UPDATE IN MIGRAINE MANAGEMENT
|
|
|
- Kenneth Hicks
- 5 years ago
- Views:
Transcription


1 UPDATE IN MIGRAINE MANAGEMENT Eric P. Baron, DO Cleveland Clinic Neurological Institute Center for Neurological Restoration Headache and Chronic Pain
2 Disclosures Some medications discussed may be used off label No relevant personal disclosures
3 Goals and Objectives Review migraine pathophysiology Discuss selection and use of acute migraine treatments and other management Review preventive strategies and options Discuss updates in new migraine treatments
4 Migraine Epidemiology 18% of women, 6% of men 38 million migraineurs in the US 12% of US population 1 in 4 households have someone w/ migraine
5 Migraine Societal Impact 2 nd leading cause of all global disability 2 nd leading cause of all neurological disease burden 50% of all neurologic disability Costs $20 billion/year 113 million lost work days/year
6 Migraine Under-treatment Nearly 1/2 of all migraine sufferers never diagnosed Majority of migraineurs do not seek medical care for their pain Only 4% of migraine sufferers who seek medical care consult headache and pain specialists
7 Migraine Diagnostic Criteria: A) At least 5 attacks fulfilling criteria B D B) Headache attacks lasting 4-72 hours (untreated or unsuccessfully treated) C) Headache has at least 2 of the following 4 characteristics: 1. unilateral location 2. pulsating quality 3. moderate or severe pain intensity 4. aggravation by or causing avoidance of routine physical activity (e.g. walking or climbing stairs) D) During headache at least 1 of the following: 1. nausea and/or vomiting 2. photophobia and phonophobia E) Not better accounted for by another ICHD-3 diagnosis
8 Migraine aura 25% have aura (classic migraine), 75% no aura (common migraine) 5-60 minutes in duration (up to 72 hrs for motor) Aura Types - Visual (most common) - Sensory (2 nd most common) - Speech and/or language (3 rd most common) - Motor (hemiplegic migraine) - Brainstem (previously basilar migraine) - Retinal
9 ID Migraine questionnaire screening tool Patient is given 3 questions - Have your headaches interfered with your ability to work, study, or do what you needed to do? - Have you felt nauseated or sick to your stomach when you have a headache? - Does light bother you when you have a headache (a lot more than when you don t have a headache)? Yes to 3 of these questions: 97% chance of migraine Yes to 2 of these questions: 93% chance of migraine Lipton RB, Dodick D, Sadovsky R et al (2003) A self-administered screener for migraine in primary care: the ID migraine validation study. Neurology 61:
10 Migraine is an ELECTRICAL NEUROLOGICAL event! The vascular theory of migraine is DEFUNCT!
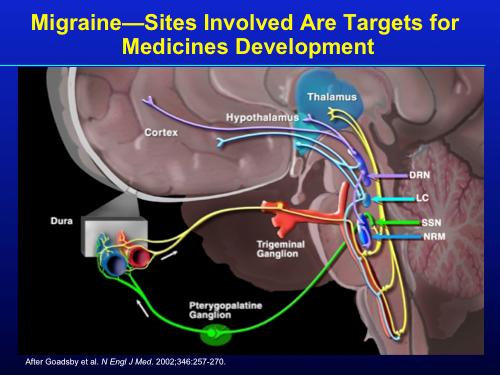
11 Migraine Pathophysiology 1. Site of initiation debated: Cortical spreading depression vs. brainstem generator 2. Spreading wave of neuronal activation and hyperemia (aura) 3. Followed by spreading wave of neuronal depression and oligemia at 3 mm/minute (aura)


12
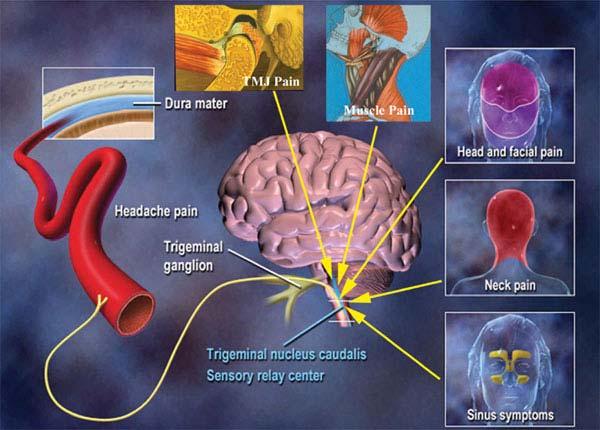
13 Migraine Pathophysiology 4. Trigeminovascular activation: release of inflammatory cytokines, neuroinflammatory peptides, and CGRP 5. Cerebral vasodilatation and neurogenic inflammation 6. Sensitized trigeminovascular pain signals travel to trigeminal ganglion (peripheral sensitization) 7. Pain signals travel from trigeminal ganglion to trigeminal nucleus caudalis thalamus cortex (central sensitization)

14
15
16
17 Standard of Care Goals of Acute Migraine Treatment 1. Treat attacks effectively, rapidly, consistently 2. Restore ability to function 3. Minimize need for back-up and rescue meds 4. Optimize self-care and reduce subsequent use of resources 5. Provide cost-effective management 6. Cause minimal or no adverse events
18 Treatment Strategy Stratified vs Step Care?
19 Stratified Care Treatment selection based on migraine severity and disability Supported by Class I evidence Stratified care more cost effective - May include initial use of more costly meds, but - ED/office visits + procedures Williams, et al. Pharmacoeconomics Sculpher, et al. Pharmacoeconomics. 2002
20 Step Care Treatment escalated within or across attacks If simple analgesics ineffective, other combos given later in same attack or for future attacks Triptans or DHE considered after other steps have failed Step care causes a delay in necessary migraine-specific administration Long process of trial and error; many patients lapse from care untreated = unnecessary pain and impairment
21 Stratified Care vs Step Care across 6 attacks: Headache Resolution Attacks (%) Stratified care Stepped care across attacks * * * hour 2 hours 4 hours Time post-dose *p<0.001 vs stepped care across attacks Lipton RB, et al. JAMA. 2000;284(20): Courtesy of Dr. Stewart Tepper, MD

22 Delay in migraine specific meds wastes time as migraine pathways become stronger and more refractory
23 2015: The Acute Treatment of Migraine in Adults: The American Headache Society Evidence Assessment of Migraine Pharmacotherapies
24
25 Mild-moderate attacks: 1) NSAIDs 2) Combination analgesics Treatment Strategy: Individualize Treatment Moderate-severe attacks or poor response to NSAIDs or combo analgesics: 1) Triptans 2) Dihydroergotamine (DHE)
26 NSAIDs Inhibit arachidonic acid cascade and trigeminovascular inflammation Inhibit dural plasma extravasation Help prevent central sensitization Use max dose possible for most efficacy Evidence based support as a 1st line option for mild-moderate disability
27 Triptans Sumatriptan: PO, SC, Needle-less SC, NS, breath-powered intranasal delivery system Zolmitriptan: NS, PO, ODT Rizatriptan: PO, ODT Almotriptan: PO Eletriptan: PO Sumatriptan/Naproxen: PO Frovatriptan: PO Naratriptan: PO
28 Triptans Group 1: - Faster onset, higher potency, higher 24 hr recurrence -Sumatriptan -Sumatriptan/Naproxen -Zolmitriptan -Rizatriptan -Almotriptan -Eletriptan Group 2: - Slower onset, lower potency, lower 24 hr recurrence -Naratriptan -Frovatriptan Rapoport AM, Tepper SJ, et al. CNS Drugs
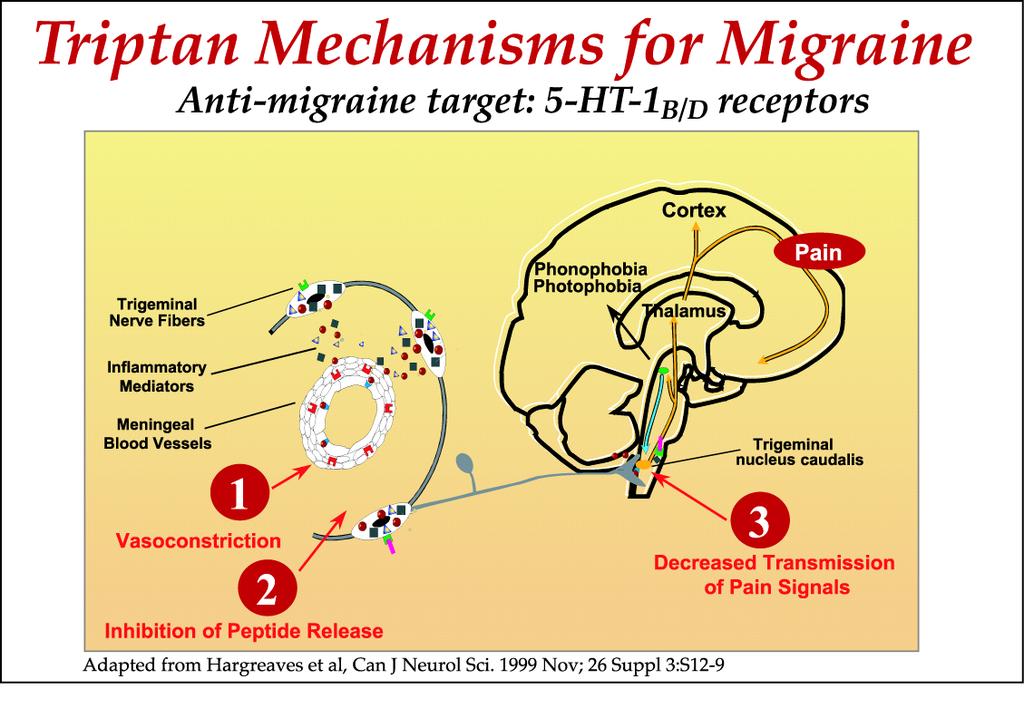
29 Triptans 5-HT1B agonists: - Constrict pain-producing meningeal blood vessels - Also present in brainstem, significance uncertain - Intracranial arteries > periphery arteries (coronary arteries) Coronary vasoconstriction up to 10-20% may occur MaassenVanDenBrink A, et al. Circulation MacIntyre PD, et al. Circulation. 1993
30 Triptans 5-HT1D agonists: - Presynaptically inhibit trigeminal peptide release - Inhibit trigeminal nucleus caudalis pain processing - Inhibit nausea/vomiting in nucleus tractus solitariuus Tepper SJ, Millson D. Expert Opin Drug Saf Tepper SJ. Med Clin North Am
31 Triptans End result: - Reversal of vasodilation - neurogenic inflammation - central pain signal transmission to thalamus, cortex - Cessation of ascending cortical pathways which lead to photo/phonophobia, N/V, central sensitization
32

