Glaucoma Surgery Louis B. Cantor, MD Jay C. and Lucile L. Kahn Chair and Professor Director of Glaucoma Service
|
|
|
- Leslie Phelps
- 5 years ago
- Views:
Transcription
1 Glaucoma Surgery 2018 Louis B. Cantor, MD Jay C. and Lucile L. Kahn Chair and Professor Director of Glaucoma Service
2 Disclosures Research Support: Allergan, InnFocus, Bausch and Lomb Consultant: Zeiss Meditec, Santen Investor: Mati Speakers Bureau: None
3 Laser surgery for glaucoma
4 Indications Laser peripheral iridotomy pupillary block angle closure glaucoma chronic angle closure prophylaxis for narrow angles pigment dispersion syndrome?
5 Contraindications Laser peripheral iridotomy corneal opacification or edema flat or shallow anterior chamber synechial closure of angle
6 Pre-operative treatment iopidine pilocarpine topical anesthesia Laser peripheral iridotomy
7 Argon Laser Laser peripheral iridotomy more effective in brown irises? Nd:YAG laser more effective in light-colored irises?
8 Location Laser peripheral iridotomy base of crypt in peripheral iris between 11:00 and 1:00

9 Abraham lens Laser peripheral iridotomy +66D planoconvex button magnifies and concentrates laser energy
10 Argon laser iridotomy 3 phases: μm sec mw Contraction Punch Cleanup (may take up to 300 shots!)

11
12 Nd:YAG peripheral iridotomy 3 to 10 millijoules 1 or 2 pulses per burst 1 to 10 bursts usually suffices

13
14 Complications Laser peripheral iridotomy blurred vision monocular diplopia and glare corneal damage iritis pigment dispersion

15
16 Complications (continued) hemorrhage IOP spike lens opacities closure of iridotomy site Laser peripheral iridotomy

17
18 Post-operative care Laser peripheral iridotomy re-check IOP in one hour steroid drops re-examine in one week patency of iridotomy gonioscopy
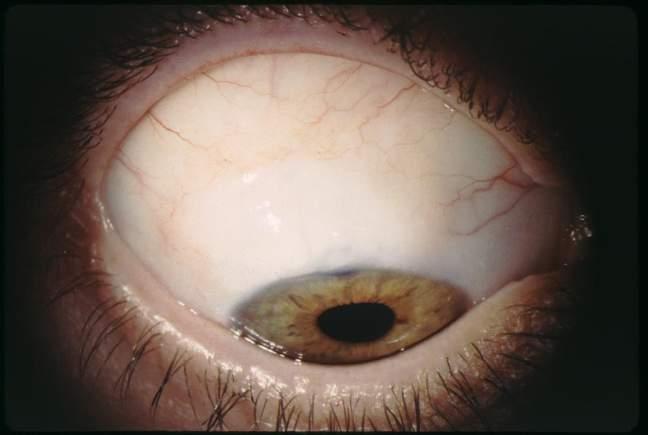
19 Case 2 58 year old WM, s/p peripheral iridotomy OU for acute angle closure attack OD 2 years ago, now presents with painful, red, blurred right eye. Va is 20/400 OD. SLE reveals hyperemia, cornea edema, patent PI OD. IOP is 45 OD, 25 OS.
20 What else do you look for? Diagnosis? Treatment? Case 2
21 Case 2 Gonioscopy reveals appositional closure of the angle with a steep iris insertion

22
23 Indications Argon laser peripheral iridoplasty acute angle closure glaucoma not responding to medical therapy plateau iris syndrome other forms of angle closure adjunct to ALT
24 Argon laser peripheral iridoplasty Contraindications severe corneal edema or opacification flat anterior chamber synechial angle closure
25 Argon laser peripheral iridoplasty Pre-operative care pilocarpine iopidine topical anesthesia
26 Argon laser peripheral iridoplasty Laser parameters 500 μm spot size sec duration mw power

27 Aim at extreme peripheral iris spots over 360 degrees
28 Argon laser peripheral iridoplasty Post-operative care steroids iopidine gonioscopy
29 Complications Argon laser peripheral iridoplasty iritis corneal damage need for retreatment
30
31 Case 3 73 year old WF with 15 year hx of POAG. IOPs are 19 OD, 20 OS on betaxolol, brimonidine, dorzolamide, and latanoprost. Cup:disc 0.8 OU. HVF reveal worsening of nasal step and arcuate defects OU.
32 Indications Argon laser trabeculoplasty maximally tolerated medical therapy poor compliance initial therapy?
33 Pre-operative care iopidine Argon laser trabeculoplasty
34 Laser parameters Argon laser trabeculoplasty 50 μm spot, 0.1 second, mw 50 spots per 180 degrees 180 or 360 degrees Location anterior half of trabecular meshwork

35

36
37 Post-operative care Argon laser trabeculoplasty re-check IOP in one hour steroids continue all glaucoma medications
38 Argon laser trabeculoplasty Effectiveness of ALT for POAG About 75-80% at one year About 50% at five years Failure rate about 6-10% per year
39 IOP reduction Argon laser trabeculoplasty Depends on initial IOP Pre-laser IOP usually respond best
40 Effectiveness of ALT Argon laser trabeculoplasty good for phakic POAG, PXE, and pigmentary glaucoma less effective in aphakic eyes, younger persons (<40yrs), previously filtered eyes, uveitic glaucoma, angle recession glaucoma
41 Effectiveness of ALT Argon laser trabeculoplasty effectiveness more short-lived in pseudoexfoliation glaucoma, pigmentary glaucoma, African-Americans.
42 Onset of effect Argon laser trabeculoplasty 4 to 6 weeks for most POAG earlier effect for PXE and pigmentary glaucoma

43 Argon laser trabeculoplasty
44 Repeat ALT Argon laser trabeculoplasty Usually not as effective as initial treatment If initial ALT was not effective then a repeat ALT will probably not be effective either
45 Complications increased IOP iritis PAS hemorrhage corneal damage Argon laser trabeculoplasty

46 Selective Laser Trabeculoplasty Frequency-doubled Q-switched 532 Nd:YAG laser 532 nm 3 nanosecond pulse 400 micron spot size mj spots over 180 or 360 o

47 ALT versus SLT
48 Selective Laser Trabeculoplasty Ophthalmology 1998;105:

49 ALT Ophthalmology 2001;108:

50 SLT Ophthalmology 2001;108:
51 SLT as primary treatment Arch Ophthalmol 2003;121:
52 Treatment Algorithm for Lowering IOP SLT, selective laser trabeculoplasty; ALT, argon laser trabeculoplasty. Initiating Glaucoma Therapy IOP controlled Monotherapy: Prostaglandin analogs IOP still high AAO considers 20% reduction in baseline IOP to be clinically significant Continue prostaglandin analog Surgery SLT or ALT Switch to another agent Add another agent
53 Incisional surgery for glaucoma
54 Trabeculectomy A guarded partial-thickness filtering procedure --- removal of a block of peripheral cornea tissue beneath a scleral flap
55 Trabeculectomy- Indications When IOP cannot be maintained by nonsurgical therapies at a level considered low enough to prevent further pressure-related damage to the optic nerve or visual field loss. Maximum tolerable medical therapy Maximum laser benefit Optic nerve function is failing or likely to fail
56 Relative contraindications Blind eye Ocular neoplasm Active rubeosis irides Active iritis Extensive conjunctival injury eg, s/p RD repair, chemical burn Extremely thin sclera
57 Trabeculectomy- Technique Conjunctival flap: limbus based vs fornix based Antifibrotic agent use Split thickness scleral flap Limbal fistula Iridectomy Scleral flap closure Conjunctival wound closure
58 Limbus-based vs fornix-based Limbus-based: incision 8-10 mm posterior to the limbus Fornix-based: incision at the limbus Each has advantages and disadvantages Success rates: no significant difference IOP reduction: no significant difference


59 Limbus-based vs fornix-based Limbus-based conjunctival flap Technically more challenging Usually used with SR traction suture Less likely to leak at cut edge Easier to place MMC posteriorly Subconjunctiva scar posterior to scleral flap, ring of steel More cystic, anteriorly draining bleb Fornix-based conjunctival flap Easier and faster to perform Usually used with corneal traction suture More likely to leak at cut edge More difficult to place MMC posteriorly Subconjunctiva scar anterior to scleral flap More diffused, posteriorly draining bleb

60 Antifibrotic agents Action- inhibit fibro-cellular proliferation Indications previous surgery: failed trab aphakia or pseudophakia young patients black race uveitis neovascular glaucoma Every case? Be cautious in young myope: hypotony maculopathy
61 5-Fluorouracil Pyrimidine analog: inhibit fibroblast proliferation Intra-op: 50mg/ml, sponges Post-op: 5-10mg/ ml, injections Advantage: titrated dose Disadvantage: multiple injections
62 Mitomycin-C Alkylating agent causing DNA cross-linking Intra-op: mg/ml x mins, sponges (typical dose: mg/ml x 1-3 mins) Pre-op: intra-tenon injection 5-20ug/ ml Advantage: no need for multiple injections Disadvantage: imprecise dosing for sponges
63 Antifibrotic agents Application Sponges: - LASIK shields cut in half, four halfs - Weck-cel Large surface area treated - Results in more diffuse, noncystic bleb - No Ring of Steel formation
64 Scleral flap Matter: relationship of the flap to the sclerostomy thickness: 1/2 scleral thickness Not matter: shape or size of the flap shapes: triangular, trapezoid, rectangular sizes: 3-4mm x 2-3mm

65 Limbal fistula Sclerostomy/keratectomy (punch or blade) - Anteriorly placed - Avoid ciliary body exposure - Reduce bleeding - Perpendicular alignment Ex-PRESS Shunt




66 Ex-PRESS mini glaucoma shunt
67 Ex-PRESS mini glaucoma shunt J Glaucoma 2007;16:14-19

68 Iridectomy Reduce the risk of iris occluding the sclerostomy Prevent pupillary block Avoid amputation of ciliary processes Avoid disruption of the zonular fibers or hyaloid face


