Trends in U.S. Cardiovascular Care: 2016 Report from 4 ACC National Cardiovascular Data Registries
|
|
|
- Stanley Bond
- 6 years ago
- Views:
Transcription
1 Accepted Manuscript Trends in U.S. Cardiovascular Care: 2016 Report from 4 ACC National Cardiovascular Data Registries Frederick A. Masoudi, MD, MSPH, Angelo Ponirakis, PhD, James A. de Lemos, MD, James G. Jollis, MD, Mark Kremers, MD, John C. Messenger, MD, John W.M. Moore, MD, MPH, Issam Moussa, MD, William J. Oetgen, MD, MBA, Paul D. Varosy, MD, Robert N. Vincent, MD, CM, Jessica Wei, MD, MS, Jeptha P. Curtis, MD, Matthew T. Roe, MD, MHS, John A. Spertus, MD, MPH PII: S (16) DOI: /j.jacc Reference: JAC To appear in: Journal of the American College of Cardiology Received Date: 18 July 2016 Revised Date: 8 December 2016 Accepted Date: 16 December 2016 Please cite this article as: Masoudi FA, Ponirakis A, de Lemos JA, Jollis JG, Kremers M, Messenger JC, Moore JWM, Moussa I, Oetgen WJ, Varosy PD, Vincent RN, Wei J, Curtis JP, Roe MT, Spertus JA, Trends in U.S. Cardiovascular Care: 2016 Report from 4 ACC National Cardiovascular Data Registries, Journal of the American College of Cardiology (2017), doi: /j.jacc This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
2 Trends in U.S. Cardiovascular Care: 2016 Report from 4 ACC National Cardiovascular Data Registries Brief Title: NCDR Cardiovascular Care Trends Frederick A. Masoudi, MD, MSPH*,y; Angelo Ponirakis, PhDz; James A. de Lemos, MDx; James G. Jollis, MDjj; Mark Kremers, MD{; John C. Messenger, MD*; John W. M. Moore, MD, MPH#; Issam Moussa, MDyy; William J. Oetgen, MD, MBAz; Paul D. Varosy, MDzz; Robert N. Vincent, MD, CMxx; Jessica Wei, MD, MSz; Jeptha P. Curtis, MDjjjj; Matthew T. Roe, MD, MHS{{; John A. Spertus, MD, MPH## Affiliations: *Department of Medicine, University of Colorado Anschutz Medical Campus, Aurora, Colorado; ycolorado Cardiovascular Outcomes Research Consortium, Denver, Colorado; zamerican College of Cardiology Foundation, Washington, DC; xdepartment of Medicine, University of Texas Southwestern, Dallas, Texas; jjuniversity of North Carolina, Chapel Hill, North Carolina; {Novant Health Heart and Vascular Institute, Charlotte, North Carolina; #Division of Cardiology, Department of Pediatrics, Rady Children s Hospital, University of California-San Diego, San Diego, California; yydivision of Cardiology, Department of Medicine, Rutgers Robert Wood Johnson Medical School, New Brunswick, New Jersey; zzva Eastern Colorado Health Care System, University of Colorado, and the Colorado Cardiovascular Outcomes Research Group, Denver, Colorado; xxdivision of Cardiology, Department of Pediatrics, Children s Healthcare of Atlanta, Emory University, Atlanta, Georgia; jjjjdepartment of Medicine, Yale University, New Haven, Connecticut; {{Duke Cardiovascular Research Institute, Durham, North Carolina; ##Division of Cardiovascular Diseases, Mid- America Heart Institute, Kansas City, Kansas Disclosures: Dr. Masoudi has a contract with the ACCF for his role as Chief Science Officer of the NCDR ; Dr. Ponirakis, Dr. Oetgen, and Ms. Wei are employed by the ACCF; Dr. de Lemos has received grant support from Roche Diagnostics and Abbott Diagnostics, consulting income from Roche Diagnostics, and honoraria for participation in DSMB or steering committees from Novo Nordisc, St. Jude Medical and Amgen; Dr. Kremers has equity <$20K in Boston Scientific, provides consulting for Medtronic, and is a member of the Speaker's Bureau for Boston Scientific; Dr. Messenger is an investigator in Clinical Research Studies, Philips Medical Systems and a member of the Clinical Events Committee of Novate Medical; Dr. Moore is a consultant for pfm Medical, an investigator in research protocols funded by Medtronic and St. Jude s, and on the Medical Advisory Boards for 480 BioMedical and Transmural Systems; Dr. Curtis receives salary support through a contract with the American College of Cardiology to provide data analytic services; Dr. Roe has received research funding from Eli Lilly, Sanofi- Aventis, Daiichi-Sanko, Janssen Pharmaceuticals, Ferring Pharmaceuticals, Astra Zeneca, American College of Cardiology, American Heart Association, Familial Hypercholesterolemia Foundation and consulting fees or honoraria from PriMed, Astra Zeneca, Boehringer-Ingelheim, Merck, Amgen, Myokardia, Eli Lilly, Daiichi-Sanyko, and Elsevier Publishers. All conflicts of interest are listed at Dr. Spertus is affiliated with the Saint Luke s Mid America Heart and Institute, which is the major analytic center for the PINNACLE program and receives funding from the American College of Cardiology for this role and is also on the Scientific Advisory Board of United Healthcare, provides consulting 1
3 (United Healthcare, Novartis, Amgen, Bayer which are all moderate), has copyright to the SAQ, KCCQ and PAQ (significant), grants from Gilead, Lilly, Novartis and Abbott Vascular (all significant), and has equity in Health Outcomes Sciences (Significant). All other authors have reported that they have no relationships relevant to the contents of this paper to disclose. Acknowledgments: The authors wish to thank Jim Beachy, RCIS, Christina Koutras, BSN, RN, CPHQ, Beth Pruski, MSN, RN, CPHQ, Traci Connolly, RN, MS, and Cornelia Anderson, BSN, RN, CPHQ, for assistance in compiling the data for this report. Address for correspondence: Frederick A Masoudi, MD, MSPH E 17 th Ave Room 522, Campus Box B132 Aurora, Colorado Telephone: Fax: fred.masoudi@ucdenver.edu 2
4 Abstract Cardiovascular disease (CVD) is a leading cause of death and disability in the United States. National quality programs such as the National Cardiovascular Data Registry (NCDR ) permit assessments of the quality of care and outcomes for broad populations of patients with CVD. This report provides data from 2014 from four NCDR hospital quality programs: 1) CathPCI for coronary angiography and percutaneous coronary intervention (667,424 procedures performed in 1,612 hospitals) ICD for implantable cardioverter defibrillators (158,649 procedures performed in 1,715 hospitals); 3) ACTION -GWTG for acute coronary syndromes (182,903 patients admitted to 907 hospitals); and 4) IMPACT for cardiac catheterization and intervention for pediatric and adult congenital heart disease (20,169 procedures in 76 hospitals). The report provides perspectives on the demographic and clinical characteristics of enrolled patients; characteristics of participating centers; selected measures of processes and outcomes of care. Condensed Abstract National quality programs such as the National Cardiovascular Data Registry (NCDR ) permit assessments of the quality of care and outcomes for broad populations of patients with CVD. This report provides data from 2014 from four NCDR hospital quality programs: 1) CathPCI for coronary angiography and percutaneous coronary intervention (667,424 procedures performed in 1,612 hospitals) ICD for implantable cardioverter defibrillators (158,649 procedures performed in 1,715 hospitals); 3) ACTION -GWTG for acute coronary syndromes (182,903 patients admitted to 907 hospitals); and 4) IMPACT for cardiac catheterization and intervention for pediatric and adult congenital heart disease (20,169 procedures in 76 hospitals). Keywords: percutaneous coronary intervention, acute coronary syndromes, implantable cardioverter defibrillators, congenital heart disease, quality of care Abbreviations AUC: Appropriate Use Criteria CABG: Coronary artery bypass graft surgery ICD: Implantable cardioverter defibrillator NCDR: National Cardiovascular Data Registries NCDR ACTION -GWTG : NCDR program for acute coronary syndromes NCDR CathPCI : NCDR program for coronary angiography and percutaneous coronary intervention NCDR ICD : NCDR program for implantable cardioverter defibrillators NCDR IMPACT : NCDR program for cardiac catheterization and percutaneous structural intervention for congenital heart disease NSTEMI: Non-ST-segment elevation myocardial infarction PCI: Percutaneous coronary intervention STEMI: ST-segment elevation myocardial infarction 3
5 Background The mission of the American College of Cardiology s (ACC s) National Cardiovascular Data Registries (NCDR ) is to improve the quality of cardiovascular care by measuring adherence to performance metrics and establishing the foundation for new quality assessment measures, providing direct feedback to participating sites together to improve performance; implementing quality initiatives; and supporting research that improves patient care and outcomes. NCDR data provide a US national perspective on the care and outcomes of highimpact cardiovascular conditions and procedures that are not available elsewhere. The first NCDR program, CathPCI, was launched in 1998 and has collected detailed clinical information on more than 17.5 million coronary angiography and percutaneous coronary intervention procedures performed in the United States since that time (1). The NCDR has subsequently expanded to include ten programs across the spectrum of cardiovascular disease. Of these, eight are hospital-based, including: Diagnostic Catheterization and Percutaneous Coronary Intervention (CathPCI), Implantable Cardioverter Defibrillator (ICD), Acute Coronary Treatment and Intervention Outcomes Network (ACTION) Get With The Guidelines (GWTG), Improving Pediatric and Adult Congenital Treatment (IMPACT), Left Atrial Appendage Occlusion (LAAO), Peripheral Vascular Intervention (PVI), Atrial Fibrillation (AFib) Ablation, and The Society of Thoracic Surgeons/American College of Cardiology Transcatheter Valve Therapy (STS/ACC TVT) Registry (2). The remaining two are outpatient programs for the ambulatory care setting including Practice Innovation and Clinical Excellence (PINNACLE) and the Diabetes Collaborative Registry (DCR) (3). NCDR programs have also been initiated internationally, facilitating quality improvement in health systems outside of the United States. 4
6 This report provides a description and overview of the patient populations, participating centers, and patterns of care from four NCDR hospital quality programs (CathPCI, ICD, ACTION-GWTG, and IMPACT) for which comprehensive data from 2014 are available (Central Illustration), similar to a prior report summarizing 2011 data (4). As PVI replaced Carotid Artery Revascularization and Endarterectomy (CARE) in 2014, PVI data will be presented in a future report. Data from recently initiated programs (Atrial Fibrillation Ablation and Left Atrial Appendage Occlusion) will be presented in future reports as data become available; those from the outpatient programs (PINNACLE and the Diabetes Collaborative Registry) will be presented separately. STS/ACC TVT Registry data are presented in a separate annual report (5). This report intended to provide a national perspective on the quality of cardiovascular care for common procedures and inform clinical practice and health policy. While NCDR programs include international participants, the summary data from this report are limited to those submitted by US participants. NCDR Program Methods Program datasets are developed using an established methodology and employ explicit data definitions. Committees of experts from multiple disciplines and professional societies, reflecting both clinical quality improvement and research priorities, identify key data elements and define metrics to assess the quality of care. Proposed data elements and definitions undergo review and iterative refinement, which includes a ranking process and public comment period. Upon completion of the final dataset and data dictionary, a data collection form is designed and tested. Datasets are regularly revised to reflect current clinical practice and on-going scientific relevance. 5
