7/13/2017. The Process. To Bridge Or Not To Bridge. Periprocedural Management of Anticoagulation in Nonvalvular Atrial Fibrillation: The Problem
|
|
|
- Madlyn Richard
- 6 years ago
- Views:
Transcription
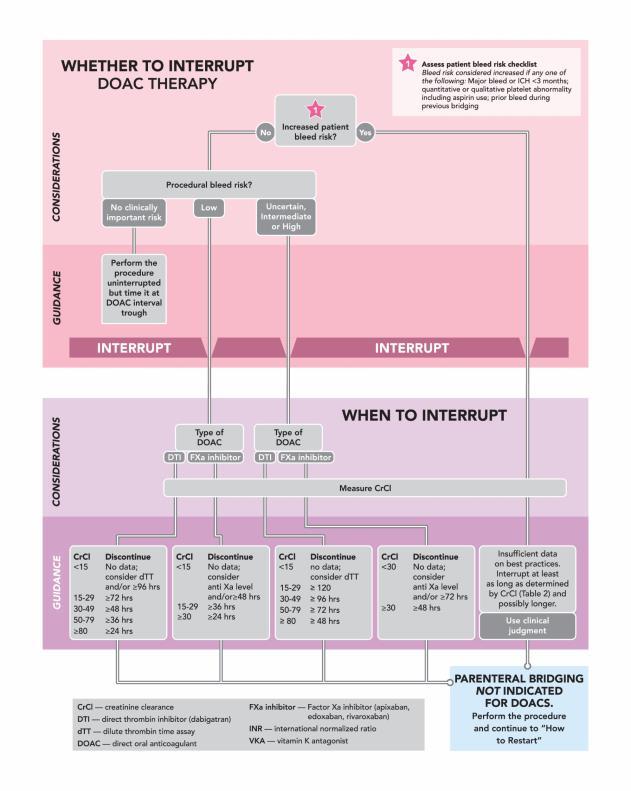
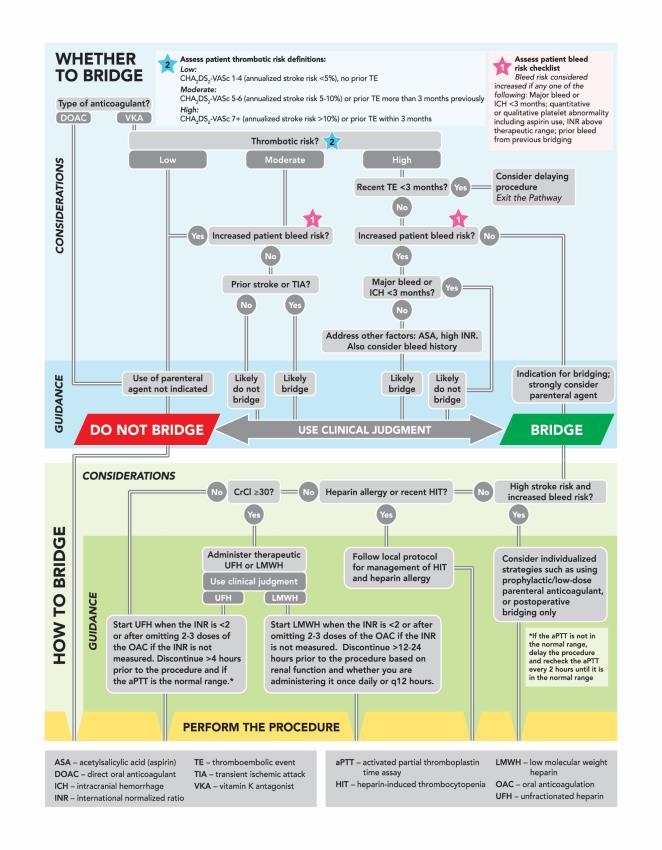
1 Periprocedural Management of Anticoagulation in Nonvalvular Atrial Fibrillation: The Problem 35 million prescriptions written annually in the United States for oral anticoagulation (OAC) 15-20% of these prescriptions are potentially interrupted in a given year placing patients at risk of thrombo-embolic events (TE), bleeding, or death Management of such patients is spread across providers with poor coordination in decision making To Bridge Or Not To Bridge The risk of a TE with an interruption Based on pooled data: (non-randomized in most studies) 0.52% for interruption without bridging 0.94% for those interrupted and bridged In BRIDGE trial alone: 0.4% for interruption without bridging 0.3% for those interrupted and bridged The Process Should the patient be anti-coagulated in the first place? Assess TE risk of interruption (patient specific) Assess risk of bleeding (procedure specific) Are some procedures such low risk that clinicians can fast track decision not to interrupt Are there procedures of sufficient bleeding risk that we would always interrupt? 1

2 The Process Recognize that there are instances where clinical judgment needs to prevail Attempt to give guidance that is procedure-specific 2

3 3
4 Guidance Statement for consideration of postprocedural parenteral anticoagulation: 1. Postprocedural bridging with a parenteral agent can be considered in patients with moderate or high risk of stroke or thromboembolic event. 2. VKA therapy should be resumed (in most cases at the patient s usual therapeutic dose) without use of parenteral anticoagulation in cases associated with high risk for bleeding. Guidance Statement for the initiation of postprocedural therapeutic parenteral anticoagulation in patients with moderate or high thrombotic risk: 1. Establish that hemostasis has been achieved, procedure-specific bleeding complications have been considered, patient-specific bleeding factors have been evaluated, and the proceduralist and the primary managing service are involved in the decision to restart anticoagulation. 2. Following procedures with a lower postprocedural risk of bleeding, therapeutic parenteral anticoagulation, if indicated, can be started within the first 24 hours after the procedure in collaboration with the proceduralist and care team. Guidance Statement for the initiation of postprocedural therapeutic parenteral anticoagulation in patients with moderate or high thrombotic risk: 3. Following procedures with a higher post procedural risk of bleeding, therapeutic parenteral anticoagulation should be delayed for at least hours after the procedure. 4. When VKA therapy is reinitiated, careful monitoring of the INR during bridging is required to mitigate bleed risk. 4
5 Guidance Statement for restarting DOAC therapy post procedure: 1. Establish that hemostasis has been achieved, procedure-specific bleeding complications have been considered, patient-specific bleeding factors have been evaluated, and the proceduralist and primary managing service have been involved in the decision to restart anticoagulation. 2. Following procedures with low postprocedural bleed risk where TI is indicated, it is reasonable to resume DOAC therapy at full dose on the day following the procedure. Guidance Statement for restarting DOAC therapy postprocedure: 3. Following high postprocedural bleed risk procedures, it is reasonable to wait at least hours before resuming DOAC therapy at full dose if complete hemostasis has been achieved. 4. DOAC dosing should reflect postprocedural renal function. Bridging therapeutic anticoagulation with a parenteral agent is generally not required Implications of Pathway Primary goal was to provide a framework for the multiple decisions that are made when managing the anticoagulated patient undergoing a procedure Currently an area of high case volume handled with high variability Management of anticoagulation crosses many specialties Literature informed guidance when possible In areas where clinical judgment is needed, the pathway provided guidance by expert consensus Use of app provides point-of-care guidance available to multiple specialties 5
6 Effectiveness and Safety of Novel Oral Anticoagulants (NOACs) in VTE Treatment JOSHUA A. BECKMAN, MD, FACC, FAHA, MSVM DIRECTOR, SECTION OF VASCULAR MEDICINE VANDERBILT UNIVERSITY MEDICAL CENTER Disclosures Consulting: Astra Zeneca, Janssen, Aralez, Abbott Research Grant: Merck Board: VIVA While Mortality Decreases, Readmission Rate Remains High Retrospective cohort study of 100% Medicare fee-for-service beneficiaries hospitalized from 1999 to 2010 with a principal discharge diagnosis code for PE. Minges, KE. AJC 2015;116(9):

7 New Anticoagulants ORAL TTP889 X TF/VIIa IX PARENTERAL TFPI (tifacogin) Rivaroxaban Apixaban Edoxaban YM150 DU-176b Betrixaban TAK 442 IXa VIIIa Va Xa II AT APC (drotrecogin alfa) stm (ART-123) Fondaparinux Idraparinux DX-9065a Dabigatran IIa Fibrinogen Fibrin Adapted from Weitz & Bates, J Thromb Haemost 2007 Disadvantages of Warfarin Delayed onset/offset Variable dose response Narrow therapeutic window Drug-drug, drug-food interactions Inconvenient monitoring High bleeding rate Emergency Hospitalizations for Adverse Drug Events in Older U.S. Adults ( ) Budnitz DS, et al. N Engl J Med 2011;365:2002 2

8 The Ideal Oral Anticoagulant Oral, preferably once daily Rapid onset and offset of action Predictable PK and PD Low propensity for food and drug interactions Fixed doses Wide therapeutic window Easy to use with no need for monitoring RE-COVER: Dabigatran for VTE Recurrent VTE or VTE-related death 2,564 patients with objectively confirmed VTE were randomized to parenteral anticoagulation followed by fixed-dose dabigatran or dose-adjusted warfarin. p < for noninferiority Major or any bleeding p < p = 0.38 Schulman S, et al. N Engl J Med 2009;361:2342 EINSTEIN-DVT: Rivaroxaban for DVT Immediate initiation with rivaroxaban and no parenteral anticoagulant required n = 2,449 N Engl J Med 2010;363:2499 3


9 EINSTEIN-PE: Rivaroxaban for PE 4,832 patients with objectively confirmed PE were randomized to oral rivaroxaban (15 mg 2x/d for 3 weeks and then 20 mg daily) or parenteral anticoagulation followed by doseadjusted warfarin. Symptomatic Recurrent VTE p = p = for noninferiority N Engl J Med 2012;366:1287 AMPLIFY: Oral Apixaban for Treatment of VTE Agnelli G, et al. N Engl J Med. 2013; 369:799 Hokusai-VTE: Edoxaban vs. Warfarin NOTE: Among 938 patients with PE and RV dysfunction, the rate of recurrent VTE was 3.3% in the edoxaban group and 6.2% in the warfarin group (HR, 0.52; 95% CI, 0.28 to 0.98) p < for noninferiority p = for superiority The Hokusai-VTE Investigators. N Engl J Med 2013;369:1406 4
10 Anticoagulation Strategy in Evolution Overlapping LMWH/Warfarin Bridge UFH/Warfarin Bridge Switching LMWH to Dabigatran (RE-COVER) LMWH to Edoxaban (HOKUSAI-VTE) Oral Monotherapy Rivaroxaban (15 mg 2x/d for 3 wks, then 20 mg/d) (EINSTEIN) Apixaban (10 mg 2x/d for 1 wk, then 5 mg 2x/d) (AMPLIFY) Efficacy of NOACs for VTE Treatment: Meta-Analysis van der Hulle T, et al. J Thromb Haemost. 2014;12:320 Safety of NOACs for VTE Treatment: Meta-Analysis 1.2 Relative Risk Major Bleed Clin Rel Non Major Nonfatal ICH Fatal Bleed van der Hulle T, et al. J Thromb Haemost. 2014;12:320 5
11 Optimal Anticoagulation for Treatment of Acute VTE NOACs offer similar efficacy but improved safety compared with warfarin. NOACs may facilitate home therapy of patients presenting with low-risk VTE to the outpatient and Emergency Department settings. Optimal Anticoagulation for Acute VTE: 2016 CHEST Guideline Update In patients with DVT of the leg or PE and no cancer, as long-term (first 3 months) anticoagulant therapy, we suggest dabigatran, rivaroxaban, apixaban or edoxaban over VKA therapy (all Grade 2B). Kearon C, et al. CHEST (2016), doi: /j.chest

