Objectives DISCLOSURES NONE. Hypertensive Urgency & Hypertensive Emergency. Define Hypertensive Urgency vs Emergency
|
|
|
- Caren Wade
- 6 years ago
- Views:
Transcription
1 Hypertensive Urgency & Hypertensive Emergency 15 th Annual Rocky mountain Hospital Medicine Symposium November 6-7 th, 2017 Renaissance Hotel Denver DISCLOSURES NONE Objectives Define Hypertensive Urgency vs Emergency Describe pathophysiology, epidemiology & prognosis Understand the fundamentals of evaluation and management Understand the fundamentals of the treatments and goals
2 Case: H.L. 57 y/o AAM with history DM and HTN. One week of headache, squinting and mild dyspnea on exertion. PMH: DM All: NDKA Meds: FH: DM SH: 20 pk history HTN Lisinopril Metformin HTN CAD CVA Postman Case: H.L. Physical Exam Vitals: T 97.9F HR 93 RR 20 BP 230/120 SpO2 94% on RA Gen: Awake and alert, mild distress HEENT: PERRL, EOMI, anicteric, MMM, normal posterior oropharynx, neck supple Resp: Clear to auscultation bilaterally, no w/r/r CV: Normal S1/S2, no m/g/r; Abd: Protuberant, soft, non-tender, BS+ Ext: warm to the touch, no cyanosis, 1+ pretibial edema Skin: no jaundice, lesions or rashes noted Neuro: alert and oriented, no meningismus, CN II-XII grossly intact Case: H.L. Initial Work-Up Total protein 4.5 Albumin 3.9 Total bili 1.4 AST 77 ALT 49 AlkP 55 Lactate 2.1
3 Case: H.L. Diagnosis Headache SOB HTN, severe Anemia Scr Transaminitis AST 77 ALT Unifying diagnosis? Definition Hypertensive Urgency Elevated Blood Pressure WITHOUT evidence of acute end-organ damage Hypertensive Emergency Elevated Blood Pressure WITH evidence acute end-organ damage Malignant Hypertension has been removed from guidelines Case: H.L.Diagnosis Hypertensive Emergency Scr Headache SOB Anemia NAFLD AST 77 ALT (0.8) (AST 65) (ALT 41) (14.4)
4 Hypertensive Emergency Epidemiology Systemic hypertension is common 65 million Americans 1% of all patients with HTN will experience Hypertensive emergency at any point in their lives Elderly African-American Men > female Urgency vs Emergency Urgency Emergency BP SBP >180 mmhg or DBP > 110mmHG SBP >180 mmhg or DBP > 110mmHG EndOrgan Damage ABSENT PRESENT Time to Target BP hours Immediately Level of Care Inpatient ICU Medications Oral IV, titratable Marik PE, Rivera R.. Curr Opin Crit Care. 2011;17(6): Padilla Ramos A, Varon J. Curr Hypertens Rep. 2014;16(7):450. Hypertensive Emergency Prognosis Mortality 5 year survival 32% prior to 1977 The Studying the Treatment of Acute hypertensive (STAT) 25-institution U.S patients with severe acute hypertension Hospital mortality was 6.9% with an aggregate 90-day mortality of 11% and a 90-day readmission rate of 37%. Median Survival of 144 months 5 year 74% Katz JN et al. Am Heart J. 2009;158(4): e1. Deal. Et. al Arch Dis Child 1992
 Acute heart failure (14%) Encephalopathy (8.")
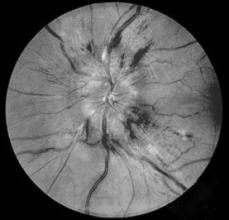
5 Clinical Presentation Shortness of breath (29%) Chest pain (26%) Headache (23%) Acute Encephalopathy (20%) Focal Deficit (11%) Katz JN et al. Am Heart J. 2009;158(4): e1. Van den Born BJ, Honnebier UP, Koopmans RP, et al.hypertension 2005; 45: Patterns of End-Organ Damage Reversible renal dysfunction (22%) Acute heart failure (14%) Encephalopathy (8.3%) Acute MI/ACS (11%) Intracerebral hemorrhage (11%) Subarachnoid hemorrhage (12%) Retinal hemorrhage and/or papilledema (0.9%)* Katz JN et al. Am Heart J. 2009;158(4): e1. *Funduscopic exam documented 13% Van den Born BJ, Honnebier UP, Koopmans RP, et al.hypertension 2005; 45: Pathophysiology HTN Emergency Circulating Vasoconstrictors End Organ Ischemia Loss of Autoregulatory function Abrupt SVR Abrupt BP Endothelial Damage Pressure Naturesis Vasoconstriction Renin Angiotensin System Volume Depletion
6 Pathophysiology Autoregulation BP = PVR x CO (SV x HR) Increase in BP Increase in BP Vasoconstriction Ineffective Vasoconstriction Normal flow of circulating blood Shear Stress (endothelial damage) Wallach R, Karp RB, Reves JG, et al.. Am J Cardiol 1980; 46: Vascular Autoregulation Flynn JT. Severe hypertension. Ped Nephrol 2009; Pathophysiology Rate of increase in BP more important the absolute number Organ dysfunction is uncommon with DBP <130 Children and pregnant women are notable exceptions




 Plts")

7 Case: H.L. Given IVP labetalol 20mg 190/105 Medically adherent to outpatient treatment plan. Drinks 2 beers after work, 6-8 during Bronco games. No recreational drugs but Doc, marijuana isn t illegal anymore Old and new Initial Evaluation CBC w/smear LDH (>220U/l) Plts (<150x10 9 /l) CMP Cardiac enzymes UA Proteinuria Microscopic hematuria Urine Pregnancy Test Initial Evaluation




8 Initial Testing Initial Evaluation -Neuro Acute Encephalopathy Headache SAH Nausea/Vomitting - ICP Focal findings rare (11) Initial Evaluation Cardiac Check BP in both arms



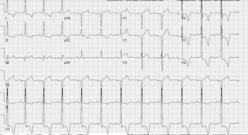
9 Initial Evaluation Renal Worsening Scr, hematuria, proteinuria or RBC cast formation Case: H.L. MICU Right radial arterial line placed Foley placed LVH, Repolarization Pulmonary Edema No acute abnormality Vascular Autoregulation
 T1 normal T2 occipital hyperintensity Visual disturbances Seizures B.E. Hamilton, and G.")
