Takashi Muraki, MD, PhD*, Norikazu Arakura, MD, PhD, Ryou Kodama, MD*, Suguru Yoneda, MD, PhD*, Masafumi Maruyama, MD*, Tetsuya Itou,
|
|
|
- Ethan Peters
- 5 years ago
- Views:
Transcription
1 Comparison of carbon dioxide and air insufflation use by non-expert endoscopists during endoscopic retrograde cholangiopancreatography Takashi Muraki, MD, PhD*, Norikazu Arakura, MD, PhD, Ryou Kodama, MD*, Suguru Yoneda, MD, PhD*, Masafumi Maruyama, MD*, Tetsuya Itou, MD,, PhD*, Takayuki Watanabe, MD*, Masahiro Maruyama, MD*, Akihiro Matsumoto, MD, PhD*, Shigeyuki Kawa, MD, PhD*, Eiji Tanaka, MD, PhD* *Department of Medicine, Gastroenterology, Endoscopic Examination Center, Shinshu University School of Medicine, Asahi, Matsumoto , Japan Correspondence to: Takashi Muraki, MD, PhD Department of Medicine, Gastroenterology, Shinshu University School of Medicine Asahi, Matsumoto , Japan Tel.: , Fax: Running head: CO2 insufflation during ERCP 1
2 Abstract Background: ERCP are subject to several complications which include a lengthy procedure time, technical difficulty, and active bowel movement induced by air insufflation. In ERCP performed by non-expert endoscopists who are prone to excessive luminal insufflation, insufflation with carbon dioxide (CO2) may provide better and safer outcomes. We aimed to assess the efficacy and safety of CO2 insufflation during ERCP by non-expert endoscopists. Methods: This study included 208 consecutive patients who received ERCP, excluding those in poor general health or with obstructive lung disease. The first operator for each patient was a non-expert endoscopist having done 50 or less ERCP procedures. Primary outcomes were the changes in cardiopulmonary state during ERCP. Secondary outcomes were ERCP complications. We designed a single center, randomized, prospective, double-blind, controlled trial with CO2 and air insufflation during ERCP. Results: CO2 insufflation did not affect overall procedure progression or results. A positive correlation was observed between procedure time and change in maximal systolic blood pressure from baseline among patients in the air insufflation group, but not in the CO2 insufflation group (correlation coefficient vs , change in the maximal systolic blood pressure from baseline +4.2 vs mmhg/ 10 minutes). This was consistent with our findings in patients treated by the first operator alone. The occurrence rate of post-ercp pancreatitis tended to be lower in the CO2 group than the air 2
3 group (4/102 [3.9%] vs. 0/106 [0%], P=0.056). Conclusions: CO2 insufflation during ERCP by non-expert endoscopists is recommended from the standpoints of efficacy and safety. Keywords: carbon dioxide, ERCP, post-ercp pancreatitis, non-expert endoscopist 3
4 Introduction ERCP and its related procedures have become essential techniques in the examination and treatment of pancreato-biliary diseases. However, such procedures are more complicated than traditional examination techniques, resulting in post ERCP-pancreatitis among other serious complications. Procedure-related complications are more frequently seen when ERCP is performed by a non-expert interventionalist, which has raised a need for the development of improved safety measures. 1, 2) Most notably, prolonged examination time and over-insufflation during ERCP by non-experts may trigger active bowel movement and result in unsuccessful tests and complications. The advantage of insufflation with CO2 instead of air during endoscopy has been well established 3-8). CO2 is absorbed by the body faster than air and is rapidly excreted through respiration 9). CO2 insufflation is especially favored in time-consuming endoscopic procedures, such as double-balloon enteroscopy, endoscopic submucosal dissection, and ERCP 10-11). Furthermore, it was reported that insufflation with CO2 could reduce procedure-related abdominal pain and complications compared with air insufflation due to less bowel hyperextension. Several studies showed that ERCP with CO2 insufflation decreased the incidence and severity of post-procedural abdominal pain and did not affect the incidence of post-ercp pancreatitis 12-15). However, as these reports did not weigh its merits with regard to operator experience, it is plausible that CO2 insufflation may be of greater benefit when used during ERCP by non-expert operators. There have 4
5 been no previous reports about changes in cardiopulmonary state and complication rate during ERCP by non-expert endoscopists as well. The present trial was conducted to assess the usefulness of CO2 insufflation during ERCP by non-experts, focusing on the efficacy and safety parameters of changes in cardiopulmonary state during ERCP and occurrence of complications. Methods Study design This study was designed as a prospective, single center, double-blind, randomized, control trial. Patients were assigned to one of two groups: the CO2 insufflation group or the air insufflation group. The study protocol was approved by the institutional review board. All participants provided informed consent prior to study enrollment. Patients Between November 2010 and September 2011, 208 consecutive adult patients undergoing ERCP for pancreato-biliary disease at Shinshu University Hospital were enrolled in this study. Each first operator was a non-expert endoscopist having done 50 or less ERCP procedures. The exclusion criteria for patients were as follows: (1) no informed consent, (2) younger than 20 years of age, (3) chronic obstructive pulmonary disease, (4) pregnancy, (5) use of sedative drugs within 12 hours prior to ERCP, (6) 5
6 receiving endoscopic ultrasonography or gastrointestinal endoscopy within 12 hours before or after ERCP, (7) receiving ERCP at a non-urgent time, (8) use of a double-balloon enteroscope for ERCP, (9) inaccessibility of the papilla of Vater for endoscopic examination, (10) poor general status requiring ERCP by an expert endoscopist (consciousness disorder, systolic blood pressure <80 mmhg, body temperature >39ºC, or pulse oxymeter [SpO2] <90%), and (11) judged as inappropriate by a doctor. Randomization and blinding of the study Enrolled patients were randomized into two groups designated as the CO2 insufflation group (CO2 group, n=106) and the air insufflation group (air group, n=102) by a computer-generated sequence just before ERCP. The procedure room set-up was virtually identical for each procedure. Endoscopic retrograde cholangiopancreatography All patients underwent ERCP and related procedures in a prone position after receiving 5 mg midazolam and 7.5 mg pentazocine hydrochloride intravenously for deep conscious sedation. The operator and assistants checked the sedation level of each patient and increased the doses of sedatives accordingly until deep sedation was achieved. Administration of anti-spastic drugs by intramuscular injection of 20 mg scopolamine butylbromide or 1 U.S.P glucagon and introduction of 2 l/min oxygen by a nasal tube were also performed if the need arose. Bile or pancreatic duct 6
7 cannulation was performed using standard methods with an ERCP catheter (PR-4Q-1, Olympus, Tokyo, Japan). After cannulation, routine procedures, such as sphincterotomy, biceps, biliary stenting, or intraductal ultrasonography, were performed on each patient. Expert endoscopists assumed control of ERCP sessions when procedure duration endangered the health of the patient. As each first operator was a novice endoscopist, an expert endoscopist took control of the procedure at any time when it did not progress for 10 minutes. Clinical care and assessment All patients were routinely measured for SpO2, pulse rate, and arterial blood pressure using a bedside monitor before administration of sedative drugs and every 5 minutes thereafter during procedures. If the patient showed pain or anxiety by unintentional body movement, additional sedatives were administered until deep sedation was re-established. If bowel movements increased during procedures, additional anti-spastic drugs were administered. Oxygen supply by a nasal tube was performed at 2l/min and routinely adjusted to maintain a SpO2 level of 95% during procedures. The change in maximal systolic blood pressure from baseline was defined as the maximal systolic blood pressure during ERCP minus the systolic blood pressure before administration of sedative drugs. This change in cardiopulmonary state was set as the primary end point. Total examination time was routinely recorded and defined as the time period from insertion to 7
