Patient Encounters in the Primary Care Setting
|
|
|
- Camron White
- 5 years ago
- Views:
Transcription

1 Patient Encounters in the Primary Care Setting Carmine D Amico, D.O. Clinical Cases Overview Learning objectives Clinical case presentations Questions for audience participation 1
2 Clinical Cases Learning Objectives 1. Realize that patients with undiagnosed cardiovascular disease will sometimes present to their primary care physician s office. 2. Appreciate that web-based resources are available that can be very useful to health care providers in managing patients with cardiovascular disease. 3. Apply current practice guidelines to clinical scenarios. Case 1 A 60-year-old female presents to your office as a new patient. She recently moved here from out of town and she would like to establish care with you. What has prompted her to seek medical attention at this time is a 1-2 week history of palpitations (feeling like her heart was stopping) associated with lightheadedness and chest tightness. These symptoms seem to be getting worse, although she denies syncope. Her medical history is significant for osteoarthritis, hypertension, venous insufficiency, and schizophrenia. She has no known allergies. Her medications include meloxicam 15 mg PO daily, amlodipine 10 mg PO daily, furosemide 80 mg PO daily, metolazone 2.5 mg PO daily, and thioridazine 200 mg PO BID. She smokes cigarettes, and she has a 40- pack-year history of smoking (one pack of cigarettes per day for 40 years). She denies use of alcohol or illicit drugs. She has had no previous surgeries. Her family history is unknown, as she is adopted. 2
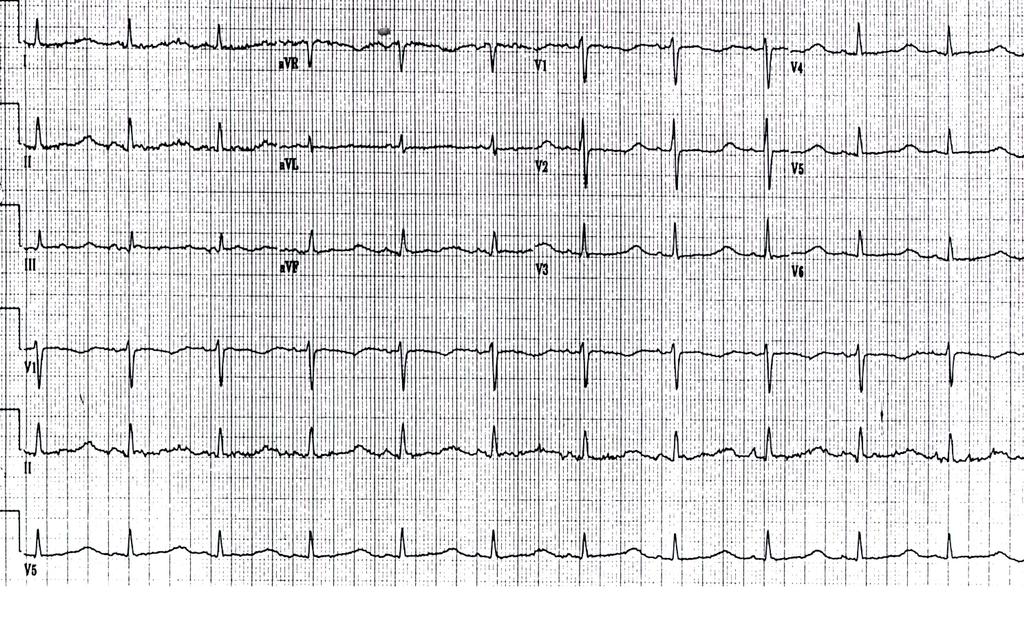
3 Case 1 (cont.) Physical examination reveals: blood pressure 126/82 mmhg, pulse 64 bpm, and respirations 12 per min. There is no jugular venous distension. There are no carotid bruits. Lungs are clear to auscultation bilaterally. Cardiac rhythm is regular. S1 and S2 are normal. There is no third or fourth heart sound. There is no cardiac murmur. There is no pericardial friction rub. The abdomen is soft and nontender, with no palpable masses or organomegaly. Bowel sounds are active. There is mild pitting edema of the distal aspects of both lower extremities. Stasis dermatitis changes are present on the distal aspects of both lower extremities. Distal pulses are intact and bilaterally equal in both the upper and the lower extremities. There is no evidence of gross motor or sensory neurological deficits. Case 1 (cont.) Prior to sending this patient elsewhere for further evaluation, is there anything else that can done in the office that could be of value in determining the cause of her symptoms? 3
 The following rhythm change occurred 29 minutes after the")
4 Cardiovascular Case 1 Case 1 (cont.) The following rhythm change occurred 29 minutes after the preceding EKG was recorded 4
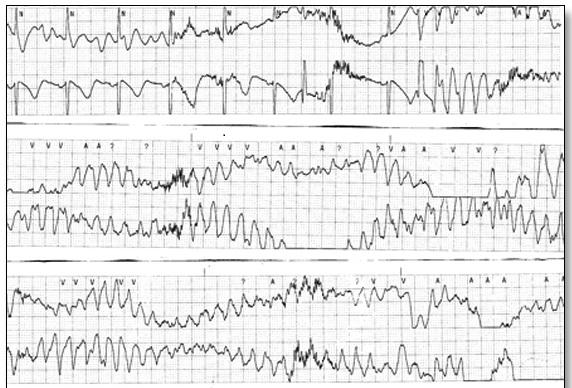
5 Cardiovascular Case 1 5
 Is any")

6 Case 1 (cont.) Is any additional testing indicated at this time? 6
7 Cardiovascular Case 1 Glucose (65-99 mg/dl) 108 BUN (7-18 mg/dl) 32 Creatinine ( mg/dl) 1.2 Na+ ( mmol/l) 131 K+ ( mmol/l) 2.1 Cl- ( mmol/l) 96 CO2 (21-31 mmol/l) 35 Calcium ( mg/dl) 9.9 Phosphorous ( mg/dl) 3.7 Uric acid ( mg/dl) 5 Total protein ( g/dl) 6.4 Albumin ( g/dl) 3.5 Globulin ( g/dl) 2.9 A / G ratio ( ) 1.2 Total bilirubin ( mg/dl) 0.8 Alk. Phosphatase ( U/L) 47 AST (15-37 U/L) 60 ALT (30-65 U/L) 45 LDH ( U/L) 146 Cholesterol (0-200 mg/dl) 167 Triglycerides ( mg/dl) 169 HDL (40-60 mg/dl) 46 LDL (0-100 mg/dl) 87 Chol. / HDL ratio (< 4.5) 3.6 Cardiovascular Case 1 Glucose (65-99 mg/dl) 108 BUN (7-18 mg/dl) 32 Creatinine ( mg/dl) 1.2 Na+ ( mmol/l) 131 K+ ( mmol/l) 2.1 Cl- ( mmol/l) 96 CO2 (21-31 mmol/l) 35 Calcium ( mg/dl) 9.9 Phosphorous ( mg/dl) 3.7 Uric acid ( mg/dl) 5 Total protein ( g/dl) 6.4 Albumin ( g/dl) 3.5 Globulin ( g/dl) 2.9 A / G ratio ( ) 1.2 Total bilirubin ( mg/dl) 0.8 Alk. Phosphatase ( U/L) 47 AST (15-37 U/L) 60 ALT (30-65 U/L) 45 LDH ( U/L) 146 Cholesterol (0-200 mg/dl) 167 Triglycerides ( mg/dl) 169 HDL (40-60 mg/dl) 46 LDL (0-100 mg/dl) 87 Chol. / HDL ratio (< 4.5) 3.6 7
8 Case 1 (cont.) How could this problem have been prevented? Case 2 A 46-year-old female presents for preoperative evaluation prior to elective total abdominal hysterectomy. Her medical history is significant for uterine fibroids, hypertension, and paroxysmal atrial fibrillation. An echocardiogram performed last month revealed normal left ventricular systolic function, mild tricuspid regurgitation, trace mitral regurgitation, and no significant structural abnormalities. Her medications include warfarin 2 mg PO daily and atenolol 25 mg PO BID. Her INR is 2.8. The remainder of her lab work (CBC and CMP) is within normal limits. Physical examination reveals: blood pressure 126/82 mmhg, pulse 80 bpm, and respirations 12 per min. There is no jugular venous distension, lungs are clear to auscultation bilaterally (no crackles or wheezes), cardiac rhythm is regular and there is no S3, S4, murmur, or rub. There is no peripheral edema. 8
9 Case 2 (cont.) Which of the following is the most appropriate recommendation regarding anticoagulation prior to surgery? A. Discontinue warfarin now, as anticoagulation is not indicated in this patient. B. Discontinue warfarin four days prior to scheduled surgery. Check the INR daily. When the INR is < 2, begin enoxaparin 1 mg/kg SQ BID and continue it until the morning of surgery. C. Discontinue warfarin four days prior to scheduled surgery. Check the INR the morning of scheduled surgery. Proceed with surgery if the INR is < 2. D. Continue warfarin through the day before scheduled surgery. Withhold warfarin on the morning of surgery and initiate a continuous intravenous infusion of unfractionated heparin, which may then be discontinued on call to the operating room. Case 2 (cont.) What is this patient s CHADS2 score? A. 0 B. 1 C. 2 D. 3 E. 4 F. 5 G. 6 9
10 Atrial Fibrillation Anticoagulation CHADS 2 Risk Stratification Scheme Risk Factors Score C Congestive heart failure 1 H Hypertension 1 A Age ³75 years 1 D Diabetes mellitus 1 S 2 History of stroke or transient ischemic attack 2 Rockson et al. J Am Coll Cardiol. 2004;43: Atrial Fibrillation Anticoagulation CHADS 2 Risk Stratification Scheme Risk Factors Score C Congestive heart failure 1 H Hypertension 1 A Age ³75 years 1 D Diabetes mellitus 1 S 2 History of stroke or transient ischemic attack 2 Rockson et al. J Am Coll Cardiol. 2004;43:
11 Case 2 (cont.) What is this patient s CHADS2 score? A. 0 B. 1 C. 2 D. 3 E. 4 F. 5 G. 6 Case 2 (cont.) What is this patient s CHADS2 score? A. 0 B. 1 C. 2 D. 3 E. 4 F. 5 G. 6 11
