Safety assessment 2018
|
|
|
- Phillip Atkinson
- 5 years ago
- Views:
Transcription
1 Safety assessment 2018
2 Safety and efficacy What is the most important? You can t have one without the other! Equally important but with very different characteristics
3 Safety and efficacy Hypotheses for efficacy are (should be) well-defined Clinical trials are most often dimensioned for the primary efficacy variable Hypotheses concerning safety assessments are less well-defined Dimensioning for safety would require very large studies, since also very rare events could be of outmost importance
4 Safety assessments in clinical trials We don t know what we are looking for, just that we will not like it when we find it! Adverse events Laboratory data (bilirubin, creatinine, calcium, haemoglobin, ) Vital signs (pulse, blood pressure) ECG Physical examination (skin, head and neck, lungs, )
5 Extent of exposure How many? Number of patients exposed to drug How long? Duration of exposure How much? Dose Toxicity =f (exposure)
6 Extent of exposure: Examples Number of subjects Number of doses Doses received mg mg mg mg mg Treatment A (n = 1698) Treatment B (n = 1699) Duration (patient years) Total Duration (days) Total Mean SD Range
7 Terminology for adverse events Adverse drug reaction Toxicities Side effect Severe adverse event Risk Significant adverse event Adverse experience Adverse event Serious adverse event
8 Adverse event Definition (ICH): An adverse event is any untoward medical occurrence in a patient or clinical investigational subject administered a pharmaceutical product and that does not necessarily have a causal relationship with this treatment. An AE can therefore be any unfavorable and unintended sign (including an abnormal laboratory finding), symptom, or disease temporally associated with the use of a medicinal (investigational) product, whether or not it is related to the medicinal (investigational) product.
9 Serious adverse event Definition (ICH): A serious adverse event or reaction is any untoward medical occurrence that any dose: Results in death Is life-threatening Requires inpatient hospitalization or prolongation of existing hospitalisation Results in persistent of significant disability/incapacity Is a congenital anomaly/birth defect

10 Issues Multiplicity to test or not to test Population vs individual one patient can kill the drug Data cleaning What is extreme multiplicity again
11 Background The Regulations/ requirements cover: Definitions of adverse events, The responsibilities of investigators for recording of adverse events and the notification of adverse events to sponsors The responsibilities of sponsors for providing to regulatory authorities regular Safety Reports.
12 Adverse Reaction (AR) Adverse Reaction (AR) Any unintended responses to an investigational medicinal product related to any dose administered Comment: All adverse events judged by either the reporting investigator or the sponsor as having a reasonable causal relationship to a medicinal product qualify as adverse reactions. The expression reasonable causal relationship means to convey in general that there is evidence or argument to suggest a causal relationship.
13 Unexpected Adverse Reaction Unexpected Adverse Reaction (UAR) An adverse reaction, the nature or severity of which is not consistent with the applicable product information (e.g. investigator s brochure for an unauthorised investigational product or summary of product characteristics for an authorised product) Comment: When the outcome of the adverse reaction is not consistent with the applicable product information this adverse reaction should be considered as unexpected.
14 Definition of Seriousness Serious Adverse Event (SAE) or Serious Adverse Reaction (SAR) or Suspected Unexpected Serious Adverse Reaction (SUSAR) Any AE, AR or UAR that at any dose: results in death is life-threatening* requires hospitalisation or prolongation of existing hospitalisation results in persistent or significant disability or incapacity consists of a congenital anomaly or birth defect
15 Assessment Assessment of an adverse event covers three main areas: Assessment of Seriousness Assessment of Causality Assessment of Expectedness
16 Assessment of Seriousness results in death is life-threatening requires hospitalisation hospitalisation or prolongation of existing results in incapacity persistent or significant disability or consists of a congenital anomaly or birth defect Note: The term severe is often used to describe the intensity (clinical severity) of a specific event. This is not the same as serious, which is a regulatory definition based on patient/event outcome or action criteria. For example, a headache may be severe but not serious while a minor stroke may be serious but not severe.
17 Assessment of Expectedness The evaluation of expectedness is based on knowledge of the adverse reaction and any relevant product information. What might we expect to see? very little it is very safe AE s reported have been..
18 Coding of adverse events Dictionaries needed in order to group similar events Many different dictionaries available: Coding Symbols for a Theaurus of a Adverse Reaction Term (COSTART) World Health Orginasation Adverse Reaction Terminology (WHOART) Medical Dictionary for Regulatory Activities (MedDRA)
19 MedDRA coding MedDRA Structure Hierarchy System Organ Class (SOC) Example Infections and infestations High Level Group Term (HLGT) Infections pathogen unspecified High Level Term (HLT) Upper respiratory tract infections Preferred Term (PT) Nasopharyngitis Lowest Level Term (LLT) Common cold
20 Types of adverse events Different types of events: Absorbing events (e.g. death) Probability of occurrence Recurrent events with negligible duration (e.g. ) Number of events Recurrent events with nonnegligible duration (e.g. headache) Proportion of time affected Different measures and analysis are relevant!
21 Analysis of adverse events Descriptive statistics often the primary approach Number and proportion of AEs Number and proportion of patients with AEs Rates of occurrence of adverse events Number of events per patient years Relative risks used to compare treatments Hazard rate Stratified Mantel-Haenszel estimate of relative risk
22 Example Number (%) of patients with at least one AE and total number of AEs Number (%) of patients with AE Treatment A N = 87 Treatment B N = 83 Any AE 57 (65.5%) 64 (77.1%) SAE with outcome death 0 (0%) 1 (1.2%) SAE 5 (5.7%) 4 (4.8%) AE leading to discontinuation of study drug 4 (4.6%) 11 (13.3%) AE leading to discontinuation of study 0 (0%) 0 (0%) Total number of AEs Any AE SAE 6 5
23 Analysis of adverse events Number (%) of patients with SAEs by preferred term Treatment A N = 87 Treatment B N = 83 Patients with any SAE 5 (5.7%) 4 (4.8%) Preferred term Back pain 1 (1.1%) 1 (1.2%) Cerebrovascular accident 1 (1.1%) Hypotension 2 (2.3%) 1 (1.2%) Lower limb fracture 1 (1.2%) Major depression 1 (1.1%) Pneumonia 1 (1.1%) 2 (2.4%)
24 Detecting Signals from Clinical Trial Data Data standards make it possible to automate statistical screening to systematically explore safety issues and generate hypotheses Can use techniques such as 2 x 2 table analyses or logistic regression after blind is broken Depends on effective visualizations to identify potential signals and outliers Bayesian models can be helpful Multivariate estimation of possibly related AEs Searching for syndromes (different AEs in the same patients) associated with treatment and subgroup effects Borrowing strength across medically related AEs But requires a priori comparator distribution.
25 Estimating relative risk Assume k trials, each with two treatments (A and B). The relative risk of a certain (absorbing!) event is assumed to be the same in each trial and the number of events are assumed to follow a Poisson distribution. i = 1,,k (trials); j = A,B (treatments) E ij = number of events in trial i on treatment j e ij = observed number of events in trial i on treatment j t ij = total exposure time in trial i on treatment j E ij ϵ Po(λ ij t ij ) Var[E ij ] = λ ij t ij λ ij = e ij / t ij
26 The Mantel-Haenszel estimate Mantel-Haenszel estimate (stratified by trial) of the common relative risk, RR MH : λ j = Σ i w i λ ij / Σ i w i w i = 2 / (1/t ia + 1/t ib ) RR MH = λ A / λ B log RR MH = log λ A log λ B
27 Variance Variance of the Mantel-Haenszel estimate : Var [λ j ] = (Σ i w i2 e ij / t ij2 ) / (Σ i w i ) 2 Var [log λ j ] = 1/λ j2 Var [λ j ] = (Σ i w i2 e ij / t ij2 ) / (Σ i w i e ij / t ij ) 2
28 Confidence intervals Confidence intervals: CI λj = λ j ± 1.96 (Var [λ j ]) 1/2 CI λa - λ B = λ A - λ B ± 1.96 (Var [λ A ] + Var [λ B ]) 1/2 CI logrrmh = log λ A - log λ B ± 1.96 (Var [log λ A ] + Var [log λ B ]) 1/2 CI RRMH = λ A / λ B exp { ±1.96 (Var [log λ A ] + Var [log λ B ]) 1/2 }
29 Example Summary of exposure and number of patients with renal impairment Treatment A N Events Exposure (pt yrs) Event rate (per pt yr) Treatment B N Events Exposure (pt yrs) Event rate (per pt yr) Trial Trial Trial Trial
30 Example Mantel-Haenszel estimates of the event rate (per pt yr) for renal impairment Estimate 95% confidence interval Treatment A [0.025, 0.056] Treatment B [0.014, 0.048] Mantel-Haenszel estimates of the risk for renal impairment for treatment A compared to treatment B Estimate 95% confidence interval Risk difference (A-B) [ , ] Relative risk (A versus B) 1.44 [0.68, 3.05]
31 Safety variables Adverse Events Vital signs (pulse, weight, blood pressure) Labvariables by organ class Lab Variable = Variable indicating biological function observed from biological sample (analysed in a lab)
32 Clinical chemistry aspartate aminotransferase, alanine aminotransferase, alkaline phosphatase, bilirubin (total), creatinine, thyroid stimulating hormone, thyroxin (free), urate, albumin, C-reactive protein Haematology haemoglobin, haptoglobin, leukocyte count, thrombocyte count, reticulocyte count, leukocyte differential count, mean corpuscular volume, mean corpuscular haemoglobin concentration glucose, sodium, potassium, calcium (albumin corrected), creatine kinase Urinalysis protein, glucose, haemoglobin
33 Reference limits Created from a population data set, often specific to each lab leading to different labs having different reference limits Used to indicate abnormal values. Lower limit of normal Upper limit of normal May differ between males, females, age groups
34 What are we looking for? Long term gradual effects Acute toxic reactios Shift in population average Reactions in few sensitive patients
35 24 hours post-dose Percentage of patients with ALT>3*ULN (%) Examples ALAT (µkat/l) AZDXXXX, 4 1 0,75 n=29 3,5 3 2,5 n=1 n=1 n=1 0,5 2 1,5 0,25 1 0, ,25 0,5 0,75 1 Pre-dose 0 Predose(n=1465) 1 week (n=1462) 2 weeks (n=1414) 4 weeks (n=914)8 weeks (n=123) No indication of acute effect of a single dose on the liver. An increase in the percentage of patients with ALT>3*ULN indicates potential liver issues developing over time.