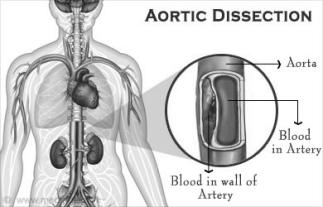
10 Hypertensive Encephalopathy Rapid increase in BP (DBP >140) Uncontrolled Cerebral Blood Flow Cerebral vasospam, punctate hemorrhage, ischemia, increased vascular permeability Cerebral Edema Reversible Posterior Leukoencephalopathy Syndrome formerly Posterior Reversible Encephalopathy Syndrome (PRES) T1 normal T2 occipital hyperintensity Visual disturbances Seizures B.E. Hamilton, and G.M. Nesbit AJNR Am J Neuroradio2008;29: Associated Conditions Pulmonary Edema Systolic Diastolic Acute Myocardial Infarction Hypertensive Encephalopathy Acute Aortic Dissection Acute Renal failure Microangiopathic Hemolytic Anemia (MAHA) Preeclampsia, eclampsia Cocaine use/overdose Acute postoperative HTN Ischemic Stroke (SBP > ) Hemorrhagic Stroke (SBP > )

11 Treatment Goals Preserve organ function Reduce BP in controlled fashion Minimize complications Management HTN Urgency Inpt vs outpatient Telemetry Unit Intermediate if comorbid HTN Emergency ICU Cardiopulmonary Monitoring Pulse Ox Telemetry BP monitoring Cycling BP cuff Cardiopulmonary Monitoring Pulse Ox Telemetry BP monitoring Arterial Line Case: H.L. No evidence of RPLS 190/105 (MAP 133) Continued headache What are the treatment goals? Which medication should be initiated?
12 Treatment Goals Dysfunctional autoregulation of BP prevents normal response to hypotension MAP lowered by 10 20% in first hour MAP lowered to 25% of initial MAP in 1 st 8-12 hours Then decrease by another 25% in the next 8-12 hrs Final 50% by 48 hrs Treatment Goals 2 Main Classes of Medications Vasodilators Adrenergic inhibitors Case: H.L. Repeat BP 190/105 Nicardipine infusion started 1L NS Goal 173/90 (MAP 117) in 24 hours Neuro checks Q2hrs
13 Vasodilators MEDICATION DOSAGE ONSET OF ACTION Nitroprusside mcg/kg/min DURATION OF ACTION ADVERSE REACTION Immediate 1-2 min Thiocyanate toxicity Nitroglycerine mcg/min 1-5 min 3-5 min Flushing, h/a, methgb Nicardipine 5-15 mg/hr 5-10 min 1-4 hr HR, flushing Fenoldopam mcg/kg/min 5 min `10-15 min Flushing, h/a, HR Clevidipine 1-2 mg/hr Immediate 5-15 min HR, Afib, h/a, nausea Hydralazine mg 5-15 min 3-8 hrs Flushing, HR Enalapril mg IM mg IV min 6 hrs BP, SCr, hyperkalemia Adrenergic Inhibitors MEDICATION DOSAGE ONSET OF ACTION Labetalol 20-80mg IV x 10min, 2 mg/min gtt DURATION OF ACTION ADVERSE REACTION 5-10 min 3-6 hrs CV block, BP Esmolol 200 mcg/kg/min 1-2 min min BP Phetolamine 5-15 mg 1-2 min 3-10 min HR, flushing, h/a Condition Consideration Medication Pulmonary Edema -- Systolic Pulmonary Edema -- Diastolic Hypertensive Encephalopathy Acute Aortic Dissection Ischemic Stroke (SBP > ) Hemorrhagic Stroke (SBP > ) Concomitant CHF Nicardipine or clevidipine + nitro + loop diuretic Goal MAP < 25% or DBP <100mmHg 1 st hour Decrease vessel wall sheer stress (dp/dt) Hemorrhagic conversion with SBP CPP=MAP-ICP Esmolol or labetalol or metoprolol or verapamil + nitro + loop diuretic Nicardipine, labetolol, fenoldopam, clevidipine Avoid nitroprusside Labetalol or nicardipine + beta-blocker or nitroprusside + beta-blocker Nicardipine, labetolol, fenoldopam, clevidipine Labetalol, nicardipine or esmolol Cocaine use/overdose Avoid beta-blocker Nitroprusside Pregnancy Fetal effects of medications Hydralazine, labetalol, **nitroprusside (4hrs)

14 Case: H.L. Over the course of 2 days, BP titrated to 150/80 Scr 1.0 Lisinopril restarted HCTZ PO Discharge to PCP follow-up in 1 week Thank you
Hypertensives Emergency and Urgency
 Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of
Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of
Hypertensive Crises. Controlling high blood pressure prevents disease. Recognition and Management of Acute Hypertensive Emergencies
 Controlling high blood pressure prevents disease Recognition and Management of Acute Hypertensive Emergencies David idweiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Functional Genomics
Controlling high blood pressure prevents disease Recognition and Management of Acute Hypertensive Emergencies David idweiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Functional Genomics
Hypertensive Urgency and Emergency. Definitions. Emergency or Urgency?