8 pullout of the scope. Measurements of arterial pco2 and transcutaneous pco2 were not performed in this study because previous studies on CO2 insufflation during ERCP, colonoscopy, and double-balloon enteroscopy did not show any increases in these parameters 12-14, 16, 17). Blood cell counts and serum amylase values were evaluated immediately before and 2 hours and the following morning after ERCP. ERCP complications were defined according to Cotton s criteria 18). ERCP complications were defined as the secondary end point in this study. Statistical methods The Fisher s exact and Pearson s chi-square tests were adopted to test for differences between subgroups of patients. To compare continuous data, the Mann-Whitney U test was employed. All tests were performed using the IBM SPSS Statistics Desktop for Japan ver (IBM Japan Inc., Tokyo, Japan). P values of less than 0.05 were considered to be statistically significant. Sample size ERCP-related complication rates have been reported by prospective studies to range from 4.2% to 16.8% 19-30). The occurrence of hypotension during ERCP with midazolam sedation was reported to be from 2.0% to 9.8%, and that of hypoxia was determined to be from 8.2 to 31.3% 31-35). Since the first operator in this study was a non-expert endoscopist, we predicted 8
9 complication rates for hypotension or hypoxia to be approximately 20% each. In another study 13), the incidence of post-ercp pain with CO2 insufflation was approximately half of that with insufflation with air. Under these conditions, we estimated that analysis of over 100 patients per treatment group were required to provide 80% detection power at an significance value of Results Patients A total of 208 patients requiring urgent ERCP were enrolled in this study and separated into 102 patients who received air insufflation and 106 patients who received CO2 insufflation (Fig. 1). There were no statistical differences with regard to age, sex, incidence of first ERCP, prior sphincterotomy, or prior post-ercp pancreatitis between the two groups (Table 1). The prevalences of final diagnosis and ERCP-related procedures were also similar between the groups (Table 2, 3). Time and success rate of procedures There were no statistical differences in procedure time or success rate between the two groups. The progress of ERCP and related procedures was not affected by CO2 insufflation (Table 4). Changes in cardiopulmonary state during ERCP 9
10 There were no statistical differences regarding the addition of anti-spastic or sedative drugs between the two groups. However, oxygen supply demand tended to be lower in the CO2 group than in the air group (p=0.088) (Table 4). A positive correlation was observed between procedure time and change in maximal systolic blood pressure from baseline among patients in the air insufflation group, but not in the CO2 insufflation group (correlation coefficient vs , change in the maximal systolic blood pressure from baseline +4.2 vs mmhg/10 minutes) (Fig. 2A). It was the same result in patients treated by the first operator alone (Fig. 2B). Although procedure time was long for these operators, there was no significant change in blood pressure elevation in the CO2 insufflation group. Adverse events No statistical differences were observed in white blood cell count and serum amylase level comparisons between the two groups (Table 4). Overall, adverse events occurred in 7/208 patients (3.3%; 6 in the air group and 1 in the CO2 group), and were significantly higher in the air group (P=0.048). Post-ERCP pancreatitis occurred in 4/208 patients (1.9%; 3 mild and 1 severe), all of whom were in the air group, albeit not significantly different (P=0.056). Other adverse events were an allergy in 1 patient in each group and vagovagal reflex in 1 air group patient. No serious cardiopulmonary complications occurred (Table 5). 10
11 Discussion ERCP requires a lengthy procedure time with high levels of sedation and a potentially high amount of air insufflation, which makes CO2 an attractive candidate to improve outcome and safety. The utility of CO2 insufflation during ERCP was reported in previous studies of non-uniformly experienced operators, indicating reductions in abdominal distention and nausea compared with air insufflation 12-15). Furthermore, CO2 insufflation in enteroscopy and related procedures was shown to reduce bowel hyperextension accompanying luminal over-insufflation, since distended bowels would frequently limit or prevent the flexibility and controllability of the endoscope. In ERCP for patients with a very small papilla of Vater, body movement and active bowel movement during procedures introduce not only operation difficulty, but also edema in the papilla, which in turn may result in post-ercp pancreatitis. In a previous study, CO2 insufflation during ERCP mitigated abdominal distention and nausea after procedures, but adverse events, such as post-ercp pancreatitis, were not affected. The present study assessed the utility and safety of CO2 insufflation in ERCP operations done by non-experts and showed that CO2 may reduce complications and the risk of post-ercp pancreatitis. Since novice operators tend to over-insufflate during ERCP, insufflation with CO2 may have reduced the demand for oxygen in comparison with air insufflation in our study, but procedure time and success rate were not 11
12 affected. CO2 insufflation may have also lowered upward pressure on the diaphragm by reducing pressure changes in the intestinal lumen and intra-abdominal pressure, which reduced pain during ERCP. The frequency of complications associated with ERCP and related procedures with air insufflation in our study (5.9%) was similar to that previously reported in a recent systematic survey of prospective studies (6.85%) 36) However, the complication rate with CO2 insufflation in our cohort (0.9%) was clearly lower. CO2 insufflation during ERCP appeared to reduce the incidence post-ercp pancreatitis in comparison with air insufflation in the present study. This may be due to the reasons of 1) CO2 insufflation reduced edema in the papilla of Vater by limiting body movement accompanying pain, as well as movement of the intestinal tract, and 2) CO2 insufflation reduced the pressure in the intra-pancreatic duct by limiting bowel hyperextension. In ERCP with prolonged procedure times, we observed that CO2 insufflation reduced the negative effects of this procedure on dynamic blood circulation. We also demonstrated that CO2 insufflation reduced pain not only after, but also during, ERCP, although previous studies showed that CO2 reduced abdominal distention and nausea after ERCP only 12-15). Although we decided to recruit procedures being started by a non-expert, eventually only half of the cases in each group were completed by the non-expert alone. The complexity of ERCP-related procedures may thus affect the final clinical outcomes from the study. In our investigation, ERCP 12
13 for patients in poor general condition and those done by an expert endoscopist were excluded. Thus, it remains unclear whether CO2 insufflation is more useful in patients in poor health due to factors like acute cholangitis or elderly age. Conclusion CO2 insufflation during ERCP by non-expert endoscopists could be considered from the standpoints of efficacy and safety. References 1. J.-M. Dumonceau, A. Andriulli, J. Deviere, et al. European Society of Gastrointestinal Endoscopy (ESGE) Guideline: Prophylaxis of post-ercp pancreatitis. Endoscopy 2010; 42: Rabenstein T, Roggenbuck S, Framke B, et al. Complications of endoscopic sphincterotomy: can heparin prevent acute pancreatitis after ERCP? Gastrointest Endosc 2002; 55: Hussein AM, Bartram CI, Williams CB. Carbon dioxide insufflation for more comfortable colonoscopy. Gastrointest Endosc 1984; 30: Stevenson GW, Wilson JA, Wilkinson J et al. Pain following colonoscopy: elimination with carbon dioxide. Gastrointest Endosc 1992; 38: Church J, Delaney C, Randomized, et al. controlled trial of carbon dioxide insufflation during colonoscopy. Dis Colon Rectum 2003; 46: Bretthauer M, Thiis-Evensen E, Huppertz-Hauss G, et al. NORCCAP 13
14 (Norwegian colorectal cancer prevention):a randomised trial to assess the safety and efficacy of carbon dioxide versus air insufflation in colonoscopy. Gut 2002; 50: Bretthauer M, Lynge AB, Thiis-Evensen E, et al. Carbon dioxide insufflation in colonoscopy: safe and effective in sedated patients. Endoscopy 2005; 37: Yamano HO, Yoshikawa K, Kimura T, et al. Carbon dioxide insufflation for colonoscopy: evaluation of gas volume, abdominal pain, examination time and transcutaneous partial CO2 pressure. J Gastroenterol 2010; 45: Saltzman HA, Siecker HO. Intestinal response to changing gaseous environments: normobaric and hyperbaric observations. Ann N Y Acad Sci 1968; 150: Uemura M, Ishii N, Itoh T, Suzuki K, et al. Effects of Carbon Dioxide Insufflation in Esophageal Endoscopic Submucosal Dissection. Hepatogastroenterology 2011; 59: Fumihito Hirai, Takahiro Beppu, Taku Nishimura, et al. Carbon dioxide insufflation compared with air insufflation in double-balloon enteroscopy: a prospective, randomized, double-blind trial. Gastrointest Endosc 2011; 73: Bretthauer M, Seip B, Aasen S, et al. Carbon dioxide insufflation for more comfortable endoscopic retrograde cholangiopancreatography: a randomized, controlled, double-blind trial. Endoscopy 2007; 39: John T. Maple, DO, et al. Carbon dioxide insufflation during ERCP for 14
15 reduction of post procedure pain: a randomized, double-blind, controlled trial. Gastrointest Endosc 2009; 70: Evan S. Dellon, MPH, et al. A randomized, controlled, double-blind trial of air insufflation versus carbon dioxide insufflation during ERCP. Gastrointest Endosc 2010; 72: Masaki Kuwatani, Hiroshi Kawakami, Tsuyoshi Hayashi, et al. Carbon dioxide insufflation during endoscopic retrograde cholangiopancreatography reduces bowel gas volume but does not affect visual analogue scale scores of suffering: a prospective, double-blind, randomized, controlled trial. Surg Endosc 2011; 25: Stevenson GW, Wilson JA, Wilkinson J, et al. Pain following colonoscopy: elimination with carbon dioxide. Gastrointest Endosc 1992; 38: Dellon ES, Hawk JS, Grimm IS, Shaheen NJ, et al. The use of carbon dioxide for insufflation during GI endoscopy: a systematic review. Gastrointest Endosc 2009; 69: Cotton PB, Lehman G, Vennes J, et al. Endoscopic sphincterotomy complications and their management: an attempt at consensus. Gastrointest Endosc 1991; 37: Barthet M, Lesavre N, Desjeux A, et al. Complications of endoscopic sphincterotomy: Results form a single tertiary referral center. Endoscopy 2002; 34: Choudari CP, Sherman S, Fogel EL, et al. Success of ERCP at a referral center after a previously unsuccessful attempt. Gastrointest Endosc 2000; 52:
16 21. Christensen M, Matzen P, Schulze S, et al. Complications of ERCP: A prospective study. Gastrointest Endosc 2004; 60: Christoforidis E, Goulimaris I, Kanellos I, et al. Post-ERCP pancreatitis and hyperamylasemia: Patient-related and operative risk factors. Endoscopy 2002; 34: K okl u S, Parlak E, Y uksel O, et al. Endoscopic retrograde cholangiopancreatography in the elderly: A prospective and comparative study. Age Ageing 2005; 34: Lal D, Lane M, Wong P. Complications of endoscopic retrograde cholangiopancreatography. N Z Med J 2003; 116: U Masci E, Toti G, Mariani A, et al. Complications of diagnostic and therapeutic ERCP: A prospective multicenter study. Am J Gastroenterol 2001; 96: Ong TZ, Khor JL, Selamat DS, et al. Complications of endoscopic retrograde cholangiography in the post MRCP era: A tertiary center experience. World J Gastroenterol 2005; 11: Rabenstein T, Schneider HT, Bulling D, et al. Analysis of the risk factors associated with endoscopic sphincterotomy techniques: Preliminary results of a prospective study, with emphasis on the reduced risk of acute pancreatitis with low dose anticoagulation treatment. Endoscopy 2000; 32: Suissa A, Yassin K, Lavy A, et al. Outcome and early complications of ERCP: A prospective single center study. 2005; 52: Tzovaras G, Shukla P, Kow L, et al. What are the risks of diagnostic and 16
17 therapeutic endoscopic retrograde cholangiopancreatography? Aust N Z J Surg 2000; 70: Vandervoort J, Soetikno RM, Tham TCT, et al. Risks factors for complications after performance of ERCP. Gastrointest Endosc 2002; 56: Riphaus A, Stergiou N, Wehrmann T. Sedation with propofol for routine ERCP in high-risk octogenarians: a randomized, controlled study. Am J Gastroenterol 2005; 100: Wehrmann T, Kokabpick S, Lembcke B, et al. Efficacy and safety of intravenous propofol sedation during routine ERCP: a prospective, controlled study. Gastrointest Endosc 1999; 49: Jung M, Hofmann C, Kiesslich R, et al. Improved sedation in diagnostic and therapeutic ERCP: propofol is an alternative to midazolam. Endoscopy 2000; 32: Chen WX, Lin HJ, Zhang WF, et al. Sedation and safety of propofol for therapeutic endoscopic retrograde cholangiopancreatography. Hepatobiliary Pancreat Dis Int 2005; 4: Kongkam P, Rerknimitr R, Punyathavorn S, et al. Propofol infusion versus intermittent meperidine and midazolam injection for conscious sedation in ERCP. J Gastrointestin Liver Dis 2008; 17: Angelo Andriulli, M.D., Silvano Loperfido, M.D., Grazia Napolitano, M.D., et al. Incidence Rates of Post-ERCP Complications: A Systematic Survey of Prospective Studies. Am J Gastroenterol 2007; 102:
18 Table 1. Characteristics of the study population Type of insufflation during ERCP Air CO2 p value* (n=102) (n=106) Age (years) a 63.5 (26-87) 65.0 (27-93) Male b 74 (72.5%) 71 (67.0%) First ERCP b 26 (25.5%) 22 (20.8%) Prior sphincterotomy b 60 (58.8%) 56 (52.8%) Prior post-ercp pancreatitis b 11 (10.7%) 5 ( 4.7%) Comorbidities Ischemic heart disease b 7 (6.9%) 8 (7.5%) Hypertension b 13 (12.7%) 20 (18.9%) Atrial fibrillation b 2 (2.0%) 4 (3.8%) Diabetes b 21 (20.6%) 13 (12.3%) Previous abdominal surgery b 35 (34.3%) 40 (37.7%) Cerebrovascular disease b 7 (6.9%) 5 (4.7%) a : Data are expressed as median (range). b : Data are expressed as a positive number (%). * p values were calculated using the Mann-Whitney U test and Pearson s chi-square test. 18
19 Table 2. ERCP characteristics Type of insufflation during ERCP Air CO2 p value* (n=102) (n=106) Diagnostic ERCP 14 (13.7%) 15 (14.2%) Endoscopic procedure Forceps biopsy of biliary tract 10 (9.8%) 15 (14.1%) Brush cytology of pancreatic duct 2 (2.0%) 2 (1.9%) 1 Aspiration cytology of pancreatic juice 0 (0%) 3 (2.8%) IDUS of biliary tract 13 (12.7%) 17 (16.0%) IDUS of pancreatic duct 2 (2.0%) 4 (3.8%) Biliary sphincterotomy 11 (10.8%) 14 (13.2%) Pancreatic sphincterotomy 3 ( 2.9%) 3 ( 2.8%) Papillary balloon dilatation 2 ( 2.0%) 1 ( 0.9%) Endoscopic nasobiliary drainage 20 (19.6%) 16 (15.1%) Endoscopic nasopancreatic drainage 2 (2.0%) 0 (0%) Biliary plastic stenting 25 (24.5%) 29 (27.4%) Pancreatic plastic stenting 10 (9.8%) 13 (12.3%) Biliary metallic stenting 9 ( 8.8%) 6 ( 5.7%) Removal of CBD stones 15 (14.7%) 14 (13.2%) Removal of pancreatic stones 5 ( 4.9%) 10 ( 9.4%) CBD: common bile duct, IDUS: intra-ductal ultrasonography * p values were calculated using Pearson s chi-square test. 19
20 Table 3. Final diagnosis Type of insufflation during ERCP Air CO2 p value* (n=102) (n=106) Final diagnosis CBD stones 22 (21.6%) 24 (22.6%) Benign BD stricture 20 (19.6%) 23 (21.7%) Pancreatic stones 23 (22.5%) 23 (21.7%) Cholangiocarcinoma 10 ( 9.8%) 11 (10.4%) BD stricture by lymph nodes 8 ( 7.8%) 6 ( 5.7%) Pancreatic cancer 7 ( 6.9%) 4 ( 3.8%) GB cancer 4 ( 3.9%) 5 ( 4.7%) IPMN 2 ( 2.0%) 3 ( 2.8%) GB stones 2 ( 2.0%) 4 ( 3.8%) Pancreatic divisum 2 ( 2.0%) 0 ( 0%) Autoimmune pancreatitis 0 ( 0%) 2 ( 1.9%) Other 2 ( 2.0%) 1 ( 0.9%) CBD: common bile duct, BD: bile duct, GB: gall bladder, IPMN: intra-ductal mucinous neoplasm * p values were calculated using Pearson s chi-square test. 20
21 Table 4. Duration and success rate of procedures and rates of additional sedatives, anti-spastic drugs, and oxygen supply Type of insufflation during ERCP Air CO2 p value* (n=102) (n=106) Achieved by first operator alone a 49 (48.0%) 53 (50.0%) Total examination time b 31.7 (6-139) 34.4 (8-134) Success rate of insertion into bile or pancreatic duct a 99 (97.1%) 104 (98.1%) Rate of additional anti-spastic drugs a 0 (0%) 0 (0%) Rate of additional sedative drugs a 45 (44.1%) 53 (50.0%) Rate of increased oxygen supply a 14 (13.7%) 7 ( 6.6%) White blood cell count > ULN (9130 /μl) 2 hours after ERCP a 19 (18.8%) 16 (15.1%) Morning after ERCP a 13 (12.7%) 8 ( 7.5%) Serum amylase > 3xULN (381 IU/l ) 2 hours after ERCP a 6 ( 5.9%) 4 ( 3.8%) Morning after ERCP a 11 (10.8%) 6 ( 5.7%) ULN: upper limit of normal a : Data are expressed as median (range). b : Data are expressed as a positive number (%). * p values were calculated using Pearson s chi-square test. 21
22 Table 5. Adverse events Type of insufflation during ERCP Air CO2 p value* (n=102) (n=106) Post-ERCP pancreatitis 4 (3.9%) 0 (0%) Mild 3 0 Moderate 0 0 Severe 1 0 Allergy 1 (1.0%) 1 (0.9%) Vagovagal reflex 1 (1.0%) 0 ( 0%) Total 6 (5.9%) 1 (0.9%) * p values were calculated using Pearson s chi-square test. 22

23 Figure legends Figure 1. Flowchart diagram of study participants 23
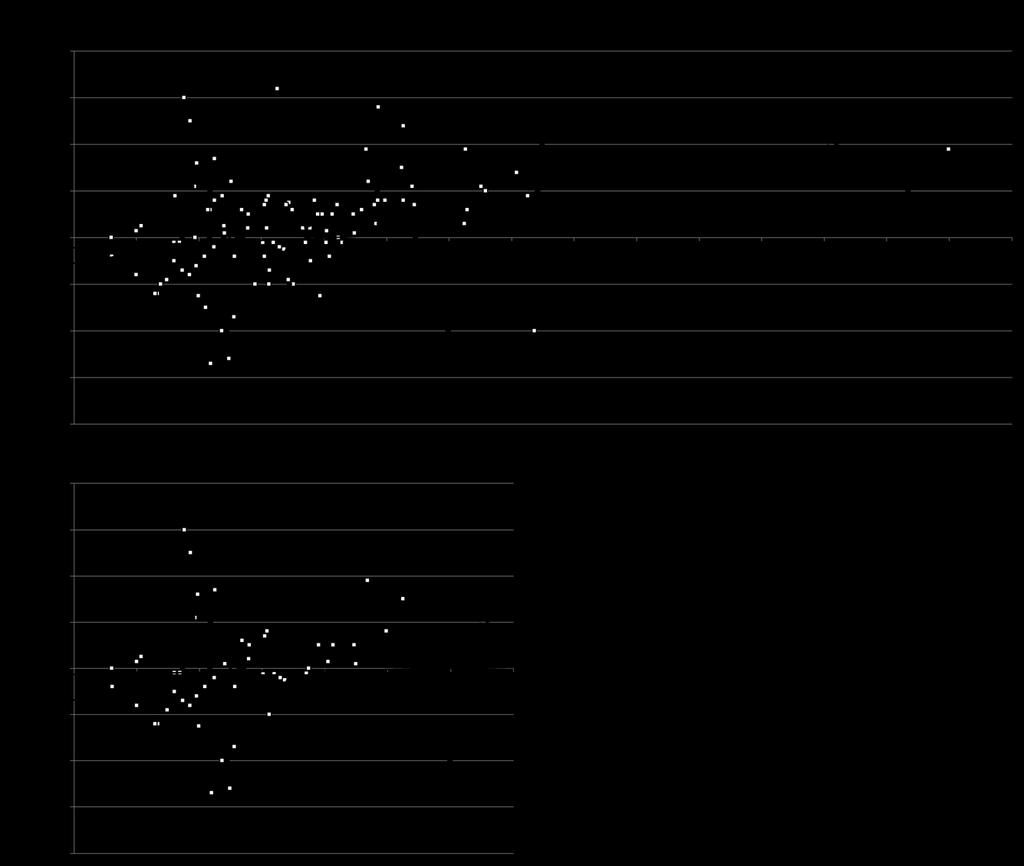
24 Figure 2. A: Correlation between procedure time and change in sbp in all patients. In the CO2 insufflation group, the change in sbp was +1.2 mmhg/10 minutes (correlation coefficient: 0.114, p=0.052). In the air insufflation group, sbp was +4.2 mmhg/10 minutes (correlation coefficient: 0.408, p =<0.001). B: Correlation between procedure time and change in sbp in patients treated by the first operator alone. In the CO2 insufflation group, the change in sbp was +0.6 mmhg/10 minutes (correlation coefficient: , p=0.973). In the air insufflation group, sbp was +5.4 mmhg/10 minutes (correlation coefficient: 0.342, p=0.018). The change in sbp was defined as the change in maximal systolic blood pressure from baseline. sbp: systolic blood pressure. 24
