La stimulation biventriculaire (Traitement par Resynchronisation Cardiaque) Indications et Résultats. Daniel Gras, DIU, Paris 2007
|
|
|
- Roland French
- 6 years ago
- Views:
Transcription
1 La stimulation biventriculaire (Traitement par Resynchronisation Cardiaque) Indications et Résultats, DIU, Paris 2007
2 CRT: Results and indications Background Results of CRT Studies Today s classical CRT indications Potential Role of ICD during CRT Particular Indications for CRT
3 The evolving perspective of HF HF Prevalence Will Double in 30 Years HF Prevalence in Western Europe (Millions) Ageing population CAD management Source: New Medicine Reports 1997 ; 1999 Heart and Stroke Statistical Update, AHA
4 HF patients die primarily from CV death (mortality by cause in control groups of selected HF trials*) non CV death 18.5% Consensus, Solvd T, Solvd P, Save, Aire, Trace, Rales, Ephesus, Cibis, US Carvedilol, Merit HF, Cibis II, Best, Capricorn, Copernicus, Comet all-cause mortality: 81.5% CV death Publications reporting all-cause mortality, CV death, SCD, death by progression of HF (N= pts, control groups, 16 studies)
5 Care-HF pts also die primarily from CV death non CV death 46/255 (18.1%) Unclassifiable 12/255 (4.7%) CV Death: 197/255 (77.2%)
6 SCD is the leading cause of CV death (mortality by cause in control groups of selected HF trials*) Other CV death Consensus, Solvd T, Solvd P, Save, Aire, Trace, Rales, Ephesus, Cibis, US Carvedilol, Merit HF, Cibis II, Best, Capricorn, Copernicus, Comet HF Progression 36% Sudden Cardiac Death 42% Publications reporting all-cause mortality, CV death, SCD, death by progression of HF (N= pts, control groups, 16 studies)
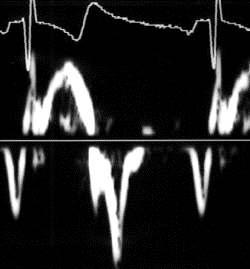
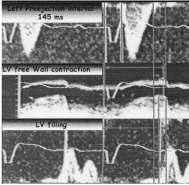
7 Functional abnormalities in isolated LBBB LBBB Normal Radionuclide images showing the onset of RV and LV contraction Grines, Circulation 1989
8 Functional abnormalities in Isolated LBBB IVCT IVRT Grines, Circulation 1989


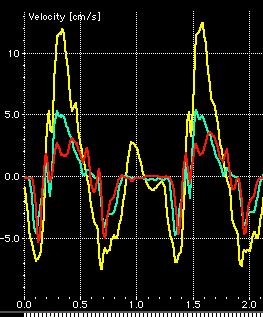
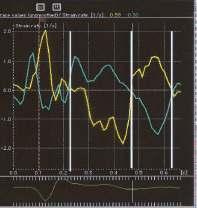
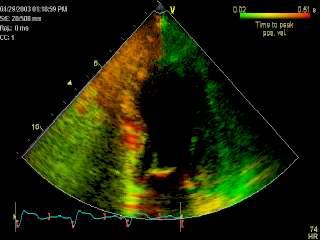
9 Rationale for CRT: Abnormal LV segmental contraction
10

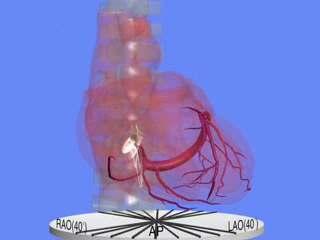
11 CRT system implantation


12 CRT-D System Implantation (Right Side) AP view LAO view
13 Mechanisms of benefit during CRT Systolic function ( increase in CO) Coordination in LV contraction Shorter LV contraction duration Diastolic function Longer LV filling duration Decrease in Mitral regurgitation Effects on neurohormones, Remodelling...
 Nelson et al. Circulation 2000 n=7 Nowak.")
14 CRT Improves LV Function Without Oxidative Stress MVO2/HR (Relative Units) 0,24 0,22 0,20 0,18 0,16 0,14 P<0.05 Dobutamine LV Pacing dp/dt max (mm/hg/s) Nelson et al. Circulation 2000 n=7 Nowak. JACC 2003

15 Mechanisms of CRT Decrease in Mitral Regurgitation
16 CRT: Results and indications Background Results of CRT Studies Today s classical CRT indications Potential Role of ICD during CRT Particular indications for CRT
17 What we know from morbi-mortality trials Cumulative Enrollment in CRT Trials Cumulative Patients Open Studies CARE HF MIRACLE ICD MIRACLE MUSTIC AF MIRACLE ICD II MUSTIC SR COMPANION PATH CHF PATH CHF II CONTAK CD Results Presented
18 Outcomes and Follow-up of CRT patients Randomized Controlled Trials on CRT Study (n randomized) MIRACLE (453) MUSTIC SR (58) MUSTIC AF (43) PATH CHF (41) MIRACLE ICD (369) CONTAK CD (490) COMPANION (1520) PATH CHF II (89) MIRACLE ICD II (186) CARE HF (814) NYHA III, IV III, IV 120 Normal No Published + Exercise III, IV 130 Capacity: Normal 6 Yes MW, Published Peak VO2 + LV II-IVfunction: 120 Normal EF, MR Yes Published + Reverse III, IV 120 remodeling: Normal NoLV Published EDV, ESV + III, IV 120 Normal Both Published + III, IV QRS 130 III >150 Normal NYHA III >200* Class, AF 120 Sinus CRT Improves: Normal Normal Normal ICD? No No No Yes No Status Published Published Published Quality of life score (MLWHF), Hospitalization, II 130 Mortality Published Published Results LVEF 35% for all trials * RV paced QRS
19 CRT Improves Exercise Capacity Average Change in 6 Minute Walk Distance Average Change in Peak VO 2 m MIRACLE * MUSTIC SR * CONTAK CD * MIRACLE ICD ml/kg/min MIRACLE * MUSTIC SR * CONTAK CD * * 0 MIRACLE ICD Control CRT Control CRT Abraham et al., 2003 * P < 0.05