 Hypertensive Urgency and Emergency Joel Handler MD Kaiser Permanente Care Management Institute/ SCal Region Hypertension Lead Definitions Hypertensive Emergency: -Severe elevation in BP with evidence of
Hypertensive Urgency and Emergency Joel Handler MD Kaiser Permanente Care Management Institute/ SCal Region Hypertension Lead Definitions Hypertensive Emergency: -Severe elevation in BP with evidence of
Agenda. Management of Accelerated Hypertension (Updated in 2017) Salwa Roshdy Prof. of Cardiology Assiut University CardioEgypt 23/2/2017 2/27/2017
 Salwa Roshdy Prof. of Cardiology Assiut University CardioEgypt 23/2/2017 2/27/2017") Management of Accelerated Hypertension (Updated in 2017) By Salwa Roshdy Prof. of Cardiology Assiut University CardioEgypt 23/2/2017 Agenda Definition of Accelerated HTN Pathophysiology & Etiology Prognosis
Management of Accelerated Hypertension (Updated in 2017) By Salwa Roshdy Prof. of Cardiology Assiut University CardioEgypt 23/2/2017 Agenda Definition of Accelerated HTN Pathophysiology & Etiology Prognosis
Franklin Delano Roosevelt. Learning Objectives. Severe hypertension is relatively common. Current State of Hypertensive Crisis Management
 3 3:45 pm Presenter Disclosure Information What Every Primary Care Clinician Needs to Know about Hypertension Crises SPEAKER Karol E. Watson, MD, PhD, FACC The following relationships exist related to
3 3:45 pm Presenter Disclosure Information What Every Primary Care Clinician Needs to Know about Hypertension Crises SPEAKER Karol E. Watson, MD, PhD, FACC The following relationships exist related to
How to Handle Hypertension Crisis
 How to Handle Hypertension Crisis Learning Objectives 1. Define hypertensive crises: Hypertension urgency and hypertension emergency 2. Outline the pathophysiology of hypertensive urgencies and emergencies
How to Handle Hypertension Crisis Learning Objectives 1. Define hypertensive crises: Hypertension urgency and hypertension emergency 2. Outline the pathophysiology of hypertensive urgencies and emergencies
HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP
 HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP What is normal blood pressure? Prehypertension 130-139/80-90 Compared with normal BP Double the risk for developing hypertension. Lifestyle
HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP What is normal blood pressure? Prehypertension 130-139/80-90 Compared with normal BP Double the risk for developing hypertension. Lifestyle
Categories of HTN. Overview of Hypertension. Types of Hypertension
 Categories of HTN Overview of Hypertension Normal SBP 100 Quick review of the Basics: What is
Categories of HTN Overview of Hypertension Normal SBP 100 Quick review of the Basics: What is
Children with Hypertension in ED
 Children with Hypertension in ED By Prof. Sanaa AK Helmy Professor of Anesthesia, Intensive Care and Pain Management, Faculty of Medicine, Cairo University Vice-chairman of the Egyptian Society of Emergency
Children with Hypertension in ED By Prof. Sanaa AK Helmy Professor of Anesthesia, Intensive Care and Pain Management, Faculty of Medicine, Cairo University Vice-chairman of the Egyptian Society of Emergency
LEARNING OBJECTIVES 2/20/2017
 HYPERTENSION IN PREGNANCY: PREVENTING SEVERE MATERNAL MORBIDITY & MORTALITY THROUGH THE IMPLEMENTATION OF EVIDENCED BASED PROTOCOLS Laura Senn, RN, PhD, CNS Sutter Medical Center, Sacramento LEARNING OBJECTIVES
HYPERTENSION IN PREGNANCY: PREVENTING SEVERE MATERNAL MORBIDITY & MORTALITY THROUGH THE IMPLEMENTATION OF EVIDENCED BASED PROTOCOLS Laura Senn, RN, PhD, CNS Sutter Medical Center, Sacramento LEARNING OBJECTIVES
Current State of Hypertensive Crisis Management. Learning Objectives. Severe hypertension is relatively common. Hypertension Emergencies in context
 2:30 3:15 pm Presenter Disclosure Information What Every Primary Care Clinician Needs to Know about Hypertension Crises SPEAKER Karol E. Watson, MD, PhD, FACC The following relationships exist related
2:30 3:15 pm Presenter Disclosure Information What Every Primary Care Clinician Needs to Know about Hypertension Crises SPEAKER Karol E. Watson, MD, PhD, FACC The following relationships exist related
Blood Pressure Management in Acute Ischemic Stroke
 Blood Pressure Management in Acute Ischemic Stroke Kimberly Clark, PharmD, BCCCP Clinical Pharmacy Specialist Critical Care, Greenville Health System Adjunct Assistant Professor, South Carolina College
Blood Pressure Management in Acute Ischemic Stroke Kimberly Clark, PharmD, BCCCP Clinical Pharmacy Specialist Critical Care, Greenville Health System Adjunct Assistant Professor, South Carolina College
Presentation of hypertensive emergency
 Presentation of hypertensive emergency Definitions surrounding hypertensive emergency Hypertension: elevated blood pressure (BP), usually defined as BP >140/90; pathological both in isolation and in association
Presentation of hypertensive emergency Definitions surrounding hypertensive emergency Hypertension: elevated blood pressure (BP), usually defined as BP >140/90; pathological both in isolation and in association
Current State of Hypertensive Crisis Management. Learning Objectives. Severe hypertension is relatively common. Hypertension Emergencies in context
 3:30 4:30 pm Presenter Disclosure Information What Every Primary Care Clinician Needs to Know About Hypertension Crises SPEAKER Karol E. Watson, MD, PhD, FACC The following relationships exist related
3:30 4:30 pm Presenter Disclosure Information What Every Primary Care Clinician Needs to Know About Hypertension Crises SPEAKER Karol E. Watson, MD, PhD, FACC The following relationships exist related
What is hypertension?
 HYPERTENSION What is hypertension? Abnormally elevated arterial blood pressure that is usually indicated by an adult systolic blood pressure of 140 mm Hg or greater or a diastolic blood pressure of 90
HYPERTENSION What is hypertension? Abnormally elevated arterial blood pressure that is usually indicated by an adult systolic blood pressure of 140 mm Hg or greater or a diastolic blood pressure of 90
HYPERTENSION. Background for understanding the Hypertension literature. Case presentation. Approach to Treatment. Jeffrey J. Kaufhold, MD Nephrology
 HYPERTENSION Background for understanding the Hypertension literature. Case presentation Approach to Treatment Jeffrey J. Kaufhold, MD Nephrology 2009 HYPERTENSION SUMMARY Background for understanding
HYPERTENSION Background for understanding the Hypertension literature. Case presentation Approach to Treatment Jeffrey J. Kaufhold, MD Nephrology 2009 HYPERTENSION SUMMARY Background for understanding
ACUTE HEART FAILURE. Julie Gorchynski MD, MSc, FACEP, FAAEM. Department of Emergency Medicine Emergency Residency Program UTHSC, San Antonio TCEP 2014
 ACUTE HEART FAILURE Julie Gorchynski MD, MSc, FACEP, FAAEM Department of Emergency Medicine Emergency Residency Program UTHSC, San Antonio TCEP 2014 No disclosures Objectives Overview Cases Current Therapy
ACUTE HEART FAILURE Julie Gorchynski MD, MSc, FACEP, FAAEM Department of Emergency Medicine Emergency Residency Program UTHSC, San Antonio TCEP 2014 No disclosures Objectives Overview Cases Current Therapy
MANAGEMENT OF HYPERTENSION IN PREGNANCY, THE ALGORHITHM
 MANAGEMENT OF HYPERTENSION IN PREGNANCY, THE ALGORHITHM Are Particular Anti-hypertensives More Effective or Harmful Than Others in Hypertension in Pregnancy? Existing data is inadequate Methyldopa and
MANAGEMENT OF HYPERTENSION IN PREGNANCY, THE ALGORHITHM Are Particular Anti-hypertensives More Effective or Harmful Than Others in Hypertension in Pregnancy? Existing data is inadequate Methyldopa and
Severe hypertension is relatively common. Franklin Delano Roosevelt. Current State of Hypertensive Crisis Management
 Franklin Delano Roosevelt Severe hypertension is relatively common There are ~100,000 ER visits each year for hypertension ~15,000 of those visits are for severely high BP Messerli N Engl J Med 1995;3321038.
Franklin Delano Roosevelt Severe hypertension is relatively common There are ~100,000 ER visits each year for hypertension ~15,000 of those visits are for severely high BP Messerli N Engl J Med 1995;3321038.
Incidental Findings; Management of patients presenting with high BP. Phil Swales
 Incidental Findings; Management of patients presenting with high BP Phil Swales Consultant Physician Acute & General Medicine University Hospitals of Leicester NHS Trust Objectives The approach to an incidental
Incidental Findings; Management of patients presenting with high BP Phil Swales Consultant Physician Acute & General Medicine University Hospitals of Leicester NHS Trust Objectives The approach to an incidental
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs
 Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Hypertension in the ED - management tips that will bring down your own BP
 27th Annual Update in Emergency Medicine Hypertension in the ED - management tips that will bring down your own BP February 24, 2014 Clare Atzema, MD MSc FRCPC Staff Physician, Sunnybrook Health Sciences
27th Annual Update in Emergency Medicine Hypertension in the ED - management tips that will bring down your own BP February 24, 2014 Clare Atzema, MD MSc FRCPC Staff Physician, Sunnybrook Health Sciences
Cesarean section for breech presentation. Jonathan H. Waters, M.D.
 Cesarean section for breech presentation Jonathan H. Waters, M.D. 1 26 y.o. G1P0 presented to triage in labor at 38 weeks. Patient was a known breech with a failed version 5 days before presentation. PMH
Cesarean section for breech presentation Jonathan H. Waters, M.D. 1 26 y.o. G1P0 presented to triage in labor at 38 weeks. Patient was a known breech with a failed version 5 days before presentation. PMH
TREATMENT OF HYPERTENSION
 TREATMENT OF HYPERTENSION Aim of treatment BP Goals Main items of treatment Lifestyle modification When to start drug Rx Pharmacological therapy 1. Relief of symptoms 2. Prevention of complications and
TREATMENT OF HYPERTENSION Aim of treatment BP Goals Main items of treatment Lifestyle modification When to start drug Rx Pharmacological therapy 1. Relief of symptoms 2. Prevention of complications and
Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept
 Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept Continents 1- introduction 2- classification/definition 3- classification/etiology 4-etiology in both categories 5- complications
Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept Continents 1- introduction 2- classification/definition 3- classification/etiology 4-etiology in both categories 5- complications
Policy REVISED: 6/30/2016 3:30 PM. Applies To: ObGyn Responsible Department: ObGyn Revised: June 30, 2016
 Title: Antihypertensive Treatment for Severe Hypertension During Pregnancy Applies To: ObGyn Responsible Department: ObGyn Revised: June 30, 2016 Policy POLICY STATEMENT: Pregnant or postpartum patients
Title: Antihypertensive Treatment for Severe Hypertension During Pregnancy Applies To: ObGyn Responsible Department: ObGyn Revised: June 30, 2016 Policy POLICY STATEMENT: Pregnant or postpartum patients
Based on 2014 SOGC Guidelines