7 Data are collected by participants for entry into central repositories maintained by the ACC. The NCDR applies a comprehensive data quality program to enhance data validity and reliability (6). This program focuses on data completeness, consistency, and accuracy. All data submitted by participating hospitals is subjected to a Data Quality Report process, which applies criteria for data field completeness and consistency (ie assessments for implausible outlier values). Transactional steps during the construction of data sets for analytic purposes further ensure data consistency. Finally, audits are conducted on an annual basis to assess data validity and reliability. Sites are selected either at random or as the result of outlier analysis that identifies patterns of data that may be indicative of inconsistent data entry. This audit focuses primarily on data elements that are required to calculate performance metrics or that are used in risk-adjustment outcomes models. All program metrics are based on ACC guidelines. Many are adopted directly from ACC/AHA Performance Measures documents. Others are recommended by the individual registry Steeering Commitees and are developed by the NCDR Measures and Risk Adjustment Subcommittee. Measures developed by NCDR are subject ot a 30-day open comment period and are reviewed and approved by the NCDR Science and Quality Oversight Committee. A subset of metrics are considered Performance Measures, which are measures meeting the criteria for inclusion in accountability programs (e.g. public reporting) (7). Others are considered Quality Metrics, which are those measures that are not currently considered suitable for accountability but that are useful for quality improvement purposes. When available, NCDR also reports ACC Appropriate Use Criteria (AUC), which provides feedback on the extent to which proccedures are performed according to evidence-based clinical parameters. APPLICATIONS OF NCDR DATA 6
8 Since 1998, NCDR programs have provided a mechanism for centers to identify opportunities for quality improvement based upon evidence-based performance feedback that includes national benchmarks. Using these data, hospitals can identify gaps in care as well as understand the range of performance that can be achieved in other participating centers in the US and with an increasing international presence. NCDR hospital programs are now employed in more than 2,000 US healthcare facilities, and thus in many cases, the benchmarks reported by the programs can be considered accurate reflections of care provided across the US. Key performance metrics are provided to participating hospitals on a quarterly basis accompanied by an explanation of the benchmarking methodology used to facilitate comparison of one institution s outcomes to national results. The NCDR also participates in state- and nation-wide quality reporting initiatives. Program metrics are used by a number of payers as well several US states as part of efforts to assess and ensure quality within their jurisdictions (8,9). The ACC has initiated a voluntary hospital-level public reporting program (10,11) that includes Performance Measures from the CathPCI and ICD programs available on the ACC CardioSmart patient website (12). The measures used in this voluntary program are only those that satisfy the reliability and validity criteria for the purposes of accountability. To this point, all measures employed in the NCDR public reporting program have been endorsed by the National Quality Forum. US News also includes NCDR participation in its Best Hospital Rankings. Specifically, hospitals that participate in the NCDR public reporting program receive credit in the Best Hospitals in Cardiology & Heart Surgery rankings (13). Participation in the IMPACT registry results in credit in the Children s Cardiology and Heart Surgery specialty rankings (14). Thus, the evidence- 7
9 based metrics developed by NCDR have become established as national standards for cardiovascular care. The NCDR also supports generalizable health services, outcomes, and policy research. Each contributes to the broader understanding of cardiovascular care in the US and illustrates the power of the large community of NCDR participants collectively to improve cardiovascular health. The NCDR has been employed to elucidate myriad aspects of care and outcomes in contemporary practice across the registries. Recent examples include procedural success and complications after pulmonary artery stenting from IMPACT (15); observational comparative effectiveness of CRT-D vs. ICD in patients with chronic kidney disease from ICD (16); or outcomes of interventions for chronic total occlusions from CathPCI (17). Risk models from the NCDR have been developed for death (18), bleeding (19), and acute kidney injury (20), allowing clinicians to target more intensive risk reduction strategies to the highest risk patients (21). The NCDR programs have generated insights into the appropriateness of cardiovascular procedures (22); analysis of trends from the CathPCI program suggest that the benchmarking and feedback of procedural appropriateness has resulted in meaningful improvements in patient selection for procedures (23). The NCDR also contributes to the science of quality of care, including the assessment of the validity of the program outcome metrics (24) or the potential impact of new practice guidelines on clinical care (25,26). NCDR Programs NCDR CathPCI Diagnostic Catheterization and Percutaneous Coronary Intervention (CathPCI) is sponsored by ACCF in conjunction with the Society for Cardiovascular Angiography and Interventions. The CathPCI was designed to create a national surveillance system to assess the 8
10 characteristics, treatments, and outcomes of patients who undergo procedures in cardiac catheterization (Cath) laboratories including coronary angiography and percutaneous coronary intervention (PCI). As of the end of 2014, CathPCI included data on over 17,600,000 records since its inception in The program does not mandate data collection for all angiography procedures but does require inclusion of all PCIs. In 2014, CathPCI was used in more than 90% of PCI-capable hospitals in the US. Currently, 70% of sites submit data for all diagnostic catheterization and PCI procedures; the remaining 30% of sites provide all PCI procedures and the associated diagnostic catheterizations but do not include all diagnostic only procedures (1). Eligible patients are adults (18 years and older) undergoing an eligible procedure. For diagnostic catheterization, eligible procedures include catheterization with the passage of a catheter into the aortic root for pressure measurements and/or angiography, and can include left ventricular (LV) pressure measurements, LV angiography, coronary angiography, and coronary artery bypass angiography. For PCI, eligible procedures include those where PCI was attempted and/or performed, defined so by the introduction of a guidewire for the purpose of achieving mechanical revascularization. In 2014, 667,424 patients who underwent PCI were included in the program, with a mean age of 64.6 years (SD = ); most (86.5%) were White (Table 1). Prior coronary events, including prior MI (30.4%), prior PCI (41.2%), and prior CABG (17.8%) were relatively common (Table 2). Approximately one third of procedures were for elective indications. The number of participating hospitals was 1,612, the majority of which (87%) were private or community hospitals and in urban or suburban locations (81%, Table 3). The geographic distribution of participating centers is shown in Figure 1; CathPCI is used 11 sites outside of the US and US territories. 9
11 The median time to primary PCI for patients with STEMI was stable between (Figure 2). Among patients who were not transferred for the procedure, the median time to primary PCI in 2014 was 59 minutes (10 th, 50 th, 90 th percentiles of 70, 60, 48 minutes, respectively), below the guideline-recommended threshold of 90 minutes; the corresponding proportion of patients receiving PCI within this threshold was 93.5% (Figure 3). Among patients transferred for treatment, the median time to primary PCI was 105 minutes (10 th, 50 th, 90 th percentiles of 161, 108, 80 minutes, respectively); 32.3% of transferred patients were treated within 90 minutes of presentation (Figure 3). In 2014, 93.5% of patients undergoing PCI received aspirin, P2Y12 inhibitors, and statins provided they met eligibility for treatment at hospital discharge, compared with 89.1% in 2011 (Figure 4). The CathPCI program also collects information regarding patient selection and technical aspects of procedures. Patient selection in CathPCI is assessed with the application of appropriate use criteria (AUC, Table 4) (27). In 2104, nearly all of the 563,448 PCIs performed for acute coronary syndromes that could be classified were appropriate indications (98.3%). Among patients without ACS, 53.5% of PCIs were performed for appropriate indications; 32.6% were classified as may be appropriate and 13.9% as rarely appropriate. In 2014, 25.2% of cases/procedures were performed by means of a radial approach, compared with 10.9% in 2011 (Figure 5). A total of 2.4% of PCI cases in 2014 involved the use of mechanical ventricular support during the hospitalization, most of which (1.7%) was provided by intra-aortic balloon pump (Figure 6). Mechanical support with an IABP was initiated prior to the PCI in 36.7% of cases (Figure 7); other forms of support (e.g. Impella, percutaneous left ventricular assist device) were more commonly initiated before PCI (77.6%). 10
12 Procedure-related complications are also reported in CathPCI (Figure 8). Between 2011 and 2014, unadjusted rates of acute kidney injury were 2.3% and 2.6% respectively; rates of blood transfusion were 1.9% and 1.4%, repectively. In 2014, post-procedural stroke occurred in 0.2% of procedures; emergency CABG surgery was performed after 0.2% of procedures; and vascular access site injury occurred in 1.3% of procedures. NCDR ICD In January 2005, the Centers for Medicaid and Medicare Services (CMS) expanded coverage of implantable cardioverter defibrillators (ICDs) based on the results of three major published randomized controlled trials (RCTs) (28). Concurrently, CMS mandated a national database for Medicare patients receiving ICDs for primary prevention. In response, the NCDR developed the Implantable Cardioverter Defibrillator (ICD) Program to assess the characteristics, care, and outcomes of patients undergoing ICD placement at participating centers; to determine if the findings from RCTs of ICDs are applicable to the general population; and to provide additional insights on outcomes after ICD implantation in subpopulations of particular interest (29). As of the end of 2014, ICD included data on over 1,300,000 records since its inception in The program is used in all hospitals implanting devices if they provide primary prevention therapy to patients insured by Medicare given the coverage with evidence decision. Eligible patients include all adults and pediatric patients undergoing ICD implantation, including device and lead replacements. CMS mandates that all Medicare beneficiaries receiving an ICD for primary prevention are reported in the program; 90% of all sites also choose to submit data on other patient populations, including those receiving a device for secondary prevention or those insured by other payers. 11
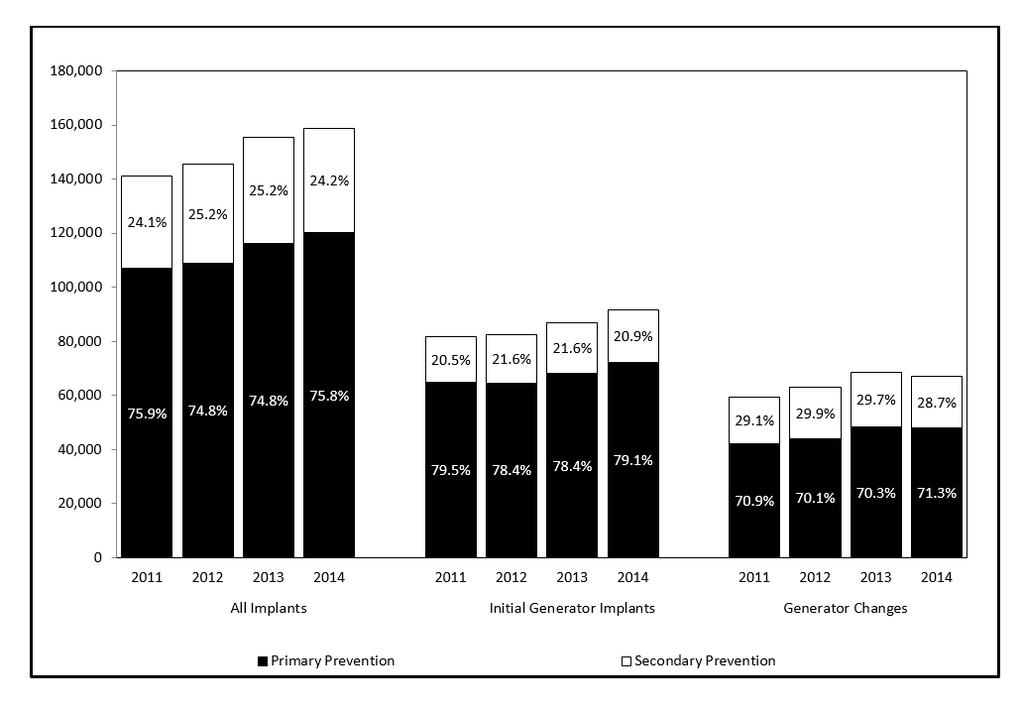
13 In 2014, 158,649 patient records were included in the program, the majority of which (81,406 or 51%) were patients with Medicare insurance coverage receiving a device for a primary prevention indication (Table 5). The mean age of the population was 67,1 years (SD = ), and 17.2% were at least 80 years old; the majority (82.9%) were white. Most patients (83.4%) had heart failure documented prior to device implantation, and evidence of coronary disease was common (48.2% with prior myocardial infarction; 32.9% with prior PCI, and 28.8% with prior CABG, Table 6). The number of participating hospitals was 1,715, the majority of which (90%) were private or community hospitals and in urban or suburban locations (79%, Table 7). The geographic distribution of participating centers is shown in Figure 9; NCDR ICD is used 3 sites outside of the US and US territories. Although the majority of patients included in NCDR ICD received a device for primary prevention, the program also included data on 38,421 patients receiving a device for a secondary prevention indication in The number of devices registered in NCDR ICD increased annually since 2011, when slightly more than 141,000 implantations were included, primarily attributable to an increase in initial generator implants (Figure 10). The proportions of secondary prevention devices in 2014 was 24.2%. In 2014, 25.0% of devices implanted for any indication were single lead, 32.0% dual lead, and 42.7% were biventricular devices (Figure 11); since 2011, there was an increase in the proportion of single lead devices (from 19.4%) and a decrease in the dual lead devices (from 37.0%) and in biventricular devices (43.5%). Patient selection in NCDR ICD is assessed with the application of ACC/AHA guideline criteria. The proportion of devices meeting class I, IIa, and IIb indications was 88.3% in 2014 compared with 86.2% in 2011 (Figure 12). The prescription of evidence based medications for patients with prior myocardial infarction and left ventricular 12
