Basal & GLP-1 Fixed Combination Use
|
|
|
- Antonia Sutton
- 5 years ago
- Views:
Transcription




1 Basal & GLP-1 Fixed Combination Use Michelle M. Mangual, MD Diplomate of the American board of Internal Medicine and Endocrinology, Diabetes and Metabolism San Juan City hospital
2 Learning Objectives o Brief description of T2DM pathogenesis o Guidelines approach to T2DM treatment according to ADA and AACE guidelines o Rationale for starting basal insulin o Role of GLP-1 Receptor agonists in the treatment of T2DM o Rationale for combining GLP-1 RAs with basal insulin o Basal insulin/glp-1 RAs fixed combination: clinical trials
 1994 2000 2015 No Data <14.0% 14.0% 17.9% 18.0% 21.9% 22.0% 25.9% > 26.")

3 Age-adjusted Prevalence of Obesity and Diagnosed Diabetes Among US Adults Obesity (BMI 30 kg/m 2 ) No Data <14.0% 14.0% 17.9% 18.0% 21.9% 22.0% 25.9% > 26.0% Diabetes No Data <4.5% 4.5% 5.9% 6.0% 7.4% 7.5% 8.9% >9.0% CDC s Division of Diabetes Translation. United States Surveillance System available at
4 % %

5 Relative -Cell Function, % Glucose, mg/dl Natural History of T2DM PPG Fasting glucose Insulin resistance β-cell failure Insulin level Diabetes, y PPG = postprandial plasma glucose. Adapted with permission from Bergenstal R et al. Endocrinology. Philadelphia, PA: WB Saunders Co; 2001:
6 Figure 1 First and second phase insulin release and corresponding glycaemia after an intravenous glucose challenge Jenssen, T. & Hartmann, A. (2015) Emerging treatments for post-transplantation diabetes mellitus Nat. Rev. Nephrol. doi: /nrneph Jenssen, T. & Hartmann, A. (2015) Emerging treatments for post-transplantation diabetes mellitus Nat. Rev. Nephrol. doi: /nrneph
7

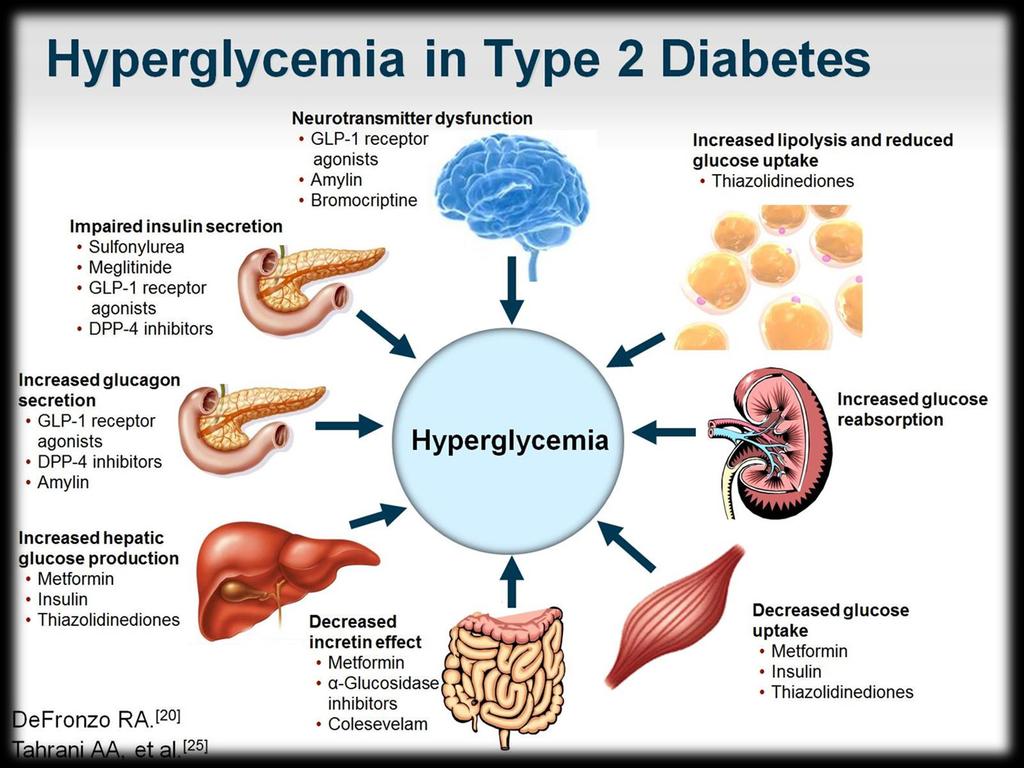
8 Pathogenesis of type 2 diabetes: Effective Tx of T2DM multiple drugs in combination to correct multiple pathophysiological defects. Tx should be based on known pathogenic abnormalities, Flexibility NOT SIMPLY on A1C Tx must be started early in the natural Hx of T2DM prevention of progressive β-cell failure. Implications for therapy
9
10
: S64-S74")
11 Antihyperglycemic Therapy in T2DM American Diabetes Association Standards of Medical Care in Diabetes. Approaches to glycemic treatment. Diabetes Care 2017; 40 (Suppl. 1): S64-S74


12 Glycemia Reduction Approaches in Diabetes: A Comparative Effectiveness Study To provide unbiased comparison of most commonly used drugs to Tx DM in metformin treated patients with relatively recentonset T2DM. To determine patient characteristics and mechanisms associated with differential responses to medications to facilitate individualization of diabetes care. To compare drugs over a clinically meaningful period of time (>4 years).


 N = 1250 GLP Analog (Liraglutide")
13 Screening T2DM Tx: Metformin alone A1C: 6.8% at screening < 10 year duration at screening Metformin Run-In Titrate Metformin to 1000(min) 2000 (goal) mg/dl A1C % at final run-in visit GRADE Design Randomization n = 5000 eligible subjects Sulfonylurea (Glimepiride) n = 1250 DPP-4 Inhibitor (Sitagliptin) N = 1250 GLP Analog (Liraglutide 1) N = 1250 Insulin (Glargine) N = 1250

 2 to 0.")
14 Rationale for Starting Basal Insulin Oral hypoglycemic agents no longer maintain control Adding basal insulin shown to entire 24-h fasting blood glucose profile 1 Suppression of overnight hepatic glucose production, through direct effects on the liver & indirect effects through suppression of free fatty release by adipose tissue Effective control with basal insulin added to oral hypoglycemic angents Requires: adequate dose titration Target A1c & Various studies: AVG doses of basal insulin from 0.33 units/kg BW (with insulin glargine) 2 to 0.78 units/kg (with insulin detemir) 3 If Titration is stopped at lower doses hypoglycemia improvement results from optimal glycemic control


15 Directly compared: once-daily bedtime insulin glargine vs once-daily NPH + oral hypoglycemic agents Insulin titration: Fasting <100 mg/dl When Basal Insulin is Not Enough Similar mean fasting blood glucose and HbA1c between groups 42% of patients treated with basal insulin and oral agents did not achieved target HbA1c <7.0% 6 years after initiation of basal insulin 24% of patients needed additional short-acting insulin to limit hyperglycemia following meals Treat to Target trial UKPDS
16

17 Combination Injectable Therapy in T2DM American Diabetes Association Standards of Medical Care in Diabetes. Approaches to glycemic treatment. Diabetes Care 2017; 40 (Suppl. 1): S64-S74



18 Adding Prandial Insulin Disadvantages Weight gain Hypoglycemia Challenge for patients Advantages What if we could reduce risk of hypoglycemia, weight gain and regimen complexity in many or most patients? Effectively achieve glycemic control Greater flexibility for patients
19 Rationale for Combining GLP-1 RAs with Basal Insulin














20 Exenatide Is Not Inactivated by DPP-4


21 GLP-1 Modulates Numerous Functions in Humans GLP-1: Secreted upon the ingestion of food Promotes satiety and reduces appetite Alpha cells: Glucose-dependent postprandial glucagon secretion Beta cells: Enhances glucosedependent insulin secretion Liver: Glucagon reduces hepatic glucose output Stomach: Helps regulate gastric emptying Data from Flint A, et al. J Clin Invest 1998;101: Data from Larsson H, et al. Acta Physiol Scand 1997;160: Data from Nauck MA, et al. Diabetologia 1996;39: Data from Drucker DJ. Diabetes 1998;47:
22 Potential benefits of combining insulin with GLP-1 RAs GLP-1 based therapies Basal insulin therapy Insulin secretion (glucose dependant) Glucagon secretion Body weight PPG/FPG Low risk of hypoglycemia Insulin levels (non-insulin dependant) Beta cell rest Body weight FPG/PPG Moderate risk of hypoglycemia Potentially complementary benefits if used in combination
23 GLP-1 Release is Reduced in Type 2 Diabetes *P<0.05 between type 2 diabetes and NGT groups NGT (n=33) IGT (n=15) Type 2 diabetes (n=54) From: Determinants of the Impaired Secretion of Glucagon-Like Peptide-1 in Type 2 Diabetic Patients J Clin Endocrinol Metab. 2001;86(8): doi: /jcem