 Based on 2014 SOGC Guidelines 22nd Edition 2015 1 ICH + gestational hypertension by far the biggest cause of direct maternal deaths New stats coming in 2013 OCR 22nd Edition 2015 2 Diastolic 90 mmhg is
Based on 2014 SOGC Guidelines 22nd Edition 2015 1 ICH + gestational hypertension by far the biggest cause of direct maternal deaths New stats coming in 2013 OCR 22nd Edition 2015 2 Diastolic 90 mmhg is
Objectives: HYPERTENSIVE EMERGENCIES:
 HYPERTENSIVE EMERGENCIES: Acute Care Evaluation and Management Charles V. Pollack, Jr., MD Christopher J. Rees, MD Department of Emergency Medicine, Pennsylvania Hospital University of Pennsylvania, Philadelphia,
HYPERTENSIVE EMERGENCIES: Acute Care Evaluation and Management Charles V. Pollack, Jr., MD Christopher J. Rees, MD Department of Emergency Medicine, Pennsylvania Hospital University of Pennsylvania, Philadelphia,
Managing Hypertension in the Perioperative Arena
 Managing Hypertension in the Perioperative Arena Optimizing Perioperative Management Strategies for Hypertension in the Cardiac Surgical Patient Objectives: Treatment of hypertensive emergencies. ALBERT
Managing Hypertension in the Perioperative Arena Optimizing Perioperative Management Strategies for Hypertension in the Cardiac Surgical Patient Objectives: Treatment of hypertensive emergencies. ALBERT
Mercy San Juan Medical Center. Preeclampsia and Other Hypertensive Disorders of Pregnancy
 SUBJECT: Preeclampsia and Other Hypertensive Disorders of Pregnancy DEPARTMENTS: FBC, Emergency Department PURPOSE: To outline the nursing management of inpatients who have preeclampsia or other hypertensive
SUBJECT: Preeclampsia and Other Hypertensive Disorders of Pregnancy DEPARTMENTS: FBC, Emergency Department PURPOSE: To outline the nursing management of inpatients who have preeclampsia or other hypertensive
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Management of Hypertension. Ahmed El Hawary MD Suez Canal University
 Management of Hypertension Ahmed El Hawary MD Suez Canal University Minimal vs. Optimal Care Resources more than science affect type of care and level of management. what is possible (minimal care) and
Management of Hypertension Ahmed El Hawary MD Suez Canal University Minimal vs. Optimal Care Resources more than science affect type of care and level of management. what is possible (minimal care) and
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE
 DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
CHAPTER 12 HYPERTENSION IN SPECIAL GROUPS HYPERTENSION IN PREGNANCY
 CHAPTER 12 HYPERTENSION IN SPECIAL GROUPS HYPERTENSION IN PREGNANCY v Mild preeclampsia is managed by close observation of the mother and fetus preferably in hospital. If the diastolic blood pressure remains
CHAPTER 12 HYPERTENSION IN SPECIAL GROUPS HYPERTENSION IN PREGNANCY v Mild preeclampsia is managed by close observation of the mother and fetus preferably in hospital. If the diastolic blood pressure remains
Postpartum hypertension, preeclampsia and eclampsia. Arun Jeyabalan, MD MS University of Pittsburgh
 Postpartum hypertension, preeclampsia and eclampsia Arun Jeyabalan, MD MS University of Pittsburgh Confusing concept Preeclampsia only occurs in pregnancy placenta is required Delivery cures preeclampsia
Postpartum hypertension, preeclampsia and eclampsia Arun Jeyabalan, MD MS University of Pittsburgh Confusing concept Preeclampsia only occurs in pregnancy placenta is required Delivery cures preeclampsia
Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight
 Treatment of a Stroke patient: A look at how to care for the Stroke patient in the aeromedical setting Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight Objectives 1. Discuss the assessment
Treatment of a Stroke patient: A look at how to care for the Stroke patient in the aeromedical setting Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight Objectives 1. Discuss the assessment
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS. ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS
 FOR THROMBOLYSIS") NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
7/7/ CHD/MI LVH and LV dysfunction Dysrrhythmias Stroke PVD Renal insufficiency and failure Retinopathy. Normal <120 Prehypertension
 Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Protocol for IV rtpa Treatment of Acute Ischemic Stroke
 Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Preeclampsia: What s old is new again. Gene Chang, MD Maternal Fetal Medicine
 Preeclampsia: What s old is new again Gene Chang, MD Maternal Fetal Medicine Objectives Define Preeclampsia Review current guidelines Role of proteinuria Timing of delivery Seizure prevention Severe Hypertension
Preeclampsia: What s old is new again Gene Chang, MD Maternal Fetal Medicine Objectives Define Preeclampsia Review current guidelines Role of proteinuria Timing of delivery Seizure prevention Severe Hypertension
Stroke in Pregnancy. Stroke in Pregnancy 6/23/13
 G5#$#Preven*ng#Maternal#Morbidity#and#Mortality#Via# Expanded#Scope#of#Nursing#Prac*ce#As#First#Responder# in#hypertensive#crisis#of#preeclampsia# The$presenter$reports$no$relevant,$influencing$financial$rela5onships.$
G5#$#Preven*ng#Maternal#Morbidity#and#Mortality#Via# Expanded#Scope#of#Nursing#Prac*ce#As#First#Responder# in#hypertensive#crisis#of#preeclampsia# The$presenter$reports$no$relevant,$influencing$financial$rela5onships.$
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
A CASE OF HYPERTENSION AND ACUTE RENAL FAILURE OBJECTIVES
