Current Concepts in the Management of Patients With Vestibular Dysfunction
|
|
|
- Laureen Newton
- 5 years ago
- Views:
Transcription

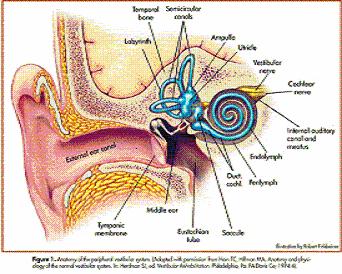
1 Current Concepts in the Management of Patients With Vestibular Dysfunction Kathleen M Gill-Body, PT, MS, NCS Objectives After reading this continuing education (CE) article, you should be able to: Describe the anatomy and physiology of the vestibular system. Understand disorders of the vestibular system. Describe the physical therapist management of patients with vestibular dysfunction. Discuss the anticipated goals and expected outcomes of vestibular rehabilitation. Kathleen Gill-Body, PT, MS, NCS, is Clinical Associate Professor in the Graduate Programs in Physical Therapy, MGH Institute of Health Professions, Boston, Mass. This work was supported in part by grants from the National Institute for Disability and Rehabilitation Research (H133G600045) and the National Institutes of Health (R01AG11255). Introduction Vestibular dysfunction impairs 1 of the 3 primary sensory modalities that contribute to postural control. Even when the visual and somatosensory systems are intact, many patients with vestibular dysfunction are unsteady as they walk or climb stairs. Although individual symptoms vary and many people experience spontaneous resolution of their symptoms within 3 to 6 months of onset, others report persistent sensations of abnormal movement, dizziness, vertigo, oscillopsia, and postural instability. For many patients, postural instability worsens as sensory inputs are altered, such as when walking in the dark. Other patients may be unable to read or drive because of their perceptions of the world moving or jumping as they move. These disabilities may severely impede normal work and activities of daily living, including taking a shower or washing the face, because head movement (especially with eyes closed) can worsen dizziness or lead to falls. It has been estimated that 42% of the adult population report episodes of dizziness or vertigo to their physicians; in 85% of patients reporting these symptoms, the cause is vestibular system dysfunction. 1 Vertigo refers to the illusion of movement (rotation, tilt, or movement in a forward or backward direction) caused by an imbalance of vestibular input. Vertigo is experienced by the majority of all patients with mild brain injury and nearly all patients with moderate brain injury, with symptoms persisting for up to 5 years in patients with moderate brain injury. 2 Vestibular rehabilitation is an exercise approach that has been increasingly used over the last 15 years to manage persistent dizziness and dysequilibrium in people with vestibular dysfunction. The purpose of this article is to review vestibular system anatomy and physiology, describe disorders of the vestibular system and the physical therapist management of patients with vestibular dysfunction, and review studies concerning anticipated goals and expected outcomes following vestibular rehabilitation. Vestibular System: Anatomy and Physiology The vestibular system has 3 major components: a peripheral sensory apparatus (located in the inner ear), a central processing system (located in the vestibular nuclear complex in the brain stem and the cerebellum), and a motor output system (mediated through the vestibuloocular reflex [VOR] and the vestibulospinal reflex [VSR]). 3 The peripheral sensory apparatus is responsible for detecting and relaying information about head angular and linear velocity to the central processing system in addition to orienting the head with respect to gravity. The central processing system processes this information in conjunction with other sensory inputs (somatosensory and visual) to provide accurate information about the position and movement of the head in space. Motor outputs primarily serve to generate compensatory eye movements (for gaze stability) and compensatory body movements (for postural stability) during head movements, posture, and locomotion. Peripheral Sensory Apparatus The peripheral vestibular system in each inner ear is composed of a bony labyrinth, a membranous labyrinth, and specialized hair cells that are responsible for detecting motion. Located within each temporal bone of the skull is
2 a bony labyrinth that contains the 3 semicircular canals and a central chamber called the vestibule (Fig. 1). The bony labyrinth is filled with perilymphatic fluid, and the membranous labyrinth is suspended in this fluid. The 5 sensory organs of the peripheral vestibular system are located within the membranous labyrinth in each inner ear. The membranous labyrinth consists of 2 swellings within the vestibule the utricle and saccule (collectively called the otolith) and 3 semicircular canals. Each of these 5 sensory organs of the peripheral sensory apparatus serves a distinct function. Specialized hair cells within each of the sensory organs are responsible for converting mechanical information due to head motion (displacement of the hair) into neural firing. Utricle and saccule (otoliths). The saccule and utricle are responsible for detecting linear acceleration of the head and are known collectively as labyrinth organs. The saccule detects vertical linear accelerations of the head in the sagittal plane, and the utricle responds to horizontal plane linear accelerations. The otoliths are also sensitive to tilts of the head with respect to gravity. The otoliths are most sensitive to lower-frequency motion, such as motion that occurs while standing in place. Semicircular canals. The 3 semicircular canals (anterior, posterior, and lateral) lie perpendicular to each other (Fig. 1). The anterior and posterior canals are oriented about 45 degrees from the sagittal plane, and the lateral canal is tilted upward about 30 degrees from the transverse plane. The primary function of the semicircular canals is to sense angular acceleration of the head. The semicircular canals are maximally sensitive to higher-frequency motion, such as motion that occurs during locomotion. Each canal is maximally sensitive to movement in the plane of that canal. Hair cells. The hair cell is the basic sensory element of the peripheral sensory apparatus. Present in the saccule, utricle, and the cristae of the semicircular canals, the hair cell transduces mechanical force into electrical nerve action potentials. Each hair cell is innervated by an afferent neuron and has a large number of small cilia and one very large cilium, called the kinocilium. A gelatinous membrane (called the cupula in the semicircular canals) overlies each set of hair cells. In the otoliths, calcium carbonate crystals (called otoconia) are located within the gelatinous membrane resting on top of the hair cells. This makes the otoliths gravity-sensitive, an attribute not true of the semicircular canals. When the cilia of the hair cells are displaced toward the kinocilium, firing rates increase in the neuron and the vestibular nerve is excited. This occurs because of the endolymph flow associated with head movement. Conversely, when the cilia are displaced away from the kinocilium, firing rates decrease and the vestibular nerve is inhibited. Displacement of the cilia, therefore, is transduced into an electrical response that is then carried to the brain through the vestibular nerve (cranial nerve VIII). Central Processing System The central processors of the vestibular system are the vestibular nuclei and the cerebellum. 3 Afferent signals from the labyrinths ascend the eighth cranial nerve to the vestibular nuclear complex and to the flocculonodular lobe of the cerebellum (or vestibulocerebellum). The vestibular nuclear complex, located in the pons and medulla oblongata, consists of 4 major vestibular nuclei (superior, medial, lateral, and inferior). The vestibular nuclei receive input from the ipsilateral vestibular nerve (carrying inputs from the semicircular canals and otoliths), 4 contralateral vestibular nuclear complex, cerebellum, brainstem reticular activating systems, spinal cord, and other sensory systems (including somatic, visual, and auditory modalities). 5,6 Fast, direct connections are made between incoming afferent information and efferent output. Efferent signals from the vestibular nuclear complex reflect input from all these sensory systems and go to oculomotor nuclei (via the medial longitudinal fasciculus), cerebellum (flocculonodular lobe and vermis), brainstem reticular activating systems, parietal cortex (via the thalamus), ipsilateral vestibulospinal tract, and contralateral vestibular nuclear complex. Each vestibular nucleus maintains a baseline firing rate that is symmetrical at rest. Head movements cause changes in the firing rates of both vestibular nerves but in opposite directions (eg, head movement to the left causes an increase in the firing rate of the left vestibular nerve and a decrease in the firing rate of the right vestibular nerve). Consequently, a balanced input (or message) to the central nervous system (CNS) is maintained during head movements in the person who is healthy. The vestibulocerebellum receives its input from the vestibular nuclei and relays signals directly back to the nuclei. In addition, central connections are extensive and include projections to the cerebellar cortex and ultimately to the fastigial nuclei. The primary roles of the cerebellum related to the vestibular system are to serve as an adaptive processor and to monitor vestibular performance. 3 Various portions of the cerebellum appear to have primary responsibility for select functions. For example, the gain (ratio of head to compensatory eye movement) of the VOR is regulated in part by the cerebellar flocculus, and the duration of VOR responses and otolith input are adjusted and processed in the nodulus. 3 Lesions of the anterosuperior portion of the vermis (middle part) of the cerebellum primarily affect the VSR, resulting in postural and gait instability. 3 2
3 Motor Output System The vestibular system functions as both a sensory system and a motor system. During functional tasks, sensory information relayed to the CNS from vestibular sensory organs is constantly being influenced and altered by motor signals originating from the vestibular system. The output of the central vestibular system (through the vestibular nuclei) goes to the ocular muscles and to the spinal cord to serve 2 vestibular reflexes: the VOR and the VSR. The VOR and the VSR work in conjunction with other motor systems to control gaze stability and whole-body equilibrium during head movements, posture, and locomotion. Vestibulo-ocular reflexes (VOR). The primary function of the VOR is to maintain gaze stability during head motion. In a healthy person, the gain of the VOR at velocities associated with most functional activities is approximately equal to 1.0. This indicates that, for example, 30 degrees of head rotation to the left is typically accompanied by 30 degrees of lateral eye movements to the right; these compensatory eye movements are produced by activation of the left medial rectus and right lateral rectus muscles and inhibition of their antagonists. Therefore, eye orientation in space (angle of gaze) remains relatively constant during head movement, allowing clear and accurate visual acuity. For head movement in any direction, therefore, the VOR mediates compensatory movement of the eyes in the orbit in the opposite direction. Afferent input from the semicircular canals ascends to the vestibular nuclei and is primarily responsible for producing these compensatory eye movements. The ascending Deiter s tract and the medial longitudinal fasciculus transmit efferent input from the vestibular nuclear complex to the ocular motor nuclei. The motoneurons of the ocular motor nuclei of cranial nerves III, IV, and VI (which drive the extra-ocular muscles) comprise the output neurons of the VOR. 3 Vestibulospinal reflexes. Vestibulospinal reflexes affect whole-body equilibrium by facilitating and inhibiting skeletal extensor muscle activity. These reflexes include the vestibulocollic reflex (which acts on the neck muscles to stabilize the head) and the labyrinthine reflexes. Spinal anterior horn cell activity is influenced by information from the semicircular canals and the otoliths through 3 major pathways: the lateral vestibulospinal tract (LVST), the medial vestibulospinal tract (MVST), and the reticulospinal tract (RST). The LVST links directly with alpha and gamma motoneurons in the medial portions of the anterior horn cell 7 and controls otolith-mediated postural responses (eg, responses to acceleration, deceleration, and tilting of the body). 8,9 For example, a head tilt to one side stimulates both the otoliths and semicircular canals. Stimulation of the otoliths results in the transmission of impulses to the spinal cord via the LVST, resulting in an increase in extensor activity on the side of the body to which the head is tilted and an increase in flexor activity on the contralateral side. Thus, the head and body are stabilized. Fibers of the MVST terminate primarily at the upper cervical and thoracic motoneurons, having a primarily inhibitory effect on most neurons. Many MVST neurons have branches that extend to the extra-ocular nuclei, 8,9 contributing to the theory that the MVST is involved in maintaining gaze stability. The RST receives sensory input from all of the 4 vestibular nuclei. Fibers of RST traverse the length of the spinal cord, terminate in the seventh and eighth laminae of the gray matter, 10,11 and primarily mediate postural adjustments. The cerebellum interacts with each of these 3 pathways. Afferent input from the otoliths and, to a lesser degree, from the semicircular canals, contribute to the generation of postural responses through the VSRs. Disorders of the Vestibular System One method of categorizing disorders of the vestibular system is by their location. Peripheral vestibular dysfunction typically includes disorders that affect the peripheral sensory apparatus or the vestibular nerve. Central vestibular disorders occur with damage to the vestibular nuclear complex, central pathways that serve the VOR and VSR (ie, projections to the ocular motor nuclei or spinal cord), brain stem, or cerebellum. Peripheral Vestibular Disorders Peripheral vestibular disorders have been further classified by Black 12 based on the type of dysfunction that results from the pathology or pathophysiology. Reduced vestibular function or hypofunction) refers to conditions that result in the reduced sensitivity of the peripheral sensory apparatus to stimuli. Direct damage to the vestibular nerve, labyrinth, or hair cells is an example of pathologies that may produce reduced vestibular function. The damage may be unilateral or bilateral and partial or complete. Examples of specific underlying etiologies that may produce reduced vestibular function include labyrinthitis, neuronitis, age-related degeneration of hair cells, drug-induced ototoxicity that causes hair cell damage, brain trauma, vascular occlusions, and acoustic neuroma. Initially, patients with reduced vestibular function often have vertigo, dysequilibrium, and impaired gaze stability if the pathology is unilateral. Patients with bilaterally reduced vestibular function may have no vertigo (if there is no asymmetry between right and left sides), but they often have marked dysequilibrium, gait ataxia, and oscillopsia (the inability to stabilize an image on the retina). Empirical and experimental
4 evidence supports the use of vestibular rehabilitation programs for patients with reduced vestibular function. Distorted vestibular function refers to conditions that result in inaccurate transduction of sensory stimuli within the peripheral sensory apparatus. Typically, this is due to a mechanical disruption. A common etiology of this type of dysfunction is benign paroxysmal positional vertigo (BPPV), a particular mechanical disruption that occurs when otoconia from the utricle are either displaced into the cupula of one of the semicircular canals (cupulolithiasis) or are free floating in the endolymph (canalithiasis). With both conditions, the involved canal becomes gravity-sensitive and thereby produces abnormal input to the vestibular nuclei. Patients with distorted vestibular function often have position- or motion-induced vertigo and may have dysequilibrium. There is strong evidence to support the use of canal repositioning maneuvers for patients with BPPV Fluctuating vestibular function refers to conditions that produce occasional disruptions in vestibular input within the peripheral sensory apparatus. Periods of normal function may be followed by periods of abnormal function that are characterized by abnormal input to the CNS. Examples of conditions that may result in fluctuating vestibular function are endolymphatic hydrops (of which Ménière disease is one form) and perilymphatic fistula. Endolymphatic hydrops is characterized by fluctuations in fluid and electrolyte control in the inner ear. Periplymphatic fistulas are characterized by pressure changes within the inner ear due to an opening in the round or oval window between the middle and inner ear. The etiology of these conditions may be idiopathic, autoimmune, or due to brain trauma or infection. Patients with fluctuating vestibular function may have episodic or persistent vertigo or generalized dizziness, hearing loss, tinnitus, and dysequilibrium. The fluctuating nature of this type of vestibular dysfunction makes it less amenable to vestibular rehabilitation because it is more difficult for the CNS to compensate when sensory input fluctuates. Central Vestibular Disorders Central vestibular disorders may result from vascular disorders, ischemia, or hemorrhage to the brain stem or cerebellum; the most commonly involved vessels are the vertebral, basilar, subclavian, and anterior or posterior inferior cerebellar arteries. 28 Examples of some of the more commonly encountered central vestibular disorders are briefly identified here. Infarction of the dorsal lateral aspect of the medulla can occur with ischemia of the vertebral or posterior inferior cerebellar arteries and produce Wallenberg (or lateral medullary) syndrome. 28 Diffuse damage to long white fiber tracts, such as damage that occurs with brain trauma, may be another source of central vestibular dysfunction. 28 Demyelinating disease may 4 affect the vestibular nuclear complex, medial longitudinal fasciculus, or cerebellum, causing patients with disorders such as multiple sclerosis to have central vestibular dysfunction. 29 Tumors in the brain stem or cerebellum may affect the vestibular nuclei or vestibulocerebellum. Patients with central vestibular disorders may have myriad symptoms, including vertigo, nausea, nystagmus, ataxia, and dysequilibrium. In addition, they may demonstrate clinical signs of central vestibular (or nervous system) dysfunction such as visual field deficits, diplopia, headache, impaired smooth-pursuit eye movements, impaired VOR cancellation, sensory loss, and hemiparesis (depending on the site of the neuropathology). Less is known about the benefits associated with vestibular rehabilitation for patients with central vestibular disorders as compared with those patients with peripheral vestibular disorders, but evidence does exist to support its potential usefulness for some patients Many physical therapists apply several of the principles that are described below, which are intended for patients with peripheral vestibular disorders, to patients with central vestibular disorders as well. Patient Examination History The following information is critical to obtain from the patient or medical record: a detailed history of the patient s functional status and activity level, current condition (concerns that bring the patient to physical therapy, onset and pattern of symptoms, onset of vestibular dysfunction, and course of events until the present time), medication usage, and the results of diagnostic tests. It is important to identify the use of medications to reduce symptoms of dizziness (such as meclizine or scopolamine) because these drugs act by depressing the vestibular system and may therefore limit compensation (or adaptation) by the CNS following peripheral vestibular damage. 35(p336) A description of the patient s current and prior functional status provides insight regarding the impact that vestibular dysfunction has on the patient s daily activities. It is often helpful to elaborate on the differences among vertigo (eg, a feeling of movement or spinning ), dizziness (a vague term that may be interpreted differently by individual patients and that can refer to feelings of disorientation or lightheadedness or to illusions of movement), and dysequilibrium (eg, a feeling of being off balance as if you might fall ) in a manner that is understandable and meaningful to the patient. Probing questions regarding the specific symptoms experienced by the patient (ie, dizziness versus dysequilibrium), the frequency and severity of these symptoms, and how they are exacerbated or relieved are particularly helpful in allowing the physical therapist to establish a diagnosis.
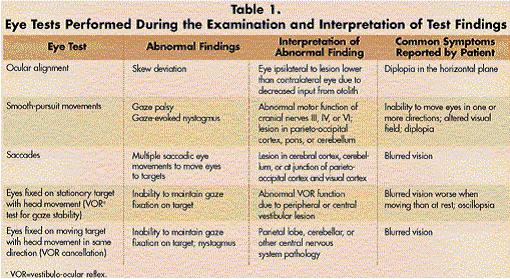
5 To determine the impact of a patient s dizziness or dysequilibrium on daily life, the Dizziness Handicap Inventory can be used to provide reliable, valid, and sensitive measurements of patients perceptions of the effects of dizziness and unsteadiness. 36 The Dizziness Handicap Inventory is a questionnaire developed specifically to measure perception of handicap in people with vestibular dysfunction. It consists of 25 items, including items related to daily activities that cause dizziness and unsteadiness and items related to emotional well-being. The questionnaire can be completed by the patient or administered by questioning the patient. Each question is answered yes, sometimes, or no, and these responses are converted into scores of 4, 2, and 0, respectively. Patients who perceive a greater level of disability related to their dizziness and unsteadiness receive higher scores (closer to the total possible score of 100) than those who perceive lower levels of disability. Another questionnaire that may be used by clinicians is the Activities-Specific Balance Confidence scale, a tool that is completed by the patient and measures his or her level of confidence in performing 16 common functional activities without falling. 37 Both the Dizziness Handicap Inventory and the Activities-Specific Balance Confidence scale can be used as efficient ways to gain insight into the specific areas that should be targeted as intervention priorities for individual patients. Patients with a diagnostic evaluation of the vestibular system prior to referral to a physical therapist may have undergone the following vestibular function tests and measures: an electronystagmogram, a rotary chair test, and a visual-vestibular interaction rotation test (VVI). These tests are described elsewhere in detail and are outlined briefly below. Dynamic posturography is also useful in characterizing the patient s postural stability. The electronystagmogram is the basic screening test for vestibular function and includes tests for oculomotor screening (which includes documenting saccades, pursuit, and nystagmus eye movements) and vestibular function (which includes positional and caloric testing). The electronystagmogram is helpful in testing individual lateral semicircular canal and vestibular nerve function and can provide information regarding which peripheral vestibular sensory apparatus is damaged. 5 The rotary chair test is a sensitive measure of bilateral lateral canal function 41 but does not localize dysfunction to one side or differentiate between peripheral vestibular system and CNS involvement. During the rotary chair test, the patient is rotated to the left and right at various frequencies while sitting in a chair in the dark with the eyes open and the head stabilized; this produces a vestibularocular reflex of nystagmus, which is measured during the test. 38 The VVI is another rotational test useful for demonstrating and localizing CNS lesions that involve the vestibular, cerebellar, or ocular pathways. During this test, the patient is rotated at a single frequency in a chair under various visual conditions; characteristics of the nystagmus that are produced by this test are measured. 38 Finally, dynamic posturography testing enables standing balance function to be quantified under various sensory conditions and in response to perturbations Overall, vestibular function tests and measures assess VOR function. Vestibulospinal reflex function is assessed through posturography and clinical balance tests, although these tests are not able to distinguish between function of the vestibulospinal pathways and other motor systems. Systems Review Clinical examination should include a screen of all systems (cardiopulmonary, integumentary, musculoskeletal, and neuromuscular) through medical record review and patient self-report. A screening examination is critical to detect possible impairments in flexibility, muscle performance, motor function (including coordination), and sensory integrity that may affect balance or functional performance. For patients with vestibular dysfunction, the focus of the clinical examination is on the integrity of the eighth cranial nerve (ie, vestibulo-ocular and vestibulospinal function). Major components of the clinical examination include an assessment of gaze stabilization; positional provocation testing (if indicated); motor function (ie, eye-head coordination); gait, locomotion, and balance; and self-care and home management (basic and instrumental activities of daily living). Tests and Measures Examination of gaze stabilization and eye-head coordination. Testing the extra-ocular muscles and the vestibulo-ocular system includes assessing ocular alignment, smooth-pursuit and saccadic extra-ocular eye movements with the head fixed, and movement of the head in all directions (vertical and horizontal) with the eyes fixed on a stationary target (the test for VOR function or gaze stability) and fixed on a moving target (the test for VOR cancellation) (Tab. 1). Ocular alignment is assessed through observation of alignment of the eyes. Smoothpursuit eye movements are tracking movements of the eyes performed to hold the image of a moving target stable on the fovea; testing involves asking the patient to follow a moving target in all directions with his or her eyes while keeping the head stable. Saccadic eye movements are quick eye movements performed to bring an image onto the fovea; testing involves asking the patient to look back and forth quickly between 2 targets placed vertically and horizontally.
6 Vestibulo-ocular reflex testing can be performed actively or passively, in a sitting or standing position, with a simple or complex visual background, and at various speeds of head movement. One simple way of objectively measuring VOR function in the clinic is to perform a test of dynamic visual acuity by assessing the degradation of visual acuity that occurs with different speeds of head movement. 45 To perform a test of dynamic visual acuity, the patient is asked to read a visual acuity wall chart (modified ETDRS) with the head stationary and then to read the chart again when the head is either actively or passively rotated side to side at a frequency of 2 Hz. A drop in visual acuity of more than one line signifies difficulty with gaze stability (VOR function). 35(p342) The sensitivity and specificity of a computerized version of this test for people with vestibular disorders have been reported to be 94.5% and 95.2%, respectively. 46 The sensitivity and specificity of the manual version of this test have not been established. Another method of examining gaze stability is to perform rapid head thrusts. 35(p ) During this procedure, the patient is positioned sitting looking at a target, and the examiner passively turns the patient s head to one side, at first slowly and then rapidly. The patient is asked to report if the target can still be read during the rapid head thrust. The sensitivity and specificity of rapid head thrusts in classifying people with vestibular loss are 35% and 95%, respectively. 47 The low sensitivity of this test is believed to be related to the variance in the speed of head movements that the examiner can use. It is important to include some test of rapid head movement during the examination of gaze stability because it is possible to use smooth-pursuit and other eye movements to substitute for gaze stability at slower velocities of head movement. Vestibulo-ocular reflex cancellation (a function of the parietal lobe) is tested by asking the patient to focus on a horizontally moving target while the head is moving at the same rate in the same direction; changes in visual acuity and the ability to keep the eye on the target are noted and considered abnormal. Typical abnormal findings for each of these tests and their interpretation are presented in Table 1. During all eye-head coordination and gaze stabilization tests, the therapist should note any changes from baseline in symptoms of vertigo, dizziness, or nausea (using a 0 10 rating scale of intensity); presence of nystagmus or signs of extra-ocular muscle weakness; and the ability to see the target clearly. Positional provocation testing. Identifying which positions and movements cause dizziness or vertigo is an important part of the examination of patients who have known or suspected movement-related dizziness or vertigo. Testing involves having the patient quickly move into and out of the various positions typically assumed in daily life (eg, moving from sitting to lying down on either side, bending forward) and noting the presence and intensity of symptoms elicited by each change in position. 6 A commonly performed positional test used to specifically diagnose BPPV related to posterior canal dysfunction is the Hallpike-Dix maneuver. 48 To perform this test, the patient is positioned sitting on an examination table with the head rotated toward one side; then the patient is moved rapidly from the sitting position into a supine position with the head hanging back over the edge of the table with approximately 30 degrees of neck extension (Fig. 2). If the patient s head is turned to the right, the right posterior semicircular canal is tested. The patient is observed for signs of nystagmus; torsional nystagmus with the eyes directed toward the affected side is classically associated with BPPV related to posterior canal involvement, if the Hallpike-Dix maneuver is performed with the involved ear down. 49 Reports of vertigo are also important to note. After a brief rest period, the patient is quickly repositioned into sitting. In patients with BPPV, the motion-induced vertigo and torsional nystagmus typically occur with a 1- to 40-second latency after the head is inverted over the edge of the table; vertigo increases in intensity for a short period of time, and then both vertigo and nystagmus resolve within 30 to 60 seconds. 49 Typically, vertigo and nystagmus subside if the ear-down position is repeatedly assumed within a short period of time. Although the posterior semicircular canal is by far the most common site of dysfunction (accounting for about 63% of all cases of BPPV 50 ), other semicircular canals may alternately be involved. The specific canal that is functioning abnormally must be identified through the appropriate positioning test and observation of the direction of the nystagmus that occurs during testing. Herdman 50 has detailed alternate testing methods and a system of classification of canal involvement in patients with peripheral positional vertigo. In patients with central vestibular disorders, the position-induced nystagmus that may be observed is characteristically different from the nystagmus for peripheral vestibular disorders described above because it occurs immediately on assumption of the offending position, it lasts longer than 30 to 60 seconds, and it typically does not subside with repetition. 28 Examination of gait, locomotion, and balance. A comprehensive assessment of vestibulospinal function includes (1) tests performed in a standing position and during gait and (2) tests that analyze both the sensory and motor organization aspects of balance control. The depth of the evaluation and appropriate difficulty of tests to use depend on the patient s reported symptoms and functional problems. A qualitative assessment of the specific balance strategies used in various postures and tasks (ie, ankle, hip, or stepping strategy) 51,52 may be useful for intervention planning. Overall, the tests should help the physical therapist determine the underlying physical impairments associated with postural control and functional abilities and quantify or classify balance in a reliable and clinically feasible manner.
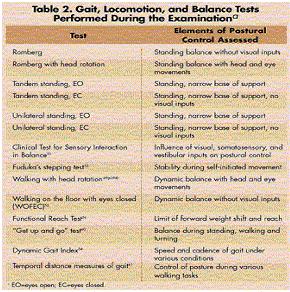
7 Gait, locomotion, and balance tests that are often useful are listed in Table 2 along with the various elements of postural control that each test assesses. Many of these tests are not specific to patients with vestibular dysfunction and are relatively well-known to clinicians. Other tests have been described or developed to specifically detect postural control deficits commonly found in people with vestibular dysfunction or other balance disorders. Examples include Fuduka s stepping test, 53 walking with head rotation, 35(p354) Dynamic Gait Index, 54 walking on the floor with eyes closed (WOFEC), 55 and the Functional Reach Test. 56 Fuduka s stepping test assesses postural control during marching in place, a self-initiated weight-shifting and postural-control task. The patient marches in place for 50 steps, first with the eyes open and then with the eyes closed, on a floor grid or markings on the floor that allow the distance the patient moves from the starting position during each trial to be quantified. Patients with unilateral vestibular dysfunction often turn excessively toward their involved side during the eyes-closed trial 35(p353) whereas patients with bilateral vestibular loss typically fall during this test. 57(p429) Standardized performance of walking with head rotation requires the patient to ambulate on a measured straight walkway rotating the head side to side with every second or third step. The time to perform the measured gait distance can be documented and staggering can be quantified by counting the number of cross steps or steps outside the walkway. Walking with head rotation is 1 of the 7 tests included in the Dynamic Gait Index, 54 a tool designed to evaluate the ability to modify gait in response to various tasks. For patients who are able to walk without physical assistance, the Dynamic Gait Index is a particularly helpful tool that can be used to quantify the degree of unsteadiness associated with the performance of specific tasks in situations encountered in everyday life (eg, walking around or over obstacles and performing turns). The walking on the floor with eyes closed (WOFEC) test is a test of tandem walking with eyes closed for up to 10 steps, which Fregly et al 55 describe as a useful addition to their original Ataxia Test Battery. 58 The components of the battery are listed in Table 2 The patient s arms are folded across the chest during the WOFEC, and particular attention is placed on proper foot placement during tandem gait. Age-related norms for the WOFEC have been established 55 and can be used to classify a person s test performance. The Functional Reach Test is a measure of functional balance developed by Duncan and colleagues 56 that quantifies the distance a patient can reach forward without altering the base of support. A level yardstick mounted on the wall at the height of the patient s acromion is used to measure the distance reached. A reach of less than 6 inches is 7 associated with an increased risk of falling in elderly men. 59 Interrater reliability has been demonstrated in healthy adults. 56 The reliability, predictive validity, and sensitivity of the Functional Reach Test have not been established in people with vestibular dysfunction. Finally, the timed and qualitatively rated Get Up and Go test, 60 temporal-distance gait measurements, 61 and qualitative gait analysis also may be useful. A temporaldistance gait assessment can be conducted by timing the patient s ability to walk with eyes open and with eyes closed along a measured pathway: (1) with a normal base, (2) with a tandem base, and (3) on a foam surface. For each test of postural stability, a subjective rating of the patient s dizziness and sense of dysequilibrium can be recorded using a rating scale of 0 to 10. Examination of functiona l abilities (activities of daily living). Basic and instrumental activities of daily living should be assessed through self-report or the use of a standardized questionnaire. Two standardized questionnaires that measure functional abilities with respect to activities of daily living are the Lawton and Brody Instrumental Activities of Daily Living Scale 62 and the Frenchay Activities Index. 63 Each questionnaire has been developed for initial use with patients with conditions other than vestibular dysfunction and have yet to be validated for use with people with vestibular dysfunction. Nonetheless, they may serve as a guide for obtaining information from the patient and are being used by clinicians at the present time for assessing functional limitations in adults with balance disorders. Evaluation, Diagnosis, and Prognosis The results of vestibular function tests help determine whether the patient with peripheral vestibular dysfunction has a unilateral or bilateral lesion, whether any residual vestibular function is present, and whether deficits in VOR function exist. A complete medical examination, in combination with vestibular function tests, helps to determine whether central vestibular dysfunction or CNS pathology exists. Damage to CNS structures such as the vestibular nuclei or cerebellum may prevent or limit functional recovery in people with vestibular dysfunction, thereby affecting the prognosis. 17 Other CNS structures, such as the spinal cord and visual cortex, also play important roles in compensation in people with vestibular system injury or disease. 64 As part of the evaluation, diagnosis, and prognosis, it is helpful to interpret the history and the results of vestibular function tests and the clinical examination to determine whether the patient has deficits in vestibulo-ocular function, vestibulospinal function, both elements of
8 vestibular system function, or motion-induced vertigo. If motion-induced vertigo or nystagmus is present, the characteristics of the nystagmus and dizziness should be assessed to determine, if possible, whether the patient has nystagmus of peripheral or central origin. If the patient has peripheral motion-induced nystagmus, the specific semicircular canal involved should be identified. Deficits in VOR function that may be seen can be further classified into static and dynamic VOR disturbances. A static VOR imbalance may present as nystagmus and is caused by differences between sides in the tonic firing rate within the vestibular nuclei related to the lesion. This nystagmus is commonly seen at rest in people with acute unilateral vestibular dysfunction, and it typically resolves within a few days as the CNS automatically adjusts to the injury. Dynamic VOR disturbances refer to abnormalities in the gain or timing of eye movements in relation to head movements and are caused by the abnormal or reduced input from one or both vestibular nuclei. Loss of visual acuity with fast head movements and oscillopsia are examples of dynamic disturbances in VOR function. Deficits in VSR function can be further classified into problems with sensory organization, problems with motor organization, or a combination of problems relating to both aspects of postural control. With respect to sensory organization aspects of postural control, the patient s ability to use visual, somatosensory, and vestibular inputs for postural control can be interpreted from the patient s performance on clinical balance testing, the Clinical Test for Sensory Interaction in Balance, 51 and posturography testing, if available. Interventions aimed at improving the patient s sensory organization should focus on the patient s baseline function in each of these 3 sensory systems (visual, somatorsensory, vestibular) as well as the ability to selectively use various sensory information for postural control. With respect to the motor organization aspect of postural control, any underlying musculoskeletal or neuromuscular impairments that may contribute to abnormal balance must be identified. Previous models for clinical decision making can be useful in characterizing the exact nature of patients balance difficulties and directing the focus of the plan of care. 65 For example, for a patient with deficits in flexibility, strength, coordination, or postural alignment, the initial intervention plan should focus on reducing these impairments, assuming that these impairments can be altered. For patients with abnormalities in the motor strategies utilized for postural control, the findings of Diener et al 66 and Herdman et al 67 should be considered when interpreting the results of the clinical examination. Diener et al 66 reported that patients with bilateral peripheral vestibular loss may not be able to use hip strategies effectively because these strategies may be monitored primarily by the damaged vestibular system. Similarly, patients with proprioceptive loss may not be able to use ankle strategies for postural control effectively because these strategies may be mediated through the somatosensory system. Herdman et al, 67 however, report an increased use of hip strategies among patients with bilateral peripheral vestibular loss compared with healthy subjects. More recently, Asai and colleagues 68 reported, in a series on 3 patients, that 2 of the 3 patients (1 with unilateral reduced vestibular function and 1 with bilateral reduced vestibular function) switched from the unsuccessful use of ankle strategies to the successful use of hip strategies to maintain balance after a course of vestibular rehabilitation. Whether or not these changes in the use of balance strategies for these patients were related to vestibular rehabilitation is not known. Therefore, one must consider whether specific motor strategies can and should be retrained in patients with these underlying sensory deficits, but conflicting information currently exists regarding this issue. Intervention Vestibular rehabilitation is an exercise program aimed at reducing dizziness and vertigo and improving gaze stabilization, postural stability, and overall functional abilities. The main components of a vestibular rehabilitation program are gaze stabilization exercises (to retrain VOR function), balance retraining (to retrain VSR function), conditioning exercises (to improve overall fitness), and, if indicated, habituation or canal repositioning maneuvers (to reduce position- or motioninduced dizziness or vertigo). In the 1940s, Cawthorne 69 and Cooksey 70 were the first to describe an exercise approach for people with persistent symptoms of unsteadiness and dizziness related to unilateral vestibular dysfunction and postconcussive disorders. Since that time, others have advocated modification and expansion of their original ideas. As more knowledge has become available regarding how the CNS compensates after peripheral vestibular loss or damage, ideas for intervention have been refined. Major contributors to the advancement of this clinical theory over the last 20 years include Norre and De Weerdt, 20 Shumway-Cook and Horak, 71,72 and Herdman. 73 Knowledge of the mechanisms of recovery that occur after peripheral vestibular damage is critical to understanding the interventions that are used today. Experiments with animals and humans suggest that compensation (or a progressive decrease in symptoms of dizziness or dysequilibrium) can be enhanced by active movements and the processing of visual, vestibular, and somatosensory stimuli. 74(p392) 8
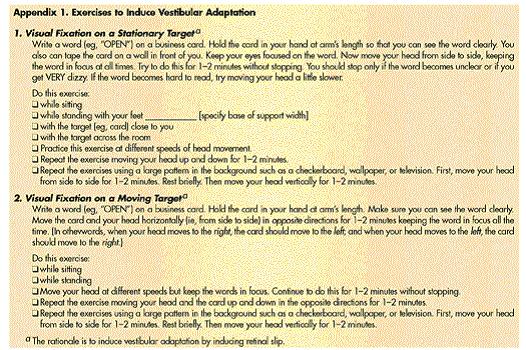
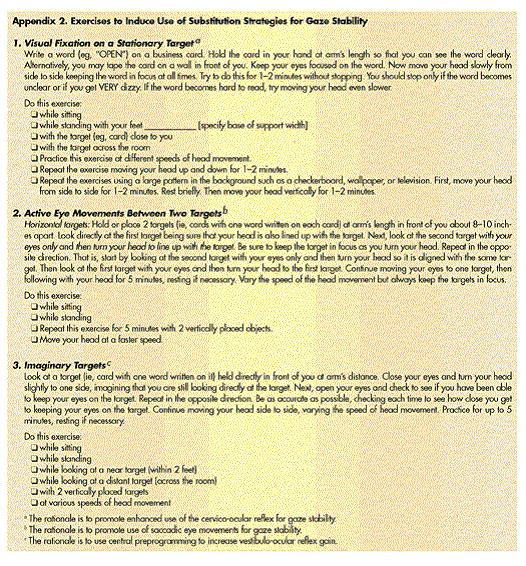
9 Compensation results from changes that occur within the CNS rather than from changes in the peripheral vestibular system itself. Possible mechanisms of compensation that have been identified are a rebalancing of tonic activity within the vestibular nuclei (also known as spontaneous recovery), recovery of VOR gain (also known as vestibular adaptation), and habituation (a progressive decline in the response to the same stimulus). 50 Each of these mechanisms may contribute to recovery in people with some residual peripheral vestibular function but are unlikely to contribute to recovery if the damage to the peripheral vestibular system is bilateral and complete. 50 A separate mechanism of recovery (substitution of alternative strategies) is theorized to contribute to the recovery of gaze stability and postural stability in people with complete loss of peripheral vestibular function and also likely contributes to recovery even in people with remaining vestibular function. 50 Each of these mechanisms of recovery or CNS compensation will be discussed further as they relate to the various interventions for people with peripheral vestibular dysfunction. There is no evidence at this time regarding the extent to which these mechanisms of recovery or CNS compensation may be altered for people with central vestibular dysfunction. Patient/Client-Related Instruction Patients with vestibular system dysfunction benefit from education about the vestibular system, symptoms common to people with their particular type of vestibular problem, typical course of recovery, and strategies regarding how to manage their particular symptoms and functional difficulties. The specific training and education given will vary from patient to patient. For example, it may be beneficial for some patients to purposefully place themselves in situations with reduced lighting as a method of training them to use vestibular and somatosensory inputs for postural control, whereas these situations should be avoided for other patients with complete loss of vestibular function. Most patients benefit from an explanation of vestibular rehabilitation as an exercise approach, because it is often an unfamiliar concept. It is important to explain to patients that performing the prescribed exercises will likely cause an increase in their symptoms (dizziness, vertigo, dysequilibrium), that this is a necessary part of the plan of care, and that often the exercises need to be performed in the presence of their symptoms for the intervention to be most effective. Emphasizing the importance of daily repetition of the activities or exercises as prescribed is also helpful to most patients. 9 Procedural Interventions: Reduced Vestibular Function Herdman 75 has described 2 main intervention approaches related to retraining VOR and VSR function for people with reduced peripheral vestibular dysfunction: the adaptation approach (appropriate for patients with reduced vestibular function) and the substitution of alternative strategies (for patients with no remaining vestibular function). The vestibular system s ability to adapt to changes in demand or changes in the sensory information received is key to the adaptation approach for patients with residual vestibular function. 73,76 The patient performs eye-head coordination exercises that include stimuli that induce adaptation of the VOR (such as combining movement of an image across the retina with head movement) (Appendix 1). These vestibular adaptation exercises require visual fixation on a target during head movement; this combination produces an error signal (retinal slip), which the CNS then tries to reduce by increasing the VOR gain. 73,77 These exercises can be performed with head movement in various directions and at various speeds, as described in Appendix 1. Patients are instructed to keep their eyes focused on a target during the head movements and to increase the speed of head movement over time as dizziness (during the exercise) diminishes and visual acuity improves. In a study involving 23 subjects with chronic peripheral vestibular dysfunction, Szturm and colleagues 78 investigated the effects on VOR function of performing specific vestibular adaptation exercises (Appendix 1) versus the head and eye movements originally described by Cawthorne 69 and Cooksey. 70 Szturm et al reported that adaptive gains in the VOR can be induced by performing exercises that incorporate gaze fixation exercises on stationary and moving targets (such as the vestibular adaptation exercises described in Appendix 1), but not by exercises that do not require combining head oscillations and gaze fixation (such as Cawthorne-Cooksey exercises). This study provides experimental support for the use of vestibular adaptation exercises to improve gaze stability in people with reduced vestibular function. Balance retraining activities to improve VSR function that are typically included for people with reduced vestibular dysfunction are discussed below. Substitution strategies are taught to patients with no remaining vestibular function. In this approach, the patient is encouraged to rely on visual and somatosensory information in place of vestibular information to stabilize gaze and maintain postural stability. 73 Strategies that may be used in place of VOR function to improve gaze stability include the enhanced use of the cervico-ocular reflex, 79
10 corrective eye saccades, and slower velocity head movements. 73,77 Specific exercises are taught to the patient that allow the practice of these various alternative strategies without choosing a particular strategy for the patient (Appendix 2). The rationale for the use of substitution strategies for patients with no remaining vestibular function is derived from animal studies, which suggest that the CNS produces postural compensation for vestibular lesions from cervical spine proprioception and visual input during active head movement. 80,81 In addition, increased use of cervical spine inputs to stabilize gaze during low-frequency head movements has been documented in people with bilateral vestibular loss. 82,83 All patients with vestibular dysfunction should perform exercises aimed at improving postural control to retrain VSR function. The exercises should include attention to any underlying musculoskeletal impairments as well as any problematic areas in the sensory and motor organization of balance that are identified during the examination. Table 3 outlines specific exercises that can be used to help improve the motor and sensory organization aspects (or components) of postural control. Exercises should be individually tailored to focus on either sensory organization or motor organization as appropriate. The application of these specific concepts to 2 patients with reduced vestibular function is described elsewhere, and clinicians may find it helpful to review this application. 13 walking and functional activities. For example, the intervention can include standing activities that alter the base of support, support surface, or arm position. Walking and functional activities that incorporate turning and maneuvering around obstacles and balance board activities that aim to elicit appropriate hip or ankle strategy movement patterns can also be included. It is important to include balance and functional retraining activities that incorporate VOR and VSR function simultaneously, such as walking with head rotation, which requires that the patient maintain (or quickly regain) gaze stability during a dynamic balance activity. Progression over time should include activities that also require the patient to process distorted or confusing visual information while maintaining postural stability. Finally, general conditioning exercises are often useful to help improve tolerance for performing functional activities in environments with busy visual backgrounds, tolerance to body and head movements as a whole, and overall fitness level. Suggested activities include progressive walking programs, treadmill walking, stationary cycling, step aerobics, or the use of a step machine. Participation in some element of general conditioning 3 to 5 times per week at an intensity that does not produce disabling dizziness, vertigo, or fatigue is generally added to the home exercise program at a time when the patient is able to perform such activities. Specific sensory organization exercises involve maintaining balance during progressively more difficult static and dynamic movement tasks while the availability and accuracy of input from 1 or more of the 3 sensory systems (vestibular, somatosensory, or visual) is systematically varied. 52 For example, a patient with symptoms of dizziness or unsteadiness in busy visual environments could be trained to optimize the use of vestibular and somatosensory inputs (and perhaps reduce reliance on visual inputs). An appropriate intervention might include standing with a narrowed base of support with eyes closed and walking with a narrowed base of support on a firm surface. Alternately, the patient might be best trained to optimize the use of visual and vestibular inputs by practicing standing or walking on a foam surface with eyes open and closed. Because the therapist does not know the particular sensory reorganization strategy that will be most useful for a particular patient, a number of exercises are ideally taught to the patient for practice at home. A patient with no residual vestibular function and the same clinical presentation noted above could practice activities that enhance the use of somatosensory inputs during balance activities by standing or walking with a narrowed base of support with eyes closed. Specific motor organization exercises focus on improving the coordination of muscle responses during standing and 10 Procedural Interventions: Distorted Vestibular Function Various interventions have been described to manage motion-induced vertigo (including BPPV) of peripheral origin. All interventions involve performing a repositioning maneuver with the patient to either dislodge or reposition debris within one of the semicircular canals. In addition, habituation exercises may be useful for patients with motion-induced vertigo of either peripheral or central origin. Balance retraining and conditioning exercises may also be indicated. Four of the more commonly used repositioning techniques for peripheral motion-induced vertigo will be described here. Brandt-Daroff exercises 23 require the patient to repeatedly move from the sitting position into the side-lying provoking position several times in a row, several times a day (Fig. 3). Torsional nystagmus and vertigo often occur with each change in position, so the patient is instructed to wait until the vertigo has resolved before moving on to the next position. These exercises can be performed by the patient at home (once proper patient instruction has occurred) until the patient experiences no symptoms during performance of the exercise for at least 2 days. The mechanism underlying Brandt-Daroff exercises may be
11 either that the debris is dislodged from the cupula of the posterior canal or that habituation occurs. Brandt and Daroff 23 reported improvements in BPPV within 2 weeks in 95% of patients who received these exercises (no control group was used), suggesting that this may be an effective intervention for patients with posterior canal involvement. The Liberatory maneuver, a single maneuver that is performed once, was originally described by Semont et al 24 and later modified by Herdman. 50 This maneuver is indicated for patients with posterior canal involvement and is theorized to cause debris in the cupula to become dislodged and float to the common crus. 50 The patient is moved quickly from a sitting position into the side-lying position with the affected ear down and is kept in this position for 2 to 3 minutes (Fig. 4). Next, the patient is moved up through the sitting position to side lying on the opposite side with the unaffected ear down for another 5 minutes. The patient is then assisted to a sitting position and must maintain a vertical (upright) head position for 48 hours. A remission rate of between 70% and 95% has been reported with this maneuver in studies performed without control groups. 21,84 Herdman 50 and Epley 85 advocate the use of the canalith repositioning maneuver (Fig. 5) for patients who have BPPV that is believed to be due to canalithiasis. Various canalith repositioning maneuvers have been described to treat the various semicircular canals that may be involved. 50 For involvement of the posterior semicircular canal (Fig. 5), the patient moves from a sitting position to the Hallpike-Dix position with the affected ear down. After 2 to 3 minutes, the patient s head is slowly rotated to the opposite side. The patient is then assisted to turn onto this side maintaining the same head-neck alignment and remains in this position for 2 to 3 minutes. Finally, the patient is slowly assisted to a sitting position. Immediately following the maneuver, the patient is fitted with a soft collar and instructed to remain upright and not tilt the head for 48 hours. A remission rate of 70% after intervention with this maneuver has been reported by Li 86 in a study using an untreated control group. More recently, Ruckenstein 27 reported resolution of vertigo in 70% of patients with BPPV immediately following one canalith repositioning maneuver. One reported complication of the canalith repositioning maneuver is the possibility of moving the debris in the semicircular canal into a different canal, thereby producing BPPV of a different canal following intervention. If this occurs, further testing and observation is then required to correctly identify the involved canal before proceeding with the appropriate canalith repositioning maneuver. 11 Norre and De Weerdt 20 described a fourth intervention (called habituation exercises) in which patients move repeatedly into any position that provokes symptoms, not limited to the Hallpike-Dix position or side lying with the affected ear down. Each set of provoking positions performed by the patient is unique to that patient. Habituation is the theoretical mechanism underlying the resolution of symptoms with this approach. Norre and Beckers 26 studied 23 patients treated with the Liberatory maneuver and 28 patients treated with habituation exercises. They reported that habituation exercises, as described here, are equally effective (over 90% remission rate after 6 weeks of intervention) as the Liberatory maneuver in resolving symptoms. 26 Procedural Interventions: Central Vestibular Dysfunction The components of a vestibular rehabilitation program for people with central vestibular dysfunction are similar to those described above for people with peripheral vestibular dysfunction; however, they may need to be modified as appropriate for a given patient. For example, the gaze stabilization exercises in Appendix 1 are based on the premise that the patient has a reduced VOR gain; patients with cerebellar pathology, in fact, may have an increased VOR gain, so prescribing eye-head exercises aimed at increasing VOR gain would be inappropriate. Instead, exercises that require the patient to practice canceling VOR gain (such as tracking a moving target with the eyes while the head moves in the same direction as the object as opposed to moving in the opposite direction as described above) 32 or substitution exercises (Appendix 2) would be indicated. Performing habituation exercises may be beneficial if the patient has dizziness or vertigo and the examination does not reveal involvement of one specific semicircular canal. However, it is important to distinguish between positional vertigo of central versus peripheral origin because central vertigo may be due to damage to parts of the CNS other than the central vestibular structures or pathways and habituation exercises may not benefit the patient. Finally, the presence of cognitive deficits may affect the person s ability to adhere to the recommended frequency and specifics involved in carrying out an independent exercise program, a critical component of a vestibular rehabilitation program. Supervision by a family member or more frequent visits to the physical therapist may be required for an optimal outcome. Anticipated Goals/Expected Outcomes It can be difficult to specify exact outcomes that will be achieved for individual patients with vestibular dysfunction, although published reports exist to support the use of vestibular rehabilitation programs for various, although not all, groups of patients. For example, Norre
12 and De Weerdt 20 reported several case series suggesting that rehabilitation is effective for patients with unilateral vestibular dysfunction or BPPV. Published retrospective case series reviews 14,71 and case reports 71 suggest that patients who not compensate spontaneously within 2 months following the onset of unilateral vestibular dysfunction may respond to rehabilitation. Horak et al 16 have published preliminary results comparing 6 weeks of a vestibular rehabilitation program (n=13), medications (n=4), and general exercise (n=8). Patients (age range=18 60 years) with either unilateral or bilateral peripheral vestibular dysfunction were each randomly assigned to a group. Balance (measured by posturography) improved 88% to 211% over baseline in subjects receiving the vestibular rehabilitation program; no change occurred in the other 2 groups. Dizziness improved in all 3 groups, suggesting that vestibular rehabilitation was the best intervention choice for these subjects, who had both dizziness and dysequilibrium. Herdman and colleagues 17 reported the results of a controlled clinical trial of vestibular adaptation exercises in patients immediately following acoustic neuroma resection. An experimental group and a control group were used. The experimental group demonstrated significantly reduced dysequilibrium and reduced postural sway on the sixth postoperative day compared with the control group, suggesting that early intervention may aid in recovery of VSR function in these patients. Gill-Body and colleagues 13 reported the response to treatment for 2 patients one with unilateral peripheral vestibular dysfunction and one with bilateral peripheral vestibular hypofunction. After 8 weeks of treatment, both patients reported improvements in symptoms of dizziness and dysequilibrium as well as improved scores on the Dizziness Handicap Inventory; they also demonstrated objective improvements in clinical balance tests and computerized kinematic indicators of stability measured during the performance of standing, rising to stand, and walking tests. Vestibular function (rotary chair test) improved during the course of treatment only for the patient with unilateral dysfunction. These results suggest that vestibular rehabilitation may help promote functional improvements in patients with peripheral vestibular dysfunction, although different mechanisms for the improvement may exist for patients with different pathologies. The improvements in vestibular function tests that the patient with unilateral involvement made may suggest that vestibular adaptation occurred. The selfreported and functional improvements of the patient with bilateral involvement may be explained by substitution of alternative strategies for gaze stability and postural control. 12 This same group of researchers also reported preliminary results of a double-blind randomized clinical trial of vestibular rehabilitation in a group of subjects (N=8) with bilateral peripheral vestibular dysfunction. 18 Patients were randomly assigned to 1 of 2 groups. Subjects in group A received 8 weeks of vestibular rehabilitation with weekly physical therapy appointments, were retested at 8 weeks, and then continued their home program independently for another 8 weeks. Subjects in group B performed isometric exercises (as a control intervention) for the first 8 weeks and then vestibular rehabilitation for the second 8 weeks. Tests performed to monitor patient changes during and after different the various phases of intervention included the rotary chair test; posturography; kinematic and kinetic analysis of standing, gait, stair ascent, and chair rise; timed clinical balance tests; and patient self-reports of symptom frequency, intensity, and perception of handicap (Dizziness Handicap Inventory). According to the results, the symptoms and balance testing scores in the subjects in group A improved the most during the first treatment period and improved more modestly during the second 8-week period; group B subjects demonstrated little improvement during the first (control treatment) period but improved significantly during their second (vestibular rehabilitation) period. Rotary chair test changes were not evident in either group. These results suggest that vestibular damage is not obviated by the intervention but that functional ability improves nonetheless, lending support to the theoretical foundation of vestibular rehabilitation as an intervention. Much less is known about the specific benefits associated with vestibular rehabilitation for individuals with central vestibular system dysfunction. Shepard and colleagues 14 performed a prospective study on 152 people with various etiologies of vestibular dysfunction some subjects had peripheral dysfunction, some had central dysfunction, and some had both peripheral and central dysfunction (called the mixed group). Twenty-six patients with traumatic brain injury were included in the mixed group. Outcomes after intervention were measured using self-report of symptoms and disability as well as posturography tests. Although outcome was not found to be influenced by classification of the dysfunction as peripheral, central, or mixed, patients with mixed dysfunction had a longer duration of care compared with the other 2 groups. Patients with brain injury had poorer outcomes overall. In the total group of subjects, 85% of the patients reported decreased symptoms and 80% reported decreased disability after the intervention compared with 62% and 54%, respectively, for the patients with brain injury. Eighty-five percent of the entire group improved on posturography testing. It appears that people with central vestibular dysfunction may benefit from vestibular
13 rehabilitation, but it is unclear what degree of improvement should be expected, which patients might benefit the most, and what factors may alter their response to intervention. This is a promising area for further research in physical therapy. Summary Vestibular rehabilitation is an exciting group of interventions for physical therapists to learn about and use with their patients. Beginning evidence supports its efficacy, although more research is needed to clarify which patients might best benefit from intervention, what the critical components of the intervention are, and what degree of improvement can be expected in people with different types of vestibular dysfunction. References 1. Watson MA, Sinclair H. Balancing Act for People With Dizziness and Balance Disorders. Portland, Ore: Vestibular Disorders Association; 1992: Peterson BW, Fukushima K. The reticulospinal system and its role in generating vestibular and visuomotor reflexes. In: Sjolund B, Borkland A, eds. Brainstem Control of Spinal Mechanisms. Amsterdam, the Netherlands: Elsevier Science Publishers BV; 1987: Black FO. Peripheral vestibular disorders. In: Harker LA, ed. Ear and Skull Base. St Louis, Mo: Mosby-Year Book; 1986: Otolaryngology: Head and Neck Surgery; Vol Gill-Body KM, Krebs DE, Parker SW, Riley PO. Physical therapy management of peripheral vestibular dysfunction: two clinical case reports. Phys Ther. 1994;74: Shepard NT, Telian SA, Smith-Wheelock M. Habituation and balance retraining therapy: a retrospective review. Neurol Clin. 1990;8: Calder JH, Jacobson GP. Acquired bilateral peripheral vestibular system impairment: rehabilitative options and potential outcomes. J Am Acad Audiol. 2000;11: Berman JM, Fredrickson JM. Vertigo after head injury: a fiveyear follow-up. J Otolaryngol. 1978;7: Hain TC, Hillman MA. Anatomy and physiology of the normal vestibular system. In: Herdman SJ, ed. Vestibular Rehabilitation. Philadelphia, Pa: FA Davis Co; 1994: Carleton SC, Carpenter MB. Afferent and efferent connections of the medial, inferior, and lateral vestibular nuclei in the cat and monkey. Brain Res. 1983;278: Petrosini L, Troiani D, Zannoni B. Trigeminal stimulation modulates vestibular unitary activity. Experientia. 1982;38: Tickle DR, Schneider GE. Projection of the auditory nerve to the medial vestibular nucleus. Neurosci Lett. 1982;28: Peterson BW, Fukushima K, Hirai N, et al. Responses of vestibulospinal and reticulospinal neurons to sinusoidal vestibular stimulation. J Neurophysiol. 1980;43: Minor LB. Physiological principles of vestibular function on earth and in space. Otolaryngol Head Neck Surg. 1998;118(3 Pt 2):S5-S Baloh RW, Honrubia V. Clinical Neurophysiology of the Vestibular System. 2nd ed. Philadelphia, Pa: FA Davis Co; 1990: Peterson BW, Pitts NG, Fukushima K, Mackel R. Reticulospinal excitation and inhibition of neck motoneurons. Exp Brain Res. 1978;32: Horak FB, Jones-Rycewicz C, Black FO, Shumway-Cook A. Effects of vestibular rehabilitation on dizziness and imbalance. Otolaryngol Head Neck Surg. 1992;106: Herdman SJ, Clendaniel RA, Mattox DE, et al. Vestibular adaptation exercises and recovery: acute stage after acoustic neuroma resection. Otolaryngol Head Neck Surg. 1995;113: Krebs DE, Gill-Body KM, Riley PO, Parker SW. Doubleblind, placebo-controlled trial of rehabilitation for bilateral vestibular hypofunction: preliminary report. Otolaryngol Head Neck Surg. 1993;109: Black FO, Angel CR, Pesznecker SC, Gianna C. Outcome analysis of individualized vestibular rehabilitation protocols. Am J Otol. 2000;21: Norre ME, De Weerdt W. Treatment of vertigo based on habituation, 2: technique and results of habituation training. J Laryngol Otol. 1980;94: Herdman SJ, Tusa RJ, Zee DS, et al. Single treatment approaches to benign paroxysmal positional vertigo. Arch Otolaryngol Head Neck Surg. 1993;119: Herdman SJ. Physical therapy in the treatment of patients with benign paroxysmal positional vertigo. Neurology Report. 1996;20: Brandt T, Daroff RB. Physical therapy for benign paroxysmal positional vertigo. Arch Otolaryngol. 1980;106:
14 24. Semont A, Freyss G, Vitte E. Curing the BPPV with a Liberatory maneuver. Adv Otorhinolaryngol. 1988;42: Norre ME, Beckers A. Exercise treatment for paroxysmal positional vertigo: comparison of two types of exercises. Arch Otorhinolaryngol. 1987;244: Norre ME, Beckers A. Comparative study of two types of exercise treatment for paroxysmal positioning vertigo. Adv Otorhinolaryngol. 1988;42: Ruckenstein MJ. Therapeutic efficacy of the Epley canalith repositioning maneuver. Laryngoscope. 2001;111: Cooke DL. Central vestibular disorders. Neurology Report. 1996;20: Herrera WG. Vestibular and other balanace disorders in multiple sclerosis: differential diagnosis of disquilibrium and topognostic localization. Neurol Clin. 1990;8: Gizzi M. The efficacy of vestibular rehabilitation for patients with head trauma. J Head Trauma Rehabil. 1995;10: Shepard NT, Telian SA. Programmatic vestibular rehabilitation. Otolaryngol Head Neck Surg. 1995;112: Gill-Body KM, Popat RA, Parker SW, Krebs DE. Rehabilitation of balance in two patients with cerebellar dysfunction. Phys Ther. 1997;77: Cass SP, Borello-France D, Furman JM. Functional outcome of vestibular rehabilitation in patients with abnormal sensoryorganization testing. Am J Otol. 1996;17: Burton JM. Physical therapy management of a patient with central vestibular dysfunction: a case report. Neurology Report. 1996;22: Whitney SL, Herdman SJ. Physical therapy assessment of vestibular hypofunction. In: Herdman SJ, ed. Vestibular Rehabilitation. 2nd ed. Philadelphia, Pa: FA Davis Co; 2000: Jacobson GP, Newman CW. The development of the Dizziness Handicap Inventory. Arch Otolaryngol Head Neck Surg. 1990;116: Powell LE, Myers AM. The Activities-specific Balance Confidence Scale. J Gerontol A Biol Sci Med Sci. 1995;50:M28- M Parker SW. Vestibular evaluation: electronystagmography, rotational testing, and posturography. Clin Electroencephalogr. 1993;24: Bhansali SA, Hunrubia V. Current status of electronystagmography testing. Otolaryngol Head Neck Surg. 1999;120: Fife TD, Tusa RJ, Furman JM, et al. Assessment: vestibular testing techniques in adults and children, report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology. 2000;55: Hess K, Baloh RW, Honrubia V, Yee RD. Rotational testing in patients with bilateral peripheral vestibular disease. Laryngoscope. 1985;95: Nashner LM. Adapting reflexes controlling the human posture. Exp Brain Res. 1976;26: Nashner LM. Fixed patterns of rapid postural responses among leg muscles during stance. Exp Brain Res. 1977;30: Allum JH, Shepard NT. An overview of the clinical use of dynamic posturography in the differential diagnosis of balance disorders. J Vestib Res. 1999;9: McKinnon AG, Malamut DB, Denham TV. An objective measure of gaze stability: speed of gaze stability exercise performance using a computerized motion sensor and flashing numbers [abstract]. Neurology Report. 1997;21: Herdman SJ, Blatt PJ, Venuto P, Tusa RJ. Quantitative dynamic visual acuity test (DVA): clinical utility in diagnosis [abstract]. Phys Ther. 1998;78:S Harvey SA, Wood DJ, Feroah JR. Relationship of the head impulse test and head-shake nystagmus in reference to caloric testing. Am J Otol. 1997;18: Baloh RW, Honrubia V. Clinical Neurophysiology of the Vestibular System. 2nd ed. Philadelphia, Pa: FA Davis Co; 1990: Herdman SJ. Treatment of benign paroxysmal positional vertigo. Phys Ther. 1990;70: Herdman SJ. Advances in the treatment of vestibular disorders. Phys Ther. 1997;77: Horak FB. Clinical measurement of postural control in adults. Phys Ther. 1987:67:
15 52. Shumway-Cook A, Horak FB. Assessing the influence of sensory interaction on balance: suggestion from the field. Phys Ther. 1986;66: Diener HC, Horak FB, Nashner LM. Influence of stimulus parameters on human postural responses. J Neurophysiol. 1988;59: Fuduka T. Statokinetic Reflexes in Equilibrium and Movement. Tokyo, Japan: Tokyo University Press; Shumway-Cook A, Woollacott M. Motor Control: Theory and Practical Applications. Baltimore, Md: Williams & Wilkins; 1995: Fregly AR, Graybiel A, Smith MJ. Walk on floor eyes closed (WOFEC): a new addition to an ataxia battery. Aerosp Med. 1972;43: Herdman SJ, Sandusky AL, Hain TC, et al. Characteristics of postural stability in patients with aminoglycoside toxicity. J Vestib Res. 1994;4: Asai M, Watanabe Y, Shimizu K. Effects of vestibular rehabilitation on postural control. Acta Otolaryngol Suppl. 1997;528: Cawthorne T. The physiological basis for head exercises. Journal of the Chartered Society of Physiotherapy. 1944;30: Duncan PW, Weiner DK, Chandler J, Studenski S. Functional reach: a new clinical measure of balance. J Gerontol. 1990;45:M192-M Herdman SJ, Clendaniel RA. Assessment and treatment of complete vestibular loss. In: Herdman SJ, ed. Vestibular Rehabilitation. 2nd ed. Phildelphia, Pa: FA Davis Co: 2000: Graybiel A, Fregly AR. A new quantitative ataxia test battery. Acta Otolaryngol. 1966;61: Duncan PW, Studenski S, Chandler J, Prescott B. Functional reach: predictive validity in a sample of elderly male veterans. J Gerontol. 1992;47:M93-M Podsiadlo D, Richardson S. The timed Up & Go : a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc. 1991;39: Holden MK, Gill KM, Magliozzi MR. Gait assessment for neurologically impaired patients: standards for outcome assessment. Phys Ther. 1986;66: Lawton MP, Brody EM. Assessment of older people: selfmaintaining and instrumental activities of daily living. Gerontology. 1969;9: Holbrook M, Skilbeck CE. An activities index for use with stroke patients. Age Ageing. 1983;12: Herdman SJ. Balance rehabilitation: background, techniques, and usefulness. In: Jacobson GP, Newman CW, Kurtash JM, eds. Handbook of Balance Function and Testing. St Louis, Mo: CV Mosby Co; 1993: chap Gill-Body KM, Krebs DE. Locomotor stability problems associated with vestibulopathy: assessment and treatment. Physical Therapy Practice. 1994;3: Cooksey FS. Rehabilitation in vestibular injuries. Proc R Soc Med. 1946;39: Shumway-Cook A, Horak FB. Vestibular rehabilitation: an exercise approach to managing symptoms of vestibular dysfunction. Seminars in Hearing. 1989;10: Shumway-Cook A, Horak FB. Rehabilitation strategies for patients with vestibular deficits. Neurol Clin. 1990;8: Herdman SJ. Exercise strategies for vestibular disorders. Ear Nose Throat J. 1989;68: Herdman SJ, Whitney SL. Treatment of vestibular hypofunction. In: Herdman SJ, ed. Vestibular Rehabilitation. 2nd ed. Philadelphia, Pa: FA Davis Co; 2000: Herdman SJ. Assessment and treatment of balance disorders in the vestibular-deficient patient. In: Duncan P, ed. Balance: Proceedings of the APTA Forum. Alexandria, Va: American Physical Therapy Association; 1990: Gauthier GM, Robinson DA. Adaptation of the human vestibulo-ocular reflex to magnifying lenses. Brain Res. 1975;92: Herdman SJ. Role of vestibular adaptation in vestibular rehabilitation. Otolaryngol Head Neck Surg. 1998;119: Szturm T, Ireland DJ, Lessing-Turner M. Comparison of different exercise programs in the rehabilitation of patients with chronic peripheral vestibular dysfunction. J Vestib Res. 1994;4: Bronstein AM, Hood JD. The cervico-ocular reflex in normal subjects and patients with absent vestibular function. Brain Res. 1986;373:
16 80. Newlands SD, Perachio AA. Effect of T2 spinal transection on compensation of horizontal canal related activity in the medial vestibular nucleus following unilateral labyrinth ablation in the decerebrate gerbil. Brain Res. 1991;541: Lisberger SG. The latency of pathways containing the site of motor learning in the monkey vestibulo-ocular reflex. Science. 1984;225: Ireland D. The Semont maneuver. In: Proceedings of the Barany Society Meeting. Prague, Czechoslovakia: Barany Society; 1994: Epley JM. The canalith repositioning procedure: for treatment of benign paroxysmal positional vertigo. Otolaryngol Head Neck Surg. 1992;107: Bronstein AM, Hood JD. The cervical-ocular reflex in normal subjects and patients with absent vestibular function. Brain Res. 1986;373: Li JC. Mastoid oscillation: a critical factor for success in the canalith repositioning procedure. Otolaryngol Head Neck Surg. 1995;112: Kasai T, Zee DS. Eye-head coordination in labrynthinedefective human beings. Brain Res. 1978;144:
17 17
18 18
19 19

20 Figure 1. 20

21 Figure 2. Figure 3. 21

22 Figure 4. Figure 5. 22
VESTIBULAR SYSTEM. Deficits cause: Vertigo. Falling Tilting Nystagmus Nausea, vomiting
 VESTIBULAR SYSTEM Objectives: Understand the functions of the vestibular system: What is it? How do you stimulate it? What are the consequences of stimulation? Describe the vestibular apparatus, the 2
VESTIBULAR SYSTEM Objectives: Understand the functions of the vestibular system: What is it? How do you stimulate it? What are the consequences of stimulation? Describe the vestibular apparatus, the 2
Vestibular System. Dian Yu, class of 2016
 Vestibular System Dian Yu, class of 2016 Objectives 1. Describe the functions of the vestibular system: What is it? How do you stimulate it? What are the consequences of stimulation? 2. Describe the vestibular
Vestibular System Dian Yu, class of 2016 Objectives 1. Describe the functions of the vestibular system: What is it? How do you stimulate it? What are the consequences of stimulation? 2. Describe the vestibular
Vestibular Physiology Richard M. Costanzo, Ph.D.
 Vestibular Physiology Richard M. Costanzo, Ph.D. OBJECTIVES After studying the material of this lecture, the student should be able to: 1. Describe the structure and function of the vestibular organs.
Vestibular Physiology Richard M. Costanzo, Ph.D. OBJECTIVES After studying the material of this lecture, the student should be able to: 1. Describe the structure and function of the vestibular organs.
OBJECTIVES BALANCE EVALUATION COMMON CAUSES OF BALANCE DEFICITS POST TBI BRAIN INJURY BALANCE RELATIONSHIP
 OBJECTIVES Understand variables that contribute to balance deficits Understand the relationship between a brain injury and balance Become familiar with the components of a vestibular/balance assessment
OBJECTIVES Understand variables that contribute to balance deficits Understand the relationship between a brain injury and balance Become familiar with the components of a vestibular/balance assessment
What is the effect on the hair cell if the stereocilia are bent away from the kinocilium?
 CASE 44 A 53-year-old man presents to his primary care physician with complaints of feeling like the room is spinning, dizziness, decreased hearing, ringing in the ears, and fullness in both ears. He states
CASE 44 A 53-year-old man presents to his primary care physician with complaints of feeling like the room is spinning, dizziness, decreased hearing, ringing in the ears, and fullness in both ears. He states
Control of eye movement
 Control of eye movement Third Nerve Palsy Eye down and out Trochlear Nerve Palsy Note: Right eye Instead of intorsion and depression action of superior oblique See extorsion and elevation Observe how
Control of eye movement Third Nerve Palsy Eye down and out Trochlear Nerve Palsy Note: Right eye Instead of intorsion and depression action of superior oblique See extorsion and elevation Observe how
Vestibular physiology
 Vestibular physiology 2017 Utricle A flat epithelium: horizontal in the upright head Utricle Hair cells: no axons hair cells Utricle Hair cells synapse onto 8th nerve afferents. 8th nerve afferents Hair
Vestibular physiology 2017 Utricle A flat epithelium: horizontal in the upright head Utricle Hair cells: no axons hair cells Utricle Hair cells synapse onto 8th nerve afferents. 8th nerve afferents Hair
The Physiology of the Senses Lecture 10 - Balance
 The Physiology of the Senses Lecture 10 - Balance www.tutis.ca/senses/ Contents Objectives... 1 The sense of balance originates from the labyrinth... 2 The auditory and vestibular systems have a common
The Physiology of the Senses Lecture 10 - Balance www.tutis.ca/senses/ Contents Objectives... 1 The sense of balance originates from the labyrinth... 2 The auditory and vestibular systems have a common
Vestibular Differential Diagnosis
 Vestibular Differential Diagnosis P R E S E N T E D B Y : S H A R I K I C K E R, P T, M P T C E R T I F I C A T E I N V E S T I B U L A R R E H A B I L I T A T I O N 2 0 1 7 L A C E Y H A L E, P T, D P
Vestibular Differential Diagnosis P R E S E N T E D B Y : S H A R I K I C K E R, P T, M P T C E R T I F I C A T E I N V E S T I B U L A R R E H A B I L I T A T I O N 2 0 1 7 L A C E Y H A L E, P T, D P
Course: PG- Pathshala Paper number: 13 Physiological Biophysics Module number M23: Posture and Movement Regulation by Ear.
 Course: PG- Pathshala Paper number: 13 Physiological Biophysics Module number M23: Posture and Movement Regulation by Ear Principal Investigator: Co-Principal Investigator: Paper Coordinator: Content Writer:
Course: PG- Pathshala Paper number: 13 Physiological Biophysics Module number M23: Posture and Movement Regulation by Ear Principal Investigator: Co-Principal Investigator: Paper Coordinator: Content Writer:
Defining Dizziness: An Acute Approach to Vestibular Dysfunction in the Hospital Setting Friday, February 17, :00 AM-10:00 AM
 Defining Dizziness: An Acute Approach to Vestibular Dysfunction in the Hospital Setting Friday, February 17, 2017 8:00 AM-10:00 AM Kerry Lammers, PT, DPT Gabrielle Steinhorn, PT, DPT, NCS Vestibular dysfunction
Defining Dizziness: An Acute Approach to Vestibular Dysfunction in the Hospital Setting Friday, February 17, 2017 8:00 AM-10:00 AM Kerry Lammers, PT, DPT Gabrielle Steinhorn, PT, DPT, NCS Vestibular dysfunction
THE VESTIBULAR APPRATUS AND PATHWAY
 Dental Neuroanatomy February 23, 2012 Suzanne Stensaas, Ph.D. Reading: Waxman Chapter 17 Also pp 105-108 on control of eye movments Computer Resources: HyperBrain Ch. 8 Vestibulospinal Pathway Quiz http://library.med.utah.edu/kw/animations/hyperbrain/pathways/
Dental Neuroanatomy February 23, 2012 Suzanne Stensaas, Ph.D. Reading: Waxman Chapter 17 Also pp 105-108 on control of eye movments Computer Resources: HyperBrain Ch. 8 Vestibulospinal Pathway Quiz http://library.med.utah.edu/kw/animations/hyperbrain/pathways/
Saccades. Assess volitional horizontal saccades with special attention to. Dysfunction indicative of central involvement (pons or cerebellum)
") Saccades Assess volitional horizontal saccades with special attention to Amplitude? Duration? Synchrony? Dysfunction indicative of central involvement (pons or cerebellum) Dynamic Visual Acuity Compare
Saccades Assess volitional horizontal saccades with special attention to Amplitude? Duration? Synchrony? Dysfunction indicative of central involvement (pons or cerebellum) Dynamic Visual Acuity Compare
Sasan Dabiri, MD, Assistant Professor
 Sasan Dabiri, MD, Assistant Professor Department of Otorhinolaryngology Head & Neck Surgery Amir A lam hospital Tehran University of Medical Sciences October 2015 Outlines Anatomy of Vestibular System
Sasan Dabiri, MD, Assistant Professor Department of Otorhinolaryngology Head & Neck Surgery Amir A lam hospital Tehran University of Medical Sciences October 2015 Outlines Anatomy of Vestibular System
VESTIBULAR SYSTEM ANATOMY AND PHYSIOLOGY. Professor.Dr. M.K.Rajasekar MS., DLO.,
 VESTIBULAR SYSTEM ANATOMY AND PHYSIOLOGY Professor.Dr. M.K.Rajasekar MS., DLO., Life is hard for those who don t have a VOR During a walk I found too much motion in my visual picture of the surroundings
VESTIBULAR SYSTEM ANATOMY AND PHYSIOLOGY Professor.Dr. M.K.Rajasekar MS., DLO., Life is hard for those who don t have a VOR During a walk I found too much motion in my visual picture of the surroundings
The Vestibular System
 The Vestibular System Vestibular and Auditory Sensory Organs Bill Yates, Ph.D. Depts. Otolaryngology & Neuroscience University of Pittsburgh Organization of Sensory Epithelium Displacement of Stereocilia
The Vestibular System Vestibular and Auditory Sensory Organs Bill Yates, Ph.D. Depts. Otolaryngology & Neuroscience University of Pittsburgh Organization of Sensory Epithelium Displacement of Stereocilia
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: vestibular_function_testing 5/2017 N/A 10/2017 5/2017 Description of Procedure or Service Dizziness, vertigo,
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: vestibular_function_testing 5/2017 N/A 10/2017 5/2017 Description of Procedure or Service Dizziness, vertigo,
University of Connecticut Schools of Medicine and Dental Medicine Systems Neuroscience Meds Vestibular System
 University of Connecticut Schools of Medicine and Dental Medicine Systems Neuroscience Meds 371 2007-08 Vestibular System S. Kuwada Reading: Purves et al. (2008, 4 th edition), Neuroscience, Chapter 14.
University of Connecticut Schools of Medicine and Dental Medicine Systems Neuroscience Meds 371 2007-08 Vestibular System S. Kuwada Reading: Purves et al. (2008, 4 th edition), Neuroscience, Chapter 14.
Extraocular Muscles and Ocular Motor Control of Eye Movements
 Extraocular Muscles and Ocular Motor Control of Eye Movements Linda K. McLoon PhD mcloo001@umn.edu Department of Ophthalmology and Visual Neurosciences Your Eyes Are Constantly Moving. Yarbus, 1967 Eye
Extraocular Muscles and Ocular Motor Control of Eye Movements Linda K. McLoon PhD mcloo001@umn.edu Department of Ophthalmology and Visual Neurosciences Your Eyes Are Constantly Moving. Yarbus, 1967 Eye
Auditory and Vestibular Systems
 Auditory and Vestibular Systems Objective To learn the functional organization of the auditory and vestibular systems To understand how one can use changes in auditory function following injury to localize
Auditory and Vestibular Systems Objective To learn the functional organization of the auditory and vestibular systems To understand how one can use changes in auditory function following injury to localize
Vestibular Evaluation
 Chris Carpino, MPT Vestibular Evaluation 1. History Most important aspect of evaluation (see DHI) 2. Vital Signs Check blood pressure in supine and sitting 3. Eye Exam 4. Positional Testing 5. Balance
Chris Carpino, MPT Vestibular Evaluation 1. History Most important aspect of evaluation (see DHI) 2. Vital Signs Check blood pressure in supine and sitting 3. Eye Exam 4. Positional Testing 5. Balance
Vestibular System Dr. Bill Yates Depts. Otolaryngology and Neuroscience 110 Eye and Ear Institute
 Vestibular System Dr. Bill Yates Depts. Otolaryngology and Neuroscience 110 Eye and Ear Institute 412-647-9614 byates@pitt.edu What is the Vestibular System? The vestibular system is the sensory system,
Vestibular System Dr. Bill Yates Depts. Otolaryngology and Neuroscience 110 Eye and Ear Institute 412-647-9614 byates@pitt.edu What is the Vestibular System? The vestibular system is the sensory system,
Cross Country Education Leading the Way in Continuing Education and Professional Development.
 To comply with professional boards/associations standards: I declare that I or my family do not have any financial relationship in any amount, occurring in the last 12 months with a commercial interest
To comply with professional boards/associations standards: I declare that I or my family do not have any financial relationship in any amount, occurring in the last 12 months with a commercial interest
Otoconia: Calcium carbonate crystals Gelatinous mass. Cilia. Hair cells. Vestibular nerve. Vestibular ganglion
 VESTIBULAR SYSTEM (Balance/Equilibrium) The vestibular stimulus is provided by Earth s, and. Located in the of the inner ear, in two components: 1. Vestibular sacs - gravity & head direction 2. Semicircular
VESTIBULAR SYSTEM (Balance/Equilibrium) The vestibular stimulus is provided by Earth s, and. Located in the of the inner ear, in two components: 1. Vestibular sacs - gravity & head direction 2. Semicircular
CITY & HACKNEY PATHFINDER CLINICAL COMMISSIONING GROUP. Vertigo. (1) Vertigo. (4) Provisional Diagnosis. (5) Investigations. lasting days or weeks
 Vertigo. (4) Provisional Diagnosis. (5) Investigations. lasting days or weeks") Authors: Dr Lucy O'Rouke and Mr N Eynon-Lewis Review date: January 2017 Vertigo (1) Vertigo (2) History (3) Examination (4) Provisional Diagnosis (5) Investigations (6) Medical Cause (7) Psychiatric Cause
Authors: Dr Lucy O'Rouke and Mr N Eynon-Lewis Review date: January 2017 Vertigo (1) Vertigo (2) History (3) Examination (4) Provisional Diagnosis (5) Investigations (6) Medical Cause (7) Psychiatric Cause
Cervical reflex Giovanni Ralli. Dipartimento di Organi di Senso, Università di Roma La Sapienza
 Cervical reflex Giovanni Ralli Dipartimento di Organi di Senso, Università di Roma La Sapienza The development of the neck in vertebrates allows the individual to rotate the head independently of the trunk
Cervical reflex Giovanni Ralli Dipartimento di Organi di Senso, Università di Roma La Sapienza The development of the neck in vertebrates allows the individual to rotate the head independently of the trunk
Acoustic neuroma s/p removal BPPV (Crystals)- 50% of people over 65 y/ o with dizziness will have this as main reason for dizziness
- 50% of people over 65 y/ o with dizziness will have this as main reason for dizziness") Dizziness and the Heart Mended Hearts Inservice Karen Hansen, PT, DPT, Cert Vestibular Rehab, CEAS Tennessee Therapy & Balance Center, LLC July 21, 2016 Balance We maintain balance with input from our
Dizziness and the Heart Mended Hearts Inservice Karen Hansen, PT, DPT, Cert Vestibular Rehab, CEAS Tennessee Therapy & Balance Center, LLC July 21, 2016 Balance We maintain balance with input from our
Unit VIII Problem 5 Physiology: Cerebellum
 Unit VIII Problem 5 Physiology: Cerebellum - The word cerebellum means: the small brain. Note that the cerebellum is not completely separated into 2 hemispheres (they are not clearly demarcated) the vermis
Unit VIII Problem 5 Physiology: Cerebellum - The word cerebellum means: the small brain. Note that the cerebellum is not completely separated into 2 hemispheres (they are not clearly demarcated) the vermis
Differential Diagnosis: Vestibular Pathology. Causes of Dizziness. Benign Paroxysmal Positional Vertigo
 Differential Diagnosis: Vestibular Learning objective: The participant will identify the pathologies associated with complaints of imbalance and dizziness Anne K Galgon PT, PhD, NCS Vestibular and Related
Differential Diagnosis: Vestibular Learning objective: The participant will identify the pathologies associated with complaints of imbalance and dizziness Anne K Galgon PT, PhD, NCS Vestibular and Related
Cranial Nerve VIII (The Vestibulo-Cochlear Nerve)
") Cranial Nerve VIII (The Vestibulo-Cochlear Nerve) Please view our Editing File before studying this lecture to check for any changes. Color Code Important Doctors Notes Notes/Extra explanation Objectives
Cranial Nerve VIII (The Vestibulo-Cochlear Nerve) Please view our Editing File before studying this lecture to check for any changes. Color Code Important Doctors Notes Notes/Extra explanation Objectives
Peripheral vestibular disorders will affect 1 of 13 people in their lifetime
 Peripheral vestibular disorders will affect 1 of 13 people in their lifetime 80% of affected persons seek medical consultation Unclear how many of these are for peripheral vs central disorders Generally:
Peripheral vestibular disorders will affect 1 of 13 people in their lifetime 80% of affected persons seek medical consultation Unclear how many of these are for peripheral vs central disorders Generally:
Vertigo: A practical approach to diagnosis and treatment. John Waterston
 Vertigo: A practical approach to diagnosis and treatment John Waterston Background. Vertigo is a symptom that has diverse causes. The diagnosis may remain elusive even after exhaustive clinical enquiry
Vertigo: A practical approach to diagnosis and treatment John Waterston Background. Vertigo is a symptom that has diverse causes. The diagnosis may remain elusive even after exhaustive clinical enquiry
The Physiology of the Senses Lecture 10 - Balance
 The Physiology of the Senses Lecture 10 - Balance www.tutis.ca/senses/ Contents Objectives... 1 The sense of balance originates in the labyrinth.... 2 The vestibular system has two parts.... 3 The Anatomy
The Physiology of the Senses Lecture 10 - Balance www.tutis.ca/senses/ Contents Objectives... 1 The sense of balance originates in the labyrinth.... 2 The vestibular system has two parts.... 3 The Anatomy
3/2/2017. Vestibular and Visual Systems, and Considerations for Hippotherapy. Carol A. Huegel, PT, HPCS
 Vestibular and Visual Systems, and Considerations for Hippotherapy Carol A. Huegel, PT, HPCS Objectives The participant will: Have an understanding of the anatomy of the vestibular system and related neuroanatomy
Vestibular and Visual Systems, and Considerations for Hippotherapy Carol A. Huegel, PT, HPCS Objectives The participant will: Have an understanding of the anatomy of the vestibular system and related neuroanatomy
Predictors of Protracted Recovery
 CONCUSSION MANAGEMENT SPECIALIST ON LINE CURRICULUM Protracted Recovery and Clinical Rehabilitation All rights reserved. Sports Medicine Concepts Concussion Management Specialist Program 1 Predictors of
CONCUSSION MANAGEMENT SPECIALIST ON LINE CURRICULUM Protracted Recovery and Clinical Rehabilitation All rights reserved. Sports Medicine Concepts Concussion Management Specialist Program 1 Predictors of
Vestibular/Auditory Systems
 Vestibular/Auditory Systems Jay Zenner on February 3, 2012 Dental Neuroanatomy Scott Rogers Office: SOM 2C132 Boney Labyrinth Vestibular Apparatus Two Major Divisions Cochlea (anterior) VIII VII Semicircular
Vestibular/Auditory Systems Jay Zenner on February 3, 2012 Dental Neuroanatomy Scott Rogers Office: SOM 2C132 Boney Labyrinth Vestibular Apparatus Two Major Divisions Cochlea (anterior) VIII VII Semicircular
Ear. Utricle & saccule in the vestibule Connected to each other and to the endolymphatic sac by a utriculosaccular duct
 Rahaf Jreisat *You don t have to go back to the slides. Ear Inner Ear Membranous Labyrinth It is a reflection of bony labyrinth but inside. Membranous labyrinth = set of membranous tubes containing sensory
Rahaf Jreisat *You don t have to go back to the slides. Ear Inner Ear Membranous Labyrinth It is a reflection of bony labyrinth but inside. Membranous labyrinth = set of membranous tubes containing sensory
Update '08: Vestibular and Balance Rehabilitation Therapy
 Update '08: Vestibular and Balance Rehabilitation Therapy In Context with Surgery Medicine & Diet Symptoms of Dizziness Dizziness non-specific term; encompasses any and all of the specific symptoms: Vertigo
Update '08: Vestibular and Balance Rehabilitation Therapy In Context with Surgery Medicine & Diet Symptoms of Dizziness Dizziness non-specific term; encompasses any and all of the specific symptoms: Vertigo
Window to an Unusual Vestibular Disorder By Mark Parker
 WELCOME BACK to an ongoing series that challenges the audiologist to identify a diagnosis for a case study based on a listing and explanation of the nonaudiology and audiology test battery. It is important
WELCOME BACK to an ongoing series that challenges the audiologist to identify a diagnosis for a case study based on a listing and explanation of the nonaudiology and audiology test battery. It is important
Vestibular and Visual Systems
 15 Vestibular and Visual Systems Laurie Lundy-Ekman, PhD, PT INTRODUCTION Vestibular receptors and cranial nerve axons in the periphery, vestibular nuclei in the brainstem, and an area of the cerebral
15 Vestibular and Visual Systems Laurie Lundy-Ekman, PhD, PT INTRODUCTION Vestibular receptors and cranial nerve axons in the periphery, vestibular nuclei in the brainstem, and an area of the cerebral
9/6/2017. Physical Therapist Role in Management of Concussions. Areas where Physical Therapy Can Help. What is the Vestibular System?
 Physical Therapist Role in Management of Concussions The APTA recognizes that physical therapists are part of the multidisciplinary team of licensed healthcare providers that assist in concussion management,
Physical Therapist Role in Management of Concussions The APTA recognizes that physical therapists are part of the multidisciplinary team of licensed healthcare providers that assist in concussion management,
met het oog op evenwicht
 met het oog op evenwicht Herman Kingma, Department of ORL, Maastricht University Medical Centre Faculty of Biomedical Technology, Technical University Eindhoven problems in patients with dizziness and
met het oog op evenwicht Herman Kingma, Department of ORL, Maastricht University Medical Centre Faculty of Biomedical Technology, Technical University Eindhoven problems in patients with dizziness and
Vestibular Symptoms in Concussion: Medical/Surgical Perspective. Jacob R. Brodsky, MD Boston Children s Hospital
 Vestibular Symptoms in Concussion: Medical/Surgical Perspective Jacob R. Brodsky, MD Boston Children s Hospital jacob.brodsky@childrens.harvard.edu On Field Symptoms Headache Dizziness Confusion Fatigue
Vestibular Symptoms in Concussion: Medical/Surgical Perspective Jacob R. Brodsky, MD Boston Children s Hospital jacob.brodsky@childrens.harvard.edu On Field Symptoms Headache Dizziness Confusion Fatigue
Current Perspectives in Balance Assessment. Topics for Today. How are we doing? 3/5/2010. Scott K. Griffiths, Ph.D. March 26, 2010
 Current Perspectives in Balance Assessment Scott K. Griffiths, Ph.D. March 26, 2010 Topics for Today Evaluating the Dizzy Patient looking back, looking ahead The (Not So) New Kids on the Block: VEMPs,
Current Perspectives in Balance Assessment Scott K. Griffiths, Ph.D. March 26, 2010 Topics for Today Evaluating the Dizzy Patient looking back, looking ahead The (Not So) New Kids on the Block: VEMPs,
Acute Vestibular Syndrome (AVS) 12/5/2017
 12/5/2017") Sharon Hartman Polensek, MD, PhD Dept of Neurology, Emory University Atlanta VA Medical Center DIAGNOSTIC GROUPS FOR PATIENTS PRESENTING WITH DIZZINESS TO EMERGENCY DEPARTMENTS Infectious 2.9% Genitourinary
Sharon Hartman Polensek, MD, PhD Dept of Neurology, Emory University Atlanta VA Medical Center DIAGNOSTIC GROUPS FOR PATIENTS PRESENTING WITH DIZZINESS TO EMERGENCY DEPARTMENTS Infectious 2.9% Genitourinary
to vibrate the fluid. The ossicles amplify the pressure. The surface area of the oval window is
 Page 1 of 6 Question 1: How is the conduction of sound to the cochlea facilitated by the ossicles of the middle ear? Answer: Sound waves traveling through air move the tympanic membrane, which, in turn,
Page 1 of 6 Question 1: How is the conduction of sound to the cochlea facilitated by the ossicles of the middle ear? Answer: Sound waves traveling through air move the tympanic membrane, which, in turn,
cortical and brain stem control of motor function
 cortical and brain stem control of motor function cortical and brain stem control of motor function most voluntary movements initiated by the cerebral cortex are achieved when the cortex activates patterns
cortical and brain stem control of motor function cortical and brain stem control of motor function most voluntary movements initiated by the cerebral cortex are achieved when the cortex activates patterns
Chapter 19 Dizziness and Vertigo
 Chapter 19 Dizziness and Vertigo Episode overview: 1) Compare characteristics of peripheral and central vertigo 2) What are risk factors for central causes of vertigo? 3) List 4 vestibulotoxic drugs. 4)
Chapter 19 Dizziness and Vertigo Episode overview: 1) Compare characteristics of peripheral and central vertigo 2) What are risk factors for central causes of vertigo? 3) List 4 vestibulotoxic drugs. 4)
Role of brainstem in somatomotor (postural) functions
 functions") Role of brainstem in somatomotor (postural) functions (vestibular apparatus) The muscle tone and its regulation VESTIBULAR SYSTEM (Equilibrium) Receptors: Otolith organs Semicircular canals Sensation (information):
Role of brainstem in somatomotor (postural) functions (vestibular apparatus) The muscle tone and its regulation VESTIBULAR SYSTEM (Equilibrium) Receptors: Otolith organs Semicircular canals Sensation (information):
A&P 1. Ear, Hearing & Equilibrium Lab. Basic Concepts. Pre-lab Exercises
 A&P 1 Ear, Hearing & Equilibrium Lab Basic Concepts Pre-lab Exercises In this "Lab Exercise Guide", we will be looking at the basics of hearing and equilibrium. NOTE: these notes do not follow the order
A&P 1 Ear, Hearing & Equilibrium Lab Basic Concepts Pre-lab Exercises In this "Lab Exercise Guide", we will be looking at the basics of hearing and equilibrium. NOTE: these notes do not follow the order
INCIDENCE OF SUSPECTED OTOLITHIC ABNORMALITIES IN MILD TRAUMATIC BRAIN INJURED VETERANS OBSERVATIONS FROM A LARGE VA POLYTRAUMA NETWORK SITE
 INCIDENCE OF SUSPECTED OTOLITHIC ABNORMALITIES IN MILD TRAUMATIC BRAIN INJURED VETERANS OBSERVATIONS FROM A LARGE VA POLYTRAUMA NETWORK SITE David Domoracki Ph.D. Cleveland VAMC Audiology Service Jennifer
INCIDENCE OF SUSPECTED OTOLITHIC ABNORMALITIES IN MILD TRAUMATIC BRAIN INJURED VETERANS OBSERVATIONS FROM A LARGE VA POLYTRAUMA NETWORK SITE David Domoracki Ph.D. Cleveland VAMC Audiology Service Jennifer
Building Better Balance
 Building Better Balance The Effects of MS on Balance Individuals with MS experience a decline in their balance due to various MS related impairments. Some of these impairments can be improved with exercise
Building Better Balance The Effects of MS on Balance Individuals with MS experience a decline in their balance due to various MS related impairments. Some of these impairments can be improved with exercise
TEMPLATES FOR COMPREHENSIVE BALANCE EVALUATION REPORTS. David Domoracki PhD Cleveland Louis Stokes VA Medical Center
 TEMPLATES FOR COMPREHENSIVE BALANCE EVALUATION REPORTS David Domoracki PhD Cleveland Louis Stokes VA Medical Center The following templates are in outline form. I designed them so that the IRM local network
TEMPLATES FOR COMPREHENSIVE BALANCE EVALUATION REPORTS David Domoracki PhD Cleveland Louis Stokes VA Medical Center The following templates are in outline form. I designed them so that the IRM local network
Subject: Vestibular Rehabilitation
 01-92502-14 Original Effective Date: 06/15/05 Reviewed: 09/27/18 Revised: 10/15/18 Subject: Vestibular Rehabilitation THIS MEDICAL COVERAGE GUIDELINE IS NOT AN AUTHORIZATION, CERTIFICATION, EXPLANATION
01-92502-14 Original Effective Date: 06/15/05 Reviewed: 09/27/18 Revised: 10/15/18 Subject: Vestibular Rehabilitation THIS MEDICAL COVERAGE GUIDELINE IS NOT AN AUTHORIZATION, CERTIFICATION, EXPLANATION
Paediatric Balance Assessment
 BAA regional meeting 11 th March 2016 Paediatric Balance Assessment Samantha Lear, Lead Clinical Scientist, Hearing Services, SCH overview The balance system Vestibular disorders referrals Vestibular assessment
BAA regional meeting 11 th March 2016 Paediatric Balance Assessment Samantha Lear, Lead Clinical Scientist, Hearing Services, SCH overview The balance system Vestibular disorders referrals Vestibular assessment
Chapter 17, Part 2! The Special Senses! Hearing and Equilibrium!
 Chapter 17, Part 2! The Special Senses! Hearing and Equilibrium! SECTION 17-5! Equilibrium sensations originate within the inner ear, while hearing involves the detection and interpretation of sound waves!
Chapter 17, Part 2! The Special Senses! Hearing and Equilibrium! SECTION 17-5! Equilibrium sensations originate within the inner ear, while hearing involves the detection and interpretation of sound waves!
Chapter 17, Part 2! Chapter 17 Part 2 Special Senses! The Special Senses! Hearing and Equilibrium!
 Chapter 17, Part 2! The Special Senses! Hearing and Equilibrium! SECTION 17-5! Equilibrium sensations originate within the inner ear, while hearing involves the detection and interpretation of sound waves!
Chapter 17, Part 2! The Special Senses! Hearing and Equilibrium! SECTION 17-5! Equilibrium sensations originate within the inner ear, while hearing involves the detection and interpretation of sound waves!
Vestibular Function and Anatomy. UTMB Grand Rounds April 14, 2004 Gordon Shields, MD Arun Gadre, MD
 Vestibular Function and Anatomy UTMB Grand Rounds April 14, 2004 Gordon Shields, MD Arun Gadre, MD System of balance Membranous and bony labyrinth embedded in petrous bone 5 distinct end organs 3 semicircular
Vestibular Function and Anatomy UTMB Grand Rounds April 14, 2004 Gordon Shields, MD Arun Gadre, MD System of balance Membranous and bony labyrinth embedded in petrous bone 5 distinct end organs 3 semicircular
latest development in advanced testing the vestibular function
 latest development in advanced testing the vestibular function how to explore the vestibular function in detail Herman Kingma ENT Department Maastricht University Medical Centre The Netherlands how I do
latest development in advanced testing the vestibular function how to explore the vestibular function in detail Herman Kingma ENT Department Maastricht University Medical Centre The Netherlands how I do
Cerebellum. Steven McLoon Department of Neuroscience University of Minnesota
 Cerebellum Steven McLoon Department of Neuroscience University of Minnesota 1 Anatomy of the Cerebellum The cerebellum has approximately half of all the neurons in the central nervous system. The cerebellum
Cerebellum Steven McLoon Department of Neuroscience University of Minnesota 1 Anatomy of the Cerebellum The cerebellum has approximately half of all the neurons in the central nervous system. The cerebellum
Dizziness is a Health Concern. Vestibular Disorders and Rehabilitation. ReZlexes. ReZlex (cont.) Functions of Vestibular System. Dysfunction 2/24/13
 Functions of Vestibular System. Dysfunction 2/24/13") Vestibular Disorders and Rehabilitation Week 8: Dr. E Dizziness is a Health Concern From 2001-2004, 35.4% of US adults age 40 y/o and > had vestibular dysfunction. People with a measured vestibular dysfunction
Vestibular Disorders and Rehabilitation Week 8: Dr. E Dizziness is a Health Concern From 2001-2004, 35.4% of US adults age 40 y/o and > had vestibular dysfunction. People with a measured vestibular dysfunction
functiestoornissen van het evenwichtssysteem: een wereld van onbegrip
 functiestoornissen van het evenwichtssysteem: een wereld van onbegrip Herman Kingma, department of ORL, Maastricht University Medical Centre Maastricht Research Institute Mental Health and Neuroscience
functiestoornissen van het evenwichtssysteem: een wereld van onbegrip Herman Kingma, department of ORL, Maastricht University Medical Centre Maastricht Research Institute Mental Health and Neuroscience
Clinical aspects of vestibular and ocular motor physiology: bringing physiology and anatomy to the bedside. Skews Nystagmus Tilts
 Clinical aspects of vestibular and ocular motor physiology: bringing physiology and anatomy to the bedside Skews Nystagmus Tilts dzee@dizzy.med.jhu.edu Outline of the presentation Physiological principal
Clinical aspects of vestibular and ocular motor physiology: bringing physiology and anatomy to the bedside Skews Nystagmus Tilts dzee@dizzy.med.jhu.edu Outline of the presentation Physiological principal
Gathering information the sensory systems; Vision
 Visual System Gathering information the sensory systems; Vision The retina is the light-sensitive receptor layer at the back of the eye. - Light passes through the cornea, the aqueous chamber, the lens,
Visual System Gathering information the sensory systems; Vision The retina is the light-sensitive receptor layer at the back of the eye. - Light passes through the cornea, the aqueous chamber, the lens,
Balance Assessment and Rehabilitation in Audiology. Andy Phillips Director of Therapies and Health Science ABMU Health Board
 Balance Assessment and Rehabilitation in Audiology Andy Phillips Director of Therapies and Health Science ABMU Health Board Balance Mechanism This has 3 components -Sensory Input -Central Processing -Motor
Balance Assessment and Rehabilitation in Audiology Andy Phillips Director of Therapies and Health Science ABMU Health Board Balance Mechanism This has 3 components -Sensory Input -Central Processing -Motor
Evaluation & Management of Vestibular Disorders
 Evaluation & Management of Vestibular Disorders Richard A. Roberts, Ph.D., FAAA Alabama Hearing & Balance Associates, Inc. Disclosure and Copyright Statements Richard Roberts has no financial or nonfinancial
Evaluation & Management of Vestibular Disorders Richard A. Roberts, Ph.D., FAAA Alabama Hearing & Balance Associates, Inc. Disclosure and Copyright Statements Richard Roberts has no financial or nonfinancial
VESTIBULAR LABYRINTHS comprising of 3 semicircular canals, saccule, utricle VESTIBULAR NERVE with the sup. & inf. vestibular nerves VESTIBULAR
 VESTIBULAR LABYRINTHS comprising of 3 semicircular canals, saccule, utricle VESTIBULAR NERVE with the sup. & inf. vestibular nerves VESTIBULAR NUCLEUS BRAINSTEM CEREBELLUM VESTIBULAR CORTEX EYES SPINAL
VESTIBULAR LABYRINTHS comprising of 3 semicircular canals, saccule, utricle VESTIBULAR NERVE with the sup. & inf. vestibular nerves VESTIBULAR NUCLEUS BRAINSTEM CEREBELLUM VESTIBULAR CORTEX EYES SPINAL
UNIVERSITY OF JORDAN FACULTY OF MEDICINE DEPARTMENT OF PHYSIOLOGY & BIOCHEMISTRY NEUROPHYSIOLOGY (MEDICAL) Spring, 2014
 Spring, 2014") UNIVERSITY OF JORDAN FACULTY OF MEDICINE DEPARTMENT OF PHYSIOLOGY & BIOCHEMISTRY NEUROPHYSIOLOGY (MEDICAL) Spring, 2014 Textbook of Medical Physiology by: Guyton & Hall, 12 th edition 2011 Eman Al-Khateeb,
UNIVERSITY OF JORDAN FACULTY OF MEDICINE DEPARTMENT OF PHYSIOLOGY & BIOCHEMISTRY NEUROPHYSIOLOGY (MEDICAL) Spring, 2014 Textbook of Medical Physiology by: Guyton & Hall, 12 th edition 2011 Eman Al-Khateeb,
I: To describe the pyramidal and extrapyramidal tracts. II: To discuss the functions of the descending tracts.
 Descending Tracts I: To describe the pyramidal and extrapyramidal tracts. II: To discuss the functions of the descending tracts. III: To define the upper and the lower motor neurons. 1. The corticonuclear
Descending Tracts I: To describe the pyramidal and extrapyramidal tracts. II: To discuss the functions of the descending tracts. III: To define the upper and the lower motor neurons. 1. The corticonuclear
The Nervous System: Sensory and Motor Tracts of the Spinal Cord
 15 The Nervous System: Sensory and Motor Tracts of the Spinal Cord PowerPoint Lecture Presentations prepared by Steven Bassett Southeast Community College Lincoln, Nebraska Introduction Millions of sensory
15 The Nervous System: Sensory and Motor Tracts of the Spinal Cord PowerPoint Lecture Presentations prepared by Steven Bassett Southeast Community College Lincoln, Nebraska Introduction Millions of sensory
Taste buds Gustatory cells extend taste hairs through a narrow taste pore
 The Special Senses Objectives Describe the sensory organs of smell, and olfaction. Identify the accessory and internal structures of the eye, and explain their function. Explain how light stimulates the
The Special Senses Objectives Describe the sensory organs of smell, and olfaction. Identify the accessory and internal structures of the eye, and explain their function. Explain how light stimulates the
3) Approach to Ataxia - Dr. Zana
 Approach to Ataxia - Dr. Zana") 3) Approach to Ataxia - Dr. Zana Introduction Ataxia is derived from Greek word a -not, taxis -orderly, (not orderly/ not in order) Ataxia is the inability to make smooth, accurate and coordinated movements
3) Approach to Ataxia - Dr. Zana Introduction Ataxia is derived from Greek word a -not, taxis -orderly, (not orderly/ not in order) Ataxia is the inability to make smooth, accurate and coordinated movements
International Journal of Medical and Exercise Science (Multidisciplinary, Peer Reviewed and Indexed Journal)
") ORIGINAL ARTICLE International Journal of Medical and Exercise Science (Multidisciplinary, Peer Reviewed and Indexed Journal) PHYSICAL THERAPY MANAGEMENT IN PATIENTS WITH CERVICOGENIC DIZZINESS-A CASE
ORIGINAL ARTICLE International Journal of Medical and Exercise Science (Multidisciplinary, Peer Reviewed and Indexed Journal) PHYSICAL THERAPY MANAGEMENT IN PATIENTS WITH CERVICOGENIC DIZZINESS-A CASE
Vertigo. Tunde Magyar MD, PhD
 Vertigo Tunde Magyar MD, PhD What could be reffered to as dizziness by the patient? Rotational vertigo Sense of instability Ataxia of gait Disturbance of vision Loss of contact with surroundings Nausea
Vertigo Tunde Magyar MD, PhD What could be reffered to as dizziness by the patient? Rotational vertigo Sense of instability Ataxia of gait Disturbance of vision Loss of contact with surroundings Nausea
VESTIBULAR FUNCTION TESTING
 VESTIBULAR FUNCTION TESTING Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices
VESTIBULAR FUNCTION TESTING Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices
Because dizziness is an imprecise term, a major role of the clinician is to sort patients out into categories
 Dizziness and Imbalance Timothy C. Hain, MD Clinical Professor of Neurology, Otolaryngology, Physical Therapy Chicago Dizziness and Hearing 645 N. Michigan, Suite 410 312-274-0197 Lecture Goals 1. What
Dizziness and Imbalance Timothy C. Hain, MD Clinical Professor of Neurology, Otolaryngology, Physical Therapy Chicago Dizziness and Hearing 645 N. Michigan, Suite 410 312-274-0197 Lecture Goals 1. What
CNS MCQ 2 nd term. Select the best answer:
 Select the best answer: CNS MCQ 2 nd term 1) Vestibular apparatus: a) Represent the auditory part of the labyrinth. b) May help in initiating the voluntary movements. c) Contains receptors concerned with
Select the best answer: CNS MCQ 2 nd term 1) Vestibular apparatus: a) Represent the auditory part of the labyrinth. b) May help in initiating the voluntary movements. c) Contains receptors concerned with
Katrina Williams 2017 Specialist Neurological Physiotherapist FACP
 Your stroke patient is dizzy challenges of assessment and treatment. Katrina Williams Specialist Neurological Physiotherapist FACP 2008 Clinical Academic University of Queensland Senior Neurological Ageing
Your stroke patient is dizzy challenges of assessment and treatment. Katrina Williams Specialist Neurological Physiotherapist FACP 2008 Clinical Academic University of Queensland Senior Neurological Ageing
Acute Vestibular Syndrome (VS or Stroke?) Three-step H.I.N.T.S. eye examination
 Three-step H.I.N.T.S. eye examination") Acute Vestibular Syndrome (VS or Stroke?) Three-step H.I.N.T.S. eye examination Head Impulse (right- and leftward) Nystagmus type Test of Skew (cover test for skew deviation) Stroke findings: I.N.F.A.R.C.T.
Acute Vestibular Syndrome (VS or Stroke?) Three-step H.I.N.T.S. eye examination Head Impulse (right- and leftward) Nystagmus type Test of Skew (cover test for skew deviation) Stroke findings: I.N.F.A.R.C.T.
What could be reffered to as dizziness by the patient?
 What could be reffered to as dizziness by the patient? Rotational vertigo Sense of instability Ataxia of gait Disturbance of vision Loss of contact with surroundings Nausea Loss of memory Loss of confidence
What could be reffered to as dizziness by the patient? Rotational vertigo Sense of instability Ataxia of gait Disturbance of vision Loss of contact with surroundings Nausea Loss of memory Loss of confidence
COGS 107B Week 2. Hyun Ji Friday 4:00-4:50pm
 COGS 107B Week 2 Hyun Ji Friday 4:00-4:50pm Lecture 3: Proprioception Principles: The Neuron Doctrine and The Law of Dynamic Polarization Proprioception Joint-protecting reflexes (ex. Knee jerk reflex)
COGS 107B Week 2 Hyun Ji Friday 4:00-4:50pm Lecture 3: Proprioception Principles: The Neuron Doctrine and The Law of Dynamic Polarization Proprioception Joint-protecting reflexes (ex. Knee jerk reflex)
Video Head Impulse Testing
 Authored by: David J. Coffin, Au.D. e3 Gordon Stowe Chicago Chicago, Illinois The video Head Impulse Test (vhit) is a relatively new test that provides diagnostic and functional information about the vestibular
Authored by: David J. Coffin, Au.D. e3 Gordon Stowe Chicago Chicago, Illinois The video Head Impulse Test (vhit) is a relatively new test that provides diagnostic and functional information about the vestibular
Structure-Function: Central vestibular syndromes
 Structure-Function: Central vestibular syndromes Skews Nystagmus Tilts dzee@dizzy.med.jhu.edu Objectives An introduction to the basic principles of eye movement control An introduction to the types of
Structure-Function: Central vestibular syndromes Skews Nystagmus Tilts dzee@dizzy.med.jhu.edu Objectives An introduction to the basic principles of eye movement control An introduction to the types of
VERTIGO. Tuesday 20 th February 2018 Dr Rukhsana Hussain. Disclaimers apply:
 VERTIGO Tuesday 20 th February 2018 Dr Rukhsana Hussain WHAT IS VERTIGO? 4 Vertigo is defined as an illusory sensation of motion of either the self or the surroundings in the absence of true motion. Explaining
VERTIGO Tuesday 20 th February 2018 Dr Rukhsana Hussain WHAT IS VERTIGO? 4 Vertigo is defined as an illusory sensation of motion of either the self or the surroundings in the absence of true motion. Explaining
Abducens nucleus (VI) Baclofen, nystagmus treatment 202, 203,
 Baclofen, nystagmus treatment 202, 203,") ... Abducens nucleus (VI) Baclofen, nystagmus treatment 202, 203, afferent and efferent connections 10 205, 206, 209, 212, 220 structure and function 9, 10 Benign paroxysmal positioning vertigo transmitters
... Abducens nucleus (VI) Baclofen, nystagmus treatment 202, 203, afferent and efferent connections 10 205, 206, 209, 212, 220 structure and function 9, 10 Benign paroxysmal positioning vertigo transmitters
b. The groove between the two crests is called 2. The neural folds move toward each other & the fuse to create a
 Chapter 13: Brain and Cranial Nerves I. Development of the CNS A. The CNS begins as a flat plate called the B. The process proceeds as: 1. The lateral sides of the become elevated as waves called a. The
Chapter 13: Brain and Cranial Nerves I. Development of the CNS A. The CNS begins as a flat plate called the B. The process proceeds as: 1. The lateral sides of the become elevated as waves called a. The
Afternystagmus and Headshaking Nystagmus. David S. Zee
 442 `447, 1993 Afternystagmus and Headshaking Nystagmus David S. Zee Departments of Neurology, Ophthalmology and Otolaryngology The Johns Hopkins University School of Medicine Recent advances in vestibular
442 `447, 1993 Afternystagmus and Headshaking Nystagmus David S. Zee Departments of Neurology, Ophthalmology and Otolaryngology The Johns Hopkins University School of Medicine Recent advances in vestibular
Vestibular testing: what patients can expect
 American Hearing Research Foundation Symposium on Dizziness & Balance Disorders April 6, 2013 Vestibular testing: what patients can expect Marcello Cherchi, MD PhD Assistant Professor of Neurology Northwestern
American Hearing Research Foundation Symposium on Dizziness & Balance Disorders April 6, 2013 Vestibular testing: what patients can expect Marcello Cherchi, MD PhD Assistant Professor of Neurology Northwestern
I m dizzy-what can I expect at my doctor visit? Dennis M. Moore, M.D. Lutheral General
 I m dizzy-what can I expect at my doctor visit? Dennis M. Moore, M.D. Lutheral General Dizziness and Balance is a broad area encompassing multiple fields: primary care (internal medicine, pediatrics),
I m dizzy-what can I expect at my doctor visit? Dennis M. Moore, M.D. Lutheral General Dizziness and Balance is a broad area encompassing multiple fields: primary care (internal medicine, pediatrics),
 Spinal Cord Tracts DESCENDING SPINAL TRACTS: Are concerned with somatic motor function, modification of ms. tone, visceral innervation, segmental reflexes. Main tracts arise form cerebral cortex and others
Spinal Cord Tracts DESCENDING SPINAL TRACTS: Are concerned with somatic motor function, modification of ms. tone, visceral innervation, segmental reflexes. Main tracts arise form cerebral cortex and others
Benign Paroxysmal Positional Vertigo
 Benign Paroxysmal Positional Vertigo Information for patients and families Read this booklet to learn about: What Benign Paroxysmal Positional Vertigo (BPPV) is Symptoms How your doctor will diagnose it
Benign Paroxysmal Positional Vertigo Information for patients and families Read this booklet to learn about: What Benign Paroxysmal Positional Vertigo (BPPV) is Symptoms How your doctor will diagnose it
Motor tracts Both pyramidal tracts and extrapyramidal both starts from cortex: Area 4 Area 6 Area 312 Pyramidal: mainly from area 4 Extrapyramidal:
 Motor tracts Both pyramidal tracts and extrapyramidal both starts from cortex: Area 4 Area 6 Area 312 Pyramidal: mainly from area 4 Extrapyramidal: mainly from area 6 area 6 Premotorarea: uses external
Motor tracts Both pyramidal tracts and extrapyramidal both starts from cortex: Area 4 Area 6 Area 312 Pyramidal: mainly from area 4 Extrapyramidal: mainly from area 6 area 6 Premotorarea: uses external
Vertigo. David Clark, DO Oregon Neurology Associates Springfield, OR
 Vertigo David Clark, DO Oregon Neurology Associates Springfield, OR 44F vertigo, nausea & vomiting Unidirectional Nystagmus 44F vertigo, nausea & vomiting Impaired VOR Gain to the right Vertigo History
Vertigo David Clark, DO Oregon Neurology Associates Springfield, OR 44F vertigo, nausea & vomiting Unidirectional Nystagmus 44F vertigo, nausea & vomiting Impaired VOR Gain to the right Vertigo History
By Dr. Saeed Vohra & Dr. Sanaa Alshaarawy
 By Dr. Saeed Vohra & Dr. Sanaa Alshaarawy 1 By the end of the lecture, students will be able to : Distinguish the internal structure of the components of the brain stem in different levels and the specific
By Dr. Saeed Vohra & Dr. Sanaa Alshaarawy 1 By the end of the lecture, students will be able to : Distinguish the internal structure of the components of the brain stem in different levels and the specific
Basal nuclei, cerebellum and movement
 Basal nuclei, cerebellum and movement MSTN121 - Neurophysiology Session 9 Department of Myotherapy Basal Nuclei (Ganglia) Basal Nuclei (Ganglia) Role: Predict the effects of various actions, then make
Basal nuclei, cerebellum and movement MSTN121 - Neurophysiology Session 9 Department of Myotherapy Basal Nuclei (Ganglia) Basal Nuclei (Ganglia) Role: Predict the effects of various actions, then make
This article describes the clinically relevant anatomic components
 3 CE Credits Vestibular Disease: Anatomy, Physiology, and Clinical Signs Mark Lowrie, MA VetMB, MVM, DECVN, MRCVS Davies Veterinary Specialists Higham Gobion, Hertfordshire United Kingdom Abstract: The
3 CE Credits Vestibular Disease: Anatomy, Physiology, and Clinical Signs Mark Lowrie, MA VetMB, MVM, DECVN, MRCVS Davies Veterinary Specialists Higham Gobion, Hertfordshire United Kingdom Abstract: The
Quick Guides Vestibular Diagnosis and Treatment:
 VNG - Balance Testing Quick Guides Vestibular Diagnosis and Treatment: Utilizing Videonystagmography (VNG) Spontaneous Nystagmus Gaze Test Smooth Pursuit Tracking Saccade Test Optokinetics (OKN) Dix-Hallpike
VNG - Balance Testing Quick Guides Vestibular Diagnosis and Treatment: Utilizing Videonystagmography (VNG) Spontaneous Nystagmus Gaze Test Smooth Pursuit Tracking Saccade Test Optokinetics (OKN) Dix-Hallpike
Νευροφυσιολογία και Αισθήσεις
 Biomedical Imaging & Applied Optics University of Cyprus Νευροφυσιολογία και Αισθήσεις Διάλεξη 11 Ακουστικό και Αιθουσιαίο Σύστημα (Auditory and Vestibular Systems) Introduction Sensory Systems Sense of
Biomedical Imaging & Applied Optics University of Cyprus Νευροφυσιολογία και Αισθήσεις Διάλεξη 11 Ακουστικό και Αιθουσιαίο Σύστημα (Auditory and Vestibular Systems) Introduction Sensory Systems Sense of
Cervical Spine Exercise and Manual Therapy for the Autonomous Practitioner
 Cervical Spine Exercise and Manual Therapy for the Autonomous Practitioner Eric Chaconas PT, PhD, DPT, FAAOMPT Assistant Professor and Assistant Program Director Doctor of Physical Therapy Program Eric
Cervical Spine Exercise and Manual Therapy for the Autonomous Practitioner Eric Chaconas PT, PhD, DPT, FAAOMPT Assistant Professor and Assistant Program Director Doctor of Physical Therapy Program Eric
An Introduction to Dizziness and Vertigo
 An Introduction to Dizziness and Vertigo Tamara Mijovic MD CM FRCSC Clinical Assistant Professor Department of Otolaryngology Head and Neck Surgery Otology, Neurotology & Skull Base Surgery McGill University
An Introduction to Dizziness and Vertigo Tamara Mijovic MD CM FRCSC Clinical Assistant Professor Department of Otolaryngology Head and Neck Surgery Otology, Neurotology & Skull Base Surgery McGill University