Disclosure Statement 8/25/2014. Lecture Goals. Sports Concussion: The Diagnostic and Return to Play Dilemma
|
|
|
- Barrie Washington
- 5 years ago
- Views:
Transcription

1 Evidence-Based Clinical Management of Sports Concussion: What are we Learning? Micky Collins, PhD University of Pittsburgh Medical Center Department of Orthopaedic Surgery Department of Neurological Surgery Program Director UPMC Sports Concussion Program Disclosure Statement Micky Collins, PhD is a Co-Founder and Board Member of ImPACT Applications, a computerized neurocognitive test battery developed to assess sports concussion and Mild Traumatic Brain Injury. Lecture Goals Discuss the biomechanics, pathophysiology, and signs/symptoms of sports-related mtbi Discuss clinical recovery rates following sports-related mtbi and risk profiles that predict more protracted recovery Discuss the role of computerized neurocognitive testing and vestibular-ocular screening as effective tools in the assessment and management of sports-mtbi Discuss the role of a multidisciplinary treatment team and the concept of targeted clinical pathways for the rehabilitation of sports mtbi Present a case study of effective concussion management Sports Concussion: The Diagnostic and Return to Play Dilemma 1




2 Linear Injury Rotational Injury 2


3 3
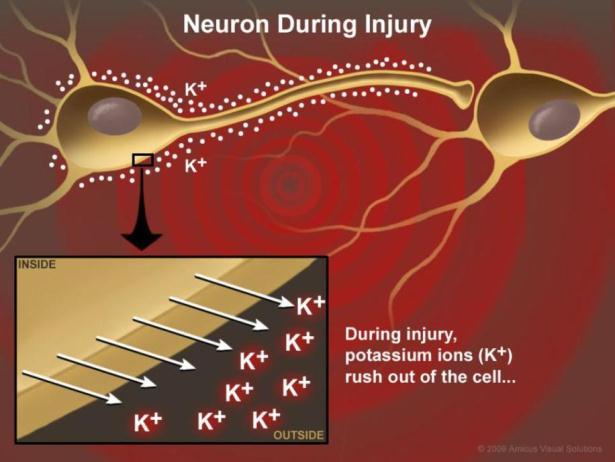
 400 Calcium % of normal 300 200 K+")

4 Neurometabolic Cascade Following Cerebral Concussion/MTBI 500 (Giza & Hovda, 2001) 400 Calcium % of normal K+ Glucose Glutamate minutes hours days Cerebral Blood Flow UCLA Brain Injury Research Center 4

5 Concussion Management: Areas of Focus Rule out more serious intracranial pathology CT, MRI, neurologic examination primary diagnostic tests Prevent against Second Impact Syndrome Prevent against cumulative effects of injury Less biomechanical force causing extension of injury Prevent presence of Post-Concussion Syndrome 5

6 Most Commonly Reported Symptoms 1-7 days following concussion SYMPTOM # 1 Headache 75% PERCENT # 2 Difficulty Concentrating 57 % # 3 Fatigue 52 % # 4 Drowsiness 51 % # 5 Dizziness 49 % # 6 Foggy 47 % # 7 Feeling Slowed Down 46 % # 8 Light Sensitivity 45 % # 9 Balance Problems 39 % # 10 Difficulty with Memory 38 % Kontos, Elbin, French Collins, AJSM, 2012; N = 1,438 Symptoms may evolve over time. Delayed symptoms may occur Factor Analysis, Post-Concussion Symptom Scale N=1,438 High School & University Athletes at 1-7 Days Post- Concussion Vomiting Numbness Diff. Remembering Foggy Dizziness Sadness More Emotional Nervous Diff. Concentrating Sensitivity Light/Noise Slowed Down Drowsiness Fatigue Headache Sleep Less Trouble Falling Asleep Kontos, Elbin, Schatz, Covassin, Henry, Pardini, Collins; AJSM, 2012 The Evolving Definition of Concussion Centers for Disease Control A concussion (or mild traumatic brain injury) is a complex pathophysiological process affecting the brain, induced by traumatic biomechanical forces secondary to direct or indirect forces to the head. Disturbance of brain function is related to neurometabolic dysfunction, rather than structural brain injury, and is typically associated with normal structural imaging findings (CT Scan, MRI). Concussion may or may not involve a loss of consciousness. Concussion results in a constellation of physical, cognitive, emotional, and sleep-related symptoms. Recovery is a sequential process and symptoms may last from several minutes to days, weeks, months, or even longer in some cases. Management of Sports Concussion: Topics of Concern No imaging technique or biomarker available to diagnose injury Lack of well controlled, prospective studies on long-term outcomes Lack of targeted clinical and treatment pathways Variability in clinical management and treatment recommendations Rest does not cure all concussions Media hysteria driving public perception Self-report predicating management directives. 6
7 Return to Play Following mtbi: In some cases (not all), athletes will minimize difficulties Athletes are naïve to the subtleties of the injury (particularly youth athletes) Relying on subjective status of a patient with brain injury Studies suggest that up to 50% of athletes experience concussion symptoms per year but only 10 % report having an injury Need for comprehensive understanding of athletes recovery status 25 Computer-Based Neurocognitive Testing Cogsport (Axon) Headminders (CRI) ANAM CNS Vital Signs ImPACT Computerized Neurocognitive Testing: Post-Concussion Evaluation Minute, On-Line Office-Based Tool Concussion Symptom Scale 21 Item Likert Scale (e.g. headache, dizziness, nausea, etc) 8 Neurocognitive Measures Verbal Memory, Visual Memory, Reaction Time, Processing Speed Summary Scores Detailed Clinical Report Outlines Demographic, Symptom, Neurocognitive Data Internal baseline validity checks built into program (demarcates poor effort) On-Line Version Available Extensive normative data available from ages Over 175 peer-reviewed research articles published since 2000 Extensive data published on reliability, validity, sensitivity/specificity, added value, and prognostic ability of test 7



 (Probability that that a concussion is present when test is positive) Specificity (70.1%) (Probability that a concussion is not present when test is negative) 8")
8 Concussion Evaluation Timeline- Computerized Neurocognitive Testing Pre-season 1-3 Days Does Computerized Neurocognitive Testing Work? Examining Sensitivity/Specificity of Testing Baseline testing Concussion First follow-up Follow-up testing as needed Supervised by ATC, PT Physician, Clinic, or School Sideline Evaluation -Any symptoms of mtbi precludes RTP for remainder of contest Post-Injury Office/Clinic Evaluation -Interpreted by Trained Clinician Return to play Sensitivity and Specificity of Computerized Neurocognitive Testing Schatz P, Sandel N. Sensitivity and Specificity of the online version of ImPACT in high school and collegiate athletes. American Journal of Sports Medicine, Two Athlete Groups Examined Study 1 (Concussed symptomatic athletes) 162 athletes 81 concussed athletes (diagnosed by ATC/Physician) 81 carefully matched controls (non-concussed) matched on specific basis of gender, sport, concussion history, absence of LD/ADD Discriminate Function Analysis on subscale scores; no clinician input Testing completed within 3 days post injury Sensitivity/Specificity of neurocognitive testing determined Sensitivity and Specificity of Computerized Neurocognitive Testing Schatz P, Sandel N. Sensitivity and Specificity of the online version of ImPACT in high school and collegiate athletes. American Journal of Sports Medicine, Study 1 (Concussed symptomatic athletes) Sensitivity (91.4%) (Probability that that a concussion is present when test is positive) Specificity (70.1%) (Probability that a concussion is not present when test is negative) 8
9 Sensitivity and Specificity of Computerized Neurocognitive Testing Schatz P, Sandel N. Sensitivity and Specificity of the online version of ImPACT in high school and collegiate athletes. American Journal of Sports Medicine, Study 2 (Asymptomatic concussed athletes) 74 Athletes 37 athletes diagnosed with on-field concussion by ATC/physician, seen within 3 days of injury, and symptom score of 0 37 carefully matched controls (non-concussed) matched on specific basis of gender, sport, concussion history, absence of LD/ADD Discriminate Function Analysis on Subscale scores; no clinician input Testing completed within 3 days post injury Sensitivity/Specificity of Computerized Neurocognitive Testing determined Sensitivity and Specificity of Computerized Neurocognitive Testing Schatz P, Sandel N. Sensitivity and Specificity of the online version of ImPACT in high school and collegiate athletes. American Journal of Sports Medicine, Study 2 (Asymptomatic concussed athletes) Sensitivity (94.6%) (Probability that that a concussion is present when test is positive) Specificity (97.3%) (Probability that a concussion is not present when test is negative) Does Computerized Neurocognitive Testing Work? Examining the Reliability of Testing One Year Stability of Computer NP Testing in a High School Sample (On-Line Version) Verbal Memory Visual Memory Process Speed RT Symptoms Time Time r Inter-class correlation coefficients. N=369 non concussed athletes, DF=368, Bonferonni correct alpha p<.01 Schatz, AJSM,

10 Domain Mean RCI 90% Confidence Interval Verbal Memory Score Time Time Visual Memory Score Time Time Processing Speed Score Time Time Reaction Time Score Time Time Symptom Score Time Time Test-Retest Reliable Change Index Scores for Test Battery Reliable change methodology is designed to identify cutoffs that can be used for meaningful comparisons of test scores that are independent of practice effects and other sources of variance Iverson et al, TCN 2005 Composite Score Summary of Results Summary composite scores for Verbal Memory, Visual Memory, Reaction Time, Processing Speed, and Impulse Control Authors Sample Size Population Tests Utilized Total Days Cognitive Resolution Total Days Symptom Resolution Measuring Neurocognitive Recovery from Sports mtbi Lovell et al McCrea et al McCrea et al Echemendia 2001 Guskiewicz et al Pro (NFL) Paper and Pencil NP 1 day 1 day 94 College SAC <1 Day 7 days 94 College Paper and 5-7 days 7 days Pencil NP 29 College Paper and Pencil 3 days 3 days NP 94 College Balance 3-5 Days 7 Days BESS Bleiberg et al Iverson et al McClincy et al Lovell, Collins et al 2008 Covassin et al 2011 Maugans et al College Computer NP 30 High School Computer NP 104 High School Computer NP 208 High School Computer NP 72 High School Computer NP 12 Ages Computer NP 3-7 days Did Not Evaluate 10 days 7 Days 14 days 7-10 Days 26 days 17 Days 21 days 7 Days 30 days 14 Days 10
11 Individual Recovery From High School Football- Related Concussion: How Long Does it Take? WEEK 1 WEEK 2 WEEK 3 WEEK 4 WEEK 5 40% RECOVERED 60% RECOVERED 80% RECOVERED N=134 Concussions All Athletes No Previous Concussions 1 or More Previous Concussions Collins et al., Neurosurgery 3 Year Prospective Study of 17 High School American FootballTeams N=2,141 Prognosticating Complicated Concussion Outcomes: An Evidence-Based Analysis Which On-Field Symptoms Predict Protracted Recovery (> 3 weeks of recovery time) Lau B, Kontos A, Lovell MR, Collins MW; AJSM 2011 Which On-Field Symptoms Predict Protracted Recovery Time? Methodology 176 male high school and college football players Athletes had baseline neurocognitive testing and were revaluated within three days of injury. All followed until clinical recovery Within RCI of baseline on for neurocognitive/symptom scores 32% of sample required < 7 days until recovery (N =56) Rapid Recovery (Mean=4.9 days) 17% of sample required > 21 Days until recovery (N=31) Protracted Recovery (Mean =33.2 days) 39% of sample required 7-14 days until recovery (N = 68) (Continued) 11
 (N = 21) MANOVA used to determine differences between rapid/> 3 week recovery ATC s documented on-field markers (e.g.")
 Which On-Field Markers/Symptoms Predict 3 or More Week Recovery from MTBI In High School Football Players On-Field Marker N Chi 2 P Odds Ratio 95% Confidence Interval Posttraumatic Amnesia 92 1.")

12 Which On-Field Symptoms Increase Risk of Post Concussion Syndrome in Football Players? (Continued) 12% lost to follow up (e.g. did not RTP or no follow-up in clinic) (N = 21) MANOVA used to determine differences between rapid/> 3 week recovery ATC s documented on-field markers (e.g. LOC, Confusion, Amnesia) and onfield Symptoms (e.g. headache, dizziness, balance, photosensitivity, etc.) Which On-Field Markers/Symptoms Predict 3 or More Week Recovery from MTBI In High School Football Players On-Field Marker N Chi 2 P Odds Ratio 95% Confidence Interval Posttraumatic Amnesia Retrograde Amnesia Confusion LOC On-Field Symptom N Chi 2 P Odds Ratio 95% Confidence Interval Dizziness** Headache Sensitivity LT/Noise Visual Problems Fatigue Balance Problems Personality Change Vomiting **p<.01 Lau B, Kontos A, Lovell MR, Collins MW, AJSM 2011 The total sample was 107. Due to the normal difficulties with collecting on-field markers, there were varying degrees of missing data. The number of subjects who had each coded ranged from The N column represents the number of subjects for whom data were available for each category. Markers of injury are not mutually exclusive. Lau, Kontos, Collins, AJSM 2011 Which Symptoms at 3 Days Post Injury Best Predict Protracted Recovery? Lau B, Lovell MR, Collins MW; Pardini J; CJSM 2009 (3): Current Symptoms Headache Nausea Vomiting Balance Problems Dizziness Fatigue Trouble falling asleep Sleeping more than usual Sleeping less than usual Drowsiness Sensitivity to light Sensitivity to noise Irritability Sadness Nervousness Feeling more emotional Numbness or tingling Feeling slowed down Feeling mentally foggy Difficulty concentrating Difficulty remembering Lau B, Lovell MR, Collins MW; Pardini J; CJSM 2009 (3): Visual problems (blurry or double vision) 12
. Only includes symptoms with large (greater than.80) effect sizes. Sample is composed of 108 male high school football athletes. Lau, Lovell, Collins et al.")

13 Top 11 Symptom Predictors of Protracted Recovery Do Post-Traumatic Migraine Symptoms Predict Protracted Recovery Following Concussion? Kontos A, Elbin RJ, Collins MW et al. AJSM, Expressed as Effect Sizes (Cohen s D). Only includes symptoms with large (greater than.80) effect sizes. Sample is composed of 108 male high school football athletes. Lau, Lovell, Collins et al. 2009, CJSM Post-traumatic Migraine (PTM) Defined Post-traumatic Migraine Headache, nausea, AND sensitivity to light OR noise (International Headache Society Guidelines) Determined by utilizing PCSS at 1-7 days post-concussion Kontos AP, Elbin RJ, Lau B, Simensky S, Freund B, French J, Collins MW; AJSM, 2013 Study Overview 174 high school athletes with a concussion No prior hx of LD, moderate TBI, psychiatric disorder Athletes followed until recovery Neurocognitive scores returned to baseline (w/in RCI) Symptom free and rest and exertion 97 athletes met Rapid or Protracted Criteria for Recovery: Rapid ( 7 days)= 61 Protracted ( 21 days)= 36 Recovery studied for three groups No headache group Headache only group Post-traumatic migraine group (headache with nausea and/or light and noise sensitivity) Data Analysis Chi-square analysis with Odds Ratios for Recovery Time Groups Repeated measures ANOVAs for computerized neurocognitive test scores across 3 time periods Kontos AP, Elbin RJ, Lau B, Simensky S, Freund B, French J, Collins MW; AJSM,
-Kontos, Elbin, Collins et al, AJSM, In Press. Variable Wald p PTM v. No Headache Headache v.")
14 How do Sub-acute Post-traumatic Migraine (PTM) symptoms compare to No Headache and Headache groups in predicting Protracted (>21 days) Recovery from Sports Concussion? (N= 97)-Kontos, Elbin, Collins et al, AJSM, In Press. Variable Wald p PTM v. No Headache Headache v. No Headache PTM Group = Headache with Nausea and/or Light or Noise Sensitivity-IHS criteria Headache Group= Headache only Odds Ratio 95% CI PTM v. Headache It s More than Just a Headache! Visual Memory Raw Score PTM = Post Traumatic Migraine N = 97 HS Athletes with concussion Comparison of Visual Memory scores for PTM, Headache, and No PTM or Headache groups (λ=.88, F= 4.24, p=.002, η 2 =.06)* *PTM significantly different than both groups at 1-7 and 8-14 days PTM defined as headache with nausea and sensitivity to light or noise (IHS Classification) Determination of Neurocognitive Cutoff Scores that Predict 3 or more weeks of recovery Lau B, Collins MW, Lovell MR Neurosurgery 2012;Feb 70(2): Cutoff Values of Neurocognitive Scores at 2 Days Post Injury That Predict Protracted Recovery 75% Sensitivity 80% Sensitivity 85% Sensitivity Neurocognitive Domain Cutoff Cutoff Cutoff Verbal Memory Visual Memory Processing Speed Reaction Time Sensitivity is defined as the ability of the cutoff to accurately identify protracted recovery (Mean = 1 month) in an athlete. Lau B, Collins MW, Lovell MR. Neurosurgery
15 Case Example: NFL Defensive Back Established (?) Constitutional Risk Factors For More Complicated Recovery Following Concussion Younger Age - Field, Lovell, Collins et al. J of Pediatrics, Pellman, Lovell et al. Neurosurgery, 2006 Migraine History & Symptoms - Mihalik, Collins, Lovell et al, J Neurosurgery, Kontos, Collins, Elbin, French, Simenski, AJSM, Learning Disability - Collins, Lovell et al, JAMA, Kontos, Elbin, Collins, Brain, 2013 Repetitive Concussion - Collins, Lovell et al, Neurosurgery, Iverson et al, CJSM, Moser et al, JCEN, 2011 Female Gender - Colvin, Lovell, Pardini, Mullin, Collins, AJSM, Covassin et al, CJSM, 2009 What We Know Outcomes are highly variable Vestibular-related symptoms (dizziness/fogginess) and migraine history/symptoms best predict protracted recoveries Effective sideline management is key-removal from play a must when symptoms occur Return to play prior to full recovery from concussion will result in worse outcome and less force causing re-injury. Neurocognitive testing is an effective tool to help quantify the injury and guide the management and RTP process. The mild injuries may become complicated and the severe injuries may become mild Proper Clinical management is best form of prevention Targeted clinical pathways for treatment and rehabilitation are being established Establishing a Clinical Model of Care for Managing Sports Concussion: Targeted Assessment, Treatment and Rehabilitation Micky Collins, PhD University of Pittsburgh Medical Center Department of Orthopaedic Surgery Department of Neurological Surgery Program Director UPMC Sports Concussion Program 15


16 The UPMC Sports Medicine Concussion Program Department of Orthopaedic Surgery UPMC Sports Medicine Concussion Program Referral Sources Emergency Departments Pediatric Practices Certified Athletic Trainers Primary Care Physicians UPMC Sports Concussion Program: Comprehensive Assessment Approach Neurocognitive Over 20, 000 patient visits annually UPMC Concussion Program (Neuropsychology) Vestibular Physical Exertion Concussion Primary Care Sports Med PM & R Vestibular / Physical Therapy Neuro Radiology Orthopaedic /Neurosurgery Behavioral Neuro- Optometry Ocular- Motor Symptoms Further Assessment and Treatment-If Indicated 16




17 Concussion Clinical Trajectories: A New Model for Understanding Assessment, Treatment and Rehabilitation? Vestibular Using Concussion Clinical Trajectories to Inform Targeted Treatment Pathways Pre-Existing Risk Factors Extensive Data Published on Risk Factors Concussion Concussion Clinical Trajectories Treatment and Rehab Pathways Anxiety/ Mood Concussion Ocular Previous Concussions Migraine LD/ADHD Ocular Vestibular Cognitive Cervical Post- Traumatic Migraine Cognitive/ Fatigue Female Gender Age Motion sensitivity, Ocular Dysfunction Migraine Cervical Anxiety/ Mood UPMC Clinical Evaluation Detailed Clinical Interview Computerized Neurocognitive Testing Vestibular-Ocular Screening Patient feedback Severity of Injury Subtype-Trajectory of Injury? Prognosis for Recovery? Need for Further Assessment/Treatment? Vestibular Therapy? Vision Therapy? Medication Management? Type/Level of Physical Exertion Allowed? Academic Accommodations? Return to Play? In-Office Evaluation Clinical Interview Computerized Neurocognitive Testing Vestibular-Ocular Screening 17

 Symptoms Reported By Patient on 0-10 Point Scale UPMC Vestibular/Ocular Motor Screening Form (VOMS) 0 0 0 0 0 0 0 0 2 0")
18 Why Assess the Vestibular-Ocular Systems? Subjective Complaints of Dysfunction Dizziness, Fogginess, Feeling detached, Fatigue Motion discomfort, Nausea Intolerance to busy places Anxiety/Irritability Difficulty focusing, Blurred vision, Difficulty with Math/Reading Impaired balance UPMC Vestibular/Ocular Motor Screening Form (VOMS) Symptoms Reported By Patient on 0-10 Point Scale UPMC Vestibular/Ocular Motor Screening Form (VOMS) cm 10 cm 12 cm Symptoms Reported By Patient on 0-10 Point Scale 18
19 Purpose Vestibular-Ocular Motor Screening (VOMS) Assessment Preliminary Findings for the Validity, Reliability, and Relationship of the VOMS to Established Measures 1. Describe the VOMS and provide initial support for the validity and reliability of the measure. 2. Examine the relationship of the VOMS to established measures (e.g., computerized neurocogntive testing, symptoms, and clinical balance measures). Mucha, Collins, Elbin, Furman, Troutman-Enseki, DeWolf, Kontos. (In Review). Mucha, Collins, Elbin, Furman, Troutman-Enseki, DeWolf, Kontos. (In Review). Overview Participants: 85 consecutive patients (M = 14.07, +/ yrs) seen at 5.66 days (SD = 5.18) following a diagnosed sport-related concussion. 85 controls (M= ± 1.80 yrs) randomly selected from 112 consecutive athletes who participated in a concussion education and outreach testing program. Procedures: Trained clinicians administered the following assessments: Vestibular/Ocular Motor Screening (VOMS), Post-concussion Symptom Scale (PCSS), Immediate Post-concussion Assessment and Cognitive Test (ImPACT), and Balance Error Scoring System (BESS)- concussed only Vestibular-Ocular Motor Screening (VOMS) Assessment Is the VOMS reliable? Mucha, Collins, Elbin, Furman, Troutman-Enseki, DeWolf, Kontos. (In Review). 19
20 The VOMS is Reliable The internal consistency of the VOMS total symptom scores and the NPC distance was high: Cronbach s alpha = 0.91 All of the items contributed positively to the overall reliability of the VOMS Mucha, Collins, Elbin, Furman, Troutman-Enseki, DeWolf, Kontos. (In Review). Vestibular-Ocular Motor Screening (VOMS) Assessment Is the VOMS Sensitive? What is the Diagnostic Accuracy of the VOMS? Nearly 60% of patients report at least one provoked symptom following the VOMS (N = 85). Concussed patients (n=85) score higher on ALL VOMS items* than controls (n=85). Symptomatic (n) Smooth Pursuits 33% (28) Horizontal Saccades 42% (36) Vertical Saccades 38% (32) Vestibular Ocular Reflex 58% (49) Visual-Motion Sensitivity 49% (42) Convergence 34% (29) VOR was associated with the highest percentage (58%) of patients reporting symptom provocation AND the highest average number of total endorsed symptoms (3.99) *p< * Smooth Pursuits 2.9 * 2.6 * 4 * 3.5 * Hor. Saccades Ver. Saccades Concussed 6.1 * 1.8 VOR VMS NPC (cm) Controls Mucha, Collins, Elbin, Furman, Troutman-Enseki, DeWolf, Kontos. (In Review). Mucha, Collins, Elbin, Furman, Troutman-Enseki, DeWolf, Kontos. (In Review). 20
21 Strongest predictors were: VOR (OR = 4.11) and VMS (OR = 3.62) Mucha, Collins, Elbin, Furman, Troutman-Enseki, DeWolf, Kontos. (In Review). ALL VOMS symptom scores and NPC distance were significant predictors of being in the concussed group (N=170). Variable Significance Odds Ratio Smooth Pursuit Saccades Horizontal Saccades Vertical NPC (Symptoms) NPC (Distance) Vestibular Ocular Reflex Visual Motion Sensitivity R- Squared < < Increasing Diagnostic Accuracy with Cut-off Scores NPC distance 5 cm = 34% increase in probability of identifying a patient with concussion. A symptom score > 2 on any VOMS item= 46% increase in probability of identifying a patient with concussion. 50% 16% NPC Chance > 5cm 50% 84% VOMS Item Sx > 2 4% 96% Correct Incorrect Correct Incorrect 1 The Diagnostic Accuracy of the VOR, VMS and NPC (adj. for age) for Predicting Concussed Patients is Excellent (.90 [95% CI= ], p<.001). 3 VOMS Items=.90! Dotted line=.50 or no better than chance Vestibular-Ocular Motor Screening (VOMS) Assessment Receiver Operating Characteristic Curve Positive Prediction Rate of 90% Are there Gender Differences on the VOMS? * Model variables: ln(age), VOR, VMS and NPC distance, dotted line indicates AUC =
, BESS (balance), and ImPACT (neurocognitive function)? Mucha, Collins, Elbin, Furman, Troutman-Enseki, DeWolf, Kontos. (In Review).")
22 Females (n= 35) report more symptoms on the VOR, VMS, and higher NPC distance than males (n= 50) Vestibular-Ocular Motor Screening (VOMS) Assessment What is the Relationship of the VOMS to PCSS (symptoms), BESS (balance), and ImPACT (neurocognitive function)? Mucha, Collins, Elbin, Furman, Troutman-Enseki, DeWolf, Kontos. (In Review). VOMS Items Correlate with Total Concussion Symptom Scores on PCSS (N= 85) VOMS is NOT Balance (N= 85) Smooth Pursuit Symptom Score Hor. Saccades Symptom Score Ver. Saccades Symptom Score Correlation with PCSS Total.36*.52*.48* NPC Symptoms.49* NPC Distance.21 VOR Symptoms.44* VMS Symptoms.40* All VOMS symptom scores were moderately positively correlated to PCSS total scores NPC Distance was not correlated to PCSS total score *p<.05 Smooth Pursuit Symptom Score Hor. Saccades Symptom Score Ver. Saccades Symptom Score Correlation with BESS Total Error Score NPC Symptoms.06 NPC Distance.15 VOR Symptoms -.05 VMS Symptoms.11 The average total BESS error score in concussed patients=

23 VOMS Correlates with Computerized Neurocognitive Performance (N= 85) Verbal Memory Visual Memory Process. Speed Reaction Time Smooth Pursuits Hor. Saccades Ver. Saccades VOR VMS NPC Distance -.23* -.26* -.28* * -.26* -.22* -.20* -.30** * -.27* -.25* -.29** * -.27*.40**.31*.33**.20.27*.48** *p<.05, **p<.01 Nearly all VOMS symptom scores and NPC Distance were moderately negatively correlated with ImPACT neurocognitive performance (except VOR) Conclusion Nearly 60% of concussed patients report at least one provoked symptom on the VOMS. The VOMS is a reliable and brief clinical screen for vestibular and ocular motor impairment/symptoms. Females report more symptoms on the VOMS and higher NPC distances. Cut-off for VOMS symptom score (>2) and NPC distance (>5cm) increased diagnostic accuracy 34% and 46% respectively. Mucha, Collins, Elbin, Furman, Troutman-Enseki, DeWolf, Kontos. (In Review). Conclusion VOR, VMS and NPC Distance items of the VOMS resulted in a 90% positive prediction rate for patients with concussion. The VOMS is related to total concussion symptom scores. The VOMS assesses a construct that is unique from balance following sport-related concussion. The VOMS is related to ImPACT neurocognitive performance following sport-related concussion. Mucha, Collins, Elbin, Furman, Troutman-Enseki, DeWolf, Kontos. (In Review). PART II: Using Concussion Clinical Trajectories to Inform Targeted Clinical Management Pathways: Putting it all Together Micky Collins, PhD Collins MW, Kontos A, et al, KSST,



24 Concussion Clinical Trajectories: A Model for Understanding Assessment, Treatment and Rehabilitation Anxiety/ Mood Cervical Vestibular Concussion Post- Traumatic Migraine Ocular Cognitive/ Fatigue Clinical Trajectories Determined by: Clinical Interview *Constitutional risk factors *Symptom clusters *What questions to ask? Vestibular-Ocular Screening *Provocative or not? *Specific findings help determine level/type of exertional activity Computerized Neurocognitive Testing *Specific cognitive profiles for specific clinical trajectories Findings lead to individually determined treatment and rehabilitation plan Assessment Vestibular Constitutional risk factors- car sickness/motion sensitivity Symptoms: slow/wavy dizziness, foggy, one-step behind, nausea, feeling of being overwhelmed in high stimulus areas Some Questions to Ask Do busy environments cause you to have a headache or feel foggy, dizzy, anxious, tired? Do you become dizzy when looking up/down, turning head, walking down busy hallways? Do quick movements make you dizzy, foggy, anxious? Vestibular-Ocular Screening symptom provocation VOR (vertical and/or horizontal) Visual motion sensitivity Computerized Neurocognitive Test Results Deficits predominantly with Visual Motor Speed 93 Collins MW, Kontos A, et al, KSST, Collins MW, Kontos A, et al, KSST, 2014 Vestibular Treatment 95 Vestibular therapy Dynamic physical exertion protocol-at end stages of vestibular therapy Pharmacological (done only if there is mood, migraine, sleep overlay) Clonazepam-if anxiety/rumination is present Tricyclics-If migraine overlay SSRIs--mood overlay Melatonin, Trazodone, Zolpidem-if sleep overlay 24
25 97 Anxiety/ Mood Cervical Concussion Clinical Trajectories Vestibular Concussion Post- Traumatic Migraine Ocular Cognitive/ Fatigue Clinical Trajectories Determined by: Clinical Interview *Constitutional risk factors *Symptom clusters *What questions to ask? Vestibular-Ocular Screening *Provocative or not? *Specific findings help determine level/type of exertional activity Computerized Neurocognitive Testing *Specific cognitive profiles for specific clinical trajectories Findings lead to individually determined treatment and rehabilitation plan Collins MW, Kontos A, et al, KSST, Assessment Anxiety/ Mood Constitutional Risk Factors- Personal/Family hx of Anxiety, entire Engineering profession, Mom of child has thick notebook Symptoms: ruminative thoughts, hypervigilant, fastidious, feelings of being overwhelmed, difficulties initiating/maintaining sleep. Some Questions to Ask How often do you take inventory on your symptoms? Do you have a difficult time turning off your thoughts? Do you become symptomatic when thinking about your symptoms? Have social activities been restricted? How often do your parents ask about your symptoms? Vestibular-Ocular Screening symptom provocation Normal or only mildly provocative (more provocative if vestibular overlay) Computerized Neurocognitive Test Results NORMAL- if no vestibular component If vestibular component-deficits with Visual Motor Speed (treat vestibular component first!!) Collins MW, Kontos A, et al, KSST, 2014 Treatment Anxiety/ Mood Supervised Exertional Therapy (if vestibular component resolved)-push them hard!! Grandma Talk! (Regulated schedule, sleep, exercise, diet, hydration, stress) Psychotherapy Pharmacological Antidepressants SSRIs Benzodiazepines Clonazepam Anxiety/ Mood Cervical Concussion Clinical Trajectories Vestibular Concussion Post- Traumatic Migraine Ocular Cognitive/ Fatigue Clinical Trajectories Determined by: Clinical Interview *Constitutional risk factors *Symptom clusters *What questions to ask? Vestibular-Ocular Screening *Provocative or not? *Specific findings help determine level/type of exertional activity Computerized Neurocognitive Testing *Specific cognitive profiles for specific clinical trajectories Findings lead to individually determined treatment and rehabilitation plan Collins MW, Kontos A, et al, KSST,


26 Exam Type Post-Injury Date Tested 10/12/12 Assessment Ocular Constitutional Risk Factor- Personal/Family hx of ocular dysfunction Symptoms: Frontal headache, fatigue, distractible, difficulties with visually based classes, pressure behind the eyes, focus issues Some Questions to Ask Do you feel a frontal pressure in your head /behind eyes when reading/computer work/taking notes in class? Do you have blurred or fuzzy vision while reading or difficulty reading? Are you having more significant difficulty in Math and/or Science? Computerized neurocognitive test results Deficits with Visual Memory, Reaction Time Deficits with encoding rather than retrieval Vestibular Ocular Screening symptom provocation Pursuits/Saccades Near Point of Convergence (>5cm) 101 Collins MW, Kontos A, et al, KSST, 2014 Word Memory WG = 1 Hits (immediate) 6 Correct distractors (immed.) 6 Learning percent correct 100% Hits (delay) 6 Correct distractors (delay) 9 Delayed memory pct. Correct 57% Total percent correct 61% Design Memory Hits (immediate) 5 Correct distractors (immed.) 6 Learning percent correct 71% Hits (delay) 7 Correct distractors (delay) 8 Delayed memory pct. Correct 50% Total percent correct 67% X's and O's Total correct (memory) 6 Total correct (interference) 115 Avg. correct RT (interference) 0.71 Total incorrect (interference) 7 Avg. incorrect RT (interfer.) 0.37 Symbol Match Total correct (visible) 27 Avg. correct RT (visible) 1.89 Total correct (hidden) 4 Avg. correct RT (hidden) 1.06 Color Match Total correct 9 Avg. correct RT 0.92 Total commissions 1 Avg commissions RT 0.57 Three Letters Total sequence correct 3 Total letters correct 11 Pct. Of total letters correct 71% Avg. time to first click 1.95 Avg. counted 13.2 Avg. counted correctly Treatment Ocular Vestibular therapy with ocular-motor focus (if NPC < 20cm) Vision therapy (if NPC > 20cm or other complicated presentation) Dynamic physical exertion protocol (isolated binocular dysfunction will not result in symptoms with dynamic exertion) Anxiety/ Mood Cervical 103 Concussion Clinical Trajectories Vestibular Concussion Post- Traumatic Migraine Ocular Cognitive/ Fatigue Clinical Trajectories Determined by: Clinical Interview *Constitutional risk factors *Symptom clusters *What questions to ask? Vestibular-Ocular Screening *Provocative or not? *Specific findings help determine level/type of exertional activity Computerized Neurocognitive Testing *Specific cognitive profiles for specific clinical trajectories Findings lead to individually determined treatment and rehabilitation plan Collins MW, Kontos A, et al, KSST, 2014 Assessment Cognitive/ Fatigue Constitutional Risk Factor-Hx of Learning Disability Symptoms: fatigue, general headache, end of day symptoms, may have sleep deficits Some Questions to Ask Do you have a generalized headache that increases as day progresses? Do you feel more fatigued than normal at the end of the day? Do you feel more distractible in school than normal? Vestibular-ocular screening symptom provocation Normal Computerized Neurocognitive Test Results Global mild deficits across all composites Deficits with retrieval rather than encoding 104 Exam Type Post-Injury Date Tested 09/03/12 Word Memory WG = 1 Hits (immediate) 12 Correct distractors (immed.) 12 Learning percent correct 100% Hits (delay) 11 Correct distractors (delay) 8 Delayed memory pct. Correct 79% Total percent correct 90% Design Memory Hits (immediate) 12 Correct distractors (immed.) 11 Learning percent correct 84% Hits (delay) 9 Correct distractors (delay) 9 Delayed memory pct. Correct 62% Total percent correct 73% X's and O's Total correct (memory) 8 Total correct (interference) 115 Avg. correct RT (interference) 0.45 Total incorrect (interference) 7 Avg. incorrect RT (interfer.) 0.37 Symbol Match Total correct (visible) 27 Avg. correct RT (visible) 1.19 Total correct (hidden) 8 Avg. correct RT (hidden) 1.06 Color Match Total correct 9 Avg. correct RT 0.78 Total commissions 1 Avg commissions RT 0.57 Three Letters Total sequence correct 3 Total letters correct 11 Pct. Of total letters correct 71% Avg. time to first click 1.95 Avg. counted 13.2 Avg. counted correctly



 Computerized Neurocognitive Test Results Verbal and")
27 Treatment Cognitive/ Fatigue Physical/Cognitive Breaks throughout day (no naps) Monitored exertional progression Pharmacological Amantadine Methylphenidate Sleep aid if indicated Cognitive Therapy if protracted Anxiety/ Mood Cervical Concussion Clinical Trajectories Vestibular Concussion Post- Traumatic Migraine Ocular Cognitive/ Fatigue Clinical Trajectories Determined by: Clinical Interview *Constitutional risk factors *Symptom clusters *What questions to ask? Vestibular-Ocular Screening *Provocative or not? *Specific findings help determine level/type of exertional activity Computerized Neurocognitive Testing *Specific cognitive profiles for specific clinical trajectories Findings lead to individually determined treatment and rehabilitation plan Collins MW, Kontos A, et al, KSST, 2014 Assessment Post- Traumatic Migraine Constitutional Risk Factor- Personal or family hx of migraine Symptoms: Variable headache and intermittently severe Nausea with Photo and/or phono-sensitivity Stress, anxiety, lack of exercise, dysregulation May present with vestibular-migraine symptoms Some Questions to Ask Did you get migraines before injury? Is your sleep dysregulated? Do headaches occur after poor sleep? Are you experiencing more stress than normal Vestibular-Ocular Screening symptom provocation Normal (abnormal if vestibular component present) Computerized Neurocognitive Test Results Verbal and Visual Memory deficits (if vestibular component present-speed deficits as well) 107 Collins MW, Kontos A, et al, KSST, Post- Traumatic Migraine Treatment Pharmacological Tricyclic Antidepressants Amitriptyline Anticonvulsants Migraine abortives Imitrex, Maxalt Increased cardiovascular activity-get them active! Grandma Talk -Regulation! 1 Regulated Sleep 2 Hydration 3 Regulated diet 4 Reduce Stress 5 Exertion/Activity 27


28 Case Example Collegiate Hockey Player Concussion Clinical Trajectories Anxiety/ Mood Cervical Vestibular Concussion Clinical Trajectories Determined by: Clinical Interview Vestibular-Ocular Screening Computerized Neurocognitive Testing Ocular Cognitive/ Fatigue Post- Traumatic Migraine Hit Video September 25, 2012 Brief loss of consciousness, 2 hour PTA, 45 second retrograde amnesia Spine-boarded and transported to hospital-ct unremarkable Attempted return to school 1 week later Significant symptoms of frontal headache, fatigue, academic difficulties, mood changes Removal from school for remainder of academic year Told to rest with no physical activity No Other significant medical history Referred to UPMC Concussion Program 28
, frontal headache")

29 UPMC Vestibular-Ocular Motor Screening Form (UPMC VOMS) UPMC Evaluation November 5, 2012 (6 weeks post injury) Convalescing at home-no exertion allowed Previously underwent local vestibular evaluation and determined vestibular therapy not warranted Significant symptoms of fatigue (8/10 daily), frontal headache (7/10 daily), difficulties with focus, mood concerns (irritability, concern, dysphoria). Headache/fatigue increased with reading and computer work UPMC Assessment and Evaluation Clinical Interview Computerized Neurocognitive Testing Vestibular-Ocular Exertional Testing Neck Mucha, Collins, Kontos, Troutman Elbin, Data under review 29


30 Testing November 5, 2012 Smooth pursuits, saccades, gaze stability, optokinetic stimulation, balance WNL Near point of convergence = 22cm Convergence insufficiency Marked right side exophoria Exertional testing WNL Ecstatic with working out-mood improved immediately Neck Evaluation WNL Impaired computerized neurocognitive data Baseline 9/02/2011 Post-Injury 1 11/05/2012 Convergence Insufficiency Hit Video Recommendations for November 5, 2012 evaluation Vision therapy through Behavioral Optometry No restrictions on exertion-full conditioning Become socially active Limited reading, computer work during initial stages of vision therapy Prognosis excellent for resolution of symptoms/deficits/return to play with treatment (10 weeks) 30

31 Follow-up evaluation December 28, 2012 (3 months post injury-7 weeks after first eval) Patient improving significantly One headache per week (2/10-30 minutes in duration); fatigue/mood issues resolved No other symptoms endorsed Patient involved in full aerobic activity, lifting, skating- Stage 5 hockey-specific activity with no contact Testing December 28, 2012 Computerized neurocognitive testing Near point convergence improved from 22 cm to approximately 9 cm Right-side exophoria still present Baseline Post-Injury 1 9/02/ /05/2012 Post-Injury 2 10/28/2012 Recommendations for December 28, 2012 Finish vision therapy Return after vision therapy and prior to school year for clearance Continue exertional activity with no restriction 31



32 Final evaluation June 20, 2013 (9 months post injury) Had felt 100% since mid-feb 2013 Exertional testing WNL Finished vision therapy (Feb)-NPC = 4 cm Baseline Post-Injury 1 Post-Injury 2 Post-Injury 3 9/02/ /05/ /28/2012 6/20/2013 Computerized Neurocognitive Testing Final Interview Video Case Example: NFL Defensive Back 32
33 Past medical history unremarkable - no prior concussion history August 11, 2012 Hit helmet to helmet in left temporal region Loss of consciousness briefly (seconds) 30 minutes of retrograde amnesia, 90 minutes post-traumatic amnesia - overt confusion and initial vomiting Hospitalized 3 day inpatient stay Continual vomiting Severe headaches, photosensitivity, fatigue, cognitive deficits Initial CT scan unremarkable August 16, 2012 Meets with team physician Flattened affect, slowed speech, intact reflexes Ordered MRI of brain - revealed contusion in posterior temporal area of left hemisphere September 12, 2012 Second MRI revealed small focus of low attenuation in left temporal area Less notable than first MRI Continued experiencing headaches, dizziness, emotional changes, fatigue, fogginess, sleep problems Referred to UPMC Concussion Program by team physician Evaluation 10/17/2012 at UPMC (2 months postinjury) Left occipital and bilateral temporal headache; 6/10 in severity; 7/7 days per week Blurred and double vision when reading Moderate sleep deficits and fatigue Dizziness which triggers nausea, irritability, headache, fogginess More noticeable in busy places Everyone in grocery store moving around me quickly, Car rides make me sick Wife significantly concerned regarding emotional changes 33
34 Vestibular and Neurocognitive Testing 10/17/2012 Gaze stability and optokinetic sensitivity highly provocative for dizziness and fogginess Both tests produced immediate anxiety and emotionality Saccadic eye movements (vertical/horizontal) cause moderate frontal headache Near point convergence measured at 26 cm ImPACT neurocognitive testing Recommendations for 10/17/2012 evaluation: Post-Concussion Syndrome Targeted treatments Vestibular Therapy to address optokinetic sensitivity/gaze instability Vision Therapy to address convergence insufficiency Exertional Therapy - Stage 1 Prescribed Pharmacological Intervention 5 mg Ambien to address sleep problems 100 mg Amantadine twice daily to address fatigue/cognitive deficits 34
 6 weeks of vision therapy remaining Progressed to Stage 5 of exertional")

35 Follow-up Evaluation 11/29/2012 Compliant with all therapies Amantadine twice daily, no longer on Ambien Vestibular screening normal Near point of convergence 9cm (previously 26cm) 6 weeks of vision therapy remaining Progressed to Stage 5 of exertional therapy 14 Year Old Sophomore 3.4 High School GPA ; Standardized testing Average-High Average range Medical History No prior concussion/neurologic history Hx of migraine - onset at age 12, no formal tx Strong family history of migraine Concussion sustained 10/20/11 35

36 October 11, 2011 Base Cheerleader - hit by teammate, fell to ground, striking face off floor Epistaxis - focus on nose No LOC, no retrograde amnesia, 30 second period of PTA/confusion Acute symptoms of bilateral blurred vision, dizziness, nausea, moderate headache, fatigue Mom took to ED - CT conducted - unremarkable That evening, car ride home increased symptoms of headache, fatigue, fogginess, feeling detached, feeling anxious Subsequently managed by pediatrician for 6 weeks, light academic accommodations, no sports allowed No improvement in symptoms Referred for evaluation at UPMC Evaluation 11/28/11 (5 weeks post injury) Clinical/symptom interview Headaches 7/7 days, 8/10 severity with associated photo/phonophobia, dizziness, nausea, difficulties with sleep, fatigue Much more irritable as reported by parents Vestibular screening Provoked with horizontal saccades and horizontal gaze stability, VOR cancellation NPC = 11cm ImPACT Testing Referral to Vestibular Therapy Avoid busy environments, avoid long car rides, avoid heavy ocular activity ½ days of school - full accommodations (ocular and vestibular-based) Return evaluation in 3 weeks - Return Evaluation 12/27/11 (2 months post injury) Had attended 1 session of vestibular therapy and discontinued Half-days of school very helpful Minimal symptoms - mild headaches 2/7 days, mild fatigue Vestibular exam much improved - mild provocation; NPC WNL ImPACT Testing Recommended full days of school, exertional progression, reeval for clearance - Return Evaluation 02/14/12 Stated she was normal - Headaches 1/14 days, no other sx Full exertion with no increase in sx ImPACT testing Rx clearance back to low-risk activity Rx final follow up in 1 month for closure on case/full clearance 36



37 - Return Evaluation 05/24/12 Never followed up with clearance eval New injury 05/19/12 - Hit in larynx by teammate while cheering - No mental status change but immediate headache, dizziness, nausea Was attending school - severe headaches, dizziness, nausea, fogginess, sleep deficits, moderate anxiety/emotional sequelae Playing on phone until 2am, sleeping 4 hours per night Vestibular Exam ImPACT Testing Out of school for 10 days/vestibular therapy /Vision therapy referrals/out of cheering 37

 Re")
; no impact activities; balance and vestibular treatment by specialist (prn); limit head movement/position")
38 - Return Evaluation 07/13/12 Finished Vision therapy Finished Vestibular therapy Reported 100% symptom free - last headache 2 weeks prior Excellent compliance with regulated sleep schedule, hydration, diet, exercise ImPACT testing Stage Stage 1 Target Heart Rate : 30-40% of maximum exertion 5 Stage Post-Concussion Exertion Program Target Exertion calculated by Karvonen s equation: [ {Max. H.R. (220-Age) Resting H.R.} X Target % ] + Resting H.R. Recommendations: exercise in quiet area (treatment rooms recommended); no impact activities; balance and vestibular treatment by specialist (prn); limit head movement/position change; limit concentration activities; minutes of light cardio exercise Activity - Very light aerobic conditioning - Static balance activities - Limit head movement (weight machines, squats/lunges with focusing) - Core exercises without head movements Stage 5 Stage Post-Concussion Exertion Program Target Exertion calculated by Karvonen s equation: [ {Max. H.R. (220-Age) Resting H.R.} X Target % ] + Resting H.R. Stage 4 (Sports Performance Training) Target Heart Rate: 80-90% of maximum exertion Recommendations: continue to avoid contact activity, resume aggressive training in all environments Activity - Non-contact physical training - Aggressive strength exercise - Impact activities/ plyometrics - Sports specific training activities Stage 2 Target Heart Rate : 40-60% of maximum exertion Recommendations: exercise in gym areas recommended; allow some positional changes and head movement; low level concentration activities (counting repetitions); minutes of cardio exercise - Light to moderate aerobic conditioning - Balance activity with head movement - Resistance exercises with head movements (e.g. lateral squats with head movement) - Low intensity sport specific activity - Core exercises with head movement (e.g. side planks with arm/head turn, bicycles, Russian Twists) Stage 5 (Sports Performance Training) Target Heart Rate: Full exertion Recommendations: initiate contact activities as appropriate to sport activity; full exertion for sport - Resume full physical training activities with contact - Continue aggressive strength/ conditioning exercise - Sport specific activities Stage 3 Target Heart Rate: 60-80% of maximum exertion Recommendations: any environment okay for exercise (indoor/outdoor); integrate strength, conditioning, and balance/proprioceptive exercise; can incorporate concentration challenges (counting exercises, visual games) - Moderately aggressive aerobic exercise (intervals, pyramids, stair running) - All forms of strength exercise (80% max) - Dynamic warmups - Impact activities running, plyometrics (no contact) - Challenging positional changes (burpees, mountain climbers) - More aggressive sports-specific activities 38
39 Case Example Major League Baseball Catcher Case Example: MLB Catcher 27 year-old-mlb player (Catcher) Medical history-remarkable for four prior concussions 2003-Beaned by fastball-reported symptoms for 7 days then RTP 2005-Beaned by fastball-symptoms for 5 days then RTP 2008-Foul tip to facemask while catching-symptoms 15 days then RTP 2010-Foul tip to facemask while catching-symptoms 30 days then RTP Tendency for foul tips to produce dizziness, vision changes, headaches, foggy -never taken out of play Idiopathic issues with vision for 6 weeks-visited opthamologist-no formal diagnosis or treatment recommendations History of motion sensitivity (car sickness) as child No other medical or psychiatric history Academic history-did well in limited schooling-no history of LD or ADD Drafted at Age 16 from Venezuela Concussion sustained 03/11/12 Case Example: MLB Catcher March 11, 2012 Foul tip to facemask while catching-linear blow Acute symptoms of dizziness, bilateral blurred vision, feeling detached Symptoms worsened over next three innings, told ATC and removed from game Sent to Emergency Room-CT Scan of head, X-ray of neck unremarkable Rested for 3 weeks with minimal improvement Continued to report headaches (8 hours per day; 6/10 severity), moderate levels of photosensitivity, phonophobia, fatigue, fogginess, cognitive deficits, significant sleep concerns, emotional flatness Referred to UPMC Concussion Program on 04/04/12 (3.5 weeks post injury) Case Example: MLB Catcher-History of four prior concussions and event on March 11, 2012 UPMC Evaluation April 4, 2012 Clinical Interview All symptoms persistent and severe across vestibular, ocular, cognitive, mood, sleep domains Vestibular-Ocular Examination NPC (Near Point of Convergence = 27cm) Significant provocation with vertical and horizontal VOR Significant provocation with Visual Motion sensitivity Exertional Testing Only able to tolerate stationary bike for 15 minutes Unable to tolerate more dynamic activity No other exertional testing due to severity of provocation Computerized Neurocognitive Testing Severe deficits with Reaction Time, Visual-Motor Speed-moderate deficits with Verbal and Visual Memory 39
 for convergence insufficiency Exertional therapy (stationary bike, core")
40 Case Example: MLB Catcher Impressions-Chronic post-concussion syndrome from recent and prior mtbi s 2011 symptoms likely post concussive in nature Difficulties chronic Symptom concerns-vestibular, Ocular, Cognitive, Anxiety April 4, 2012 Treatment Recommendations Targeted Vestibular therapy Vision therapy (HTS program) for convergence insufficiency Exertional therapy (stationary bike, core work, strengthening-quiet gym) PMR-prescribed Amantadine, Ambien, Clonazepam, Monthly follow-up appointments at UPMC Concussion Clinical Trajectories: A New Model for Understanding Assessment, Treatment and Rehabilitation? Anxiety/ Mood Cervical Vestibular Concussion Post- Traumatic Migraine Ocular Cognitive/ Fatigue Case Example: MLB Catcher August 7, 2012 Clinical interview Had progressed significantly with Vision, Vestibular and Exertional therapies Reported being 95%-no physical symptoms reported-sleep/mood WNL Had discontinued Ambien/Klonopin (continued on Amantadine) NPC=3cm; All Vestibular-Ocular testing WNL Computerized neurocognitive testing improved significantly Recommended progression to baseball activities, continue with exertional training (discontinue vestibular, vision therapies) Wean off meds Return for clearance September 6, 2012-Final Evaluation 100% asymptomatic, off all medications, Neuroocognitive data WNL Full clearance to Winter League Baseball Now playing successfully in Major Leagues 40






41 Thank you 41
Prognosticating Protracted Recoveries from Sports Concussion: What are we Learning?
 Prognosticating Protracted Recoveries from Sports Concussion: What are we Learning? Associate Professor UPMC Department of Orthopaedic Surgery UPMC Department of Neurological Surgery Director UPMC Sports
Prognosticating Protracted Recoveries from Sports Concussion: What are we Learning? Associate Professor UPMC Department of Orthopaedic Surgery UPMC Department of Neurological Surgery Director UPMC Sports
Clinical Profile and Active Treatment Approach to Concussion Management Micky Collins, PhD
 Clinical Profile and Active Treatment Approach to Concussion Management Micky Collins, PhD University of Pittsburgh Medical Center Associate Professor Department of Orthopaedic Surgery Department of Neurological
Clinical Profile and Active Treatment Approach to Concussion Management Micky Collins, PhD University of Pittsburgh Medical Center Associate Professor Department of Orthopaedic Surgery Department of Neurological
Disclosure Statement. Objectives. Micky Collins May Rehabilitation and Treatment of Sports Concussion: What are we Learning?
 Rehabilitation and Treatment of Sports Concussion: What are we Learning? Micky Collins, Ph.D. University of Pittsburgh Medical Center Associate Professor Department of Orthopaedic Surgery Department of
Rehabilitation and Treatment of Sports Concussion: What are we Learning? Micky Collins, Ph.D. University of Pittsburgh Medical Center Associate Professor Department of Orthopaedic Surgery Department of
Vestibular Oculomotor Screening (VOMS) and Concussion Challenge
 and Concussion Challenge") Vestibular Oculomotor Screening (VOMS) and Concussion Challenge Keely Battaglini, PT, SCS, ATC Courage Kenny Sports and PT Eagan Erin Baldridge, DPT, OCS, CLT Courage Kenny Sports and PT Mercy Specialty
Vestibular Oculomotor Screening (VOMS) and Concussion Challenge Keely Battaglini, PT, SCS, ATC Courage Kenny Sports and PT Eagan Erin Baldridge, DPT, OCS, CLT Courage Kenny Sports and PT Mercy Specialty
Clinical Profiles and Recovery Trajectories Concussion Management
 Disclosures and Recovery Trajectories Concussion Management I have no disclosures Aimee Custer, PsyD, LP Clinical Sports Neuropsychologist The following slides are property of Aimee Custer, PsyD. Do not
Disclosures and Recovery Trajectories Concussion Management I have no disclosures Aimee Custer, PsyD, LP Clinical Sports Neuropsychologist The following slides are property of Aimee Custer, PsyD. Do not
Sport-Related Concussion
 Sport-Related Concussion Bill Meehan, MD Micheli Center for Sports Injury Prevention Sports Concussion Clinic, Boston Children s Biomechanics Biomechanics Rotational acceleration Slaughterhouses free to
Sport-Related Concussion Bill Meehan, MD Micheli Center for Sports Injury Prevention Sports Concussion Clinic, Boston Children s Biomechanics Biomechanics Rotational acceleration Slaughterhouses free to
Concussion: A Treatable Injury MELISSA N. WOMBLE, PHD NEUROPSYCHOLOGIST, DIRECTOR INOVA SPORTS MEDICINE CONCUSSION PROGRAM
 Concussion: A Treatable Injury MELISSA N. WOMBLE, PHD NEUROPSYCHOLOGIST, DIRECTOR INOVA SPORTS MEDICINE CONCUSSION PROGRAM THE CURRENT PROBLEM 1. WHAT IS A CONCUSSION? 2. ACUTE/SIDELINE EVALUATION 3. AT
Concussion: A Treatable Injury MELISSA N. WOMBLE, PHD NEUROPSYCHOLOGIST, DIRECTOR INOVA SPORTS MEDICINE CONCUSSION PROGRAM THE CURRENT PROBLEM 1. WHAT IS A CONCUSSION? 2. ACUTE/SIDELINE EVALUATION 3. AT
Active Intervention in Concussion: Results from TEAM (Targeted Evaluation and Active Management)
") Active Intervention in Concussion: Results from TEAM (Targeted Evaluation and Active Management) Erin Reynolds, Psy.D Fellowship Director UPMC Sports Medicine Concussion Program Assistant Professor Department
Active Intervention in Concussion: Results from TEAM (Targeted Evaluation and Active Management) Erin Reynolds, Psy.D Fellowship Director UPMC Sports Medicine Concussion Program Assistant Professor Department
MELISSA N. WOMBLE, PHD NEUROPSYCHOLOGIST/DIRECTOR INOVA SPORTS MEDICINE COMPREHENSIVE CONCUSSION PROGRAM
 MELISSA N. WOMBLE, PHD NEUROPSYCHOLOGIST/DIRECTOR INOVA SPORTS MEDICINE COMPREHENSIVE CONCUSSION PROGRAM THE CURRENT PROBLEM 1. PATHOPHYSIOLOGY OF CONCUSSION 2. SIGNS AND SYMPTOMS OF CONCUSSION 3. TYPICAL
MELISSA N. WOMBLE, PHD NEUROPSYCHOLOGIST/DIRECTOR INOVA SPORTS MEDICINE COMPREHENSIVE CONCUSSION PROGRAM THE CURRENT PROBLEM 1. PATHOPHYSIOLOGY OF CONCUSSION 2. SIGNS AND SYMPTOMS OF CONCUSSION 3. TYPICAL
mtbi/concussion in Children, Adolescents & Young Adults: What it is and Why we should be Concerned Ronald C. Savage, Ed.D.
 mtbi/concussion in Children, Adolescents & Young Adults: What it is and Why we should be Concerned Ronald C. Savage, Ed.D. rcsavage@comcast.net 1 How Common Are mtbi/concussions? CDC reports indicate that
mtbi/concussion in Children, Adolescents & Young Adults: What it is and Why we should be Concerned Ronald C. Savage, Ed.D. rcsavage@comcast.net 1 How Common Are mtbi/concussions? CDC reports indicate that
Physiotherapy management of concussion
 Physiotherapy management of concussion Ms. Mairead Daly, Senior Physiotherapist, Bon Secours Health System Saturday November 17 th Silver Springs Hotel Cork Concussion Physiotherapy Assessment and Management
Physiotherapy management of concussion Ms. Mairead Daly, Senior Physiotherapist, Bon Secours Health System Saturday November 17 th Silver Springs Hotel Cork Concussion Physiotherapy Assessment and Management
Concussion: Pressure to Play in Sports: Can We Trust What the Athlete Tells Us? How I Manage Concussion: A Neuropsychologist s Perspective
 How I Manage Concussion: A Neuropsychologist s Perspective Jamie Pardini, Ph.D. UPMC Concussion Program University of Pittsburgh Medical Center Department of Orthopaedic Surgery UPMC Sports Concussion
How I Manage Concussion: A Neuropsychologist s Perspective Jamie Pardini, Ph.D. UPMC Concussion Program University of Pittsburgh Medical Center Department of Orthopaedic Surgery UPMC Sports Concussion
Outline. A brief history of concussion 4/25/2018. Understanding the Impact of Concussions: From Injury through Recovery
 Understanding the Impact of Concussions: From Injury through Recovery Luke C. Henry, PhD Clinical Neuropsychologist UPMC Department of Neurological Surgery 05.04.2018 Concussions Brief history Definition
Understanding the Impact of Concussions: From Injury through Recovery Luke C. Henry, PhD Clinical Neuropsychologist UPMC Department of Neurological Surgery 05.04.2018 Concussions Brief history Definition
Beyond the Basics, Bringing Concussion Out of the Dark
 Beyond the Basics, Bringing Concussion Out of the Dark Objectives Recognize different types of concussion based on symptomatology Identify risk factors for prolonged recovery after a concussion Predict
Beyond the Basics, Bringing Concussion Out of the Dark Objectives Recognize different types of concussion based on symptomatology Identify risk factors for prolonged recovery after a concussion Predict
Concussion Assessment, Management, and Return to Play Guidelines
 Concussion Assessment, Management, and Return to Play Guidelines The following policy and procedures on neurocognitive baseline testing and subsequent assessment and management of concussions as well as
Concussion Assessment, Management, and Return to Play Guidelines The following policy and procedures on neurocognitive baseline testing and subsequent assessment and management of concussions as well as
Concussions: the evidenced based office evaluation for primary care and beyond.
 Concussions: the evidenced based office evaluation for primary care and beyond. Presented By: Dr. Corey Dean MD, FAAP, FACP, and CAQSM Associate Program Director of Ambulatory Education St. Joseph Hospital
Concussions: the evidenced based office evaluation for primary care and beyond. Presented By: Dr. Corey Dean MD, FAAP, FACP, and CAQSM Associate Program Director of Ambulatory Education St. Joseph Hospital
New Frontiers in the Science of Concussion
 New Frontiers in the Science of Concussion Mark R. Lovell, Ph.D., FACPN Chairman and Chief Scientific Officer Founding Director and Professor University of Pittsburgh Sports Concussion Program Copyright
New Frontiers in the Science of Concussion Mark R. Lovell, Ph.D., FACPN Chairman and Chief Scientific Officer Founding Director and Professor University of Pittsburgh Sports Concussion Program Copyright
5/15/13. Disclosure. Objectives. Pharmacological Management of Concussion. Anthony P. Kontos, PhD
 Pharmacological Management of Concussion Anthony P. Kontos, PhD Assistant Research Director UPMC Sports Medicine Concussion Program Associate Professor Department of Orthopaedic Surgery University of Pittsburgh
Pharmacological Management of Concussion Anthony P. Kontos, PhD Assistant Research Director UPMC Sports Medicine Concussion Program Associate Professor Department of Orthopaedic Surgery University of Pittsburgh
Common Modifying Factors for Baseline VOMS Performance 2018 Big Sky Athletic Training Sports Medicine Conference. Disclosure. Objectives 2/13/18
 Common Modifying Factors for Baseline VOMS Performance 2018 Big Sky Athletic Training Sports Medicine Conference Ryan N. Moran, PhD, ATC Disclosure I have no actual or potential conflict of interest in
Common Modifying Factors for Baseline VOMS Performance 2018 Big Sky Athletic Training Sports Medicine Conference Ryan N. Moran, PhD, ATC Disclosure I have no actual or potential conflict of interest in
Concussion Rehabilitation Specialist
 Concussion Rehabilitation Specialist Complex pathophysiological process affecting the brain, induced by biomechanical forces Common Features Direct or transmitted blow the the head/neck Rapid onset, short-lived
Concussion Rehabilitation Specialist Complex pathophysiological process affecting the brain, induced by biomechanical forces Common Features Direct or transmitted blow the the head/neck Rapid onset, short-lived
April 28, Katie Barnes Wood, PT, DPT Orthotennessee Therapy. Concussion Therapy. How and Why Physical Therapy Can Help Concussions
 April 28, 2018 Katie Barnes Wood, PT, DPT Orthotennessee Therapy Concussion Therapy How and Why Physical Therapy Can Help Concussions Background Concussion Rehab at KOC Our Care Team Athletic Trainers
April 28, 2018 Katie Barnes Wood, PT, DPT Orthotennessee Therapy Concussion Therapy How and Why Physical Therapy Can Help Concussions Background Concussion Rehab at KOC Our Care Team Athletic Trainers
POLICY / PROCEDURE DOCUMENT Effective Date 08/19/2010. Concussion Assessment, Management, and Return to Play Guidelines
 Beacon Medical Group Sports Medicine POLICY / PROCEDURE DOCUMENT Effective Date 08/19/2010 TITLE: Document of (Entity) POLICY: PATIENT POPULATION: Concussion Assessment, Management, and Return to Play
Beacon Medical Group Sports Medicine POLICY / PROCEDURE DOCUMENT Effective Date 08/19/2010 TITLE: Document of (Entity) POLICY: PATIENT POPULATION: Concussion Assessment, Management, and Return to Play
Concussion Facts & Stats
 Jeffrey Liang, MD Concussion Facts & Stats 10% of all contact sport athletes sustain concussions yearly. 63% of all concussions occur in football. Estimated that up to 20% of football players will sustain
Jeffrey Liang, MD Concussion Facts & Stats 10% of all contact sport athletes sustain concussions yearly. 63% of all concussions occur in football. Estimated that up to 20% of football players will sustain
St. John Fisher College Intercollegiate Athletics Concussion Management Protocol
 St. John Fisher College Intercollegiate Athletics Concussion Management Protocol Definition of Concussion Concussion is defined as a complex pathophysiological process affecting the brain, induced by traumatic
St. John Fisher College Intercollegiate Athletics Concussion Management Protocol Definition of Concussion Concussion is defined as a complex pathophysiological process affecting the brain, induced by traumatic
CONCUSSIONS: What You Really Need to Know Dr. Emily Dixon
 CONCUSSIONS: What You Really Need to Know Dr. Emily Dixon TriHealth Heads Count Concussion Medical Director Emily Dixon, DO Born and raised north of Kansas City, Missouri. Earned her medical degree from
CONCUSSIONS: What You Really Need to Know Dr. Emily Dixon TriHealth Heads Count Concussion Medical Director Emily Dixon, DO Born and raised north of Kansas City, Missouri. Earned her medical degree from
Texas State University Concussion Program for Varsity Athletes
 Administrative Considerations o Emergency Action Plan placed in all venues including the Concussion Plan for all high risk sports. o Coaching education regarding EAP & Concussion Plan including signs &
Administrative Considerations o Emergency Action Plan placed in all venues including the Concussion Plan for all high risk sports. o Coaching education regarding EAP & Concussion Plan including signs &
IT S ALL IN YOUR HEAD!
 IT S ALL IN YOUR HEAD! CARING FOR CONCUSSIONS IN YOUR COMMUNITY Stephen K Stacey, DO CPT, MC, USA OUTLINE Definition Epidemiology Diagnosis Evaluation Recovery Sequelae Prevention Resources for providers
IT S ALL IN YOUR HEAD! CARING FOR CONCUSSIONS IN YOUR COMMUNITY Stephen K Stacey, DO CPT, MC, USA OUTLINE Definition Epidemiology Diagnosis Evaluation Recovery Sequelae Prevention Resources for providers
Concussion 2013 A Program For Logan County
 Concussion 2013 A Program For Logan County Boyd C Hoddinott MD, MPH Logan County Health Commissioner ----------------------------------- Kristy Wisner PT, DPT Mary Rutan Physical Rehab Center Consensus
Concussion 2013 A Program For Logan County Boyd C Hoddinott MD, MPH Logan County Health Commissioner ----------------------------------- Kristy Wisner PT, DPT Mary Rutan Physical Rehab Center Consensus
PEDIATRIC SPORTS RELATED CONCUSSIONS
 Anna Mazur, PhD PEDIATRIC SPORTS RELATED CONCUSSIONS Disclosure No financial interests or funding 1 Presentation Outline Prevalence Predicting recovery: Post Traumatic Amnesia and Loss of Consciousness
Anna Mazur, PhD PEDIATRIC SPORTS RELATED CONCUSSIONS Disclosure No financial interests or funding 1 Presentation Outline Prevalence Predicting recovery: Post Traumatic Amnesia and Loss of Consciousness
Building Evidence for Concussion Clinical Profiles
 Building Evidence for Concussion Clinical Profiles Micky Collins, PhD Executive and Clinical Director- UPMC Sports Medicine Concussion Program Associate Professor- Departments of Orthopaedic and Neurological
Building Evidence for Concussion Clinical Profiles Micky Collins, PhD Executive and Clinical Director- UPMC Sports Medicine Concussion Program Associate Professor- Departments of Orthopaedic and Neurological
CONCUSSION AWARENESS, MANAGEMENT, AND ASSESSMENT FROM AN ATHLETIC TRAINER
 CONCUSSION AWARENESS, MANAGEMENT, AND ASSESSMENT FROM AN ATHLETIC TRAINER Dr. Ryan Krzyzanowicz, DAT, ATC Clinical Associate Professor Program Director - Athletic Training Education University at Buffalo
CONCUSSION AWARENESS, MANAGEMENT, AND ASSESSMENT FROM AN ATHLETIC TRAINER Dr. Ryan Krzyzanowicz, DAT, ATC Clinical Associate Professor Program Director - Athletic Training Education University at Buffalo
Carleton College Concussion Safety Protocol
 Carleton College Introduction Carleton College is committed to ensuring the health and safety of its student-athletes. To this end, and in accordance with NCAA legislation [Division III Constitution 3.2.4.16],
Carleton College Introduction Carleton College is committed to ensuring the health and safety of its student-athletes. To this end, and in accordance with NCAA legislation [Division III Constitution 3.2.4.16],
Concussion Management and Update. Objectives
 Concussion Management and Update Ricardo Guirola MD M Ed Pediatric Rheumatology Primary Care Sports Medicine Objectives Review definition, signs and symptoms Discuss the initial evaluation of a patient
Concussion Management and Update Ricardo Guirola MD M Ed Pediatric Rheumatology Primary Care Sports Medicine Objectives Review definition, signs and symptoms Discuss the initial evaluation of a patient
Concussion Management
 Concussion Management Jennifer Gray, DO Medical Co-Director, ThinkSMART! Concussion Management Program Department of Physical Medicine and Rehabilitation St. Charles Hospital Residency Program Director,
Concussion Management Jennifer Gray, DO Medical Co-Director, ThinkSMART! Concussion Management Program Department of Physical Medicine and Rehabilitation St. Charles Hospital Residency Program Director,
Pre and Post Concussion Management
 Pre and Post Concussion Management Timothy A. Tolbert, Ph.D., ATC Clinical Coordinator Marshall University Athletic Training Program 1 Concussion A complex pathophysiological process affecting the brain,
Pre and Post Concussion Management Timothy A. Tolbert, Ph.D., ATC Clinical Coordinator Marshall University Athletic Training Program 1 Concussion A complex pathophysiological process affecting the brain,
Concussion: Recognizing, Managing and Assisting Athletes to Return to Play Safely
 Concussion: Recognizing, Managing and Assisting Athletes to Return to Play Safely Todd Barron, MD Medical Director, WellSpan Neurosciences Medical Director, WellSpan Pediatric Neurology Agenda Safety in
Concussion: Recognizing, Managing and Assisting Athletes to Return to Play Safely Todd Barron, MD Medical Director, WellSpan Neurosciences Medical Director, WellSpan Pediatric Neurology Agenda Safety in
The Master s Academy Concussion Policy
 The Master s Academy Concussion Policy Ann Williams,M.S.N., R.N. Robert O Quinn, MS, ATC, LAT Updated 2/6/2018 Outline I. Abbreviated policy II. Introduction III. Prevention and Education IV. Recognition
The Master s Academy Concussion Policy Ann Williams,M.S.N., R.N. Robert O Quinn, MS, ATC, LAT Updated 2/6/2018 Outline I. Abbreviated policy II. Introduction III. Prevention and Education IV. Recognition
ImPACT Concussion Management Program
 ImPACT Concussion Management Program Carver Athletic Department * Information obtained in this presentation came directly from the Impact website at www.impacttest.com What is a Concussion? A concussion
ImPACT Concussion Management Program Carver Athletic Department * Information obtained in this presentation came directly from the Impact website at www.impacttest.com What is a Concussion? A concussion
When a concussion occurs:
 When a concussion occurs: Once an athlete has experienced any type of potential head injury initiate the following checklist: 1. n Remove athlete from all activity and use the Concussion Recognition Tool
When a concussion occurs: Once an athlete has experienced any type of potential head injury initiate the following checklist: 1. n Remove athlete from all activity and use the Concussion Recognition Tool
VESTIBULAR THERAPY AND ASSESSMENT
 VESTIBULAR THERAPY AND ASSESSMENT July 29, 2016 Marc Hinze, PT, MPT, CIMT Bronson Rehabilitation Services Objectives Vestibular Assessment Vestibular Rehabilitation Progression of Vestibular Exercise Vestibular
VESTIBULAR THERAPY AND ASSESSMENT July 29, 2016 Marc Hinze, PT, MPT, CIMT Bronson Rehabilitation Services Objectives Vestibular Assessment Vestibular Rehabilitation Progression of Vestibular Exercise Vestibular
ADHD and Concussion. Mary Alexis Iaccarino, MD
 ADHD and Concussion Mary Alexis Iaccarino, MD Department of Physical Medicine and Rehabilitation Harvard Medical School Spaulding Rehabilitation Hospital MassGeneral Hospital for Children Sport Concussion
ADHD and Concussion Mary Alexis Iaccarino, MD Department of Physical Medicine and Rehabilitation Harvard Medical School Spaulding Rehabilitation Hospital MassGeneral Hospital for Children Sport Concussion
Community Partnerships for Youth Concussion Care: Power of the Medical Neighborhood
 Community Partnerships for Youth Concussion Care: Power of the Medical Neighborhood Gerard A. Gioia, Ph.D. Pediatric Neuropsychologist Chief, Division of Pediatric Neuropsychology Director, Safe Concussion
Community Partnerships for Youth Concussion Care: Power of the Medical Neighborhood Gerard A. Gioia, Ph.D. Pediatric Neuropsychologist Chief, Division of Pediatric Neuropsychology Director, Safe Concussion
CCYFL Concussion Information Sheet
 CCYFL Concussion Information Sheet Why am I getting this information sheet? You are receiving this information sheet about concussions because of California state law AB 2007, (effective January 1, 2017),
CCYFL Concussion Information Sheet Why am I getting this information sheet? You are receiving this information sheet about concussions because of California state law AB 2007, (effective January 1, 2017),
Concussion: The Basics. Bill Meehan, MD Micheli Center for Sports Injury Prevention Sports Concussion Clinic, Boston Children s Hospital
 Concussion: The Basics Bill Meehan, MD Micheli Center for Sports Injury Prevention Sports Concussion Clinic, Boston Children s Hospital Definition Working definition Characteristics Trauma Impulse
Concussion: The Basics Bill Meehan, MD Micheli Center for Sports Injury Prevention Sports Concussion Clinic, Boston Children s Hospital Definition Working definition Characteristics Trauma Impulse
Coastal Carolina University Athletic Training Department Policy and Procedure Manual Concussion Management Revised/Reviewed 6/2012
 Coastal Carolina University Athletic Training Department Policy and Procedure Manual Concussion Management Revised/Reviewed 6/2012 INTRODUCTION: Concussion classification, management, and protocols have
Coastal Carolina University Athletic Training Department Policy and Procedure Manual Concussion Management Revised/Reviewed 6/2012 INTRODUCTION: Concussion classification, management, and protocols have
10/23/2018. What is a Concussion? Understand What is a concussion? Learn typical signs and symptoms and red flags
 Maria Chininis, Sports Medicine and Concussion Institute Understand What is a concussion? Learn typical signs and symptoms and red flags Understand trajectories that affect concussion recovery What is
Maria Chininis, Sports Medicine and Concussion Institute Understand What is a concussion? Learn typical signs and symptoms and red flags Understand trajectories that affect concussion recovery What is
CONCUSSION UPDATE 2017
 CONCUSSION UPDATE 2017 Shannon Woods MD Medical Director CoxHealth Sports Medicine Team Physician Evangel University Team Physician Drury University 1 Cognitive Fogginess Difficulty concentrating Memory
CONCUSSION UPDATE 2017 Shannon Woods MD Medical Director CoxHealth Sports Medicine Team Physician Evangel University Team Physician Drury University 1 Cognitive Fogginess Difficulty concentrating Memory
INTERCOLLEGIATE ATHLETICS CONCUSSION ACKNOWLEDGEMENT AND STATEMENT
 ACKNOWLEDGEMENT AND STATEMENT A FACT SHEET FOR STUDENT-ATHLETES WHAT IS A? A concussion is a brain injury that: Is caused by a blow to the head or body -From contact with another player, hitting a hard
ACKNOWLEDGEMENT AND STATEMENT A FACT SHEET FOR STUDENT-ATHLETES WHAT IS A? A concussion is a brain injury that: Is caused by a blow to the head or body -From contact with another player, hitting a hard
Seth Smith MD, PharmD. Thank You!
 Seth Smith MD, PharmD Thank You! Concussion Headlines!!! Concussion Headlines!!! Concussion rules put kids health before winning games The Miami Herald 8/21/12 FHSAA's implementation of legislation goes
Seth Smith MD, PharmD Thank You! Concussion Headlines!!! Concussion Headlines!!! Concussion rules put kids health before winning games The Miami Herald 8/21/12 FHSAA's implementation of legislation goes
Sports Concussion After the Injury. Carol Scott, MD UNR Student Health Center Sports Medicine September 22, 2016
 Sports Concussion After the Injury Carol Scott, MD UNR Student Health Center Sports Medicine September 22, 2016 Goals Understand the initial assessment of concussion Become familiar with tools that aid
Sports Concussion After the Injury Carol Scott, MD UNR Student Health Center Sports Medicine September 22, 2016 Goals Understand the initial assessment of concussion Become familiar with tools that aid
Your guide to recovery. Treating concussions
 Your guide to recovery Treating concussions About concussions A concussion is a condition, usually caused when a blow to the head or body causes the brain to move rapidly within the skull, that can temporarily
Your guide to recovery Treating concussions About concussions A concussion is a condition, usually caused when a blow to the head or body causes the brain to move rapidly within the skull, that can temporarily
Sports Concussions: Return to Learn
 Sports Concussions: Return to Learn Jonathan Santana, DO Adolescent & Sports Medicine Objectives Be able to perform a brief cognitive assessment in the athlete with a head injury Be able to prescribe return
Sports Concussions: Return to Learn Jonathan Santana, DO Adolescent & Sports Medicine Objectives Be able to perform a brief cognitive assessment in the athlete with a head injury Be able to prescribe return
Sport-Related Concussion. Daniel Seidman DO 6 August 2016
 Sport-Related Concussion Daniel Seidman DO 6 August 2016 My Pertinent Qualifications - Current Fellow, PCSM - Henry Ford Hospital - Recent Graduate, FM - St. John Macomb-Oakland Hospital - Involved in
Sport-Related Concussion Daniel Seidman DO 6 August 2016 My Pertinent Qualifications - Current Fellow, PCSM - Henry Ford Hospital - Recent Graduate, FM - St. John Macomb-Oakland Hospital - Involved in
Disclosures. Objectives 2/15/2014. Wright, Concussion Assessment, Management and Return to Sports
 Concussion Assessment, Management and Return to Sports Wendy L. Wright, MS, APRN, FNP, FAANP Adult/Family Nurse Practitioner Owner Wright & Associates Family Healthcare Amherst Owner Wright & Associates
Concussion Assessment, Management and Return to Sports Wendy L. Wright, MS, APRN, FNP, FAANP Adult/Family Nurse Practitioner Owner Wright & Associates Family Healthcare Amherst Owner Wright & Associates
UNIVERSITY OF MASSACHUSETTS SPORTS MEDICINE PROGRAM Concussion Management Plan
 UNIVERSITY OF MASSACHUSETTS SPORTS MEDICINE PROGRAM Concussion Management Plan University of Massachusetts Sports Medicine personnel will evaluate student-athletes with a suspected concussion as follows:
UNIVERSITY OF MASSACHUSETTS SPORTS MEDICINE PROGRAM Concussion Management Plan University of Massachusetts Sports Medicine personnel will evaluate student-athletes with a suspected concussion as follows:
Signs and Symptoms of Concussion
 Signs and Symptoms of Concussion These signs and symptoms following a witnessed or suspected blow to the head or body are indicative of probable concussion. Signs (observed by others) Appears dazed or
Signs and Symptoms of Concussion These signs and symptoms following a witnessed or suspected blow to the head or body are indicative of probable concussion. Signs (observed by others) Appears dazed or
Mark J. Harary, MD Primary Care Sports Medicine St Charles Orthopedics, LLP
 Mark J. Harary, MD Primary Care Sports Medicine St Charles Orthopedics, LLP Facts, Definitions, etc Appropriate Recognition Comprehensive Management Treatment Consequences of Concussions Neurocognitive
Mark J. Harary, MD Primary Care Sports Medicine St Charles Orthopedics, LLP Facts, Definitions, etc Appropriate Recognition Comprehensive Management Treatment Consequences of Concussions Neurocognitive
New Developments in the Management of Concussions. David Marshall, MD Medical Director Sports Medicine Program Children s Healthcare of Atlanta
 New Developments in the Management of Concussions David Marshall, MD Medical Director Sports Medicine Program Children s Healthcare of Atlanta Concussions in the News June 7, 2009 New Guidelines on Young
New Developments in the Management of Concussions David Marshall, MD Medical Director Sports Medicine Program Children s Healthcare of Atlanta Concussions in the News June 7, 2009 New Guidelines on Young
Director of Athletics
 3341-8-1 Concussion Management Policy. Applicability Intercollegiate Athletics Responsible Unit Policy Administrator Intercollegiate Athletics/Director of Athletics Director of Athletics (A) Policy Purpose
3341-8-1 Concussion Management Policy. Applicability Intercollegiate Athletics Responsible Unit Policy Administrator Intercollegiate Athletics/Director of Athletics Director of Athletics (A) Policy Purpose
Craig Davidson, MD University Health Center Team Physician Department of Athletic Medicine University of Oregon
 Craig Davidson, MD University Health Center Team Physician Department of Athletic Medicine University of Oregon In the news Definition Pathophysiology Signs and symptoms Review current clinical guidelines
Craig Davidson, MD University Health Center Team Physician Department of Athletic Medicine University of Oregon In the news Definition Pathophysiology Signs and symptoms Review current clinical guidelines
PRE-SEASON INFORMATION SHEET CONCUSSIONS
 PRE-SEASON INFORMATION SHEET CONCUSSIONS HOW TO USE THIS EDUCATION SHEET: Distribute this pre-season concussion education sheet to your athletes and their parents or legal guardians during a pre-season
PRE-SEASON INFORMATION SHEET CONCUSSIONS HOW TO USE THIS EDUCATION SHEET: Distribute this pre-season concussion education sheet to your athletes and their parents or legal guardians during a pre-season
CONCUSSION PROTOCOL STEPS FOR RETURN TO PLAY
 Winnacunnet High School Concussion Protocol All coaches must take the NFHS Concussion course prior to working with students in their coaching season. Coaches must retake the course on even numbered years.
Winnacunnet High School Concussion Protocol All coaches must take the NFHS Concussion course prior to working with students in their coaching season. Coaches must retake the course on even numbered years.
The University of Nebraska Omaha Concussion Management Plan
 Definition: The University of Nebraska Omaha Concussion Management Plan A concussion is a complex pathophysiological process affecting the brain, induced by traumatic biomechanical forces secondary to
Definition: The University of Nebraska Omaha Concussion Management Plan A concussion is a complex pathophysiological process affecting the brain, induced by traumatic biomechanical forces secondary to
Return-to-Play Protocol After Concussion/mild TBI
 Return-to-Play Protocol After Concussion/mild TBI Return to activity and play is a medical decision. The athlete must meet all of the following criteria to progress to activity: Asymptomatic at rest and
Return-to-Play Protocol After Concussion/mild TBI Return to activity and play is a medical decision. The athlete must meet all of the following criteria to progress to activity: Asymptomatic at rest and
Mild TBI (Concussion) Not Just Less Severe But Different
 Not Just Less Severe But Different") Mild TBI (Concussion) Not Just Less Severe But Different Disclosures Funded research: 1. NIH: RO1 Physiology of concussion 2016-2021, Co-PI, $2,000,000 2. American Medical Society of Sports Medicine: RCT
Mild TBI (Concussion) Not Just Less Severe But Different Disclosures Funded research: 1. NIH: RO1 Physiology of concussion 2016-2021, Co-PI, $2,000,000 2. American Medical Society of Sports Medicine: RCT
Davidson College Sports Medicine Concussion Management Policy
 Davidson College Sports Medicine Concussion Management Policy Davidson College practices concussion management care based on the most current research and consensus statements from noted concussion experts.
Davidson College Sports Medicine Concussion Management Policy Davidson College practices concussion management care based on the most current research and consensus statements from noted concussion experts.
Lower Moreland School District: Athletic Department Protocol and Procedures for Management of Sports-Related Concussion
 Lower Moreland School District: Athletic Department Protocol and Procedures for Management of Sports-Related Concussion Preamble: Medical management of sports-related concussion is evolving. In recent
Lower Moreland School District: Athletic Department Protocol and Procedures for Management of Sports-Related Concussion Preamble: Medical management of sports-related concussion is evolving. In recent
Paramus Athletics. Paramus High School Athletic Department Protocol and Procedures for Management of Sports - Related Concussion
 Paramus Athletics Paramus High School Athletic Department Protocol and Procedures for Management Medical management of sports-related concussions is evolving. In recent years, there has been significant
Paramus Athletics Paramus High School Athletic Department Protocol and Procedures for Management Medical management of sports-related concussions is evolving. In recent years, there has been significant
Berlin 2016 SRC. Concussion Management: An Update 7/26/2017. Sport related concussion. mtbi often used. Rapid onset, short lived
 Concussion Management: An Update Jeff Sellman, MD, CAQSM Primary Care Sports Medicine Physician Florida Orthopedic Institute July 22, 2017 Berlin 2016 5th International conference on concussion in sport
Concussion Management: An Update Jeff Sellman, MD, CAQSM Primary Care Sports Medicine Physician Florida Orthopedic Institute July 22, 2017 Berlin 2016 5th International conference on concussion in sport
Concussion Information
 What is a Concussion? Concussion Information Information taken from the Sports Concussion Institute http://www.concussiontreatment.com A concussion is defined as a complex pathophysiological process that
What is a Concussion? Concussion Information Information taken from the Sports Concussion Institute http://www.concussiontreatment.com A concussion is defined as a complex pathophysiological process that
Disclaimer. Objectives 4/7/2013
 Post-Concussion Management in the Clinic Steve Lauer PhD MD Department of Pediatrics Center for Concussion Management University of Kansas Medical Center April 19, 2013 Disclaimer I have no relevant financial
Post-Concussion Management in the Clinic Steve Lauer PhD MD Department of Pediatrics Center for Concussion Management University of Kansas Medical Center April 19, 2013 Disclaimer I have no relevant financial
Forney ISD Protocol and Procedures for the Management of the Sports-Related Concussion
 Forney ISD Protocol and Procedures for the Management of the Sports-Related Concussion Medical management of sports-related concussion is evolving. Recently, there has been a significant amount of research
Forney ISD Protocol and Procedures for the Management of the Sports-Related Concussion Medical management of sports-related concussion is evolving. Recently, there has been a significant amount of research
UNIVERSITY OF WISCONSIN-STOUT ATHLETIC TRAINING CONCUSSION PROTOCOL & GUIDELINES
 UNIVERSITY OF WISCONSIN-STOUT ATHLETIC TRAINING CONCUSSION PROTOCOL & GUIDELINES The health and safety of our student-athletes is a high priority. This document establishes (1) the educational procedures
UNIVERSITY OF WISCONSIN-STOUT ATHLETIC TRAINING CONCUSSION PROTOCOL & GUIDELINES The health and safety of our student-athletes is a high priority. This document establishes (1) the educational procedures
Disclosure Statement. Objectives 1/18/2016
 In-Office Evaluation of Sports Related Concussion Micky Collins, PhD University of Pittsburgh Medical Center Associate Professor Department of Orthopaedic Surgery Department of Neurological Surgery Program
In-Office Evaluation of Sports Related Concussion Micky Collins, PhD University of Pittsburgh Medical Center Associate Professor Department of Orthopaedic Surgery Department of Neurological Surgery Program
1. Begin light aerobic exercise such as walking, stationary bike, etc. No resistance training.
 POLICY: Any athlete displaying signs or symptoms of a concussion, or if there is a high suspicion for concussion, an athlete will not be returned to competition or practice until they have written clearance
POLICY: Any athlete displaying signs or symptoms of a concussion, or if there is a high suspicion for concussion, an athlete will not be returned to competition or practice until they have written clearance
Concussion Research-NCAA and DoD Concussion Study
 Jim Messerly DO Nothing to Disclose Concussion Research-NCAA and DoD Concussion Study May 29, 2014: The NCAA and the US Department of Defense announce a landmark $30 million initiative to enhance the safety
Jim Messerly DO Nothing to Disclose Concussion Research-NCAA and DoD Concussion Study May 29, 2014: The NCAA and the US Department of Defense announce a landmark $30 million initiative to enhance the safety
Completing the Loop: Management of the Adolescent Sports Injury. Marisa Frank PT, DPT, CSCS
 : Management of the Adolescent Sports Injury Marisa Frank PT, DPT, CSCS OBJECTIVES Describe patients who are appropriate for physical therapy. Demonstrate an understanding of the phases of concussion rehabilitation.
: Management of the Adolescent Sports Injury Marisa Frank PT, DPT, CSCS OBJECTIVES Describe patients who are appropriate for physical therapy. Demonstrate an understanding of the phases of concussion rehabilitation.
SPRINGFIELD CLINIC S
 SPRINGFIELD CLINIC S HEAD INJURY MANAGEMENT GUIDE FOR PARENTS Given the complexities of concussion management, Springfield Clinic recognizes the importance of managing concussions on an individualized
SPRINGFIELD CLINIC S HEAD INJURY MANAGEMENT GUIDE FOR PARENTS Given the complexities of concussion management, Springfield Clinic recognizes the importance of managing concussions on an individualized
Management of the Concussed Adolescent
 Management of the Concussed Adolescent Tamara C. Valovich McLeod, PhD, ATC, FNATA John P. Wood, D.O., Endowed Chair for Sports Medicine Professor and Director, Athletic Training Program Director, Athletic
Management of the Concussed Adolescent Tamara C. Valovich McLeod, PhD, ATC, FNATA John P. Wood, D.O., Endowed Chair for Sports Medicine Professor and Director, Athletic Training Program Director, Athletic
1. Injury Description
 ACUTE CONCUSSION EVALUATION (ACE) Physician/Clinician Office Version Gerard Gioia, PhD 1 & Micky Collins, PhD 2 1 Children's National Medical Center 2 University of Pittsburgh Medical Center Patient Name
ACUTE CONCUSSION EVALUATION (ACE) Physician/Clinician Office Version Gerard Gioia, PhD 1 & Micky Collins, PhD 2 1 Children's National Medical Center 2 University of Pittsburgh Medical Center Patient Name
Review of: NATA Position Statement Management of Sport Concussion.
 Review of: NATA Position Statement Management of Sport Concussion www.csm-institute.com Topics: Education and Prevention Documentation and Legal Aspects Evaluation and RTP Other Considerations Strength
Review of: NATA Position Statement Management of Sport Concussion www.csm-institute.com Topics: Education and Prevention Documentation and Legal Aspects Evaluation and RTP Other Considerations Strength
Please feel free to contact me if you have any questions. HOME INSTRUCTIONS FOR CONCUSSION. Recommendations for monitoring symptoms at home:
 Recommendations for monitoring symptoms at home: What should I do when I m recovering? Physical and mental rest are very important to your recovery. Keep your heart rate low and do not do any physical
Recommendations for monitoring symptoms at home: What should I do when I m recovering? Physical and mental rest are very important to your recovery. Keep your heart rate low and do not do any physical
Multi-disciplinary TBI evaluation
 Multi-disciplinary TBI evaluation Date: September 16, 2017 Ryan Rockwood, ATC Jennifer Wilhelm, PT, DPT, NCS Kyla Laraway, OT, DOT Haley Landau, M.S., CCC- SLP Adapted from Collins MW et al; Knee Surg
Multi-disciplinary TBI evaluation Date: September 16, 2017 Ryan Rockwood, ATC Jennifer Wilhelm, PT, DPT, NCS Kyla Laraway, OT, DOT Haley Landau, M.S., CCC- SLP Adapted from Collins MW et al; Knee Surg
Concussion Management Plan
 Concussion Management Plan Table of Contents Purpose of the plan 2 Definition of concussion 2 Common signs and symptoms of concussion 3 Prior Education 3 Baseline testing 3 Management and return to play
Concussion Management Plan Table of Contents Purpose of the plan 2 Definition of concussion 2 Common signs and symptoms of concussion 3 Prior Education 3 Baseline testing 3 Management and return to play
Sport Related Concussion Update 2017
 Sport Related Concussion Update 2017 HAYLEY QUELLER, MD ST. CHARLES ORTHOPEDICS, SPORTS MEDICINE DIRECTOR THINKSMART! CONCUSSION MANAGEMENT, CO-DIRECTOR Consensus Statement: 5 th Annual Meeting, Berlin
Sport Related Concussion Update 2017 HAYLEY QUELLER, MD ST. CHARLES ORTHOPEDICS, SPORTS MEDICINE DIRECTOR THINKSMART! CONCUSSION MANAGEMENT, CO-DIRECTOR Consensus Statement: 5 th Annual Meeting, Berlin
Outline Cases in Sport Related Concussion Management The Team Approach. Initial Findings. Case 1: Initial Findings, recommendations: Referral
 Outline Cases in Sport Related Concussion Management The Team Approach Panel: - Aimee Custer, PsyD - Amy Hamilton, ATC - Carly Mattson, DPT - Alex Noll, DO Case 1: 16 y/o FB Player, helmet to helmet contact
Outline Cases in Sport Related Concussion Management The Team Approach Panel: - Aimee Custer, PsyD - Amy Hamilton, ATC - Carly Mattson, DPT - Alex Noll, DO Case 1: 16 y/o FB Player, helmet to helmet contact
Disclosure Statement. Dr. Kadish has no relevant financial relationships with any commercial interests mentioned in this talk.
 Disclosure Statement Dr. Kadish has no relevant financial relationships with any commercial interests mentioned in this talk. Head Trauma Evaluation Primary and secondary injury Disposition Sports related
Disclosure Statement Dr. Kadish has no relevant financial relationships with any commercial interests mentioned in this talk. Head Trauma Evaluation Primary and secondary injury Disposition Sports related
CONCUSSION INFORMATION When in Doubt, Sit Them Out!
 CONCUSSION INFORMATION When in Doubt, Sit Them Out! A concussion is a type of traumatic brain injury that interferes with normal function of the brain. All concussions are brain injuries. The WIAA recommends
CONCUSSION INFORMATION When in Doubt, Sit Them Out! A concussion is a type of traumatic brain injury that interferes with normal function of the brain. All concussions are brain injuries. The WIAA recommends
Post Concussion Instructions and Return to Play Clearance Form. To: Parent/Guardian: Page 1. From:, at School
 Post Concussion Instructions and Return to Play Clearance Form To: Parent/Guardian: From:, at School Name of School Representative* Name of School, Position of School Representative* Phone Number of School
Post Concussion Instructions and Return to Play Clearance Form To: Parent/Guardian: From:, at School Name of School Representative* Name of School, Position of School Representative* Phone Number of School
Wisconsin Lacrosse Federation
 The purpose of this policy is to insure the safety of the players and to limit the liability of those protecting the safety of the players. The responsibility of player safety falls on everyone involved
The purpose of this policy is to insure the safety of the players and to limit the liability of those protecting the safety of the players. The responsibility of player safety falls on everyone involved
Concussion. Concussion is a disturbance of brain function caused by a direct or indirect force to the head.
 Concussion Concussion is a disturbance of brain function caused by a direct or indirect force to the head. Disturbances of brain tissue is largely related to neurometabolic dysfunction rather then structural
Concussion Concussion is a disturbance of brain function caused by a direct or indirect force to the head. Disturbances of brain tissue is largely related to neurometabolic dysfunction rather then structural
Notre Dame of Maryland University Athletics Concussion Management Protocol
 Notre Dame of Maryland University Athletics Concussion Management Protocol Neuropsychological (NP) Baseline Testing: All NCAA sports will utilize baseline NP testing. All athletes will receive baseline
Notre Dame of Maryland University Athletics Concussion Management Protocol Neuropsychological (NP) Baseline Testing: All NCAA sports will utilize baseline NP testing. All athletes will receive baseline
Centers for Disease Control and Prevention Guideline on the Diagnosis and Management of Mild Traumatic Brain Injury Among Children September 2018
 Centers for Disease Control and Prevention Guideline on the Diagnosis and Management of Mild Traumatic Brain Injury Among Children September 2018 Nothing to Disclose CDC Guidelines- Objective Question-
Centers for Disease Control and Prevention Guideline on the Diagnosis and Management of Mild Traumatic Brain Injury Among Children September 2018 Nothing to Disclose CDC Guidelines- Objective Question-
Concussion Management. Michael Reardon, M.D. April 24,2016
 Concussion Management Michael Reardon, M.D. April 24,2016 Objectives Understand what a concussion is Know how to recognize it Understand the differential diagnosis Know how to manage and treat symptoms
Concussion Management Michael Reardon, M.D. April 24,2016 Objectives Understand what a concussion is Know how to recognize it Understand the differential diagnosis Know how to manage and treat symptoms
CONCUSSIONS. Recognition, Assessment, Management, and Return to Play
 CONCUSSIONS Recognition, Assessment, Management, and Return to Play What is a concussion? A concussion is a traumatic injury to the soft tissue of the brain as a result of a violent blow. The brain tissue
CONCUSSIONS Recognition, Assessment, Management, and Return to Play What is a concussion? A concussion is a traumatic injury to the soft tissue of the brain as a result of a violent blow. The brain tissue
Clinical Interpretation Manual
 The Best Approach to Concussion Management ImPACT 2007 (6.0) Clinical Interpretation Manual Fall 2007 IMPACT CONCUSSION MANAGEMENT SOFTWARE 2007 Clinical Interpretation Manual Table of Contents 1 About
The Best Approach to Concussion Management ImPACT 2007 (6.0) Clinical Interpretation Manual Fall 2007 IMPACT CONCUSSION MANAGEMENT SOFTWARE 2007 Clinical Interpretation Manual Table of Contents 1 About
Little League Concussion Information Sheet
 Little League Concussion Information Sheet Why am I getting this information sheet? You are receiving this information sheet about concussion because of California Assembly Bill 2007 (2016), which added
Little League Concussion Information Sheet Why am I getting this information sheet? You are receiving this information sheet about concussion because of California Assembly Bill 2007 (2016), which added
Sam Houston State University Department of Athletics Concussion Management Policy
 Sam Houston State University Department of Athletics Concussion Management Policy Sam Houston State University will evaluate all student athletes who exhibit signs, symptoms or behaviors consistent with
Sam Houston State University Department of Athletics Concussion Management Policy Sam Houston State University will evaluate all student athletes who exhibit signs, symptoms or behaviors consistent with
Concussion Management Policy Overview. City School District of Albany Department of Health, Physical Education & Athletics
 Concussion Management Policy Overview City School District of Albany Department of Health, Physical Education & Athletics CSDA Concussion Management Policy After 6 months of research and development, the
Concussion Management Policy Overview City School District of Albany Department of Health, Physical Education & Athletics CSDA Concussion Management Policy After 6 months of research and development, the