20 6 Min. WT: + 13/20% QoL (MLWHF): + 30% NYHA: - 0.5/0.8 NO CRT CRT Miracle ICD
21 Comparison with Drug Trials: Digoxin, ACE-I and Beta-blocker Therapies Change from baseline in 6 minute walk distance Change from baseline in CPX Duration Change from baseline in QoL (MLWHF) Score * 5 meters Dig (1) * BB (2) CRT (6) seconds * Dig (1) Control ACE (3) CRT (6) Treatment Improvement score ACE (4) NS BB (5) CRT (6) * P.05 P.01 P NEJM 1993;329:1-7 (RADIANCE) 2 Circulation 1996;94: (PRECISE) 3 JAMA 1988;259: Am J Cardiol 1993;71: (SOLVD Treatment) 5 J Cardiac Failure 1997;3: NEJM 2002;346: (MIRACLE)
22 Effects of CRT on Hospitalization Rate MUSTIC Monthly rate of hospitalisations for CHF (Randomisation to M 12) MIRACLE Total Days Hospitalized for Heart Failure 0,14 0,12 0,10 0,08 0,06 0,04 0,02 0 / 7 CR - CR Control N=225 77% p = CRT N=228
23 Euro Karolinska Study Hospital costs per patient before implant Differenz: after implant Costs for CRT: 8.019/Patient. Costs for the device balance the saved money within one year. Braunschweig F. Eur J Heart Failure 2: (2000)
24 COMPANION: Primary Endpoint All cause Mortality + Hospitalization Bristow et al. NEJM. 2004; 350: Companion reinforces previous results of CRT trials
25 COMPANION : Mortality and HF hospitalization Death: 24% Hosp: 76%
26 Cardiac Resynchronisation in Heart Failure: CARE-HF Baseline Evaluation Randomization (1:1) OMT CRT (CRT+OMT) Minimum 18 Month Follow-up 813 patients, 82 centers,12 countries, FU: 29.4 M NYHA class III/IV, LVSD: EF 35%; EDD > 30mm/hm QRS 150 ms or Echo if QRS ms Primary composite endpoint: All-cause mortality or unplanned hosp. for a major CVS event (time to first event analysis, Hosp adjudicated by a blinded EP committee)
27 Care-HF: Baseline Characteristics Age [yr] - median (IQR) Male (%) NYHA IV (%) Ischaemic heart disease (%) Treatment (%) ACEIs / ARBs Beta blockers Furosemide Eq 80 mg/day Digitalis Spironolactone Control n = (59 to 72) 293 (73%) 27 (6.7%) 142 (35%) 383 (95%) 298 (73%) 177 (44%) 181 (45%) 238 (59%) CRT n = (60 to 73) 304 (74%) 23 (5.6%) 167 (41%) 387 (95%) 288 (71%) 175 (43%) 165 (40%) 219 (54%)
28 SAE Groupings Care-HF: Serious Adverse Events Patients with Procedure or device related Adverse Event (Assessed by Independent Expert) Procedure related death Lead problems Coronary sinus dissection Pocket complications Patients with Other Serious Adverse Events (Investigator Reported) Myocardial Isch & MI Worsening HF Atrial arrhythmia Ventricular arrhythmia Respiratory infection AVB or bradycardia Control CRT P value P = 0.99 P < P < P = P = 0.21 P < P = 0.02 P = 0.74 P = 0.15 P = 0.12
29 CARE-HF: Improved NYHA, QoL, LVEF Euro Qualit of Life Score NYHA Class 0,8 0,70 0,6 0,4 0,2 Daniel 0,0 Gras NYHA Class at 90 days p< ,0 2,5 2,1 2,0 1,5 1,0 0,5 0,0 2,7 Euro QoL Score at 90 days p< ,63 CRT Control 0,35 0,3 0,25 0,2 0,15 0,1 0,05 0 Mean LVEF at 18 Months p< ,9% CRT 25,0% Control Patients in the CRT group had a lower NYHA class and a higher Euro Quality of Life score at 90 days. Mean LV ejection fraction was higher on average in the CRT group compared with the medical therapy alone group. Cleland et al. New England Journal of Medicine. 2005; 352:
30 Care-HF: Changes in LVES volume & LVEF Volume (ml) Ejection Fraction (%) Baseline 3 months P< months P< months P< Baseline 3 months P< months P< months P< Control Group CRT Group Control Group CRT Group LV End-Systolic Volumes LV ejection Fraction
31 Changes in IVMD (ms) and MRI in Care HF Time (ms) LA area index (%) Baseline 3 months P< months P< months P< Baseline 3 months P< months P= months P=0.015 Control Group CRT Group Control Group CRT Group Interventricular Mechanical Delay Mitral Regurgitation index
32 CARE-HF: Primary endpoint All-cause Mortality or Unplanned Hosp. for Major CVS Event Event-free Survival No statistical significant heterogeneity in subgroups HR 0.63 (95% CI 0.51 to 0.77) Death : 20% Hospitalizations : 80% CRT P <.0001 Medical Tx 0.00 Number at risk CRT Medical Tx Days Cleland. N Engl J Med. 2005;352
33 Care-HF: All-Cause Mortality Event-free Survival HR 0.64 (95% CI 0.48 to 0.85) CRT (20%) P =.0019 Medical Therapy (29.7%) 0.00 Number at risk CRT Medical Therapy Days
34 CRT impacts on Mortality & Hospitalization rates 100 Survival 10 Annual survival (%) CRT Hospitalization 1 Hospitalizations / year 0 I II III IV NYHA CLASS.1
35 Care-HF extension phase Cross Over Control Group (n= 404) Main Study 19 prior to Primary EP (5%) 50 in total (12.4%) Extension Phase 45 (11.1%) One lost to follow-up Total 95 (23.5%) Implant Failures CRT Group (n = 409) Main Study 19 (4.6%) Extension Phase None Total 19 (4.6%)
36 CARE-HF Extension Study Effect of CRT on All-Cause Mortality 1.00 Hazard Ratio 0.60 (95% CI 0.47 to 0.77; P<0.0001) 0.75 CRT Survival 0.50 Mean Follow-up Medical Therapy Number at risk 0.25 CRT Medical therapy Mean Follow-up 36.4 months (range 26.1 to 52.6) CRT Deaths = 101 (24.7%) Medical Therapy Deaths = 154 (38.1%) Time (days)
37 CARE-HF Extension Study Time to Death from Worsening Heart Failure 1.00 Survival Hazard Ratio 0.55 (95% CI 0.37 to 0.82; P=0.003) CRT Medical Therapy CRT = 38 HF deaths (9.3%) Medical Therapy = 64 HF deaths (15.8%) Time (days)
38 CARE-HF Extension Study Time to Sudden Death 1.00 CRT Survival Hazard Ratio 0.54 (95% CI 0.35 to 0.84; P=0.006) Medical Therapy CRT = 32 sudden deaths (7.8%) Medical Therapy = 54 sudden deaths (13.4%) Time (days)
39 CRT: Results and indications Background Results of CRT Studies Today s classical CRT indications Potential Role of ICD during CRT Particular indications for CRT
40 CRT in Clinical Practice ACC/AHA; HFSA; CCS; ESC Guidelines 2005 CRT: Indication Class I, Level A

