PCI for Stable Ischemic Heart Disease: What Happened in the Last Week?
|
|
|
- Lizbeth Doyle
- 6 years ago
- Views:
Transcription

1 PCI for Stable Ischemic Heart Disease: What Happened in the Last Week? Ajay J. Kirtane, MD, SM Center for Interventional Vascular Therapy Columbia University Medical Center / NewYork Presbyterian
2 Disclosure Statement of Financial Interest Ajay J. Kirtane Institutional grants to Columbia University and/or Cardiovascular Research Foundation from Medtronic, Boston Scientific, Abbott Vascular, Abiomed, CSI, CathWorks, Siemens, Philips, ReCor Medical
3 Last Thursday Morning (at TCT)
4 Objective Randomised Blinded Investigation with optimal medical Therapy of Angioplasty in stable angina (ORBITA) Rasha Al-Lamee, MA (Oxon) MB BS MRCP Imperial College London

5 Inclusion criteria Stable angina One or more 70% stenosis in a single vessel Suitable for PCI

6 Randomization Trial design Enrolment assessment CCS SAQ EQ-5D-5L MEDICAL OPTIMIZATION PHASE Prerandomization assessment CCS SAQ EQ-5D-5L Exercise test Stress echo Blinded procedure Research angiogram: ifr, FFR Sedation PCI BLINDED FOLLOW UP PHASE Follow-up Assessment CCS SAQ EQ-5D-5L Exercise test Stress echo Placebo Six weeks Six weeks
7 ORBITA trial 230 enrolled Dec Jul 2017 in 5 UK sites Medical optimization phase 30 patients exited 200 patients randomized PCI (n=105) Placebo (n=95) Blinded follow-up phase 4 patients did not complete follow-up Follow-up (n=105) Follow-up (n=91)

8




9 Number of antianginal drugs Medical therapy optimization PCI Placebo % 1.90% 12.40% 13.30% 24.80% 22.90% 31.60% 2.10% 23.20% 4.20% 5.30% 18.90% % 38.90% % 63.80% 74.70% 71.60% 24.20% % 1.00% Enrolment Pre-randomization Follow-up 5.30% Enrolment Pre-randomization Follow-up
10 Stenosis severity Area stenosis by QCA (%) Area stenosis by QCA (%) PCI PCI n = (SD ) (SD 10.2) Placebo Placebo n = (SD ) (SD 10.3) P FFR FFR (SD 0.16) (SD 0.16) (SD 0.16) (SD 0.16) ifr ifr (SD 0.22) (SD 0.22) (SD 0.21) (SD 0.21)
11 Change in exercise time (seconds) Primary endpoint result Change in total exercise time (SD 86.3) p=0.001 PCI 11.8 (SD 93.3) p=0.235 Placebo Error bars are standard errors of the mean

 p=0.")
12 Change in exercise time (seconds) Primary endpoint result Change in total exercise time (SD 86.3) p= sec (-8.9 to 42.0) p= PCI 11.8 (SD 93.3) p=0.235 Placebo Error bars are standard errors of the mean
13 Secondary endpoint results Blinded evaluation of ischaemia reduction Peak stress wall motion index score PCI n = 80 Placebo n = 57 Pre-randomization 1.11 (0.18) 1.11 (0.18) Follow-up Δ (Pre-randomization to follow-up) Difference in Δ between arms 1.03 (0.06) (0.17) p< (0.19) 0.02 (0.16) p= (-0.15 to -0.04) p=0.0011
14 Secondary endpoint results: Quality of Life Scores PCI Placebo Baseline 6 weeks Baseline 6 weeks SAQ Physical Limitation SAQ Anginal Frequency SAQ Angina Stability Bold values represent significant changes from baseline No between-group differences between arms were detected
15 Secondary endpoint results CCS class improved in both groups CCS class at enrolment CCS class at prerandomization CCS class at followup CCS IV 37% 40% 24% 33% 0% 1% 12% 16% CCS III 35% 34% CCS II CCS I CCS 0 61% 57% 2% 3% PCI Placebo 53% 14% 9% PCI 43% 11% 14% Placebo 13% 39% PCI 20% 29% Placebo
16 ORBITA Results Summary PCI relieved hemodynamic significance of stenoses by physiologic criteria and relieved ischemia by DSE (placebo did not) Exercise time increased by +28 seconds in PCI arm (but not significantly in placebo arm: +12 seconds) Difference between arms (16 seconds) was not significant Most QoL Measures were no different between arms but improved in both (slightly greater with PCI)
17 The implications of ORBITA are profound and farreaching. First and foremost, the results of ORBITA show unequivocally that there are no benefits for PCI compared with medical therapy for stable angina, even when angina is refractory to medical therapy. Based upon these data, all cardiology guidelines should be revised to downgrade the recommendation for PCI in patients with angina despite medical therapy.


18




19 Two Goals of Therapy in Patients with Stable CAD 1. Improve Symptoms and Quality of Life Measured by soft endpoints (i.e. angina/qol scales) 2. Improve Prognosis Measured by hard endpoints (i.e. death, MI)
20 Appropriateness of Revascularization and Outcomes in the UK Studies using [the RAND] method have shown that overuse of invasive techniques in the management of coronary disease is uncommon, and attention has turned to the issue of underuse Angina at 1 year Hemingway et al. NEJM 2001




21 COURAGE: Effect of Medical Therapy SAQ Freedom From Angina PCI + OMT OMT p Baseline 21% 23% NS 3 Months 53% 42% < Year 57% 50% Years 59% 53% Years 59% 56% NS Minimal DES Use and 32% of Medically Treated Patients in the Trial Crossed Over to PCI Weintraub et al, NEJM 2008


 Significantly less use of Ca +2 channel")
 - 3 years (43% vs. 50%) - 5 years (42% vs.")
22 Freedom from Anti-anginal Meds Despite 32% XO to PCI in the OMT group PCI + OMT compared to OMT resulted in: Significantly less use of nitrates at: - 1 year (53% vs. 67%) - 3 years (47% vs. 61%) - 5 years (40% vs. 57%) Significantly less use of Ca +2 channel blockers at: - 1 year (40% vs. 49%) - 3 years (43% vs. 50%) - 5 years (42% vs. 52%) Boden WE et al. NEJM 2007;356:
 J.")
23 Crossover Rate COURAGE: Cross-Overs from OMT Arm 50% 45% 40% 35% 30% 25% 20% 15% 10% 5% 0% daily weekly monthly none Baseline SAQ Angina Frequency Score In a matched analysis, MT with 1 st yr x-over was not associated with death, MI, or SAQ but was associated with worse health status and unstable angina admissions (OR 2.78, 95% CI [1.1,7.5], p=0.04) J. Spertus et al, TCT 2010 and Circ CV Qual Outcomes 2013

24 Cumulative Incidence of Worsening Angina: BARI 2D Additionally, among patients with angina at baseline, freedom from angina after randomization was higher among revascularized patients compared to medical therapy Dagenais et al, Circulation 2011
25 FAME-2: Stable CAD patients scheduled for 1, 2 or 3 vessel DES-PCI N = 1220 Randomized Trial FFR in all target lesions Registry At least 1 stenosis with FFR 0.80 (n=888) When all FFR > 0.80 (n=332) Randomization 1:1 PCI + MT 73% MT 27% MT 50% randomly assigned to FU Follow-up after 1, 6 months, 1, 2, 3 and 5 years

26 % with CCS II-IV Angina FAME-2: Quality of Life % of Patients with Class II-IV Angina at each Time Point

27 FAME-2: Quality of Life Mean Number of Antianginal Medications/Patient at each Time Point


28 Results: Clinical Outcome Three Year Rate of Death, MI, or Urgent Revascularization

29 Results: Clinical Outcome Three Year Rate of Death, MI, or Urgent Revascularization *P value compares PCI + MT patients with MT patients

30 FAME-2: Costs
31 Key Characteristics of the ORBITA Population Single vessel disease ~30% FFR negative But angiographically legitimate (real-world practice) Intense medical therapy prior to randomization At randomization, patients symptoms were well-controlled as assessed by SAQ Approximately monthly angina Good exercise tolerance by VO2Max Minimal ischemia by DSE and DTS