25 25
26 Figure 1.
27 Figure 2.
Carbon Dioxide Role in GI Endoscopy
 The Egyptian Journal of Hospital Medicine (January 2018) Vol. 70 (4), Page 577-583 Carbon Dioxide Role in GI Endoscopy Mohanad Obaid Mohsen Alkhamash 4, Hussam Musallam Alfarsi 2, Abdullah Khalid Aljadi
The Egyptian Journal of Hospital Medicine (January 2018) Vol. 70 (4), Page 577-583 Carbon Dioxide Role in GI Endoscopy Mohanad Obaid Mohsen Alkhamash 4, Hussam Musallam Alfarsi 2, Abdullah Khalid Aljadi
Making ERCP Easy: Tips From A Master
 Making ERCP Easy: Tips From A Master Raj J. Shah, M.D., FASGE Associate Professor of Medicine University of Colorado School of Medicine Co-Director, Endoscopy Director, Pancreaticobiliary Endoscopy Services
Making ERCP Easy: Tips From A Master Raj J. Shah, M.D., FASGE Associate Professor of Medicine University of Colorado School of Medicine Co-Director, Endoscopy Director, Pancreaticobiliary Endoscopy Services
History of Post-Endoscopic Retrograde Cholangiopancreatography Pancreatitis and Acute Pancreatitis as Risk Factors for Post-ERCP Pancreatitis
 Kobe J. Med. Sci., Vol. 63, No. 1, pp. E1-E8, 2017 History of Post-Endoscopic Retrograde Cholangiopancreatography Pancreatitis and Acute Pancreatitis as Risk Factors for Post-ERCP Pancreatitis EIJI FUNATSU
Kobe J. Med. Sci., Vol. 63, No. 1, pp. E1-E8, 2017 History of Post-Endoscopic Retrograde Cholangiopancreatography Pancreatitis and Acute Pancreatitis as Risk Factors for Post-ERCP Pancreatitis EIJI FUNATSU
THE DIAGNOSTIC ACCURACY OF RAISED SERUM AMYLASE LEVEL AT 4 HOURS POST ERCP IN PREDICTING ACUTE PANCREATITIS
 ORIGINAL ARTICLE THE DIAGNOSTIC ACCURACY OF RAISED SERUM AMYLASE LEVEL AT 4 HOURS POST ERCP IN PREDICTING ACUTE PANCREATITIS UMBREEN ASLAM KHAN, SABEEN FARHAN, MUHAMMAD ARIF NADEEM, SIDRA RASHEED Department
ORIGINAL ARTICLE THE DIAGNOSTIC ACCURACY OF RAISED SERUM AMYLASE LEVEL AT 4 HOURS POST ERCP IN PREDICTING ACUTE PANCREATITIS UMBREEN ASLAM KHAN, SABEEN FARHAN, MUHAMMAD ARIF NADEEM, SIDRA RASHEED Department
Principles of ERCP: papilla cannulation, indications/contraindications and risks. Dr. med. Henrik Csaba Horváth PhD
 Principles of ERCP: papilla cannulation, indications/contraindications and risks Dr. med. Henrik Csaba Horváth PhD Evolution of ERCP 1968. 1970s ECPG Endoscopic CholangioPancreatoGraphy Japan 1974 Biliary
Principles of ERCP: papilla cannulation, indications/contraindications and risks Dr. med. Henrik Csaba Horváth PhD Evolution of ERCP 1968. 1970s ECPG Endoscopic CholangioPancreatoGraphy Japan 1974 Biliary
The Incidence of Complications in Single-stage Endoscopic Stone Removal for Patients with Common Bile Duct Stones: A Propensity Score Analysis
 doi: 10.2169/internalmedicine.9123-17 http://internmed.jp ORIGINAL ARTICLE The Incidence of Complications in Single-stage Endoscopic Stone Removal for Patients with Common Bile Duct Stones: A Propensity
doi: 10.2169/internalmedicine.9123-17 http://internmed.jp ORIGINAL ARTICLE The Incidence of Complications in Single-stage Endoscopic Stone Removal for Patients with Common Bile Duct Stones: A Propensity
ACUTE CHOLANGITIS AS a result of an occluded
 Digestive Endoscopy 2017; 29 (Suppl. 2): 88 93 doi: 10.1111/den.12836 Current status of biliary drainage strategy for acute cholangitis Endoscopic treatment for acute cholangitis with common bile duct
Digestive Endoscopy 2017; 29 (Suppl. 2): 88 93 doi: 10.1111/den.12836 Current status of biliary drainage strategy for acute cholangitis Endoscopic treatment for acute cholangitis with common bile duct
The Use of Pancreatoscopy in the Diagnosis of Intraductal Papillary Mucinous Tumor Lesions of the Pancreas
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:S53 S57 The Use of Pancreatoscopy in the Diagnosis of Intraductal Papillary Mucinous Tumor Lesions of the Pancreas KENJIRO YASUDA, MUNEHIRO SAKATA, MOOSE
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:S53 S57 The Use of Pancreatoscopy in the Diagnosis of Intraductal Papillary Mucinous Tumor Lesions of the Pancreas KENJIRO YASUDA, MUNEHIRO SAKATA, MOOSE
A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY
 A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center Welcome The St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center is a leader
A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center Welcome The St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center is a leader
Is Endoscopic Retrograde Cholangiopancreatography Safe in Patients 90 Years of Age and Older?
 Gut and Liver, Vol. 8, No. 5, September 2014, pp. 552-556 ORiginal Article Is Endoscopic Retrograde Cholangiopancreatography Safe in Patients 90 Years of Age and Older? Dae Young Yun, Jimin Han, Jang Seok
Gut and Liver, Vol. 8, No. 5, September 2014, pp. 552-556 ORiginal Article Is Endoscopic Retrograde Cholangiopancreatography Safe in Patients 90 Years of Age and Older? Dae Young Yun, Jimin Han, Jang Seok
Safety of endoscopic retrograde cholangiopancreatography in patients 80 years of age and older
 Original paper Safety of endoscopic retrograde cholangiopancreatography in patients 80 years of age and older Baydar Behlül 1, Serin Ayfer 2, Vatansever Sezgin 3, Kandemir Altay 3, Çelik Mustafa 3, Çekiç
Original paper Safety of endoscopic retrograde cholangiopancreatography in patients 80 years of age and older Baydar Behlül 1, Serin Ayfer 2, Vatansever Sezgin 3, Kandemir Altay 3, Çelik Mustafa 3, Çekiç
Unresolved Issues about Post-ERCP Pancreatitis: An Overview
 Unresolved Issues about Post-ERCP Pancreatitis: An Overview Pier Alberto Testoni Division of Gastroenterology and Gastrointestinal Endoscopy, University Vita-Salute San Raffaele, IRCCS San Raffaele Hospital.
Unresolved Issues about Post-ERCP Pancreatitis: An Overview Pier Alberto Testoni Division of Gastroenterology and Gastrointestinal Endoscopy, University Vita-Salute San Raffaele, IRCCS San Raffaele Hospital.
ERCP and EUS: What s New and What Should We Do?
 ERCP and EUS: What s New and What Should We Do? Rajesh N. Keswani, MD Associate Professor of Medicine Division of Gastroenterology Northwestern University Feinberg School of Medicine EUS/ERCP in 2015 THE
ERCP and EUS: What s New and What Should We Do? Rajesh N. Keswani, MD Associate Professor of Medicine Division of Gastroenterology Northwestern University Feinberg School of Medicine EUS/ERCP in 2015 THE
Patients with primary sclerosing cholangitis require more sedation during endoscopic retrograde cholangiography
 Patients with primary sclerosing cholangitis require more sedation during endoscopic retrograde cholangiography Authors Carsten Keil 1, Lukas Aguirre Dávila 2, Theodor Framke 2, Henrike Lenzen 1, Michael
Patients with primary sclerosing cholangitis require more sedation during endoscopic retrograde cholangiography Authors Carsten Keil 1, Lukas Aguirre Dávila 2, Theodor Framke 2, Henrike Lenzen 1, Michael
Prophylaxis of Post Endoscopic Retrograde Cholangiopancreatography Pancreatitis by an Endoscopic Pancreatic Spontaneous Dislodgement Stent
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2007;5:1339 1346 Prophylaxis of Post Endoscopic Retrograde Cholangiopancreatography Pancreatitis by an Endoscopic Pancreatic Spontaneous Dislodgement Stent ATSUSHI
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2007;5:1339 1346 Prophylaxis of Post Endoscopic Retrograde Cholangiopancreatography Pancreatitis by an Endoscopic Pancreatic Spontaneous Dislodgement Stent ATSUSHI
Management of the Mucin Filled Bile Duct. A Complication of Intraductal Papillary Mucinous Tumor of the Pancreas
 CASE REPORT Management of the Mucin Filled Bile Duct. A Complication of Intraductal Papillary Mucinous Tumor of the Pancreas Anand Patel, Louis Lambiase, Antonio Decarli, Ali Fazel Division of Gastroenterology
CASE REPORT Management of the Mucin Filled Bile Duct. A Complication of Intraductal Papillary Mucinous Tumor of the Pancreas Anand Patel, Louis Lambiase, Antonio Decarli, Ali Fazel Division of Gastroenterology
Propofol Infusion versus Intermittent Meperidine and Midazolam Injection for Conscious Sedation in ERCP
 Propofol Infusion versus Intermittent Meperidine and Midazolam Injection for Conscious Sedation in ERCP Pradermchai Kongkam 1, Rungsun Rerknimitr 1, Sahadol Punyathavorn 2, Chitr Sitthi-Amorn 3, Yuwadee
Propofol Infusion versus Intermittent Meperidine and Midazolam Injection for Conscious Sedation in ERCP Pradermchai Kongkam 1, Rungsun Rerknimitr 1, Sahadol Punyathavorn 2, Chitr Sitthi-Amorn 3, Yuwadee
Introduction. Patients and methods. Patients. Background and study aims Failure to recognize the
 A simple and novel marking method for correctly identifying the precutting direction to achieve safe and efficacious precut sphincterotomy (with video) Authors Kazumasa Nagai, Akio Katanuma, Kuniyuki Takahashi,
A simple and novel marking method for correctly identifying the precutting direction to achieve safe and efficacious precut sphincterotomy (with video) Authors Kazumasa Nagai, Akio Katanuma, Kuniyuki Takahashi,
Sex-related differences in predicting choledocholithiasis using current American Society of Gastrointestinal Endoscopy risk criteria
 ORIGINAL ARTICLE Annals of Gastroenterology (2018) 31, 1-6 Sex-related differences in predicting choledocholithiasis using current American Society of Gastrointestinal Endoscopy risk criteria Ankit Chhoda
ORIGINAL ARTICLE Annals of Gastroenterology (2018) 31, 1-6 Sex-related differences in predicting choledocholithiasis using current American Society of Gastrointestinal Endoscopy risk criteria Ankit Chhoda
A cute pancreatitis is a common complication of endoscopic
 1768 PANCREAS Intravenous bolus somatostatin after diagnostic cholangiopancreatography reduces the incidence of pancreatitis associated with therapeutic endoscopic retrograde cholangiopancreatography procedures:
1768 PANCREAS Intravenous bolus somatostatin after diagnostic cholangiopancreatography reduces the incidence of pancreatitis associated with therapeutic endoscopic retrograde cholangiopancreatography procedures:
The role of ERCP in chronic pancreatitis
 The role of ERCP in chronic pancreatitis Marianna Arvanitakis Erasme University Hospital, ULB, Brussels, Belgium 10 th Nottingham Endoscopy Masterclass SPEAKER DECLARATIONS This presenter has the following
The role of ERCP in chronic pancreatitis Marianna Arvanitakis Erasme University Hospital, ULB, Brussels, Belgium 10 th Nottingham Endoscopy Masterclass SPEAKER DECLARATIONS This presenter has the following
Prevention and management of complications
 Prevention and management of complications Endoscopic retrograde cholangiopancreatography (ERCP) H.-J. Schulz, H. Schmidt Oskar-Ziethen-Hospital Sana Clinic Lichtenberg Teaching Hospital of Charité Humboldt
Prevention and management of complications Endoscopic retrograde cholangiopancreatography (ERCP) H.-J. Schulz, H. Schmidt Oskar-Ziethen-Hospital Sana Clinic Lichtenberg Teaching Hospital of Charité Humboldt
Increased risk and severity of ERCP-related complications associated with asymptomatic common bile duct stones
 Increased risk and severity of ERCP-related complications associated with asymptomatic common bile duct stones Authors Hirokazu Saito 1, 2, Tatsuyuki Kakuma 3, Yoshihiro Kadono 4,AtsushiUrata 4,KentaroKamikawa
Increased risk and severity of ERCP-related complications associated with asymptomatic common bile duct stones Authors Hirokazu Saito 1, 2, Tatsuyuki Kakuma 3, Yoshihiro Kadono 4,AtsushiUrata 4,KentaroKamikawa
Pilot Study of Aprepitant for Prevention of Post-ERCP Pancreatitis in High Risk Patients: A Phase II Randomized, Double-Blind Placebo Controlled Trial
 ORIGINAL ARTICLE Pilot Study of Aprepitant for Prevention of Post-ERCP Pancreatitis in High Risk Patients: A Phase II Randomized, Double-Blind Placebo Controlled Trial Tilak Upendra Shah, Rodger Liddle,
ORIGINAL ARTICLE Pilot Study of Aprepitant for Prevention of Post-ERCP Pancreatitis in High Risk Patients: A Phase II Randomized, Double-Blind Placebo Controlled Trial Tilak Upendra Shah, Rodger Liddle,
Research Article Risk Factors for Migration, Fracture, and Dislocation of Pancreatic Stents
 Gastroenterology Research and Practice Volume 2015, Article ID 365457, 6 pages http://dx.doi.org/10.1155/2015/365457 Research Article Risk Factors for Migration, Fracture, and Dislocation of Pancreatic
Gastroenterology Research and Practice Volume 2015, Article ID 365457, 6 pages http://dx.doi.org/10.1155/2015/365457 Research Article Risk Factors for Migration, Fracture, and Dislocation of Pancreatic
What can you expect after your ERCP?
 ERCP Explained and respond to bed rest, pain relief and fasting to rest the gut with the patient needing to stay in hospital for only a few days. Some patients develop severe pancreatitis and may require
ERCP Explained and respond to bed rest, pain relief and fasting to rest the gut with the patient needing to stay in hospital for only a few days. Some patients develop severe pancreatitis and may require
Journal of Interventional Gastroenterology A Combination of Snare Polypectomy and APC Therapy for Prolapsing Common Bile Duct Adenoma
 Journal of Interventional Gastroenterology A Combination of Snare Polypectomy and APC Therapy for Prolapsing Common Bile Duct Adenoma --Manuscript Draft-- Manuscript Number: Full Title: Article Type: Section/Category:
Journal of Interventional Gastroenterology A Combination of Snare Polypectomy and APC Therapy for Prolapsing Common Bile Duct Adenoma --Manuscript Draft-- Manuscript Number: Full Title: Article Type: Section/Category:
Endoscopic Management of Biliary Strictures. Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center
 Endoscopic Management of Biliary Strictures Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center Malignant Biliary Strictures Etiologies: Pancreatic
Endoscopic Management of Biliary Strictures Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center Malignant Biliary Strictures Etiologies: Pancreatic
Clinical Study Covered Metal Stenting for Malignant Lower Biliary Stricture with Pancreatic Duct Obstruction: Is Endoscopic Sphincterotomy Needed?
 Gastroenterology Research and Practice Volume 2013, Article ID 375613, 6 pages http://dx.doi.org/10.1155/2013/375613 Clinical Study Covered Metal Stenting for Malignant Lower Biliary Stricture with Pancreatic
Gastroenterology Research and Practice Volume 2013, Article ID 375613, 6 pages http://dx.doi.org/10.1155/2013/375613 Clinical Study Covered Metal Stenting for Malignant Lower Biliary Stricture with Pancreatic
Endoscopic Retrograde Cholangiopancreatography (ERCP)
") Endoscopic Retrograde Cholangiopancreatography (ERCP) Medical Imaging and Treatment of the Bile and Pancreatic Ducts CIE-02718 Understanding ERCP Brochure Update_F.indd 1 7/11/18 9:51 A Minimally Invasive
Endoscopic Retrograde Cholangiopancreatography (ERCP) Medical Imaging and Treatment of the Bile and Pancreatic Ducts CIE-02718 Understanding ERCP Brochure Update_F.indd 1 7/11/18 9:51 A Minimally Invasive
7/11/2017. We re gonna help a lot of people today. Biliary/Pancreatic Endoscopy. AGS July 1-2, Kenneth M. Sigman, MD
 Biliary/Pancreatic Endoscopy AGS July 1-2, 2017 Kenneth M. Sigman, MD We re gonna help a lot of people today 1 2 3 4 Cannulation It all starts with cannulation Double Wire Cannulation Difficult cannulations
Biliary/Pancreatic Endoscopy AGS July 1-2, 2017 Kenneth M. Sigman, MD We re gonna help a lot of people today 1 2 3 4 Cannulation It all starts with cannulation Double Wire Cannulation Difficult cannulations
Intraductal Ultrasonography for the Assessment of Preoperative Biliary and Pancreatic Strictures
 CLINICAL IMAGING Intraductal Ultrasonography for the Assessment of Preoperative Biliary and Pancreatic Strictures Marcel Tantau 1, Teodora Pop 1, Radu Badea 1, Zeno Spirchez 1, Ofelia Moşteanu 1, Alina
CLINICAL IMAGING Intraductal Ultrasonography for the Assessment of Preoperative Biliary and Pancreatic Strictures Marcel Tantau 1, Teodora Pop 1, Radu Badea 1, Zeno Spirchez 1, Ofelia Moşteanu 1, Alina
Gary M. Annunziata, D.O., F.A.C.P. / Anh T. Duong, M.D. / Jonathan C. Lin, M.D., MPH Phone- (760) Fax- (760) Preparation for ERCP
 Fax- (760) Preparation for ERCP") Gary M. Annunziata, D.O., F.A.C.P. / Anh T. Duong, M.D. / Jonathan C. Lin, M.D., MPH Phone- (760) 321-2500 Fax- (760) 321-5720 Preparation for ERCP Patient Name- Procedure Date and Time- Please do not
Gary M. Annunziata, D.O., F.A.C.P. / Anh T. Duong, M.D. / Jonathan C. Lin, M.D., MPH Phone- (760) 321-2500 Fax- (760) 321-5720 Preparation for ERCP Patient Name- Procedure Date and Time- Please do not
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,100 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,100 116,000 120M Open access books available International authors and editors Downloads Our
CPT COD1NG UPDATES Gastroenterology CPT Advisors
 2014 CPT COD1NG UPDATES Gastroenterology CPT Advisors Joel V. Brill, MD, AGA CPT Advisor Daniel C. DeMarco, MD, ACG CPT Advisor Glenn D. Littenberg, MD, ASGE CPT Advisor The American College of Gastroenterology
2014 CPT COD1NG UPDATES Gastroenterology CPT Advisors Joel V. Brill, MD, AGA CPT Advisor Daniel C. DeMarco, MD, ACG CPT Advisor Glenn D. Littenberg, MD, ASGE CPT Advisor The American College of Gastroenterology
6/17/2016. ERCP in June 26, Kenneth M. Sigman, M.D. Birmingham Gastroenterology Associates
 ERCP in 2016 June 26, 2016 Kenneth M. Sigman, M.D. Birmingham Gastroenterology Associates 1 2 3 Diagnostic/Therapeutic ERCP Biliary Obstruction Benign stricture Malignant Stones Ductal injuries Cholangitis
ERCP in 2016 June 26, 2016 Kenneth M. Sigman, M.D. Birmingham Gastroenterology Associates 1 2 3 Diagnostic/Therapeutic ERCP Biliary Obstruction Benign stricture Malignant Stones Ductal injuries Cholangitis
Endoscopic treatment is now the first-line management
 Original Article / Biliary Success rate and complications of endoscopic extraction of common bile duct stones over 2 cm in diameter Xin-Jian Wan, Zheng-Jie Xu, Feng Zhu and Lei Li Shanghai, China BACKGROUND:
Original Article / Biliary Success rate and complications of endoscopic extraction of common bile duct stones over 2 cm in diameter Xin-Jian Wan, Zheng-Jie Xu, Feng Zhu and Lei Li Shanghai, China BACKGROUND:
Research Article The Diagnostic Accuracy of Linear Endoscopic Ultrasound for Evaluating Symptoms Suggestive of Common Bile Duct Stones
 Gastroenterology Research and Practice Volume 2016, Article ID 6957235, 5 pages http://dx.doi.org/10.1155/2016/6957235 Research Article The Diagnostic Accuracy of Linear Endoscopic Ultrasound for Evaluating
Gastroenterology Research and Practice Volume 2016, Article ID 6957235, 5 pages http://dx.doi.org/10.1155/2016/6957235 Research Article The Diagnostic Accuracy of Linear Endoscopic Ultrasound for Evaluating
Comparison of rectal suction versus rectal tube insertion for reducing abdominal symptoms immediately after unsedated colonoscopy
 E725 Comparison of rectal suction versus rectal tube insertion for reducing abdoal symptoms immediately after unsedated colonoscopy Authors Institution Tso-Tsai Liu, Chih-Hsun Yi, Wei-Yi Lei, Hao-Chun
E725 Comparison of rectal suction versus rectal tube insertion for reducing abdoal symptoms immediately after unsedated colonoscopy Authors Institution Tso-Tsai Liu, Chih-Hsun Yi, Wei-Yi Lei, Hao-Chun
Colangitis Esclerosante Primaria: Manejo Clínico y Endoscópico
 Colangitis Esclerosante Primaria: Manejo Clínico y Endoscópico Andrés Cárdenas, MD, MMSc, PhD, AGAF, FAASLD GI / Liver Unit, Hospital Clinic Institut de Malalties Digestives i Metaboliques Associate Professor
Colangitis Esclerosante Primaria: Manejo Clínico y Endoscópico Andrés Cárdenas, MD, MMSc, PhD, AGAF, FAASLD GI / Liver Unit, Hospital Clinic Institut de Malalties Digestives i Metaboliques Associate Professor
Title. CitationEndoscopic Ultrasound, 3(3): Issue Date Doc URL. Rights(URL)
: Issue Date Doc URL. Rights(URL)") Title Effect of antispasmodic drugs on endoscopic ultrasou multicenter randomized controlled trial Kuwatani, Masaki; Kawakami, Hiroshi; Hayashi, Tsuyos Author(s) Naruse, Hirohito; Oba, Koji CitationEndoscopic
Title Effect of antispasmodic drugs on endoscopic ultrasou multicenter randomized controlled trial Kuwatani, Masaki; Kawakami, Hiroshi; Hayashi, Tsuyos Author(s) Naruse, Hirohito; Oba, Koji CitationEndoscopic
Clinical features of gallstone impaction at the ampulla of Vater and the effectiveness of endoscopic biliary drainage without papillotomy
 E806 THIEME Clinical features of gallstone impaction at the ampulla of Vater and the effectiveness of endoscopic biliary drainage without Authors Yuichi Takano 1, Masatsugu Nagahama 1, Naotaka Maruoka
E806 THIEME Clinical features of gallstone impaction at the ampulla of Vater and the effectiveness of endoscopic biliary drainage without Authors Yuichi Takano 1, Masatsugu Nagahama 1, Naotaka Maruoka
Evaluation and Management of Refractory Biliary Stricture. J. David Horwhat, MD, FACG Director of Endoscopy Lancaster Gastroenterology, Inc.
 Evaluation and Management of Refractory Biliary Stricture J. David Horwhat, MD, FACG Director of Endoscopy Lancaster Gastroenterology, Inc Outline What defines a refractory biliary stricture Endoscopic
Evaluation and Management of Refractory Biliary Stricture J. David Horwhat, MD, FACG Director of Endoscopy Lancaster Gastroenterology, Inc Outline What defines a refractory biliary stricture Endoscopic
Impact of Periampullary Diverticulum on ERCP Performance: A Matched Case-Control Study
 ORIGINAL ARTICLE 2018 Aug 21. [Epub ahead of print] https://doi.org/10.5946/ce.2018.070 Print ISSN 2234-2400 On-line ISSN 2234-2443 Open Access Impact of Periampullary Diverticulum on ERCP Performance:
ORIGINAL ARTICLE 2018 Aug 21. [Epub ahead of print] https://doi.org/10.5946/ce.2018.070 Print ISSN 2234-2400 On-line ISSN 2234-2443 Open Access Impact of Periampullary Diverticulum on ERCP Performance:
Source of effectiveness data The evidence for the final outcomes and resource use were derived from a single study.
 Gastroenterologist-administered propofol versus meperidine and midazolam for advanced upper endoscopy: a prospective, randomized trial Vargo J J, Zuccaro G, Dumot J A, Shermock K M, Morrow J B, Conwell
Gastroenterologist-administered propofol versus meperidine and midazolam for advanced upper endoscopy: a prospective, randomized trial Vargo J J, Zuccaro G, Dumot J A, Shermock K M, Morrow J B, Conwell
Single-operator cholangioscopy is useful for visual assessment of bile duct pathology
 Single-operator cholangioscopy is useful for visual assessment of bile duct pathology Finnur Mellemgaard, Rune B. Strandby, Julie Blockmann, Steen C. Kofoed, Lars B. Svendsen & Michael P. Achiam SUMMARY
Single-operator cholangioscopy is useful for visual assessment of bile duct pathology Finnur Mellemgaard, Rune B. Strandby, Julie Blockmann, Steen C. Kofoed, Lars B. Svendsen & Michael P. Achiam SUMMARY
Title: The endoscopic ultrasound-assisted Rendez-Vous technique for treatment of recurrent pancreatitis due to pancreas divisum and ansa pancreatica
 Title: The endoscopic ultrasound-assisted Rendez-Vous technique for treatment of recurrent pancreatitis due to pancreas divisum and ansa pancreatica Authors: Sergio López-Durán, Celia Zaera, Juan Ángel
Title: The endoscopic ultrasound-assisted Rendez-Vous technique for treatment of recurrent pancreatitis due to pancreas divisum and ansa pancreatica Authors: Sergio López-Durán, Celia Zaera, Juan Ángel
Pancreatoscopy-Directed Electrohydraulic Lithotripsy for Pancreatic Ductal Stones in Painful
 Pancreatoscopy-Directed Electrohydraulic Lithotripsy for Pancreatic Ductal Stones in Painful Chronic Pancreatitis Using SpyGlass Short title: EHL for Pancreatic Ductal Stones Noor LH Bekkali 1, MD, PhD;
Pancreatoscopy-Directed Electrohydraulic Lithotripsy for Pancreatic Ductal Stones in Painful Chronic Pancreatitis Using SpyGlass Short title: EHL for Pancreatic Ductal Stones Noor LH Bekkali 1, MD, PhD;
ERCP in altered anatomy. Lars Aabakken Oslo University Hospital - Rikshospitalet Oslo, Norway
 ERCP in altered anatomy Lars Aabakken Oslo University Hospital - Rikshospitalet Oslo, Norway CO2 as insufflation gas Reduces post-procedure pain Reduces in-procedure bowel distension Improves the intubation
ERCP in altered anatomy Lars Aabakken Oslo University Hospital - Rikshospitalet Oslo, Norway CO2 as insufflation gas Reduces post-procedure pain Reduces in-procedure bowel distension Improves the intubation
Having an ERCP (endoscopic retrograde cholangio pancreatogram)
") Having an ERCP (endoscopic retrograde cholangio pancreatogram) The aim of this information sheet is to help answer some of the questions you may have about having an ERCP. It explains what it is, why it
Having an ERCP (endoscopic retrograde cholangio pancreatogram) The aim of this information sheet is to help answer some of the questions you may have about having an ERCP. It explains what it is, why it
Primary Sclerosing Cholangitis and Cholestatic liver diseases. Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants
 Primary Sclerosing Cholangitis and Cholestatic liver diseases Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants I have nothing to disclose Educational Objectives What is PSC? Understand the cholestatic
Primary Sclerosing Cholangitis and Cholestatic liver diseases Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants I have nothing to disclose Educational Objectives What is PSC? Understand the cholestatic
Endoscopic Papillary Balloon Dilation with Large Balloon after Limited Sphincterotomy for Retrieval of Choledocholithiasis
 Yonsei Medical Journal Vol. 47, No. 6, pp. 805-810, 2006 Endoscopic Papillary Balloon Dilation with Large Balloon after Limited Sphincterotomy for Retrieval of Choledocholithiasis Seungmin Bang, Myoung
Yonsei Medical Journal Vol. 47, No. 6, pp. 805-810, 2006 Endoscopic Papillary Balloon Dilation with Large Balloon after Limited Sphincterotomy for Retrieval of Choledocholithiasis Seungmin Bang, Myoung
Sphincter of Oddi Dysfunction: What s the Verdict in 2014?
 SGNA March 2014 Sphincter of Oddi Dysfunction: What s the Verdict in 2014? Evan L. Fogel, M.D. Professor of Clinical Medicine ERCP Fellowship Director Division of Gastroenterology/Hepatology Indiana University
SGNA March 2014 Sphincter of Oddi Dysfunction: What s the Verdict in 2014? Evan L. Fogel, M.D. Professor of Clinical Medicine ERCP Fellowship Director Division of Gastroenterology/Hepatology Indiana University
New approach to decrease post-ercp adverse events in patients with primary sclerosing cholangitis
 Original article New approach to decrease post-ercp adverse events in patients with primary sclerosing cholangitis Authors Udayakumar Navaneethan 1, 2, Dennisdhilak Lourdusamy 2, Norma G Gutierrez 2,XiangZhu
Original article New approach to decrease post-ercp adverse events in patients with primary sclerosing cholangitis Authors Udayakumar Navaneethan 1, 2, Dennisdhilak Lourdusamy 2, Norma G Gutierrez 2,XiangZhu
RESEARCH ARTICLE. Clinical Efficacy of Endoscopic Pancreatic Drainage for Pain Relief with Malignant Pancreatic Duct Obstruction
 DOI:http://dx.doi.org/10.7314/APJCP.2014.15.16.6823 RESEARCH ARTICLE Clinical Efficacy of Endoscopic Pancreatic Drainage for Pain Relief with Malignant Pancreatic Duct Obstruction Fei Gao 1 *, Shuren Ma
DOI:http://dx.doi.org/10.7314/APJCP.2014.15.16.6823 RESEARCH ARTICLE Clinical Efficacy of Endoscopic Pancreatic Drainage for Pain Relief with Malignant Pancreatic Duct Obstruction Fei Gao 1 *, Shuren Ma
Erratum with Corrected and Republished Article
 CopyrightC 2017 by Okayama University Medical School. Erratum with Corrected and Republished Article http : escholarship.lib.okayama u.ac.jp amo In the article by et al. entitled, which appeared in the
CopyrightC 2017 by Okayama University Medical School. Erratum with Corrected and Republished Article http : escholarship.lib.okayama u.ac.jp amo In the article by et al. entitled, which appeared in the
Approach to the Biliary Stricture
 Approach to the Biliary Stricture ACG Eastern Postgraduate Course Washington DC June 8, 2014 Steven A. Edmundowicz MD FASGE Chief of Endoscopy Division of Gastroenterology Professor of Medicine Disclosures
Approach to the Biliary Stricture ACG Eastern Postgraduate Course Washington DC June 8, 2014 Steven A. Edmundowicz MD FASGE Chief of Endoscopy Division of Gastroenterology Professor of Medicine Disclosures
THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 96, No. 10, by Am. Coll. of Gastroenterology ISSN /01/$20.00
 THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 96, No. 10, 2001 2001 by Am. Coll. of Gastroenterology ISSN 0002-9270/01/$20.00 Published by Elsevier Science Inc. PII S0002-9270(01)02807-6 Can Endoscopic
THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 96, No. 10, 2001 2001 by Am. Coll. of Gastroenterology ISSN 0002-9270/01/$20.00 Published by Elsevier Science Inc. PII S0002-9270(01)02807-6 Can Endoscopic
Title: Pancreatic stents in ERCP. Where are we? Authors: Francisco Pérez Roldán, Pedro González Carro
 Title: Pancreatic stents in ERCP. Where are we? Authors: Francisco Pérez Roldán, Pedro González Carro DOI: 10.17235/reed.2018.5670/2018 Link: PubMed (Epub ahead of print) Please cite this article as: Pérez
Title: Pancreatic stents in ERCP. Where are we? Authors: Francisco Pérez Roldán, Pedro González Carro DOI: 10.17235/reed.2018.5670/2018 Link: PubMed (Epub ahead of print) Please cite this article as: Pérez
Chronic pancreatitis mimicking intraductal papillary mucinous neoplasm of the pancreas; Report of tow cases
 Jichi Medical University Journal Chronic pancreatitis mimicking intraductal papillary mucinous neoplasm of the pancreas; Report of tow cases Noritoshi Mizuta, Hiroshi Noda, Nao Kakizawa, Nobuyuki Toyama,
Jichi Medical University Journal Chronic pancreatitis mimicking intraductal papillary mucinous neoplasm of the pancreas; Report of tow cases Noritoshi Mizuta, Hiroshi Noda, Nao Kakizawa, Nobuyuki Toyama,
Efficacy and safety of sedation during endoscopic submucosal dissection of gastric cancers using a comparative trial of propofol versus midazolam
 Efficacy and safety of sedation during endoscopic submucosal dissection of gastric cancers using a comparative trial of propofol versus midazolam Authors Hitomi Kikuchi 1, 2,TakutoHikichi 1, Ko Watanabe
Efficacy and safety of sedation during endoscopic submucosal dissection of gastric cancers using a comparative trial of propofol versus midazolam Authors Hitomi Kikuchi 1, 2,TakutoHikichi 1, Ko Watanabe
Young Hoon Youn Hyun Chul Lim Jae Hoon Jahng Sung Il Jang Jung Hwan You Jung Soo Park Se Joon Lee Dong Ki Lee
 Dig Dis Sci (2011) 56:1572 1577 DOI 10.1007/s10620-010-1438-4 ORIGINAL ARTICLE The Increase in Balloon Size to Over 15 mm Does Not Affect the Development of Pancreatitis After Endoscopic Papillary Large
Dig Dis Sci (2011) 56:1572 1577 DOI 10.1007/s10620-010-1438-4 ORIGINAL ARTICLE The Increase in Balloon Size to Over 15 mm Does Not Affect the Development of Pancreatitis After Endoscopic Papillary Large
During endoscopic retrograde cholangiopancreatography CLINICAL BILIARY
 GASTROENTEROLOGY 2013;144:341 345 CLINICAL BILIARY Randomized Trial of Endoscopic Sphincterotomy With Balloon Dilation Versus Endoscopic Sphincterotomy Alone for Removal of Bile Duct Stones ANTHONY YUEN
GASTROENTEROLOGY 2013;144:341 345 CLINICAL BILIARY Randomized Trial of Endoscopic Sphincterotomy With Balloon Dilation Versus Endoscopic Sphincterotomy Alone for Removal of Bile Duct Stones ANTHONY YUEN
ACG Clinical Guideline: Primary Sclerosing Cholangitis
 ACG Clinical Guideline: Primary Sclerosing Cholangitis Keith D. Lindor, MD, FACG 1, Kris V. Kowdley, MD, FACG 2, and M. Edwyn Harrison, MD 3 1 College of Health Solutions, Arizona State University, Phoenix,
ACG Clinical Guideline: Primary Sclerosing Cholangitis Keith D. Lindor, MD, FACG 1, Kris V. Kowdley, MD, FACG 2, and M. Edwyn Harrison, MD 3 1 College of Health Solutions, Arizona State University, Phoenix,
Clinical Study Utility and Safety of ERCP in the Elderly: A Comparative Study in Iran
 Hindawi Publishing Corporation Diagnostic and Therapeutic Endoscopy Volume 2012, Article ID 439320, 5 pages doi:10.1155/2012/439320 Clinical Study Utility and Safety of ERCP in the Elderly: A Comparative
Hindawi Publishing Corporation Diagnostic and Therapeutic Endoscopy Volume 2012, Article ID 439320, 5 pages doi:10.1155/2012/439320 Clinical Study Utility and Safety of ERCP in the Elderly: A Comparative
Tratamiento endoscópico de la CEP. En quien como y cuando?
 Tratamiento endoscópico de la CEP. En quien como y cuando? Andrés Cárdenas, MD, MMSc, PhD, AGAF, FAASLD GI / Liver Unit, Hospital Clinic Institut de Malalties Digestives i Metaboliques University of Barcelona
Tratamiento endoscópico de la CEP. En quien como y cuando? Andrés Cárdenas, MD, MMSc, PhD, AGAF, FAASLD GI / Liver Unit, Hospital Clinic Institut de Malalties Digestives i Metaboliques University of Barcelona
CPT 2014 Overview of GI Changes
 CPT 2014 Overview of GI Changes The following table is a listing of the new,, and deleted codes in the Esophagus/Endoscopy section effective January 1, 2014. The table lists the CPT code, a brief description
CPT 2014 Overview of GI Changes The following table is a listing of the new,, and deleted codes in the Esophagus/Endoscopy section effective January 1, 2014. The table lists the CPT code, a brief description
stents she/he is providing appropriate or inappropriate care?
 Pancreatic Stents Are They Now State of the Art Care? To Help Limit Post ERCP Pancreatitis Glen A. Lehman, M.D. Professor of Medicine and Radiology Division of Gastroenterology/Hepatology Indiana University
Pancreatic Stents Are They Now State of the Art Care? To Help Limit Post ERCP Pancreatitis Glen A. Lehman, M.D. Professor of Medicine and Radiology Division of Gastroenterology/Hepatology Indiana University
E ndoscopic retrograde cholangiopancreatography (ERCP)
") 240 BILIARY DISEASE Endoscopic transpapillary biopsies and intraductal ultrasonography in the diagnostics of bile duct strictures: a prospective study D Domagk, C Poremba, K-H Dietl, N Senninger, A Heinecke,
240 BILIARY DISEASE Endoscopic transpapillary biopsies and intraductal ultrasonography in the diagnostics of bile duct strictures: a prospective study D Domagk, C Poremba, K-H Dietl, N Senninger, A Heinecke,
Tools of the Gastroenterologist: Introduction to GI Endoscopy
 Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Pictorial review of Benign Biliary tract abnormality on MRCP/MRI Liver with Endoscopic (including splyglass) and Endoscopic Ultrasound correlation
 and Endoscopic Ultrasound correlation") Pictorial review of Benign Biliary tract abnormality on MRCP/MRI Liver with Endoscopic (including splyglass) and Endoscopic Ultrasound correlation Poster No.: C-2617 Congress: ECR 2015 Type: Educational
Pictorial review of Benign Biliary tract abnormality on MRCP/MRI Liver with Endoscopic (including splyglass) and Endoscopic Ultrasound correlation Poster No.: C-2617 Congress: ECR 2015 Type: Educational
Oral anti-thrombotic therapy-management in patients requiring endoscopy
 Oral anti-thrombotic therapy-management in patients requiring endoscopy Management of anti-thrombotic therapy in patients requiring endoscopy This guideline suggests appropriate management of patients
Oral anti-thrombotic therapy-management in patients requiring endoscopy Management of anti-thrombotic therapy in patients requiring endoscopy This guideline suggests appropriate management of patients
A comparison of 4-Fr with 5-Fr endoscopic nasopancreatic drainage catheters: A randomized, controlled trial
 bs_bs_banner doi:10.1111/jgh.13314 GASTROENTEROLOGY A comparison of 4-Fr with 5-Fr endoscopic nasopancreatic drainage catheters: A randomized, controlled trial Teruo Mouri, Tamito Sasaki, Masahiro Serikawa,
bs_bs_banner doi:10.1111/jgh.13314 GASTROENTEROLOGY A comparison of 4-Fr with 5-Fr endoscopic nasopancreatic drainage catheters: A randomized, controlled trial Teruo Mouri, Tamito Sasaki, Masahiro Serikawa,
Diagnosis of tumor extension in biliary carcinoma has. Differential Diagnosis and Treatment of Biliary Strictures
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2009;7:S79 S83 Differential Diagnosis and Treatment of Biliary Strictures KAZUO INUI, JUNJI YOSHINO, and HIRONAO MIYOSHI Department of Internal Medicine, Second
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2009;7:S79 S83 Differential Diagnosis and Treatment of Biliary Strictures KAZUO INUI, JUNJI YOSHINO, and HIRONAO MIYOSHI Department of Internal Medicine, Second
Diagnosis and Management of Primary Sclerosing Cholangitis:
 Diagnosis and Management of Primary Sclerosing Cholangitis: The Role of the Endoscopist Adam Slivka MD-PhD Associate Chief of the Division Gastroenterology Hepatology and Nutrition University of Pittsburgh
Diagnosis and Management of Primary Sclerosing Cholangitis: The Role of the Endoscopist Adam Slivka MD-PhD Associate Chief of the Division Gastroenterology Hepatology and Nutrition University of Pittsburgh
ENDOSCOPY IN COMPETITION DIAGNOSTICS. Dr. med. Dirk Hartmann Klinikum Ludwigshafen
 Falk Symposium 166 GI Endoscopy Standards and Innovations Mainz, 18. 19. September 2008 ENDOSCOPY IN COMPETITION DIAGNOSTICS Dr. med. Dirk Hartmann Klinikum Ludwigshafen ENDOSCOPY IN COMPETITION Competing
Falk Symposium 166 GI Endoscopy Standards and Innovations Mainz, 18. 19. September 2008 ENDOSCOPY IN COMPETITION DIAGNOSTICS Dr. med. Dirk Hartmann Klinikum Ludwigshafen ENDOSCOPY IN COMPETITION Competing
ORIGINAL PAPER. Feasibility of the unilateral-flange stent for the treatment of benign pancreatic duct stricture: a pilot study
 Nagoya J. Med. Sci. 79. 453 ~ 458, 2017 doi:10.18999/nagjms.79.4.453 ORIGINAL PAPER Feasibility of the unilateral-flange stent for the treatment of benign pancreatic duct stricture: a pilot study Patommatat
Nagoya J. Med. Sci. 79. 453 ~ 458, 2017 doi:10.18999/nagjms.79.4.453 ORIGINAL PAPER Feasibility of the unilateral-flange stent for the treatment of benign pancreatic duct stricture: a pilot study Patommatat
The Pancreas. Basic Anatomy. Endocrine pancreas. Exocrine pancreas. Pancreas vasculature. Islets of Langerhans. Acinar cells Ductal System
 SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
Perforations Occurring during ERCP: A Complication to Take into Account
 Case report Perforations Occurring during ERCP: A Complication to Take into Account Martín Alonso Gómez Zuleta, MD, 1 David Andrés Viveros Carreño, MD. 2 1 Gastroenterology Unit at the Universidad Nacional
Case report Perforations Occurring during ERCP: A Complication to Take into Account Martín Alonso Gómez Zuleta, MD, 1 David Andrés Viveros Carreño, MD. 2 1 Gastroenterology Unit at the Universidad Nacional
RX Biliary System. Start
 Start We re in! When you control the wire, efficiency comes along for the ride. The of Physician-Controlled Wireguided Cannulation Physician-controlled wireguided cannulation (WGC) facilitates deep biliary
Start We re in! When you control the wire, efficiency comes along for the ride. The of Physician-Controlled Wireguided Cannulation Physician-controlled wireguided cannulation (WGC) facilitates deep biliary
Takayuki; Eguchi, Susumu; Kanematsu. Citation Pediatric surgery international, 27
 NAOSITE: Nagasaki University's Ac Title Author(s) Endoscopic balloon dilatation for c jejunum in an infant. Mochizuki, Kyoko; Obatake, Masayuki Takayuki; Eguchi, Susumu; Kanematsu Citation Pediatric surgery
NAOSITE: Nagasaki University's Ac Title Author(s) Endoscopic balloon dilatation for c jejunum in an infant. Mochizuki, Kyoko; Obatake, Masayuki Takayuki; Eguchi, Susumu; Kanematsu Citation Pediatric surgery
The modified pancreatic stent system for prevention of post-ercp pancreatitis: a case-control study
 Zhang et al. BMC Gastroenterology (2017) 17:108 DOI 10.1186/s12876-017-0661-2 TECHNICAL ADVANCE Open Access The modified pancreatic stent system for prevention of post-ercp pancreatitis: a case-control
Zhang et al. BMC Gastroenterology (2017) 17:108 DOI 10.1186/s12876-017-0661-2 TECHNICAL ADVANCE Open Access The modified pancreatic stent system for prevention of post-ercp pancreatitis: a case-control
Title. CitationHepato-Gastroenterology, 61(135): Issue Date Doc URL. Type. File Information. IgG4-Related Sclerosing Cholangitis
: Issue Date Doc URL. Type. File Information. IgG4-Related Sclerosing Cholangitis") Title Difference from Bile Duct Cancer and Relationship be IgG4-Related Sclerosing Cholangitis Kuwatani, Masaki; Kawakami, Hiroshi; Zen, Yoh; Kawak Author(s) Sakamoto, Naoya CitationHepato-Gastroenterology,
Title Difference from Bile Duct Cancer and Relationship be IgG4-Related Sclerosing Cholangitis Kuwatani, Masaki; Kawakami, Hiroshi; Zen, Yoh; Kawak Author(s) Sakamoto, Naoya CitationHepato-Gastroenterology,
The authors have declared no conflicts of interest.
 Diagnostic Accuracy of Magnetic Resonance Cholangiopancreatography Versus Endoscopic Retrograde Cholangiopancreatography Findings in the Postorthotopic Liver Transplant Population Authors: *Ashok Shiani,
Diagnostic Accuracy of Magnetic Resonance Cholangiopancreatography Versus Endoscopic Retrograde Cholangiopancreatography Findings in the Postorthotopic Liver Transplant Population Authors: *Ashok Shiani,
Congenital dilatation of the common bile duct and pancreaticobiliary maljunction clinical implications
 Langenbecks Arch Surg (2009) 394:209 213 DOI 10.1007/s00423-008-0330-6 CURRENT CONCEPT IN CLINICAL SURGERY Congenital dilatation of the common bile duct and pancreaticobiliary maljunction clinical implications
Langenbecks Arch Surg (2009) 394:209 213 DOI 10.1007/s00423-008-0330-6 CURRENT CONCEPT IN CLINICAL SURGERY Congenital dilatation of the common bile duct and pancreaticobiliary maljunction clinical implications
Magnetic Resonance Cholangiopancreatography (MRCP) in a District General Hospital
 in a District General Hospital") Magnetic Resonance Cholangiopancreatography (MRCP) in a District General Hospital Poster No.: C-1790 Congress: ECR 2012 Type: Authors: Scientific Exhibit J. A. Maguire 1, H. Kasem 2, M. Akhtar 2, M. Strauss
Magnetic Resonance Cholangiopancreatography (MRCP) in a District General Hospital Poster No.: C-1790 Congress: ECR 2012 Type: Authors: Scientific Exhibit J. A. Maguire 1, H. Kasem 2, M. Akhtar 2, M. Strauss
Research paper 37. European Journal of Cancer Prevention 2015, 24: Keywords: carbon dioxide, cecal intubation, colonoscopy, screening
 Research paper 37 Carbon dioxide insufflation during screening unsedated colonoscopy: a randomised clinical trial Miroslaw Szura, Radoslaw Pach, Andrzej Matyja and Jan Kulig One of the methods used to
Research paper 37 Carbon dioxide insufflation during screening unsedated colonoscopy: a randomised clinical trial Miroslaw Szura, Radoslaw Pach, Andrzej Matyja and Jan Kulig One of the methods used to
Research Article Safety and Yield of Diagnostic ERCP in Liver Transplant Patients with Abnormal Liver Function Tests
 Diagnostic and erapeutic Endoscopy, Article ID 314927, 5 pages http://dx.doi.org/10.1155/2014/314927 Research Article Safety and Yield of Diagnostic ERCP in Liver Transplant Patients with Abnormal Liver
Diagnostic and erapeutic Endoscopy, Article ID 314927, 5 pages http://dx.doi.org/10.1155/2014/314927 Research Article Safety and Yield of Diagnostic ERCP in Liver Transplant Patients with Abnormal Liver
Endoscopic Ultrasonography Clinical Impact. Giancarlo Caletti. Gastroenterologia Università di Bologna. Caletti
 Clinical Impact Giancarlo Gastroenterologia Università di Bologna AUSL di Imola,, Castel S. Pietro Terme (BO) 1982 Indications Diagnosis of Submucosal Tumors (SMT) Staging of Neoplasms Evaluation of Pancreato-Biliary
Clinical Impact Giancarlo Gastroenterologia Università di Bologna AUSL di Imola,, Castel S. Pietro Terme (BO) 1982 Indications Diagnosis of Submucosal Tumors (SMT) Staging of Neoplasms Evaluation of Pancreato-Biliary
Role of Therapeutic Endoscopy in Hepatic Hydatid Disease after Surgical Intervention: Case Report
 ISPUB.COM The Internet Journal of Gastroenterology Volume 10 Number 2 Role of Therapeutic Endoscopy in Hepatic Hydatid Disease after Surgical Intervention: Case Report H Ono, M Okabe, T Kimura, M Kawakami,
ISPUB.COM The Internet Journal of Gastroenterology Volume 10 Number 2 Role of Therapeutic Endoscopy in Hepatic Hydatid Disease after Surgical Intervention: Case Report H Ono, M Okabe, T Kimura, M Kawakami,
A patient with an unusual congenital anomaly of the pancreaticobiliary tree
 A patient with an unusual congenital anomaly of the pancreaticobiliary tree Thomas Hocker, HMS IV BIDMC Core Radiology Case Presentation September 17, 2007 Review of Normal Pancreaticobiliary Tract Anatomy
A patient with an unusual congenital anomaly of the pancreaticobiliary tree Thomas Hocker, HMS IV BIDMC Core Radiology Case Presentation September 17, 2007 Review of Normal Pancreaticobiliary Tract Anatomy
LIVER, PANCREAS, AND BILIARY TRACT
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2012;10:1157 1161 LIVER, PANCREAS, AND BILIARY TRACT Delayed and Unsuccessful Endoscopic Retrograde Cholangiopancreatography Are Associated With Worse Outcomes
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2012;10:1157 1161 LIVER, PANCREAS, AND BILIARY TRACT Delayed and Unsuccessful Endoscopic Retrograde Cholangiopancreatography Are Associated With Worse Outcomes
IgG4-Negative Autoimmune Pancreatitis with Sclerosing Cholangitis and Colitis: Possible Association with Primary Sclerosing Cholangitis?
 CASE REPORT IgG4-Negative Autoimmune Pancreatitis with Sclerosing Cholangitis and Colitis: Possible Association with Primary Sclerosing Cholangitis? Keita Saeki 1, Shigenari Hozawa 1, Naoteru Miyata 1,
CASE REPORT IgG4-Negative Autoimmune Pancreatitis with Sclerosing Cholangitis and Colitis: Possible Association with Primary Sclerosing Cholangitis? Keita Saeki 1, Shigenari Hozawa 1, Naoteru Miyata 1,
Naoyuki Toyota, Tadahiro Takada, Hodaka Amano, Masahiro Yoshida, Fumihiko Miura, and Keita Wada
 J Hepatobiliary Pancreat Surg (2006) 13:80 85 DOI 10.1007/s00534-005-1062-4 Endoscopic naso-gallbladder drainage in the treatment of acute cholecystitis: alleviates inflammation and fixes operator s aim
J Hepatobiliary Pancreat Surg (2006) 13:80 85 DOI 10.1007/s00534-005-1062-4 Endoscopic naso-gallbladder drainage in the treatment of acute cholecystitis: alleviates inflammation and fixes operator s aim
ORIGINAL ARTICLE Gastroenterology & Hepatology INTRODUCTION MATERIALS AND METHODS
 ORIGINAL ARTICLE Gastroenterology & Hepatology https://doi.org/10.3346/jkms.2017.32.11.1814 J Korean Med Sci 2017; 32: 1814-1819 Prediction of Post-Endoscopic Retrograde Cholangiopancreatography Pancreatitis
ORIGINAL ARTICLE Gastroenterology & Hepatology https://doi.org/10.3346/jkms.2017.32.11.1814 J Korean Med Sci 2017; 32: 1814-1819 Prediction of Post-Endoscopic Retrograde Cholangiopancreatography Pancreatitis
Figure 2: Post-cholecystectomy biliary-like pain
 Figure 2: Post-cholecystectomy biliary-like pain 1 patient with recurrent episodes of pain (not daily), in the epigastrium/right upper quadrant, lasting >30 mins, building to a steady level, interrupting
Figure 2: Post-cholecystectomy biliary-like pain 1 patient with recurrent episodes of pain (not daily), in the epigastrium/right upper quadrant, lasting >30 mins, building to a steady level, interrupting
INTRODUCTION ORIGINAL ARTICLE
 ORIGINAL ARTICLE Clin Endosc 2017;50:464-472 https://doi.org/10.5946/ce.2016.161 Print ISSN 2234-2400 On-line ISSN 2234-2443 Open Access Carbon Dioxide versus Air Insufflation in Gastric Endoscopic Submucosal
ORIGINAL ARTICLE Clin Endosc 2017;50:464-472 https://doi.org/10.5946/ce.2016.161 Print ISSN 2234-2400 On-line ISSN 2234-2443 Open Access Carbon Dioxide versus Air Insufflation in Gastric Endoscopic Submucosal
Effectiveness and safety of metallic stent for ileocecal obstructive colon cancer: a report of 4 cases
 Effectiveness and safety of metallic stent for ileocecal obstructive colon cancer: a report of 4 cases Authors Tatsuya Ishii 1,KosukeMinaga 2, Satoshi Ogawa 3, Maiko Ikenouchi 1, Tomoe Yoshikawa 1,TakujiAkamatsu
Effectiveness and safety of metallic stent for ileocecal obstructive colon cancer: a report of 4 cases Authors Tatsuya Ishii 1,KosukeMinaga 2, Satoshi Ogawa 3, Maiko Ikenouchi 1, Tomoe Yoshikawa 1,TakujiAkamatsu
Sphincter of Oddi Dysfunction Type III, Manometry and Sphincterotomy: Sham Won, Game Over
 Sphincter of Oddi Dysfunction Type III, Manometry and Sphincterotomy: Sham Won, Game Over C. Mel Wilcox, M.D., M.S.P.H. Professor of Medicine, Surgery and Pediatrics University of Alabama, Birmingham Basil
Sphincter of Oddi Dysfunction Type III, Manometry and Sphincterotomy: Sham Won, Game Over C. Mel Wilcox, M.D., M.S.P.H. Professor of Medicine, Surgery and Pediatrics University of Alabama, Birmingham Basil