12 Atrial Fibrillation Anticoagulation CHADS 2 Risk Stratification Scheme (cont.) Score Recommended therapy 0 Aspirin (81 to 325 mg daily) 1 Aspirin (81 to 325 mg daily) or Warfarin (INR ) 2-6 Warfarin (INR ) Rockson et al. J Am Coll Cardiol. 2004;43: Atrial Fibrillation Anticoagulation CHADS 2 Risk Stratification Scheme (cont.) Score Recommended therapy 0 Aspirin (81 to 325 mg daily) 1 Aspirin (81 to 325 mg daily) or Warfarin (INR ) 2-6 Warfarin (INR ) Rockson et al. J Am Coll Cardiol. 2004;43:
13 Case 2 (cont.) What is this patient s CHA2DS2-VASc score? A. 0 B. 1 C. 2 D. 3 E. 4 F. 5 G. 6 H. 7 I. 8 J. 9 Atrial Fibrillation Anticoagulation CHA 2 DS 2 VASc Risk Stratification Scheme Risk Factors Score C Congestive heart failure 1 H Hypertension 1 A 2 Age ³75 years 2 D Diabetes mellitus 1 S 2 History of stroke or transient ischemic attack 2 V Vascular disease 1 A Age years 1 Sc Sex category (female gender) 1 Lip et al. Chest. 2010;137:
14 Atrial Fibrillation Anticoagulation CHA 2 DS 2 VASc Risk Stratification Scheme Risk Factors Score C Congestive heart failure 1 H Hypertension 1 A 2 Age ³75 years 2 D Diabetes mellitus 1 S 2 History of stroke or transient ischemic attack 2 V Vascular disease 1 A Age years 1 Sc Sex category (female gender) 1 Lip et al. Chest. 2010;137: Case 2 (cont.) What is this patient s CHA2DS2-VASc score? A. 0 B. 1 C. 2 D. 3 E. 4 F. 5 G. 6 H. 7 I. 8 J. 9 14
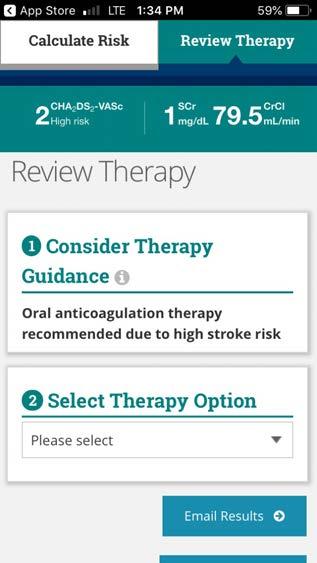
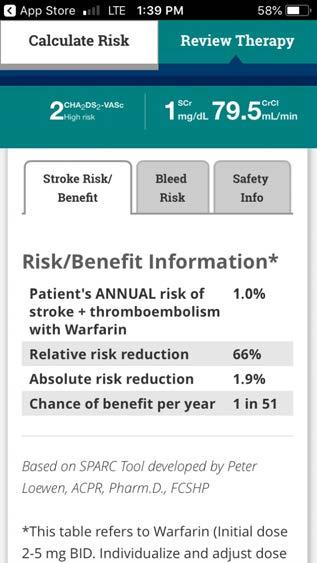
15 Case 2 (cont.) What is this patient s CHA2DS2-VASc score? A. 0 B. 1 C. 2 D. 3 E. 4 F. 5 G. 6 H. 7 I. 8 J. 9 Atrial Fibrillation Anticoagulation CHA 2 DS 2 VASc Risk Stratification Scheme (cont.) Score 0 1 > 2 Recommended therapy It is reasonable to omit antithrombotic therapy. **** No antithrombotic therapy, treatment with oral anticoagulant, or aspirin may be considered. Oral anticoagulants recommended. January et al. J Am Coll Cardiol. 2014;64(21):
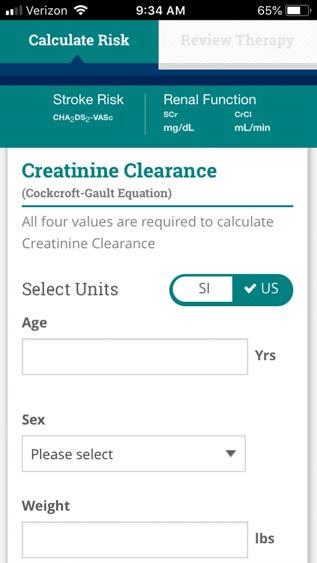
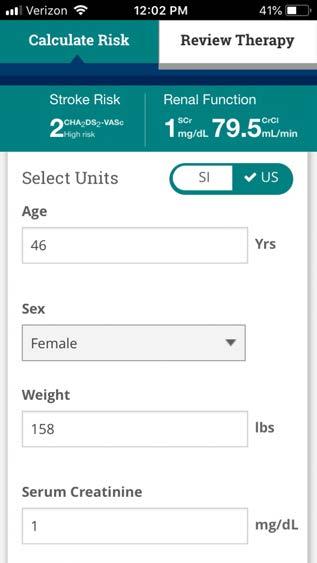
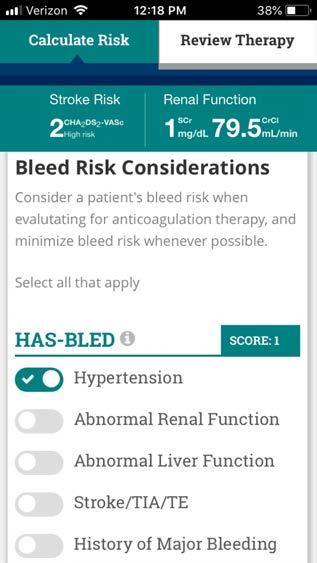
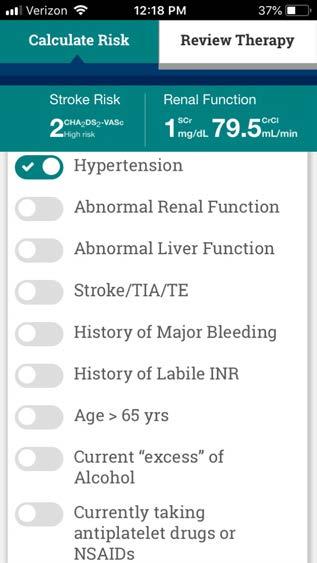
16 Atrial Fibrillation Anticoagulation CHA 2 DS 2 VASc Risk Stratification Scheme (cont.) Score 0 1 > 2 Recommended therapy It is reasonable to omit antithrombotic therapy. **** No antithrombotic therapy, treatment with oral anticoagulant, or aspirin may be considered. Oral anticoagulants recommended. January et al. J Am Coll Cardiol. 2014;64(21): ACC/AHA Guidelines Current ACC Guidelines (AF and many others): There s an app for that! Enter: ACC Guideline Clinical Apps 16
17 17
18 18
19 19


20 20
21 21
22 22
23 23
24 24
25 25
26 26
27 27
28 28

29 29
30 30
31 31
32 Case 2 (cont.) Which of the following is the most appropriate recommendation regarding anticoagulation prior to surgery? A. Discontinue warfarin now, as anticoagulation is not indicated in this patient. B. Discontinue warfarin four days prior to scheduled surgery. Check the INR daily. When the INR is < 2, begin enoxaparin 1 mg/kg SQ BID and continue it until the morning of surgery. C. Discontinue warfarin four days prior to scheduled surgery. Check the INR the morning of scheduled surgery. Proceed with surgery if the INR is < 2. D. Continue warfarin through the day before scheduled surgery. Withhold warfarin on the morning of surgery and initiate a continuous intravenous infusion of unfractionated heparin, which may then be discontinued on call to the operating room. Case 2 (cont.) Which of the following is the most appropriate recommendation regarding anticoagulation prior to surgery? A. Discontinue warfarin now, as anticoagulation is not indicated in this patient. B. Discontinue warfarin four days prior to scheduled surgery. Check the INR daily. When the INR is < 2, begin enoxaparin 1 mg/kg SQ BID and continue it until the morning of surgery. C. Discontinue warfarin four days prior to scheduled surgery. Check the INR the morning of scheduled surgery. Proceed with surgery if the INR is < 2. D. Continue warfarin through the day before scheduled surgery. Withhold warfarin on the morning of surgery and initiate a continuous intravenous infusion of unfractionated heparin, which may then be discontinued on call to the operating room. 32
33 Case 2 (cont.) Provided that the surgery was uneventful, which of the following is the most appropriate recommendation regarding anticoagulation postoperatively? A. Do not resume anticoagulation postoperatively, as it is not indicated in this patient. B. Resume warfarin as soon as the surgeon feels that the patient is at a low risk for bleeding. Discharge the patient when the INR is > 2. C. Begin enoxaparin 1 mg/kg SQ BID and resume warfarin 2 mg PO daily as soon as the surgeon feels that the patient is at a low risk for bleeding. Check the INR daily. Discontinue enoxaparin and discharge the patient when the INR is > 2. D. Begin enoxaparin 1 mg/kg SQ BID and resume warfarin 2 mg PO daily as soon as the surgeon feels that the patient is at a low risk for bleeding. Check the INR daily until the INR is > 2. Discontinue enoxaparin after 10 doses regardless of INR. Case 2 (cont.) Provided that the surgery was uneventful, which of the following is the most appropriate recommendation regarding anticoagulation postoperatively? A. Do not resume anticoagulation postoperatively, as it is not indicated in this patient. B. Resume warfarin as soon as the surgeon feels that the patient is at a low risk for bleeding. Discharge the patient when the INR is > 2. C. Begin enoxaparin 1 mg/kg SQ BID and resume warfarin 2 mg PO daily as soon as the surgeon feels that the patient is at a low risk for bleeding. Check the INR daily. Discontinue enoxaparin and discharge the patient when the INR is > 2. D. Begin enoxaparin 1 mg/kg SQ BID and resume warfarin 2 mg PO daily as soon as the surgeon feels that the patient is at a low risk for bleeding. Check the INR daily until the INR is > 2. Discontinue enoxaparin after 10 doses regardless of INR. 33
34 Case 3 62-year-old African American male without clinical CVD presents for routine medical evaluation. He is a nonsmoker and he is not diabetic. He has a history of asthma, for which he takes montelukast 10 mg PO daily. His total cholesterol is 192 mg/dl, his HDL-cholesterol is 38 mg/dl, triglycerides are 180 mg/dl, and his LDL-cholesterol is 118 mg/dl. His blood pressure is 134/76 mmhg, averaged from two separate occasions. Does his blood pressure require pharmacologic treatment at this time? 34

35 35
36 36

37 Yes! 37
38 Summary 1. Patients with undiagnosed cardiovascular disease are commonly encountered in the primary care setting. 2. Web-based resources are available that can be very useful to health care providers in managing patients with cardiovascular disease. 3. Never be too proud to ask for help. 38
39 39
Perioperative Management. Perioperative Management of Cardiovascular Medications
 of Cardiovascular Medications Carmine D Amico, D.O. Overview Learning objectives Beta-blockers Statins Alpha-2 agonists Calcium channel blockers ACE inhibitors and ARB s Anticoagulants Antiplatelet agents