33 Does it matter which triptan I pick??

34 Which Triptan Do I Pick? CORN
35 Contraindications Onset to peak pain Recurrence of migraine after treatment (within 24 hours?) Nausea and vomiting severity
36 Contraindications - Vascular disease (CAD, CVD, PAD) - Uncontrolled HTN - Pregnancy (Category C) - Breastfeeding (Sumatriptan ok) - Renal or hepatic failure - Sepsis - Prinz-Metal angina - Hemiplegic or basilar-type migraine
37 Contraindications Risk factors for arterial disease - Poorly controlled HTN, HLP, DM, smoking, premature CAD family hx (men < 55, women < 65), postmenopausal women 1 risk factor: ECG suggested in prescribing info >1 Framingham risk factor: further work-up suggested such as stress test
38 Onset to migraine peak pain Group 1 (quicker onset) vs. Group 2 (slower onset) - SC or NS triptan if: Patient wakes w/ migraines Peak pain within 30 minutes
39 Return of migraine after treatment If migraine recurrence occurs within 24 hours: - Combine triptan 1 st dose w/ NSAID (Naproxen) - Group 2 triptan (Naratriptan vs. Frovatriptan)
40 Nausea and vomiting severity If N/V occur early in attack or are severe: - SC or NS triptan should be used - *dissolvable tablets absorbed via GI tract, not sublingually
41 Triptan Pearls Sumatriptan: - Highest potency (SC) and quickest onset (SC+NS) of triptans - Greatest flexibility Rizatriptan: - Fastest onset of oral triptans - Greatest likelihood of 2h pain-free and sustained pain-free response - Propranolol increases its serum concentration so 5mg per dose if used together Rapoport AM, Tepper SJ, et al. CNS Drugs Rapoport AM, Tepper SJ. Arch Neurol
42 Zolmitriptan: - Most likely to treat persistent HA when 1st dose fails Almotriptan: - Group 1 triptan w/ least side effects Eletriptan: - Highest potential for drug interactions. Decrease dosage w/ CYP3A4 drugs macrolides, fungal, HIV, etc. Rapoport AM, Tepper SJ, et al. CNS Drugs Rapoport AM, Tepper SJ. Arch Neurol
43 Naratriptan: - The "gentle triptan", least side effects - Slower onset of action - Low 24 hr recurrence rate - Does not have monoamine oxidase metabolism, so can be given w/ MAOI (as can Eletriptan and Frovatriptan) Rapoport AM, Tepper SJ, et al. CNS Drugs Rapoport AM, Tepper SJ. Arch Neurol
44 Frovatriptan - Slower onset of action - Longest half life - Low 24 hr recurrence rate - Good choice to give night prior to expected migraine and known trigger (menstruation, travel, etc.) Rapoport AM, Tepper SJ, et al. CNS Drugs Rapoport AM, Tepper SJ. Arch Neurol
45 Triptan + NSAID Combination Increased efficacy and reduced recurrence for - Sumatriptan and Rizatriptan + NSAID - Rizatriptan + COX-2 inhibitors Krymchantowski A. Cephalalalgia 2001;21: Krymchantowski AV, Barbosa JS. Cephalalgia 2002; 22: Krymchantowski AV, Bigal ME. BMC Neurol 2004; 28; 4(1):10. Sumatriptan 85 mg/naproxen 500 mg combo pill: - Faster Sumatriptan Tmax w/ combo vs. Sumatriptan 100 mg alone (1h vs. 1.5 hrs) - Naproxen Cmax 36% lower w/ combo vs. Naproxen 550 mg alone - Naproxen Tmax 4 hrs later w/ combo vs. Naproxen 550 mg alone (5h vs. 1-2h)
46 The bad news on triptans 25% do not respond to triptans Only 1/3 pain-free at 2 hrs Only 25% remain pain-free
47 Ergots Dihydroergotamine (DHE), Ergotamine - Broader spectrum of receptors than triptans - Additional side effects possible, but additional efficacy in many triptan non-responders - Interact with adrenergic and dopaminergic receptors, 5-HT 1A, 1B, 1D, 1F, 2A, 2C, 3, 4 subtypes - Side effect profiles reflect agonist activity at: 5-HT1A receptors: nausea, dysphoria 5-HT2A and adrenergic receptors: peripheral vasoconstriction Dopamine D2 receptors: nausea, vomiting Bigal ME, Tepper SJ. Curr Pain Headache Rep Baron EP, Tepper SJ. Headache. 2010
48 Dihydroergotamine (DHE) IV, SC, IM, IN formulations, (oral inhalation pending FDA approval) IV DHE is very useful to break status migrainosus No triptan use in pre or post 24 hours of DHE Contraindications same as triptans except pregnancy is Category X
49 IV DHE Raskins Protocol 1. IV Antiemetic +/- IV Diphenhydramine 30 mins prior to IV DHE (1 mg/1 ml) mg IV. Then, 0.25 mg q15 mins until 1 of the following: a) HA resolves b) Severe nausea or other intolerable side effects occur c) Cumulative dose of 1 mg reached 3. Repeat max tolerated dose (up to 1 mg) q8h with IV Antiemetic +/- IV Diphenhydramine 30 mins prior to IV DHE **AAN Practice Parameter Guidelines suggest IV DHE safe up to 3 mg/day and 20 mg/week (packaging says 6 mg/week)
50 IM / SC DHE 1 mg (1 ml) at onset of migraine Then, q1h x 2 for a max dose of 3 mg/attack Status migrainosus: Once every 8 hrs x 3-5 days or until HA free x 24 hrs IM and SC DHE are limited to 3 mg/day and 20 mg/week (packaging says 6 mg/week)
51 IN DHE Insert in nostril, aim away from face, don't sniff 1 spray in each nostril (0.5 mg each nostril = 1 mg total dose) In 15 minutes, repeat 1 spray in each nostril (0.5 mg each nostril = 1 mg total dose) Total treatment dose: 4 sprays = 2 mg; May repeat this cycle q8h x 72h or until HA is resolved (whichever comes first) Per packaging, max dose: 4 sprays (2mg)/attack, 6 sprays (3 mg)/day and 8 sprays (4 mg)/week. (As prior, we often use higher doses)
52 When to consider DHE? Long migraines including menstrually-related migraines Migraines w/ high 24 hr recurrence Waking migraines (therapeutic triptan window missed) Moderate to severe pain with central sensitization (allodynia) when triptans less effective Baron EP, Tepper SJ. Headache
53 When to consider DHE? To break status migrainosis (migraine lasting > 72 hours) Repetitively for rescue Repetitively as a bridge to wean a patient out of medication overuse headache With nausea and vomiting, when a non-oral alternative is necessary Baron EP, Tepper SJ. Headache

54 Butalbital Meds and Opiates/Opioids No class I studies support use of butalbital-containing meds in acute migraine treatment Butalbital meds and opiates/opioids pose a high risk of MOH (Rebound HA), dependency, best avoided - >5 days/month for butalbital - >8 days/month for opiates/opioids Limited role for opiate/opioid use in acute migraine treatment - Occasionally when abortives have failed, as rescue - When standard abortives are contraindicated


55 RESCUE
56 RESCUE AND/OR CONTRAINDICATIONS TO STANDARD MEDS Anti-emetics IV/PO - Prochlorperazine 10 mg, Metoclopramide 10 mg, Dolasetron 12.5 mg, Ondansetron 4-8 mg, Granisetron 1 mg, Promethazine 25 mg Anticonvulsants IV/PO - Valproic acid mg IV - Valproic acid 1000 mg PO QHS x 5 days, then 500 mg QHS x 5 days Magnesium IV - 2 g IV NSAIDS IV/PO - Ketorolac 30 mg IV; 60 mg IM - Ketorolac 10 mg PO TID until HA free x 24 hours, or have used 5 days
57 RESCUE AND/OR CONTRAINDICATIONS TO STANDARD MEDS Steroids IV/PO - Dexamethasone 4-10 mg IV - Dexamethasone 4 mg PO TID day 1, BID day 2, once day 3 - Prednisone 60 mg PO x 5 days, then decrease by 10 mg/day - Methylprednisolone mg IV Muscle Relaxers IV/PO - Methocarbamol 1-2 g IV - Chlorzoxazone mg PO qid x 5 days Neuroleptics/Antipsychotics PO - Olanzapine, Quetiapine, Haloperidol
58 MOH / Rebound Headache Causes of MOH - NSAIDS or Triptans: > 10 days/month - Opioids/Opiates: > 8 days/month - Butalbital meds > 5 days/month Weaning/detox - Headaches worsen before improving - Use bridge (prednisone, DHE, etc.) - Can take 4-8 weeks to improve AFTER wean Bigal ME, Lipton RB. Overuse of acute migraine medications and migraine chronification. Curr Pain Headache Rep Aug;13(4):301-7.
