Joo-Yong Hahn, MD/PhD
|
|
|
- Abraham Booth
- 5 years ago
- Views:
Transcription

1 Sungkyunkwan University School of Medicine Joo-Yong Hahn, MD/PhD Heart Vascular Stork Institute, Samsung Medical Center Sungkyunkwan University School of Medicine
2 Grant support Korean Society of Interventional Cardiology Ministry of Health & Welfare, Republic of Korea Sungkyunkwan University Foundation for Corporate Collaboration Abbott Vascular, Boston Scientific, Biotronik, Biometrics, and Medtronic Consulting Fees/Honoraria Abbott Vascular, Astra Zeneca, Biotronik, Biometrics, Daiichi Sankyo, Pfizer, and Sanofi-Aventis
3 Class I 1. Oral beta blockers should be initiated in the first 24 hours in patients with STEMI who do not have any of the following: signs of HF, evidence of a low output state, increased risk for cardiogenic shock, or other contraindications to use of oral beta blockers (PR interval more than 0.24 seconds, second- or third-degree heart block, active asthma, or reactive airways disease). (Level of Evidence: B) 2. Beta blockers should be continued during and after hospitalization for all patients with STEMI and with no contraindications to their use. (Level of Evidence: B) 3. Patients with initial contraindications to the use of beta blockers in the first 24 hours after STEMI should be reevaluated to determine their subsequent eligibility. (Level of Evidence: C)
4 Chen ZM et al. Lancet 2005; 366:
5 Effects of metoprolol allocation on death before first discharge from hospital Patients scheduled for primary PCI were to be excluded. Chen ZM et al. Lancet 2005; 366:
6 No randomized trial of beta-blocker therapy in patients with STEMI undergoing PCI without fibrinolytic therapy has been performed.

7 J Am Coll Cardiol 2004;43:


8 Am J Cardiol 2010;106: J-Cypher registry Beta group = 349 No-beta group = 561
9 Yang JH, Hahn JY et al. J Am Coll Cardiol Intv 2014;7:
10 J Am Coll Cardiol Intv 2014;7:
11 Propensity-Matched Population (n=3,975) β-blocker Group (n=2650) No-β-Blocker Group (n=1325) Adjusted HR * (95% CI) p value All-cause death 74 (2.8) 54 (4.1) 0.46 ( ) Cardiac death 40 (1.5) 37 (2.8) 0.39 ( ) 0.01 Myocardial infarction 30 (1.1) 19 (1.4) 0.61 ( ) 0.23 All-cause death or MI 101 (3.8) 70 (5.3) 0.60 ( ) 0.02 Any coronary revascularization 141 (5.3) 85 (6.4) 0.85 ( ) 0.38 Major adverse cardiac events 219 (8.3) 140 (10.6) 0.78 ( ) 0.07 J Am Coll Cardiol Intv 2014;7:
12 J Am Coll Cardiol Intv 2014;7:
13 J Am Coll Cardiol Intv 2014;7:
14 β-blocker therapy at discharge was associated with lower mortality. This result was maintained in propensity-matched populations. Furthermore, the association with better outcome of β- blocker therapy in terms of all-cause death was consistent across various subgroups.
15 Avoid/Caution Signs of HF, Low output state, Increased risk of cardiogenic shock, Prolonged firstdegree or high-grade AV block, Reactive airways disease
16 Am J Med Oct;127(10):

17
18 In the primary PCI era, no randomized trial of betablocker therapy in patients with STEMI has been performed. The role of beta blockers in patients with STEMI undergoing primary PCI remains controversial. Beneficial or useless or harmful? Which drug? How long? Future studies are needed.
19 Class I 1. An angiotensin-converting enzyme (ACE) inhibitor should be administered within the first 24 hours to all patients with STEMI with anterior location, HF, or ejection fraction (EF) less than or equal to 0.40, unless contraindicated (Level of Evidence: A) 2. An angiotensin receptor blocker (ARB) should be given to patients with STEMI who have indications for but are intolerant of ACE inhibitors.424,425 (Level of Evidence: B) Class IIa 1. ACE inhibitors are reasonable for all patients with STEMI and no contraindications to their use (Level of Evidence: A)
20 Class I ACE inhibitors are indicated starting within the first 24 h of STEMI in patients with evidence of heart failure, LV systolic dysfunction, diabetes or an anterior infarct. (Level of Evidence: A) An ARB, preferably valsartan, is an alternative to ACE inhibitors in patients with heart failure or LV systolic dysfunction, particularly those who are intolerant to ACE inhibitors. (Level of Evidence: B) Class IIa ACE inhibitors should be considered in all patients in the absence of contraindications. (Level of Evidence: A)
21 VALIANT trial AMI patients with CHF or LV systolic dysfunction N Engl J Med 2003;349:
22 One-year mortality 6.7% for primary PCI from the Korean AMI registry Song YB, Hahn JY, Gwon HC et al. Am J Cardiol 2010;106: Primary PCI The overwhelmingly preferred reperfusion strategy Performed in 85% of reperfusion eligible patients with STEMI Song YB, Hahn JY, Gwon HC et al. J Korean Med Sci 2008; 23: LV systolic function is preserved in most patients. Yang JH, Hahn JY et al. J Am Coll Cardiol Intv 2014 Cough developed commonly after ACE inhibor use. Upto 40%. Na SH et al. Korean Circulation J 2000;30:
23 Class I 1. An angiotensin-converting enzyme (ACE) inhibitor should be administered within the first 24 hours to all patients with STEMI with anterior location, HF, or ejection fraction (EF) less than or equal to 0.40, unless contraindicated (Level of Evidence: A) 2. An angiotensin receptor blocker (ARB) should be given to patients with STEMI who have indications for but are intolerant of ACE inhibitors.424,425 (Level of Evidence: B) Class IIa 1. ACE inhibitors are reasonable for all patients with STEMI and no contraindications to their use (Level of Evidence: A)
24
25
26
27
28 Yang JH, Hahn JY, submitted
29 Yang JH, Hahn JY, submitted
30 Yang JH, Hahn JY, submitted
31 Yang JH, Hahn JY, submitted
32 Non-randomized nature of the registry data Underpowered study The actual power was only around 50%. Lack of data on the specifics of the renin angiotensin system blocker, dose administered, and duration Adverse clinical events were not centrally adjudicated in our registry. A median follow-up of 12-months.

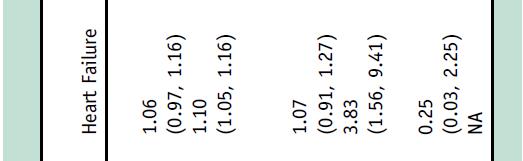
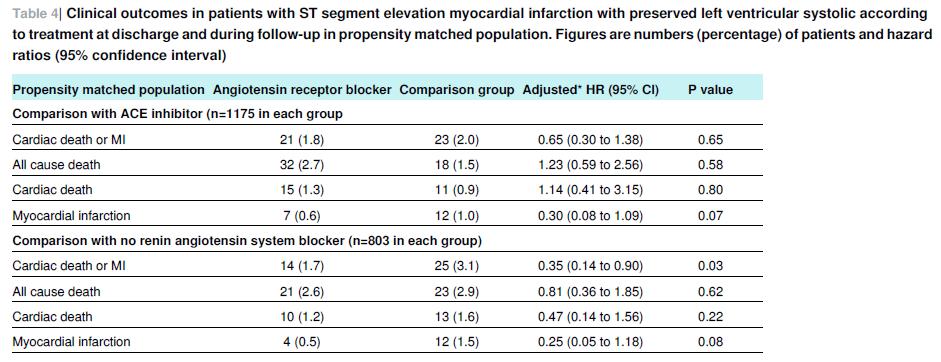
33 In STEMI patients with preserved LV systolic function who underwent primary PCI, The ARB group had a similar risk of cardiac death or MI compared with the ACE inhibitor group and a lower risk of cardiac death or MI compared with the no RAS blocker group. Furthermore, the association with favorable outcomes of ARB therapy in terms of cardiac death or MI was consistent across various subgroups.
34
35 Am J Cardiol 2014;114:1-8
36 Am J Cardiol 2014;114:1-8
37 Am J Cardiol 2014;114:1-8
38 N Engl J Med 2008;358: ON TARGET trial CV death, MI, stroke, or hospitalization for heart failure
39 Am J Cardiol 2014;114:1-8
40 An ARB, preferably valsartan, is an alternative to ACE inhibitors in patients with heart failure or LV systolic dysfunction. Data from the Korean registry suggest that ARBs can be used an alternative to ACE inhibitors in STEMI patients with preserved LV systolic function. However, the role of ARB in AMI patients with preserved LV systolic function remains controversial. Which ARB? Long-term follow-up. A large randomized trial is needed.


41 Sungkyunkwan University School of Medicine
42 Patients with AMI LV ejection fraction <40% Captopril 50 mg tid SAVE trial N Engl J Med. 1992;327:
43
44 ISIS-4 Patients with suspected AMI Captopril 50 mg bid STEMI 79% Fibrinolytic therapy 70% Larger benefit in patients with heart failure Lancet. 1995;345:
45
46 GISSI-3 Patients with AMI (n=19394) Lisinopril 50 mg bid Fibrinolytic therapy 70% Lancet. 1994;343:
47 Am J Cardiol 2014;114:1-8
Should All Patients Be Treated with Ace-inh /ARB after STEMI with Preserved LV Function?
 Should All Patients Be Treated with Ace-inh /ARB after STEMI with Preserved LV Function? Avi Shimony, MD, FESC Cardiology Division Soroka University Medical Center Ben-Gurion University, Beer-Sheva Disclosure
Should All Patients Be Treated with Ace-inh /ARB after STEMI with Preserved LV Function? Avi Shimony, MD, FESC Cardiology Division Soroka University Medical Center Ben-Gurion University, Beer-Sheva Disclosure
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes
 Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
ACE inhibitors: still the gold standard?
 ACE inhibitors: still the gold standard? Session: Twenty-five years after CONSENSUS What have we learnt about the RAAS in heart failure? Lars Køber, MD, D.Sci Department of Cardiology Rigshospitalet University
ACE inhibitors: still the gold standard? Session: Twenty-five years after CONSENSUS What have we learnt about the RAAS in heart failure? Lars Køber, MD, D.Sci Department of Cardiology Rigshospitalet University
STEMI Linee guida ESC Maddalena Lettino, Italy
 STEMI Linee guida ESC 2017 Maddalena Lettino, Italy Disclosure Speaker fee: Aspen, Astra Zeneca, BMS, Boehringer, Eli Lilly, DaichiiSankio, Bayer, Pfizer, Sanofi Advisory board member: Astra Zeneca, Eli
STEMI Linee guida ESC 2017 Maddalena Lettino, Italy Disclosure Speaker fee: Aspen, Astra Zeneca, BMS, Boehringer, Eli Lilly, DaichiiSankio, Bayer, Pfizer, Sanofi Advisory board member: Astra Zeneca, Eli
Subsequent management and therapies
 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation Subsequent management and therapies Marco Valgimigli, MD, PhD University of Ferrara ITALY
ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation Subsequent management and therapies Marco Valgimigli, MD, PhD University of Ferrara ITALY
Controversies in Cardiac Pharmacology
 Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Xi Li, Jing Li, Frederick A Masoudi, John A Spertus, Zhenqiu Lin, Harlan M Krumholz, Lixin Jiang for the China PEACE Collaborative Group
 China PEACE risk estimation tool for inhospital death from acute myocardial infarction: an early risk classification tree for decisions about fibrinolytic therapy Xi Li, Jing Li, Frederick A Masoudi, John
China PEACE risk estimation tool for inhospital death from acute myocardial infarction: an early risk classification tree for decisions about fibrinolytic therapy Xi Li, Jing Li, Frederick A Masoudi, John
ST-elevation myocardial infarctions (STEMIs)
") Guidelines for Treating STEMI: Case-Based Questions As many as 25% of eligible patients presenting with STEMI do not receive any form of reperfusion therapy. The ACC/AHA guidelines highlight steps to improve
Guidelines for Treating STEMI: Case-Based Questions As many as 25% of eligible patients presenting with STEMI do not receive any form of reperfusion therapy. The ACC/AHA guidelines highlight steps to improve
*NOTE: When reporting C P T code and 99239, it is recommended the measure be reported each time the code is submitted for hospital discharge.
 Measure #5 (NQF 0081): Heart Failure (HF): Angiotensin-Converting Enzyme (ACE) Inhibitor or Angiotensin Receptor Blocker (ARB) Therapy for Left Ventricular Systolic Dysfunction (LVSD) 2014 PQRS OPTIONS
Measure #5 (NQF 0081): Heart Failure (HF): Angiotensin-Converting Enzyme (ACE) Inhibitor or Angiotensin Receptor Blocker (ARB) Therapy for Left Ventricular Systolic Dysfunction (LVSD) 2014 PQRS OPTIONS
Metoprolol Succinate SelokenZOC
 Metoprolol Succinate SelokenZOC Blood Pressure Control and Far Beyond Mohamed Abdel Ghany World Health Organization - Noncommunicable Diseases (NCD) Country Profiles, 2014. 1 Death Rates From Ischemic
Metoprolol Succinate SelokenZOC Blood Pressure Control and Far Beyond Mohamed Abdel Ghany World Health Organization - Noncommunicable Diseases (NCD) Country Profiles, 2014. 1 Death Rates From Ischemic
Φαρμακευτική θεραπεία της μετεμφραγματικής καρδιακής ανεπάρκειας. Α. Καραβίδας Υπεύθυνος ιατρείου καρδιακής ανεπάρκειας Γ.Ν.Α Γ.
 Φαρμακευτική θεραπεία της μετεμφραγματικής καρδιακής ανεπάρκειας Α. Καραβίδας Υπεύθυνος ιατρείου καρδιακής ανεπάρκειας Γ.Ν.Α Γ.Γεννηματάς Clinical Trials on Fibrinolysis N = 61.41 AMI pts, ( GUSTO I, GUSTOIIb,
Φαρμακευτική θεραπεία της μετεμφραγματικής καρδιακής ανεπάρκειας Α. Καραβίδας Υπεύθυνος ιατρείου καρδιακής ανεπάρκειας Γ.Ν.Α Γ.Γεννηματάς Clinical Trials on Fibrinolysis N = 61.41 AMI pts, ( GUSTO I, GUSTOIIb,
Acute Coronary Syndromes: Different Continents, Different Guidelines?
 Acute Coronary Syndromes: Different Continents, Different Guidelines? Robert A. Harrington MD, MACC, FAHA, FESC Arthur L. Bloomfield Professor of Medicine Chair, Department of Medicine Stanford University
Acute Coronary Syndromes: Different Continents, Different Guidelines? Robert A. Harrington MD, MACC, FAHA, FESC Arthur L. Bloomfield Professor of Medicine Chair, Department of Medicine Stanford University
2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction
 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction Developed in Collaboration with American College of Emergency Physicians and Society for Cardiovascular Angiography and
2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction Developed in Collaboration with American College of Emergency Physicians and Society for Cardiovascular Angiography and
Clinical Seminar. Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective
 Clinical Seminar Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical
Clinical Seminar Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical
SHOULD BETA BLOCKERS BE USED ROUTINELY IN POST MI PATIENTS WITH PRESERVED LV FUNCTION?
 SHOULD BETA BLOCKERS BE USED ROUTINELY IN POST MI PATIENTS WITH PRESERVED LV FUNCTION? Doron Zahger, MD Department of Cardiology, Soroka University Medical Center, Faculty of Health Sciences, Ben Gurion
SHOULD BETA BLOCKERS BE USED ROUTINELY IN POST MI PATIENTS WITH PRESERVED LV FUNCTION? Doron Zahger, MD Department of Cardiology, Soroka University Medical Center, Faculty of Health Sciences, Ben Gurion
The role of angiotensin II receptor blockers in the management of heart failure
 European Heart Journal Supplements (2005) 7 (Supplement J), J10 J14 doi:10.1093/eurheartj/sui057 The role of angiotensin II receptor blockers in the management of heart failure John J.V. McMurray* Department
European Heart Journal Supplements (2005) 7 (Supplement J), J10 J14 doi:10.1093/eurheartj/sui057 The role of angiotensin II receptor blockers in the management of heart failure John J.V. McMurray* Department
Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist. Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI
 Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist physician Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI Outcome objectives of the discussion: At the end of the
Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist physician Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI Outcome objectives of the discussion: At the end of the
Periprocedural Myocardial Infarction and Clinical Outcome In Bifurcation Lesion
 Periprocedural Myocardial Infarction and Clinical Outcome In Bifurcation Lesion Hyeon-Cheol Gwon Cardiac and Vascular Center Samsung Medical Center Sungkyunkwan University School of Medicine Dr. Hyeon-Cheol
Periprocedural Myocardial Infarction and Clinical Outcome In Bifurcation Lesion Hyeon-Cheol Gwon Cardiac and Vascular Center Samsung Medical Center Sungkyunkwan University School of Medicine Dr. Hyeon-Cheol
Combination of renin-angiotensinaldosterone. how to choose?
 Combination of renin-angiotensinaldosterone system inhibitors how to choose? Karl Swedberg Professor of Medicine Sahlgrenska Academy University of Gothenburg karl.swedberg@gu.se Disclosures Research grants
Combination of renin-angiotensinaldosterone system inhibitors how to choose? Karl Swedberg Professor of Medicine Sahlgrenska Academy University of Gothenburg karl.swedberg@gu.se Disclosures Research grants
2014 PQRS OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY
 Measure #7 (NQF 0070): Coronary Artery Disease (CAD): Beta-Blocker Therapy Prior Myocardial Infarction (MI) or Left Ventricular Systolic Dysfunction (LVEF < 40%) 2014 PQRS OPTIONS F INDIVIDUAL MEASURES:
Measure #7 (NQF 0070): Coronary Artery Disease (CAD): Beta-Blocker Therapy Prior Myocardial Infarction (MI) or Left Ventricular Systolic Dysfunction (LVEF < 40%) 2014 PQRS OPTIONS F INDIVIDUAL MEASURES:
The Hearth Rate modulators. How to optimise treatment
 The Hearth Rate modulators How to optimise treatment Munich, ESC Congress 2012 Prof. Luigi Tavazzi GVM Care&Research E.S. Health Science Foundation Cotignola, IT Disclosure Cooperation with: Servier, Medtronic,
The Hearth Rate modulators How to optimise treatment Munich, ESC Congress 2012 Prof. Luigi Tavazzi GVM Care&Research E.S. Health Science Foundation Cotignola, IT Disclosure Cooperation with: Servier, Medtronic,
Abstract Background: Methods: Results: Conclusions:
 Two-Year Clinical and Angiographic Outcomes of Overlapping Sirolimusversus Paclitaxel- Eluting Stents in the Treatment of Diffuse Long Coronary Lesions Kang-Yin Chen 1,2, Seung-Woon Rha 1, Yong-Jian Li
Two-Year Clinical and Angiographic Outcomes of Overlapping Sirolimusversus Paclitaxel- Eluting Stents in the Treatment of Diffuse Long Coronary Lesions Kang-Yin Chen 1,2, Seung-Woon Rha 1, Yong-Jian Li
ESC Guidelines for the Diagnosis and Treatment of Chronic Heart Failure
 ESC Guidelines for the Diagnosis and Treatment of Chronic Heart Failure - 2005 Karl Swedberg Professor of Medicine Department of Medicine Sahlgrenska University Hospital/Östra Göteborg University Göteborg
ESC Guidelines for the Diagnosis and Treatment of Chronic Heart Failure - 2005 Karl Swedberg Professor of Medicine Department of Medicine Sahlgrenska University Hospital/Östra Göteborg University Göteborg
Optimal blockade of the Renin- Angiotensin-Aldosterone. in chronic heart failure
 Optimal blockade of the Renin- Angiotensin-Aldosterone Aldosterone- (RAA)-System in chronic heart failure Jan Östergren Department of Medicine Karolinska University Hospital Stockholm, Sweden Key Issues
Optimal blockade of the Renin- Angiotensin-Aldosterone Aldosterone- (RAA)-System in chronic heart failure Jan Östergren Department of Medicine Karolinska University Hospital Stockholm, Sweden Key Issues
Diabetic Patients: Current Evidence of Revascularization
 Diabetic Patients: Current Evidence of Revascularization Alexandra J. Lansky, MD Yale University School of Medicine University College of London The Problem with Diabetic Patients Endothelial dysfunction
Diabetic Patients: Current Evidence of Revascularization Alexandra J. Lansky, MD Yale University School of Medicine University College of London The Problem with Diabetic Patients Endothelial dysfunction
Belinda Green, Cardiologist, SDHB, 2016
 Acute Coronary syndromes All STEMI ALL Non STEMI Unstable angina Belinda Green, Cardiologist, SDHB, 2016 Thrombus in proximal LAD Underlying pathophysiology Be very afraid for your patient Wellens
Acute Coronary syndromes All STEMI ALL Non STEMI Unstable angina Belinda Green, Cardiologist, SDHB, 2016 Thrombus in proximal LAD Underlying pathophysiology Be very afraid for your patient Wellens
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
LXIV: DRUGS: 4. RAS BLOCKADE
 LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
Understanding and Development of New Therapies for Heart Failure - Lessons from Recent Clinical Trials -
 Understanding and Development of New Therapies for Heart Failure - Lessons from Recent Clinical Trials - Clinical trials Evidence-based medicine, clinical practice Impact upon Understanding pathophysiology
Understanding and Development of New Therapies for Heart Failure - Lessons from Recent Clinical Trials - Clinical trials Evidence-based medicine, clinical practice Impact upon Understanding pathophysiology
Hyeon-Cheol Gwon, On the behalf of SMART-DATE trial investigators ACC LBCT 2018
 Six-month versus 12-month or longer dual antiplatelet therapy after percutaneous coronary intervention in patients with acute coronary syndromes (SMART-DATE): a randomized, openlabel, multicenter trial
Six-month versus 12-month or longer dual antiplatelet therapy after percutaneous coronary intervention in patients with acute coronary syndromes (SMART-DATE): a randomized, openlabel, multicenter trial
STEMI Care 2014 at the Crossroads: Taking the right road
 STEMI Care 2014 at the Crossroads: Taking the right road Robert C. Welsh, MD, FRCPC, FESC, FAHA, FACC Professor of Medicine Vice President, The Canadian Association of Interventional Cardiology Director,
STEMI Care 2014 at the Crossroads: Taking the right road Robert C. Welsh, MD, FRCPC, FESC, FAHA, FACC Professor of Medicine Vice President, The Canadian Association of Interventional Cardiology Director,
When Conventional Heart Failure Therapy is not Enough: Angiotensin Receptor Blocker, Direct Renin Inhibitor or Aldosterone Antagonist?
 When Conventional Heart Failure Therapy is not Enough: Angiotensin Receptor Blocker, Direct Renin Inhibitor or Aldosterone Antagonist? Sripal Bangalore, MD, MHA, Sunil Kumar, MD, Franz H Messerli, MD,
When Conventional Heart Failure Therapy is not Enough: Angiotensin Receptor Blocker, Direct Renin Inhibitor or Aldosterone Antagonist? Sripal Bangalore, MD, MHA, Sunil Kumar, MD, Franz H Messerli, MD,
Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend )
") Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend ) Stephen G. Ellis, MD Section Head, Interventional Cardiology Professor of Medicine Cleveland
Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend ) Stephen G. Ellis, MD Section Head, Interventional Cardiology Professor of Medicine Cleveland
presenters 2010 Sameh Sabet Ain Shams University
 Guidelines for PCI in late STEMI presenters 2010 Sameh Sabet Assistant Professor of Cardiology Ain Shams University 29% of MI patients have STEMI. NRMI 4 (Fourth National Registry of Myocardial Infarction),
Guidelines for PCI in late STEMI presenters 2010 Sameh Sabet Assistant Professor of Cardiology Ain Shams University 29% of MI patients have STEMI. NRMI 4 (Fourth National Registry of Myocardial Infarction),
The Therapeutic Potential of Novel Approaches to RAAS. Professor of Medicine University of California, San Diego
 The Therapeutic Potential of Novel Approaches to RAAS Inhibition in Heart Failure Barry Greenberg, M.D. Professor of Medicine University of California, San Diego Chain of Events Leading to End-Stage Heart
The Therapeutic Potential of Novel Approaches to RAAS Inhibition in Heart Failure Barry Greenberg, M.D. Professor of Medicine University of California, San Diego Chain of Events Leading to End-Stage Heart
Guideline-Directed Medical Therapy
 Guideline-Directed Medical Therapy Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation OPTIMAL THERAPY (As defined in
Guideline-Directed Medical Therapy Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation OPTIMAL THERAPY (As defined in
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Scottish Medicines Consortium
 Scottish Medicines Consortium valsartan 40mg, 80mg and 160mg capsules and tablets (Diovan ) No. (162/05) Novartis Pharmaceuticals New Indication: following myocardial infarction in patients with clinical
Scottish Medicines Consortium valsartan 40mg, 80mg and 160mg capsules and tablets (Diovan ) No. (162/05) Novartis Pharmaceuticals New Indication: following myocardial infarction in patients with clinical
Acute Coronary Syndromes
 Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Revascularization in Severe LV Dysfunction: The Role of Inducible Ischemia and Viability Testing
 Revascularization in Severe LV Dysfunction: The Role of Inducible Ischemia and Viability Testing Evidence and Uncertainties Robert O. Bonow, MD, MS, MACC Northwestern University Feinberg School of Medicine
Revascularization in Severe LV Dysfunction: The Role of Inducible Ischemia and Viability Testing Evidence and Uncertainties Robert O. Bonow, MD, MS, MACC Northwestern University Feinberg School of Medicine
Guidelines PATHOLOGY: FATAL PERIOPERATIVE MI NON-PMI N = 25 PMI N = 42. Prominent Dutch Cardiovascular Researcher Fired for Scientific Misconduct
 PATHOLOGY: FATAL PERIOPERATIVE MI NON-PMI N = 25 PMI N = 42 Preoperative, Intraoperative, and Postoperative Factors Associated with Perioperative Cardiac Complications in Patients Undergoing Major Noncardiac
PATHOLOGY: FATAL PERIOPERATIVE MI NON-PMI N = 25 PMI N = 42 Preoperative, Intraoperative, and Postoperative Factors Associated with Perioperative Cardiac Complications in Patients Undergoing Major Noncardiac
Decline in CV-Mortality
 Lipids id 2013 What s Changed? Christopher Granger, MD Disclosure Research contracts: AstraZeneca, GSK, Merck, Sanofi- Aventis, BMS, Pfizer, The Medicines Company, Medtronic Foundation, and Boehringer
Lipids id 2013 What s Changed? Christopher Granger, MD Disclosure Research contracts: AstraZeneca, GSK, Merck, Sanofi- Aventis, BMS, Pfizer, The Medicines Company, Medtronic Foundation, and Boehringer
The MAIN-COMPARE Registry
 Long-Term Outcomes of Coronary Stent Implantation versus Bypass Surgery for the Treatment of Unprotected Left Main Coronary Artery Disease Revascularization for Unprotected Left MAIN Coronary Artery Stenosis:
Long-Term Outcomes of Coronary Stent Implantation versus Bypass Surgery for the Treatment of Unprotected Left Main Coronary Artery Disease Revascularization for Unprotected Left MAIN Coronary Artery Stenosis:
The ACC Heart Failure Guidelines
 The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
Evidence Supporting Post-MI Use of
 Addressing the Gap in the Management of Patients After Acute Myocardial Infarction: How Good Is the Evidence Supporting Current Treatment Guidelines? Michael B. Fowler, MB, FRCP Beta-adrenergic blocking
Addressing the Gap in the Management of Patients After Acute Myocardial Infarction: How Good Is the Evidence Supporting Current Treatment Guidelines? Michael B. Fowler, MB, FRCP Beta-adrenergic blocking
Hospital Ranking Based on Discharge Prescriptions After Acute Myocardial Infarction: A National Assessment over Three Consecutive Years
 Hospital Ranking Based on Discharge Prescriptions After Acute Myocardial Infarction: A National Assessment over Three Consecutive Years François Schiele 1, Frédéric Capuano 2, Geneviève Derumeaux 3, Nicolas
Hospital Ranking Based on Discharge Prescriptions After Acute Myocardial Infarction: A National Assessment over Three Consecutive Years François Schiele 1, Frédéric Capuano 2, Geneviève Derumeaux 3, Nicolas
Treating HF Patients with ARNI s Why, When and How?
 Treating HF Patients with ARNI s Why, When and How? 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La Jolla, CA Barry Greenberg M.D. Distinguished Professor
Treating HF Patients with ARNI s Why, When and How? 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La Jolla, CA Barry Greenberg M.D. Distinguished Professor
Program Metrics. New Unique ID. Old Unique ID. Metric Set Metric Name Description. Old Metric Name
 Program Metrics The list below includes the metrics that will be calculated by the PINNACLE Registry for the outpatient office setting. These include metrics for, Atrial Fibrillation, Hypertension and.
Program Metrics The list below includes the metrics that will be calculated by the PINNACLE Registry for the outpatient office setting. These include metrics for, Atrial Fibrillation, Hypertension and.
2) Patients who are 18 years and older with a diagnosis of CAD or history of cardiac surgery who have a prior myocardial infarction
 Patients who are 18 years and older with a diagnosis of CAD or history of cardiac surgery who have a prior myocardial infarction") Measure #7 (NQF 0070): Coronary Artery Disease (CAD): Beta-Blocker Therapy Prior Myocardial Infarction (MI) or Left Ventricular Systolic Dysfunction (LVEF < 40%) National Quality Strategy Domain: Effective
Measure #7 (NQF 0070): Coronary Artery Disease (CAD): Beta-Blocker Therapy Prior Myocardial Infarction (MI) or Left Ventricular Systolic Dysfunction (LVEF < 40%) National Quality Strategy Domain: Effective
Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary
 Prior Authorization and Quantity Limit Program Summary") Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Indication Entresto Reduce the risk of cardiovascular (sacubitril/valsartan) death
Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Indication Entresto Reduce the risk of cardiovascular (sacubitril/valsartan) death
A Future for the IABP in Cardiogenic Shock? Holger Thiele Medical Clinic II (Cardiology/Angiology/Intensive Care) University of Lübeck, Germany
 University of Lübeck, Germany") A Future for the in Cardiogenic Shock? Holger Thiele Medical Clinic II (Cardiology/Angiology/Intensive Care) University of Lübeck, Germany Disclosures Funding: German Research Foundation German Heart Research
A Future for the in Cardiogenic Shock? Holger Thiele Medical Clinic II (Cardiology/Angiology/Intensive Care) University of Lübeck, Germany Disclosures Funding: German Research Foundation German Heart Research
New evidences in heart failure: the GISSI-HF trial. Aldo P Maggioni, MD ANMCO Research Center Firenze, Italy
 New evidences in heart failure: the GISSI-HF trial Aldo P Maggioni, MD ANMCO Research Center Firenze, Italy % Improving survival in chronic HF and LV systolic dysfunction: 1 year all-cause mortality 20
New evidences in heart failure: the GISSI-HF trial Aldo P Maggioni, MD ANMCO Research Center Firenze, Italy % Improving survival in chronic HF and LV systolic dysfunction: 1 year all-cause mortality 20
Management of new-onset AF: Initial rate control treatment
 Geneva Acute Crdiovascular Care Congress 2014 - October 18-20, 2014 Management of new-onset AF: Initial rate control treatment Antonio Raviele, MD, FESC, FHRS ALFA Alliance to Fight Atrial fibrillation,
Geneva Acute Crdiovascular Care Congress 2014 - October 18-20, 2014 Management of new-onset AF: Initial rate control treatment Antonio Raviele, MD, FESC, FHRS ALFA Alliance to Fight Atrial fibrillation,
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Quality ID #7 (NQF 0070): Coronary Artery Disease (CAD): Beta-Blocker Therapy Prior Myocardial Infarction (MI) or Left Ventricular Systolic Dysfunction (LVEF < 40%) National Quality Strategy Domain: Effective
Quality ID #7 (NQF 0070): Coronary Artery Disease (CAD): Beta-Blocker Therapy Prior Myocardial Infarction (MI) or Left Ventricular Systolic Dysfunction (LVEF < 40%) National Quality Strategy Domain: Effective
Severe Left Ventricular Dysfunction: Evolving Revascularization Strategies
 Severe Left Ventricular Dysfunction: Evolving Revascularization Strategies Robert O. Bonow, MD, MS, MACC Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern
Severe Left Ventricular Dysfunction: Evolving Revascularization Strategies Robert O. Bonow, MD, MS, MACC Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern
Heart Failure 101 The Basic Principles of Diagnosis & Management
 Heart Failure 101 The Basic Principles of Diagnosis & Management Bill Tran, MD Non Invasive Cardiologist February 24, 2018 What the eye does not see and the mind does not know, does not exist. DH Lawrence
Heart Failure 101 The Basic Principles of Diagnosis & Management Bill Tran, MD Non Invasive Cardiologist February 24, 2018 What the eye does not see and the mind does not know, does not exist. DH Lawrence
ACE inhibitors vs ARBs Myths and Facts
 ACE inhibitors vs ARBs Myths and Facts Prof. Dr. med. Frank Ruschitzka, FRCP (Edinburgh) Director Heart Failure/Transplantation Clinic University Clinic Zurich Switzerland Conflict of interest: Bayer,
ACE inhibitors vs ARBs Myths and Facts Prof. Dr. med. Frank Ruschitzka, FRCP (Edinburgh) Director Heart Failure/Transplantation Clinic University Clinic Zurich Switzerland Conflict of interest: Bayer,
Experience of Korea Acute Myocardial Infarction Registry (KAMIR)
") Japan-Korea Joint AMI Symposium Korean Society of Myocardial Infarction Apr 18-19 2014 Experience of Korea Acute Myocardial Infarction Registry (KAMIR) Myung Ho Jeong, MD, PhD, FACC, FAHA, FESC, FSCAI,
Japan-Korea Joint AMI Symposium Korean Society of Myocardial Infarction Apr 18-19 2014 Experience of Korea Acute Myocardial Infarction Registry (KAMIR) Myung Ho Jeong, MD, PhD, FACC, FAHA, FESC, FSCAI,
DISCUSSION QUESTION - 1
 CASE PRESENTATION 87 year old male No past history of diabetes, HTN, dyslipidemia or smoking Very active Medications: omeprazole for heart burn Admitted because of increasing retrosternal chest pressure
CASE PRESENTATION 87 year old male No past history of diabetes, HTN, dyslipidemia or smoking Very active Medications: omeprazole for heart burn Admitted because of increasing retrosternal chest pressure
*NOTE: When submitting CPT code and 99239, it is recommended the measure be submitted each time the code is submitted for hospital discharge.
 Quality ID #5 (NQF 0081): Heart Failure (HF): Angiotensin-Converting Enzyme (ACE) Inhibitor or Angiotensin Receptor Blocker (ARB) Therapy for Left Ventricular Systolic Dysfunction (LVSD) National Quality
Quality ID #5 (NQF 0081): Heart Failure (HF): Angiotensin-Converting Enzyme (ACE) Inhibitor or Angiotensin Receptor Blocker (ARB) Therapy for Left Ventricular Systolic Dysfunction (LVSD) National Quality
The Need for Rescue PCI after Failed Fibrinolysis: Who, When and Why.
 Implementing the pharmacoinvasive strategy in STEMI The Need for Rescue PCI after Failed Fibrinolysis: Who, When and Why. 7:20-7:40 Robert C. Welsh, MD, FRCPC, FESC, FAHA, FACC Professor of Medicine Director,
Implementing the pharmacoinvasive strategy in STEMI The Need for Rescue PCI after Failed Fibrinolysis: Who, When and Why. 7:20-7:40 Robert C. Welsh, MD, FRCPC, FESC, FAHA, FACC Professor of Medicine Director,
ANGIOTENSIN II RECEPTOR BLOCKERS: MORE THAN THE ALTERNATIVE PRESENTATION BY: PATRICK HO, USC PHARM D. CANDIDATE OF 2017 MENTOR: DR.
 ANGIOTENSIN II RECEPTOR BLOCKERS: MORE THAN THE ALTERNATIVE PRESENTATION BY: PATRICK HO, USC PHARM D. CANDIDATE OF 2017 MENTOR: DR. CRAIG STERN, PHARMD, MBA, RPH, FASCP, FASHP, FICA, FLMI, FAMCP RENIN-ANGIOTENSIN
ANGIOTENSIN II RECEPTOR BLOCKERS: MORE THAN THE ALTERNATIVE PRESENTATION BY: PATRICK HO, USC PHARM D. CANDIDATE OF 2017 MENTOR: DR. CRAIG STERN, PHARMD, MBA, RPH, FASCP, FASHP, FICA, FLMI, FAMCP RENIN-ANGIOTENSIN
Lack of Effect of Beta-blocker Therapy in Patients with ST-elevation Acute Myocardial Infarction in PCI Era
 Lack of Effect of Beta-blocker Therapy in Patients with ST-elevation Acute Myocardial Infarction in PCI Era B. Bao 1, N. Ozasa 1, T. Morimoto 2, Y. Furukawa 3, M. Shirotani 4, H. Ogawa 5, C. Tei 6, H.
Lack of Effect of Beta-blocker Therapy in Patients with ST-elevation Acute Myocardial Infarction in PCI Era B. Bao 1, N. Ozasa 1, T. Morimoto 2, Y. Furukawa 3, M. Shirotani 4, H. Ogawa 5, C. Tei 6, H.
SESSION 5 2:20 3:35 pm
 SESSION 2:2 3:3 pm Strategies to Reduce Cardiac Risk for Noncardiac Surgery SPEAKER Lee A. Fleisher, MD Presenter Disclosure Information The following relationships exist related to this presentation:
SESSION 2:2 3:3 pm Strategies to Reduce Cardiac Risk for Noncardiac Surgery SPEAKER Lee A. Fleisher, MD Presenter Disclosure Information The following relationships exist related to this presentation:
Use of Sacubitril/Valsartan in Heart Failure
 Use of Sacubitril/Valsartan in Heart Failure & the PARADIGM-HF trial Sarah Mackenzie, PharmD student, University of Toronto Presentation Outline Overview of: Entresto PARADIGM-HF trial Critical Appraisal
Use of Sacubitril/Valsartan in Heart Failure & the PARADIGM-HF trial Sarah Mackenzie, PharmD student, University of Toronto Presentation Outline Overview of: Entresto PARADIGM-HF trial Critical Appraisal
The Strategic Reperfusion Early After STEMI study Implications for clinical practice
 The Strategic Reperfusion Early After STEMI study Implications for clinical practice Robert C. Welsh, MD, FRCPC Associate Professor of Medicine Director, Adult Cardiac Catheterization and Interventional
The Strategic Reperfusion Early After STEMI study Implications for clinical practice Robert C. Welsh, MD, FRCPC Associate Professor of Medicine Director, Adult Cardiac Catheterization and Interventional
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST Multivessel disease and cardiogenic shock: CABG is the optimal revascularization therapy. Contra Prof. Christian JM Vrints Cardiogenic Shock Spiral Acute Myocardial
DECLARATION OF CONFLICT OF INTEREST Multivessel disease and cardiogenic shock: CABG is the optimal revascularization therapy. Contra Prof. Christian JM Vrints Cardiogenic Shock Spiral Acute Myocardial
Acute Coronary Syndrome. Sonny Achtchi, DO
 Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
7 th Munich Vascular Conference
 7 th Munich Vascular Conference Secondary prevention of major cardiovascular events in patients with CHD or PAD - What can we learn from EUCLID and COMPASS, evaluating Clopidogrel, Ticagrelor and Univ.-Prof.
7 th Munich Vascular Conference Secondary prevention of major cardiovascular events in patients with CHD or PAD - What can we learn from EUCLID and COMPASS, evaluating Clopidogrel, Ticagrelor and Univ.-Prof.
Revascularization after Drug-Eluting Stent Implantation or Coronary Artery Bypass Surgery for Multivessel Coronary Disease
 Impact of Angiographic Complete Revascularization after Drug-Eluting Stent Implantation or Coronary Artery Bypass Surgery for Multivessel Coronary Disease Young-Hak Kim, Duk-Woo Park, Jong-Young Lee, Won-Jang
Impact of Angiographic Complete Revascularization after Drug-Eluting Stent Implantation or Coronary Artery Bypass Surgery for Multivessel Coronary Disease Young-Hak Kim, Duk-Woo Park, Jong-Young Lee, Won-Jang
STEMI update. Vijay Krishnamoorthy M.D. Interventional Cardiology
 STEMI update Vijay Krishnamoorthy M.D. Interventional Cardiology OVERVIEW Current Standard of Care in Management of STEMI Update in management of STEMI Pre-Cath Lab In the ED/Office/EMS. Cath Lab Post
STEMI update Vijay Krishnamoorthy M.D. Interventional Cardiology OVERVIEW Current Standard of Care in Management of STEMI Update in management of STEMI Pre-Cath Lab In the ED/Office/EMS. Cath Lab Post
Saudi Arabia February Pr Michel KOMAJDA. Université Pierre et Marie Curie Hospital Pitié Salpétrière
 Prevention of Cardiovascular events with Ivabradine: The SHIFT Study Saudi Arabia February 2011 Pr Michel KOMAJDA Université Pierre et Marie Curie Hospital Pitié Salpétrière Paris FRANCE Declaration Of
Prevention of Cardiovascular events with Ivabradine: The SHIFT Study Saudi Arabia February 2011 Pr Michel KOMAJDA Université Pierre et Marie Curie Hospital Pitié Salpétrière Paris FRANCE Declaration Of
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
DES in primary PCI for STEMI: contra
 DES in primary PCI for STEMI: contra Philippe Gabriel Steg Department of Cardiology Hôpital Bichat Claude Bernard, AP-HP Université Paris VII Denis Diderot INSERM U-698 Paris, France Ph. Gabriel Steg -
DES in primary PCI for STEMI: contra Philippe Gabriel Steg Department of Cardiology Hôpital Bichat Claude Bernard, AP-HP Université Paris VII Denis Diderot INSERM U-698 Paris, France Ph. Gabriel Steg -
Relationship between body mass index, coronary disease extension and clinical outcomes in patients with acute coronary syndrome
 Relationship between body mass index, coronary disease extension and clinical outcomes in patients with acute coronary syndrome Helder Dores, Luís Bronze Carvalho, Ingrid Rosário, Sílvio Leal, Maria João
Relationship between body mass index, coronary disease extension and clinical outcomes in patients with acute coronary syndrome Helder Dores, Luís Bronze Carvalho, Ingrid Rosário, Sílvio Leal, Maria João
Polypharmacy - arrhythmic risks in patients with heart failure
 Influencing sudden cardiac death by pharmacotherapy Polypharmacy - arrhythmic risks in patients with heart failure Professor Dan Atar Head, Dept. of Cardiology Oslo University Hospital Ullevål Norway 27.8.2012
Influencing sudden cardiac death by pharmacotherapy Polypharmacy - arrhythmic risks in patients with heart failure Professor Dan Atar Head, Dept. of Cardiology Oslo University Hospital Ullevål Norway 27.8.2012
A patient with decompensated HF
 A patient with decompensated HF Professor Michel KOMAJDA University Pierre & Marie Curie Pitie Salpetriere Hospital Department of Cardiology Paris (France) Declaration Of Interest 2010 Speaker : Servier,
A patient with decompensated HF Professor Michel KOMAJDA University Pierre & Marie Curie Pitie Salpetriere Hospital Department of Cardiology Paris (France) Declaration Of Interest 2010 Speaker : Servier,
ESC Guidelines for diagnosis and management of HF 2012: What s new? John Parissis, MD Athens, GR
 ESC Guidelines for diagnosis and management of HF 2012: What s new? John Parissis, MD Athens, GR Disclosures ALARM INVESTIGATOR RESEARCH GRANTS BY ABBOTT USA AND ORION PHARMA The principal changes from
ESC Guidelines for diagnosis and management of HF 2012: What s new? John Parissis, MD Athens, GR Disclosures ALARM INVESTIGATOR RESEARCH GRANTS BY ABBOTT USA AND ORION PHARMA The principal changes from
Side Branch Occlusion
 Side Branch Occlusion Mechanism, Outcome, and How to avoid it From COBIS II Registry Hyeon-Cheol Gwon Cardiac&Vascular Center, Samsung Medical Center Sungkyunkwan University School of Medicine SB occlusion
Side Branch Occlusion Mechanism, Outcome, and How to avoid it From COBIS II Registry Hyeon-Cheol Gwon Cardiac&Vascular Center, Samsung Medical Center Sungkyunkwan University School of Medicine SB occlusion
Journal of the American College of Cardiology Vol. 35, No. 4, by the American College of Cardiology ISSN /00/$20.
 Journal of the American College of Cardiology Vol. 35, No. 4, 2000 2000 by the American College of Cardiology ISSN 0735-1097/00/$20.00 Published by Elsevier Science Inc. PII S0735-1097(99)00643-9 Early
Journal of the American College of Cardiology Vol. 35, No. 4, 2000 2000 by the American College of Cardiology ISSN 0735-1097/00/$20.00 Published by Elsevier Science Inc. PII S0735-1097(99)00643-9 Early
Quale terapia antiaggregante nello STEMI? Prasugrel vs ticagrelor
 Quale terapia antiaggregante nello STEMI? Prasugrel vs ticagrelor Leonardo Bolognese Cardiovascular Department, Arezzo, Italy Platelet Reactivity in Patients with STEMI Undergoing Primary PCI Campo G et
Quale terapia antiaggregante nello STEMI? Prasugrel vs ticagrelor Leonardo Bolognese Cardiovascular Department, Arezzo, Italy Platelet Reactivity in Patients with STEMI Undergoing Primary PCI Campo G et
Cardiovascular Health Practice Guideline Outpatient Management of Coronary Artery Disease 2003
 Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
Current Advances and Best Practices in Acute STEMI Management A pharmacoinvasive approach
 Current Advances and Best Practices in Acute STEMI Management A pharmacoinvasive approach Frans Van de Werf, MD, PhD University Hospitals, Leuven, Belgium Frans Van de Werf: Disclosures Research grants
Current Advances and Best Practices in Acute STEMI Management A pharmacoinvasive approach Frans Van de Werf, MD, PhD University Hospitals, Leuven, Belgium Frans Van de Werf: Disclosures Research grants
SHOULD A REGIONAL STEMI CENTRE ONLY OFFER PRIMARY PCI?
 SHOULD A REGIONAL STEMI CENTRE ONLY OFFER PRIMARY PCI? Kurt Huber, MD 3 Department of Internal Medicine, Cardiology and Intensive Care Medicine, Wilhelminenhospital, Vienna, Austria Disclosures DISCLOSURE
SHOULD A REGIONAL STEMI CENTRE ONLY OFFER PRIMARY PCI? Kurt Huber, MD 3 Department of Internal Medicine, Cardiology and Intensive Care Medicine, Wilhelminenhospital, Vienna, Austria Disclosures DISCLOSURE
What s new in 2016 Guidelines of the European Society of Cardiology? HEART FAILURE. Marc Ferrini (Lyon Fr)
") What s new in 2016 Guidelines of the European Society of Cardiology? HEART FAILURE Marc Ferrini (Lyon Fr) Palermo (I) 1 04 2017 Consulting Fees, Honoraria: BAYER PHARMA BOEHRINGER INGELHEIM BRISTOL MEYERS
What s new in 2016 Guidelines of the European Society of Cardiology? HEART FAILURE Marc Ferrini (Lyon Fr) Palermo (I) 1 04 2017 Consulting Fees, Honoraria: BAYER PHARMA BOEHRINGER INGELHEIM BRISTOL MEYERS
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Cardiovascular Guideline-Driven Pharmacotherapies: Optimizing Management
 Cardiovascular Guideline-Driven Pharmacotherapies: Optimizing Management David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management
Cardiovascular Guideline-Driven Pharmacotherapies: Optimizing Management David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management
Effect of upstream clopidogrel treatment in patients with ST-segment elevation myocardial infarction undergoing primary PCI
 Effect of upstream clopidogrel treatment in patients with ST-segment elevation myocardial infarction undergoing primary PCI Dr Sasha Koul, MD Dept of Cardiology, Lund University Hospital, Lund, Sweden
Effect of upstream clopidogrel treatment in patients with ST-segment elevation myocardial infarction undergoing primary PCI Dr Sasha Koul, MD Dept of Cardiology, Lund University Hospital, Lund, Sweden
2010 ACLS Guidelines. Primary goals of therapy for patients
 2010 ACLS Guidelines Part 10: Acute Coronary Syndrome Present : 內科 R1 鍾伯欣 Supervisor: F1 吳亮廷 991110 Primary goals of therapy for patients of ACS Reduce the amount of myocardial necrosis that occurs in
2010 ACLS Guidelines Part 10: Acute Coronary Syndrome Present : 內科 R1 鍾伯欣 Supervisor: F1 吳亮廷 991110 Primary goals of therapy for patients of ACS Reduce the amount of myocardial necrosis that occurs in
THERE ARE TWO SUBMISSION CRITERIA FOR THIS MEASURE: 1) Patients who are 18 years and older with a diagnosis of CAD with LVEF < 40%
 Patients who are 18 years and older with a diagnosis of CAD with LVEF < 40%") Quality ID #118 (NQF 0066): Coronary Artery Disease (CAD): Angiotensin-Converting Enzyme (ACE) Inhibitor or Angiotensin Receptor Blocker (ARB) Therapy - Diabetes or Left Ventricular Systolic Dysfunction
Quality ID #118 (NQF 0066): Coronary Artery Disease (CAD): Angiotensin-Converting Enzyme (ACE) Inhibitor or Angiotensin Receptor Blocker (ARB) Therapy - Diabetes or Left Ventricular Systolic Dysfunction
Rikshospitalet, University of Oslo
 Rikshospitalet, University of Oslo Preventing heart failure by preventing coronary artery disease progression European Society of Cardiology Dyslipidemia 29.08.2010 Objectives The trends in cardiovascular
Rikshospitalet, University of Oslo Preventing heart failure by preventing coronary artery disease progression European Society of Cardiology Dyslipidemia 29.08.2010 Objectives The trends in cardiovascular
Non ST Elevation-ACS. Michael W. Cammarata, MD
 Non ST Elevation-ACS Michael W. Cammarata, MD Case Presentation 65 year old man PMH: CAD s/p stent in 2008 HTN HLD Presents with chest pressure, substernally and radiating to the left arm and jaw, similar
Non ST Elevation-ACS Michael W. Cammarata, MD Case Presentation 65 year old man PMH: CAD s/p stent in 2008 HTN HLD Presents with chest pressure, substernally and radiating to the left arm and jaw, similar
Quality Payment Program: Cardiology Specialty Measure Set
 Quality Payment Program: Cardiology Specialty Set Title Number CMS Reporting Method(s) Heart Failure (HF): Angiotensin- Converting Enzyme (ACE) Inhibitor or Angiotensin Receptor Blocker (ARB) Therapy for
Quality Payment Program: Cardiology Specialty Set Title Number CMS Reporting Method(s) Heart Failure (HF): Angiotensin- Converting Enzyme (ACE) Inhibitor or Angiotensin Receptor Blocker (ARB) Therapy for
STEMI 2014 YAHYA KIWAN. Consultant Cardiologist Head Of Cardiology Belhoul Specialty Hospital
 STEMI 2014 YAHYA KIWAN Consultant Cardiologist Head Of Cardiology Belhoul Specialty Hospital Aspiration Thrombectomy Manual aspiration thrombectomy is reasonable for patients undergoing primary PCI. I
STEMI 2014 YAHYA KIWAN Consultant Cardiologist Head Of Cardiology Belhoul Specialty Hospital Aspiration Thrombectomy Manual aspiration thrombectomy is reasonable for patients undergoing primary PCI. I
4. Which survey program does your facility use to get your program designated by the state?
 STEMI SURVEY Please complete one survey for each TCD designation you have in your facility. There would be a maximum of three surveys completed if your facility was designated as a trauma, stroke and STEMI
STEMI SURVEY Please complete one survey for each TCD designation you have in your facility. There would be a maximum of three surveys completed if your facility was designated as a trauma, stroke and STEMI
Management of ST-elevation myocardial infarction Update 2009 Late comers: which options?
 European Society of Cardiology Annual Session 2009 Management of ST-elevation myocardial infarction Update 2009 Late comers: which options? Antonio Abbate, MD Assistant Professor of Medicine Virginia Commonwealth
European Society of Cardiology Annual Session 2009 Management of ST-elevation myocardial infarction Update 2009 Late comers: which options? Antonio Abbate, MD Assistant Professor of Medicine Virginia Commonwealth
ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure
 Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Cardiovascular Health Nova Scotia Update to Antiplatelet Sections of the Nova Scotia Guidelines for Acute Coronary Syndromes, 2008.
 Cardiovascular Health Nova Scotia Update to Antiplatelet Sections of the Nova Scotia Guidelines for Acute Coronary Syndromes, 2008. ST Elevation Myocardial Infarction (STEMI)-Acute Coronary Syndrome Guidelines:
Cardiovascular Health Nova Scotia Update to Antiplatelet Sections of the Nova Scotia Guidelines for Acute Coronary Syndromes, 2008. ST Elevation Myocardial Infarction (STEMI)-Acute Coronary Syndrome Guidelines:
Update on pharmacological treatment of heart failure. Aldo Pietro Maggioni, MD, FESC ANMCO Research Center Firenze, Italy
 Update on pharmacological treatment of heart failure Aldo Pietro Maggioni, MD, FESC ANMCO Research Center Firenze, Italy Presenter Disclosures Dr. Maggioni : Serving in Committees of studies sponsored
Update on pharmacological treatment of heart failure Aldo Pietro Maggioni, MD, FESC ANMCO Research Center Firenze, Italy Presenter Disclosures Dr. Maggioni : Serving in Committees of studies sponsored
2012 Core Measures. Acute Myocardial Infarction (AMI)
") 2012 Core Measures Acute Myocardial Infarction (AMI) Aspirin at Arrival Aspirin Prescribed at Discharge Angiotensin converting enzyme inhibitor (ACEI) or angiotensin receptor blocker (ARB) for left ventricular
2012 Core Measures Acute Myocardial Infarction (AMI) Aspirin at Arrival Aspirin Prescribed at Discharge Angiotensin converting enzyme inhibitor (ACEI) or angiotensin receptor blocker (ARB) for left ventricular