Commercial Bundling. National Bundled Payment Summit Integrated Healthcare Association. George Washington University, Washington, DC.
|
|
|
- Miranda Freeman
- 6 years ago
- Views:
Transcription




1 Commercial Bundling National Bundled Payment Summit Integrated Healthcare Association George Washington University, Washington, DC June 12, 2012 Copyright This presentation as a whole and all of its individual parts are the exclusive property of The Camden Group.

2 Agenda National Trends Critical Success Factors Partnership Strategies Metrics Contract Considerations Structural Considerations Common Mistakes Questions and Discussion

3 Nearly One-third of the Nation Now Testing Bundled Payment Bundling for Obstetrics Participating in Prometheus Pilot Reimbursing for Baskets of Care Participating in Prometheus Pilot Exploring Cardiac Bundling Orthopedic Bundling BCBS² Developing Orthopedic Bundling Bundling for CABG 1 Blue Cross Blue Shield of MA Global Bundled Payment Bundling Joint Replacements, Procedures with Defined Outcomes Denver, CO - Cardiac Albuquerque, NM - ACE Orthopedic 1 Coronary Artery Bypass Graft 2 Blue Cross Blue Shield Source: Advisory Board Oklahoma City, OK - ACE Cardiac Tulsa, OK ACE Cardiac and Orthopedic Houston, TX ACE Orthopedic and Cardiac Ambulatory Oncology Bundling San Antonio, TX ACE orthopedic and cardiac Bundling Total Joint Replacement Blue Cross and Blue Shield of FL Prostate Surgery Bundled Payment Participating in Prometheus Pilot Bundling Total Knee Replacement Bundling for Cardiac Surgery Oncology ACO Bundling Bundling for prostate surgery 6/12/2012 ι 3




4 Drivers of Readmissions and Variation in Care Care Delivery/Management Central line infections Limited/No patient education pre-discharge Incomplete/ Ineffective discharge process Limited/Ineffective communication in patient hand-off to post-acute provider Post-discharge follow-up with PCP lags or unscheduled Patient Characteristics Culture, literacy, language barriers Socioeconomic status Co-morbidities Number of medications prescribed and adherence Access to social support Psychological status 6/12/2012 ι 4
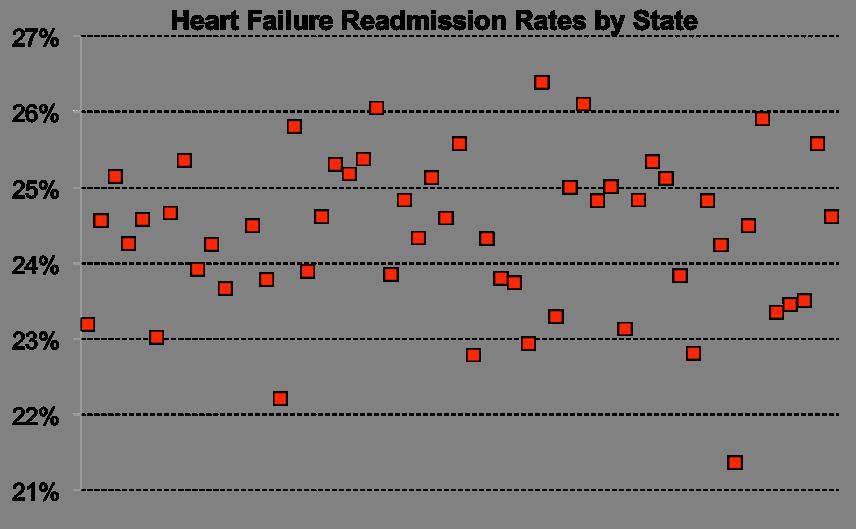
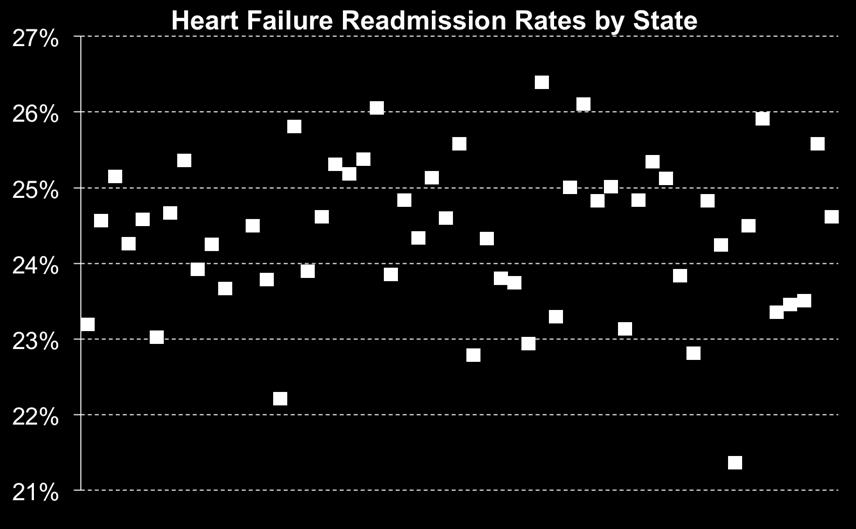


5 Significant Variation in HF Readmissions by State 6/12/2012 ι 5




6 Heart Failure Readmission Rates Are Not Improving Source: Dartmouth Atlas 10/20/2011 6/12/2012 ι 6

7 Pending Penalties for High Readmission Rates Under Hospital Readmission Reduction Program, Medicare will penalize hospitals for higher than expected rates of readmissions within 30 days of discharge for patients with: AMI CHF Pneumonia There will be a payment reduction for each Medicare readmission October 2012 October 2013 October 2014 One percent of Medicare billings penalty begins Two percent of Medicare billings penalty begins Three percent of Medicare billings penalty begins Commercial payers are expected to follow CMS lead 6/12/2012 ι 7
8 Agenda National Trends Critical Success Factors Partnership Strategies Metrics Contract Considerations Structural Considerations Common Mistakes Questions and Discussion
9 Cardiac Historical Volume Hospital A CMMI Bundled Payments for Care Improvement Initiative Sample Model 4 - Inpatient Stay Only Historical Cases by Proposed Episode of Care for Cardiac Services CY 2010 Medicare FFS Commercial Cardiac Services Cases % of Total Cases % of Total Valves (MS-DRGs ) % % Defibrillators (MS-DRGs ) % % CABGs (MS-DRGs ) % % Pacemakers (MS-DRGs ) % % Stents (MS-DRGs ) % % Total Cases 1, % % Source: Hospital A. Black border denotes highest number of cases for each payer category. Payer Mix Pacer Revs 0.0% Medicare FFS Volume Defibs 9.0% Valves 10.0% Commercial 41% Medicare FFS 59% CABGs 10.5% Stents 44.9% Pacers 25.5% 6/12/2012 ι 9
10 Cardiac Historical ALOS Hospital A CMMI Bundled Payments for Care Improvement Initiative Sample Model 4 - Inpatient Stay Only Historical Average Length-of-Stay Compared to 2009 Premier 90th Percentile by Proposed Episode of Care for Cardiac Services CY 2010 Medicare FFS Commercial Cardiac Services Historical ALOS Premier 90th %tile Variance Historical ALOS Premier 90th %tile Variance Valves (MS-DRGs ) Defibrillators (MS-DRGs ) CABGs (MS-DRGs ) Pacemakers (MS-DRGs ) Stents (MS-DRGs ) Total ALOS Source: Hospital A and Centers for Medicare and Medicaid Services. Black border denotes potential opportunity for reducing average length-of-stay Medicare FFS Historical 90th %tile Valves Defibs CABGs Pacers Stents Commercial Historical 90th %tile Valves Defibs CABGs Pacers Stents 6/12/2012 ι 10
11 Cardiac Historical Financials Hospital A CMMI Bundled Payments for Care Improvement Initiative Sample Model 4 - Inpatient Stay Only Historical Financial Performance by Proposed Episode of Care for Cardiac Services CY 2010 Medicare FFS Commercial Cardiac Services Contribution Margin (CM) CM per Case Net Profit/ (Loss) Contribution Margin (CM) CM per Case Net Profit/ (Loss) Valves (MS-DRGs ) $1,345,588 $13,456 ($966,813) $2,438,053 $48,761 $1,608,121 Defibrillators (MS-DRGs ) 578,080 6,423 ($327,480) 3,331,806 75,723 $2,972,400 CABGs (MS-DRGs ) 1,047,754 9,979 ($909,733) 4,996,487 40,294 $2,756,267 Pacemakers (MS-DRGs ) 231, ($1,692,888) 1,558,482 47,227 $1,306,311 Stents (MS-DRGs ) 1,370,393 3,052 ($1,994,579) 19,272,101 42,171 $16,589,181 Total $4,573,046 $3,815 ($5,891,493) $31,596,929 $37,190 $25,232,281 Source: Hospital A, commercial data needs to be updated Black border denotes highest contribution margin per case. $80,000 CM per Case $70,000 $60,000 $50,000 $40,000 $30,000 $20,000 $10,000 $0 Valves Defibs CABGs Pacers Stents Medicare FFS Commercial 6/12/2012 ι 11
12 Cardiac Historical Market Hospital A CMMI Bundled Payments for Care Improvement Initiative Sample Model 4 - Inpatient Stay Only Historical Market Discharges in Service Area by Proposed Episode of Care for Cardiac Services CY 2010 Cardiac Services Hospital A % of Total Hospital B % of Total Hospital C Medicare FFS % of Total Hospital D % of Total All Other % of Total Total % of Total Valves (MS-DRGs ) % % % 5 2.0% % % Defibrillators (MS-DRGs ) % 5 2.9% % % % % CABGs (MS-DRGs ) % % % % % % Pacemakers (MS-DRGs ) % % % % % % Stents (MS-DRGs ) % % % % % 1, % Total 1, % % % % % 2, % Cardiac Services Hospital A % of Total Commercial (Blue Cross, Blue Cross HMO, PPO, HMO, Fee for Service) % of % of % of % of Hospital B Total Hospital C Total Hospital D Total All Other Total Total % of Total Valves (MS-DRGs ) % 4 2.2% % % % % Defibrillators (MS-DRGs ) % 5 5.1% 4 3.8% 4 3.8% % % CABGs (MS-DRGs ) % % % % % % Pacemakers (MS-DRGs ) % 1 1.3% 5 5.1% 5 5.1% % % Stents (MS-DRGs ) % % % % % 1, % Total % % % % % 1, % sharepoint.thecamdengroup.com/ planning/ Bundled_Payment / Bundled_Payment _for_care_improvement _Initiative/Presentations/ Scrubbed Files/ [ CM M I_Business_Case_M odel_4_updated_ _sent _to_client.xlsx]hist _M arket _Cardiac Source: Hospital A, market data may not match internal data provided by the Hospital Black border denotes the organization with the highest number of cases in each episode of care category Medicare FFS Valves Defibs CABGs Pacers Stents 305 Hospital A Hospital B Hospital C Hospital D All Other Commercial Valves Defibs CABGs Pacers Stents Hospital A Hospital B Hospital C Hospital D All Other 270 6/12/2012 ι 12

13 Agenda National Trends Critical Success Factors Partnership Strategies Metrics Contract Considerations Structural Considerations Common Mistakes Questions and Discussion
14 How Do You plan to Leverage EOC risk? More Risk for More Volume? Commercial Health Plans are just now starting to expand into EOC contracting Are there IPAs or other risk managing organizations you could partner with? Once you can prove you are able to operate an EOC arrangement, which Commercial plans in your area are ready to use EOC payments? Do you know this now? When? What are you planning to ask of the Health Plan in exchange for undertaking more risk? Are you able to undertake greater volumes? i.e., Can you advocate to narrow the network if you have enough access points in your system of care? 6/12/2012 ι 14