14 systolic dysfunction in 2014 ranged from 83.9% for ACE-inhibitor or angiotensin receptor blocker for LVSD (compared with 81.2% in 2012); to 94.1% for beta blocker for LVSD (compared with 92.4% in 2012, Figure 13). Performance with respect to a composite medication measure for all these therapies among eligible patients, however, was only 80.3% in 2014, identifying an important target for improvement. Rates of in-hospital death in 2014 were 1.3%, compared with 1.4% in 2011 (Figure 14). NCDR ACTION GWTG Acute Coronary Treatment and Intervention Outcomes Network (ACTION) Get With The Guidelines (GWTG) is sponsored jointly by the ACCF and the American Heart Association in partnership with the Society of Cardiovascular Patient Care and The American College of Emergency Physicians (30). ACTION -GWTG assesses the characteristics, treatments, and outcomes of patients with acute myocardial infarction (AMI) [both ST segment elevation myocardial infarction (STEMI) and non-st segment elevation myocardial infarction (NSTEMI)]. As of the end of 2014, ACTION -GWTG included data on over 800,000 records since its inception in Eligible patients are those older than 18 years of age hospitalized with a diagnosis of AMI who have acute ischemic symptoms within 24 hours of first hospital presentation. Patients admitted for other conditions who subsequently develop AMI during hospitalization are not included. In 2014, 182,903 patients were included in the ACTION -GWTG program, of which 71,368 (39.0%) had STEMI, and 111,535 (61.0%) had NSTEMI. The mean age was 64.6 years (SD = ), 34.4% were women, and the majority (84.3%) were white (Table 8). Diabetes mellitus was present in 34.8%, a history of heart failure in 12.8%, and stroke in 7.7%, Table 9). Approximately one quarter (24.8%) had a history of prior myocardial infarction, 25.7% had a 13
15 prior PCI, and 13.2% had previously undergone bypass surgery. The number of participating hospitals in 2014 was 907, which is estimated to represent 27% of acute care hospitals providing care for AMI. The majority of hospitals (89%) were private or community hospitals and in urban or suburban locations (82%, Table 10). The geographic distribution of participating centers is shown in Figure 15; ACTION -GWTG is used 9 sites outside of the US and US territories. Almost all patients with STEMI (95.8%) undergo coronary angiography during hospitalization; the proportion of patients with NSTEMI undergoing angiography was 81.9% (Figure 16). The ACTION -GWTG reports a wide range of evidence-based quality measures and metrics pertinent to the care of acute myocardial infarction. With respect to the Performance Measures, institutional level performance is reported in Table 11. While the performance of centers in the 90 th percentile is uniformly excellent, rates of performance in the 10 th percentile identifies important opportunities for improvement, such as the evaluation of left ventricular ejection fraction during hospitalization (performed 88% of the time in centers in the 10 th percentile), prescription of an ACE inhibitor or ARB at discharge among patients with myocardial infarction and left ventricular systolic dysfunction (71.6% in centers in the 10 th percentile), and referral to cardiac rehabilitation (11.1%). Temporal trends in reperfusion times and the proportions of patients receiving reperfusion within 90 minutes between 2011 and 2014 are shown in Figures 17 and 18, respectively. Not all ACTION -GWTG participants have PCI capability and in some cases treat patients with fibrinolysis; the proportions of patients receiving fibrinolytic therapy with a door-to-needle time within the 30 minutes recommended by guidelines ranged from 46.8% in 2011 to 54.0% in 2014 (Figure 18). ACTION -GWTG also reports a number of metrics that combine various process metrics to provide more comprehensive assessments of the care provided for patients with acute 14
16 myocardial infarction (Table 12, see Appendix for definitions of composites). To further guide quality improvement, the program provides centers with data on performance on a wider range of quality metrics (Table 13). The program also permits insights into the safety of care. Errors in dosing of anticoagulant and antiplatelet agents, particularly unfractionated heparin, are relatively common and represent an important target for protocols (Figure 19). The ACTION - GWTG program also collects data on in-hospital outcomes, including death, re-infarction, heart failure, cardiogenic shock, stroke, and bleeding events (Figure 20). With the exception of stroke, these outcomes occur more commonly in patients with STEMI compared with those presenting with NSTEMI. Temporal trends in the risks of the more common in-hospital events of death, heart failure, and major bleeding between are shown in Figure 21 for STEMI and Figure 22 for NSTEMI. NCDR IMPACT IMproving Pediatric and Adult Congenital Treatment (IMPACT) is sponsored by the ACCF. IMPACT was designed to assess the prevalence, demographics, management and outcomes of pediatric patients (<18 years of age) and adult patients with congenital heart disease (CHD) (age 18years of age) who undergo diagnostic catheterization-based interventions. As of the end of 2014, IMPACT included data on over 54,600 records since its inception in Its data support the development of evidence-based guidelines for CHD treatment that will improve outcomes for patients of all ages. In 2014, IMPACT collected data on procedures for 20,169 patients. Almost half (46.4%) were female, and 86% were younger than 18 years old; 71.2% were white (Table 14). Serious coexisting conditions were generally uncommon; 19.6% of patients had single ventricle physiology (Table 15). IMPACT was used in 76 hospitals, which is estimated to represent 57% 15
17 of hospitals that provide interventional services for patients with congential heart disease. Half of these hospitals (51%) were community centers; almost all (93%) were urban or suburban (Table 16). The geographic distribution of participating centers in 2014 is shown in Figure 23; IMPACT was used in 9 sites outside of the US and US territories. Success rates for selected procedures are shown in Figure 24. Closures of atrial septal defects and patent ductus arteriosus exceeded 94%; rates of success for pulmonary valvuloplasty (84.3%), aortic coarctation stenting (87.4%); and aortic coarctation balloon angioplasty (55.1%) were lower. With respect to adverse procedural events, device embolization during atrial septal defect (1.2%) and patent ductus arteriosus (1.1%) occurred rarely; increases in aortic regurgitation after balloon valvuloplasty were 10.6% (Figure 25). Trends in major adverse events or death during the episode of care following diagnostic catheterization for congential heart disease as a function of age are shown in Figure 26; adverse events were more common in younger age groups. Because these data include all events during hospitalization, these events are not necessarily directly attributable to the procedure itself. Conclusions The mission of the NCDR is to improve the quality of cardiovascular patient care by providing information, knowledge and tools; implementing quality initiatives; and supporting research that improves patient care and outcomes. As this report demonstrates, NCDR programs provide unique opportunities to advance the understanding of the clinical characteristics, care, and outcomes of patients with cardiovascular disease in the US, and more recently, internationally. These programs collect data for a broad range of patients undergoing cardiovascular procedures or in the outpatient setting in geographically and structurally diverse care settings characterizing the clinical characteristics of patients with high impact 16
18 cardiovascular conditions and undergoing common cardiovascular procedures; the extent of use of evidence-based cardiovascular therapies; and patient outcomes. The data in this report provide unique perspectives into the care and outcomes of cardiovascular care in the US that are not available elsewhere. NCDR programs, through the contributions of the participating hospitals and practices, generate the benchmarks for local, regional, and national quality improvement and support health services research that informs practice and health policy. This report illustrates the strength of national quality programs using standardized data to advance the effectiveness and safety of patients with cardiovascular disease nationwide. 17
19 References 1. Moussa I, Hermann A, Messenger JC et al. The NCDR CathPCI Registry: a US national perspective on care and outcomes for percutaneous coronary intervention. Heart 2013;99: Masoudi FA, Ponirakis A, Yeh RW, et al. Cardiovascular Care Facts: A Report From the National Cardiovascular Data Registry: J Am Coll Cardiol. 2013;62(21): Holmes DR, Jr., Nishimura RA, Grover FL, et al. Annual Outcomes With Transcatheter Valve Therapy: From the STS/ACC TVT Registry. J Am Coll Cardiol. 2015;66(25): Messenger JC, Ho KK, Young CH et al. The National Cardiovascular Data Registry (NCDR) Data Quality Brief: The NCDR Data Quality Program in J Am Coll Cardiol 2012;60: Bonow RO et al. ACC/AHA classification of care metrics: performance measures and quality metrics: a report of the American College of Cardiology/American Heart Association Task Force on Performance Measures. J Am Coll Cardiol 2008;52: Dehmer GJ, Jennings J, Madden RA, et al. The National Cardiovascular Data Registry Voluntary Public Reporting Program: An Interim Report From the NCDR Public Reporting Advisory Group. J Am Coll Cardiol. 2016;67(2): Dehmer et al Public reporting of clinical quality data: an update for cardiovascular specialists JACC 2014;63:
20 /methodology-change-will-credit-hospitals-for-transparency-reduce-reputation Lewis MJ, Kennedy KF, Ginns J, et al. Procedural Success and Adverse Events in Pulmonary Artery Stenting: Insights From the NCDR. J Am Coll Cardiol. 2016;67(11): Friedman DJ, Singh JP, Curtis JP, et al. Comparative Effectiveness of CRT-D Versus Defibrillator Alone in HF Patients With Moderate-to-Severe Chronic Kidney Disease. J Am Coll Cardiol. 2015;66(23): Brilakis ES, Banerjee S, Karmpaliotis D, et al. Procedural Outcomes of Chronic Total Occlusion Percutaneous Coronary Intervention: A Report From the NCDR (National Cardiovascular Data Registry). J Am Coll Cardiol Intv. 2015;8(2): Peterson ED, Dai D, DeLong ER, et al. Contemporary Mortality Risk Prediction for Percutaneous Coronary Intervention: Results From 588,398 Procedures in the National Cardiovascular Data Registry. J Am Coll Cardiol. 2010;55(18): Rao SV, McCoy LA, Spertus JA, et al. An Updated Bleeding Model to Predict the Risk of Post-Procedure Bleeding Among Patients Undergoing Percutaneous Coronary Intervention: A Report Using an Expanded Bleeding Definition From the National Cardiovascular Data Registry CathPCI Registry. J Am Coll Cardiol Intv. 2013;6(9): Thomas TT, Uptal DP, Tara IC, et al. Validated Contemporary Risk Model of Acute Kidney Injury in Patients Undergoing Percutaneous Coronary Interventions: Insights From the National Cardiovascular Data Registry Cath-PCI Registry. JAHA. 2014; 3(6). 19
21 21. Strauss CE, Porten BR, Chavez, IJ, Garberich, RF, Chambers, JW, Baran, KW, Poulose, AK, Henry, TD. Real-Time Decision Support to Guide Percutaneous Coronary Intervention Bleeding Avoidance Strategies Effectively Changes Practice Patterns. Circ Cardiovasc Qual Outcomes. 2014;7: Chan PS, Patel MR, Klein LW, et al. Appropriateness of Percutaneous Coronary Intervention. JAMA. 2011;306(1): Desai NR, Bradley SM, Parzynski CS, et al. Appropriate Use Criteria for Coronary Revascularization and Trends in Utilization, Patient Selection, and Appropriateness of Percutaneous Coronary Intervention. JAMA. 2015;314(19): Sherwood MW, Brennan J, Ho KK, et al. The Impact of Extreme-Risk Cases on Hospitals Risk-Adjusted Percutaneous Coronary Intervention Mortality Ratings. J Am Coll Cardiol Intv. 2015;8(1_PA): Borden WB, Maddox TM, Tang F, et al. Impact of the 2014 Expert Panel Recommendations for Management of High Blood Pressure on Contemporary Cardiovascular Practice: Insights From the NCDR PINNACLE Registry. J Am Coll Cardiol. 2014;64(21): Shah RU, de Lemos JA, Wang TY, et al. Post-Hospital Outcomes of Patients With Acute Myocardial Infarction With Cardiogenic Shock: Findings From the NCDR. J Am Coll Cardiol. 2016;67(7): Patel MR, Dehmer GJ, Hirshfeld JW, Smith PK, Spertus JA. ACCF/SCAI/STS/AATS/AHA/ASNC/HFSA/SCCT 2012 Appropriate Use Criteria for Coronary Revascularization Focused Update: A Report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, Society for Cardiovascular Angiography and Interventions, 20
