Measuring Complications of Treatment: Diagnoses Not Present on Admission. Henry Johnson, MD MPH Medical Director June 6, 2007
|
|
|
- Kory Walsh
- 5 years ago
- Views:
Transcription

1 Measuring Complications of Treatment: Diagnoses Not Present on Admission Henry Johnson, MD MPH Medical Director June 6, 2007
2 Summary Present on Admission (POA) Field for Secondary Diagnoses. History. Research supporting its use to find complications of care. UB 04. Deficit Reductions Act of 2005, use by Medicare. Profile of POA frequency in a sample hospital. Current use of the field in DataVision. ReporTrack use for Care Management 7.0 rev8 or higher.
3 Introduction 2007: All secondary diagnoses will be designated as Present on Admission (POA) or not. UB 04 has fields for this data. Medicare begins collecting data October : Medicare will choose at least two sets of two or more DRG s where there is a secondary diagnosis which triggers a CC DRG, and deny payment for the higher paying DRG [with CC], if the secondary diagnosis that triggers the CC was not present at admission.
4 How can POA help us? Knowing which secondary diagnoses were present on admission, allows you (as well as Medicare) to find those patients who went home with that little extra something: UTI Pneumonia CHF Hip Fracture
5 Current State At discharge, every inpatient chart is abstracted. ICD-9 codes are assigned for every diagnosis and procedure. A grouper assigns a DRG.
6 Current State, continued Principal Diagnosis: That condition established after study to be chiefly responsible for occasioning the admission. (Uniform Hospital Discharge Data Set, UHDDS)
7 Current State, continued Secondary Diagnoses: Everything else. UB-92: All secondary diagnoses listed without further notation. UB-04: All diagnoses will be designated as present on admission (Y), not present at admission (N), No information in the record (U), Clinically undetermined (W), or Exempt from POA Reporting (Unreported/Not Used).
8 Current State, continued All other data must be entered manually. Core measures. Specialty databases: Society of Thoracic Surgeons. Transplant databases. There is little tolerance for collecting more data manually: Abstracted/Coded data is our Interstate and we must make best use of it.
9 Background: Measuring performance based on administrative data: 1991: Naessens et. al. reported that the separation of secondary diagnoses into preexisting vs. acquired could: Be reliably undertaken by discharge abstractors. Be efficient in adding minimal time to coding. Enhance the validity and usefulness of data and increase physician acceptance. Naessens JM, Brennan MD, Boberg CJ, Amadio PC, Karver PH, Podratz RO. Acquired conditions: an improvement to hospital discharge abstracts. Qual Assur Helath Care 1991;3(4):257-62
10 Background, continued: 1990 s: California Office of Statewide Health Planning and Development (OSHPD) ran the California Hospital Outcomes Project: Romano, Remy and Luft (UC Davis and UCSF) created regression models to risk adjust the data. Problem: Is a secondary diagnosis a pre-existing condition that puts patients in a higher risk category, or a complication of care (adverse outcome). Example: AMI patients with secondary diagnosis of CHF: Risk factor, or complication of care?
11 Background, continued:... misclassifying conditions diagnosed after admission as risk factors leads to significant bias in the Model B regression coefficients.... This finding supports OSHPD s decision to report the results of the two models separately, and confirms the importance of adding a data element indicating whether each diagnosis was present at admission to the hospital discharge data system. Romano, Remy and Luft, Second Report of the California Hospital Outcomes Project (1996): Acute MI Volume Two: Technical Appendix-Chapter 15 The data element for diagnosis present at admission added to California hospital reporting in January 1996.
12 83 yo woman, 12 day admission. DRG 557 PCI w/ drug eluting stent w/ maj CV Dx Code Diagnosis POA DX AMI LATERAL NEC, INITIAL Present on Admission DX CRNRY ATHRSCL NATVE VSSL Present on Admission DX ATRIAL FIBRILLATION Not Present on Admission DX ULCER OTH PART LOW LIMB Present on Admission DX CHF NOS Present on Admission DX ACUTE RENAL FAILURE NOS Not Present on Admission DX7 570 ACUTE NECROSIS OF LIVER Not Present on Admission DX HYPOSMOLALITY Not Present on Admission DX VENOUS INSUFFICIENCY NOS Present on Admission DX HYPERTENSION NOS Present on Admission DX CHOLELITHIASIS NOS Present on Admission DX PHLBTS VN NOS UP EXTRM Not Present on Admission DX DMII WO CMP NT ST UNCNTR Present on Admission DX STAPHYLOCOCCUS AUREUS Present on Admission DX15 V09.0 INF MCRG RSTN PNCLLINS Present on Admission
13 83 yo woman, 12 day admission. DRG 557 PCI w/ drug eluting stent w/ maj CV Dx Code Diagnosis POA DX AMI LATERAL NEC, INITIAL Present on Admission DX CRNRY ATHRSCL NATVE VSSL Present on Admission DX ATRIAL FIBRILLATION Not Present on Admission DX ULCER OTH PART LOW LIMB Present on Admission DX CHF NOS Present on Admission DX ACUTE RENAL FAILURE NOS Not Present on Admission DX7 570 ACUTE NECROSIS OF LIVER Not Present on Admission DX HYPOSMOLALITY Not Present on Admission DX VENOUS INSUFFICIENCY NOS Present on Admission DX HYPERTENSION NOS Present on Admission DX CHOLELITHIASIS NOS Present on Admission DX PHLBTS VN NOS UP EXTRM Not Present on Admission DX DMII WO CMP NT ST UNCNTR Present on Admission DX STAPHYLOCOCCUS AUREUS Present on Admission DX15 V09.0 INF MCRG RSTN PNCLLINS Present on Admission
14 41 yo man, 18 day admission. DRG 110, Mayor CV procedures with CC Code Diagnosis POA DX AMI ANTERIOR WALL, INIT Present on Admission DX ACUTE RESPIRATRY FAILURE Present on Admission DX ACUTE RENAL FAILURE NOS Present on Admission DX VENTRICULAR FIBRILLATION Present on Admission DX CARDIAC ARREST Present on Admission DX CARDIOGENIC SHOCK Present on Admission DX CHF NOS Present on Admission DX COMP-OTH CARDIAC DEVICE Not Present on Admission DX FOOD/VOMIT PNEUMONITIS Not Present on Admission DX URIN TRACT INFECTION NOS Not Present on Admission DX ENCEPHALOPATHY NOS Not Present on Admission DX CRNRY ATHRSCL NATVE VSSL Present on Admission DX HYPERTENSION NOS Present on Admission DX ANXIETY STATE NOS Present on Admission DX HYPERLIPIDEMIA NEC/NOS Present on Admission
15 41 yo man, 18 day admission. DRG 110, Mayor CV procedures with CC Code Diagnosis POA DX AMI ANTERIOR WALL, INIT Present on Admission DX ACUTE RESPIRATRY FAILURE Present on Admission DX ACUTE RENAL FAILURE NOS Present on Admission DX VENTRICULAR FIBRILLATION Present on Admission DX CARDIAC ARREST Present on Admission DX CARDIOGENIC SHOCK Present on Admission DX CHF NOS Present on Admission DX COMP-OTH CARDIAC DEVICE Not Present on Admission DX FOOD/VOMIT PNEUMONITIS Not Present on Admission DX URIN TRACT INFECTION NOS Not Present on Admission DX ENCEPHALOPATHY NOS Not Present on Admission DX CRNRY ATHRSCL NATVE VSSL Present on Admission DX HYPERTENSION NOS Present on Admission DX ANXIETY STATE NOS Present on Admission DX HYPERLIPIDEMIA NEC/NOS Present on Admission
16 Is there any evidence to support collecting this data (POA) on all secondary diagnoses? CAUTION: Research
17 Naessens JM, Huschka TR: Distinguishing hospital complications of care from pre-existing conditions. International Journal for Quality in Health Care 2004: Volume 16, Supplement 1: pp i27-i35 Objective: To compare cases identified through the Complications Screening Program (CSP) with cases using the same ICD-9 secondary diagnosis codes, where the identifying diagnosis is also indicated as not present at admission. Setting: 84,436 discharges from Mayo Clinic Rochester.
18 Naessens JM, Huschka TR: Distinguishing hospital complications of care from pre-existing conditions. International Journal for Quality in Health Care 2004: Volume 16, Supplement 1: pp i27-i35 Outcome: % of algorithm complication cases indicated as developing in the hospital. % of acquired conditions of that type detected by the computer algorithms. Incremental hospital charges, length of stay and mortality associated with acquired complications.
19 All admissions CSP Dx Acquired
20 Naessens JM, Huschka TR: Distinguishing hospital complications of care from pre-existing conditions. International Journal for Quality in Health Care 2004: Volume 16, Supplement 1: pp i27-i35 Results: % of cases identified through the computer algorithm that were also coded as acquired varied from 8.8% to 100%. The ability of the computer algorithms to detect acquired conditions of that type varied from 2% to 99%.
21 Complication Cases with complication as defined by algorithm, N Positive Predictive Value % algorithm complications identified as developing in hospital Cases with acquired conditiion coded, N Sensitivity Percent of acquired conditions detected by algorithm % Septicemia % % Shock or cardiorespiratory arrest in hospital % % Postoperative acute myocardial infarction % % Venous thrombosis and pulmonary embolism % % Wound infection % % Post-procedural hemorrhage or hematoma % % Inhospital hip fracture or fall % %
22 Naessens JM, Huschka TR: Distinguishing hospital complications of care from pre-existing conditions. International Journal for Quality in Health Care 2004: volume 16, Supplement 1: pp i27-i35 Conclusions: Complication rates based strictly on standard discharge abstracts prior to UB-04 have limited use due to insensitivity of existing computer algorithms to exclude conditions present on admission from true complications. Adding an indicator identifying which diagnoses were present on admission greatly increases the accurate identification of complications for internal quality and patient safety improvement.