69 Sclerostomy and iridectomy
70 Scleral Flap Closure Appose edges of scleral incision, 10-0 nylon sutures Adjustment of suture numbers and tension Check filtration with sponges (minimal spontaneous flow) Releasable sutures


71 Conjunctival Closure Limbus-based close conjunctiva and Tenon seperately or in a single layer Fornix-based wing sutures - purse-string sutures +/- Central sutures -compression running closure modified condon-wise sutures

72 Conjunctival closure (limbus-based)

73 Conjunctival closure (fornix-based, wing suture)


74 Conjunctival closure (fornix-based, Condon-Wise suture)
75 Close follow-up Post-op management success = 50% surgery + 50% post-op care POD#1, then qwk x 2-3, then q2wks -1mon Topical steroids (weeks to months) Maintaining aqueous flowing Fibrosis of scleral flap within 2-3 weeks Up to 2-3+ months with antimetabolite Methods: digital pressure/ massage /releasable sutures/laser suture lysis




76 Lens edge of Zeiss goniolens Hoskins lens Blumenthal lens (2-3 x) laser suture lysis Argon laser mw, S, um
77 IBAGS (Indiana Bleb Appearance Grading Scale)

78
 Bleb migration Hypotony Ptosis Eyelid")
79 Complications Early Late Infection Hypotony Shallow or flat AC Aqueous misdirecttion Hyphema Cataract Transient IOP elevation CME Hypotony maculopathy Choroidal effusion Suprachoroidal hemorrhage Persistent uveitis Dellen formation Loss of vision Leakage or failure of the filtering bleb Cataract Blebitis Endophthalmitis Symptomatic bleb (dysesthetic bleb) Bleb migration Hypotony Ptosis Eyelid retraction
80 leakage Low IOP choroidal effusion Low Bleb overfiltration/leak Shallow/Flat AC high IOP aqueous misdirection pupillary block Low IOP overfiltration High Bleb High IOP suprachoroidal hemorrhage
 trauma (eyelid rubbing) contact")
81 Bleb Leak Hypotony, Siedel s (+) Early: wound leaks buttonholes from surgery Late: thin, avascular, cystic blebs after antimetabolites (5-FU, MMC) trauma (eyelid rubbing) contact lens wear
82 Early bleb leak management -Observation: small ones heal spontaneously -Pressure patch -Large CTL that completely covers leak -Aqueous suppressants -Hold/decrease steroids -After 3-4 days, consider closure
83 Late bleb leak management -Observation -Large CTL that completely covers leak -Aqueous suppressants -Glue: cyanoacrylate, fibrin -Tissue destruction: TCA, cryo, laser (argon, YAG) -Autologous blood injection -Tamponade compression suture -Bleb revision with advancement graft (+/- conjunctival autograft)



84 Autologous blood injection

85 Glue


86 Shallow or flat AC -Iridocorneal touch Most spontaneous deepening in 7-14 days -Corneolenticular touch Quickly causes cornea decompensation and cataract Aggressive intervention- reform AC
87 Management of Flat AC Observation Reformation of AC: Viscoelastic Air SF6 C3F8 May need choroidal drainage
88 Choroidal Effusion -Consequence of hypotony and inflammation -Usually maximum on POD #5

89 Choroidal effusion Symptoms and signs -Decrease in vision -Lens induced myopia -Decrease in peripheral visual field -Photophobia, epiphora, pain -Typically hypotonous -Shallow or flat AC -Choroidal detachment on exam -Ultrasound appearance
90 Choroidal Effusion Predisposing Factors -Hypotony and vasodilation after any ocular surgery -Choroidal hemangioma, Sturge-Weber, Nanophthalmos, Increased EVP -More common and persistent in older patients
 Failing filtering bleb Acute secondary")
91 Management of choroidal effusion Observation: Usually resolves spontaneously Mydriatics/ Cycloplegics Topical and/or systemic steroids Drain if : PAS concern Corneo-lenticular touch Corneal decompensation Kissing choroids Prolonged hypotony (no signs of improvement within 4 weeks) Failing filtering bleb Acute secondary angle closure


92 Hypotony maculopathy More common with 5-FU and MMC Primary procedure, young myopes >6 months: maculopathy may be permanent

93 Suprachoroidal hemorrhage H/O of straining, laughing, coughing or sneezing Occurs first 4 to 5 days post-op Acute onset of severe pain Sudden visual loss Risk factors: Advanced age Systemic vascular disease Aphakia High myopia Previous vitrectomy High pre-op IOP, hypotony post-op Nanophthalmos

94 Management of Suprachoroidal Hemorrhage -Same medical treatment as choroidal effusion -Surgical drainage: clot lysis takes 4 to 5 days so try to delay surgery if possible -Indications: Severe, intractable pain, uncontrolled IOP, Prolonged retinal apposition, RD, Vitreous hemorrhage
 may be")
95 Failing bleb Elevated IOP, no bleb R/o obstruction of internal sclerostomy by gonioscopy Blood, fibrin, iris, vitreous, lens material If fibrin or blood blocks outflow, tissue plasminogen activator (tpa) may be helpful

96 Late Bleb Failure Internal: iris, ciliary processes, capsule, blood Intrascleral: small ostomy, tight flap Extrascleral: episcleral fibrosis-most common cause for failure

97 Bleb encapsulation Elevated IOP with vascular, localized bleb High-domed, taut encapsulation of the bleb -- limits aqueous filtration Up to 15% the 1st post-op month Less common with antimetabolites But 5-FU > MMC
98 Management of bleb encapsulation -Minimal response to digital massage -Medical management (Aqeous suppressants) Often all that is needed (up to 90%) -Surgical management Needling w/ 5-FU or MMC injections Revision (excision)


99 Late complication Bleb associated infection Transconjunctival migration of microorganisms through leaks, holes, breaks, or weakened thin tissue
100 Risk Factors -Thin avascular blebs -Use of antimetabolities -Bleb leaks -Blepharitis -Dacryocystitis -Inferior or interpalpebral blebs
101 Common Causative Organisms Staphyococcus sp. Streptococcus sp. Hemophilus sp. Pseudomonas sp.



102 Blebitis Pain, blurred vision, redness Inflamed eye White bleb surrounded by conjunctival injection Purulent areas in bleb Often with bleb leak Anterior chamber reaction vitreous clear (B scan)
103 Bleb associated infection Stage 1 Bleb purulence + mild AC inflammation Stage 2 Bleb purulence + moderate AC inflammation Stage 3 Bleb purulence, marked AC inflammation, vitritis Bleb related endophthalmitis
104 Incidence of bleb associated infection Retrospective chart review Trab with mmc 0.5 mg/ml minutes 239 eyes/198 patients Average f/u 2.7 yrs ( yrs) Bleb leak 20 (8%) Blebitis 5 (2%) Endophthalmitis 8 (3%) DeBry, et al. Incidence of late-onset bleb-related complications Following trab w/mmc. Arch Ophthal 120: , year probability of bleb leak 17.9%, blebitis 6.3%, endophthalmitis 7.5%
105 Management Stage 1 & 2 blebitis + Culture conjunctiva Hourly fluoroquinolone (4 th gen) and cycloplegia Daily f/u until signs of improvement, then can decrease antibiotic frequency Change to fortified drops if no improvement Consider subconj cefazolin/tobra if bolus needed or poor compliance May consider topical steroids after 48 hours of improvement Oral fluoroquinolone for Stage 2
106 Management Stage 3 endophthalmitis Frequent topical antibiotics as in stage 1 & 2 Vitreous tap for C&S Intravitreal antibiotic injection Oral antibiotics EVS protocol for treatment
107 Indications Glaucoma tube implants Previous trabeculectomy failure Excessive conjunctival scarring Neovascular glaucoma Uveitic glaucoma ICE syndrome glaucoma


108 Glaucoma tube implants - types Non-valved Molteno Baerveldt



109 Glaucoma tube implants - types Valved Ahmed Krupin

110 Glaucoma tube implants sizes (mm 2 )



111
112 Conj incision Tenons dissection +/- Muscle dissection Prime Tube Plate Placement Suture Plate Trim & Occlude tube +/-Tube Slits Scleral/AC tract/tube placement +/- Tube fixation/tutoplast Conj Closure +/- Viscoelastic Tube Shunt Steps
113 Medications Post-op care Topical steroid drop Antibiotic drop Glaucoma medications if tube tied off** Hypotony precautions
114 Glaucoma tube implants - benefits Less prone to infection More amenable to contact lens wear Comfort Repeatable
115 Trabeculectomy vs Tube implant Am J Ophthalmol. 2007;143:9-22.
116 Trabeculectomy vs Tube implant Am J Ophthalmol. 2007;143:9-22.
117 Trabeculectomy vs Tube implant Am J Ophthalmol. 2007;143:9-22. IOP > 17 mm Hg IOP > 14 mm Hg
118 Postoperative Complications Tube (n = 107) Trabeculectomy (n = 105) P-value Choroidal effusion Shallow or flat AC Wound leak Hyphema Persistent corneal edema Encapsulated bleb Dysethesia CME Suprachoroidal hemorrhage Persistent diplopia Am J Ophthalmol. 2007;143:23-31.
119 Evolution of glaucoma surgery: MIGS and beyond!
120 MIGS Ab-interno (clear corneal) micro-incisional Minimal operative tissue manipulation High safety profile Rapid visual recovery Efficacious

121 Steven Vold, MD MIGS


122 Outflow Pathway Top View Distal Outflow System

123 Sources of Outflow Resistance Collector Channels / Distal System Schlemm s Canal Trabecular Meshwork


 and viscosurgical device used to cannulate and viscodilate Schlemm's canal Crescent-shaped")
124 Canal Based MIGS MIGS: Increase Trabecular Outflow istent Micro-Bypass Gonioscopy-assisted transluminal trabeculotomy (GATT) Trabectome OMNI 360 Trabeculotomy Kahook Dual Blade Ab interno canaloplasty Hydrus Microstent Specifics / Procedure: Heparin-coated, non-ferromagnetic titanium stent; 1.0 mm x 0.3 mm. Ab interno insertion into Schlemm's canal Ab interno trabeculotomy using illuminated microcatheter (itrack; Ellex) or prolene/nylon suture passed through a 1-2 mm goniotomy into Schlemm's canal 360 and lysed through the trabecular tissue Ab interno trabeculectomy using combination of electrocautery, irrigation and aspiration Ab interno trabeculotomy using disposable, non-powered device from which a flexible nylon-like trabeculotome is advanced into Schlemm's canal for 180 and then lysed (x2 to perform up to 360 trabeculotomy) Ab interno trabeculotomy using a single use, tapered, stainless steel blade Illuminated microcatheter (itrack; Ellex) and viscosurgical device used to cannulate and viscodilate Schlemm's canal Crescent-shaped scaffold (8-mm long) composed of nickel-titanium alloy, Ab interno insertion into Schlemm's canal
125 Suprachoroidal Based MIGS Increase Uveoscleral / Suprachoroidal/ Supraciliary Outflow CyPass Micro-Stent istent Supra Fenestrated micro-stent, composed of biocompatible, polyimide material (6.35 mm x 510 mm, 300 mm lumen) Ab interno insertion between anterior chamber/sclera and suprachoroidal space Heparin-coated stent (4mm long, mm lumen) composed of polyethersulfone (PES) with a titanium sleeve. Ab interno insertion between anterior chamber/sclera and suprachoroidal space
126 Translimbal Based MIGS Increase Subconjunctival Outflow XEN Glaucoma Treatment System InnFocus MicroShunt Tissue-conforming tube implant (6-mm long) composed of gelatin and glutaraldehyde material Ab interno insertion from the anterior chamber, through sclera into the subconjunctival space, bleb forming Flexible microshunt (8.5 mm x mm, 70 μm lumen) composed of SIBS (poly(styrene-block-isobutylene-blockstyrene)) Ab-externo, subconjunctival (via peritomy) insertion through scleral needle tract into anterior chamber, connecting it to sub-tenon's space, bleb forming
127 Ciliodestructive Based MIGS Decrease Aqueous Production Endocyclophotocoagulation (Trans-scleral options also) Ab interno cyclodestruction of ciliary body epithelium using continuous energy (810nm wavelength)
128 Canaloplasty Re-establish flow from anterior chamber to the restored canal of Schlemm and the collectors: Achieve physiologic control of IOP Without requiring a bleb Without developing bleb related post operative problems Non-penetrating surgical procedure with: 360º cannulation and viscodilation of Schlemm s canal Circumferential suture tensioning of trabecular meshwork / stenting of Schlemm s canal Trabeculo-descemetic window




129 Canaloplasty



130 Canaloplasty, Viscodilation Dilation of Schlemm s canal visualized with UltraSound Imaging Preoperative Dilation of Schlemm s canal Dilation of Schlemm s canal and collector channels



131 Canaloplasty, Suture Tension Distension of Trabecular Meshwork visualized with UltraSound Imaging Grade 0- No distension Grade 1 Good distension Grade 2 Maximum desired distension

132 Canaloplasty J Cataract Refract Surg 2007;33:

 Hydrus")
133 Trabecular microstents istent (Glaukos, Laguna Hills, CA) Hydrus (Ivantix, Irvine, CA)


134 Trabeculotomy/goniotomy Trabeculectomy ab interno (Trabectome Study Group)

135 Suprachoroidal microstents CyPass (Alcon/Novartis/Transcend Medical, Menlo Park, Calif.) istent Supra (Glaukos, Laguna Hills, CA)


136 CyPass PubMed search yields 7 results Saheb H, et al. BJO 2014;98: OCT imaging
137 CyPass and Endothelial Cell Loss Voluntary FDA Withdrawal 8/2018 Alcon COMPASS-XT 2018


138 FDA IDE trials underway istent Supra


139 Subconjunctival microstent Xen implant(aquesys/allergan, Irvine, CA) Soft flexible, permanent, gelatin/collagen implant InnFocus- conj incision

140

141



142
143

144

145
146


147
148
149
150

151

152

153

154

155

156
MIGS Rapid Fire Outline 1 st talk: Goniotomy, Lisa Young, OD, FAAO
 Rapid Fire MIGS A Modern Solution to a Complex Problem Course Description: Minimally (or Micro-) Invasive Glaucoma Surgeries, or MIGS, are an increasingly popular treatment modality in the management of
Rapid Fire MIGS A Modern Solution to a Complex Problem Course Description: Minimally (or Micro-) Invasive Glaucoma Surgeries, or MIGS, are an increasingly popular treatment modality in the management of
Subject Index. Canaloplasty aqueous outflow system evaluation 110, 111 complications 118, 119 historical perspective 109, 110
 Subject Index Ab externo Schlemm canal surgery, see Canaloplasty, Viscocanalostomy Ab interno Schlemm canal surgery, see istent, Trabectome Adjustable sutures 14, 15 AGV glaucoma drainage implants 43,
Subject Index Ab externo Schlemm canal surgery, see Canaloplasty, Viscocanalostomy Ab interno Schlemm canal surgery, see istent, Trabectome Adjustable sutures 14, 15 AGV glaucoma drainage implants 43,
Developments in Glaucoma Surgery
 Developments in Glaucoma Surgery Marlene R. Moster, MD Professor of Ophthalmology Thomas Jefferson University School of Medicine Wills Eye Hospital Philadelphia, PA When is surgery indicated? Poor control
Developments in Glaucoma Surgery Marlene R. Moster, MD Professor of Ophthalmology Thomas Jefferson University School of Medicine Wills Eye Hospital Philadelphia, PA When is surgery indicated? Poor control
TRABECULECTOMY. Dr. Sandra M. Johnson, MD
 TRABECULECTOMY Dr. Sandra M. Johnson, MD FILTRATION OPTIONS Trabeculotomy, Schlemn s canal, internal Deep Non-penetrating Sclerectomy filtering to a scleral lake, or viscocanulostomy Trabeculectomy shunting
TRABECULECTOMY Dr. Sandra M. Johnson, MD FILTRATION OPTIONS Trabeculotomy, Schlemn s canal, internal Deep Non-penetrating Sclerectomy filtering to a scleral lake, or viscocanulostomy Trabeculectomy shunting
Optometrist's Guide to Glaucoma Surgery. Goals. Glaucoma Philosophy. I have no financial disclosures
 Optometrist's Guide to Glaucoma Surgery Anthony DeWilde, OD FAAO I have no financial disclosures 1 2 Goals Glaucoma Philosophy Glaucoma can be a visually debilitating disease. How glaucoma surgery works
Optometrist's Guide to Glaucoma Surgery Anthony DeWilde, OD FAAO I have no financial disclosures 1 2 Goals Glaucoma Philosophy Glaucoma can be a visually debilitating disease. How glaucoma surgery works
GLAUCOMA SURGERY: FROM THEN TIL NOW (COPE Course ID: GL)
") MIGS: How did we get here? GLAUCOMA SURGERY: FROM THEN TIL NOW (COPE Course ID: 55570-GL) John Gelvin, O.D., F.A.A.O. MOYES EYE CENTER Kansas City, Missouri jgelvin@moyeseye.com 1. Tube vs Trabeculectomy?
MIGS: How did we get here? GLAUCOMA SURGERY: FROM THEN TIL NOW (COPE Course ID: 55570-GL) John Gelvin, O.D., F.A.A.O. MOYES EYE CENTER Kansas City, Missouri jgelvin@moyeseye.com 1. Tube vs Trabeculectomy?
WGA. The Global Glaucoma Network
 The Global Glaucoma Network Fort Lauderdale April 30, 2005 Indications for Surgery 1. The decision for surgery should consider the risk/benefit ratio. Note: Although a lower IOP is generally considered
The Global Glaucoma Network Fort Lauderdale April 30, 2005 Indications for Surgery 1. The decision for surgery should consider the risk/benefit ratio. Note: Although a lower IOP is generally considered
XEN GEL STENT MIGS 4/5/2018 OMAHA AND LINCOLN EYE AND LASER INSTITUTES XEN45 GEL STENT WHY ARE WE LOOKING FOR NEW INNOVATIONS IN GLAUCOMA SURGERY?
 XEN GEL STENT OMAHA AND LINCOLN EYE AND LASER INSTITUTES MARK R. YOUNG, M.D. April 7, 2018 QUESTION: Why are we looking for alternatives to current glaucoma treatment? Look at current surgical glaucoma
XEN GEL STENT OMAHA AND LINCOLN EYE AND LASER INSTITUTES MARK R. YOUNG, M.D. April 7, 2018 QUESTION: Why are we looking for alternatives to current glaucoma treatment? Look at current surgical glaucoma
Corporate Medical Policy
 Corporate Medical Policy Aqueous Shunts and Devices for Glaucoma File Name: Origination: Last CAP Review: Next CAP Review: Last Review: aqueous_shunts_and_devices_for_glaucoma 3/2010 6/2017 6/2018 6/2017
Corporate Medical Policy Aqueous Shunts and Devices for Glaucoma File Name: Origination: Last CAP Review: Next CAP Review: Last Review: aqueous_shunts_and_devices_for_glaucoma 3/2010 6/2017 6/2018 6/2017
Glaucoma Surgical Treatments. Murray Fingeret, OD Justin Schweitzer, OD Joe Sowka, OD
 Glaucoma Surgical Treatments Murray Fingeret, OD Justin Schweitzer, OD Joe Sowka, OD Disclosures Murray Fingeret Consultant Bausch & Lomb, Alcon, Allergan Justin Schweitzer Allergan, Glaukos, Bausch and
Glaucoma Surgical Treatments Murray Fingeret, OD Justin Schweitzer, OD Joe Sowka, OD Disclosures Murray Fingeret Consultant Bausch & Lomb, Alcon, Allergan Justin Schweitzer Allergan, Glaukos, Bausch and
Microinvasive Glaucoma Surgery (MIGS) Nathan Radcliffe, MD New York University New York Eye Surgical Center WAEPS April 1, 2016
 Nathan Radcliffe, MD New York University New York Eye Surgical Center WAEPS April 1, 2016") Microinvasive Glaucoma Surgery (MIGS) Nathan Radcliffe, MD New York University New York Eye Surgical Center WAEPS April 1, 2016 Financial Disclosures Surgical Glaucoma History Glaucoma Surgery Trends 1994-2012
Microinvasive Glaucoma Surgery (MIGS) Nathan Radcliffe, MD New York University New York Eye Surgical Center WAEPS April 1, 2016 Financial Disclosures Surgical Glaucoma History Glaucoma Surgery Trends 1994-2012
>$500m. Assessing New Implants. Minimally-Invasive Surgery & Other new devices -a Foretaste
 Minimally-Invasive Surgery & Other new devices -a Foretaste Keith Barton Consultant Ophthalmologist Moorfields Eye Hospital, London Market capitalisation of new glaucoma surgical device companies >$500m
Minimally-Invasive Surgery & Other new devices -a Foretaste Keith Barton Consultant Ophthalmologist Moorfields Eye Hospital, London Market capitalisation of new glaucoma surgical device companies >$500m
WHY MIGS 7/26/18. MIGs in the BIGs A professional level understanding of MIGs. Human Cost of Glaucoma. Standard Treatment Options for Glaucoma
 Financial Disclosures for Mitch Ibach OD, FAAO MIGs in the BIGs A professional level understanding of MIGs Glaukos Alcon Equinox LLC. Mitch Ibach OD, FAAO Vance Thompson Vision Human Cost of Glaucoma WHY
Financial Disclosures for Mitch Ibach OD, FAAO MIGs in the BIGs A professional level understanding of MIGs Glaukos Alcon Equinox LLC. Mitch Ibach OD, FAAO Vance Thompson Vision Human Cost of Glaucoma WHY
A REVIEW OF MINIMALLY-INVASIVE GLAUCOMA SURGERY (MIGS) Felise May Barte, MD CECOM Symposium 2019
 Felise May Barte, MD CECOM Symposium 2019") I. Traditional glaucoma surgery A. Trabeculectomy B. Tube Shunt C. Tube versus Trabeculectomy Study Gedde SJ, Herndon LW, Brandt JD, Budenz DL, Feuer WJ, Schiffman JC, Tube Versus Trabeculectomy Study
I. Traditional glaucoma surgery A. Trabeculectomy B. Tube Shunt C. Tube versus Trabeculectomy Study Gedde SJ, Herndon LW, Brandt JD, Budenz DL, Feuer WJ, Schiffman JC, Tube Versus Trabeculectomy Study
These devices, when FDA approved, are covered for patients with glaucoma that is not adequately controlled with medical therapy.
 Medical Policy Title: Aqueous Shunts and ARBenefits Approval: 10/26/2011 Devices for Glaucoma Effective Date: 01/01/2012 Document: ARB0168 Revision Date: Code(s): 66174, Transluminal dilation of aqueous
Medical Policy Title: Aqueous Shunts and ARBenefits Approval: 10/26/2011 Devices for Glaucoma Effective Date: 01/01/2012 Document: ARB0168 Revision Date: Code(s): 66174, Transluminal dilation of aqueous
EXP11677SK. Financial Disclosure. None to be Declared EXP11677SK
 Financial Disclosure None to be Declared Presentation overview Glaucoma Surgical History Complications of trabeculectomy Express Device Specifications Surgical Steps Clinical advantages, indications and
Financial Disclosure None to be Declared Presentation overview Glaucoma Surgical History Complications of trabeculectomy Express Device Specifications Surgical Steps Clinical advantages, indications and
TRABECULECTOMY THE BEST AND WORST CANDIDATES
 TRABECULECTOMY THE BEST AND WORST CANDIDATES MICHAEL F. OATS, MD OPHTHALMIC CONSULTANTS OF BOSTON ASCRS 2014 FINANCIAL DISCLOSURES None TRABECULECTOMY Performed for over 100 years Most commonly performed
TRABECULECTOMY THE BEST AND WORST CANDIDATES MICHAEL F. OATS, MD OPHTHALMIC CONSULTANTS OF BOSTON ASCRS 2014 FINANCIAL DISCLOSURES None TRABECULECTOMY Performed for over 100 years Most commonly performed
Aqueous Shunts and Stents for Glaucoma. (90321) (Formerly Aqueous Shunts for Glaucoma)
 (Formerly Aqueous Shunts for Glaucoma)") Protocol Aqueous Shunts and Stents for Glaucoma (90321) (Formerly Aqueous Shunts for Glaucoma) Medical Benefit Effective Date: 01/01/13 Next Review Date: 01/14 Preauthorization* No Review Dates: 03/10,
Protocol Aqueous Shunts and Stents for Glaucoma (90321) (Formerly Aqueous Shunts for Glaucoma) Medical Benefit Effective Date: 01/01/13 Next Review Date: 01/14 Preauthorization* No Review Dates: 03/10,
Aqueous Shunts and Stents for Glaucoma
 Protocol Aqueous Shunts and Stents for Glaucoma (90321) Medical Benefit Effective Date: 04/01/14 Next Review Date: 01/15 Preauthorization No Review Dates: 03/10, 03/11, 07/11, 01/12, 09/12, 01/13, 01/14
Protocol Aqueous Shunts and Stents for Glaucoma (90321) Medical Benefit Effective Date: 04/01/14 Next Review Date: 01/15 Preauthorization No Review Dates: 03/10, 03/11, 07/11, 01/12, 09/12, 01/13, 01/14
Aqueous Shunts and Stents for Glaucoma
 Aqueous Shunts and Stents for Glaucoma Policy Number: 9.03.21 Last Review: 1/2018 Origination: 9/2008 Next Review: 1/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage
Aqueous Shunts and Stents for Glaucoma Policy Number: 9.03.21 Last Review: 1/2018 Origination: 9/2008 Next Review: 1/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage
The second most common causes of blindness worldwide. ( after cataract) The commonest cause of irreversible blindness in the world Estimated that 3%
 The commonest cause of irreversible blindness in the world Estimated that 3%") The second most common causes of blindness worldwide. ( after cataract) The commonest cause of irreversible blindness in the world Estimated that 3% of our population age > 40 have glaucoma In the past:
The second most common causes of blindness worldwide. ( after cataract) The commonest cause of irreversible blindness in the world Estimated that 3% of our population age > 40 have glaucoma In the past:
EFFICACY AND SAFETY OF CANALOPLASTY IN SAUDI PATIENTS WITH UNCONTROLLED OPEN ANGLE GLAUCOMA
 EFFICACY AND SAFETY OF CANALOPLASTY IN SAUDI PATIENTS WITH UNCONTROLLED OPEN ANGLE GLAUCOMA DR.FAISAL ALMOBARAK ASSISTANT PROFESSOR AND CONSULTANT DEPARTMENT OF OPHTHALMOLOGY COLLEGE OF MEDICINE AND KING
EFFICACY AND SAFETY OF CANALOPLASTY IN SAUDI PATIENTS WITH UNCONTROLLED OPEN ANGLE GLAUCOMA DR.FAISAL ALMOBARAK ASSISTANT PROFESSOR AND CONSULTANT DEPARTMENT OF OPHTHALMOLOGY COLLEGE OF MEDICINE AND KING
Corporate Medical Policy
 Corporate Medical Policy Viscocanalostomy and Canaloplasty File Name: Origination: Last CAP Review: Next CAP Review: Last Review: viscocanalostomy_and_canaloplasty 11/2011 6/2017 6/2018 6/2017 Description
Corporate Medical Policy Viscocanalostomy and Canaloplasty File Name: Origination: Last CAP Review: Next CAP Review: Last Review: viscocanalostomy_and_canaloplasty 11/2011 6/2017 6/2018 6/2017 Description
Objectives. Tubes, Ties and Videotape: Financial Disclosure. Five Year TVT Results IOP Similar
 Tubes, Ties and Videotape: Surgical Video of Glaucoma Implants and Financial Disclosure I have no financial interests or relationships to disclose. Herbert P. Fechter MD, PE Eye Physicians and Surgeons
Tubes, Ties and Videotape: Surgical Video of Glaucoma Implants and Financial Disclosure I have no financial interests or relationships to disclose. Herbert P. Fechter MD, PE Eye Physicians and Surgeons
CHARTING THE NEW COURSE FOR MIGS
 CHARTING THE NEW COURSE FOR MIGS SEE WHAT S ON THE HORIZON CyPass Micro-Stent the next wave in micro-invasive glaucoma surgery. MICRO-INVASIVE GLAUCOMA SURGERY (MIGS) OFFERS A REVOLUTIONARY APPROACH TO
CHARTING THE NEW COURSE FOR MIGS SEE WHAT S ON THE HORIZON CyPass Micro-Stent the next wave in micro-invasive glaucoma surgery. MICRO-INVASIVE GLAUCOMA SURGERY (MIGS) OFFERS A REVOLUTIONARY APPROACH TO
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of microinvasive subconjunctival insertion of a trans-scleral gelatin stent for primary
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of microinvasive subconjunctival insertion of a trans-scleral gelatin stent for primary
PRINCIPLES AND TYPES OF GLAUCOMA SURGERIES
 PRINCIPLES AND TYPES OF GLAUCOMA SURGERIES DR.FAISAL ALMOBARAK ASSISTANT PROFESSOR AND CONSULTANT DEPARTMENT OF OPHTHALMOLOGY COLLEGE OF MEDICINE AND KING SAUD UNIVERSITY SAUDI ARABIA INTRODUCTION AQUEOUS
PRINCIPLES AND TYPES OF GLAUCOMA SURGERIES DR.FAISAL ALMOBARAK ASSISTANT PROFESSOR AND CONSULTANT DEPARTMENT OF OPHTHALMOLOGY COLLEGE OF MEDICINE AND KING SAUD UNIVERSITY SAUDI ARABIA INTRODUCTION AQUEOUS
Keeping Current in Glaucoma Surgery
 Keeping Current in Glaucoma Surgery #51596-GL COPE April 2018 Ilya Rozenbaum, MD Matossian Eye Associates Financial Disclosures Alcon Allergan B+L Glaukos Human Cost of Glaucoma Glaucoma is the second
Keeping Current in Glaucoma Surgery #51596-GL COPE April 2018 Ilya Rozenbaum, MD Matossian Eye Associates Financial Disclosures Alcon Allergan B+L Glaukos Human Cost of Glaucoma Glaucoma is the second
Aqueous Shunts and Stents for Glaucoma
 Aqueous Shunts and Stents for Glaucoma Policy Number: 9.03.21 Last Review: 8/2018 Origination: 9/2008 Next Review: 1/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage
Aqueous Shunts and Stents for Glaucoma Policy Number: 9.03.21 Last Review: 8/2018 Origination: 9/2008 Next Review: 1/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage
Challenging complications of valve implantation. Salah M Al-Mosallamy MD Assistant professor of ophthalmology 2014
 Challenging complications of valve implantation by Salah M Al-Mosallamy MD Assistant professor of ophthalmology 2014 PREDISPOSING FACTORS It is important to consider the case mix for these devices on dealing
Challenging complications of valve implantation by Salah M Al-Mosallamy MD Assistant professor of ophthalmology 2014 PREDISPOSING FACTORS It is important to consider the case mix for these devices on dealing
Cronicon EC OPHTHALMOLOGY. Research Article Trephine Assisted Trabeculectomy Technique. Idrees* Introduction
 Cronicon OPEN ACCESS EC OPHTHALMOLOGY Research Article Idrees* Al Dara Hospital and Medical Center at Riyadh, Saudi Arabia *Corresponding Author: Dr Idrees, Al Dara Hospital and Medical Center at Riyadh,
Cronicon OPEN ACCESS EC OPHTHALMOLOGY Research Article Idrees* Al Dara Hospital and Medical Center at Riyadh, Saudi Arabia *Corresponding Author: Dr Idrees, Al Dara Hospital and Medical Center at Riyadh,
New Horizons in Glaucoma Devices. Steven Vold MD Vold Vision February 4, 2017
 1 New Horizons in Glaucoma Devices Steven Vold MD Vold Vision February 4, 2017 2 Financial Disclosures Vold Vision, P.L.L.C BK Ventures Group Company Nature of Affiliation Founder and Chief Executive Office
1 New Horizons in Glaucoma Devices Steven Vold MD Vold Vision February 4, 2017 2 Financial Disclosures Vold Vision, P.L.L.C BK Ventures Group Company Nature of Affiliation Founder and Chief Executive Office
Microinvasive surgical
 Improved efficacy expected with second-generation microinvasive glaucoma surgery (MIGS) devices BY ROD MCNEIL Microinvasive surgical approaches to primary openangle glaucoma (POAG) offer minimally traumatic
Improved efficacy expected with second-generation microinvasive glaucoma surgery (MIGS) devices BY ROD MCNEIL Microinvasive surgical approaches to primary openangle glaucoma (POAG) offer minimally traumatic
1/16/2018. Brett J. Teague, M.D. Big Country Eye Center Abilene, Texas
 Brett J. Teague, M.D. Big Country Eye Center Abilene, Texas I developed the course material/information independently No relevant financial relationship exists by anyone in control of presentation content
Brett J. Teague, M.D. Big Country Eye Center Abilene, Texas I developed the course material/information independently No relevant financial relationship exists by anyone in control of presentation content
Glaucoma. How is Glaucoma Diagnosed? Glaucoma Testing
 Glaucoma How is Glaucoma Diagnosed? Glaucoma Testing There is no single test for glaucoma. The diagnosis is made by evaluating the patient from a number of perspectives, using specialized instruments.
Glaucoma How is Glaucoma Diagnosed? Glaucoma Testing There is no single test for glaucoma. The diagnosis is made by evaluating the patient from a number of perspectives, using specialized instruments.
Aqueous Shunts and Stents for Glaucoma
 Aqueous Shunts and Stents for Glaucoma Policy Number: 9.03.21 Last Review: 1/2014 Origination: 9/2008 Next Review: 1/2015 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage
Aqueous Shunts and Stents for Glaucoma Policy Number: 9.03.21 Last Review: 1/2014 Origination: 9/2008 Next Review: 1/2015 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage
Viscocanalostomy and Canaloplasty. Description. Section: Other Effective Date: July 15, 2015
 Subject: Viscocanalostomy and Canaloplasty Page: 1 of 10 Last Review Status/Date: June 2015 Viscocanalostomy and Canaloplasty Description Glaucoma surgery is intended to reduce intraocular pressure (IOP)
Subject: Viscocanalostomy and Canaloplasty Page: 1 of 10 Last Review Status/Date: June 2015 Viscocanalostomy and Canaloplasty Description Glaucoma surgery is intended to reduce intraocular pressure (IOP)
THE CURRENT TREATMENT OF GLAUCOMA IS DIrected
 Three-Year Follow-up of the Tube Versus Trabeculectomy Study STEVEN J. GEDDE, JOYCE C. SCHIFFMAN, WILLIAM J. FEUER, LEON W. HERNDON, JAMES D. BRANDT, AND DONALD L. BUDENZ, ON BEHALF OF THE TUBE VERSUS
Three-Year Follow-up of the Tube Versus Trabeculectomy Study STEVEN J. GEDDE, JOYCE C. SCHIFFMAN, WILLIAM J. FEUER, LEON W. HERNDON, JAMES D. BRANDT, AND DONALD L. BUDENZ, ON BEHALF OF THE TUBE VERSUS
PRESENTED By DR. FAISAL ALMOBARAK, MD
 PRESENTED By DR. FAISAL ALMOBARAK, MD Early FAC associated with hypotony is an important complication after glaucoma filtering procedures, especially trabeculectomy. The reported incidence after trabeculectomy
PRESENTED By DR. FAISAL ALMOBARAK, MD Early FAC associated with hypotony is an important complication after glaucoma filtering procedures, especially trabeculectomy. The reported incidence after trabeculectomy
Beginner (score = 3) Can hold goniolens but hesitates to move to visualize a different angle.
 Can hold goniolens but hesitates to move to visualize a different angle.") Instructions: Use one form per trainee For each competency, allocate a score to the trainee s level of execution of said skill: Novice (Score = 2), Beginner (Score = 3), Advanced (Score 4), and Competent
Instructions: Use one form per trainee For each competency, allocate a score to the trainee s level of execution of said skill: Novice (Score = 2), Beginner (Score = 3), Advanced (Score 4), and Competent
Surgery for COEXISTING CATARACT AND GLAUCOMA:
 Surgery for COEXISTING CATARACT AND GLAUCOMA: UNEASY RELATIONSHIP Session: 20-107 Monday, April 20, 2015 Time: 8:00 AM-9:30 AM Room 7B (San Diego Convention Center) Course Instructors Ahmad K Khalil Alan
Surgery for COEXISTING CATARACT AND GLAUCOMA: UNEASY RELATIONSHIP Session: 20-107 Monday, April 20, 2015 Time: 8:00 AM-9:30 AM Room 7B (San Diego Convention Center) Course Instructors Ahmad K Khalil Alan
9/25/2018. New Generation Glaucoma Care. Disclosures. Overview
 New Generation Glaucoma Care MARK MARAMAN, O.D. NOA MEETING KEARNEY, NE OCT 4 TH, 2018 Disclosures I have no financial relationships or conflicts of interest with the manufacturers of any commercial products
New Generation Glaucoma Care MARK MARAMAN, O.D. NOA MEETING KEARNEY, NE OCT 4 TH, 2018 Disclosures I have no financial relationships or conflicts of interest with the manufacturers of any commercial products
and done ONE CYPASS MICRO-STENT IS ALL IT TAKES TO DELIVER ON THE PROMISE OF MIGS SAFE, CONSISTENT, LONG-TERM IOP CONTROL
 FOR THE REDUCTION OF IOP IN MILD TO MODERATE PRIMARY OPEN-ANGLE GLAUCOMA AT THE TIME OF CATARACT SURGERY and done ONE CYPASS MICRO-STENT IS ALL IT TAKES TO DELIVER ON THE PROMISE OF MIGS SAFE, CONSISTENT,
FOR THE REDUCTION OF IOP IN MILD TO MODERATE PRIMARY OPEN-ANGLE GLAUCOMA AT THE TIME OF CATARACT SURGERY and done ONE CYPASS MICRO-STENT IS ALL IT TAKES TO DELIVER ON THE PROMISE OF MIGS SAFE, CONSISTENT,
Trabeculectomy A Review and 2 Year Follow Up
 ORIGINAL ARTICLE Trabeculectomy A Review and 2 Year Follow Up F Jaais, (MRCOphth) Department of Ophthalmology, University Malaya Medical Center, Faculty of Medicine, 50603 Kuala Lumpur Summary This study
ORIGINAL ARTICLE Trabeculectomy A Review and 2 Year Follow Up F Jaais, (MRCOphth) Department of Ophthalmology, University Malaya Medical Center, Faculty of Medicine, 50603 Kuala Lumpur Summary This study
AC & ACG Instruction Course Surgical Treatments for PACG
 AC & ACG Instruction Course Surgical Treatments for PACG Presented by APGS Clement C.Y. THAM Professor, The Chinese University of Hong Kong Chief of Service, Hong Kong Eye Hospital Deputy Secretary-General,
AC & ACG Instruction Course Surgical Treatments for PACG Presented by APGS Clement C.Y. THAM Professor, The Chinese University of Hong Kong Chief of Service, Hong Kong Eye Hospital Deputy Secretary-General,
Viscocanalostomy and Canaloplasty
 Viscocanalostomy and Canaloplasty Policy Number: 9.03.26 Last Review: 9/2014 Origination: 9/2012 Next Review: 9/2015 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for
Viscocanalostomy and Canaloplasty Policy Number: 9.03.26 Last Review: 9/2014 Origination: 9/2012 Next Review: 9/2015 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for
AB-INTERNO CANALOPLASTY THE MINIMALLY INVASIVE GLAUCOMA SURGERY THAT KEEPS ITS PROMISE
 WHITEPAPER AB-INTERNO CANALOPLASTY THE MINIMALLY INVASIVE GLAUCOMA SURGERY THAT KEEPS ITS PROMISE AB-INTERNO CANALOPLASTY: TREATMENT STEPS 12-MONTH CASE SERIES REVIEW ABiC Canaloplasty performed with an
WHITEPAPER AB-INTERNO CANALOPLASTY THE MINIMALLY INVASIVE GLAUCOMA SURGERY THAT KEEPS ITS PROMISE AB-INTERNO CANALOPLASTY: TREATMENT STEPS 12-MONTH CASE SERIES REVIEW ABiC Canaloplasty performed with an
Surgical outcomes of Trab and Tube for Uveitic glaucoma - Experience from a Tertiary Institution
 Surgical outcomes of Trab and Tube for Uveitic glaucoma - Experience from a Tertiary Institution Hye Jin Kwon, George YX Kong, William Tao, Lyndell Lim, Keith R Martin, Cathy Green, Jonathan Ruddle, Jonathan
Surgical outcomes of Trab and Tube for Uveitic glaucoma - Experience from a Tertiary Institution Hye Jin Kwon, George YX Kong, William Tao, Lyndell Lim, Keith R Martin, Cathy Green, Jonathan Ruddle, Jonathan
Aqueous Shunts and Stents for Glaucoma. Description
 Subject: Aqueous Shunts and Stents for Glaucoma Page: 1 of 13 Last Review Status/Date: June 2015 Aqueous Shunts and Stents for Glaucoma Description Glaucoma is not a single entity; there are many subcategories
Subject: Aqueous Shunts and Stents for Glaucoma Page: 1 of 13 Last Review Status/Date: June 2015 Aqueous Shunts and Stents for Glaucoma Description Glaucoma is not a single entity; there are many subcategories
POLICY PRODUCT VARIATIONS DESCRIPTION/BACKGROUND RATIONALE DEFINITIONS BENEFIT VARIATIONS DISCLAIMER CODING INFORMATION REFERENCES POLICY HISTORY
 Original Issue Date (Created): June 4, 2013 Most Recent Review Date (Revised): March 25, 2014 Effective Date: June 1, 2014 POLICY PRODUCT VARIATIONS DESCRIPTION/BACKGROUND RATIONALE DEFINITIONS BENEFIT
Original Issue Date (Created): June 4, 2013 Most Recent Review Date (Revised): March 25, 2014 Effective Date: June 1, 2014 POLICY PRODUCT VARIATIONS DESCRIPTION/BACKGROUND RATIONALE DEFINITIONS BENEFIT
Nate Lighthizer, O.D., F.A.A.O. Assistant Professor, NSUOCO Assistant Dean, Clinical Care Services Director of CE Chief of Specialty Care Clinics
 Nate Lighthizer, O.D., F.A.A.O. Assistant Professor, NSUOCO Assistant Dean, Clinical Care Services Director of CE Chief of Specialty Care Clinics Chief of Electrodiagnostics Clinic lighthiz@nsuok.edu YAG
Nate Lighthizer, O.D., F.A.A.O. Assistant Professor, NSUOCO Assistant Dean, Clinical Care Services Director of CE Chief of Specialty Care Clinics Chief of Electrodiagnostics Clinic lighthiz@nsuok.edu YAG
Optometric Postoperative Cataract Surgery Management
 Financial Disclosures Optometric Postoperative Cataract Surgery Management David Dinh, OD Oak Cliff Eye Clinic Dallas Eye Consultants March 10, 2015 Comanagement Joint cooperation between two or more specialists
Financial Disclosures Optometric Postoperative Cataract Surgery Management David Dinh, OD Oak Cliff Eye Clinic Dallas Eye Consultants March 10, 2015 Comanagement Joint cooperation between two or more specialists
Chronicity. Narrow Minded. Course Outline. Acute angle closure. Subacute angle closure. Classification of Angle Closure 5/19/2014
 Chronicity Narrow Minded The management of narrow angles in the optometric practice Acute Subacute Chronic Aaron McNulty, OD, FAAO Course Outline Classification of Angle Closure Evaluation of narrow angles
Chronicity Narrow Minded The management of narrow angles in the optometric practice Acute Subacute Chronic Aaron McNulty, OD, FAAO Course Outline Classification of Angle Closure Evaluation of narrow angles
Aqueous Shunts and Stents for Glaucoma. Populations Interventions Comparators Outcomes Individuals: With refractory open-angle glaucoma.
 Protocol Aqueous Shunts and Stents for Glaucoma (90321) Medical Benefit Effective Date: 04/01/15 Next Review Date: 11/18 Preauthorization No Review Dates: 03/10, 03/11, 07/11, 01/12, 09/12, 01/13, 01/14,
Protocol Aqueous Shunts and Stents for Glaucoma (90321) Medical Benefit Effective Date: 04/01/15 Next Review Date: 11/18 Preauthorization No Review Dates: 03/10, 03/11, 07/11, 01/12, 09/12, 01/13, 01/14,
5/18/2014. Fundamentals of Gonioscopy Workshop Aaron McNulty, OD, FAAO Walt Whitley, OD, MBA, FAAO
 1 Fundamentals of Gonioscopy Workshop Aaron McNulty, OD, FAAO Walt Whitley, OD, MBA, FAAO 2 3 4 5 6 Optometry s Meeting 2014 The Most Valuable Glaucoma Tool Glaucoma Diagnosis Gonioscopy Central corneal
1 Fundamentals of Gonioscopy Workshop Aaron McNulty, OD, FAAO Walt Whitley, OD, MBA, FAAO 2 3 4 5 6 Optometry s Meeting 2014 The Most Valuable Glaucoma Tool Glaucoma Diagnosis Gonioscopy Central corneal
Aqueous Shunts for the Treatment of Glaucoma
 TITLE: Aqueous Shunts for the Treatment of Glaucoma AUTHOR: Jeffrey A. Tice, MD Assistant Professor of Medicine Division of General Internal Medicine Department of Medicine University of California San
TITLE: Aqueous Shunts for the Treatment of Glaucoma AUTHOR: Jeffrey A. Tice, MD Assistant Professor of Medicine Division of General Internal Medicine Department of Medicine University of California San
Secondary Glaucomas. Mr Nick Strouthidis MBBS MD PhD FRCS FRCOphth FRANZCO Consultant Ophthalmologist, Glaucoma Service, Moorfields Eye Hospital
 Secondary Glaucomas Mr Nick Strouthidis MBBS MD PhD FRCS FRCOphth FRANZCO Consultant Ophthalmologist, Glaucoma Service, Moorfields Eye Hospital Introduction: What is glaucoma? Glaucoma is the name given
Secondary Glaucomas Mr Nick Strouthidis MBBS MD PhD FRCS FRCOphth FRANZCO Consultant Ophthalmologist, Glaucoma Service, Moorfields Eye Hospital Introduction: What is glaucoma? Glaucoma is the name given
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of ab interno supraciliary microstent insertion with phacoemulsification for primary
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of ab interno supraciliary microstent insertion with phacoemulsification for primary
Financial Disclosure. The TVT Mentality. Outline. A Case-based Approach to Caring for the Glaucoma Patient: Malik Y. Kahook, MD
 A Case-based Approach to Caring for the Glaucoma Patient: Advances in Glaucoma Surgery Malik Y. Kahook, MD The Slater Family Endowed Chair in Ophthalmology Professor of Ophthalmology Vice Chair, Clinical
A Case-based Approach to Caring for the Glaucoma Patient: Advances in Glaucoma Surgery Malik Y. Kahook, MD The Slater Family Endowed Chair in Ophthalmology Professor of Ophthalmology Vice Chair, Clinical
Considerations in the Cataract Patient with Glaucoma. Robert Noecker, MD, MBA Ophthalmic Consultants of Connecticut Fairfield, CT
 Considerations in the Cataract Patient with Glaucoma Robert Noecker, MD, MBA Ophthalmic Consultants of Connecticut Fairfield, CT Financial Disclosure Dr. Noecker has been a paid consultant to Allergan,
Considerations in the Cataract Patient with Glaucoma Robert Noecker, MD, MBA Ophthalmic Consultants of Connecticut Fairfield, CT Financial Disclosure Dr. Noecker has been a paid consultant to Allergan,
03/04/2015. LOC Talk Anterior Chamber & Gonioscopy 1st April Methods of Assessing Anterior Chamber Depth (and angle width) Outline
 Outline") LOC Talk Anterior & 1st April 2015 Mr. Areeb Moosavi MBBS BSc FRCOphth Glaucoma Consultant Milton Keynes University Hospital NHS Foundation Trust Methods of Assessing Anterior Open Versus Closed angle
LOC Talk Anterior & 1st April 2015 Mr. Areeb Moosavi MBBS BSc FRCOphth Glaucoma Consultant Milton Keynes University Hospital NHS Foundation Trust Methods of Assessing Anterior Open Versus Closed angle
GENERAL INFORMATION GLAUCOMA GLAUCOMA
 GENERAL INFORMATION GLAUCOMA GLAUCOMA WHAT IS GLAUCOMA? Glaucoma is commonly known as the sneak thief of sight because it can cause irreversible vision loss without any obvious symptoms. The term glaucoma
GENERAL INFORMATION GLAUCOMA GLAUCOMA WHAT IS GLAUCOMA? Glaucoma is commonly known as the sneak thief of sight because it can cause irreversible vision loss without any obvious symptoms. The term glaucoma
4/24/2018. Management of Patients with Conjoint Cataract and Glaucoma. Prevalence of Glaucoma C: NEW WORLD MEDICAL
 Management of Patients with Conjoint Cataract and Glaucoma Bryan Lee, MD, JD 40 th Annual Dallas Spring Ophthalmology Symposium April 27, 2018 Consultant: Allergan, Katena, New World Medical Financial
Management of Patients with Conjoint Cataract and Glaucoma Bryan Lee, MD, JD 40 th Annual Dallas Spring Ophthalmology Symposium April 27, 2018 Consultant: Allergan, Katena, New World Medical Financial
Hydrus. What is a Hydrus Microstent? By Nathan Kerr and Keith Barton. Eye words to know. MIGS.org
 MIGS.org Hydrus By Nathan Kerr and Keith Barton What is a Hydrus Microstent? The Hydrus Microstent is a small flexible scaffold inserted into the natural drainage channel of the eye to lower eye pressure
MIGS.org Hydrus By Nathan Kerr and Keith Barton What is a Hydrus Microstent? The Hydrus Microstent is a small flexible scaffold inserted into the natural drainage channel of the eye to lower eye pressure
STAB INCISION GLAUCOMA SURGERY (SIGS)
") STAB INCISION GLAUCOMA SURGERY (SIGS) Dr. Soosan Jacob, MS, FRCS, DNB Senior Consultant Ophthalmologist, Dr. Agarwal's Eye Hospital, Chennai, India dr_soosanj@hotmail.com Videos available in Youtube channel:
STAB INCISION GLAUCOMA SURGERY (SIGS) Dr. Soosan Jacob, MS, FRCS, DNB Senior Consultant Ophthalmologist, Dr. Agarwal's Eye Hospital, Chennai, India dr_soosanj@hotmail.com Videos available in Youtube channel:
New Technologies for Treating Glaucoma in Patients Undergoing Cataract Surgery
 New Technologies for Treating Glaucoma in Patients Undergoing Cataract Surgery Joseph L Lin 1 and Hylton R Mayer 2 1. Ophthalmology Resident; 2. Assistant Professor, Department of Ophthalmology and Visual
New Technologies for Treating Glaucoma in Patients Undergoing Cataract Surgery Joseph L Lin 1 and Hylton R Mayer 2 1. Ophthalmology Resident; 2. Assistant Professor, Department of Ophthalmology and Visual
Novel Glaucoma Procedures
 Ophthalmic Technology Assessment Novel Glaucoma Procedures A Report by the American Academy of Ophthalmology Brian A. Francis, MD, 1 Kuldev Singh, MD, MPH, 2 Shan C. Lin, MD, 3 Elizabeth Hodapp, MD, 4
Ophthalmic Technology Assessment Novel Glaucoma Procedures A Report by the American Academy of Ophthalmology Brian A. Francis, MD, 1 Kuldev Singh, MD, MPH, 2 Shan C. Lin, MD, 3 Elizabeth Hodapp, MD, 4
Written by Administrator Wednesday, 13 January :27 - Last Updated Thursday, 21 January :34
 angle closure glaucoma A type of glaucoma caused by a sudden and severe rise in eye pressure. Occurs when the pupil enlarges too much or too quickly, and the outer edge of the iris blocks the eye s drainage
angle closure glaucoma A type of glaucoma caused by a sudden and severe rise in eye pressure. Occurs when the pupil enlarges too much or too quickly, and the outer edge of the iris blocks the eye s drainage
Save time at your check-in and register online before your appointment! It s as easy as 1-2-3
 Save time at your check-in and register online before your appointment! It s as easy as 1-2-3 1. Go online to www.blackhillseyes.com 2. Click this logo on our home page for the link to register: 3. Set-up
Save time at your check-in and register online before your appointment! It s as easy as 1-2-3 1. Go online to www.blackhillseyes.com 2. Click this logo on our home page for the link to register: 3. Set-up
Aqueous Shunts and Stents for Glaucoma Section 9.0 Other Subsection 9.03 Vision
 9.03.21 Aqueous Shunts and Stents for Glaucoma Section 9.0 Other Subsection 9.03 Vision Effective Date January 30, 2015 Original Policy Date January 30, 2015 Next Review Date January 2016 Description Glaucoma
9.03.21 Aqueous Shunts and Stents for Glaucoma Section 9.0 Other Subsection 9.03 Vision Effective Date January 30, 2015 Original Policy Date January 30, 2015 Next Review Date January 2016 Description Glaucoma
Ab-Interno Canaloplasty A Comprehensive Minimally Invasive Glaucoma Surgery
 Ab-Interno Canaloplasty A Comprehensive Minimally Invasive Glaucoma Surgery AB-INTERNO CANALOPLASTY: TREATMENT STEPS Primary open-angle glaucoma (POAG) is a sightthreatening condition caused by suboptimal
Ab-Interno Canaloplasty A Comprehensive Minimally Invasive Glaucoma Surgery AB-INTERNO CANALOPLASTY: TREATMENT STEPS Primary open-angle glaucoma (POAG) is a sightthreatening condition caused by suboptimal
Implants in glaucoma: a minor review
 Implants in glaucoma: a minor review Dr. Kumar Ravi, Dr. Prashant Srivastava, Dr. Mayav Movdawalla, Dr. Surajit Sen and Dr. Prerna Kedia Author for Correspondence: Dr. Kumar Ravi, Consultant Introduction
Implants in glaucoma: a minor review Dr. Kumar Ravi, Dr. Prashant Srivastava, Dr. Mayav Movdawalla, Dr. Surajit Sen and Dr. Prerna Kedia Author for Correspondence: Dr. Kumar Ravi, Consultant Introduction
Anterior segment imaging
 Article Date: 11/1/2016 Anterior segment imaging AS OCT vs. UBM vs. endoscope; case based approaches BY BENJAMIN BERT, MD, FACS AND BRIAN FRANCIS, MD, MS Currently, numerous imaging modalities are available
Article Date: 11/1/2016 Anterior segment imaging AS OCT vs. UBM vs. endoscope; case based approaches BY BENJAMIN BERT, MD, FACS AND BRIAN FRANCIS, MD, MS Currently, numerous imaging modalities are available
Scope Surgical Management of Co-existing Glaucoma and Cataract
 Scope Surgical Management of Co-existing Glaucoma and Cataract < single image > 4.3cm x 5.5cm Desmond QUEK Jocelyn CHUA Daniel SU What are the options? How is it done? What to look out for and how to get
Scope Surgical Management of Co-existing Glaucoma and Cataract < single image > 4.3cm x 5.5cm Desmond QUEK Jocelyn CHUA Daniel SU What are the options? How is it done? What to look out for and how to get
Contents Optic Nerve: The Glaucomatous Optic Nerve Optic Nerve: Clinical Examination Optic Nerve: Heidelberg Retinal Tomography
 Contents 1 Optic Nerve: The Glaucomatous Optic Nerve................... 1 1.1 Why Is the Optic Nerve Important in the Diagnosis and Management of Glaucoma?............................ 1 References.................................................
Contents 1 Optic Nerve: The Glaucomatous Optic Nerve................... 1 1.1 Why Is the Optic Nerve Important in the Diagnosis and Management of Glaucoma?............................ 1 References.................................................
Retrospective analysis of the success and safety of Gold Micro Shunt Implantation in glaucoma
 Hueber et al. BMC Ophthalmology 2013, 13:35 RESEARCH ARTICLE Open Access Retrospective analysis of the success and safety of Gold Micro Shunt Implantation in glaucoma Arno Hueber 1*, Sigrid Roters 1, Jens
Hueber et al. BMC Ophthalmology 2013, 13:35 RESEARCH ARTICLE Open Access Retrospective analysis of the success and safety of Gold Micro Shunt Implantation in glaucoma Arno Hueber 1*, Sigrid Roters 1, Jens
Gonioscopy and Slit Lamp Exam for the Glaucoma Suspect. Disclosure GONIOSCOPY: Gonioscopy Why?? What should I look for? GONIOSCOPY
 Gonioscopy and Slit Lamp Exam for the Glaucoma Suspect Disclosure Michael Chaglasian has the following disclosures:» 1. Advisory Board: Alcon, Allergan, Bausch+Lomb, Carl Zeiss Meditec, Merck, Sucampo»
Gonioscopy and Slit Lamp Exam for the Glaucoma Suspect Disclosure Michael Chaglasian has the following disclosures:» 1. Advisory Board: Alcon, Allergan, Bausch+Lomb, Carl Zeiss Meditec, Merck, Sucampo»
Case Report Managing Drawbacks in Unconventional Successful Glaucoma Surgery: A Case Report of Stent Exposure
 Case Reports in Ophthalmological Medicine Volume 2015, Article ID 847439, 4 pages http://dx.doi.org/10.1155/2015/847439 Case Report Managing Drawbacks in Unconventional Successful Glaucoma Surgery: A Case
Case Reports in Ophthalmological Medicine Volume 2015, Article ID 847439, 4 pages http://dx.doi.org/10.1155/2015/847439 Case Report Managing Drawbacks in Unconventional Successful Glaucoma Surgery: A Case
Trabeculectomy is the most commonly performed surgery
 ORIGINAL STUDY Standard Trabeculectomy and Ex-PRESS Miniature Glaucoma Shunt: A Comparative Study and Literature Review Elad Moisseiev, MD, Eran Zunz, MD, Rotem Tzur, MD, Shimon Kurtz, MD, and Gabi Shemesh,
ORIGINAL STUDY Standard Trabeculectomy and Ex-PRESS Miniature Glaucoma Shunt: A Comparative Study and Literature Review Elad Moisseiev, MD, Eran Zunz, MD, Rotem Tzur, MD, Shimon Kurtz, MD, and Gabi Shemesh,
STAB INCISION GLAUCOMA SURGERY (SIGS) AMAR AGARWAL
 AMAR AGARWAL") STAB INCISION GLAUCOMA SURGERY (SIGS) AMAR AGARWAL SIGS or Stab Incision Glaucoma Surgery is a guarded filtration procedure that was introduced by me and is slowly but surely becoming popular amongst many
STAB INCISION GLAUCOMA SURGERY (SIGS) AMAR AGARWAL SIGS or Stab Incision Glaucoma Surgery is a guarded filtration procedure that was introduced by me and is slowly but surely becoming popular amongst many
One-year Results of a Schlemm s Canal Microstent for IOP Reduction in Open Angle Glaucoma
 One-year Results of a Schlemm s Canal Microstent for IOP Reduction in Open Angle Glaucoma Thomas W. Samuelson, MD Minnesota Eye Consultants On Behalf of the HYDRUS I Investigators 1 Disclosures This study
One-year Results of a Schlemm s Canal Microstent for IOP Reduction in Open Angle Glaucoma Thomas W. Samuelson, MD Minnesota Eye Consultants On Behalf of the HYDRUS I Investigators 1 Disclosures This study
Recurrent intraocular hemorrhage secondary to cataract wound neovascularization (Swan Syndrome)
") Recurrent intraocular hemorrhage secondary to cataract wound neovascularization (Swan Syndrome) John J. Chen MD, PhD; Young H. Kwon MD, PhD August 6, 2012 Chief complaint: Recurrent vitreous hemorrhage,
Recurrent intraocular hemorrhage secondary to cataract wound neovascularization (Swan Syndrome) John J. Chen MD, PhD; Young H. Kwon MD, PhD August 6, 2012 Chief complaint: Recurrent vitreous hemorrhage,
Understanding Angle Closure
 Case Understanding Angle Closure Dominick L. Opitz, OD, FAAO Associate Professor Illinois College of Optometry 56 year old Caucasian Male Primary Eye Exam BCVA: 20/25 OD with+1.25 DS 20/25 OS with +1.75
Case Understanding Angle Closure Dominick L. Opitz, OD, FAAO Associate Professor Illinois College of Optometry 56 year old Caucasian Male Primary Eye Exam BCVA: 20/25 OD with+1.25 DS 20/25 OS with +1.75
BrightFocus Foundation is the new name for American Health Assistance Foundation.
 In this section, you will find the following: Glaucoma Medications Laser Therapies Conventional Surgical Procedures In the second section, you will find information on how to search for potential treatments
In this section, you will find the following: Glaucoma Medications Laser Therapies Conventional Surgical Procedures In the second section, you will find information on how to search for potential treatments
Clinical Study XEN Glaucoma Implant with Mitomycin C 1-Year Follow-Up: Result and Complications
 Hindawi Journal of Ophthalmology Volume 2017, Article ID 5457246, 5 pages http://dx.doi.org/10.1155/2017/5457246 Clinical Study XEN Glaucoma Implant with Mitomycin C 1-Year Follow-Up: Result and Complications
Hindawi Journal of Ophthalmology Volume 2017, Article ID 5457246, 5 pages http://dx.doi.org/10.1155/2017/5457246 Clinical Study XEN Glaucoma Implant with Mitomycin C 1-Year Follow-Up: Result and Complications
John A. McGreal Jr., O.D. Missouri Eye Associates Old Ballas Rd. St. Louis, MO FAX
 John A. McGreal Jr., O.D. Missouri Eye Associates 11710 Old Ballas Rd. St. Louis, MO. 63141 314.569.2020 314.569.1596 FAX jamod1@aol.com Glaucoma Evolution Glaucoma Evaluation is Transforming In the past,
John A. McGreal Jr., O.D. Missouri Eye Associates 11710 Old Ballas Rd. St. Louis, MO. 63141 314.569.2020 314.569.1596 FAX jamod1@aol.com Glaucoma Evolution Glaucoma Evaluation is Transforming In the past,
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of microinvasive subconjunctival insertion of a trans-scleral gelatin stent for primary
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of microinvasive subconjunctival insertion of a trans-scleral gelatin stent for primary
Chirurgia del Glaucoma: perché tecniche differenti portano a risultati diversi sulla pressione intraoculare
 Università di Verona Dipartimento di Neuroscienze, Biomedicina e Movimento Sezione di Oftalmologia Scuola di Specializzazione in Oftalmologia Direttore: Prof. Giorgio Marchini AOUI di Verona Dipart. Assist.
Università di Verona Dipartimento di Neuroscienze, Biomedicina e Movimento Sezione di Oftalmologia Scuola di Specializzazione in Oftalmologia Direttore: Prof. Giorgio Marchini AOUI di Verona Dipart. Assist.
STAB INCISION GLAUCOMA SURGERY (SIGS)
") STAB INCISION GLAUCOMA SURGERY (SIGS) DR. SOOSAN JACOB Dr. Agarwal's Eye Hospital, Chennai, India dr_soosanj@hotmail.com Youtube channel*: Dr. Soosan Jacob SIGS or Stab Incision Glaucoma Surgery is a guarded
STAB INCISION GLAUCOMA SURGERY (SIGS) DR. SOOSAN JACOB Dr. Agarwal's Eye Hospital, Chennai, India dr_soosanj@hotmail.com Youtube channel*: Dr. Soosan Jacob SIGS or Stab Incision Glaucoma Surgery is a guarded
5-Fluorouracil as an Adjunct in Glaucoma Filtration Surgery in Younger Age Group
 Original Article 5-Fluorouracil as an Adjunct in Glaucoma Filtration Surgery in Younger Age Group Norin Iftikhar Bano, Tariq Mehmood Qureshi, Muhammad Tariq Khan, Harris Muzammil Ansari Pak J Ophthalmol
Original Article 5-Fluorouracil as an Adjunct in Glaucoma Filtration Surgery in Younger Age Group Norin Iftikhar Bano, Tariq Mehmood Qureshi, Muhammad Tariq Khan, Harris Muzammil Ansari Pak J Ophthalmol
Technicians & Nurses Program
 ASCRS ASOA Symposium & Congress Technicians & Nurses Program May 6-10, 2016 New Orleans I have none Sunday, May 8, 2016, 10:30-11:30am Amy Jost, BS, COMT, CCRC Cincinnati Eye Institute Identify the tech
ASCRS ASOA Symposium & Congress Technicians & Nurses Program May 6-10, 2016 New Orleans I have none Sunday, May 8, 2016, 10:30-11:30am Amy Jost, BS, COMT, CCRC Cincinnati Eye Institute Identify the tech
MEDICAL POLICY POLICY TITLE AQUEOUS SHUNTS AND STENTS FOR GLAUCOMA POLICY NUMBER
 Original Issue Date (Created): October 1, 2010 Most Recent Review Date (Revised): January 28, 2014 Effective Date: May 1, 2014 I. POLICY Insertion of aqueous shunts approved by the U.S. Food and Drug Administration
Original Issue Date (Created): October 1, 2010 Most Recent Review Date (Revised): January 28, 2014 Effective Date: May 1, 2014 I. POLICY Insertion of aqueous shunts approved by the U.S. Food and Drug Administration
Managing & Avoiding Post-Op Complications in Tube Surgeries
 Managing & Avoiding Post-Op Complications in Tube Surgeries K. Sheng Lim St. Thomas Hospital, London shenglim@gmail.com Current GDD Molteno 1969 Baerveldt 1990 Ahmed 1993 Current GDD GDD Plate Material
Managing & Avoiding Post-Op Complications in Tube Surgeries K. Sheng Lim St. Thomas Hospital, London shenglim@gmail.com Current GDD Molteno 1969 Baerveldt 1990 Ahmed 1993 Current GDD GDD Plate Material
MEDICAL POLICY. SUBJECT: AQUEOUS DRAINAGE DEVICES (STENTS AND SHUNTS) POLICY NUMBER: CATEGORY: Technology Assessment
 POLICY NUMBER: CATEGORY: Technology Assessment") MEDICAL POLICY PAGE: 1 OF: 8 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical policy criteria are not applied.
MEDICAL POLICY PAGE: 1 OF: 8 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical policy criteria are not applied.
Aqueous Shunts and Stents for Glaucoma Corporate Medical Policy
 Aqueous Shunts and Stents for Glaucoma Corporate Medical Policy File name: Aqueous Shunts and Stents for Glaucoma File code: UM.SURG.18 Origination: New Policy Last Review: 06/2017 Next Review: 06/2018
Aqueous Shunts and Stents for Glaucoma Corporate Medical Policy File name: Aqueous Shunts and Stents for Glaucoma File code: UM.SURG.18 Origination: New Policy Last Review: 06/2017 Next Review: 06/2018
SAFE, PERMANENT EYE-COLOR CHANGE
 SAFE, PERMANENT EYE-COLOR CHANGE Prepared by Gregg Homer JSD (PhD) February 1, 2012 THE PIGMENTARY GLAUCOMA ISSUE Glaucoma Defined Glaucoma is currently defined as a disturbance of the structural or functional
SAFE, PERMANENT EYE-COLOR CHANGE Prepared by Gregg Homer JSD (PhD) February 1, 2012 THE PIGMENTARY GLAUCOMA ISSUE Glaucoma Defined Glaucoma is currently defined as a disturbance of the structural or functional
Viscocanalostomy and Canaloplasty
 Viscocanalostomy and Canaloplasty Policy Number: 9.03.26 Last Review: 9/2017 Origination: 9/2012 Next Review: 9/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for
Viscocanalostomy and Canaloplasty Policy Number: 9.03.26 Last Review: 9/2017 Origination: 9/2012 Next Review: 9/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for
GLAUCOMA SURGICAL TREATMENTS
 GLAUCOMA SURGICAL TREATMENTS UnitedHealthcare Commercial Medical Policy Policy Number: OPT014 Effective Date: May 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE... 1 BENEFIT CONSIDERATIONS... 1 COVERAGE
GLAUCOMA SURGICAL TREATMENTS UnitedHealthcare Commercial Medical Policy Policy Number: OPT014 Effective Date: May 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE... 1 BENEFIT CONSIDERATIONS... 1 COVERAGE
MEDICAL POLICY. SUBJECT: AQUEOUS DRAINAGE DEVICES (STENTS AND SHUNTS) POLICY NUMBER: CATEGORY: Technology Assessment
 POLICY NUMBER: CATEGORY: Technology Assessment") MEDICAL POLICY Clinical criteria used to make utilization review decisions are based on credible scientific evidence published in peer reviewed medical literature generally recognized by the medical community.
MEDICAL POLICY Clinical criteria used to make utilization review decisions are based on credible scientific evidence published in peer reviewed medical literature generally recognized by the medical community.