of Cardiovascular Medications Carmine D Amico, D.O. Overview Learning objectives Beta-blockers Statins Alpha-2 agonists Calcium channel blockers ACE inhibitors and ARB s Anticoagulants Antiplatelet agents
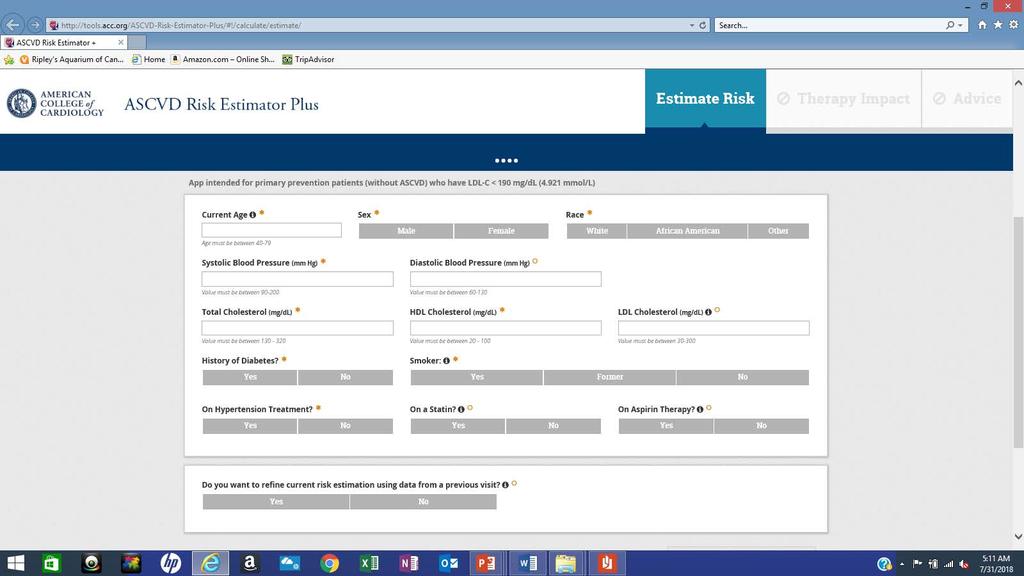
Medical Apps for Cardiology Uses. There s an App for That!
 Medical Apps for Cardiology Uses There s an App for That! Audience Participation Question #1 1. ASCVD Risk App What is the predicted 10 year CV event rate for a 57 y/o black male patient with treated
Medical Apps for Cardiology Uses There s an App for That! Audience Participation Question #1 1. ASCVD Risk App What is the predicted 10 year CV event rate for a 57 y/o black male patient with treated
AF in the ER: Common Scenarios CASE 1. Fast facts. Diagnosis. Management
 AF in the ER: Common Scenarios Atrial fibrillation is a common problem with a wide spectrum of presentations. Below are five common emergency room scenarios and the management strategies for each. Evan
AF in the ER: Common Scenarios Atrial fibrillation is a common problem with a wide spectrum of presentations. Below are five common emergency room scenarios and the management strategies for each. Evan
Topic: Chronic Heart Failure Cases for Monday s March 21th lecture.
 1 Phar6122: CV section Date: 3/10/05 Topic: Chronic Heart Failure Cases for Monday s March 21th lecture. Directions: This handout includes three chronic heart failure cases of increasing difficulty. In
1 Phar6122: CV section Date: 3/10/05 Topic: Chronic Heart Failure Cases for Monday s March 21th lecture. Directions: This handout includes three chronic heart failure cases of increasing difficulty. In
2017 Bryan Health Primary Care Conference. Dale Hansen MD Bryan Heart 5/20/17
 2017 Bryan Health Primary Care Conference Dale Hansen MD Bryan Heart 5/20/17 I have no financial disclosures or conflicts of interest Bridging Anticoagulation Primum Non Nocere 67 y.o. male with mechanical
2017 Bryan Health Primary Care Conference Dale Hansen MD Bryan Heart 5/20/17 I have no financial disclosures or conflicts of interest Bridging Anticoagulation Primum Non Nocere 67 y.o. male with mechanical
Mechanical versus bioprosthetic valve. Intern: Supervisor: VS
 Mechanical versus bioprosthetic valve Intern: Supervisor: VS Patient basic data ID: N102110716 Name: Age: 64 years old Sex: male Occupation: Admission date: 0960528 Chief complaint Exertional dyspnea for
Mechanical versus bioprosthetic valve Intern: Supervisor: VS Patient basic data ID: N102110716 Name: Age: 64 years old Sex: male Occupation: Admission date: 0960528 Chief complaint Exertional dyspnea for
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE General practice Indicators for the NICE menu
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE General practice Indicators for the NICE menu Indicator area: Pulse rhythm assessment for AF Indicator: NM146 Date: June 2017 Introduction There is evidence
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE General practice Indicators for the NICE menu Indicator area: Pulse rhythm assessment for AF Indicator: NM146 Date: June 2017 Introduction There is evidence
Transient Atrial Fibrillation and Risk of Stroke after Acute Myocardial Infarction
 Transient Atrial Fibrillation and Risk of Stroke after Acute Myocardial Infarction Doron Aronson MD, Gregory Telman MD, Fadel BahouthMD, Jonathan Lessick MD, DSc and Rema Bishara MD Department of Cardiology
Transient Atrial Fibrillation and Risk of Stroke after Acute Myocardial Infarction Doron Aronson MD, Gregory Telman MD, Fadel BahouthMD, Jonathan Lessick MD, DSc and Rema Bishara MD Department of Cardiology
Apixaban for Atrial Fibrillation in Patients with End-Stage Renal Disease on Dialysis
 Apixaban for Atrial Fibrillation in Patients with End-Stage Renal Disease on Dialysis Caitlin Reedholm, PharmD PGY1 Pharmacy Resident St. David s South Austin Medical Center November 2, 2018 Abbreviations
Apixaban for Atrial Fibrillation in Patients with End-Stage Renal Disease on Dialysis Caitlin Reedholm, PharmD PGY1 Pharmacy Resident St. David s South Austin Medical Center November 2, 2018 Abbreviations
MHD I Session VIII Renal Disease November 6, 2013 STUDENT COPY
 MHD I, Session VIII, Student Copy Page 1 MHD I Session VIII Renal Disease November 6, 2013 STUDENT COPY MHD I, Session VIII, Student Copy Page 2 Case #1 Chief Complaint: I have been feeling just lousy
MHD I, Session VIII, Student Copy Page 1 MHD I Session VIII Renal Disease November 6, 2013 STUDENT COPY MHD I, Session VIII, Student Copy Page 2 Case #1 Chief Complaint: I have been feeling just lousy
County General Hospital 546 That Street. Some Town, YY DISCHARGE SUMMARY
 County General Hospital 546 That Street. Some Town, YY 12347 111-222-9998 DISCHARGE SUMMARY PATIENT: Collette Rose UNIT#: 345678 ADMISSION DATE: June 5, 1995 ACCT#: 98734513 DISCHARGE DATE: June 13, 1995
County General Hospital 546 That Street. Some Town, YY 12347 111-222-9998 DISCHARGE SUMMARY PATIENT: Collette Rose UNIT#: 345678 ADMISSION DATE: June 5, 1995 ACCT#: 98734513 DISCHARGE DATE: June 13, 1995
2018 HPN Provider Summary Guide. Adult Cardiology Patients (18 Years and Older) Referral Guidelines
 Referral Guidelines") 12.2 CARDIOLOGY REFERRAL GUIDELINES Contracted Group: Southwest Medical Associates For Appointments: 888 S. Rancho Las Vegas, NV 89109 Phone: (702) 877-8654 Fax: (702) 242-7998 Adult Cardiology Patients
12.2 CARDIOLOGY REFERRAL GUIDELINES Contracted Group: Southwest Medical Associates For Appointments: 888 S. Rancho Las Vegas, NV 89109 Phone: (702) 877-8654 Fax: (702) 242-7998 Adult Cardiology Patients
Atrial Fibrillation. A guide for Southwark General Practice. Key Messages. Always work within your knowledge and competency
 Atrial Fibrillation A guide for Southwark General Practice Key Messages 1. Routinely offer pulse checks to patients at high risk of AF 2. Use the CHA 2 DS 2 VASc score to identify patients for anticoagulation
Atrial Fibrillation A guide for Southwark General Practice Key Messages 1. Routinely offer pulse checks to patients at high risk of AF 2. Use the CHA 2 DS 2 VASc score to identify patients for anticoagulation
NUOVI ANTICOAGULANTI NELL ANZIANO: indicazioni e controindicazioni. Mario Cavazza Medicina d Urgenza Pronto Soccorso AOU di Bologna
 NUOVI ANTICOAGULANTI NELL ANZIANO: indicazioni e controindicazioni Mario Cavazza Medicina d Urgenza Pronto Soccorso AOU di Bologna Two major concerns Atrial Fibrillation: Epidemiology The No. 1 preventable
NUOVI ANTICOAGULANTI NELL ANZIANO: indicazioni e controindicazioni Mario Cavazza Medicina d Urgenza Pronto Soccorso AOU di Bologna Two major concerns Atrial Fibrillation: Epidemiology The No. 1 preventable
Atrial Fibrillation and the NOAC s. John Raymond MS, PA-C, MHP February 10, 2018
 Atrial Fibrillation and the NOAC s John Raymond MS, PA-C, MHP February 10, 2018 Pathogenesis EPIDEMIOLOGY Arrhythmia-related hospitalisations in the US Ventricular fibrillation 2% Atrial fibrillation 34%