23 UB-04 Expanded field size to accommodate ICD-10 for both procedures and diagnoses. Box to indicate which ICD version hospital is using. Room for 16 diagnosis codes (UB-92 had 9). Larger field size for procedure codes on outpatient claims. Fields to designate each diagnosis as Y Yes N No U No information in the record W Clinically Undetermined (unreported, not used) Exempt from POA reporting
24 Medicare: Deficit Reduction Act of 2005
25
26 Deficit Reduction Act of 2005 In addition, this section would reduce payments to hospitals in some cases when the patient acquires an infection during a hospital stay. In particular, the Secretary of Health and Human Services would be required to select at least two sets of two or more diagnosis-related groups (DRGs) in which it is common for patients who otherwise would be assigned to a lowerpaying DRG to be assigned to the higher-paying DRG when there is a secondary diagnosis that results from infections acquired during the hospital stay. For discharges occurring on or after October 1, 2008, Medicare would set the payment rate for cases involving those DRGs at the level of the lower-paying DRG if the secondary diagnoses that resulted in assignment to the higher-paying DRG were not present at the time of admission.
27 CMS, Proposed Rules for 2008 include: [Released April 13, 2007] Severity adjust DRG s. No payment for additional costs of hospital acquired conditions. Expanded list of publicly reported measures.
28 CMS: Proposed Selection of Hospital-Acquired Conditions: Proposed Rule FY2008 [April 13, 2007] Catheter associated urinary tract infections. Pressure ulcers (decubitus ulcers). Serious preventable event object left in surgery. Serious preventable event air embolism. Serious preventable event blood incompatibility. Staphylococcus aureus septicema. Ventilator associated pneumonia. Vascular catheter associated infections. Clostridium difficile-associated disease. Methicillin-resistent staphylococcus aureus. Surgical site infections. Serious preventable event wrong surgery. Falls.
29 Top Six: Catheter associated urinary tract infections: Good codes, triggers CC pair, prevention guidelines exist, high cost and high frequency. Pressure ulcers (decubitus ulcers): Good codes, high volume, high cost, prevention guidelines exist, codes triggers CC in a pair, Serious preventable event object left in surgery. Good codes, rare event with high costs (removal), prevention exists, triggers CC, Serious preventable event air embolism: Rare, but meets criteria. Serious preventable event blood incompatibility. Rare, but meets criteria. Staphylococcus aureus septicema. Codes complex, but meets criteria.
30 Also Ran: Ventilator associated pneumonia. No unique codes. Vascular catheter associated infections. No specific code. Clostridium difficile-associated disease. Preventable? No best practice. Methicillin-resistent staphylococcus aureus. Prevention issues. Surgical site infections. Code too broad Serious preventable event wrong surgery. No DRG CC pair for this. Falls. Cannot identify coding issue.
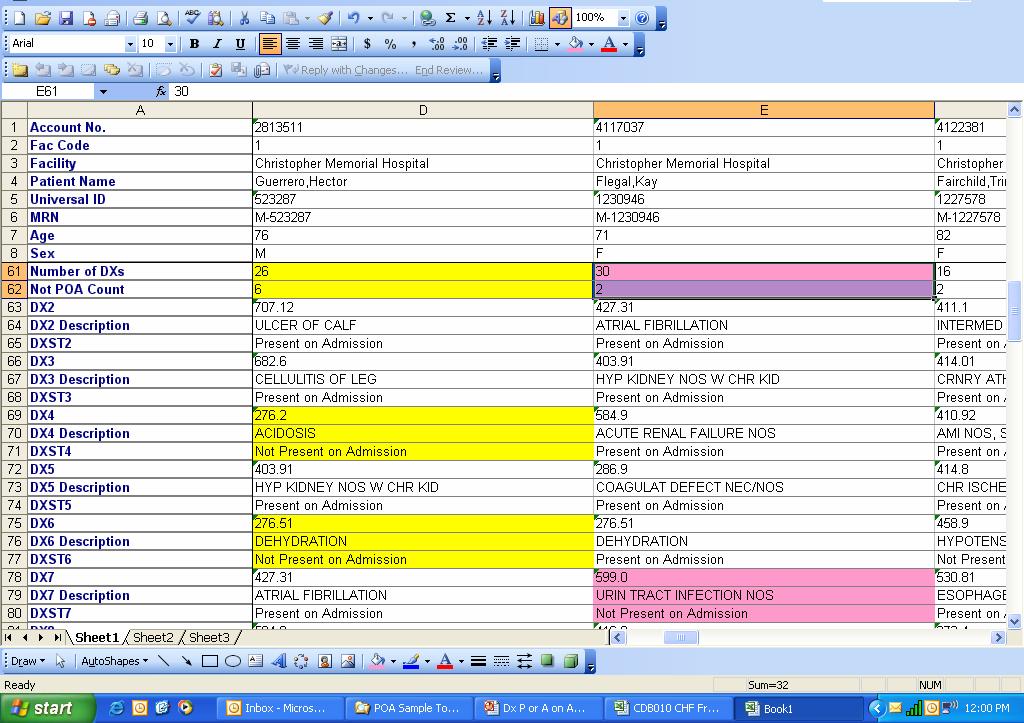
31 Sample Frequency Distributions: What to expect when we begin to code secondary diagnoses as present (or not) on admission.
32 Sample Hospital: Discharges by MDC, 12 months MDC Description Total % NPOA Totals 1 Nervous System Sum of All POA 1026 Sum of 1 or More NPOA % Eye Sum of All POA 53 Sum of 1 or More NPOA 3 5.7% 56 3 ENT Sum of All POA 322 Sum of 1 or More NPOA % Respiratory Sum of All POA 1518 Sum of 1 or More NPOA % Circulatory Sum of All POA 2051 Sum of 1 or More NPOA % Digestive Sum of All POA 1240 Sum of 1 or More NPOA % Hepatobiliary and Pancreas Sum of All POA 526 Sum of 1 or More NPOA % Muscuskeletal System and Conn T. Sum of All POA 1802 Sum of 1 or More NPOA % Skin, SQ Tissue, and Breast Sum of All POA 777 Sum of 1 or More NPOA % Endo, Nutrit, Metabolic Sum of All POA 1984 Sum of 1 or More NPOA % 2244
33 MDC 5, Circulatory, top 19 DRG s by volume DRG DRG Desc Cases >= 1 Dx Total %NPOA NPOA 127 HEART FAILURE & SHOCK % 124 CIRCULATORY DISORDERS EXCEPT AMI, W CAR % 138 CARDIAC ARRHYTHMIA & CONDUCTION DISORD % 143 CHEST PAIN % 121 CIRCULATORY DISORDERS W AMI & MAJOR COM % 144 OTHER CIRCULATORY SYSTEM DIAGNOSES W C % 141 SYNCOPE & COLLAPSE W CC % 107 CORONARY BYPASS W CARDIAC CATH % 116 OTH PERM CARDIAC PACEMAKER IMPLANT OR P % 130 PERIPHERAL VASCULAR DISORDERS W CC % 125 CIRCULATORY DISORDERS EXCEPT AMI, W CAR % 132 ATHEROSCLEROSIS W CC % 110 MAJOR CARDIOVASCULAR PROCEDURES W CC % 122 CIRCULATORY DISORDERS W AMI W/O MAJOR C % 120 OTHER CIRCULATORY SYSTEM O.R. PROCEDUR % 109 CORONARY BYPASS W/O CARDIAC CATH % 134 HYPERTENSION % 113 AMPUTATION FOR CIRC SYSTEM DISORDERS EX % 105 CARDIAC VALVE & OTH MAJ CARDIOTHORACIC P %
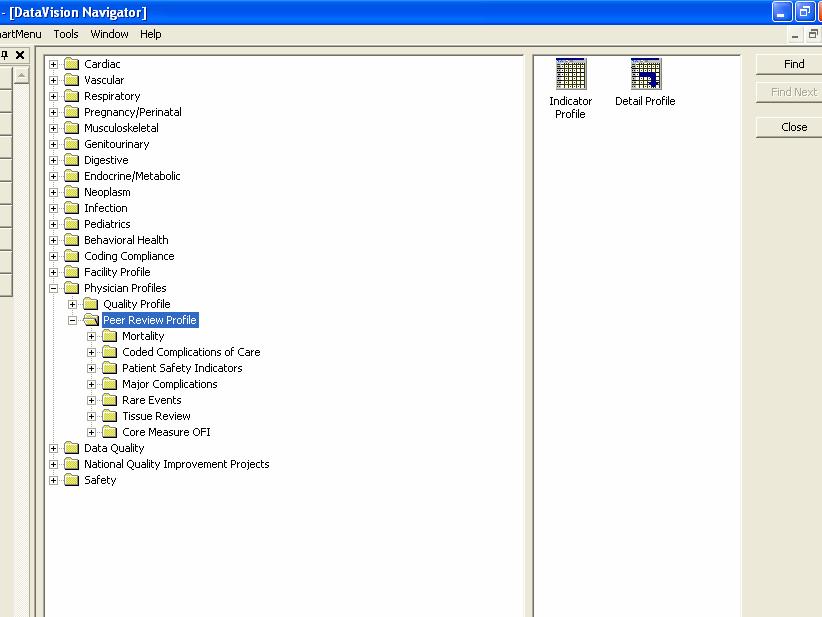
34 Uses in MIDAS+/DV Software On server: DV Navigator: Excel export and macros. Physician Profiles. ReporTrack Reporting. Care Management 7.0 rev 8 or higher.