15 Agenda National Trends Critical Success Factors Partnership Strategies Metrics Contract Considerations Structural Considerations Common Mistakes Questions and Discussion
16 Early Insights into High-value Measures Expanding episode of care to include readmission and post-acute Readmission compared to market PAC cost per case compared to market Predictability on cost and quality Patient experience Cost and Quality profile compared to market 6/12/2012 ι 16


17 30-Day Readmission Rate is the Burning Platform 6/12/2012 ι 17
18 Top Readmissions for MS-DRG 227 Defibrillator Hospital A Sample Distribution of Top 25 DRGs for Readmission within 30 Days of Discharge for Anchor DRG 227 MS-DRG Description: Cardiac defibrillator implant w/o cardiac cath w/o MCC DRG of Readmission Readmissions per 100 Anchor Cases within 30 Days of Anchor Discharge % of Total Readmissions within 30 Days of Anchor Discharge Heart failure & shock w CC % Heart failure & shock w/o CC/MCC % Heart failure & shock w MCC % Cardiac pacemaker revision except device replacement w CC % Other circulatory system diagnoses w CC % Cardiac pacemaker revision except device replacement w/o CC/MCC % Cardiac arrhythmia & conduction disorders w/o CC/MCC % Other circulatory system diagnoses w MCC % Renal failure w MCC % Respiratory system diagnosis w ventilator support <96 hours % Perc cardiovasc proc w/o coronary artery stent w/o MCC % Acute myocardial infarction, discharged alive w MCC % Circulatory disorders except AMI, w card cath w MCC % Peripheral vascular disorders w CC % Cardiac arrhythmia & conduction disorders w MCC % Syncope & collapse % Esophagitis, gastroent & misc digest disorders w/o MCC % Cellulitis w/o MCC % Diabetes w CC % Other O.R. procedures for injuries w CC % Craniotomy & endovascular intracranial procedures w CC % Extracranial procedures w/o CC/MCC % Transient ischemia % Other ear, nose, mouth & throat O.R. procedures w CC/MCC % Epistaxis w/o MCC % Source: Milliman 6/12/2012 ι 18
19 Top Readmissions for MS-DRG 244 Pacemaker Hospital A Sample Distribution of Top 25 DRGs for Readmission within 30 Days of Discharge for Anchor DRG 244 MS-DRG Description: Permanent cardiac pacemaker implant w/o CC/MCC DRG of Readmission Readmissions per 100 Anchor Cases within 30 Days of Anchor Discharge % of Total Readmissions within 30 Days of Anchor Discharge Cardiac arrhythmia & conduction disorders w/o CC/MCC % Heart failure & shock w/o CC/MCC % Syncope & collapse % Cardiac arrhythmia & conduction disorders w CC % Chest pain % Cardiac pacemaker revision except device replacement w CC % Heart failure & shock w MCC % Misc Disorders of Nutrition, Metabolism, Fluids/Electrolytes w/o MCC % Peripheral vascular disorders w CC % Atherosclerosis w/o MCC % Perc cardiovasc proc w drug-eluting stent w/o MCC % Cardiac pacemaker revision except device replacement w/o CC/MCC % Heart failure & shock w CC % Peripheral vascular disorders w/o CC/MCC % Other circulatory system diagnoses w/o CC/MCC % Transient ischemia % Seizures w/o MCC % Major cardiovasc procedures w MCC % Other vascular procedures w CC % Circulatory disorders except AMI, w card cath w/o MCC % Other circulatory system diagnoses w CC % Esophagitis, gastroent & misc digest disorders w/o MCC % Kidney & urinary tract infections w/o MCC % Other disorders of nervous system w CC % Pulmonary edema & respiratory failure % Source: Milliman 6/12/2012 ι 19
20 Top Readmissions for MS-DRG 470 Hip-Knee Hospital A Sample Distribution of Top 25 DRGs for Readmission within 30 Days of Discharge for Anchor DRG 470 MS-DRG Description: Major joint replacement or reattachment of lower extremity w/o MCC DRG of Readmission Readmissions per 100 Anchor Cases within 30 Days of Anchor Discharge % of Total Readmissions within 30 Days of Anchor Discharge Postoperative & post-traumatic infections w/o MCC % Pulmonary embolism w/o MCC % G.I. hemorrhage w CC % Major joint replacement or reattachment of lower extremity w/o MCC % Esophagitis, gastroent & misc digest disorders w/o MCC % Revision of hip or knee replacement w CC % Aftercare, musculoskeletal system & connective tissue w CC % Cellulitis w/o MCC % Misc Disorders of Nutrition, Metabolism, Fluids/Electrolytes w/o MCC % Aftercare, musculoskeletal system & connective tissue w/o CC/MCC % Septicemia or severe sepsis w/o MV 96+ hours w MCC % Revision of hip or knee replacement w/o CC/MCC % Red blood cell disorders w/o MCC % Complications of treatment w CC % Cardiac arrhythmia & conduction disorders w/o CC/MCC % Syncope & collapse % Psychoses % Simple pneumonia & pleurisy w CC % Peripheral vascular disorders w MCC % Hip & femur procedures except major joint w CC % Kidney & urinary tract infections w/o MCC % Heart failure & shock w CC % Revision of hip or knee replacement w MCC % Other digestive system diagnoses w CC % Knee procedures w pdx of infection w CC % Source: Milliman 6/12/2012 ι 20
21 CY 2009 (2 Quarters) Post-acute Utilization All MS-DRGs 25.0% 20.0% CY 2009 (2 Quarters) Average Post-acute Utilization 30-days Post-discharge 19.2% 22.1% 20.8% 23.4% 16.8% 15.0% 12.7% 10.0% 5.0% 3.1% 3.4% 0.0% 1.4% 1.1% 0.0% 0.1% Acute Inpatient Rehab Long Term Acute Care Skilled Nursing Facility Home Care Hospital HRC National 6/12/2012 ι 21


22 Benchmarks To Use In System Improvement 6/12/2012 ι 22


23 Healthcare Costs Are Part of the National Mandate 6/12/2012 ι 23

24 Agenda National Trends Critical Success Factors Partnership Strategies Metrics Contract Considerations Structural Considerations Common Mistakes Questions and Discussion
25 Key Contracting issues Exclusivity volume for value? Term...Multiple years??? Annual Opener to reset rates if EOC rates are chronically off or revert to a stop loss? Annual Inflator to Healthcare CPI? Shared data for transparency and to promote your better outcomes to beneficiaries Exclusions such as ED admits? Your employee health plan? 6/12/2012 ι 25
26 Agenda National Trends Critical Success Factors Partnership Strategies Metrics Contract Considerations Structural Considerations Common Mistakes Questions and Discussion
27 Considerations around Structure Hospital can hold contract directly, however.cannot do gainsharing directly due to OIG, Stark, et al. In this case, health plan would have to administer any gainsharing arrangements with Physicians. Alternatively, if a hospital based IPA (Independent Practice Association) is available, it can hold the payer contract and administer gainsharing. A mature service line structure is key to managing an EOC. Di-Ad leadership structures work well with a Medical Director and Service line Administrator are resources that have shown consistent success. A Service Line Counsel comprised of key clinicians empowered to make all key decisions around care redesign, resources through the EOC, clinical protocol design and use are minimally required to achieve success. 6/12/2012 ι 27
28 Agenda National Trends Critical Success Factors Partnership Strategies Metrics Contract Considerations Structural Considerations Common Mistakes Questions and Discussion
29 Common Errors Little to no organizational preparation that this is your direction.major work must be done to align those needed for an EOC arrangement Math is incomplete, poorly understood, or just wrong We can do this with what we have incremental investment is needed to successfully manage an EOC. Un-empowered Medical Leaders they MUST have the authority to decide who s in, who stays in, and who s out. No prior investment in a Lean process or technology good enough is not. You must be ready to commit to a process of continually finding waste and cost to pull out of an EOC. 6/12/2012 ι 29

30 Agenda National Trends Critical Success Factors Partnership Strategies Metrics Contract Considerations Inclusions and Exclusions Structural Considerations Common Mistakes Questions and Discussion
, MBA, RN Vice President The Camden Group DBaggot@TheCamdenGroup.")

31 Questions and Discussion Robert Minkin, MBA Senior Vice President The Camden Group Deirdre Baggot, Ph.D.(c), MBA, RN Vice President The Camden Group 6/12/2012 ι 31
SEPTICEMIA OR SEVERE SEPSIS W/O MV >96 HOURS W MCC 84, ,037.80
 Inpatient Visits by DRG Inpatient Discharges between 10/01/17 and 09/30/18 DRG DRG Description Average Charge Self-Pay Price VAGINAL DELIVERY W/O COMPLICATING 775 DIAGNOSES 14,680.67 5,578.66 795 NORMAL
Inpatient Visits by DRG Inpatient Discharges between 10/01/17 and 09/30/18 DRG DRG Description Average Charge Self-Pay Price VAGINAL DELIVERY W/O COMPLICATING 775 DIAGNOSES 14,680.67 5,578.66 795 NORMAL
Supplementary Online Content
 Supplementary Online Content Likosky DS, Zhou W, Malenka DJ, Borden WB, Nallamothu BK, Skinner JS. rowth in Medicare expenditures for patients with acute myocardial infarction: a comparison of 1998 through
Supplementary Online Content Likosky DS, Zhou W, Malenka DJ, Borden WB, Nallamothu BK, Skinner JS. rowth in Medicare expenditures for patients with acute myocardial infarction: a comparison of 1998 through
Objectives. Medicare Spending per Beneficiary: Analyzing MSPB Data to Identify Primary Drivers
 Medicare Spending per Beneficiary: Analyzing MSPB Data to Identify Primary Drivers August 22, 2017 Objectives Understand the basics of the hospital specific MSPB data files and reports Review the factors
Medicare Spending per Beneficiary: Analyzing MSPB Data to Identify Primary Drivers August 22, 2017 Objectives Understand the basics of the hospital specific MSPB data files and reports Review the factors
National Medicare RAC Summit March 5, 2009 Provider Lessons From Demonstration States
 National Medicare RAC Summit March 5, 2009 Provider Lessons From Demonstration States Lynn H. Grieves Chief Compliance Officer MemorialCare Medical Centers lgrieves@memorialcare.org MemorialCare Health
National Medicare RAC Summit March 5, 2009 Provider Lessons From Demonstration States Lynn H. Grieves Chief Compliance Officer MemorialCare Medical Centers lgrieves@memorialcare.org MemorialCare Health
DRG Code DRG Description FY18 Average Charge
 DRG Code DRG Description FY18 Average Charge 3 ECMO OR TRACH W MV 96+ HRS OR PDX EXC FACE, MOUTH & NECK W MAJ O $ 665,511 4 TRACH W MV 96+ HRS OR PDX EXC FACE, MOUTH & NECK W/O MAJ O.R. $ 422,497 37 EXTRACRANIAL
DRG Code DRG Description FY18 Average Charge 3 ECMO OR TRACH W MV 96+ HRS OR PDX EXC FACE, MOUTH & NECK W MAJ O $ 665,511 4 TRACH W MV 96+ HRS OR PDX EXC FACE, MOUTH & NECK W/O MAJ O.R. $ 422,497 37 EXTRACRANIAL
Bundle Payments. Healthcare Systems & Services Presenters: Larry Litman, Tyler Litman
 Bundle Payments Healthcare Systems & Services Presenters: Larry Litman, Tyler Litman To determine the average cost of the SNF portion of a bundle through the analysis of our client data-base. Our Objective:
Bundle Payments Healthcare Systems & Services Presenters: Larry Litman, Tyler Litman To determine the average cost of the SNF portion of a bundle through the analysis of our client data-base. Our Objective:
Medicare Payments. PHC4 Hospital Performance Report Oct 2015 through Sept 2016 Data 2015 Medicare Payments 1
 The following table includes information about payments made by for the 16 medical conditions/surgical procedures included in this Hospital Performance Report. This analysis is based on data from calendar
The following table includes information about payments made by for the 16 medical conditions/surgical procedures included in this Hospital Performance Report. This analysis is based on data from calendar
Medicare Payments. PHC4 Hospital Performance Report Oct 2016 through Sept 2017 Data FFY 2017 Medicare Payments 1
 The following table includes information about payments made by for the 16 medical conditions/surgical procedures included in this Hospital Performance Report. This analysis is based on data from federal
The following table includes information about payments made by for the 16 medical conditions/surgical procedures included in this Hospital Performance Report. This analysis is based on data from federal
Medicare and Medicaid Payments
 and Payments The following table includes information about payments made by and for the 17 medical conditions/surgical procedures included in this Hospital Performance Report. This analysis is based on
and Payments The following table includes information about payments made by and for the 17 medical conditions/surgical procedures included in this Hospital Performance Report. This analysis is based on
APC/DRG Code APC/DRG Name # of Discharges Average of Charges 5341 Abdominal/Peritoneal/Biliary and Related Procedures 71 $9, ACUTE ADJUSTMENT
 5341 Abdominal/Peritoneal/Biliary and Related Procedures 71 $9,950 880 ACUTE ADJUSTMENT REACTION & PSYCHOSOCIAL DYSFUNCTION MS 3 $8,161 62 ACUTE ISCHEMIC STROKE W USE OF THROMBOLYTIC AGENT W CC MS 10 $30,145
5341 Abdominal/Peritoneal/Biliary and Related Procedures 71 $9,950 880 ACUTE ADJUSTMENT REACTION & PSYCHOSOCIAL DYSFUNCTION MS 3 $8,161 62 ACUTE ISCHEMIC STROKE W USE OF THROMBOLYTIC AGENT W CC MS 10 $30,145
BPCI Advanced Episode Selection
 BPCI Advanced Episode Selection Analytic Framework and Strategies from Northwestern Medicine Presented June 7, 2018 to: Insert relevant presenter information Calibri 16pt Presented Jessica Walradt on:
BPCI Advanced Episode Selection Analytic Framework and Strategies from Northwestern Medicine Presented June 7, 2018 to: Insert relevant presenter information Calibri 16pt Presented Jessica Walradt on:
Kansas Care Coordination Quarterly Report October 2018
 Kansas Care Coordination Quarterly Report October 2018 Background Communities across the Great Plains Quality Innovation Network (QIN) region are collaborating to improve care coordination and medication
Kansas Care Coordination Quarterly Report October 2018 Background Communities across the Great Plains Quality Innovation Network (QIN) region are collaborating to improve care coordination and medication
Fiscal Year (FY) 2019 Hospital Inpatient Proposed Rule Interventional Cardiology, Peripheral Interventions & Rhythm Management
 2019 Hospital Inpatient Proposed Rule Interventional Cardiology, Peripheral Interventions & Rhythm Management") Fiscal Year (FY) 2019 Hospital Inpatient Proposed Rule Interventional Cardiology, Peripheral Interventions & Rhythm Management On April 24, 2018, the Centers for Medicare & Medicaid Services (CMS) released
Fiscal Year (FY) 2019 Hospital Inpatient Proposed Rule Interventional Cardiology, Peripheral Interventions & Rhythm Management On April 24, 2018, the Centers for Medicare & Medicaid Services (CMS) released
Average Gross Charges ACUTE MYOCARDIAL INFARCTION, DISCHARGED ALIVE W CC ,254 ACUTE MYOCARDIAL INFARCTION, DISCHARGED ALIVE W MCC - 280
 ACUTE MYOCARDIAL INFARCTION, DISCHARGED ALIVE W CC - 281 15,254 ACUTE MYOCARDIAL INFARCTION, DISCHARGED ALIVE W MCC - 280 24,827 ACUTE MYOCARDIAL INFARCTION, DISCHARGED ALIVE W/O CC/MCC - 282 11,575 AFTERCARE,
ACUTE MYOCARDIAL INFARCTION, DISCHARGED ALIVE W CC - 281 15,254 ACUTE MYOCARDIAL INFARCTION, DISCHARGED ALIVE W MCC - 280 24,827 ACUTE MYOCARDIAL INFARCTION, DISCHARGED ALIVE W/O CC/MCC - 282 11,575 AFTERCARE,
004 TRACH W MV >96 HRS OR PDX EXC FACE, MOUTH & NECK W/O MAJ O.R. $134, TRACHEOSTOMY FOR FACE,MOUTH & NECK DIAGNOSES W MCC $27,845.
 DRG Number DRG Name DRG Average Charge 004 TRACH W MV >96 HRS OR PDX EXC FACE, MOUTH & NECK W/O MAJ O.R. $134,495.54 011 TRACHEOSTOMY FOR FACE,MOUTH & NECK DIAGNOSES W MCC $27,845.14 012 TRACHEOSTOMY FOR
DRG Number DRG Name DRG Average Charge 004 TRACH W MV >96 HRS OR PDX EXC FACE, MOUTH & NECK W/O MAJ O.R. $134,495.54 011 TRACHEOSTOMY FOR FACE,MOUTH & NECK DIAGNOSES W MCC $27,845.14 012 TRACHEOSTOMY FOR
Randolph Health Average Inpatient DRG Charge
 004 Trach W Mv >96 Hrs Or Pdx Exc Face, Mouth & Neck W/O Maj O.R. 244,470 040 Periph/Cranial Nerve & Other Nerv Syst Proc W Mcc 61,412 041 Periph/Cranial Nerve & Other Nerv Syst Proc W Cc Or Periph Neurostim
004 Trach W Mv >96 Hrs Or Pdx Exc Face, Mouth & Neck W/O Maj O.R. 244,470 040 Periph/Cranial Nerve & Other Nerv Syst Proc W Mcc 61,412 041 Periph/Cranial Nerve & Other Nerv Syst Proc W Cc Or Periph Neurostim
The Cost Burden of Worsening Heart Failure in the Medicare Fee For Service Population: An Actuarial Analysis
 Client Report Milliman Client Report The Cost Burden of Worsening Heart Failure in the Medicare Fee For Service Population: An Actuarial Analysis Prepared by Kathryn Fitch, RN, MEd Principal and Healthcare
Client Report Milliman Client Report The Cost Burden of Worsening Heart Failure in the Medicare Fee For Service Population: An Actuarial Analysis Prepared by Kathryn Fitch, RN, MEd Principal and Healthcare
Risk Mitigation in Bundled Payment
 Risk Mitigation in Bundled Payment When to Hold Them and When To Fold Them Lily Pazand, MPH NYU Langone Medical Center Jonathan Pearce, MBA, CPA, FHFMA Singletrack Analytics Jessica Walradt, MS Association
Risk Mitigation in Bundled Payment When to Hold Them and When To Fold Them Lily Pazand, MPH NYU Langone Medical Center Jonathan Pearce, MBA, CPA, FHFMA Singletrack Analytics Jessica Walradt, MS Association
Analysis of Variation in Medicare Margins for Inpatient Rehabilitation Facilities (IRFs)
") Analysis of Variation in Medicare s for Inpatient Rehabilitation Facilities (IRFs) Dobson DaVanzo & Associates, LLC Vienna, VA 703.260.1760 www.dobsondavanzo.com Analysis of Variation in Medicare s for
Analysis of Variation in Medicare s for Inpatient Rehabilitation Facilities (IRFs) Dobson DaVanzo & Associates, LLC Vienna, VA 703.260.1760 www.dobsondavanzo.com Analysis of Variation in Medicare s for
More than 1.8 million New York State residents have diabetes, 1
 September 1 New York State Health Foundation s DIABETES Policy Center DIABETES: A HIDDEN HEALTH CARE COST DRIVER IN NEW YORK An Analysis of Health Care Utilization and Trends of Patients with Diabetes
September 1 New York State Health Foundation s DIABETES Policy Center DIABETES: A HIDDEN HEALTH CARE COST DRIVER IN NEW YORK An Analysis of Health Care Utilization and Trends of Patients with Diabetes
Proprietary Acute Care Indicators
 Proprietary Acute Care Indicators Indicator 1a: Device-Associated Infections in the Intensive Care Unit Central Line-Associated Bloodstream Infections in the APICU, CCU, MICU, M/S ICU, & SICU Ventilator-Associated
Proprietary Acute Care Indicators Indicator 1a: Device-Associated Infections in the Intensive Care Unit Central Line-Associated Bloodstream Infections in the APICU, CCU, MICU, M/S ICU, & SICU Ventilator-Associated
Medicare Fee-for-Service 2010 Improper Payment Report
 U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES The Supplementary Appendices for the Medicare Fee-for-Service 2010 Improper Payment Report Appendix Organization Appendix A: List of Acronyms Appendix B: Projected
U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES The Supplementary Appendices for the Medicare Fee-for-Service 2010 Improper Payment Report Appendix Organization Appendix A: List of Acronyms Appendix B: Projected
Key Trends for Ambulatory Surgery Centers in 2018
 Key Trends for Ambulatory Surgery Centers in 2018 Don Phalen Vice President Business Development, Regent Surgical Health Mark Murphy Chief Strategy Officer, St Joseph s Hospital MOVING TOWARDS VALUE-BASED
Key Trends for Ambulatory Surgery Centers in 2018 Don Phalen Vice President Business Development, Regent Surgical Health Mark Murphy Chief Strategy Officer, St Joseph s Hospital MOVING TOWARDS VALUE-BASED
National Average Payment (Ver 30.0) Average Length of Stay (in days) Average Charge Per Stay. Average Charge Per Day.
 Average Length of Stay (in days) Average Charge Per Stay. Average Charge Per Day.") Per 2013 1 HEART TRANSPLANT OR IMPLANT OF HEART ASSIST SYSTEM W MCC 221 11,675 $223,519,640 1 $139,225.55 $1,011,401 $19,145 52.8 2013 2 HEART TRANSPLANT OR IMPLANT OF HEART ASSIST SYSTEM W/O MCC 54 1,440
Per 2013 1 HEART TRANSPLANT OR IMPLANT OF HEART ASSIST SYSTEM W MCC 221 11,675 $223,519,640 1 $139,225.55 $1,011,401 $19,145 52.8 2013 2 HEART TRANSPLANT OR IMPLANT OF HEART ASSIST SYSTEM W/O MCC 54 1,440
FY2015 Proposed Hospital Inpatient Rule Summary
 FY2015 Proposed Hospital Inpatient Rule Summary Cardiac Rhythm Management (CRM) Electrophysiology (EP) Interventional Cardiology (IC) Peripheral Intervention (PI) On April 30, 2014, the Centers for Medicare
FY2015 Proposed Hospital Inpatient Rule Summary Cardiac Rhythm Management (CRM) Electrophysiology (EP) Interventional Cardiology (IC) Peripheral Intervention (PI) On April 30, 2014, the Centers for Medicare
FY2014 Final Hospital Inpatient Rule Summary
 FY2014 Final Hospital Inpatient Rule Summary Reimbursement Update Cardiac Rhythm Management (CRM) Electrophysiology (EP) Interventional Cardiology (IC) Peripheral Intervention (PI) On August 2, 2013, the
FY2014 Final Hospital Inpatient Rule Summary Reimbursement Update Cardiac Rhythm Management (CRM) Electrophysiology (EP) Interventional Cardiology (IC) Peripheral Intervention (PI) On August 2, 2013, the
Appendix 1: Supplementary tables [posted as supplied by author]
![Appendix 1: Supplementary tables [posted as supplied by author]](/thumbs/81/83505567.jpg "Appendix 1: Supplementary tables [posted as supplied by author]") Appendix 1: Supplementary tables [posted as supplied by author] Table A. International Classification of Diseases, Ninth Revision, Clinical Modification Codes Used to Define Heart Failure, Acute Myocardial
Appendix 1: Supplementary tables [posted as supplied by author] Table A. International Classification of Diseases, Ninth Revision, Clinical Modification Codes Used to Define Heart Failure, Acute Myocardial
DRG DRG DESCRIPTION AVE CHARGE AVE DAYS 4 TRACH W MV >96 HRS OR PDX EXC FACE, MOUTH & NECK W/O MAJ O.R. $176, TRACHEOSTOMY FOR
 DRG DRG DESCRIPTION AVE CHARGE AVE DAYS 4 TRACH W MV >96 HRS OR PDX EXC FACE, MOUTH & NECK W/O MAJ O.R. $176,341.00 13.0 11 TRACHEOSTOMY FOR FACE,MOUTH & NECK DIAGNOSES W MCC $82,442.00 11.0 25 CRANIOTOMY
DRG DRG DESCRIPTION AVE CHARGE AVE DAYS 4 TRACH W MV >96 HRS OR PDX EXC FACE, MOUTH & NECK W/O MAJ O.R. $176,341.00 13.0 11 TRACHEOSTOMY FOR FACE,MOUTH & NECK DIAGNOSES W MCC $82,442.00 11.0 25 CRANIOTOMY
Using Observation and Inpatient Metrics to Maximize Net Reimbursement
 Using Observation and Inpatient Metrics to Maximize Net Reimbursement Colleen Hall, Crowe Horwath Stephen Crouch MD, Advocate Good Samaritan Hospital 2 Objectives Identify industry benchmarks related to
Using Observation and Inpatient Metrics to Maximize Net Reimbursement Colleen Hall, Crowe Horwath Stephen Crouch MD, Advocate Good Samaritan Hospital 2 Objectives Identify industry benchmarks related to
Maine Workers' Compensation Board Medical Fee Schedule
 001 SURG HEART TRANSPLANT OR IMPLANT OF HEART ASSIST SYSTEM W MCC 29.1 26.4106 $243,431.25 $257,869.40 002 SURG SYSTEM W/O MCC 15.1 13.4227 $123,719.44 $131,057.36 003 SURG MOUTH & NECK W MAJ O.R. 23.4
001 SURG HEART TRANSPLANT OR IMPLANT OF HEART ASSIST SYSTEM W MCC 29.1 26.4106 $243,431.25 $257,869.40 002 SURG SYSTEM W/O MCC 15.1 13.4227 $123,719.44 $131,057.36 003 SURG MOUTH & NECK W MAJ O.R. 23.4
APR-DRG Description Ave Charge
 Abdominal Pain 16,500.25 2.8 6,000.09 Acute & Subacute Endocarditis 15,339.30 3.0 5,113.10 Acute Myocardial Infarction 17,687.46 2.6 6,802.87 Alcohol Abuse & Dependence 19,126.64 4.2 4,553.96 Alcoholic
Abdominal Pain 16,500.25 2.8 6,000.09 Acute & Subacute Endocarditis 15,339.30 3.0 5,113.10 Acute Myocardial Infarction 17,687.46 2.6 6,802.87 Alcohol Abuse & Dependence 19,126.64 4.2 4,553.96 Alcoholic
Health Services Utilization and Medical Costs Among Medicare Atrial Fibrillation Patients / September 2010
 Health Services Utilization and Medical Costs Among Medicare Atrial Fibrillation Patients / September 2010 AF Stat is sponsored by sanofi-aventis, U.S. LLC, which provided funding for this report. Avalere
Health Services Utilization and Medical Costs Among Medicare Atrial Fibrillation Patients / September 2010 AF Stat is sponsored by sanofi-aventis, U.S. LLC, which provided funding for this report. Avalere
Short-term Acute Care Program for Evaluating Payment Patterns Electronic Report. User s Guide Twenty-second Edition. Prepared by
 Short-term Acute Care Program for Evaluating Payment Patterns Electronic Report User s Guide Twenty-second Edition Prepared by 1 Short-term Acute Care Program for Evaluating Payment Patterns Electronic
Short-term Acute Care Program for Evaluating Payment Patterns Electronic Report User s Guide Twenty-second Edition Prepared by 1 Short-term Acute Care Program for Evaluating Payment Patterns Electronic
Orange Regional Medical Center Average Charge Per Inpatient Case - based on MS DRG
 Per Inpatient Case - based on MS DRG 003 ECMO or trach w MV 96+ hrs or pdx exc face, mouth & neck w maj O.R. 737,213 004 Trach w MV 96+ hrs or pdx exc face, mouth & neck w/o maj O.R. 298,769 011 Tracheostomy
Per Inpatient Case - based on MS DRG 003 ECMO or trach w MV 96+ hrs or pdx exc face, mouth & neck w maj O.R. 737,213 004 Trach w MV 96+ hrs or pdx exc face, mouth & neck w/o maj O.R. 298,769 011 Tracheostomy
INPATIENT REIMBURSEMENT PROSPECTUS
 2018 CARDIOVASCULAR SERVICE LINE INPATIENT REIMBURSEMENT PROSPECTUS Increasing financial risk to U.S. health care providers, including physicians and hospitals, has been centered on outcomes-based modifiers
2018 CARDIOVASCULAR SERVICE LINE INPATIENT REIMBURSEMENT PROSPECTUS Increasing financial risk to U.S. health care providers, including physicians and hospitals, has been centered on outcomes-based modifiers
Fractional Flow Reserve (FFR) and instant wave-free Ratio (The ifr modality)
 and instant wave-free Ratio (The ifr modality)") 2017 Coding and Medicare payment guide Fractional Flow Reserve (FFR) and instant wave-free Ratio (The ifr modality) All coding, coverage, billing and payment information provided herein by Philips Volcano
2017 Coding and Medicare payment guide Fractional Flow Reserve (FFR) and instant wave-free Ratio (The ifr modality) All coding, coverage, billing and payment information provided herein by Philips Volcano
Average DRG Description
 Leesburg Regional Medical Center Inpatient Data Average Charge per DRG 12 Months Ending Quarter 1 of 2018 Average DRG Description Charge 3 ECMO OR TRACH W MV >96 HRS OR PDX EXC FACE, MOUTH & NECK W MAJ
Leesburg Regional Medical Center Inpatient Data Average Charge per DRG 12 Months Ending Quarter 1 of 2018 Average DRG Description Charge 3 ECMO OR TRACH W MV >96 HRS OR PDX EXC FACE, MOUTH & NECK W MAJ
Frightening Scenario or Manageable Change? Determining the Realistic Reimbursement Impact of ICD-10 on MS-DRGs. Lori Jayne, RHIA Donna Smith, RHIA
 Frightening Scenario or Manageable Change? Determining the Realistic Reimbursement Impact of ICD-10 on MS-DRGs Lori Jayne, RHIA Donna Smith, RHIA Objectives Speaker introductions Processes to determine
Frightening Scenario or Manageable Change? Determining the Realistic Reimbursement Impact of ICD-10 on MS-DRGs Lori Jayne, RHIA Donna Smith, RHIA Objectives Speaker introductions Processes to determine
Sample page. DRG Desk Reference. The ultimate resource for improving MS-DRG assignment practices DESK REFERENCE
 DESK REFERENCE 2018 DRG Desk Reference The ultimate resource for improving MS-DRG assignment practices POWER UP YOUR CODING with Optum360, your trusted coding partner for 32 years. Visit optum360coding.com.
DESK REFERENCE 2018 DRG Desk Reference The ultimate resource for improving MS-DRG assignment practices POWER UP YOUR CODING with Optum360, your trusted coding partner for 32 years. Visit optum360coding.com.
Bundled Payments in Post Acute Care: Put on Your Crash Helmets or Fasten Your Seatbelts
 Bundled Payments in Post Acute Care: Put on Your Crash Helmets or Fasten Your Seatbelts Presented by: Rodney Farley, Vice President of Post Acute Services 5925 Stevenson Avenue Suite G Harrisburg, PA 17112
Bundled Payments in Post Acute Care: Put on Your Crash Helmets or Fasten Your Seatbelts Presented by: Rodney Farley, Vice President of Post Acute Services 5925 Stevenson Avenue Suite G Harrisburg, PA 17112
Short-term Acute Care Program for Evaluating Payment Patterns Electronic Report. User s Guide Twenty-third Edition. Prepared by
 Short-term Acute Care Program for Evaluating Payment Patterns Electronic Report User s Guide Twenty-third Edition Prepared by 1 Short-term Acute Care Program for Evaluating Payment Patterns Electronic
Short-term Acute Care Program for Evaluating Payment Patterns Electronic Report User s Guide Twenty-third Edition Prepared by 1 Short-term Acute Care Program for Evaluating Payment Patterns Electronic
APR DRG Data Discovery
 APR DRG Data Discovery Henry Johnson MD, MPH Midas+ Vice President and Medical Director Vanessa Dorr RN MSN Midas+ DataVision Clinical Consultant Review: Agenda 3M APR DRG Methodology DataVision: Web and
APR DRG Data Discovery Henry Johnson MD, MPH Midas+ Vice President and Medical Director Vanessa Dorr RN MSN Midas+ DataVision Clinical Consultant Review: Agenda 3M APR DRG Methodology DataVision: Web and
ALL Other (MS) DRG 2015
 DRG 2015") ALL Other (MS) DRG 2015 DRG DRG Description Avg. Charge 770 ABORTION W D&C, ASPIRATION CURETTAGE OR HYSTEROTOMY $8,072.48 779 ABORTION W/O D&C $9,405.76 289 ACUTE & SUBACUTE ENDOCARDITIS W CC $20,196.02
ALL Other (MS) DRG 2015 DRG DRG Description Avg. Charge 770 ABORTION W D&C, ASPIRATION CURETTAGE OR HYSTEROTOMY $8,072.48 779 ABORTION W/O D&C $9,405.76 289 ACUTE & SUBACUTE ENDOCARDITIS W CC $20,196.02
WakeMed DRG* Data 2019
 WakeMed DRG* Data 2019 *Diagnosis-Related Groups (DRGs or MS-DRGs) A DRG (diagnosis-related group) is the system Medicare and some insurance companies use to classify and categorize charges for inpatient
WakeMed DRG* Data 2019 *Diagnosis-Related Groups (DRGs or MS-DRGs) A DRG (diagnosis-related group) is the system Medicare and some insurance companies use to classify and categorize charges for inpatient
Acute Coronary Syndrome
 ACUTE CORONOARY SYNDROME, ANGINA & ACUTE MYOCARDIAL INFARCTION Administrative Consultant Service 3/17 Acute Coronary Syndrome Acute Coronary Syndrome has evolved as a useful operational term to refer to
ACUTE CORONOARY SYNDROME, ANGINA & ACUTE MYOCARDIAL INFARCTION Administrative Consultant Service 3/17 Acute Coronary Syndrome Acute Coronary Syndrome has evolved as a useful operational term to refer to
COMMUNITY MEMORIAL HOSPITAL ACUTE INPATIENT CASES BY DRG (diagnosis related group) AVERAGE AVERAGE ALL PAYER CHARGE PAYMENT MSDRG DESCRIPTION PER
 AVERAGE AVERAGE ALL PAYER CHARGE PAYMENT MSDRG DESCRIPTION PER") COMMUNITY MEMORIAL HOSPITAL ACUTE INPATIENT CASES BY DRG (diagnosis related group) AVERAGE AVERAGE ALL PAYER CHARGE PAYMENT MSDRG DESCRIPTION PER CASE PER CASE 1 CARDIOMYOPATHY 536,923.14 221,201.34 100
COMMUNITY MEMORIAL HOSPITAL ACUTE INPATIENT CASES BY DRG (diagnosis related group) AVERAGE AVERAGE ALL PAYER CHARGE PAYMENT MSDRG DESCRIPTION PER CASE PER CASE 1 CARDIOMYOPATHY 536,923.14 221,201.34 100
Coronary intravascular ultrasound (IVUS)
") 2017 Coding and Medicare payment guide Coronary intravascular ultrasound (IVUS) All coding, coverage, billing and payment information provided herein by Philips Volcano is gathered from third-party sources
2017 Coding and Medicare payment guide Coronary intravascular ultrasound (IVUS) All coding, coverage, billing and payment information provided herein by Philips Volcano is gathered from third-party sources
Policy Brief June 2014
 Policy Brief June 2014 Which Medicare Patients Are Transferred from Rural Emergency Departments? Michelle Casey MS, Jeffrey McCullough PhD, and Robert Kreiger PhD Key Findings Among Medicare beneficiaries
Policy Brief June 2014 Which Medicare Patients Are Transferred from Rural Emergency Departments? Michelle Casey MS, Jeffrey McCullough PhD, and Robert Kreiger PhD Key Findings Among Medicare beneficiaries
PfP Quality Metrics: Readmissions, Value-Based Purchasing and Beyond
 PfP Quality Metrics: Readmissions, Value-Based Purchasing and Beyond Presented to ASHNHA Alaska Partnership for Patients Advisory Group February 4, 2015 Gloria Kupferman Readmissions Calculation methods
PfP Quality Metrics: Readmissions, Value-Based Purchasing and Beyond Presented to ASHNHA Alaska Partnership for Patients Advisory Group February 4, 2015 Gloria Kupferman Readmissions Calculation methods
Dana L. Gilbert Chief Operating Officer Sharon Rudnick Vice President Outpatient Care Management
 Ambulatory Sensitive Admissions Dana L. Gilbert Chief Operating Officer Sharon Rudnick Vice President Outpatient Care Management 1 Sites Of Care Advocate Health Care 12 Hospitals 10 acute care hospitals
Ambulatory Sensitive Admissions Dana L. Gilbert Chief Operating Officer Sharon Rudnick Vice President Outpatient Care Management 1 Sites Of Care Advocate Health Care 12 Hospitals 10 acute care hospitals
Average DRG DRG Description
 s by DRG 3 ECMO OR TRACH W MV >96 HRS OR PDX EXC FACE, MOUTH & NECK W MAJ O.R. $466,547 4 TRACH W MV >96 HRS OR PDX EXC FACE, MOUTH & NECK W/O MAJ O.R. $513,102 11 TRACHEOSTOMY FOR FACE,MOUTH & NECK DIAGNOSES
s by DRG 3 ECMO OR TRACH W MV >96 HRS OR PDX EXC FACE, MOUTH & NECK W MAJ O.R. $466,547 4 TRACH W MV >96 HRS OR PDX EXC FACE, MOUTH & NECK W/O MAJ O.R. $513,102 11 TRACHEOSTOMY FOR FACE,MOUTH & NECK DIAGNOSES
Determining MS-DRGs. Kimberly Cunningham CPC, CIC, CCS. Copyright/Disclaimer text
 Determining MS-DRGs Kimberly Cunningham CPC, CIC, CCS Copyright/Disclaimer text No part of this presentation may be reproduced or transmitted in any form or by any means (graphically, electronically, or
Determining MS-DRGs Kimberly Cunningham CPC, CIC, CCS Copyright/Disclaimer text No part of this presentation may be reproduced or transmitted in any form or by any means (graphically, electronically, or
THE NATIONAL QUALITY FORUM
 THE NATIONAL QUALITY FORUM National Voluntary Consensus Standards for Patient Outcomes Table of Measures Submitted-Phase 1 As of March 5, 2010 Note: This information is for personal and noncommercial use
THE NATIONAL QUALITY FORUM National Voluntary Consensus Standards for Patient Outcomes Table of Measures Submitted-Phase 1 As of March 5, 2010 Note: This information is for personal and noncommercial use
Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care
 Accelero Health Partners, 2015 WHITE PAPER Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care Jason Pry, Senior Director ABSTRACT Every year more than a quarter of a million
Accelero Health Partners, 2015 WHITE PAPER Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care Jason Pry, Senior Director ABSTRACT Every year more than a quarter of a million
Measure Applications Partnership. Hospital Workgroup In-Person Meeting Follow- Up Call
 Measure Applications Partnership Hospital Workgroup In-Person Meeting Follow- Up Call December 21, 2016 Feedback on Current Measure Sets for IQR, HACs, Readmissions, and VBP 2 Previously Identified Crosscutting
Measure Applications Partnership Hospital Workgroup In-Person Meeting Follow- Up Call December 21, 2016 Feedback on Current Measure Sets for IQR, HACs, Readmissions, and VBP 2 Previously Identified Crosscutting
Leveraging Analytics to Mitigate Financial Risks in ICD-10
 Leveraging Analytics to Mitigate Financial Risks in ICD-10 Deborah Szymanski, RN, BSN Revenue Cycle Manager Steve Ross, MD Physician Informaticist Chris Cummins Director of Sales October 14, 2014 Today
Leveraging Analytics to Mitigate Financial Risks in ICD-10 Deborah Szymanski, RN, BSN Revenue Cycle Manager Steve Ross, MD Physician Informaticist Chris Cummins Director of Sales October 14, 2014 Today
SmartIX EMPI Taking It to the Next Level
 SmartIX EMPI Taking It to the Next Level Theresa Mendoza Director of Quality, BI, and Data Services Dallas-Fort Worth Education and Research Foundation Agenda Welcome Introduction History Next Level of
SmartIX EMPI Taking It to the Next Level Theresa Mendoza Director of Quality, BI, and Data Services Dallas-Fort Worth Education and Research Foundation Agenda Welcome Introduction History Next Level of
Technical Appendix for Outcome Measures
 Study Overview Technical Appendix for Outcome Measures This is a report on data used, and analyses done, by MPA Healthcare Solutions (MPA, formerly Michael Pine and Associates) for Consumers CHECKBOOK/Center
Study Overview Technical Appendix for Outcome Measures This is a report on data used, and analyses done, by MPA Healthcare Solutions (MPA, formerly Michael Pine and Associates) for Consumers CHECKBOOK/Center
HEART FAILURE QUALITY IMPROVEMENT. American Heart Association Shawni Smith Regional Director, Quality & Systems Improvement
 HEART FAILURE QUALITY IMPROVEMENT American Heart Association Shawni Smith Regional Director, Quality & Systems Improvement 1 DISCLOSURES NONE 2 3 WHY IS THIS IMPORTANT? WHY? Heart Failure Currently, an
HEART FAILURE QUALITY IMPROVEMENT American Heart Association Shawni Smith Regional Director, Quality & Systems Improvement 1 DISCLOSURES NONE 2 3 WHY IS THIS IMPORTANT? WHY? Heart Failure Currently, an
Critical Access Hospital (CAH) PEPPER Update
 PEPPER Update") Critical Access Hospital (CAH) PEPPER Update April, 2016 Kimberly Hrehor Agenda Updates to the Q4FY15 CAH PEPPER release Revised target areas: Medical DRGs with CC or MCC Surgical DRGs with CC or MCC 3-day
Critical Access Hospital (CAH) PEPPER Update April, 2016 Kimberly Hrehor Agenda Updates to the Q4FY15 CAH PEPPER release Revised target areas: Medical DRGs with CC or MCC Surgical DRGs with CC or MCC 3-day
TECHNICAL NOTES APPENDIX SUMMER
 TECHNICAL NOTES APPENDIX SUMMER Hospital Performance Report Summer Update INCLUDES PENNSYLVANIA INPATIENT HOSPITAL DISCHARGES FROM JULY 1, 2006 THROUGH JUNE 30, 2007 The Pennsylvania Health Care Cost Containment
TECHNICAL NOTES APPENDIX SUMMER Hospital Performance Report Summer Update INCLUDES PENNSYLVANIA INPATIENT HOSPITAL DISCHARGES FROM JULY 1, 2006 THROUGH JUNE 30, 2007 The Pennsylvania Health Care Cost Containment
Short-term Acute Care Program for Evaluating Payment Patterns Electronic Report. User s Guide Sixteenth Edition. Prepared by
 Short-term Acute Care Program for Evaluating Payment Patterns Electronic Report User s Guide Sixteenth Edition Prepared by 1 Short-term Acute Care Program for Evaluating Payment Patterns Electronic Report
Short-term Acute Care Program for Evaluating Payment Patterns Electronic Report User s Guide Sixteenth Edition Prepared by 1 Short-term Acute Care Program for Evaluating Payment Patterns Electronic Report
What ASMBS Members Need to Know About: New Medicare Payment Policy Governing Bariatric Surgery and Hospital Acquired Conditions (HACs)
") What ASMBS Members Need to Know About: New Medicare Payment Policy Governing Bariatric Surgery and Hospital Acquired Conditions (HACs) Robin Blackstone, MD, FACS, FASMBS Beginning October 1, 2008, Medicare
What ASMBS Members Need to Know About: New Medicare Payment Policy Governing Bariatric Surgery and Hospital Acquired Conditions (HACs) Robin Blackstone, MD, FACS, FASMBS Beginning October 1, 2008, Medicare
The Future of Cardiac Care: Managing Our Patients Together
 The Future of Cardiac Care: Managing Our Patients Together Charles R. Caldwell, MD, FACC Disclosures: iheartdoc,inc. Telemedicine 1 MACRA Medicare Access and CHIP Reauthorization Act of 2015 Repealed the
The Future of Cardiac Care: Managing Our Patients Together Charles R. Caldwell, MD, FACC Disclosures: iheartdoc,inc. Telemedicine 1 MACRA Medicare Access and CHIP Reauthorization Act of 2015 Repealed the
In Pursuit of Excellence: The CheckPoint Journey
 Focus On Quality... In Pursuit of Excellence: The CheckPoint Journey Charles Shabino, MD; Dana Richardson, RN, MHA Abstract In March 2004, the Wisconsin Hospital Association launched CheckPoint sm (www.wicheckpoint.org)
Focus On Quality... In Pursuit of Excellence: The CheckPoint Journey Charles Shabino, MD; Dana Richardson, RN, MHA Abstract In March 2004, the Wisconsin Hospital Association launched CheckPoint sm (www.wicheckpoint.org)
MCCG AVG CHARGE PER DRG-FY18 12/27/2018 1
 1 HEART TRANSPLANT OR IMPLANT OF HEART ASSIST SYSTEM W MCC $762,065.15 2 HEART TRANSPLANT OR IMPLANT OF HEART ASSIST SYSTEM W/O MCC $552,519.55 3 ECMO OR TRACH W MV >96 HRS OR PDX EXC FACE, MOUTH & NECK
1 HEART TRANSPLANT OR IMPLANT OF HEART ASSIST SYSTEM W MCC $762,065.15 2 HEART TRANSPLANT OR IMPLANT OF HEART ASSIST SYSTEM W/O MCC $552,519.55 3 ECMO OR TRACH W MV >96 HRS OR PDX EXC FACE, MOUTH & NECK
Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care
 Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care Every year more than a quarter of a million people over the age of 65 are admitted to a hospital with a hip fracture. Mortality
Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care Every year more than a quarter of a million people over the age of 65 are admitted to a hospital with a hip fracture. Mortality
Mandatory Elements of Healthcare Reform Walter Coleman. healthcare consulting
 Mandatory Elements of Healthcare Reform Walter Coleman 1 Agenda ACA Mandatory Elements of Reform Value Based Purchasing Readmission Reduction Program Hospital Acquired Conditions Best practices to analyze
Mandatory Elements of Healthcare Reform Walter Coleman 1 Agenda ACA Mandatory Elements of Reform Value Based Purchasing Readmission Reduction Program Hospital Acquired Conditions Best practices to analyze
ENROLLMENT : Line of Business Summary
 ENROLLMENT : Line of Business Summary Date Range : JAN 2017 through DEC 2017 COMPREHENSIVE MAJOR MEDICAL Print Date : 1/19/2018 9:43:49AM Page 1 of 1 Month Year Single 2 Person : Emp/Spouse 2 Person :
ENROLLMENT : Line of Business Summary Date Range : JAN 2017 through DEC 2017 COMPREHENSIVE MAJOR MEDICAL Print Date : 1/19/2018 9:43:49AM Page 1 of 1 Month Year Single 2 Person : Emp/Spouse 2 Person :
Some key findings from ABC Clinic's report: Risk Score Clinic. Summary by Service Category
 Dear Administrator or Medical Director, QCorp is pleased to release its second round of Comparison Reports. This report includes claims incurred from January 2014 to December 2014. As a reminder, the goal
Dear Administrator or Medical Director, QCorp is pleased to release its second round of Comparison Reports. This report includes claims incurred from January 2014 to December 2014. As a reminder, the goal
Lee Health Average Charge per DRG FY 2018 (10/1/2017-9/30/2018) Inpatients, All Payors AVERAGE DRG DRG NAME CHG/ CASE
 Inpatients, All Payors AVERAGE DRG DRG NAME CHG/ CASE") Lee Health Average Charge per DRG FY 2018 (10/1/2017-9/30/2018) Inpatients, All Payors AVERAGE DRG DRG NAME CHG/ CASE 795 NORMAL NEWBORN 3,285 849 RADIOTHERAPY 5,383 794 NEONATE W OTHER SIGNIFICANT PROBLEMS
Lee Health Average Charge per DRG FY 2018 (10/1/2017-9/30/2018) Inpatients, All Payors AVERAGE DRG DRG NAME CHG/ CASE 795 NORMAL NEWBORN 3,285 849 RADIOTHERAPY 5,383 794 NEONATE W OTHER SIGNIFICANT PROBLEMS
Key Performance Indicators to Direct Audit Plans
 Key Performance Indicators to Direct Audit Plans Lori Laubach, Principal MD Audit User Group June 15 17, 2014 1 The material appearing in this presentation is for informational purposes only and is not
Key Performance Indicators to Direct Audit Plans Lori Laubach, Principal MD Audit User Group June 15 17, 2014 1 The material appearing in this presentation is for informational purposes only and is not
Supplementary Online Content
 Supplementary Online Content Dharmarajan K, Wang Y, Lin Z, et al. Association of changing hospital readmission rates with mortality rates after hospital discharge. JAMA. doi:10.1001/jama.2017.8444 etable
Supplementary Online Content Dharmarajan K, Wang Y, Lin Z, et al. Association of changing hospital readmission rates with mortality rates after hospital discharge. JAMA. doi:10.1001/jama.2017.8444 etable
LIST OF MEDICARE SEVERITY DIAGNOSIS-RELATED GROUPS (MS-DRGS) FY 2019 MS-DRG MDC TYPE MS-DRG Title 001 PRE SURG HEART TRANSPLANT OR IMPLANT OF HEART
 FY 2019 MS-DRG MDC TYPE MS-DRG Title 001 PRE SURG HEART TRANSPLANT OR IMPLANT OF HEART") LIST OF MEDICARE SEVERITY DIAGNOSIS-RELATED GROUPS (MS-DRGS) FY 2019 MS-DRG MDC TYPE MS-DRG Title 001 PRE SURG HEART TRANSPLANT OR IMPLANT OF HEART ASSIST SYSTEM W MCC 002 PRE SURG HEART TRANSPLANT OR
LIST OF MEDICARE SEVERITY DIAGNOSIS-RELATED GROUPS (MS-DRGS) FY 2019 MS-DRG MDC TYPE MS-DRG Title 001 PRE SURG HEART TRANSPLANT OR IMPLANT OF HEART ASSIST SYSTEM W MCC 002 PRE SURG HEART TRANSPLANT OR
LIST OF MEDICARE SEVERITY DIAGNOSIS-RELATED GROUPS (LTC-MS-DRGS) FY 2018 MS-DRG MDC TYPE MS-DRG Title 001 PRE SURG HEART TRANSPLANT OR IMPLANT OF
 FY 2018 MS-DRG MDC TYPE MS-DRG Title 001 PRE SURG HEART TRANSPLANT OR IMPLANT OF") LIST OF MEDICARE SEVERITY DIAGNOSIS-RELATED GROUPS (LTC-MS-DRGS) FY 2018 MS-DRG MDC TYPE MS-DRG Title 001 PRE SURG HEART TRANSPLANT OR IMPLANT OF HEART ASSIST SYSTEM W MCC 002 PRE SURG HEART TRANSPLANT
LIST OF MEDICARE SEVERITY DIAGNOSIS-RELATED GROUPS (LTC-MS-DRGS) FY 2018 MS-DRG MDC TYPE MS-DRG Title 001 PRE SURG HEART TRANSPLANT OR IMPLANT OF HEART ASSIST SYSTEM W MCC 002 PRE SURG HEART TRANSPLANT
HQID Hospital Performance Update & Analysis of Quality, Cost and Mortality Trends Fact Sheet
 HQID Hospital Performance Update & Analysis of Quality, Cost and Mortality Trends Fact Sheet I.) Performance of Hospitals in the Hospital Quality Incentive Demonstration over 15 Quarters* (pages 2-5) Launched
HQID Hospital Performance Update & Analysis of Quality, Cost and Mortality Trends Fact Sheet I.) Performance of Hospitals in the Hospital Quality Incentive Demonstration over 15 Quarters* (pages 2-5) Launched
Medical Review Robin Leigh, R.N., B.S.N.
 Medical Review Robin Leigh, R.N., B.S.N. Medical Review The List Going Beyond The List It s not what we do, it s why we do it Accuracy of Problem Identification Efficiency of Review Process Efficiency
Medical Review Robin Leigh, R.N., B.S.N. Medical Review The List Going Beyond The List It s not what we do, it s why we do it Accuracy of Problem Identification Efficiency of Review Process Efficiency
Initial Hospital Care/Day. Subsequent Hospital Care/Day
 Inpatient Charges Daily Room Rates CM CM Intensive Care $4,305 Maternity $1,137 Cardiovascular Care $3,338 Newborn Care $669 Medical/Surgical $1,297 NICU $2,938 Hospital Care Hospital New Patient Consult
Inpatient Charges Daily Room Rates CM CM Intensive Care $4,305 Maternity $1,137 Cardiovascular Care $3,338 Newborn Care $669 Medical/Surgical $1,297 NICU $2,938 Hospital Care Hospital New Patient Consult
WORKING P A P E R. Comparative Performance of the MS-DRGS and RDRGS in Explaining Variation in Cost for Medicare Hospital Discharges BARBARA O.
 WORKING P A P E R Comparative Performance of the MS-DRGS and RDRGS in Explaining Variation in Cost for Medicare Hospital Discharges BARBARA O. WYNN WR-606 This product is part of the RAND Health working
WORKING P A P E R Comparative Performance of the MS-DRGS and RDRGS in Explaining Variation in Cost for Medicare Hospital Discharges BARBARA O. WYNN WR-606 This product is part of the RAND Health working
The table below includes the quality measures an ACO is required to submit to CMS as a participant in an MSSP Track 3 ACO
 The table below includes the quality measures an ACO is required to submit to CMS as a participant in an MSSP Track 3 ACO ACO-1 ACO-2 Getting Timely Care, Appointments, and Information How Well Your Providers
The table below includes the quality measures an ACO is required to submit to CMS as a participant in an MSSP Track 3 ACO ACO-1 ACO-2 Getting Timely Care, Appointments, and Information How Well Your Providers
The Centers for Medicare & Medicaid Services (CMS) Acute Care Hospital Fiscal Year (FY) 2018 Quality Improvement Program Measures
 Acute Care Hospital Fiscal Year (FY) 2018 Quality Improvement Program Measures") ID M easure Name NQF # H os pital M easurement Period H os pital H os pital Value-Bas ed Purchas ing M easurement Period H os pital H ealth Record (EH R) Incentive M easurement Period H os pital H os pital-
ID M easure Name NQF # H os pital M easurement Period H os pital H os pital Value-Bas ed Purchas ing M easurement Period H os pital H ealth Record (EH R) Incentive M easurement Period H os pital H os pital-
NQF-ENDORSED VOLUNTARY CONSENSUS STANDARD FOR HOSPITAL CARE. Measure Information Form Collected For: CMS Outcome Measures (Claims Based)
") Last Updated: Version 4.3 NQF-ENDORSED VOLUNTARY CONSENSUS STANDARD FOR HOSPITAL CARE Measure Information Form Collected For: CMS Outcome Measures (Claims Based) Measure Set: CMS Readmission Measures Set
Last Updated: Version 4.3 NQF-ENDORSED VOLUNTARY CONSENSUS STANDARD FOR HOSPITAL CARE Measure Information Form Collected For: CMS Outcome Measures (Claims Based) Measure Set: CMS Readmission Measures Set
Madelia Community Hospital & Clinic
 Madelia Community Hospital & Clinic 194 SIMPLE PNEUMONIA & PLEURISY W CC * * 195 SIMPLE PNEUMONIA & PLEURISY W/O CC/MCC * * 392 ESOPHAGITIS, GASTROENT & MISC DIGEST DISORDERS W/O MCC * * 292 HEART FAILURE
Madelia Community Hospital & Clinic 194 SIMPLE PNEUMONIA & PLEURISY W CC * * 195 SIMPLE PNEUMONIA & PLEURISY W/O CC/MCC * * 392 ESOPHAGITIS, GASTROENT & MISC DIGEST DISORDERS W/O MCC * * 292 HEART FAILURE
A Pause in the Availability of Risk Adjusted National Benchmarks for AHRQ Indicators and an Alternative Measurement Approach
 A Pause in the Availability of Risk Adjusted National Benchmarks for AHRQ Indicators and an Alternative Measurement Approach Joseph Greenway, MPH Director of the Center for Health Information Analysis
A Pause in the Availability of Risk Adjusted National Benchmarks for AHRQ Indicators and an Alternative Measurement Approach Joseph Greenway, MPH Director of the Center for Health Information Analysis
CMS Hospital Inpatient Quality Reporting (IQR) Program Measures for the FY 2019 Payment Update
 Program Measures for the FY 2019 Payment Update") CMS Inpatient Quality Reporting (IQR) Program Measures for the Update Measures Required to Meet IQR Program APU Requirements NHSN Submission CAUTI National Healthcare Safety Network (NHSN) Catheter-Associated
CMS Inpatient Quality Reporting (IQR) Program Measures for the Update Measures Required to Meet IQR Program APU Requirements NHSN Submission CAUTI National Healthcare Safety Network (NHSN) Catheter-Associated
A Comprehensive Scorecard for Board and Staff Larry Hegland, MD
 A Comprehensive Scorecard for Board and Staff Larry Hegland, MD System Medical Director for Recovery Audit and Appeal Services Chief Medical Officer for Ministry Saint Clare s Hospital and the Diagnostic
A Comprehensive Scorecard for Board and Staff Larry Hegland, MD System Medical Director for Recovery Audit and Appeal Services Chief Medical Officer for Ministry Saint Clare s Hospital and the Diagnostic
2018 Diagnosis Coding Fact Sheet
 The information contained in this document is provided for informational purposes only and represents no statement, promise, or guarantee by Cordis Corporation concerning levels of reimbursement, payment,
The information contained in this document is provided for informational purposes only and represents no statement, promise, or guarantee by Cordis Corporation concerning levels of reimbursement, payment,
Across The Chasm: The Transition From Volume To Value
 Across The Chasm: The Transition From Volume To Value Joseph Bisordi, MD, Executive Vice President & CMO Ochsner Health System Our Mission is to Serve, Heal, Lead, Educate, and Innovate $1.6 Revenue ($B)
Across The Chasm: The Transition From Volume To Value Joseph Bisordi, MD, Executive Vice President & CMO Ochsner Health System Our Mission is to Serve, Heal, Lead, Educate, and Innovate $1.6 Revenue ($B)
Patient Navigator Program: Focus MI Diplomat Hospital Metrics
 Patient Navigator Program: Focus MI Diplomat Hospital Metrics Goal Statement: To reduce avoidable hospital readmissions for patients discharged with acute myocardial infarction (AMI) by supporting a culture
Patient Navigator Program: Focus MI Diplomat Hospital Metrics Goal Statement: To reduce avoidable hospital readmissions for patients discharged with acute myocardial infarction (AMI) by supporting a culture
Arkansas Health Care Payment Improvement Initiative Percutaneous Coronary Intervention Algorithm Summary
 Arkansas Health Care Payment Improvement Initiative Percutaneous Coronary Intervention Algorithm Summary Percutaneous Coronary Intervention (PCI) Algorithm Summary v1.0 Page 2 of 8 Triggers PAP assignment
Arkansas Health Care Payment Improvement Initiative Percutaneous Coronary Intervention Algorithm Summary Percutaneous Coronary Intervention (PCI) Algorithm Summary v1.0 Page 2 of 8 Triggers PAP assignment
CMS Hospital Inpatient Quality Reporting (IQR) Program Measures for the FY 2020 Payment Update
 Program Measures for the FY 2020 Payment Update") CMS Inpatient Quality Reporting (IQR) Program Measures for the Payment Update Measures Required to Meet IQR Program APU Requirements Healthcare-Associated Infection on CAUTI National Healthcare Safety
CMS Inpatient Quality Reporting (IQR) Program Measures for the Payment Update Measures Required to Meet IQR Program APU Requirements Healthcare-Associated Infection on CAUTI National Healthcare Safety
North Carolina Inpatient Hospital Discharge Data - Data Dictionary FY 2016 Alphabetic List of Variables and Attributes Standard Research File
 North Carolina Inpatient Hospital Discharge Data - Data Dictionary FY 2016 Alphabetic List of Variables and Attributes Standard Research File For a standard research file request one of three variables
North Carolina Inpatient Hospital Discharge Data - Data Dictionary FY 2016 Alphabetic List of Variables and Attributes Standard Research File For a standard research file request one of three variables
Analysis of CAH Inpatient Hospitalizations and Transfers: Implications for National Quality Measurement and Reporting
 Flex Monitoring Team Briefing Paper No. 13 Analysis of CAH Inpatient Hospitalizations and Transfers: Implications for National Quality Measurement and Reporting October 2006 The Flex Monitoring Team is
Flex Monitoring Team Briefing Paper No. 13 Analysis of CAH Inpatient Hospitalizations and Transfers: Implications for National Quality Measurement and Reporting October 2006 The Flex Monitoring Team is
DOUBLE YOUR AMBULATORY PLATFORM
 KEY STRATEGIES TO DOUBLE YOUR AMBULATORY PLATFORM BY 2020 Chris Bishop CEO OUTPATIENT EXPANSION Healthcare market is at a tipping point Innovators are committing significant resources to outpatient growth
KEY STRATEGIES TO DOUBLE YOUR AMBULATORY PLATFORM BY 2020 Chris Bishop CEO OUTPATIENT EXPANSION Healthcare market is at a tipping point Innovators are committing significant resources to outpatient growth
Hu J, Gonsahn MD, Nerenz DR. Socioeconomic status and readmissions: evidence from an urban teaching hospital. Health Aff (Millwood). 2014;33(5).
. 2014;33(5).") Appendix Definitions of Index Admission and Readmission Definitions of index admission and readmission follow CMS hospital-wide all-cause unplanned readmission (HWR) measure as far as data are available.
Appendix Definitions of Index Admission and Readmission Definitions of index admission and readmission follow CMS hospital-wide all-cause unplanned readmission (HWR) measure as far as data are available.
How health plans can improve cancer care: from utilization management to delivery reform
 Quality health plans & benefits Healthier living Financial well being Intelligent solutions How health plans can improve cancer care: from utilization management to delivery reform Michael Kolodziej, M.D.,
Quality health plans & benefits Healthier living Financial well being Intelligent solutions How health plans can improve cancer care: from utilization management to delivery reform Michael Kolodziej, M.D.,
PA Optometric Association Annual Congress
 May 18, 2012 PA Optometric Association Annual Congress Andrew Bloschichak MD, MBA Senior Medical Director, Highmark Emerging Health Care Reform Delivery and Reimbursement Systems Introduction Key Drivers
May 18, 2012 PA Optometric Association Annual Congress Andrew Bloschichak MD, MBA Senior Medical Director, Highmark Emerging Health Care Reform Delivery and Reimbursement Systems Introduction Key Drivers
Getting to Safe, Affordable, Effective, Patient-Centered Care: Good Data Are Only the Beginning
 Getting to Safe, Affordable, Effective, Patient-Centered Care: Good Data Are Only the Beginning Dana Gelb Safran, Sc.D. Senior Vice President Performance Measurement & Improvement Transformation Vision:
Getting to Safe, Affordable, Effective, Patient-Centered Care: Good Data Are Only the Beginning Dana Gelb Safran, Sc.D. Senior Vice President Performance Measurement & Improvement Transformation Vision:
SCORES FOR 4 TH QUARTER, RD QUARTER, 2014
 SCORES FOR 4 TH QUARTER, 2013 3 RD QUARTER, 2014 PATIENT SATISFACTION SCORES (HCAHPS): 4 STARS OUT OF 5 (ONLY 4 AREA ACUTE CARE HOSPITALS RECEIVED A 4-STAR RATING. NONE ACHIEVED 5-STARS). STRUCTURAL MEASURES:
SCORES FOR 4 TH QUARTER, 2013 3 RD QUARTER, 2014 PATIENT SATISFACTION SCORES (HCAHPS): 4 STARS OUT OF 5 (ONLY 4 AREA ACUTE CARE HOSPITALS RECEIVED A 4-STAR RATING. NONE ACHIEVED 5-STARS). STRUCTURAL MEASURES:
Putting the Patient First: How Advocate Healthcare Reduced Readmissions, LOS and Costs Through an Integrated Nutrition Care Process
 Putting the Patient First: How Advocate Healthcare Reduced Readmissions, LOS and Costs Through an Integrated Nutrition Care Process Gretchen VanDerBosch, Senior Dietitian, Advocate Good Shepherd Hospital
Putting the Patient First: How Advocate Healthcare Reduced Readmissions, LOS and Costs Through an Integrated Nutrition Care Process Gretchen VanDerBosch, Senior Dietitian, Advocate Good Shepherd Hospital