24 Lixisenatide the number of apoptotic β cells by 50-60% An 80% reduction was seen with lixi + Glargine 1 Stimulation of insulin secretion Increase β-cell mass Effect of the GLP-1 on the β- cell Stimulation of insulin gene transcription Stimulation of insulin synthesis 1. TEWS D, ET AL. HORM METAB RES 2008; 40(3):
25 Comparison of physiologic effects of short-acting and long acting GLP-1 RAs. GIORGINO F, ET AL. DIABETES METAB RES REV 2016; 32:
 2 Lixisenatide QD vs Liraglutide QD 3 Greater reduction in PPG with BID Greater reductions in FPG and HbA1c with lira Greater reduction in PPG with lixi Greater delay of gastric emptying with")
26 Differences in mechanism of action and clinical profiles between short-acting and long-acting GLP-1 RAs: Headto-head studies Exenatide BID vs QW 1 Liraglutide QD vs Exenatide BID (added to Met, SU or both) 2 Lixisenatide QD vs Liraglutide QD 3 Greater reduction in PPG with BID Greater reductions in FPG and HbA1c with lira Greater reduction in PPG with lixi Greater delay of gastric emptying with BID Greater reduction in PPG with exenatide Greater reductions in PP glucagon and insulin with lixi Greater reduction in FPG and HbA1c with QW 1. DRUCKER DJ, ET AL. LANCET 2008; 372(9645): BUSE JB, ET AL. LEAD-6. LANCET 2009; 374(9683): KAPITZA C, ET AL. DIABETES OBES METAB 2013; 15(7):
 2 Greater reduction in PPG with lixi No difference in A1c Delayed gastric emptying and glucagon")
: 1263-1273. 2. Wysham C, et al. AWARD-1.")
27 Differences in mechanism of action and clinical profiles between short-acting and long-acting GLP-1 RAs: Head-to-head studies Lixi QD vs Lira QD as addon to basal insulin 1 Dulaglutide QW vs Exenetide BID (added to Met and pio) 2 Greater reduction in PPG with lixi No difference in A1c Delayed gastric emptying and glucagon suppression with lixi Increased insulin release with lira Greater reduction in A1c with dulaglutide Greater reduction in prandial glucose excursions with exenatide Greater reduction in FPG and overall hyperglycemia with dulaglutide 1. Meier JJ, et al. Diabetes Care 2015; 38(7): Wysham C, et al. AWARD-1. Diabetes Care 2014; 37(8):
28 Glycemic parameters from clinical studies combining GLP-1 RAs and basal insulin Giorgino F, et al. Diabetes Metab Res Rev 2016; 32:
29 Meta-analysis showing the likelihood of patients reaching the composite endpoint of HbA1c <7% with no symptomatic hypoglycemia and no weight gain Giorgino F, et al. Diabetes Metab Res Rev 2016; 32:
30 Fixed-Combination Products Available ideglira 1 dose steps= 1 unit of insulin degludec mg of liraglutide 16 dose steps= 16 units of insulin degludec mg of liraglutide 32 dose steps= 32 units of insulin degludec mg of liraglutide 50 dose steps= 50 units of insulin degludec mg of liraglutide LixiLan 2 units of insulin glargine + 1 mcg lixisenatide 10 units of glargine + 5 mcg lixisenatide 60 units of glargine + 30 mcg lixisenatide

31 IDegLira Clinical Trials: Summary of Trial Designs DUAL 1 DUAL II DUAL III DUAL IV DUAL V
 Inclusion Criteria Type 2 diabetes SU ± metformin")
")

32 DUAL IV: IDegLira vs Placebo Study Design Subjects with type 2 diabetes (N=435) Inclusion Criteria Type 2 diabetes SU ± metformin HbA1c % Age 18 years BMI 40 kg/m 2 IDegLira + SU ± metformin (n=289) Placebo + SU ± metformin (n=146) IDegLira/Placebo: Starting Dose: 10 dose steps Maximum Dose: 50 dose steps Titrate to target FPG 4-6 mmol/l ( mg/dl) Rodbard HW, et al. Diabetes 2015; 64
33 DUAL IV: HbA1c over time Mean observed values with error bars (standard error mean) based on full analysis set and last observation carried forward imputed data. Treatment difference estimated using ANCOVA model on full analysis set and last observation carried forward. RODBARD HW, ET AL. DIABETES 2015; 64

34 DUAL IV: 9-point SMBG profile Greater reduction in mean 9-P SMBG profile with IDegLira vs Placebo Treatment difference mg/dl, P<0.001 *p<0.05 based on lineal mixed model with an unstructured residual covariance matrix. Mean observed values based on full analysis set and last observation carried forward imputed data. Rodbard HW, et al. Diabetes 2015; 64
35 DUAL IV: Change in body weight over time Mean observed values with error bars (SEM) based on FAS and LOCF imputed data. Treatment difference estimated using an ANCOVA model. ETD [95% CI], *P < RODBARD HW, ET AL. DIABETES 2015; 64
36 DUAL IV: Confirmed hypoglycemia Severe Confirmed % Subjects (# subjects) 0.7% (2/288) 41.7% (120/288) IDegLira (n=288) Rate (Episodes/PYE) % Subjects (# subjects) Placebo (n=146) Rate (Episodes/PYE) % (25/146) 1.35* End-of-trial HbA1c: IDegLira 6.4% Placebo 7.4% *P< for IDegLira vs Placebo Data based on safety analysis set. Estimated treatment ratios are from a negative binomial model. %, percentage of participants; N, number of participants with 1 event. RODBARD HW, ET AL. DIABETES 2015; 64
37 DUAL I: IDegLira vs IDeg vs Liraglutide Patients with type 2 diabetes (n=1663) IDegLira OD ⱡ + metformin ± pioglitazone (n=834) IDeg OD ⱡ + metformin ± pioglitazone (n=414) Liraglutide OD (1.8 mg) + metformin ± pioglitazone (n=415) 0 26 weeks Titration algorithm: IDegLira and IDeg Mean Fasting PG Dose Change mg/dl mmol/l Dose steps or U <72 < >90 > Randomized 2:1:1 Open label Inclusion Criteria Type 2 Diabetes Insulin naïve-treated with metformin ± pioglitazone HbA1c % BMI 40 kg/m 2 Age 18 years* *Singapore age >21 years GOUGH, BODE ET AL. LANCET DIAB ENDO 2014

38 DUAL I: IDegLira vs IDeg vs Liraglutide Mean Daily Doses 53 U 38 U 1.8 μg 1.4 μg Gough, Bode Et al. Lancet Diab Endo 2014
39 DUAL I: IDegLira vs IDeg vs Liraglutide HbA1 over time GOUGH, BODE ET AL. LANCET DIAB ENDO 2014
40 % of Subjects DUAL I: IDegLira vs IDeg vs Liraglutide Percentage of subjects to target Liraglutide (n=414) IDeg (n=413) IDegLira (n=833) p< p< p< HbA1c < 7.0% HbA1c < 6.5% p< Gough, Bode Et al. Lancet Diab Endo 2014
41 DUAL I: 9-point SMBG: Post-prandial PG increment
42 DUAL I: Change in body weight over time kg (p < ) 2.44 kg (p < ) GOUGH, BODE ET AL. LANCET DIAB ENDO 2014
43 DUAL I: Rate of confirmed hypoglycemia by HbA1c GOUGH, BODE ET AL. LANCET DIAB ENDO 2014
44 DUAL I: Nausea over time Gough, Bode Et al. Lancet Diab Endo 2014
45 DUAL II: IDegLira vs Degludec in patients on basal insulin 199 patients per group Glycemic efficacy, insulin dose, body weight, and AEs. Data are means (SE). John B. Buse et al. Dia Care 2014;37:

. JOHN B. BUSE ET AL.")
46 DUAL II: IDegLira vs Degludec in patients on basal insulin Mean 9-point self-monitored blood glucose profiles at baseline (dotted line) and after 26 weeks (full line). JOHN B. BUSE ET AL. DIA CARE 2014;37:
47 DUAL III: IDegLira vs unchanged GLP-1 RA Study Design Insulin naïve patients with T2DM (n=438) IDegLira + metformin ± pio ± SU (n=292) Unchanged GLP-1 RA + metformin (n=146) Week Randomized 2:1 End of trial Follow up IDegLira Starting dose: 16 dose steps (16 U IDeg mg liraglutide Maximum dose: 50 dose steps (50 U IDeg and 1.8 mg liraglutide Inclusion Criteria Type 2 diabetes GLP-1 RA max dose + met ± pio ± SU HbA1c % Age 18 years BMI 40 kg/m 2 Mean Fasting PG Titration Dose Change mg/dl mmol/l Dose steps/u <72 < >90 > LINJAWI S, ET AL.DIABETES THER (2017) 8:
48 DUAL III: IDegLira vs unchanged GLP-1 RA HbA1c over time Mean observed values with error bars (standard error of the mean) based on FAS and LOCF imputed data. ETD is from ANCOVA analysis, and change in HbA1c (D) values are observed; both are based on FAS and LOCF imputed data. Dotted lines represent ADA/EASD and AACE HbA1c targets of 7.0% and 6.5%, respectively. LINJAWI S, ET AL.DIABETES THER (2017) 8:
49 DUAL III: IDegLira vs unchanged GLP-1 RA FPG over time (-47.6 mg/dl) LINJAWI S, ET AL.DIABETES THER (2017) 8:
50 DUAL III: IDegLira vs unchanged GLP-1 RA Change in body weight over time LINJAWI S, ET AL.DIABETES THER (2017) 8:
51 DUAL III: IDegLira vs unchanged GLP-1 RA 9-point SMBG profile Greater reduction in mean 9-P SMBG profile with IDegLira versus GLP-1 RA Treatment difference: <32 mg/dl, P<0.001 Linjawi S, et al.diabetes Ther (2017) 8: *p<0.001 (post hoc analysis).

52 DUAL Studies: IDegLira Fixed Dose Combination vs Comparators Better efficacy, ie HbA1c lower than either idegludec, liraglutide or other basal insulin Lower insulin doses than basal insulin comparators Shorter time to max insulin dose Less titration steps Less hypoglycemia than insulin comparators Less weight gain than insulin comparators More weight gain than GLP-1 comparator
53 LixiLan Proof of Concept Lixilan vs iglargine in insulin Naïve T2DM Patients Parameter LixiLan iglargine Baseline HbA1c 8.1 ± 0.8% 8.0 ± 0.8% Week 26 HbA1c 6.3% 6.5% Final daily insulin doses 36 Units 39 Units Symptomatic hypoglycemia 21.7% 22.8% Nausea 15.5% 9.3% AEs leading to discontinuation 3.7% 0 ROSENSTOCK J, ET AL. DIABETES CARE 2016
 Lixisenatide + Glargine + metformin (n=161) LixiLan Glargine Lixisenatide Fixed ratio 2 U 1 μg Initial dose 10 U 5 μg Max dose 60 U 10")
54 LixiLan Proof of Concept: Study Design Inclusion Criteria Type 2 Diabetes Metformin 1500 mg/day A1c 7.0 and 10.0% BMI >20 and 40 kg/m 2 R Insulin Glargine + metformin (n=162) Lixisenatide + Glargine + metformin (n=161) LixiLan Glargine Lixisenatide Fixed ratio 2 U 1 μg Initial dose 10 U 5 μg Max dose 60 U 10 μg Titration Target: FPG mg/dl Insulin Glargine dose no upper limit LixiLan capped at 60 U / 30 μg ROSENSTOCK J, ET AL. DIABETES CARE 2016
55 GetGoal Duo 2 Trial Lixisenatide + Basal Insulin vs Insulin Glulisine either as basal-plus or basal-bolus in T2DM Entry criteria: patients with T2DM on OAD + basal insulin 298 patients per group Lixisenatide 20 mcg once daily Insulin glulisine once daily Insulin glulisine 3x daily Screening HbA1c 8.5%, after run-in, % Insulin glargine dose: screening units, after run-in, units ROSENSTOCK J, ET AL. DIABETES CARE 2016; 39:
56 GetGoal-2 Trial: Results Parameter Lixi 20 μg daily iglulisine 1x iglulisine 3x HbA1c, % baseline HbA1c, % week Change body weight -0.6 kg +1.0 kg +1.4 kg iglargine dose, units/day iglulisine dose, units/day - 10 ± 8 20 ± 13 TDD 67 ± ± ± 34 Symptomatic hypoglycemia 35.9% 46.5% 52.4% Lixi vs iglu Hypo ROSENSTOCK J, ET AL. DIABETES CARE 2016; 39:

57 LixiLan-O: LixiLan vs Lixi vs Glargine Change in FBG and Weight Rosenstock J, et al. Diabetes Care 2016; 39:
58 LixiLan-O: LixiLan vs Lixi vs Glargine Change in FBG and Weight Rosenstock J, et al. Diabetes Care 2016; 39:
59 LixiLan-O: LixiLan vs Lixi vs Glargine Change in 2-h PPG and 7-pt profile
60 LixiLan-O: LixiLan vs Lixi vs Glargine
61 GLP-1 RA and Insulin: Efficacy Outcomes Study Study Drug and Comparator Overall Hypoglycemia Severe Hypoglycemia Overall Hypoglycemia Definition Diamant 1,a EXN BID + GLAR BBT 335 events 881 events 3 events 11 events Minor symptomatic or self-treated, BG < 54 mg/dl Mathieu 2,b LIRA QD + DEG BBT 1.00 EPY 8.15 EPY 0 events 0 events Confirmed, BG < 56 mg/dl or severe Gough 3,c,f LIRA FRC QD DEG 1.77 EPY 2.79 EPY 3 events 2 events Confirmed, BG < 56 mg/dl or severe Rosenstock 4,d LIXI FRC QD GLAR 22% 23% 0 events 0 events Confirmed, BG < 70 mg/dl Blonde 5,e DULA QW + LIS BBT EPY EPY 0.06 EPY 0.09 EPY Documented symptomatic, PG < 54 mg/dl a. BL A1c 8.5%, BL Wt 89 kg; 30 weeks; b. 26-weeks, BL A1c 7.7%, BL Wt kg, BL BMI kg/m2, age 61 y, diabetes duration y; c. 26-weeks BL A1c 8.3%, BL Wt 87 kg; d. 24 weeks, BL A1c 8.0%, BL BMI 32.1 kg/m2, e. DULA 1.5 mg, BL A1c 8.5%, BL Wt 91 kg, 26 wk results 1. Diamant M, et al. Diabetes Care 2014; 37: Mathieu C, et al. Diabetes Obes Metab, 2014; 16: Gough SC, et al. Lancet Diabetes Endocrinol. 2014; 2: Rosenstock J, et al. Diabetologia 2014; 57 (suppl 1) [abstract 241}. 3. Blonde L, et al. Lancet 2015; 385:

62 Patients Achieving Endpoint, % GLP-1 RA and Insulin: Efficacy Outcomes HbA1c < 7.0% GLP-1 + ins Comparator 100 P NS P NS P < P NS P EXN BID + GLAR vs BBT 1,a EXN BID + GLAR vs BBT 1,a EXN BID + GLAR vs BBT 1,a EXN BID + GLAR vs BBT 1,a EXN BID + GLAR vs BBT 1,a a. BL A1c 8.5%, BL Wt 89 kg; 30 weeks; b. 26-weeks, BL A1c 7.7%, BL Wt kg, BL BMI kg/m2, age 61 y, diabetes duration y; c. 26-weeks BL A1c 8.3%, BL Wt 87 kg; d. 24 weeks, BL A1c 8.0%, BL BMI 32.1 kg/m2, e. DULA 1.5 mg, BL A1c 8.5%, BL Wt 91 kg, 26 wk results 1. Diamant M, et al. Diabetes Care 2014; 37: Mathieu C, et al. Diabetes Obes Metab, 2014; 16: Gough SC, et al. Lancet Diabetes Endocrinol. 2014; 2: Rosenstock J, et al. Diabetologia 2014; 57 (suppl 1) [abstract 241}. 3. Blonde L, et al. Lancet 2015; 385:
63 PATIENTS ACHIEVING ENDPOINT, % GLP-1 RA and Insulin: Efficacy Outcomes A1c < 7.0% and no hypoglycemia NR 19 NR NR NR EXN BID + GLAR vs BBT 1,a P < LIRA QD + DEG vs BBT 2,b GLP-1 + ins P < Comparator 41 LIRA FRC QD vs DEG 3,c P < LIXI FRC QD vs GLAR 4,d 0 0 DULA QW + LIS vs BBT 5,e a. BL A1c 8.5%, BL Wt 89 kg; 30 weeks; b. 26-weeks, BL A1c 7.7%, BL Wt kg, BL BMI kg/m2, age 61 y, diabetes duration y; c. 26-weeks BL A1c 8.3%, BL Wt 87 kg; d. 24 weeks, BL A1c 8.0%, BL BMI 32.1 kg/m2, e. DULA 1.5 mg, BL A1c 8.5%, BL Wt 91 kg, 26 wk results. 1. Diamant M, et al. Diabetes Care 2014; 37: Mathieu C, et al. Diabetes Obes Metab, 2014; 16: Gough SC, et al. Lancet Diabetes Endocrinol. 2014; 2: Rosenstock J, et al. Diabetologia 2014; 57 (suppl 1) [abstract 241}. 3. Blonde L, et al. Lancet 2015; 385:
64 Patients Achieving Endpoint, % GLP-1 RA and Insulin: Efficacy Outcomes A1c < 7.0%, no hypoglycemia, and no weight gain 100 GLP-1 + INS Comparator P < P < P < 0.05 P < NR 0 0 EXN BID + GLAR vs BBT 1,a 7 LIRA QD + DEG vs BBT 2,b 14 LIRA FRC QD vs DEG 3,c LIXI FRC QD vs GLAR 4,d 6 DULA QW + LIS vs BBT 5,e a. BL A1c 8.5%, BL Wt 89 kg; 30 weeks; b. 26-weeks, BL A1c 7.7%, BL Wt kg, BL BMI kg/m2, age 61 y, diabetes duration y; c. 26-weeks BL A1c 8.3%, BL Wt 87 kg; d. 24 weeks, BL A1c 8.0%, BL BMI 32.1 kg/m2, e. DULA 1.5 mg, BL A1c 8.5%, BL Wt 91 kg, 26 wk results. 1. Diamant M, et al. Diabetes Care 2014; 37: Mathieu C, et al. Diabetes Obes Metab, 2014; 16: Gough SC, et al. Lancet Diabetes Endocrinol. 2014; 2: Rosenstock J, et al. Diabetologia 2014; 57 (suppl 1) [abstract 241}. 3. Blonde L, et al. Lancet 2015; 385:
65 Safety Considerations: GLP-1 RAs Used with Insulin GLP-1 Approved for Use with Insulin Contraindications Not indicated for treatment of DKA a,b,c,d Personal or family history of MTC a,b,d, or MEN syndrome type 2 a,b,d Prior history of hypersensitivity reaction to specific agent or components a,b,c,d Warnings and precautions Hypoglycemia (with SUs or insulin) a,b,c,d Thyroid C-cell tumors in preclinical studies a,b,d Discontinue if pancreatitis is suspected a,b,c,d Hypersensitivity reactions a,b,c,d Use caution in renal impairment a,b,d ; reduce dose or monitor renal function in renal impairment b,d ; do not use exenatide BID in severe renal impairment c Pregnancy category C a,b,c,d Adverse reaction Gastrointestinal (mild-severe) a,b,c,d Allergic reactions (mild-severe) a,b Neurological (mild-moderate) b,c,d Respiratory (mild-moderate) a Hypoglycemia c,d Orthopedic (mild-moderate) a a albiglutide; b liraglutide; c exenatide BID; d dulaglutide Drugs@FDA,
66 Summary Fixed dose combinations of a GLP1-RA and basal insulin have been extensively tested for safety and efficacy. Two FDC have been recently approved by the FDA. Benefits of FDC: Limitations of FDC: Better efficacy than either component given alone Improved fasting and post-prandial glucose levels Lower rates of hypoglycemia and Wt gain than insulin monotherapy Nausea remains problematic Dose titration is required Cost

67 Aprende como si fueses a vivir siempre M. Gandhi
Francesca Porcellati
 XX Congresso Nazionale AMD Razionali e Benefici dell Aggiunta del GLP-1 RA Short-Acting all Insulina Basale Francesca Porcellati Dipartimento di Medicina Interna, Sezione di Medicina Interna, Endocrinologia
XX Congresso Nazionale AMD Razionali e Benefici dell Aggiunta del GLP-1 RA Short-Acting all Insulina Basale Francesca Porcellati Dipartimento di Medicina Interna, Sezione di Medicina Interna, Endocrinologia
ADA and AACE Glycemic Targets
 ADA and AACE Glycemic Targets HbA1C target should be individualized based on a number of factors including: Age Life expectancy Comorbidities Duration of diabetes Risk of hypoglycemia Patient motivation
ADA and AACE Glycemic Targets HbA1C target should be individualized based on a number of factors including: Age Life expectancy Comorbidities Duration of diabetes Risk of hypoglycemia Patient motivation
GLP-1 agonists. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
Early treatment for patients with Type 2 Diabetes
 Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Chief of Endocrinology East Orange General Hospital
 Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Update on Insulin-based Agents for T2D
 Update on Insulin-based Agents for T2D Injectable Therapies for Type 2 Diabetes Mellitus (T2DM) and Obesity This presentation will: Describe established and newly available insulin therapies for treatment
Update on Insulin-based Agents for T2D Injectable Therapies for Type 2 Diabetes Mellitus (T2DM) and Obesity This presentation will: Describe established and newly available insulin therapies for treatment
Achieving and maintaining good glycemic control is an
 Glycemic Efficacy, Weight Effects, and Safety of Once-Weekly Glucagon-Like Peptide-1 Receptor Agonists Yehuda Handelsman, MD, FACP, FNLA, FASPC, MACE; Kathleen Wyne, MD, PhD, FACE, FNLA; Anthony Cannon,
Glycemic Efficacy, Weight Effects, and Safety of Once-Weekly Glucagon-Like Peptide-1 Receptor Agonists Yehuda Handelsman, MD, FACP, FNLA, FASPC, MACE; Kathleen Wyne, MD, PhD, FACE, FNLA; Anthony Cannon,
UKPDS: Over Time, Need for Exogenous Insulin Increases
 UKPDS: Over Time, Need for Exogenous Insulin Increases Patients Requiring Additional Insulin (%) 60 40 20 Oral agents By 6 Chlorpropamide years, Glyburide more than 50% of UKPDS patients required insulin
UKPDS: Over Time, Need for Exogenous Insulin Increases Patients Requiring Additional Insulin (%) 60 40 20 Oral agents By 6 Chlorpropamide years, Glyburide more than 50% of UKPDS patients required insulin
Management of Type 2 Diabetes
 Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES
 INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES ARSHNA SANGHRAJKA DIABETES SPECIALIST PRESCRIBING PHARMACIST OBJECTIVES EXPLORE THE TYPES OF INSULIN AND INJECTABLE DIABETES TREATMENTS AND DEVICES AVAILABLE
INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES ARSHNA SANGHRAJKA DIABETES SPECIALIST PRESCRIBING PHARMACIST OBJECTIVES EXPLORE THE TYPES OF INSULIN AND INJECTABLE DIABETES TREATMENTS AND DEVICES AVAILABLE
Newer Insulins. Boca Raton Regional Hospital 15th Annual Internal Medicine Conference
 Newer Insulins Boca Raton Regional Hospital 15th Annual Internal Medicine Conference Luigi F. Meneghini, MD, MBA Professor of Internal Medicine, UT Southwestern Medical Center Executive Director, Global
Newer Insulins Boca Raton Regional Hospital 15th Annual Internal Medicine Conference Luigi F. Meneghini, MD, MBA Professor of Internal Medicine, UT Southwestern Medical Center Executive Director, Global
Progressive Loss of β-cell Function in T2DM
 Disclaimer This slide deck in its original and unaltered format is for educational purposes and is current as of November 2015. The content and views presented in this educational activity are those of
Disclaimer This slide deck in its original and unaltered format is for educational purposes and is current as of November 2015. The content and views presented in this educational activity are those of
Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE. CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010
 Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE Robert R. Henry, MD Authors and Disclosures CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010 Introduction Type 2 diabetes
Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE Robert R. Henry, MD Authors and Disclosures CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010 Introduction Type 2 diabetes
Disclosure. Learning Objectives. Case. Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare
 Disclosure Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare Spring Therapeutics Update 2011 CSHP BC Branch Anar Dossa BScPharm Pharm D CDE April 20, 2011
Disclosure Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare Spring Therapeutics Update 2011 CSHP BC Branch Anar Dossa BScPharm Pharm D CDE April 20, 2011
The first stop for professional medicines advice
 London Medicines Evaluation Network Overview: Glucagon-Like Peptide-1 receptor analogues The first stop for professional medicines advice 1 London Medicines Evaluation Network Overview: Glucagon-Like Peptide-1
London Medicines Evaluation Network Overview: Glucagon-Like Peptide-1 receptor analogues The first stop for professional medicines advice 1 London Medicines Evaluation Network Overview: Glucagon-Like Peptide-1
T2DM and Need for Insulin. Insulin Pharmacokinetics. When To Start Insulin in T2DM. FDA-approved Insulins for Subcutaneous Injection
 Plasma Insulin Levels Patients Requiring Insulin (%) Effective Use of Insulin in the Primary Care Practice: Insulin Therapy Initiation, Intensification, and the Insulinizing Complex Patients with T2DM:
Plasma Insulin Levels Patients Requiring Insulin (%) Effective Use of Insulin in the Primary Care Practice: Insulin Therapy Initiation, Intensification, and the Insulinizing Complex Patients with T2DM:
Timely!Insulinization In!Type!2! Diabetes,!When!and!How
 Timely!Insulinization In!Type!2! Diabetes,!When!and!How, FACP, FACE, CDE Professor of Internal Medicine UT Southwestern Medical Center Dallas, Texas Current Control and Targets 1 Treatment Guidelines for
Timely!Insulinization In!Type!2! Diabetes,!When!and!How, FACP, FACE, CDE Professor of Internal Medicine UT Southwestern Medical Center Dallas, Texas Current Control and Targets 1 Treatment Guidelines for
The Highlights of the AWARD Clinical Program FRANCESCO GIORGINO
 The Highlights of the AWARD Clinical Program FRANCESCO GIORGINO DEPARTMENT OF EMERGENCY AND ORGAN TRANSPLANTATION SECTION OF INTERNAL MEDICINE, ENDOCRINOLOGY, ANDROLOGY AND METABOLIC DISEASES Disclaimer
The Highlights of the AWARD Clinical Program FRANCESCO GIORGINO DEPARTMENT OF EMERGENCY AND ORGAN TRANSPLANTATION SECTION OF INTERNAL MEDICINE, ENDOCRINOLOGY, ANDROLOGY AND METABOLIC DISEASES Disclaimer
Quando l insulina basale non basta più: differenti e nuove strategie terapeutiche
 Quando l insulina basale non basta più: differenti e nuove strategie terapeutiche Giorgio Sesti Università Magna Graecia di Catanzaro Potenziali conflitti di interesse Il Prof Giorgio Sesti dichiara di
Quando l insulina basale non basta più: differenti e nuove strategie terapeutiche Giorgio Sesti Università Magna Graecia di Catanzaro Potenziali conflitti di interesse Il Prof Giorgio Sesti dichiara di
Agenda. Indications Different insulin preparations Insulin initiation Insulin intensification
 Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM
 Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM Disclosures Jennifer D Souza has no conflicts of interest to disclose. 2 When Basal Insulin Is Not Enough Learning
Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM Disclosures Jennifer D Souza has no conflicts of interest to disclose. 2 When Basal Insulin Is Not Enough Learning
Individualizing Therapy int2dm With Insulin
 Individualizing Therapy int2dm With Insulin Etie Moghissi, MD, FACP, FACE Clinical Associate Professor University of California, Los Angeles Los Angeles, California OBJECTIVES: At the conclusion of this
Individualizing Therapy int2dm With Insulin Etie Moghissi, MD, FACP, FACE Clinical Associate Professor University of California, Los Angeles Los Angeles, California OBJECTIVES: At the conclusion of this
Advances in Outpatient Diabetes Care: Algorithms for Care and the Role of Injectable Therapies. Module D
 Advances in Outpatient Diabetes Care: Algorithms for Care and the Role of Injectable Therapies Module D 1 Learning Objectives Apply the principles of the comprehensive diabetes algorithms to patients with
Advances in Outpatient Diabetes Care: Algorithms for Care and the Role of Injectable Therapies Module D 1 Learning Objectives Apply the principles of the comprehensive diabetes algorithms to patients with
Initiating Injectable Therapy in Type 2 Diabetes
 Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes
 Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
Diabetes: Three Core Deficits
 Diabetes: Three Core Deficits Fat Cell Dysfunction Impaired Incretin Function Impaired Appetite Suppression Obesity and Insulin Resistance in Muscle and Liver Hyperglycemia Impaired Insulin Secretion Islet
Diabetes: Three Core Deficits Fat Cell Dysfunction Impaired Incretin Function Impaired Appetite Suppression Obesity and Insulin Resistance in Muscle and Liver Hyperglycemia Impaired Insulin Secretion Islet
Optimizing Treatment Strategies to Improve Patient Outcomes in the Management of Type 2 Diabetes
 Optimizing Treatment Strategies to Improve Patient Outcomes in the Management of Type 2 Diabetes Philip Raskin, MD Professor of Medicine The University of Texas, Southwestern Medical Center NAMCP Spring