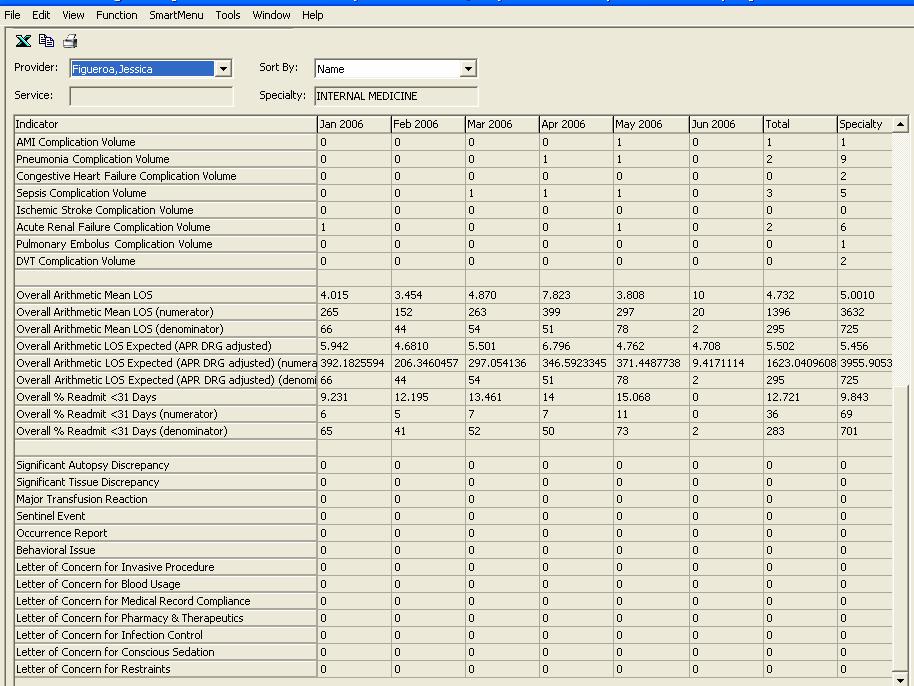
35 CHF Frequency/1000 ACA DRG 127: July 05 to June 06
36 CHF Frequency/1000 ACA DRG 127: July 05 to June 06 Complications of Care Total Cases 232 # Cases with all Dx present on admission 212 # Cases with one or more Dx Not Present on Admission 20 Major Complications Not Present On Admission Acute Myocardial Infarction 0 Pneumonia 3 Congestive Heart Failure 0 Acute Renal Failure 1 Ischemic Stroke 0 Sepsis 0 Pulmonary Embolus 0 Deep Venous Thrombosis 0
37 CHF Frequency/1000 ACA DRG 127: July 05 to June 06 Other Complications Not Present On Admission Diagnosis Total URIN TRACT INFECTION NOS 3 ACUTE RESPIRATRY FAILURE 3 ATRIAL FIBRILLATION 2 CARDIAC ARREST 2 HYPOPOTASSEMIA 2 HYPOSMOLALITY 2 HYPOTENSION NOS 2 NAUSEA WITH VOMITING 2
38 Pivot Table Count of Account No. Not POA Count2 One or More Years End Dt 0 Dx Not POA Grand Total 2005 Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Grand Total
39

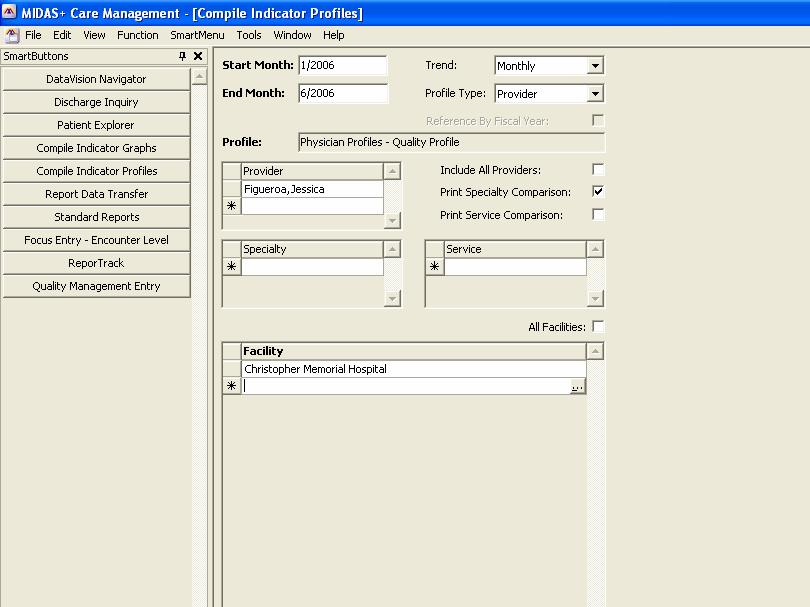
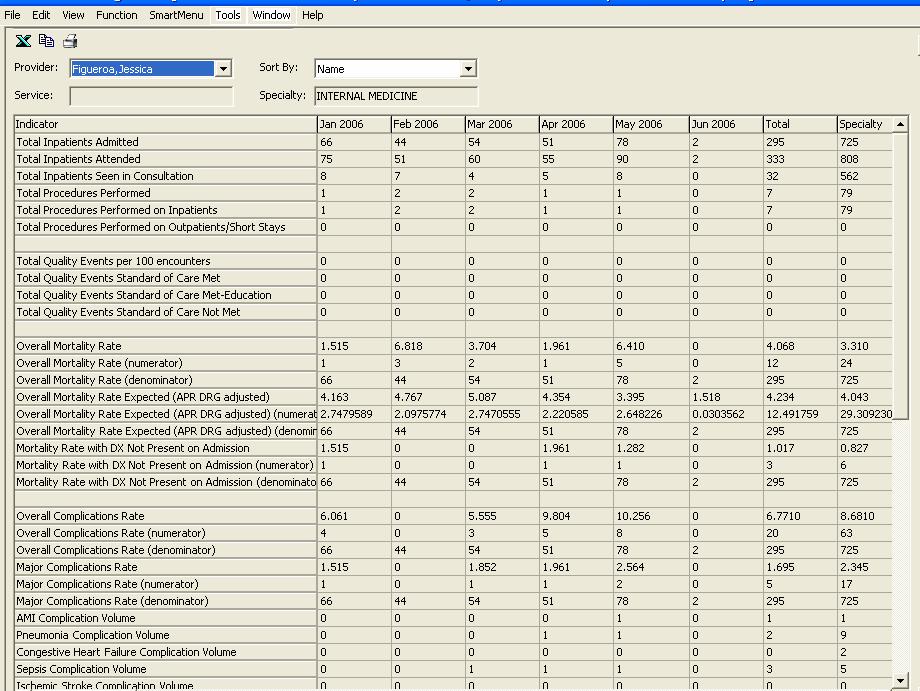
40 DV Navigator: Physician Profiles
41
42
43
44

45 All inpatient encounters, all providers
46 ReporTrack Reporting You can identify patients based on any secondary diagnosis not present on admission in Care Management 7.0 rev 8 or higher.
47
48 Summary Present on Admission (POA) Field for Secondary Diagnoses. History. Research supporting its use to find complications of care. UB 04. Deficit Reductions Act of 2005, use by Medicare. Profile of POA frequency in a sample hospital. Current use of the field in DataVision. ReporTrack use for Care Management 7.0 rev8 or higher.
Medicare and Medicaid Payments
 and Payments The following table includes information about payments made by and for the 17 medical conditions/surgical procedures included in this Hospital Performance Report. This analysis is based on
and Payments The following table includes information about payments made by and for the 17 medical conditions/surgical procedures included in this Hospital Performance Report. This analysis is based on
Supplementary Online Content
 Supplementary Online Content Likosky DS, Zhou W, Malenka DJ, Borden WB, Nallamothu BK, Skinner JS. rowth in Medicare expenditures for patients with acute myocardial infarction: a comparison of 1998 through
Supplementary Online Content Likosky DS, Zhou W, Malenka DJ, Borden WB, Nallamothu BK, Skinner JS. rowth in Medicare expenditures for patients with acute myocardial infarction: a comparison of 1998 through
Appendix. Potentially Preventable Complications (PPCs) identify. complications that can occur during an admission. There are 64
 identify. complications that can occur during an admission. There are 64") Calikoglu S, Murray R, Feeney D. Hospital pay-for-performance programs in Maryland produced strong results, including reduced hospital-acquired infections. Health Aff (Millwood). 2012;31(12). Appendix
Calikoglu S, Murray R, Feeney D. Hospital pay-for-performance programs in Maryland produced strong results, including reduced hospital-acquired infections. Health Aff (Millwood). 2012;31(12). Appendix
A Pause in the Availability of Risk Adjusted National Benchmarks for AHRQ Indicators and an Alternative Measurement Approach
 A Pause in the Availability of Risk Adjusted National Benchmarks for AHRQ Indicators and an Alternative Measurement Approach Joseph Greenway, MPH Director of the Center for Health Information Analysis
A Pause in the Availability of Risk Adjusted National Benchmarks for AHRQ Indicators and an Alternative Measurement Approach Joseph Greenway, MPH Director of the Center for Health Information Analysis
APR DRG Data Discovery
 APR DRG Data Discovery Henry Johnson MD, MPH Midas+ Vice President and Medical Director Vanessa Dorr RN MSN Midas+ DataVision Clinical Consultant Review: Agenda 3M APR DRG Methodology DataVision: Web and
APR DRG Data Discovery Henry Johnson MD, MPH Midas+ Vice President and Medical Director Vanessa Dorr RN MSN Midas+ DataVision Clinical Consultant Review: Agenda 3M APR DRG Methodology DataVision: Web and
Medicare Payments. PHC4 Hospital Performance Report Oct 2015 through Sept 2016 Data 2015 Medicare Payments 1
 The following table includes information about payments made by for the 16 medical conditions/surgical procedures included in this Hospital Performance Report. This analysis is based on data from calendar
The following table includes information about payments made by for the 16 medical conditions/surgical procedures included in this Hospital Performance Report. This analysis is based on data from calendar
Appendix 1: Supplementary tables [posted as supplied by author]
![Appendix 1: Supplementary tables [posted as supplied by author]](/thumbs/81/83505567.jpg "Appendix 1: Supplementary tables [posted as supplied by author]") Appendix 1: Supplementary tables [posted as supplied by author] Table A. International Classification of Diseases, Ninth Revision, Clinical Modification Codes Used to Define Heart Failure, Acute Myocardial
Appendix 1: Supplementary tables [posted as supplied by author] Table A. International Classification of Diseases, Ninth Revision, Clinical Modification Codes Used to Define Heart Failure, Acute Myocardial
SEPTICEMIA OR SEVERE SEPSIS W/O MV >96 HOURS W MCC 84, ,037.80
 Inpatient Visits by DRG Inpatient Discharges between 10/01/17 and 09/30/18 DRG DRG Description Average Charge Self-Pay Price VAGINAL DELIVERY W/O COMPLICATING 775 DIAGNOSES 14,680.67 5,578.66 795 NORMAL
Inpatient Visits by DRG Inpatient Discharges between 10/01/17 and 09/30/18 DRG DRG Description Average Charge Self-Pay Price VAGINAL DELIVERY W/O COMPLICATING 775 DIAGNOSES 14,680.67 5,578.66 795 NORMAL
6/30/2015. Lunch and Learn. Objectives. Who owns Quality and Patient Safety? We all do It s a Balance of Responsibility
 Lunch and Learn Patient Safety Indicators June 11, 2014 Objectives List at least 3 entities that drive patient quality and safety initiatives Define AHRQ Patient Safety Indicators Describe the 10 diagnoses
Lunch and Learn Patient Safety Indicators June 11, 2014 Objectives List at least 3 entities that drive patient quality and safety initiatives Define AHRQ Patient Safety Indicators Describe the 10 diagnoses
Medicare Payments. PHC4 Hospital Performance Report Oct 2016 through Sept 2017 Data FFY 2017 Medicare Payments 1
 The following table includes information about payments made by for the 16 medical conditions/surgical procedures included in this Hospital Performance Report. This analysis is based on data from federal
The following table includes information about payments made by for the 16 medical conditions/surgical procedures included in this Hospital Performance Report. This analysis is based on data from federal
2018 Diagnosis Coding Fact Sheet
 The information contained in this document is provided for informational purposes only and represents no statement, promise, or guarantee by Cordis Corporation concerning levels of reimbursement, payment,
The information contained in this document is provided for informational purposes only and represents no statement, promise, or guarantee by Cordis Corporation concerning levels of reimbursement, payment,
Distinguishing hospital complications of care from pre-existing conditions
 International Journal for Quality in Health Care 2004; Volume 16, Supplement 1: pp. i27 i35 10.1093/intqhc/mzh012 Distinguishing hospital complications of care from pre-existing conditions JAMES M. NAESSENS
International Journal for Quality in Health Care 2004; Volume 16, Supplement 1: pp. i27 i35 10.1093/intqhc/mzh012 Distinguishing hospital complications of care from pre-existing conditions JAMES M. NAESSENS
What ASMBS Members Need to Know About: New Medicare Payment Policy Governing Bariatric Surgery and Hospital Acquired Conditions (HACs)
") What ASMBS Members Need to Know About: New Medicare Payment Policy Governing Bariatric Surgery and Hospital Acquired Conditions (HACs) Robin Blackstone, MD, FACS, FASMBS Beginning October 1, 2008, Medicare
What ASMBS Members Need to Know About: New Medicare Payment Policy Governing Bariatric Surgery and Hospital Acquired Conditions (HACs) Robin Blackstone, MD, FACS, FASMBS Beginning October 1, 2008, Medicare
ENROLLMENT : Line of Business Summary