 A CASE OF HYPERTENSION AND ACUTE RENAL FAILURE Maricel Pilapil-Pureza WLA Nephrology OBJECTIVES After the presentation, the attendee will be able to: 1. Discuss when to suspect for secondary causes of
A CASE OF HYPERTENSION AND ACUTE RENAL FAILURE Maricel Pilapil-Pureza WLA Nephrology OBJECTIVES After the presentation, the attendee will be able to: 1. Discuss when to suspect for secondary causes of
Approach to patient with hypertension. Dr. Amitesh Aggarwal
 Approach to patient with hypertension Dr. Amitesh Aggarwal Definition A systolic blood pressure ( SBP) >139 mmhg and/or A diastolic (DBP) >89 mmhg. Based on the average of two or more properly measured,
Approach to patient with hypertension Dr. Amitesh Aggarwal Definition A systolic blood pressure ( SBP) >139 mmhg and/or A diastolic (DBP) >89 mmhg. Based on the average of two or more properly measured,
Blood Pressure Management in Acute Stroke. Bradley Molyneaux, M.D., Ph.D. Departments of Neurology & Critical Care Medicine University of Pittsburgh
 Blood Pressure Management in Acute Stroke Bradley Molyneaux, M.D., Ph.D. Departments of Neurology & Critical Care Medicine University of Pittsburgh 80 yo M w/ R MCA syndrome NIHSS 14 A balancing act Cerebral
Blood Pressure Management in Acute Stroke Bradley Molyneaux, M.D., Ph.D. Departments of Neurology & Critical Care Medicine University of Pittsburgh 80 yo M w/ R MCA syndrome NIHSS 14 A balancing act Cerebral
Practical Aspects of Hypertension: Simple Strategies to Help You and Your Patients Meet Guideline Blood Pressure Targets
 Practical Aspects of Hypertension: Simple Strategies to Help You and Your Patients Meet Guideline Blood Pressure Targets Robert J. Herman University of Calgary herman@ucalgary.ca Conflict of Interest Disclosure
Practical Aspects of Hypertension: Simple Strategies to Help You and Your Patients Meet Guideline Blood Pressure Targets Robert J. Herman University of Calgary herman@ucalgary.ca Conflict of Interest Disclosure
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure. No relevant financial relationships. Blood Pressure and Risk
 MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Chapter 10. Learning Objectives. Learning Objectives 9/11/2012. Congestive Heart Failure
 Chapter 10 Congestive Heart Failure Learning Objectives Explain concept of polypharmacy in treatment of congestive heart failure Explain function of diuretics Learning Objectives Discuss drugs used for
Chapter 10 Congestive Heart Failure Learning Objectives Explain concept of polypharmacy in treatment of congestive heart failure Explain function of diuretics Learning Objectives Discuss drugs used for
Antihypertensive Agents Part-2. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
Primary Stroke Center Acute Stroke Transfer Guidelines When to Consider a Transfer:
 When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
Managing Hypertension in 2016
 Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
HST 071. IN SUMMARY PREGNANCY INDUCED HYPERTENSION Classification of Hypertensive Disorders of Pregnancy
 Harvard-MIT Division of Health Sciences and Technology HST.071: Human Reproductive Biology Course Director: Professor Henry Klapholz IN SUMMARY Classification of Hypertensive Disorders of Pregnancy HST
Harvard-MIT Division of Health Sciences and Technology HST.071: Human Reproductive Biology Course Director: Professor Henry Klapholz IN SUMMARY Classification of Hypertensive Disorders of Pregnancy HST
Managing HTN in the Elderly: How Low to Go
 Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
Section 3, Lecture 2
 59-291 Section 3, Lecture 2 Diuretics: -increase in Na + excretion (naturesis) Thiazide and Related diuretics -decreased PVR due to decreases muscle contraction -an economical and effective treatment -protect
59-291 Section 3, Lecture 2 Diuretics: -increase in Na + excretion (naturesis) Thiazide and Related diuretics -decreased PVR due to decreases muscle contraction -an economical and effective treatment -protect
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
M2 TEACHING UNDERSTANDING PHARMACOLOGY
 M2 TEACHING UNDERSTANDING PHARMACOLOGY USING CVS SYSTEM AS AN EXAMPLE NIGEL FONG 2 JAN 2014 TODAY S OBJECTIVE Pharmacology often seems like an endless list of mechanisms and side effects to memorize. To
M2 TEACHING UNDERSTANDING PHARMACOLOGY USING CVS SYSTEM AS AN EXAMPLE NIGEL FONG 2 JAN 2014 TODAY S OBJECTIVE Pharmacology often seems like an endless list of mechanisms and side effects to memorize. To
Special Lecture 11/08/2013. Hypertension Dr. HN Mayrovitz
 Special Lecture 11/08/2013 Hypertension Dr. HN Mayrovitz Arterial Blood Pressure (ABP) Major Factors Summarized Sympathetic Hormones Arteriole MAP ~ Q x TPR + f (V / C) SV x HR Renal SBP Hypertension =
Special Lecture 11/08/2013 Hypertension Dr. HN Mayrovitz Arterial Blood Pressure (ABP) Major Factors Summarized Sympathetic Hormones Arteriole MAP ~ Q x TPR + f (V / C) SV x HR Renal SBP Hypertension =
OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA
 OMED 17 OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA 29.5 Category 1-A CME credits anticipated ACOFP / AOA s 122 nd Annual Osteopathic Medical Conference & Exposition ACOFP - The Heart of the Matter - An Evidence
OMED 17 OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA 29.5 Category 1-A CME credits anticipated ACOFP / AOA s 122 nd Annual Osteopathic Medical Conference & Exposition ACOFP - The Heart of the Matter - An Evidence
A very short lecture.