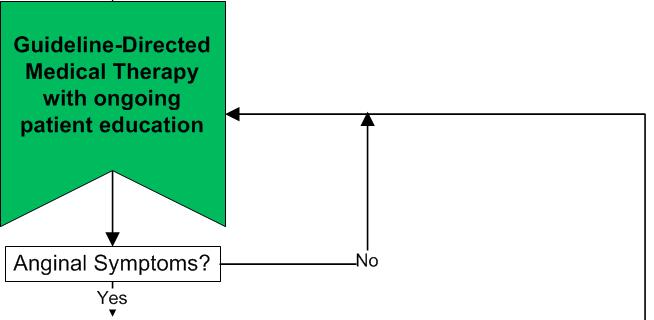
32 Algorithm for GDMT for SIHD

 0.")
33 SYNTAX: Generic QOL and Utilities 55 SF - 36 Physical Component Summary SF - 36 Mental Component Summary P<0.001 P=0.50 P=0.07 P<0.001 P=0.23 P= Baseline 1 month 6 months 12 months 30 Baseline 1 month 6 months 12 months 1 EQ - 5D Utilities (US) PCI 0.9 CABG P<0.001 P=0.16 P=0.99 Quality Adjusted Life Years D = 0.02 (P<0.01) 0.5 Baseline 1 month 6 months 12 months SYNTAX 3VD 5-year Outcomes TCT 2012 Mohr 23 October 2012 Slide 60 Cohen DJ et al. NEJM 2011;364:

34 Quality of Life Angina frequency, physical limitations, and quality-of-life domains of the SAQ assessed at baseline, at 1, 6, and 12 months, and annually thereafter. SAQ Angina Frequency SAQ Physical Limitations SAQ Quality of Life Adjusted: * P<0.05 favoring PCI *P<0.05 favoring CABG Abdallah MS et al. JAMA 2013;on-line

35 SAQ-Angina Frequency 100 PCI CABG Δ = 1.5 p = 0.03 Δ = -0.3 p = Months Δ = -0.8 p = 0.21 Baron et al, JACC 2017


36 1: n=5 2: n=5 3: n=13 4: n=8 5: n=8 6: n=7 7: n=5 8: n=14 9: n=7 10: n=6 11: n=8 12: n=5 13: n=5 14: n=15 15: n=18 16: n=21 17: n=8 18: n=6 19: n=9 20: n=5 21: n=15 22: n=6 23: n=15 24: n=6 25: n=6 26: n=7 Rates of Under-recognition APPEAR: Under-recognition of Angina Individual Physician Reporting compared with SAQ 100% 80% 60% 40% 20% 0% Physicians in APPEAR: Number of Patients Seen Arnold, S. et al. Circ Cardiovasc Qual Outcomes. 2016; 9:00-00

37 How Do Our Patients with Real Symptoms Actually Feel After Revascularization?

38 GDMT vs. Revasc for Stable Ischemic Heart Disease Factors favoring GDMT Factors favoring Revasc + GDMT Symptoms: Exercise capacity: Ischemia/Risk: Anti-anginal drug tolerance: Revasc. risk (pt factors, cor anat): DAPT compliance: None to mild Normal None to mild Good High Poor Moderate to severe Reduced Moderate to severe Poor Low Good Adapted from G. Stone







39 An It Unnecessary wasn t their Procedure? LAD! * This is really American medicine at its worst - Steven Nissen He is the poster child for the inappropriate use of stenting - David Brown *G. W. Bush, CRT 2014
Management of stable CAD FFR guided therapy: the new gold standard
 Management of stable CAD FFR guided therapy: the new gold standard Suleiman Kharabsheh, MD Director; CCU, Telemetry and CHU Associate professor of Cardiology, Alfaisal Univ. KFHI - KFSHRC Should patients
Management of stable CAD FFR guided therapy: the new gold standard Suleiman Kharabsheh, MD Director; CCU, Telemetry and CHU Associate professor of Cardiology, Alfaisal Univ. KFHI - KFSHRC Should patients
The Case for PCI as the Preferred Therapy in Most Patients with Chronic Stable Angina
 The Case for PCI as the Preferred Therapy in Most Patients with Chronic Stable Angina Ajay J. Kirtane,, MD Columbia University Medical Center The Cardiovascular Research Foundation Conflict of Interest
The Case for PCI as the Preferred Therapy in Most Patients with Chronic Stable Angina Ajay J. Kirtane,, MD Columbia University Medical Center The Cardiovascular Research Foundation Conflict of Interest
Benefit of Performing PCI Based on FFR
 Benefit of Performing PCI Based on FFR William F. Fearon, MD Associate Professor Director, Interventional Cardiology Stanford University Medical Center Benefit of FFR-Guided PCI FFR-Guided PCI vs. Angiography-Guided
Benefit of Performing PCI Based on FFR William F. Fearon, MD Associate Professor Director, Interventional Cardiology Stanford University Medical Center Benefit of FFR-Guided PCI FFR-Guided PCI vs. Angiography-Guided
Left Main Intervention: Where are we in 2015?
 Left Main Intervention: Where are we in 2015? David A. Cox, MD FSCAI Director, Cardiology Research Associate Director, Cardiac Cath Lab Lehigh Valley Health Network Allentown, PA Fall Fellows Course Laa
Left Main Intervention: Where are we in 2015? David A. Cox, MD FSCAI Director, Cardiology Research Associate Director, Cardiac Cath Lab Lehigh Valley Health Network Allentown, PA Fall Fellows Course Laa
3 Year Clinical Outcome and Cost-Effectiveness of FFR- Guided PCI in Stable Patients with Coronary Artery Disease: FAME 2 Trial
 3 Year Clinical Outcome and Cost-Effectiveness of FFR- Guided PCI in Stable Patients with Coronary Artery Disease: FAME 2 Trial William F. Fearon, MD, Takeshi Nishi, MD, Bernard De Bruyne, MD, PhD, Derek
3 Year Clinical Outcome and Cost-Effectiveness of FFR- Guided PCI in Stable Patients with Coronary Artery Disease: FAME 2 Trial William F. Fearon, MD, Takeshi Nishi, MD, Bernard De Bruyne, MD, PhD, Derek
Relations of Interest
 Relations of Interest Consulting Fees on my behalf go to the Cardiovascular Research Center Aalst Contracted Research between the Cardiovascular Research Center Aalst and several pharmaceutical and device
Relations of Interest Consulting Fees on my behalf go to the Cardiovascular Research Center Aalst Contracted Research between the Cardiovascular Research Center Aalst and several pharmaceutical and device
Fractional Flow Reserve: Review of the latest data
 Fractional Flow Reserve: Review of the latest data Michalis Hamilos, MD, PhD, FESC University Hospital of Heraklion Fractional Flow Reserve (FFR) Coronary angiography does not always tell the truth Most
Fractional Flow Reserve: Review of the latest data Michalis Hamilos, MD, PhD, FESC University Hospital of Heraklion Fractional Flow Reserve (FFR) Coronary angiography does not always tell the truth Most
PCIs on Intermediate Lesions NCDR Cath-PCI Registry
 Practical Application Of Coronary Physiology in The Cath Lab Talal T Attar, MD, MBA, FACC PCIs on Intermediate Lesions NCDR Cath-PCI Registry Fraction of stenoses 50-70% treated with PCI without further
Practical Application Of Coronary Physiology in The Cath Lab Talal T Attar, MD, MBA, FACC PCIs on Intermediate Lesions NCDR Cath-PCI Registry Fraction of stenoses 50-70% treated with PCI without further
Trial. International Study of Comparative Health Effectiveness with Medical and Invasive Approaches
 Trial International Study of Comparative Health Effectiveness with Medical and Invasive Approaches Stable Ischemic Heart Disease What is the best initial management strategy for patients with SIHD? What
Trial International Study of Comparative Health Effectiveness with Medical and Invasive Approaches Stable Ischemic Heart Disease What is the best initial management strategy for patients with SIHD? What
Controversies in Coronary Revascularization. Atlanta CCU April 15, 2016
 Controversies in Coronary Revascularization Atlanta CCU April 15, 2016 Habib Samady MD FACC FSCAI Professor of Medicine Director, Interventional Cardiology, Emory University Director, Cardiac Catheterization
Controversies in Coronary Revascularization Atlanta CCU April 15, 2016 Habib Samady MD FACC FSCAI Professor of Medicine Director, Interventional Cardiology, Emory University Director, Cardiac Catheterization
Cost-Effectiveness of Fractional Flow Reserve
 Cost-Effectiveness of Fractional Flow Reserve William F. Fearon, MD Associate Professor of Medicine Director, Interventional Cardiology Stanford University Medical Center Cost-Effectiveness of FFR What
Cost-Effectiveness of Fractional Flow Reserve William F. Fearon, MD Associate Professor of Medicine Director, Interventional Cardiology Stanford University Medical Center Cost-Effectiveness of FFR What
Angor Stable: de COURAGE à FAME 2. Maladie coronaire stable et coronarographie en De COURAGE à FAME 2
 Maladie coronaire stable et coronarographie en 2013 De COURAGE à FAME 2 Bernard De Bruyne, MD, PhD Cardiovascular Center Aalst OLV-Clinic Aalst, Belgium COURAGE Trial Aim To compare optimal medical therapy
Maladie coronaire stable et coronarographie en 2013 De COURAGE à FAME 2 Bernard De Bruyne, MD, PhD Cardiovascular Center Aalst OLV-Clinic Aalst, Belgium COURAGE Trial Aim To compare optimal medical therapy
Quality of Life After Everolimus- Eluting Stents or Bypass Surgery for Treatment of Left Main Coronary Artery Disease:
 Quality of Life After Everolimus- Eluting Stents or Bypass Surgery for Treatment of Left Main Coronary Artery Disease: Results from the EXCEL Trial Suzanne J. Baron MD MSC on behalf of the EXCEL Investigators
Quality of Life After Everolimus- Eluting Stents or Bypass Surgery for Treatment of Left Main Coronary Artery Disease: Results from the EXCEL Trial Suzanne J. Baron MD MSC on behalf of the EXCEL Investigators
FRACTIONAL FLOW RESERVE: STANDARD OF CARE
 FRACTIONAL FLOW RESERVE: FROM INVESTIGATIONAL TOOL TO STANDARD OF CARE TCT ASIA Seoul, Korea, april 26 th, 2012 Nico H. J. Pijls, MD, PhD Catharina Hospital, Eindhoven, The Netherlands FRACTIONAL FLOW
FRACTIONAL FLOW RESERVE: FROM INVESTIGATIONAL TOOL TO STANDARD OF CARE TCT ASIA Seoul, Korea, april 26 th, 2012 Nico H. J. Pijls, MD, PhD Catharina Hospital, Eindhoven, The Netherlands FRACTIONAL FLOW
FFR in Multivessel Disease
 FFR in Multivessel Disease April, 26 2013 Coronary Physiology in the Catheterization Laboratory Location: European Heart House, Nice, France Pim A.L. Tonino, MD, PhD Hartcentrum, Eindhoven, the Netherlands
FFR in Multivessel Disease April, 26 2013 Coronary Physiology in the Catheterization Laboratory Location: European Heart House, Nice, France Pim A.L. Tonino, MD, PhD Hartcentrum, Eindhoven, the Netherlands
Left Main Intervention: Will it become standard of care?
 Left Main Intervention: Will it become standard of care? David Cox, MD FSCAI, FACC Director, Interventional Cardiology Research Associate Director, Cardiac Cath Lab Lehigh Valley Health Network Allentown,
Left Main Intervention: Will it become standard of care? David Cox, MD FSCAI, FACC Director, Interventional Cardiology Research Associate Director, Cardiac Cath Lab Lehigh Valley Health Network Allentown,
How to approach non-infarct related artery disease in patients with STEMI in a limited resource setting
 How to approach non-infarct related artery disease in patients with STEMI in a limited resource setting Ahmed A A Suliman, MBBS, FACP, FESC Associate Professor, University of Khartoum Interventional Cardiologist,
How to approach non-infarct related artery disease in patients with STEMI in a limited resource setting Ahmed A A Suliman, MBBS, FACP, FESC Associate Professor, University of Khartoum Interventional Cardiologist,
Treatment Options for Angina
 Treatment Options for Angina Interventional Cardiology Perspective Michael A. Robertson, M.D. 10/30/10 Prevalence of CAD in USA 15 million Americans with CAD 2 million diagnostic catheterizations 1 million
Treatment Options for Angina Interventional Cardiology Perspective Michael A. Robertson, M.D. 10/30/10 Prevalence of CAD in USA 15 million Americans with CAD 2 million diagnostic catheterizations 1 million
Fractional Flow Reserve: Basics, FAME 1, FAME 2. William F. Fearon, MD Associate Professor Stanford University Medical Center
 Fractional Flow Reserve: Basics, FAME 1, FAME 2 William F. Fearon, MD Associate Professor Stanford University Medical Center Conflict of Interest Advisory Board for HeartFlow Research grant from St. Jude
Fractional Flow Reserve: Basics, FAME 1, FAME 2 William F. Fearon, MD Associate Professor Stanford University Medical Center Conflict of Interest Advisory Board for HeartFlow Research grant from St. Jude
Advances in Cardiovascular Diagnosis and Therapy. No disclosure or conflicts. Outline
 Advances in Cardiovascular Diagnosis and Therapy Firas Zahr, MD Assistant Professor of Medicine Interventional Cardiology University Of Iowa No disclosure or conflicts Outline What is new with revascularization?
Advances in Cardiovascular Diagnosis and Therapy Firas Zahr, MD Assistant Professor of Medicine Interventional Cardiology University Of Iowa No disclosure or conflicts Outline What is new with revascularization?
Better CABGs vs Better PCI Devices
 CABG vs PCI 2017 Multivessel Coronary Disease Better CABGs vs Better PCI Devices ACC New York, Dec 8, 2017 No Disclosures CABG vs PCI 2017 Stable Multivessel Coronary Disease 1. Are These The two Critical
CABG vs PCI 2017 Multivessel Coronary Disease Better CABGs vs Better PCI Devices ACC New York, Dec 8, 2017 No Disclosures CABG vs PCI 2017 Stable Multivessel Coronary Disease 1. Are These The two Critical
Three-Year Clinical Outcomes with Everolimus-Eluting Bioresorbable Scaffolds: Results from the Randomized ABSORB III Trial Stephen G.
 Three-Year Clinical Outcomes with Everolimus-Eluting Bioresorbable Scaffolds: Results from the Randomized ABSORB III Trial Stephen G. Ellis MD Dean J. Kereiakes MD and Gregg W. Stone MD for the ABSORB
Three-Year Clinical Outcomes with Everolimus-Eluting Bioresorbable Scaffolds: Results from the Randomized ABSORB III Trial Stephen G. Ellis MD Dean J. Kereiakes MD and Gregg W. Stone MD for the ABSORB
Management of Stable Ischemic Heart Disease. Vinay Madan MD February 10, 2018
 Management of Stable Ischemic Heart Disease Vinay Madan MD February 10, 2018 1 Disclosure No financial disclosure. 2 Overview of SIHD Diagnosis Outline of talk Functional vs. Anatomic assessment Management
Management of Stable Ischemic Heart Disease Vinay Madan MD February 10, 2018 1 Disclosure No financial disclosure. 2 Overview of SIHD Diagnosis Outline of talk Functional vs. Anatomic assessment Management
The top 5 trials in the last year: Ischemic Heart Disease
 The top 5 trials in the last year: Ischemic Heart Disease Malcolm R. Bell, MBBS, FRACP, FACC Vice Chair, Department of Cardiovascular Medicine Mayo Clinic, Rochester MN, USA 2018 MFMER 3718476-1 Conflicts
The top 5 trials in the last year: Ischemic Heart Disease Malcolm R. Bell, MBBS, FRACP, FACC Vice Chair, Department of Cardiovascular Medicine Mayo Clinic, Rochester MN, USA 2018 MFMER 3718476-1 Conflicts
Debate Should we use FFR? I will say NO.
 Debate Should we use FFR? I will say NO. Hyeon-Cheol Gwon Cardiac and Vascular Center Samsung Medical Center Sungkyunkwan University School of Medicine Dr. Hyeon-Cheol Gwon Research fund from Abbott Korea
Debate Should we use FFR? I will say NO. Hyeon-Cheol Gwon Cardiac and Vascular Center Samsung Medical Center Sungkyunkwan University School of Medicine Dr. Hyeon-Cheol Gwon Research fund from Abbott Korea
2/17/2010. Grace Lin, MD Assistant Professor of Medicine University of California, San Francisco
 Modern Management of Patients with Stable Coronary Artery Disease Grace Lin, MD Assistant Professor of Medicine University of California, San Francisco Scope of the Problem Prevalence of CAD: 17.6 million
Modern Management of Patients with Stable Coronary Artery Disease Grace Lin, MD Assistant Professor of Medicine University of California, San Francisco Scope of the Problem Prevalence of CAD: 17.6 million
James M. Kirshenbaum, MD, FACC
 James M. Kirshenbaum, MD, FACC Associate Professor of Medicine Harvard Medical School Co-Director, Clinical Cardiology Director, Acute Interventional Cardiology Brigham and Women s Hospital Boston, MA
James M. Kirshenbaum, MD, FACC Associate Professor of Medicine Harvard Medical School Co-Director, Clinical Cardiology Director, Acute Interventional Cardiology Brigham and Women s Hospital Boston, MA
Coronary Artery Disease: Revascularization (Teacher s Guide)
") Stephanie Chan, M.D. Updated 3/15/13 2008-2013, SCVMC (40 minutes) I. Objectives Coronary Artery Disease: Revascularization (Teacher s Guide) To review the evidence on whether percutaneous coronary intervention
Stephanie Chan, M.D. Updated 3/15/13 2008-2013, SCVMC (40 minutes) I. Objectives Coronary Artery Disease: Revascularization (Teacher s Guide) To review the evidence on whether percutaneous coronary intervention
Medical Rx vs PCI vs CABG
 Medical Rx vs PCI vs CABG S. Hinan Ahmed, MD Associate Professor: Cardiology and Cardiothoracic Surgery Program Director: Interventional Fellowship Program Assoc Editor: Cath and Cardiovasc Intervention
Medical Rx vs PCI vs CABG S. Hinan Ahmed, MD Associate Professor: Cardiology and Cardiothoracic Surgery Program Director: Interventional Fellowship Program Assoc Editor: Cath and Cardiovasc Intervention
ROLE OF CORONARY PRESSURE & FFR IN MULTIVESSEL DISEASE
 ROLE OF CORONARY PRESSURE & FFR IN MULTIVESSEL DISEASE Angioplasty Summit TCT ASIA Seoul, Korea, april 24th, 2008 Nico H. J. Pijls, MD, PhD Catharina Hospital, Eindhoven, The Netherlands A rather common
ROLE OF CORONARY PRESSURE & FFR IN MULTIVESSEL DISEASE Angioplasty Summit TCT ASIA Seoul, Korea, april 24th, 2008 Nico H. J. Pijls, MD, PhD Catharina Hospital, Eindhoven, The Netherlands A rather common
Assessing Myocardium at Risk: Applying SYNTAX
 Assessing Myocardium at Risk: Applying SYNTAX Farouc Jaffer MD PhD FSCAI FACC FAHA Associate Professor of Medicine, Harvard Medical School Director, CAD Program and Chronic Total Occlusion PCI Program
Assessing Myocardium at Risk: Applying SYNTAX Farouc Jaffer MD PhD FSCAI FACC FAHA Associate Professor of Medicine, Harvard Medical School Director, CAD Program and Chronic Total Occlusion PCI Program
Cindy L. Grines MD FACC FSCAI
 Cindy L. Grines MD FACC FSCAI Hofstra Northwell School of Medicine Chair, Cardiology Academic Chief of Cardiology, Northwell Health North Shore University Hospital, Manhasset NY Multivessel Disease in
Cindy L. Grines MD FACC FSCAI Hofstra Northwell School of Medicine Chair, Cardiology Academic Chief of Cardiology, Northwell Health North Shore University Hospital, Manhasset NY Multivessel Disease in
STEMI AND MULTIVESSEL CORONARY DISEASE
 STEMI AND MULTIVESSEL CORONARY DISEASE ΤΣΙΑΦΟΥΤΗΣ Ν. ΙΩΑΝΝΗΣ ΕΠΕΜΒΑΤΙΚΟΣ ΚΑΡΔΙΟΛΟΓΟΣ Α ΚΑΡΔΙΟΛΟΓΙΚΗ ΝΟΣ ΕΡΥΘΡΟΥ ΣΤΑΥΡΟΥ IRA 30-50% of STEMI patients have additional stenoses other than the infarct related
STEMI AND MULTIVESSEL CORONARY DISEASE ΤΣΙΑΦΟΥΤΗΣ Ν. ΙΩΑΝΝΗΣ ΕΠΕΜΒΑΤΙΚΟΣ ΚΑΡΔΙΟΛΟΓΟΣ Α ΚΑΡΔΙΟΛΟΓΙΚΗ ΝΟΣ ΕΡΥΘΡΟΥ ΣΤΑΥΡΟΥ IRA 30-50% of STEMI patients have additional stenoses other than the infarct related
Complex CAD (5) PVD-P Valv. CM. Sub-Clinical Arterial (2) DBD/Frailty (2) Health Political (1) Personal (3)
 PVD-P Valv. CM. Sub-Clinical Arterial (2) DBD/Frailty (2) Health Political (1) Personal (3)") 1. A Transition From Disease to Health 2. Heart Brain Integration 3. Imaging / Omics / Regeneration / Life Style Complex CAD (5) PVD-P Valv. CM AF Sub-Clinical Arterial (2) DBD/Frailty (2) Health Political
1. A Transition From Disease to Health 2. Heart Brain Integration 3. Imaging / Omics / Regeneration / Life Style Complex CAD (5) PVD-P Valv. CM AF Sub-Clinical Arterial (2) DBD/Frailty (2) Health Political
Culprit PCI vs MultiVessel PCI for Acute Myocardial Infarction
 Culprit PCI vs MultiVessel PCI for Acute Myocardial Infarction Dipti Itchhaporia, MD, FACC, FESC Trustee, American College of Cardiology Director of Disease Management, Hoag Hospital Robert and Georgia
Culprit PCI vs MultiVessel PCI for Acute Myocardial Infarction Dipti Itchhaporia, MD, FACC, FESC Trustee, American College of Cardiology Director of Disease Management, Hoag Hospital Robert and Georgia
PCI reduces death/myocardial infarction in stable patients with silent ischemia
 PCI reduces death/myocardial infarction in stable patients with silent ischemia Stephane Fournier, Yuhei Kobayashi, William F. Fearon, Bruno Roza da Costa, Carlos Collet, Panos Xaplanteris, Frederik Zimmerman,
PCI reduces death/myocardial infarction in stable patients with silent ischemia Stephane Fournier, Yuhei Kobayashi, William F. Fearon, Bruno Roza da Costa, Carlos Collet, Panos Xaplanteris, Frederik Zimmerman,
VCU Pauley Heart Center: A 2009 US News Top 50 Heart and Heart Surgery Hospital
 VCU Pauley Heart Center: A 2009 US News Top 50 Heart and Heart Surgery Hospital Complex PCI: Multivessel Disease George W. Vetrovec, MD. Kimmerling Chair of Cardiology VCU Pauley Heart Center Virginia
VCU Pauley Heart Center: A 2009 US News Top 50 Heart and Heart Surgery Hospital Complex PCI: Multivessel Disease George W. Vetrovec, MD. Kimmerling Chair of Cardiology VCU Pauley Heart Center Virginia
Diabetic Patients: Current Evidence of Revascularization
 Diabetic Patients: Current Evidence of Revascularization Alexandra J. Lansky, MD Yale University School of Medicine University College of London The Problem with Diabetic Patients Endothelial dysfunction
Diabetic Patients: Current Evidence of Revascularization Alexandra J. Lansky, MD Yale University School of Medicine University College of London The Problem with Diabetic Patients Endothelial dysfunction
FFR-Guided PCI. 4 th Imaging and Physiology Summit October 29 th, 2010 Seoul, Korea. Stanford
 4 th Imaging and Physiology Summit October 29 th, 2010 Seoul, Korea FFR-Guided PCI William F. Fearon, M.D. Associate Professor Division of Cardiovascular Medicine University Medical Center Disclosure Statement
4 th Imaging and Physiology Summit October 29 th, 2010 Seoul, Korea FFR-Guided PCI William F. Fearon, M.D. Associate Professor Division of Cardiovascular Medicine University Medical Center Disclosure Statement
Can Angiographic Complete Revascularization Improve Outcomes for Patients with Decreased LV Function? NO!
 Can Angiographic Complete Revascularization Improve Outcomes for Patients with Decreased LV Function? NO! Young-Hak Kim, MD, PhD Heart Institute, University of Ulsan College of Medicine Asan Medical Center,
Can Angiographic Complete Revascularization Improve Outcomes for Patients with Decreased LV Function? NO! Young-Hak Kim, MD, PhD Heart Institute, University of Ulsan College of Medicine Asan Medical Center,
ΑΓΓΕΙΟΠΛΑΣΤΙΚΗ ΣΤΟ ΔΙΑΒΗΤΙΚΟ ΑΣΘΕΝΗ
 ΑΓΓΕΙΟΠΛΑΣΤΙΚΗ ΣΤΟ ΔΙΑΒΗΤΙΚΟ ΑΣΘΕΝΗ Νίκος Μεζίλης MD, FESC Κλινική Άγιος Λουκάς Why diabetes is associated with restenosis endothelial dysfunction metabolic alterations accelerated platelet deposition
ΑΓΓΕΙΟΠΛΑΣΤΙΚΗ ΣΤΟ ΔΙΑΒΗΤΙΚΟ ΑΣΘΕΝΗ Νίκος Μεζίλης MD, FESC Κλινική Άγιος Λουκάς Why diabetes is associated with restenosis endothelial dysfunction metabolic alterations accelerated platelet deposition
Quality of Life Outcomes: The Trial to Assess Chelation Therapy
 Quality of Life Outcomes: The Trial to Assess Chelation Therapy Daniel B. Mark, MD, MPH Professor of Medicine Director, Outcomes Research Duke University Medical Center Duke Clinical Research Institute
Quality of Life Outcomes: The Trial to Assess Chelation Therapy Daniel B. Mark, MD, MPH Professor of Medicine Director, Outcomes Research Duke University Medical Center Duke Clinical Research Institute
Surgery Grand Rounds
 Surgery Grand Rounds Coronary Artery Bypass Grafting versus Coronary Artery Stenting Charles Ted Lord, R1 Coronary Artery Disease Stenosis of epicardial vessels Metabolic & hematologic Statistics 500,000
Surgery Grand Rounds Coronary Artery Bypass Grafting versus Coronary Artery Stenting Charles Ted Lord, R1 Coronary Artery Disease Stenosis of epicardial vessels Metabolic & hematologic Statistics 500,000
Imaging ischemic heart disease: role of SPECT and PET. Focus on Patients with Known CAD
 Imaging ischemic heart disease: role of SPECT and PET. Focus on Patients with Known CAD Hein J. Verberne Academic Medical Center, University of Amsterdam, Amsterdam, Netherlands International Conference
Imaging ischemic heart disease: role of SPECT and PET. Focus on Patients with Known CAD Hein J. Verberne Academic Medical Center, University of Amsterdam, Amsterdam, Netherlands International Conference
Mise à Jour sur le traitement du Pluritronculaire Philippe Généreux, MD
 Mise à Jour sur le traitement du Pluritronculaire Philippe Généreux, MD Columbia University Medical Center and The Cardiovascular Research Foundation, New York, USA Hôpital du Sacré-Coeur de Montréal,
Mise à Jour sur le traitement du Pluritronculaire Philippe Généreux, MD Columbia University Medical Center and The Cardiovascular Research Foundation, New York, USA Hôpital du Sacré-Coeur de Montréal,
Reconciling the Results of the Randomized Trials
 Management of Stable Angina in Multivessel Disease: Reconciling the Results of the Randomized Trials Eric A. Cohen MD, FRCPC Schulich Heart Centre Sunnybrook Health Sciences Centre Toronto ON ACC Rockies
Management of Stable Angina in Multivessel Disease: Reconciling the Results of the Randomized Trials Eric A. Cohen MD, FRCPC Schulich Heart Centre Sunnybrook Health Sciences Centre Toronto ON ACC Rockies
Guidelines/Appropriateness ARCH 2015 St Louis, Missouri April 9-11, 2015 Manish A. Parikh, MD, FACC,FSCAI
 Guidelines/Appropriateness ARCH 2015 St Louis, Missouri April 9-11, 2015 Manish A. Parikh, MD, FACC,FSCAI Center for Interventional Vascular Therapy Columbia University Medical Center / New York Presbyterian
Guidelines/Appropriateness ARCH 2015 St Louis, Missouri April 9-11, 2015 Manish A. Parikh, MD, FACC,FSCAI Center for Interventional Vascular Therapy Columbia University Medical Center / New York Presbyterian
Approach to Multi Vessel disease with STEMI
 Approach to Multi Vessel disease with STEMI MANAGEMENT OF ST-ELEVATION MYOCARDIAL INFARCTION Dr. Thomas Alexander, M.D; D.M; F.A.C.C. Senior Consultant and Interventional Cardiologist Kovai Medical Centre
Approach to Multi Vessel disease with STEMI MANAGEMENT OF ST-ELEVATION MYOCARDIAL INFARCTION Dr. Thomas Alexander, M.D; D.M; F.A.C.C. Senior Consultant and Interventional Cardiologist Kovai Medical Centre
Evaluating Clinical Risk and Guiding management with SPECT Imaging
 Evaluating Clinical Risk and Guiding management with SPECT Imaging Raffaele Giubbini Chair and Nuclear Medicine Unit University & Spedali Civili Brescia- Italy U.S. Congressional Budget Office. Technological
Evaluating Clinical Risk and Guiding management with SPECT Imaging Raffaele Giubbini Chair and Nuclear Medicine Unit University & Spedali Civili Brescia- Italy U.S. Congressional Budget Office. Technological
FFR-CT Not Ready for Primetime
 FFR-CT Not Ready for Primetime Leslee J. Shaw, PhD, MASNC, FACC, FAHA, FSCCT R. Bruce Logue Professor of Medicine Co-Director, Emory Clinical CV Research Institute Emory University School of Medicine Atlanta,
FFR-CT Not Ready for Primetime Leslee J. Shaw, PhD, MASNC, FACC, FAHA, FSCCT R. Bruce Logue Professor of Medicine Co-Director, Emory Clinical CV Research Institute Emory University School of Medicine Atlanta,
Coronary stenting: the appropriate use of FFR
 Coronary stenting: the appropriate use of FFR Morton J. Kern, MD Professor of Medicine Chief of Cardiology LBVA Associate Chief Cardiology University California Irvine Orange, California To treat or not
Coronary stenting: the appropriate use of FFR Morton J. Kern, MD Professor of Medicine Chief of Cardiology LBVA Associate Chief Cardiology University California Irvine Orange, California To treat or not
FRACTIONAL FLOW RESERVE USE IN THE CATH LAB BECAUSE ANGIOGRAPHY ALONE IS NOT ENOUGH!!!!!!!!
 FRACTIONAL FLOW RESERVE USE IN THE CATH LAB BECAUSE ANGIOGRAPHY ALONE IS NOT ENOUGH!!!!!!!! Juan Antonio Pastor-Cervantes,M.D FSCAI, FACC Cardiovascular Institute Memorial Regional Hospital Hollywood Florida
FRACTIONAL FLOW RESERVE USE IN THE CATH LAB BECAUSE ANGIOGRAPHY ALONE IS NOT ENOUGH!!!!!!!! Juan Antonio Pastor-Cervantes,M.D FSCAI, FACC Cardiovascular Institute Memorial Regional Hospital Hollywood Florida
Fractional Flow Reserve and the Results of the FAME Study
 Imaging and Physiology Summit Seoul, Korea November 21 st, 2009 Fractional Flow Reserve and the Results of the FAME Study William F. Fearon, M.D. Assistant Professor Division of Cardiovascular Medicine
Imaging and Physiology Summit Seoul, Korea November 21 st, 2009 Fractional Flow Reserve and the Results of the FAME Study William F. Fearon, M.D. Assistant Professor Division of Cardiovascular Medicine
Practical Office Management of Stable Angina
 Practical Office Management of Stable Angina All you need to know about it in 30 minutes Andy Ignaszewski MD FRCPC Head, Division of Cardiology PHC Physician Director, PHC Heart Centre Clinical Professor,
Practical Office Management of Stable Angina All you need to know about it in 30 minutes Andy Ignaszewski MD FRCPC Head, Division of Cardiology PHC Physician Director, PHC Heart Centre Clinical Professor,
The SYNTAX-LE MANS Study
 The SYNTAX-LE MANS Study Synergy Between PCI with TAXUS Express and Cardiac Surgery: Late (15-month) Left Main Angiographic Substudy A. Pieter Kappetein, MD, PhD Erasmus MC, Rotterdam, NL SYNTAX-LE MANS
The SYNTAX-LE MANS Study Synergy Between PCI with TAXUS Express and Cardiac Surgery: Late (15-month) Left Main Angiographic Substudy A. Pieter Kappetein, MD, PhD Erasmus MC, Rotterdam, NL SYNTAX-LE MANS
FFR Incorporating & Expanding it s use in Clinical Practice
 FFR Incorporating & Expanding it s use in Clinical Practice Suleiman Kharabsheh, MD Consultant Invasive Cardiology Assistant professor, Alfaisal Univ. KFHI - KFSHRC Concept of FFR Maximum flow down a vessel
FFR Incorporating & Expanding it s use in Clinical Practice Suleiman Kharabsheh, MD Consultant Invasive Cardiology Assistant professor, Alfaisal Univ. KFHI - KFSHRC Concept of FFR Maximum flow down a vessel
CABG vs PCI: What do the Guidelines Say?
 AATS International Cardiovascular Symposium: Sao Paolo 2017 CABG vs PCI: What do the Guidelines Say? David P Taggart MD PhD FRCS FESC Professor of Cardiovascular Surgery, University of Oxford Conflicts
AATS International Cardiovascular Symposium: Sao Paolo 2017 CABG vs PCI: What do the Guidelines Say? David P Taggart MD PhD FRCS FESC Professor of Cardiovascular Surgery, University of Oxford Conflicts
Michael Mack, M.D. Baylor Healthcare System Heart Hospital Baylor Plano Dallas, TX
 Michael Mack, M.D. Baylor Healthcare System Heart Hospital Baylor Plano Dallas, TX Maquet, Inc.,- unpaid consultant Cordis, Inc.,- unpaid consultant Boston Scientific, Inc.,- travel expenses paid for Syntax
Michael Mack, M.D. Baylor Healthcare System Heart Hospital Baylor Plano Dallas, TX Maquet, Inc.,- unpaid consultant Cordis, Inc.,- unpaid consultant Boston Scientific, Inc.,- travel expenses paid for Syntax
Do stents deserve the bad press? Mark A. Tulli MD, FACC
 Do stents deserve the bad press? Mark A. Tulli MD, FACC Disclosures: None Introduction Stents don t help people. Stents are bad for patients. Heart Treatment Overused WSJ Study Finds Doctors Often Too
Do stents deserve the bad press? Mark A. Tulli MD, FACC Disclosures: None Introduction Stents don t help people. Stents are bad for patients. Heart Treatment Overused WSJ Study Finds Doctors Often Too
Management of cardiovascular disease - coronary interventions -
 Master Classes in Preventive Cardiology I Management of diabetes in patients with CVD European Heart House Management of cardiovascular disease - coronary interventions - Francesco Cosentino MD, PhD, FESC
Master Classes in Preventive Cardiology I Management of diabetes in patients with CVD European Heart House Management of cardiovascular disease - coronary interventions - Francesco Cosentino MD, PhD, FESC
CLINICAL CONSEQUENCES OF THE
 CLINICAL CONSEQUENCES OF THE FAME STUDY TCT ASIA Seoul, Korea, april 26 th, 2012 Nico H. J. Pijls, MD, PhD Catharina Hospital, Eindhoven, The Netherlands GUIDELINES ESC SEPTEMBER 2010 FFR UPGRADED TO LEVEL
CLINICAL CONSEQUENCES OF THE FAME STUDY TCT ASIA Seoul, Korea, april 26 th, 2012 Nico H. J. Pijls, MD, PhD Catharina Hospital, Eindhoven, The Netherlands GUIDELINES ESC SEPTEMBER 2010 FFR UPGRADED TO LEVEL
Left Main PCI. Integrated Use of IVUS and FFR. Seung-Jung Park, MD, PhD
 Left Main PCI Integrated Use of IVUS and FFR Seung-Jung Park, MD, PhD Professor of Medicine, University of Ulsan College of Medicine, Heart Institute, Asan Medical Center, Seoul, Korea Efficacy of Left
Left Main PCI Integrated Use of IVUS and FFR Seung-Jung Park, MD, PhD Professor of Medicine, University of Ulsan College of Medicine, Heart Institute, Asan Medical Center, Seoul, Korea Efficacy of Left
Blinded Physiological Assessment of Residual Ischemia after Successful Angiographic PCI Allen Jeremias, MD, MSc
 Blinded Physiological Assessment of Residual Ischemia after Successful Angiographic PCI Allen Jeremias, MD, MSc On behalf of Justin Davies, Manesh Patel, Gregg Stone and the DEFINE PCI Investigators Disclosure
Blinded Physiological Assessment of Residual Ischemia after Successful Angiographic PCI Allen Jeremias, MD, MSc On behalf of Justin Davies, Manesh Patel, Gregg Stone and the DEFINE PCI Investigators Disclosure
Disclosures. Speaker s bureau: Research grant: Advisory Board: Servier International, Bayer, Merck Serono, Novartis, Boehringer Ingelheim, Lupin
 Disclosures Speaker s bureau: Research grant: Advisory Board: Servier International, Bayer, Merck Serono, Novartis, Boehringer Ingelheim, Lupin Servier International, Boehringer Ingelheim Servier International,
Disclosures Speaker s bureau: Research grant: Advisory Board: Servier International, Bayer, Merck Serono, Novartis, Boehringer Ingelheim, Lupin Servier International, Boehringer Ingelheim Servier International,
CHIP Complex Higher-risk (and indicated) PCI
 PCI") CHIP Complex Higher-risk (and indicated) PCI Ziad A Ali MD DPhil Columbia University Medical Center Cardiovascular Research Foundation Disclosure Statement of Financial Interest Within the past 12 months,
CHIP Complex Higher-risk (and indicated) PCI Ziad A Ali MD DPhil Columbia University Medical Center Cardiovascular Research Foundation Disclosure Statement of Financial Interest Within the past 12 months,
COMMENT DEFINIR UN PLURITRONCULAIRE. Didier Carrié CHU Toulouse Rangueil
 COMMENT DEFINIR UN PLURITRONCULAIRE VISION ANGIOGRAHIQUE DU PLURITRONCULAIRE Didier Carrié CHU Toulouse Rangueil Congrès GRCI 03 Décembre 2010 Pôle Cardiovasculaire et Métabolique Avec quel œil je regarde
COMMENT DEFINIR UN PLURITRONCULAIRE VISION ANGIOGRAHIQUE DU PLURITRONCULAIRE Didier Carrié CHU Toulouse Rangueil Congrès GRCI 03 Décembre 2010 Pôle Cardiovasculaire et Métabolique Avec quel œil je regarde
David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine The Ohio State University Division of Cardiovascular Medicine Columbus, Ohio
 1 STABLE ISCHEMIC HEART DISEASE: A NON-INVASIVE CARDIOLOGIST S PERSECTIVE 2018 Cardiovascular Course for Trainees and Early Career Physicians APRIL 20, 2018 David A. Orsinelli, MD, FACC, FASE Professor,
1 STABLE ISCHEMIC HEART DISEASE: A NON-INVASIVE CARDIOLOGIST S PERSECTIVE 2018 Cardiovascular Course for Trainees and Early Career Physicians APRIL 20, 2018 David A. Orsinelli, MD, FACC, FASE Professor,
Background. After PCI for MI, angina has important implications on quality of life and healthcare utilization
 Angina Prevalence and Management for Myocardial Infarction Patients Treated with Percutaneous Coronary Intervention: Insights from the TRANSLATE-ACS Study Alexander C. Fanaroff, Lisa A. Kaltenbach, Eric
Angina Prevalence and Management for Myocardial Infarction Patients Treated with Percutaneous Coronary Intervention: Insights from the TRANSLATE-ACS Study Alexander C. Fanaroff, Lisa A. Kaltenbach, Eric
Δημήτριος Αγγοσράς, FETCS
 ΣΕΜΙΝΑΡΙΟ ΟΜΑΔΩΝ ΕΡΓΑΣΙΑΣ Δημήτριος Αγγοσράς, FETCS Επίκοσρος Καθηγηηής Καρδιοτειροσργικής Ιαηρική Πανεπιζηημίοσ Αθηνών Πανεπιζηημιακό Γενικό Νοζοκομείο Αηηικόν Randomized Controlled Trials (RCTs) Why
ΣΕΜΙΝΑΡΙΟ ΟΜΑΔΩΝ ΕΡΓΑΣΙΑΣ Δημήτριος Αγγοσράς, FETCS Επίκοσρος Καθηγηηής Καρδιοτειροσργικής Ιαηρική Πανεπιζηημίοσ Αθηνών Πανεπιζηημιακό Γενικό Νοζοκομείο Αηηικόν Randomized Controlled Trials (RCTs) Why
Complete Revascularization: The Future Mode of Revascularization in STEMI
 Complete Revascularization: The Future Mode of Revascularization in STEMI Alan C. Yeung, MD Li Ka Shing Professor of Medicine Chief, Division of Cardiovascular Medicine Stanford University School of Medicine
Complete Revascularization: The Future Mode of Revascularization in STEMI Alan C. Yeung, MD Li Ka Shing Professor of Medicine Chief, Division of Cardiovascular Medicine Stanford University School of Medicine
Coronary interventions
 Controversial issues in the management of ischemic heart failure Coronary interventions Maciej Lesiak Department of Cardiology, University Hospital in Poznan none DECLARATION OF CONFLICT OF INTEREST CHF
Controversial issues in the management of ischemic heart failure Coronary interventions Maciej Lesiak Department of Cardiology, University Hospital in Poznan none DECLARATION OF CONFLICT OF INTEREST CHF
Management of High-Risk CAD : Surgeons Perspective
 Management of High-Risk CAD : Surgeons Perspective Steven F. Bolling, M.D. Professor of Cardiac Surgery University of Michigan Conflict : Cardiac Surgeon! High Risk CABG 77 year old with prior large anterior
Management of High-Risk CAD : Surgeons Perspective Steven F. Bolling, M.D. Professor of Cardiac Surgery University of Michigan Conflict : Cardiac Surgeon! High Risk CABG 77 year old with prior large anterior
EXCEL vs. NOBLE: How to Treat Left Main Disease in 2017 AATS International Cardiovascular Symposium December 8-9, 2017
 EXCEL vs. NOBLE: How to Treat Left Main Disease in 2017 AATS International Cardiovascular Symposium December 8-9, 2017 Igor F. Palacios, MD Director of Interventional Cardiology Professor of Medicine Massachusetts
EXCEL vs. NOBLE: How to Treat Left Main Disease in 2017 AATS International Cardiovascular Symposium December 8-9, 2017 Igor F. Palacios, MD Director of Interventional Cardiology Professor of Medicine Massachusetts
Master Class in Preventive Cardiology Focus on Diabetes and Cardiovascular Disease Geneva April
 Master Class in Preventive Cardiology Focus on Diabetes and Cardiovascular Disease Geneva April 14 2011 Coronary interventions in patients with diabetes Lars Rydén Karolinska Institutet Stockholm, Sweden
Master Class in Preventive Cardiology Focus on Diabetes and Cardiovascular Disease Geneva April 14 2011 Coronary interventions in patients with diabetes Lars Rydén Karolinska Institutet Stockholm, Sweden
Revascularization In HFrEF: Are We Close To The Truth. Ali Almasood
 Revascularization In HFrEF: Are We Close To The Truth Ali Almasood HF epidemic 1-2% of the population have HF At least one-half have heart failure with reduced ejection fraction (HF- REF) The most common
Revascularization In HFrEF: Are We Close To The Truth Ali Almasood HF epidemic 1-2% of the population have HF At least one-half have heart failure with reduced ejection fraction (HF- REF) The most common
Health Status after Transcatheter Mitral- Valve Repair in Patients with Heart Failure and Secondary Mitral Regurgitation: Results from the COAPT Trial
 Health Status after Transcatheter Mitral- Valve Repair in Patients with Heart Failure and Secondary Mitral Regurgitation: Results from the COAPT Trial Suzanne V. Arnold, MD, MHA Saint Luke s Mid America
Health Status after Transcatheter Mitral- Valve Repair in Patients with Heart Failure and Secondary Mitral Regurgitation: Results from the COAPT Trial Suzanne V. Arnold, MD, MHA Saint Luke s Mid America
FAME STUDY: 2-year Follow-Up & CLINICAL SUBGROUP ANALYSIS
 Coronary Physiology In The Cathlab FAME STUDY: 2-year Follow-Up & CLINICAL SUBGROUP ANALYSIS Educational Training Program ESC European Heart House april 7th 9th 2011 Nico H.J.Pijls, MD, PhD Catharina Hospital,
Coronary Physiology In The Cathlab FAME STUDY: 2-year Follow-Up & CLINICAL SUBGROUP ANALYSIS Educational Training Program ESC European Heart House april 7th 9th 2011 Nico H.J.Pijls, MD, PhD Catharina Hospital,
PCI vs. CABG From BARI to Syntax, Is The Game Over?
 PCI vs. CABG From BARI to Syntax, Is The Game Over? Seung-Jung Park, MD, PhD Professor of Medicine, University of Ulsan College of Medicine Asan Medical Center, Seoul, Korea PCI vs CABG Multi-Vessel Disease
PCI vs. CABG From BARI to Syntax, Is The Game Over? Seung-Jung Park, MD, PhD Professor of Medicine, University of Ulsan College of Medicine Asan Medical Center, Seoul, Korea PCI vs CABG Multi-Vessel Disease
CMR stress Perfusion: what's new?
 CMR stress Perfusion: what's new? John P. Greenwood Professor of Cardiology, Leeds University, UK Consultant Cardiologist Leeds Teaching Hospitals NHS Trust, UK CMR: multi-parametric CMR: multi-parametric
CMR stress Perfusion: what's new? John P. Greenwood Professor of Cardiology, Leeds University, UK Consultant Cardiologist Leeds Teaching Hospitals NHS Trust, UK CMR: multi-parametric CMR: multi-parametric
Controversies in Cardiac Surgery
 Controversies in Cardiac Surgery 3 years after SYNTAX : Percutaneous Coronary Intervention for Multivessel / Left main stem Coronary artery disease Pro ESC Congress 2010, 28 August 1 September Stockholm
Controversies in Cardiac Surgery 3 years after SYNTAX : Percutaneous Coronary Intervention for Multivessel / Left main stem Coronary artery disease Pro ESC Congress 2010, 28 August 1 September Stockholm
CARDIOLOGY GRAND ROUNDS
 CARDIOLOGY GRAND ROUNDS Title: Fractional flow reserve (FFR) Computed tomography (CT) Speaker: John R. Lesser, MD Senior Consulting Cardiologist, Medical Director CT/CMR Minneapolis Heart Institute at
CARDIOLOGY GRAND ROUNDS Title: Fractional flow reserve (FFR) Computed tomography (CT) Speaker: John R. Lesser, MD Senior Consulting Cardiologist, Medical Director CT/CMR Minneapolis Heart Institute at
What do the guidelines say?
 Percutaneous coronary intervention in 3-vessel disease and main stem What do the guidelines say? Nothing to disclose Dariusz Dudek Institute of Cardiology, Jagiellonian University Krakow, Poland The European
Percutaneous coronary intervention in 3-vessel disease and main stem What do the guidelines say? Nothing to disclose Dariusz Dudek Institute of Cardiology, Jagiellonian University Krakow, Poland The European
Fractional Flow Reserve and instantaneous wave -free Ratio. Λάμπρος Κ. Μόσιαλος Επεμβατικός Καρδιολόγος ΓΝ Παπαγεωργίου
 Fractional Flow Reserve and instantaneous wave -free Ratio Λάμπρος Κ. Μόσιαλος Επεμβατικός Καρδιολόγος ΓΝ Παπαγεωργίου DISCLOSURES There are no financial conflicts of interest relevant to this presentation
Fractional Flow Reserve and instantaneous wave -free Ratio Λάμπρος Κ. Μόσιαλος Επεμβατικός Καρδιολόγος ΓΝ Παπαγεωργίου DISCLOSURES There are no financial conflicts of interest relevant to this presentation
Implications of the New ESC/EACTS Guidelines for Myocardial Revascularization in 2011
 Implications of the New ESC/EACTS Guidelines for Myocardial Revascularization in 2011 Prof. Dr. Volkmar Falk Klinik für Herz- und Gefäßchirurgie, Universitätsspital Zürich, Schweiz In 2004 headlines were
Implications of the New ESC/EACTS Guidelines for Myocardial Revascularization in 2011 Prof. Dr. Volkmar Falk Klinik für Herz- und Gefäßchirurgie, Universitätsspital Zürich, Schweiz In 2004 headlines were
Dave Kettles, St Dominics Hospital East London.
 Dave Kettles, St Dominics Hospital East London. 110 x 150 Angina for a couple of months Trop T negative T wave inversion across the chest leads Not wanting to risk radial Huge struggle with femoral
Dave Kettles, St Dominics Hospital East London. 110 x 150 Angina for a couple of months Trop T negative T wave inversion across the chest leads Not wanting to risk radial Huge struggle with femoral
Southern Thoracic Surgical Association CABG in 2012: Implications of the New ESC/EACTS Guidelines
 Southern Thoracic Surgical Association 2011 CABG in 2012: Implications of the New ESC/EACTS Guidelines David P Taggart MD PhD FRCS Professor of Cardiovascular Surgery, University of Oxford Conflicts of
Southern Thoracic Surgical Association 2011 CABG in 2012: Implications of the New ESC/EACTS Guidelines David P Taggart MD PhD FRCS Professor of Cardiovascular Surgery, University of Oxford Conflicts of
Management of High-Risk Coronary Artery Disease
 Management of High-Risk Coronary Artery Disease Jeffrey J. Popma, MD Director, Interventional Cardiology Clinical Services Beth Israel Deaconess Medical Center Associate Professor of Medicine Harvard Medical
Management of High-Risk Coronary Artery Disease Jeffrey J. Popma, MD Director, Interventional Cardiology Clinical Services Beth Israel Deaconess Medical Center Associate Professor of Medicine Harvard Medical
Clinical Seminar. Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective
 Clinical Seminar Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical
Clinical Seminar Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical
Michael Mack, M.D. Baylor Healthcare System Heart Hospital Baylor Plano Dallas, TX
 Michael Mack, M.D. Baylor Healthcare System Heart Hospital Baylor Plano Dallas, TX Boston Scientific, Inc.- Syntax Trial Steering Committee Member- travel expenses paid by trial sponsor Maquet, Inc.- unpaid
Michael Mack, M.D. Baylor Healthcare System Heart Hospital Baylor Plano Dallas, TX Boston Scientific, Inc.- Syntax Trial Steering Committee Member- travel expenses paid by trial sponsor Maquet, Inc.- unpaid
The Future of Coronary Physiology
 The Future of Coronary Physiology Morton J. Kern, MD Chief of Medicine, VA Long Beach HCS Professor of Medicine University California Irvine Orange, California Disclosure: Morton J. Kern, MD Within the
The Future of Coronary Physiology Morton J. Kern, MD Chief of Medicine, VA Long Beach HCS Professor of Medicine University California Irvine Orange, California Disclosure: Morton J. Kern, MD Within the
New Insight about FFR and IVUS MLA
 New Insight about FFR and IVUS MLA Can IVUS MLA Predict FFR
New Insight about FFR and IVUS MLA Can IVUS MLA Predict FFR
Can Angioplasty Improve Quality of Life for CAD Patients?
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/clinicians-roundtable/can-angioplasty-improve-quality-of-life-for-cadpatients/4000/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/clinicians-roundtable/can-angioplasty-improve-quality-of-life-for-cadpatients/4000/
Cardiogenic Shock. Carlos Cafri,, MD
 Cardiogenic Shock Carlos Cafri,, MD SHOCK= Inadequate Tissue Mechanisms: Perfusion Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and
Cardiogenic Shock Carlos Cafri,, MD SHOCK= Inadequate Tissue Mechanisms: Perfusion Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and
What oral antiplatelet therapy would you choose? a) ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor
 ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor") 76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
Σεμινάριο Ομάδων Εργασίας Fractional Flow Reserve (FFR) Σε ποιούς ασθενείς; ΔΗΜΗΤΡΗΣ ΑΥΖΩΤΗΣ Επιστ. υπεύθυνος Αιμοδυναμικού Τμήματος, Βιοκλινική
 Σε ποιούς ασθενείς; ΔΗΜΗΤΡΗΣ ΑΥΖΩΤΗΣ Επιστ. υπεύθυνος Αιμοδυναμικού Τμήματος, Βιοκλινική") ΕΛΛΗΝΙΚΗΚΑΡΔΙΟΛΟΓΙΚΗΕΤΑΙΡΕΙΑ Σεμινάριο Ομάδων Εργασίας 2011 Fractional Flow Reserve (FFR) Σε ποιούς ασθενείς; ΔΗΜΗΤΡΗΣ ΑΥΖΩΤΗΣ Επιστ. υπεύθυνος Αιμοδυναμικού Τμήματος, Βιοκλινική GUIDELINES ON MYOCARDIAL
ΕΛΛΗΝΙΚΗΚΑΡΔΙΟΛΟΓΙΚΗΕΤΑΙΡΕΙΑ Σεμινάριο Ομάδων Εργασίας 2011 Fractional Flow Reserve (FFR) Σε ποιούς ασθενείς; ΔΗΜΗΤΡΗΣ ΑΥΖΩΤΗΣ Επιστ. υπεύθυνος Αιμοδυναμικού Τμήματος, Βιοκλινική GUIDELINES ON MYOCARDIAL
Instantaneous Wave-Free Ratio
 Instantaneous Wave-Free Ratio Alejandro Aquino MD Interventional Cardiology Fellow Washington University in St. Louis Barnes-Jewish Hospital Instantaneous Wave-Free Ratio Alejandro Aquino MD Disclosure
Instantaneous Wave-Free Ratio Alejandro Aquino MD Interventional Cardiology Fellow Washington University in St. Louis Barnes-Jewish Hospital Instantaneous Wave-Free Ratio Alejandro Aquino MD Disclosure
Perioperative Cardiology Consultations for Noncardiac Surgery Ischemic Heart Disease
 2012 대한춘계심장학회 Perioperative Cardiology Consultations for Noncardiac Surgery Ischemic Heart Disease 울산의대울산대학병원심장내과이상곤 ECG CLASS IIb 1. Preoperative resting 12-lead ECG may be reasonable in patients with
2012 대한춘계심장학회 Perioperative Cardiology Consultations for Noncardiac Surgery Ischemic Heart Disease 울산의대울산대학병원심장내과이상곤 ECG CLASS IIb 1. Preoperative resting 12-lead ECG may be reasonable in patients with
Patrick W. Serruys MD. PhD. 1 Bernard Chevalier MD. 2 Yoshinobu Onuma MD. PhD. 3 on behalf of ABSORB II investigators
 TCT 216, Washington convention center October 3 th 216, 8:3 am- Room 159 Level 1 Late breaking clinical trial and First report investigations Press Conf.1 ABSORB II: Three-year Clinical Outcomes from a
TCT 216, Washington convention center October 3 th 216, 8:3 am- Room 159 Level 1 Late breaking clinical trial and First report investigations Press Conf.1 ABSORB II: Three-year Clinical Outcomes from a
Percutaneous Coronary Intervention: Update
 Percutaneous Coronary Intervention: Update Alphonse M. Ambrosia, DO, FACC Interventional Cardiologist CardioVascular Associates of Mesa Mesa, Arizona Disclosures Speakers Bureau Boston Scientific Medtronics
Percutaneous Coronary Intervention: Update Alphonse M. Ambrosia, DO, FACC Interventional Cardiologist CardioVascular Associates of Mesa Mesa, Arizona Disclosures Speakers Bureau Boston Scientific Medtronics
Intervention: How and to which extent is technology helping us?
 Cardiological Society of India Congress 12th February 2016 Chennai, India Intervention: How and to which extent is technology helping us? SIMONE BISCAGLIA MD CARDIOVASCULAR INSTITUTE, FERRARA, ITALY Introduction
Cardiological Society of India Congress 12th February 2016 Chennai, India Intervention: How and to which extent is technology helping us? SIMONE BISCAGLIA MD CARDIOVASCULAR INSTITUTE, FERRARA, ITALY Introduction