 ENROLLMENT : Line of Business Summary Date Range : JAN 2017 through DEC 2017 COMPREHENSIVE MAJOR MEDICAL Print Date : 1/19/2018 9:43:49AM Page 1 of 1 Month Year Single 2 Person : Emp/Spouse 2 Person :
ENROLLMENT : Line of Business Summary Date Range : JAN 2017 through DEC 2017 COMPREHENSIVE MAJOR MEDICAL Print Date : 1/19/2018 9:43:49AM Page 1 of 1 Month Year Single 2 Person : Emp/Spouse 2 Person :
Address: Ownership Type: Proprietary Not-for Prepared by: Ben Spence
 Hospital Name: Gulf Coast Medical Center Lee Memorial Health System Address: Ownership Type: Proprietary Not-for Prepared by: Ben Spence Hospital Website: leememorial.org Charge Master Website: www.leememorial.org/price/index.asp
Hospital Name: Gulf Coast Medical Center Lee Memorial Health System Address: Ownership Type: Proprietary Not-for Prepared by: Ben Spence Hospital Website: leememorial.org Charge Master Website: www.leememorial.org/price/index.asp
TECHNICAL NOTES APPENDIX SUMMER
 TECHNICAL NOTES APPENDIX SUMMER Hospital Performance Report Summer Update INCLUDES PENNSYLVANIA INPATIENT HOSPITAL DISCHARGES FROM JULY 1, 2006 THROUGH JUNE 30, 2007 The Pennsylvania Health Care Cost Containment
TECHNICAL NOTES APPENDIX SUMMER Hospital Performance Report Summer Update INCLUDES PENNSYLVANIA INPATIENT HOSPITAL DISCHARGES FROM JULY 1, 2006 THROUGH JUNE 30, 2007 The Pennsylvania Health Care Cost Containment
EACTS Adult Cardiac Database
 EACTS Adult Cardiac Database Quality Improvement Programme List of changes to Version 2.0, 13 th Dec 2018, compared to version 1.0, 1 st May 2014. INTRODUCTORY NOTES This document s purpose is to list
EACTS Adult Cardiac Database Quality Improvement Programme List of changes to Version 2.0, 13 th Dec 2018, compared to version 1.0, 1 st May 2014. INTRODUCTORY NOTES This document s purpose is to list
APR-DRG Description Ave Charge
 Abdominal Pain 16,500.25 2.8 6,000.09 Acute & Subacute Endocarditis 15,339.30 3.0 5,113.10 Acute Myocardial Infarction 17,687.46 2.6 6,802.87 Alcohol Abuse & Dependence 19,126.64 4.2 4,553.96 Alcoholic
Abdominal Pain 16,500.25 2.8 6,000.09 Acute & Subacute Endocarditis 15,339.30 3.0 5,113.10 Acute Myocardial Infarction 17,687.46 2.6 6,802.87 Alcohol Abuse & Dependence 19,126.64 4.2 4,553.96 Alcoholic
Policy Brief June 2014
 Policy Brief June 2014 Which Medicare Patients Are Transferred from Rural Emergency Departments? Michelle Casey MS, Jeffrey McCullough PhD, and Robert Kreiger PhD Key Findings Among Medicare beneficiaries
Policy Brief June 2014 Which Medicare Patients Are Transferred from Rural Emergency Departments? Michelle Casey MS, Jeffrey McCullough PhD, and Robert Kreiger PhD Key Findings Among Medicare beneficiaries
Objectives. Medicare Spending per Beneficiary: Analyzing MSPB Data to Identify Primary Drivers
 Medicare Spending per Beneficiary: Analyzing MSPB Data to Identify Primary Drivers August 22, 2017 Objectives Understand the basics of the hospital specific MSPB data files and reports Review the factors
Medicare Spending per Beneficiary: Analyzing MSPB Data to Identify Primary Drivers August 22, 2017 Objectives Understand the basics of the hospital specific MSPB data files and reports Review the factors
Performance Measure. Inpatient Clinical Process of Care Measures
 Acute Myocardial Infarction (AMI) 's Maryland Hospital Performance Evaluation System: Inpatient s Quality Based Reimbursement () Measures Highlighted in Green (02/27/2014) Inpatient Clinical Process of
Acute Myocardial Infarction (AMI) 's Maryland Hospital Performance Evaluation System: Inpatient s Quality Based Reimbursement () Measures Highlighted in Green (02/27/2014) Inpatient Clinical Process of
TECHNICAL NOTES APPENDIX SUMMER
 TECHNICAL NOTES APPENDIX SUMMER Hospital Performance Report Summer Update INCLUDES PENNSYLVANIA INPATIENT HOSPITAL DISCHARGES FROM July 1, 2005 through June 30, 2006 The Pennsylvania Health Care Cost Containment
TECHNICAL NOTES APPENDIX SUMMER Hospital Performance Report Summer Update INCLUDES PENNSYLVANIA INPATIENT HOSPITAL DISCHARGES FROM July 1, 2005 through June 30, 2006 The Pennsylvania Health Care Cost Containment
Acute Coronary Syndrome
 ACUTE CORONOARY SYNDROME, ANGINA & ACUTE MYOCARDIAL INFARCTION Administrative Consultant Service 3/17 Acute Coronary Syndrome Acute Coronary Syndrome has evolved as a useful operational term to refer to
ACUTE CORONOARY SYNDROME, ANGINA & ACUTE MYOCARDIAL INFARCTION Administrative Consultant Service 3/17 Acute Coronary Syndrome Acute Coronary Syndrome has evolved as a useful operational term to refer to
Appendix 1. Validation studies of Agency for Healthcare Research and Quality (AHRQ) patient safety indicator (PSI) Validated PSI and author
 patient safety indicator (PSI) Validated PSI and author") Appendix 1. Validation studies of Agency for Healthcare Research and Quality (AHRQ) patient safety indicator (PSI) Validated PSI and author Reference standard, Year of data PPV ( % of N) Conclusion made
Appendix 1. Validation studies of Agency for Healthcare Research and Quality (AHRQ) patient safety indicator (PSI) Validated PSI and author Reference standard, Year of data PPV ( % of N) Conclusion made
Reporting Period and Reliability of AHRQ, CMS 30-day and HAC Quality Measures - Revised
 MEMORANDUM TO: Sophia Chan SUBJECT: Reporting Period and Reliability of AHRQ, CMS 30-day and HAC Quality Measures - Revised Reliability of an outcome measure is the extent to which variation in the measure
MEMORANDUM TO: Sophia Chan SUBJECT: Reporting Period and Reliability of AHRQ, CMS 30-day and HAC Quality Measures - Revised Reliability of an outcome measure is the extent to which variation in the measure
Determining MS-DRGs. Kimberly Cunningham CPC, CIC, CCS. Copyright/Disclaimer text
 Determining MS-DRGs Kimberly Cunningham CPC, CIC, CCS Copyright/Disclaimer text No part of this presentation may be reproduced or transmitted in any form or by any means (graphically, electronically, or
Determining MS-DRGs Kimberly Cunningham CPC, CIC, CCS Copyright/Disclaimer text No part of this presentation may be reproduced or transmitted in any form or by any means (graphically, electronically, or
Measure Applications Partnership. Hospital Workgroup In-Person Meeting Follow- Up Call
 Measure Applications Partnership Hospital Workgroup In-Person Meeting Follow- Up Call December 21, 2016 Feedback on Current Measure Sets for IQR, HACs, Readmissions, and VBP 2 Previously Identified Crosscutting
Measure Applications Partnership Hospital Workgroup In-Person Meeting Follow- Up Call December 21, 2016 Feedback on Current Measure Sets for IQR, HACs, Readmissions, and VBP 2 Previously Identified Crosscutting
Bundle Payments. Healthcare Systems & Services Presenters: Larry Litman, Tyler Litman
 Bundle Payments Healthcare Systems & Services Presenters: Larry Litman, Tyler Litman To determine the average cost of the SNF portion of a bundle through the analysis of our client data-base. Our Objective:
Bundle Payments Healthcare Systems & Services Presenters: Larry Litman, Tyler Litman To determine the average cost of the SNF portion of a bundle through the analysis of our client data-base. Our Objective:
Measuring Nursing Outcomes, with a Focus on Inpatient Complications
 1 Measuring Nursing Outcomes, with a Focus on Inpatient Complications Barbara Doyle MSN, CRNP Clinical Consultant CareScience, a Quovadx Division barbara.doyle@quovadx.com Agenda 2 Nursing Outcomes Measurement
1 Measuring Nursing Outcomes, with a Focus on Inpatient Complications Barbara Doyle MSN, CRNP Clinical Consultant CareScience, a Quovadx Division barbara.doyle@quovadx.com Agenda 2 Nursing Outcomes Measurement
Health Services Utilization and Medical Costs Among Medicare Atrial Fibrillation Patients / September 2010
 Health Services Utilization and Medical Costs Among Medicare Atrial Fibrillation Patients / September 2010 AF Stat is sponsored by sanofi-aventis, U.S. LLC, which provided funding for this report. Avalere
Health Services Utilization and Medical Costs Among Medicare Atrial Fibrillation Patients / September 2010 AF Stat is sponsored by sanofi-aventis, U.S. LLC, which provided funding for this report. Avalere
WORKING P A P E R. Comparative Performance of the MS-DRGS and RDRGS in Explaining Variation in Cost for Medicare Hospital Discharges BARBARA O.