12 6/28/2017 Effectiveness and Safety of Direct Oral Anticoagulants (DOACs) Versus Warfarin in Nonvalvular Atrial Fibrillation Ty J. Gluckman, MD, FACC, FAHA Medical Director, Clinical Transformation Providence Heart and Vascular Institute Portland, Oregon Disclosures Boehringer-Ingelheim Consultant Efficacy, Safety, and Practical Considerations Items to consider when choosing an antithrombotic agent Reduced Risk of Stroke or Systemic Embolism Increased Risk of Bleeding Pharmacokinetics Risk of Drug-Food and Drug-Drug Interactions Availability of a reversal agent Ease of dosing Cost 1
13 Percent/Year Percent/Year 6/28/2017 Aspirin or Warfarin in Nonvalvular Atrial Fibrillation (NVAF) Pooled analyses comparing the impact of aspirin to placebo and warfarin to placebo on rates of ischemic stroke Aspirin vs. Placebo Warfarin vs. Placebo Atrial Fibrillation Investigators. Arch Intern Med. 1994;154: Dabigatran versus Warfarin in NVAF RE-LY Trial 18,113 patients with NVAF randomized to warfarin (INR of 2-3), dabigatran (150 mg BID), or dabigatran (110 mg BID) for a median of 2 years P= P=0.31 Dabigatran 150 mg BID 3.5 Warfarin, TTR=64% 3.0 Superiority 2.5 Noninferiority 2.0 P= Stroke or Systemic Embolism Ischemic Stroke Connolly SJ et al. NEJM 2009;361: Hemorrhagic All Cause Stroke Mortality Major Bleed Intracranial Hemorrhage Major GI Bleed Rivaroxaban versus Warfarin in NVAF ROCKET AF Trial ,264 patients with NVAF randomized to warfarin (INR of 2-3) or rivaroxaban (15-20 mg QD) for 1.6 years Superiority P=0.12 Noninferiority Stroke or Systemic Embolism P=0.58 Ischemic Stroke Patel MR et al. NEJM 2011;365: Rivaroxaban 20 mg QD Warfarin, TTR=55% P=0.024 P=0.07 Hemorrhagic All Cause Stroke Mortality P=0.58 Major Bleed P=0.02 Intracranial Hemorrhage Major GI Bleed 2
 or apixaban (5 mg BID) for 1.8 years Superiority P=0.01 Noninferiority Stroke or Systemic Embolism P=0.")
 or edoxaban (30 or 60 mg QD) for 2.")
14 Percent/Year Percent/Year 6/28/2017 Apixaban versus Warfarin in NVAF ARISTOTLE Trial ,201 patients with NVAF randomized to warfarin (INR of 2-3) or apixaban (5 mg BID) for 1.8 years Superiority P=0.01 Noninferiority Stroke or Systemic Embolism P=0.42 Ischemic Stroke Granger CB et al. NEJM 2011;365: P=0.047 Hemorrhagic All Cause Stroke Mortality Major Bleed Apixaban 5 mg BID Warfarin, TTR=66% Intracranial Hemorrhage P=0.37 Major GI Bleed Edoxaban versus Warfarin in NVAF ENGAGE AF Trial ,105 patients with NVAF randomized to warfarin (INR of 2-3) or edoxaban (30 or 60 mg QD) for 2.8 years Noninferiority P=0.005 Superiority P=0.44 Stroke or Systemic Embolism Ischemic Stroke Giugliano RP et al. NEJM 2013;369: P=0.08 P=0.006 Noninferiority Superiority P=0.02 P=0.97 Hemorrhagic Stroke All Cause Mortality Major Bleed Intracranial Hemorrhage Edoxaban 30 mg QD Edoxaban 60 mg QD Warfarin, TTR=68% P=0.03 Major GI Bleed DOACs and Risk of Intracranial Hemorrhage Meta-analysis of 6 randomized controlled trials of antithrombotic therapy in NVAF Favors DOACs Favors Comparators Chatterjee S et al. JAMA Neurol 2013;70:

15 Major bleeding rate (%) 6/28/2017 Efficacy and Safety of DOACs in Nonvalvular Atrial Fibrillation Meta-analysis comparing the impact of the direct oral anticoagulants (DOACs) to warfarin on rates of stroke or system embolism and major bleeding Stroke or system embolism Major bleeding Ruff CT et al. Lancet 2014;383: Real World Efficacy of DOACs in Nonvalvular Atrial Fibrillation Real-world cohort of 61,678 nonvalvular atrial fibrillation Danish patients comparing the impact of the direct oral anticoagulants (DOACs) to warfarin on outcomes Ischemic Stroke or Systemic Embolism All-cause Death Larsen TB et al. BMJ 2016;353:i3189 Years Since Start of Treatment Apixaban Dabigatran Rivaroxaban Warfarin Real World Safety of DOACs in Nonvalvular Atrial Fibrillation Real-world cohort of 54,321 nonvalvular atrial fibrillation Danish patients comparing the impact of the direct oral anticoagulants (DOACs) to warfarin on major bleeding Compared to apixaban: HR for rivaroxaban=1.49 ( ) HR for warfarin=1.23 ( ) HR for dabigatran=1.17 ( ) Follow-up (Years) Lamberts M et al. JAHA 2017;Epub aheadof print 4
![6/28/2017 Advantages and Disadvantages of DOACs Superior (apixaban, dabigatran, edoxaban [60 mg]) or comparable (rivaroxaban and edoxaban [30 mg]) efficacy in RCTs Significantly lower risk of ICH](/docs-images/80/80483256/images/16-0.jpg "Rapid onset and offset No need for anticoagulation monitoring Minimal risk of drug-food interaction Lower risk of drug-drug interaction Compared to warfarin, the DOACs have: Higher risk of GI")
![bleeding with some agents (dabigatran, rivaroxaban, and edoxaban [60 mg] but not apixaban or edoxaban [30 mg]) in RCTs Lack of an FDA approved reversal agent (except for dabigatran) Higher cost In](/docs-images/80/80483256/images/16-1.jpg "spite of this, both types of agents are significantly underutilized Contemporary Antithrombotic Practice Patterns Cohort study of 655,000 nonvalvular atrial fibrillation patients from the NCDR")
16 6/28/2017 Advantages and Disadvantages of DOACs Superior (apixaban, dabigatran, edoxaban [60 mg]) or comparable (rivaroxaban and edoxaban [30 mg]) efficacy in RCTs Significantly lower risk of ICH Rapid onset and offset No need for anticoagulation monitoring Minimal risk of drug-food interaction Lower risk of drug-drug interaction Compared to warfarin, the DOACs have: Higher risk of GI bleeding with some agents (dabigatran, rivaroxaban, and edoxaban [60 mg] but not apixaban or edoxaban [30 mg]) in RCTs Lack of an FDA approved reversal agent (except for dabigatran) Higher cost In spite of this, both types of agents are significantly underutilized Contemporary Antithrombotic Practice Patterns Cohort study of 655,000 nonvalvular atrial fibrillation patients from the NCDR PINNACLE registry with CHA 2 DS 2 -VASc score >1 Warfarin Dabigatran Rivaroxaban Apixaban Marzec LN et al. JACC 2017;69: Questions and Discussion 5

17 Clinical Advances in Anticoagulation in AF and VTE: Anticoagulant Reversal Agents George A. Davis, PharmD, BCPS UK HealthCare Gill Heart and Vascular Institute UK College of Pharmacy University of Kentucky July 17, 2017 Objective Discuss potential treatment strategies for anticoagulant reversal Goals of Anticoagulation Reversal Optimize Benefits, Minimize Risk Excessive Reversal Unnecessary interruption Increase thrombosis risk Inadequate Reversal Mortality Functional outcomes Hematoma expansion Surgical/procedural bleeding Choose an evidence-based reversal regimen Reversal warranted based on clinical status, urgency, and anticoagulant characteristics Appropriate dosage Appropriate monitoring An ideal anticoagulation reversal will provide the greatest reduction in further bleeding complications with the lowest incidence of thromboembolism. 1
18 Conventional anticoagulants and approve specific reversal and investigational agents Drug characteristic Oral warfarin unfractionated heparin Parenteral Anticoagulants low-molecular fondaparinux argatroban bivalirudin weight heparin Mode of action inhibition of vitamin K dependent carboxylation of clotting factors antithrombin-mediated inhibition of serine proteases (predominantly factor IIa and Xa inhibition) antithrombin-mediated inhibition of serine proteinases (predominantely factor Xa inhibition) antithrombinmediated factor Xa inhibition reversible factor IIa inhibition factor IIa inhibition Half-life h min 3-6 h 17 h 45 min 30 min Clearance hepatic and renal phagocytosis renal renal hepatic renal Approved specific direct reversal vitamin K, FFP PCC protamine partial reversal by protamine none modified thrombin none Investigational specific direct reversal none ciraparantag (PER977) andexanet alpha, ciraparantag (PER977) andexanet alpha none none Hematology Am Soc Hematol Educ Program Dec 2;2016(1): NOAC Reversal Practical consideration: Factors that impact PK/PD onset/offset Patient specific factors to assess last NOAC dose and half-life Time of last dose? Indication for reversal? How urgent is reversal? Indication for anticoagulant? Age Body weight Creatinine - Renal function Drug-drug interactions Dabigatran Rivaroxaban Apixaban Edoxaban Betrixaban Drug target Thrombin Factor Xa Factor Xa Factor Xa Factor Xa Time to max h 2h 3-4h 1-2h 3-4h effects Half-life 12-17h 5-9h 8-15h 8-10h 19-27h Plasma protein 35% 92-95% 87% 40-59% 60% binding Volume L 50 L Low >300 L >200 L distribution Renal 80% 33% 25% 35-39% 11% Elimination Pgp, Pgp, Drug interactions Pgp Pgp, CYP3A4 Pgp CYP3A4 CYP3A4 Arterioscler Thromb Vasc Biol. 2015;35: ; Vasc Health Risk Manag. 2015;11: ; BEVYXXA (betrixaban) [prescribing information], Portola Pharmaceuticals Inc, 6/2017. Renal impairment increases NOAC half-life Property Dabigatran Rivaroxaban Apixaban Edoxaban Betrixaban Renal clearance of absorbed dose, % Half-life in renal impairment, h CrCl >80 ml/min CrCl ml/min NA CrCl ml/min NA CrCl <30 ml/min NA Dialyzable Yes No Yes No NA Nutescu EA. Am J Health-Syst Pharm. 2013;70(Suppl 1):S3-11. Pradaxa (dabigatran etexilate mesylate) [prescribing information]. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals Inc.; 11/2015. Xarelto (rivaroxaban) [prescribing information]. Titusville, NJ: Janssen Pharmaceuticals, Inc.; 5/2016. Eliquis (apixaban) [prescribing information]. Princeton, NJ: Bristol-Myers Squibb Company; 9/2015. Savaysa (edoxaban) [prescribing information]. Parsippany, NJ: Daiichi Sankyo, Inc; 9/2015. DeVriese AS et al. Am J Kidney Dis. 2015;66(1): Heidbuchel H et al. Europace. 2015;17(10): ; BEVYXXA (betrixaban) [prescribing information], Portola Pharmaceuticals Inc, 6/
19 NOAC reversal: Potential strategies to date Strategy Removal Bypassing Example Activated charcoal after recent ingestion (with caution) Hemodialysis (dabigatran only, probably not necessary with target specific reversal agent) Prothrombin complex concentrate (PCC) Activated PCC rfviia (not recommended by some guidelines) Sequestration Idarucizumab (dabigatran only) Andexanet alfa (FXa inhibitors only; in development, not FDA approved but possible approval by YE2017) Ciraparantag (in development, not FDA approved) 2016 ISTH NOAC Reversal Guidelines: Indications for Reversal Life-threatening bleeding ICH, symptomatic or expanding extradural hemorrhage or uncontrolled hemorrhage Bleeding in a closed space or critical organ Intraspinal, intraocular, pericardial, pulmonary, retroperitoneal, or intramuscular with compartment syndrome Persistent major bleeding despite local hemostatic measures, or risk of recurrent bleeding because of delayed NOAC clearance or NOAC overdose Urgent reversal for procedural Need for urgent intervention that associated with high risk of bleeding, cannot be delayed to allow for drug clearance Emergency surgery, intervention in patients at high risk for procedural bleeding Neurosurgery (intracranial, extradural, spinal), lumbar puncture, cardiac or vascular surgery (aortic dissection/aneurysm repair), hepatic or other major organ surgery Potential indication for use Need for urgent surgery, intervention in patients with acute kidney injury Reversal agents should NOT be used Elective surgery GI bleeds that respond to supportive measures High drug levels, excessive anticoagulation without associated bleeding Need for surgery or intervention that can be delayed long enough to permit drug clearance Levy JH, et al. J Thromb Haemost. 2016;14: NOAC Reversal Guidelines: Lab testing Drug Class Laboratory testing for NOACs Normal aptt makes it unlikely dabigatran is major contributor to bleeding Normal TT indicates absence of dabigatran Normal PT does not exclude significant apixaban effects Quantification NOAC Chromogenic anti-fxa assay may be used for apixaban, edoxaban, rivaroxaban (if available) Conventional Coagulation Testing dtt, ECT, ecarin chromogenic assay may be used for dabigatran Specialized Coagulation Testing PT aptt TT dtt ECT/ECA Anti-Xa Activity Direct thrombin inhibitor dabigatran / N/A Factor Xa Inhibitor rivaroxaban / / N/A N/A N/A apixaban / / N/A N/A N/A edoxaban / / N/A N/A N/A betrixaban / / N/A N/A N/A, increase;, decrease;, no change; N/A, not advised; Color key: red, inappropriate testing; yellow, may be useful for excluding clinically relevant drug levels and may approximate drug levels; green, best test available. Do not wait for laboratory tests for lifethreatening bleeding Determine time of last dose if possible Estimate drug half-life with CrCl For patients with CrCl >60 ml/min, half-lives are no longer than 12 hr Consider if NOAC levels rising or falling if available J Thromb Haemost. 2016;14: ; Hematology Am Soc Hematol Educ Program Dec 2;2016(1):
 as non-activated PCC 50u/kg")
20 NOAC Reversal Guidelines (AC Forum, 2016) Non-specific reversal strategies PCC (Factors II, VII, IX, and X) as non-activated PCC 50u/kg (e.g. KCentra) or activated 80u/kg (e.g. FEIBA) Limited to in-vitro studies, animal models, or healthy volunteers Conflicting results Evidence remains low quality, limited data on clinical outcomes (hemostasis, mortality) Recombinant Factor VIIa is generally not recommended as first line agent for NOAC reversal FFP may not be practical due to volume required to reverse thrombin or FXa may lead to fluid overload 2017 status: Further comparative effectiveness studies are needed to understand the risks/benefits of PCC for NOAC reversal J Thromb Thrombolysis (2016) 41: ; Specific Reversal Agents for NOACs: Approved and in Development Idarucizumab FDA approved Andexanet alfa Investigational Ciraparantag Investigational Reverses dabigatran Approved Oct 2015 for rapid reversal of dabigatran for emergency procedures or lifethreatening or uncontrolled bleeding Reverses factor Xa inhibitors Phase 3: apixaban, rivaroxaban, enoxaparin Phase 2: edoxaban; planned for betrixaban August 2016 PDUFA date: FDA asked for more data; projected FDA approval in YE2017 Reverses all NOACs (broad-spectrum) FDA Fast Track Status Phase 2: edoxaban, enoxaparin PDUFA, Prescription Drug User Fee Act; Praxbind (idarucizumab) [prescribing information]. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals, Inc. 10/2015. Portola Pharmaceuticals. [news release]. 1/8/ Accessed 5/11/16. Perosphere. Accessed 5/11/16. Specific Reversal Agents for NOACs: Characteristics Idarucizumab Andexanet alfa Ciraparantag Monoclonal antibody Mechanism of Action fragment that binds dabigatran 350X more than between dabigatran and Decoy Xa molecule that binds FXa inhibitor anticoagulants restoring function of endogenous FXa Anticoagulant binding via noncovalent hydrogen bonds and charge-charge interactions thrombin NOAC(s) reversed Dabigitran Apixaban, Edoxaban, Rivaroxaban Dabigatran, Apixaban, Edoxaban, Rivaroxaban Apixaban: 400mg IV bolus + 480mg Studied doses 5gm IV given as two 2.5gm boluses over 5-10 min within 15min infusion over 2h Rivaroxaban, edoxaban: 800mg IV bolus + 960mg infusion over 2h; if < 7hrs since last rivaroxaban dose, mg IV single dose dose decrease by 50% Onset of action <5min <2min 5-10min Half-life Biphasic, Initial 45min; Terminal ~10hrs 1h Duration of action: 24h Elimination Renal Not reported Renal 4
21 Idarucizumab: Summary of REVERSE-AD32 Phase III multicenter, prospective cohort n=494 adult patients on dabigatran requiring: Reversal for life threatening bleeding (Group A; n=298) Need for urgent surgery (Group B, n=196) Primary outcome Maximal % reversal of anticoagulant effect (dtt) Group A (235/238; >98%); Group B (141/143; >98%) Similar results for ECT Secondary outcomes Time to hemostasis Group A: 3.5 h Group B: 4-5 h Periprocedural hemostasis 178/191 (93%) Thrombotic events 30d: Group A (4.4%); Group B (4.6%) 90d: Groups A and B (6.3%) 7 MI, 8 CVA, 15 VTE, 1 systemic embolism ~2/3 occurred OFF antithrombotic therapy Mortality 30d: Group A (12.3%); Group B (12.4%) 90d: Group A (18.7%); Group B (18.5%) Pollack et al., N Engl J Med 2015;373:511; AHA 2016 available at downloadable/ucm_ pdf Idarucizumab: Summary of REVERSE-AD32: Remaining questions Does idarucizumab improve clinical outcomes in bleeding patients? How should patients be selected to receive idarucizumab (up to 25% had insignificant dabigatran levels at study entry)? What is the significance of increased dabigatran levels at 12 and 24 hrs? Should these patients be re-dosed? Cost not discussed but current reversal strategies are expensive Our institution approach: Criteria based, restrictive use of reversal agents per hospital-specific guidelines reviewed by Anticoagulation Subcommittee of P&T Pharmacist evaluation at time of order (provided 24/7/365) to assess criteria and prepare dose/delivery in timely manner Pollack et al., N Engl J Med 2015;373:511; AHA 2016 available at downloadable/ucm_ pdf NOAC Reversal Summary Era of specific reversal agents is on the horizon Most associated bleeding (minor to moderate) can be managed by supportive care Pertinent laboratory parameters and clinical response should be considered but warrant further study Baseline TT, aptt, Factor Xa If NOAC reversal is indicated: FXa inhibitors: Consider PCC 50 units/kg; andexanet approval pending and ciraparantag in the pipeline Dabigatran: Use idarucizumab 5g Consider developing hospital-based guidance Re-initiation of anticoagulant after bleeding event warrants further study 5

22 Extended Use of Anticoagulation in Patients Previously Not Considered for Long-term Therapy Rachel P. Rosovsky, MD, MPH July 17, 2017 Conflicts of Interest Research support: Janssen and Daiichi Sanko 2 Scope of the problem What is the risk of recurrent VTE after stopping anticoagulation? 3 1
23 Risk of recurrent VTE Type of VTE 1 year risk 5 year risk Provoked by surgery 1% 3% Provoked by non surgical reversible risk 5% 15% Unprovoked VTE 10% 30% Cancer associated 15% 4 * Not predicted due to high mortality rate from cancer VTE = venous thromboembolism Kearon et al. CHEST Risk of recurrent VTE Cumulative incidence of recurrent thromboembolism in patients with idiopathic and secondary VTE. Key points: 1. At 10 years, risk is over 50% in unprovoked patients 2. Even at 10 years, risk increasing VTE = venous thromboembolism 5 Prandoni, Hematologica Who warrants long term anticoagulation? Depends on: patient-specific bleeding risks patient-specific thrombotic risks patient values and preferences 6 2

24 Who warrants long term anticoagulation? Most likely to benefit Idiopathic VTE Active cancer Antiphospholipid syndrome Recurrent VTE high risk thrombophilia Possible benefit Provoked VTE with persistent risk factors Unprovoked isolated distal DVT with persistent risk factors Unprovoked incidental PE 7 VTE = venous thromboembolism Clinical features associated with recurrent risk Several clinical features associated with recurrence; however, not completely defined on how to weigh each one. proximal location of DVT or PE obesity male sex several thrombophilic defects D-dimer residual vein thrombosis IVC filter 8 Recurrent Risk Prognostic Models HERDOO2 Ddimer, age, BMI, post thrombotic signs Vienna Ddimer, sex, site of index event DASH Ddimer, age, sex, hormones DAMOVES Ddimer, age, mutation, obesity, varicose veins, eight, sex 9 3



25 Bleeding Prediction Scores VTE bleeding scores Kuijer RIETE Atrial fibrillation bleeding scores HAS-BLED ATRIA HEMORR 2 HAGES 10 VTE = venous thromboembolism RIETE score Score for fatal bleeding in patients on anticoagulation for VTE 11 Nieto et al. JTH and Thrombosis Research RIETE Score Risk categories of patients according to score, and corresponding rates of fatal bleeding. 12 Nieto et al. Thrombosis Research

 Apixaban Amplify Extension (vs placebo) Rivaroxaban Einstein Extension (vs placebo) Einstein")
26 Bleeding Risk 13 Kearon et al. CHEST Who warrants long term anticoagulation How do we decide who to anticoagulated and with what? 14 Trials of long term anticoagulation Warfarin (vs placebo) Aspirin (vs placebo) Dabigatran RE-MEDY (vs warfarin): non inferior RE-SONATE (vs placebo) Apixaban Amplify Extension (vs placebo) Rivaroxaban Einstein Extension (vs placebo) Einstein Choice (vs aspirin) Primary efficacy: symptomatic recurrent fatal or nonfatal VTE Principal safety: major bleeding. Equipoise 15 5

27 RE-SONATE: Dabigatran 1343 patients, completed 6-12 months of anticoagulation (equipoise) randomized to dabigatran 150 mg bid or placebo. Dabigatran reduced the risk of recurrent VTE compared to placebo with an increase in bleeding Agnelli et al. NEJM AMPLIFY Extension: Apixaban 2482 patients, completed 6-12 months of anticoagulation (equipoise) randomized to apixaban 5 mg (treatment dose) or 2.5 mg (prophylactic dose) or placebo. Apixaban reduced the risk of recurrent VTE without increasing the rate of major bleeding Agnelli et al. NEJM Einstein Extension: Rivaroxaban 1196 patients, completed 6-12 months of anticoagulation remained on 20 mg, the continued-treatment study. Rivaroxaban had superior efficacy and no significant difference in bleeding Einstein Investigators. NEJM

28 Einstein CHOICE: Rivaroxaban 3396 patients, completed 6-12 months AC, randomized to either once-daily rivaroxaban (20 mg or 10 mg) or 100 mg of aspirin. Equipoise regarding need for continued AC. AC = anticoagulation Weitz et al. NEJM Einstein CHOICE: Rivaroxaban Risk of recurrent event was significantly lower with rivaroxaban both 20 mg (treatment dose) and 10 mg (prophylactic dose) compared to aspirin, without a significant increase in bleeding rates. Weitz et al. NEJM Einstein CHOICE: Rivaroxaban Weitz et al. NEJM
 decrease risk of recurrent VTE when compared to placebo in extension studies where there is equipoise in deciding on whether to continue AC.")

29 Question: What do all these studies tell us? Appears that DOACs (dabigatran, apixaban and rivaroxaban) decrease risk of recurrent VTE when compared to placebo in extension studies where there is equipoise in deciding on whether to continue AC. Apixaban and rivaroxaban had no significant increase in major bleeding. AC = anticoagulation 22 Have these studies changed guidelines? 23 Jaff et al. Circulation Have these studies changed guidelines? It is not possible to give a definitive guidance statement as to which patients should or should not receive long-term anticoagulant therapy after an episode of an unprovoked PE or DVT. Patients should be assessed on an individual basis, taking into consideration factors contributing to thrombosis recurrence risk and bleeding risk, and should be offered information outlining the risks and benefits of long-term anticoagulation. Moreover, patients values and preferences should be considered, relating to the impact of thrombosis recurrence (if anticoagulation is stopped) and bleeding (if anticoagulation is continued). 24 Baglin et al. JTH


30 Have these studies changed guidelines? Remarks: Patient sex and D-dimer level measured a month after stopping anticoagulant therapy may influence the decision to stop or extend anticoagulant therapy. In all patients who receive extended anticoagulant therapy, continuing use of treatment should be reassessed at periodic intervals (eg, annually). 25 Kearon et al. CHEST How do I apply these results to my patients? Provoked vs unprovoked Dose Equipoise What about needing to wait the 6 months One possible algorithm Kearon et al. Blood
31 Who warrants long term anticoagulation? Individualize treatment decision Risk of recurrent VTE Risk of bleed Patient preference and values Availability of drug Re-evaluate Thank you 10
Warfarin for Long-Term Anticoagulation. Disadvantages of Warfarin. Narrow Therapeutic Window. Warfarin vs. NOACs. Challenges Monitoring Warfarin
 1 2:15 pm The Era of : Selecting the Best Approach to Treatment SPEAKER Gregory Piazza, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Gregory Piazza,
1 2:15 pm The Era of : Selecting the Best Approach to Treatment SPEAKER Gregory Piazza, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Gregory Piazza,
Reversal of Novel Oral Anticoagulants. Angelina The, MD March 22, 2016
 Reversal of Novel Oral Anticoagulants Angelina The, MD March 22, 2016 Argatroban Bivalirudin Enoxaparin Lepirudin Heparin Dabigatran Apixaban 1939 1954 1998 2000 1999 2001 10/2010 7/2011 12/2012 1/2015
Reversal of Novel Oral Anticoagulants Angelina The, MD March 22, 2016 Argatroban Bivalirudin Enoxaparin Lepirudin Heparin Dabigatran Apixaban 1939 1954 1998 2000 1999 2001 10/2010 7/2011 12/2012 1/2015
Oral Anticoagulants Update. Elizabeth Renner, PharmD, BCPS, BCACP, CACP Outpatient Cardiology and Anticoagulation
 Oral Anticoagulants Update Elizabeth Renner, PharmD, BCPS, BCACP, CACP Outpatient Cardiology and Anticoagulation Objectives List the direct oral anticoagulant (DOAC) drugs currently available Describe
Oral Anticoagulants Update Elizabeth Renner, PharmD, BCPS, BCACP, CACP Outpatient Cardiology and Anticoagulation Objectives List the direct oral anticoagulant (DOAC) drugs currently available Describe
Updates in Anticoagulation for Atrial Fibrillation and Venous Thromboembolism
 Disclosures Updates in Anticoagulation for Atrial Fibrillation and Venous Thromboembolism No financial conflicts of interest Member of the ABIM Focused- Practice in Hospital Medicine Self Examination Process
Disclosures Updates in Anticoagulation for Atrial Fibrillation and Venous Thromboembolism No financial conflicts of interest Member of the ABIM Focused- Practice in Hospital Medicine Self Examination Process
Clinical issues which drug for which patient
 Anticoagulants - a matter of heart! Towards a bright future? Clinical issues which drug for which patient Sabine Eichinger Dept. of Medicine I Medical University of Vienna/Austria Conflicts of interest
Anticoagulants - a matter of heart! Towards a bright future? Clinical issues which drug for which patient Sabine Eichinger Dept. of Medicine I Medical University of Vienna/Austria Conflicts of interest
Anticoagulation with Direct oral anticoagulants (DOACs) and advances in peri-procedural interruption of anticoagulation-- Bridging
 and advances in peri-procedural interruption of anticoagulation-- Bridging") Anticoagulation with Direct oral anticoagulants (DOACs) and advances in peri-procedural interruption of anticoagulation-- Bridging Scott C. Woller, MD Co-Director, Thrombosis Program Intermountain Medical
Anticoagulation with Direct oral anticoagulants (DOACs) and advances in peri-procedural interruption of anticoagulation-- Bridging Scott C. Woller, MD Co-Director, Thrombosis Program Intermountain Medical
Practical Considerations for Using Oral Anticoagulants in Patients with Chronic Kidney Disease
 Practical Considerations for Using Oral Anticoagulants in Patients with Chronic Kidney Disease Cyrille K. Cornelio, Pharm.D. PGY2 Cardiology Pharmacy Resident The University of Oklahoma College of Pharmacy
Practical Considerations for Using Oral Anticoagulants in Patients with Chronic Kidney Disease Cyrille K. Cornelio, Pharm.D. PGY2 Cardiology Pharmacy Resident The University of Oklahoma College of Pharmacy
What s new with DOACs? Defining place in therapy for edoxaban &
 What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
Oral Anticoagulation Drug Class Prior Authorization Protocol
 Oral Anticoagulation Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review
Oral Anticoagulation Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review
Old and New Anticoagulants For Stroke Prevention Benefits and Risks
 Old and New Anticoagulants For Stroke Prevention Benefits and Risks September 15, 2014 Jonathan L. Halperin, M.D. The Cardiovascular Institute Mount Sinai Medical Center Disclosure Relationships with Industry
Old and New Anticoagulants For Stroke Prevention Benefits and Risks September 15, 2014 Jonathan L. Halperin, M.D. The Cardiovascular Institute Mount Sinai Medical Center Disclosure Relationships with Industry
New Anticoagulants Therapies
 New Anticoagulants Therapies Rachel P. Rosovsky, MD, MPH October 22, 2015 Conflicts of Interest No disclosures 2 Agenda 3 Historical perspective Novel oral anticoagulants Stats Trials Approval Concerns/Limitations
New Anticoagulants Therapies Rachel P. Rosovsky, MD, MPH October 22, 2015 Conflicts of Interest No disclosures 2 Agenda 3 Historical perspective Novel oral anticoagulants Stats Trials Approval Concerns/Limitations
Update on Oral Anticoagulants. Dr. Miten R. Patel Cancer Specialists of North Florida Cell
 Update on Oral Anticoagulants Dr. Miten R. Patel Cancer Specialists of North Florida Cell 904-451-9820 Email miten.patel@csnf.us Overview Highlights of the 4 new approved oral anticoagulants Results from
Update on Oral Anticoagulants Dr. Miten R. Patel Cancer Specialists of North Florida Cell 904-451-9820 Email miten.patel@csnf.us Overview Highlights of the 4 new approved oral anticoagulants Results from
Anticoagulation: Novel Agents
 Anticoagulation: Novel Agents Scott C. Woller, MD Medical Director, Anticoagulation Management, Intermountain Healthcare Central Region, co-director Venous Thromboembolism Program, Intermountain Medical
Anticoagulation: Novel Agents Scott C. Woller, MD Medical Director, Anticoagulation Management, Intermountain Healthcare Central Region, co-director Venous Thromboembolism Program, Intermountain Medical
Direct Oral Anticoagulants (DOACs). Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT
. Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT") Direct Oral Anticoagulants (DOACs). Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT OAC WARFARIN Gold standard DABIGATRAN RIVAROXABAN APIXABAN EDOXABAN BETRIXABAN
Direct Oral Anticoagulants (DOACs). Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT OAC WARFARIN Gold standard DABIGATRAN RIVAROXABAN APIXABAN EDOXABAN BETRIXABAN
Managing Bleeding in the Patient on DOACs
 Managing Bleeding in the Patient on DOACs Spring 2016 Jean M. Connors, MD Anticoagulation Management Services BWH/DFCI Hemostatic Antithrombotic Stewardship BWH Assistant Professor of Medicine, HMS Conflicts
Managing Bleeding in the Patient on DOACs Spring 2016 Jean M. Connors, MD Anticoagulation Management Services BWH/DFCI Hemostatic Antithrombotic Stewardship BWH Assistant Professor of Medicine, HMS Conflicts
Atrial Fibrillation: Risk Stratification and Treatment New Cardiovascular Horizons St. Louis September 19, 2015
 Atrial Fibrillation: Risk Stratification and Treatment New Cardiovascular Horizons St. Louis September 19, 2015 Christopher E. Bauer, MD, FACC, FHRS SSM Health Heart & Vascular Care Clinical Cardiac Electrophysiology
Atrial Fibrillation: Risk Stratification and Treatment New Cardiovascular Horizons St. Louis September 19, 2015 Christopher E. Bauer, MD, FACC, FHRS SSM Health Heart & Vascular Care Clinical Cardiac Electrophysiology
3/25/2016. Objectives for Pharmacists. Stop the Bleeding! New Reversal Agents. Objectives for Pharmacy Technicians. Assessment Pre-test
 Objectives for Pharmacists Stop the Bleeding! New Reversal Agents Gary D Peksa, Pharm.D., BCPS Clinical Pharmacy Specialist, Emergency Medicine Rush University Medical Center Review current strategies
Objectives for Pharmacists Stop the Bleeding! New Reversal Agents Gary D Peksa, Pharm.D., BCPS Clinical Pharmacy Specialist, Emergency Medicine Rush University Medical Center Review current strategies
A Brief History of the World of Anticoagulation
 A Brief History of the World of Anticoagulation Allison Burnett, PharmD, CACP, PhC Clinical Assistant Professor- UNM College of Rx Antithrombosis Stewardship Pharmacist University of New Mexico Hospital
A Brief History of the World of Anticoagulation Allison Burnett, PharmD, CACP, PhC Clinical Assistant Professor- UNM College of Rx Antithrombosis Stewardship Pharmacist University of New Mexico Hospital
Emergency Management of Patients on Direct Oral Anticoagulants (DOACs)
") Emergency Management of Patients on Direct Oral Anticoagulants (DOACs) Dr Tina Biss Consultant Haematologist Newcastle upon Tyne Hospitals NHS Foundation Trust NE RTC Annual Education Symposium 11 th October
Emergency Management of Patients on Direct Oral Anticoagulants (DOACs) Dr Tina Biss Consultant Haematologist Newcastle upon Tyne Hospitals NHS Foundation Trust NE RTC Annual Education Symposium 11 th October
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC
 Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC DEBATE: DOAC vs Good Old Warfarin André Roussin MD, FRCP, CSPQ CHUM and ICM/MHI Associate professor University of Montreal A. Roussin
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC DEBATE: DOAC vs Good Old Warfarin André Roussin MD, FRCP, CSPQ CHUM and ICM/MHI Associate professor University of Montreal A. Roussin
Reversal Agents for NOACs (Novel Oral Anticoagulants)
") Reversal Agents for NOACs (Novel Oral Anticoagulants) Current status and future challenges Paul A Reilly, PhD Clinical Research, Boehringer Ingelheim, Inc CSRC Symposium Washington DC Oct 18, 2016 Atrial
Reversal Agents for NOACs (Novel Oral Anticoagulants) Current status and future challenges Paul A Reilly, PhD Clinical Research, Boehringer Ingelheim, Inc CSRC Symposium Washington DC Oct 18, 2016 Atrial
3/19/2012. What is the indication for anticoagulation? Has the patient previously been on warfarin? If so, what % of the time was the INR therapeutic?
 Abigail E. Miller, PharmD, BCPS Clinical Specialist, Cardiology University of North Carolina Hospitals I have no personal financial relationships with the manufacturers of the products to disclose. Boehringer
Abigail E. Miller, PharmD, BCPS Clinical Specialist, Cardiology University of North Carolina Hospitals I have no personal financial relationships with the manufacturers of the products to disclose. Boehringer
The Direct Oral Anticoagulants: Practical Considerations. David Garcia, MD University of Washington Seattle Cancer Care Alliance September 2015
 The Direct Oral Anticoagulants: Practical Considerations David Garcia, MD University of Washington Seattle Cancer Care Alliance September 2015 Disclosure Occasional consultant to : BMS, Pfizer, Daiichi
The Direct Oral Anticoagulants: Practical Considerations David Garcia, MD University of Washington Seattle Cancer Care Alliance September 2015 Disclosure Occasional consultant to : BMS, Pfizer, Daiichi
A Cascade of Updates: Hot Topics in Anticoagulation
 A Cascade of Updates: Hot Topics in Anticoagulation Heather A. Powell, PharmD, BCPS Assistant Professor of Clinical Sciences Roosevelt University College of Pharmacy Golden L. Peters, PharmD, BCPS Associate
A Cascade of Updates: Hot Topics in Anticoagulation Heather A. Powell, PharmD, BCPS Assistant Professor of Clinical Sciences Roosevelt University College of Pharmacy Golden L. Peters, PharmD, BCPS Associate
Anticoagulation Task Force
 Anticoagulation Task Force Newest Recommendations Donald Zabriskie, BPharm, MBA, RPh Pharmacy Patient Care Services Cleveland Clinic- Fairview Hospital THE DRUGS THE PERFECT ANTICOAGULANT Oral administration
Anticoagulation Task Force Newest Recommendations Donald Zabriskie, BPharm, MBA, RPh Pharmacy Patient Care Services Cleveland Clinic- Fairview Hospital THE DRUGS THE PERFECT ANTICOAGULANT Oral administration
Disclosure and Conflict of Interest
 A Cascade of Updates: Hot Topics in Anticoagulation Heather A. Powell, PharmD, BCPS Assistant Professor of Clinical Sciences Roosevelt University College of Pharmacy Golden L. Peters, PharmD, BCPS Associate
A Cascade of Updates: Hot Topics in Anticoagulation Heather A. Powell, PharmD, BCPS Assistant Professor of Clinical Sciences Roosevelt University College of Pharmacy Golden L. Peters, PharmD, BCPS Associate
Professional Practice Minutes December 7, 2016
 Professional Practice Minutes December 7, 2016 **New Opportunity for Patient Education** We can now request the educational videos we want our patients to watch after our visit. Video topics include colon
Professional Practice Minutes December 7, 2016 **New Opportunity for Patient Education** We can now request the educational videos we want our patients to watch after our visit. Video topics include colon
DEEP VEIN THROMBOSIS (DVT): TREATMENT
: TREATMENT") DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
New Oral Anticoagulant Drugs in the Prevention of DVT
 New Oral Anticoagulant Drugs in the Prevention of DVT Targets for Anticoagulants ORAL DIRECT VKAs inhibit the hepatic synthesis of several coagulation factors Rivaroxaban Apixaban Edoxaban Betrixaban X
New Oral Anticoagulant Drugs in the Prevention of DVT Targets for Anticoagulants ORAL DIRECT VKAs inhibit the hepatic synthesis of several coagulation factors Rivaroxaban Apixaban Edoxaban Betrixaban X
Managing Hemorrhagic Complications of Non-Vitamin K Antagonist Oral Anticoagulants
 Managing Hemorrhagic Complications of Non-Vitamin K Antagonist Oral Anticoagulants MICHAEL E. MULLINS MD FAACT FACEP Washington University School Of Medicine Chair, BJH Anticoagulation Subcommittee Chair,
Managing Hemorrhagic Complications of Non-Vitamin K Antagonist Oral Anticoagulants MICHAEL E. MULLINS MD FAACT FACEP Washington University School Of Medicine Chair, BJH Anticoagulation Subcommittee Chair,
Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute
 Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute Disclosures Research Support/P.I. Employee Leo Pharma
Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute Disclosures Research Support/P.I. Employee Leo Pharma
When and How to Use the Newly Approved Oral Anticoagulants to Treat Acute Deep Vein Thrombosis (DVT) and Pulmonary Embolism (PE) Ian del Conde, MD
 and Pulmonary Embolism (PE) Ian del Conde, MD") When and How to Use the Newly Approved Oral Anticoagulants to Treat Acute Deep Vein Thrombosis (DVT) and Pulmonary Embolism (PE) Ian del Conde, MD December 12, 2015 Disclosures CONSULTANT Merck; New Haven
When and How to Use the Newly Approved Oral Anticoagulants to Treat Acute Deep Vein Thrombosis (DVT) and Pulmonary Embolism (PE) Ian del Conde, MD December 12, 2015 Disclosures CONSULTANT Merck; New Haven
Do s and Don t of DOACs DISCLOSURE
 Do s and Don t of DOACs Tom DeLoughery, MD MACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant/Research none Content Expert: Elsevier
Do s and Don t of DOACs Tom DeLoughery, MD MACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant/Research none Content Expert: Elsevier
The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center
 The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center What is the INR? Tissue Factor (Factor III) is added to
The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center What is the INR? Tissue Factor (Factor III) is added to
Leading the Charge in Anticoagulation Reversal: Benefits, Risks, and Key Factors in Application to the Traumatically Injured Patient
 Leading the Charge in Anticoagulation Reversal: Benefits, Risks, and Key Factors in Application to the Traumatically Injured Patient Emily Hutchison, PharmD BCPS Clinical Pharmacy Specialist, Trauma/Adult
Leading the Charge in Anticoagulation Reversal: Benefits, Risks, and Key Factors in Application to the Traumatically Injured Patient Emily Hutchison, PharmD BCPS Clinical Pharmacy Specialist, Trauma/Adult
Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism. Rajat Deo, MD, MTR
 Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism Rajat Deo, MD, MTR Director of Translational Research in Cardiac Arrhythmias Division of Cardiovascular Medicine
Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism Rajat Deo, MD, MTR Director of Translational Research in Cardiac Arrhythmias Division of Cardiovascular Medicine
Novel Oral An,coagulants: Prac,cal Aspects. Caroline Berube, MD Clinical Associate Professor Division of Hematology November 2015
 Novel Oral An,coagulants: Prac,cal Aspects Caroline Berube, MD Clinical Associate Professor Division of Hematology November 2015 The New Oral An,coagulants (NOACs) The Non VKA Oral An,coagulants (NOACs)
Novel Oral An,coagulants: Prac,cal Aspects Caroline Berube, MD Clinical Associate Professor Division of Hematology November 2015 The New Oral An,coagulants (NOACs) The Non VKA Oral An,coagulants (NOACs)
Role of NOACs in AF Management. From Evidence to Real World Data Focus on Cardioversion
 Role of NOACs in AF Management. From Evidence to Real World Data Focus on Cardioversion John Rickard MD, MPH Staff Electrophysiologist Cleveland Clinic Agenda NOACs: Update on Real World Data NOAC reversal:
Role of NOACs in AF Management. From Evidence to Real World Data Focus on Cardioversion John Rickard MD, MPH Staff Electrophysiologist Cleveland Clinic Agenda NOACs: Update on Real World Data NOAC reversal:
Reversal of direct oral anticoagulants in the patient with GI bleeding. Marc Carrier
 Reversal of direct oral anticoagulants in the patient with GI bleeding Marc Carrier Disclosure Faculty: Dr. Marc Carrier Relationships with commercial interests: Grants/Research Support: Leo Pharma, Bristol
Reversal of direct oral anticoagulants in the patient with GI bleeding Marc Carrier Disclosure Faculty: Dr. Marc Carrier Relationships with commercial interests: Grants/Research Support: Leo Pharma, Bristol
Reversal of DOACs Breakthroughs and Their Aftermath
 Reversal of DOACs Breakthroughs and Their Aftermath Geno J Merli, MD, MACP, FSVM, FHM Professor Medicine & Surgery Co-Director Jefferson Vascular Center Sidney Kimmel Medical College Thomas Jefferson University
Reversal of DOACs Breakthroughs and Their Aftermath Geno J Merli, MD, MACP, FSVM, FHM Professor Medicine & Surgery Co-Director Jefferson Vascular Center Sidney Kimmel Medical College Thomas Jefferson University
Ischemic and hemorrhagic strokes in the context of the direct acting oral anticoagulants
 Ischemic and hemorrhagic strokes in the context of the direct acting oral anticoagulants Van Hellerslia, PharmD, BCPS, CACP Clinical Assistant Professor Temple University School of Pharmacy Over 4 million
Ischemic and hemorrhagic strokes in the context of the direct acting oral anticoagulants Van Hellerslia, PharmD, BCPS, CACP Clinical Assistant Professor Temple University School of Pharmacy Over 4 million
Dr Tina Biss Consultant Haematologist Newcastle Hospitals NHS Foundation Trust. North East RTC Annual Education Symposium 16 th October 2014
 Dr Tina Biss Consultant Haematologist Newcastle Hospitals NHS Foundation Trust North East RTC Annual Education Symposium 16 th October 2014 The extent of the problem 1-2% of the UK population are anticoagulated
Dr Tina Biss Consultant Haematologist Newcastle Hospitals NHS Foundation Trust North East RTC Annual Education Symposium 16 th October 2014 The extent of the problem 1-2% of the UK population are anticoagulated
New drugs for anticoagulation so much choice, how do they compare? Dr Patrick Kesteven Newcastle
 New drugs for anticoagulation so much choice, how do they compare? Dr Patrick Kesteven Newcastle CONCLUSIONS 1. Arrival of new anticoagulants is a Good Thing. CONCLUSIONS 1. Arrival of new anticoagulants
New drugs for anticoagulation so much choice, how do they compare? Dr Patrick Kesteven Newcastle CONCLUSIONS 1. Arrival of new anticoagulants is a Good Thing. CONCLUSIONS 1. Arrival of new anticoagulants
Direct Oral Anticoagulants An Update
 Oct. 26, 2017 Direct Oral Anticoagulants An Update Kathleen Heintz, DO, FACC Assistant Professor of Medicine Cooper Heart Institute Direct Oral Anticoagulants: DISCLAIMERS No Conflicts of Interest So what
Oct. 26, 2017 Direct Oral Anticoagulants An Update Kathleen Heintz, DO, FACC Assistant Professor of Medicine Cooper Heart Institute Direct Oral Anticoagulants: DISCLAIMERS No Conflicts of Interest So what
INR as a Biomarker: Anticoagulation in Atrial Fib, Heart Failure, and Cardiovascular Disease Daniel Blanchard, MD, FACC, FAHA
 INR as a Biomarker: Anticoagulation in Atrial Fib, Heart Failure, and Cardiovascular Disease Daniel Blanchard, MD, FACC, FAHA Professor of Medicine Director, Cardiology Fellowship Program Sulpizio Cardiovascular
INR as a Biomarker: Anticoagulation in Atrial Fib, Heart Failure, and Cardiovascular Disease Daniel Blanchard, MD, FACC, FAHA Professor of Medicine Director, Cardiology Fellowship Program Sulpizio Cardiovascular
UPDATE ON TREATMENT OF ACUTE VENOUS THROMBOSIS
 UPDATE ON TREATMENT OF ACUTE VENOUS THROMBOSIS Armando Mansilha MD, PhD, FEBVS 16 th National Congress of the Italian Society of Vascular and Endovascular Surgery Bologna, 2017 Disclosure I have the following
UPDATE ON TREATMENT OF ACUTE VENOUS THROMBOSIS Armando Mansilha MD, PhD, FEBVS 16 th National Congress of the Italian Society of Vascular and Endovascular Surgery Bologna, 2017 Disclosure I have the following
Acute Care: Understanding Direct Oral Anticoagulants (DOACs)
") Acute Care: Understanding Direct Oral Anticoagulants (DOACs) National Conference for Nurse Practitioners (NCNP) October 11, 2017 John Togami, PharmD, PhC Pharmacist Clinician - Outpatient Anticoagulation
Acute Care: Understanding Direct Oral Anticoagulants (DOACs) National Conference for Nurse Practitioners (NCNP) October 11, 2017 John Togami, PharmD, PhC Pharmacist Clinician - Outpatient Anticoagulation
The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center
 The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center What is the INR? Tissue Factor (Factor III) is added to
The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center What is the INR? Tissue Factor (Factor III) is added to
True/False: Idarucizumab can be utilized for the management of bleeding associated with dabigatran.
 Discuss the role of idarucizumab for the management of bleeding associated with dabigatran Understand dosing, preparation and administration of idarucizumab I have no financial interest/arrangement or
Discuss the role of idarucizumab for the management of bleeding associated with dabigatran Understand dosing, preparation and administration of idarucizumab I have no financial interest/arrangement or
NUOVI ANTICOAGULANTI NELL ANZIANO: indicazioni e controindicazioni. Mario Cavazza Medicina d Urgenza Pronto Soccorso AOU di Bologna
 NUOVI ANTICOAGULANTI NELL ANZIANO: indicazioni e controindicazioni Mario Cavazza Medicina d Urgenza Pronto Soccorso AOU di Bologna Two major concerns Atrial Fibrillation: Epidemiology The No. 1 preventable
NUOVI ANTICOAGULANTI NELL ANZIANO: indicazioni e controindicazioni Mario Cavazza Medicina d Urgenza Pronto Soccorso AOU di Bologna Two major concerns Atrial Fibrillation: Epidemiology The No. 1 preventable
Direct Oral Anticoagulants
 Direct Oral Anticoagulants Holly Jahn, PharmD, CACP Objectives Identify the FDA approved indications for use, appropriate dosing, and monitoring parameters for each direct oral anticoagulant. Distinguish
Direct Oral Anticoagulants Holly Jahn, PharmD, CACP Objectives Identify the FDA approved indications for use, appropriate dosing, and monitoring parameters for each direct oral anticoagulant. Distinguish
Individual Therapeutic Selection Of Anti-coagulants And Periprocedural. Miguel Valderrábano, MD
 Individual Therapeutic Selection Of Anti-coagulants And Periprocedural Management Miguel Valderrábano, MD Outline Does the patient need anticoagulation? Review of clinical evidence for each anticoagulant
Individual Therapeutic Selection Of Anti-coagulants And Periprocedural Management Miguel Valderrábano, MD Outline Does the patient need anticoagulation? Review of clinical evidence for each anticoagulant
Drug Class Monograph
 Drug Class Monograph Class: Oral Anticoagulants Drug: Coumadin (warfarin), Eliquis (apixaban), Pradaxa (dabigatran), Savaysa (edoxaban), arelto (rivaroxaban) Formulary Medications: Eliquis (apixaban),
Drug Class Monograph Class: Oral Anticoagulants Drug: Coumadin (warfarin), Eliquis (apixaban), Pradaxa (dabigatran), Savaysa (edoxaban), arelto (rivaroxaban) Formulary Medications: Eliquis (apixaban),
Updates in Coagulation Thrombophilia testing and direct oral anticoagulants. Kevin Y. Chen, MD Hematology and Medical Oncology October 13, 2017
 Updates in Coagulation Thrombophilia testing and direct oral anticoagulants Kevin Y. Chen, MD Hematology and Medical Oncology October 13, 2017 No conflicts of interest Introduction to thrombosis Hemostasis
Updates in Coagulation Thrombophilia testing and direct oral anticoagulants Kevin Y. Chen, MD Hematology and Medical Oncology October 13, 2017 No conflicts of interest Introduction to thrombosis Hemostasis
Let s Gi e The So ethi g To Clot About: Controversies in Anticoagulation
 Let s Gi e The So ethi g To Clot About: Controversies in Anticoagulation Janna Beavers, MS, PharmD, BCPS Cardiology Clinical Pharmacy Specialist WakeMed Health & Hospitals Raleigh, NC March 13, 2018 Pharmacist
Let s Gi e The So ethi g To Clot About: Controversies in Anticoagulation Janna Beavers, MS, PharmD, BCPS Cardiology Clinical Pharmacy Specialist WakeMed Health & Hospitals Raleigh, NC March 13, 2018 Pharmacist
New Options for Anticoagulation Reversal: A Practical Approach
 New Options for Anticoagulation Reversal: A Practical Approach Hyung Wook Park Chonnam National University Hospital, Gwangju, Korea 4 NOACs Prevention of TE No. of events (%/yr..) NOAC Warfarin HR 95%
New Options for Anticoagulation Reversal: A Practical Approach Hyung Wook Park Chonnam National University Hospital, Gwangju, Korea 4 NOACs Prevention of TE No. of events (%/yr..) NOAC Warfarin HR 95%
NOAC s across indications
 Sektion CAMPUS INNENSTADT Med. Klinik und Poliklinik IV NOAC s across indications Ulrich Hoffmann, M.D. Division of Vascular Medicine University Hospital Munich, Germany Disclosure Speaker name: Ulrich
Sektion CAMPUS INNENSTADT Med. Klinik und Poliklinik IV NOAC s across indications Ulrich Hoffmann, M.D. Division of Vascular Medicine University Hospital Munich, Germany Disclosure Speaker name: Ulrich
An Overview of Non Vitamin-K Antagonist Oral Anticoagulants. Helen Williams Consultant Pharmacist for CV Disease South London
 An Overview of Non Vitamin-K Antagonist Oral Anticoagulants Helen Williams Consultant Pharmacist for CV Disease South London Contents Drugs and drug classes Licensed indications and NICE recommendations
An Overview of Non Vitamin-K Antagonist Oral Anticoagulants Helen Williams Consultant Pharmacist for CV Disease South London Contents Drugs and drug classes Licensed indications and NICE recommendations
Discuss the role of idarucizumab for the management of bleeding associated with dabigatran
 Discuss the role of idarucizumab for the management of bleeding associated with dabigatran Understand dosing, preparation and administration of idarucizumab I have no financial interest/arrangement or
Discuss the role of idarucizumab for the management of bleeding associated with dabigatran Understand dosing, preparation and administration of idarucizumab I have no financial interest/arrangement or
6 th ACC-SHA Joint Meeting Jeddah, Saudi Arabia
 6 th ACC-SHA Joint Meeting Jeddah, Saudi Arabia October 31 st - November 1 st, 2015 NOACS vs. Coumadin in Atrial Fibrillation: Is It Worth to Switch? Raed Sweidan, MD, FACC Consultant and Head of Cardiac
6 th ACC-SHA Joint Meeting Jeddah, Saudi Arabia October 31 st - November 1 st, 2015 NOACS vs. Coumadin in Atrial Fibrillation: Is It Worth to Switch? Raed Sweidan, MD, FACC Consultant and Head of Cardiac
New and old anticoagulants. Anticoagulation Focus on Direct Oral Anticoagulants
 Anticoagulation Focus on Direct Oral Anticoagulants Tzu-Fei Wang, MD Assistant Professor Department of Internal Medicine Division of Hematology The Ohio State University Wexner Medical Center Objectives
Anticoagulation Focus on Direct Oral Anticoagulants Tzu-Fei Wang, MD Assistant Professor Department of Internal Medicine Division of Hematology The Ohio State University Wexner Medical Center Objectives
Disclosures. Practical Considerations for Anticoagulation for Prevention of Venous Thromboembolism and Stroke Due to Atrial Fibrillation
 12:45 1:45 pm Practical Considerations for Anticoagulation for Prevention of Venous Thromboembolism and Stroke Due to Atrial Fibrillation SPEAKER Christian Ruff, MD, MPH Presenter Disclosure Information
12:45 1:45 pm Practical Considerations for Anticoagulation for Prevention of Venous Thromboembolism and Stroke Due to Atrial Fibrillation SPEAKER Christian Ruff, MD, MPH Presenter Disclosure Information
REVERSAL STRATEGIES FOR ORAL ANTICOAGULATION
 REVERSAL STRATEGIES FOR ORAL ANTICOAGULATION Wesley R. Zemrak, Pharm.D., BCPS Clinical Pharmacy Specialist, Anticoagulation Maine Medical Center, Portland, ME zemraw@mmc.org 1 OBJECTIVES 1. Discuss the
REVERSAL STRATEGIES FOR ORAL ANTICOAGULATION Wesley R. Zemrak, Pharm.D., BCPS Clinical Pharmacy Specialist, Anticoagulation Maine Medical Center, Portland, ME zemraw@mmc.org 1 OBJECTIVES 1. Discuss the
BLOOD DISEASE RESEARCH FOUNDATION
 BLOOD DISEASE RESEARCH FOUNDATION BLOOD DISEASE RESEARCH FOUNDATION The mission of Blood Disease Research Foundation is to support hematological research, e.g. by donating grants for thesis work and abstract
BLOOD DISEASE RESEARCH FOUNDATION BLOOD DISEASE RESEARCH FOUNDATION The mission of Blood Disease Research Foundation is to support hematological research, e.g. by donating grants for thesis work and abstract
Idarucizumab for Dabigatran Reversal Pollack CV, Reilly PA, Eikelboom J, et al. N Engl J Med 2015; 373(6):
:") Idarucizumab for Dabigatran Reversal Pollack CV, Reilly PA, Eikelboom J, et al. N Engl J Med 2015; 373(6):511-520. Objective: To measure the safety of idarucizumab to reverse dabigatran anticoagulant effects
Idarucizumab for Dabigatran Reversal Pollack CV, Reilly PA, Eikelboom J, et al. N Engl J Med 2015; 373(6):511-520. Objective: To measure the safety of idarucizumab to reverse dabigatran anticoagulant effects
Update on the Management of Cancer Associated VTE
 Update on the Management of Cancer Associated VTE Jean M. Connors, MD 2018 Master Class Course Anticoagulation Management Services BWH/DFCI Hemostatic Antithrombotic Stewardship BWH Associate Professor
Update on the Management of Cancer Associated VTE Jean M. Connors, MD 2018 Master Class Course Anticoagulation Management Services BWH/DFCI Hemostatic Antithrombotic Stewardship BWH Associate Professor
Afib, Stroke, and DOAC. Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS
 Afib, Stroke, and DOAC Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS Disclosure of Relevant Financial Relationships I have no relevant financial relationships with commercial
Afib, Stroke, and DOAC Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS Disclosure of Relevant Financial Relationships I have no relevant financial relationships with commercial
Introduction. Blood Pressure
 Introduction Spontaneous intracerebral hemorrhage (ICH) is a major cause of morbidity and mortality worldwide [1]. Of a number of factors that have been linked to ICH (e.g., higher rates in Asians and
Introduction Spontaneous intracerebral hemorrhage (ICH) is a major cause of morbidity and mortality worldwide [1]. Of a number of factors that have been linked to ICH (e.g., higher rates in Asians and
A Review of the Role of Non-Vitamin K Oral Anticoagulants in the Acute and Long-Term Treatment of Venous Thromboembolism
 Cardiol Ther (2018) 7:1 13 https://doi.org/10.1007/s40119-018-0107-0 REVIEW A Review of the Role of Non-Vitamin K Oral Anticoagulants in the Acute and Long-Term Treatment of Venous Thromboembolism Andrew
Cardiol Ther (2018) 7:1 13 https://doi.org/10.1007/s40119-018-0107-0 REVIEW A Review of the Role of Non-Vitamin K Oral Anticoagulants in the Acute and Long-Term Treatment of Venous Thromboembolism Andrew
Anticoagulants: Agents, Pharmacology and Reversal
 Anticoagulants: Agents, Pharmacology and Reversal Lori B Heller, M.D. Cardiac Anesthesiology Swedish Heart and Vascular Institute Medical Director, Swedish Blood Management Clinical Instructor, University
Anticoagulants: Agents, Pharmacology and Reversal Lori B Heller, M.D. Cardiac Anesthesiology Swedish Heart and Vascular Institute Medical Director, Swedish Blood Management Clinical Instructor, University
Use of Anticoagulant Reversal Agents
 Use of Anticoagulant Reversal Agents Lori Shutter, MD shutterla@upmc.edu Vice Chair of Education Director, Neurocritical Care Program Professor, Critical Care Medicine, Neurology & Neurosurgery University
Use of Anticoagulant Reversal Agents Lori Shutter, MD shutterla@upmc.edu Vice Chair of Education Director, Neurocritical Care Program Professor, Critical Care Medicine, Neurology & Neurosurgery University
New Oral Anticoagulants in treatment of VTE, PE DR.AMR HANAFY (LECTURER OF CARDIOLOGY ) ASWAN UNIVERSITY
 ASWAN UNIVERSITY") New Oral Anticoagulants in treatment of VTE, PE DR.AMR HANAFY (LECTURER OF CARDIOLOGY ) ASWAN UNIVERSITY Fact VTE is deadly! It nibbles after it bites! The 30-day mortality rates for first-time DVT or
New Oral Anticoagulants in treatment of VTE, PE DR.AMR HANAFY (LECTURER OF CARDIOLOGY ) ASWAN UNIVERSITY Fact VTE is deadly! It nibbles after it bites! The 30-day mortality rates for first-time DVT or
Debate: New Generation Anti-Coagulation Agents are a Better Choice than Warfarin in the Management of AF
 Debate: New Generation Anti-Coagulation Agents are a Better Choice than Warfarin in the Management of AF Bradley P. Knight, MD Director of Cardiac Electrophysiology Bluhm Cardiovascular Institute Northwestern
Debate: New Generation Anti-Coagulation Agents are a Better Choice than Warfarin in the Management of AF Bradley P. Knight, MD Director of Cardiac Electrophysiology Bluhm Cardiovascular Institute Northwestern
Kelly Rudd, PharmD, FCCP, BCPS, CACP Basset Medical Center, Cooperstown, NY
 Jedi Training 101: Mind-tricks & Evidence -Based Approaches to Combating Clinical Controversies in Anticoagulation Therapy Kelly Rudd, PharmD, FCCP, BCPS, CACP Basset Medical Center, Cooperstown, NY LEARNING
Jedi Training 101: Mind-tricks & Evidence -Based Approaches to Combating Clinical Controversies in Anticoagulation Therapy Kelly Rudd, PharmD, FCCP, BCPS, CACP Basset Medical Center, Cooperstown, NY LEARNING
The Treatment of Venous Thromboembolism (VTE): Has Warfarin Met Its Match? Michael P. Gulseth, Pharm. D., BCPS, FASHP Program Director for
: Has Warfarin Met Its Match? Michael P. Gulseth, Pharm. D., BCPS, FASHP Program Director for") The Treatment of Venous Thromboembolism (VTE): Has Warfarin Met Its Match? Michael P. Gulseth, Pharm. D., BCPS, FASHP Program Director for Anticoagulation Services Sanford USD Medical Center Sioux Falls,
The Treatment of Venous Thromboembolism (VTE): Has Warfarin Met Its Match? Michael P. Gulseth, Pharm. D., BCPS, FASHP Program Director for Anticoagulation Services Sanford USD Medical Center Sioux Falls,
to a DOAC anticoagulants (DOACs) dosing of DOACs for various indications switching from a DOAC and switching
 dosing of DOACs for various indications switching from a DOAC and switching") Linda Kelly, PharmD, PhC, CACP Presbyterian Healthcare Services } Identify the FDA approved direct oral anticoagulants (DOACs) } Distinguish the differences in the dosing of DOACs for various indications
Linda Kelly, PharmD, PhC, CACP Presbyterian Healthcare Services } Identify the FDA approved direct oral anticoagulants (DOACs) } Distinguish the differences in the dosing of DOACs for various indications
Anticoagulant therapy, coumadines or direct antithrombins
 ATRIAL FIBRILLATION (AF) Anticoagulant therapy, coumadines or direct antithrombins Felicita Andreotti, MD PhD Aggregated Professor Dept of Cardiovascular Sciences, Catholic University, Rome, IT Consultant
ATRIAL FIBRILLATION (AF) Anticoagulant therapy, coumadines or direct antithrombins Felicita Andreotti, MD PhD Aggregated Professor Dept of Cardiovascular Sciences, Catholic University, Rome, IT Consultant
A Review of Direct-Acting Oral Anticoagulants (DOACs) and Their Use in Special Populations
 and Their Use in Special Populations") A Review of Direct-Acting Oral Anticoagulants (DOACs) and Their Use in Special Populations Allison Bernard, PharmD PGY2 Ambulatory Care Resident University of Iowa Hospitals and Clinics October 25 th,
A Review of Direct-Acting Oral Anticoagulants (DOACs) and Their Use in Special Populations Allison Bernard, PharmD PGY2 Ambulatory Care Resident University of Iowa Hospitals and Clinics October 25 th,
ADVANCES IN ANTICOAGULATION
 ADVANCES IN ANTICOAGULATION The Clinicians Perspective Claudine M. Lewis Cardiologist OUTLINE Indications for anticoagulants Review - Physiology of Hemostasis Types of anticoagulants New anticoagulants
ADVANCES IN ANTICOAGULATION The Clinicians Perspective Claudine M. Lewis Cardiologist OUTLINE Indications for anticoagulants Review - Physiology of Hemostasis Types of anticoagulants New anticoagulants
Content 1. Relevance 2. Principles 3. Manangement
 Intracranial haemorrhage and anticoagulation Department of Neurology,, Germany Department of Neurology, Heidelberg University Hospital, Germany Department of Clinical Medicine Copenhagen University, Denmark
Intracranial haemorrhage and anticoagulation Department of Neurology,, Germany Department of Neurology, Heidelberg University Hospital, Germany Department of Clinical Medicine Copenhagen University, Denmark
Treatment Options and How They Work
 Treatment Options and How They Work Robin Offord Director of Clinical Pharmacy UCL Hospitals NHS Foundation Trust robin.offord@uclh.nhs.uk Introducing the term anticoagulant... What they do Inhibit the
Treatment Options and How They Work Robin Offord Director of Clinical Pharmacy UCL Hospitals NHS Foundation Trust robin.offord@uclh.nhs.uk Introducing the term anticoagulant... What they do Inhibit the
Dabigatran Evidence in Real Practice
 ADVANCES IN CARDIAC ARRHYTHMIAS and GREAT INNOVATIONS IN CARDIOLOGY XXVII GIORNATE CARDIOLOGICHE TORINESI Torino, Centro Congressi Unione Industriale 23-24 Ottobre 2015 Dabigatran Evidence in Real Practice
ADVANCES IN CARDIAC ARRHYTHMIAS and GREAT INNOVATIONS IN CARDIOLOGY XXVII GIORNATE CARDIOLOGICHE TORINESI Torino, Centro Congressi Unione Industriale 23-24 Ottobre 2015 Dabigatran Evidence in Real Practice
NOACs for Primary and Secondary Stroke Prevention: From Clinical Trials to Real-World Data To Practical Considerations
 NOACs for Primary and Secondary Stroke Prevention: From Clinical Trials to Real-World Data To Practical Considerations Mark J. Alberts, MD, FAHA Hartford HealthCare Hartford, CT USA AF confers an increased
NOACs for Primary and Secondary Stroke Prevention: From Clinical Trials to Real-World Data To Practical Considerations Mark J. Alberts, MD, FAHA Hartford HealthCare Hartford, CT USA AF confers an increased
DOACs Advances and Limitations in Real World. Lee Lai Heng Haematology Singapore General Hospital
 DOACs Advances and Limitations in Real World Lee Lai Heng Haematology Singapore General Hospital Disclosures for In compliance with COI policy, ISTH requires the following disclosures to the session audience:
DOACs Advances and Limitations in Real World Lee Lai Heng Haematology Singapore General Hospital Disclosures for In compliance with COI policy, ISTH requires the following disclosures to the session audience:
Perioperative Management of Novel Oral Anticoagulants (NOACs) Hardy Shah PharmD NEANA March 2017
 Hardy Shah PharmD NEANA March 2017") Perioperative Management of Novel Oral Anticoagulants (NOACs) Hardy Shah PharmD NEANA March 2017 Disclosures Presenter has no actual or potential conflicts of interest in relation to this program Question
Perioperative Management of Novel Oral Anticoagulants (NOACs) Hardy Shah PharmD NEANA March 2017 Disclosures Presenter has no actual or potential conflicts of interest in relation to this program Question
The DOACs. Update on Anticoagulation 10/20/2017. Dabigatran (Pradaxa ) Rivaroxaban (Xarelto ) Apixaban (Eliquis ) Edoxaban (Savaysa ) Objectives
 Rivaroxaban (Xarelto ) Apixaban (Eliquis ) Edoxaban (Savaysa ) Objectives") Objectives Update on Anticoagulation JEFF REIST PHARMD, BCPS CLINICAL ASSOCIATE PROFESSOR UNIVERSITY OF IOWA COLLEGE OF PHARMACY At the conclusion of this program, the participant should be able to: List
Objectives Update on Anticoagulation JEFF REIST PHARMD, BCPS CLINICAL ASSOCIATE PROFESSOR UNIVERSITY OF IOWA COLLEGE OF PHARMACY At the conclusion of this program, the participant should be able to: List
Update on the NOAC s: 2018 Daniel Blanchard, MD, FACC, FAHA
 Update on the NOAC s: 2018 Daniel Blanchard, MD, FACC, FAHA Professor of Medicine Director, Cardiology Fellowship Program Sulpizio Cardiovascular Center UC San Diego The NOACS, chronologically Dabigatran:
Update on the NOAC s: 2018 Daniel Blanchard, MD, FACC, FAHA Professor of Medicine Director, Cardiology Fellowship Program Sulpizio Cardiovascular Center UC San Diego The NOACS, chronologically Dabigatran:
A VENOUS THROMBOEMBOLISM (VTE) TOWN HALL: Answering Your Top Questions on Treatment and Secondary Prevention
 TOWN HALL: Answering Your Top Questions on Treatment and Secondary Prevention") A VENOUS THROMBOEMBOLISM (VTE) TOWN HALL: Answering Your Top Questions on Treatment and Secondary Prevention This handout is a supplemental resource to an educational video activity released on Medscape
A VENOUS THROMBOEMBOLISM (VTE) TOWN HALL: Answering Your Top Questions on Treatment and Secondary Prevention This handout is a supplemental resource to an educational video activity released on Medscape
With All the New Drugs, This is How I Treat Acute DVT and Superficial Phlebitis
 BRIGHAM AND WOMEN S HOSPITAL With All the New Drugs, This is How I Treat Acute DVT and Superficial Phlebitis Gregory Piazza, MD, MS Division of Cardiovascular Medicine Brigham and Women s Hospital April
BRIGHAM AND WOMEN S HOSPITAL With All the New Drugs, This is How I Treat Acute DVT and Superficial Phlebitis Gregory Piazza, MD, MS Division of Cardiovascular Medicine Brigham and Women s Hospital April
Reversal Agents for Anticoagulants Understanding the Options. Katisha Vance, MD, FACP Alabama Oncology January 28, 2017
 Reversal Agents for Anticoagulants Understanding the Options Katisha Vance, MD, FACP Alabama Oncology January 28, 2017 Objectives Appropriately recommend reversal agents for Vitamin K antagonists Appropriately
Reversal Agents for Anticoagulants Understanding the Options Katisha Vance, MD, FACP Alabama Oncology January 28, 2017 Objectives Appropriately recommend reversal agents for Vitamin K antagonists Appropriately
Latest News and Clinical Applications of NOACs: What about Antidotes?
 Optimizing outcomes in Atrial Fibrillation Latest News and Clinical Applications of NOACs: What about Antidotes? McMaster Cardiology Update September 11, 2015 Agenda Real world data on the use of NOACs
Optimizing outcomes in Atrial Fibrillation Latest News and Clinical Applications of NOACs: What about Antidotes? McMaster Cardiology Update September 11, 2015 Agenda Real world data on the use of NOACs
Results from RE-COVER RE-COVER II RE-MEDY RE-SONATE EXECUTIVE SUMMARY
 Assessment of the safety and efficacy of dabigatran etexilate (Pradaxa ) in the treatment of deep vein thrombosis (DVT) and pulmonary embolism (PE) and the prevention of recurrent DVT and PE Results from
Assessment of the safety and efficacy of dabigatran etexilate (Pradaxa ) in the treatment of deep vein thrombosis (DVT) and pulmonary embolism (PE) and the prevention of recurrent DVT and PE Results from
Overview of the Direct Oral Anticoagulants
 Original Article Nedaa Skeik, MD Abhishek Sethi Michele Shepherd, PharmD From: Minneapolis Heart Institute at Abbott Northwestern Hospital, Minneapolis, MN Address for correspondence: Nedaa Skeik, MD Minneapolis
Original Article Nedaa Skeik, MD Abhishek Sethi Michele Shepherd, PharmD From: Minneapolis Heart Institute at Abbott Northwestern Hospital, Minneapolis, MN Address for correspondence: Nedaa Skeik, MD Minneapolis
Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine
 Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine Antithrombotics Antiplatelets Aspirin Ticlopidine Prasugrel Dipyridamole
Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine Antithrombotics Antiplatelets Aspirin Ticlopidine Prasugrel Dipyridamole
Direct Oral Anticoagulant Reversal
 08 June 2018 No. 08 Direct Oral Anticoagulant Reversal M Khattab Moderator: E Hodgson School of Clinical Medicine Discipline of Anaesthesiology and Critical Care CONTENTS INTRODUCTION... 3 Pharmacokinetics
08 June 2018 No. 08 Direct Oral Anticoagulant Reversal M Khattab Moderator: E Hodgson School of Clinical Medicine Discipline of Anaesthesiology and Critical Care CONTENTS INTRODUCTION... 3 Pharmacokinetics
The clinical relevance of AMPLIFY programme
 Venice October 16th 2015 The clinical relevance of AMPLIFY programme Francesco Dentali Department of Clinical Medicine Insubria University Varese Disclosures Bayer Bristol-Myers Squibb/Pfizer Boehringer
Venice October 16th 2015 The clinical relevance of AMPLIFY programme Francesco Dentali Department of Clinical Medicine Insubria University Varese Disclosures Bayer Bristol-Myers Squibb/Pfizer Boehringer
Updates in Management of Venous Thromboembolic Disease
 Updates in Management of Venous Thromboembolic Disease November 7 th 2018 UHN Emergency Conference Susan Jenkins RN(EC) NP-Adult Thrombosis and Hemostasis Program University Health Network Disclosures
Updates in Management of Venous Thromboembolic Disease November 7 th 2018 UHN Emergency Conference Susan Jenkins RN(EC) NP-Adult Thrombosis and Hemostasis Program University Health Network Disclosures
Atrial Fibrillation. 2 nd Annual National Hospitalist Conference San Antonio, TX September 7, 2018
 2 nd Annual National Hospitalist Conference San Antonio, TX September 7, 2018, MSc, FACP, SFHM Division of Hospital Medicine Henry Ford Hospital Detroit, USA Clinical Associate Professor of Medicine Wayne
2 nd Annual National Hospitalist Conference San Antonio, TX September 7, 2018, MSc, FACP, SFHM Division of Hospital Medicine Henry Ford Hospital Detroit, USA Clinical Associate Professor of Medicine Wayne
Guidance for management of bleeding in patients taking the new oral anticoagulant drugs: rivaroxaban, dabigatran or apixaban
 Guidance for management of bleeding in patients taking the new oral anticoagulant drugs: rivaroxaban, dabigatran or apixaban Purpose The aim of this guidance is to outline the management of patients presenting
Guidance for management of bleeding in patients taking the new oral anticoagulant drugs: rivaroxaban, dabigatran or apixaban Purpose The aim of this guidance is to outline the management of patients presenting