Introduction to Epilepsy Surgery ผศ.นพ.บรรพต ส ทธ นามส วรรณ สาขาว ชาประสาทศ ลยศาสตร ภาคว ชาศ ลยศาสตร คณะแพทยศาสตร ศ ร ราชพยาบาล มหาว ทยาล ยมห ดล
|
|
|
- Ferdinand Barrett
- 6 years ago
- Views:
Transcription
1 Introduction to Epilepsy Surgery ผศ.นพ.บรรพต ส ทธ นามส วรรณ สาขาว ชาประสาทศ ลยศาสตร ภาคว ชาศ ลยศาสตร คณะแพทยศาสตร ศ ร ราชพยาบาล มหาว ทยาล ยมห ดล
2 Overview Drug resistant epilepsy Cortical zones Presurgical evaluation Operative procedures
3 Drug resistant (intractable) epilepsy Failure of adequate trials of two tolerated, appropriately chosen and used antiepileptic drug schedules (whether as monotherapy or in combination) to achieve sustained seizure freedom 40% of patients with epilepsy
4
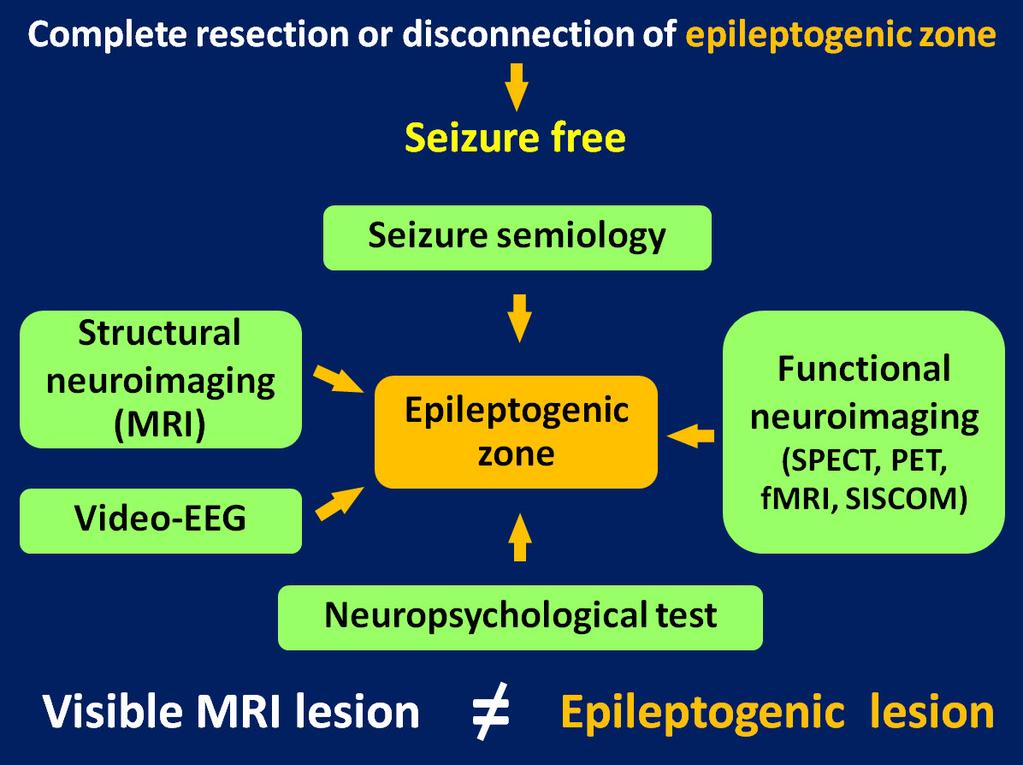
5 Cortical zones Zone Period Investigation Symptomatogenic zone Ictal Semiology, video EEG Irritative zone Interictal Interictal EEG (scalp, invasive), ECoG, MEG, fmri EEG Ictal onset zone Ictal Ictal EEG (scalp, invasive), ictal SPECT Functional deficit zone Interictal PE, neuropsychological test, Wada test, PET, interictal SPECT Epileptogenic lesion Neuroimaging Epileptogenic zone None
6 Operative procedures Resective surgery Temporal lobe surgery: anterior temporal lobectomy, selective amygdalohippocampectomy, lesionectomy, tailored resection Extratemporal lobe surgery: topectomy, lobectomy, multilobar resection, lesionectomy, tailored resection Hemispheric surgery: hemispherectomy, hemispherotomy Palliative surgery Disconnection: corpus callosotomy, multiple subpial transections, hippocampal transections Neurostimulation: vagus nerve stimulation, deep brain stimulation, responsive cortical stimulation
7 Standard anterior temporal lobectomy Anterior 2/3 temporal lobectomy Neocortical resection + amydalohippocampectomy The median length of resection from temporal tip Non dominant: 5.5 cm Dominant: 4.5 cm Hippocampus: 3 cm




8 Hippocampal sclerosis Anterior temporal lobectomy

9 Selective amygdalohippocampectomy Resection of mesial temporal structures without neocortical resection Indication: clear evidence of MTLE without lateral temporal involvement
10 Dual pathology Hippocampal sclerosis + extra hippocampal lesion Extra hippocampal lesion: temporal or extratemporal Which one is (are) epileptogenic lesion? Removal of both lesions: the greatest chance of seizure freedom Seizure free is less than single pathology
11 Tailored resection Intraoperative electrocorticography (ECoG) recording on the cerebral cortex Identification of epileptogenic area Useful in cortical lesion e.g. cortical dysplasia Limitations Inter ictal EEG (irritative zone): cannot demarcate the epileptogenic zone definitely Need a period of time during the operation
12 Surgery for hemispheric epilepsy Hemispheric epilepsy Hemimegalencephaly Rasmussen s encephalitis Struge Weber syndrome Ischemic/anoxic brain injury Goal: early control of catastrophic epilepsy
13 Hemispherectomy techniques Resection Disconnection Anatomical hemispherectomy Modified anatomical hemispherectomy (Oxford modification) Hemicorticectomy (hemidecortication) Functional hemispherectomy Modified hemispheric disconnection Hemipheric deafferentiation Keyhole hemispherectomy Transopercular hemispherotomy Hemispherotomy Peri insular (lateral) hemispherotomy Vertical hemispherotomy

14 Anatomical hemispherectomy McKenzie 1938 Indications: hemimegalencephaly, reoperation after failed functional hemispherectomy En bloc resection vs. piecemeal resection
15 Anatomical hemispherectomy Early postoperative complications Aseptic meningitis Brain shift and herniation Hydrocephalus Late postoperative complications Superficial cerebral hemosiderosis (SCH) Spontaneous or post traumatic hemorrhage

16 Modified anatomical hemispherectomy (Oxford modification) Adams 1968 Procedures 1. Anatomical hemispherectomy 2. Muscle plug at foramen of Monroe 3. Dural plication for reducing subdural space 4. Expansion extradural cavity

17 Hemicorticectomy (hemidecortication) Ignelzi and Bucy 1968 Degloving of the cortex from the white matter Minimize ventricular exposure Disadvantages Blood loss Obliteration of arachnoid granulation: hydrocephalus Incomplete disconnection
18 Functional hemispherectomy Rasmussen 1974 Modern technique for hemispheric epilepsy Avoidance of SCH Procedures 1. Temporal lobectomy (neocortex + hippocampus + amygdala) 2. Central (frontoparietal operculum) resection 3. Transventricular total corpus callosotomy 4. Disconnection of mesial frontal and parieto occipital lobes 5. Insular cortex aspiration

19 Functional hemispherectomy
20 Peri insular hemispherotomy Villemure 1995 Minimal brain removal to achieve complete hemispheric disconnection Procedures 1. Suprasylvian window: removal of frontoparietal operculum, transventricular total corpus callosotomy, disconnection of frontal lobe
21 Peri insular hemispherotomy Procedures 2. Infrasylvian window: removal of temporal operculum, total resection of temporal stem from trigone to anterior temporal horn, amygdalectomy, hippocampectomy (or posterior hippocampotomy) 3. Insular resection: two techniques 3.1 Insular cortex aspiration 3.2 Insular disconnection

22 Corpus callosotomy (interhemispheric disconnection) Rostrum and genu Body Splenium Cut the pathway of seizure propagation from one to the other hemisphere
23 Corpus callosotomy Intractable generalized seizures Atonic seizure (drop attack) Lennox Gastaut syndrome West syndrome Anterior vs. total corpus callosotomy
24 Anterior vs. total corpus callosotomy Anterior corpus callosotomy Spare of splenium Diminish risk of complications, esp. callosal disconnection syndrome Total corpus callosotomy Second stage procedure following failed anterior corpus callosotomy Initial procedure for patients with severe cognitive impairment or significant unilateral hemispheric disease (low risk of callosal disconnection syndrome)
25 Complications Retraction brain edema Callosal disconnection syndrome Language impairment and transient aphasia Transient akinetic state Memory deficits New types of seizure: esp. simple partial seizure Aseptic meningitis and ventriculitis after exposure of 3 rd ventricle (prevent by extraependymal disconnection and short term steroid)
26 Callosal disconnection syndrome (split brain syndrome) Alien hand syndrome and intermanual conflict Left hand apraxia Left hand agraphia Left tactile anomia Right constructional apraxia Visual anomia Hemineglect


27 Multiple subpial transections Disconnection of epileptogenic focus in the eloquent cortex to avoid permanent neurological deficit
 Others: cortical dysplasia, epilepsia partialis continua (EPC) caused by Rasmussen s")
28 Multiple subpial transections Indications Focal seizure arising in eloquent cortex (motor, sensory, language, memory) Landau Kleffner syndrome (LKS) Malignant rodandic sylvian epilepsy syndrome (MRSE) Others: cortical dysplasia, epilepsia partialis continua (EPC) caused by Rasmussen s encephalitis

29 Multiple hippocampal transections Seizure control with preservation of verbal memory Surgical candidate: intractable MTLE without hippocampal atrophy or sclerosis on MRI

30 Multiple hippocampal transections Intraoperative ECoG before and after transections If no spike on amygdala: partial resection of amygdala to expose the hippocampal head If there is active spikes on amygdala: amygdalectomy

31 Multiple hippocampal transections 5 mm distance to the next transection
32 Vagus nerve stimulation VNS therapy Neurotransmitter Cerebral blood flow EEG changes Norepinephrine GABA Serotonin Aspartate Thalamus Cerebral cortex Desynchronization of EEG rhythms Anti convulsive effect
33 Vagus nerve stimulation Unknown mechanism of action Vagal afferents project to diffuse areas of CNS, many of them are potential sites of epileptogenesis Key structures of VNS action Locus ceruleus (LC) Dorsal raphe nucleus (DRN) Release norepinephrine and serotonin Anti convulsive effect Anti depressive effect
34 Vagus nerve stimulation Indications Patients who are not candidates for resective surgical procedure Not possible to predict response to VNS therapy VNS can decrease seizure duration, frequency or severe, may reduce amount of AEDs
35 Vagus nerve stimulation The right vagus nerve preferentially supplies the sino atrial (SA) node VNS electrode is usually applied to the left side to avoid stimulation related asystole or bradycardia Implantation of VNS electrode at the midcervical level because the vagus nerve is relatively free of branches
36 VNS complications Vocal cord abnormalities Transient vocal cord paralysis 0.7 % Spontaneous remission Infection Bradycardia/asystole (very rare) Sleep related breathing disorders Decreased respiratory airflow, OSA Resolve with decrease VNS setting Patients with known OSA should be monitored carefully after VNS implantation

37 Anterior thalamic deep brain stimulation
38 Ce cerebellum, CMN central medial nucleus of the thalamus, St striatum, SNr pars reticularis of substantia nigra, STN subthalamic nucleus, Ca corpus amygdaloideum, DMAZ dorsal midbrain anticonvulsant zone, EF epileptic focus, Hip hippocampus, ANT anterior nucleus of thalamus
39 Responsive cortical stimulation Treatment of intractable partial onset epilepsy Subdural cortical strip or depth electrode is placed in the brain according to the seizure focus Responsive stimulation directly to the seizure focus when epileptic activity is detected Aim to disrupt epileptiform activity before seizure developed
40 Intracranial EEG Indications Disconcordant results of non invasive methods Absent structural lesion on MRI Scalp EEG cannot detect seizure origin Localization of eloquent cortex by functional brain mapping Types (subdural, depth, stereo EEG)
41 Postoperative seizure outcome Engel vs. ILAE classification
42 Timing of AED withdrawal after Controversial successful epilepsy surgery Most studies: tapering off AED after one year of postoperative seizure freedom is safe Early AED withdrawal may increase risk of seizure recurrence An important predictor of seizure outcome and cure is incomplete resection of epileptogenic lesion Early AED withdrawal seems safe in patients with presumed complete resection of epileptogenic lesion

43
44
Epilepsy Surgery: Who should be considered? How will patients do? Bassel Abou-Khalil, M.D.
 Epilepsy Surgery: Who should be considered? How will patients do? Bassel Abou-Khalil, M.D. Disclosures none Self-assessment questions Q1- Which qualify for drug resistance in focal epilepsy? A. Failure
Epilepsy Surgery: Who should be considered? How will patients do? Bassel Abou-Khalil, M.D. Disclosures none Self-assessment questions Q1- Which qualify for drug resistance in focal epilepsy? A. Failure
Approximately 70% of childhood SURGICAL TREATMENTS FOR PEDIATRIC EPILEPSY PROCEEDINGS. Ronald P. Lesser, MD KEY POINTS
 ASIM May p153-158 5/14/01 9:19 AM Page 153 SURGICAL TREATMENTS FOR PEDIATRIC EPILEPSY Ronald P. Lesser, MD KEY POINTS Most children with epilepsy refractory to drugs can improve with surgery Temporal lobe
ASIM May p153-158 5/14/01 9:19 AM Page 153 SURGICAL TREATMENTS FOR PEDIATRIC EPILEPSY Ronald P. Lesser, MD KEY POINTS Most children with epilepsy refractory to drugs can improve with surgery Temporal lobe
5/22/2009. Pediatric Neurosurgery Pediatric Neurology Neuroradiology Neurophysiology Neuropathology Neuropsychology
 Current Surgical Treatment Strategies for the Management of Pediatric Epilepsy University of California, San Francisco Department of Neurological Surgery San Francisco, California Kurtis Ian Auguste, M.D.
Current Surgical Treatment Strategies for the Management of Pediatric Epilepsy University of California, San Francisco Department of Neurological Surgery San Francisco, California Kurtis Ian Auguste, M.D.
EPILEPSY SURGERY- SURGICAL PROCEDURES
 EPILEPSY SURGERY- SURGICAL PROCEDURES When to consider epilepsy surgery? Persistent Seizures despite adequate pharmacological treatment Drug resistant epilepsy may be defined as failure of adequate trials
EPILEPSY SURGERY- SURGICAL PROCEDURES When to consider epilepsy surgery? Persistent Seizures despite adequate pharmacological treatment Drug resistant epilepsy may be defined as failure of adequate trials
Surgical Modalities for Epilepsy Treatment. C.J. Bui, MD, FAANS Ochsner Neuroscience Symposium 2016
 Surgical Modalities for Epilepsy Treatment C.J. Bui, MD, FAANS Ochsner Neuroscience Symposium 2016 Conflict of Interest Nothing to disclose Surgical Modalities Diagnostic Subdural Grids Depth Electrodes
Surgical Modalities for Epilepsy Treatment C.J. Bui, MD, FAANS Ochsner Neuroscience Symposium 2016 Conflict of Interest Nothing to disclose Surgical Modalities Diagnostic Subdural Grids Depth Electrodes
EMG, EEG, and Neurophysiology in Clinical Practice
 Mayo School of Continuous Professional Development EMG, EEG, and Neurophysiology in Clinical Practice Matthew T. Hoerth, M.D. Ritz-Carlton, Amelia Island, Florida January 29-February 4, 2017 2016 MFMER
Mayo School of Continuous Professional Development EMG, EEG, and Neurophysiology in Clinical Practice Matthew T. Hoerth, M.D. Ritz-Carlton, Amelia Island, Florida January 29-February 4, 2017 2016 MFMER
Surgery for Medically Refractory Focal Epilepsy
 Surgery for Medically Refractory Focal Epilepsy Seth F Oliveria, MD PhD The Oregon Clinic Neurosurgery Director of Functional Neurosurgery: Providence Brain and Spine Institute Portland, OR Providence
Surgery for Medically Refractory Focal Epilepsy Seth F Oliveria, MD PhD The Oregon Clinic Neurosurgery Director of Functional Neurosurgery: Providence Brain and Spine Institute Portland, OR Providence
Candidates for Epilepsy Surgery. Presurgical Evaluation. Presurgical Evaluation. Presurgical Evaluation. Presurgical Evaluation 8/27/2017
 PresurgicalEpilepsy Eval: A multidisciplinary approach to intractable epilepsy Tayard Desudchit MD Faculty Of Medicine Chulalongkorn U. Candidates for Epilepsy Surgery Persistent seizures despite appropriate
PresurgicalEpilepsy Eval: A multidisciplinary approach to intractable epilepsy Tayard Desudchit MD Faculty Of Medicine Chulalongkorn U. Candidates for Epilepsy Surgery Persistent seizures despite appropriate
Presurgical Evaluation before Epilepsy Surgery
 Presurgical Evaluation before Epilepsy Surgery Epilepsy Course for Neurology Resident 2015 Kanjana Unnwongse- Wehner, MD Prasat Neurological Epilepsy Center Facts About Epilepsy & Surgery Localization-related
Presurgical Evaluation before Epilepsy Surgery Epilepsy Course for Neurology Resident 2015 Kanjana Unnwongse- Wehner, MD Prasat Neurological Epilepsy Center Facts About Epilepsy & Surgery Localization-related
Epilepsy surgery. Loránd Eross. National Institute of Clinical Neurosciences. Semmelweis University, 2018.
 Epilepsy surgery Loránd Eross National Institute of Clinical Neurosciences Semmelweis University, 2018. Epilepsy surgery Medicaltreatment Seizure free:70% Surgical treatment Seizure fee:15% Neuromodulation
Epilepsy surgery Loránd Eross National Institute of Clinical Neurosciences Semmelweis University, 2018. Epilepsy surgery Medicaltreatment Seizure free:70% Surgical treatment Seizure fee:15% Neuromodulation
Epilepsy & Functional Neurosurgery
 Epilepsy & Functional Neurosurgery An Introduction The LSU-Shreveport Department of Neurosurgery Presenting Authors: Neurosurgery Residents & Faculty Epilepsy Neurosurgery What is a seizure? continuous
Epilepsy & Functional Neurosurgery An Introduction The LSU-Shreveport Department of Neurosurgery Presenting Authors: Neurosurgery Residents & Faculty Epilepsy Neurosurgery What is a seizure? continuous
SEIZURE OUTCOME AFTER EPILEPSY SURGERY
 SEIZURE OUTCOME AFTER EPILEPSY SURGERY Prakash Kotagal, M.D. Head, Pediatric Epilepsy Cleveland Clinic Epilepsy Center LEFT TEMPORAL LOBE ASTROCYTOMA SEIZURE OUTCOME 1 YEAR AFTER EPILEPSY SURGERY IN ADULTS
SEIZURE OUTCOME AFTER EPILEPSY SURGERY Prakash Kotagal, M.D. Head, Pediatric Epilepsy Cleveland Clinic Epilepsy Center LEFT TEMPORAL LOBE ASTROCYTOMA SEIZURE OUTCOME 1 YEAR AFTER EPILEPSY SURGERY IN ADULTS
Methods of epilepsy surgery
 Chapter 47 Methods of epilepsy surgery ANDREW W. McEVOY 1 and WILLIAM J.F. HARKNESS 2 1 Institute of Neurology, University College, London, National Hospital for Neurology and Neurosurgery, Queen Square,
Chapter 47 Methods of epilepsy surgery ANDREW W. McEVOY 1 and WILLIAM J.F. HARKNESS 2 1 Institute of Neurology, University College, London, National Hospital for Neurology and Neurosurgery, Queen Square,
Epilepsy. Hyunmi Choi, M.D., M.S. Columbia Comprehensive Epilepsy Center The Neurological Institute. Seizure
 Epilepsy Hyunmi Choi, M.D., M.S. Columbia Comprehensive Epilepsy Center The Neurological Institute Seizure Symptom Transient event Paroxysmal Temporary physiologic dysfunction Caused by self-limited, abnormal,
Epilepsy Hyunmi Choi, M.D., M.S. Columbia Comprehensive Epilepsy Center The Neurological Institute Seizure Symptom Transient event Paroxysmal Temporary physiologic dysfunction Caused by self-limited, abnormal,
AMERICAN BOARD OF PSYCHIATRY AND NEUROLOGY, INC. SUBSPECIALTY CERTIFICATION EXAMINATION IN EPILEPSY MEDICINE
 SUBSPECIALTY CERTIFICATION EXAMINATION IN EPILEPSY MEDICINE 2014 Content Blueprint (November 26, 2012) Number of questions: 200 I. Classification 7 9% II. Routine EEG 16 20% III. Evaluation 22 26% IV.
SUBSPECIALTY CERTIFICATION EXAMINATION IN EPILEPSY MEDICINE 2014 Content Blueprint (November 26, 2012) Number of questions: 200 I. Classification 7 9% II. Routine EEG 16 20% III. Evaluation 22 26% IV.
9/30/2016. Advances in Epilepsy Surgery. Epidemiology. Epidemiology
 Advances in Epilepsy Surgery George Jallo, M.D. Director, Institute for Brain Protection Sciences Johns Hopkins All Children s Hospital St Petersburg, Florida Epidemiology WHO lists it as the second most
Advances in Epilepsy Surgery George Jallo, M.D. Director, Institute for Brain Protection Sciences Johns Hopkins All Children s Hospital St Petersburg, Florida Epidemiology WHO lists it as the second most
AMERICAN BOARD OF CLINICAL NEUROPHYSIOLOGY
 AMERICAN BOARD OF CLINICAL NEUROPHYSIOLOGY Part I Content Outline I. Physiology and Instrumentation 30% A. Physiology 1. Anatomy of neural generation 2. Mechanisms of EEG and evoked potential generation
AMERICAN BOARD OF CLINICAL NEUROPHYSIOLOGY Part I Content Outline I. Physiology and Instrumentation 30% A. Physiology 1. Anatomy of neural generation 2. Mechanisms of EEG and evoked potential generation
PRESURGICAL EVALUATION. ISLAND OF COS Hippocrates: On the Sacred Disease. Disclosure Research-Educational Grants. Patients with seizure disorders
 PRESURGICAL EVALUATION Patients with seizure disorders Gregory D. Cascino, MD Mayo Clinic Disclosure Research-Educational Grants Mayo Foundation Neuro Pace, Inc. American Epilepsy Society American Academy
PRESURGICAL EVALUATION Patients with seizure disorders Gregory D. Cascino, MD Mayo Clinic Disclosure Research-Educational Grants Mayo Foundation Neuro Pace, Inc. American Epilepsy Society American Academy
ChosingPhase 2 Electrodes
 ChosingPhase 2 Electrodes ACNS Course ECoG/Invasive EEG Houston, February 4 th, 2015 Stephan Schuele, MD, MPH Comprehensive Epilepsy Center Northwestern Memorial Hospital Northwestern University, Feinberg
ChosingPhase 2 Electrodes ACNS Course ECoG/Invasive EEG Houston, February 4 th, 2015 Stephan Schuele, MD, MPH Comprehensive Epilepsy Center Northwestern Memorial Hospital Northwestern University, Feinberg
Epilepsy Surgery, Imaging, and Intraoperative Neuromonitoring: Surgical Perspective
 Epilepsy Surgery, Imaging, and Intraoperative Neuromonitoring: Surgical Perspective AC Duhaime, M.D. Director, Pediatric Neurosurgery, Massachusetts General Hospital Professor, Neurosurgery, Harvard Medical
Epilepsy Surgery, Imaging, and Intraoperative Neuromonitoring: Surgical Perspective AC Duhaime, M.D. Director, Pediatric Neurosurgery, Massachusetts General Hospital Professor, Neurosurgery, Harvard Medical
Multimodal Imaging in Extratemporal Epilepsy Surgery
 Open Access Case Report DOI: 10.7759/cureus.2338 Multimodal Imaging in Extratemporal Epilepsy Surgery Christian Vollmar 1, Aurelia Peraud 2, Soheyl Noachtar 1 1. Epilepsy Center, Dept. of Neurology, University
Open Access Case Report DOI: 10.7759/cureus.2338 Multimodal Imaging in Extratemporal Epilepsy Surgery Christian Vollmar 1, Aurelia Peraud 2, Soheyl Noachtar 1 1. Epilepsy Center, Dept. of Neurology, University
Diagnosing Complicated Epilepsy: Mapping of the Epileptic Circuitry. Michael R. Sperling, M.D. Thomas Jefferson University Philadelphia, PA
 Diagnosing Complicated Epilepsy: Mapping of the Epileptic Circuitry Michael R. Sperling, M.D. Thomas Jefferson University Philadelphia, PA Overview Definition of epileptic circuitry Methods of mapping
Diagnosing Complicated Epilepsy: Mapping of the Epileptic Circuitry Michael R. Sperling, M.D. Thomas Jefferson University Philadelphia, PA Overview Definition of epileptic circuitry Methods of mapping
SUBSPECIALTY CERTIFICATION EXAMINATION IN EPILEPSY MEDICINE Content Blueprint (December 21, 2015)
") SUBSPECIALTY CERTIFICATION EXAMINATION IN EPILEPSY MEDICINE 2016 Content Blueprint (December 21, 2015) Number of questions: 200 1. Classification 8-12% 2. Routine EEG 16-20% 3. Evaluation 23-27% 4. Management
SUBSPECIALTY CERTIFICATION EXAMINATION IN EPILEPSY MEDICINE 2016 Content Blueprint (December 21, 2015) Number of questions: 200 1. Classification 8-12% 2. Routine EEG 16-20% 3. Evaluation 23-27% 4. Management
The American Approach to Depth Electrode Insertion December 4, 2012
 The American Approach to Depth Electrode Insertion December 4, 2012 Jonathan Miller, MD Director, Epilepsy Surgery University Hospitals Case Medical Center/Case Western Reserve University Cleveland, Ohio
The American Approach to Depth Electrode Insertion December 4, 2012 Jonathan Miller, MD Director, Epilepsy Surgery University Hospitals Case Medical Center/Case Western Reserve University Cleveland, Ohio
Surgical Treatment of Epilepsy
 Presurgical Assessment and the Surgical Treatment of Epilepsy Michael C., MD Director, Rush Epilepsy Center Associate Professor and Senior Attending Neurologist Rush University Medical Center Chicago,
Presurgical Assessment and the Surgical Treatment of Epilepsy Michael C., MD Director, Rush Epilepsy Center Associate Professor and Senior Attending Neurologist Rush University Medical Center Chicago,
Epilepsy surgery. John S Duncan. Who are candidates for epilepsy surgery? The context of epilepsy surgery ORIGINAL PAPERS
 ORIGINAL PAPERS Epilepsy surgery John S Duncan ABSTRACT If the first two or three antiepileptic drugs used do not control epilepsy, there is little chance that subsequent medications will be effective.
ORIGINAL PAPERS Epilepsy surgery John S Duncan ABSTRACT If the first two or three antiepileptic drugs used do not control epilepsy, there is little chance that subsequent medications will be effective.
Interictal High Frequency Oscillations as Neurophysiologic Biomarkers of Epileptogenicity
 Interictal High Frequency Oscillations as Neurophysiologic Biomarkers of Epileptogenicity December 10, 2013 Joyce Y. Wu, MD Associate Professor Division of Pediatric Neurology David Geffen School of Medicine
Interictal High Frequency Oscillations as Neurophysiologic Biomarkers of Epileptogenicity December 10, 2013 Joyce Y. Wu, MD Associate Professor Division of Pediatric Neurology David Geffen School of Medicine
Accepted Manuscript. Editorial. Responsive neurostimulation for epilepsy: more than stimulation. Jayant N. Acharya
 Accepted Manuscript Editorial Responsive neurostimulation for epilepsy: more than stimulation Jayant N. Acharya PII: S2467-981X(18)30022-2 DOI: https://doi.org/10.1016/j.cnp.2018.06.002 Reference: CNP
Accepted Manuscript Editorial Responsive neurostimulation for epilepsy: more than stimulation Jayant N. Acharya PII: S2467-981X(18)30022-2 DOI: https://doi.org/10.1016/j.cnp.2018.06.002 Reference: CNP
Vagus nerve stimulation for refractory epilepsy
 Seizure 2001; 10: 456 460 doi:10.1053/seiz.2001.0628, available online at http://www.idealibrary.com on CASE REPORT Vagus nerve stimulation for refractory epilepsy PAUL BOON, KRISTL VONCK, JACQUES DE REUCK
Seizure 2001; 10: 456 460 doi:10.1053/seiz.2001.0628, available online at http://www.idealibrary.com on CASE REPORT Vagus nerve stimulation for refractory epilepsy PAUL BOON, KRISTL VONCK, JACQUES DE REUCK
The Changing Surgical Landscape in Kids
 The Changing Surgical Landscape in Kids December 7, 2013 Howard L. Weiner, MD NYU Langone Medical Center American Epilepsy Society Annual Meeting Disclosure none American Epilepsy Society 2013 Annual Meeting
The Changing Surgical Landscape in Kids December 7, 2013 Howard L. Weiner, MD NYU Langone Medical Center American Epilepsy Society Annual Meeting Disclosure none American Epilepsy Society 2013 Annual Meeting
Epilepsy & Behavior Case Reports
 Epilepsy & Behavior Case Reports 1 (2013) 45 49 Contents lists available at ScienceDirect Epilepsy & Behavior Case Reports journal homepage: www.elsevier.com/locate/ebcr Case Report Partial disconnection
Epilepsy & Behavior Case Reports 1 (2013) 45 49 Contents lists available at ScienceDirect Epilepsy & Behavior Case Reports journal homepage: www.elsevier.com/locate/ebcr Case Report Partial disconnection
How do we evaluate patients before epilepsy surgery?
 How do we evaluate patients before epilepsy surgery? Yotin Chinvarun, MD Chaiyos Khongkhatithum, MD How do we evaluate patients before epilepsy surgery? Chaiyos Khongkhatithum, MD Division of Neurology
How do we evaluate patients before epilepsy surgery? Yotin Chinvarun, MD Chaiyos Khongkhatithum, MD How do we evaluate patients before epilepsy surgery? Chaiyos Khongkhatithum, MD Division of Neurology
Epilepsies of Childhood: An Over-view of Treatment 2 nd October 2018
 Epilepsies of Childhood: An Over-view of Treatment 2 nd October 2018 Dr Sophia Varadkar MRCPI, PhD Consultant Paediatric Neurologist and Honorary Senior Lecturer Great Ormond Street Hospital for Children
Epilepsies of Childhood: An Over-view of Treatment 2 nd October 2018 Dr Sophia Varadkar MRCPI, PhD Consultant Paediatric Neurologist and Honorary Senior Lecturer Great Ormond Street Hospital for Children
Case reports functional imaging in epilepsy
 Seizure 2001; 10: 157 161 doi:10.1053/seiz.2001.0552, available online at http://www.idealibrary.com on Case reports functional imaging in epilepsy MARK P. RICHARDSON Medical Research Council Fellow, Institute
Seizure 2001; 10: 157 161 doi:10.1053/seiz.2001.0552, available online at http://www.idealibrary.com on Case reports functional imaging in epilepsy MARK P. RICHARDSON Medical Research Council Fellow, Institute
EPILEPSY. New Ideas about an Old Disease. Gregory D. Cascino, MD
 EPILEPSY New Ideas about an Old Disease Gregory D. Cascino, MD Disclosure Research-Educational Grants Neuro Pace, Inc. American Epilepsy Society American Academy of Neurology Neurology (Associate Editor)
EPILEPSY New Ideas about an Old Disease Gregory D. Cascino, MD Disclosure Research-Educational Grants Neuro Pace, Inc. American Epilepsy Society American Academy of Neurology Neurology (Associate Editor)
Surgery Insight: surgical management of epilepsy
 Surgery Insight: surgical management of epilepsy Ruben Kuzniecky* and Orrin Devinsky SUMMARY Epilepsy surgery has been shown to be an effective treatment for patients with intractable epilepsy. The only
Surgery Insight: surgical management of epilepsy Ruben Kuzniecky* and Orrin Devinsky SUMMARY Epilepsy surgery has been shown to be an effective treatment for patients with intractable epilepsy. The only
High Resolution Ictal SPECT: Enhanced Epileptic Source Targeting?
 High Resolution Ictal SPECT: Enhanced Epileptic Source Targeting? Marvin A Rossi MD, PhD RUSH Epilepsy Center Research Lab http://www.synapticom.net Chicago, IL USA Medically-Refractory Epilepsy 500,000-800,000
High Resolution Ictal SPECT: Enhanced Epileptic Source Targeting? Marvin A Rossi MD, PhD RUSH Epilepsy Center Research Lab http://www.synapticom.net Chicago, IL USA Medically-Refractory Epilepsy 500,000-800,000
Est-ce que l'eeg a toujours sa place en 2019?
 Est-ce que l'eeg a toujours sa place en 2019? Thomas Bast Epilepsy Center Kork, Germany Does EEG still play a role in 2019? What a question 7T-MRI, fmri, DTI, MEG, SISCOM, Of ieeg course! /HFO, Genetics
Est-ce que l'eeg a toujours sa place en 2019? Thomas Bast Epilepsy Center Kork, Germany Does EEG still play a role in 2019? What a question 7T-MRI, fmri, DTI, MEG, SISCOM, Of ieeg course! /HFO, Genetics
Pediatric Epilepsy Surgery. W. Donald Shields, MD Emeritus Professor of Neurology and Pediatrics David Geffen School of Medicine at UCLA
 Pediatric Epilepsy Surgery W. Donald Shields, MD Emeritus Professor of Neurology and Pediatrics David Geffen School of Medicine at UCLA PEDIATRIC EPILEPSY SURGERY A THING OF BEAUTY IF DONE RIGHT PEDIATRIC
Pediatric Epilepsy Surgery W. Donald Shields, MD Emeritus Professor of Neurology and Pediatrics David Geffen School of Medicine at UCLA PEDIATRIC EPILEPSY SURGERY A THING OF BEAUTY IF DONE RIGHT PEDIATRIC
Neuromodulation in Epilepsy. Gregory C. Mathews, M.D., Ph.D.
 Neuromodulation in Epilepsy Gregory C. Mathews, M.D., Ph.D. Disclosure There are no disclosures to share with regards to this presentation. Epilepsy Basics What is epilepsy? Partial versus generalized
Neuromodulation in Epilepsy Gregory C. Mathews, M.D., Ph.D. Disclosure There are no disclosures to share with regards to this presentation. Epilepsy Basics What is epilepsy? Partial versus generalized
PART I EXAMINATION INFOMATION. Part I Content Outline
 PART I EXAMINATION INFOMATION The three-hour examination will be administered during an established two-week testing period at PSI Computer Testing, Inc. The examination consists of 120 objective, multiple-choice
PART I EXAMINATION INFOMATION The three-hour examination will be administered during an established two-week testing period at PSI Computer Testing, Inc. The examination consists of 120 objective, multiple-choice
Intracranial Studies Of Human Epilepsy In A Surgical Setting
 Intracranial Studies Of Human Epilepsy In A Surgical Setting Department of Neurology David Geffen School of Medicine at UCLA Presentation Goals Epilepsy and seizures Basics of the electroencephalogram
Intracranial Studies Of Human Epilepsy In A Surgical Setting Department of Neurology David Geffen School of Medicine at UCLA Presentation Goals Epilepsy and seizures Basics of the electroencephalogram
The Surgical Treatment of Epilepsy
 The Surgical Treatment of Epilepsy Jeffrey S. Schweitzer, MD, PhD Kaiser Los Angeles Medical Center Division of Restorative Neurosurgery Ancient craniotomy When Cao started complaining about splitting
The Surgical Treatment of Epilepsy Jeffrey S. Schweitzer, MD, PhD Kaiser Los Angeles Medical Center Division of Restorative Neurosurgery Ancient craniotomy When Cao started complaining about splitting
Faculty/Presenter Disclosure. Intracranial EEG Recording. Objectives. General Themes. Why invasive recordings? 6/27/2018
 CFPC CoI Templates: Slide 1 used in Faculty presentation only. Faculty/Presenter Disclosure Intracranial EEG Recording Faculty: Dr Richard S McLachlan Relationships with financial sponsors: None currently
CFPC CoI Templates: Slide 1 used in Faculty presentation only. Faculty/Presenter Disclosure Intracranial EEG Recording Faculty: Dr Richard S McLachlan Relationships with financial sponsors: None currently
Epilepsy. Epileptic seizures: an abnormal and excessive discharge of brain neurons involving hypersynchrony accompanied by some behavioral change.
 Epilepsy Epileptic seizures: an abnormal and excessive discharge of brain neurons involving hypersynchrony accompanied by some behavioral change. Hystory of epilepsy 1. Origin of the name of epilepsy:
Epilepsy Epileptic seizures: an abnormal and excessive discharge of brain neurons involving hypersynchrony accompanied by some behavioral change. Hystory of epilepsy 1. Origin of the name of epilepsy:
Attending: a medical doctor (MD or OD) who has completed medical school, residency, and often a specialized fellowship
 who has completed medical school, residency, and often a specialized fellowship") Descriptions for members of the Epilepsy Team Attending: a medical doctor (MD or OD) who has completed medical school, residency, and often a specialized fellowship Fellow: a medical doctor (MD or OD)
Descriptions for members of the Epilepsy Team Attending: a medical doctor (MD or OD) who has completed medical school, residency, and often a specialized fellowship Fellow: a medical doctor (MD or OD)
EPILEPSY SURGERY EVALUATION IN ADULTS WITH SCALP VIDEO-EEG MONITORING. Meriem Bensalem-Owen, MD University of Kentucky
 EPILEPSY SURGERY EVALUATION IN ADULTS WITH SCALP VIDEO-EEG MONITORING Meriem Bensalem-Owen, MD University of Kentucky DISCLOSURES Received grants for sponsored research as investigator from: UCB Eisai
EPILEPSY SURGERY EVALUATION IN ADULTS WITH SCALP VIDEO-EEG MONITORING Meriem Bensalem-Owen, MD University of Kentucky DISCLOSURES Received grants for sponsored research as investigator from: UCB Eisai
Subject: Magnetoencephalography/Magnetic Source Imaging
 01-95805-16 Original Effective Date: 09/01/01 Reviewed: 07/26/18 Revised: 08/15/18 Subject: Magnetoencephalography/Magnetic Source Imaging THIS MEDICAL COVERAGE GUIDELINE IS NOT AN AUTHORIZATION, CERTIFICATION,
01-95805-16 Original Effective Date: 09/01/01 Reviewed: 07/26/18 Revised: 08/15/18 Subject: Magnetoencephalography/Magnetic Source Imaging THIS MEDICAL COVERAGE GUIDELINE IS NOT AN AUTHORIZATION, CERTIFICATION,
EPILEPSY 2018: UPDATE ON MODERN SURGICAL MANAGEMENT. Robert Kellogg, MD Advocate Children s Hospital Park Ridge, IL April 20, 2018
 EPILEPSY 2018: UPDATE ON MODERN SURGICAL MANAGEMENT Robert Kellogg, MD Advocate Children s Hospital Park Ridge, IL April 20, 2018 No disclosures OBJECTIVES Brief history of epilepsy surgery Pre-operative
EPILEPSY 2018: UPDATE ON MODERN SURGICAL MANAGEMENT Robert Kellogg, MD Advocate Children s Hospital Park Ridge, IL April 20, 2018 No disclosures OBJECTIVES Brief history of epilepsy surgery Pre-operative
SURGICAL MANAGEMENT OF DRUG-RESISTANT FOCAL EPILEPSY
 SURGICAL MANAGEMENT OF DRUG-RESISTANT FOCAL EPILEPSY Gregory D. Cascino, MD, FAAN Epilepsy surgery is underutilized in patients with focal seizures refractory to appropriate antiepileptic drug (AED) trials
SURGICAL MANAGEMENT OF DRUG-RESISTANT FOCAL EPILEPSY Gregory D. Cascino, MD, FAAN Epilepsy surgery is underutilized in patients with focal seizures refractory to appropriate antiepileptic drug (AED) trials
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Functional Neurosurgery Brian L. Hoh, MD 1 and Gregory J. Zipfel, MD 2 1 University of Florida, 2 Washington University Functional Neurosurgery Functional
Introduction to Neurosurgical Subspecialties: Functional Neurosurgery Brian L. Hoh, MD 1 and Gregory J. Zipfel, MD 2 1 University of Florida, 2 Washington University Functional Neurosurgery Functional
The relevance of somatosensory auras in refractory temporal lobe epilepsies
 BRIEF COMMUNICATION The relevance of somatosensory auras in refractory temporal lobe epilepsies Ghazala Perven, Ruta Yardi, Juan Bulacio, Imad Najm, William Bingaman, Jorge Gonzalez-Martinez, and Lara
BRIEF COMMUNICATION The relevance of somatosensory auras in refractory temporal lobe epilepsies Ghazala Perven, Ruta Yardi, Juan Bulacio, Imad Najm, William Bingaman, Jorge Gonzalez-Martinez, and Lara
Responsive Neurostimulation for the Treatment of Refractory Partial Epilepsy. Summary
 Page: 1 of 12 Last Review Status/Date: March 2015 Refractory Partial Epilepsy Summary Responsive neurostimulation (RNS) for the treatment of epilepsy involves the use of 1 or more implantable electric
Page: 1 of 12 Last Review Status/Date: March 2015 Refractory Partial Epilepsy Summary Responsive neurostimulation (RNS) for the treatment of epilepsy involves the use of 1 or more implantable electric
Level 4 comprehensive epilepsy program in Malaysia, a resource-limited country
 Neurology Asia 2017; 22(4) : 299 305 Level 4 comprehensive epilepsy program in Malaysia, a resource-limited country 1 Kheng-Seang Lim, 1 Sherrini Ahmad Bazir Ahmad, 2 Vairavan Narayanan, 3 Kartini Rahmat,
Neurology Asia 2017; 22(4) : 299 305 Level 4 comprehensive epilepsy program in Malaysia, a resource-limited country 1 Kheng-Seang Lim, 1 Sherrini Ahmad Bazir Ahmad, 2 Vairavan Narayanan, 3 Kartini Rahmat,
Surgical Management of Post- Traumatic Epilepsy Complexities-Adhesions and Multifocality
 Surgical Management of Post- Traumatic Epilepsy Complexities-Adhesions and Multifocality December 2, 2012 Jeffrey P. Blount MD Division of Neurosurgery University of Alabama at Birmingham Children s of
Surgical Management of Post- Traumatic Epilepsy Complexities-Adhesions and Multifocality December 2, 2012 Jeffrey P. Blount MD Division of Neurosurgery University of Alabama at Birmingham Children s of
Invasive Evaluation for Epilepsy Surgery Lesional Cases NO DISCLOSURES. Mr. Johnson. Seizures at 29 Years of Age. Dileep Nair, MD Juan Bulacio, MD
 Invasive Evaluation for Epilepsy Surgery Lesional Cases NO DISCLOSURES Dileep Nair, MD Juan Bulacio, MD Mr. Johnson Seizures at 29 Years of Age Onset of seizures at 16 years of age bed wetting episodes
Invasive Evaluation for Epilepsy Surgery Lesional Cases NO DISCLOSURES Dileep Nair, MD Juan Bulacio, MD Mr. Johnson Seizures at 29 Years of Age Onset of seizures at 16 years of age bed wetting episodes
Fu n c t i o n a l hemispherotomy has been used since the. Hemispherotomy: efficacy and analysis of seizure recurrence.
 J Neurosurg Pediatrics 4:000 000, 4:323 332, 2009 Hemispherotomy: efficacy and analysis of seizure recurrence Clinical article Dav i d D. Li m b r i c k Jr., M.D., Ph.D., 1 Pr i t h v i Na r aya n, M.D.,
J Neurosurg Pediatrics 4:000 000, 4:323 332, 2009 Hemispherotomy: efficacy and analysis of seizure recurrence Clinical article Dav i d D. Li m b r i c k Jr., M.D., Ph.D., 1 Pr i t h v i Na r aya n, M.D.,
Diffusion Tensor Imaging 12/06/2013
 12/06/2013 Beate Diehl, MD PhD FRCP University College London National Hospital for Neurology and Neurosurgery Queen Square London, UK American Epilepsy Society Annual Meeting Disclosure None Learning
12/06/2013 Beate Diehl, MD PhD FRCP University College London National Hospital for Neurology and Neurosurgery Queen Square London, UK American Epilepsy Society Annual Meeting Disclosure None Learning
Epilepsy Research: SLATE
 Epilepsy Research: SLATE Jason M. Schwalb, MD, FAANS, FACS Clinical Associate Professor of Neurosurgery Surgical Director, Movement Disorder & Comprehensive Epilepsy Centers Research Scientist, Center
Epilepsy Research: SLATE Jason M. Schwalb, MD, FAANS, FACS Clinical Associate Professor of Neurosurgery Surgical Director, Movement Disorder & Comprehensive Epilepsy Centers Research Scientist, Center
Common Ictal Patterns in Patients with Documented Epileptic Seizures
 THE ICTAL IRAQI PATTERNS POSTGRADUATE IN EPILEPTIC MEDICAL JOURNAL PATIENTS Common Ictal Patterns in Documented Epileptic Seizures Ghaieb Bashar ALJandeel, Gonzalo Alarcon ABSTRACT: BACKGROUND: The ictal
THE ICTAL IRAQI PATTERNS POSTGRADUATE IN EPILEPTIC MEDICAL JOURNAL PATIENTS Common Ictal Patterns in Documented Epileptic Seizures Ghaieb Bashar ALJandeel, Gonzalo Alarcon ABSTRACT: BACKGROUND: The ictal
Early seizure propagation from the occipital lobe to medial temporal structures and its surgical implication
 Original article Epileptic Disord 2008; 10 (4): 260-5 Early seizure propagation from the occipital lobe to medial temporal structures and its surgical implication Naotaka Usui, Tadahiro Mihara, Koichi
Original article Epileptic Disord 2008; 10 (4): 260-5 Early seizure propagation from the occipital lobe to medial temporal structures and its surgical implication Naotaka Usui, Tadahiro Mihara, Koichi
Surgical therapy for medically intractable epilepsy. Department of Neurological Surgery, University of Washington, Seattle, Washington
 J Neurosurg 66:489-499, 1987 Review Article Surgical therapy for medically intractable epilepsy GEORGE A. OJEMANN, M.D. Department of Neurological Surgery, University of Washington, Seattle, Washington
J Neurosurg 66:489-499, 1987 Review Article Surgical therapy for medically intractable epilepsy GEORGE A. OJEMANN, M.D. Department of Neurological Surgery, University of Washington, Seattle, Washington
Epilepsy: diagnosis and treatment. Sergiusz Jóźwiak Klinika Neurologii Dziecięcej WUM
 Epilepsy: diagnosis and treatment Sergiusz Jóźwiak Klinika Neurologii Dziecięcej WUM Definition: the clinical manifestation of an excessive excitation of a population of cortical neurons Neurotransmitters:
Epilepsy: diagnosis and treatment Sergiusz Jóźwiak Klinika Neurologii Dziecięcej WUM Definition: the clinical manifestation of an excessive excitation of a population of cortical neurons Neurotransmitters:
Review Article Development of a Comprehensive Epilepsy Surgery Programme in Pakistan Introduction and Background
 Review Article Development of a Comprehensive Epilepsy Surgery Programme in Pakistan Mughis Sheerani Section of Neurology, Department of Medicine, Aga Khan University Hospital, Karachi. Introduction and
Review Article Development of a Comprehensive Epilepsy Surgery Programme in Pakistan Mughis Sheerani Section of Neurology, Department of Medicine, Aga Khan University Hospital, Karachi. Introduction and
The Sonification of Human EEG and other Biomedical Data. Part 3
 The Sonification of Human EEG and other Biomedical Data Part 3 The Human EEG A data source for the sonification of cerebral dynamics The Human EEG - Outline Electric brain signals Continuous recording
The Sonification of Human EEG and other Biomedical Data Part 3 The Human EEG A data source for the sonification of cerebral dynamics The Human EEG - Outline Electric brain signals Continuous recording
Difficult-to-Localize Intractable Focal Epilepsy: An In-Depth Look
 Current Literature In Clinical Science Difficult-to-Localize Intractable Focal Epilepsy: An In-Depth Look Stereoelectroencephalography in the Difficult to Localize Refractory Focal Epilepsy: Early Experience
Current Literature In Clinical Science Difficult-to-Localize Intractable Focal Epilepsy: An In-Depth Look Stereoelectroencephalography in the Difficult to Localize Refractory Focal Epilepsy: Early Experience
FUNCTIONAL MRI IN EPILEPSY December 6 th 2013
 FUNCTIONAL MRI IN EPILEPSY December 6 th 2013 Matthias J Koepp, MD, PhD UCL Institute of Neurology National Hospital for Neurology and Neurosurgery London, UK American Epilepsy Society Annual Meeting Disclosure
FUNCTIONAL MRI IN EPILEPSY December 6 th 2013 Matthias J Koepp, MD, PhD UCL Institute of Neurology National Hospital for Neurology and Neurosurgery London, UK American Epilepsy Society Annual Meeting Disclosure
Name: Chusak Limotai Student ID: Ph.D. Clinical Epidemiology
 RACE 611: Clinical Epidemiology and Evidence-based Medicine Assignment VII: CAT presentation CAT FOR PROGNOSIS Temporal plus epilepsy is a major determinant of temporal lobe surgery failures Clinical Question:
RACE 611: Clinical Epidemiology and Evidence-based Medicine Assignment VII: CAT presentation CAT FOR PROGNOSIS Temporal plus epilepsy is a major determinant of temporal lobe surgery failures Clinical Question:
Epilepsy, a common chronic neurological disorder, is a
 10 SUPPLEMENT TO Journal of the association of physicians of india august 2013 VOL. 61 Epilepsy: Diagnostic Evaluation JMK Murthy* Epilepsy, a common chronic neurological disorder, is a potentially treatable
10 SUPPLEMENT TO Journal of the association of physicians of india august 2013 VOL. 61 Epilepsy: Diagnostic Evaluation JMK Murthy* Epilepsy, a common chronic neurological disorder, is a potentially treatable
Review of Epilepsy Surgery and its Practical Applications
 Review of Epilepsy Surgery and its Practical Applications Dr Vijaykumar S Shabadi 1, Dr J Chandramohan 2 M.Ch Neurosurgery. Consultant Neurosurgeon, Dhanush Hospital, Bagalkot 587101 MS, Consultant and
Review of Epilepsy Surgery and its Practical Applications Dr Vijaykumar S Shabadi 1, Dr J Chandramohan 2 M.Ch Neurosurgery. Consultant Neurosurgeon, Dhanush Hospital, Bagalkot 587101 MS, Consultant and
Depth/Surface Relationships: Confronting noninvasive measures to intracerebral EEG
 Depth/Surface Relationships: Confronting noninvasive measures to intracerebral EEG Christian G Bénar Institut de Neurosciences des Systèmes; INSERM, Aix-Marseille Université christian.benar@univ-amu.fr
Depth/Surface Relationships: Confronting noninvasive measures to intracerebral EEG Christian G Bénar Institut de Neurosciences des Systèmes; INSERM, Aix-Marseille Université christian.benar@univ-amu.fr
Epilepsy: Medical and Surgical Approaches
 Focus on CME at the University of Calgary Epilepsy: Medical and Surgical Approaches There are several relatively new options for physicians to explore in the areas of epilepsy diagnosis and treatment.
Focus on CME at the University of Calgary Epilepsy: Medical and Surgical Approaches There are several relatively new options for physicians to explore in the areas of epilepsy diagnosis and treatment.
EEG IN FOCAL ENCEPHALOPATHIES: CEREBROVASCULAR DISEASE, NEOPLASMS, AND INFECTIONS
 246 Figure 8.7: FIRDA. The patient has a history of nonspecific cognitive decline and multiple small WM changes on imaging. oligodendrocytic tumors of the cerebral hemispheres (11,12). Electroencephalogram
246 Figure 8.7: FIRDA. The patient has a history of nonspecific cognitive decline and multiple small WM changes on imaging. oligodendrocytic tumors of the cerebral hemispheres (11,12). Electroencephalogram
epilepsy center About Epilepsy Surgery
 epilepsy center About Epilepsy Surgery Epilepsy Surgery Advances in Epilepsy Surgery Are You a Candidate for Surgery? If anticonvulsant medications have failed to control your epilepsy, or you are experiencing
epilepsy center About Epilepsy Surgery Epilepsy Surgery Advances in Epilepsy Surgery Are You a Candidate for Surgery? If anticonvulsant medications have failed to control your epilepsy, or you are experiencing
Toward a more accurate delimitation of the epileptic focus from a surgical perspective
 Toward a more accurate delimitation of the epileptic focus from a surgical perspective Margitta Seeck Department of Clinical Neurosciences EEG & Epilepsy Unit University Hospital of Geneva Geneva, Switzerland
Toward a more accurate delimitation of the epileptic focus from a surgical perspective Margitta Seeck Department of Clinical Neurosciences EEG & Epilepsy Unit University Hospital of Geneva Geneva, Switzerland
Epilepsy is a common neurological comorbidity in. Epilepsy surgery in patients with autism
 clinical article J Neurosurg Pediatr 19:196 207, 2017 Epilepsy surgery in patients with autism Malgosia A. Kokoszka, PhD, 1 Patricia E. McGoldrick, MSN, MPA, CNP, 2 Maite La Vega-Talbott, MD, 2 Hillary
clinical article J Neurosurg Pediatr 19:196 207, 2017 Epilepsy surgery in patients with autism Malgosia A. Kokoszka, PhD, 1 Patricia E. McGoldrick, MSN, MPA, CNP, 2 Maite La Vega-Talbott, MD, 2 Hillary
Surgery in temporal lobe epilepsy patients without cranial MRI lateralization
 Acta neurol. belg., 2006, 106, 9-14 Surgery in temporal lobe epilepsy patients without cranial MRI lateralization Y. B. GOMCELI 1, A. ERDEM 2, E. BILIR 3, G. KUTLU 1, S. KURT 4, E. ERDEN 5,A. KARATAS 2,
Acta neurol. belg., 2006, 106, 9-14 Surgery in temporal lobe epilepsy patients without cranial MRI lateralization Y. B. GOMCELI 1, A. ERDEM 2, E. BILIR 3, G. KUTLU 1, S. KURT 4, E. ERDEN 5,A. KARATAS 2,
Epilepsy surgery in the elderly
 Clinical commentary Epileptic Disord 2009; 11 (1): 1-6 Epilepsy surgery in the elderly An unusual case of a 75-year-old man with recurrent status epilepticus Jose F. Tellez-Zenteno 1, Venkatraman Sadanand
Clinical commentary Epileptic Disord 2009; 11 (1): 1-6 Epilepsy surgery in the elderly An unusual case of a 75-year-old man with recurrent status epilepticus Jose F. Tellez-Zenteno 1, Venkatraman Sadanand
Epilepsy. Seizures and Epilepsy. Buccal Midazolam vs. Rectal Diazepam for Serial Seizures. Epilepsy and Seizures 6/18/2008
 Seizures and Epilepsy Paul Garcia, M.D. UCSF Epilepsy Epileptic seizure: the physical manifestation of aberrant firing of brain cells Epilepsy: the tendency to recurrent, unprovoked epileptic seizures
Seizures and Epilepsy Paul Garcia, M.D. UCSF Epilepsy Epileptic seizure: the physical manifestation of aberrant firing of brain cells Epilepsy: the tendency to recurrent, unprovoked epileptic seizures
Subtotal hemispherectomy in children with intractable focal epilepsy
 FULL-LENGTH ORIGINAL RESEARCH Subtotal hemispherectomy in children with intractable focal epilepsy * Harry T. Chugani, * Eishi Asano, * Csaba Juhasz, * Ajay Kumar, William J. Kupsky, and Sandeep Sood SUMMARY
FULL-LENGTH ORIGINAL RESEARCH Subtotal hemispherectomy in children with intractable focal epilepsy * Harry T. Chugani, * Eishi Asano, * Csaba Juhasz, * Ajay Kumar, William J. Kupsky, and Sandeep Sood SUMMARY
Successful Treatment of Mesial Temporal Lobe Epilepsy with Bilateral Hippocampal Atrophy and False Temporal Scalp Ictal Onset: A case report
 Hiroshima J. Med. Sci. Vol. 61, No. 2, 37~41, June, 2012 HIJM 61 7 37 Successful Treatment of Mesial Temporal Lobe Epilepsy with Bilateral Hippocampal Atrophy and False Temporal Scalp Ictal Onset: A case
Hiroshima J. Med. Sci. Vol. 61, No. 2, 37~41, June, 2012 HIJM 61 7 37 Successful Treatment of Mesial Temporal Lobe Epilepsy with Bilateral Hippocampal Atrophy and False Temporal Scalp Ictal Onset: A case
Spike frequency is dependent on epilepsy duration and seizure frequency in temporal lobe epilepsy
 Original article Epileptic Disord 2005; 7 (4): 355-9 Spike frequency is dependent on epilepsy duration and seizure frequency in temporal lobe epilepsy Jozsef Janszky 1,2,3, M. Hoppe 1, Z. Clemens 3, I.
Original article Epileptic Disord 2005; 7 (4): 355-9 Spike frequency is dependent on epilepsy duration and seizure frequency in temporal lobe epilepsy Jozsef Janszky 1,2,3, M. Hoppe 1, Z. Clemens 3, I.
Review Articles. Surgical treatment of epilepsy Manuel Gongalves*, Rita Almeida**
 Review Articles Surgical treatment of epilepsy Manuel Gongalves*, Rita Almeida** Abstract Antiepileptic drugs continue to be the mainstay of treatment of patients with epilepsy. However, we must have surgical
Review Articles Surgical treatment of epilepsy Manuel Gongalves*, Rita Almeida** Abstract Antiepileptic drugs continue to be the mainstay of treatment of patients with epilepsy. However, we must have surgical
Sleep in Epilepsy. Kurupath Radhakrishnan,
 Sleep in Epilepsy Kurupath Radhakrishnan, Retired Senior Professor (Emeritus), R. Madavan Nayar Center for Comprehensive Epilepsy Care, Retired Director, Sree Chitra Tirunal Institute for Medical Sciences
Sleep in Epilepsy Kurupath Radhakrishnan, Retired Senior Professor (Emeritus), R. Madavan Nayar Center for Comprehensive Epilepsy Care, Retired Director, Sree Chitra Tirunal Institute for Medical Sciences
Original Article Nepal Journal of Neuroscience 1:
 Original Article Nepal Journal of Neuroscience 1:98-103, 2004 Initial Experience of Different Surgical Techniques in Temporal Lobe Epilepsy in Nepal Basant Pant, MD, PhD Prabin Shrestha, MBBS Pranaya Shrestha,
Original Article Nepal Journal of Neuroscience 1:98-103, 2004 Initial Experience of Different Surgical Techniques in Temporal Lobe Epilepsy in Nepal Basant Pant, MD, PhD Prabin Shrestha, MBBS Pranaya Shrestha,
RASMUSSEN S ENCEPHALITIS - A CASE REPORT. Dr. Suchithra.J DNB PG RAILWAY HOSPITAL
 RASMUSSEN S ENCEPHALITIS - A CASE REPORT Dr. Suchithra.J DNB PG RAILWAY HOSPITAL Master Naveen Kumar, 7/Mch, first born of nonconsanguinous marriage presented to us with Left hemiparesis Seizures on L
RASMUSSEN S ENCEPHALITIS - A CASE REPORT Dr. Suchithra.J DNB PG RAILWAY HOSPITAL Master Naveen Kumar, 7/Mch, first born of nonconsanguinous marriage presented to us with Left hemiparesis Seizures on L
Interview. News & Views. The importance of surgery for epilepsy. Jerome Engel Jr
 Interview The importance of surgery for epilepsy Jerome Engel Jr, MD, PhD, is the Jonathan Sinay Distinguished Professor of Neurology, Neurobiology, and Psychiatry and Biobehavioral Sciences at the David
Interview The importance of surgery for epilepsy Jerome Engel Jr, MD, PhD, is the Jonathan Sinay Distinguished Professor of Neurology, Neurobiology, and Psychiatry and Biobehavioral Sciences at the David
Neuromodulation in Epilepsy. Frederick Langendorf,, MD Department of Neurology Univ of MN and Hennepin Co Medical Center June 4, 2007
 Neuromodulation in Epilepsy Frederick Langendorf,, MD Department of Neurology Univ of MN and Hennepin Co Medical Center June 4, 2007 disclosures No financial conflicts-of of-interest Epilepsy the problem
Neuromodulation in Epilepsy Frederick Langendorf,, MD Department of Neurology Univ of MN and Hennepin Co Medical Center June 4, 2007 disclosures No financial conflicts-of of-interest Epilepsy the problem
Depth/surface relationships: Confronting noninvasive measures to intracerebral EEG
 Depth/surface relationships: Confronting noninvasive measures to intracerebral EEG Christian G Bénar Institut de Neurosciences des Systèmes; INSERM, Aix-Marseille Université christian.benar@univ-amu.fr
Depth/surface relationships: Confronting noninvasive measures to intracerebral EEG Christian G Bénar Institut de Neurosciences des Systèmes; INSERM, Aix-Marseille Université christian.benar@univ-amu.fr
ICD-9 to ICD-10 Conversion of Epilepsy
 ICD-9-CM 345.00 Generalized nonconvulsive epilepsy, without mention of ICD-10-CM G40.A01 Absence epileptic syndrome, not intractable, with status G40.A09 Absence epileptic syndrome, not intractable, without
ICD-9-CM 345.00 Generalized nonconvulsive epilepsy, without mention of ICD-10-CM G40.A01 Absence epileptic syndrome, not intractable, with status G40.A09 Absence epileptic syndrome, not intractable, without
Update in Pediatric Epilepsy
 Update in Pediatric Epilepsy Cherie Herren, MD Assistant Professor OUHSC, Department of Neurology September 20, 2018 Disclosures None Objectives 1. Identify common pediatric epilepsy syndromes 2. Describe
Update in Pediatric Epilepsy Cherie Herren, MD Assistant Professor OUHSC, Department of Neurology September 20, 2018 Disclosures None Objectives 1. Identify common pediatric epilepsy syndromes 2. Describe
Case report. Epileptic Disord 2005; 7 (1): 37-41
: 37-41") Case report Epileptic Disord 2005; 7 (1): 37-41 Periodic lateralized epileptiform discharges (PLEDs) as the sole electrographic correlate of a complex partial seizure Gagandeep Singh, Mary-Anne Wright,
Case report Epileptic Disord 2005; 7 (1): 37-41 Periodic lateralized epileptiform discharges (PLEDs) as the sole electrographic correlate of a complex partial seizure Gagandeep Singh, Mary-Anne Wright,
Seizure Semiology CHARCRIN NABANGCHANG, M.D. PHRAMONGKUTKLAO COLLEGE OF MEDICINE
 Seizure Semiology CHARCRIN NABANGCHANG, M.D. PHRAMONGKUTKLAO COLLEGE OF MEDICINE Seizure Semiology Differentiate between epileptic and nonepileptic seizures Classification of epileptic syndrome Presurgical
Seizure Semiology CHARCRIN NABANGCHANG, M.D. PHRAMONGKUTKLAO COLLEGE OF MEDICINE Seizure Semiology Differentiate between epileptic and nonepileptic seizures Classification of epileptic syndrome Presurgical
Epilepsy Currents and Pearls. Eniko Nagy-Wilde, MD Medical Director of Epilepsy and Clinical Neurophysiology Sutter Medical Center, Sacramento
 Epilepsy Currents and Pearls Eniko Nagy-Wilde, MD Medical Director of Epilepsy and Clinical Neurophysiology Sutter Medical Center, Sacramento No disclosures Presenter Disclosure Information Learning Objectives
Epilepsy Currents and Pearls Eniko Nagy-Wilde, MD Medical Director of Epilepsy and Clinical Neurophysiology Sutter Medical Center, Sacramento No disclosures Presenter Disclosure Information Learning Objectives
Treatment of Epilepsy with Implanted Devices: What Are Indications and Benefits? 11/30/2012
 Treatment of Epilepsy with Implanted Devices: What Are Indications and Benefits? 11/30/2012 Barbara C. Jobst, MD Dartmouth-Hitchcock Epilepsy Center Geisel School of Medicine at Dartmouth American Epilepsy
Treatment of Epilepsy with Implanted Devices: What Are Indications and Benefits? 11/30/2012 Barbara C. Jobst, MD Dartmouth-Hitchcock Epilepsy Center Geisel School of Medicine at Dartmouth American Epilepsy
Surgery of posterior fossa arachnoid cyst causing hydrocephalus unmasking the cause of epilepsy
 CASE REPORTS ALBANIAN MEDICAL JOURNAL Surgery of posterior fossa arachnoid cyst causing hydrocephalus unmasking the cause of epilepsy Florian Dashi 1, Arben Rroji 1, Eugen Enesi 1, Suzana Gjeci 1, Ridvan
CASE REPORTS ALBANIAN MEDICAL JOURNAL Surgery of posterior fossa arachnoid cyst causing hydrocephalus unmasking the cause of epilepsy Florian Dashi 1, Arben Rroji 1, Eugen Enesi 1, Suzana Gjeci 1, Ridvan
Epilepsy surgery in patients with normal or nonfocal MRI scans: Integrative strategies offer long-term seizure relief
 FULL-LENGTH ORIGINAL RESEARCH Epilepsy surgery in patients with normal or nonfocal MRI scans: Integrative strategies offer long-term seizure relief Prasanna Jayakar, Catalina Dunoyer, Pat Dean, John Ragheb,
FULL-LENGTH ORIGINAL RESEARCH Epilepsy surgery in patients with normal or nonfocal MRI scans: Integrative strategies offer long-term seizure relief Prasanna Jayakar, Catalina Dunoyer, Pat Dean, John Ragheb,
Epilepsy 101. Overview of Treatment Georgette Smith, PhD, APRN, CPNP. American Epilepsy Society
 Epilepsy 101 Overview of Treatment Georgette Smith, PhD, APRN, CPNP American Epilepsy Society Overview of Treatment Rescue Therapies Non-Medication Therapies Epilepsy surgery Vagus nerve stimulation Dietary
Epilepsy 101 Overview of Treatment Georgette Smith, PhD, APRN, CPNP American Epilepsy Society Overview of Treatment Rescue Therapies Non-Medication Therapies Epilepsy surgery Vagus nerve stimulation Dietary
The running down phenomenon in temporal lobe epilepsy
 Brain (1996), 119, 989-996 The running down phenomenon in temporal lobe epilepsy Vicenta Salanova,* Frederick Andermann, Theodore Rasmussen, Andre Olivier and Luis Quesney Department of Neurology and Neurosurgery,
Brain (1996), 119, 989-996 The running down phenomenon in temporal lobe epilepsy Vicenta Salanova,* Frederick Andermann, Theodore Rasmussen, Andre Olivier and Luis Quesney Department of Neurology and Neurosurgery,
Scalp EEG Findings in Temporal Lobe Epilepsy
 Scalp EEG Findings in Temporal Lobe Epilepsy Seyed M Mirsattari M.D., Ph.D., F.R.C.P.(C) Assistant Professor Depts. of CNS, Medical Biophysics, Medical Imaging, and Psychology University of Western Ontario
Scalp EEG Findings in Temporal Lobe Epilepsy Seyed M Mirsattari M.D., Ph.D., F.R.C.P.(C) Assistant Professor Depts. of CNS, Medical Biophysics, Medical Imaging, and Psychology University of Western Ontario