 WORKING P A P E R Comparative Performance of the MS-DRGS and RDRGS in Explaining Variation in Cost for Medicare Hospital Discharges BARBARA O. WYNN WR-606 This product is part of the RAND Health working
WORKING P A P E R Comparative Performance of the MS-DRGS and RDRGS in Explaining Variation in Cost for Medicare Hospital Discharges BARBARA O. WYNN WR-606 This product is part of the RAND Health working
Nov FromAtoZCodesMatter
 Nov 2017 FromAtoZCodesMatter From A to Z-Codes Matter Susan Wallace, MEd, RHIA, CCS, CDIP, CCDS, FAHIMA The implementation of ICD-10 brought tens of thousands of new codes. Ranging from A to Z, they portray
Nov 2017 FromAtoZCodesMatter From A to Z-Codes Matter Susan Wallace, MEd, RHIA, CCS, CDIP, CCDS, FAHIMA The implementation of ICD-10 brought tens of thousands of new codes. Ranging from A to Z, they portray
DRG Code DRG Description FY18 Average Charge
 DRG Code DRG Description FY18 Average Charge 3 ECMO OR TRACH W MV 96+ HRS OR PDX EXC FACE, MOUTH & NECK W MAJ O $ 665,511 4 TRACH W MV 96+ HRS OR PDX EXC FACE, MOUTH & NECK W/O MAJ O.R. $ 422,497 37 EXTRACRANIAL
DRG Code DRG Description FY18 Average Charge 3 ECMO OR TRACH W MV 96+ HRS OR PDX EXC FACE, MOUTH & NECK W MAJ O $ 665,511 4 TRACH W MV 96+ HRS OR PDX EXC FACE, MOUTH & NECK W/O MAJ O.R. $ 422,497 37 EXTRACRANIAL
Optimal Diabetes Care Specifications 2015 (01/01/2014 to 12/31/2014 Dates of Service) October 2014
 October 2014") Summary of Changes Removal of LDL Component The LDL component has been removed for numerator calculation. Additional Ischemic Vascular Disease ICD-9 Codes Codes indicating atherosclerosis of bypass grafted
Summary of Changes Removal of LDL Component The LDL component has been removed for numerator calculation. Additional Ischemic Vascular Disease ICD-9 Codes Codes indicating atherosclerosis of bypass grafted
Keeping Up with the Regulatory Requirements and Other Hocus Pocus. Vicky A. Mahn-DiNicola RN, MS, CPHQ Vice President and Product Manager ACS MIDAS+
 Keeping Up with the Regulatory Requirements and Other Hocus Pocus Vicky A. Mahn-DiNicola RN, MS, CPHQ Vice President and Product Manager ACS MIDAS+ Session Objectives Review Medicare s proposed strategies
Keeping Up with the Regulatory Requirements and Other Hocus Pocus Vicky A. Mahn-DiNicola RN, MS, CPHQ Vice President and Product Manager ACS MIDAS+ Session Objectives Review Medicare s proposed strategies
Who's Driving the DRG Bus: Selecting the Appropriate Principal Diagnosis
 7th Annual Association for Clinical Documentation Improvement Specialists Conference Who's Driving the DRG Bus: Selecting the Appropriate Principal Diagnosis MedPartners CDI: Karen Newhouser, RN, BSN,
7th Annual Association for Clinical Documentation Improvement Specialists Conference Who's Driving the DRG Bus: Selecting the Appropriate Principal Diagnosis MedPartners CDI: Karen Newhouser, RN, BSN,
TECHNICAL NOTES. for the Cardiac Surgery Report
 TECHNICAL NOTES for the Cardiac Surgery Report September 2013 Pennsylvania Health Care Cost Containment Council Report Period: July 1, 2011 through December 31, 2012 225 Market Street, Suite 400, Harrisburg,
TECHNICAL NOTES for the Cardiac Surgery Report September 2013 Pennsylvania Health Care Cost Containment Council Report Period: July 1, 2011 through December 31, 2012 225 Market Street, Suite 400, Harrisburg,
Technical Appendix for Outcome Measures
 Study Overview Technical Appendix for Outcome Measures This is a report on data used, and analyses done, by MPA Healthcare Solutions (MPA, formerly Michael Pine and Associates) for Consumers CHECKBOOK/Center
Study Overview Technical Appendix for Outcome Measures This is a report on data used, and analyses done, by MPA Healthcare Solutions (MPA, formerly Michael Pine and Associates) for Consumers CHECKBOOK/Center
Hu J, Gonsahn MD, Nerenz DR. Socioeconomic status and readmissions: evidence from an urban teaching hospital. Health Aff (Millwood). 2014;33(5).
. 2014;33(5).") Appendix Definitions of Index Admission and Readmission Definitions of index admission and readmission follow CMS hospital-wide all-cause unplanned readmission (HWR) measure as far as data are available.
Appendix Definitions of Index Admission and Readmission Definitions of index admission and readmission follow CMS hospital-wide all-cause unplanned readmission (HWR) measure as far as data are available.
Cardiothoracic and Cardiothoracic Surgery ICD-10-CM 2014: Reference Mapping Card
 2014: Reference Mapping Card 162.3 Malignant neoplasm upper lobe lung 162.5 Malignant neoplasm lower lobe lung 162.9 lung/bronchus 396.2 396.3 Mitral insufficiency, aortic stenosis Mitral aortic valve
2014: Reference Mapping Card 162.3 Malignant neoplasm upper lobe lung 162.5 Malignant neoplasm lower lobe lung 162.9 lung/bronchus 396.2 396.3 Mitral insufficiency, aortic stenosis Mitral aortic valve
Risk Mitigation in Bundled Payment
 Risk Mitigation in Bundled Payment When to Hold Them and When To Fold Them Lily Pazand, MPH NYU Langone Medical Center Jonathan Pearce, MBA, CPA, FHFMA Singletrack Analytics Jessica Walradt, MS Association
Risk Mitigation in Bundled Payment When to Hold Them and When To Fold Them Lily Pazand, MPH NYU Langone Medical Center Jonathan Pearce, MBA, CPA, FHFMA Singletrack Analytics Jessica Walradt, MS Association
TENNCARE Bundled Payment Initiative: Description of Bundle Risk Adjustment for Wave 8 Episodes
 TENNCARE Bundled Payment Initiative: Description of Bundle Risk Adjustment for Wave 8 Episodes Acute Seizure, Syncope, Acute Gastroenteritis, Pediatric Pneumonia, Bronchiolitis, Colposcopy, Hysterectomy,
TENNCARE Bundled Payment Initiative: Description of Bundle Risk Adjustment for Wave 8 Episodes Acute Seizure, Syncope, Acute Gastroenteritis, Pediatric Pneumonia, Bronchiolitis, Colposcopy, Hysterectomy,
From A to Z-Codes Matter
 From A to Z-Codes Matter Susan Wallace, MEd, RHIA, CCS, CDIP, CCDS, FAHIMA While ALL ICD-10-CM codes are important, the Z-codes in ICD-10-CM are frequently considered step-children, supplemental codes
From A to Z-Codes Matter Susan Wallace, MEd, RHIA, CCS, CDIP, CCDS, FAHIMA While ALL ICD-10-CM codes are important, the Z-codes in ICD-10-CM are frequently considered step-children, supplemental codes
CMS Hospital Inpatient Quality Reporting (IQR) Program Measures for the FY 2019 Payment Update
 Program Measures for the FY 2019 Payment Update") CMS Inpatient Quality Reporting (IQR) Program Measures for the Update Measures Required to Meet IQR Program APU Requirements NHSN Submission CAUTI National Healthcare Safety Network (NHSN) Catheter-Associated
CMS Inpatient Quality Reporting (IQR) Program Measures for the Update Measures Required to Meet IQR Program APU Requirements NHSN Submission CAUTI National Healthcare Safety Network (NHSN) Catheter-Associated
Table 1. Proposed Measures for Use in Establishing Quality Performance Standards that ACOs Must Meet for Shared Savings
 CMS-1345-P 174 Table 1. Proposed Measures for Use in Establishing Quality Performance Standards that ACOs Must Meet for Shared Savings AIM: Better Care for Individuals 1. Patient/Care Giver Experience
CMS-1345-P 174 Table 1. Proposed Measures for Use in Establishing Quality Performance Standards that ACOs Must Meet for Shared Savings AIM: Better Care for Individuals 1. Patient/Care Giver Experience
Supplementary Online Content
 Supplementary Online Content Dharmarajan K, Wang Y, Lin Z, et al. Association of changing hospital readmission rates with mortality rates after hospital discharge. JAMA. doi:10.1001/jama.2017.8444 etable
Supplementary Online Content Dharmarajan K, Wang Y, Lin Z, et al. Association of changing hospital readmission rates with mortality rates after hospital discharge. JAMA. doi:10.1001/jama.2017.8444 etable
Optimal Diabetes Care Specifications 2013 (01/01/2012 to 12/31/2012 Dates of Service) Revised 08/10/2012
 Revised 08/10/2012") Summary of Changes Date of birth clarification Added language to clarify date of birth range. Please note the changes in the denominator section. Description Methodology Rationale Measurement Period Denominator
Summary of Changes Date of birth clarification Added language to clarify date of birth range. Please note the changes in the denominator section. Description Methodology Rationale Measurement Period Denominator
50198 Federal Register / Vol. 75, No. 157 / Monday, August 16, 2010 / Rules and Regulations
 50198 Federal Register / Vol. 75, No. 157 / Monday, August 16, 2010 / Rules and Regulations mstockstill on DSKH9S0YB1PROD with RULES2 VerDate Mar2010 17:02 Aug 13, 2010 Jkt 220001 PO 00000 Frm 00158
50198 Federal Register / Vol. 75, No. 157 / Monday, August 16, 2010 / Rules and Regulations mstockstill on DSKH9S0YB1PROD with RULES2 VerDate Mar2010 17:02 Aug 13, 2010 Jkt 220001 PO 00000 Frm 00158
Optimal Vascular Care Specifications 2015 (01/01/2014 to 12/31/2014 Dates of Service) October 2014
 October 2014") Summary of Changes Removal of LDL Component The LDL component has been removed for numerator calculation. Additional Ischemic Vascular Disease ICD-9 Codes Codes indicating atherosclerosis of bypass grafted
Summary of Changes Removal of LDL Component The LDL component has been removed for numerator calculation. Additional Ischemic Vascular Disease ICD-9 Codes Codes indicating atherosclerosis of bypass grafted
CMS Hospital Inpatient Quality Reporting (IQR) Program Measures for the FY 2020 Payment Update
 Program Measures for the FY 2020 Payment Update") CMS Inpatient Quality Reporting (IQR) Program Measures for the Payment Update Measures Required to Meet IQR Program APU Requirements Healthcare-Associated Infection on CAUTI National Healthcare Safety
CMS Inpatient Quality Reporting (IQR) Program Measures for the Payment Update Measures Required to Meet IQR Program APU Requirements Healthcare-Associated Infection on CAUTI National Healthcare Safety
ICD-10 Physician Education. Palliative Care SIP
 ICD-10 Physician Education Palliative Care SIP 1 Training Objectives ICD-9 to ICD-10 Comparison Documentation Tips Additional Educational Opportunities Questions 2 ICD-9 to ICD-10 Comparison Code Structure
ICD-10 Physician Education Palliative Care SIP 1 Training Objectives ICD-9 to ICD-10 Comparison Documentation Tips Additional Educational Opportunities Questions 2 ICD-9 to ICD-10 Comparison Code Structure
Clinical Documentation Improvement: Reporting Opportunities
 Clinical Documentation Improvement: Reporting Opportunities Karee Burns, RN, BSN Midas+ Solutions Consultant Waheed Baqai, MPH, CPH Director Clinical Decision Support Loma Linda University Medical Center
Clinical Documentation Improvement: Reporting Opportunities Karee Burns, RN, BSN Midas+ Solutions Consultant Waheed Baqai, MPH, CPH Director Clinical Decision Support Loma Linda University Medical Center
Leveraging the Value of Midas+ DataVision Toolpacks. Brenda Pettyjohn RN, CPHQ Midas+ DataVision Clinical Consultant
 Leveraging the Value of Midas+ DataVision Toolpacks Brenda Pettyjohn RN, CPHQ Midas+ DataVision Clinical Consultant Objectives Identify at least 1-2 uses for each of the Toolpacks Identify populations
Leveraging the Value of Midas+ DataVision Toolpacks Brenda Pettyjohn RN, CPHQ Midas+ DataVision Clinical Consultant Objectives Identify at least 1-2 uses for each of the Toolpacks Identify populations
Short-term Acute Care Program for Evaluating Payment Patterns Electronic Report. User s Guide Twenty-second Edition. Prepared by
 Short-term Acute Care Program for Evaluating Payment Patterns Electronic Report User s Guide Twenty-second Edition Prepared by 1 Short-term Acute Care Program for Evaluating Payment Patterns Electronic
Short-term Acute Care Program for Evaluating Payment Patterns Electronic Report User s Guide Twenty-second Edition Prepared by 1 Short-term Acute Care Program for Evaluating Payment Patterns Electronic
Arkansas Health Care Payment Improvement Initiative Percutaneous Coronary Intervention Algorithm Summary
 Arkansas Health Care Payment Improvement Initiative Percutaneous Coronary Intervention Algorithm Summary Percutaneous Coronary Intervention (PCI) Algorithm Summary v1.0 Page 2 of 8 Triggers PAP assignment
Arkansas Health Care Payment Improvement Initiative Percutaneous Coronary Intervention Algorithm Summary Percutaneous Coronary Intervention (PCI) Algorithm Summary v1.0 Page 2 of 8 Triggers PAP assignment
TENNCARE Bundled Payment Initiative: Description of Bundle Risk Adjustment for Wave 4 Episodes
 TENNCARE Bundled Payment Initiative: Description of Bundle Risk Adjustment for Wave 4 Episodes Attention deficit hyperactivity disorder (ADHD); Opposition defiance disorder (ODD); Coronary artery bypass
TENNCARE Bundled Payment Initiative: Description of Bundle Risk Adjustment for Wave 4 Episodes Attention deficit hyperactivity disorder (ADHD); Opposition defiance disorder (ODD); Coronary artery bypass
Coronary Artery Bypass Graft (CABG) Surgery 2002 Data. Technical Notes
 Surgery 2002 Data. Technical Notes") Coronary Artery Bypass Graft (CABG) Surgery 2002 Data Technical Notes The Pennsylvania Health Care Cost Containment Council February 2004 TABLE OF CONTENTS Outcome Measures Reported... 1 Study Population...
Coronary Artery Bypass Graft (CABG) Surgery 2002 Data Technical Notes The Pennsylvania Health Care Cost Containment Council February 2004 TABLE OF CONTENTS Outcome Measures Reported... 1 Study Population...
Medicare Hospital Acquired Conditions Reduction Program Andrew B. Wheeler Vice President of Federal Finance
 Medicare Hospital Acquired Conditions Reduction Program - 201 Andrew B. Wheeler Vice President of Federal Finance Value-Based Hospital Acquired Purchasing Conditions FFY 2018 FFY -2016 2020 AHRQ Claims
Medicare Hospital Acquired Conditions Reduction Program - 201 Andrew B. Wheeler Vice President of Federal Finance Value-Based Hospital Acquired Purchasing Conditions FFY 2018 FFY -2016 2020 AHRQ Claims
Reliability and Validity of PPCs in the MHAC Program
 Reliability and Validity of PPCs in the MHAC Program Presentation at the November Work Group Meeting November 20 th, 2015 Fei Xing Huihua Lu Haixia Xu Emily McPherson Frank Yoon Eric Schone Overview of
Reliability and Validity of PPCs in the MHAC Program Presentation at the November Work Group Meeting November 20 th, 2015 Fei Xing Huihua Lu Haixia Xu Emily McPherson Frank Yoon Eric Schone Overview of
TOTAL HIP AND KNEE REPLACEMENTS. FISCAL YEAR 2002 DATA July 1, 2001 through June 30, 2002 TECHNICAL NOTES
 TOTAL HIP AND KNEE REPLACEMENTS FISCAL YEAR 2002 DATA July 1, 2001 through June 30, 2002 TECHNICAL NOTES The Pennsylvania Health Care Cost Containment Council April 2005 Preface This document serves as
TOTAL HIP AND KNEE REPLACEMENTS FISCAL YEAR 2002 DATA July 1, 2001 through June 30, 2002 TECHNICAL NOTES The Pennsylvania Health Care Cost Containment Council April 2005 Preface This document serves as
Optimal Vascular Care Specifications 2013 (01/01/2012 to 12/31/2012 Dates of Services) Revised 08/10/2012
 Revised 08/10/2012") Summary of Changes Date of birth clarification Added language to clarify date of birth range. Please note the changes in the denominator section. Description Methodology Rationale Measurement Period Denominator
Summary of Changes Date of birth clarification Added language to clarify date of birth range. Please note the changes in the denominator section. Description Methodology Rationale Measurement Period Denominator
Short-term Acute Care Program for Evaluating Payment Patterns Electronic Report. User s Guide Twenty-third Edition. Prepared by
 Short-term Acute Care Program for Evaluating Payment Patterns Electronic Report User s Guide Twenty-third Edition Prepared by 1 Short-term Acute Care Program for Evaluating Payment Patterns Electronic
Short-term Acute Care Program for Evaluating Payment Patterns Electronic Report User s Guide Twenty-third Edition Prepared by 1 Short-term Acute Care Program for Evaluating Payment Patterns Electronic
The paper provides an update for the Trust Board on hospital mortality and presents the updated Trust Mortality Action Plan.
 ENC No 13 Meeting Trust Board Date 28 th November 2013 Title of Paper Lead Director Author Hospital Mortality Update Mr Amir Khan, Medical Director Mr Amir Khan, Medical Director PURPOSE OF THE PAPER The
ENC No 13 Meeting Trust Board Date 28 th November 2013 Title of Paper Lead Director Author Hospital Mortality Update Mr Amir Khan, Medical Director Mr Amir Khan, Medical Director PURPOSE OF THE PAPER The
SCORES FOR 4 TH QUARTER, RD QUARTER, 2014
 SCORES FOR 4 TH QUARTER, 2013 3 RD QUARTER, 2014 PATIENT SATISFACTION SCORES (HCAHPS): 4 STARS OUT OF 5 (ONLY 4 AREA ACUTE CARE HOSPITALS RECEIVED A 4-STAR RATING. NONE ACHIEVED 5-STARS). STRUCTURAL MEASURES:
SCORES FOR 4 TH QUARTER, 2013 3 RD QUARTER, 2014 PATIENT SATISFACTION SCORES (HCAHPS): 4 STARS OUT OF 5 (ONLY 4 AREA ACUTE CARE HOSPITALS RECEIVED A 4-STAR RATING. NONE ACHIEVED 5-STARS). STRUCTURAL MEASURES:
Statit pimd Client Panel. Guy March, Product Lead, Midas+ Statit
 Statit pimd Client Panel Guy March, Product Lead, Midas+ Statit Statit pimd/ppr Statit Software Started ~25 years ago Currently serving 650 hospitals Guy March Working with Statit QC products for over
Statit pimd Client Panel Guy March, Product Lead, Midas+ Statit Statit pimd/ppr Statit Software Started ~25 years ago Currently serving 650 hospitals Guy March Working with Statit QC products for over
Prescribe appropriate immunizations for. Prescribe childhood immunization as per. Prescribe influenza vaccinations in high-risk
 Supplemental Digital Appendix 1 46 Health Care Problems and the Corresponding 59 Practice Indicators Expected of All Physicians Entering or in Practice Infectious and parasitic diseases Avoidable complications/death
Supplemental Digital Appendix 1 46 Health Care Problems and the Corresponding 59 Practice Indicators Expected of All Physicians Entering or in Practice Infectious and parasitic diseases Avoidable complications/death
A Comprehensive Scorecard for Board and Staff Larry Hegland, MD
 A Comprehensive Scorecard for Board and Staff Larry Hegland, MD System Medical Director for Recovery Audit and Appeal Services Chief Medical Officer for Ministry Saint Clare s Hospital and the Diagnostic
A Comprehensive Scorecard for Board and Staff Larry Hegland, MD System Medical Director for Recovery Audit and Appeal Services Chief Medical Officer for Ministry Saint Clare s Hospital and the Diagnostic
Mandatory Elements of Healthcare Reform Walter Coleman. healthcare consulting
 Mandatory Elements of Healthcare Reform Walter Coleman 1 Agenda ACA Mandatory Elements of Reform Value Based Purchasing Readmission Reduction Program Hospital Acquired Conditions Best practices to analyze
Mandatory Elements of Healthcare Reform Walter Coleman 1 Agenda ACA Mandatory Elements of Reform Value Based Purchasing Readmission Reduction Program Hospital Acquired Conditions Best practices to analyze
Sample page. DRG Desk Reference. The ultimate resource for improving MS-DRG assignment practices DESK REFERENCE
 DESK REFERENCE 2018 DRG Desk Reference The ultimate resource for improving MS-DRG assignment practices POWER UP YOUR CODING with Optum360, your trusted coding partner for 32 years. Visit optum360coding.com.
DESK REFERENCE 2018 DRG Desk Reference The ultimate resource for improving MS-DRG assignment practices POWER UP YOUR CODING with Optum360, your trusted coding partner for 32 years. Visit optum360coding.com.
ERRATA. To: Recipients of TR-213-CMS, RAND Corporation Publications Department
 ERRATA To: Recipients of TR-213-CMS, 2005 From: RAND Corporation Publications Department Date: July 2006 (Please note that this incorporates an Errata from December 2005) Re: Corrected page (p. iii); updated
ERRATA To: Recipients of TR-213-CMS, 2005 From: RAND Corporation Publications Department Date: July 2006 (Please note that this incorporates an Errata from December 2005) Re: Corrected page (p. iii); updated
National Medicare RAC Summit March 5, 2009 Provider Lessons From Demonstration States
 National Medicare RAC Summit March 5, 2009 Provider Lessons From Demonstration States Lynn H. Grieves Chief Compliance Officer MemorialCare Medical Centers lgrieves@memorialcare.org MemorialCare Health
National Medicare RAC Summit March 5, 2009 Provider Lessons From Demonstration States Lynn H. Grieves Chief Compliance Officer MemorialCare Medical Centers lgrieves@memorialcare.org MemorialCare Health
APC/DRG Code APC/DRG Name # of Discharges Average of Charges 5341 Abdominal/Peritoneal/Biliary and Related Procedures 71 $9, ACUTE ADJUSTMENT
 5341 Abdominal/Peritoneal/Biliary and Related Procedures 71 $9,950 880 ACUTE ADJUSTMENT REACTION & PSYCHOSOCIAL DYSFUNCTION MS 3 $8,161 62 ACUTE ISCHEMIC STROKE W USE OF THROMBOLYTIC AGENT W CC MS 10 $30,145
5341 Abdominal/Peritoneal/Biliary and Related Procedures 71 $9,950 880 ACUTE ADJUSTMENT REACTION & PSYCHOSOCIAL DYSFUNCTION MS 3 $8,161 62 ACUTE ISCHEMIC STROKE W USE OF THROMBOLYTIC AGENT W CC MS 10 $30,145
BPCI Advanced Episode Selection
 BPCI Advanced Episode Selection Analytic Framework and Strategies from Northwestern Medicine Presented June 7, 2018 to: Insert relevant presenter information Calibri 16pt Presented Jessica Walradt on:
BPCI Advanced Episode Selection Analytic Framework and Strategies from Northwestern Medicine Presented June 7, 2018 to: Insert relevant presenter information Calibri 16pt Presented Jessica Walradt on:
Appendix G Explanation/Clarification Summary
 Appendix G Explanation/Clarification Summary Summary of Changes for Recommendations Alignment of measures with VBP by fiscal year Measures and service dates were adjusted to be consistent with the FY2016
Appendix G Explanation/Clarification Summary Summary of Changes for Recommendations Alignment of measures with VBP by fiscal year Measures and service dates were adjusted to be consistent with the FY2016
4. Which survey program does your facility use to get your program designated by the state?
 TRAUMA SURVEY Please complete one survey for each TCD designation you have in your facility. There would be a maximum of three surveys completed if your facility was designated as a trauma, stroke and
TRAUMA SURVEY Please complete one survey for each TCD designation you have in your facility. There would be a maximum of three surveys completed if your facility was designated as a trauma, stroke and
Update on the CoreValve Experience
 TCT Asia Pacific April 22-24, 2009 Update on the CoreValve Experience Eberhard Grube HELIOS Klinikum, Germany Instituto Dante Pazzanese de Cardiología, São Paulo, Brazil Stanford University, Palo Alto,
TCT Asia Pacific April 22-24, 2009 Update on the CoreValve Experience Eberhard Grube HELIOS Klinikum, Germany Instituto Dante Pazzanese de Cardiología, São Paulo, Brazil Stanford University, Palo Alto,
Present-on-Admission (POA) Coding
 Coding") 1 Present-on-Admission (POA) Coding Michael Pine, MD, MBA Michael Pine and Associates, Inc 2 POA and Coding Guidelines (1) Unless otherwise specified, a POA modifier must be assigned to each principal
1 Present-on-Admission (POA) Coding Michael Pine, MD, MBA Michael Pine and Associates, Inc 2 POA and Coding Guidelines (1) Unless otherwise specified, a POA modifier must be assigned to each principal
INPATIENT REIMBURSEMENT PROSPECTUS
 2018 CARDIOVASCULAR SERVICE LINE INPATIENT REIMBURSEMENT PROSPECTUS Increasing financial risk to U.S. health care providers, including physicians and hospitals, has been centered on outcomes-based modifiers
2018 CARDIOVASCULAR SERVICE LINE INPATIENT REIMBURSEMENT PROSPECTUS Increasing financial risk to U.S. health care providers, including physicians and hospitals, has been centered on outcomes-based modifiers
Proposed Expansion of the Patient Safety Indicator Set Patrick S. Romano, MD MPH UC Davis/USA
 Proposed Expansion of the Patient Safety Indicator Set Patrick S. Romano, MD MPH UC Davis/USA OECD Health Care Quality Indicators Patient Safety Subgroup 9 May 2012 AHRQ PSIs endorsed by OECD (after review
Proposed Expansion of the Patient Safety Indicator Set Patrick S. Romano, MD MPH UC Davis/USA OECD Health Care Quality Indicators Patient Safety Subgroup 9 May 2012 AHRQ PSIs endorsed by OECD (after review
A National Cardiogenic Shock Initiative (CSI):
:") A National Cardiogenic Shock Initiative (CSI): Insights from the Impella Quality (IQ) Program, cvad Registry and the Detroit CSI Experience William O Neill, MD, FACC Medical Director Structural Heart Disease
A National Cardiogenic Shock Initiative (CSI): Insights from the Impella Quality (IQ) Program, cvad Registry and the Detroit CSI Experience William O Neill, MD, FACC Medical Director Structural Heart Disease
The American Experience
 The American Experience Jay F. Piccirillo, MD, FACS, CPI Department of Otolaryngology Washington University School of Medicine St. Louis, Missouri, USA Acknowledgement Dorina Kallogjeri, MD, MPH- Senior
The American Experience Jay F. Piccirillo, MD, FACS, CPI Department of Otolaryngology Washington University School of Medicine St. Louis, Missouri, USA Acknowledgement Dorina Kallogjeri, MD, MPH- Senior
Author: K. Ketchum Date: July 2015
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Quality ID #358: Patient-Centered Surgical Risk Assessment and Communication National Quality Strategy Domain: Person and Caregiver-Centered Experience and Outcomes 2018 OPTIONS FOR INDIVIDUAL MEASURES:
Quality ID #358: Patient-Centered Surgical Risk Assessment and Communication National Quality Strategy Domain: Person and Caregiver-Centered Experience and Outcomes 2018 OPTIONS FOR INDIVIDUAL MEASURES:
Commercial Bundling. National Bundled Payment Summit Integrated Healthcare Association. George Washington University, Washington, DC.
 Commercial Bundling National Bundled Payment Summit Integrated Healthcare Association George Washington University, Washington, DC June 12, 2012 Copyright 2012. This presentation as a whole and all of
Commercial Bundling National Bundled Payment Summit Integrated Healthcare Association George Washington University, Washington, DC June 12, 2012 Copyright 2012. This presentation as a whole and all of
Yes No Unknown. Major Infection Information
 Rehospitalization Intervention Check any that occurred during this hospitalization. Pacemaker without ICD ICD Atrial arrhythmia ablation Ventricular arrhythmia ablation Cardioversion CABG (coronary artery
Rehospitalization Intervention Check any that occurred during this hospitalization. Pacemaker without ICD ICD Atrial arrhythmia ablation Ventricular arrhythmia ablation Cardioversion CABG (coronary artery
Catheter-based mitral valve repair MitraClip System
 Percutaneous Mitral Valve Repair: Results of the EVEREST II Trial William A. Gray MD Director of Endovascular Services Associate Professor of Clinical Medicine Columbia University Medical Center The Cardiovascular
Percutaneous Mitral Valve Repair: Results of the EVEREST II Trial William A. Gray MD Director of Endovascular Services Associate Professor of Clinical Medicine Columbia University Medical Center The Cardiovascular
FY2014 Final Hospital Inpatient Rule Summary
 FY2014 Final Hospital Inpatient Rule Summary Reimbursement Update Cardiac Rhythm Management (CRM) Electrophysiology (EP) Interventional Cardiology (IC) Peripheral Intervention (PI) On August 2, 2013, the
FY2014 Final Hospital Inpatient Rule Summary Reimbursement Update Cardiac Rhythm Management (CRM) Electrophysiology (EP) Interventional Cardiology (IC) Peripheral Intervention (PI) On August 2, 2013, the
Episodes of Care Risk Adjustment
 Episodes of Care Risk Adjustment Episode Types Wave 1 Asthma Acute Exacerbation Perinatal Total Joint Replacement Wave 2 Acute Percutaneous Coronary Intervention COPD Acute Exacerbation Non-acute Percutaneous
Episodes of Care Risk Adjustment Episode Types Wave 1 Asthma Acute Exacerbation Perinatal Total Joint Replacement Wave 2 Acute Percutaneous Coronary Intervention COPD Acute Exacerbation Non-acute Percutaneous
Ischemic Heart Disease Interventional Treatment
 Ischemic Heart Disease Interventional Treatment Cardiac Catheterization Laboratory Procedures (N = 89) is a regional and national referral center for percutaneous coronary intervention (PCI). A total of
Ischemic Heart Disease Interventional Treatment Cardiac Catheterization Laboratory Procedures (N = 89) is a regional and national referral center for percutaneous coronary intervention (PCI). A total of
THE NATIONAL QUALITY FORUM
 THE NATIONAL QUALITY FORUM National Voluntary Consensus Standards for Patient Outcomes Table of Measures Submitted-Phase 1 As of March 5, 2010 Note: This information is for personal and noncommercial use
THE NATIONAL QUALITY FORUM National Voluntary Consensus Standards for Patient Outcomes Table of Measures Submitted-Phase 1 As of March 5, 2010 Note: This information is for personal and noncommercial use
Supplementary Online Content
 Supplementary Online Content Khera R, Dharmarajan K, Wang Y, et al. Association of the hospital readmissions reduction program with mortality during and after hospitalization for acute myocardial infarction,
Supplementary Online Content Khera R, Dharmarajan K, Wang Y, et al. Association of the hospital readmissions reduction program with mortality during and after hospitalization for acute myocardial infarction,
The Centers for Medicare & Medicaid Services (CMS) Acute Care Hospital Fiscal Year (FY) 2018 Quality Improvement Program Measures
 Acute Care Hospital Fiscal Year (FY) 2018 Quality Improvement Program Measures") ID M easure Name NQF # H os pital M easurement Period H os pital H os pital Value-Bas ed Purchas ing M easurement Period H os pital H ealth Record (EH R) Incentive M easurement Period H os pital H os pital-
ID M easure Name NQF # H os pital M easurement Period H os pital H os pital Value-Bas ed Purchas ing M easurement Period H os pital H ealth Record (EH R) Incentive M easurement Period H os pital H os pital-
Common Codes for ICD-10
 Common Codes for ICD-10 Specialty: Cardiology *Always utilize more specific codes first. ABNORMALITIES OF HEART RHYTHM ICD-9-CM Codes: 427.81, 427.89, 785.0, 785.1, 785.3 R00.0 Tachycardia, unspecified
Common Codes for ICD-10 Specialty: Cardiology *Always utilize more specific codes first. ABNORMALITIES OF HEART RHYTHM ICD-9-CM Codes: 427.81, 427.89, 785.0, 785.1, 785.3 R00.0 Tachycardia, unspecified
Quality Measures MIPS CV Specific
 Quality Measures MIPS CV Specific MEASURE NAME Atrial Fibrillation and Atrial Flutter: Chronic Anticoagulation Therapy CAHPS for MIPS Clinician/Group Survey Cardiac Rehabilitation Patient Referral from
Quality Measures MIPS CV Specific MEASURE NAME Atrial Fibrillation and Atrial Flutter: Chronic Anticoagulation Therapy CAHPS for MIPS Clinician/Group Survey Cardiac Rehabilitation Patient Referral from
WATCHMAN. For questions regarding WATCHMAN reimbursement, please contact:
 WATCHMAN IMPORTANCE OF DOCUMENTATION & THE IMPACT ON MS- DRG ASSIGNMENT This guide stresses the importance of documentation in capturing the appropriate acuity level for patients considered WATCHMAN candidates.
WATCHMAN IMPORTANCE OF DOCUMENTATION & THE IMPACT ON MS- DRG ASSIGNMENT This guide stresses the importance of documentation in capturing the appropriate acuity level for patients considered WATCHMAN candidates.
Analysis of Variation in Medicare Margins for Inpatient Rehabilitation Facilities (IRFs)
") Analysis of Variation in Medicare s for Inpatient Rehabilitation Facilities (IRFs) Dobson DaVanzo & Associates, LLC Vienna, VA 703.260.1760 www.dobsondavanzo.com Analysis of Variation in Medicare s for
Analysis of Variation in Medicare s for Inpatient Rehabilitation Facilities (IRFs) Dobson DaVanzo & Associates, LLC Vienna, VA 703.260.1760 www.dobsondavanzo.com Analysis of Variation in Medicare s for
Average Gross Charges ACUTE MYOCARDIAL INFARCTION, DISCHARGED ALIVE W CC ,254 ACUTE MYOCARDIAL INFARCTION, DISCHARGED ALIVE W MCC - 280
 ACUTE MYOCARDIAL INFARCTION, DISCHARGED ALIVE W CC - 281 15,254 ACUTE MYOCARDIAL INFARCTION, DISCHARGED ALIVE W MCC - 280 24,827 ACUTE MYOCARDIAL INFARCTION, DISCHARGED ALIVE W/O CC/MCC - 282 11,575 AFTERCARE,
ACUTE MYOCARDIAL INFARCTION, DISCHARGED ALIVE W CC - 281 15,254 ACUTE MYOCARDIAL INFARCTION, DISCHARGED ALIVE W MCC - 280 24,827 ACUTE MYOCARDIAL INFARCTION, DISCHARGED ALIVE W/O CC/MCC - 282 11,575 AFTERCARE,
patients actual drug exposure for every single-day of contribution to monthly cohorts, either before or
 SUPPLEMENTAL MATERIAL Methods Monthly cohorts and exposure Exposure to generic or brand-name drugs were captured at an individual level, reflecting each patients actual drug exposure for every single-day
SUPPLEMENTAL MATERIAL Methods Monthly cohorts and exposure Exposure to generic or brand-name drugs were captured at an individual level, reflecting each patients actual drug exposure for every single-day
CMS Measures - Fiscal Year 2019
 ID Me asure Name NQF # Value- (VBP) - (HACRP) (HRRP) ID Me asure Name NQF # Value- (VBP) - (HACRP) (HRRP) CMS s - Fiscal Year 2019 ID Name NQF # The Centers for Medicare & Medicaid Services (CMS) Improvement
ID Me asure Name NQF # Value- (VBP) - (HACRP) (HRRP) ID Me asure Name NQF # Value- (VBP) - (HACRP) (HRRP) CMS s - Fiscal Year 2019 ID Name NQF # The Centers for Medicare & Medicaid Services (CMS) Improvement