36 ALT, AST, ALP (µkat/l) Bilirubin (µmol/l) Examples 7 6 1,4 1, ,8 0,6 0,4 0, Time from randomisation (Days) ALT (µkat/l) AST (µkat/l) ALP (µkat/l) Bilirubin (µmol/l) Liver values for a single patient
37 Table 1 Pre-dose and last visit observations of clinical chemistry variables, Safety Population Pre-dose Last visit a Change b Lab variable (unit) Treatment Mean (SD) Mean (SD) Mean (SD) ALT (µkat/l ) AZDXXXX 25 mg 0.51 (0.30) 0.52 (0.30) 0.01 (0.22) AZDXXXX50 mg 0.50 (0.27) 0.54 (0.30) 0.05 (0.21) AZDXXXX5 75 mg 0.51 (0.29) 0.53 (0.34) 0.02 (0.22) AST (µkat/l ) AZDXXXX5 25 mg 0.41 (0.20) 0.41 (0.15) 0.00 (0.17) AZDXXXX5 50 mg 0.39 (0.14) 0.42 (0.18) 0.03 (0.13) AZDXXXX5 75 mg 0.40 (0.15) 0.41 (0.16) 0.01 (0.14) ALP (µkat/l ) AZDXXXX5 25 mg 1.37 (0.40) 1.34 (0.39) (0.18) AZDXXXX5 50 mg 1.35 (0.40) 1.34 (0.39) (0.17) AZDXXXX5 75 mg 1.36 (0.39) 1.33 (0.37) (0.19) CK (µkat/l ) AZDXXXX5 25 mg 2.84 (14.54) 2.18 (1.57) (14.36) AZDXXXX5 50 mg 2.20 (1.55) 2.17 (1.77) (1.81) AZDXXXX5 75 mg 2.13 (1.44) 2.14 (1.37) 0.01 (1.37) Creatinine (µmol/l ) AZDXXXX5 25 mg (17.45) (16.71) (11.00) AZDXXXX5 50 mg (18.03) (16.06) (13.78) AZDXXXX5 75 mg (17.59) (16.48) (10.54) Bilirubin, tot (µmol/l ) AZDXXXX5 25 mg 9.66 (4.53) 9.56 (4.81) (3.57) AZDXXXX5 50 mg (5.36) 9.33 (4.45) (3.82) AZDXXXX5 75 mg 9.69 (4.80) 8.90 (4.00) (3.55) Sodium (mmol/l ) AZDXXXX5 25 mg (2.51) (2.75) 0.41 (2.90) AZDXXXX5 50 mg (2.49) (2.71) 0.14 (2.70) AZDXXXX5 75 mg (2.38) (2.57) 0.42 (2.75)

38
39 Regulatory Considerations Patient safety is the paramount concern Ensuring validity of statistical inferences and minimizing bias Maintaining study integrity (preplanning endpoints and analyses and maintaining blind) Data Safety Review Committees to have access to blinded data is accepted practice No official regulatory opinion on validity of using prior distributions and surrogate placebo populations as comparators
40 Further issues in Drug Safety Data Monitoring Committees stopping for harm/futility quality reporting of harms absolute risk matters balancing efficacy and harm scare stories good evidence posting-licencing safety trials meta-analyses (good and bad) observational data (tricky) 40
41 Data Monitoring for Safety Apparent harm with a new treatment ILLUMINATE trial Torcetrapib vs. placebo In patients at high risk of CVD Primary endpoint: CHD death, MI, stroke + unstable angina Accrual Aug 2004 to Dec 2005 Torcetrapib raises HDL cholesterol (but also raises BP) 41
42 the agonizing negative trend emerging evidence of excess deaths on torcetrapib monthly safety report 30 Nov vs 51 deaths P=0.007 statistical stopping guideline for safety: P<0.01 DSMB teleconference 1 Dec 2006, recommendation to stop Sponsor stopped torcetrapib trials on 2 Dec
43 Stopping for futility HEART2D Trial: insulin lispro vs standard insulin planned 1355 patients with type 2 diabetes and acute MI primary endpoint: major CV events over mean 3 years stopping guideline for futility in 4 th interim analyses: stop if conditional power < 40%, assuming true effect corresponds to observed hazard ratio The DMC has the authority to overrule the stated guidelines 4 th interim analysis lispro vs control primary endpoints 170/ /557 hazard ratio 0.98 (95%CI 0.79, 1.21) conditional power < 1% DMC recommended stopping, sponsor agreed 43
44 Stopping for efficacy: need overwhelming evidence ASCOT trial in hypertension [Lancet p 895-] amlodipine-based vs atenolol-based regimes in patients DSMB recommended stopping in Nov 2003 amlodipine atenolol coronary events (primary) P =.14 strokes P =
45 Trial Executive informed much debate, collective decision to continue tricky to stop on basis of secondary endpoint, even if in hindsight primary endpoint debatable DSMB again recommends stopping, October 2004: mortality difference significant other differences unchanged 45
46 ASCOT final results (N=19257, median 5.5 years) amlodipine atenolol hazard ratio non-fatal MI & fatal CHD P=.11 stroke P=.0003 CV deaths P=.001 all deaths P=.02 new diabetes P<
47 Improving the Reporting of Harms (Safety) CONSORT extension [Ann Intern Med 2004; 141 p 781-] essentials: collect quality data on harms include harms in any trial report quantify them appropriately 47
48 START trial budesonide vs placebo in recent-onset asthma 7241 patients, including 1974 aged 10 or less initial manuscript Early intervention with budesonide in mild persistent asthma: a worldwide effectiveness study no mention of reduced growth in children published paper [Lancet 2003: 361 p 1071-] Early intervention with budesonide in mild persistent asthma: a randomised double blind trial 3 year growth was reduced in budesonide group by 1.34cm 44% reduction in hazard of severe asthma exacerbation 48
49 Prasugrel vs Clopidogrel in acute coronary syndromes [NEJM 2007; 357 p 2001-] more bleeding events on prasugrel sensational approach: four-fold increase in fatal bleeds on prasugrel switching from clopidogrel to prasugrel would cause thousands more major bleeds per year worldwide 49
50 The data as published TRITON TIMI 38 trial, 15 months follow-up prasugrel clopidogrel hazard ratio(95%ci) N fatal bleed 21(0.4%) 5(0.1%) 4.19( ) major bleed (non CABG related) 146(2.4%) 111(1.8%) 1.32( ) bleeding requiring transfusion 244(4.0%) 182(3.0%) 1.34( ) all bleeds 303(5.5%) 231(3.8%) 1.31( ) 50
51 Absolute risk is key major bleeds increased by 0.6% (35 events) [95% CI 0.1% to 1.1%] no. needed to harm is around 170, with wide CI 51
52 Balancing efficacy and harm prasugrel clopidogrel N hazard ratio (95%CI) CV death non fatal MI 475(7.3%) 620(9.5%) 0.76 ( ) non-fatal stroke composite ( ) stent thrombosis
53 major bleeds increased by 0.6% (35 events) [95% CI 0.1% to 1.1%] no. needed to harm is around 170, with wide CI myocardial infarction reduced by 2.2% (145 events) [95% CI 1.2% to 3.2%] no. needed to treat (NNT) is around 45 overall, benefit outweighs risk of harm but need to assess individual risk who s at high risk of bleed? Eg women 53
54 Scare stories, politics and the media 1)Avandia (Rosiglitazone) 2) Drug-eluting stents how can we avoid over-reaction what s the real evidence what s the appropriate consequences 54
55 Safety issues in the real world activists defensive companies objective unbiassed evidence clinical trials, meta-analyses, observational data, media distortions decisions by: regulatory authorities treating physicians patients 55
56 Rosiglitazone (rosi) and cardiovascular risk Meta-analysis of 42 trials [NEJM 14 June 2007] Rosi vs Control odds ratio (95% CI) Myocardial infarction 1.43 (1.03 to 1.98) CV death 1.64 (0.98 to 2.74) limited evidence, mostly small trials, unvalidated events high profile, Congress involved, FDA under attack 56
57 I was truly frightened on behalf of our patients The Times (business section) Alarmist headlines and confident declarations help nobody The Lancet Meta-analysis seems a rushed and incomplete examination Nature 57
58 RECORD Trial Interim Analysis [NEJM 5 July 2007] Rosi + M or S vs Metformin + Sulfonylurea 4458 diabetic patients, mean 3.75 years follow-up Rosi Control CV death P=.46 Myocardial infarction P=.34 Heart failure P=.003 Any CV hosp/death P=.43 58
59 no excess of CV deaths inconclusive evidence re myocardial infarction the real problem is heart failure other trials and meta-analyses: applies to rosi and pioglitazone avoid their use in high-risk patients A thunderstorm from scarce and fragile data Ann Int Med Thiazolidinediones, deadly sins, surrogates and elephants Lancet 59
60 Rosiglitazone (rosi) increases risk of fractures? ADOPT trial [NEJM 2006; 355 p 2427-] 4360 diabetic patients, mean 4.0 years follow-up incidence of fractures rosi metformin glyburide men 32 (4.0%) 29 (3.4%) 28 (3.4%) women 60 (9.3%) 30 (5.1%) 21 (3.5%) a problem in women only? also happens with pioglitazone? probably doubtful 60
61 Fracture risks of rosi and pioglitazone lack of trial data try observational registries Case-Control Study using GPRD [Archives Int Med 2008; 168 p 820-] 1020 fracture cases and 3728 matched controls (all diabetic) adjusted Rosi or Pio cases controls odds ratio (95% CI) prescriptions versus no use < ( ) ( ) ( ) 61
62 search for consistency with alternative analyses self-controlled case series approach also using GPRD 1819 diabetic patients with fracture before or after start of rosi or pioglitazone [unpublished] compare pre-and post-exposure periods in same patient conditional Poisson regression, age adjusted rate ratio (95% CI) females 1.42 (1.20, 1.69) males 1.44 (1.18, 1.77) Increasing risk by duration of exposure 62
63 safety concerns re drug-eluting stents scare story sensible risk-benefit assessment drug-eluting stent (DES) vs bare-metal stent (BMS) in PCI ACC presentation March 2006 BASKET LATE trial (N=743) cardiac death and MI 4.9% vs 1.3% P=.01 ESC presentations Sept 2006 two poor quality meta-analyses and large Swedish registry all showing mortality risks of DES major outcry, reduced use of DES 63
64 Drug-Eluting Stent (DES) vs Bare Metal Stent (BMS) a meta-analysis update re mortality risk by Ajay Kirtane, Gregg Stone et al (2008) 21 RCTs: 8867 patients, mean f/u 2.9 years 31 Registries: 169,595 patients, mean f/u 2.5years 64
65 Hazard Ratios for Mortality 21 RCTs Fixed Effect % CI 0.81, 1.15 P= Registries Fixed Effect % CI 0.78, 0.85 P<.001 Random Effects % CI 0.71, 0.86 Heart. Org Sept 2008 the latest registry [JACC 2008; 52 p1041-] DES in real-world setting lower mortality Cleveland Clinic: 6053 DES, 1983 BMS, mean f/u 4.5 years hazard ratio % CI 0.45, 0.66 with propensity matching too good to be true? 65
66 Why such discrepancies between RCTs and Registries? RCTs not representative of real-world use Registries prone to selection bias, not captured by adjustment for confounders, which vary enormously across registries mortality risk depends on so many factors not related to specific PCI any true effect (DES vs BMS) should be small? 66
67 Interpretation of Surprises, especially re Safety Excess of Cancers in the SEAS trial [NEJM Sept 2008] simvastatin + ezetimibe placebo N with aortic stenosis median 1 year follow-up primary CV outcome P=.59 incident cancer P=.01 cancer death P=.05 when faced with a surprise (benefit or harm) collect more data and expect regression to the truth 67
68 interim results from SHARP and IMPROVE-IT [NEJM Sept 2008] ezetimibe placebo N incident cancer P=.61 cancer death P=.07 illogical pattern, no specific cancers the available results do not provide credible evidence of any adverse effect of ezetimibe on rates of cancer? 68
69 New trends There is a clear renewed emphasis on drug safety in today on drug safety in today s regulatory s regulatory environment with impact on study design and environment with impact on st udy design and statistical analyses: statistical analyses: Specialized studies designed to test hypotheses Specialized stu dies designed to test hypotheses about safety about safety New requirements for additional analyses New requirements for additional analyses involving inferential statistical methods app lied to involving inferential statistical methods applied to indivi dual studies and safety databases for entire individual studies and safety databases for entire development programs

70

71

72
73

74
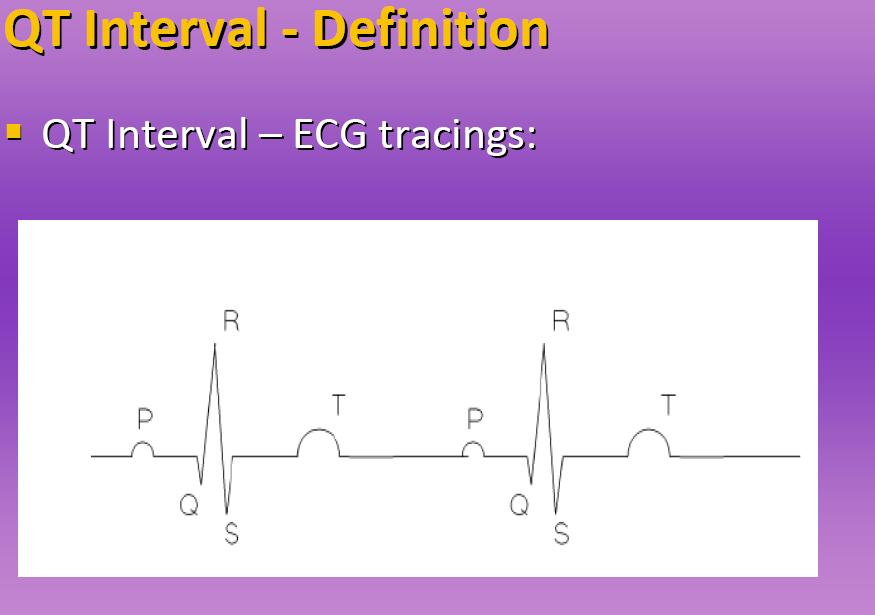
75 QT Drugs that have been withdrawn from the market because they cause torsade de pointes had a population mean increase in the QT interval estimated to be as small as 5 to 10 ms There is an inverse relationship between QT interval and heart rate. Therefore, it is necessary to correct QT for the heart rate and calculate a corrected QT or QTc. It is not clear whether arrhythmia development is more closely related to an increase in the absolute QT interval or QTc. ICH E14 October 2005: Clinical Evaluation of QT/QTc Interval Prolongation and Pro arrhythmic Potential for Non Anti arrhythmic Drugs
76 Guidance: Thorough investigation of potential for QT/QTc prolongation is recommended for All systemically bio available new drugs Excludes topically active medications and antiarrhythmic medications Includes approved drugs investigated for new routes of administration or higher dosages, new patient populations/indications Especially important for drugs within a suspect drug class
ESC Geoffrey Rose Lecture on Population Sciences Cholesterol and risk: past, present and future
 ESC Geoffrey Rose Lecture on Population Sciences Cholesterol and risk: past, present and future Rory Collins BHF Professor of Medicine & Epidemiology Clinical Trial Service Unit & Epidemiological Studies
ESC Geoffrey Rose Lecture on Population Sciences Cholesterol and risk: past, present and future Rory Collins BHF Professor of Medicine & Epidemiology Clinical Trial Service Unit & Epidemiological Studies
LATE BREAKING STUDIES IN DM AND CAD. Will this change the guidelines?
 LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
Seeing Chickens at Window Recording Adverse Events and GeneratingQuality Data. Margaret Band, Clinical Trial Manager, TCTU
 Seeing Chickens at Window Recording Adverse Events and GeneratingQuality Data Margaret Band, Clinical Trial Manager, TCTU Adverse Event Reporting Monitoring of adverse events (AEs) is critical to the patient
Seeing Chickens at Window Recording Adverse Events and GeneratingQuality Data Margaret Band, Clinical Trial Manager, TCTU Adverse Event Reporting Monitoring of adverse events (AEs) is critical to the patient
Adverse Experience Reporting
 Managing and reporting adverse events Key learning objectives By the end of this session, you will be able to: Define and classify an adverse event; Differentiate between serious and severe adverse events;
Managing and reporting adverse events Key learning objectives By the end of this session, you will be able to: Define and classify an adverse event; Differentiate between serious and severe adverse events;
ST. MICHAEL S HOSPITAL Guidelines for Reporting Serious Adverse Events / Unanticipated Problems to the SMH Research Ethics Board (REB) July 09, 2014
 July 09, 2014") ST. MICHAEL S HOSPITAL Guidelines for Reporting Serious Adverse Events / Unanticipated Problems to the SMH Research Ethics Board (REB) July 09, 2014 1. Introduction The St. Michael s Hospital (SMH) REB
ST. MICHAEL S HOSPITAL Guidelines for Reporting Serious Adverse Events / Unanticipated Problems to the SMH Research Ethics Board (REB) July 09, 2014 1. Introduction The St. Michael s Hospital (SMH) REB
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not
 The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
Study No.: Title: Rationale: Phase: Study Period: Study Design: Centres: Indication: Treatment: Objectives: Primary Outcome/Efficacy Variable:
 The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES
 ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
JAMA. 2011;305(24): Nora A. Kalagi, MSc
: Nora A. Kalagi, MSc") JAMA. 2011;305(24):2556-2564 By Nora A. Kalagi, MSc Cardiovascular disease (CVD) is the number one cause of mortality and morbidity world wide Reducing high blood cholesterol which is a risk factor for
JAMA. 2011;305(24):2556-2564 By Nora A. Kalagi, MSc Cardiovascular disease (CVD) is the number one cause of mortality and morbidity world wide Reducing high blood cholesterol which is a risk factor for
Sponsor Novartis. Generic Drug Name Fluvastatin. Therapeutic Area of Trial Dyslipidemia
 Page 1 Sponsor Novartis Generic Drug Name Fluvastatin Therapeutic Area of Trial Dyslipidemia Approved Indication Therapeutic area and approved indications in Germany: Hypercholesterolemia (HC), combined
Page 1 Sponsor Novartis Generic Drug Name Fluvastatin Therapeutic Area of Trial Dyslipidemia Approved Indication Therapeutic area and approved indications in Germany: Hypercholesterolemia (HC), combined
Occurrence of Bleeding and Thrombosis during Antiplatelet therapy In Non-cardiac surgery. A prospective observational study.
 Occurrence of Bleeding and Thrombosis during Antiplatelet therapy In Non-cardiac surgery A prospective observational study OBTAIN Study Statistical Analysis Plan of Final Analysis Final Version: V1.1 from
Occurrence of Bleeding and Thrombosis during Antiplatelet therapy In Non-cardiac surgery A prospective observational study OBTAIN Study Statistical Analysis Plan of Final Analysis Final Version: V1.1 from
DECLARATION OF CONFLICT OF INTEREST. Lecture fees: AstraZeneca, Ely Lilly, Merck.
 DECLARATION OF CONFLICT OF INTEREST Lecture fees: AstraZeneca, Ely Lilly, Merck. Risk of stopping dual therapy. S D Kristensen, FESC Aarhus Denmark Acute coronary syndrome: coronary thrombus Platelets
DECLARATION OF CONFLICT OF INTEREST Lecture fees: AstraZeneca, Ely Lilly, Merck. Risk of stopping dual therapy. S D Kristensen, FESC Aarhus Denmark Acute coronary syndrome: coronary thrombus Platelets
Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease. Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.
 Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.Κιλκίς Primary CVD Prevention A co-ordinated set of actions,
Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.Κιλκίς Primary CVD Prevention A co-ordinated set of actions,
Benefit/Risk Assessment A Critical Need
 Benefit/Risk Assessment A Critical Need Christy Chuang-Stein, PhD Statistics, Pfizer Inc Society for Clinical Trials 30 th Annual Meeting 1 Some Basic Facts All pharmaceutical products have side effects
Benefit/Risk Assessment A Critical Need Christy Chuang-Stein, PhD Statistics, Pfizer Inc Society for Clinical Trials 30 th Annual Meeting 1 Some Basic Facts All pharmaceutical products have side effects
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and
What oral antiplatelet therapy would you choose? a) ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor
 ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor") 76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
Regulatory Hurdles for Drug Approvals
 Regulatory Hurdles for Drug Approvals William R. Hiatt, MD Professor of Medicine/Cardiology University of Colorado School of Medicine President, CPC Clinical Research 25 min Conflicts CPC Clinical Research
Regulatory Hurdles for Drug Approvals William R. Hiatt, MD Professor of Medicine/Cardiology University of Colorado School of Medicine President, CPC Clinical Research 25 min Conflicts CPC Clinical Research
Regulatory Experience in Reviewing CV Safety for Diabetes
 Regulatory Experience in Reviewing CV Safety for Diabetes Drugs Kristina Dunder MD, PhD, Alternate CHMP member MPA, Sweden Disclaimer The views and opinions expressed in the following PowerPoint slides
Regulatory Experience in Reviewing CV Safety for Diabetes Drugs Kristina Dunder MD, PhD, Alternate CHMP member MPA, Sweden Disclaimer The views and opinions expressed in the following PowerPoint slides
Safety Assessment in Clinical Trials and Beyond
 Safety Assessment in Clinical Trials and Beyond Yuliya Yasinskaya, MD Medical Team Leader Division of Anti-Infective Products Center for Drug Evaluation and Research FDA Clinical Investigator Training
Safety Assessment in Clinical Trials and Beyond Yuliya Yasinskaya, MD Medical Team Leader Division of Anti-Infective Products Center for Drug Evaluation and Research FDA Clinical Investigator Training
Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland
 Advances in Antiplatelet Therapy in PCI and ACS Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland Targets for Platelet
Advances in Antiplatelet Therapy in PCI and ACS Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland Targets for Platelet
Macrovascular Residual Risk. What risk remains after LDL-C management and intensive therapy?
 Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
Ischemic Heart Disease: The 5 Most Important Trials in the Last Year
 Torino, IT October 2015 Ischemic Heart Disease: The 5 Most Important Trials in the Last Year Malcolm R. Bell, MBBS, FRACP Director Ischemic Heart Disease Program Mayo Clinic, MN, USA 2013 MFMER slide-1
Torino, IT October 2015 Ischemic Heart Disease: The 5 Most Important Trials in the Last Year Malcolm R. Bell, MBBS, FRACP Director Ischemic Heart Disease Program Mayo Clinic, MN, USA 2013 MFMER slide-1
þ INVOLVED OR PROLONGED INPATIENT HOSPITALISATION
 CIOMS FORM SUSPECT ADVERSE REACTION REPORT DE-BFARM-17182698 I. REACTION INFORMATION 1. PATIENT INITIALS 1a. COUNTRY 2. DATE OF BIRTH 2a. AGE 3. SEX 4-6 REACTION ONSET privacy DE DA MO YR [ MedDRA 20.0
CIOMS FORM SUSPECT ADVERSE REACTION REPORT DE-BFARM-17182698 I. REACTION INFORMATION 1. PATIENT INITIALS 1a. COUNTRY 2. DATE OF BIRTH 2a. AGE 3. SEX 4-6 REACTION ONSET privacy DE DA MO YR [ MedDRA 20.0
This clinical study synopsis is provided in line with Boehringer Ingelheim s Policy on Transparency and Publication of Clinical Study Data.
 abcd Clinical Study Synopsis for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the
abcd Clinical Study Synopsis for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the
GSK Clinical Study Register
 In February 2013, GlaxoSmithKline (GSK) announced a commitment to further clinical transparency through the public disclosure of GSK Clinical Study Reports (CSRs) on the GSK Clinical Study Register. The
In February 2013, GlaxoSmithKline (GSK) announced a commitment to further clinical transparency through the public disclosure of GSK Clinical Study Reports (CSRs) on the GSK Clinical Study Register. The
Dyslipidemia: Lots of Good Evidence, Less Good Interpretation.