22 Society of Thoracic Surgeons, American Association for Thoracic Surgery, American Heart Association, American Society of Nuclear Cardiology, and the Society of Cardiovascular Computed Tomography. J Am Coll Cardiol. 2012;59(9): McClellan MB, Tunis SR. Medicare coverage of ICDs. New Engl J Med 2005;352: Hammill SC, Stevenson LW, Kadish AH et al. Review of the registry's first year, data collected, and future plans. Heart Rhythm 2007;4: Peterson ED, Roe MT, Chen AY et al. The NCDR ACTION Registry-GWTG: transforming contemporary acute myocardial infarction clinical care. Heart 2010;96:
23 Figure Legends Central Illustration: NCDR Programs in This Report: CathPCI, ICD, ACTION GWTG, IMPACT. The Four NCDR Quality Programs Presented in This Report include CathPCI for Coronary Angiography and Percutaneous Coronary Intervention, ICD for Implantable Cardioverter Defibrillators, ACTION GWTG for Acute Coronary Syndromes, and IMPACT for Cardiac Catheterization and Percutaneous Structural Intervention for Congenital Heart Disease. The enrollment characteristics and numbers of patients and participating sites in 2014 are noted. Figure 1. Geographic Distribution of US Hospitals/Centers participating in the NCDR CathPCI Program in Numbers of NCDR CathPCI sites in the US by state in Additional participants include Washington DC (n=4), US Virgin Islands (n=2), United Arab Emirates (n=2), Bahrain (n=1), Brazil (n=4), India (n=1), Pakistan (n=1), Saudi Arabia (n=1), and Thailand (n=1). Figure 2. Temporal Trends in Median Time to Primary PCI for Patients with STEMI in the CathPCI Program, Median times from patient presentation to the performance of primary PCI in patients with STEMI among patients who were not transferred for the procedure (solid line) and those transferred from another facility to a STEMI receiving center (dashed line) annually between 2011 and 2014 in the CathPCI Program (see Appendix for measure definition). PCI=percutaneous coronary intervention; STEMI=ST segment elevation myocardial infarction. Figure 3. Temporal Trends in Proportion of Patients with STEMI Receiving Primary PCI within 90 minutes in the CathPCI Program, Proportions of patients receiving primary PCI within 90 minutes of initial presentation among those who were not transferred for 22
24 the procedure (solid line) and those transferred from another facility to a STEMI receiving center (dashed line) annually between 2011 and 2014 in the CathPCI Program (see Appendix for measure definition). The 10 th, 50 th, and 90 th percentiles are included in paretheses. PCI=percutaneous coronary intervention; STEMI=ST segment elevation myocardial infarction. Figure 4. Temporal Trends in Discharge Medications Composite Measure in Eligible Patients Undergoing PCI in the CathPCI Program, The proportion of patients receiving all evidence-based therapies (aspirin, P2Y12 inhibitor, and statin) for which they were eligible in the CathPCI Program between 2011 and 2014 (see Appendix for measure definition). Figure 5. Temporal Trends in Arterial Access Site for PCI in CathPCI Program, Proportions of PCI procedures performed using femoral (solid line) and radial (dashed line) access in the CathPCI Program between 2011 and Figure 6. Temporal Trends in Mechanical Ventricular Support for PCI in the CathPCI Program, Proportions of PCI procedures where mechanical ventricular support was used, including intra-aortic balloon pump (solid line) and other devices (dashed line) in the CathPCI Program between Other devices include Impella TM, percutaneous left ventricular assist devices, or extracorporeal membrane oxygenation. Figure 7. Temporal Trends in the Use and Timing of Mechanical Ventricular Support for PCI in the CathPCI Program, Numbers of PCI procedures in which mechanical ventricular support was used and the timing of institution of support (before procedure, during procedure prior to PCI, or after PCI peformed) in the in the CathPCI Program between Stratification by procedures in which intra-aortic balloon pump or other devices were used. 23
25 Figure 8. Temporal Trends in Complications Related to PCI in the CathPCI Program, Unadjusted rates of PCI-related complications in the CathPCI Program between , including acute kidney injury (solid line); blood transfusion (dotted line, diamonds); stroke (dashed line, squares); vascular access site injury (dashed line, triangles); and emergency CABG (dashed line, circles). See Appendix for definitions. CABG=coronary artery bypass graft surgery; RBC=red blood cell. Figure 9. Geographic Distribution of Hospitals/Centers participating in the NCDR ICD Program in Numbers of ICD Program sites in the US by state in Additional participants include Washington DC (n=7), Puerto Rico (n=5), US Virgin Islands (n=1), United Arab Emirates (n=1), Bahrain (n=1), and Brazil (n=1). Figure 10. Temporal Trends in Device Implantations by Indication in the NCDR ICD Program, Numbers of device implantations reported in the NCDR ICD Program between 2011 and 2014 according to device type, including single chamber (black), dual chamber (white) and cardiac resynchronization therapy with defibrillator (grey). Stratification performed according to initial implantation procedures and generator changes. Figure 11. Temporal Trends in Device Implantations by Device Type in the NCDR ICD Program, Numbers of device implantations reported in the NCDR ICD Program between 2011 and 2014 for primary prevention (black) and secondary prevention (white) indications. Stratification performed according to initial implantation procedures and generator changes. Figure 12. Temporal Trends in Proportion of Initial ICD Implants for Primary Prevention meeting ACC/AHA Class I, IIa, and IIb Guideline Indications in the NCDR ICD Program, Proportions of initial ICD procedures meeting ACC/AHA Class I (black); 24
26 class IIa (white) and class IIb (grey) indications in the NCDR ICD Program between 2011 and ACC=American College of Cardiology; AHA=American Heart Association. Figure 13. Temporal Trends in Medications Prescribed at Discharge in the NCDR ICD Program, Proportions of patients receiving evidence-based medications at discharge after ICD implantation including ACE-inhibitor or ARB among patients with left ventricular systolic dysfunction; beta blockers among patients with systolic dysfunction; and beta blocker among patients with prior myocardial infarction in the NCDR ICD Program between 2011 and Composite measure represents the proportions of patients who receive either or both of the evidence-based therapies based upon clinical eligibility (see Appendix for measure definitions). ACE-I=angiotensin converting enzyme inhibitor; ARB=angiotensin receptor blocker; LVSD=left ventricular systolic dysfunction; MI=myocardial infarction. Figure 14. Rates of in-hospital death in the NCDR ICD Program, Unadjusted proportion of deaths among patients undergoing ICD implantation for any indication in the NCDR ICD Program between 2011 and Figure 15. Geographic Distribution of Hospitals/Centers participating in the ACTION GWTG Program in Numbers of ACTION GWTG Program sites in the US by state in Additional participants include Washington DC (n=4), Puerto Rico (n=3), United Arab Emirates (n=3), Bahrain (n=1), Brazil (n=4), and Pakistan (n=1). Figure 16. Cardiac Procedures and Treatment Strategies used among Eligible Patients with in the ACTION GWTG Program in Proportions of patients undergoing cardiac catheterization, PCI, and CABG and those receiving only medical therapy stratified by MI type in the ACTION GWTG Program in CABG=coronary artery bypass graft surgery; 25
27 NSTEMI=non-ST-segment elevation myocardial infarction; PCI=percutaneous coronary intervention; STEMI=ST-segment elevation myocardial infarction. Figure 17. Temporal Trends in Median Time to Primary PCI for Patients with STEMI in the ACTION GWTG Program, (see Appendix for measure definition). Median times from patient presentation to the performance of primary PCI in patients with STEMI among patients who were not transferred for the procedure (solid line) and those transferred from another facility to a STEMI receiving center (dashed line) annually between 2011 and 2014 in the ACTION GWTG Program (see Appendix for measure definition). The 10 th, 50 th, and 90 th percentiles are included in paretheses. PCI=percutaneous coronary intervention; STEMI=ST segment elevation myocardial infarction. Figure 18. Temporal Trends in Proportion of Patients with STEMI Receiving Timely Reperfusion Therapy According to Guideline Recommendations in the ACTION GWTG Program, Proportions of patients receiving primary PCI within 90 minutes of initial presentation among those who were not transferred for the procedure (solid line); fibroniolysis within 30 minutes of presentation (dotted line), and primary PCI within 90 minutes for those transferred from another facility to a STEMI receiving center (dashed line) annually between 2011 and 2014 in the ACTION GWTG Program (see Appendix for measure definition). PCI=percutaneous coronary intervention; STEMI=ST segment elevation myocardial infarction. Figure 19. Anticoagulant/Antiplatelet Dosing Errors by MI Type in the ACTION GWTG Program, Proportions of patients treated with anticoagulants or antiplatelet agents in whom the doses provided exceeded recommendations in the ACTION GWTG Program in 2014 (see Appendix for definition). GP=glycoprotein; LMWH=low-molecular 26
28 weight heparin; NSTEMI=non-ST-segment elevation myocardial infarction; STEMI=STsegment elevation myocardial infarction; UFH=unfractionated heparin. Figure 20. In-Hospital Outcomes in the ACTION GWTG Program, Unadjusted rates of death, re-infarction, heart failure, cardiogenic shock, stroke, or bleeding occurring during hospitalization and stratified by MI type in the ACTION GWTG Program in 2014 (see Appendix for definitions). NSTEMI=non-ST-segment elevation myocardial infarction; STEMI=ST-segment elevation myocardial infarction. Figure 21. Temporal Trends in the Risks of In-hospital Outcomes among Patients with STEMI in the ACTION GWTG Program, Unadjusted rates of death (solid line), heart failure (dotted line), and major bleeding (dashed line) among patients with STEMI in the ACTION GWTG Program between (see Appendix for definitions). STEMI=ST-segment elevation myocardial infarction. Figure 22. Temporal Trends in the Risks of In-hospital Outcomes among Patients with NSTEMI in the ACTION GWTG Program, Unadjusted rates of death (solid line), heart failure (dotted line), and major bleeding (dashed line) among patients with NSTEMI in the ACTION GWTG Program between (see Appendix for definitions). NSTEMI=non-ST-segment elevation myocardial infarction. Figure 23. Geographic Distribution of Hospitals/Centers participating in the NCDR IMPACT Program in Numbers of NCDR IMPACT Program sites in the US by state in Additional participants include Washington DC (n=2), Australia (n=1), Bahrain (n=1), Brazil (n=4), and Canada (n=1). 27
29 Figure 24. Procedural Success in the NCDR IMPACT Program, Proportions of selected procedures meeting criteria for success in the IMPACT Program in 2014 (see Appendix for definitions). Figure 25. Proportion of Patients with Adverse Procedural Events Following Selected Procedures, 2014 (see Appendix for definitions). Proportions of selected procedures with an acute complication in the IMPACT Program in 2014 (see Appendix for definitions). Figure 26. Temporal Trends in Major Adverse Event or Death During the Episode of Care in the IMPACT Program, Unadjusted rates of major adverse events during hospitalization during which cardiac catheterization was performed stratified by patient age in the IMPACT Program between 2011 and 2014 (see Appendix for definitions). 28
30 Table 1. Demographic Characteristics of Patients Undergoing PCI Reported in the NCDR CathPCI Program, N 667,424 Age Mean Age (years + SD) < % 55 to < % 65 to < % % Female 31.3% Race White 86.5% Black / African American 8.8% Asian 2.8% Native American 0.7% Hawaiian / Pacific Islander 0.3% Hispanic or Latino Ethnicity 5.8% 29
31 Table 2. Clinical Characteristics Patients Undergoing PCI in the NCDR CathPCI Program, 2014 (see Appendix for definitions of procedural status) N 667,424 Diabetes Mellitus 38.8% Prior MI (> 7 days previously) 30.4% Heart Failure (within 2 weeks) 13.9% Prior PCI 41.2% Prior CABG 17.8% Status of PCI BMI (Mean + SD) Normal weight ( ) 19.3% Overweight ( ) 36.9% Obese (> 30) 43.5% Elective 35.3% Urgent 45.3% Emergent 19.0% Salvage 0.5% Table 2 abbreviations: BMI=body mass index; CABG=coronary artery bypass graft surgery; MI=myocardial infarction; PCI=percutaneous coronary intervention. 30
