Professor Richard Gearry
|
|
|
- Pearl McCarthy
- 5 years ago
- Views:
Transcription

1 Professor Richard Gearry Consultant Gastroenterologist Christchurch Hospital, Professor of Medicine, University of Otago, Christchurch 8:30-9:25 WS #140: A Revolution in Reflux: Tackling the Therapeutic Gap 9:35-10:30 WS #150: A Revolution in Reflux: Tackling the Therapeutic Gap (Repeated)


2 A revolution in reflux Tackling the therapeutic gap Richard Gearry Professor of Medicine, University of Otago, Christchurch Gastroenterologist, CDHB Gastroenterologist, Gastroenterology and Endoscopy Specialists
3 Workshop tools Quiz Case Lecture Questions Discussion


4 Key Message Slides If it was a late night last night and an early start this morning, feel free to let what I have to say drift over you.. I will let you know when we get to the key messages on these slides
5 Why have I been asked to run this Gastroenterologist (CDHB) workshop? Gastroenterologist (GAES) Professor of Medicine (UOC)

6
7 Gastroenterology consultation Endoscopy and colonoscopy Capsule endoscopy Dietitians Breath testing for carbohydrate malabsorption 24 hour ambulatory oesophageal ph and impedence monitoring
8 Quiz 1 How common is reflux? Why might GORD be becoming more common? What are the two classic reflux symptoms? What are UGI alarm symptoms? Name 5 extra-oesophageal symptoms of reflux
9 What is GORD? a condition which develops when the reflux of stomach contents causes troublesome symptoms and/or complications Montreal definition
10 Epidemiology of reflux symptoms / GORD Reflux symptom prevalence Europe / North America 11-28% Asia 2-5% Australia 11.6% Erosive oesophagitis prevalence (endoscopy) 15.5% (Sweden) 37% of these had no GORS 11.8% (Italy) 6% (China) 12% of those with GORS
11 Rising rates of reflux 50% increase in GORD prevalence in studies pre / post 1995 Barrett s oesophagus incidence is increasing Oesophageal adenocarcinoma one of the most rapidly increasing cancers

12 Rising rates of reflux
13 Rising rates of oesophageal cancer
14 Why more reflux? More obesity (especially central) Less Helicobacter pylori infection More GORD in infants / children???
15 Typical reflux syndrome Heartburn translates poorly ~50% will have a positive ph study overlap with functional dyspepsia Regurgitation
16 Upper GI alarm symptoms Dysphagia / odynophagia Unexplained weight loss Unexplained iron deficiency anaemia Haematemesis or melaena Abdominal mass Persistent / protracted vomiting New / worsening symptoms >50 years age
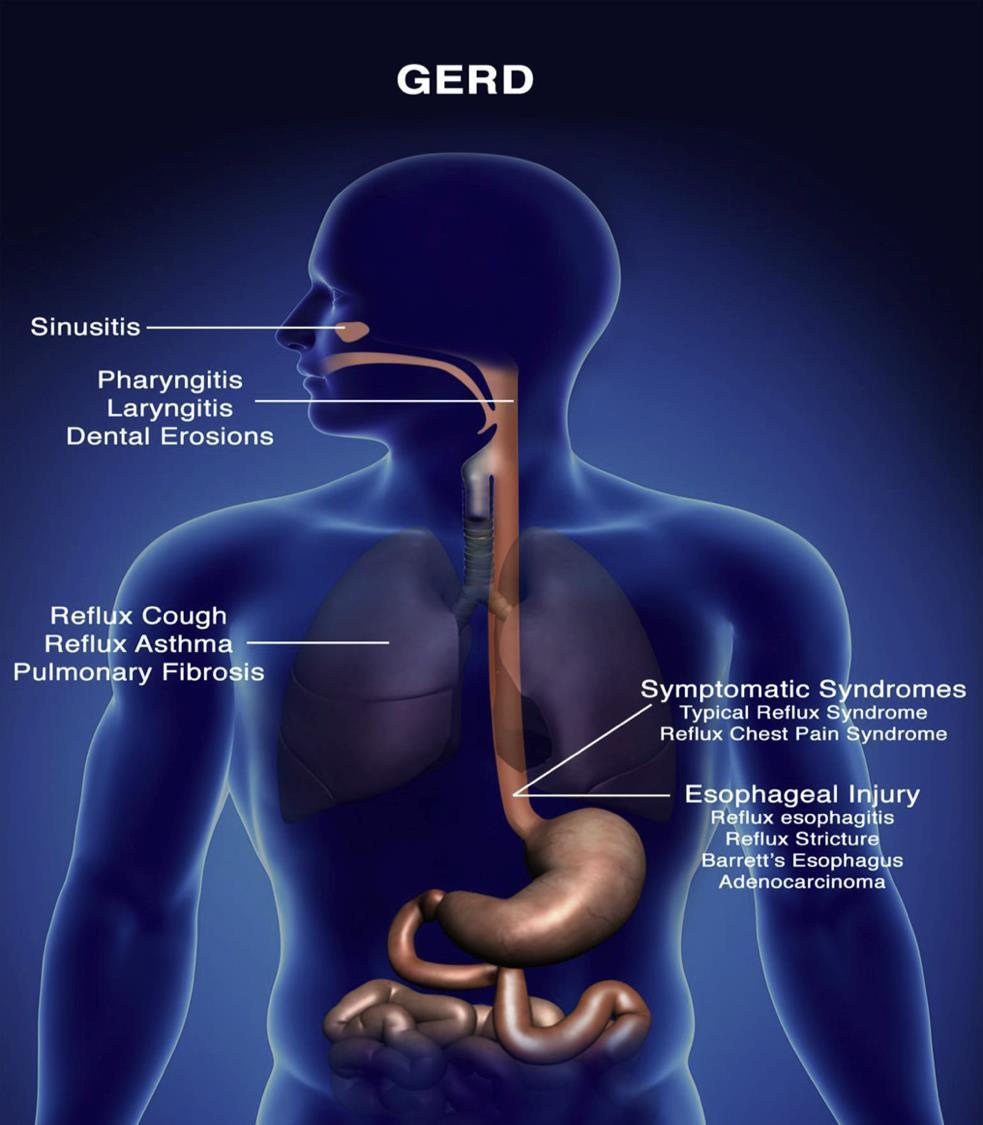
17 Extra-oesophageal symptoms 1/3 patients with GORD may have extraoesophageal symptoms (EOS) Extra-oesophageal symptom Prevalence (%) Chest pain 14.5% Chronic cough 13% Laryngeal disorders 10.4% Asthma 4.8% Dental erosions 20% Many patients with EOS do not have typical GORD symptoms

18 GORD - a common cause of chronic cough

19 Asthma and GORD
20 Symptoms associated with GORD-laryngitis Hoarseness Dysphonia Sore / burning throat Excessive throat clearing Chronic cough Globus Apnoea Laryngospasm Dysphagia Post-nasal drip Neoplasm
21



22 Remember dyspepsia is not GORD Dyspepsia post prandial fullness bloating Belching early satiety anorexia nausea Episodic Recurrent Chronic Most people with dyspepsia do not have underlying pathology, may not seek medical attention and will not require investigation




23 Key messages There is a lot of GORD out there think carefully about how patients present Typical GORD symptoms Atypical GORD symptoms Extra-oesophageal symptoms Alarm symptoms Heartburn and regurgitation Cough, laryngitis, asthma, dental erosions Dysphagia, wt loss, GI bleeding, abdo mass, ongoing vomiting, age > 50 years
24 Case 1 54 year old Caucasian male BMI 30, smoker, moderate alcohol Complains of 6 years of increasing Acid regurgitation / heartburn Nocturnal cough antacid use most days What are the issues to deal with?
25
26 Quiz 2 What is the underlying pathogenesis of GORD? What is (a) NERD? Are hiatus hernias important in reflux? How common are functional disorders of the upper GI tract?
27 How does reflux cause symptoms? Everyone refluxes, some people have symptoms Discrepancy between acid exposure / symptoms Mechanical factors Altered oesophageal sensitivity
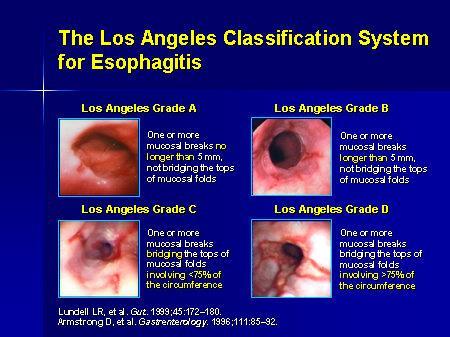
28 Sub-types of reflux How to classify reflux? Endoscopy oesophagitis (LA classification) Normal NERD (non-erosive reflux disease) Hypersensitive oesophagus Functional heartburn 24H ph study / 24 hour ph-impedance study number of episodes or duration of exposure

29 24 hour oesophageal ph study
30 Characteristics of GORS subtypes Reflux oesophagitis Non-erpsove reflux disease (NERD) Hypersensitive oesophagus Functional Heartburn Endoscopy ph study ph/impedance PPI response Oesophagitis Positive off PPI Positive on or off PPI Normal (possible subtle signs on biopsy) Normal Sometimes positive Normal acid exposure but clear association of symptoms with reflux events Always positive Normal acid exposure but clear association of symptoms with reflux events Good Variable Variable Normal Negative Negative Negative
31 Functional oesophageal disease Functional chest pain Functional heart burn Reflux hypersensitivity Globus Functional dysphagia
32 Functional heartburn 6 months of symptoms with criteria fulfilled for the last 3 months Frequency of >2X/week with all of: burning retrosternal discomfort or pain no symptom relief with optimal PPI normal ph / impedance study, no EosOes absence of oesophageal motor disorders
33 Interaction between refluxate and oesophageal sensitivity


34 How does reflux cause symptoms? Oesophageal characteristics / hypersensitivity Peripheral sensitization Central sensitization Mucosal barrier function Reflux characteristics Acidity Duodenogastric-oesophageal reflux / pepsin Gas reflux Proximal extent Sustained oesophageal contractions Psychological factors Genetic factors
35 Pathogenesis of GORD

36 How to diagnose GORD?


37 Eosinophilic oesophagitis Typically.. Young males History of atopy / asthma Recurrent dysphagia / food bolus obtruction
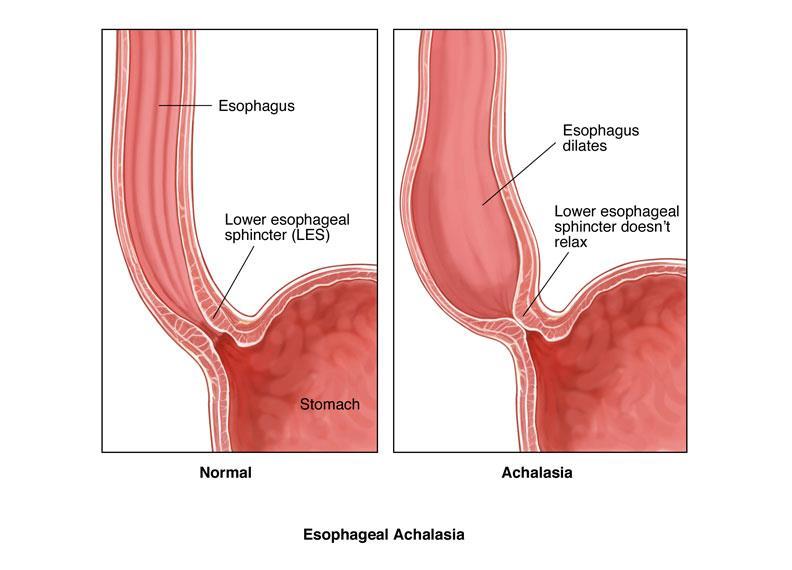
38 Achalasia
39 Case 26 year old woman 12 months of intermittent regurgitation and heartburn, atypical chest pains Normal gastroscopy no evidence of reflux oesophagitis Partial response to PPI Where to from here?
40 Key Messages Most people who reflux will not have erosive oesophagitis NERD / functional heartburn comprise most patients The pathogenesis of GORD is complex multiple targets for therapy Eosinophilic oesophagitis is also becoming more common
41
42 Quiz 3 How do we diagnose GORD What investigations are required for GORD? Which is the most useful test for GORD
43 Investigation-based testing of GORD Endoscopy 24 hour ph / impedance study The PPI test
44 Endoscopy In primary care 50% of patients with GORD symptoms have a normal endoscopy Expensive and invasive
45 What is the role of endoscopy in GORD management? Eosophageal symptoms unresponsive to PPI make a positive diagnosis of / rule out GORD diagnose / rule out another oesophageal condition Extra-oesophageal symptoms diagnosing or ruling out GORD Prolonged GORD / alarm features diagnose / rule out GORD injury syndromes stricture, erosions, Barrett s, adenocarcinoma

46 ph testing
47 ph / impedance testing
48 Case 45 year old male Typical reflux symptoms Controlled with prn PPI Now a change in symptoms atypical pain cough despite PPI Where to from here?
49
50 Quiz What lifestyle modifications are effective for GORD? What drugs make GORD worse? Why do H2RAs not work as well as PPIs? Which PPI is most likely to interact with other drugs?
51 Management of reflux-related symptoms Goals of therapy: symptom relief heal the oesophagus prevent long-term complications Barrett s, stricture, adenocarcimona Induction and then maintenance of symptom control
52 What are the targets of therapy? GORD has multiple aetiologies lower oesophageal sphincter dysfunction Noxious refluxate causes most symptoms Primary target is making refluxate less noxious PPI therapy Other targets enhancing oesophageal clearance promoting gastric emptying providing mucosal protection decreasing tissue hypersensitivity
53 Lifestyle modifications LOS pressure oesophageal ph Smoking Coffee Chocolate Alcohol Carbonated beverages Fatty food Right lateral decubitus Modification leads to GORD symptoms Elevating head of the bed Targeted weight loss Abdominal breathing
54 Review of drugs associated with GORD NSAIDs steroids calcium channel antagonists nitrates theophyllines bisphosphonates
55 Medical management of GORD Acid suppression TLOSR inhibitors Increasing oesophageal clearance Improving visceral hypersensitivity Mucosal protection Mucosal healing
56 Acid suppression Antacids H2 receptor antagonists Proton pump inhibitors

57 Antacids Aluminium hydroxide Magnesium hydroxide Sodium bicarbonate Calcium containing compounds Simeticone Alginate / raft-forming compounds Rapid No role in healing Mild or breakthough symptoms Other GI side effects Recent study of NERD patients PPI+alginate better than PPI alone (57% v 27%, p<0.005)
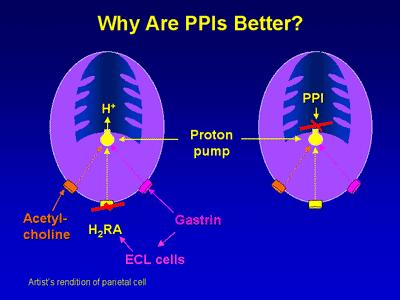
58 H2 Receptor Antagonists Cimetidine Famotidine Ranitidine Better for GI-II (80%) than III-IV (30-50%) oesophagitis Safe and cheap but ADRs, tachyphylaxis, interactions Effective in addition to PPI for nocturnal reflux
59
60 Proton Pump Inhibitors Most effective class for acid suppression Cornerstone of GORD therapy Symptom relief Mucosal healing Prevent long-term complications
61 PPIs available in NZ Omeprazole Pantoprazole Lansoprazole Formulation 20 / 40mg caps 20 / 40mg caps 15 / 30 mg caps Bioavailability Variable Constant Constant Food effect on absorption Cytochrome P450 metabolism Drug interactions Minimal Minimal Delayed absorption Mostly 2C19 Low P450 affinity Lower P450 affinity Phenytoin, warfarin, carbemazepine, diazepam No p450 interactions Minimal P450 interactions
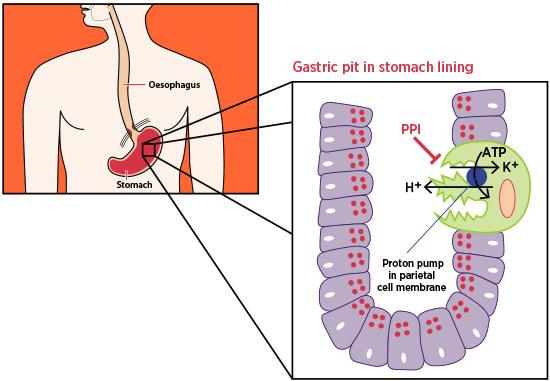
62 PPI fast facts Irreversibly binds H/K ATPase on parietal cell Pro-drugs activated in secretory canaliculus All are enteric coated (acid labile) Short half life hours Maximal acid suppression >5 days Acid suppression optimised when PPI taken with mealstimulated acid secretion
63 PPI /Reflux fast facts Oesophagitis efficacy is associated with longer gastric ph double dose PPI has an additive effect all Grade B/C patients relapse on PPI cessation NERD PPI is superior to H2RA and prokinetic 2/3 of NERD patients relapse on PPI cessation intermittent PPI may be as good as continuous PPI Barrett s oesophagus PPIs reduce the risk of dysplasia
64 Timing of PPIs Acid suppression optimised when PPI taken with meal-stimulated acid secretion Best consumed minutes before the first meal of the day Recommended by only 30% of physicians Adhered to by <10% of patients
65
66
67 Transient Lower Oesophageal Sphincter Relaxation Inhibitors Persistent reflux despite PPI is a big problem 16% GORD patients on BD PPI >50% GORD patients have reflux symptoms on PPI Baclofen 60% reduction in TLOSRs increases basal LOS pressure reduces acid, weak acid and bile reflux Poorly tolerated, multiple dosing (5-20mg tds)
68 Improving oesophageal clearance Prokinetics inferior to PPI as monotherapy given with PPI in those with gastric dysmotility Macrolides erythromycin and azithromycin have shown efficacy physiologically and clinically for those with GORD
69 Reducing visceral hypersensitivity Some efficacy for antidepressants in reducing visceral pain and hypersensitivity
70 Pain modulation in functional oesophageal disorders
71 Mucosal protection Sucralfate binds to inflamed mucosa and reduces acid exposure and promotes healing in oesophagitis Heals mild erosive oesophagitis and NERD Multiple dosing Safe in pregnancy
72 Case 34 year old woman heartburn for 5 years intermittently Normal gastroscopy Normal 24 hour ph study responds partially to PPI Where to from here?
73 Key Messages Weight loss and raising the head of the bed are the most useful lifestyle factors to improve reflux symptoms PPIs are the most effective therapy for ERD / NERD Other drugs work well in combination with PPI nocturnal H2RA, baclofen, alginate antacids Consider baclofen / anti-depressants
74
75 Quiz Which of the following does not come up on google searches of PPI adverse reactions: Pneumonia Hypomagnesaemia myocardial ischaemia Enteric infections iron deficiency Psychosis
76
77 PPI Adverse Effects Overall, PPIs are exceptionally well tolerated Common headache, diarrhoea, rash, nausea, constipation Less common but more worrying
78 Risk of fracture Possible mechanisms reduction of Ca absorption??? impairment of osteoclast activity??? Four retrospective association studies OR 1.18 [ ] 1.6 [ ] Two case-control studies No independent risk of hip fracture
79 Risk of fracture Meta-analysis of 10 observational studies (>200,000 #) overall poor quality and high heterogeneity Hip # OR 1.2 [ ] Vertebral # OR 1.5 [ ] Wrist / forearm # OR 1.1 [ ] Prospective BMD studies mixed results Concern for fracture and osteoporosis should not prevent otherwise indicated long-term PPI therapy
80 Hypomagnesaemia Mg cofactor in >300 enzymatic reactions Early signs Anorexia, nausea, fatigue, weakness Late signs tremor, agitation, fasciculation, arrhythmia, depression, seizures (often with Ca / K) First reported with PPIs 2006 likely secondary to reduced absorption Often other causes for low Mg
81 Hypomagnesaemia Rotterdam study of ~10,000 with serum [Mg] 36 cases of Mg + PPI exposed 2X increased risk of Mg with PPI 7X increased risk with PPI + loop diuretic Italian study of patients with admission for Mg 2X more likely to be on a PPI 3X more likely to have diabetes, 20X more likely to have chronic diarrhoea
82 B12 Deficiency In diet, B12 is protein bound and requires acid-activated proteolytic digestion However studies have not been conclusive positive studies are small and non-controlled The quality of available evidence does not justify routine B12 measurement in all patients receiving long-term PPI
83 Fe deficiency Gastric acid facilitates absorption of non-haem fe to more soluble ferrous form Odd case report etc Routine screening cannot be recommended
84 Enteric infections Gastric ph<4 is a major defense mechanism Gastric ph>4 allow 50% of bacteria to escape acid altered gastric and small intestinal flora Multiple retrospective cohort / C-C studies Salmonalla, Campylobacter jejuni, C difficile Salmonella 2X CC studies adjusted RR 4-8 C jejuni 4X CC studies adjusted RR 4-11 Clostrium difficile
85 Clostrium difficile Two large meta-analyses (similar results) CC, 6-12 cohort studies (~300K subjects) RR of CDI in PPI-treated patients 1.69 [ ] No duration of treatment data 15 studies suggested a reduced rate of CDI in H2RAtreated patients (RR 0.71 [ ])
86 Enteric infections PPIs may be risk factor for CDI weak association observational studies (low quality, unmeasured confounders and co-morbidity) Awareness of this association, particularly in hospitalised elderly patients
87 Pneumonia Gastric ph<4 increases pathogens in UGI tract? possible micro-aspiration Initial CC studies suggested RR Nested CC study significant confounders If there is an effect, it appears to be early effect lessens with time Biologically plausible association but not strong and significant confounding
88 Fig 2. Summary Forest Plot of Overall Risk of Community-Acquired Pneumonia with Outpatient Proton Pump Inhibitor Use, subdivided by study design and effect estimate. Lambert AA, Lam JO, Paik JJ, Ugarte-Gil C, Drummond MB, et al. (2015) Risk of Community-Acquired Pneumonia with Outpatient Proton-Pump Inhibitor Therapy: A Systematic Review and Meta-Analysis. PLoS ONE 10(6): e doi: /journal.pone
89 Acid rebound PPI >8 weeks acid secretion (temporarily) Affects ~50% of those stopping PPI healthy volunteers more likely in H pylori negative patients smaller studies of GORD patients on PPI - no effect Possible explanation for long term PPI use
90 Cancer Long term PPIs increase gastrin gastrin has a trophic effect on gut epithelium Gastric fundic gland polyps increased risk but no clinical significance Gastric cancer?h pylori increased risk eradicate first Gastric carcinoids?h pylori increased risk eradicate first Colorectal cancer no effect in large CC studies
91 Safety in Pregnancy Acid-related symptoms - common in pregnancy Meta-analysis (7 CC studies, 1500 women, T1) Major malformations OR1.29 [ ] Danish nation-wide registry study 5082 cases from 840,000 births no effect
92 Mortality Large UK study (18,000 patients on PPI) First year mortality, OR=1.4 [ ], then no risk marked confounding Mixed results from smaller studies mostly of elderly / long term facility residents
93 Case A 89 year old woman on a wide range of drugs including PPI, frusemide and B-Blocker presents with lethargy Where to from here?
94 Key Messages The risks of long-term PPI ADRs are small in comparison to a good indication for PPI The elderly are most likely to be affected by long-term PPI ADRs but are also most likely to have the poorest indications for PPI PPIs are the drug class most likely to be questioned by patients regarding ADRs
95
96 Quiz How long should patients with erosive oesophagitis remain on PPI? Why might we not perform surveillance for patients with Barrett s oesophagus? What are the risk factors for Barrett s oesophagus?
97 Complications of GORD Erosive oesophagitis Peptic strictures Barrett s oesophagus Adenocarcinoma


98 Erosive oesophagitis Population-based study 2/3 of those with reflux symptoms have no erosive oesophagitis 1/3 of those with oesophagitis had reflux Treatment with PPI higher grades heal at lower rates NERD Asymptomatic EO group
99
100 Peptic strictures Secondary to healing and fibrosis Dilatation is standard therapy Savary bougie TTS balloon

101 Savary dilator

102 TTS Ballon dilatation

103 TTS balloon dilatation
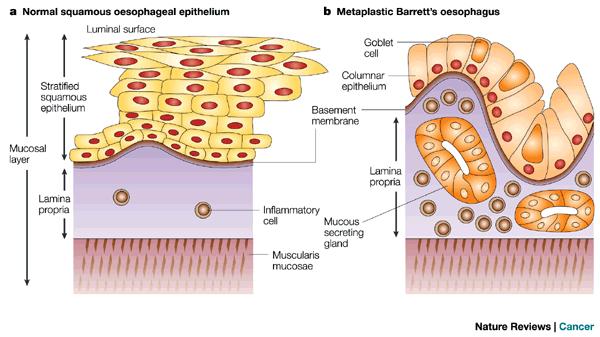
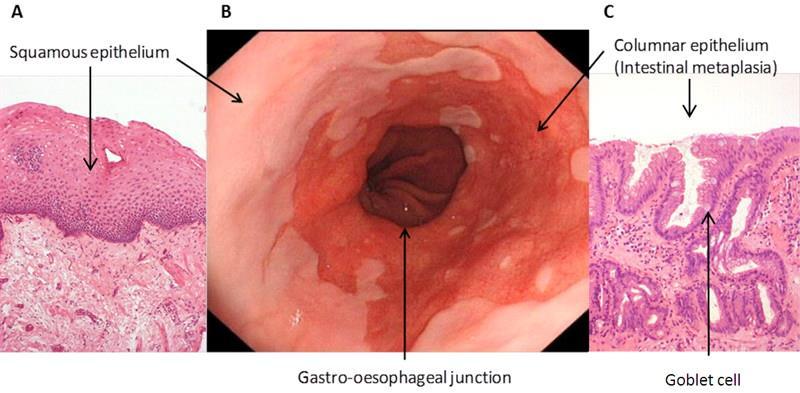
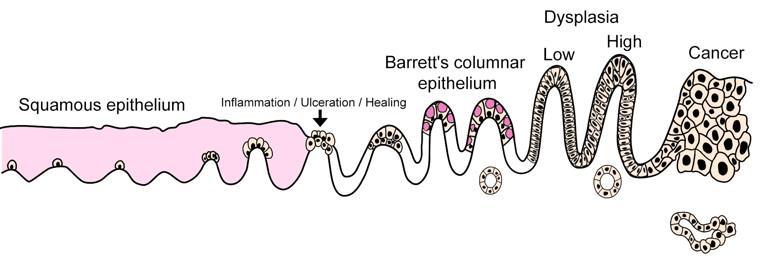
104 Barrett s oesophagus Pre-malignant condition Oesophageal squamous epithelium undergoes columnar change with metaplasia Prevalence?1.6% Rapidly increasing incidence
105 Barrett s oesophagus
106 Barrett s oesophagus
107 Barrett s oesophagus
108 Risk factors for Barrett s oesophagus GORD (EO associated with BE, OR 5.2 [1.2-23]) Hiatus hernia Smoking Central obesity / overweight White race Males Age >50 years Genetic factors
109 Barrett s oesophagus Usually found at endoscopy for those under-going evaluation for UGI symptoms? screening GORD symptoms and > 2 risk factors lower threshold for those with FHx

110 Interaction between refluxate and oesophageal sensitivity
111 How do we manage Barrett s oesophagus? Symptom control of GORD / healing Endoscopic surveillance for dysplasia / adenoca in the right groups Consideration of endoscopic / surgical treatment for those with dysplasia
112 Symptom control of GORD PPI probably at higher doses NSAIDs, aspirin and statins all risk of BE and progression of BE to dysplasia observational studies Surgery and medical therapy are equally effective in patients with BE
113 Endoscopic surveillance for dysplasia Rate of progression differs for individuals no prospective studies showing efficacy but all guidelines support surveillance Non-dysplastic BE adenoca % / year surveillance Q3-5 years Dysplastic BE adenoca 0.6-5% / year surveillance Q6-12 months

114 Endoscopic management of BE

115 Endoscopic management of BE

116 Endoscopic management of BE

117 Endoscopic management of BE

118 Dr Gary Lim, Interventional Endoscopist CDHB Gastroenterology & Endoscopy Specialists
119 Case 54 year old male with occasional reflux symptoms managed with intermittent PPI Gastroscopy for dysphagia shows 6cm length of Barrett s oesophagus Where to from here?
120 Key Messages Erosive oesophagitis is a great indication for longterm PPI Peptic stricture responds well to dilatation(s) Erosive oesophagitis, Barrett s and AdenoCa oesophagus are all becoming more frequent Endoscopic therapy for Barrett s is revolutionalising management
121 Final Quiz Bridging the therapeutic gap What are the mechanisms of PPI non-responsive GORD? How do you manage heartburn not responding to PPI?
122 PPI non-responsive GORD 10-50% of people with GORD do not completely respond to a PPI % in double dose PPI <50% of people with GORD are satisfied with Rx PPI escalation beyond potential efficacy is common PPI non-responsive GORD patients NERD / functional heartburn
123 PPI non-responsive GORD

124 Psychological comorbidity Drug adherence Improper dosing time Functional heartburn Eosinophilic oesophagitis Weakly acid reflux PPI availability Rapid PPI metabolism PPI resistance Others Duodenogastricoesophageal reflux Residual acid reflux Delayed gastric emptying Concomitant functional bowel disorder
125 PPI adherence for GORD 1 month 55% 6 months 30% Presence of symptoms Severity of symptoms Personal preference
126 PPI dose timing 30 minutes prior to eating 100 patients with persistent GORD on PPI 46% dosed optimally 39% dosed at bed time or prn
127 Weakly acidic / alkaline reflux PPIs stop acid but not volume 168 refractory GORD (ph / impedance testing) 11% acid reflux 37% non-acid reflux Need to consider the lower oesophageal junction
128 Duodenogastro-oesophageal reflux / Bile reflux less common cause of symptoms Need to consider the lower oesophageal junction
129 Oesophageal hypersensitivity 50% of GORS patients with normal endoscopy have normal ph studies People with erosive oesophagitis have lower oesophageal pain thresholds than those without 58% of BD PPI-failure patients have functional heartburn
130 Residual acid reflux Up to 40% of patients taking once daily PPI have a positive ph study PPI daily 31% PPI BD 4% BD PPI trials are worthwhile
131 Nocturnal acid breakthrough Oesophageal ph <4 for greater than one hour overnight in symptomatic GORD patients on BD PPI Nocturnal symptoms do not correlate strongly with daytime symptoms or ph testing abnormalities
132 Psychological co-morbidity Patients with a poor correlation between symptoms and acid reflux events have higher rates of anxiety and depression
133 Eosinophilic oesophagitis All have dysphagia 1/3 have classic heartburn Eosinophilic oesophagitis and GORD may co-exist
134 Investigation for PPI non-responsive GORD Upper GI endoscopy may reveal an alternative diagnosis often normal NERD / functional heartburn 24H oesophageal ph / impedance monitoring defines the physiology allows definitive diagnosis to be made Barium swallow / manometry only if considering anti-reflux surgery
135 Treatment approaches Addressing poor PPI adherence and timing Confirming lifestyle measures Nocturnal H2RA in addition to BD PPI Switching to another PPI brand / dose escalation TLOSR reducers (baclofen) Prokinetics (only if impaired gastric emptying)
136 Treatment approaches Visceral pain modifiers Botox injections of the pylorus especially with gastroparesis Anti-reflux surgery works best if a positive response to PPI patients need careful evaluation Endoscopic treatment (coming)
137 Thank you
GERD DIAGNOSIS & TREATMENT DISCLOSURES 4/18/2018
 GERD DIAGNOSIS & TREATMENT Subhash Chandra MBBS Assistant Professor CHI Health Clinic Gastroenterology Creighton University, School of Medicine April 28, 2018 DISCLOSURES None 1 OBJECTIVES Review update
GERD DIAGNOSIS & TREATMENT Subhash Chandra MBBS Assistant Professor CHI Health Clinic Gastroenterology Creighton University, School of Medicine April 28, 2018 DISCLOSURES None 1 OBJECTIVES Review update
Speaker disclosure. Objectives. GERD: Who and When to Treat 7/21/2015
 GERD: Who and When to Treat Eugenio J Hernandez, MD Gastrohealth, PL Assistant Professor of Clinical Medicine, FIU Herbert Wertheim School of Medicine Speaker disclosure I do not have any relevant commercial
GERD: Who and When to Treat Eugenio J Hernandez, MD Gastrohealth, PL Assistant Professor of Clinical Medicine, FIU Herbert Wertheim School of Medicine Speaker disclosure I do not have any relevant commercial
ACG Clinical Guideline: Diagnosis and Management of Gastroesophageal Reflux Disease
 ACG Clinical Guideline: Diagnosis and Management of Gastroesophageal Reflux Disease Philip O. Katz MD 1, Lauren B. Gerson MD, MSc 2 and Marcelo F. Vela MD, MSCR 3 1 Division of Gastroenterology, Einstein
ACG Clinical Guideline: Diagnosis and Management of Gastroesophageal Reflux Disease Philip O. Katz MD 1, Lauren B. Gerson MD, MSc 2 and Marcelo F. Vela MD, MSCR 3 1 Division of Gastroenterology, Einstein
Barrett s Oesophagus Information Leaflet THE DIGESTIVE SYSTEM. gutscharity.org.
 THE DIGESTIVE SYSTEM http://healthfavo.com/digestive-system-for-kids.html This factsheet is about Barrett s Oesophagus Barrett s Oesophagus is the term used for a pre-cancerous condition where the normal
THE DIGESTIVE SYSTEM http://healthfavo.com/digestive-system-for-kids.html This factsheet is about Barrett s Oesophagus Barrett s Oesophagus is the term used for a pre-cancerous condition where the normal
Gastro-oesophageal reflux disease and peptic ulcer disease. By: Dr. Singanamala Suman Assistant Professor Department of Pharm.D
 Gastro-oesophageal reflux disease and peptic ulcer disease By: Dr. Singanamala Suman Assistant Professor Department of Pharm.D Gastro-oesophageal reflux disease and peptic ulcer disease Learning objectives:
Gastro-oesophageal reflux disease and peptic ulcer disease By: Dr. Singanamala Suman Assistant Professor Department of Pharm.D Gastro-oesophageal reflux disease and peptic ulcer disease Learning objectives:
MANAGEMENT OF DYSPEPSIA AND GASTRO-OESOPHAGEAL REFLUX DISEASE (GORD)
") DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT OF DYSPEPSIA AND GASTRO-OESOPHAGEAL REFLUX DISEASE (GORD) Routine endoscopic investigation of patients of any age, presenting with dyspepsia
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT OF DYSPEPSIA AND GASTRO-OESOPHAGEAL REFLUX DISEASE (GORD) Routine endoscopic investigation of patients of any age, presenting with dyspepsia
Reflux of gastric contents, particularly acid, into the esophagus
 Heartburn Reflux of gastric contents, particularly acid, into the esophagus Patient assessment with GERD 1-signs and symptoms The hallmark of typical symptom of GERD is heartburn (restrosternal),acid regurgitation,
Heartburn Reflux of gastric contents, particularly acid, into the esophagus Patient assessment with GERD 1-signs and symptoms The hallmark of typical symptom of GERD is heartburn (restrosternal),acid regurgitation,
GASTROESOPHAGEAL REFLUX
 DR. PHILIP K. BLUSTEIN M.D. F.R.C.P.(C) 415 14 TH ST. NW. CALGARY AB T2N2A1 PHONE (403) 270-9555 FAX (404) 270-7479 GASTROESOPHAGEAL REFLUX DEFINITION: *MONTREAL CONSENSUS DEFINED GERD AS A CONDITION WHICH
DR. PHILIP K. BLUSTEIN M.D. F.R.C.P.(C) 415 14 TH ST. NW. CALGARY AB T2N2A1 PHONE (403) 270-9555 FAX (404) 270-7479 GASTROESOPHAGEAL REFLUX DEFINITION: *MONTREAL CONSENSUS DEFINED GERD AS A CONDITION WHICH
Peptic ulcer disease Disorders of the esophagus
 Peptic ulcer disease Disorders of the esophagus Peptic ulcer disease Burning epigastric pain Exacerbated by fasting Improved with meals Ulcer: disruption of mucosal integrity >5 mm in size, with depth
Peptic ulcer disease Disorders of the esophagus Peptic ulcer disease Burning epigastric pain Exacerbated by fasting Improved with meals Ulcer: disruption of mucosal integrity >5 mm in size, with depth
SASKATCHEWAN REGISTERED NURSES ASSOCIATION
 DEFINITION Reflux of gastric contents into the esophagus, which results in esophageal irritation or inflammation. IMMEDIATE CONSULTATION REQUIRED IN THE FOLLOWING SITUATIONS Dysphagia (solid food, progressive)
DEFINITION Reflux of gastric contents into the esophagus, which results in esophageal irritation or inflammation. IMMEDIATE CONSULTATION REQUIRED IN THE FOLLOWING SITUATIONS Dysphagia (solid food, progressive)
GASTRO-OESOPHAGEAL REFLUX DR RONALDA DELACY
 GASTRO-OESOPHAGEAL REFLUX DR RONALDA DELACY DEFINITIONS GERD -Involuntary, effortless passage of gastric contents into the oesophagus +/-ejected from the mouth resulting in troublesome symptoms or complications
GASTRO-OESOPHAGEAL REFLUX DR RONALDA DELACY DEFINITIONS GERD -Involuntary, effortless passage of gastric contents into the oesophagus +/-ejected from the mouth resulting in troublesome symptoms or complications
Oesophageal Disorders
 Oesophageal Disorders Anatomy Upper sphincter Oesophageal body Diaphragm Lower sphincter Gastric Cardia Symptoms Of Oesophageal Disorders Dysphagia Odynophagia Heartburn Atypical Chest Pain Regurgitation
Oesophageal Disorders Anatomy Upper sphincter Oesophageal body Diaphragm Lower sphincter Gastric Cardia Symptoms Of Oesophageal Disorders Dysphagia Odynophagia Heartburn Atypical Chest Pain Regurgitation
Guidelines for the Management of Dyspepsia and GORD. Gastroenterology/ Acute Adult Governance. Drugs and Therapeutics Committee
 Guidelines for the Management of Dyspepsia and GORD Document type: Version: 3.0 Author (name): Author (designation): Validated by Prescribing Dr. G. Lipscomb Date validated October 2015 Ratified by: Date
Guidelines for the Management of Dyspepsia and GORD Document type: Version: 3.0 Author (name): Author (designation): Validated by Prescribing Dr. G. Lipscomb Date validated October 2015 Ratified by: Date
GASTROINTESTINAL AND ANTIEMETIC DRUGS. Submitted by: Shaema M. Ali
 GASTROINTESTINAL AND ANTIEMETIC DRUGS Submitted by: Shaema M. Ali GASTROINTESTINAL AND ANTIEMETIC DRUGS by: Shaema M. Ali There are four common medical conditions involving the GI system 1) peptic ulcers
GASTROINTESTINAL AND ANTIEMETIC DRUGS Submitted by: Shaema M. Ali GASTROINTESTINAL AND ANTIEMETIC DRUGS by: Shaema M. Ali There are four common medical conditions involving the GI system 1) peptic ulcers
Management of Dyspepsia
 MPharm Programme Management of Dyspepsia Slide 1 of 28 Learning Objectives Understand the principles and wider implications underpinning evidence based therapeutics in the key clinical specialities Objectively
MPharm Programme Management of Dyspepsia Slide 1 of 28 Learning Objectives Understand the principles and wider implications underpinning evidence based therapeutics in the key clinical specialities Objectively
Putting Chronic Heartburn On Ice
 Putting Chronic Heartburn On Ice Over the years, gastroesophageal reflux disease has proven to be one of the most common complaints facing family physicians. With quicker diagnosis, this pesky ailment
Putting Chronic Heartburn On Ice Over the years, gastroesophageal reflux disease has proven to be one of the most common complaints facing family physicians. With quicker diagnosis, this pesky ailment
GERD: A linical Clinical Clinical Update Objectives
 GERD: A Clinical Update Jeff Gilbert, M.D. University i of Kentucky Gastroenterology 11/6/08 Objectives To review the basic pathophysiology underlying gastroesophageal reflux disease To highlight current
GERD: A Clinical Update Jeff Gilbert, M.D. University i of Kentucky Gastroenterology 11/6/08 Objectives To review the basic pathophysiology underlying gastroesophageal reflux disease To highlight current
GI Pharmacology. Dr. Alia Shatanawi 5/4/2018
 GI Pharmacology Dr. Alia Shatanawi 5/4/2018 Drugs Used in Gastrointestinal Diseases Drugs used in Peptic Ulcer Diseases. Drugs Stimulating Gastrointestinal Motility &Laxatives. Antidiarrheal Agents. Drugs
GI Pharmacology Dr. Alia Shatanawi 5/4/2018 Drugs Used in Gastrointestinal Diseases Drugs used in Peptic Ulcer Diseases. Drugs Stimulating Gastrointestinal Motility &Laxatives. Antidiarrheal Agents. Drugs
Gastro esophageal reflux disease DR. AMMAR I. ABDUL-LATIF
 Gastro esophageal reflux disease )GERD( DR. AMMAR I. ABDUL-LATIF GERD DEFINITION EPIDEMIOLOGY CAUSES PATHOGENESIS SIGNS &SYMPTOMS COMPLICATIONS DIAGNOSIS TREATMENT Definition Montreal consensus defined
Gastro esophageal reflux disease )GERD( DR. AMMAR I. ABDUL-LATIF GERD DEFINITION EPIDEMIOLOGY CAUSES PATHOGENESIS SIGNS &SYMPTOMS COMPLICATIONS DIAGNOSIS TREATMENT Definition Montreal consensus defined
Concise guide to management of reflux disease in primary care
 Drug review GORD Concise guide to management of reflux disease in primary care Kumar Kanti Basu BSc, FRCP Reflux is a common disorder often aggravated by lifestyle and other medications. Our Drug review
Drug review GORD Concise guide to management of reflux disease in primary care Kumar Kanti Basu BSc, FRCP Reflux is a common disorder often aggravated by lifestyle and other medications. Our Drug review
The usual dose is 40 mg daily with amoxycillin 1.5 g (750 mg b.d.) for 2 weeks. Up to 2 g/day of amoxycillin has been used in clinical trials.
 for 2 weeks. Up to 2 g/day of amoxycillin has been used in clinical trials.") Name Gasec - 2 Gastrocaps Composition Gasec-20 Gastrocaps Each Gastrocaps contains: Omeprazole 20 mg (in the form of enteric-coated pellets) Properties, effects Proton Pump Inhibitor Omeprazole belongs
Name Gasec - 2 Gastrocaps Composition Gasec-20 Gastrocaps Each Gastrocaps contains: Omeprazole 20 mg (in the form of enteric-coated pellets) Properties, effects Proton Pump Inhibitor Omeprazole belongs
Management of dyspepsia and of Helicobacter pylori infection
 Management of dyspepsia and of Helicobacter pylori infection The University of Nottingham John Atherton Wolfson Digestive Diseases Centre University of Nottingham, UK Community management of dyspepsia
Management of dyspepsia and of Helicobacter pylori infection The University of Nottingham John Atherton Wolfson Digestive Diseases Centre University of Nottingham, UK Community management of dyspepsia
Gastroesophageal Reflux Disease, Paraesophageal Hernias &
 530.81 553.3 & 530.00 43289, 43659 1043432842, MD Assistant Clinical Professor of Surgery, UH JABSOM Associate General Surgery Program Director Director of Minimally Invasive & Bariatric Surgery Programs
530.81 553.3 & 530.00 43289, 43659 1043432842, MD Assistant Clinical Professor of Surgery, UH JABSOM Associate General Surgery Program Director Director of Minimally Invasive & Bariatric Surgery Programs
GASTROINTESTINAL SYSTEM MANAGEMENT OF DYSPEPSIA
 GASTROINTESTINAL SYSTEM MANAGEMENT OF DYSPEPSIA MANAGEMENT Dyspepsia refers to a spectrum of usually intermittent upper gastrointestinal symptoms, including epigastric pain and heartburn. For the majority
GASTROINTESTINAL SYSTEM MANAGEMENT OF DYSPEPSIA MANAGEMENT Dyspepsia refers to a spectrum of usually intermittent upper gastrointestinal symptoms, including epigastric pain and heartburn. For the majority
GUIDELINES FOR CLINICIANS. Gastro-Oesophageal Reflux Disease in Adults. Reflux Disease. 4th Edition Digestive Health Foundation
 GUIDELINES FOR CLINICIANS Gastro-Oesophageal Reflux Disease in Adults Reflux Disease 4th Edition 2008 Digestive Health Foundation Digestive Health Foundation Table of contents Page 4 Gastro-oesophageal
GUIDELINES FOR CLINICIANS Gastro-Oesophageal Reflux Disease in Adults Reflux Disease 4th Edition 2008 Digestive Health Foundation Digestive Health Foundation Table of contents Page 4 Gastro-oesophageal
James Paget University Hospitals. NHS Foundation Trust. Hiatus hernia. Patient Information
 James Paget University Hospitals NHS Foundation Trust Hiatus hernia Patient Information What is a hiatus hernia? A hiatus hernia can cause highly irritating stomach contents, such as acid, to move up into
James Paget University Hospitals NHS Foundation Trust Hiatus hernia Patient Information What is a hiatus hernia? A hiatus hernia can cause highly irritating stomach contents, such as acid, to move up into
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT OF DYSPEPSIA
 MANAGEMENT OF DYSPEPSIA") DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT OF DYSPEPSIA o Patients of any age with ALARM signs should be referred through the 2-week referral system o Routine endoscopic investigation
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT OF DYSPEPSIA o Patients of any age with ALARM signs should be referred through the 2-week referral system o Routine endoscopic investigation
Heartburn, also referred to acid reflux, happens when stomach acid flows back (refluxes) into your esophagus.
 into your esophagus.") WHILE almost everyone experiences mild heartburn from time to time and many individuals have some antacids or another medication on hand for its relief, talk to your doctor, if you have heartburn more
WHILE almost everyone experiences mild heartburn from time to time and many individuals have some antacids or another medication on hand for its relief, talk to your doctor, if you have heartburn more
Safety Of. long-term PPI. Layli Eslami, MD Tehran, 1393
 Safety Of long-term PPI Layli Eslami, MD Tehran, 1393 n The introduction of PPIs in the late 1980s optimized the medical treatment of acidrelated disorders n In some cases such as GERD patients given the
Safety Of long-term PPI Layli Eslami, MD Tehran, 1393 n The introduction of PPIs in the late 1980s optimized the medical treatment of acidrelated disorders n In some cases such as GERD patients given the
WHAT IS GASTROESOPHAGEAL REFLUX DISEASE (GERD)?
?") WHAT IS GASTROESOPHAGEAL REFLUX DISEASE (GERD)? The term gastroesophageal reflux describes the movement (or reflux) of stomach contents back up into the esophagus, the muscular tube that extends from the
WHAT IS GASTROESOPHAGEAL REFLUX DISEASE (GERD)? The term gastroesophageal reflux describes the movement (or reflux) of stomach contents back up into the esophagus, the muscular tube that extends from the
Proton Pump Inhibitors. Description. Section: Prescription Drugs Effective Date: July 1, 2014
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.09.01 Subject: Proton Pump Inhibitors Page: 1 of 7 Last Review Date: June 12, 2014 Proton Pump Inhibitors
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.09.01 Subject: Proton Pump Inhibitors Page: 1 of 7 Last Review Date: June 12, 2014 Proton Pump Inhibitors
Module 2 Heartburn Glossary
 Absorption Antacids Antibiotic Module 2 Heartburn Glossary Barrett s oesophagus Bloating Body mass index Burping Chief cells Colon Digestion Endoscopy Enteroendocrine cells Epiglottis Epithelium Absorption
Absorption Antacids Antibiotic Module 2 Heartburn Glossary Barrett s oesophagus Bloating Body mass index Burping Chief cells Colon Digestion Endoscopy Enteroendocrine cells Epiglottis Epithelium Absorption
TBURN TBURN BURN ARTBURN EARTBURN EART HEARTBURN: HOW TO GET IT OFF YOUR CHEST
 TBURN BURN TBURN ARTBURN. EARTBURN EART N EARTBURN HEARTBURN: HOW TO GET IT OFF YOUR CHEST Do you sometimes wake up at night with a sharp, burning sensation in your chest? Does this sometimes happen during
TBURN BURN TBURN ARTBURN. EARTBURN EART N EARTBURN HEARTBURN: HOW TO GET IT OFF YOUR CHEST Do you sometimes wake up at night with a sharp, burning sensation in your chest? Does this sometimes happen during
Management of dyspepsia in adults in primary care
 Dyspepsia Management of dyspepsia in adults in primary care June 2005. The recommendations on referral for endoscopy in this NICE guideline have been amended in line with the recommendation in the NICE
Dyspepsia Management of dyspepsia in adults in primary care June 2005. The recommendations on referral for endoscopy in this NICE guideline have been amended in line with the recommendation in the NICE
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Achalasia, barium esophagography for, 57 58 Acid pocket, 18 19 Acid-sensing ion, 20 Acupuncture, 128 Adiponectin, in obesity, 166 ADX10059 metabotropic
Note: Page numbers of article titles are in boldface type. A Achalasia, barium esophagography for, 57 58 Acid pocket, 18 19 Acid-sensing ion, 20 Acupuncture, 128 Adiponectin, in obesity, 166 ADX10059 metabotropic
QUICK QUERIES. Topical Questions, Sound Answers
 QUICK QUERIES Topical Questions, Sound Answers Dyspepsia: An Evidence-Based Approach Alan B. R. Thomson, MD, PhD, FRCPC, FACP, FACG Presented at the University of Alberta s Medical Grand Rounds, University
QUICK QUERIES Topical Questions, Sound Answers Dyspepsia: An Evidence-Based Approach Alan B. R. Thomson, MD, PhD, FRCPC, FACP, FACG Presented at the University of Alberta s Medical Grand Rounds, University
PPIs: Good or Bad? 1. Basics of PPIs. Gastric Acid Basics. Outline. Gastric Acid Basics. Proton Pump Inhibitors (PPI)
") Outline Quick basics on Proton Pump Inhibitors (PPIs) PPIs: Good or Bad? What are potential risks of PPI therapy? How to approach your patients American Gastroenterology Association (AGA) recommendations
Outline Quick basics on Proton Pump Inhibitors (PPIs) PPIs: Good or Bad? What are potential risks of PPI therapy? How to approach your patients American Gastroenterology Association (AGA) recommendations
DISCLAIMER. No Conflict of Interest
 DISCLAIMER No Conflict of Interest EXCLAIMER No Interest in Conflict GORD IS SURGICAL John Dunn, FRACS Laparoscopy Auckland GOD IS SURGICAL He taua ano ta te kai (Even food can attack) PATHOGENESIS Failure
DISCLAIMER No Conflict of Interest EXCLAIMER No Interest in Conflict GORD IS SURGICAL John Dunn, FRACS Laparoscopy Auckland GOD IS SURGICAL He taua ano ta te kai (Even food can attack) PATHOGENESIS Failure
PRESCRIBING SUPPORT TEAM AUDIT: PROTON PUMP INHIBITOR PRESCRIBING REVIEW
 PRESCRIBING SUPPORT TEAM AUDIT: PROTON PUMP INHIBITOR PRESCRIBING REVIEW DATE OF AUTHORISATION: AUTHORISING GP: PRESCRIBING SUPPORT TECHNICIAN: SUMMARY Dyspepsia refers to a broad range of symptoms related
PRESCRIBING SUPPORT TEAM AUDIT: PROTON PUMP INHIBITOR PRESCRIBING REVIEW DATE OF AUTHORISATION: AUTHORISING GP: PRESCRIBING SUPPORT TECHNICIAN: SUMMARY Dyspepsia refers to a broad range of symptoms related
Burning Issues in Gastroesophageal Reflux Disease (GERD)
") 3:45 4:45pm Burning Issues in GERD SPEAKER Prateek Sharma, MD, FACG, FACP Presenter Disclosure Information The following relationships exist related to this presentation: Prateek Sharma, MD, FACG, FACP,
3:45 4:45pm Burning Issues in GERD SPEAKER Prateek Sharma, MD, FACG, FACP Presenter Disclosure Information The following relationships exist related to this presentation: Prateek Sharma, MD, FACG, FACP,
ESOPHAGEAL CANCER AND GERD. Prof Salman Guraya FRCS, Masters MedEd
 ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
Gastroesophageal Reflux Disease (GERD)
") Gastroesophageal Reflux Disease (GERD) Information for patients UHN Read this handout to learn about: What gastroesohageal reflux (GERD) is Signs and symptoms How your doctor will know if you have it Tests
Gastroesophageal Reflux Disease (GERD) Information for patients UHN Read this handout to learn about: What gastroesohageal reflux (GERD) is Signs and symptoms How your doctor will know if you have it Tests
Refractory GERD. Kenneth R. DeVault, MD, FACG President American College of Gastroenterology Chair Department of Medicine Mayo Clinic Florida
 Refractory GERD Kenneth R. DeVault, MD, FACG President American College of Gastroenterology Chair Department of Medicine Mayo Clinic Florida Objectives Define the terminology associated with refractory
Refractory GERD Kenneth R. DeVault, MD, FACG President American College of Gastroenterology Chair Department of Medicine Mayo Clinic Florida Objectives Define the terminology associated with refractory
Refractory GERD : case presentation and discussion
 Refractory GERD : case presentation and discussion Ping-Huei Tseng National Taiwan University Hospital May 19, 2018 How effective is PPI based on EGD? With GERD symptom 75% erosive 25% NERD Endoscopy 81%
Refractory GERD : case presentation and discussion Ping-Huei Tseng National Taiwan University Hospital May 19, 2018 How effective is PPI based on EGD? With GERD symptom 75% erosive 25% NERD Endoscopy 81%
Functional Heartburn and Dyspepsia
 Functional Heartburn and Dyspepsia Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina Objectives Understand the means of diagnosing functional heartburn
Functional Heartburn and Dyspepsia Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina Objectives Understand the means of diagnosing functional heartburn
GERD. Gastroesophageal reflux disease, or GERD, occurs when acid from the. stomach backs up into the esophagus. Normally, food travels from the
 GERD What is GERD? Gastroesophageal reflux disease, or GERD, occurs when acid from the stomach backs up into the esophagus. Normally, food travels from the mouth, down through the esophagus and into the
GERD What is GERD? Gastroesophageal reflux disease, or GERD, occurs when acid from the stomach backs up into the esophagus. Normally, food travels from the mouth, down through the esophagus and into the
 Page 1 of 5 Official reprint from UpToDate www.uptodate.com 2017 UpToDate Patient education: Acid reflux (gastroesophageal reflux disease) in adults (The Basics) Written by the doctors and editors at UpToDate
Page 1 of 5 Official reprint from UpToDate www.uptodate.com 2017 UpToDate Patient education: Acid reflux (gastroesophageal reflux disease) in adults (The Basics) Written by the doctors and editors at UpToDate
Indigestion (dyspepsia)
") Commissioning pathways Indigestion (dyspepsia) Supplementary information to be read in conjunction with the pathway Reference Supplementary Information 1.1 Symptom Description Annual incidence 40%. Prevalence
Commissioning pathways Indigestion (dyspepsia) Supplementary information to be read in conjunction with the pathway Reference Supplementary Information 1.1 Symptom Description Annual incidence 40%. Prevalence
Myogenic Control. Esophageal Motility. Enteric Nervous System. Alimentary Tract Motility. Determinants of GI Tract Motility.
 Myogenic Control Esophageal Motility David Markowitz, MD Columbia University, College of Physicians and Surgeons Basic Electrical Rythym: intrinsic rhythmic fluctuation of smooth muscle membrane potential
Myogenic Control Esophageal Motility David Markowitz, MD Columbia University, College of Physicians and Surgeons Basic Electrical Rythym: intrinsic rhythmic fluctuation of smooth muscle membrane potential
Esophageal Motility. Alimentary Tract Motility
 Esophageal Motility David Markowitz, MD Columbia University, College of Physicians and Surgeons Alimentary Tract Motility Propulsion Movement of food and endogenous secretions Mixing Allows for greater
Esophageal Motility David Markowitz, MD Columbia University, College of Physicians and Surgeons Alimentary Tract Motility Propulsion Movement of food and endogenous secretions Mixing Allows for greater
Proton Pump Inhibitor De-prescribing Guidance
 Amendment History Proton Pump Inhibitor De-prescribing Guidance VERSION DATE AMENDMENT HISTORY 1.0 2013 Previous version 2.0 September 2015 Comments Amendment to Flow chart and addition of Rationale page
Amendment History Proton Pump Inhibitor De-prescribing Guidance VERSION DATE AMENDMENT HISTORY 1.0 2013 Previous version 2.0 September 2015 Comments Amendment to Flow chart and addition of Rationale page
GI update. Common conditions and concerns my patients frequently asked about
 GI update Common conditions and concerns my patients frequently asked about Specific conditions I ll try to cover today 1. Colon polyps, colorectal cancer and colonoscopy 2. Crohn s disease 3. Peptic ulcer
GI update Common conditions and concerns my patients frequently asked about Specific conditions I ll try to cover today 1. Colon polyps, colorectal cancer and colonoscopy 2. Crohn s disease 3. Peptic ulcer
Disclosures. Heartburn and Barrett s Esophagus. Heartburn and Barrett s Esophagus. GERD is common in the U.S. None
 Heartburn and Barrett s Esophagus None Disclosures Christian Mathy, MD University of California, San Francisco 2015 Heartburn and Barrett s Esophagus Heartburn and GERD GERD therapy Extraesophageal GERD
Heartburn and Barrett s Esophagus None Disclosures Christian Mathy, MD University of California, San Francisco 2015 Heartburn and Barrett s Esophagus Heartburn and GERD GERD therapy Extraesophageal GERD
Dyspepsia. Dyspepsia covers upper abdominal pain, fullness, early satiety, bloating, and nausea.
 Antacids Hawler medical university Collage of pharmacy/ fourth year /pharmacy practice Sham A. Talat Shareef (B.Sc. Msc. clinical pharmacy) 2017-2018 Sham_talat@yahoo.com Head of Department Of Clinical
Antacids Hawler medical university Collage of pharmacy/ fourth year /pharmacy practice Sham A. Talat Shareef (B.Sc. Msc. clinical pharmacy) 2017-2018 Sham_talat@yahoo.com Head of Department Of Clinical
Fecal incontinence causes 196 epidemiology 8 treatment 196
 Subject Index Achalasia course 93 differential diagnosis 93 esophageal dysphagia 92 95 etiology 92, 93 treatment 93 95 work-up 93 Aminosalicylates, pharmacokinetics and aging effects 36 Antibiotics diarrhea
Subject Index Achalasia course 93 differential diagnosis 93 esophageal dysphagia 92 95 etiology 92, 93 treatment 93 95 work-up 93 Aminosalicylates, pharmacokinetics and aging effects 36 Antibiotics diarrhea
David Markowitz, MD. Physicians and Surgeons
 Esophageal Motility David Markowitz, MD Columbia University, College of Columbia University, College of Physicians and Surgeons Alimentary Tract Motility Propulsion Movement of food and endogenous secretions
Esophageal Motility David Markowitz, MD Columbia University, College of Columbia University, College of Physicians and Surgeons Alimentary Tract Motility Propulsion Movement of food and endogenous secretions
Policy Evaluation: Proton Pump Inhibitors (PPIs)
") Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
11/19/2012. Comparison between PPIs G CELL. Risk ratio (95% CI) Patient subgroup. gastrin. S-form of omeprazole. Acid sensitive. coated.
 Patient subgroup. gastrin. S-form of omeprazole. Acid sensitive. coated.") REGULATION OF GASTRIC ACID SECRETION Comparison between PPIs Omeprazole Lansoprazole Rabeprazole Pantoprazole Esomeprazole gastrin G CELL + Acid sensitive Yes T1/2 30-60 minutes Main elimination Enteric
REGULATION OF GASTRIC ACID SECRETION Comparison between PPIs Omeprazole Lansoprazole Rabeprazole Pantoprazole Esomeprazole gastrin G CELL + Acid sensitive Yes T1/2 30-60 minutes Main elimination Enteric
HEARTBURN & REFLUX FUNDING RESEARCH INTO DISEASES OF THE GUT, LIVER & PANCREAS
 ALL YOU NEED TO KNOW ABOUT HEARTBURN & REFLUX FUNDING RESEARCH INTO DISEASES OF THE GUT, LIVER & PANCREAS THIS FACTSHEET IS ABOUT HEARTBURN & REFLUX Heartburn is extremely common, affecting up to 25% of
ALL YOU NEED TO KNOW ABOUT HEARTBURN & REFLUX FUNDING RESEARCH INTO DISEASES OF THE GUT, LIVER & PANCREAS THIS FACTSHEET IS ABOUT HEARTBURN & REFLUX Heartburn is extremely common, affecting up to 25% of
When to Refer for OGD and the Work Up of Upper GI Malignancies
 When to Refer for OGD and the Work Up of Upper GI Malignancies Dr Hong Qiantai Registrar, Department of Surgery GP Forum 27 May 2017 38 year old female, non-smoker, BMI 29 Works as investment banker Presents
When to Refer for OGD and the Work Up of Upper GI Malignancies Dr Hong Qiantai Registrar, Department of Surgery GP Forum 27 May 2017 38 year old female, non-smoker, BMI 29 Works as investment banker Presents
Hiatus Hernia. Endoscopy Department. Patient information leaflet
 Hiatus Hernia Endoscopy Department Patient information leaflet You will only be given this leaflet if you have been diagnosed with a hiatus hernia. The information below outlines normal anatomy, conditions,
Hiatus Hernia Endoscopy Department Patient information leaflet You will only be given this leaflet if you have been diagnosed with a hiatus hernia. The information below outlines normal anatomy, conditions,
EMILOK Global. (omeprazole) Composition: Each capsule contains 20 mg omeprazole as enteric-coated
 Composition: Each capsule contains 20 mg omeprazole as enteric-coated") EMILOK Global (omeprazole) Composition: Each capsule contains 20 mg omeprazole as enteric-coated granules. Properties: Emilok (omeprazole) belongs to the group of proton pump inhibitors, inhibits both
EMILOK Global (omeprazole) Composition: Each capsule contains 20 mg omeprazole as enteric-coated granules. Properties: Emilok (omeprazole) belongs to the group of proton pump inhibitors, inhibits both
Nexium 24HR Pharmacy Training
 Nexium 24HR Pharmacy Training Your pharmacist's advice is required. Always read the label. Use only as directed. If symptoms persist, consult your doctor/ healthcare professional. Pfizer Consumer Healthcare
Nexium 24HR Pharmacy Training Your pharmacist's advice is required. Always read the label. Use only as directed. If symptoms persist, consult your doctor/ healthcare professional. Pfizer Consumer Healthcare
LONG -TERM USE OF PPIS: INDICATIONS, BENEFITS AND HARMS. Jihane Naous, M.D.
 LONG -TERM USE OF PPIS: INDICATIONS, BENEFITS AND HARMS Jihane Naous, M.D. Objectives Identify the conditions supported by AGA/ACG guidelines necessitating long-term use of daily PPIs, Recognize which
LONG -TERM USE OF PPIS: INDICATIONS, BENEFITS AND HARMS Jihane Naous, M.D. Objectives Identify the conditions supported by AGA/ACG guidelines necessitating long-term use of daily PPIs, Recognize which
https://www.uptodate.com/contents/acid-reflux-gastroesophageal-reflux-disease-in-adults-...
 Page 1 of 10 Official reprint from UpToDate www.uptodate.com 2017 UpToDate The content on the UpToDate website is not intended nor recommended as a substitute for medical advice, diagnosis, or treatment.
Page 1 of 10 Official reprint from UpToDate www.uptodate.com 2017 UpToDate The content on the UpToDate website is not intended nor recommended as a substitute for medical advice, diagnosis, or treatment.
Unmet Needs in the Management of Gastroesophageal Reflux Disease
 Unmet Needs in the Management of Gastroesophageal Reflux Disease Ronnie Fass MD Professor of Medicine Case Western Reserve University Chairman, Division of Gastroenterology and Hepatology Director, Esophageal
Unmet Needs in the Management of Gastroesophageal Reflux Disease Ronnie Fass MD Professor of Medicine Case Western Reserve University Chairman, Division of Gastroenterology and Hepatology Director, Esophageal
In the Name of God. Refractory GERD
 In the Name of God Refractory GERD S Nasseri-Moghaddam MD, MPH, AGAF Associate Professor of Medicine Digestive Disease Research Institute Shariati Hospital, TUMS sianasseri@yahoo.com IAGH meeting, Ordibehesht
In the Name of God Refractory GERD S Nasseri-Moghaddam MD, MPH, AGAF Associate Professor of Medicine Digestive Disease Research Institute Shariati Hospital, TUMS sianasseri@yahoo.com IAGH meeting, Ordibehesht
Definition: gas tro e soph a ge al re f lux dis ease (GERD) from Stedman's Medical Dictionary for the Health Professions and Nursing
 from Stedman's Medical Dictionary for the Health Professions and Nursing") Topic Page: Gastroesophageal reflux Definition: gas tro e soph a ge al re f lux dis ease (GERD) from Stedman's Medical Dictionary for the Health Professions and Nursing (gas trō-ĕ-sof ă-jē ăl rē flŭks
Topic Page: Gastroesophageal reflux Definition: gas tro e soph a ge al re f lux dis ease (GERD) from Stedman's Medical Dictionary for the Health Professions and Nursing (gas trō-ĕ-sof ă-jē ăl rē flŭks
Motility - Difficult Issues in Practice and How to Investigate
 Motility - Difficult Issues in Practice and How to Investigate Geoff Hebbard The Issues (Upper GI) Difficult Dysphagia Non-Cardiac Chest pain Reflux Symptoms Regurgitation Belching 1 The Tools Oesophageal
Motility - Difficult Issues in Practice and How to Investigate Geoff Hebbard The Issues (Upper GI) Difficult Dysphagia Non-Cardiac Chest pain Reflux Symptoms Regurgitation Belching 1 The Tools Oesophageal
Hiatal Hernias and Barrett s esophagus. Dr Sajida Ahad Mercy General Surgery
 Hiatal Hernias and Barrett s esophagus Dr Sajida Ahad Mercy General Surgery Objectives Identify the use of different diagnostic modalities for hiatal hernias List the different types of hiatal hernias
Hiatal Hernias and Barrett s esophagus Dr Sajida Ahad Mercy General Surgery Objectives Identify the use of different diagnostic modalities for hiatal hernias List the different types of hiatal hernias
A Trip Through the GI Tract: Common GI Diseases and Complaints. Jennifer Curtis, MD
 A Trip Through the GI Tract: Common GI Diseases and Complaints Jennifer Curtis, MD Colon Cancer How does it develop? Most cancers arise from polyps Over time these can turn into cancer Combination of genetic
A Trip Through the GI Tract: Common GI Diseases and Complaints Jennifer Curtis, MD Colon Cancer How does it develop? Most cancers arise from polyps Over time these can turn into cancer Combination of genetic
HIATUS HERNIAS. Contents What is a Hiatus Hernia?... 3
 Contents What is a Hiatus Hernia?........................ 3 What about exercise?............................ 6 YOUR GUIDE TO HIATUS HERNIAS An IPRS Guide to provide you with exercises and advice to ease
Contents What is a Hiatus Hernia?........................ 3 What about exercise?............................ 6 YOUR GUIDE TO HIATUS HERNIAS An IPRS Guide to provide you with exercises and advice to ease
 P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
BARRETT S OESOPHAGUS
 ALL YOU NEED TO KNOW ABOUT BARRETT S OESOPHAGUS FUNDING RESEARCH INTO DISEASES OF THE GUT, LIVER & PANCREAS THIS FACTSHEET IS ABOUT BARRETT S OESOPHAGUS Barrett s Oesophagus is the term used for a pre-cancerous
ALL YOU NEED TO KNOW ABOUT BARRETT S OESOPHAGUS FUNDING RESEARCH INTO DISEASES OF THE GUT, LIVER & PANCREAS THIS FACTSHEET IS ABOUT BARRETT S OESOPHAGUS Barrett s Oesophagus is the term used for a pre-cancerous
Gastro-oesophageal reflux during pregnancy. Nigel Trudgill
 Gastro-oesophageal reflux during pregnancy Nigel Trudgill Summary How common? Which pregnancies? Why? Are there complications? How do we treat reflux during pregnancy? How common is reflux during 607 ante-natal
Gastro-oesophageal reflux during pregnancy Nigel Trudgill Summary How common? Which pregnancies? Why? Are there complications? How do we treat reflux during pregnancy? How common is reflux during 607 ante-natal
Non-Ulcer Dyspepsia: what is it? What can we do with these patients? Overview. Dyspepsia Definition. Functional Dyspepsia. Dyspepsia the Basics
 Non-Ulcer : what is it? What can we do with these patients? Temporal Changes and Geographic Variations in Developing Peptic Ulcer Disease Gastric Cancer 1900 Eamonn M M Quigley MD FACG Alimentary Pharmabiotic
Non-Ulcer : what is it? What can we do with these patients? Temporal Changes and Geographic Variations in Developing Peptic Ulcer Disease Gastric Cancer 1900 Eamonn M M Quigley MD FACG Alimentary Pharmabiotic
KK College of Nursing Peptic Ulcer Badil D ass Dass, Lecturer 25th July, 2011
 KK College of Nursing Peptic Ulcer Badil Dass, Lecturer 25 th July, 2011 Objectives: By the end of this lecture, the students t will be able to: Define peptic pp ulcer Describe the etiology and pathology
KK College of Nursing Peptic Ulcer Badil Dass, Lecturer 25 th July, 2011 Objectives: By the end of this lecture, the students t will be able to: Define peptic pp ulcer Describe the etiology and pathology
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 14 September 2011
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 14 September 2011 GAVISCON PEPPERMINT, chewable tablet B/20 (CIP code: 367 909-6) GAVISCON, oral suspension 250 ml
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 14 September 2011 GAVISCON PEPPERMINT, chewable tablet B/20 (CIP code: 367 909-6) GAVISCON, oral suspension 250 ml
A. Incorrect! Histamine is a secretagogue for stomach acid, but this is not the only correct answer.
 Pharmacology - Problem Drill 21: Drugs Used To Treat GI Disorders No. 1 of 10 1. Endogenous secretagogues for stomach acid include: #01 (A) Histamine (B) Gastrin (C) PGE1 (D) A and B (E) A, B and C Histamine
Pharmacology - Problem Drill 21: Drugs Used To Treat GI Disorders No. 1 of 10 1. Endogenous secretagogues for stomach acid include: #01 (A) Histamine (B) Gastrin (C) PGE1 (D) A and B (E) A, B and C Histamine
Patient information. Laryngopharyngeal Reflux ( LPR) Ear Nose and Throat Directorate PIF 1423/V4
 Ear Nose and Throat Directorate PIF 1423/V4") Patient information Laryngopharyngeal Reflux ( LPR) Ear Nose and Throat Directorate PIF 1423/V4 You have been diagnosed with laryngopharyngeal reflux (LPR), otherwise known as extra-oesophageal reflux
Patient information Laryngopharyngeal Reflux ( LPR) Ear Nose and Throat Directorate PIF 1423/V4 You have been diagnosed with laryngopharyngeal reflux (LPR), otherwise known as extra-oesophageal reflux
Disclosures. GI Motility Disorders. Gastrointestinal Motility Disorders & Irritable Bowel Syndrome
 Gastrointestinal Motility Disorders & Irritable Bowel Syndrome None Disclosures Jasmine Zia, MD Acting Assistant Professor Division of Gastroenterology, University of Washington 6 th Asian Health Symposium
Gastrointestinal Motility Disorders & Irritable Bowel Syndrome None Disclosures Jasmine Zia, MD Acting Assistant Professor Division of Gastroenterology, University of Washington 6 th Asian Health Symposium
CHAPTER 11 Functional Gastrointestinal Disorders (FGID) Mr. Ashok Kumar Dept of Pharmacy Practice SRM College of Pharmacy SRM University
 Mr. Ashok Kumar Dept of Pharmacy Practice SRM College of Pharmacy SRM University") CHAPTER 11 Functional Gastrointestinal Disorders (FGID) Mr. Ashok Kumar Dept of Pharmacy Practice SRM College of Pharmacy SRM University 1 Definition of FGID Chronic and recurrent symptoms of the gastrointestinal
CHAPTER 11 Functional Gastrointestinal Disorders (FGID) Mr. Ashok Kumar Dept of Pharmacy Practice SRM College of Pharmacy SRM University 1 Definition of FGID Chronic and recurrent symptoms of the gastrointestinal
Helicobacter 2008;13:1-6. Am J Gastroent 2007;102: Am J of Med 2004;117:31-35.
 An Update on Helicobacter pylori and Its Treatment Trenika Mitchell, PharmD, BCPS Clinical Assistant Professor University of Kentucky College of Pharmacy October 18, 2008 Objectives Review the epidemiology
An Update on Helicobacter pylori and Its Treatment Trenika Mitchell, PharmD, BCPS Clinical Assistant Professor University of Kentucky College of Pharmacy October 18, 2008 Objectives Review the epidemiology
Catherine Kerschen DO, FACOI Michigan State University College of Osteopathic Medicine
 Catherine Kerschen DO, FACOI Michigan State University College of Osteopathic Medicine none 32 yo male presents with a burning sensation in chest following most large meals for 2-3 months. He denies dysphagia,
Catherine Kerschen DO, FACOI Michigan State University College of Osteopathic Medicine none 32 yo male presents with a burning sensation in chest following most large meals for 2-3 months. He denies dysphagia,
You May Be at Risk. You are currently taking a proton pump inhibitor (PPI):
:") PPI You are currently taking a proton pump inhibitor (PPI): Dexlansoprazole (Dexilant ) Esomeprazole (Nexium ) Omeprazole (Losec, Olex ) Lansoprazole (Prevacid, Prevacid Fast Tab ) Pantoprazole sodium
PPI You are currently taking a proton pump inhibitor (PPI): Dexlansoprazole (Dexilant ) Esomeprazole (Nexium ) Omeprazole (Losec, Olex ) Lansoprazole (Prevacid, Prevacid Fast Tab ) Pantoprazole sodium
HEARTBURN (GASTROESOPHAGEAL REFLUX)
") DR. PHILIP K. BLUSTEIN M.D. F.R.C.P.(C) 415 14 TH ST. NW. CALGARY AB T2N2A1 PHONE (403) 270-9555 FAX (403) 270-7479 HEARTBURN (GASTROESOPHAGEAL REFLUX) DOCTOR, I HAVE HAD PROBLEMS WITH A BURNING FIRE SENSATION
DR. PHILIP K. BLUSTEIN M.D. F.R.C.P.(C) 415 14 TH ST. NW. CALGARY AB T2N2A1 PHONE (403) 270-9555 FAX (403) 270-7479 HEARTBURN (GASTROESOPHAGEAL REFLUX) DOCTOR, I HAVE HAD PROBLEMS WITH A BURNING FIRE SENSATION
Esophageal Disorders. Learning Objectives. Introduction. Gastroesophageal Reflux Disease. Reza Shaker, MD, and Benson T.
 Esophageal Disorders Reza Shaker, MD, and Benson T. Massey, MD, FACP Learning Objectives AFTER COMPLETING THIS CHAPTER, THE LEARNER SHOULD BE ABLE TO: 1. Recognize the typical and atypical presentations
Esophageal Disorders Reza Shaker, MD, and Benson T. Massey, MD, FACP Learning Objectives AFTER COMPLETING THIS CHAPTER, THE LEARNER SHOULD BE ABLE TO: 1. Recognize the typical and atypical presentations
Interventional procedures guidance Published: 16 December 2015 nice.org.uk/guidance/ipg540
 Electrical stimulation of the lower oesophageal sphincter for treating gastro-oesophageal reflux disease Interventional procedures guidance Published: 16 December 2015 nice.org.uk/guidance/ipg540 Your
Electrical stimulation of the lower oesophageal sphincter for treating gastro-oesophageal reflux disease Interventional procedures guidance Published: 16 December 2015 nice.org.uk/guidance/ipg540 Your
AGA SECTION. Gastroenterology 2016;150:
 Gastroenterology 2016;150:1026 1030 April 2016 AGA Section 1027 Procedural intervention (3) Upper endoscopy indications 3 6 Non-response of symptoms to a 4 8 week empiric trial of twice-daily PPI Troublesome
Gastroenterology 2016;150:1026 1030 April 2016 AGA Section 1027 Procedural intervention (3) Upper endoscopy indications 3 6 Non-response of symptoms to a 4 8 week empiric trial of twice-daily PPI Troublesome
National Digestive Diseases Information Clearinghouse
 Gastritis National Digestive Diseases Information Clearinghouse U.S. Department of Health and Human Services NATIONAL INSTITUTES OF HEALTH What is gastritis? Gastritis is a condition in which the stomach
Gastritis National Digestive Diseases Information Clearinghouse U.S. Department of Health and Human Services NATIONAL INSTITUTES OF HEALTH What is gastritis? Gastritis is a condition in which the stomach
Proton Pump Inhibitors Drug Class Prior Authorization Protocol
 Proton Pump Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medi-Cal P&T Approval Date: November 15, 2017 Effective Date: January 1, 2018 This policy has been developed through review
Proton Pump Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medi-Cal P&T Approval Date: November 15, 2017 Effective Date: January 1, 2018 This policy has been developed through review
Copy right protected Page 1
 DRUGS USED IN ULCERS AND GIT DISORDERS A peptic ulcer, also known as PUD or peptic ulcer disease is an ulcer of an area of the gastrointestinal tract that is usually acidic and thus extremely painful.
DRUGS USED IN ULCERS AND GIT DISORDERS A peptic ulcer, also known as PUD or peptic ulcer disease is an ulcer of an area of the gastrointestinal tract that is usually acidic and thus extremely painful.
GASTROESOPHAGEAL REFLUX DISEASE. William M. Brady
 Drugs of Today 1998, 34(1): 25-30 Copyright PROUS SCIENCE GASTROESOPHAGEAL REFLUX DISEASE William M. Brady Section of General Internal Medicine, Temple University School of Medicine, Philadelphia, Pennsylvania,
Drugs of Today 1998, 34(1): 25-30 Copyright PROUS SCIENCE GASTROESOPHAGEAL REFLUX DISEASE William M. Brady Section of General Internal Medicine, Temple University School of Medicine, Philadelphia, Pennsylvania,
Identifying patients who may benefit from stepping down PPI treatment
 CLINICAL AUDIT Identifying patients who may benefit from stepping down PPI treatment Valid to January 2024 bpac nz better medicin e This audit identifies patients who are prescribed the proton pump inhibitor
CLINICAL AUDIT Identifying patients who may benefit from stepping down PPI treatment Valid to January 2024 bpac nz better medicin e This audit identifies patients who are prescribed the proton pump inhibitor
Gastroesophageal Reflux Disease (GERD)
") Quality Department Guidelines for Clinical Care Ambulatory GERD Guideline Team Team Leader Joel J Heidelbaugh, MD Family Medicine Team Members R Van Harrison, PhD Learning Health Sciences Mark A McQuillan,
Quality Department Guidelines for Clinical Care Ambulatory GERD Guideline Team Team Leader Joel J Heidelbaugh, MD Family Medicine Team Members R Van Harrison, PhD Learning Health Sciences Mark A McQuillan,
Understanding GERD. & Stretta Therapy. GERD (gĕrd): Gastroesophageal Reflux Disease
: Gastroesophageal Reflux Disease") Understanding GERD & Stretta Therapy GERD (gĕrd): Gastroesophageal Reflux Disease What is GERD? When the muscle between your stomach and esophagus is weak, stomach contents like acid or bile can reflux
Understanding GERD & Stretta Therapy GERD (gĕrd): Gastroesophageal Reflux Disease What is GERD? When the muscle between your stomach and esophagus is weak, stomach contents like acid or bile can reflux
Gastrointestinal problems in individuals with CdLS. Peter Gillett Consultant Gastroenterologist RHSC Edinburgh UK Cork 2011
 Gastrointestinal problems in individuals with CdLS Peter Gillett Consultant Gastroenterologist RHSC Edinburgh UK Cork 2011 Major problems Gastro-oesophageal reflux and GORD Swallowing problems and
Gastrointestinal problems in individuals with CdLS Peter Gillett Consultant Gastroenterologist RHSC Edinburgh UK Cork 2011 Major problems Gastro-oesophageal reflux and GORD Swallowing problems and
Gastroesophageal reflux (GER) Gastroesophageal reflux (GER), the passage of gastric contents into the esophagus, is a normal physiologic process that
 Gastroesophageal reflux (GER), the passage of gastric contents into the esophagus, is a normal physiologic process that") Gastroesophageal reflux (GER) Gastroesophageal reflux (GER), the passage of gastric contents into the esophagus, is a normal physiologic process that may occur daily in healthy infants, children and adults.
Gastroesophageal reflux (GER) Gastroesophageal reflux (GER), the passage of gastric contents into the esophagus, is a normal physiologic process that may occur daily in healthy infants, children and adults.