59 Migraine Prevention Initiate meds w/ highest level of evidence Initiate meds w/ lowest effective dose. Increase slowly every couple weeks until: - Benefit, - Side effects, or - Ineffective trial Adequate trial mandatory weeks to start taking effect months for full effect (assuming therapeutic dose)
60 Migraine Prevention Avoid/eliminate interfering meds - MOH interferes with preventive med efficacy Long-acting formulations improve compliance If doing well at 6 months, consider tapering off Limit polypharmacy, take coexisting conditions into account (HTN, epilepsy, mood disorders, weight, etc.) - Treat migraine and coexistent conditions if possible
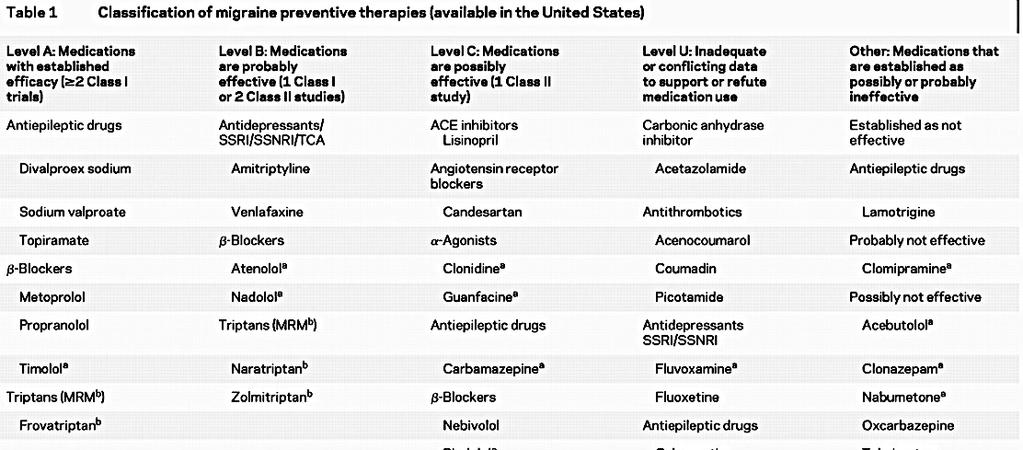
61 2012: American Headache Society/American Academy of Neurology Guidelines for Prevention of Episodic Migraine
62
63
64 Chronic Migraine Chronic migraine: - HA 15 days/month for 3 months, which, on at least 8 days/month, has migraine features Onabotulinum Toxin Type A - Only FDA-approved treatment of chronic migraine (approved for age 18)

65 OMT 70% of migraine attacks associated with neck pain - Trigeminocervical Nucleus OMT effective for both preventive + acute treatments directed at these regions
66 WHAT S NEW??
67 Calcitonin Gene-Related Peptide (CGRP) Antagonists Pathophysiology - CGRP released from trigeminal nerves during migraine - Blood vessel dilatation, inflammation - Cascade of pain, photo/phonophobia, nausea/vomiting 2 groups - Monoclonal antibodies - Gepants
68 Calcitonin Gene-Related Peptide (CGRP) Antagonists - Mabs Monoclonal Antibodies (Mabs) - Larger size, cannot cross blood-brain barrier - Cut migraine days by 50% in 50% of pts; small % eliminate migraine CGRP receptor antagonist (1) - Erenumab-aooe FDA approved 5/17/18 for migraine prevention in adults (episodic, chronic) Monthly injection, 70 mg or 140 mg
69 Calcitonin Gene-Related Peptide (CGRP) Antagonists - Mabs Target CGRP (3) - Fremanezumab-vfrm FDA approved 9/14/18 for migraine prevention in adults Monthly injection 225 mg, or 675 mg quarterly injections - Galcanezumab FDA approved 9/28/18 for migraine prevention in adults 240 mg loading dose x 1 in 2 consecutive 120 mg injections, followed by 120 mg monthly injection - Eptinezumab coming soon
70 Calcitonin Gene-Related Peptide (CGRP) Antagonists - Gepants Small Molecules (Gepants) - Smaller size, can cross blood-brain barrier - Gepants in trials (all PO) Acute/abortive: Rimegepant, Ubrogepant Preventive: Atogepant, BHV Expected to be a safe option in vascular disease (where triptans are contraindicated)


 2 hours 2 needed)")


71 Vagus Nerve Stimulator FDA approved 1/2018 for acute migraine tx 2 two-min stimulations 20 mins 2 two-min stimulations (if needed) 2 hours 2 two-min stimulations (if needed) Significant relief as soon as 30 mins 50% of pts had mild or no pain at 2 hrs for 50% of all HAs

72 To Image or Not to Image. That is the Question
73 Conclusions 1. Educate pts about migraine, its treatment and encourage participation in management (triggers, HA diaries to determine need for prevention, etc.). 2. Use migraine specific meds (triptans, DHE) early with moderate-severe migraine and those poorly responsive to NSAIDS or combination analgesics. 3. Tailor triptan use based on patient and migraine characteristics (CORN).
74 Conclusions 4. Consider a self-administered rescue med for severe migraine failing all other treatments. 5. Guard against medication-overuse headache (MOH; rebound HA). Causes of MOH: -NSAIDS or triptans: > 10 days/month -Opioids: > 8 days/month -Butalbital compounds > 5 days/month 6. Preventives should target other comorbidities, at same time of decreasing overall HA burden.

75
Adult & Pediatric Patients. Stanford Health Care, Division Pain Medicine
 Acute Treatment Strategies in Adult & Pediatric Patients Theresa Mallick Searle, MS, RN BC, ANP BC Disclosures Speakers Bureau: Allergan, Depomed Acute Treatment Strategies in Adult & Pediatric Patients
Acute Treatment Strategies in Adult & Pediatric Patients Theresa Mallick Searle, MS, RN BC, ANP BC Disclosures Speakers Bureau: Allergan, Depomed Acute Treatment Strategies in Adult & Pediatric Patients
Faculty Disclosures. Learning Objectives. Acute Treatment Strategies
 WWW.AMERICANHEADACHESOCIETY.ORG Acute Treatment Strategies Content developed by: Lawrence C. Newman, MD, FAHS Donna Gutterman, PharmD Faculty Disclosures LAWRENCE C. NEWMAN, MD, FAHS Dr. Newman has received
WWW.AMERICANHEADACHESOCIETY.ORG Acute Treatment Strategies Content developed by: Lawrence C. Newman, MD, FAHS Donna Gutterman, PharmD Faculty Disclosures LAWRENCE C. NEWMAN, MD, FAHS Dr. Newman has received
ADVANCES IN MIGRAINE MANAGEMENT
 ADVANCES IN MIGRAINE MANAGEMENT Joanna Girard Katzman, M.D.MSPH Assistant Professor, Dept. of Neurology Project ECHO, Chronic Pain Program University of New Mexico Outline Migraine throughout the decades
ADVANCES IN MIGRAINE MANAGEMENT Joanna Girard Katzman, M.D.MSPH Assistant Professor, Dept. of Neurology Project ECHO, Chronic Pain Program University of New Mexico Outline Migraine throughout the decades
ONZETRA XSAIL (sumatriptan) nasal powder
 nasal powder") ONZETRA XSAIL (sumatriptan) nasal powder Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
ONZETRA XSAIL (sumatriptan) nasal powder Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
SUMAVEL DOSEPRO (sumatriptan succinate) solution for injection
 solution for injection") SUMAVEL DOSEPRO (sumatriptan succinate) solution for injection Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit
SUMAVEL DOSEPRO (sumatriptan succinate) solution for injection Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit
HMFP Comprehensive Headache Center Department of Anesthesia, Critical Care and Pain Medicine Beth Israel Deaconess Medical Center Instructor in
 HMFP Comprehensive Headache Center Department of Anesthesia, Critical Care and Pain Medicine Beth Israel Deaconess Medical Center Instructor in Anesthesia and Neurology Harvard Medical School Limited time
HMFP Comprehensive Headache Center Department of Anesthesia, Critical Care and Pain Medicine Beth Israel Deaconess Medical Center Instructor in Anesthesia and Neurology Harvard Medical School Limited time
MIGRAINE UPDATE. Objectives & Disclosures. Learn techniques used to diagnose headaches. Become familiar with medications used for headache treatment.
 MIGRAINE UPDATE Karen L. Bremer, MD November 16, 2018 Objectives & Disclosures Learn techniques used to diagnose headaches. Become familiar with medications used for headache treatment. Disclosure: I am
MIGRAINE UPDATE Karen L. Bremer, MD November 16, 2018 Objectives & Disclosures Learn techniques used to diagnose headaches. Become familiar with medications used for headache treatment. Disclosure: I am
Clinical Learning Days November 10, 2017
 Migraine Clinical Learning Days November 10, 2017 Alyssa Lettich. MD Neurosciences Institute/Neurosciences Clinical Program Medical Director Headache Disclosures: none Learning Objectives: At the conclusion
Migraine Clinical Learning Days November 10, 2017 Alyssa Lettich. MD Neurosciences Institute/Neurosciences Clinical Program Medical Director Headache Disclosures: none Learning Objectives: At the conclusion
Update on Diagnosis and Management of Migraines
 Update on Diagnosis and Management of Migraines Joel J. Heidelbaugh, MD, FAAFP, FACG Clinical Professor Departments of Family Medicine and Urology University of Michigan Learning Objectives To distinguish
Update on Diagnosis and Management of Migraines Joel J. Heidelbaugh, MD, FAAFP, FACG Clinical Professor Departments of Family Medicine and Urology University of Michigan Learning Objectives To distinguish
Disclosures. Triptans for Kids 5/16/13
 5/16/13 Disclosures Triptans for Kids Amy A. Gelfand, MD GelfandA@neuropeds.ucsf.edu Departments of Neurology and Pediatrics UCSF Child Neurology and Headache Center I receive grant funding from: NIH/NINDS
5/16/13 Disclosures Triptans for Kids Amy A. Gelfand, MD GelfandA@neuropeds.ucsf.edu Departments of Neurology and Pediatrics UCSF Child Neurology and Headache Center I receive grant funding from: NIH/NINDS
ACUTE MIGRAINE: OLD AND NEW DRUGS JOHN ROBROCK MD FORT WILLIAM FAMILY HEALTH TEAM
 ACUTE MIGRAINE: OLD AND NEW DRUGS JOHN ROBROCK MD FORT WILLIAM FAMILY HEALTH TEAM Conflict of Interest Declaration: Nothing to Disclose Presenter: John Robrock, MD Title of Presentation: Acute Migraine:
ACUTE MIGRAINE: OLD AND NEW DRUGS JOHN ROBROCK MD FORT WILLIAM FAMILY HEALTH TEAM Conflict of Interest Declaration: Nothing to Disclose Presenter: John Robrock, MD Title of Presentation: Acute Migraine:
ACUTE TREATMENT FOR MIGRAINE. Cristina Tassorelli
 The European Headache School 2012 ACUTE TREATMENT FOR MIGRAINE Cristina Tassorelli Headache Science Centre, IRCCS Neurological Institute C. Mondino Foundation - Pavia University Centre for Adaptive Disorders
The European Headache School 2012 ACUTE TREATMENT FOR MIGRAINE Cristina Tassorelli Headache Science Centre, IRCCS Neurological Institute C. Mondino Foundation - Pavia University Centre for Adaptive Disorders
The best defense is a good offense. Optimizing the Acute Treatment of Migraine. Disclosures 11/10/2017
 Optimizing the Acute Treatment of Migraine Brian M. Plato, DO, FAHS Norton Neuroscience Institute Louisville, KY Disclosures Speakers Bureau (personal): Allergan, Depomed, Avanir Research Funding (paid
Optimizing the Acute Treatment of Migraine Brian M. Plato, DO, FAHS Norton Neuroscience Institute Louisville, KY Disclosures Speakers Bureau (personal): Allergan, Depomed, Avanir Research Funding (paid
Clinical case. Clinical case 3/15/2018 OVERVIEW. Refractory headaches and update on novel treatment. Refractory headache.
 OVERVIEW Refractory headaches and update on novel treatment Definition of refractory headache Treatment approach Medications Neuromodulation In the pipeline Juliette Preston, MD OHSU Headache Center Refractory
OVERVIEW Refractory headaches and update on novel treatment Definition of refractory headache Treatment approach Medications Neuromodulation In the pipeline Juliette Preston, MD OHSU Headache Center Refractory
A case of a patient with chronic headache. Focus on Migraine. None related to the presentation Grants to conduct clinical trials from: Speaker bureau:
 Chronic Daily Headache Bassel F. Shneker, MD, MBA Associate Professor Vice Chair, OSU Neurology The Ohio State University Wexner Medical Center Financial Disclosures None related to the presentation Grants
Chronic Daily Headache Bassel F. Shneker, MD, MBA Associate Professor Vice Chair, OSU Neurology The Ohio State University Wexner Medical Center Financial Disclosures None related to the presentation Grants
Sumatriptan Tablets, Nasal Spray (Imitrex), Nasal Powder (Onzetra Xsail), sumatriptan and naproxen sodium (Treximet tablets)
, Nasal Powder (Onzetra Xsail), sumatriptan and naproxen sodium (Treximet tablets)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 0 Subject: Sumatriptan Page: 1 of 6 Last Review Date: November 30, 2018 Sumatriptan Description Sumatriptan
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 0 Subject: Sumatriptan Page: 1 of 6 Last Review Date: November 30, 2018 Sumatriptan Description Sumatriptan
How do we treat migraine? New SIGN Guidelines
 How do we treat migraine? New SIGN Guidelines Managing your migraine Migraine Trust, Edinburgh 2018 Callum Duncan Consultant Neurologist Aberdeen Royal Infirmary Chair SIGN Guideline 155 Premonitory Mood
How do we treat migraine? New SIGN Guidelines Managing your migraine Migraine Trust, Edinburgh 2018 Callum Duncan Consultant Neurologist Aberdeen Royal Infirmary Chair SIGN Guideline 155 Premonitory Mood
I have no financial relationships to disclose. I will not discuss investigational use of medication in my presentation.
 I have no financial relationships to disclose. I will not discuss investigational use of medication in my presentation. In 1962, Bille published landmark epidemiologic survey of headache among 9,000 school
I have no financial relationships to disclose. I will not discuss investigational use of medication in my presentation. In 1962, Bille published landmark epidemiologic survey of headache among 9,000 school
Headache A Practical Approach
 Headache A Practical Approach Integrated Pain Symposium December 1, 2017 Alyssa Lettich. MD Neurosciences Institute/Neurosciences Clinical Program Medical Director Headache and Pain Development Teams Disclosures:
Headache A Practical Approach Integrated Pain Symposium December 1, 2017 Alyssa Lettich. MD Neurosciences Institute/Neurosciences Clinical Program Medical Director Headache and Pain Development Teams Disclosures:
Zomig. Zomig / Zomig-ZMT (zolmitriptan) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.22 Subject: Zomig Page: 1 of 5 Last Review Date: November 30, 2018 Zomig Description Zomig / Zomig-ZMT
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.22 Subject: Zomig Page: 1 of 5 Last Review Date: November 30, 2018 Zomig Description Zomig / Zomig-ZMT
Regulatory Status FDA approved indication: Migranal Nasal Spray is indicated for the acute treatment of migraine headaches with or without aura (1).
.") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.60 Subject: Migranal Nasal Spray Page: 1 of 5 Last Review Date: November 30, 2018 Migranal Nasal Spray
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.60 Subject: Migranal Nasal Spray Page: 1 of 5 Last Review Date: November 30, 2018 Migranal Nasal Spray
Migraine Management. Dr Helen Brown Director of Neurology and Stroke The Princess Alexandra Hospital
 Migraine Management Dr Helen Brown Director of Neurology and Stroke The Princess Alexandra Hospital Referral Criteria for Migraine Migraine Management Migraine Diagnosis Spot on Health Migraine pathway
Migraine Management Dr Helen Brown Director of Neurology and Stroke The Princess Alexandra Hospital Referral Criteria for Migraine Migraine Management Migraine Diagnosis Spot on Health Migraine pathway
Daniel Kassicieh, DO, FAAN
 Daniel Kassicieh, DO, FAAN Migraine a Disease Process Migraine is a chronic disease process similar to many other chronic medical conditions Migraine has a low mortality but high morbidity 38 million Americans
Daniel Kassicieh, DO, FAAN Migraine a Disease Process Migraine is a chronic disease process similar to many other chronic medical conditions Migraine has a low mortality but high morbidity 38 million Americans
Sumatriptan Tablets, Nasal Spray (Imitrex), Nasal Powder (Onzetra Xsail), sumatriptan and naproxen sodium (Treximet tablets)
, Nasal Powder (Onzetra Xsail), sumatriptan and naproxen sodium (Treximet tablets)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 05.70.10 Subject: Sumatriptan Page: 1 of 6 Last Review Date: March 16, 2018 Sumatriptan Description Sumatriptan
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 05.70.10 Subject: Sumatriptan Page: 1 of 6 Last Review Date: March 16, 2018 Sumatriptan Description Sumatriptan
Prevention and Treatment of Migraines CAITLIN BARNES, PHARM.D. CANDIDATE AMBULATORY CARE JOE CAMMILLERI, PHARM.D. NATOHYA MALLORY, PHARM.D.
 Prevention and Treatment of Migraines CAITLIN BARNES, PHARM.D. CANDIDATE AMBULATORY CARE JOE CAMMILLERI, PHARM.D. NATOHYA MALLORY, PHARM.D. Objectives Present patient case Review epidemiology/pathophysiology
Prevention and Treatment of Migraines CAITLIN BARNES, PHARM.D. CANDIDATE AMBULATORY CARE JOE CAMMILLERI, PHARM.D. NATOHYA MALLORY, PHARM.D. Objectives Present patient case Review epidemiology/pathophysiology
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 CGRP Page 1 of 13 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: CGRP (calcitonin gene-related peptide) Prime Therapeutics will review Prior Authorization requests
CGRP Page 1 of 13 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: CGRP (calcitonin gene-related peptide) Prime Therapeutics will review Prior Authorization requests
10/17/2017 CHRONIC MIGRAINES BOTOX: TO INJECT OR NOT INJECT? IN CHRONIC MIGRAINE PROPHYLAXIS OBJECTIVES PATIENT CASE EPIDEMIOLOGY EPIDEMIOLOGY
 BOTOX: TO INJECT OR NOT INJECT? IN CHRONIC MIGRAINE PROPHYLAXIS OBJECTIVES JENNIFER SHIN, PHARMD PGY2 AMBULATORY CARE PHARMACY RESIDENT COMMUNITYCARE HEALTH CENTERS PHARMACOTHERAPY ROUNDS OCTOBER 20, 2017
BOTOX: TO INJECT OR NOT INJECT? IN CHRONIC MIGRAINE PROPHYLAXIS OBJECTIVES JENNIFER SHIN, PHARMD PGY2 AMBULATORY CARE PHARMACY RESIDENT COMMUNITYCARE HEALTH CENTERS PHARMACOTHERAPY ROUNDS OCTOBER 20, 2017
Headache. Section 1. Migraine headache. Clinical presentation
 Section 1 Headache Migraine headache 1 Clinical presentation It is important to recognize just how significant a problem migraine headache is. It has been estimated that migraine affects 11% of the United
Section 1 Headache Migraine headache 1 Clinical presentation It is important to recognize just how significant a problem migraine headache is. It has been estimated that migraine affects 11% of the United
Management options for Migraine. Prof. Dr. Khwaja Nazimuddin Head Dept. of Internal Medicine BIRDEM
 Management options for Migraine Prof. Dr. Khwaja Nazimuddin Head Dept. of Internal Medicine BIRDEM Assessment The Migraine Disability Assessment Score MIDAS Complete loss of work Partial loss of work Off
Management options for Migraine Prof. Dr. Khwaja Nazimuddin Head Dept. of Internal Medicine BIRDEM Assessment The Migraine Disability Assessment Score MIDAS Complete loss of work Partial loss of work Off
Migraine: Past, Present and Future Edward O Sullivan September 12 th 2015 Dublin 12/09/2015
 1 Migraine: Past, Present and Future Edward O Sullivan September 12 th 2015 Dublin Tour de France 2015: Mark Renshaw Yesterday at the end of the stage 17 I came down with a migraine before the final climb
1 Migraine: Past, Present and Future Edward O Sullivan September 12 th 2015 Dublin Tour de France 2015: Mark Renshaw Yesterday at the end of the stage 17 I came down with a migraine before the final climb
Current Migraine Treatment Therapy. Daniel Kassicieh, DO, FAAN
 Current Migraine Treatment Therapy Daniel Kassicieh, DO, FAAN Migraine a Disease Process Migraines are a chronic disease process similar to many other chronic medical conditions Migraine has a low mortality
Current Migraine Treatment Therapy Daniel Kassicieh, DO, FAAN Migraine a Disease Process Migraines are a chronic disease process similar to many other chronic medical conditions Migraine has a low mortality
Index. Prim Care Clin Office Pract 31 (2004) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Prim Care Clin Office Pract 31 (2004) 441 447 Index Note: Page numbers of article titles are in boldface type. A Abscess, brain, headache in, 388 Acetaminophen for migraine, 406 407 headache from, 369
Prim Care Clin Office Pract 31 (2004) 441 447 Index Note: Page numbers of article titles are in boldface type. A Abscess, brain, headache in, 388 Acetaminophen for migraine, 406 407 headache from, 369
Get ahead of the ACHE: Monoclonal Antibodies in Migraine Prevention
 Get ahead of the ACHE: Monoclonal Antibodies in Migraine Prevention Amanda Janisch, PharmD PGY2 Ambulatory Care Pharmacy Resident MCHS SWMN, Mankato, MN 2018 MFMER slide-1 Disclosures No financial interest
Get ahead of the ACHE: Monoclonal Antibodies in Migraine Prevention Amanda Janisch, PharmD PGY2 Ambulatory Care Pharmacy Resident MCHS SWMN, Mankato, MN 2018 MFMER slide-1 Disclosures No financial interest
Acute Migraine Treatment: What you and your family should know to help you make the best choices with your doctor
 Acute Migraine Treatment: What you and your family should know to help you make the best choices with your doctor TAKE CONTROL OF YOUR MIGRAINES! ABOUT THIS PATIENT GUIDE: Migraine attacks are often debilitating
Acute Migraine Treatment: What you and your family should know to help you make the best choices with your doctor TAKE CONTROL OF YOUR MIGRAINES! ABOUT THIS PATIENT GUIDE: Migraine attacks are often debilitating
10/31/2017 PRIMARY CARE AND HEADACHE DISCLOSURES WHERE DO THOSE WITH HEADACHE SEEK MEDICAL CARE? Primary Care 67%
 PRIMARY CARE AND HEADACHE Sonja Potrebic MD PhD Regional Headache Specialist Kaiser LAMC 1 WHERE DO THOSE WITH HEADACHE SEEK MEDICAL CARE? Column1 Primary Care 67% Primary Care Headache Specialty Other
PRIMARY CARE AND HEADACHE Sonja Potrebic MD PhD Regional Headache Specialist Kaiser LAMC 1 WHERE DO THOSE WITH HEADACHE SEEK MEDICAL CARE? Column1 Primary Care 67% Primary Care Headache Specialty Other
Zomig. Zomig / Zomig-ZMT (zolmitriptan) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.22 Subject: Zomig Page: 1 of 5 Last Review Date: March 16, 2018 Zomig Description Zomig / Zomig-ZMT
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.22 Subject: Zomig Page: 1 of 5 Last Review Date: March 16, 2018 Zomig Description Zomig / Zomig-ZMT
10/19/2018. Disclosures MIGRAINE PROPHYLAXIS. Objectives. Definitions Slide. What do you think the aooe stands for at the end of erenumab-aooe?
 Disclosures MIGRAINE PROPHYLAXIS Erenumab-aooe (AIMOVIG TM ) Calcitonin Gene Related Peptide Receptor Antagonist No conflicts of interest to disclose Chelsey Roscoe, PharmD PGY1 Resident - CTVHCS 2 3 Definitions
Disclosures MIGRAINE PROPHYLAXIS Erenumab-aooe (AIMOVIG TM ) Calcitonin Gene Related Peptide Receptor Antagonist No conflicts of interest to disclose Chelsey Roscoe, PharmD PGY1 Resident - CTVHCS 2 3 Definitions
Case Presentation. Case Presentation. Case Presentation. Truths about Headaches (2017) Most headaches were muscle-tension headaches
 Most headaches were muscle-tension headaches") Agenda Case presentation Migraine Morphology Primary and Premonitory Phase Secondary Headache Aura Headache Primer on Pain Medication Overuse Headache Case Presentation RT is a 25 year old woman with daily
Agenda Case presentation Migraine Morphology Primary and Premonitory Phase Secondary Headache Aura Headache Primer on Pain Medication Overuse Headache Case Presentation RT is a 25 year old woman with daily
Jessica Ailani MD FAHS Director, Georgetown Headache Center Associate Professor Neurology Medstar Georgetown University Hospital
 Jessica Ailani MD FAHS Director, Georgetown Headache Center Associate Professor Neurology Medstar Georgetown University Hospital Honorarium from Current Pain and Headache Reports; Section Editor Unusual
Jessica Ailani MD FAHS Director, Georgetown Headache Center Associate Professor Neurology Medstar Georgetown University Hospital Honorarium from Current Pain and Headache Reports; Section Editor Unusual
MEASURE #1: MEDICATION PRESCRIBED FOR ACUTE MIGRAINE ATTACK Headache
 MEASURE #1: MEDICATION PRESCRIBED FOR ACUTE MIGRAINE ATTACK Headache Measure Description Percentage of patients age 12 years and older with a diagnosis of migraine who were prescribed a guideline recommended
MEASURE #1: MEDICATION PRESCRIBED FOR ACUTE MIGRAINE ATTACK Headache Measure Description Percentage of patients age 12 years and older with a diagnosis of migraine who were prescribed a guideline recommended
Management of headache
 Management of headache TJ Steiner Imperial College London Based on European principles of management of common headache disorders TJ Steiner, K Paemeleire, R Jensen, D Valade, L Savi, MJA Lainez, H-C Diener,
Management of headache TJ Steiner Imperial College London Based on European principles of management of common headache disorders TJ Steiner, K Paemeleire, R Jensen, D Valade, L Savi, MJA Lainez, H-C Diener,
TABLE 1. Current Diagnostic Criteria for Migraine Without Aura 2 A. At least 5 attacks fulfilling criteria B-D B. Headache attacks lasting 4-72 hours
 ANSWERS CONCISE TO FREQUENTLY REVIEW ASKED QUESTIONS FOR CLINICIANS ABOUT MIGRAINE Answers to Frequently Asked Questions About Migraine IVAN GARZA, MD, AND JERRY W. SWANSON, MD Migraine is a common primary
ANSWERS CONCISE TO FREQUENTLY REVIEW ASKED QUESTIONS FOR CLINICIANS ABOUT MIGRAINE Answers to Frequently Asked Questions About Migraine IVAN GARZA, MD, AND JERRY W. SWANSON, MD Migraine is a common primary
Faculty Disclosure. Karen L. Bremer, MD. Dr. Bremer has listed no financial interest/arrangement that would be considered a conflict of interest.
 Faculty Disclosure Karen L. Bremer, MD Dr. Bremer has listed no financial interest/arrangement that would be considered a conflict of interest. HEADACHE UPDATE Karen L. Bremer, MD November 10, 2017 karen.bremer@creighton.edu
Faculty Disclosure Karen L. Bremer, MD Dr. Bremer has listed no financial interest/arrangement that would be considered a conflict of interest. HEADACHE UPDATE Karen L. Bremer, MD November 10, 2017 karen.bremer@creighton.edu
A New Era of Migraine Management: The Challenging Landscape in Prevention
 Provided by MediCom Worldwide, Inc. Supported by an educational grant from Teva Pharmaceuticals What is a Neuropeptide? Small chains of amino acids released by neural cells (neurons or glial cells) to
Provided by MediCom Worldwide, Inc. Supported by an educational grant from Teva Pharmaceuticals What is a Neuropeptide? Small chains of amino acids released by neural cells (neurons or glial cells) to
Çiçek Wöber-Bingöl HEADACHE UNIT FOR CHILDREN AND ADOLESCENCE
 Headache in children and adolescents Çiçek Wöber-Bingöl HEADACHE UNIT FOR CHILDREN AND ADOLESCENCE Dept. of Psychiatry of Childhood and Adolescence Medical University of Vienna, Vienna, Austria Impact
Headache in children and adolescents Çiçek Wöber-Bingöl HEADACHE UNIT FOR CHILDREN AND ADOLESCENCE Dept. of Psychiatry of Childhood and Adolescence Medical University of Vienna, Vienna, Austria Impact
MIGRAINE A MYSTERY HEADACHE
 MIGRAINE A MYSTERY HEADACHE The migraine is a chronic neurological disease that is characterized by moderate to severe episodes of headache that is mostly associated with other central nervous system (CNS)
MIGRAINE A MYSTERY HEADACHE The migraine is a chronic neurological disease that is characterized by moderate to severe episodes of headache that is mostly associated with other central nervous system (CNS)
THE WOMAN WHO COULD NOT DECIDE WHICH MEDICATION TO TAKE
 Rapoport Ch 05.qxd 10/15/08 1:06 PM Page 25 CHAPTER 5 THE WOMAN WHO COULD NOT DECIDE WHICH MEDICATION TO TAKE ALLAN PURDY, MD, FRCPC FRED SHEFTELL, MD ALAN RAPOPORT, MD STEWART J. TEPPER, MD Case History
Rapoport Ch 05.qxd 10/15/08 1:06 PM Page 25 CHAPTER 5 THE WOMAN WHO COULD NOT DECIDE WHICH MEDICATION TO TAKE ALLAN PURDY, MD, FRCPC FRED SHEFTELL, MD ALAN RAPOPORT, MD STEWART J. TEPPER, MD Case History
CGRP, MONOCLONAL ANTIBODIES AND SMALL MOLECULES (-GEPANTS)
") CGRP, MONOCLONAL ANTIBODIES AND SMALL MOLECULES (-GEPANTS) Hans-Christoph Diener Senior Professor of Clinical Neurosciences University Duisburg-Essen Germany CGRP, Monoclonal Antibodies and Small Molecules
CGRP, MONOCLONAL ANTIBODIES AND SMALL MOLECULES (-GEPANTS) Hans-Christoph Diener Senior Professor of Clinical Neurosciences University Duisburg-Essen Germany CGRP, Monoclonal Antibodies and Small Molecules
Goals. Primary Headache Syndromes. One-Year Prevalence of Common Headache Disorders
 Goals One-Year Prevalence of Common Headache Disorders Impact of primary headache syndromes Non pharmacologic Rx of migraine individualized to patient triggers Complementary and alternative Rx of migraine
Goals One-Year Prevalence of Common Headache Disorders Impact of primary headache syndromes Non pharmacologic Rx of migraine individualized to patient triggers Complementary and alternative Rx of migraine
Disclosures. Objectives 6/2/2017
 Classification: Migraine and Trigeminal Autonomic Cephalalgias Lauren Doyle Strauss, DO, FAHS Assistant Professor, Child Neurology Assistant Director, Child Neurology Residency @StraussHeadache No disclosures
Classification: Migraine and Trigeminal Autonomic Cephalalgias Lauren Doyle Strauss, DO, FAHS Assistant Professor, Child Neurology Assistant Director, Child Neurology Residency @StraussHeadache No disclosures
Sumatriptan Injection (Imitrex / Alsuma / Sumavel / Zembrace)
") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.11 Subject: Sumatriptan Injection Page: 1 of 6 Last Review Date: March 16, 2018 Sumatriptan Injection
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.11 Subject: Sumatriptan Injection Page: 1 of 6 Last Review Date: March 16, 2018 Sumatriptan Injection
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 CGRP Page 1 of 8 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: CGRP (calcitonin gene-related peptide) Prime Therapeutics will review Prior Authorization requests
CGRP Page 1 of 8 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: CGRP (calcitonin gene-related peptide) Prime Therapeutics will review Prior Authorization requests
An Overview of MOH. ALAN M. Rapoport, M.D. Clinical Professor of Neurology The David Geffen School of Medicine at UCLA Los Angeles, California
 An Overview of MOH IHS ASIAN HA MASTERS SCHOOL MARCH 24, 2013 ALAN M. Rapoport, M.D. Clinical Professor of Neurology The David Geffen School of Medicine at UCLA Los Angeles, California President-Elect
An Overview of MOH IHS ASIAN HA MASTERS SCHOOL MARCH 24, 2013 ALAN M. Rapoport, M.D. Clinical Professor of Neurology The David Geffen School of Medicine at UCLA Los Angeles, California President-Elect
Migraine Migraine Age Specific Prevalence in the United States. Headache International Headache Society Classification
 28 Primary Care Medicine Principles and Practice 29 October 28 Professor Peter J. Goadsby Peter.Goadsby@headache.ucsf.edu Department of Neurology Headache International Headache Society Classification
28 Primary Care Medicine Principles and Practice 29 October 28 Professor Peter J. Goadsby Peter.Goadsby@headache.ucsf.edu Department of Neurology Headache International Headache Society Classification
MEASURE #3: PREVENTIVE MIGRAINE MEDICATION PRESCRIBED Headache
 MEASURE #3: PREVENTIVE MIGRAINE MEDICATION PRESCRIBED Headache Measure Description Percentage of patients age 18 years old and older diagnosed with migraine headache whose migraine frequency is 4 migraine
MEASURE #3: PREVENTIVE MIGRAINE MEDICATION PRESCRIBED Headache Measure Description Percentage of patients age 18 years old and older diagnosed with migraine headache whose migraine frequency is 4 migraine
Migranal Nasal Spray. Migranal Nasal Spray (dihydroergotamine) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.60 Subject: Migranal Nasal Spray Page: 1 of 5 Last Review Date: June 22, 2017 Migranal Nasal Spray
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.60 Subject: Migranal Nasal Spray Page: 1 of 5 Last Review Date: June 22, 2017 Migranal Nasal Spray
Optimizing triptan therapy in clinical practice
 Review Optimizing triptan therapy in clinical practice Carlo Lisotto* & Giorgio Zanchin Practice Points The prevalence of migraine is 12 16% of the general population and is two- to threetimes higher in
Review Optimizing triptan therapy in clinical practice Carlo Lisotto* & Giorgio Zanchin Practice Points The prevalence of migraine is 12 16% of the general population and is two- to threetimes higher in
Headache Master School Japan-Osaka 2016 (HMSJ-Osaka2016) October 23, II. Management of Refractory Headaches
 October 23, II. Management of Refractory Headaches") Headache Master School Japan-Osaka 2016 (HMSJ-Osaka2016) October 23, 2016 II. Management of Refractory Headaches Case presentation 1: A case of intractable daily-persistent headache Keio University School
Headache Master School Japan-Osaka 2016 (HMSJ-Osaka2016) October 23, 2016 II. Management of Refractory Headaches Case presentation 1: A case of intractable daily-persistent headache Keio University School
Advances in the Treatment of Migraine
 Advances in the Treatment of Migraine C. Philip O Carroll, M.D. Director Neurobehavioral Medicine Hoag Neurosciences Institute Guyuron B Headache, 2015;55:1464-1473 I m sorry your head hurts, sweetie.is
Advances in the Treatment of Migraine C. Philip O Carroll, M.D. Director Neurobehavioral Medicine Hoag Neurosciences Institute Guyuron B Headache, 2015;55:1464-1473 I m sorry your head hurts, sweetie.is
OH, MY ACHING HEAD! I HAVE NO DISCLOSURES OR CONFLICTS OF INTERESTS TO DECLARE MANAGING HEADACHE IN THE OUTPATIENT SETTING SECONDARY HEADACHES
 1 JUSTIN A. OSSMAN, MD CHATTANOOGA FAMILY MEDICINE UPDATE OH, MY ACHING HEAD! MANAGING HEADACHE IN THE OUTPATIENT SETTING 2 I HAVE NO DISCLOSURES OR CONFLICTS OF INTERESTS TO DECLARE OBJECTIVES International
1 JUSTIN A. OSSMAN, MD CHATTANOOGA FAMILY MEDICINE UPDATE OH, MY ACHING HEAD! MANAGING HEADACHE IN THE OUTPATIENT SETTING 2 I HAVE NO DISCLOSURES OR CONFLICTS OF INTERESTS TO DECLARE OBJECTIVES International
Concussion. James R. Borchers, MD, MPH
 Concussion James R. Borchers, MD, MPH Associate Clinical Professor Director, Division of Sports Medicine, Department of Family Medicine Head Team Physician, Athletic Department Jameson Crane Sports Medicine
Concussion James R. Borchers, MD, MPH Associate Clinical Professor Director, Division of Sports Medicine, Department of Family Medicine Head Team Physician, Athletic Department Jameson Crane Sports Medicine
Nothing to disclose 3
 Nothing to disclose 3 PREVALENCE AND BURDEN OF HEADACHE Patient with CDH IHS migraine Recurrent severe headache Severe headache Episodic headache Have had headache Entire population CDH=chronic daily headache.
Nothing to disclose 3 PREVALENCE AND BURDEN OF HEADACHE Patient with CDH IHS migraine Recurrent severe headache Severe headache Episodic headache Have had headache Entire population CDH=chronic daily headache.
What is new in the migraine world! Modar Khalil Consultant neurologist Hull Royal Infirmary
 What is new in the migraine world! Modar Khalil Consultant neurologist Hull Royal Infirmary Overview Understanding the burden Commonly used terms Acute therapy What we currently have What we are going
What is new in the migraine world! Modar Khalil Consultant neurologist Hull Royal Infirmary Overview Understanding the burden Commonly used terms Acute therapy What we currently have What we are going
Migraine Management. Roger Cady, MD Headache Care Center Springfield, MO
 Migraine Management Roger Cady, MD Headache Care Center Springfield, MO Disclosures Objectives The evolution of migraine From benign episodic (benign) headache to potentially a devastating chronic disease
Migraine Management Roger Cady, MD Headache Care Center Springfield, MO Disclosures Objectives The evolution of migraine From benign episodic (benign) headache to potentially a devastating chronic disease
Strategies in Migraine Care
 Strategies in Migraine Care Julie L. Roth, MD Rhode Island Hospital Assistant Professor, Neurology The Warren Alpert Medical School of Brown University March 28, 2015 Financial Disclosures None. Objectives
Strategies in Migraine Care Julie L. Roth, MD Rhode Island Hospital Assistant Professor, Neurology The Warren Alpert Medical School of Brown University March 28, 2015 Financial Disclosures None. Objectives
Treatment of Primary Headache Syndromes
 Presenter Disclosure Information 2:45 3:45pm Treatment of Primary Headache Syndromes SPEAKER Gerald W. Smetana, MD The following relationships exist related to this presentation: Gerald W.Smetana, MD,
Presenter Disclosure Information 2:45 3:45pm Treatment of Primary Headache Syndromes SPEAKER Gerald W. Smetana, MD The following relationships exist related to this presentation: Gerald W.Smetana, MD,
Migraine much more than just a headache
 Migraine much more than just a headache Session hosted by Teva UK Limited PUU4 11:15 12:15 UK/NHSS/18/0021b Date of Preparation: August 2018 The views expressed in this presentation are those of the speaker
Migraine much more than just a headache Session hosted by Teva UK Limited PUU4 11:15 12:15 UK/NHSS/18/0021b Date of Preparation: August 2018 The views expressed in this presentation are those of the speaker
A Review of the Pharmacokinetics, Pharmacodynamics and Effi cacy of Zolmitriptan in the Acute Abortive Treatment of Migraine
 A Review of the Pharmacokinetics, Pharmacodynamics and Effi cacy of Zolmitriptan in the Acute Abortive Treatment of Migraine A.A. Kalanuria 1 and B.L. Peterlin 1,2 REVIEW 1 Drexel University College of
A Review of the Pharmacokinetics, Pharmacodynamics and Effi cacy of Zolmitriptan in the Acute Abortive Treatment of Migraine A.A. Kalanuria 1 and B.L. Peterlin 1,2 REVIEW 1 Drexel University College of
Migraine Management. Jane Melling Headache nurse Mater Misericordiae Hospital
 Migraine Management Jane Melling Headache nurse Mater Misericordiae Hospital Migraine facts Among the most common disorders of the nervous system 3 rd most prevalent medical disorder on the planet (lancet
Migraine Management Jane Melling Headache nurse Mater Misericordiae Hospital Migraine facts Among the most common disorders of the nervous system 3 rd most prevalent medical disorder on the planet (lancet
Page: 1 of 6. Aimovig (erenumab-aooe) injection, Ajovy (fremanezumab-vfrm) injection, Emgality (galcanezumab-gnim)
 injection, Ajovy (fremanezumab-vfrm) injection, Emgality (galcanezumab-gnim)") Page: 1 of 6 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Last Review Date: November 30, 2018 Description Aimovig (erenumab-aooe) injection, Ajovy (fremanezumab-vfrm)
Page: 1 of 6 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Last Review Date: November 30, 2018 Description Aimovig (erenumab-aooe) injection, Ajovy (fremanezumab-vfrm)
Triptans Quantity Limit Program Summary
 Triptans Quantity Limit Program Summary FDA APPROVED INDICATIONS AND DOSAGE 1-13,14,23,24 Agents Amerge (naratriptan) 1, 2.5 tablets Axert (almotriptan) 6.25, 12.5 tablets migraine attacks with/without
Triptans Quantity Limit Program Summary FDA APPROVED INDICATIONS AND DOSAGE 1-13,14,23,24 Agents Amerge (naratriptan) 1, 2.5 tablets Axert (almotriptan) 6.25, 12.5 tablets migraine attacks with/without
Managing Migraine: Primary Care for Primary Headaches
 Managing Migraine: Primary Care for Primary Headaches Faculty Jeffrey Unger, MD, FAAFP, FACE Director, Unger Primary Care Concierge Medical Group, Rancho Cucamonga, California; Director of Metabolic Studies,
Managing Migraine: Primary Care for Primary Headaches Faculty Jeffrey Unger, MD, FAAFP, FACE Director, Unger Primary Care Concierge Medical Group, Rancho Cucamonga, California; Director of Metabolic Studies,
Paediatric headaches. Dr Jaycen Cruickshank Director of Clinical Training Ballarat Health Services. Brevity, levity, repetition
 Paediatric headaches Dr Jaycen Cruickshank Director of Clinical Training Ballarat Health Services Brevity, levity, repetition Paediatric)headache?)! Headache!in!children!is!not!that!common.!The!question!is!which!headaches!do!I!
Paediatric headaches Dr Jaycen Cruickshank Director of Clinical Training Ballarat Health Services Brevity, levity, repetition Paediatric)headache?)! Headache!in!children!is!not!that!common.!The!question!is!which!headaches!do!I!
Louisiana Medicaid. Provider Update. Volume 26, Issue 4 July/August Message from the Medicaid Director Jerry Phillips
 Louisiana Medicaid Provider Update Volume 26, Issue 4 July/August 2009 Message from the Medicaid Director Jerry Phillips After careful analysis of the state fiscal year 2009-2010 budget approved by the
Louisiana Medicaid Provider Update Volume 26, Issue 4 July/August 2009 Message from the Medicaid Director Jerry Phillips After careful analysis of the state fiscal year 2009-2010 budget approved by the
10/13/17. Christy M. Jackson, MD Director, Dalessio Headache Center Scripps Clinic, La Jolla Clinical Professor, Neurosciences UCSD
 Christy M. Jackson, MD Director, Dalessio Headache Center Scripps Clinic, La Jolla Clinical Professor, Neurosciences UCSD } Depomed Consultant 2014 to present } Avanir Consultant 2014 to present } Amgen
Christy M. Jackson, MD Director, Dalessio Headache Center Scripps Clinic, La Jolla Clinical Professor, Neurosciences UCSD } Depomed Consultant 2014 to present } Avanir Consultant 2014 to present } Amgen
Migraine Acute treatment
 Migraine Acute treatment Elizabeth Loder, MD, MPH Professor of Neurology, Harvard Medical School Chief, Division of Headache, Department of Neurology, Brigham and Women s Hospital, Boston, MA Disclosures
Migraine Acute treatment Elizabeth Loder, MD, MPH Professor of Neurology, Harvard Medical School Chief, Division of Headache, Department of Neurology, Brigham and Women s Hospital, Boston, MA Disclosures
Migraine. What are the symptoms of a migraine attack?
 Migraine Migraine causes attacks of headaches, often with feeling sick or vomiting. Treatment options include: avoiding possible 'triggers', painkillers, antiinflammatory painkillers, anti-sickness medicines,
Migraine Migraine causes attacks of headaches, often with feeling sick or vomiting. Treatment options include: avoiding possible 'triggers', painkillers, antiinflammatory painkillers, anti-sickness medicines,
ARxCH. Annual Review of Changes in Healthcare. Calcitonin Gene-Related Peptide Receptors and the Prevention of Migraines. Abstract
 Calcitonin Gene-Related Peptide Receptors and the Prevention of Migraines Brian Schuler, PharmD Candidate 2018 1 1 University of Findlay College of Pharmacy Abstract Migraines are the third most prevalent
Calcitonin Gene-Related Peptide Receptors and the Prevention of Migraines Brian Schuler, PharmD Candidate 2018 1 1 University of Findlay College of Pharmacy Abstract Migraines are the third most prevalent
10/19/12. Headache: Tips and Tools for Management. Michael A. Rogawski, MD, PhD Disclosures
 10/19/12 Headache: Tips and Tools for Management Michael A. Rogawski, MD, PhD University of California, Davis Sacramento, CA Michael A. Rogawski, MD, PhD Disclosures Grants: Congressionally Directed Medical
10/19/12 Headache: Tips and Tools for Management Michael A. Rogawski, MD, PhD University of California, Davis Sacramento, CA Michael A. Rogawski, MD, PhD Disclosures Grants: Congressionally Directed Medical
Treatment of Headache in the ED
 Treatment of Headache in the ED Benjamin W. Friedman, MD, MS, FAAEM Associate professor of Emergency Medicine Albert Einstein College of Medicine Montefiore Medical Center Disclosure Topics of Discussion
Treatment of Headache in the ED Benjamin W. Friedman, MD, MS, FAAEM Associate professor of Emergency Medicine Albert Einstein College of Medicine Montefiore Medical Center Disclosure Topics of Discussion
Migraine Controversies in Women s Health. Professor Peter J. Goadsby 5 December Department of Neurology
 Migraine 2008 Controversies in Women s Health 5 December 2008 Professor Peter J. Goadsby Peter.Goadsby@headache.ucsf.edu Department of Neurology Headache International Headache Society Classification Primary
Migraine 2008 Controversies in Women s Health 5 December 2008 Professor Peter J. Goadsby Peter.Goadsby@headache.ucsf.edu Department of Neurology Headache International Headache Society Classification Primary
Imitrex for ocular migraines
 Imitrex for ocular migraines Information about ocular, optical, and ophthalmic Migraine, accurate diagnoses, and the importance of correct diagnostic and classification terminology. 14-10-2015 1 Answer
Imitrex for ocular migraines Information about ocular, optical, and ophthalmic Migraine, accurate diagnoses, and the importance of correct diagnostic and classification terminology. 14-10-2015 1 Answer
Maxalt. Maxalt / Maxalt-MLT (rizatriptan) Description. Section: Prescription Drugs Effective Date: April 1, 2016
 Description. Section: Prescription Drugs Effective Date: April 1, 2016") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Maxalt Page: 1 of 5 Last Review Date: March 18, 2016 Maxalt Description Maxalt / Maxalt-MLT (rizatriptan)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Maxalt Page: 1 of 5 Last Review Date: March 18, 2016 Maxalt Description Maxalt / Maxalt-MLT (rizatriptan)
What is the Effectiveness of OnabotulinumtoxinA (Botox ) in Reducing the Number of Chronic Migraines (CM) in Patients Years Old?
 in Reducing the Number of Chronic Migraines (CM) in Patients Years Old?") Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 2013 What is the Effectiveness of OnabotulinumtoxinA
Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 2013 What is the Effectiveness of OnabotulinumtoxinA
Clinical Policy: Triptans Reference Number: CP.CPA.217 Effective Date: Last Review Date: Line of Business: Commercial
 Clinical Policy: Reference Number: CP.CPA.217 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important regulatory
Clinical Policy: Reference Number: CP.CPA.217 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important regulatory
Headache Medicine for the Non Neurologist
 Headache Medicine for the Non Neurologist Justin DeLange, DO, FAHS Northern Arizona Healthcare Medical Group- Neurology Objectives At the end of this talk you should be able to: Explain why headache medicine
Headache Medicine for the Non Neurologist Justin DeLange, DO, FAHS Northern Arizona Healthcare Medical Group- Neurology Objectives At the end of this talk you should be able to: Explain why headache medicine
Chronic Daily Headaches
 Chronic Daily Headaches ANWARUL HAQ, MD, MRCP(UK), FAHS DIRECTOR BAYLOR HEADACHE CENTER, DALLAS, TEXAS DISCLOSURES: None OBJECTIVES AT THE CONCLUSION OF THIS ACTIVITY, PARTICIPANTS WILL BE ABLE TO: define
Chronic Daily Headaches ANWARUL HAQ, MD, MRCP(UK), FAHS DIRECTOR BAYLOR HEADACHE CENTER, DALLAS, TEXAS DISCLOSURES: None OBJECTIVES AT THE CONCLUSION OF THIS ACTIVITY, PARTICIPANTS WILL BE ABLE TO: define
Chronic Migraine in Primary Care. December 11 th, 2017 Werner J. Becker University of Calgary
 Chronic Migraine in Primary Care December 11 th, 2017 Werner J. Becker University of Calgary Disclosures Faculty: Werner J. Becker Relationships with commercial interests: Grants/Research Support: Clinical
Chronic Migraine in Primary Care December 11 th, 2017 Werner J. Becker University of Calgary Disclosures Faculty: Werner J. Becker Relationships with commercial interests: Grants/Research Support: Clinical
ABORTIVE AGENTS. Average cost per 30 days. Form Limits SEROTONIN AGONISTS $ $ Reserved for treatment failure to either Sumatriptan PA; QL
 MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Migraine Therapy P&T DATE: 12/11/2018 CLASS: Neurological Disorders REVIEW HISTORY 9/17, 12/16, 9/15, 2/15, 2/10, LOB: MCL
MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Migraine Therapy P&T DATE: 12/11/2018 CLASS: Neurological Disorders REVIEW HISTORY 9/17, 12/16, 9/15, 2/15, 2/10, LOB: MCL
Mark W. Green, MD, FAAN
 Mark W. Green, MD, FAAN Professor of Neurology, Anesthesiology, and Rehabilitation Medicine Director of Headache and Pain Medicine Icahn School of Medicine at Mt Sinai New York Pain-sensitive structures
Mark W. Green, MD, FAAN Professor of Neurology, Anesthesiology, and Rehabilitation Medicine Director of Headache and Pain Medicine Icahn School of Medicine at Mt Sinai New York Pain-sensitive structures
MIGRAINE A CAUSE OF INTENSE THROBBING; A MINI REVIEW
 IJBPAS, January, 2016, 5(1): 87-92 ISSN: 2277 4998 MIGRAINE A CAUSE OF INTENSE THROBBING; A MINI REVIEW MUHAMMAD ZAMAN 1*, RABIA HASSAN 1, MUHAMMAD SHAFEEQ UR RAHMAN 2, MUHAMMAD HAFIZ ARSHAD 3, SYED ATIF
IJBPAS, January, 2016, 5(1): 87-92 ISSN: 2277 4998 MIGRAINE A CAUSE OF INTENSE THROBBING; A MINI REVIEW MUHAMMAD ZAMAN 1*, RABIA HASSAN 1, MUHAMMAD SHAFEEQ UR RAHMAN 2, MUHAMMAD HAFIZ ARSHAD 3, SYED ATIF
Emerging drugs for migraine treatment: an update
 Expert Opinion on Emerging Drugs ISSN: 1472-8214 (Print) 1744-7623 (Online) Journal homepage: http://www.tandfonline.com/loi/iemd20 Emerging drugs for migraine : an update Giorgio Lambru, Anna P. Andreou,
Expert Opinion on Emerging Drugs ISSN: 1472-8214 (Print) 1744-7623 (Online) Journal homepage: http://www.tandfonline.com/loi/iemd20 Emerging drugs for migraine : an update Giorgio Lambru, Anna P. Andreou,
ISSN doi: /head VC 2015 American Headache Society Published by Wiley Periodicals, Inc.
 ISSN 0017-8748 Headache doi: 10.1111/head.12746 VC 2015 American Headache Society Published by Wiley Periodicals, Inc. Review Article Acute Treatment Therapies for Pediatric Migraine: A Qualitative Systematic
ISSN 0017-8748 Headache doi: 10.1111/head.12746 VC 2015 American Headache Society Published by Wiley Periodicals, Inc. Review Article Acute Treatment Therapies for Pediatric Migraine: A Qualitative Systematic
Emerging Challenges in Primary Care: Brainstorm: A Symposium on Migraine Treatment and Management
 Emerging Challenges in Primary Care: 2017 Brainstorm: A Symposium on Migraine Treatment and Management 1 Faculty Jeff Unger, MD, ABFM, FACE Director, Unger Primary Care Medical Group Rancho Cucamonga,
Emerging Challenges in Primary Care: 2017 Brainstorm: A Symposium on Migraine Treatment and Management 1 Faculty Jeff Unger, MD, ABFM, FACE Director, Unger Primary Care Medical Group Rancho Cucamonga,
Headaches: An Approach to Evaluation & Management
 Florida Osteopathic Medical Association 17 th Annual Primary Care & Cardiovascular Symposium Headaches: An Approach to Evaluation & Management Kenneth Hentschel, DO, PhD, FAANEM St. Vincent s Spine & Brain
Florida Osteopathic Medical Association 17 th Annual Primary Care & Cardiovascular Symposium Headaches: An Approach to Evaluation & Management Kenneth Hentschel, DO, PhD, FAANEM St. Vincent s Spine & Brain
Subject: Aimovig (erenumab) Original Effective Date: 7/10/2018. Policy Number: MCP-320. Revision Date(s):
 Original Effective Date: 7/10/2018. Policy Number: MCP-320. Revision Date(s):") Subject: Aimovig (erenumab) Original Effective Date: 7/10/2018 Policy Number: MCP-320 Revision Date(s): Review Date(s): MCPC Approval Date: 7/10/2018 DISCLAIMER This Molina Clinical Policy (MCP) is intended
Subject: Aimovig (erenumab) Original Effective Date: 7/10/2018 Policy Number: MCP-320 Revision Date(s): Review Date(s): MCPC Approval Date: 7/10/2018 DISCLAIMER This Molina Clinical Policy (MCP) is intended
SIGN on the pharmacological management of migraine
 GUIDELINES SIGN on the pharmacological management of migraine STEVE CHAPLIN In February 2018, the Scottish Intercollegiate Guidelines Network (SIGN) published a new guideline on the pharmacological management
GUIDELINES SIGN on the pharmacological management of migraine STEVE CHAPLIN In February 2018, the Scottish Intercollegiate Guidelines Network (SIGN) published a new guideline on the pharmacological management
ปวดศ รษะมา 5 ป ก นยาแก ปวดก ย งไม ข น นพ.พาว ฒ เมฆว ช ย โรงพยาบาลนครราชส มา
 ปวดศ รษะมา 5 ป ก นยาแก ปวดก ย งไม ข น นพ.พาว ฒ เมฆว ช ย โรงพยาบาลนครราชส มา 1 CONTENT 1 2 3 Chronic Daily Headache Medical Overused Headache Management Headaches are one of the most common symptoms List
ปวดศ รษะมา 5 ป ก นยาแก ปวดก ย งไม ข น นพ.พาว ฒ เมฆว ช ย โรงพยาบาลนครราชส มา 1 CONTENT 1 2 3 Chronic Daily Headache Medical Overused Headache Management Headaches are one of the most common symptoms List
A new questionnaire for assessment of adverse events associated with triptans: methods of assessment influence the results. Preliminary results
 J Headache Pain (2004) 5:S112 S116 DOI 10.1007/s10194-004-0123-4 Michele Feleppa Fred D. Sheftell Luciana Ciannella Amedeo D Alessio Giancarlo Apice Nino N. Capobianco Donato M.T. Saracino Walter Di Iorio
J Headache Pain (2004) 5:S112 S116 DOI 10.1007/s10194-004-0123-4 Michele Feleppa Fred D. Sheftell Luciana Ciannella Amedeo D Alessio Giancarlo Apice Nino N. Capobianco Donato M.T. Saracino Walter Di Iorio
Sumatriptan Tablets, Nasal Spray (Imitrex), Nasal Powder (Onzetra Xsail), sumatriptan and naproxen sodium (Treximet tablets)
, Nasal Powder (Onzetra Xsail), sumatriptan and naproxen sodium (Treximet tablets)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 05.70.10 Subject: Sumatriptan Page: 1 of 5 Last Review Date: December 2, 2016 Sumatriptan Description Sumatriptan
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 05.70.10 Subject: Sumatriptan Page: 1 of 5 Last Review Date: December 2, 2016 Sumatriptan Description Sumatriptan