32 Table 3. Characteristics of Hospitals/Centers Participating in the CathPCI Program, N 1,612 Hospital Type Private/Community 87% Government 5% University 8% Hospital Location Rural 20% Urban 47% Suburban 34% Teaching Hospital 34% Bed Size (Mean + SD) PCI Procedural Volume (# cases) % % % % % % > % 31
33 Table 4. Appropriate Use Criteria (AUC) Metrics for PCI,* 2014 (applying definitions from the 2012 AUC for Coronary Revascularization Focused Update (27); see Appendix for definitions) Patients with ACS N = 563,448 Appropriate 98.3% Uncertain appropriateness 1.4% Inappropriate 0.3% Patients without ACS N = 84,702 Appropriate 53.5% Uncertain appropriateness 32.6% Inappropriate 13.9% *Patients in this table are those for whom data were available to classify appropriateness. Table 5 abbreviations: ACS=acute coronary syndrome; PCI=percutaneous coronary intervention. 32
34 Table 5. Demographic Characteristics of Patients in the NCDR ICD Program, All Patients Primary Prevention (CMS) Primary Prevention (not CMS) Secondary Prevention N 158,649 81,406 38,822 38,421 Age Mean Age (years + SD) < % 5.7% 34.1% 18.8% 55 to < % 11.1% 42.3% 22.9% 65 to < % 19.2% 7.6% 14.6% 70 to < % 21.0% 6.2% 14.9% 75 to < % 19.5% 4.7% 13.0% % 23.5% 5.1% 15.8% Female 27.9% 28.3% 29.0% 25.9% Race White 82.9% 84.9% 76.3% 85.4% Black 14.2% 12.8% 19.9% 11.4% Asian 1.6% 1.2% 2.2% 1.8% Native American 0.6% 0.5% 0.8% 0.6% Hawaiian / Pacific Islander 0.3% 0.2% 0.4% 0.3% Hispanic or Latino Ethnicity 5.7% 5.5% 7.1% 4.6% 33
35 Table 6. Clinical Characteristics of Patients in the NCDR ICD Program, History and Risk Factors All Patients CMS Primary Prevention Non-CMS Primary Prevention All Secondary Prevention Diabetes Mellitus 39.0% 42.9% 36.0% 33.7% Prior MI 48.2% 51.3% 40.3% 49.6% Heart Failure 83.4% 91.3% 86.5% 63.7% Prior PCI 32.9% 35.5% 28.7% 31.5% Prior CABG 28.8% 34.2% 19.2% 27.1% BMI (excluding outliers [BMIs over 50; 3+ SD]) (Mean + SD) Underweight (< 18.5) 1.6% 1.6% 1.3% 1.8% Normal weight ( ) 23.5% 25.4% 19.2% 24.0% Overweight ( ) 33.9% 35.1% 31.4% 34.2% Obese (> 30) 38.9% 36.3% 45.4% 38.1% 34
36 Table 7. Characteristics of Hospitals/Centers Participating in the NCDR ICD Program, # of Hospitals 1,715 Hospital Type Private/Community 90% Government 2% University 8% Hospital Location Rural 21% Urban 46% Suburban 33% Teaching Hospital 36% Certified Beds (Mean + SD) Number of Generator Procedures % % % % % % Certification of Implanting Physician Board Certified Clinical Cardiac Electrophysiology (EP)/Adult or Pediatric EP Fellowship 81.7% Pacemaker / ICD COCATS Fellowship / ICD Operator Training per HRS ICD Implantation Guidelines 33.0% Thoracic/Cardiac Surgery Residency 8.0% None 9.4% 35
37 Table 8. Demographic Characteristics of Patients in the ACTION GWTG Program According to MI Type, All STEMI NSTEMI N 182,903 71, ,535 Age Mean Age (years + SD) < % 29.7% 20.3% 55 to < % 30.2% 24.7% 65 to < % 29.5% 36.0% % 10.6% 19.0% Female 34.4% 29.3% 37.7% Race White 84.3% 85.7% 83.4% Black / African American 11.8% 10.1% 13.0% Asian 2.1% 2.5% 1.9% American Indian / Alaskan 0.8% 0.7% 0.9% Hawaiian / Pacific Islander 0.2% 0.2% 0.2% Hispanic or Latino Ethnicity 6.6% 6.7% 6.6% 36
38 Table 9. Clinical Characteristics of Patients in the ACTION GWTG Program All STEMI NSTEMI History and Risk Factors (N = 182,903) (N = 71,368) Normal weight ( ) 22.8% 22.7% 22.9% Overweight ( ) 36.8% 38.7% 35.5% Obese (> 30) 39.9% 38.2% 41.1% According to MI Type, (N = 111,535) Diabetes Mellitus 34.8% 27.0% 39.7% Prior Myocardial Infarction (MI) 24.8% 18.5% 28.7% Prior Heart Failure 12.8% 5.2% 17.4% Prior Percutaneous Coronary Intervention (PCI) 25.7% 20.0% 29.3% Prior Coronary Artery Bypass Grafting 13.2% 6.1% 17.6% (CABG) Prior Stroke 7.7% 5.1% 9.5% Prior Peripheral Arterial Disease (PAD) 9.0% 5.3% 11.4% BMI (excluding outliers [BMIs over 50; 3+ SD]) (Mean + SD)
39 Table 10. Characteristics of Hospitals/Centers Participating in the ACTION GWTG Program, # of Hospitals 907 Hospital Type Private/Community 89% Government 2% University 9% Hospital Location Rural 19% Urban 48% Suburban 33% Teaching Hospital 36% Certified Beds (Mean + SD)
40 Table 11. Distribution of Hospital Performance on ACTION GWTG Institutional Percentiles 10th 50th 90th Aspirin at Arrival (excluding patients transferred in or out) 95.9% 100.0% 100.0% Aspirin Prescribed at Discharge 94.9% 99.5% 100.0% Beta-blocker Prescribed at Discharge 91.2% 98.7% 100.0% Statin Prescribed at Discharge 97.1% 99.7% 100.0% Evaluation of Left Ventricular Systolic Function (LVSF) 88.0% 96.6% 100.0% ACE-I or ARB for Left Ventricular Systolic Dysfunction (LVSD) at Discharge 71.6% 95.3% 100.0% Adult Smoking Cessation Advice Counseling 94.4% 100.0% 100.0% Cardiac Rehabilitation Patient Referral from an Inpatient Setting 11.1% 86.7% 100.0% Median Door-to-Balloon (D2B) Time for Non-Transferred Patients (minutes) Median Door-to-Balloon (D2B) Time for Transferred Patients (minutes) Median Door-in-Door-Out Time for Transferred Patients (minutes) Performance Measures, 2014 (see Appendix for definitions) 39
41 Table 12. Distribution of Hospital Performance on ACTION GWTG Composite Metrics, 2014 (see Appendix for definitions) Percentiles 10th 50th 90th Overall AMI Performance Composite 85.4% 95.8% 99.1% Overall Defect Free Care 26.5% 78.4% 94.9% STEMI Performance Composite 87.6% 97.4% 99.8% NSTEMI Performance Composite 82.9% 94.7% 99.0% Acute AMI Performance Composite 92.8% 97.3% 99.4% Discharge AMI Performance Composite 78.3% 95.6% 99.5% 40
42 Table 13. Distribution of Hospital Performance on ACTION GWTG Quality Metrics, 2014 (see Appendix for definitions) Percentiles N 10th 50th 90th Electrocardiogram (ECG) w/in 10 Minutes of Arrival 56, % 68.5% 86.3% Acute Adenosine Diphosphate (ADP) Receptor Inhibitor Therapy 41, % 96.6% 100.0% Among STEMI Patients Acute Anticoagulant Therapy Among NSTEMI Patients 51, % 94.7% 100.0% ADP Receptor Inhibitors Prescribed at Discharge for Medically 18, % 56.7% 83.5% Treated AMI Patients Aldosterone Blocking Agents for Eligible Patients (LVSD with either diabetes mellitus or heart failure) at Discharge 2, % 12.8% 41.8% Aspirin at Arrival for All Patients 160, % 99.4% 100.0% 41
43 Table 14. Demographic Characteristics of Patients in the NCDR IMPACT Program, N 20,169 Age Mean Age (years + SD) < 1 month 7.1% 1 month to 1 year 17.5% > 1 year to 18 years 61.5% > 18 years 14.0% Premature Birth (if < 1 year old) 18.7% Female 46.4% Race White 71.2% Black / African American 16.3% Asian 4.1% American Indian / Alaskan 0.7% Hawaiian / Pacific Islander 0.5% Hispanic or Latino Ethnicity 18.2% 42
44 Table 15. Clinical Characteristics of Patients in the NCDR IMPACT Program, History and Risk Factors Episodes with No Comorbidities 68.4% Episodes with 1 Comorbidity 28.2% Episodes with Unknown 3.5% Comorbidities Coagulation Disorder 1.0% Diabetes Mellitus 1.4% Hepatic Disease 1.2% Renal Insufficiency 2.9% Seizure Disorder 2.8% Sickle Cell Anemia 0.3% Single Ventricle 19.6% Bi-ventricular 80.4% Prior Stroke 3.7% 43
45 Table 16. Characteristics of Hospitals/Centers Participating in the NCDR IMPACT Program, # of Hospitals 76 Hospital Type Private/Community 51% University 49% Hospital Location Rural 7% Urban 84% Suburban 9% Teaching Hospital 87% Certified Beds (Mean + SD)
 2014 data: 182,903 MI hospitalization records 907 centers")
 2014 data: 20,169 procedure records")
46 Diagnostic coronary angiography & percutaneous coronary interventions 2014 data: 667,424 PCI records 1,612 centers Acute coronary syndromes (STEMI and NSTEMI) 2014 data: 182,903 MI hospitalization records 907 centers Implantable cardioverter defibrillators 2014 data: 158,649 ICD records 1,715 centers Catheterization and/or structural intervention for congenital heart disease (pediatric and adult) 2014 data: 20,169 procedure records 76 centers

47
48
49
50
51
52

53
54
55
56

57

58

59
60
61
62
63
64
65
66
67
68
69

70
National Cardiovascular Data Registry
 National Cardiovascular Data Registry Young and Early Career Investigators ACC/AGS/NIA Multimorbidity in Older Adults with Cardiovascular Disease Workshop Ralph Brindis, MD MPH Senior Medical Officer,
National Cardiovascular Data Registry Young and Early Career Investigators ACC/AGS/NIA Multimorbidity in Older Adults with Cardiovascular Disease Workshop Ralph Brindis, MD MPH Senior Medical Officer,
Quality Payment Program: Cardiology Specialty Measure Set
 Measure Title * Reportable via PINNACLE α Reportable via Diabetes Collaborative CQMC v1.0 Measure High Priority Measure Cross Cutting Measure Heart Failure (HF): Angiotensin- Converting Enzyme (ACE) Inhibitor
Measure Title * Reportable via PINNACLE α Reportable via Diabetes Collaborative CQMC v1.0 Measure High Priority Measure Cross Cutting Measure Heart Failure (HF): Angiotensin- Converting Enzyme (ACE) Inhibitor
Ischemic Heart Disease Interventional Treatment
 Ischemic Heart Disease Interventional Treatment Cardiac Catheterization Laboratory Procedures (N = 89) is a regional and national referral center for percutaneous coronary intervention (PCI). A total of
Ischemic Heart Disease Interventional Treatment Cardiac Catheterization Laboratory Procedures (N = 89) is a regional and national referral center for percutaneous coronary intervention (PCI). A total of
The Evolving ACC-NCDR Programs: What you need to know for your practice
 The Evolving ACC-NCDR Programs: What you need to know for your practice John S. Rumsfeld, MD PhD FACC Chief Science Officer and Chair, American College of Cardiology National Cardiovascular Data Registry
The Evolving ACC-NCDR Programs: What you need to know for your practice John S. Rumsfeld, MD PhD FACC Chief Science Officer and Chair, American College of Cardiology National Cardiovascular Data Registry
Ischemic Heart Disease Interventional Treatment
 Ischemic Heart Disease Interventional Treatment Cardiac Catheterization Laboratory Procedures (N = 11,61) is a regional and national referral center for percutaneous coronary intervention (PCI). A total
Ischemic Heart Disease Interventional Treatment Cardiac Catheterization Laboratory Procedures (N = 11,61) is a regional and national referral center for percutaneous coronary intervention (PCI). A total
Consensus Core Set: Cardiovascular Measures Version 1.0
 Consensus Core Set: Cardiovascular s NQF 0330 Hospital 30-day, all-cause, riskstandardized readmission rate (RSRR) following heart failure hospitalization 0229 Hospital 30-day, all-cause, riskstandardized
Consensus Core Set: Cardiovascular s NQF 0330 Hospital 30-day, all-cause, riskstandardized readmission rate (RSRR) following heart failure hospitalization 0229 Hospital 30-day, all-cause, riskstandardized
ACTION Registry GWTG Research and Publications Update
 ACTION Registry GWTG Research and Publications Update Dr. Michael Kontos Director, Coronary Intensive Care Unit Pauley Heart Center, Virginia Commonwealth University The following relationships exist:
ACTION Registry GWTG Research and Publications Update Dr. Michael Kontos Director, Coronary Intensive Care Unit Pauley Heart Center, Virginia Commonwealth University The following relationships exist:
Quality Payment Program: Cardiology Specialty Measure Set
 Quality Payment Program: Cardiology Specialty Set Title Number CMS Reporting Method(s) Heart Failure (HF): Angiotensin- Converting Enzyme (ACE) Inhibitor or Angiotensin Receptor Blocker (ARB) Therapy for
Quality Payment Program: Cardiology Specialty Set Title Number CMS Reporting Method(s) Heart Failure (HF): Angiotensin- Converting Enzyme (ACE) Inhibitor or Angiotensin Receptor Blocker (ARB) Therapy for
Chapter 8: Cardiovascular Disease in Patients with ESRD
 Chapter 8: Cardiovascular Disease in Patients with ESRD Cardiovascular disease (CVD) is common in adult end-stage renal disease (ESRD) patients, with coronary artery disease (CAD) and heart failure (HF)
Chapter 8: Cardiovascular Disease in Patients with ESRD Cardiovascular disease (CVD) is common in adult end-stage renal disease (ESRD) patients, with coronary artery disease (CAD) and heart failure (HF)
Program Metrics. New Unique ID. Old Unique ID. Metric Set Metric Name Description. Old Metric Name
 Program Metrics The list below includes the metrics that will be calculated by the PINNACLE Registry for the outpatient office setting. These include metrics for, Atrial Fibrillation, Hypertension and.
Program Metrics The list below includes the metrics that will be calculated by the PINNACLE Registry for the outpatient office setting. These include metrics for, Atrial Fibrillation, Hypertension and.
Version 4.4. Institutional Outcomes Report 2014Q3. National Outcomes Report Aggregation Date: Jan 12, :59:59 PM
 Version 4.4 Institutional Outcomes Report 2014Q3 National Outcomes Report 999997 Aggregation Date: Jan 12, 2015 11:59:59 PM Publish Date: Jan 29, 2015 If User desires to publish or otherwise distribute
Version 4.4 Institutional Outcomes Report 2014Q3 National Outcomes Report 999997 Aggregation Date: Jan 12, 2015 11:59:59 PM Publish Date: Jan 29, 2015 If User desires to publish or otherwise distribute
THE NATIONAL QUALITY FORUM
 THE NATIONAL QUALITY FORUM National Voluntary Consensus Standards for Patient Outcomes Table of Measures Submitted-Phase 1 As of March 5, 2010 Note: This information is for personal and noncommercial use
THE NATIONAL QUALITY FORUM National Voluntary Consensus Standards for Patient Outcomes Table of Measures Submitted-Phase 1 As of March 5, 2010 Note: This information is for personal and noncommercial use
Quality Measures MIPS CV Specific
 Quality Measures MIPS CV Specific MEASURE NAME Atrial Fibrillation and Atrial Flutter: Chronic Anticoagulation Therapy CAHPS for MIPS Clinician/Group Survey Cardiac Rehabilitation Patient Referral from
Quality Measures MIPS CV Specific MEASURE NAME Atrial Fibrillation and Atrial Flutter: Chronic Anticoagulation Therapy CAHPS for MIPS Clinician/Group Survey Cardiac Rehabilitation Patient Referral from
Coronary Catheterization and Percutaneous Coronary Intervention in China 10-Year Results From the China PEACE-Retrospective CathPCI Study
 Coronary Catheterization and Percutaneous Coronary Intervention in China 10-Year Results From the China PEACE-Retrospective CathPCI Study Xin Zheng, MD, PhD; Jeptha P. Curtis, MD; Shuang Hu, PhD; YongfeiWang,
Coronary Catheterization and Percutaneous Coronary Intervention in China 10-Year Results From the China PEACE-Retrospective CathPCI Study Xin Zheng, MD, PhD; Jeptha P. Curtis, MD; Shuang Hu, PhD; YongfeiWang,
ACTION REGISTRY New Old ID# ID #
 In Process, Unpublished NCDR Manuscripts The following pages list current research and publications proposals that have been recently approved, are under analysis, are under manuscript development, or
In Process, Unpublished NCDR Manuscripts The following pages list current research and publications proposals that have been recently approved, are under analysis, are under manuscript development, or
10-Year Mortality of Older Acute Myocardial Infarction Patients Treated in U.S. Community Practice
 10-Year Mortality of Older Acute Myocardial Infarction Patients Treated in U.S. Community Practice Ajar Kochar, MD on behalf of: Anita Y. Chen, Puza P. Sharma, Neha J. Pagidipati, Gregg C. Fonarow, Patricia
10-Year Mortality of Older Acute Myocardial Infarction Patients Treated in U.S. Community Practice Ajar Kochar, MD on behalf of: Anita Y. Chen, Puza P. Sharma, Neha J. Pagidipati, Gregg C. Fonarow, Patricia
News the. Methods Data collection. The NCDR is a national registry of patients undergoing diagnostic cardiac catheterizations
 Journal of the American College of Cardiology Vol. 52, No. 20, 2008 2008 by the American College of Cardiology Foundation ISSN 0735-1097/08/$34.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2008.08.017
Journal of the American College of Cardiology Vol. 52, No. 20, 2008 2008 by the American College of Cardiology Foundation ISSN 0735-1097/08/$34.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2008.08.017
Transfer in D2B. Scott D Friedman, MD FACC Medical Director, Cardiology Services Shore Health System of Maryland. The Problem
 Transfer in D2B Scott D Friedman, MD FACC Medical Director, Cardiology Services Shore Health System of Maryland The Problem NRMI-5: North Carolina, July 2003- June 2004 NC Nation Guidelines N 2,738 79,927
Transfer in D2B Scott D Friedman, MD FACC Medical Director, Cardiology Services Shore Health System of Maryland The Problem NRMI-5: North Carolina, July 2003- June 2004 NC Nation Guidelines N 2,738 79,927
Measurement Name Beta-Blocker Therapy Prior Myocardial Infarction (MI)
") Program Metrics The list below includes the metrics that will be calculated by the PINNACLE Registry for the outpatient office setting. These include metrics for Artery, Atrial Fibrillation, Hypertension
Program Metrics The list below includes the metrics that will be calculated by the PINNACLE Registry for the outpatient office setting. These include metrics for Artery, Atrial Fibrillation, Hypertension
Cardiothoracic Department October 9, Deborah Winters, RN BSN Clinical Excellence
 Cardiothoracic Department October 9, 2013 Deborah Winters, RN BSN Clinical Excellence Quarterly Executive Summary CathPCI Registry PCI Performance Measures PCI Process/Outcome Metrics Diagnostic Cath Process/Outcome
Cardiothoracic Department October 9, 2013 Deborah Winters, RN BSN Clinical Excellence Quarterly Executive Summary CathPCI Registry PCI Performance Measures PCI Process/Outcome Metrics Diagnostic Cath Process/Outcome
The NCDR and Clinical Practice Guideline Development
 The NCDR and Clinical Practice Guideline Development Gregory J. Dehmer, MD, FACC, FACP, FSCAI Professor of Medicine Texas A&M HSC College of Medicine Director, Cardiology Division Baylor Scott & White
The NCDR and Clinical Practice Guideline Development Gregory J. Dehmer, MD, FACC, FACP, FSCAI Professor of Medicine Texas A&M HSC College of Medicine Director, Cardiology Division Baylor Scott & White
Chapter 4: Cardiovascular Disease in Patients with CKD
 Chapter 4: Cardiovascular Disease in Patients with CKD The prevalence of cardiovascular disease (CVD) was 65.8% among patients aged 66 and older who had chronic kidney disease (CKD), compared to 31.9%
Chapter 4: Cardiovascular Disease in Patients with CKD The prevalence of cardiovascular disease (CVD) was 65.8% among patients aged 66 and older who had chronic kidney disease (CKD), compared to 31.9%
CLINICAL SYMPTOMS AND ANGIOGRAPHIC FINDINGS OF PATIENTS UNDERGOING ELECTIVE CORONARY ANGIOGRAPHY WITHOUT PRIOR STRESS TESTING. Mouin S.
 CLINICAL SYMPTOMS AND ANGIOGRAPHIC FINDINGS OF PATIENTS UNDERGOING ELECTIVE CORONARY ANGIOGRAPHY WITHOUT PRIOR STRESS TESTING BY Mouin S. Abdallah Submitted to the graduate degree program in Clinical research
CLINICAL SYMPTOMS AND ANGIOGRAPHIC FINDINGS OF PATIENTS UNDERGOING ELECTIVE CORONARY ANGIOGRAPHY WITHOUT PRIOR STRESS TESTING BY Mouin S. Abdallah Submitted to the graduate degree program in Clinical research
From the a Duke Clinical Research Institute, Durham, NC, Singapore, Singapore,
 Comparison of percutaneous coronary intervention for previously treated versus de novo culprit lesions in acute myocardial infarction patients: insights from the National Cardiovascular Data Registry Chee
Comparison of percutaneous coronary intervention for previously treated versus de novo culprit lesions in acute myocardial infarction patients: insights from the National Cardiovascular Data Registry Chee
Performance and Quality Measures 1. NQF Measure Number. Coronary Artery Disease Measure Set
 Unless indicated, the PINNACLE Registry measures are endorsed by the American College of Cardiology Foundation and the American Heart Association and may be used for purposes of health care insurance payer
Unless indicated, the PINNACLE Registry measures are endorsed by the American College of Cardiology Foundation and the American Heart Association and may be used for purposes of health care insurance payer
In Process, Unpublished NCDR Manuscripts
 In Process, Unpublished NCDR Manuscripts The following pages list current research and publications proposals that have been recently approved, are under analysis, are under manuscript development, or
In Process, Unpublished NCDR Manuscripts The following pages list current research and publications proposals that have been recently approved, are under analysis, are under manuscript development, or
STEMI Care 2014 at the Crossroads: Taking the right road
 STEMI Care 2014 at the Crossroads: Taking the right road Robert C. Welsh, MD, FRCPC, FESC, FAHA, FACC Professor of Medicine Vice President, The Canadian Association of Interventional Cardiology Director,
STEMI Care 2014 at the Crossroads: Taking the right road Robert C. Welsh, MD, FRCPC, FESC, FAHA, FACC Professor of Medicine Vice President, The Canadian Association of Interventional Cardiology Director,
Subsequent management and therapies
 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation Subsequent management and therapies Marco Valgimigli, MD, PhD University of Ferrara ITALY
ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation Subsequent management and therapies Marco Valgimigli, MD, PhD University of Ferrara ITALY
Impella Versus Intra-Aortic Balloon Pump For Treatment Of Cardiogenic Shock: A Meta-Analysis of Randomized Controlled Trials
 Accepted Manuscript Impella Versus Intra-Aortic Balloon Pump For Treatment Of Cardiogenic Shock: A Meta-Analysis of Randomized Controlled Trials Dagmar M. Ouweneel, MSc, Erlend Eriksen, MD, Melchior Seyfarth,
Accepted Manuscript Impella Versus Intra-Aortic Balloon Pump For Treatment Of Cardiogenic Shock: A Meta-Analysis of Randomized Controlled Trials Dagmar M. Ouweneel, MSc, Erlend Eriksen, MD, Melchior Seyfarth,
Fiscal Year (FY) 2019 Hospital Inpatient Proposed Rule Interventional Cardiology, Peripheral Interventions & Rhythm Management
 2019 Hospital Inpatient Proposed Rule Interventional Cardiology, Peripheral Interventions & Rhythm Management") Fiscal Year (FY) 2019 Hospital Inpatient Proposed Rule Interventional Cardiology, Peripheral Interventions & Rhythm Management On April 24, 2018, the Centers for Medicare & Medicaid Services (CMS) released
Fiscal Year (FY) 2019 Hospital Inpatient Proposed Rule Interventional Cardiology, Peripheral Interventions & Rhythm Management On April 24, 2018, the Centers for Medicare & Medicaid Services (CMS) released
Joo-Yong Hahn, MD/PhD
 Sungkyunkwan University School of Medicine Joo-Yong Hahn, MD/PhD Heart Vascular Stork Institute, Samsung Medical Center Sungkyunkwan University School of Medicine Grant support Korean Society of Interventional
Sungkyunkwan University School of Medicine Joo-Yong Hahn, MD/PhD Heart Vascular Stork Institute, Samsung Medical Center Sungkyunkwan University School of Medicine Grant support Korean Society of Interventional
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Myocardial infarction: secondary prevention in primary and secondary care for patients following a myocardial infarction 1.1
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Myocardial infarction: secondary prevention in primary and secondary care for patients following a myocardial infarction 1.1
In Process, Unpublished NCDR Manuscripts
 In Process, Unpublished NCDR Manuscripts The following pages list current research and publications proposals that have been recently approved, are under analysis, are under manuscript development, or
In Process, Unpublished NCDR Manuscripts The following pages list current research and publications proposals that have been recently approved, are under analysis, are under manuscript development, or
Accepted Manuscript. Improving Survival in Cardiogenic shock: Is Impella the Answer?,, James J Glazier MD, Amir Kaki MD S (18)
") Accepted Manuscript Improving Survival in Cardiogenic shock: Is Impella the Answer?,, James J Glazier MD, Amir Kaki MD PII: S0002-9343(18)30496-0 DOI: 10.1016/j.amjmed.2018.04.045 Reference: AJM 14684
Accepted Manuscript Improving Survival in Cardiogenic shock: Is Impella the Answer?,, James J Glazier MD, Amir Kaki MD PII: S0002-9343(18)30496-0 DOI: 10.1016/j.amjmed.2018.04.045 Reference: AJM 14684
3309 Risk-Standardized Survival Rate (RSSR) for In-Hospital Cardiac Arrest (American Heart Association)
 for In-Hospital Cardiac Arrest (American Heart Association)") Memo March 8, 2018 To: NQF Members and the Public From: NQF Staff Re: Commenting Draft Report: National Voluntary Consensus Standards for Cardiovascular Background This report reflects the review of measures
Memo March 8, 2018 To: NQF Members and the Public From: NQF Staff Re: Commenting Draft Report: National Voluntary Consensus Standards for Cardiovascular Background This report reflects the review of measures
Data Requirements. Accreditation for Cardiovascular Excellence Quality in Invasive Cardiovascular Care
 2011 Data Requirements Accreditation for Cardiovascular Excellence Quality in Invasive Cardiovascular Care 2400 N Street NW, Suite 500 Washington, D.C. 20037-1153 T: 202-657-6859 1 1. 2. It is required
2011 Data Requirements Accreditation for Cardiovascular Excellence Quality in Invasive Cardiovascular Care 2400 N Street NW, Suite 500 Washington, D.C. 20037-1153 T: 202-657-6859 1 1. 2. It is required
NATIONAL QUALITY FORUM
 Cardiovascular and Diabetes Task Force Summary of In-Person Meeting #2 An in-person meeting of the Measure Applications Partnership (MAP) Cardiovascular and Diabetes Task Force was held on Tuesday, July
Cardiovascular and Diabetes Task Force Summary of In-Person Meeting #2 An in-person meeting of the Measure Applications Partnership (MAP) Cardiovascular and Diabetes Task Force was held on Tuesday, July
Know the Quality of our Care at Every Step. Kansas City ACS Summit BI-State Cardiovascular Education Consortium
 Know the Quality of our Care at Every Step Kansas City ACS Summit BI-State Cardiovascular Education Consortium Welcome to the Kansas City ACS Summit Objectives: Follow the flow and care of an ACS patient
Know the Quality of our Care at Every Step Kansas City ACS Summit BI-State Cardiovascular Education Consortium Welcome to the Kansas City ACS Summit Objectives: Follow the flow and care of an ACS patient
Quality Improvement in the Cath Lab Today and Tomorrow. Sunil V. Rao MD The Duke Clinical Research Institute Duke University Medical Center
 Quality Improvement in the Cath Lab Today and Tomorrow Sunil V. Rao MD The Duke Clinical Research Institute Duke University Medical Center Disclosures Consultant, Honoraria ZOLL, BMS, The Medicines Company,
Quality Improvement in the Cath Lab Today and Tomorrow Sunil V. Rao MD The Duke Clinical Research Institute Duke University Medical Center Disclosures Consultant, Honoraria ZOLL, BMS, The Medicines Company,
Adult Cardiology Clinical Privileges
 Name: Effective from / / to / / Initial privileges (initial appointment) (reappointment) Renewal of privileges All new applicants should meet the following requirements as approved by the governing body,
Name: Effective from / / to / / Initial privileges (initial appointment) (reappointment) Renewal of privileges All new applicants should meet the following requirements as approved by the governing body,
Published Manuscripts Based in the STS/ACC TVT Registry
 Published Manuscripts Based in the STS/ACC TVT Registry June 2018 Legend Manuscript Status is designated as follows: Abbreviations: Published/Full Citation Provided: Manuscript is in print. In Press: Manuscript
Published Manuscripts Based in the STS/ACC TVT Registry June 2018 Legend Manuscript Status is designated as follows: Abbreviations: Published/Full Citation Provided: Manuscript is in print. In Press: Manuscript
Timing of Surgery After Percutaneous Coronary Intervention
 Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
4. Which survey program does your facility use to get your program designated by the state?
 STEMI SURVEY Please complete one survey for each TCD designation you have in your facility. There would be a maximum of three surveys completed if your facility was designated as a trauma, stroke and STEMI
STEMI SURVEY Please complete one survey for each TCD designation you have in your facility. There would be a maximum of three surveys completed if your facility was designated as a trauma, stroke and STEMI
Summary of Research and Writing Activities In Cardiovascular Disease
 Summary of Research and Writing Activities In Cardiovascular Disease Carole Alison Chrvala, PhD 919.545.2149 (Work) 919.951.5230 (Mobile) cchrvala@centurylink.net www.healthmattersmedwriting.com 1 Manuscripts
Summary of Research and Writing Activities In Cardiovascular Disease Carole Alison Chrvala, PhD 919.545.2149 (Work) 919.951.5230 (Mobile) cchrvala@centurylink.net www.healthmattersmedwriting.com 1 Manuscripts
CLINICIAN INTERVIEW RECOGNIZING ACS AND STRATIFYING RISK IN PRIMARY CARE. An interview with A. Michael Lincoff, MD, and Eric R. Bates, MD, FACC, FAHA
 RECOGNIZING ACS AND STRATIFYING RISK IN PRIMARY CARE An interview with A. Michael Lincoff, MD, and Eric R. Bates, MD, FACC, FAHA Dr Lincoff is an interventional cardiologist and the Vice Chairman for Research
RECOGNIZING ACS AND STRATIFYING RISK IN PRIMARY CARE An interview with A. Michael Lincoff, MD, and Eric R. Bates, MD, FACC, FAHA Dr Lincoff is an interventional cardiologist and the Vice Chairman for Research
Practice-Level Executive Summary Report
 PINNACLE Registry Metrics 0003, Test Practice_NextGen [Rolling: 1st April 2015 to 31st March 2016 ] Generated on 5/11/2016 11:37:35 AM American College of Cardiology Foundation National Cardiovascular
PINNACLE Registry Metrics 0003, Test Practice_NextGen [Rolling: 1st April 2015 to 31st March 2016 ] Generated on 5/11/2016 11:37:35 AM American College of Cardiology Foundation National Cardiovascular
Comparing Effectively: The Role of Registries in Comparative Effectiveness Research
 Comparing Effectively: The Role of Registries in Comparative Effectiveness Research National Comparative Effectiveness Summit Washington DC September 16, 2009 Ralph Brindis, MD, MPH, FACC, FSCAI President-
Comparing Effectively: The Role of Registries in Comparative Effectiveness Research National Comparative Effectiveness Summit Washington DC September 16, 2009 Ralph Brindis, MD, MPH, FACC, FSCAI President-
Chapter 9: Cardiovascular Disease in Patients With ESRD
 Chapter 9: Cardiovascular Disease in Patients With ESRD Cardiovascular disease is common in adult ESRD patients, with atherosclerotic heart disease and congestive heart failure being the most common conditions
Chapter 9: Cardiovascular Disease in Patients With ESRD Cardiovascular disease is common in adult ESRD patients, with atherosclerotic heart disease and congestive heart failure being the most common conditions
New PINNACLE Measures The below measures for PINNACLE will be added as new measures to the outcomes reporting starting with Version 2.0.
 New PINNACLE Measures The below measures for PINNACLE will be added as new measures to the outcomes reporting starting with Version 2.0. Measure Steward Measure Name Measure Description Rationale for Adding
New PINNACLE Measures The below measures for PINNACLE will be added as new measures to the outcomes reporting starting with Version 2.0. Measure Steward Measure Name Measure Description Rationale for Adding
Cover Page. The handle holds various files of this Leiden University dissertation
 Cover Page The handle http://hdl.handle.net/1887/21543 holds various files of this Leiden University dissertation Author: Dharma, Surya Title: Perspectives in the treatment of cardiovascular disease :
Cover Page The handle http://hdl.handle.net/1887/21543 holds various files of this Leiden University dissertation Author: Dharma, Surya Title: Perspectives in the treatment of cardiovascular disease :
Patient Navigator Program: Focus MI Diplomat Hospital Metrics
 Patient Navigator Program: Focus MI Diplomat Hospital Metrics Goal Statement: To reduce avoidable hospital readmissions for patients discharged with acute myocardial infarction (AMI) by supporting a culture
Patient Navigator Program: Focus MI Diplomat Hospital Metrics Goal Statement: To reduce avoidable hospital readmissions for patients discharged with acute myocardial infarction (AMI) by supporting a culture
Centers for Medicare and Medicaid Services. National Coverage of Transcatheter Valve Technologies December 2015
 Centers for Medicare and Medicaid Services National Coverage of Transcatheter Valve Technologies December 2015 National Coverage Determination (NCD) for Transcatheter Aortic Valve Replacement (TAVR) (20.32)
Centers for Medicare and Medicaid Services National Coverage of Transcatheter Valve Technologies December 2015 National Coverage Determination (NCD) for Transcatheter Aortic Valve Replacement (TAVR) (20.32)
Published Manuscripts Based in the STS/ACC TVT Registry
 Published Manuscripts Based in the STS/ACC TVT Registry June 2018 Legend Manuscript Status is designated as follows: Abbreviations: Published/Full Citation Provided: Manuscript is in print. In Press: Manuscript
Published Manuscripts Based in the STS/ACC TVT Registry June 2018 Legend Manuscript Status is designated as follows: Abbreviations: Published/Full Citation Provided: Manuscript is in print. In Press: Manuscript
Chapter 4: Cardiovascular Disease in Patients With CKD
 Chapter 4: Cardiovascular Disease in Patients With CKD Introduction Cardiovascular disease is an important comorbidity for patients with chronic kidney disease (CKD). CKD patients are at high-risk for
Chapter 4: Cardiovascular Disease in Patients With CKD Introduction Cardiovascular disease is an important comorbidity for patients with chronic kidney disease (CKD). CKD patients are at high-risk for
Chapter 4: Cardiovascular Disease in Patients With CKD
 Chapter 4: Cardiovascular Disease in Patients With CKD The prevalence of cardiovascular disease is 68.8% among patients aged 66 and older who have CKD, compared to 34.1% among those who do not have CKD
Chapter 4: Cardiovascular Disease in Patients With CKD The prevalence of cardiovascular disease is 68.8% among patients aged 66 and older who have CKD, compared to 34.1% among those who do not have CKD
Cardiac Performance Measure Compliance in Outpatients
 Journal of the American College of Cardiology Vol. 56, No. 1, 2010 2010 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2010.03.043
Journal of the American College of Cardiology Vol. 56, No. 1, 2010 2010 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2010.03.043
Utilization and Impact of Pre-Hospital Electrocardiograms for Patients With Acute ST-Segment Elevation Myocardial Infarction
 Journal of the American College of Cardiology Vol. 53, No. 2, 2009 2009 by the American College of Cardiology Foundation ISSN 0735-1097/09/$36.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2008.09.030
Journal of the American College of Cardiology Vol. 53, No. 2, 2009 2009 by the American College of Cardiology Foundation ISSN 0735-1097/09/$36.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2008.09.030
Regional STEMI Transfer Systems: the Mayo and NC RACE Experiences
 Regional STEMI Transfer Systems: the Mayo and NC RACE Experiences Dr. Henry H. Ting, Mayo Clinic College of Medicine Dr. James G. Jollis,, Duke University Medical Center Mayo Clinic STEMI System for Transferred
Regional STEMI Transfer Systems: the Mayo and NC RACE Experiences Dr. Henry H. Ting, Mayo Clinic College of Medicine Dr. James G. Jollis,, Duke University Medical Center Mayo Clinic STEMI System for Transferred
The CSAC will review recommendations from the Cardiovascular 2015 project during its January 12, 2016 conference call.
 TO: FR: RE: Consensus Standards Approval Committee (CSAC) Melissa Marinelarena, Leslie Vicale, Donna Herring Cardiovascular 2015 Member Voting Results DA: January 12, 2016 The CSAC will review recommendations
TO: FR: RE: Consensus Standards Approval Committee (CSAC) Melissa Marinelarena, Leslie Vicale, Donna Herring Cardiovascular 2015 Member Voting Results DA: January 12, 2016 The CSAC will review recommendations
Cardiogenic Shock and Initiatives to Reduce Mortality
 Cardiogenic Shock and Initiatives to Reduce Mortality Tanveer Rab, MD, FACC William O Neill, MD, FACC Perwaiz Meraj, MD, FACC Alex Truesdell, MD, FACC The Golden Hours? 50% dead within 10 hours Overall
Cardiogenic Shock and Initiatives to Reduce Mortality Tanveer Rab, MD, FACC William O Neill, MD, FACC Perwaiz Meraj, MD, FACC Alex Truesdell, MD, FACC The Golden Hours? 50% dead within 10 hours Overall
FY2015 Proposed Hospital Inpatient Rule Summary
 FY2015 Proposed Hospital Inpatient Rule Summary Cardiac Rhythm Management (CRM) Electrophysiology (EP) Interventional Cardiology (IC) Peripheral Intervention (PI) On April 30, 2014, the Centers for Medicare
FY2015 Proposed Hospital Inpatient Rule Summary Cardiac Rhythm Management (CRM) Electrophysiology (EP) Interventional Cardiology (IC) Peripheral Intervention (PI) On April 30, 2014, the Centers for Medicare
How to treat Cardiac Resynchronization Therapy complications? C. Leclercq Departement of Cardiology Centre Cardio-Pneumologique Rennes, France
 How to treat Cardiac Resynchronization Therapy complications? C. Leclercq Departement of Cardiology Centre Cardio-Pneumologique Rennes, France Presenter Disclosure Information Christophe Leclercq, MD,
How to treat Cardiac Resynchronization Therapy complications? C. Leclercq Departement of Cardiology Centre Cardio-Pneumologique Rennes, France Presenter Disclosure Information Christophe Leclercq, MD,
Update interventional Cardiology Hans Rickli St.Gallen
 Update interventional Cardiology 2012 Hans Rickli St.Gallen 26.11.2012 Review of Literature ESC-Highlights TCT/AHA-Highlights Update interventional cardiology 2012 Structural Heart Disease Transcatheter
Update interventional Cardiology 2012 Hans Rickli St.Gallen 26.11.2012 Review of Literature ESC-Highlights TCT/AHA-Highlights Update interventional cardiology 2012 Structural Heart Disease Transcatheter
FY2014 Final Hospital Inpatient Rule Summary
 FY2014 Final Hospital Inpatient Rule Summary Reimbursement Update Cardiac Rhythm Management (CRM) Electrophysiology (EP) Interventional Cardiology (IC) Peripheral Intervention (PI) On August 2, 2013, the
FY2014 Final Hospital Inpatient Rule Summary Reimbursement Update Cardiac Rhythm Management (CRM) Electrophysiology (EP) Interventional Cardiology (IC) Peripheral Intervention (PI) On August 2, 2013, the
National Efforts to Improve Door-to-Balloon Time
 Journal of the American College of Cardiology Vol. 54, No. 25, 2009 2009 by the American College of Cardiology Foundation ISSN 0735-1097/09/$36.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2009.11.003
Journal of the American College of Cardiology Vol. 54, No. 25, 2009 2009 by the American College of Cardiology Foundation ISSN 0735-1097/09/$36.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2009.11.003
2013, American Heart Association
 2013, American Heart Association Mission: Lifeline - Data, Reports and ACTION Registry - GWTG THE MISSION: BETTER HEART ATTACK CARE FOR YOUR COMMUNITY THE LIFELINE: THE AMERICAN HEART ASSOCIATION AND YOU
2013, American Heart Association Mission: Lifeline - Data, Reports and ACTION Registry - GWTG THE MISSION: BETTER HEART ATTACK CARE FOR YOUR COMMUNITY THE LIFELINE: THE AMERICAN HEART ASSOCIATION AND YOU
Intro to Science & Quality. Prepared for Emerging Faculty September 2014 Julia Chang, VP Science & Quality
 Intro to Science & Quality Prepared for Emerging Faculty September 2014 Julia Chang, VP Science & Quality jchang@acc.org Science & Quality A division within the College ACC Science & Quality Education
Intro to Science & Quality Prepared for Emerging Faculty September 2014 Julia Chang, VP Science & Quality jchang@acc.org Science & Quality A division within the College ACC Science & Quality Education
STEMI Linee guida ESC Maddalena Lettino, Italy
 STEMI Linee guida ESC 2017 Maddalena Lettino, Italy Disclosure Speaker fee: Aspen, Astra Zeneca, BMS, Boehringer, Eli Lilly, DaichiiSankio, Bayer, Pfizer, Sanofi Advisory board member: Astra Zeneca, Eli
STEMI Linee guida ESC 2017 Maddalena Lettino, Italy Disclosure Speaker fee: Aspen, Astra Zeneca, BMS, Boehringer, Eli Lilly, DaichiiSankio, Bayer, Pfizer, Sanofi Advisory board member: Astra Zeneca, Eli
Outcomes in the Commercial Use of Self-expanding Prostheses in Transcatheter Aortic Valve Replacement: A Comparison of the Medtronic CoreValve and
 Outcomes in the Commercial Use of Self-expanding Prostheses in Transcatheter Aortic Valve Replacement: A Comparison of the Medtronic CoreValve and Evolut R platforms in the Society of Thoracic Surgeons/American
Outcomes in the Commercial Use of Self-expanding Prostheses in Transcatheter Aortic Valve Replacement: A Comparison of the Medtronic CoreValve and Evolut R platforms in the Society of Thoracic Surgeons/American
Published Manuscripts Based in the STS/ACC TVT Registry
 Published Manuscripts Based in the STS/ACC TVT Registry Legend Manuscript Status is designated as follows: Abbreviations: Published/Full Citation Provided: Manuscript is in print. In Press: Manuscript
Published Manuscripts Based in the STS/ACC TVT Registry Legend Manuscript Status is designated as follows: Abbreviations: Published/Full Citation Provided: Manuscript is in print. In Press: Manuscript
Registry Assessment of Peripheral Interventional Devices (RAPID)
") Registry Assessment of Peripheral Interventional Devices (RAPID) Adding Data Sources May 2, 2018 W. Schuyler Jones, MD Duke Clinical Research Institute Duke Heart Center Disclosures Research Grants: Agency
Registry Assessment of Peripheral Interventional Devices (RAPID) Adding Data Sources May 2, 2018 W. Schuyler Jones, MD Duke Clinical Research Institute Duke Heart Center Disclosures Research Grants: Agency
Diagnostic & Therapeutic Cardiac Catheterization Coder 2017
 Diagnostic & Therapeutic Cardiac Catheterization Coder 2017 Including peripheral and cardiovascular services and procedures Prepared and Published By: MedLearn Publishing A Division of Panacea Healthcare
Diagnostic & Therapeutic Cardiac Catheterization Coder 2017 Including peripheral and cardiovascular services and procedures Prepared and Published By: MedLearn Publishing A Division of Panacea Healthcare
Automatic External Defibrillators
 Last Review Date: April 21, 2017 Number: MG.MM.DM.10dC3v4 Medical Guideline Disclaimer Property of EmblemHealth. All rights reserved. The treating physician or primary care provider must submit to EmblemHealth
Last Review Date: April 21, 2017 Number: MG.MM.DM.10dC3v4 Medical Guideline Disclaimer Property of EmblemHealth. All rights reserved. The treating physician or primary care provider must submit to EmblemHealth
Implications of the 2013 ACC/AHA Cholesterol Guidelines for Adults in Contemporary Cardiovascular Practice
 JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY VOL. 64, NO. 21, 2014 ª 2014 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 0735-1097/$36.00 PUBLISHED BY ELSEVIER INC. http://dx.doi.org/10.1016/j.jacc.2014.08.041
JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY VOL. 64, NO. 21, 2014 ª 2014 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 0735-1097/$36.00 PUBLISHED BY ELSEVIER INC. http://dx.doi.org/10.1016/j.jacc.2014.08.041
A bs tr ac t. n engl j med 369;10 nejm.org september 5,
 The new england journal of medicine established in 1812 september 5, 213 vol. 369 no. 1 Door-to-Balloon Time and Mortality among Patients Undergoing Primary PCI Daniel S. Menees, M.D., Eric D. Peterson,
The new england journal of medicine established in 1812 september 5, 213 vol. 369 no. 1 Door-to-Balloon Time and Mortality among Patients Undergoing Primary PCI Daniel S. Menees, M.D., Eric D. Peterson,
2017 AHA/ACC Clinical Performance and Quality Measures for Adults With ST-Elevation and Non ST-Elevation Myocardial Infarction
 2017 AHA/ACC Clinical Performance and Quality Measures for Adults With ST-Elevation and Non ST-Elevation Myocardial Infarction Ramzi Khalil MD FACC Assistant Professor Allegheny Gen.Hospital AHN Speakers
2017 AHA/ACC Clinical Performance and Quality Measures for Adults With ST-Elevation and Non ST-Elevation Myocardial Infarction Ramzi Khalil MD FACC Assistant Professor Allegheny Gen.Hospital AHN Speakers
Blue Distinction Centers for Cardiac Care 2018 Provider Survey
 Blue Distinction Centers for Cardiac Care 2018 Provider Survey Printed version of this document is for reference purposes only. Paper copies of the Provider Survey and Team Table will not be accepted.
Blue Distinction Centers for Cardiac Care 2018 Provider Survey Printed version of this document is for reference purposes only. Paper copies of the Provider Survey and Team Table will not be accepted.
NHS QIS National Measurement of Audit Acute Coronary Syndrome
 NHS QIS National Measurement of Audit Acute Coronary Syndrome Things have changed based on the experience and feedback from the first cycle of measurement and, for the better we think! The Acute Coronary
NHS QIS National Measurement of Audit Acute Coronary Syndrome Things have changed based on the experience and feedback from the first cycle of measurement and, for the better we think! The Acute Coronary
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition
 Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
USRDS UNITED STATES RENAL DATA SYSTEM
 USRDS UNITED STATES RENAL DATA SYSTEM Chapter 9: Cardiovascular Disease in Patients With ESRD Cardiovascular disease is common in ESRD patients, with atherosclerotic heart disease and congestive heart
USRDS UNITED STATES RENAL DATA SYSTEM Chapter 9: Cardiovascular Disease in Patients With ESRD Cardiovascular disease is common in ESRD patients, with atherosclerotic heart disease and congestive heart
NEW JERSEY 2011 HOSPITAL PERFORMANCE REPORT TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES
 MEASURES") NEW JERSEY 2011 HOSPITAL PERFORMANCE REPORT TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES New Jersey Department of Health and Senior Services Health Care Quality Assessment
NEW JERSEY 2011 HOSPITAL PERFORMANCE REPORT TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES New Jersey Department of Health and Senior Services Health Care Quality Assessment
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes
 Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
National Intervention Council
 National Intervention Council Cardiological Society of India Registry Performa for Coronary, Non- Coronary & Peripheral Interventions Period January 1st 2016 to December 31 st 2016 Dr. (Prof.) N.N. Khanna
National Intervention Council Cardiological Society of India Registry Performa for Coronary, Non- Coronary & Peripheral Interventions Period January 1st 2016 to December 31 st 2016 Dr. (Prof.) N.N. Khanna
A Randomized Trial Evaluating Clinically Significant Bleeding with Low-Dose Rivaroxaban vs Aspirin, in Addition to P2Y12 inhibition, in ACS
 A Randomized Trial Evaluating Clinically Significant Bleeding with Low-Dose Rivaroxaban vs Aspirin, in Addition to P2Y12 inhibition, in ACS Magnus Ohman MB, on behalf of the GEMINI-ACS-1 Investigators
A Randomized Trial Evaluating Clinically Significant Bleeding with Low-Dose Rivaroxaban vs Aspirin, in Addition to P2Y12 inhibition, in ACS Magnus Ohman MB, on behalf of the GEMINI-ACS-1 Investigators
Clinical Lessons from BMC2-PCI
 Clinical Lessons from BMC2-PCI The Blue Cross Blue Shield of Michigan Cardiovascular Consortium Hitinder Gurm, M.D. University of Michigan Overview 32 papers since inception 10 papers published this year
Clinical Lessons from BMC2-PCI The Blue Cross Blue Shield of Michigan Cardiovascular Consortium Hitinder Gurm, M.D. University of Michigan Overview 32 papers since inception 10 papers published this year
Peripheral and Cardiology Coder 2018
 Peripheral and Cardiology Coder 2018 Cardiovascular Services and Procedures Prepared and Published By: MedLearn Publishing A Division of MedLearn Media, Inc. 445 Minnesota Street, Suite 514 St. Paul, MN
Peripheral and Cardiology Coder 2018 Cardiovascular Services and Procedures Prepared and Published By: MedLearn Publishing A Division of MedLearn Media, Inc. 445 Minnesota Street, Suite 514 St. Paul, MN
Title: Automatic External Defibrillators Division: Medical Management Department: Utilization Management
 Retired Date: Page 1 of 7 1. POLICY DESCRIPTION: Automatic External Defibrillators 2. RESPONSIBLE PARTIES: Medical Management Administration, Utilization Management, Integrated Care Management, Pharmacy,
Retired Date: Page 1 of 7 1. POLICY DESCRIPTION: Automatic External Defibrillators 2. RESPONSIBLE PARTIES: Medical Management Administration, Utilization Management, Integrated Care Management, Pharmacy,
Acute Coronary Syndromes: Different Continents, Different Guidelines?
 Acute Coronary Syndromes: Different Continents, Different Guidelines? Robert A. Harrington MD, MACC, FAHA, FESC Arthur L. Bloomfield Professor of Medicine Chair, Department of Medicine Stanford University
Acute Coronary Syndromes: Different Continents, Different Guidelines? Robert A. Harrington MD, MACC, FAHA, FESC Arthur L. Bloomfield Professor of Medicine Chair, Department of Medicine Stanford University
SANGER HEART & VASCULAR INSTITUTE. An inside look at outcomes and innovation
 SANGER HEART & VASCULAR INSTITUTE An inside look at outcomes and innovation The choice for advanced cardiovascular care For more than 50 years, Sanger Heart & Vascular Institute has delivered world-class
SANGER HEART & VASCULAR INSTITUTE An inside look at outcomes and innovation The choice for advanced cardiovascular care For more than 50 years, Sanger Heart & Vascular Institute has delivered world-class
Supplementary Online Content
 Supplementary Online Content Valle JA, Tamez H, Abbott JD, et al. Contemporary use and trends in unprotected left main coronary artery percutaneous coronary intervention in the United States: an analysis
Supplementary Online Content Valle JA, Tamez H, Abbott JD, et al. Contemporary use and trends in unprotected left main coronary artery percutaneous coronary intervention in the United States: an analysis
2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease
 2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease Developed in Collaboration with American Association for Thoracic Surgery, American
2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease Developed in Collaboration with American Association for Thoracic Surgery, American
The Future of Cardiac Care: Managing Our Patients Together
 The Future of Cardiac Care: Managing Our Patients Together Charles R. Caldwell, MD, FACC Disclosures: iheartdoc,inc. Telemedicine 1 MACRA Medicare Access and CHIP Reauthorization Act of 2015 Repealed the
The Future of Cardiac Care: Managing Our Patients Together Charles R. Caldwell, MD, FACC Disclosures: iheartdoc,inc. Telemedicine 1 MACRA Medicare Access and CHIP Reauthorization Act of 2015 Repealed the
Clinical Seminar. Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective
 Clinical Seminar Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical
Clinical Seminar Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical
IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT JANUARY 24, 2012
 IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT201203 JANUARY 24, 2012 The IHCP to reimburse implantable cardioverter defibrillators separately from outpatient implantation Effective March 1, 2012, the
IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT201203 JANUARY 24, 2012 The IHCP to reimburse implantable cardioverter defibrillators separately from outpatient implantation Effective March 1, 2012, the
Organizational, or Other Financial Benefit None None None None None None. None None None None None None
 Comprehensive Relationships With Industry and Other Entities AHA/ACC 2017 Update of ST-Elevation Myocardial Infarction and Non ST-Elevation Myocardial Infarction Measures Committee Jneid Hani, Chair Baylor
Comprehensive Relationships With Industry and Other Entities AHA/ACC 2017 Update of ST-Elevation Myocardial Infarction and Non ST-Elevation Myocardial Infarction Measures Committee Jneid Hani, Chair Baylor
PAD Characterization Within A Healthcare System" RAPID Face-to-Face Meeting Schuyler Jones, MD September 14, 2016
 PAD Characterization Within A Healthcare System" RAPID Face-to-Face Meeting Schuyler, MD September 14, 2016 Interventional Cardiology and Cath Labs Disclosures Research Grants: Agency for Healthcare Research
PAD Characterization Within A Healthcare System" RAPID Face-to-Face Meeting Schuyler, MD September 14, 2016 Interventional Cardiology and Cath Labs Disclosures Research Grants: Agency for Healthcare Research
The Strategic Reperfusion Early After STEMI study Implications for clinical practice
 The Strategic Reperfusion Early After STEMI study Implications for clinical practice Robert C. Welsh, MD, FRCPC Associate Professor of Medicine Director, Adult Cardiac Catheterization and Interventional
The Strategic Reperfusion Early After STEMI study Implications for clinical practice Robert C. Welsh, MD, FRCPC Associate Professor of Medicine Director, Adult Cardiac Catheterization and Interventional
JACC: CARDIOVASCULAR INTERVENTIONS VOL. 2, NO. 10, PUBLISHED BY ELSEVIER INC. DOI: /j.jcin
 JACC: CARDIOVASCULAR INTERVENTIONS VOL. 2, NO. 10, 2009 2009 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 1936-8798/09/$36.00 PUBLISHED BY ELSEVIER INC. DOI: 10.1016/j.jcin.2009.07.008 Outcomes
JACC: CARDIOVASCULAR INTERVENTIONS VOL. 2, NO. 10, 2009 2009 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 1936-8798/09/$36.00 PUBLISHED BY ELSEVIER INC. DOI: 10.1016/j.jcin.2009.07.008 Outcomes
Emergency surgery in acute coronary syndrome
 Emergency surgery in acute coronary syndrome Teerawoot Jantarawan Division of Cardiothoracic Surgery, Department of Surgery, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
Emergency surgery in acute coronary syndrome Teerawoot Jantarawan Division of Cardiothoracic Surgery, Department of Surgery, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
The MAIN-COMPARE Study
 Long-Term Outcomes of Coronary Stent Implantation versus Bypass Surgery for the Treatment of Unprotected Left Main Coronary Artery Disease Revascularization for Unprotected Left MAIN Coronary Artery Stenosis:
Long-Term Outcomes of Coronary Stent Implantation versus Bypass Surgery for the Treatment of Unprotected Left Main Coronary Artery Disease Revascularization for Unprotected Left MAIN Coronary Artery Stenosis: