Cardiac Rehabilitation for Heart Failure Patients. Jia Shen MD, MPH Assistant Professor of Medicine UC San Diego Health System
|
|
|
- Marylou Shepherd
- 6 years ago
- Views:
Transcription
1 Cardiac Rehabilitation for Heart Failure Patients Jia Shen MD, MPH Assistant Professor of Medicine UC San Diego Health System
2 Disclosures There are no conflict of interests related to this presentation.
3 Overview of Talk Historical Perspective of Cardiac Rehabilitation Current principles of Cardiac Rehabilitation Eligibility criteria for cardiac rehabilitation (Medicare) Current AHA/ACC Recommendations Evidence behind recommendations: Effect of Exercise Training on cardiac function and skeletal muscle Effect of Exercise Training on Systolic Heart Failure HF-Action Study Effect of Exercise Training on Diastolic Heart Failure Effect of Self-Care on Heart Failure Outcomes Barriers to Cardiac Rehabilitation Participation The Cardiac Rehab Program at UCSD.
4 Historical Perspective 1930 s restriction of physical activity and prolonged bedrest were standard of care for patient s with HR and MI s chair therapy s daily walks 3-5 minutes in duration s structured inpatient CR programs for early ambulation post MI. Present multidisciplinary, comprehensive CR programs.
5 AHA/ACC Recommendations Patients with HF should receive specific education to facilitate HF self-care. (Class IB) Exercise training (or regular physical activity) is recommended as safe and effective for patients with HF who are able to participate to improve functional status. (Class IA) Cardiac rehabilitation can be useful in clinically stable patients with HF to improve functional capacity, exercise duration, HRQOL, and mortality. (Class IIA)
6 Currently Covered Indications for Cardiac Rehabilitation(CR) Recent myocardial infarction (within 1 year) Post Percutaneous coronary intervention (PCI) Coronary artery bypass grafting (CABG) Chronic stable angina Cardiac transplantation Heart valve repair or replacement Stable, chronic systolic heart failure (EF<35%) Peripheral Arterial Disease *Systolic heart failure (EF >35%) and diastolic dysfunction are not currently covered.
7
8 Total Number of Sessions covered 72 (max per day is 6 sessions) over 18 weeks Ornish Ornish Versus Pritikin 72 sessions (divided into 18 sessions that are 4 hours each) Pritikin 72 sessions (can customize how many sessions per day) Diet 100% plant based Allows for lean meat and fish Format Outcome Data All with live instructors: 1 hour of exercise 1 hour of nutrition counseling 1 hour of yoga and 1 hour of group therapy Patients are in groups of and stay with the same cohort throughout the program The Lifestyle Heart Trial showed significant regression of coronary atherosclerosis measured by angiography in the experimental group randomly assigned to intensive lifestyle changes. (5 year results reported by Ornish JAMA 1998) Some parts are Video Instruction. Sessions duration can be customized over 18 weeks Data from Pritikin residential treatment centers showed improvement in lipids, A1c, blood pressure and weight. (Barnard Am J Cardiol 1992)

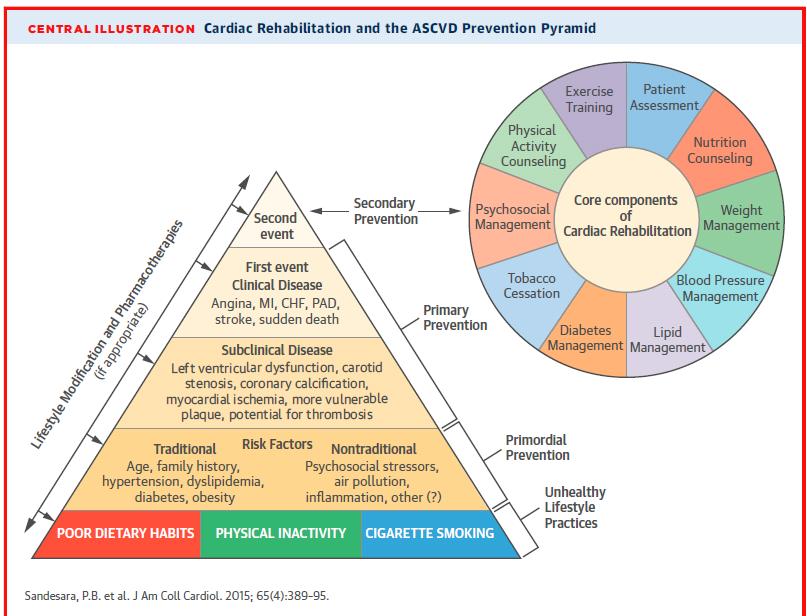
9 Pleiotropic Effects of Cardiac Rehabilitation (Sandesara et al., JACC (2015)
10 Heart Failure and Skeletal Muscle: Chronic heart failure results in structural abnormalities in skeletal muscle reflecting reduced oxidative capacity of working muscle. Skeletal muscle is more reliant on anaerobic metabolism, resulting in lactic acidosis, and early fatigue. Changes in oxidative capacity correlate with changes in exercise capacity. Drexler et al., Circulation (1992)
11 Effect of Exercise Training on Skeletal Muscle: Sustained exercise training can reverse changes in oxidative capacity in skeletal muscle. Resulting in re-shifting from type II fast-twitch fibers to type I slow- twitch fibers, and increased mitochondrial density. This is associated with increased exercise capacity unrelated to changes in peripheral perfusion. Hambrecht et al., JACC (1997)
12 Effect of Exercise Training in CHF: Controlled crossover trial of 8 weeks of exercise training against 8 weeks of rest in 17 men with stable heart failure (LVEF 19.6% ± 2.3%). Training program: exercise on stationary bicycles at 50 rpm for 20 minutes 5 days per week for a target heartrate 60-80% of maximum HR. Results: Increased exercise tolerance, peak oxygen uptake, cardiac output, vagal tone, and decreased systemic vascular resistance. Coats et al., Circulation (1992)
13 Effect of Long-Term Exercise Training in CHF: Randomized controlled trial of 99 patients (59 ± 14 years, 88 men) with stable heart failure (EF 28.4% ± 6%). Intervention: Exercise Training at 60% of VO2 3x per week x 8 weeks, then 2x per week x 1 year. Results: Increased peak VO2 (18%) and thallium activity score (24%), and improved quality of life. Reduced mortality (RR =0.37; 95% CI: , p=0.01) and hospital readmission for heart failure (RR=0.29; 95% CI: , p=0.02). Belardinelli et al., Circulation (1999)
14 Effect of Exercise Training in CHF: HF-ACTION Multicenter RCT from 82 centers in Canada, USA, and France with a median follow up of 30 months. Randomized Controlled Trial 2331 patients (median age 59 years, 28% women) with stable heart failure (median LVEF 25%, 37% NYHA Class III-IV symptoms). Intervention: Aerobic exercise training (36 supervised sessions) followed by home-based training. Primary endpoints: all-cause mortality or hospitalization. Secondary endpoints: CVD mortality, hospitalization, or HF hospitalization. O Connor et at., JAMA (2009)
 Usual Care Exercise Training Optimized medical treatment Patient education Phone calls Recommendation: Moderate")
15 Study Design Chronic heart failure, NYHA Class II-IV, LVEF 35%, optimal medical therapy, and capable of exercising. Pre-randomization CPX and ECHO Randomization 1:1 (Stratified by center and HF etiology) Usual Care Exercise Training Optimized medical treatment Patient education Phone calls Recommendation: Moderate intensity activity 30 minutes/day Optimized medical treatment Patient education Phone calls Supervised training Home training
16 Exercise Training Protocol: Structured, group-based, supervised exercise program. 3 sessions per week for a total of 36 sessions in 3 months. Performed walking, treadmill, or stationary cycling as their primary training mode. Exercise was initiated at minutes per session at a heartrate corresponding to 60% of heartrate reserve. After 6 sessions, duration of exercise was increased to minutes, and intensity increased to 70% of heartrate reserve. Home-based exercise training began after 18 supervised sessions and were fully transitioned after 36 sessions. Patients were given exercise equipment and HR monitors. Target home training was 5x per week for 40 minutes at a HR 60-70% of HR reserve.
17 HF-ACTION Results HR=0.93 (95% CI: ), p=0.13 Adjusted HR 0.89 (95% CI: ), p=0.03 O Connor et at., JAMA (2009)
18 Summary of Major Outcomes Hazard Ratio All-cause mortality and hospitalization (primary) 95% CI p-value Main analysis , Adjusted analysis , CV mortality and CV hospitalization Main analysis , Adjusted analysis , CV mortality and HF hospitalization Main analysis , Adjusted analysis , *No difference in the occurrence of adverse events.
19 Conclusions: Exercise training results in non-significant reductions in the primary end point of all-cause mortality or hospitalization. After adjustment for highly prognostic predictors of primary endpoints, exercise training was associated with a 13% risk reduction in cardiovascular mortality or heart failure hospitalization in patients already receiving standard of care. Significance may have been diluted do to high crossover rates between groups - 55% of participants in the usual care groups were dissatisfied with their assignment and likely continue some level of physical activity. Difficult for chronically ill patients to maintain exercise prescription over time minimizing effects due to drop out.
20 Exercise Training for Diastolic Heart Failure Ex-DHF Trial: Prospective, multicenter, RCT in patients with symptomatic (NYHA II/III) and HFpEF (EF 50%). 64 patients (age 65 ± 7 years, 56% female) randomized 2:1 to supervised endurance/resistance training or usual care alone. Intervention: Weeks 1-4: aerobic endurance training (cycling 2 /week) of increasing intensity and duration (from 20 to 40 min) for target HR 50-60% of peak VO2. Weeks 5-12: training 3x/week with target HR 70% of peak VO2 + resistance training 2x/week. Endpoints: Primary change in peak VO2 after 3 months. Secondary effects on cardiac structure, diastolic function, and QoL. Edelmann et al., JACC (2011)
21
22 Exercise Training in Diastolic Heart Failure Exercise training improves exercise capacity and physical functioning in patients with diastolic HF. This benefit is associated with improved diastolic function and reverse atrial remodeling. ET is safe, well-tolerated, and may be beneficial in patients with HFpEF, where there are have been few proven effective treatment modalities. Edelmann et al., JACC (2011)
23 Self-Care in Heart Failure Self-management programs aim to enable patients to assume primary role in managing their condition: monitor symptoms, adjust medications and determine when additional medical attention is necessary. Examples Include: Limit daily sodium intake <2 g and fluid intake < 2 L Obtain daily weights, monitor for early signs of volume overload Contact provider immediately if change in symptoms or weight Avoidance of drugs (cocaine/meth) and alcohol use Following heart healthy diets Self-care is associated with better quality of life, functional status, and reduced symptom burden in patients with HF. Jovicic et al., BMC (2006)
24 Self-Care and Heart Failure Outcomes 44 vs. 69%, p=0.01 OR=0.20, CI = vs. 93%, p=0.03 OR=3.85, CI = Davidson et al., Euro J of CVD Pre Rehab (2010)
25 Depression and Heart Failure 1 out of 5 patients with heart failure are clinically depressed (this proportion increases with NYHA Class). Depressed patients are less likely to engage in self-care, have increased healthcare utilization, ER visits, and readmissions. Depressed patients are more than 2x as likely to die then their non-depressed peers. Pharmacologic treatment of depression has not been shown to improve clinical outcomes or mortality. ET as a part of a structural CR program is effective in treating depression and improves long-term survival. Survival benefits of CR are concentrated to those patients that improved exercise capacity with underlying undiagnosed depression. Rutledge et al., JACC (2006), Milani et al., Am J Cardiol (2011)
26 Social Support and Heart Failure Patients with a high level of support reported significantly better self-care than patients with low or moderate levels of social support. Patients with a high level of social support reported being significantly more likely to consult with a health professional for weight gain, to limit the amount of fluids they have, take their medication, to get a flu shot, and to exercise on a regular basis than those with medium or low levels of social support. Social support provided by partners needs to be of a quality and content that matches HF patients' perception of need to influence self-care. Support networks and partners are an integral in the treatment of HF patients. Gallagher et al., J Cardiovasc Nurs (2011)
27
28 Barriers to Cardiac Rehabilitation Participation: Fewer than 20% of all eligible patients participate in a CR Of those who are referred to CR only 34% actually enroll. Systemic Barriers: lack of a centralized method for referral inadequate communication among treatment teams, patients, and CR facilities unfamiliarity with CR among potential referring physicians limited access to facilities Patient Barriers: Poor self-care and understanding of medical condition Anxiety/depression/addiction Poor social or financial support Language barriers Sandesara et al, JACC (2015)
29 Current Reimbursement for Cardiac Rehabilitation With the affordable care act there is a focus on preventive services There has been a gradual increase in reimbursement for cardiac rehabilitation Currently in California Medicare: $107 per session Commercial Payers (e.g Anthem Blue Cross): $132 per session For intensive cardiac rehab (ICR), 72 covered sessions revenue is $7700 to $9500 per patient
30 Conclusions: ET results in improvements in cardiac and skeletal muscle function and modifies the biochemical, neurohumoral, and inflammatory responses to heart failure. In patients with reduced systolic function, ET is safe and reduces HF symptoms, hospitalizations, and mortality. In patients with diastolic dysfunction, ET is safe and reduces HF symptoms, improves diastolic function and QoL. Self-care and patient education are important components heart failure therapy and can significantly reduce HF symptoms, readmissions, and mortality. Multidisciplinary cardiac rehabilitation programs are an integral component of the management of chronic heart failure and are increasingly covered by insurers. Every effort should be made to find appropriate patients for referral.
31
Rebuilding and Reinvigorating Cardiac Rehabilitation in 2018
 Rebuilding and Reinvigorating Cardiac Rehabilitation in 2018 Pam R. Taub MD, FACC Director of Step Family Cardiac Wellness and Rehabilitation Center Associate Professor of Medicine UC San Diego Health
Rebuilding and Reinvigorating Cardiac Rehabilitation in 2018 Pam R. Taub MD, FACC Director of Step Family Cardiac Wellness and Rehabilitation Center Associate Professor of Medicine UC San Diego Health
Value of Cardiac Rehabilitation for Improving Patient Outcomes
 Value of Cardiac Rehabilitation for Improving Patient Outcomes Pam R. Taub MD, FACC Director of Step Family Cardiac Wellness and Rehabilitation Center Associate Professor of Medicine UC San Diego Health
Value of Cardiac Rehabilitation for Improving Patient Outcomes Pam R. Taub MD, FACC Director of Step Family Cardiac Wellness and Rehabilitation Center Associate Professor of Medicine UC San Diego Health
HEART FAILURE AN OMINOUS DISEASE
 HEART FAILURE AN OMINOUS DISEASE Conflicts of Interest I Have No Conflicts of Interest to Disclose Objective At the conclusion of this presentation, the participants will be able to identify benefits and
HEART FAILURE AN OMINOUS DISEASE Conflicts of Interest I Have No Conflicts of Interest to Disclose Objective At the conclusion of this presentation, the participants will be able to identify benefits and
The Role of Exercise in Management of Patients with Heart Failure
 The Role of Exercise in Management of Patients with Heart Failure Pamela B. Morris, MD, FACC, FAHA, FASPC, FNLA Chair, ACC Prevention of Cardiovascular Disease Leadership Council and Section Director,
The Role of Exercise in Management of Patients with Heart Failure Pamela B. Morris, MD, FACC, FAHA, FASPC, FNLA Chair, ACC Prevention of Cardiovascular Disease Leadership Council and Section Director,
The Role of Cardiac Rehabilitation. The Role of Cardiac Rehabilitation. in Heart Failure. in Heart Failure. History of Cardiac Rehab.
 The Role of Cardiac Rehabilitation The Role of Cardiac Rehabilitation in Heart Failure in Heart Failure Kate Traynor RN MS FAACVPR Financial Disclosures No relevant financial relationship exists. History
The Role of Cardiac Rehabilitation The Role of Cardiac Rehabilitation in Heart Failure in Heart Failure Kate Traynor RN MS FAACVPR Financial Disclosures No relevant financial relationship exists. History
Intensive Cardiac Rehabilitation R U T H A D A M I E C, M A, M S, R D N, L D, C C R P
 Intensive Cardiac Rehabilitation R U T H A D A M I E C, M A, M S, R D N, L D, C C R P None to disclose. Financial Disclosures Overview Evolution of Cardiac Rehab and Influence of Lifestyle Medicine Introduction
Intensive Cardiac Rehabilitation R U T H A D A M I E C, M A, M S, R D N, L D, C C R P None to disclose. Financial Disclosures Overview Evolution of Cardiac Rehab and Influence of Lifestyle Medicine Introduction
The Role of Cardiac Rehabilitation in Recovery & Secondary Prevention. Loren M Stabile, MS Cardiac & Pulmonary Rehab Program Manager
 The Role of Cardiac Rehabilitation in Recovery & Secondary Prevention Loren M Stabile, MS Cardiac & Pulmonary Rehab Program Manager Objectives Core Components of Cardiac Rehab Program CR Indications &
The Role of Cardiac Rehabilitation in Recovery & Secondary Prevention Loren M Stabile, MS Cardiac & Pulmonary Rehab Program Manager Objectives Core Components of Cardiac Rehab Program CR Indications &
The importance of follow-up after a cardiac event: CARDIAC REHABILITATION. Dr. Guy Letcher
 The importance of follow-up after a cardiac event: CARDIAC REHABILITATION Dr. Guy Letcher The National Medicare Experience Mortality After Angioplasty 225,915 patients Mortality After Bypass Surgery 357,885
The importance of follow-up after a cardiac event: CARDIAC REHABILITATION Dr. Guy Letcher The National Medicare Experience Mortality After Angioplasty 225,915 patients Mortality After Bypass Surgery 357,885
Outpatient Cardiac Rehabilitation
 Last Review Date: May 12, 2017 Number: MG.MM.ME.26bC3v2 Medical Guideline Disclaimer Property of EmblemHealth. All rights reserved. The treating physician or primary care provider must submit to EmblemHealth
Last Review Date: May 12, 2017 Number: MG.MM.ME.26bC3v2 Medical Guideline Disclaimer Property of EmblemHealth. All rights reserved. The treating physician or primary care provider must submit to EmblemHealth
Biological Correlates of Frailty in Older Heart Failure Patients
 Biological Correlates of Frailty in Older Heart Failure Patients Dalane W. Kitzman, MD Professor of Internal Medicine: Cardiovascular Medicine and Geriatrics Kermit Glenn Phillips II Chair in Cardiology
Biological Correlates of Frailty in Older Heart Failure Patients Dalane W. Kitzman, MD Professor of Internal Medicine: Cardiovascular Medicine and Geriatrics Kermit Glenn Phillips II Chair in Cardiology
Introducing the COAPT Trial
 physician INFORMATION Eligible patients Symptomatic functional mitral regurgitation 3+ Not suitable candidates for open mitral valve surgery NYHA functional class II, III, or ambulatory IV Introducing
physician INFORMATION Eligible patients Symptomatic functional mitral regurgitation 3+ Not suitable candidates for open mitral valve surgery NYHA functional class II, III, or ambulatory IV Introducing
CARDIAC REHABILITATION
 CARDIAC REHABILITATION A N A B A R A C M D, P H D M E D S T A R H E A R T A N D V A S C U L A R I N S T I T U T E, M E D S T A R W A S H I N G T O N H O S P I T A L C E N T E R OBJECTIVES Rationale for
CARDIAC REHABILITATION A N A B A R A C M D, P H D M E D S T A R H E A R T A N D V A S C U L A R I N S T I T U T E, M E D S T A R W A S H I N G T O N H O S P I T A L C E N T E R OBJECTIVES Rationale for
Clinical Policy Title: Cardiac rehabilitation
 Clinical Policy Title: Cardiac rehabilitation Clinical Policy Number: 04.02.02 Effective Date: September 1, 2013 Initial Review Date: February 19, 2013 Most Recent Review Date: February 6, 2018 Next Review
Clinical Policy Title: Cardiac rehabilitation Clinical Policy Number: 04.02.02 Effective Date: September 1, 2013 Initial Review Date: February 19, 2013 Most Recent Review Date: February 6, 2018 Next Review
Cardiac Rehabilitation Program for LVAD Patients. Dr Katherine Fan Consultant Cardiologist Grantham Hospital, Hong Kong SAR
 Cardiac Rehabilitation Program for LVAD Patients Dr Katherine Fan Consultant Cardiologist Grantham Hospital, Hong Kong SAR Left Ventricular Assist Devices (LVAD) Improved Survival Following LVAD Implantations
Cardiac Rehabilitation Program for LVAD Patients Dr Katherine Fan Consultant Cardiologist Grantham Hospital, Hong Kong SAR Left Ventricular Assist Devices (LVAD) Improved Survival Following LVAD Implantations
Cardiac Rehabilitation Should be Paid in Korea?
 Cardiac Rehabilitation Should be Paid in Korea? Cardiac prevention & Rehabilitation Center, Heart Institute, Asan Medical Center, Seoul, Korea Jong-Young Lee, MD. NO CONFLICT OF INTEREST TO DECLARE Before
Cardiac Rehabilitation Should be Paid in Korea? Cardiac prevention & Rehabilitation Center, Heart Institute, Asan Medical Center, Seoul, Korea Jong-Young Lee, MD. NO CONFLICT OF INTEREST TO DECLARE Before
Value of cardiac rehabilitation Prof. Dr. L Vanhees
 Session: At the interface of hypertension and coronary heart disease haemodynamics, heart and hypertension Value of cardiac rehabilitation Prof. Dr. L Vanhees ESC Stockholm August 2010 Introduction There
Session: At the interface of hypertension and coronary heart disease haemodynamics, heart and hypertension Value of cardiac rehabilitation Prof. Dr. L Vanhees ESC Stockholm August 2010 Introduction There
Therapeutic Targets and Interventions
 Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
Curtin University is a trademark of Curtin University of Technology CRICOS Provider Code 00301J
 Exercise-based cardiac rehabilitation for people with ventricular assist devices: Associate Professor Andrew Maiorana School of Physiotherapy and Exercise Science, Curtin University; Advanced Heart Failure
Exercise-based cardiac rehabilitation for people with ventricular assist devices: Associate Professor Andrew Maiorana School of Physiotherapy and Exercise Science, Curtin University; Advanced Heart Failure
The Best Kept Secret in Your Medical Neighborhood. Evidence Based Cardiac and Pulmonary Rehabilitation
 The Best Kept Secret in Your Medical Neighborhood Evidence Based Cardiac and Pulmonary Rehabilitation Marjorie King, MD, FACC, MAACVPR Past President, AACVPR Chief Medical Officer Helen Hayes Hospital
The Best Kept Secret in Your Medical Neighborhood Evidence Based Cardiac and Pulmonary Rehabilitation Marjorie King, MD, FACC, MAACVPR Past President, AACVPR Chief Medical Officer Helen Hayes Hospital
The life after myocardial infarction: a long quiet river?
 The life after myocardial infarction: a long quiet river? Cardiac rehabilitation: for whom and how? Dr. Barnabas GELLEN MD, PhD, FESC Poitiers JESFC 2018 - Paris Conflicts of interest Speaker honoraria
The life after myocardial infarction: a long quiet river? Cardiac rehabilitation: for whom and how? Dr. Barnabas GELLEN MD, PhD, FESC Poitiers JESFC 2018 - Paris Conflicts of interest Speaker honoraria
The role of CPX testing in the rehabilitation of cardiac patients.
 Cardiopulmonary exercise testing (CPX) for comprehensive cardiac evaluations The role of CPX testing in the rehabilitation of cardiac patients. Viviane M Conraads, MD, PhD Department of Cardiology Cardiac
Cardiopulmonary exercise testing (CPX) for comprehensive cardiac evaluations The role of CPX testing in the rehabilitation of cardiac patients. Viviane M Conraads, MD, PhD Department of Cardiology Cardiac
Rehabilitation for Cardiovascular Disease: Updates and Opportunities. Jonathan R. Murrow, MD Associate Professor of Medicine (Cardiology)
") Rehabilitation for Cardiovascular Disease: Updates and Opportunities Jonathan R. Murrow, MD Associate Professor of Medicine (Cardiology) Disclosures Grants: American Heart Association Grant-in-Aid Novartis
Rehabilitation for Cardiovascular Disease: Updates and Opportunities Jonathan R. Murrow, MD Associate Professor of Medicine (Cardiology) Disclosures Grants: American Heart Association Grant-in-Aid Novartis
Cardiac Rehabilitation
 Easy Choice Health Plan Harmony Health Plan of Illinois Missouri Care Ohana Health Plan, a plan offered by WellCare Health Insurance of Arizona OneCare (Care1st Health Plan Arizona, Inc.) Staywell of Florida
Easy Choice Health Plan Harmony Health Plan of Illinois Missouri Care Ohana Health Plan, a plan offered by WellCare Health Insurance of Arizona OneCare (Care1st Health Plan Arizona, Inc.) Staywell of Florida
CHRONIC HEART FAILURE : WHAT ELSE COULD WE OFFER TO OUR PATIENTS? Cardiac Rehabilitation Society of Thailand
 CHRONIC HEART FAILURE : WHAT ELSE COULD WE OFFER TO OUR PATIENTS? Cardiac Rehabilitation Society of Thailand ENHANCED EXTERNAL COUNTER PULSATION Piyanuj Ruckpanich, MD. Cardiac Rehabilitation Center Perfect
CHRONIC HEART FAILURE : WHAT ELSE COULD WE OFFER TO OUR PATIENTS? Cardiac Rehabilitation Society of Thailand ENHANCED EXTERNAL COUNTER PULSATION Piyanuj Ruckpanich, MD. Cardiac Rehabilitation Center Perfect
PHYSICAL AND SEXUAL ACTIVITIES
 Forgotten problems in HF PHYSICAL AND SEXUAL ACTIVITIES Massimo F Piepoli, MD, PhD, FESC, FACC Heart Failure Unit, Guglielmo da Saliceto Hospital, Piacenza m.piepoli@alice.it No disclosures Massimo Speaker
Forgotten problems in HF PHYSICAL AND SEXUAL ACTIVITIES Massimo F Piepoli, MD, PhD, FESC, FACC Heart Failure Unit, Guglielmo da Saliceto Hospital, Piacenza m.piepoli@alice.it No disclosures Massimo Speaker
Summary/Key Points Introduction
 Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Performance and Quality Measures 1. NQF Measure Number. Coronary Artery Disease Measure Set
 Unless indicated, the PINNACLE Registry measures are endorsed by the American College of Cardiology Foundation and the American Heart Association and may be used for purposes of health care insurance payer
Unless indicated, the PINNACLE Registry measures are endorsed by the American College of Cardiology Foundation and the American Heart Association and may be used for purposes of health care insurance payer
Catheter-based mitral valve repair MitraClip System
 Percutaneous Mitral Valve Repair: Results of the EVEREST II Trial William A. Gray MD Director of Endovascular Services Associate Professor of Clinical Medicine Columbia University Medical Center The Cardiovascular
Percutaneous Mitral Valve Repair: Results of the EVEREST II Trial William A. Gray MD Director of Endovascular Services Associate Professor of Clinical Medicine Columbia University Medical Center The Cardiovascular
Individualizing and Expanding Care ( Perspectives for the VCN from )
") Cardiac Rehabilitation 2018: Individualizing and Expanding Care ( Perspectives for the VCN from 1984 2018) Philip A. Ades MD University of Vermont College of Medicine Director, CR and Preventive Cardiology
Cardiac Rehabilitation 2018: Individualizing and Expanding Care ( Perspectives for the VCN from 1984 2018) Philip A. Ades MD University of Vermont College of Medicine Director, CR and Preventive Cardiology
Quality Payment Program: Cardiology Specialty Measure Set
 Quality Payment Program: Cardiology Specialty Set Title Number CMS Reporting Method(s) Heart Failure (HF): Angiotensin- Converting Enzyme (ACE) Inhibitor or Angiotensin Receptor Blocker (ARB) Therapy for
Quality Payment Program: Cardiology Specialty Set Title Number CMS Reporting Method(s) Heart Failure (HF): Angiotensin- Converting Enzyme (ACE) Inhibitor or Angiotensin Receptor Blocker (ARB) Therapy for
HFpEF, Mito or Realidad?
 HFpEF, Mito or Realidad? Ileana L. Piña, MD, MPH Professor of Medicine and Epidemiology/Population Health Associate Chief for Academic Affairs -- Cardiology Montefiore-Einstein Medical Center Bronx, NY
HFpEF, Mito or Realidad? Ileana L. Piña, MD, MPH Professor of Medicine and Epidemiology/Population Health Associate Chief for Academic Affairs -- Cardiology Montefiore-Einstein Medical Center Bronx, NY
Cardiac Rehabilitation in the Outpatient Setting. Description
 Subject: Cardiac Rehabilitation in the Outpatient Setting Page: 1 of 10 Last Review Status/Date: September 2014 Cardiac Rehabilitation in the Outpatient Setting Description Cardiac rehabilitation refers
Subject: Cardiac Rehabilitation in the Outpatient Setting Page: 1 of 10 Last Review Status/Date: September 2014 Cardiac Rehabilitation in the Outpatient Setting Description Cardiac rehabilitation refers
Focus on Rehabilitation, Exercise and Surgical Coronary Revascularization
 Focus on Rehabilitation, Exercise and Surgical Coronary Revascularization Sam Haddad, MD Kenneth O Reilly, MD Disclosure of Commercial or Pharma Support NTD Learning Objectives At the conclusion of this
Focus on Rehabilitation, Exercise and Surgical Coronary Revascularization Sam Haddad, MD Kenneth O Reilly, MD Disclosure of Commercial or Pharma Support NTD Learning Objectives At the conclusion of this
Management of Stable Ischemic Heart Disease. Vinay Madan MD February 10, 2018
 Management of Stable Ischemic Heart Disease Vinay Madan MD February 10, 2018 1 Disclosure No financial disclosure. 2 Overview of SIHD Diagnosis Outline of talk Functional vs. Anatomic assessment Management
Management of Stable Ischemic Heart Disease Vinay Madan MD February 10, 2018 1 Disclosure No financial disclosure. 2 Overview of SIHD Diagnosis Outline of talk Functional vs. Anatomic assessment Management
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Cardiac Rehabilitation in the Outpatient Setting Page 1 of 17 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Cardiac Rehabilitation in the Outpatient Setting Professional
Cardiac Rehabilitation in the Outpatient Setting Page 1 of 17 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Cardiac Rehabilitation in the Outpatient Setting Professional
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Cardiac Rehabilitation in the Outpatient Setting Page 1 of 16 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Cardiac Rehabilitation in the Outpatient Setting Professional
Cardiac Rehabilitation in the Outpatient Setting Page 1 of 16 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Cardiac Rehabilitation in the Outpatient Setting Professional
The Future of Cardiac Care: Managing Our Patients Together
 The Future of Cardiac Care: Managing Our Patients Together Charles R. Caldwell, MD, FACC Disclosures: iheartdoc,inc. Telemedicine 1 MACRA Medicare Access and CHIP Reauthorization Act of 2015 Repealed the
The Future of Cardiac Care: Managing Our Patients Together Charles R. Caldwell, MD, FACC Disclosures: iheartdoc,inc. Telemedicine 1 MACRA Medicare Access and CHIP Reauthorization Act of 2015 Repealed the
Scope
 Scope Global burden of heart disease Physical activity trends Overview of CR A happy problem Principles of CR in athletes Classification of sport Existing guidelines Exercise testing & prescription HIIT
Scope Global burden of heart disease Physical activity trends Overview of CR A happy problem Principles of CR in athletes Classification of sport Existing guidelines Exercise testing & prescription HIIT
CARDIAC REHABILITATION AFTER TRANSCATHETER AORTIC VALVE IMPLANTATION: A SINGLE CENTRE EXPERIENCE
 ESC Congress 2011 27 Aug - 31 Aug 2011, Paris - France CARDIAC REHABILITATION AFTER TRANSCATHETER AORTIC VALVE IMPLANTATION: A SINGLE CENTRE EXPERIENCE N.Russo, L.Compostella, T.Setzu, M.Napodano, L.Testolin,
ESC Congress 2011 27 Aug - 31 Aug 2011, Paris - France CARDIAC REHABILITATION AFTER TRANSCATHETER AORTIC VALVE IMPLANTATION: A SINGLE CENTRE EXPERIENCE N.Russo, L.Compostella, T.Setzu, M.Napodano, L.Testolin,
Quality Payment Program: Cardiology Specialty Measure Set
 Measure Title * Reportable via PINNACLE α Reportable via Diabetes Collaborative CQMC v1.0 Measure High Priority Measure Cross Cutting Measure Heart Failure (HF): Angiotensin- Converting Enzyme (ACE) Inhibitor
Measure Title * Reportable via PINNACLE α Reportable via Diabetes Collaborative CQMC v1.0 Measure High Priority Measure Cross Cutting Measure Heart Failure (HF): Angiotensin- Converting Enzyme (ACE) Inhibitor
Controversies in Cardiac Pharmacology
 Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Cardiac Rehabilitation & Exercise Training in Congenital Heart Disease. Jidong Sung Division of Cardiology Sungkyunkwan University School of Medicine
 Cardiac Rehabilitation & Exercise Training in Congenital Heart Disease Jidong Sung Division of Cardiology Sungkyunkwan University School of Medicine Cardiac rehabilitation Agency of Health Care Policy
Cardiac Rehabilitation & Exercise Training in Congenital Heart Disease Jidong Sung Division of Cardiology Sungkyunkwan University School of Medicine Cardiac rehabilitation Agency of Health Care Policy
High Intensity Interval Exercise Training in Cardiac Rehabilitation
 High Intensity Interval Exercise Training in Cardiac Rehabilitation Prof. Leonard S.W. Li Hon. Clinical Professor, Department of Medicine, The University of Hong Kong Director, Rehabilitation Virtus Medical
High Intensity Interval Exercise Training in Cardiac Rehabilitation Prof. Leonard S.W. Li Hon. Clinical Professor, Department of Medicine, The University of Hong Kong Director, Rehabilitation Virtus Medical
Exercise Testing and Training in Heart Failure Patients Robert S. McKelvie, MD, PhD, FRCPC, Hamilton Health Sciences - General Division
 Exercise Testing and Training in Heart Failure Patients Robert S. McKelvie, MD, PhD, FRCPC, Hamilton Health Sciences - General Division Studies have demonstrated that there is no relationship between left
Exercise Testing and Training in Heart Failure Patients Robert S. McKelvie, MD, PhD, FRCPC, Hamilton Health Sciences - General Division Studies have demonstrated that there is no relationship between left
Surgery Grand Rounds
 Surgery Grand Rounds Coronary Artery Bypass Grafting versus Coronary Artery Stenting Charles Ted Lord, R1 Coronary Artery Disease Stenosis of epicardial vessels Metabolic & hematologic Statistics 500,000
Surgery Grand Rounds Coronary Artery Bypass Grafting versus Coronary Artery Stenting Charles Ted Lord, R1 Coronary Artery Disease Stenosis of epicardial vessels Metabolic & hematologic Statistics 500,000
H2H Early Follow-up Challenge: See You in 7. Webinar #1 Thursday, March 3, :00 pm 4:00 pm ET. Welcome
 H2H Early Follow-up Challenge: See You in 7 Webinar #1 Thursday, March 3, 2011 3:00 pm 4:00 pm ET 1 Welcome Take Home Messages Renew your H2H commitment Participate in the first H2H Challenge Help build
H2H Early Follow-up Challenge: See You in 7 Webinar #1 Thursday, March 3, 2011 3:00 pm 4:00 pm ET 1 Welcome Take Home Messages Renew your H2H commitment Participate in the first H2H Challenge Help build
Cardiac Rehabilitation Individualized Healing for Patients with Cardiovascular Disease
 Cardiac Rehabilitation Individualized Healing for Patients with Cardiovascular Disease Richard A. Josephson MS, MD FACC, FAHA, FACP, FAACVPR Director of Cardiac Intensive Care Director of Cardiovascular
Cardiac Rehabilitation Individualized Healing for Patients with Cardiovascular Disease Richard A. Josephson MS, MD FACC, FAHA, FACP, FAACVPR Director of Cardiac Intensive Care Director of Cardiovascular
Burden of Mitral Regurgitation (MR) in the US Why is This Important?
 in the US Why is This Important?") Secondary (Functional) Mitral Regurgitation as a Target for Heart Failure Therapy William T. Abraham, MD, FACP, FACC, FAHA, FESC, FRCP Professor of Medicine, Physiology, and Cell Biology Chair of Excellence
Secondary (Functional) Mitral Regurgitation as a Target for Heart Failure Therapy William T. Abraham, MD, FACP, FACC, FAHA, FESC, FRCP Professor of Medicine, Physiology, and Cell Biology Chair of Excellence
Patient-Reported Outcomes: A Critical Insight into the Impact of Therapy
 Patient-Reported Outcomes: A Critical Insight into the Impact of Therapy John Spertus MD MPH Missouri/Lauer Endowed Chair and Professor, UMKC Saint Luke s Mid America Heart Institute Presentation Overview
Patient-Reported Outcomes: A Critical Insight into the Impact of Therapy John Spertus MD MPH Missouri/Lauer Endowed Chair and Professor, UMKC Saint Luke s Mid America Heart Institute Presentation Overview
Exercise after CABG: The Good The Bad and the Ugly
 Exercise after CABG: The Good The Bad and the Ugly Ph Meurin. Les Grands Prés (Villeneuve Saint Denis) No conflict of Interest After CABG, the Prognosis is Good.. Age 65 ± 10 Male Gender 80 % Pre-op LVEF
Exercise after CABG: The Good The Bad and the Ugly Ph Meurin. Les Grands Prés (Villeneuve Saint Denis) No conflict of Interest After CABG, the Prognosis is Good.. Age 65 ± 10 Male Gender 80 % Pre-op LVEF
Program Metrics. New Unique ID. Old Unique ID. Metric Set Metric Name Description. Old Metric Name
 Program Metrics The list below includes the metrics that will be calculated by the PINNACLE Registry for the outpatient office setting. These include metrics for, Atrial Fibrillation, Hypertension and.
Program Metrics The list below includes the metrics that will be calculated by the PINNACLE Registry for the outpatient office setting. These include metrics for, Atrial Fibrillation, Hypertension and.
Revascularization in Severe LV Dysfunction: The Role of Inducible Ischemia and Viability Testing
 Revascularization in Severe LV Dysfunction: The Role of Inducible Ischemia and Viability Testing Evidence and Uncertainties Robert O. Bonow, MD, MS, MACC Northwestern University Feinberg School of Medicine
Revascularization in Severe LV Dysfunction: The Role of Inducible Ischemia and Viability Testing Evidence and Uncertainties Robert O. Bonow, MD, MS, MACC Northwestern University Feinberg School of Medicine
Rational use of imaging for viability evaluation
 EUROECHO and other imaging modalities 2011 Rational use of imaging for viability evaluation Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology, CHU Liège, Belgium
EUROECHO and other imaging modalities 2011 Rational use of imaging for viability evaluation Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology, CHU Liège, Belgium
BACPR Annual Conference Generic versus Specialist Rehabilitation FOR
 BACPR Annual Conference 2016 Generic versus Specialist Rehabilitation FOR Dr William Man 1) Organ-specific rehabilitation for heart failure and COPD is an outdated concept... 2) Rehabilitation should
BACPR Annual Conference 2016 Generic versus Specialist Rehabilitation FOR Dr William Man 1) Organ-specific rehabilitation for heart failure and COPD is an outdated concept... 2) Rehabilitation should
Minimally invasive therapies for the mitral valve: How will you incorporate into your clinical practice? Guilherme F.
 Minimally invasive therapies for the mitral valve: How will you incorporate into your clinical practice? Guilherme F. Attizzani, MD UH Harrington Heart and Vascular Institute Interventional Cardiologist/Structural
Minimally invasive therapies for the mitral valve: How will you incorporate into your clinical practice? Guilherme F. Attizzani, MD UH Harrington Heart and Vascular Institute Interventional Cardiologist/Structural
Subject: Outpatient Phase Ii Cardiac Rehab Individualized Treatment Plan And Exercise Prescription
 CARDIAC REHAB POLICY & PROCEDURES Policy #: CR 208 Subject: Outpatient Phase Ii Cardiac Rehab Individualized Treatment Plan And Exercise Prescription Purpose: To establish guidelines for developing and
CARDIAC REHAB POLICY & PROCEDURES Policy #: CR 208 Subject: Outpatient Phase Ii Cardiac Rehab Individualized Treatment Plan And Exercise Prescription Purpose: To establish guidelines for developing and
Tuesday, October 4, chapter CHAPTER 11
 chapter CHAPTER 11 11 chapter CHAPTER 11 Physiology of Physical Activity Jennifer L. Caputo PHYSIOLOGY OF PHYSICAL ACTIVITY The study of acute (immediate) physiological responses to physical activity and
chapter CHAPTER 11 11 chapter CHAPTER 11 Physiology of Physical Activity Jennifer L. Caputo PHYSIOLOGY OF PHYSICAL ACTIVITY The study of acute (immediate) physiological responses to physical activity and
Long-Term Management Of the ACS Patient: State-of-the-Art. Kim Newlin, CNS, NP-C, FPCNA Sutter Roseville Medical Center Roseville, CA
 Long-Term Management Of the ACS Patient: State-of-the-Art Kim Newlin, CNS, NP-C, FPCNA Sutter Roseville Medical Center Roseville, CA Disclosures I have no disclosures. Case Study 45 y/o male admitted to
Long-Term Management Of the ACS Patient: State-of-the-Art Kim Newlin, CNS, NP-C, FPCNA Sutter Roseville Medical Center Roseville, CA Disclosures I have no disclosures. Case Study 45 y/o male admitted to
Evidence-Based Management of CAD: Last Decade Trials and Updated Guidelines
 Evidence-Based Management of CAD: Last Decade Trials and Updated Guidelines Enrico Ferrari, MD Cardiac Surgery Unit Cardiocentro Ticino Foundation Lugano, Switzerland Conflict of Interests No conflict
Evidence-Based Management of CAD: Last Decade Trials and Updated Guidelines Enrico Ferrari, MD Cardiac Surgery Unit Cardiocentro Ticino Foundation Lugano, Switzerland Conflict of Interests No conflict
Women s Ischemia and cardiac rehabilitation
 Women s Ischemia and cardiac rehabilitation Dr. Pallavi Bellamkonda MD, FACC Financial Disclosures: None 1 Objectives Understanding the Unique presentations of Ischemic Disease in Women: Obstructive Coronary
Women s Ischemia and cardiac rehabilitation Dr. Pallavi Bellamkonda MD, FACC Financial Disclosures: None 1 Objectives Understanding the Unique presentations of Ischemic Disease in Women: Obstructive Coronary
Patient characteristics Intervention Comparison Length of followup
 ISCHAEMIA TESTING CHAPTER TESTING FOR MYCOCARDIAL ISCHAEMIA VERSUS NOT TESTING FOR MYOCARDIAL ISCHAEMIA Ref ID: 4154 Reference Wienbergen H, Kai GA, Schiele R et al. Actual clinical practice exercise ing
ISCHAEMIA TESTING CHAPTER TESTING FOR MYCOCARDIAL ISCHAEMIA VERSUS NOT TESTING FOR MYOCARDIAL ISCHAEMIA Ref ID: 4154 Reference Wienbergen H, Kai GA, Schiele R et al. Actual clinical practice exercise ing
Populations Interventions Comparators Outcomes Individuals: With diagnosed heart disease. rehabilitation
 Protocol Cardiac Rehabilitation in the Outpatient Setting (80308) Medical Benefit Effective Date: 01/01/17 Next Review Date: 05/18 Preauthorization No Review Dates: 07/07, 07/08, 05/09, 05/10, 05/11, 05/12,
Protocol Cardiac Rehabilitation in the Outpatient Setting (80308) Medical Benefit Effective Date: 01/01/17 Next Review Date: 05/18 Preauthorization No Review Dates: 07/07, 07/08, 05/09, 05/10, 05/11, 05/12,
What the Cardiologist needs to know from Medical Images
 What the Cardiologist needs to know from Medical Images Gerald Maurer Department of Cardiology Medical University of Vienna What kinds of Cardiologists Plumbers Electricians Photographers And then there
What the Cardiologist needs to know from Medical Images Gerald Maurer Department of Cardiology Medical University of Vienna What kinds of Cardiologists Plumbers Electricians Photographers And then there
Heart Failure with Preserved Left Ventricular Ejection Fraction. (HFpEF)
") Thessaloniki, May 27, 2017 Heart Failure with Preserved Left Ventricular Ejection Fraction Filippos Triposkiadis, MD, FESC, FACC Professor of Cardiology Director, Department of Cardiology Larissa University
Thessaloniki, May 27, 2017 Heart Failure with Preserved Left Ventricular Ejection Fraction Filippos Triposkiadis, MD, FESC, FACC Professor of Cardiology Director, Department of Cardiology Larissa University
Role of Cardiopulmonary Exercise Testing in Exercise Prescription
 Role of Cardiopulmonary Exercise Testing in Exercise Prescription Jonathan Myers, PhD VA Palo Alto Health Care System Stanford University There are no conflicts of interest to disclose Role of Cardiopulmonary
Role of Cardiopulmonary Exercise Testing in Exercise Prescription Jonathan Myers, PhD VA Palo Alto Health Care System Stanford University There are no conflicts of interest to disclose Role of Cardiopulmonary
Chapter 21 Training for Anaerobic and Aerobic Power
 Section 06: Exercise Training to Improve Performance Chapter 21 Training for Anaerobic and Aerobic Power Chapter 22 Muscular Strength: Training Muscles to Become Stronger Chapter 23 Special Aids to Exercise
Section 06: Exercise Training to Improve Performance Chapter 21 Training for Anaerobic and Aerobic Power Chapter 22 Muscular Strength: Training Muscles to Become Stronger Chapter 23 Special Aids to Exercise
The Failing Heart in Primary Care
 The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
11/19/2013. Cardiac Rehabilitation Coverage and Documentation Requirements. Phases of Cardiac Rehabilitation. Phase II
 Cardiac Rehabilitation Coverage and Documentation Requirements Phases of Cardiac Rehabilitation Phase I: Acute in-hospital phase of CR Phase II: is the initial outpatient phase of the program Phase III:
Cardiac Rehabilitation Coverage and Documentation Requirements Phases of Cardiac Rehabilitation Phase I: Acute in-hospital phase of CR Phase II: is the initial outpatient phase of the program Phase III:
Reliability of the incremental shuttle walk test and the Chester step test in cardiac rehabilitation
 Reliability of the incremental shuttle walk test and the Chester step test in cardiac rehabilitation Item Type Thesis or dissertation Authors Reardon, Melanie Publisher University of Chester Download date
Reliability of the incremental shuttle walk test and the Chester step test in cardiac rehabilitation Item Type Thesis or dissertation Authors Reardon, Melanie Publisher University of Chester Download date
Management of Heart Failure in Adult with Congenital Heart Disease
 Management of Heart Failure in Adult with Congenital Heart Disease Ahmed Krimly Interventional and ACHD consultant King Faisal Cardiac Center National Guard Jeddah Background 0.4% of adults have some form
Management of Heart Failure in Adult with Congenital Heart Disease Ahmed Krimly Interventional and ACHD consultant King Faisal Cardiac Center National Guard Jeddah Background 0.4% of adults have some form
The Bypassing the Blues Trial: Telephone-Delivered Collaborative Care for Treating Post-CABG Depression
 The Bypassing the Blues Trial: Telephone-Delivered Collaborative Care for Treating Post-CABG Depression www.bypassingtheblues.pitt.edu Bruce L. Rollman, MD, MPH Professor of Medicine, Psychiatry, and Clinical
The Bypassing the Blues Trial: Telephone-Delivered Collaborative Care for Treating Post-CABG Depression www.bypassingtheblues.pitt.edu Bruce L. Rollman, MD, MPH Professor of Medicine, Psychiatry, and Clinical
Understanding the guidelines for Interventions in MR. Ali AlMasood
 Understanding the guidelines for Interventions in MR Ali AlMasood Mitral regurgitation The most diverse from all acquired valve diseases About 50% of patients with an LVEF 35 percent had moderate to severe
Understanding the guidelines for Interventions in MR Ali AlMasood Mitral regurgitation The most diverse from all acquired valve diseases About 50% of patients with an LVEF 35 percent had moderate to severe
ST2 in Heart Failure. ST2 as a Cardiovascular Biomarker. Competitive Model of ST2/IL-33 Signaling. ST2 and IL-33: Cardioprotective
 ST2 as a Cardiovascular Biomarker Lori B. Daniels, MD, MAS, FACC Professor of Medicine Director, Coronary Care Unit University of California, San Diego ST2 and IL-33: Cardioprotective ST2: member of the
ST2 as a Cardiovascular Biomarker Lori B. Daniels, MD, MAS, FACC Professor of Medicine Director, Coronary Care Unit University of California, San Diego ST2 and IL-33: Cardioprotective ST2: member of the
Interest of PVO2 assesment in HFpEF patients
 Interest of PVO2 assesment in HFpEF patients Jean Yves TABET CRCB, Villeneuve Saint Denis Institut Jacques Cartier, Massy Conflits of interest none Interest of PVO2 in HFr EF Evaluation of exercise tolerance
Interest of PVO2 assesment in HFpEF patients Jean Yves TABET CRCB, Villeneuve Saint Denis Institut Jacques Cartier, Massy Conflits of interest none Interest of PVO2 in HFr EF Evaluation of exercise tolerance
Congestive Heart Failure: Outpatient Management
 The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend )
") Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend ) Stephen G. Ellis, MD Section Head, Interventional Cardiology Professor of Medicine Cleveland
Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend ) Stephen G. Ellis, MD Section Head, Interventional Cardiology Professor of Medicine Cleveland
Take-home Messages from Recent Heart Failure Trials: Heart Rate as a Target
 Take-home Messages from Recent Heart Failure Trials: Heart Rate as a Target JEFFREY S. BORER, M.D. Professor and Chairman, Department of Medicine and Chief, Division of Cardiovascular Medicine; Director,
Take-home Messages from Recent Heart Failure Trials: Heart Rate as a Target JEFFREY S. BORER, M.D. Professor and Chairman, Department of Medicine and Chief, Division of Cardiovascular Medicine; Director,
Patient Navigator Program: Focus MI Diplomat Hospital Metrics
 Patient Navigator Program: Focus MI Diplomat Hospital Metrics Goal Statement: To reduce avoidable hospital readmissions for patients discharged with acute myocardial infarction (AMI) by supporting a culture
Patient Navigator Program: Focus MI Diplomat Hospital Metrics Goal Statement: To reduce avoidable hospital readmissions for patients discharged with acute myocardial infarction (AMI) by supporting a culture
New PINNACLE Measures The below measures for PINNACLE will be added as new measures to the outcomes reporting starting with Version 2.0.
 New PINNACLE Measures The below measures for PINNACLE will be added as new measures to the outcomes reporting starting with Version 2.0. Measure Steward Measure Name Measure Description Rationale for Adding
New PINNACLE Measures The below measures for PINNACLE will be added as new measures to the outcomes reporting starting with Version 2.0. Measure Steward Measure Name Measure Description Rationale for Adding
Glenn Bean, M.S., FAACVPR
 Glenn Bean, M.S., FAACVPR Tacoma General Hospital/Preventive Cardiology 6/18/2014 1 Journey to Date: 2001: AACVPR formal request for coverage of CR for HF patients 2006: CMS- No (Yes for PCI, valve repair/replacement,
Glenn Bean, M.S., FAACVPR Tacoma General Hospital/Preventive Cardiology 6/18/2014 1 Journey to Date: 2001: AACVPR formal request for coverage of CR for HF patients 2006: CMS- No (Yes for PCI, valve repair/replacement,
Impaired Chronotropic Response to Exercise Stress Testing in Patients with Diabetes Predicts Future Cardiovascular Events
 Diabetes Care Publish Ahead of Print, published online May 28, 2008 Chronotropic response in patients with diabetes Impaired Chronotropic Response to Exercise Stress Testing in Patients with Diabetes Predicts
Diabetes Care Publish Ahead of Print, published online May 28, 2008 Chronotropic response in patients with diabetes Impaired Chronotropic Response to Exercise Stress Testing in Patients with Diabetes Predicts
Supplement materials:
 Supplement materials: Table S1: ICD-9 codes used to define prevalent comorbid conditions and incident conditions Comorbid condition ICD-9 code Hypertension 401-405 Diabetes mellitus 250.x Myocardial infarction
Supplement materials: Table S1: ICD-9 codes used to define prevalent comorbid conditions and incident conditions Comorbid condition ICD-9 code Hypertension 401-405 Diabetes mellitus 250.x Myocardial infarction
Measurement Name Beta-Blocker Therapy Prior Myocardial Infarction (MI)
") Program Metrics The list below includes the metrics that will be calculated by the PINNACLE Registry for the outpatient office setting. These include metrics for Artery, Atrial Fibrillation, Hypertension
Program Metrics The list below includes the metrics that will be calculated by the PINNACLE Registry for the outpatient office setting. These include metrics for Artery, Atrial Fibrillation, Hypertension
LIZ MIDENCE A DISSERTATION SUBMITTED TO THE FACULTY OF GRADUATE STUDIES IN PARTIAL FULFILMENT OF THE REQUIREMENTS FOR THE DEGREE OF
 WOMEN S CARDIAC REHABILITATION PROGRAM ADHERENCE AND HEALTH BEHAVIOURS FOLLOWING REFERRAL TO THREE DIFFERENT PROGRAM MODELS: A RANDOMIZED CONTROLLED TRIAL LIZ MIDENCE A DISSERTATION SUBMITTED TO THE FACULTY
WOMEN S CARDIAC REHABILITATION PROGRAM ADHERENCE AND HEALTH BEHAVIOURS FOLLOWING REFERRAL TO THREE DIFFERENT PROGRAM MODELS: A RANDOMIZED CONTROLLED TRIAL LIZ MIDENCE A DISSERTATION SUBMITTED TO THE FACULTY
Heart Failure with Preserved EF (HFPEF) Epidemiology and management
 Epidemiology and management") Heart Failure with Preserved EF (HFPEF) Epidemiology and management Karl Swedberg Senior Professor of Medicine Sahlgrenska Academy University of Gothenburg Gothenburg, Sweden e-mail: karl.swedberg@gu.se
Heart Failure with Preserved EF (HFPEF) Epidemiology and management Karl Swedberg Senior Professor of Medicine Sahlgrenska Academy University of Gothenburg Gothenburg, Sweden e-mail: karl.swedberg@gu.se
Cardiac Rehabilitation after Primary Coronary Intervention CONTRA
 DEBATE SESSION Is there a role for cardiac rehabilitation in the modern era of Percutaneous coronary intervention and coronary artery bypass grafting? Cardiac Rehabilitation after Primary Coronary Intervention
DEBATE SESSION Is there a role for cardiac rehabilitation in the modern era of Percutaneous coronary intervention and coronary artery bypass grafting? Cardiac Rehabilitation after Primary Coronary Intervention
Reducing the Population Health Burden of Cardiovascular Disease
 Reducing the Population Health Burden of Cardiovascular Disease Joseph A. Ladapo, MD, PhD Assistant Professor of Medicine Department of Population Health NYU School of Medicine Disclosures: K23 HL116787
Reducing the Population Health Burden of Cardiovascular Disease Joseph A. Ladapo, MD, PhD Assistant Professor of Medicine Department of Population Health NYU School of Medicine Disclosures: K23 HL116787
Quality Measures MIPS CV Specific
 Quality Measures MIPS CV Specific MEASURE NAME Atrial Fibrillation and Atrial Flutter: Chronic Anticoagulation Therapy CAHPS for MIPS Clinician/Group Survey Cardiac Rehabilitation Patient Referral from
Quality Measures MIPS CV Specific MEASURE NAME Atrial Fibrillation and Atrial Flutter: Chronic Anticoagulation Therapy CAHPS for MIPS Clinician/Group Survey Cardiac Rehabilitation Patient Referral from
Steven S. Saliterman, MD, FACP
 Ashley Wagner, Sochi 2014 www.gotceleb.com Steven S. Saliterman, MD, FACP Adjunct Professor Department of Biomedical Engineering, University of Minnesota http://saliterman.umn.edu/ Aerobic (Oxidative Phosphorylation)
Ashley Wagner, Sochi 2014 www.gotceleb.com Steven S. Saliterman, MD, FACP Adjunct Professor Department of Biomedical Engineering, University of Minnesota http://saliterman.umn.edu/ Aerobic (Oxidative Phosphorylation)
What is Spontaneous Coronary Artery Dissection (SCAD) & Why is Cardiac Rehabilitation Important?
 & Why is Cardiac Rehabilitation Important?") What is Spontaneous Coronary Artery Dissection (SCAD) & Why is Cardiac Rehabilitation Important? Marysia Tweet, MD 25 th Annual MNACVPR State Conference October 3 rd, 2015 2015 MFMER slide-1 Goals: Learn
What is Spontaneous Coronary Artery Dissection (SCAD) & Why is Cardiac Rehabilitation Important? Marysia Tweet, MD 25 th Annual MNACVPR State Conference October 3 rd, 2015 2015 MFMER slide-1 Goals: Learn
To Correlate Ejection Fraction with 6 Minute Walked Distance and Quality of Life in Patients with Left Ventricular Heart Failure
 To Correlate Ejection Fraction with 6 Minute Walked Distance and Quality of Life in Patients with Left Ventricular Heart Failure Pramila S Kudtarkar*, Mariya P Jiandani*, Ashish Nabar** Abstract Purpose
To Correlate Ejection Fraction with 6 Minute Walked Distance and Quality of Life in Patients with Left Ventricular Heart Failure Pramila S Kudtarkar*, Mariya P Jiandani*, Ashish Nabar** Abstract Purpose
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes
 Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
HFpEF. April 26, 2018
 HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
Cardiac rehabilitation: a beneficial effect in CHD?
 Cardiac rehabilitation: a beneficial effect in CHD? An Van Berendoncks Department of Cardiology Antwerp University Hospital Outline Why exercise training in CHD? Risk and benefits? Feasibility? Why should
Cardiac rehabilitation: a beneficial effect in CHD? An Van Berendoncks Department of Cardiology Antwerp University Hospital Outline Why exercise training in CHD? Risk and benefits? Feasibility? Why should
Chronic Primary Mitral Regurgitation
 Chronic Primary Mitral Regurgitation The Case For Early Surgical Intervention William K. Freeman, MD, FACC, FASE DISCLOSURES Relevant Financial Relationship(s) None Off Label Usage None Watchful Waiting......
Chronic Primary Mitral Regurgitation The Case For Early Surgical Intervention William K. Freeman, MD, FACC, FASE DISCLOSURES Relevant Financial Relationship(s) None Off Label Usage None Watchful Waiting......
Dual Antiplatelet Therapy Made Practical
 Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
Transcatheter Mitral Valve Repair and Replacement: Where is the Latest Randomized Evidence Taking US Mitral-Fr, COAPT
 Transcatheter Mitral Valve Repair and Replacement: Where is the Latest Randomized Evidence Taking US Mitral-Fr, COAPT and Saibal Kar, MD, FACC, FSCAI Professor of Medicine Director of Interventional Cardiac
Transcatheter Mitral Valve Repair and Replacement: Where is the Latest Randomized Evidence Taking US Mitral-Fr, COAPT and Saibal Kar, MD, FACC, FSCAI Professor of Medicine Director of Interventional Cardiac
Cardiogenic Shock. Carlos Cafri,, MD
 Cardiogenic Shock Carlos Cafri,, MD SHOCK= Inadequate Tissue Mechanisms: Perfusion Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and
Cardiogenic Shock Carlos Cafri,, MD SHOCK= Inadequate Tissue Mechanisms: Perfusion Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and
Checklist for Treating Heart Failure. Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute
 Checklist for Treating Heart Failure Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute Novartis Disclosure Heart Failure (HF) a complex clinical syndrome that arises secondary to abnormalities
Checklist for Treating Heart Failure Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute Novartis Disclosure Heart Failure (HF) a complex clinical syndrome that arises secondary to abnormalities
Diagnosis is it really Heart Failure?
 ESC Congress Munich - 25-29 August 2012 Heart Failure with Preserved Ejection Fraction From Bench to Bedside Diagnosis is it really Heart Failure? Prof. Burkert Pieske Department of Cardiology Med.University
ESC Congress Munich - 25-29 August 2012 Heart Failure with Preserved Ejection Fraction From Bench to Bedside Diagnosis is it really Heart Failure? Prof. Burkert Pieske Department of Cardiology Med.University