 Dyslipidemia: Lots of Good Evidence, Less Good Interpretation. G Michael Allan Evidence & CPD Program, ACFP Associate Professor, Dept of Family, U of A. CFPC CoI Templates: Slide 1 Faculty/Presenter Disclosure
Dyslipidemia: Lots of Good Evidence, Less Good Interpretation. G Michael Allan Evidence & CPD Program, ACFP Associate Professor, Dept of Family, U of A. CFPC CoI Templates: Slide 1 Faculty/Presenter Disclosure
Adverse Events- Love them, hate them, report them!
 Adverse Events- Love them, hate them, report them! Billi Tatum, RN, CCRC Regional Vascular Center Harborview Medical Center and the University of Washington Medical Center Objectives Define and identify
Adverse Events- Love them, hate them, report them! Billi Tatum, RN, CCRC Regional Vascular Center Harborview Medical Center and the University of Washington Medical Center Objectives Define and identify
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
New insights in stent thrombosis: Platelet function monitoring. Franz-Josef Neumann Herz-Zentrum Bad Krozingen
 New insights in stent thrombosis: Platelet function monitoring Franz-Josef Neumann Herz-Zentrum Bad Krozingen New insights in stent thrombosis: Platelet function monitoring Variability of residual platelet
New insights in stent thrombosis: Platelet function monitoring Franz-Josef Neumann Herz-Zentrum Bad Krozingen New insights in stent thrombosis: Platelet function monitoring Variability of residual platelet
Is there enough evidence for DAPT after endovascular intervention for PAOD?
 Is there enough evidence for DAPT after endovascular intervention for PAOD? Prof. I. Baumgartner Head Clinical & Interventional Angiology University Hospital Bern Disclosure Speaker name:...i. Baumgartner...
Is there enough evidence for DAPT after endovascular intervention for PAOD? Prof. I. Baumgartner Head Clinical & Interventional Angiology University Hospital Bern Disclosure Speaker name:...i. Baumgartner...
Optimal Duration and Dose of Antiplatelet Therapy after PCI
 Optimal Duration and Dose of Antiplatelet Therapy after PCI Donghoon Choi, MD, PhD Severance Cardiovascular Center Yonsei University College of Medicine Optimal Duration of Antiplatelet Therapy after PCI
Optimal Duration and Dose of Antiplatelet Therapy after PCI Donghoon Choi, MD, PhD Severance Cardiovascular Center Yonsei University College of Medicine Optimal Duration of Antiplatelet Therapy after PCI
ILLUMINATE. Effects of torcetrapib in patients at high risk for coronary events NEJM. 2007; 357:
 ILLUMINATE. Effects of torcetrapib in patients at high risk for coronary events NEJM. 2007; 357: 2109-2122. ILLUMINATE The most important trial since 2000? Background Inhibition of cholesteryl ester transfer
ILLUMINATE. Effects of torcetrapib in patients at high risk for coronary events NEJM. 2007; 357: 2109-2122. ILLUMINATE The most important trial since 2000? Background Inhibition of cholesteryl ester transfer
GSK Medicine: Study Number: Title: Rationale: Phase: Study Period: Study Design: Centres: Indication: Treatment: Objectives:
 The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
PHARMACOVIGILANCE GLOSSARY
 PHARMACOVIGILANCE GLOSSARY Section 1 Section 2 Section 3 Section 4 Definitions of terminology used for side effects Definitions of drug safety terms Definitions of risk terminology Definitions of general
PHARMACOVIGILANCE GLOSSARY Section 1 Section 2 Section 3 Section 4 Definitions of terminology used for side effects Definitions of drug safety terms Definitions of risk terminology Definitions of general
Prasugrel vs. Ticagrelor in ACS/PCI Which one to choose? V. Voudris MD FESC FACC 2 nd Cardiology Division Onassis Cardiac Surgery Center
 Prasugrel vs. Ticagrelor in ACS/PCI Which one to choose? V. Voudris MD FESC FACC 2 nd Cardiology Division Onassis Cardiac Surgery Center Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes
Prasugrel vs. Ticagrelor in ACS/PCI Which one to choose? V. Voudris MD FESC FACC 2 nd Cardiology Division Onassis Cardiac Surgery Center Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes
תרופות מעכבות טסיות חדשות ד"ר אלי לב מנהל שרות הצנתורים ח השרון מרכז רפואי רבין
 תרופות מעכבות טסיות חדשות ד"ר אלי לב מנהל שרות הצנתורים ח השרון בי""י מרכז רפואי רבין 1. Why should clopidogrel be replaced? 2. Prasugrel 3. Ticagrelor 4. Conclusions CURE TRIAL ACS pts 20 % reduction
תרופות מעכבות טסיות חדשות ד"ר אלי לב מנהל שרות הצנתורים ח השרון בי""י מרכז רפואי רבין 1. Why should clopidogrel be replaced? 2. Prasugrel 3. Ticagrelor 4. Conclusions CURE TRIAL ACS pts 20 % reduction
Preoperative Cardiac Evaluation:
 Preoperative Cardiac Evaluation: The New Guidelines Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Disclosures No financial relationships with pharmaceutical
Preoperative Cardiac Evaluation: The New Guidelines Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Disclosures No financial relationships with pharmaceutical
WELCOME TO ONLINE TRAINING FOR CLINICAL RESEARCH COORDINATORS
 UCLA CTSI WELCOME TO ONLINE TRAINING FOR CLINICAL RESEARCH COORDINATORS ROLE OF THE RESEARCH COORDINATOR Adverse Events in Clinical Trials: Definitions and Documentation May 2016 Objectives Recognize the
UCLA CTSI WELCOME TO ONLINE TRAINING FOR CLINICAL RESEARCH COORDINATORS ROLE OF THE RESEARCH COORDINATOR Adverse Events in Clinical Trials: Definitions and Documentation May 2016 Objectives Recognize the
Summary ID#7029. Clinical Study Summary: Study F1D-MC-HGKQ
 CT Registry ID# 7029 Page 1 Summary ID#7029 Clinical Study Summary: Study F1D-MC-HGKQ Clinical Study Report: Versus Divalproex and Placebo in the Treatment of Mild to Moderate Mania Associated with Bipolar
CT Registry ID# 7029 Page 1 Summary ID#7029 Clinical Study Summary: Study F1D-MC-HGKQ Clinical Study Report: Versus Divalproex and Placebo in the Treatment of Mild to Moderate Mania Associated with Bipolar
John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam
 Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Quale terapia antiaggregante nello STEMI? Prasugrel vs ticagrelor
 Quale terapia antiaggregante nello STEMI? Prasugrel vs ticagrelor Leonardo Bolognese Cardiovascular Department, Arezzo, Italy Platelet Reactivity in Patients with STEMI Undergoing Primary PCI Campo G et
Quale terapia antiaggregante nello STEMI? Prasugrel vs ticagrelor Leonardo Bolognese Cardiovascular Department, Arezzo, Italy Platelet Reactivity in Patients with STEMI Undergoing Primary PCI Campo G et
Cardiovascular Risk of Celecoxib in 6 Randomized Placebo-controlled Trials: The Cross Trial Safety Analysis
 Cardiovascular Risk of Celecoxib in 6 Randomized Placebo-controlled Trials: The Cross Trial Safety Analysis Scott D. Solomon, MD, Janet Wittes, PhD, Ernest Hawk, MD, MPH for the Celecoxib Cross Trials
Cardiovascular Risk of Celecoxib in 6 Randomized Placebo-controlled Trials: The Cross Trial Safety Analysis Scott D. Solomon, MD, Janet Wittes, PhD, Ernest Hawk, MD, MPH for the Celecoxib Cross Trials
Understanding Adverse Events
 The Fundamentals of International Clinical Research Workshop Understanding Adverse Events Deborah Hilgenberg Family Health International Goals of the Presentation Definition of Adverse Event (AE) Definitions
The Fundamentals of International Clinical Research Workshop Understanding Adverse Events Deborah Hilgenberg Family Health International Goals of the Presentation Definition of Adverse Event (AE) Definitions
Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona,
 Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona, Jamaica At the end of this presentation the participant
Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona, Jamaica At the end of this presentation the participant
(For National Authority Use Only) Name of Study Drug: to Part of Dossier:
 Name of Study Drug: to Part of Dossier:") 2.0 Synopsis Abbott Laboratories Individual Study Table Referring to Part of Dossier: (For National Authority Use Only) Name of Study Drug: Volume: Niaspan Name of Active Ingredient: Page: Niacin extended-release
2.0 Synopsis Abbott Laboratories Individual Study Table Referring to Part of Dossier: (For National Authority Use Only) Name of Study Drug: Volume: Niaspan Name of Active Ingredient: Page: Niacin extended-release
Anti-platelet therapies and dual inhibition in practice
 Anti-platelet therapies and dual inhibition in practice Therapeutics; Sept. 25 th 2007 Craig Williams, Pharm.D. Associate Professor of Pharmacy Objectives 1. Understand the pharmacology of thienopyridine
Anti-platelet therapies and dual inhibition in practice Therapeutics; Sept. 25 th 2007 Craig Williams, Pharm.D. Associate Professor of Pharmacy Objectives 1. Understand the pharmacology of thienopyridine
Sponsor Novartis. Generic Drug Name Vildagliptin/Metformin. Therapeutic Area of Trial Type 2 diabetes. Approved Indication Type 2 diabetes
 Clinical Trial Results Database Page 1 Sponsor Novartis Generic Drug Name Vildagliptin/Metformin Therapeutic Area of Trial Type 2 diabetes Approved Indication Type 2 diabetes Study Number CLMF237A2309
Clinical Trial Results Database Page 1 Sponsor Novartis Generic Drug Name Vildagliptin/Metformin Therapeutic Area of Trial Type 2 diabetes Approved Indication Type 2 diabetes Study Number CLMF237A2309
Supplementary webappendix
 Supplementary webappendix This webappendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Ray K K, Seshasai S R K, Wijesuriya S,
Supplementary webappendix This webappendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Ray K K, Seshasai S R K, Wijesuriya S,
A Randomized Trial Evaluating Clinically Significant Bleeding with Low-Dose Rivaroxaban vs Aspirin, in Addition to P2Y12 inhibition, in ACS
 A Randomized Trial Evaluating Clinically Significant Bleeding with Low-Dose Rivaroxaban vs Aspirin, in Addition to P2Y12 inhibition, in ACS Magnus Ohman MB, on behalf of the GEMINI-ACS-1 Investigators
A Randomized Trial Evaluating Clinically Significant Bleeding with Low-Dose Rivaroxaban vs Aspirin, in Addition to P2Y12 inhibition, in ACS Magnus Ohman MB, on behalf of the GEMINI-ACS-1 Investigators
Using Statistical Principles to Implement FDA Guidance on Cardiovascular Risk Assessment for Diabetes Drugs
 Using Statistical Principles to Implement FDA Guidance on Cardiovascular Risk Assessment for Diabetes Drugs David Manner, Brenda Crowe and Linda Shurzinske BASS XVI November 9-13, 2009 Acknowledgements
Using Statistical Principles to Implement FDA Guidance on Cardiovascular Risk Assessment for Diabetes Drugs David Manner, Brenda Crowe and Linda Shurzinske BASS XVI November 9-13, 2009 Acknowledgements
Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1)
") Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1) Caitlin C. Akerman, PharmD PGY2 Cardiology Resident WakeMed Health & Hospitals Raleigh,
Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1) Caitlin C. Akerman, PharmD PGY2 Cardiology Resident WakeMed Health & Hospitals Raleigh,
CHOLESTEROL-LOWERING THERAPHY
 CHOLESTEROL-LOWERING THERAPHY TRIALS NUMBER OF PARTICIPANTS NUMBER OF WOMEN PERCENTAGE OF WOMEN MEAN AGE MEAN - (YEARS) TRIALS WITH ANALYSIS BY GENDER N, (%) 50,194 15,036 30.0% 60.8 3.2 1/ 6 (16.7%) HR
CHOLESTEROL-LOWERING THERAPHY TRIALS NUMBER OF PARTICIPANTS NUMBER OF WOMEN PERCENTAGE OF WOMEN MEAN AGE MEAN - (YEARS) TRIALS WITH ANALYSIS BY GENDER N, (%) 50,194 15,036 30.0% 60.8 3.2 1/ 6 (16.7%) HR
(For National Authority Use Only) Name of Study Drug: to Part of Dossier:
 Name of Study Drug: to Part of Dossier:") 2.0 Synopsis Abbott Laboratories Individual Study Table Referring to Part of Dossier: (For National Authority Use Only) Name of Study Drug: Volume: ABT-335 Name of Active Ingredient: Page: ABT-335, A-7770335.115
2.0 Synopsis Abbott Laboratories Individual Study Table Referring to Part of Dossier: (For National Authority Use Only) Name of Study Drug: Volume: ABT-335 Name of Active Ingredient: Page: ABT-335, A-7770335.115
Manual for Expedited Reporting of Adverse Events to DAIDS Version 2.0 January 2010
 Manual for Expedited Reporting of Adverse Events to DAIDS Version 2.0 January 2010 January 2010 Version 2.0 Table of Contents 1. INTRODUCTION...1 1.1 Scope... 1 1.2 Purpose... 1 1.3 Responsibilities...
Manual for Expedited Reporting of Adverse Events to DAIDS Version 2.0 January 2010 January 2010 Version 2.0 Table of Contents 1. INTRODUCTION...1 1.1 Scope... 1 1.2 Purpose... 1 1.3 Responsibilities...
Clinical Seminar. Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective
 Clinical Seminar Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical
Clinical Seminar Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical
Clinical Trial Synopsis TL-OPI-518, NCT#
 Clinical Trial Synopsis, NCT# 00225264 Title of Study: A Double-Blind, Randomized, Comparator-Controlled Study in Subjects With Type 2 Diabetes Mellitus Comparing the Effects of Pioglitazone HCl vs Glimepiride
Clinical Trial Synopsis, NCT# 00225264 Title of Study: A Double-Blind, Randomized, Comparator-Controlled Study in Subjects With Type 2 Diabetes Mellitus Comparing the Effects of Pioglitazone HCl vs Glimepiride
New Evidence reports on presentations given at EULAR Safety and Efficacy of Tocilizumab as Monotherapy and in Combination with Methotrexate
 New Evidence reports on presentations given at EULAR 2009 Safety and Efficacy of Tocilizumab as Monotherapy and in Combination with Methotrexate Report on EULAR 2009 presentations Tocilizumab inhibits
New Evidence reports on presentations given at EULAR 2009 Safety and Efficacy of Tocilizumab as Monotherapy and in Combination with Methotrexate Report on EULAR 2009 presentations Tocilizumab inhibits
PRASUGREL HYDROCHLORIDE (Effient Eli Lilly Canada Inc.) Indication: Acute Coronary Syndrome
 Indication: Acute Coronary Syndrome") CEDAC FINAL RECOMMENDATION PRASUGREL HYDROCHLORIDE (Effient Eli Lilly Canada Inc.) Indication: Acute Coronary Syndrome Recommendation: The Canadian Expert Drug Advisory Committee (CEDAC) recommends that
CEDAC FINAL RECOMMENDATION PRASUGREL HYDROCHLORIDE (Effient Eli Lilly Canada Inc.) Indication: Acute Coronary Syndrome Recommendation: The Canadian Expert Drug Advisory Committee (CEDAC) recommends that
Clinical Controversies in Perioperative Medicine
 Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Evaluation: New Guidelines A 70-y.o. man with progressive
Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Evaluation: New Guidelines A 70-y.o. man with progressive
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009
 The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
Treating Hypertension in 2018: What Makes the Most Sense Today?
 Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
Primary Endpoint The primary endpoint is overall survival, measured as the time in weeks from randomization to date of death due to any cause.
 CASE STUDY Randomized, Double-Blind, Phase III Trial of NES-822 plus AMO-1002 vs. AMO-1002 alone as first-line therapy in patients with advanced pancreatic cancer This is a multicenter, randomized Phase
CASE STUDY Randomized, Double-Blind, Phase III Trial of NES-822 plus AMO-1002 vs. AMO-1002 alone as first-line therapy in patients with advanced pancreatic cancer This is a multicenter, randomized Phase
Anticoagulants and antiplatelet therapy in the older patient: Choosing wisely
 Anticoagulants and antiplatelet therapy in the older patient: Choosing wisely Rajiv Gulati, MD PhD Advances in Cardiac Arrhythmias & Great Innovations in Cardiology Torino, October 2015 2015 MFMER 3477310-1
Anticoagulants and antiplatelet therapy in the older patient: Choosing wisely Rajiv Gulati, MD PhD Advances in Cardiac Arrhythmias & Great Innovations in Cardiology Torino, October 2015 2015 MFMER 3477310-1
Benefit-Risk Assessment via Case Studies: Key Considerations & Best Practices
 Benefit-Risk Assessment via Case Studies: Key Considerations & Best Practices George Quartey (PhD), Genentech Inc. (Acknowledgements: Qi Jiang, Amgen & Weili He, Merck) EFSPI Regulatory Statistics Meeting,
Benefit-Risk Assessment via Case Studies: Key Considerations & Best Practices George Quartey (PhD), Genentech Inc. (Acknowledgements: Qi Jiang, Amgen & Weili He, Merck) EFSPI Regulatory Statistics Meeting,
A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes
 A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes Hypotheses: Among individuals with type 2 diabetes, the risks of major microvascular
A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes Hypotheses: Among individuals with type 2 diabetes, the risks of major microvascular
Fasting or non fasting?
 Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
Integrating Effectiveness and Safety Outcomes in the Assessment of Treatments
 Integrating Effectiveness and Safety Outcomes in the Assessment of Treatments Jessica M. Franklin Instructor in Medicine Division of Pharmacoepidemiology & Pharmacoeconomics Brigham and Women s Hospital
Integrating Effectiveness and Safety Outcomes in the Assessment of Treatments Jessica M. Franklin Instructor in Medicine Division of Pharmacoepidemiology & Pharmacoeconomics Brigham and Women s Hospital
Supplementary Table S1: Proportion of missing values presents in the original dataset
 Supplementary Table S1: Proportion of missing values presents in the original dataset Variable Included (%) Missing (%) Age 89067 (100.0) 0 (0.0) Gender 89067 (100.0) 0 (0.0) Smoking status 80706 (90.6)
Supplementary Table S1: Proportion of missing values presents in the original dataset Variable Included (%) Missing (%) Age 89067 (100.0) 0 (0.0) Gender 89067 (100.0) 0 (0.0) Smoking status 80706 (90.6)
Ticagrelor compared with clopidogrel in patients with acute coronary syndromes the PLATO trial
 compared with clopidogrel in patients with acute coronary syndromes the PLATO trial August 30, 2009 at 08.00 CET PLATO background In NSTE-ACS and STEMI, current guidelines recommend 12 months aspirin and
compared with clopidogrel in patients with acute coronary syndromes the PLATO trial August 30, 2009 at 08.00 CET PLATO background In NSTE-ACS and STEMI, current guidelines recommend 12 months aspirin and
Reflection paper on assessment of cardiovascular safety profile of medicinal products
 25 February 2016 EMA/CHMP/50549/2015 Committee for Medicinal Products for Human Use (CHMP) Reflection paper on assessment of cardiovascular safety profile of medicinal products Draft agreed by Cardiovascular
25 February 2016 EMA/CHMP/50549/2015 Committee for Medicinal Products for Human Use (CHMP) Reflection paper on assessment of cardiovascular safety profile of medicinal products Draft agreed by Cardiovascular
(ClinicalTrials.gov ID: NCT ) Title: The Italian Elderly ACS Study Author: Stefano Savonitto. Date: 29 August 2011 Meeting: ESC congress, Paris
 Title: The Italian Elderly ACS Study Author: Stefano Savonitto. Date: 29 August 2011 Meeting: ESC congress, Paris") Early aggressive versus initially conservative strategy in elderly patients with non-st- elevation acute coronary syndrome: the Italian randomised trial (ClinicalTrials.gov ID: NCT00510185) Stefano Savonitto,
Early aggressive versus initially conservative strategy in elderly patients with non-st- elevation acute coronary syndrome: the Italian randomised trial (ClinicalTrials.gov ID: NCT00510185) Stefano Savonitto,
GSK Medicine: Study Number: Title: Rationale: Phase: Study Period: Study Design: Centres: Indication: Treatment:
 The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
UPDATES FROM THE 2018 ANTIPLATELET GUIDELINES
 UPDATES FROM THE 2018 ANTIPLATELET GUIDELINES Claudia Bucci BScPhm, PharmD Clinical Coordinator, Cardiovascular Diseases Sunnybrook Health Sciences Centre 21st Annual Contemporary Therapeutic Issues in
UPDATES FROM THE 2018 ANTIPLATELET GUIDELINES Claudia Bucci BScPhm, PharmD Clinical Coordinator, Cardiovascular Diseases Sunnybrook Health Sciences Centre 21st Annual Contemporary Therapeutic Issues in
Research & Development. J H Pacynko and J Illingworth. Research, pharmacy and R&D staff
 Department Title of SOP Research & Development Safety reporting SOP SOP reference no: R&D GCP SOP 07 Authors: Current version number and date: J H Pacynko and J Illingworth Version 9, 31.01.18 Next review
Department Title of SOP Research & Development Safety reporting SOP SOP reference no: R&D GCP SOP 07 Authors: Current version number and date: J H Pacynko and J Illingworth Version 9, 31.01.18 Next review
The Clinical Unmet need in the patient with Diabetes and ACS
 The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
DEMOGRAPHICS PHYSICAL ATTRIBUTES VITAL SIGNS. Protocol: ABC-123 SCREENING. Subject ID. Subject Initials. Visit Date: / / [ YYYY/MM/DD]
![DEMOGRAPHICS PHYSICAL ATTRIBUTES VITAL SIGNS. Protocol: ABC-123 SCREENING. Subject ID. Subject Initials. Visit Date: / / [ YYYY/MM/DD]](/thumbs/78/78699510.jpg "DEMOGRAPHICS PHYSICAL ATTRIBUTES VITAL SIGNS. Protocol: ABC-123 SCREENING. Subject ID. Subject Initials. Visit Date: / / [ YYYY/MM/DD]") SCREENING Visit Date: DEMOGRAPHICS / / [YYYY/MM/DD] Consent Signed Date and time / / [YYYY/MM/DD] : Has written assent been obtained? If no, why not? YES NO Gender: Male Female Birthdate: Permission given
SCREENING Visit Date: DEMOGRAPHICS / / [YYYY/MM/DD] Consent Signed Date and time / / [YYYY/MM/DD] : Has written assent been obtained? If no, why not? YES NO Gender: Male Female Birthdate: Permission given
Rikshospitalet, University of Oslo
 Rikshospitalet, University of Oslo Preventing heart failure by preventing coronary artery disease progression European Society of Cardiology Dyslipidemia 29.08.2010 Objectives The trends in cardiovascular
Rikshospitalet, University of Oslo Preventing heart failure by preventing coronary artery disease progression European Society of Cardiology Dyslipidemia 29.08.2010 Objectives The trends in cardiovascular
PAR-1 Antagonist: What Do Clinical Trials Teach Us?
 Prevention of Atherothrombotic Events: What s the New Evidence? PAR-1 Antagonist: What Do Clinical Trials Teach Us? David A. Morrow, MD, MPH Director, Levine Cardiac Intensive Care Unit Senior Investigator,
Prevention of Atherothrombotic Events: What s the New Evidence? PAR-1 Antagonist: What Do Clinical Trials Teach Us? David A. Morrow, MD, MPH Director, Levine Cardiac Intensive Care Unit Senior Investigator,
Clinical and Economic Value of Rivaroxaban in Coronary Artery Disease
 CHRISTOPHER B. GRANGER, MD Professor of Medicine Division of Cardiology, Department of Medicine; Director, Cardiac Care Unit Duke University Medical Center, Durham, NC Clinical and Economic Value of Rivaroxaban
CHRISTOPHER B. GRANGER, MD Professor of Medicine Division of Cardiology, Department of Medicine; Director, Cardiac Care Unit Duke University Medical Center, Durham, NC Clinical and Economic Value of Rivaroxaban
CANVAS Program Independent commentary
 CANVAS Program Independent commentary Cliff Bailey Aston University, Birmingham, UK 2017 Disclosures and disclaimers Clifford J Bailey CJB has attended advisory boards, undertaken ad hoc consultancy, received
CANVAS Program Independent commentary Cliff Bailey Aston University, Birmingham, UK 2017 Disclosures and disclaimers Clifford J Bailey CJB has attended advisory boards, undertaken ad hoc consultancy, received
Chemistry Reference Ranges and Critical Values
 Alanine Aminotransferase (ALT, SGPT) 3-9 years 9-18 years 1-9 years 9-18 years 10-25 U/L 10-35 U/L 10-30 U/L 10-25 U/L 10-30 U/L 10-35 U/L 10-25 U/L 10-35 U/L 10-25 U/L 10-20 U/L 10-35 U/L Albumin 0-6
Alanine Aminotransferase (ALT, SGPT) 3-9 years 9-18 years 1-9 years 9-18 years 10-25 U/L 10-35 U/L 10-30 U/L 10-25 U/L 10-30 U/L 10-35 U/L 10-25 U/L 10-35 U/L 10-25 U/L 10-20 U/L 10-35 U/L Albumin 0-6
Chemistry Reference Ranges and Critical Values
 Alanine Aminotransferase (ALT, SGPT) 3-9 years 9-18 years 1-9 years 9-18 years 10-30 U/L 10-30 U/L 10-20 U/L Albumin 0-6 days 6 days - 37 months 37 months - 7 years 7-20 years 2.6-3.6 g/dl 3.4-4.2 g/dl
Alanine Aminotransferase (ALT, SGPT) 3-9 years 9-18 years 1-9 years 9-18 years 10-30 U/L 10-30 U/L 10-20 U/L Albumin 0-6 days 6 days - 37 months 37 months - 7 years 7-20 years 2.6-3.6 g/dl 3.4-4.2 g/dl
egfr > 50 (n = 13,916)
") Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
GENERAL INFORMATION. Adverse Event (AE) Definition (ICH GUIDELINES E6 FOR GCP 1.2):
 Definition (ICH GUIDELINES E6 FOR GCP 1.2):") Make copies of the blank SAE report form as needed. Retain originals with confirmation of all information faxed to DMID Pharmacovigilance Group Clinical Research Operations and Management Support (CROMS
Make copies of the blank SAE report form as needed. Retain originals with confirmation of all information faxed to DMID Pharmacovigilance Group Clinical Research Operations and Management Support (CROMS
Effect of the PCSK9 Inhibitor Evolocumab on Cardiovascular Outcomes
 Effect of the PCSK9 Inhibitor Evolocumab on Cardiovascular Outcomes MS Sabatine, RP Giugliano, SD Wiviott, FJ Raal, CM Ballantyne, R Somaratne, J Legg, SM Wasserman, R Scott, MJ Koren, and EA Stein for
Effect of the PCSK9 Inhibitor Evolocumab on Cardiovascular Outcomes MS Sabatine, RP Giugliano, SD Wiviott, FJ Raal, CM Ballantyne, R Somaratne, J Legg, SM Wasserman, R Scott, MJ Koren, and EA Stein for
Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre
 Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre Objectives To learn what s new in stroke care 2010-11 1) Acute stroke management Carotid artery stenting versus surgery for symptomatic
Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre Objectives To learn what s new in stroke care 2010-11 1) Acute stroke management Carotid artery stenting versus surgery for symptomatic
ISCHEMIC HEART DISEASE
 ESC CONGRESS HIGHLIGHTS ISCHEMIC HEART DISEASE Francesco Cosentino (Stockholm, S) Declaration of Interest Advisory Board/Speaker: AstraZeneca, Roche, Boehringer-Ingelheim, Bristol-Myers Squibb, Merck,
ESC CONGRESS HIGHLIGHTS ISCHEMIC HEART DISEASE Francesco Cosentino (Stockholm, S) Declaration of Interest Advisory Board/Speaker: AstraZeneca, Roche, Boehringer-Ingelheim, Bristol-Myers Squibb, Merck,
Clopidogrel vs New Antiplatelet Therapy (Prasugrel) Adnan Kastrati, MD Deutsches Herzzentrum, Technische Universität München, Germany
 Adnan Kastrati, MD Deutsches Herzzentrum, Technische Universität München, Germany") Clopidogrel vs New Antiplatelet Therapy () Adnan Kastrati, MD Deutsches Herzzentrum, Technische Universität München, Germany Seoul, April 3, 21 Dual Antiplatelet Therapy for Stenting MACE, % 12 1 8 6 In
Clopidogrel vs New Antiplatelet Therapy () Adnan Kastrati, MD Deutsches Herzzentrum, Technische Universität München, Germany Seoul, April 3, 21 Dual Antiplatelet Therapy for Stenting MACE, % 12 1 8 6 In
PROlonging Dual antiplatelet treatment after Grading stent-induced Intimal hyperplasia study
 ESC, Hotline III, Paris, August, 30, 2011 PROlonging Dual antiplatelet treatment after Grading stent-induced Intimal hyperplasia study M. Valgimigli, MD, PhD University of Ferrara, ITALY On behalf of the
ESC, Hotline III, Paris, August, 30, 2011 PROlonging Dual antiplatelet treatment after Grading stent-induced Intimal hyperplasia study M. Valgimigli, MD, PhD University of Ferrara, ITALY On behalf of the
Surveying the Landscape of Oral Antiplatelet Therapy in Acute Coronary Syndrome Management
 Surveying the Landscape of Oral Antiplatelet Therapy in Acute Coronary Syndrome Management Jeffrey S Berger, MD, MS Assistant Professor of Medicine and Surgery Director of Cardiovascular Thrombosis Disclosures
Surveying the Landscape of Oral Antiplatelet Therapy in Acute Coronary Syndrome Management Jeffrey S Berger, MD, MS Assistant Professor of Medicine and Surgery Director of Cardiovascular Thrombosis Disclosures
Optimal lenght of DAPT in different clinical scenarios
 Optimal lenght of DAPT in different clinical scenarios After PCI with DES in the light of recent and ongoing studies Dr Grégoire Rangé / CH Chartres / France DAPT duration depend on the evolution of risk
Optimal lenght of DAPT in different clinical scenarios After PCI with DES in the light of recent and ongoing studies Dr Grégoire Rangé / CH Chartres / France DAPT duration depend on the evolution of risk
CVD risk assessment using risk scores in primary and secondary prevention
 CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
HYPERTENSION: UPDATE 2018
 HYPERTENSION: UPDATE 2018 From the Cardiologist point of view Richard C Padgett, MD I have no disclosures HYPERTENSION ALWAYS THE ELEPHANT IN THE EXAM ROOM BUT SOMETIMES IT CHARGES HTN IN US ~78 million
HYPERTENSION: UPDATE 2018 From the Cardiologist point of view Richard C Padgett, MD I have no disclosures HYPERTENSION ALWAYS THE ELEPHANT IN THE EXAM ROOM BUT SOMETIMES IT CHARGES HTN IN US ~78 million
Coronary Artery Stenosis. Insight from MAIN-COMPARE Study
 PCI for Unprotected Left Main Coronary Artery Stenosis Insight from MAIN-COMPARE Study Young-Hak Kim, MD, PhD Cardiac Center, University of Ulsan College of Medicine, Asan Medical Center Current Practice
PCI for Unprotected Left Main Coronary Artery Stenosis Insight from MAIN-COMPARE Study Young-Hak Kim, MD, PhD Cardiac Center, University of Ulsan College of Medicine, Asan Medical Center Current Practice
Diabetes Mellitus: A Cardiovascular Disease
 Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
The top 5 trials in the last year: Ischemic Heart Disease
 The top 5 trials in the last year: Ischemic Heart Disease Malcolm R. Bell, MBBS, FRACP, FACC Vice Chair, Department of Cardiovascular Medicine Mayo Clinic, Rochester MN, USA 2018 MFMER 3718476-1 Conflicts
The top 5 trials in the last year: Ischemic Heart Disease Malcolm R. Bell, MBBS, FRACP, FACC Vice Chair, Department of Cardiovascular Medicine Mayo Clinic, Rochester MN, USA 2018 MFMER 3718476-1 Conflicts
Role of Clopidogrel in Acute Coronary Syndromes. Hossam Kandil,, MD. Professor of Cardiology Cairo University
 Role of Clopidogrel in Acute Coronary Syndromes Hossam Kandil,, MD Professor of Cardiology Cairo University ACS Treatment Strategies Reperfusion/Revascularization Therapy Thrombolysis PCI (with/ without
Role of Clopidogrel in Acute Coronary Syndromes Hossam Kandil,, MD Professor of Cardiology Cairo University ACS Treatment Strategies Reperfusion/Revascularization Therapy Thrombolysis PCI (with/ without
Sponsor Novartis. Generic Drug Name Pasireotide. Therapeutic Area of Trial Cushing s disease. Protocol Number CSOM230B2208E1
 Sponsor Novartis Generic Drug Name Pasireotide Therapeutic Area of Trial Cushing s disease Protocol Number CSOM230B2208E1 Title Extension to a multicenter, open-label study to assess the safety and efficacy
Sponsor Novartis Generic Drug Name Pasireotide Therapeutic Area of Trial Cushing s disease Protocol Number CSOM230B2208E1 Title Extension to a multicenter, open-label study to assess the safety and efficacy
Faculty/Presenter Disclosure
 Faculty/Presenter Disclosure Faculty: Andre Lamy Relationships with commercial interests: Grants/Research Support: None Speakers Bureau/Honoraria: None Consulting Fees: None Other: None CORONARY: The Coronary
Faculty/Presenter Disclosure Faculty: Andre Lamy Relationships with commercial interests: Grants/Research Support: None Speakers Bureau/Honoraria: None Consulting Fees: None Other: None CORONARY: The Coronary
Dual Antiplatelet duration in ACS: too long or too short?
 Dual Antiplatelet duration in ACS: too long or too short? Leonardo Bolognese, MD, FESC, FACC Cardiovascular Department, Arezzo, Italy Paradigm Shift the ideal duration of DAPT: a moving target Early (stent-related)
Dual Antiplatelet duration in ACS: too long or too short? Leonardo Bolognese, MD, FESC, FACC Cardiovascular Department, Arezzo, Italy Paradigm Shift the ideal duration of DAPT: a moving target Early (stent-related)