Atrial Fibrillation and the NOAC s John Raymond MS, PA-C, MHP February 10, 2018 Pathogenesis EPIDEMIOLOGY Arrhythmia-related hospitalisations in the US Ventricular fibrillation 2% Atrial fibrillation 34%
Cost and Prevalence of A fib. Atrial Fibrillation: Guideline Directed Treatment. Prevalence of A Fib. Risk Factors for A Fib. Risk Factors for A Fib
 Atrial Fibrillation: Guideline Directed Treatment Melissa Wendell, FNP-C, MSN Heart Failure - Lead Nurse Practitioner, Aspirus Wausau Hospital and Aspirus Cardiology Cost and Prevalence of A fib 33.5 million
Atrial Fibrillation: Guideline Directed Treatment Melissa Wendell, FNP-C, MSN Heart Failure - Lead Nurse Practitioner, Aspirus Wausau Hospital and Aspirus Cardiology Cost and Prevalence of A fib 33.5 million
Management of ATRIAL FIBRILLATION. in general practice. 22 BPJ Issue 39
 Management of ATRIAL FIBRILLATION in general practice 22 BPJ Issue 39 What is atrial fibrillation? Atrial fibrillation (AF) is the most common cardiac arrhythmia encountered in primary care. It is often
Management of ATRIAL FIBRILLATION in general practice 22 BPJ Issue 39 What is atrial fibrillation? Atrial fibrillation (AF) is the most common cardiac arrhythmia encountered in primary care. It is often
Updates in Stroke Management. Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy
 Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
Table 1 Baseline characteristics of 60 hemodialysis patients with atrial fibrillation and warfarin use
 Table 1 Baseline characteristics of 60 hemodialysis patients with atrial fibrillation and warfarin use Baseline characteristics Users (n = 28) Non-users (n = 32) P value Age (years) 67.8 (9.4) 68.4 (8.5)
Table 1 Baseline characteristics of 60 hemodialysis patients with atrial fibrillation and warfarin use Baseline characteristics Users (n = 28) Non-users (n = 32) P value Age (years) 67.8 (9.4) 68.4 (8.5)
AF Diagnosis. Incorporated into over 75 health checks and Public Health Checks
 AF Diagnosis Incpated into over 75 health checks and Public Health Checks Pulse Feel the pulse in all >65yrs If irregular do a 12 Lead ECG with Rhythm strip Check Thyroid and FBC and heart rate Refer to
AF Diagnosis Incpated into over 75 health checks and Public Health Checks Pulse Feel the pulse in all >65yrs If irregular do a 12 Lead ECG with Rhythm strip Check Thyroid and FBC and heart rate Refer to
CASE IN... Anticoagulation: When to Start,When to Stop. The management of patients who require an. Meet Tracey. Anticoagulation
 Anticoagulation: When to Start,When to Stop Ebtisam Bakhsh, MD; and James D. Douketis, MD, FRCPC Presented at McMaster University s Thrombosis and Hematology Update, October 2006. CASE IN... Anticoagulation
Anticoagulation: When to Start,When to Stop Ebtisam Bakhsh, MD; and James D. Douketis, MD, FRCPC Presented at McMaster University s Thrombosis and Hematology Update, October 2006. CASE IN... Anticoagulation
Acute Stroke with Alteplase Administration Order Set
 Review Due Date: 2017 October PATIENT CARE DERS Weight: Adverse Reactions or Intolerances Drug No Yes (list) Food No Yes (list) _ Latex No Yes Admission Admit to Neurology service: Dr. Critical Care Diagnosis:
Review Due Date: 2017 October PATIENT CARE DERS Weight: Adverse Reactions or Intolerances Drug No Yes (list) Food No Yes (list) _ Latex No Yes Admission Admit to Neurology service: Dr. Critical Care Diagnosis:
A 45 year old African American man presents to the IMC with a chief complaint of my
 AN EVIDENCE BASED APPROACH TO HYPERTENSION AND HYPERLIPIDENIA: A CASE STUDY A 45 year old African American man presents to the IMC with a chief complaint of my pressure is high. Apparently he recently
AN EVIDENCE BASED APPROACH TO HYPERTENSION AND HYPERLIPIDENIA: A CASE STUDY A 45 year old African American man presents to the IMC with a chief complaint of my pressure is high. Apparently he recently
Chemistry Reference Ranges and Critical Values
 Alanine Aminotransferase (ALT, SGPT) 3-9 years 9-18 years 1-9 years 9-18 years 10-25 U/L 10-35 U/L 10-30 U/L 10-25 U/L 10-30 U/L 10-35 U/L 10-25 U/L 10-35 U/L 10-25 U/L 10-20 U/L 10-35 U/L Albumin 0-6
Alanine Aminotransferase (ALT, SGPT) 3-9 years 9-18 years 1-9 years 9-18 years 10-25 U/L 10-35 U/L 10-30 U/L 10-25 U/L 10-30 U/L 10-35 U/L 10-25 U/L 10-35 U/L 10-25 U/L 10-20 U/L 10-35 U/L Albumin 0-6
Chemistry Reference Ranges and Critical Values
 Alanine Aminotransferase (ALT, SGPT) 3-9 years 9-18 years 1-9 years 9-18 years 10-30 U/L 10-30 U/L 10-20 U/L Albumin 0-6 days 6 days - 37 months 37 months - 7 years 7-20 years 2.6-3.6 g/dl 3.4-4.2 g/dl
Alanine Aminotransferase (ALT, SGPT) 3-9 years 9-18 years 1-9 years 9-18 years 10-30 U/L 10-30 U/L 10-20 U/L Albumin 0-6 days 6 days - 37 months 37 months - 7 years 7-20 years 2.6-3.6 g/dl 3.4-4.2 g/dl
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Quality ID #326 (NQF 1525): Atrial Fibrillation and Atrial Flutter: Chronic Anticoagulation Therapy National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS F INDIVIDUAL MEASURES: REGISTRY
Quality ID #326 (NQF 1525): Atrial Fibrillation and Atrial Flutter: Chronic Anticoagulation Therapy National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS F INDIVIDUAL MEASURES: REGISTRY
County General Hospital 546 That Street Some Town, YY DISCHARGE SUMMARY
 County General Hospital 546 That Street Some Town, YY 12345 111-222-9998 DISCHARGE SUMMARY PATIENT: Michael F. Byrnes UNIT#: 345678 ADMISSION DATE: June 5, 2006 ACCT#: 98734512 DISCHARGE DATE: June 6,
County General Hospital 546 That Street Some Town, YY 12345 111-222-9998 DISCHARGE SUMMARY PATIENT: Michael F. Byrnes UNIT#: 345678 ADMISSION DATE: June 5, 2006 ACCT#: 98734512 DISCHARGE DATE: June 6,
Documentation Dissection
 History of Present Illness: Documentation Dissection The patient is a 50-year-old male c/o symptoms for past 4 months 1, severe 2 bloating and stomach cramps, some nausea, vomiting, diarrhea. In last 3
History of Present Illness: Documentation Dissection The patient is a 50-year-old male c/o symptoms for past 4 months 1, severe 2 bloating and stomach cramps, some nausea, vomiting, diarrhea. In last 3
Intrinsic + Common = aptt. Extrinsic + Common = PT. Common Pathway
 Anticoagulant Cases 12 11 Intrinsic + Common = aptt 9 8 10 7 4 Extrinsic + Common = PT 5 2 Common Pathway 1 Xa Inhibitors rivaroxaban (Xarelto) apixaban (Eliquis) edoxaban (Savaysa) What is true regarding
Anticoagulant Cases 12 11 Intrinsic + Common = aptt 9 8 10 7 4 Extrinsic + Common = PT 5 2 Common Pathway 1 Xa Inhibitors rivaroxaban (Xarelto) apixaban (Eliquis) edoxaban (Savaysa) What is true regarding
Controversies in Atrial Fibrillation and HF
 Controversies in Atrial Fibrillation and HF Dr.Yahya Al Hebaishi Cardiac electrophysiology division, PSCC, Riyadh Atrial Fibrillation: Rate or Rhythm? HF and AF: the twin epidemic of cardiovascular disease.
Controversies in Atrial Fibrillation and HF Dr.Yahya Al Hebaishi Cardiac electrophysiology division, PSCC, Riyadh Atrial Fibrillation: Rate or Rhythm? HF and AF: the twin epidemic of cardiovascular disease.
Topic: Chronic Heart Failure Cases for Monday s March 21th lecture.
 1 Phar6122: CV section Date: 3/21/05 Topic: Chronic Heart Failure Cases for Monday s March 21th lecture. Directions: This handout includes three chronic heart failure cases of increasing difficulty. In
1 Phar6122: CV section Date: 3/21/05 Topic: Chronic Heart Failure Cases for Monday s March 21th lecture. Directions: This handout includes three chronic heart failure cases of increasing difficulty. In
MODULE 1: Stroke Prevention in Atrial Fibrillation Benjamin Bell, MD, FRCPC
 MODULE 1: Stroke Prevention in Atrial Fibrillation Benjamin Bell, MD, FRCPC Specialty: General Internal Medicine Lecturer, Department of Medicine University of Toronto Staff Physician, General Internal
MODULE 1: Stroke Prevention in Atrial Fibrillation Benjamin Bell, MD, FRCPC Specialty: General Internal Medicine Lecturer, Department of Medicine University of Toronto Staff Physician, General Internal
Clinical Practice Committee Anticoagulation Bridging Document
 Original: 10/23/06 Last Updated: 10/30/07 Clinical Practice Committee Do patients on long term oral anticoagulant therapy who require short term interruption of warfarin for an elective invasive procedure
Original: 10/23/06 Last Updated: 10/30/07 Clinical Practice Committee Do patients on long term oral anticoagulant therapy who require short term interruption of warfarin for an elective invasive procedure
Mohammad Zubaid, MB, ChB, FRCPC, FACC
 Management and one year outcome of atrial fibrillation in Middle Eastern cohort enrolled in the observational Gulf Survey of Atrial Fibrillation Events (Gulf SAFE) Mohammad Zubaid, MB, ChB, FRCPC, FACC
Management and one year outcome of atrial fibrillation in Middle Eastern cohort enrolled in the observational Gulf Survey of Atrial Fibrillation Events (Gulf SAFE) Mohammad Zubaid, MB, ChB, FRCPC, FACC
Følgende dias er fremlagt ved DCS / DTS Fællesmøde 13. januar 2011 og alle rettigheder tilhører foredragsholderen. Gengivelse må kun foretages ved
 . Følgende dias er fremlagt ved DCS / DTS Fællesmøde 13. januar 2011 og alle rettigheder tilhører foredragsholderen. Gengivelse må kun foretages ved tilladelse Antithrombotic therapy in Atrial Fibrillation
. Følgende dias er fremlagt ved DCS / DTS Fællesmøde 13. januar 2011 og alle rettigheder tilhører foredragsholderen. Gengivelse må kun foretages ved tilladelse Antithrombotic therapy in Atrial Fibrillation
Objectives. Falling Down on Warfarin Therapy. CHADS 2 Score. CHADS 2 & CHA 2 DS 2 -VASc Score. HAS-BLED Score 04/08/2014. Real World Application
 Falling Down on Warfarin Therapy David Andrew Jacob, PharmD Pharmacy Resident 2013-2014 Dayton VA Medical Center Dayton, Ohio Objectives Describe CHADS 2 score and the decision to anticoagulate patients
Falling Down on Warfarin Therapy David Andrew Jacob, PharmD Pharmacy Resident 2013-2014 Dayton VA Medical Center Dayton, Ohio Objectives Describe CHADS 2 score and the decision to anticoagulate patients
Management of Patients with Atrial Fibrillation Undergoing Coronary Artery Stenting 경북대의전원내과조용근
 Management of Patients with Atrial Fibrillation Undergoing Coronary Artery Stenting 경북대의전원내과조용근 Case (2011, 5) 74-years old gentleman Exertional chest pain Warfarin with good INR control Ex-smoker, social(?)
Management of Patients with Atrial Fibrillation Undergoing Coronary Artery Stenting 경북대의전원내과조용근 Case (2011, 5) 74-years old gentleman Exertional chest pain Warfarin with good INR control Ex-smoker, social(?)
What s new with DOACs? Defining place in therapy for edoxaban &
 What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
2019 COLLECTION TYPE: MIPS CLINICAL QUALITY MEASURES (CQMS) MEASURE TYPE: Process
 MEASURE TYPE: Process") Quality ID #326 (NQF 1525): Atrial Fibrillation and Atrial Flutter: Chronic Anticoagulation Therapy National Quality Strategy Domain: Effective Clinical Care Meaningful Measure Area: Management of Chronic
Quality ID #326 (NQF 1525): Atrial Fibrillation and Atrial Flutter: Chronic Anticoagulation Therapy National Quality Strategy Domain: Effective Clinical Care Meaningful Measure Area: Management of Chronic
Long-Term Complications of Diabetes Mellitus Macrovascular Complication
 Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
1 Week Followup - Intermacs
 version date: 9/27/2017 1 Week Followup - Intermacs Followup Status (1 Week Followup (+/- 3 days)) Select one of the following Inpatient Outpatient Other Facility Unable to obtain follow-up information
version date: 9/27/2017 1 Week Followup - Intermacs Followup Status (1 Week Followup (+/- 3 days)) Select one of the following Inpatient Outpatient Other Facility Unable to obtain follow-up information
A walk through a STEMI
 A walk through a STEMI M.M. s Story Kim Robison Ashley Corcoran Situation M.M. is an 82 year old male brought in by private vehicle on 10/22/17 to the Emergency Department Pt. c/o left arm numbness, pain
A walk through a STEMI M.M. s Story Kim Robison Ashley Corcoran Situation M.M. is an 82 year old male brought in by private vehicle on 10/22/17 to the Emergency Department Pt. c/o left arm numbness, pain
Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute
 Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute Disclosures Research Support/P.I. Employee Leo Pharma
Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute Disclosures Research Support/P.I. Employee Leo Pharma
10 Essential Blood Tests PART 1
 Presents 10 Essential Blood Tests PART 1 The Blood Chemistry Webinars With DR. DICKEN WEATHERBY Creator of the Blood Chemistry Software Essential Blood Test #1: Basic Chem Screen and CBC http://bloodchemsoftware.com
Presents 10 Essential Blood Tests PART 1 The Blood Chemistry Webinars With DR. DICKEN WEATHERBY Creator of the Blood Chemistry Software Essential Blood Test #1: Basic Chem Screen and CBC http://bloodchemsoftware.com
Atrial Fibrillaiton and Heart Failure: Anticoagulation therapy in all cases?
 Atrial Fibrillaiton and Heart Failure: Anticoagulation therapy in all cases? Nicolas Lellouche Fédération de Cardiologie Hôpital Henri Mondor Créteil Disclosure Statement of Financial Interest I currently
Atrial Fibrillaiton and Heart Failure: Anticoagulation therapy in all cases? Nicolas Lellouche Fédération de Cardiologie Hôpital Henri Mondor Créteil Disclosure Statement of Financial Interest I currently
SMALL GROUP DISCUSSION
 MHD II, Session 1 Student Copy Page 1 SMALL GROUP DISCUSSION MHD II Session 1 Gastroinestinal Monday, January 9, 2017 STUDENT COPY MHD II, Session 1 Student Copy Page 2 CASE 1 CHIEF CONCERN: "I'm passing
MHD II, Session 1 Student Copy Page 1 SMALL GROUP DISCUSSION MHD II Session 1 Gastroinestinal Monday, January 9, 2017 STUDENT COPY MHD II, Session 1 Student Copy Page 2 CASE 1 CHIEF CONCERN: "I'm passing
Anti-thromboticthrombotic drugs
 Atrial Fibrillation 2011: Anticoagulation strategies and clinical outcomes Panos E. Vardas President Elect of the ESC, Prof. of Cardiology, University Hospital of Crete Clinical outcomes affected by AF
Atrial Fibrillation 2011: Anticoagulation strategies and clinical outcomes Panos E. Vardas President Elect of the ESC, Prof. of Cardiology, University Hospital of Crete Clinical outcomes affected by AF
Heart Failure with Johnny Crash: LEFT VENTRICULAR EJECTION FRACTION (LVEF) SYMPTOMATOLOGY: Assess VENTRICULAR DYSFUNCTION HEART FAILURE:
 SYMPTOMATOLOGY: Assess VENTRICULAR DYSFUNCTION HEART FAILURE:") Heart Failure with Johnny Crash: Joan E. King, PhD, ACNP-BC, ANP-BC Melissa Smith, DNP, ANP-BC Vanderbilt University School of Nursing HEART FAILURE: Heart Failure (HF): a complex clinical syndrome resulting
Heart Failure with Johnny Crash: Joan E. King, PhD, ACNP-BC, ANP-BC Melissa Smith, DNP, ANP-BC Vanderbilt University School of Nursing HEART FAILURE: Heart Failure (HF): a complex clinical syndrome resulting
Chapter 1. Perioperative Evaluation and Management of Surgical Patients. Oral Exam Questions
 Chapter 1 Perioperative Evaluation and Management of Surgical Patients Oral Exam Questions Case 1 A 62-year-old man with a PMH significant for hypertension, and a 40-pack-year history of smoking is found
Chapter 1 Perioperative Evaluation and Management of Surgical Patients Oral Exam Questions Case 1 A 62-year-old man with a PMH significant for hypertension, and a 40-pack-year history of smoking is found
Slide 1: Perioperative Management of Anticoagulation
 Perioperative Management of Anticoagulation by Steven L. Cohn, MD, FACP Director, Medical Consultation Service, Kings County Hospital Center, Clinical Professor of Medicine, SUNY Downstate, Brooklyn, NY
Perioperative Management of Anticoagulation by Steven L. Cohn, MD, FACP Director, Medical Consultation Service, Kings County Hospital Center, Clinical Professor of Medicine, SUNY Downstate, Brooklyn, NY
POTENTIAL LINKAGES BETWEEN THE QUALITY AND OUTCOMES FRAMEWORK (QOF) AND THE NHS HEALTH CHECK
 AND THE NHS HEALTH CHECK") POTENTIAL LINKAGES BETWEEN THE QUALITY AND OUTCOMES FRAMEWORK (QOF) AND THE NHS HEALTH CHECK Author: CHARLOTTE SIMPSON, SPECIALTY REGISTAR PUBLIC HEALTH (ST3), CHESHIRE EAST COUNCIL/MERSEY DEANERY SUMMARY
POTENTIAL LINKAGES BETWEEN THE QUALITY AND OUTCOMES FRAMEWORK (QOF) AND THE NHS HEALTH CHECK Author: CHARLOTTE SIMPSON, SPECIALTY REGISTAR PUBLIC HEALTH (ST3), CHESHIRE EAST COUNCIL/MERSEY DEANERY SUMMARY
Perioperative Management of Anticoagulation
 Perioperative Management of Anticoagulation Presented By: Nibal R. Chamoun, PharmD, BCPS Clinical Assistant Professor, Clinical Coordinator Lebanese American University, School of Pharmacy Presented at:
Perioperative Management of Anticoagulation Presented By: Nibal R. Chamoun, PharmD, BCPS Clinical Assistant Professor, Clinical Coordinator Lebanese American University, School of Pharmacy Presented at:
Use of Anticoagulants in Geriatrics: Current Evidence and Special Considerations
 Use of Anticoagulants in Geriatrics: Current Evidence and Special Considerations Aryn You, PharmD Assistant Professor, Pharmacy Practice The Daniel K. Inouye College of Pharmacy Aida Wen, MD Associate
Use of Anticoagulants in Geriatrics: Current Evidence and Special Considerations Aryn You, PharmD Assistant Professor, Pharmacy Practice The Daniel K. Inouye College of Pharmacy Aida Wen, MD Associate
The contractor establishes and maintains a register of patients with AF
 Atrial Fibrillation The contractor establishes and maintains a register of patients with AF G5731 Those patients with AF in whom there is a record of CHADS2 score of 1, the % of patients who are currently
Atrial Fibrillation The contractor establishes and maintains a register of patients with AF G5731 Those patients with AF in whom there is a record of CHADS2 score of 1, the % of patients who are currently
Current Guideline for AF Treatment. Young Keun On, MD, PhD, FHRS Samsung Medical Center Sungkyunkwan University School of Medicine
 Current Guideline for AF Treatment Young Keun On, MD, PhD, FHRS Samsung Medical Center Sungkyunkwan University School of Medicine Case 1 59 year-old lady Sudden palpitation and breathlessness for 12 hours
Current Guideline for AF Treatment Young Keun On, MD, PhD, FHRS Samsung Medical Center Sungkyunkwan University School of Medicine Case 1 59 year-old lady Sudden palpitation and breathlessness for 12 hours
SUMMARY OF CHANGES TO QOF 2017/18 - ENGLAND CLINICAL
 SUMMARY OF CHANGES TO QOF 2017/18 - ENGLAND KEY No change Retired/replaced Wording and/or timeframe change Point or threshold change Indicator ID change 1/17 QOF ID 17/18 QOF ID NICE ID Indicator wording
SUMMARY OF CHANGES TO QOF 2017/18 - ENGLAND KEY No change Retired/replaced Wording and/or timeframe change Point or threshold change Indicator ID change 1/17 QOF ID 17/18 QOF ID NICE ID Indicator wording
Undiagnosed Non-Valvular Atrial Fibrillation and Stroke Risk: A Call to Action. PCNA Annual Symposium, April 2018
 Undiagnosed Non-Valvular Atrial Fibrillation and Stroke Risk: A Call to Action PCNA Annual Symposium, April 2018 Presenter Moderator and Speaker: Kathy Berra MSN, ANP, FAHA, FPCNA, FAAN Stanford Prevention
Undiagnosed Non-Valvular Atrial Fibrillation and Stroke Risk: A Call to Action PCNA Annual Symposium, April 2018 Presenter Moderator and Speaker: Kathy Berra MSN, ANP, FAHA, FPCNA, FAAN Stanford Prevention
Anticoagulation Overview Jed Delmore, MD, FACS, FACOG Professor Obstetrics and Gynecology University of Kansas School of Medicine, Wichita
 Anticoagulation Overview 2018 Jed Delmore, MD, FACS, FACOG Professor Obstetrics and Gynecology University of Kansas School of Medicine, Wichita The ideal lecture is like a miniskirt. Short enough to get
Anticoagulation Overview 2018 Jed Delmore, MD, FACS, FACOG Professor Obstetrics and Gynecology University of Kansas School of Medicine, Wichita The ideal lecture is like a miniskirt. Short enough to get
17/18 Threshold 18/19 Points 18/19. Points NO CHANGE NO CHANGE NO CHANGE
 SUMMARY OF CHANGES TO QOF 2018/19 - ENGLAND 18-19 QOF005 KEY No change Retired/replaced Wording and/or timeframe change Point or threshold change Indicator ID change 17/18 QOF ID 18/19 QOF ID NICE ID Indicator
SUMMARY OF CHANGES TO QOF 2018/19 - ENGLAND 18-19 QOF005 KEY No change Retired/replaced Wording and/or timeframe change Point or threshold change Indicator ID change 17/18 QOF ID 18/19 QOF ID NICE ID Indicator
Show Me the Outcomes!
 Show Me the Outcomes! Real-World Safety Data on Oral Anticoagulants in Nonvalvular Atrial Fibrillation Gabby Anderson, PharmD PGY1 Pharmacy Resident anderson.gabrielle@mayo.edu Pharmacy Grand Rounds October
Show Me the Outcomes! Real-World Safety Data on Oral Anticoagulants in Nonvalvular Atrial Fibrillation Gabby Anderson, PharmD PGY1 Pharmacy Resident anderson.gabrielle@mayo.edu Pharmacy Grand Rounds October
Incorporating KT Concepts within Clinical Trials
 Incorporating KT Concepts within Clinical Trials The RELY-ABLE Trial as an Example Stuart Connolly & Robby Nieuwlaat Background - Dabigatran RE-LY Atrial fibrillation (AF) patients at high risk for stroke
Incorporating KT Concepts within Clinical Trials The RELY-ABLE Trial as an Example Stuart Connolly & Robby Nieuwlaat Background - Dabigatran RE-LY Atrial fibrillation (AF) patients at high risk for stroke
NeuroPI Case Study: Anticoagulant Therapy
 Case: An 82-year-old man presents to the hospital following a transient episode of left visual field changes. His symptoms lasted 20 minutes and resolved spontaneously. He has a normal neurological examination
Case: An 82-year-old man presents to the hospital following a transient episode of left visual field changes. His symptoms lasted 20 minutes and resolved spontaneously. He has a normal neurological examination
Dr Micheal Looney Consultant Anaesthetist Connolly Hospital Blanchardstown. To Delay or Not to Delay Hip Fracture Surgery
 Dr Micheal Looney Consultant Anaesthetist Connolly Hospital Blanchardstown To Delay or Not to Delay Hip Fracture Surgery "You may delay, but time will not, and lost time is never found again." Benjamin
Dr Micheal Looney Consultant Anaesthetist Connolly Hospital Blanchardstown To Delay or Not to Delay Hip Fracture Surgery "You may delay, but time will not, and lost time is never found again." Benjamin
Evaluate Risk of Stroke & Bleeding in AF Patients
 XV World Congress of Arrhythmias, Beijing, China - 17-20 September, 2015 Evaluate Risk of Stroke & Bleeding in AF Patients Antonio Raviele, MD, FESC, FHRS President ALFA Alliance to Fight Atrial fibrillation
XV World Congress of Arrhythmias, Beijing, China - 17-20 September, 2015 Evaluate Risk of Stroke & Bleeding in AF Patients Antonio Raviele, MD, FESC, FHRS President ALFA Alliance to Fight Atrial fibrillation
Atrial Fibrillation Implementation challenges. Lesley Edgar Ross Maconachie
 Atrial Fibrillation Implementation challenges Lesley Edgar Ross Maconachie Atrial Fibrillation Most common heart rhythm disturbance Rapid and irregular electrical signals Reduced efficiency of blood flow
Atrial Fibrillation Implementation challenges Lesley Edgar Ross Maconachie Atrial Fibrillation Most common heart rhythm disturbance Rapid and irregular electrical signals Reduced efficiency of blood flow
1 Week Followup 5/27/2014. Nursing Home/Assisted Care Hospice Another hospital Rehabilitation Facility Unknown
 1 Week Followup t Started Please answer all questions considering all time since the previous visit and current follow-up date. Print this Form Followup Status t Started Select one of the following Inpatient
1 Week Followup t Started Please answer all questions considering all time since the previous visit and current follow-up date. Print this Form Followup Status t Started Select one of the following Inpatient
Atrial Fibrillation Topics for Today. Clinical Controversies Management of Atrial Fibrillation. Atrial Fibrillation in the ER Topics for Today
 Clinical Controversies Management of Atrial Fibrillation Yerem Yeghiazarians, M.D. Associate Professor of Medicine Leone-Perkins Family Endowed Chair in Cardiology Atrial Fibrillation Topics for Today
Clinical Controversies Management of Atrial Fibrillation Yerem Yeghiazarians, M.D. Associate Professor of Medicine Leone-Perkins Family Endowed Chair in Cardiology Atrial Fibrillation Topics for Today
Subject ID: I N D # # U A * Consent Date: Day Month Year
 IND Study # Eligibility Checklist Pg 1 of 15 Instructions: Check the appropriate box for each Inclusion and Exclusion Criterion below. Each criterion must be marked and all protocol criteria have to be
IND Study # Eligibility Checklist Pg 1 of 15 Instructions: Check the appropriate box for each Inclusion and Exclusion Criterion below. Each criterion must be marked and all protocol criteria have to be
Oral Anticoagulation Drug Class Prior Authorization Protocol
 Oral Anticoagulation Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review
Oral Anticoagulation Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review
Detection Of Heart. By Dr Gary Mo
 Detection Of Heart Disease By Dr Gary Mo Types Of Heart Disease A. Coronary Heart Disease B. Valvular Heart Disease C. Cardiac Arrhythmia ( Rhythm disturbance ) D. Heart Blocks ( Conduction Abnormalities
Detection Of Heart Disease By Dr Gary Mo Types Of Heart Disease A. Coronary Heart Disease B. Valvular Heart Disease C. Cardiac Arrhythmia ( Rhythm disturbance ) D. Heart Blocks ( Conduction Abnormalities
Supplementary Online Content
 Supplementary Online Content Inohara T, Xian Y, Liang L, et al. Association of intracerebral hemorrhage among patients taking non vitamin K antagonist vs vitamin K antagonist oral anticoagulants with in-hospital
Supplementary Online Content Inohara T, Xian Y, Liang L, et al. Association of intracerebral hemorrhage among patients taking non vitamin K antagonist vs vitamin K antagonist oral anticoagulants with in-hospital
Incorporated Dosing Guidelines: Intravenous Heparin Therapy Initial Dose
 Intravenous Heparin Therapy Initial Dose (Max Dose) IV Infusion Rate IV Infusion Rate (Max Dose) Lab Tests High Dose 80 units/kg 8,000 units 18 units/kg/hr 1,800 units/hr Intermediate Dose 5,000 units
Intravenous Heparin Therapy Initial Dose (Max Dose) IV Infusion Rate IV Infusion Rate (Max Dose) Lab Tests High Dose 80 units/kg 8,000 units 18 units/kg/hr 1,800 units/hr Intermediate Dose 5,000 units
To Bridge or Not to Bridge? Preop Evaluation of the Patient on Coumadin
 To Bridge or Not to Bridge? Preop Evaluation of the Patient on Coumadin Omprakash Pansara, MD Brian Kline, MD St. Joseph s Health Family Medicine Residency Program, Syracuse, NY Case 75yr old male, who
To Bridge or Not to Bridge? Preop Evaluation of the Patient on Coumadin Omprakash Pansara, MD Brian Kline, MD St. Joseph s Health Family Medicine Residency Program, Syracuse, NY Case 75yr old male, who
Stratificazione del rischio, corretto bilancio tra ischemia e bleeding: il beneficio clinico netto
 Fibrillazione atriale: rischio tromboembolico, Venezia - 27/28 Novembre 2015 Stratificazione del rischio, corretto bilancio tra ischemia e bleeding: il beneficio clinico netto Antonio Raviele, MD, FESC,
Fibrillazione atriale: rischio tromboembolico, Venezia - 27/28 Novembre 2015 Stratificazione del rischio, corretto bilancio tra ischemia e bleeding: il beneficio clinico netto Antonio Raviele, MD, FESC,
Professor DA Fitzmaurice Primary Care Clinical Sciences University of Birmingham
 New Guidelines for SPAF Professor DA Fitzmaurice Primary Care Clinical Sciences University of Birmingham Stroke prevention and atrial fibrillation Epidemiology of atrial fibrillation How common is it?
New Guidelines for SPAF Professor DA Fitzmaurice Primary Care Clinical Sciences University of Birmingham Stroke prevention and atrial fibrillation Epidemiology of atrial fibrillation How common is it?
ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION
 ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION Frederick Schaller, DO, MACOI,FACP Adjunct Clinical Professor Touro University Nevada DISCLOSURES I have no financial relationships
ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION Frederick Schaller, DO, MACOI,FACP Adjunct Clinical Professor Touro University Nevada DISCLOSURES I have no financial relationships
BC Cancer Protocol for Treatment of Platinum Resistant Epithelial Ovarian Cancer with Bevacizumab and PACLitaxel
 BC Cancer Protocol for Treatment of Platinum Resistant Epithelial Ovarian Cancer with Bevacizumab and PACLitaxel Protocol Code Tumour Group Contact Physician UGOOVBEVP Gynecologic Oncology Dr. Anna Tinker
BC Cancer Protocol for Treatment of Platinum Resistant Epithelial Ovarian Cancer with Bevacizumab and PACLitaxel Protocol Code Tumour Group Contact Physician UGOOVBEVP Gynecologic Oncology Dr. Anna Tinker
14/15 Threshold 15/16 Points 15/16. Points. Retired Replaced by NM82/AF007. Replacement NO CHANGE
 SUMMARY OF CHANGES TO QOF 2015/1 - ENGLAND KEY No change Retired/replaced Wording and/or change Point or threshold change Indicator ID change 14/15 QOF ID 15/1 QOF ID NICE ID Indicator wording Changes
SUMMARY OF CHANGES TO QOF 2015/1 - ENGLAND KEY No change Retired/replaced Wording and/or change Point or threshold change Indicator ID change 14/15 QOF ID 15/1 QOF ID NICE ID Indicator wording Changes
DUKECATHR Dataset Dictionary
 DUKECATHR Dataset Dictionary Version of DUKECATH dataset for educational use that has been modified to be unsuitable for clinical research or publication (Created Date and Time: 28OCT16 14:35) Table of
DUKECATHR Dataset Dictionary Version of DUKECATH dataset for educational use that has been modified to be unsuitable for clinical research or publication (Created Date and Time: 28OCT16 14:35) Table of
Individual Therapeutic Selection Of Anti-coagulants And Periprocedural. Miguel Valderrábano, MD
 Individual Therapeutic Selection Of Anti-coagulants And Periprocedural Management Miguel Valderrábano, MD Outline Does the patient need anticoagulation? Review of clinical evidence for each anticoagulant
Individual Therapeutic Selection Of Anti-coagulants And Periprocedural Management Miguel Valderrábano, MD Outline Does the patient need anticoagulation? Review of clinical evidence for each anticoagulant
The focus of this week s lab will be pathology of the cardiovascular system.
 LAB 3: THE MUSCLE AND CARDIOVASCULAR SYSTEM The focus of this week s lab will be pathology of the cardiovascular system. The cases we will cover are: A. Atherosclerosis Refer to virtual slide p_8, should
LAB 3: THE MUSCLE AND CARDIOVASCULAR SYSTEM The focus of this week s lab will be pathology of the cardiovascular system. The cases we will cover are: A. Atherosclerosis Refer to virtual slide p_8, should
Periprocedural Anticoagulation Adult Inpatient and Ambulatory Clinical Practice Guideline
 Periprocedural Anticoagulation Adult Inpatient and Ambulatory Clinical Practice Guideline A. Scope (disease/condition, treatment, clinical specialty) 1. Adult patients undergoing a procedure or surgery
Periprocedural Anticoagulation Adult Inpatient and Ambulatory Clinical Practice Guideline A. Scope (disease/condition, treatment, clinical specialty) 1. Adult patients undergoing a procedure or surgery
Gestione peri-operatoria del paziente in terapia con antagonisti della vitamina K. B. Cosmi
 Gestione peri-operatoria del paziente in terapia con antagonisti della vitamina K B. Cosmi Department of Angiology and Blood Coagulation S. Orsola-Malpighi University Hospital Bologna, Italy Overview Background
Gestione peri-operatoria del paziente in terapia con antagonisti della vitamina K B. Cosmi Department of Angiology and Blood Coagulation S. Orsola-Malpighi University Hospital Bologna, Italy Overview Background
Survey patients for Sx, signs of AF. Establish AF Dx. Evaluate & Tx underlying heart disease/other causes. Assess adequacy of rate or rhythm control
 Suggested General Approach to Managing Atrial Fibrillation Survey patients for Sx, signs of AF Establish AF Dx ECG Holter Event monitor Implanted device (pacer) Determine & Tx stroke risk (CHA 2 DS 2 VASc)
Suggested General Approach to Managing Atrial Fibrillation Survey patients for Sx, signs of AF Establish AF Dx ECG Holter Event monitor Implanted device (pacer) Determine & Tx stroke risk (CHA 2 DS 2 VASc)
DIAGNOSIS AND MANAGEMENT OF DIURETIC RESISTANCE. Jules B. Puschett, M.D.
 DIAGNOSIS AND MANAGEMENT OF DIURETIC RESISTANCE Jules B. Puschett, M.D. Diuretic Resistance A clinical circumstance in which patients do not respond to a combination of salt restriction and even large
DIAGNOSIS AND MANAGEMENT OF DIURETIC RESISTANCE Jules B. Puschett, M.D. Diuretic Resistance A clinical circumstance in which patients do not respond to a combination of salt restriction and even large
Atrial Fibrillation Version 2 11/4/15 This order set must be used with an admission order set if patient not already admitted.
 Patient Name: Diagnosis: Allergies with reaction type: Atrial Fibrillation Version 2 11/4/15 This order set must be used with an admission order set if patient not already admitted. Telemetry Medical Telemetry:
Patient Name: Diagnosis: Allergies with reaction type: Atrial Fibrillation Version 2 11/4/15 This order set must be used with an admission order set if patient not already admitted. Telemetry Medical Telemetry:
Rural STEMI System of Care Success. Nicole Huber, PA-C Cumberland Healthcare Emergency Department
 Rural STEMI System of Care Success Nicole Huber, PA-C Cumberland Healthcare Emergency Department DISCLOSURES I HAVE NO ACTUAL OR POTENTIAL CONFLICT OF INTEREST IN RELATION TO THIS PRESENTATION Ideal Process
Rural STEMI System of Care Success Nicole Huber, PA-C Cumberland Healthcare Emergency Department DISCLOSURES I HAVE NO ACTUAL OR POTENTIAL CONFLICT OF INTEREST IN RELATION TO THIS PRESENTATION Ideal Process
Subclinical AF: Implications of device based episodes
 Subclinical AF: Implications of device based episodes Michael R Gold, MD, PhD Medical University of South Carolina Charleston, SC Disclosures: Clinical Trials and Consulting: Medtronic, Boston Scientific
Subclinical AF: Implications of device based episodes Michael R Gold, MD, PhD Medical University of South Carolina Charleston, SC Disclosures: Clinical Trials and Consulting: Medtronic, Boston Scientific
Complicanze aritmiche in riabilitazione dopo CCH.
 Complicanze aritmiche in riabilitazione dopo CCH www.fisiokinesiterapia.biz Post-Operative Atrial Fibrillation The rate of AF after cardiac surgery in the 1970s was about 10%, and is now consistently at
Complicanze aritmiche in riabilitazione dopo CCH www.fisiokinesiterapia.biz Post-Operative Atrial Fibrillation The rate of AF after cardiac surgery in the 1970s was about 10%, and is now consistently at
Preoperative Management of Patients Receiving Antithrombotics
 Preoperative Management of Patients Receiving Antithrombotics Bleeding complications remain an important concern for most surgical procedures. Attempts to minimize the risk of these complications by removing
Preoperative Management of Patients Receiving Antithrombotics Bleeding complications remain an important concern for most surgical procedures. Attempts to minimize the risk of these complications by removing
Atrial Fibrillation (AF)
") Coronary Heart Disease Managed Clinical Network Atrial Fibrillation (AF) Guidelines for Primary Care Definition Atrial Fibrillation (AF) is defined as a cardiac arrhythmia with the following characteristics:
Coronary Heart Disease Managed Clinical Network Atrial Fibrillation (AF) Guidelines for Primary Care Definition Atrial Fibrillation (AF) is defined as a cardiac arrhythmia with the following characteristics:
CASE-BASED SMALL GROUP DISCUSSION
 MHD I, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD I SESSION 11 Renal Block Acid- Base Disorders November 7, 2016 MHD I, Session 11, Student Copy Page 2 Case #1 Cc: I have had
MHD I, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD I SESSION 11 Renal Block Acid- Base Disorders November 7, 2016 MHD I, Session 11, Student Copy Page 2 Case #1 Cc: I have had
Manuel Castellá Cardiovascular Surgery Hospital Clínic, Universidad de
 When not to exclude the LAA Manuel Castellá Cardiovascular Surgery Hospital Clínic, Universidad de Barcelona mcaste@clinic.ub.es @mcastellamd Normal hearts Patient in sinus rhythm Patient in AF (with
When not to exclude the LAA Manuel Castellá Cardiovascular Surgery Hospital Clínic, Universidad de Barcelona mcaste@clinic.ub.es @mcastellamd Normal hearts Patient in sinus rhythm Patient in AF (with
Anticoagulation in Special populations. Ng Heng Joo Department of Haematology Singapore General Hospital
 Anticoagulation in Special populations Ng Heng Joo Department of Haematology Singapore General Hospital roymatheson.com Objectives Safer anticoagulation for The elderly Chronic kidney disease Obese patients
Anticoagulation in Special populations Ng Heng Joo Department of Haematology Singapore General Hospital roymatheson.com Objectives Safer anticoagulation for The elderly Chronic kidney disease Obese patients
SUPPLEMENTAL MATERIAL
 SUPPLEMENTAL MATERIAL Table S1: Number and percentage of patients by age category Distribution of age Age
SUPPLEMENTAL MATERIAL Table S1: Number and percentage of patients by age category Distribution of age Age
Routine Clinic Lab Studies
 Routine Lab Studies Routine Clinic Lab Studies With all lab studies, a Tacrolimus level will be obtained. These drug levels are routinely assessed to ensure that there is enough or not too much anti-rejection
Routine Lab Studies Routine Clinic Lab Studies With all lab studies, a Tacrolimus level will be obtained. These drug levels are routinely assessed to ensure that there is enough or not too much anti-rejection
New options in Stroke Prevention in AF Paul Dorian University of Toronto St Michael s Hospital
 New options in Stroke Prevention in AF Paul Dorian University of Toronto St Michael s Hospital Disclosures: Honoraria, research support, and consulting f Sanofi, Boehringer-Ingleheim, Portola, BMS, Bayer,
New options in Stroke Prevention in AF Paul Dorian University of Toronto St Michael s Hospital Disclosures: Honoraria, research support, and consulting f Sanofi, Boehringer-Ingleheim, Portola, BMS, Bayer,
BC Cancer Protocol Summary for Treatment of Platinum Resistant Epithelial Ovarian Cancer with Bevacizumab and Vinorelbine
 BC Cancer Protocol Summary for Treatment of Platinum Resistant Epithelial Ovarian Cancer with Bevacizumab and Vinorelbine Protocol Code Tumour Group Contact Physician UGOOVBEVV Gynecologic Oncology Dr.
BC Cancer Protocol Summary for Treatment of Platinum Resistant Epithelial Ovarian Cancer with Bevacizumab and Vinorelbine Protocol Code Tumour Group Contact Physician UGOOVBEVV Gynecologic Oncology Dr.
ESC Stockholm Arrhythmias & pacing
 ESC Stockholm 2010 Take Home Messages for Practitioners Arrhythmias & pacing Prof. Panos E. Vardas Professor of Cardiology Heraklion University Hospital Crete, Greece Disclosures Small teaching fees from
ESC Stockholm 2010 Take Home Messages for Practitioners Arrhythmias & pacing Prof. Panos E. Vardas Professor of Cardiology Heraklion University Hospital Crete, Greece Disclosures Small teaching fees from
Question 1: Between 1 July 2014 and 30 June 2015, in the area covered by your CCG:
 Atrial Fibrillation in Your Area Question 1: Between 1 July 2014 and 30 June 2015, in the area covered by your CCG: a) What was the prevalence of atrial fibrillation (AF)? 6636 (as of 22/10/2015) 2.1%
Atrial Fibrillation in Your Area Question 1: Between 1 July 2014 and 30 June 2015, in the area covered by your CCG: a) What was the prevalence of atrial fibrillation (AF)? 6636 (as of 22/10/2015) 2.1%