Optimizing Treatment Strategies to Improve Patient Outcomes in the Management of Type 2 Diabetes Philip Raskin, MD Professor of Medicine The University of Texas, Southwestern Medical Center NAMCP Spring
Insulin Initiation and Intensification. Disclosure. Objectives
 Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Basal Insulin Use With GLP-1 Receptor Agonists
 Basal Insulin Use With GLP-1 Receptor Agonists Sarah L. Anderson and Jennifer M. Trujillo University of Colorado Skaggs School of Pharmacy and Pharmaceutical Sciences, Aurora, CO Corresponding author:
Basal Insulin Use With GLP-1 Receptor Agonists Sarah L. Anderson and Jennifer M. Trujillo University of Colorado Skaggs School of Pharmacy and Pharmaceutical Sciences, Aurora, CO Corresponding author:
Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors
 Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors Timothy Bailey, MD, FACE, CPI Director, AMCR Institute,
Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors Timothy Bailey, MD, FACE, CPI Director, AMCR Institute,
Activity Overview. Target Audience
 Activity Overview In this Webinar, experts in endocrinology and primary care present clinical evidence and answer participant questions regarding insulin intensification with glucagon-like peptide-1 receptor
Activity Overview In this Webinar, experts in endocrinology and primary care present clinical evidence and answer participant questions regarding insulin intensification with glucagon-like peptide-1 receptor
GLP-1RA and insulin: friends or foes?
 Tresiba Expert Panel Meeting 28/06/2014 GLP-1RA and insulin: friends or foes? Matteo Monami Careggi Teaching Hospital. Florence. Italy Dr Monami has received consultancy and/or speaking fees from: Merck
Tresiba Expert Panel Meeting 28/06/2014 GLP-1RA and insulin: friends or foes? Matteo Monami Careggi Teaching Hospital. Florence. Italy Dr Monami has received consultancy and/or speaking fees from: Merck
Intensifying Treatment Beyond Monotherapy in T2DM: Where Do Newer Therapies Fit?
 Intensifying Treatment Beyond Monotherapy in T2DM: Where Do Newer Therapies Fit? Vanita R. Aroda, MD Scientific Director & Physician Investigator MedStar Community Clinical Research Center MedStar Health
Intensifying Treatment Beyond Monotherapy in T2DM: Where Do Newer Therapies Fit? Vanita R. Aroda, MD Scientific Director & Physician Investigator MedStar Community Clinical Research Center MedStar Health
Convenience of Fixed-Ratio Basal Insulin GLP-1 RA Combination Therapy
 Convenience of Fixed-Ratio Basal Insulin GLP-1 RA Combination Therapy Xavier Cos Catalonian Health Institute Barcelona, Spain Stewart B. Harris Western University London, ON, Canada Basal Insulin GLP-1
Convenience of Fixed-Ratio Basal Insulin GLP-1 RA Combination Therapy Xavier Cos Catalonian Health Institute Barcelona, Spain Stewart B. Harris Western University London, ON, Canada Basal Insulin GLP-1
Update on Insulin-based Agents for T2D. Harry Jiménez MD, FACE
 Update on Insulin-based Agents for T2D Harry Jiménez MD, FACE Harry Jiménez MD, FACE Has received honorarium as Speaker and/or Consultant for the following pharmaceutical companies: Eli Lilly Merck Boehringer
Update on Insulin-based Agents for T2D Harry Jiménez MD, FACE Harry Jiménez MD, FACE Has received honorarium as Speaker and/or Consultant for the following pharmaceutical companies: Eli Lilly Merck Boehringer
GLP-1 (glucagon-like peptide-1) Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary
 Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary") OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
Injectable Agents for Type 2 Diabetes. Richard Christensen, MD AACE Diabetes Day, Boise, ID September 2017
 Injectable Agents for Type 2 Diabetes Richard Christensen, MD AACE Diabetes Day, Boise, ID September 2017 Financial Disclosures Sanofi speaker honoraria No other relevant financial disclosures Injectable
Injectable Agents for Type 2 Diabetes Richard Christensen, MD AACE Diabetes Day, Boise, ID September 2017 Financial Disclosures Sanofi speaker honoraria No other relevant financial disclosures Injectable
Emerging Challenges in Primary Care: GLP-1 Receptor Agonists: New Insights and New Strategies for Successful Long-Term Diabetes Management
 Emerging Challenges in Primary Care: 2017 GLP-1 Receptor Agonists: New Insights and New Strategies for Successful Long-Term Diabetes Management 1 Faculty Richard S. Beaser, MD Senior Staff Physician, Medical
Emerging Challenges in Primary Care: 2017 GLP-1 Receptor Agonists: New Insights and New Strategies for Successful Long-Term Diabetes Management 1 Faculty Richard S. Beaser, MD Senior Staff Physician, Medical
Drug List. Drug List (cont.) Objectives. Case 1 Bruce. Presenter Disclosure Information
 Objectives. Case 1 Bruce. Presenter Disclosure Information") 1:15 :3 PM GLP-1 Receptor Agonists and Basal Insulin Combination: A Complementary Strategy for Type Diabetes Treatment Intensification SPEAKERS Vivian Fonseca, MD Dace Trence, MD, FACE Presenter Disclosure
1:15 :3 PM GLP-1 Receptor Agonists and Basal Insulin Combination: A Complementary Strategy for Type Diabetes Treatment Intensification SPEAKERS Vivian Fonseca, MD Dace Trence, MD, FACE Presenter Disclosure
la prise en charge du diabète de
 N21 XIII Congrès National de Diabétologie, 29 mai 2011, Alger Intérêt et place des Anti DPP4 dans la prise en charge du diabète de type 2 Nicolas PAQUOT, MD, PhD CHU Sart-Tilman, Université de Liège Belgique
N21 XIII Congrès National de Diabétologie, 29 mai 2011, Alger Intérêt et place des Anti DPP4 dans la prise en charge du diabète de type 2 Nicolas PAQUOT, MD, PhD CHU Sart-Tilman, Université de Liège Belgique
Natural History of Type 2 Diabetes
 Key Points About Insulin to Discuss Today We should be using insulin earlier in the natural history of type 2 diabetes How early and how do we know when to start insulin? Barriers to insulin therapy Goals
Key Points About Insulin to Discuss Today We should be using insulin earlier in the natural history of type 2 diabetes How early and how do we know when to start insulin? Barriers to insulin therapy Goals
What s New? An Antihyperglycemic Medications Update
 What s New? An Antihyperglycemic Medications Update WADE 2016 Annual Conference Josh Neumiller, PharmD, CDE, FASCP Associate Professor Department of Pharmacotherapy Washington State University Disclosures
What s New? An Antihyperglycemic Medications Update WADE 2016 Annual Conference Josh Neumiller, PharmD, CDE, FASCP Associate Professor Department of Pharmacotherapy Washington State University Disclosures
GLP-1-based therapies in the management of type 2 diabetes
 GLP-1-based therapies in the management of type 2 diabetes Makbul Aman Mansyur Division Endocrine & Metabolism Department of Internal Medicine Faculty of Medicine Hasanuddin University/ RSUP Dr. Wahidin
GLP-1-based therapies in the management of type 2 diabetes Makbul Aman Mansyur Division Endocrine & Metabolism Department of Internal Medicine Faculty of Medicine Hasanuddin University/ RSUP Dr. Wahidin
9/6/18. Clinical Updates for Nurse Practitioners and Physician Assistants: Faculty. Disclosures
 Clinical Updates for Nurse Practitioners and Physician Assistants: 218 Combination Basal Insulin and GLP-1 RA Therapy: A Physiologic Approach to Diabetes Care Faculty Robert S. Busch, MD, FACE Director
Clinical Updates for Nurse Practitioners and Physician Assistants: 218 Combination Basal Insulin and GLP-1 RA Therapy: A Physiologic Approach to Diabetes Care Faculty Robert S. Busch, MD, FACE Director
MYTH VS FACT #1: GLP-1 RECEPTOR AGONISTS SHOULD BE RESERVED FOR PATIENTS WITH LONG-STANDING T2DM
 9:45 11: AM Separating Myth from Fact: The Role of Receptor Agonists for the Treatment of T2DM SPEAKERS James R. Gavin, III, MD, PhD John E. Anderson, MD Presenter Disclosure Information The following
9:45 11: AM Separating Myth from Fact: The Role of Receptor Agonists for the Treatment of T2DM SPEAKERS James R. Gavin, III, MD, PhD John E. Anderson, MD Presenter Disclosure Information The following
T2DM Treatment Intensification after Basal Insulin: GLP-1 RA or Rapid-Acting Insulin?
 T2DM Treatment Intensification after Basal Insulin: GLP-1 RA or Rapid-Acting Insulin? Francesco Giorgino Department of Emergency and Organ Transplantation, Section of Internal Medicine, Endocrinology,
T2DM Treatment Intensification after Basal Insulin: GLP-1 RA or Rapid-Acting Insulin? Francesco Giorgino Department of Emergency and Organ Transplantation, Section of Internal Medicine, Endocrinology,
Selecting GLP-1 RA Treatment
 Selecting GLP-1 RA Treatment Dr Felicity Kaplan March 2017 Objectives Review the progressive nature of type 2 diabetes Understand the need for timely treatment intensification Examine the place of GLP-1
Selecting GLP-1 RA Treatment Dr Felicity Kaplan March 2017 Objectives Review the progressive nature of type 2 diabetes Understand the need for timely treatment intensification Examine the place of GLP-1
Albiglutide, a Once-Weekly GLP-1RA, for the Treatment of Type 2 Diabetes
 St. Onge et al. Medical Research Archives, vol. 5, issue 11, November 2017 issue Page 1 of 10 REVIEW ARTICLE Albiglutide, a Once-Weekly GLP-1RA, for the Treatment of Type 2 Diabetes Erin St. Onge 1*, Shannon
St. Onge et al. Medical Research Archives, vol. 5, issue 11, November 2017 issue Page 1 of 10 REVIEW ARTICLE Albiglutide, a Once-Weekly GLP-1RA, for the Treatment of Type 2 Diabetes Erin St. Onge 1*, Shannon
COPYRIGHT. Advancing to Insulin Replacement Therapy: When, Why, and How? Update in Internal Medicine December 5, Richard S.
 Advancing to Insulin Replacement Therapy: When, Why, and How? Update in Internal Medicine - 2016 December 5, 2016 Richard S. Beaser, MD Medical Director, Professional Education Joslin Diabetes Center Associate
Advancing to Insulin Replacement Therapy: When, Why, and How? Update in Internal Medicine - 2016 December 5, 2016 Richard S. Beaser, MD Medical Director, Professional Education Joslin Diabetes Center Associate
Pathogenesis of Type 2 Diabetes
 9/23/215 Multiple, Complex Pathophysiological Abnmalities in T2DM incretin effect gut carbohydrate delivery & absption pancreatic insulin secretion pancreatic glucagon secretion HYPERGLYCEMIA? Pathogenesis
9/23/215 Multiple, Complex Pathophysiological Abnmalities in T2DM incretin effect gut carbohydrate delivery & absption pancreatic insulin secretion pancreatic glucagon secretion HYPERGLYCEMIA? Pathogenesis
New and Emerging Therapies for Type 2 DM
 Dale Clayton MHSc, MD, FRCPC Dalhousie University/Capital Health April 28, 2011 New and Emerging Therapies for Type 2 DM The science of today, is the technology of tomorrow. Edward Teller American Physicist
Dale Clayton MHSc, MD, FRCPC Dalhousie University/Capital Health April 28, 2011 New and Emerging Therapies for Type 2 DM The science of today, is the technology of tomorrow. Edward Teller American Physicist
Newer and Expensive treatment of diabetes. Endocrinology Visiting Associate Professor Institute of Medicine TUTH
 Newer and Expensive treatment of diabetes Jyoti Bhattarai MD Endocrinology Visiting Associate Professor Institute of Medicine TUTH Four out of every five people with diabetes now live in developing countries.
Newer and Expensive treatment of diabetes Jyoti Bhattarai MD Endocrinology Visiting Associate Professor Institute of Medicine TUTH Four out of every five people with diabetes now live in developing countries.
New Drug Evaluation: lixisenatide injection, subcutaneous
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
 Learning Objectives Understand and appropriately individualize treatments based on evidencebased guideline recommendations across the continuum of care in patients with T2DM Key = Clinical Pearl Identify
Learning Objectives Understand and appropriately individualize treatments based on evidencebased guideline recommendations across the continuum of care in patients with T2DM Key = Clinical Pearl Identify
What's New in Insulin Related Therapies 2018
 What's New in Insulin Related Therapies 2018 James Lenhard, MD (JLenhard@ChristianaCare.org) Section Chief, Endocrinology and Metabolism Christiana Care Health System Newark, DE Disclosures Speaker:Eli
What's New in Insulin Related Therapies 2018 James Lenhard, MD (JLenhard@ChristianaCare.org) Section Chief, Endocrinology and Metabolism Christiana Care Health System Newark, DE Disclosures Speaker:Eli
Diabetes Update: Intensifying Insulin Therapy Nuts, Bolts and Other Items
 Diabetes Update: Intensifying Insulin Therapy Nuts, Bolts and Other Items Hayley A. Miller, MD Physician, Internal Medicine, Diabetes and Metabolism, Sandy Clinic, Intermountain Healthcare Objectives:
Diabetes Update: Intensifying Insulin Therapy Nuts, Bolts and Other Items Hayley A. Miller, MD Physician, Internal Medicine, Diabetes and Metabolism, Sandy Clinic, Intermountain Healthcare Objectives:
Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol
 Agonists Drug Class Prior Authorization Protocol") Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
New basal insulins Are they any better? Matthew C. Riddle, MD Professor of Medicine Oregon Health & Science University Keystone Colorado 15 July 2011
 New basal insulins Are they any better? Matthew C. Riddle, MD Professor of Medicine Oregon Health & Science University Keystone Colorado 15 July 2011 Presenter Disclosure I have received the following
New basal insulins Are they any better? Matthew C. Riddle, MD Professor of Medicine Oregon Health & Science University Keystone Colorado 15 July 2011 Presenter Disclosure I have received the following
Individualizing Care for Patients with Type 2 Diabetes
 Individualizing Care for Patients with Type 2 Diabetes Disclosures Speaker: AstraZeneca, Novo Nordisk, BI/Lilly, Valeritas, Takeda Advisor: Tandem Diabetes, Sanofi Objectives Develop individualized approaches
Individualizing Care for Patients with Type 2 Diabetes Disclosures Speaker: AstraZeneca, Novo Nordisk, BI/Lilly, Valeritas, Takeda Advisor: Tandem Diabetes, Sanofi Objectives Develop individualized approaches
Tips and Tricks for Starting and Adjusting Insulin. MC MacSween The Moncton Hospital
 Tips and Tricks for Starting and Adjusting Insulin MC MacSween The Moncton Hospital Progression of type 2 diabetes Beta cell apoptosis Natural History of Type 2 Diabetes The Burden of Treatment Failure
Tips and Tricks for Starting and Adjusting Insulin MC MacSween The Moncton Hospital Progression of type 2 diabetes Beta cell apoptosis Natural History of Type 2 Diabetes The Burden of Treatment Failure
Incredible Incretins Abby Frye, PharmD, BCACP
 Incredible Incretins Abby Frye, PharmD, BCACP Objectives & Disclosures Review the pathophysiology of T2DM and the impact of the incretin system Describe the defining characteristics of the available glucagonlike
Incredible Incretins Abby Frye, PharmD, BCACP Objectives & Disclosures Review the pathophysiology of T2DM and the impact of the incretin system Describe the defining characteristics of the available glucagonlike
New Drug Evaluation: Dulaglutide
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
No Increased Cardiovascular Risk for Lixisenatide in ELIXA
 ON ISSUES IN THE MANAGEMENT OF TYPE 2 DIABETES JUNE 2015 Coverage of data from ADA 2015, June 5 9 in Boston, Massachusetts No Increased Cardiovascular Risk for Lixisenatide in ELIXA First Cardiovascular
ON ISSUES IN THE MANAGEMENT OF TYPE 2 DIABETES JUNE 2015 Coverage of data from ADA 2015, June 5 9 in Boston, Massachusetts No Increased Cardiovascular Risk for Lixisenatide in ELIXA First Cardiovascular
Lilly Diabetes: Pipeline Update
 Lilly Diabetes: Pipeline Update June 16, 2014 Safe Harbor Provision This presentation contains forward-looking statements that are based on management's current expectations, but actual results may differ
Lilly Diabetes: Pipeline Update June 16, 2014 Safe Harbor Provision This presentation contains forward-looking statements that are based on management's current expectations, but actual results may differ
Reviewing Diabetes Guidelines. Newsletter compiled by Danny Jaek, Pharm.D. Candidate
 Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
Pramlintide & Weight. Diane M Karl MD. The Endocrine Clinic & Oregon Health & Science University Portland, Oregon
 Pramlintide & Weight Diane M Karl MD The Endocrine Clinic & Oregon Health & Science University Portland, Oregon Conflict of Interest Speakers Bureau: Amylin Pharmaceuticals Consultant: sanofi-aventis Grant
Pramlintide & Weight Diane M Karl MD The Endocrine Clinic & Oregon Health & Science University Portland, Oregon Conflict of Interest Speakers Bureau: Amylin Pharmaceuticals Consultant: sanofi-aventis Grant
Faculty. Timothy S. Reid, MD (Co-Chair, Presenter) Medical Director Mercy Diabetes Center Janesville, WI
 Medical Director Mercy Diabetes Center Janesville, WI") Activity Overview In this case-based webcast, meet Jackie, a 62-year-old woman with type 2 diabetes. Her glycated hemoglobin (HbA1C) is 9.2%, and she is taking 2 oral agents and basal insulin; however,
Activity Overview In this case-based webcast, meet Jackie, a 62-year-old woman with type 2 diabetes. Her glycated hemoglobin (HbA1C) is 9.2%, and she is taking 2 oral agents and basal insulin; however,
PHARMACOLOGIC APPROACH TO ACHIEVE GLYCEMIC GOAL
 Dr Aurora Alcantara Endocrinology PHARMACOLOGIC APPROACH TO ACHIEVE GLYCEMIC GOAL SPED Convention and Diabetes Postgraduate Course May26-29 Wyndham Grand Rio Mar, PR DISCLOSURES Speaker for the following
Dr Aurora Alcantara Endocrinology PHARMACOLOGIC APPROACH TO ACHIEVE GLYCEMIC GOAL SPED Convention and Diabetes Postgraduate Course May26-29 Wyndham Grand Rio Mar, PR DISCLOSURES Speaker for the following
MYTH VS FACT #1: GLP-1 RECEPTOR AGONISTS SHOULD BE RESERVED FOR PATIENTS WITH LONG-STANDING T2DM
 15 mins for presentation & ARS MYTH VS FACT #1: GLP-1 RECEPTOR AGONISTS SHOULD BE RESERVED FOR PATIENTS WITH LONG-STANDING T2DM Carol Hatch Wysham, MD Clinical Associate Professor of Medicine University
15 mins for presentation & ARS MYTH VS FACT #1: GLP-1 RECEPTOR AGONISTS SHOULD BE RESERVED FOR PATIENTS WITH LONG-STANDING T2DM Carol Hatch Wysham, MD Clinical Associate Professor of Medicine University
Next Generation Diabetes Management:
 Next Generation Diabetes Management: Titratable Fixed-Ratio Combination Therapy with Basal Insulin/GLP-1 RA to Better Manage Type 2 Diabetes Supported by an educational grant from Sanofi US Learning Objectives
Next Generation Diabetes Management: Titratable Fixed-Ratio Combination Therapy with Basal Insulin/GLP-1 RA to Better Manage Type 2 Diabetes Supported by an educational grant from Sanofi US Learning Objectives
Diabetes: Definition Pathophysiology Treatment Goals. By Scott Magee, MD, FACE
 Diabetes: Definition Pathophysiology Treatment Goals By Scott Magee, MD, FACE Disclosures No disclosures to report Definition of Diabetes Mellitus Diabetes Mellitus comprises a group of disorders characterized
Diabetes: Definition Pathophysiology Treatment Goals By Scott Magee, MD, FACE Disclosures No disclosures to report Definition of Diabetes Mellitus Diabetes Mellitus comprises a group of disorders characterized
Houston, TX. March 12th, 2015
 March 12th, 215 George R. Brown Conven on Center Houston, TX P F Dace L. Trence, MD, FACE Professor, Department of Medicine Director, Endocrine Fellowship Program Director, Diabetes Care Center University
March 12th, 215 George R. Brown Conven on Center Houston, TX P F Dace L. Trence, MD, FACE Professor, Department of Medicine Director, Endocrine Fellowship Program Director, Diabetes Care Center University
ABSTRACT. uncontrolled on basal insulin? OADs;
 Diabetes Ther (2017) 8:673 682 DOI 10.1007/s13300-017-0252-9 BRIEF REPORT Efficacy and Safety of IDegLira in Participants with Type 2 Diabetes in India Uncontrolled on Oral Antidiabetic Drugs and Basal
Diabetes Ther (2017) 8:673 682 DOI 10.1007/s13300-017-0252-9 BRIEF REPORT Efficacy and Safety of IDegLira in Participants with Type 2 Diabetes in India Uncontrolled on Oral Antidiabetic Drugs and Basal
DPP-4 inhibitor. The new class drug for Diabetes
 DPP-4 inhibitor The new class drug for Diabetes 1 Cause of Death in Korea 1 st ; Neoplasm 2 nd ; Cardiovascular Disease 3 rd ; Cerebrovascular Disease Diabetes 2 Incidence of Fatal or Nonfatal MI During
DPP-4 inhibitor The new class drug for Diabetes 1 Cause of Death in Korea 1 st ; Neoplasm 2 nd ; Cardiovascular Disease 3 rd ; Cerebrovascular Disease Diabetes 2 Incidence of Fatal or Nonfatal MI During
Xultophy 100/3.6. (insulin degludec, liraglutide) New Product Slideshow
 New Product Slideshow") Xultophy 100/3.6 (insulin degludec, liraglutide) New Product Slideshow Introduction Brand name: Xultophy Generic name: Insulin degludec, liraglutide Pharmacological class: Human insulin analog + glucagon-like
Xultophy 100/3.6 (insulin degludec, liraglutide) New Product Slideshow Introduction Brand name: Xultophy Generic name: Insulin degludec, liraglutide Pharmacological class: Human insulin analog + glucagon-like
Supplementary Data. Formula S1. Calculation of IG fluctuation from continuous glucose monitoring profiles Z T 1 T
 Supplementary Data Formula S1. Calculation of IG fluctuation from continuous glucose monitoring profiles 1 T Z T O jig(t) IGjdt IG, interstitial glucose; IG(t), IG value at time t; IG, mean IG from the
Supplementary Data Formula S1. Calculation of IG fluctuation from continuous glucose monitoring profiles 1 T Z T O jig(t) IGjdt IG, interstitial glucose; IG(t), IG value at time t; IG, mean IG from the
Clinical Overview of Combination Therapy with Sitagliptin and Metformin
 Clinical Overview of Combination Therapy with Sitagliptin and Metformin 1 Contents Pathophysiology of type 2 diabetes and mechanism of action of sitagliptin Clinical data overview of sitagliptin: Monotherapy
Clinical Overview of Combination Therapy with Sitagliptin and Metformin 1 Contents Pathophysiology of type 2 diabetes and mechanism of action of sitagliptin Clinical data overview of sitagliptin: Monotherapy
What s New in Diabetes Treatment. Disclosures
 What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
Mechanisms and Clinical Efficacy of Lixisenatide for the Management of Type 2 Diabetes
 Adv Ther (2013) 30(2):81 101. DOI 10.1007/s12325-013-0009-4 REVIEW Mechanisms and Clinical Efficacy of Lixisenatide for the Management of Type 2 Diabetes Michael Horowitz Christopher K. Rayner Karen L.
Adv Ther (2013) 30(2):81 101. DOI 10.1007/s12325-013-0009-4 REVIEW Mechanisms and Clinical Efficacy of Lixisenatide for the Management of Type 2 Diabetes Michael Horowitz Christopher K. Rayner Karen L.
exenatide 2mg powder and solvent for prolonged-release suspension for injection (Bydureon ) SMC No. (748/11) Eli Lilly and Company Limited
 SMC No. (748/11) Eli Lilly and Company Limited") exenatide 2mg powder and solvent for prolonged-release suspension for injection (Bydureon ) SMC No. (748/11) Eli Lilly and Company Limited 09 December 2011 The Scottish Medicines Consortium (SMC) has completed
exenatide 2mg powder and solvent for prolonged-release suspension for injection (Bydureon ) SMC No. (748/11) Eli Lilly and Company Limited 09 December 2011 The Scottish Medicines Consortium (SMC) has completed
What s New on the Horizon: Diabetes Medication Update
 What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
Professor Rudy Bilous James Cook University Hospital
 Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Approaches to Addressing Incretin Deficiency. Non-Insulin Injectable Agents. Incretin Mimetics. Exendin-4 in the Gila Monster
 Non-Insulin Injectable Agents Approaches to Addressing Incretin Deficiency Longer-acting analogs? (Incretin mimetics) GLP-1 Analogs Inhibition of inactivation? (Incretin enhancers) DPP-4 Inhibitors Drucker
Non-Insulin Injectable Agents Approaches to Addressing Incretin Deficiency Longer-acting analogs? (Incretin mimetics) GLP-1 Analogs Inhibition of inactivation? (Incretin enhancers) DPP-4 Inhibitors Drucker
The Many Faces of T2DM in Long-term Care Facilities
 The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
GLP-1 receptor agonists for type 2 diabetes currently available in the U.S.
 GLP-1 receptor agonists for type 2 diabetes currently available in the U.S. GLP-1 agonists are a class of antidiabetic agents that mimic the actions of the glucagon-like peptide. GLP-1 is one of several
GLP-1 receptor agonists for type 2 diabetes currently available in the U.S. GLP-1 agonists are a class of antidiabetic agents that mimic the actions of the glucagon-like peptide. GLP-1 is one of several
NEW DIABETES CARE MEDICATIONS
 NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
Parenteral Agents in Type 2 DM
 Parenteral Agents in Type 2 DM CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright
Parenteral Agents in Type 2 DM CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright
What s New on the Horizon: Diabetes Medication Update. Michael Shannon, MD Providence Endocrinology, Olympia WA
 What s New on the Horizon: Diabetes Medication Update Michael Shannon, MD Providence Endocrinology, Olympia WA 1 Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors,
What s New on the Horizon: Diabetes Medication Update Michael Shannon, MD Providence Endocrinology, Olympia WA 1 Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors,
New Treatment Options for Type 2 Diabetes: Incretin-Based Therapy
 New Treatment Options for Type 2 Diabetes: Incretin-Based Therapy New Treatment Options for Type 2 Diabetes: Incretin-Based Therapy is supported by an educational grant from Novo Nordisk Inc. This program
New Treatment Options for Type 2 Diabetes: Incretin-Based Therapy New Treatment Options for Type 2 Diabetes: Incretin-Based Therapy is supported by an educational grant from Novo Nordisk Inc. This program
Individualising Insulin Regimens: Premixed or basal plus/bolus?
 Individualising Insulin Regimens: Premixed or basal plus/bolus? Dr. Ted Wu Director, Diabetes Centre, Hospital Sydney, Australia Turkey, April 2015 Centre of Health Professional Education Optimising insulin
Individualising Insulin Regimens: Premixed or basal plus/bolus? Dr. Ted Wu Director, Diabetes Centre, Hospital Sydney, Australia Turkey, April 2015 Centre of Health Professional Education Optimising insulin
Oral Agents. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
Soliqua (insulin glargine and lixisenatide), Xultophy (insulin degludec and liraglutide)
, Xultophy (insulin degludec and liraglutide)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.48 Subject: Insulin GLP-1 Combinations Page: 1 of 5 Last Review Date: September 15, 2017 Insulin GLP-1
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.48 Subject: Insulin GLP-1 Combinations Page: 1 of 5 Last Review Date: September 15, 2017 Insulin GLP-1
Le incretine: un passo avanti. Francesco Dotta
 Le incretine: un passo avanti Francesco Dotta U.O.C. Diabetologia, Policlinico Le Scotte Università di Siena Fondazione Umberto Di Mario ONLUS Toscana Life Science Park Incretins: multiple targets multiple
Le incretine: un passo avanti Francesco Dotta U.O.C. Diabetologia, Policlinico Le Scotte Università di Siena Fondazione Umberto Di Mario ONLUS Toscana Life Science Park Incretins: multiple targets multiple
10/15/18. Clinical Updates for Nurse Practitioners and Physician Assistants: Faculty. Disclosures
 Clinical Updates for Nurse Practitioners and Physician Assistants: 2018 Combination Basal Insulin and GLP-1 RA Therapy: A Physiologic Approach to Diabetes Care Faculty Robert S. Busch, MD, FACE Director
Clinical Updates for Nurse Practitioners and Physician Assistants: 2018 Combination Basal Insulin and GLP-1 RA Therapy: A Physiologic Approach to Diabetes Care Faculty Robert S. Busch, MD, FACE Director
Type 2 Diabetes Mellitus 2011
 2011 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetes Mellitus Diagnosis 2011 Diabetes Mellitus Fasting Glucose
2011 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetes Mellitus Diagnosis 2011 Diabetes Mellitus Fasting Glucose
What s New in Type 2? Peter Hammond Consultant Physician Harrogate District Hospital
 What s New in Type 2? Peter Hammond Consultant Physician Harrogate District Hospital Therapy considerations in T2DM Thiazoledinediones DPP IV inhibitors GLP 1 agonists Insulin Type Delivery Horizon scanning
What s New in Type 2? Peter Hammond Consultant Physician Harrogate District Hospital Therapy considerations in T2DM Thiazoledinediones DPP IV inhibitors GLP 1 agonists Insulin Type Delivery Horizon scanning
OBESITY IN TYPE 2 DIABETES
 OBESITY IN TYPE 2 DIABETES Ashley Crowl, PharmD, BCACP Assistant Professor University of Kansas Objectives Review how to manage obesity in patients with type-2 diabetes mellitus Compare antiobesity agents
OBESITY IN TYPE 2 DIABETES Ashley Crowl, PharmD, BCACP Assistant Professor University of Kansas Objectives Review how to manage obesity in patients with type-2 diabetes mellitus Compare antiobesity agents
Type 2 Diabetes Management: Case 1: Reducing Hypoglycemic Risk Case 2: Reducing Cardiovascular Risk
 Type 2 Diabetes Management M. Susan Burke, MD, FACP Clinical Associate Professor of Medicine Sidney Kimmel Medical College at Thomas Jefferson University Senior Advisor, Lankenau Medical Associates Lankenau
Type 2 Diabetes Management M. Susan Burke, MD, FACP Clinical Associate Professor of Medicine Sidney Kimmel Medical College at Thomas Jefferson University Senior Advisor, Lankenau Medical Associates Lankenau