Sugar / Hyperglycemia: Causes, Complications and Management
 Anne Leake, PhD, APRN, BC-ADM ECHO Diabetes Learning Group 4/4/18 High Sugar / Hyperglycemia: Causes, Complications and Management Case Presentation A 45 year old obese man comes to your clinic with a
Anne Leake, PhD, APRN, BC-ADM ECHO Diabetes Learning Group 4/4/18 High Sugar / Hyperglycemia: Causes, Complications and Management Case Presentation A 45 year old obese man comes to your clinic with a
Diabetes in Pregnancy Registrar Induction Programme. Dr Anna Dover August 29 th 2016
 Diabetes in Pregnancy Registrar Induction Programme Dr Anna Dover August 29 th 2016 Diabetes in pregnancy Why it matters What our service looks like How we diagnose and manage GDM Patients with pre-existing
Diabetes in Pregnancy Registrar Induction Programme Dr Anna Dover August 29 th 2016 Diabetes in pregnancy Why it matters What our service looks like How we diagnose and manage GDM Patients with pre-existing
Managing Diabetes Before, During, and After Pregnancy
 Managing Diabetes Before, During, and After Pregnancy This program is supported by an educational grant from Novo Nordisk Inc. It has been accredited by AADE for pharmacists, nurses, and dietitians. This
Managing Diabetes Before, During, and After Pregnancy This program is supported by an educational grant from Novo Nordisk Inc. It has been accredited by AADE for pharmacists, nurses, and dietitians. This
10. ACUTE COMPLICATIONS OF DIABETES MELLITUS
 10. ACUTE COMPLICATIONS OF DIABETES MELLITUS Prof. Oren Zinder, Ph.D. Rambam Medical Center, and the Technion Faculty of Medicine, Haifa, Israel 1.1. Hypoglycaemia Hypoglycaemia is a lowered blood glucose
10. ACUTE COMPLICATIONS OF DIABETES MELLITUS Prof. Oren Zinder, Ph.D. Rambam Medical Center, and the Technion Faculty of Medicine, Haifa, Israel 1.1. Hypoglycaemia Hypoglycaemia is a lowered blood glucose
Diabetes in pregnancy
 Issue date: March 2008 Diabetes in pregnancy Management of diabetes and its complications from pre-conception to the postnatal period Developed by the National Collaborating Centre for Women s and Children
Issue date: March 2008 Diabetes in pregnancy Management of diabetes and its complications from pre-conception to the postnatal period Developed by the National Collaborating Centre for Women s and Children
SARASOTA MEMORIAL HOSPITAL NURSING PROCEDURE
 SARASOTA MEMORIAL HOSPITAL NURSING PROCEDURE TITLE: ISSUED FOR: DKA / HHNS PATIENTS REQUIRING INTRAVENOUS INSULIN DRIPS -ADULTS Nursing DATE: REVIEWED: PAGES: 12/14 5/18 1 of 8 RESPONSIBILITY: *RN (Renal/Diabetes/Wound
SARASOTA MEMORIAL HOSPITAL NURSING PROCEDURE TITLE: ISSUED FOR: DKA / HHNS PATIENTS REQUIRING INTRAVENOUS INSULIN DRIPS -ADULTS Nursing DATE: REVIEWED: PAGES: 12/14 5/18 1 of 8 RESPONSIBILITY: *RN (Renal/Diabetes/Wound
Diabetic Ketoacidosis
 October 2015 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Case History HPI: 24 yo man with recent 8 lb. weight loss, increased thirst and frequent
October 2015 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Case History HPI: 24 yo man with recent 8 lb. weight loss, increased thirst and frequent
Gestational Diabetes. Benjamin Byers, D.O., FACOG Center for Maternal and Fetal Care Bryan Physician Network
 Gestational Diabetes Benjamin Byers, D.O., FACOG Center for Maternal and Fetal Care Bryan Physician Network Outline Definition Prevalence Risk factors complications Diagnosis Management Nonpharmacologic
Gestational Diabetes Benjamin Byers, D.O., FACOG Center for Maternal and Fetal Care Bryan Physician Network Outline Definition Prevalence Risk factors complications Diagnosis Management Nonpharmacologic
Type 1 Diabetes-Pathophysiology, Diagnosis, and Long-Term Complications. Alejandro J de la Torre Pediatric Endocrinology 10/17/2014
 Type 1 Diabetes-Pathophysiology, Diagnosis, and Long-Term Complications Alejandro J de la Torre Pediatric Endocrinology 10/17/2014 Objectives Understand the pathophysiology of Type 1 diabetes. Be familiar
Type 1 Diabetes-Pathophysiology, Diagnosis, and Long-Term Complications Alejandro J de la Torre Pediatric Endocrinology 10/17/2014 Objectives Understand the pathophysiology of Type 1 diabetes. Be familiar
DIABETES 20/02/2014 WHAT IS DIABETES? GLUCOSE WHAT IS DIABETES? GLUCOSE HOMEOSTASIS GLUCOSE METABOLISM
 WHAT IS DIABETES? DIABETES Diabetes Mellitus (DM) Chronic metabolic disorder with a predisposition of hyperglycaemia (increased blood glucose). Diabetes Insipidus (DI) Condition in which the body has lack
WHAT IS DIABETES? DIABETES Diabetes Mellitus (DM) Chronic metabolic disorder with a predisposition of hyperglycaemia (increased blood glucose). Diabetes Insipidus (DI) Condition in which the body has lack
Complete Comprehensive Diabetes Educator modules available at CCCEP File #: I-P (Expires: Mar.
 CDE Preparation Program Topics (Accredited by CCCEP for 0.5 CEUs/Module section Total = 20 CEUs) Module 1 Pathophysiology of Diabetes 5 segments Module 2 Diabetes and Nutrition 5 segments Module 3 Medications
CDE Preparation Program Topics (Accredited by CCCEP for 0.5 CEUs/Module section Total = 20 CEUs) Module 1 Pathophysiology of Diabetes 5 segments Module 2 Diabetes and Nutrition 5 segments Module 3 Medications
Improving Outcomes in Pregnancies Complicated by Diabetes Mellitus
 Improving Outcomes in Pregnancies Complicated by Diabetes Mellitus Steven G. Gabbe, M.D. Emeritus Chief Executive Officer Professor, Obstetrics and Gynecology The Ohio State University Wexner Medical Center
Improving Outcomes in Pregnancies Complicated by Diabetes Mellitus Steven G. Gabbe, M.D. Emeritus Chief Executive Officer Professor, Obstetrics and Gynecology The Ohio State University Wexner Medical Center
Objectives. Medical Complications of Pregnancy. Potential Conflicts: None. Common Complicating Medical Conditions that Precede Pregnancy
 Medical Complications of Potential Conflicts: None Ellen W. Seely, M.D. Director of Clinical Research Endocrine-Hypertension Division Brigham and Women s Hospital Professor of Medicine Harvard Medical
Medical Complications of Potential Conflicts: None Ellen W. Seely, M.D. Director of Clinical Research Endocrine-Hypertension Division Brigham and Women s Hospital Professor of Medicine Harvard Medical
CBT/OTEP 450 Diabetic Emergencies
 Seattle-King County EMS Emergency Medical Services Division Public Health - Seattle/King County 999 3 rd Avenue, Suite 700 Seattle, Washington 98104 (206) 296-4863 January 2006 CBT/OTEP 450 print version
Seattle-King County EMS Emergency Medical Services Division Public Health - Seattle/King County 999 3 rd Avenue, Suite 700 Seattle, Washington 98104 (206) 296-4863 January 2006 CBT/OTEP 450 print version
2/13/2018. Update on Gestational Diabetes. Disclosure. Objectives. I have no financial conflicts of interest.
 Update on Gestational Diabetes Lorie M. Harper, MD, MSCI Department of Obstetrics & Gynecology Division of Maternal-Fetal Medicine 2/18/2018 Disclosure I have no financial conflicts of interest. Objectives
Update on Gestational Diabetes Lorie M. Harper, MD, MSCI Department of Obstetrics & Gynecology Division of Maternal-Fetal Medicine 2/18/2018 Disclosure I have no financial conflicts of interest. Objectives
Maximizing the Role of WIC Nutritionists in Prevention of DM2 among High Risk Clients ESTHER G. SCHUSTER, MS,RD,CDE
 Maximizing the Role of WIC Nutritionists in Prevention of DM2 among High Risk Clients ESTHER G. SCHUSTER, MS,RD,CDE Heavy Numbers Surgeon General report: 68% of adults in U. S. are overweight or obese
Maximizing the Role of WIC Nutritionists in Prevention of DM2 among High Risk Clients ESTHER G. SCHUSTER, MS,RD,CDE Heavy Numbers Surgeon General report: 68% of adults in U. S. are overweight or obese
COMPLICATIONS OF PRE-GESTATIONAL AND GESTATIONAL DIABETES IN SAUDI WOMEN: ANALYSIS FROM RIYADH MOTHER AND BABY COHORT STUDY (RAHMA)
") COMPLICATIONS OF PRE-GESTATIONAL AND GESTATIONAL DIABETES IN SAUDI WOMEN: ANALYSIS FROM RIYADH MOTHER AND BABY COHORT STUDY (RAHMA) Prof. Hayfaa Wahabi, King Saud University, Riyadh Saudi Arabia Hayfaa
COMPLICATIONS OF PRE-GESTATIONAL AND GESTATIONAL DIABETES IN SAUDI WOMEN: ANALYSIS FROM RIYADH MOTHER AND BABY COHORT STUDY (RAHMA) Prof. Hayfaa Wahabi, King Saud University, Riyadh Saudi Arabia Hayfaa
Infant Of Diabetic Mother(IDM)
") Infant Of Diabetic Mother(IDM) Sangram Satish Magar 1, Sanskriti Mirashi 2 1. M.D. Sch.(Kaumarbhrutya-Balrog) 2.Guide (Kaumarbhrutya-Balrog), L.R.P.Medical college,islampur,tal- Walwa, dist- Sangli, Maharashtra,
Infant Of Diabetic Mother(IDM) Sangram Satish Magar 1, Sanskriti Mirashi 2 1. M.D. Sch.(Kaumarbhrutya-Balrog) 2.Guide (Kaumarbhrutya-Balrog), L.R.P.Medical college,islampur,tal- Walwa, dist- Sangli, Maharashtra,
Hypertension The normal radial artery blood pressures in adults are: Systolic arterial pressure: 100 to 140 mmhg. Diastolic arterial pressure: 60 to
 Hypertension The normal radial artery blood pressures in adults are: Systolic arterial pressure: 100 to 140 mmhg. Diastolic arterial pressure: 60 to 90 mmhg. These pressures are called Normal blood pressure
Hypertension The normal radial artery blood pressures in adults are: Systolic arterial pressure: 100 to 140 mmhg. Diastolic arterial pressure: 60 to 90 mmhg. These pressures are called Normal blood pressure
National Aboriginal Diabetes Association. Gestational Diabetes (developed by Sarah Smith, 4 th yr Nursing, University of Manitoba)
") National Aboriginal Diabetes Association Gestational Diabetes (developed by Sarah Smith, 4 th yr Nursing, University of Manitoba) Who we are NADA is a not-for-profit members-led organization established
National Aboriginal Diabetes Association Gestational Diabetes (developed by Sarah Smith, 4 th yr Nursing, University of Manitoba) Who we are NADA is a not-for-profit members-led organization established
Diabetes in Pregnancy Dr. Hana
 Diabetes in Pregnancy Dr. Hana Introduction Diabetes occurs in 2 5% of all UK pregnancies and its prevalence is rising. Forty years ago the majority of women with diabetes attending an antenatal clinic
Diabetes in Pregnancy Dr. Hana Introduction Diabetes occurs in 2 5% of all UK pregnancies and its prevalence is rising. Forty years ago the majority of women with diabetes attending an antenatal clinic
Vinaya Simha, M.D. Assistant Professor, Division of Endocrinology
 Vinaya Simha, M.D. Assistant Professor, Division of Endocrinology Faculty photo will be placed here Simha.aj@mayo.edu 2015 MFMER 3543652-1 Diabetic Ketoacidosis a few pearls Mayo School of Continuous Professional
Vinaya Simha, M.D. Assistant Professor, Division of Endocrinology Faculty photo will be placed here Simha.aj@mayo.edu 2015 MFMER 3543652-1 Diabetic Ketoacidosis a few pearls Mayo School of Continuous Professional
Current Trends in Diagnosis and Management of Gestational Diabetes
 Current Trends in Diagnosis and Management of Gestational Diabetes Shreela Mishra, MD Assistant Clinical Professor UCSF Fresno Medical Education Program 2/2/2019 Disclosures No disclosures 2/2/19 Objectives
Current Trends in Diagnosis and Management of Gestational Diabetes Shreela Mishra, MD Assistant Clinical Professor UCSF Fresno Medical Education Program 2/2/2019 Disclosures No disclosures 2/2/19 Objectives
INTRAVENOUS FLUIDS PRINCIPLES
 INTRAVENOUS FLUIDS PRINCIPLES Postnatal physiological weight loss is approximately 5-10% Postnatal diuresis is delayed in Respiratory Distress Syndrome (RDS) Preterm babies have limited capacity to excrete
INTRAVENOUS FLUIDS PRINCIPLES Postnatal physiological weight loss is approximately 5-10% Postnatal diuresis is delayed in Respiratory Distress Syndrome (RDS) Preterm babies have limited capacity to excrete
Pediatric Diabetic Ketoacidosis (DKA) General Pediatrics Admission Order Set
 General Pediatrics Admission Order Set") Admitting MRP: Pediatrics: Dr. / Dr. on call to cover until 08:00 am Service: Medicine Team 1 Medicine Team 2 Medical subspecialty Diagnosis: Diabetic Ketoacidosis (DKA) Estimated length of stay Less than
Admitting MRP: Pediatrics: Dr. / Dr. on call to cover until 08:00 am Service: Medicine Team 1 Medicine Team 2 Medical subspecialty Diagnosis: Diabetic Ketoacidosis (DKA) Estimated length of stay Less than
DIABETIC KETOACIDOSIS
 DIABETIC KETOACIDOSIS DANA BARTLETT, BSN, MSN, MA, CSPI Dana Bartlett is a professional nurse and author. His clinical experience includes 16 years of ICU and ER experience and over 20 years of as a poison
DIABETIC KETOACIDOSIS DANA BARTLETT, BSN, MSN, MA, CSPI Dana Bartlett is a professional nurse and author. His clinical experience includes 16 years of ICU and ER experience and over 20 years of as a poison
The Hospitalized Child with Diabetes/Hyperglycemia: Don t Sugar Coat It
 The Hospitalized Child with Diabetes/Hyperglycemia: Don t Sugar Coat It Cassie Brady, MD Assistant Professor of Pediatrics Division of Endocrinology and Diabetes Monroe Carell Junior Children s Hospital
The Hospitalized Child with Diabetes/Hyperglycemia: Don t Sugar Coat It Cassie Brady, MD Assistant Professor of Pediatrics Division of Endocrinology and Diabetes Monroe Carell Junior Children s Hospital
Counseling and Long-term Follow up After Gestational Disorders
 Counseling and Long-term Follow up After Gestational Disorders Tanya Melnik, MD Assistant Professor, University of Minnesota Sarina Martini, MD Ob/Gyn Resident, PGY4 University of Minnesota Counseling
Counseling and Long-term Follow up After Gestational Disorders Tanya Melnik, MD Assistant Professor, University of Minnesota Sarina Martini, MD Ob/Gyn Resident, PGY4 University of Minnesota Counseling
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Diabetic Ketoacidosis. These podcasts are designed to give medical students an overview of key topics in pediatrics.
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Diabetic Ketoacidosis. These podcasts are designed to give medical students an overview of key topics in pediatrics.
Diabetes in Pregnancy
 Diabetes in Pregnancy Resident School November 5 2014 Goals Be able to screen for gestational and preexisting diabetes Be able to counsel women on the diagnosis of gestational diabetes Understand glucose
Diabetes in Pregnancy Resident School November 5 2014 Goals Be able to screen for gestational and preexisting diabetes Be able to counsel women on the diagnosis of gestational diabetes Understand glucose
Management of DM in Older Adults: It s not all about sugar! Who needs treatment for DM? Peggy Odegard, Pharm.D., BCPS, CDE
 Management of DM in Older Adults: It s not all about sugar! Peggy Odegard, Pharm.D., BCPS, CDE Who needs treatment for DM? 87 year old, frail male with moderately severe dementia living in NH with persistent
Management of DM in Older Adults: It s not all about sugar! Peggy Odegard, Pharm.D., BCPS, CDE Who needs treatment for DM? 87 year old, frail male with moderately severe dementia living in NH with persistent
Exercise for Special Populations
 Exercise for Special Populations Metabolic Problems Pregnancy Advancing Age Outline Exercise and metabolic problems Obesity Diabetes Type I and Type II Exercise during pregnancy Exercise in advancing age
Exercise for Special Populations Metabolic Problems Pregnancy Advancing Age Outline Exercise and metabolic problems Obesity Diabetes Type I and Type II Exercise during pregnancy Exercise in advancing age
Neonatal Hypoglycemia. Presented By : Kamlah Olaimat 25\7\2010
 Neonatal Hypoglycemia Presented By : Kamlah Olaimat 25\7\2010 Definition The S.T.A.B.L.E. Program defines hypoglycemia as: Glucose delivery or availability is inadequate to meet glucose demand (Karlsen,
Neonatal Hypoglycemia Presented By : Kamlah Olaimat 25\7\2010 Definition The S.T.A.B.L.E. Program defines hypoglycemia as: Glucose delivery or availability is inadequate to meet glucose demand (Karlsen,
Blood Glucose Monitoring
 Blood Glucose Monitoring What is Glucose? A simple sugar that enters the diet as part of sucrose, lactose, or maltose Part of a polysaccharide called dietary starch Most of the body s energy comes from
Blood Glucose Monitoring What is Glucose? A simple sugar that enters the diet as part of sucrose, lactose, or maltose Part of a polysaccharide called dietary starch Most of the body s energy comes from
Local Anesthesia for Dental Hygienists Session III. Altered Consciousness and Diabetes Michael E. O Brien, DDS and Frank S.
 Altered Consciousness in General Dr. Michael E. O Brien Dr. Frank S. Drongowski Definitions Confusion - a mental state marked by disturbances in comprehension, understanding, and resulting in bewilderment
Altered Consciousness in General Dr. Michael E. O Brien Dr. Frank S. Drongowski Definitions Confusion - a mental state marked by disturbances in comprehension, understanding, and resulting in bewilderment
CARBOHYDRATE METABOLISM Disorders
 CARBOHYDRATE METABOLISM Disorders molecular formula C12H22O11 Major index which describes metabolism of carbohydrates, is a sugar level in blood. In healthy people it is 4,4-6,6 mmol/l (70-110 mg/dl)
CARBOHYDRATE METABOLISM Disorders molecular formula C12H22O11 Major index which describes metabolism of carbohydrates, is a sugar level in blood. In healthy people it is 4,4-6,6 mmol/l (70-110 mg/dl)
Diabetes Mellitus Case Study
 COLORADO STATE UNIVERSITY Diabetes Mellitus Case Study Medical Nutrition Therapy By: Emily Lancaster 9/28/2012 [Type the abstract of the document here. The abstract is typically a short summary of the
COLORADO STATE UNIVERSITY Diabetes Mellitus Case Study Medical Nutrition Therapy By: Emily Lancaster 9/28/2012 [Type the abstract of the document here. The abstract is typically a short summary of the
Chapter 17. Endocrine and Hematologic Emergencies
 Chapter 17 Endocrine and Hematologic Emergencies Introduction (1 of 2) Endocrine system affects nearly every: Cell Organ Bodily function Endocrine disorders can have many signs and symptoms. Introduction
Chapter 17 Endocrine and Hematologic Emergencies Introduction (1 of 2) Endocrine system affects nearly every: Cell Organ Bodily function Endocrine disorders can have many signs and symptoms. Introduction
Lynda Astbury Lead Diabetes Specialist Nurse
 Lynda Astbury Lead Diabetes Specialist Nurse WARNING SIGNS AND SYMPTOMS Is patient Feeling unwell? Blood glucose level above 13mmol/L Or higher than the patients day to day readings (even if not eating)
Lynda Astbury Lead Diabetes Specialist Nurse WARNING SIGNS AND SYMPTOMS Is patient Feeling unwell? Blood glucose level above 13mmol/L Or higher than the patients day to day readings (even if not eating)
The Ever-Changing Approaches to Diabetes in Pregnancy
 The Ever-Changing Approaches to Diabetes in Pregnancy Kirsten E. Salmeen, MD Assistant Professor Obstetrics, Gynecology & Reproductive Sciences Maternal-Fetal Medicine I have nothing to disclose. Approaches
The Ever-Changing Approaches to Diabetes in Pregnancy Kirsten E. Salmeen, MD Assistant Professor Obstetrics, Gynecology & Reproductive Sciences Maternal-Fetal Medicine I have nothing to disclose. Approaches
A Study of Gestational Diabetes in Patients in a Tertiary Care Hospital in Hyderabad Telangana State, India
 International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 6 Number 10 (2017) pp. 2586-2590 Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2017.610.304
International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 6 Number 10 (2017) pp. 2586-2590 Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2017.610.304
Pregnancy outcomes in Korean women with diabetes
 Pregnancy outcomes in Korean women with diabetes Sung-Hoon Kim Department of Medicine, Cheil General Hospital & Women s Healthcare Center, Dankook University College of Medicine, Seoul, Korea Conflict
Pregnancy outcomes in Korean women with diabetes Sung-Hoon Kim Department of Medicine, Cheil General Hospital & Women s Healthcare Center, Dankook University College of Medicine, Seoul, Korea Conflict
Diabetes Related Disclosures
 Diabetes Related Disclosures Speakers Bureau Amylin Boehringer Ingelheim Eli Lilly Takeda Classification of Diabetes Diabetes Care January 2011 vol. 34 no. Supplement 1 S11-S61 Type 1 Diabetes Mellitus
Diabetes Related Disclosures Speakers Bureau Amylin Boehringer Ingelheim Eli Lilly Takeda Classification of Diabetes Diabetes Care January 2011 vol. 34 no. Supplement 1 S11-S61 Type 1 Diabetes Mellitus