 Medical Treatment of Type A Aortic Dissection: Tales of Turkeys, Tygon Tubing, and Evolving Paradigms The Houston Aortic Symposium April 4-6, 2008 John A. Elefteriades, MD William W.L. Glenn Professor
Medical Treatment of Type A Aortic Dissection: Tales of Turkeys, Tygon Tubing, and Evolving Paradigms The Houston Aortic Symposium April 4-6, 2008 John A. Elefteriades, MD William W.L. Glenn Professor
* * FORM REV. 02/2019 Page 1 of 4. TNKASE (tenecteplase) / ACUTE STEMI ORDERS SCHEDULED MEDICATIONS:
 / ACUTE STEMI ORDERS SCHEDULED MEDICATIONS:") 1. Is this a CMS inpatient only procedure? Yes, admit as inpatient, proceed to # 3 No, proceed to # 2 2. Do you expect that the patient s condition will require a hospital stay that will cross two midnights
1. Is this a CMS inpatient only procedure? Yes, admit as inpatient, proceed to # 3 No, proceed to # 2 2. Do you expect that the patient s condition will require a hospital stay that will cross two midnights
LXIV: DRUGS: 4. RAS BLOCKADE
 LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
Estimated 5.7 million Americans with HF. 915, 000 new HF cases annually, HF incidence approaches
 Heart Failure: Management of a Chronic Disease Jenny Bauerly RN, CHFN, APRN-BC Heart Failure (HF) Definition A complex clinical syndrome that can result from any structural or functional cardiac disorder
Heart Failure: Management of a Chronic Disease Jenny Bauerly RN, CHFN, APRN-BC Heart Failure (HF) Definition A complex clinical syndrome that can result from any structural or functional cardiac disorder
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Blood Pressure. Michelle Bertram- Nephrology- OBH
 Blood Pressure Michelle Bertram- Nephrology- OBH Hypertension- how common? 29-30% white adults 46-51% uncontrolled Diagnosis Two or more properly measured BP s after an initial screen NICE guidelines also
Blood Pressure Michelle Bertram- Nephrology- OBH Hypertension- how common? 29-30% white adults 46-51% uncontrolled Diagnosis Two or more properly measured BP s after an initial screen NICE guidelines also
The Role of the Anaesthesiologist in the Perioperative Management of Preeclampsia. RA Dyer Interlaken 2017
 The Role of the Anaesthesiologist in the Perioperative Management of Preeclampsia RA Dyer Interlaken 2017 6 In preeclampsia - Understanding of pathophysiology Assessment of disease severity Prediction
The Role of the Anaesthesiologist in the Perioperative Management of Preeclampsia RA Dyer Interlaken 2017 6 In preeclampsia - Understanding of pathophysiology Assessment of disease severity Prediction
A 45 year old African American man presents to the IMC with a chief complaint of my
 AN EVIDENCE BASED APPROACH TO HYPERTENSION AND HYPERLIPIDENIA: A CASE STUDY A 45 year old African American man presents to the IMC with a chief complaint of my pressure is high. Apparently he recently
AN EVIDENCE BASED APPROACH TO HYPERTENSION AND HYPERLIPIDENIA: A CASE STUDY A 45 year old African American man presents to the IMC with a chief complaint of my pressure is high. Apparently he recently
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Management of hypertensive emergencies in children
 Indian Journal of Emergency Pediatrics Volume 2 Number 4, Oct - Dec 2010 165 P. Ramachandran Management of hypertensive emergencies in children Hypertensive emergencies are uncommon in children. A good
Indian Journal of Emergency Pediatrics Volume 2 Number 4, Oct - Dec 2010 165 P. Ramachandran Management of hypertensive emergencies in children Hypertensive emergencies are uncommon in children. A good
How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage
 How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage Rachael Scott, Pharm.D. PGY2 Critical Care Pharmacy Resident Pharmacy Grand Rounds August 21, 2018 2018 MFMER slide-1 Patient
How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage Rachael Scott, Pharm.D. PGY2 Critical Care Pharmacy Resident Pharmacy Grand Rounds August 21, 2018 2018 MFMER slide-1 Patient
Chapter 23. Media Directory. Cardiovascular Disease (CVD) Hypertension: Classified into Three Categories
 Hypertension: Classified into Three Categories") Chapter 23 Drugs for Hypertension Slide 37 Slide 41 Media Directory Nifedipine Animation Doxazosin Animation Upper Saddle River, New Jersey 07458 All rights reserved. Cardiovascular Disease (CVD) Includes
Chapter 23 Drugs for Hypertension Slide 37 Slide 41 Media Directory Nifedipine Animation Doxazosin Animation Upper Saddle River, New Jersey 07458 All rights reserved. Cardiovascular Disease (CVD) Includes
Summary/Key Points Introduction
 Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Dr Doris M. W Kinuthia
 Dr Doris M. W Kinuthia Objectives Normal blood pressures in children Measurement of blood pressure in children Aetiology of Hypertension in children Evaluation of children with hypertension Treatment of
Dr Doris M. W Kinuthia Objectives Normal blood pressures in children Measurement of blood pressure in children Aetiology of Hypertension in children Evaluation of children with hypertension Treatment of
Beta Blockade: Protection or Panacea
 Beta Blockade: Protection or Panacea Jason Axt Jason s Recommendations Perioperative β Blockade (BB) If on BB stay on If Vascular Sx + documented ischemia - start. 2+ risk factors - start Use in isolated
Beta Blockade: Protection or Panacea Jason Axt Jason s Recommendations Perioperative β Blockade (BB) If on BB stay on If Vascular Sx + documented ischemia - start. 2+ risk factors - start Use in isolated
Clinical Controversies in Perioperative Medicine
 Update on Perioperative Medicine Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Medications & Perioperative
Update on Perioperative Medicine Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Medications & Perioperative
Critical Care Meds in the Emergency Department
 Critical Care Meds in the Emergency Department Kyle Rupp DO, MBA Medical Director Emergency Services CHI Health Good Samaritan Objectives Identify and describe use of medications used in blood pressure
Critical Care Meds in the Emergency Department Kyle Rupp DO, MBA Medical Director Emergency Services CHI Health Good Samaritan Objectives Identify and describe use of medications used in blood pressure
Approach to Management of Hypertension. Prof. Abdulkareem Al-Suwaida, MD, FRCPC, MSc
 Approach to Management of Hypertension Prof. Abdulkareem Al-Suwaida, MD, FRCPC, MSc 442-2018 Objectives of The Lecture Hypertension in KSA New definitions of hypertension Understand how to diagnose hypertension
Approach to Management of Hypertension Prof. Abdulkareem Al-Suwaida, MD, FRCPC, MSc 442-2018 Objectives of The Lecture Hypertension in KSA New definitions of hypertension Understand how to diagnose hypertension
Objectives. Upon completion of the learning activity the participant will be able to: Hypertension: The Latest Treatment Options
 Objectives Hypertension: The Latest Treatment Options Margaret A. Fitzgerald, DNP, FNP-BC, NP-C, FAANP, CSP, FAAN, DCC President, Fitzgerald Health Education Associates, Inc. North Andover, MA Family Nurse
Objectives Hypertension: The Latest Treatment Options Margaret A. Fitzgerald, DNP, FNP-BC, NP-C, FAANP, CSP, FAAN, DCC President, Fitzgerald Health Education Associates, Inc. North Andover, MA Family Nurse
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Cardiac Pathophysiology
 Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
Modern Management of Hypertension: Where Do We Draw the Line?
 Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Chapter 9. Learning Objectives. Learning Objectives 9/11/2012. Cardiac Arrhythmias. Define electrical therapy
 Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Definition of Congestive Heart Failure
 Heart Failure Definition of Congestive Heart Failure A clinical syndrome of signs & symptoms resulting from the heart s inability to supply adequate tissue perfusion. CHF Epidemiology Affects 4.7 million
Heart Failure Definition of Congestive Heart Failure A clinical syndrome of signs & symptoms resulting from the heart s inability to supply adequate tissue perfusion. CHF Epidemiology Affects 4.7 million
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for
 Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
7/4/2015. Titrating Vasoactive Drips
 Leanna R. Miller RN, MN, CCRN-CMC, PCCN-CSC, CEN, NP LRM Consulting Vasoactive medications are indicated when the SBP has a decrease of > 30mmHg from the baseline or a MAP < 60mmHg and when either condition
Leanna R. Miller RN, MN, CCRN-CMC, PCCN-CSC, CEN, NP LRM Consulting Vasoactive medications are indicated when the SBP has a decrease of > 30mmHg from the baseline or a MAP < 60mmHg and when either condition
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Heart Failure. Subjective SOB (shortness of breath) Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)
 Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)") Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
OHSU Health Care System
 Acute Stroke Practice Standard for the Emergency Department (includes ischemic stroke, TIAs, intracerebral hemorrhage, and non-subarachnoid hemorrhage), PS 01.11 Last Reviewed Date: 2/2/10 STATEMENT OF
Acute Stroke Practice Standard for the Emergency Department (includes ischemic stroke, TIAs, intracerebral hemorrhage, and non-subarachnoid hemorrhage), PS 01.11 Last Reviewed Date: 2/2/10 STATEMENT OF
Byvalson. (nebivolol, valsartan) New Product Slideshow
 New Product Slideshow") Byvalson (nebivolol, valsartan) New Product Slideshow Introduction Brand name: Byvalson Generic name: Nebivolol, valsartan Pharmacological class: Beta-blocker + angiotensin II receptor blocker (ARB) Strength
Byvalson (nebivolol, valsartan) New Product Slideshow Introduction Brand name: Byvalson Generic name: Nebivolol, valsartan Pharmacological class: Beta-blocker + angiotensin II receptor blocker (ARB) Strength
PRE-RENAL AKI: DOES IT LEAD TO ATN. Sushma Bhusal
 PRE-RENAL AKI: DOES IT LEAD TO ATN Sushma Bhusal 9.9.14 CASE PRESENTATION CC : 31 AAM presented with Fatigue, malaise and body aches x 10 days HPI: STD testing done 2 weeks prior, all results negative
PRE-RENAL AKI: DOES IT LEAD TO ATN Sushma Bhusal 9.9.14 CASE PRESENTATION CC : 31 AAM presented with Fatigue, malaise and body aches x 10 days HPI: STD testing done 2 weeks prior, all results negative
Modern Management of Hypertension
 Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
OHSU HEALTH CARE SYSTEM PRACTICE GUIDELINES
 OHSU HEALTH CARE SYSTEM NEUROSCIENCES (includes ischemic stroke, TIA, intracerebral hemorrhage and non-subarachnoid hemorrhage) Last Reviewed Date: September 2013 POLICY STATEMENT: OHSU hospitals and clinics
OHSU HEALTH CARE SYSTEM NEUROSCIENCES (includes ischemic stroke, TIA, intracerebral hemorrhage and non-subarachnoid hemorrhage) Last Reviewed Date: September 2013 POLICY STATEMENT: OHSU hospitals and clinics
Susan P. D Anna MSN, APRN BC February 14, 2019
 Is there Equal Opportunity in Heart Failure?? Susan P. D Anna MSN, APRN BC February 14, 2019 Disclosures: I have no financial disclosures. I am not an expert on this topic, but see a lot of women with
Is there Equal Opportunity in Heart Failure?? Susan P. D Anna MSN, APRN BC February 14, 2019 Disclosures: I have no financial disclosures. I am not an expert on this topic, but see a lot of women with
BLOOD PRESSURE MANAGEMENT IN THE ACUTE PHASE
 BLOOD PRESSURE MANAGEMENT IN THE ACUTE PHASE Ελένη Κορομπόκη, MD, PhD, FESO Α Νευρολογική Κλινική, ΕΚΠΑ, Αιγινήτειο Νοσοκομείο Κλινική Ερευνήτρια, Department of Stroke Medicine, Imperial College London,
BLOOD PRESSURE MANAGEMENT IN THE ACUTE PHASE Ελένη Κορομπόκη, MD, PhD, FESO Α Νευρολογική Κλινική, ΕΚΠΑ, Αιγινήτειο Νοσοκομείο Κλινική Ερευνήτρια, Department of Stroke Medicine, Imperial College London,
Preeclampsia. &Eclampsia. Hypertensive Disorders of Pregnancy. What we need to know about. Hypertensive Disorders of Pregnancy.
 Preeclampsia &Eclampsia Hypertensive Disorders of Pregnancy Barbara Koop MS, RNC-OB What we need to know about Hypertensive Disorders of Pregnancy Define clinical criteria for: Gestational hypertension,
Preeclampsia &Eclampsia Hypertensive Disorders of Pregnancy Barbara Koop MS, RNC-OB What we need to know about Hypertensive Disorders of Pregnancy Define clinical criteria for: Gestational hypertension,
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
CMQCC Preeclampsia Tool Kit: Hypertensive Disorders Across the Lifespan
 CMQCC Preeclampsia Tool Kit: Hypertensive Disorders Across the Lifespan Carol J Harvey, MS, BSN, RNC-OB, C-EFM, CS Northside Hospital Atlanta Cherokee - Forsyth New! Improving Health Care Response to Preeclampsia:
CMQCC Preeclampsia Tool Kit: Hypertensive Disorders Across the Lifespan Carol J Harvey, MS, BSN, RNC-OB, C-EFM, CS Northside Hospital Atlanta Cherokee - Forsyth New! Improving Health Care Response to Preeclampsia: