Pathophysiology: Heart Failure. Objectives
|
|
|
- Roger Michael Jenkins
- 5 years ago
- Views:
Transcription
1 Pathophysiology: Heart Failure Mat Maurer, MD Associate Professor of Clinical Medicine Objectives At the conclusion of this seminar, learners will be able to: 1. Define heart failure as a clinical syndrome 2. Define and employ the terms preload, afterload, contractilty, remodeling, diastolic dysfunction, compliance, stiffness and capacitance. 3. Describe the classic pathophysiologic steps in the development of heart failure. 4. Delineate four basic mechanisms underlying the development of heart failure 5. Interpret pressure volume loops / Starling curves and identify contributing mechanisms for heart failure state. 6. Understand the common methods employed for classifying patients with heart failure. 7. Employ the classes and stages of heart failure in describing a clinical scenario 1
2 Heart Failure Not a disease A syndrome From "syn meaning "together and "dromos" meaning "a running. A group of signs and symptoms that occur together and characterize a particular abnormality. Diverse etiologies Several mechanisms Heart Failure: Definitions An inability of the heart to pump blood at a sufficient rate to meet the metabolic demands of the body (e.g. oxygen and cell nutrients) at rest and during effort or to do so only if the cardiac filling pressures are abnormally high. A complex clinical syndrome characterized by abnormalities in cardiac function and neurohormonal regulation, which are accompanied by effort intolerance, fluid retention and a reduced longevity A complex clinical syndrome that can result from any structural or functional cardiac disorder that impairs the ability of the ventricle to fill with or eject blood. 2


3 Epidemiology Heart Failure: The Problem Heart Failu re Patients in the U S (M illions) million in 1991, 4.7 million in 2000, estimated t 10 million in 2037 Incidence: 550,000 new cases/year Prevalence: 1% ages , >10% over age 80 More deaths from HF than from all forms of cancer combined Most common cause for hospitalization in age >65 Heart Failure Paradigms 3
4 Heart Failure: Classifications Right vs. Left Sided Cardiac vs. Non-cardiac Systolic vs. Diastolic Dilated vs. Hypertrophic vs. Restrcitive Heart Failure Compensated vs. Decompensated Acute vs. Chronic Forward vs. Backward High vs. Low Output Cardiac Muscle Function Preload Afterload Contractility Tension (g) d b a c Muscle Length (mm) Tension (g) b ΔL ΔL a d c a d Muscle Length (mm) Tension (g) +norepinephrine i f b g e a Muscle Length (mm) The length of a cardiac muscle fiber prior to the onset of contraction. The force against which a cardiac muscle fiber must shorten. The force of contraction independent of preload and afterload. Frank Starling Isotonic Contraction Inotropic State 4


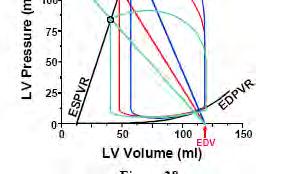
5 From Muscle to Chamber The Pressure Volume Loop astole Dia Systole 5
6 The Pressure Volume Loop P es Pressure Volume Compliance/Stiffness vs Capacitance 25 EDPVR LV Pressure (mmhg) Capacitance = volume at specified pressure LV Volume (ml) Slope = stiffness = 1/compliance LV Pressure (mmhg) 50 Diastolic Dysfunciton Normal LV Volume (ml) Remodeling 6
![Afterload (Arterial Properties) Ea (Arterial Elastance) If TPR = [MAP - CVP] /](/docs-images/91/107412034/images/7-1.jpg "CO, and CO = SV * HR Substituting the second equation into the first we obtain:")
![TPR = [MAP - CVP] / (SV*HR) Making two simplifying assumptions. 1.](/docs-images/91/107412034/images/7-2.jpg "CVP is negligible compared to MAP. 2.")
 Which can be rearranged to: Pes/SV TPR * HR.")

7 Afterload (Arterial Properties) Ea (Arterial Elastance) If TPR = [MAP - CVP] / CO, and CO = SV * HR Substituting the second equation into the first we obtain: TPR = [MAP - CVP] / (SV*HR) Making two simplifying assumptions. 1. CVP is negligible compared to MAP. 2. MAP is approximately equal to the end-systolic pressure in the ventricle (Pes). Then, TPR = Pes / (SV*HR) Which can be rearranged to: Pes/SV TPR * HR. Cardiac Chamber Function Preload Afterload Contractility EDV EDP Wall stress at end diastole Aortic Pressure Total peripheral resistance Arterial impedance Wall stress at end systole Pressure generated at given volume. Inotropic State 7

8 Frank Starling Curves Hypotension Pulmonary Congestion Pathophysiology - PV Loop 8
9 Pathophysiology of Heart Failure Myocardial Insult/Stimuli/Damage Pump dysfunction Activation i of neurohormones Catecholamines Angiontensin II Cytokines Remodeling Hypertrophy Fibrosis Apoptosis Neurohormonal Activation in Heart Failure Myocardial injury to the heart (CAD, HTN, CMP, valvular disease) Initial fall in LV performance, wall stress Activation of RAS and SNS Remodeling and progressive worsening of LV function Morbidity and mortality Arrhythmias Pump failure RAS, renin-angiotensin system; SNS, sympathetic nervous system. Fibrosis, apoptosis, hypertrophy, cellular/molecular alterations, myotoxicity Peripheral vasoconstriction Sodium retention Hemodynamic alterations ti Heart failure symptoms Fatigue Activity altered Chest congestion Edema Shortness of breath 9
10 Neurohormonal Activation in Heart Failure Angiotensin II Norepinephrine Hypertrophy, apoptosis, ischemia, arrhythmias, remodeling, fibrosis Morbidity and Mortality Adrenergic Pathway in Heart Failure Progression CNS sympathetic outflow Cardiac sympathetic activity Vascular sympathetic activity Renal sympathetic activity β 1 β 2 α 1 α 1 β 1 α 1 Myocyte hypertrophy Myocyte injury Increased arrhythmias Vasoconstriction Activation of RAS Sodium retention Disease progression 10
 Myocardial Toxicity Change in Gene")

11 Neurohormonal Balance in Heart Failure Neurohormones in Heart Failure Myocardial Injury Fall in LV Performance Activation of RAAS and SNS (endothelin, AVP, cytokines) Myocardial Toxicity Change in Gene Expression ANP BNP Peripheral Vasoconstriction Sodium/Water Retention Morbidity and Mortality Remodeling and Progressive Worsening of LV Function HF Symptoms Shah M et al. Rev Cardiovasc Med. 2001;2(suppl 2):S2 11
12 Pathophyisiology of myocardial remodeling: Insult / Remodeling Stimuli Wall Stress Cytokines Neurohormones Oxidative stress Increased Wall Stress Myocyte Hypertrophy Altered interstitial matrix Fetal Gene Expression Altered calcium handling proteins Myocyte Death Ventricular Enlargement Diastolic Dysfunction Systolic Dysfunction Response Acute and Chronic Responses Benefits and Harm Short-term Effects (mainly adaptive; hemorrhage, h acute heart failure) Long-term Effects (mainly deleterious; chronic heart tfailure) Salt and water retention Augments preload Pulmonary congestion, anasarca Vasoconstriction Maintains pressure for perfusion of vital organs (brain, heart) Exacerbates pump dysfunction, increases cardiac energy expenditure Sympathetic stimulation Increases heart rate and ejection Increases energy expenditure Cytokine activation Vasodilatation Skeletal muscle catabolism, deterioration of endothelial function, impaired contraction, LV remodeling. Hypertrophy Unloads individual muscle fibers Deterioration and death of cardiac cells: cardiomyopathy of overload Increased collagen May reduce dilatation Impairs relaxation 12

13 Laplace s Law Where P = ventricular pressure, r = ventricular chamber radius and h = ventricular wall thickness h Remodeling Concentric vs. Eccentric 13

 3.")
14 Ventricular Remodeling Pathophysiology of Heart Failure Four Basic Mechanisms 1. Increased Blood Volume (Excessive Preload) 2. Increased Resistant to Blood Flow (Excessive Afterload) 3. Decreased contractility 4. Decreased Filling 14
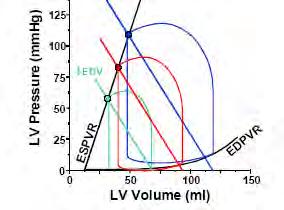
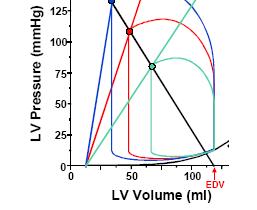
15 Aortic Regurgitation Increased Blood Volume AI + Neurohormones AI + Remodeling Na Retention Vasoconstriction Ventricular Remodeling Etiologies Mitral Regurgitation Aortic Regurgitation Volume Overload Left to Right Shunts Chronic Kidney Disease Parameter Normal AI AI+Neuro- Hormones BP (mm Hg) 140/75 128/50 130/50 SV (ml) Cardiac Output (L/min) PCWP (mm Hg) AI + Remodeling 104/ Hypertension Increased Afterload HTN + DD HTN + DD + HF Ea Diastolic Dysfunction Na Retention Vasoconstriction Remodeling Etiologies Parameter Normal HTN BP (mm Hg) 131/76 150/100 Aortic Stenosis Aortic Coarctation Hypertension SV (ml) Cardiac Output (L/min) PCWP (mm Hg) HTN + DD 140/ HTN + Heart failure 161/
16 Decreased Contractility MI MI + Heart Failure MI + Remodeling Na Retention Vasoconstriction Ventricular Remodeling Etiologies Ischemic Cardiomyopathy MI + Myocardial Infarction Parameter Normal MI Neurohormones Myocardial Ischemia BP (mm Hg) 124/81 80/40 90/54 Myocarditis SV (ml) Toxins 46 Anthracycline Cardiac Output (L/min) Alcohol PCWP (mm Hg) Cocaine 25 MI + Remodeling dli 87/ Decreased Filling Normal HCM HCM + HF Ventricular Remodeling Na Retention Vasoconstriction Etiologies Mitral Stenosis Constriction Restrictive Cardiomypoathy Cardiac Tamponade Hypertrophic Cardiomyopathy Infiltrative Cardiomyopathy Parameter Normal HCM HCM + HF BP (mm Hg) 124/81 95/47 105/53 SV (ml) Cardiac Output (L/min) PCWP (mm Hg)
17 Part II Heart Failure: Classifications Right vs. Left Sided Cardiac vs. Non-cardiac Systolic vs. Diastolic Dilated vs. Hypertrophic vs. Restrcitive Heart Failure Compensated vs. Decompensated Acute vs. Chronic Forward vs. Backward High vs. Low Output 17


18 Types of Heart Failure SHF Diastolic Pth Pathophysiologyh il Impaired Contraction Impaired filling Demographics All ages > 60 years 1 Cause Coronary Artery Disease Hypertension Systolic Versus Diastolic Failure Systolic Dysfunction Contractility Normal Diastolic Dysfunction essure essure essure Capacitance Pr Pr Pr Volume Volume Volume 18
19 Systolic Versus Diastolic Failure Heart Failure: Classifications Right vs. Left Sided Cardiac vs. Non-cardiac Systolic vs. Diastolic Dilated vs. Hypertrophic vs. Restrcitive Heart Failure Compensated vs. Decompensated Acute vs. Chronic Forward vs. Backward High vs. Low Output 19

20 Decompensated Heart Failure Heart Failure: Classifications Right vs. Left Sided Cardiac vs. Non-cardiac Systolic vs. Diastolic Dilated vs. Hypertrophic vs. Restrictive Heart Failure Compensated vs. Decompensated Acute vs. Chronic Forward vs. Backward High vs. Low Output 20

21 High vs. Low Output Failure Causes: Anemia Systemic arteriovenous fistulas Hyperthyroidism Beriberi heart disease Paget disease of bone Glomerulonephritis Polycythemia vera Carcinoid syndrome Obesity Anemia Multiple myeloma Pregnancy Cor pulmonale Polycythemia vera Heart Failure: Classifications Right vs. Left Sided Cardiac vs. Non-cardiac Systolic vs. Diastolic Dilated vs. Hypertrophic vs. Restrictive Heart Failure Compensated vs. Decompensated Acute vs. Chronic Forward vs. Backward High vs. Low Output 21
22 Dilated vs. Hypertrophic vs. Restrictive Type Definition Sample Etiologies Dilated Hypertrophic Dilated left/both ventricle(s) with impaired contraction Left and/or right ventricular hypertrophy Ischemic, idiopathic, familial, viral, alcoholic, toxic, valvular Familial with autosomal dominant inheritance Restrictive Restrictive filling and Idiopathic, amyloidosis, reduced diastolic filling of one/both ventricles, Normal/near normal systolic function endomyocardial fibrosis Dilated vs. Hypertrophic vs. Restrictive 22





23 Clinical Manifestations Symptoms Rd Reduced dexercise tolerance Shortness of breath Congestion Fluid retention Difficulty in sleeping Weight loss Diagnosis of heart failure Physical examination Chest X ray EKG Echocardiogram Blood tests: Na, BUN, Creatinine, BNP Exercise test MRI Cardiac catheterization 23
24 I II III IV Class Mild Mild Moderate Severe NYHA Classification Patient Symptoms No limitation of physical activity No undue fatigue, palpitation or dyspnea Slight limitation of physical activity Comfortable at rest Less than ordinary activity results in fatigue, palpitation, or dyspnea Marked limitation of physical activity Comfortable at rest Less than ordinary activity results in fatigue, palpitation, or dyspnea Unable to carry out any physical activity without discomfort Symptoms of cardiac insufficiency at rest Physical activity causes increased discomfort ACC/AHA Staging System STAGE A High risk for developing HF STAGE B Asymptomatic LV dysfunction STAGE C Past or current symptoms of HF STAGE D End-stage HF Hunt, et al. J Am Coll Cardiol. 2001; 38:
25 ACC/AHA Staging System Stage High risk for A developing heart failure B C D Asymptomatic heart failure Symptomatic heart failure Refractory end-stage heart failure Patient Description Hypertension Coronary artery disease Diabetes mellitus Family history of cardiomyopathy Previous myocardial infarction Left ventricular systolic dysfunction Asymptomatic valvular disease Known structural heart disease Shortness of breath and fatigue Reduced exercise tolerance Marked symptoms at rest despite maximal medical therapy (e.g., those who are recurrently hospitalized or cannot be safely discharged from the hospital without specialized interventions) Goals of Treatment 1. Identification and correction of underlying condition causing heart failure. 2. Elimination of acute precipitating cause of symptoms. 3. Modulation of neurohormonal response to prevent progression of disease. 4. Improve long term survival. 25
26 Etiologies Ischemic cardiomyopathy Valvular cardiomyopathy Hypertensive cardiomyopathy. Inflammatory cardiomyopathy Metabolic cardiomyopathy General system disease Muscular dystrophies. Neuromuscular disorders. Sensitivity and toxic reactions. Peripartal cardiomyopathy Percipients /Associated Factors Inappropriate reduction in the intensity of treatment, including Dietary sodium restriction, Physical activity reduction, Drug regimen reduction, or, most commonly, a combination of these measures. Ischemia Hypertension Anemia Vl Volume Overload Increased Metabolic Demand Infection Thyroid Disease Arrhythmia Asthma/COPD 26
")
 dysfunction (systolic) present Asymptomatic valvular disease OPT Known structural heart disease ICD Shortness if LV dysfunction of breath and (systolic)")
27 Targets of Treatment Standard Pharmacological Therapy ACE inhibitors Angiotensin Receptor Blockers Beta Blcokers Diuretics Aldosterone Antagonists Statins Vasodilators Inotropes Treatment A B C D Stage High risk for developing heart failure Asymptomatic heart failure Symptomatic heart failure Refractory end-stage heart failure Patient Treatment Hypertension Optimal pharmacologic therapy (OPT) Aspirin, Coronary ACE artery inhibitors, disease statins, b-blockers, a-b-blockers Diabetes mellitus (carvedilol) diabetic therapy Family history of cardiomyopathy OPT Previous myocardial infarction ICD Left if left ventricular systolic (LV) dysfunction (systolic) present Asymptomatic valvular disease OPT Known structural heart disease ICD Shortness if LV dysfunction of breath and (systolic) fatigue present CRT Reduced (if QRS exercise wide, LVEF 35%) tolerance OPT Marked symptoms at rest despite maximal Intermittent medical therapy IV inotropes (e.g., those who are recurrently ICD hospitalized as a bridge or to cannot transplantation be safely discharged from CRT the hospital without specialized interventions) Other devices (LVAD, pericardial restraint) 27



28 Treatment of Acute Heart Failure ACC/AHA Staging System 28
29 Summary Complex Clinical Syndrome Multiple Etiologies and Classification Systems Physiologic Understanding Essential /it /h / di l/h t i / 29
Outline. Pathophysiology: Heart Failure. Heart Failure. Heart Failure: Definitions. Etiologies. Etiologies
 Outline Pathophysiology: Mat Maurer, MD Irving Assistant Professor of Medicine Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology : Definitions An inability of the
Outline Pathophysiology: Mat Maurer, MD Irving Assistant Professor of Medicine Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology : Definitions An inability of the
Pathophysiology: Heart Failure
 Pathophysiology: Heart Failure Mat Maurer, MD Irving Assistant Professor of Medicine Outline Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology Heart Failure: Definitions
Pathophysiology: Heart Failure Mat Maurer, MD Irving Assistant Professor of Medicine Outline Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology Heart Failure: Definitions
Pathophysiology: Heart Failure. Objectives
 Pathophysiology: Heart Failure Mat Maurer, MD Irving Assistant Professor of Clinical Medicine Objectives At the conclusion of this seminar, learner will be able to: 1. Define heart failure as a clinical
Pathophysiology: Heart Failure Mat Maurer, MD Irving Assistant Professor of Clinical Medicine Objectives At the conclusion of this seminar, learner will be able to: 1. Define heart failure as a clinical
Copyright 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. Normal Cardiac Anatomy
 Mosby,, an affiliate of Elsevier Normal Cardiac Anatomy Impaired cardiac pumping Results in vasoconstriction & fluid retention Characterized by ventricular dysfunction, reduced exercise tolerance, diminished
Mosby,, an affiliate of Elsevier Normal Cardiac Anatomy Impaired cardiac pumping Results in vasoconstriction & fluid retention Characterized by ventricular dysfunction, reduced exercise tolerance, diminished
Heart Failure. Cardiac Anatomy. Functions of the Heart. Cardiac Cycle/Hemodynamics. Determinants of Cardiac Output. Cardiac Output
 Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
Definition of Congestive Heart Failure
 Heart Failure Definition of Congestive Heart Failure A clinical syndrome of signs & symptoms resulting from the heart s inability to supply adequate tissue perfusion. CHF Epidemiology Affects 4.7 million
Heart Failure Definition of Congestive Heart Failure A clinical syndrome of signs & symptoms resulting from the heart s inability to supply adequate tissue perfusion. CHF Epidemiology Affects 4.7 million
Improving Transition of Care in Congestive Heart Failure. Mark J. Gloth, DO, MBA. Vice President, Chief Medical Officer HCR ManorCare
 Improving Transition of Care in Congestive Heart Failure Mark J. Gloth, DO, MBA. Vice President, Chief Medical Officer HCR ManorCare Heart Failure Fastest growing clinical cardiac disease in the United
Improving Transition of Care in Congestive Heart Failure Mark J. Gloth, DO, MBA. Vice President, Chief Medical Officer HCR ManorCare Heart Failure Fastest growing clinical cardiac disease in the United
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
In Vivo Animal Models of Heart Disease. Why Animal Models of Disease? Timothy A Hacker, PhD Department of Medicine University of Wisconsin-Madison
 In Vivo Animal Models of Heart Disease Timothy A Hacker, PhD Department of Medicine University of Wisconsin-Madison Why Animal Models of Disease? Heart Failure (HF) Leading cause of morbidity and mortality
In Vivo Animal Models of Heart Disease Timothy A Hacker, PhD Department of Medicine University of Wisconsin-Madison Why Animal Models of Disease? Heart Failure (HF) Leading cause of morbidity and mortality
Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept
 Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept (MBBS)(SBMD) Introduction Epidemiology Pathophysiology diastolic/systolic Risk factors Signs and symptoms Classification of HF
Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept (MBBS)(SBMD) Introduction Epidemiology Pathophysiology diastolic/systolic Risk factors Signs and symptoms Classification of HF
Circulation. Blood Pressure and Antihypertensive Medications. Venous Return. Arterial flow. Regulation of Cardiac Output.
 Circulation Blood Pressure and Antihypertensive Medications Two systems Pulmonary (low pressure) Systemic (high pressure) Aorta 120 mmhg Large arteries 110 mmhg Arterioles 40 mmhg Arteriolar capillaries
Circulation Blood Pressure and Antihypertensive Medications Two systems Pulmonary (low pressure) Systemic (high pressure) Aorta 120 mmhg Large arteries 110 mmhg Arterioles 40 mmhg Arteriolar capillaries
HEART FAILURE PHARMACOLOGY. University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 HEART FAILURE PHARMACOLOGY University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 LEARNING OBJECTIVES Understand the effects of heart failure in the body
HEART FAILURE PHARMACOLOGY University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 LEARNING OBJECTIVES Understand the effects of heart failure in the body
Images have been removed from the PowerPoint slides in this handout due to copyright restrictions.
 Heart Failure Heart Failure Introduction and History AHA 2015 Statistics About 6 million Americans 870,000 new cases each year 1 in 9 deaths related to HF Almost 1 million hospitalizations each year (cost
Heart Failure Heart Failure Introduction and History AHA 2015 Statistics About 6 million Americans 870,000 new cases each year 1 in 9 deaths related to HF Almost 1 million hospitalizations each year (cost
Pre-discussion questions
 Amanda Bartlett, PA-C Dustin Bartlett, PA-C Andrea Applegate, PA-C Leslie Yearta Brown, NP CHF Round Table Discussion Objectives ANDREA- Discuss the definition and different categories of CHF DUSTIN- Define
Amanda Bartlett, PA-C Dustin Bartlett, PA-C Andrea Applegate, PA-C Leslie Yearta Brown, NP CHF Round Table Discussion Objectives ANDREA- Discuss the definition and different categories of CHF DUSTIN- Define
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Review of Cardiac Mechanics & Pharmacology 10/23/2016. Brent Dunworth, CRNA, MSN, MBA 1. Learning Objectives
 Brent Dunworth, CRNA, MSN, MBA Associate Director of Advanced Practice Division Chief, Nurse Anesthesia Vanderbilt University Medical Center Nashville, Tennessee Learning Objectives Review the principles
Brent Dunworth, CRNA, MSN, MBA Associate Director of Advanced Practice Division Chief, Nurse Anesthesia Vanderbilt University Medical Center Nashville, Tennessee Learning Objectives Review the principles
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Nora Goldschlager, M.D. SFGH Division of Cardiology UCSF
 CLASSIFICATION OF HEART FAILURE Nora Goldschlager, M.D. SFGH Division of Cardiology UCSF DISCLOSURES: NONE CLASSIFICATION C OF HEART FAILURE NYHA I IV New paradigm Stage A: Pts at high risk of developing
CLASSIFICATION OF HEART FAILURE Nora Goldschlager, M.D. SFGH Division of Cardiology UCSF DISCLOSURES: NONE CLASSIFICATION C OF HEART FAILURE NYHA I IV New paradigm Stage A: Pts at high risk of developing
Diastolic Heart Failure. Edwin Tulloch-Reid MBBS FACC Consultant Cardiologist Heart Institute of the Caribbean December 2012
 Diastolic Heart Failure Edwin Tulloch-Reid MBBS FACC Consultant Cardiologist Heart Institute of the Caribbean December 2012 Disclosures Have spoken for Merck, Sharpe and Dohme Sat on a physician advisory
Diastolic Heart Failure Edwin Tulloch-Reid MBBS FACC Consultant Cardiologist Heart Institute of the Caribbean December 2012 Disclosures Have spoken for Merck, Sharpe and Dohme Sat on a physician advisory
Congestive Heart Failure Patient Profile. Patient Identity - Mr. Douglas - 72 year old man - No drugs, smokes, moderate social alcohol consumption
 Congestive Heart Failure Patient Profile Patient Identity - Mr. Douglas - 72 year old man - No drugs, smokes, moderate social alcohol consumption Chief Complaint - SOB - When asked: Increasing difficulty
Congestive Heart Failure Patient Profile Patient Identity - Mr. Douglas - 72 year old man - No drugs, smokes, moderate social alcohol consumption Chief Complaint - SOB - When asked: Increasing difficulty
HFpEF. April 26, 2018
 HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
Topic Page: congestive heart failure
 Topic Page: congestive heart failure Definition: congestive heart f ailure from Merriam-Webster's Collegiate(R) Dictionary (1930) : heart failure in which the heart is unable to maintain an adequate circulation
Topic Page: congestive heart failure Definition: congestive heart f ailure from Merriam-Webster's Collegiate(R) Dictionary (1930) : heart failure in which the heart is unable to maintain an adequate circulation
Estimated 5.7 million Americans with HF. 915, 000 new HF cases annually, HF incidence approaches
 Heart Failure: Management of a Chronic Disease Jenny Bauerly RN, CHFN, APRN-BC Heart Failure (HF) Definition A complex clinical syndrome that can result from any structural or functional cardiac disorder
Heart Failure: Management of a Chronic Disease Jenny Bauerly RN, CHFN, APRN-BC Heart Failure (HF) Definition A complex clinical syndrome that can result from any structural or functional cardiac disorder
Cardiac Output MCQ. Professor of Cardiovascular Physiology. Cairo University 2007
 Cardiac Output MCQ Abdel Moniem Ibrahim Ahmed, MD Professor of Cardiovascular Physiology Cairo University 2007 90- Guided by Ohm's law when : a- Cardiac output = 5.6 L/min. b- Systolic and diastolic BP
Cardiac Output MCQ Abdel Moniem Ibrahim Ahmed, MD Professor of Cardiovascular Physiology Cairo University 2007 90- Guided by Ohm's law when : a- Cardiac output = 5.6 L/min. b- Systolic and diastolic BP
A Guide to the Etiology, Pathophysiology, Diagnosis, and Treatment of Heart Failure. Part I: Etiology and Pathophysiology of Heart Failure
 A Guide to the Etiology, Pathophysiology, Diagnosis, and Treatment of Heart Failure Dr Badri Paudel GMC Part I: Etiology and Pathophysiology of Heart Failure Heart Failure (HF) Definition A complex clinical
A Guide to the Etiology, Pathophysiology, Diagnosis, and Treatment of Heart Failure Dr Badri Paudel GMC Part I: Etiology and Pathophysiology of Heart Failure Heart Failure (HF) Definition A complex clinical
Diagnosis & Management of Heart Failure. Abena A. Osei-Wusu, M.D. Medical Fiesta
 Diagnosis & Management of Heart Failure Abena A. Osei-Wusu, M.D. Medical Fiesta Learning Objectives: 1) Become familiar with pathogenesis of congestive heart failure. 2) Discuss clinical manifestations
Diagnosis & Management of Heart Failure Abena A. Osei-Wusu, M.D. Medical Fiesta Learning Objectives: 1) Become familiar with pathogenesis of congestive heart failure. 2) Discuss clinical manifestations
M2 TEACHING UNDERSTANDING PHARMACOLOGY
 M2 TEACHING UNDERSTANDING PHARMACOLOGY USING CVS SYSTEM AS AN EXAMPLE NIGEL FONG 2 JAN 2014 TODAY S OBJECTIVE Pharmacology often seems like an endless list of mechanisms and side effects to memorize. To
M2 TEACHING UNDERSTANDING PHARMACOLOGY USING CVS SYSTEM AS AN EXAMPLE NIGEL FONG 2 JAN 2014 TODAY S OBJECTIVE Pharmacology often seems like an endless list of mechanisms and side effects to memorize. To
Incidence. 4.8 million in the United States. 400,000 new cases/year. 20 million patients with asymptomatic LV dysfunction
 Heart Failure Diagnosis According to the Working Group in Heart Failure, CHF is a syndrome where the diagnosis has the following essential components: A combination of: Symptoms, typically breathlessness
Heart Failure Diagnosis According to the Working Group in Heart Failure, CHF is a syndrome where the diagnosis has the following essential components: A combination of: Symptoms, typically breathlessness
Ventricular Assist Device: Are Early Interventions Superior? Hamang Patel, MD Section of Cardiomyopathy & Heart Transplantation
 Ventricular Assist Device: Are Early Interventions Superior? Hamang Patel, MD Section of Cardiomyopathy & Heart Transplantation Objectives Current rationale behind use of MCS Patient Selection Earlier?
Ventricular Assist Device: Are Early Interventions Superior? Hamang Patel, MD Section of Cardiomyopathy & Heart Transplantation Objectives Current rationale behind use of MCS Patient Selection Earlier?
The Failing Heart in Primary Care
 The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
Advanced Care for Decompensated Heart Failure
 Advanced Care for Decompensated Heart Failure Sara Kalantari MD Assistant Professor of Medicine, University of Chicago Advanced Heart Failure, Mechanical Circulatory Support and Cardiac Transplantation
Advanced Care for Decompensated Heart Failure Sara Kalantari MD Assistant Professor of Medicine, University of Chicago Advanced Heart Failure, Mechanical Circulatory Support and Cardiac Transplantation
Heart Failure. Dr. William Vosik. January, 2012
 Heart Failure Dr. William Vosik January, 2012 Questions for clinicians to ask Is this heart failure? What is the underlying cause? What are the associated disease processes? Which evidence-based treatment
Heart Failure Dr. William Vosik January, 2012 Questions for clinicians to ask Is this heart failure? What is the underlying cause? What are the associated disease processes? Which evidence-based treatment
Cardiac Output (C.O.) Regulation of Cardiac Output
 Regulation of Cardiac Output") Cardiac Output (C.O.) Is the volume of the blood pumped by each ventricle per minute (5 Litre) Stroke volume: Is the volume of the blood pumped by each ventricle per beat. Stroke volume = End diastolic
Cardiac Output (C.O.) Is the volume of the blood pumped by each ventricle per minute (5 Litre) Stroke volume: Is the volume of the blood pumped by each ventricle per beat. Stroke volume = End diastolic
Definition: A state in which the heart cannot provide sufficient cardiac output to satisfy the metabolic needs of the body
 Definition: A state in which the heart cannot provide sufficient cardiac output to satisfy the metabolic needs of the body HF is a complex clinical syndrome that can result from any structural or functional
Definition: A state in which the heart cannot provide sufficient cardiac output to satisfy the metabolic needs of the body HF is a complex clinical syndrome that can result from any structural or functional
Innovation therapy in Heart Failure
 Innovation therapy in Heart Failure P. Laothavorn September 2015 Topics of discussion Basic Knowledge about heart failure Standard therapy New emerging therapy References: standard Therapy in Heart Failure
Innovation therapy in Heart Failure P. Laothavorn September 2015 Topics of discussion Basic Knowledge about heart failure Standard therapy New emerging therapy References: standard Therapy in Heart Failure
CARDIOGENIC SHOCK. Antonio Pesenti. Università degli Studi di Milano Bicocca Azienda Ospedaliera San Gerardo Monza (MI)
") CARDIOGENIC SHOCK Antonio Pesenti Università degli Studi di Milano Bicocca Azienda Ospedaliera San Gerardo Monza (MI) Primary myocardial dysfunction resulting in the inability of the heart to mantain an
CARDIOGENIC SHOCK Antonio Pesenti Università degli Studi di Milano Bicocca Azienda Ospedaliera San Gerardo Monza (MI) Primary myocardial dysfunction resulting in the inability of the heart to mantain an
Heart Failure. Subjective SOB (shortness of breath) Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)
 Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)") Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
Heart Failure Overview. Dr Chris K Y Wong
 Heart Failure Overview Dr Chris K Y Wong Heart Failure: A Growing, Global Health Issue Heart Failure 23 Million Afflicted Global Impact Worldwide ~23 million peopleworldwide afflicted with CHF 1 Exceeds
Heart Failure Overview Dr Chris K Y Wong Heart Failure: A Growing, Global Health Issue Heart Failure 23 Million Afflicted Global Impact Worldwide ~23 million peopleworldwide afflicted with CHF 1 Exceeds
Advanced Pathophysiology Unit 5 CV Page 1 of 24. Learning Objectives:
 Advanced Pathophysiology Unit 5 CV Page 1 of 24 Learning Objectives: 1) What is the definition of HF? How can we get it? Is it just the failing heart? 2) AHA/ACC stages of HF compared to older NYHA classes
Advanced Pathophysiology Unit 5 CV Page 1 of 24 Learning Objectives: 1) What is the definition of HF? How can we get it? Is it just the failing heart? 2) AHA/ACC stages of HF compared to older NYHA classes
HEART FAILURE. Heart Failure in the US. Heart Failure (HF) 3/2/2014
 3/2/2014") HEART FAILURE Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center March 2014 Heart Failure in the US Prevalence - ~5 million 650,000 new cases annually 300,000 deaths annually Leading
HEART FAILURE Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center March 2014 Heart Failure in the US Prevalence - ~5 million 650,000 new cases annually 300,000 deaths annually Leading
Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year
![Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year](/thumbs/76/74263761.jpg "Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year") PAST MEDICAL HISTORY Has the subject had a prior episode of heart failure? o Does the subject have a prior history of exposure to cardiotoxins, such as anthracyclines? URGENT HEART FAILURE VISIT Did heart
PAST MEDICAL HISTORY Has the subject had a prior episode of heart failure? o Does the subject have a prior history of exposure to cardiotoxins, such as anthracyclines? URGENT HEART FAILURE VISIT Did heart
Medical Treatment for acute Decompensated Heart Failure. Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011
 Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
Heart failure. Failure? blood supply insufficient for body needs. CHF = congestive heart failure. increased blood volume, interstitial fluid
 Failure? blood supply insufficient for body needs CHF = congestive heart failure increased blood volume, interstitial fluid Underlying causes/risk factors Ischemic heart disease (CAD) 70% hypertension
Failure? blood supply insufficient for body needs CHF = congestive heart failure increased blood volume, interstitial fluid Underlying causes/risk factors Ischemic heart disease (CAD) 70% hypertension
CHF is a clinical syndrome in which heart failure is accompanied by symptoms and signs of pulmonary and/or peripheral congestion
 Congestive Heart Failure Lokesh Tejwani, MD Heart Failure A patho-physiological state in which abnormality of cardiac function is responsible for failure of the heart to pump blood at a rate commensurate
Congestive Heart Failure Lokesh Tejwani, MD Heart Failure A patho-physiological state in which abnormality of cardiac function is responsible for failure of the heart to pump blood at a rate commensurate
Objectives. Systolic Heart Failure: Definitions. Heart Failure: Historical Perspective 2/7/2009
 Objectives Diastolic Heart Failure and Indications for Echocardiography in the Asian Population Damon M. Kwan, MD UCSF Asian Heart & Vascular Symposium 02.07.09 Define diastolic heart failure and differentiate
Objectives Diastolic Heart Failure and Indications for Echocardiography in the Asian Population Damon M. Kwan, MD UCSF Asian Heart & Vascular Symposium 02.07.09 Define diastolic heart failure and differentiate
The right heart: the Cinderella of heart failure
 The right heart: the Cinderella of heart failure Piotr Ponikowski, MD, PhD, FESC Medical University, Centre for Heart Disease Clinical Military Hospital Wroclaw, Poland none Disclosure Look into the Heart
The right heart: the Cinderella of heart failure Piotr Ponikowski, MD, PhD, FESC Medical University, Centre for Heart Disease Clinical Military Hospital Wroclaw, Poland none Disclosure Look into the Heart
LXIV: DRUGS: 4. RAS BLOCKADE
 LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
Presenter: Steven Brust, HCS-D, HCS-H Product Manager, Home Health Coding Center
 Presenter: Steven Brust, HCS-D, HCS-H Product Manager, Home Health Coding Center Pinpoint & properly assign the appropriate heart failure codes Left- vs. Right-sided Left ventricular failure (LVF) may
Presenter: Steven Brust, HCS-D, HCS-H Product Manager, Home Health Coding Center Pinpoint & properly assign the appropriate heart failure codes Left- vs. Right-sided Left ventricular failure (LVF) may
Dysrhythmias. Dysrythmias & Anti-Dysrhythmics. EKG Parameters. Dysrhythmias. Components of an ECG Wave. Dysrhythmias
 Dysrhythmias Dysrythmias & Anti-Dysrhythmics Rhythm bad in the heart: Whitewater rafting Electrical impulses coordinate heart Reduction in Cardiac Output PEA Asystole Components of an ECG Wave EKG Parameters
Dysrhythmias Dysrythmias & Anti-Dysrhythmics Rhythm bad in the heart: Whitewater rafting Electrical impulses coordinate heart Reduction in Cardiac Output PEA Asystole Components of an ECG Wave EKG Parameters
Summary/Key Points Introduction
 Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital
 LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
CKD Satellite Symposium
 CKD Satellite Symposium Recommended Therapy by Heart Failure Stage AHA/ACC Task Force on Practice Guideline 2001 Natural History of Heart Failure Patients surviving % Mechanism of death Sudden death 40%
CKD Satellite Symposium Recommended Therapy by Heart Failure Stage AHA/ACC Task Force on Practice Guideline 2001 Natural History of Heart Failure Patients surviving % Mechanism of death Sudden death 40%
Heart Failure. Acute. Plasma [NE] (pg/ml) 24 Hours. Chronic
![Heart Failure. Acute. Plasma [NE] (pg/ml) 24 Hours. Chronic](/thumbs/90/103241154.jpg "Heart Failure. Acute. Plasma [NE] (pg/ml) 24 Hours. Chronic") Heart Failure Heart failure is the inability of the heart to deliver sufficient blood to the tissues to ensure adequate oxygen supply. Clinically it is characterized by signs of volume overload or symptoms
Heart Failure Heart failure is the inability of the heart to deliver sufficient blood to the tissues to ensure adequate oxygen supply. Clinically it is characterized by signs of volume overload or symptoms
The Causes of Heart Failure
 The Causes of Heart Failure Andy Birchall HFSN Right heart failure LVSD - HFREF Valve regurgitation or stenosis Dropsy CCF congestive cardiac failure Cor pulmonale Pulmonary hypertension HFPEF LVF Definitions
The Causes of Heart Failure Andy Birchall HFSN Right heart failure LVSD - HFREF Valve regurgitation or stenosis Dropsy CCF congestive cardiac failure Cor pulmonale Pulmonary hypertension HFPEF LVF Definitions
Cardiomyopathy. Jeff Grubbe MD FACP, Chief Medical Director, Allstate Life & Retirement
 Cardiomyopathy Jeff Grubbe MD FACP, Chief Medical Director, Allstate Life & Retirement Nebraska Home Office Life Underwriters Association March 20, 2018 1 Cardiomyopathy A myocardial disorder in which
Cardiomyopathy Jeff Grubbe MD FACP, Chief Medical Director, Allstate Life & Retirement Nebraska Home Office Life Underwriters Association March 20, 2018 1 Cardiomyopathy A myocardial disorder in which
Etiology, Classification & Management. Sheba Medical Center Cardiology Department Matthew Wright St. George s University of London
 Etiology, Classification & Management Sheba Medical Center Cardiology Department Matthew Wright St. George s University of London Introduction World Health Organization (1995): Diseases of myocardium (heart
Etiology, Classification & Management Sheba Medical Center Cardiology Department Matthew Wright St. George s University of London Introduction World Health Organization (1995): Diseases of myocardium (heart
4/11/2017. Cardiomyopathy. John Steuter, MD Bryan Heart. Disclosures. No Conflicts. Cardiomyopathy. WHO Classification
 Cardiomyopathy John Steuter, MD Bryan Heart Disclosures No Conflicts Cardiomyopathy WHO Classification Anatomy & physiology of the LV 1. Dilated Enlarged Systolic dysfunction 2. Hypertrophic Thickened
Cardiomyopathy John Steuter, MD Bryan Heart Disclosures No Conflicts Cardiomyopathy WHO Classification Anatomy & physiology of the LV 1. Dilated Enlarged Systolic dysfunction 2. Hypertrophic Thickened
THE CARDIOVASCULAR SYSTEM
 THE CARDIOVASCULAR SYSTEM AND RESPONSES TO EXERCISE Mr. S. Kelly PSK 4U North Grenville DHS THE HEART: A REVIEW Cardiac muscle = myocardium Heart divided into two sides, 4 chambers (L & R) RS: pulmonary
THE CARDIOVASCULAR SYSTEM AND RESPONSES TO EXERCISE Mr. S. Kelly PSK 4U North Grenville DHS THE HEART: A REVIEW Cardiac muscle = myocardium Heart divided into two sides, 4 chambers (L & R) RS: pulmonary
RV dysfunction and failure PATHOPHYSIOLOGY. Adam Torbicki MD, Dept Chest Medicine Institute of Tuberculosis and Lung Diseases Warszawa, Poland
 RV dysfunction and failure PATHOPHYSIOLOGY Adam Torbicki MD, Dept Chest Medicine Institute of Tuberculosis and Lung Diseases Warszawa, Poland Normal Right Ventricle (RV) Thinner wall Weaker myocytes Differences
RV dysfunction and failure PATHOPHYSIOLOGY Adam Torbicki MD, Dept Chest Medicine Institute of Tuberculosis and Lung Diseases Warszawa, Poland Normal Right Ventricle (RV) Thinner wall Weaker myocytes Differences
Introduction. Invasive Hemodynamic Monitoring. Determinants of Cardiovascular Function. Cardiovascular System. Hemodynamic Monitoring
 Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Akash Ghai MD, FACC February 27, No Disclosures
 Akash Ghai MD, FACC February 27, 2015 No Disclosures Epidemiology Lifetime risk is > 20% for American s older than 40 years old. > 650,000 new cases diagnosed each year. Incidence increases with age: 2%
Akash Ghai MD, FACC February 27, 2015 No Disclosures Epidemiology Lifetime risk is > 20% for American s older than 40 years old. > 650,000 new cases diagnosed each year. Incidence increases with age: 2%
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE
 DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Congestive Heart Failure: Outpatient Management
 The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
Drugs Used in Heart Failure. Assistant Prof. Dr. Najlaa Saadi PhD pharmacology Faculty of Pharmacy University of Philadelphia
 Drugs Used in Heart Failure Assistant Prof. Dr. Najlaa Saadi PhD pharmacology Faculty of Pharmacy University of Philadelphia Heart Failure Heart failure (HF), occurs when cardiac output is inadequate to
Drugs Used in Heart Failure Assistant Prof. Dr. Najlaa Saadi PhD pharmacology Faculty of Pharmacy University of Philadelphia Heart Failure Heart failure (HF), occurs when cardiac output is inadequate to
HEART FAILURE. Study day November 2018 Sarah Briggs
 HEART FAILURE Study day November 2018 Sarah Briggs Overview and Introduction This course is an introduction and overview of heart failure. Normal heart function and basic pathophysiology of heart failure
HEART FAILURE Study day November 2018 Sarah Briggs Overview and Introduction This course is an introduction and overview of heart failure. Normal heart function and basic pathophysiology of heart failure
Intravenous Inotropic Support an Overview
 Intravenous Inotropic Support an Overview Shaul Atar, MD Western Galilee Medical Center, Nahariya Affiliated with the Faculty of Medicine of the Galilee, Safed, Israel INOTROPES in Acute HF (not vasopressors)
Intravenous Inotropic Support an Overview Shaul Atar, MD Western Galilee Medical Center, Nahariya Affiliated with the Faculty of Medicine of the Galilee, Safed, Israel INOTROPES in Acute HF (not vasopressors)
5 Important Things to Know About Heart Failure. Kia Afshar, MD
 5 Important Things to Know About Heart Failure Kia Afshar, MD Disclosures I have no conflicts of interest to disclose I will not be discussing any off label medications and/or devices Objectives 1) Understand
5 Important Things to Know About Heart Failure Kia Afshar, MD Disclosures I have no conflicts of interest to disclose I will not be discussing any off label medications and/or devices Objectives 1) Understand
Peripartum Cardiomyopathy. Lavanya Rai Manipal
 Peripartum Cardiomyopathy Lavanya Rai Manipal Definition - PPCM - Dilated cardiomyopathy of unknown cause resulting in cardiac failure that occurs in the peripartum period in women without any preexisting
Peripartum Cardiomyopathy Lavanya Rai Manipal Definition - PPCM - Dilated cardiomyopathy of unknown cause resulting in cardiac failure that occurs in the peripartum period in women without any preexisting
During exercise the heart rate is 190 bpm and the stroke volume is 115 ml/beat. What is the cardiac output?
 The Cardiovascular System Part III: Heart Outline of class lecture After studying part I of this chapter you should be able to: 1. Be able to calculate cardiac output (CO) be able to define heart rate
The Cardiovascular System Part III: Heart Outline of class lecture After studying part I of this chapter you should be able to: 1. Be able to calculate cardiac output (CO) be able to define heart rate
Age-related changes in cardiovascular system. Dr. Rehab Gwada
 Age-related changes in cardiovascular system Dr. Rehab Gwada Objectives explain the main structural and functional changes in cardiovascular system associated with normal aging Introduction aging results
Age-related changes in cardiovascular system Dr. Rehab Gwada Objectives explain the main structural and functional changes in cardiovascular system associated with normal aging Introduction aging results
Heart Failure Overview. Dr Chris K Y Wong
 Heart Failure Overview Dr Chris K Y Wong Heart Failure: A Growing, Global Health Issue Heart Failure 23 Million Afflicted Global Impact Worldwide ~23 million peopleworldwide afflicted with CHF 1 Exceeds
Heart Failure Overview Dr Chris K Y Wong Heart Failure: A Growing, Global Health Issue Heart Failure 23 Million Afflicted Global Impact Worldwide ~23 million peopleworldwide afflicted with CHF 1 Exceeds
For more information about how to cite these materials visit
 Author(s): Louis D Alecy, D.M.D., Ph.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License:
Author(s): Louis D Alecy, D.M.D., Ph.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License:
Our Readers Have An Attitude Toward Living
 February 2007 America s Wellness Guide Number 43 FREE at Doctor s Offices, Hospitals, Clinics and Kroger Pharmacies in the Midsouth COVER Standard of Care for Heart Failure Management By Arie Szatkowski,
February 2007 America s Wellness Guide Number 43 FREE at Doctor s Offices, Hospitals, Clinics and Kroger Pharmacies in the Midsouth COVER Standard of Care for Heart Failure Management By Arie Szatkowski,
ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure
 Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
For more information about how to cite these materials visit
 Author(s): Gerald Abrams, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author(s): Gerald Abrams, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Risk Stratification in Heart Failure: The Role of Emerging Biomarkers
 Risk Stratification in Heart Failure: The Role of Emerging Biomarkers David G. Grenache, PhD Associate Professor of Pathology, University of Utah Medical Director, ARUP Laboratories Salt Lake City, UT
Risk Stratification in Heart Failure: The Role of Emerging Biomarkers David G. Grenache, PhD Associate Professor of Pathology, University of Utah Medical Director, ARUP Laboratories Salt Lake City, UT
Left ventricular hypertrophy: why does it happen?
 Nephrol Dial Transplant (2003) 18 [Suppl 8]: viii2 viii6 DOI: 10.1093/ndt/gfg1083 Left ventricular hypertrophy: why does it happen? Gerard M. London Department of Nephrology and Dialysis, Manhes Hospital,
Nephrol Dial Transplant (2003) 18 [Suppl 8]: viii2 viii6 DOI: 10.1093/ndt/gfg1083 Left ventricular hypertrophy: why does it happen? Gerard M. London Department of Nephrology and Dialysis, Manhes Hospital,
Failing Heart. Cardiac Resynchronization: novel therapy for the
 Advanced Studies in Medicine Cardiac Resynchronization: novel therapy for the Failing Heart Module 1: Understanding the Scope of Heart Failure, A Review of the Concepts of Anatomy & Physiology THE JOHNS
Advanced Studies in Medicine Cardiac Resynchronization: novel therapy for the Failing Heart Module 1: Understanding the Scope of Heart Failure, A Review of the Concepts of Anatomy & Physiology THE JOHNS
ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM. General Instructions: ID NUMBER: FORM NAME: H F A DATE: 10/13/2017 VERSION: CONTACT YEAR NUMBER:
 ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM General Instructions: The Heart Failure Hospital Record Abstraction Form is completed for all heart failure-eligible cohort hospitalizations. Refer to
ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM General Instructions: The Heart Failure Hospital Record Abstraction Form is completed for all heart failure-eligible cohort hospitalizations. Refer to
Pulmonary Hypertension: Another Use for Viagra
 Pulmonary Hypertension: Another Use for Viagra Kathleen Tong, MD Director, Heart Failure Program Assistant Clinical Professor University of California, Davis Disclosures I have no financial conflicts A
Pulmonary Hypertension: Another Use for Viagra Kathleen Tong, MD Director, Heart Failure Program Assistant Clinical Professor University of California, Davis Disclosures I have no financial conflicts A
Nothing to Disclose. Severe Pulmonary Hypertension
 Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
SPECIAL PATHOPHYSIOLOGY CARDIO-VASCULAR SYSTEM
 1. Myocardia lischemia is mainly a result of: 1.Coronary hypoxemia. 2. Coronary artery disease (CAD). 3. Acute coronaritis. 4. Coronary anemia. 5. Heart remodelling. SPECIAL PATHOPHYSIOLOGY CARDIO-VASCULAR
1. Myocardia lischemia is mainly a result of: 1.Coronary hypoxemia. 2. Coronary artery disease (CAD). 3. Acute coronaritis. 4. Coronary anemia. 5. Heart remodelling. SPECIAL PATHOPHYSIOLOGY CARDIO-VASCULAR
Review of Cardiac Imaging Modalities in the Renal Patient. George Youssef
 Review of Cardiac Imaging Modalities in the Renal Patient George Youssef ECHO Left ventricular hypertrophy (LVH) assessment Diastolic dysfunction Stress ECHO Cardiac CT angiography Echocardiography - positives
Review of Cardiac Imaging Modalities in the Renal Patient George Youssef ECHO Left ventricular hypertrophy (LVH) assessment Diastolic dysfunction Stress ECHO Cardiac CT angiography Echocardiography - positives
State-of-the-Art Management of Chronic Systolic Heart Failure
 State-of-the-Art Management of Chronic Systolic Heart Failure Michael McCulloch, MD 17 th Annual Cardiovascular Update Intermountain Medical Center December 16, 2017 Disclosures: I have no financial disclosures
State-of-the-Art Management of Chronic Systolic Heart Failure Michael McCulloch, MD 17 th Annual Cardiovascular Update Intermountain Medical Center December 16, 2017 Disclosures: I have no financial disclosures
The Pathophysiology of Cardiogenic Shock Knowledge Gaps & Opportunities
 The Pathophysiology of Cardiogenic Shock Knowledge Gaps & Opportunities Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure
The Pathophysiology of Cardiogenic Shock Knowledge Gaps & Opportunities Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure
Objectives. Let s start at the beginning 10/28/2014. What is Heart Failure? Understanding Heart Failure with Preserved LV Systolic Function
 Understanding Heart Failure with Preserved LV Systolic Function Eric Ernst, MD Medical Director C.O.R.E. Clinic Objectives Clarify the terminology surrounding right heart failure and diastolic heart failure
Understanding Heart Failure with Preserved LV Systolic Function Eric Ernst, MD Medical Director C.O.R.E. Clinic Objectives Clarify the terminology surrounding right heart failure and diastolic heart failure
DOWNLOAD PDF ABC OF HEART FAILURE
 Chapter 1 : The ABCs of managing systolic heart failure: Past, present, and future Heart failure is a multisystem disorder which is characterised by abnormalities of cardiac, skeletal muscle, and renal
Chapter 1 : The ABCs of managing systolic heart failure: Past, present, and future Heart failure is a multisystem disorder which is characterised by abnormalities of cardiac, skeletal muscle, and renal
Antialdosterone treatment in heart failure
 Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
Heart 101. Objectives. Types of Heart Failure How common is HF? Sign/Symptoms, when to see a doctor? Diagnostic testing
 EXAMING HEART FAILURE: HOW TO RECOGNIZE AND TREAT THE WEAK HEART What is Heart Failure? Treatment of Heart Failure End Stage Heart Failure Munir S. Janmohamed M.D. FACC Assistant Clinical Professor of
EXAMING HEART FAILURE: HOW TO RECOGNIZE AND TREAT THE WEAK HEART What is Heart Failure? Treatment of Heart Failure End Stage Heart Failure Munir S. Janmohamed M.D. FACC Assistant Clinical Professor of
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition
 Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Management Strategies for Advanced Heart Failure
 Management Strategies for Advanced Heart Failure Mary Norine Walsh, MD, FACC Medical Director, HF and Cardiac Transplantation St Vincent Heart Indianapolis, IN USA President American College of Cardiology
Management Strategies for Advanced Heart Failure Mary Norine Walsh, MD, FACC Medical Director, HF and Cardiac Transplantation St Vincent Heart Indianapolis, IN USA President American College of Cardiology
Treating the patient with acute heart failure. What do we really know? Principles of acute heart failure treatment
 ESC 2012 27Aug - 3Sep, 2012, Munich, Germany Treating the patient with acute heart failure. What do we really know? Principles of acute heart failure treatment Marco Metra, MD, FESC Cardiology University
ESC 2012 27Aug - 3Sep, 2012, Munich, Germany Treating the patient with acute heart failure. What do we really know? Principles of acute heart failure treatment Marco Metra, MD, FESC Cardiology University
(D) (E) (F) 6. The extrasystolic beat would produce (A) increased pulse pressure because contractility. is increased. increased
 (E) (F) 6. The extrasystolic beat would produce (A) increased pulse pressure because contractility. is increased. increased") Review Test 1. A 53-year-old woman is found, by arteriography, to have 5% narrowing of her left renal artery. What is the expected change in blood flow through the stenotic artery? Decrease to 1 2 Decrease
Review Test 1. A 53-year-old woman is found, by arteriography, to have 5% narrowing of her left renal artery. What is the expected change in blood flow through the stenotic artery? Decrease to 1 2 Decrease
Updates in Diagnosis & Management of CHF
 Updates in Diagnosis & Management of CHF N. Goldberg, DO April 30, 2011 CHF CHF is reaching an epidemic level in U.S. and continues to worsen over time Reasons are: HTN Dm with sedentary lifestyle and
Updates in Diagnosis & Management of CHF N. Goldberg, DO April 30, 2011 CHF CHF is reaching an epidemic level in U.S. and continues to worsen over time Reasons are: HTN Dm with sedentary lifestyle and
-12. -Ensherah Mokheemer - ABDULLAH ZREQAT. -Faisal Mohammad. 1 P a g e
 -12 -Ensherah Mokheemer - ABDULLAH ZREQAT -Faisal Mohammad 1 P a g e In the previous lecture we talked about: - cardiac index: we use the cardiac index to compare the cardiac output between different individuals,
-12 -Ensherah Mokheemer - ABDULLAH ZREQAT -Faisal Mohammad 1 P a g e In the previous lecture we talked about: - cardiac index: we use the cardiac index to compare the cardiac output between different individuals,
Heart Pump and Cardiac Cycle. Faisal I. Mohammed, MD, PhD
 Heart Pump and Cardiac Cycle Faisal I. Mohammed, MD, PhD 1 Objectives To understand the volume, mechanical, pressure and electrical changes during the cardiac cycle To understand the inter-relationship
Heart Pump and Cardiac Cycle Faisal I. Mohammed, MD, PhD 1 Objectives To understand the volume, mechanical, pressure and electrical changes during the cardiac cycle To understand the inter-relationship
Cor pulmonale. Dr hamid reza javadi
 1 Cor pulmonale Dr hamid reza javadi 2 Definition Cor pulmonale ;pulmonary heart disease; is defined as dilation and hypertrophy of the right ventricle (RV) in response to diseases of the pulmonary vasculature
1 Cor pulmonale Dr hamid reza javadi 2 Definition Cor pulmonale ;pulmonary heart disease; is defined as dilation and hypertrophy of the right ventricle (RV) in response to diseases of the pulmonary vasculature