41 Impact of CRT on PCWP Start pacing Stop pacing pcw Hemodynamics of CRT: beat-to-beat reduction of pcw and v-wave
42 Acute hemodynamic evaluation is not necessary Acute hemodynamic changes do not correlate with long term effect of CRT Mitral regurgitation (%) MR LVEF LV volumes Ejection fraction (%) Yu Circulation 2002 Baseline 1 w k 1 mo 3 mo off-imm 20 off-1w k off-4w k 80 Left ventricular volume (m baseline 1 wk 1mo 3 mo off-imm off-1wk off-4wk Immediate effect Delayed effect baseline 1 w k 1 mo 3 mo off-imm off-1w k off-4w k


43 CRT provides LV reverse remodeling effect Sogaard P, et al; J Am Coll Cardiol 2002
44 Today s classical CRT indications 1. Cardiomyopathy (Ischemic or not): EF<35%, EDD>55 mm 2. NYHA functional class III/IV 3. OMT (6 weeks) : ACEI, Diur., Bb., Spiron. 4. Ventricular Asynchrony QRS > 150 ms QRS < 150 ms: Echo criteria (Care-HF) 1. Aortic Pre-ejection delay > 140 ms 2. Interventricular mechanical delay > 40 ms 3. LV segmental post systolic contraction + 4. Intra LV asynchrony + 5. AV asynchrony
 (Q")
 Interventricular Mechanical")
45 Patient selection for CRT Echo parameters consideration (Q to Pulmonary Ejection = 120 ms) (Q to Aortic Ejection = 230 ms) ( 1 ) Prolonged aortic pre-ejection delay ( 2 ) Interventricular Mechanical Delay = 110 ms


 LV late systolic")
46 Patient selection for CRT Echo Parameters Under Consideration QRS-LLW: 590 ms QRS-E: 530 ms OVERLAP (3) LV late systolic contraction

47 Echocardiographic criteria to select pts for CRT S E S A Just prove it!! DESIRE and PROSPECT trials E A Courtesy of G Habib


48 Mr Seg, 63 years, DCM, NYHA Class III


49 Me Seg, 63 ans, CMD


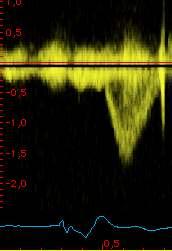
50 1. AV Dyssynchrony : LVFT < 40% Cardiac Cycle DFT at Baseline: 280 ms DFT during CRT: 400 ms

, NYHA")
51 Clinical Case: LVEF: 25%, SR, LBBB (QRS 160 ms), NYHA III/OMT

52 Complex forms of ventricular asynchrony Advanced CRT: RV septal, Dual-site LV pacing
53 CRT & reduced RV function: Interaction at 18 M 0 LVESV Control CRT 302/40 291/53 LVEF P= from baseline (cm 3 ) ,4-52,1-76,4-41,7 2,1 4,9 10,3 4, from baseline (%) -100 TAPSE >14 mm P=0.002 TAPSE 14 mm 302/40 291/53 Control CRT 0 TAPSE: Tricuspid Annular plane systolic excursion
54 Dual site RV Pacing to optimize CRT



55 Typical non responder to CRT: 84 Yo, ICM, NYHA IV, RV dysfunction
56 CRT: Results and indications Background Results of CRT Studies Today s classical CRT indications Potential Role of ICD during CRT Particular indications for CRT
57 ESC Guidelines Indications for ICD in HF Previous Cardiac Arrest, SVT: I, A ICM, LVEF < 30-35%, after 40 days of MI: I, A NYHA III-IV, LVEF < 35%, QRS > 120 ms: IIa, B 1.European Heart Journal 2005;26: Madit 1 & 2: Moss NEJM 1996, Definite: Kadish NEJM Salukhe Circulation Desai Jama SCDHefT: Bardy NEJM 2005
58 MADIT II Survival Results ICM + LVEF < 30% 1.0 Probability of Survival P = Conventional Defibrillator No. At Risk Year Defibrillator (0.91) 274 (0.94) 110 (0.78) 9 Conventional (0.90) 170 (0.78) 65 (0.69) 3 Moss AJ. N Engl J Med. 2002;346:
59 International Perspective of the evolving Role of CRT Sudden Cardiac Death despite CRT COMPANION CRT-P arm CARE-HF Sudden death as % of total mortality Sudden deaths account for ~35% of mortality in CRT-P
 Medical Therapy 0.25 0.00 CRT = 32 sudden deaths (7.8%) Medical Therapy = 54 sudden deaths (13.")
60 Time to SCD in Care HF and Companion 1.00 CRT Survival Hazard Ratio 0.54 (95% CI 0.35 to 0.84; P=0.006) Medical Therapy CRT = 32 sudden deaths (7.8%) Medical Therapy = 54 sudden deaths (13.4%) Time (days)
61 CARE-HF, COMPANION, SCD-HeFT: Mode of Death OPT CRT-P CRT-D ICD CARE-HF (29.4mth) COMPANION (16.6mth) SCD-HeFT (45.5mth) Mortality 16,0% 14,0% 12,0% 10,0% 8,0% 6,0% 4,0% 2,0% 0,0% 9,4% 7,1% SCD 13,9% 8,1% 7,8% PUMP FAILURE 5,8% 2,9% SCD 11,0% 8,6% 8,7% PUMP FAILURE 11,6% SCD 4,6% 7,8% 8,7% PUMP FAILURE Cause of death JM Cleland JGF. N Engl J Med. 2005;352: Bristow MR. N Engl J Med. 2004;350: Bardy GH. N Engl J Med. 2005;352: Packer DL. Heart Rhythm May;2 (1suppl):AB20-2.
62 Strategy to reduce mortality in HF pts treated by CRT 1 Year Mortality ACE-I, Beta-blockade, ACE-I Spironolactone & Beta Blockade Reduce Mortality 16% 12% 8% 4% 0% Reduce mortality 15,6% 12,4% 11,5% 7,8% SOLVD-T MERIT-HF + CIBIS II Placebo Adapted from McMurray JJV; Heart 1999 Treatment Further reduction expected from CRT/ICD in selected HF patients Further Reduction with CRT + ICD for Higher Risk Patients HF Mortality Sudden Cardiac Death CRT ICD Care-HF Madit, Companion, SCD-HeFT With respect to «clinical» contra indication to ICD
63 «Clinical» Contra-Indication to ICD in HF Pts Physiological: Age > 80-85, Psychological pbs... Class IV + other disease Advanced RV dysfunction, High PVR Comorbidities Renal dysfunction: creatinine clearance < 30 ml/mn Severe liver impairment Advanced other disease (diabetes )
64 Effect of Starting Age and Device Longevity on Cost per QALY Base case Incremental Cost Per QALY Gained 80,000 70,000 5 Years 60,000 50,000 40,000 8 Years 30,000 20,000 10, Age at Starting Treatment 7 Years CRT-D vs CRT-P CRT-D vs MT CRT-P vs MT Freemantle, ESC 2006 CRT+MT vs MT CRT+ICD+MT vs CRT + MT CRT+ICD+MT vs MT
65 CRT: Results and indications Background Results of CRT Studies Today s classical CRT indications Potential Role of ICD during CRT Particular indications for CRT
66 Patient selection for CRT: particular cases 1. Origin of the DCM: impact in clinical outcome? 2. NYHA class II: candidates for CRT? 3. Is long QRS duration required for CRT? 4. RBBB versus LBBB outcome? 5. Do patients with Chronic AF benefit from CRT? 6. Role of CRT in candidates for cardiac pacing?
67 Patient selection for CRT: particular cases 1. Origin of the DCM: impact in clinical outcome? YES ml 0 Left Ventricular End Diastolic Volume 2,5-16,6 6,6 0 0,5 1 1,5 2 2,5 P=0.016 Ischemic P<0.001 P<0.001 Non-Ischemic Control CRT ,7 Impact of CRT in ischemic versus non ischemic pts
68 Interaction Between CRT & Ischemic Etiology from baseline (cm 3 ) Control LVESV CRT -6,9-26,4-49,0-84,4 P=0.01 LVEF P= ,2 6,0 2,9 1,5 Control CRT from baseline (%) Non-ischemic etiology Ischemic etiology


69 Possible Reasons for Failure of CRT: ICM CRT-D combined to optimal revascularization
70 MIRACLE ICD II Study 6 Min Walk, QoL, NYHA (Circulation 2004) m Distance Walked in 6 Minutes Base P= Mo Quality of Life Score (MLWHF) Base P= Mo Proportion of Patients NYHA Class at 6 Months 70% P= % 50% 40% 30% 20% 10% 0% I II III IV Control (n=96) CRT (n=81) Control (n=98) CRT (n=82)
71 MIRACLE ICD II Study Improvements in Cardiac Volumes and Dimension suggest that CRT Improves Cardiac Function and Structure cm Left Ventricular End Diastolic Diameter P=0.04 cm Left Ventricular End Systolic Diameter P=0.01 % Left Ventricular Ejection Fraction P= Base 6 Mo 200 Base 6 Mo 20 Base 6 Mo Control (n=85) CRT (n=69) Abraham, Circulation 2004
72 Recommendations for CRT are based on the results of controlled trials: 158 < QRS < 176 Study (n) NYHA QRS Rhythm Results MUSTIC SR (58) III >150 Sinus + MUSTIC AF (43) III >200* AF + MIRACLE (453) III, IV 130 Sinus + PATH CHF (41) III, IV 120 Sinus + MIRACLE ICD (369) III-IV 130 Sinus + CONTAK CD (227) II-IV 120 Sinus + MIRACLE ICD II (186) II 130 Sinus + PATH CHF II (89) III, IV 120 Sinus + COMPANION (1520) III, IV 120 Sinus + CARE HF (814) III, IV 120 Sinus +
73 Patient selection for CRT: particular cases 4. RBBB versus LBBB LBBB aspect Common finding in DCM Conduction disturbances at distal Purkinje system RBBB aspect 1. and «hemifascicular LBBB» aspect (left axis deviation) 2. and severe RV dilatation/dysfunction
74 Patient selection for CRT 5. Role of CRT in AF Pts: Mustic trial ml/kg/min = % p = BiV-RV RV-BiV Baseline Rando CO1 CO2 Results Baseline 1 Year 2 Year Heart Rate 75±15 76 ± 7 71 ± 12 NYHA 3 ± ± ± 0.5 6MWT 325 ± ± ± 99 Peak VO2 13 ± 4 14 ± 3.5 NA QOL 45 ± ± ± 20 LVEF (%) 26 ± ± 8 NA
75 Patient Selection for CRT: Particular Cases LV Function Changes in MUSTIC AF Patients Rand n=67 BIV-CO n=48 BIV 9M n=45 BIV 12M n=43 LVEDD (mm) 74±10 69±11*** 68±10*** 67±12*** LVESD (mm) 63±10 58±12*** 56±11*** 57±12*** MR area (cm 2 ) 7.8± ± ±4.6** 4.3±4.0** DFT (ms) 375± ±137* 471±154** 425±129*
76 PAVE trial (Post AV nodal ablation Evaluation study) «Ablate and pace» for AF, NYHA I-III, 6min HWT<450m, Mean QRS ~ 100ms, LVEF ~ 45% m Change in 6-min HWT P=0.03 LVEF (%) Change in LVEF P= weeks 6 months 20 Preimplant 6 months RV (n= 106) BV (n=146) Doshi, ACC 2004
77 Impact of CRT in Patients with AF Gasparini JACC 2006
78 Patient selection for CRT: particular cases 6. CRT in candidates for cardiac pacing? On evaluation CRT in PM pts N QRS (ms) NYHA Peak VO2 (ml/min/kg) QOL LVEF (%) Leclercq 1 20 Leon 2 23 NA Bakker 3 60 NA 1. Compare 2. Prevent 3. Combat 4. Block-HF 5. X-Change HF 1- C. Leclercq. Am Heart J 2000;140: A. Leon. J Am Coll Cardiol 2002;39: C. Bakker. PACE 2002;25:
79 CRT: Results and indications (Conclusions) Cardiac asynchrony is deleterious on hemodynamics CRT improves: NYHA Class, QOL score, Exercise Capacity (6MW, Peak VO2), LV function (EF, MR), Reverse Remodeling, Hospitalization, Mortality Classical CRT indications: Drug refractory NYHA III-IV, SR, QRS > 120 ms CM (ischemic or not): EF < 35%, EDD > 55 mm Additional CRT indications Chronic AF, Classical PM indications (Biopace) Future: NYHA II (Predict, Raft, Madit CRT), Investigation of Asynchrony at Echo (Desire, Prospect)
The Role of ICD Therapy in Cardiac Resynchronization
 The Role of ICD Therapy in Cardiac Resynchronization The Korean Society of Circulation 15 April 2005 Angel R. León, MD Carlyle Fraser Heart Center Division of Cardiology Emory University School of Medicine
The Role of ICD Therapy in Cardiac Resynchronization The Korean Society of Circulation 15 April 2005 Angel R. León, MD Carlyle Fraser Heart Center Division of Cardiology Emory University School of Medicine
Cardiac Devices CRT,ICD: Who is and is not a Candidate? Who Decides
 Cardiac Devices CRT,ICD: Who is and is not a Candidate? Who Decides Colette Seifer MB(Hons) FRCP(UK) Associate Professor, University of Manitoba, Cardiologist, Cardiac Sciences Program, St Boniface Hospital
Cardiac Devices CRT,ICD: Who is and is not a Candidate? Who Decides Colette Seifer MB(Hons) FRCP(UK) Associate Professor, University of Manitoba, Cardiologist, Cardiac Sciences Program, St Boniface Hospital
Cardiac Resynchronization Therapy for Heart Failure
 Cardiac Resynchronization Therapy for Heart Failure Ventricular Dyssynchrony vs Resynchronization Ventricular Dysynchrony Ventricular Dysynchrony 1 Electrical: Inter- or Intraventricular conduction delays
Cardiac Resynchronization Therapy for Heart Failure Ventricular Dyssynchrony vs Resynchronization Ventricular Dysynchrony Ventricular Dysynchrony 1 Electrical: Inter- or Intraventricular conduction delays
Bi-Ventricular pacing after the most recent studies
 Seminars of the Hellenic Working Groups February 18th-20 20,, 2010, Thessaloniki, Greece Bi-Ventricular pacing after the most recent studies Maurizio Lunati MD Director EP Lab & Unit Cardiology Dpt. Niguarda
Seminars of the Hellenic Working Groups February 18th-20 20,, 2010, Thessaloniki, Greece Bi-Ventricular pacing after the most recent studies Maurizio Lunati MD Director EP Lab & Unit Cardiology Dpt. Niguarda
HF and CRT: CRT-P versus CRT-D
 HF and CRT: CRT-P versus CRT-D Andrew E. Epstein, MD Professor of Medicine, Cardiovascular Division University of Pennsylvania Chief, Cardiology Section Philadelphia VA Medical Center Philadelphia, PA
HF and CRT: CRT-P versus CRT-D Andrew E. Epstein, MD Professor of Medicine, Cardiovascular Division University of Pennsylvania Chief, Cardiology Section Philadelphia VA Medical Center Philadelphia, PA
Devices and Other Non- Pharmacologic Therapy in CHF. Angel R. Leon, MD FACC Division of Cardiology Emory University School of Medicine
 Devices and Other Non- Pharmacologic Therapy in CHF Angel R. Leon, MD FACC Division of Cardiology Emory University School of Medicine Disclosure None University of Miami vs. OSU Renegade Miami football
Devices and Other Non- Pharmacologic Therapy in CHF Angel R. Leon, MD FACC Division of Cardiology Emory University School of Medicine Disclosure None University of Miami vs. OSU Renegade Miami football
Implantation of a CRT-Pacemaker Rather than CRT-Defibrillator is Usually Preferred
 Implantation of a CRT-Pacemaker Rather than CRT-Defibrillator is Usually Preferred Professor John GF Cleland University of Hull Kingston-upon-Hull United Kingdom Conflict of Interest: Funding or Speakers
Implantation of a CRT-Pacemaker Rather than CRT-Defibrillator is Usually Preferred Professor John GF Cleland University of Hull Kingston-upon-Hull United Kingdom Conflict of Interest: Funding or Speakers
CRT-D or CRT-P: HOW TO CHOOSE THE RIGHT PATIENT?
 CRT-D or CRT-P: HOW TO CHOOSE THE RIGHT PATIENT? Alessandro Lipari, MD Chair and Department of Cardiology University of Study and Spedali Civili Brescia -Italy The birth of CRT in Europe, 20 years ago
CRT-D or CRT-P: HOW TO CHOOSE THE RIGHT PATIENT? Alessandro Lipari, MD Chair and Department of Cardiology University of Study and Spedali Civili Brescia -Italy The birth of CRT in Europe, 20 years ago
Heart Failure Overview. Dr Chris K Y Wong
 Heart Failure Overview Dr Chris K Y Wong Heart Failure: A Growing, Global Health Issue Heart Failure 23 Million Afflicted Global Impact Worldwide ~23 million peopleworldwide afflicted with CHF 1 Exceeds
Heart Failure Overview Dr Chris K Y Wong Heart Failure: A Growing, Global Health Issue Heart Failure 23 Million Afflicted Global Impact Worldwide ~23 million peopleworldwide afflicted with CHF 1 Exceeds
Indications for and Prediction of Successful Responses of CRT for Patients with Heart Failure
 Indications for and Prediction of Successful Responses of CRT for Patients with Heart Failure Edmund Keung, MD Clinical Chief, Cardiology Section San Francisco VAMC October 25, 2008 Presentation Outline
Indications for and Prediction of Successful Responses of CRT for Patients with Heart Failure Edmund Keung, MD Clinical Chief, Cardiology Section San Francisco VAMC October 25, 2008 Presentation Outline
Heart failure and sudden death
 Heart failure and sudden death What did we learn so far from important ICD- and CRT trials? Helmut U. Klein M.D. University of Rochester Medical Center Heart Research Follow up Program Arrhythmic substrate
Heart failure and sudden death What did we learn so far from important ICD- and CRT trials? Helmut U. Klein M.D. University of Rochester Medical Center Heart Research Follow up Program Arrhythmic substrate
Arthur J. Moss, MD Professor of Medicine/Cardiology University of Rochester Medical Center Rochester, NY. DISCLOSURE INFORMATION Arthur J.
 Saving Lives and Preventing Heart Failure: The MADIT Family of Trials Arthur J. Moss, MD Professor of Medicine/Cardiology University of Rochester Medical Center Rochester, NY Update in Electrocardiography
Saving Lives and Preventing Heart Failure: The MADIT Family of Trials Arthur J. Moss, MD Professor of Medicine/Cardiology University of Rochester Medical Center Rochester, NY Update in Electrocardiography
Effect of Ventricular Pacing on Myocardial Function. Inha University Hospital Sung-Hee Shin
 Effect of Ventricular Pacing on Myocardial Function Inha University Hospital Sung-Hee Shin Contents 1. The effect of right ventricular apical pacing 2. Strategies for physiologically optimal ventricular
Effect of Ventricular Pacing on Myocardial Function Inha University Hospital Sung-Hee Shin Contents 1. The effect of right ventricular apical pacing 2. Strategies for physiologically optimal ventricular
Understanding and Development of New Therapies for Heart Failure - Lessons from Recent Clinical Trials -
 Understanding and Development of New Therapies for Heart Failure - Lessons from Recent Clinical Trials - Clinical trials Evidence-based medicine, clinical practice Impact upon Understanding pathophysiology
Understanding and Development of New Therapies for Heart Failure - Lessons from Recent Clinical Trials - Clinical trials Evidence-based medicine, clinical practice Impact upon Understanding pathophysiology
Heart Failure Overview. Dr Chris K Y Wong
 Heart Failure Overview Dr Chris K Y Wong Heart Failure: A Growing, Global Health Issue Heart Failure 23 Million Afflicted Global Impact Worldwide ~23 million peopleworldwide afflicted with CHF 1 Exceeds
Heart Failure Overview Dr Chris K Y Wong Heart Failure: A Growing, Global Health Issue Heart Failure 23 Million Afflicted Global Impact Worldwide ~23 million peopleworldwide afflicted with CHF 1 Exceeds
CT Academy of Family Physicians Scientific Symposium October 2012 Amit Pursnani, MD
 CT Academy of Family Physicians Scientific Symposium October 2012 Amit Pursnani, MD Clinical syndrome resulting from a structural or functional cardiac disorder that impairs the ability of the heart to
CT Academy of Family Physicians Scientific Symposium October 2012 Amit Pursnani, MD Clinical syndrome resulting from a structural or functional cardiac disorder that impairs the ability of the heart to
Cardiac Resynchronization Therapy. Michelle Khoo, MD
 Cardiac Resynchronization Therapy Michelle Khoo, MD 10.7.08 HuiKuri HV NEJM 2001 Sudden Death (SD) in Subset Populations HuiKuri HV NEJM 2001 Sudden Death (SD) in Subset Populations SD in Competitive Athletes
Cardiac Resynchronization Therapy Michelle Khoo, MD 10.7.08 HuiKuri HV NEJM 2001 Sudden Death (SD) in Subset Populations HuiKuri HV NEJM 2001 Sudden Death (SD) in Subset Populations SD in Competitive Athletes
Importance of CRT team for optimization of the results: a European point of view
 Importance of CRT team for optimization of the results: a European point of view Matteo Bertini, MD, PhD Arcispedale S. Anna Azienda Ospedaliero-Universitaria Cona-Ferrara No conflict of interest to declare
Importance of CRT team for optimization of the results: a European point of view Matteo Bertini, MD, PhD Arcispedale S. Anna Azienda Ospedaliero-Universitaria Cona-Ferrara No conflict of interest to declare
Cardiac Resynchronization Therapy Guidelines and Missing Groups
 Cardiac Resynchronization Therapy Guidelines and Missing Groups Frank Pelosi, Jr., MD, FACC, FHRS Director, Cardiac Electrophysiology Fellowship Associate Professor of Medicine University of Michigan Health
Cardiac Resynchronization Therapy Guidelines and Missing Groups Frank Pelosi, Jr., MD, FACC, FHRS Director, Cardiac Electrophysiology Fellowship Associate Professor of Medicine University of Michigan Health
Primary prevention of SCD with the ICD in Nonischemic Cardiomyopathy
 Primary prevention of SCD with the ICD in Nonischemic Cardiomyopathy Michael R Gold, MD, PhD Medical University of South Carolina Charleston, SC USA Disclosures: Consulting and Clinical Trials Medtronic
Primary prevention of SCD with the ICD in Nonischemic Cardiomyopathy Michael R Gold, MD, PhD Medical University of South Carolina Charleston, SC USA Disclosures: Consulting and Clinical Trials Medtronic
Large RCT s of CRT 2002 to present
 Have We Expanded Our Use of CRT for Heart Failure Patients? Sana M. Al-Khatib, MD, MHS Associate Professor of Medicine Electrophysiology Section- Division of Cardiology Duke University Potential Conflicts
Have We Expanded Our Use of CRT for Heart Failure Patients? Sana M. Al-Khatib, MD, MHS Associate Professor of Medicine Electrophysiology Section- Division of Cardiology Duke University Potential Conflicts
Do All Patients With An ICD Indication Need A BiV Pacing Device?
 Do All Patients With An ICD Indication Need A BiV Pacing Device? Muhammad A. Hammouda, MD Electrophysiology Laboratory Department of Critical Care Medicine Cairo University Etiology and Pathophysiology
Do All Patients With An ICD Indication Need A BiV Pacing Device? Muhammad A. Hammouda, MD Electrophysiology Laboratory Department of Critical Care Medicine Cairo University Etiology and Pathophysiology
Device Therapy for Heart Failure
 Device Therapy for Heart Failure Dr. Shelley Zieroth FRCPC Assistant Professor, Cardiology, University of Manitoba Director of Cardiac Transplant and Heart Failure Clinics St Boniface General Hospital,
Device Therapy for Heart Failure Dr. Shelley Zieroth FRCPC Assistant Professor, Cardiology, University of Manitoba Director of Cardiac Transplant and Heart Failure Clinics St Boniface General Hospital,
8/8/2011. CARDIAC RESYCHRONIZATION THERAPY for Heart Failure. Case Presentation. Case Presentation
 CARDIAC RESYCHRONIZATION THERAPY for Heart Failure James Taylor, DO, FACOS Cardiothoracic and Vascular surgery San Angelo Community Medical Center San Angelo, TX Case Presentation 64 year old female with
CARDIAC RESYCHRONIZATION THERAPY for Heart Failure James Taylor, DO, FACOS Cardiothoracic and Vascular surgery San Angelo Community Medical Center San Angelo, TX Case Presentation 64 year old female with
IMPLANTABLE DEVICE THERAPY FOR HEART FAILURE
 IMPLANTABLE DEVICE THERAPY FOR HEART FAILURE Nora Goldschlager, M.D. MACP, FACC, FAHA, FHRS Cardiology San Francisco General Hospital UCSF Disclosures: None LEADING CAUSES OF DEATH IN US Sudden cardiac
IMPLANTABLE DEVICE THERAPY FOR HEART FAILURE Nora Goldschlager, M.D. MACP, FACC, FAHA, FHRS Cardiology San Francisco General Hospital UCSF Disclosures: None LEADING CAUSES OF DEATH IN US Sudden cardiac
ESC Guidelines for the Diagnosis and Treatment of Chronic Heart Failure
 ESC Guidelines for the Diagnosis and Treatment of Chronic Heart Failure - 2005 Karl Swedberg Professor of Medicine Department of Medicine Sahlgrenska University Hospital/Östra Göteborg University Göteborg
ESC Guidelines for the Diagnosis and Treatment of Chronic Heart Failure - 2005 Karl Swedberg Professor of Medicine Department of Medicine Sahlgrenska University Hospital/Östra Göteborg University Göteborg
All in the Past? Win K. Shen, MD Mayo Clinic Arizona Controversies and Advances in CV Diseases Cedars-Sinai Heart Institute, MFMER
 ICD for NICM All in the Past? Win K. Shen, MD Mayo Clinic Arizona Controversies and Advances in CV Diseases Cedars-Sinai Heart Institute, 2017 2017 MFMER 3686275-1 DISCLOSURE Relevant Financial Relationship(s)
ICD for NICM All in the Past? Win K. Shen, MD Mayo Clinic Arizona Controversies and Advances in CV Diseases Cedars-Sinai Heart Institute, 2017 2017 MFMER 3686275-1 DISCLOSURE Relevant Financial Relationship(s)
The Management of Heart Failure after Biventricular Pacing
 The Management of Heart Failure after Biventricular Pacing Juan M. Aranda, Jr., MD University of Florida College of Medicine, Division of Cardiovascular Medicine, Gainesville, Florida Approximately 271,000
The Management of Heart Failure after Biventricular Pacing Juan M. Aranda, Jr., MD University of Florida College of Medicine, Division of Cardiovascular Medicine, Gainesville, Florida Approximately 271,000
Dialysis-Dependent Cardiomyopathy Patients Demonstrate Poor Survival Despite Reverse Remodeling With Cardiac Resynchronization Therapy
 Dialysis-Dependent Cardiomyopathy Patients Demonstrate Poor Survival Despite Reverse Remodeling With Cardiac Resynchronization Therapy Evan Adelstein, MD, FHRS John Gorcsan III, MD Samir Saba, MD, FHRS
Dialysis-Dependent Cardiomyopathy Patients Demonstrate Poor Survival Despite Reverse Remodeling With Cardiac Resynchronization Therapy Evan Adelstein, MD, FHRS John Gorcsan III, MD Samir Saba, MD, FHRS
Device based CRT optimization: is there a future? Lessons learned from published trials
 Device based CRT optimization: is there a future? Lessons learned from published trials C. Leclercq Department of Cardiology Centre Cardio-Pneumologique Rennes, France Presenter Disclosure Information
Device based CRT optimization: is there a future? Lessons learned from published trials C. Leclercq Department of Cardiology Centre Cardio-Pneumologique Rennes, France Presenter Disclosure Information
Aldosterone Antagonism in Heart Failure: Now for all Patients?
 Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Risk Stratification of Sudden Cardiac Death
 Risk Stratification of Sudden Cardiac Death Michael R Gold, MD, PhD Medical University of South Carolina Charleston, SC USA Disclosures: None Sudden Cardiac Death A Major Public Health Problem > 1/2 of
Risk Stratification of Sudden Cardiac Death Michael R Gold, MD, PhD Medical University of South Carolina Charleston, SC USA Disclosures: None Sudden Cardiac Death A Major Public Health Problem > 1/2 of
Disclosures. Overview. Goal statement. Advances in Chronic Heart Failure Management 5/22/17
 Disclosures Advances in Chronic Heart Failure Management I have nothing to disclose Van N Selby, MD UCSF Advanced Heart Failure Program May 22, 2017 Goal statement To review recently-approved therapies
Disclosures Advances in Chronic Heart Failure Management I have nothing to disclose Van N Selby, MD UCSF Advanced Heart Failure Program May 22, 2017 Goal statement To review recently-approved therapies
New Strategies For Treating Patients With Chronic Heart Failure
 New Strategies For Treating Patients With Chronic Heart Failure Barry Greenberg MD Professor of Medicine Director, Advanced Heart Failure Treatment Program University of California, San Diego Disclosures
New Strategies For Treating Patients With Chronic Heart Failure Barry Greenberg MD Professor of Medicine Director, Advanced Heart Failure Treatment Program University of California, San Diego Disclosures
Cardiac Resynchronisation Therapy for all Patients Requiring Ventricular Pacing
 Cardiac Resynchronisation Therapy for all Patients Requiring Ventricular Pacing Philippe Mabo University Hospital, Rennes, France ESC Congress 2010, Stockholm 29 Aug 2010 Which Patients? Candidate for
Cardiac Resynchronisation Therapy for all Patients Requiring Ventricular Pacing Philippe Mabo University Hospital, Rennes, France ESC Congress 2010, Stockholm 29 Aug 2010 Which Patients? Candidate for
BSH Annual Autumn Meeting 2017
 BSH Annual Autumn Meeting 2017 Presentation title: The Development of CRT Speaker: John GF Cleland Conflicts of interest: I have received research support and honoraria from Biotronik, Boston Scientific,
BSH Annual Autumn Meeting 2017 Presentation title: The Development of CRT Speaker: John GF Cleland Conflicts of interest: I have received research support and honoraria from Biotronik, Boston Scientific,
Cardiac Resynchronization ICD Therapy: What is New?
 Cardiac Resynchronization ICD Therapy: What is New? Emile Daoud, MD Section Chief, Cardiac Electrophysiology Professor of Medicine The Ohio State University Normal Activation, Narrow QRS Synchrony Abnormal
Cardiac Resynchronization ICD Therapy: What is New? Emile Daoud, MD Section Chief, Cardiac Electrophysiology Professor of Medicine The Ohio State University Normal Activation, Narrow QRS Synchrony Abnormal
Comparison of clinical trials evaluating cardiac resynchronization therapy in mild to moderate heart failure
 HOT TOPIC Cardiology Journal 2010, Vol. 17, No. 6, pp. 543 548 Copyright 2010 Via Medica ISSN 1897 5593 Comparison of clinical trials evaluating cardiac resynchronization therapy in mild to moderate heart
HOT TOPIC Cardiology Journal 2010, Vol. 17, No. 6, pp. 543 548 Copyright 2010 Via Medica ISSN 1897 5593 Comparison of clinical trials evaluating cardiac resynchronization therapy in mild to moderate heart
First question: Does CRT Work in AF?
 CRT in AF Does it work and when to ablate AF versus AV node Maurizio Gasparini Chief EP and Pacing Unit Humanitas Research Hospital, Rozzano - Milano, Italy First question: Does CRT Work in AF? As any
CRT in AF Does it work and when to ablate AF versus AV node Maurizio Gasparini Chief EP and Pacing Unit Humanitas Research Hospital, Rozzano - Milano, Italy First question: Does CRT Work in AF? As any
Implantable cardioverter-defibrillators and cardiac resynchronization therapy
 Implantable cardioverter-defibrillators and cardiac resynchronization therapy Johannes Holzmeister, MD University Hospital Zurich, Zurich, Switzerland Frontiers of heart failure controversies, ESC - Paris
Implantable cardioverter-defibrillators and cardiac resynchronization therapy Johannes Holzmeister, MD University Hospital Zurich, Zurich, Switzerland Frontiers of heart failure controversies, ESC - Paris
A patient with decompensated HF
 A patient with decompensated HF Professor Michel KOMAJDA University Pierre & Marie Curie Pitie Salpetriere Hospital Department of Cardiology Paris (France) Declaration Of Interest 2010 Speaker : Servier,
A patient with decompensated HF Professor Michel KOMAJDA University Pierre & Marie Curie Pitie Salpetriere Hospital Department of Cardiology Paris (France) Declaration Of Interest 2010 Speaker : Servier,
Beta-blockers in heart failure: evidence put into practice
 Beta-blockers in heart failure: evidence put into practice John McMurray Professor of Medical Cardiology, University of Glasgow & Consultant Cardiologist,Western Infirmary, Glasgow, UK Eugene Braunwald
Beta-blockers in heart failure: evidence put into practice John McMurray Professor of Medical Cardiology, University of Glasgow & Consultant Cardiologist,Western Infirmary, Glasgow, UK Eugene Braunwald
The Role of Ventricular Electrical Delay to Predict Left Ventricular Remodeling With Cardiac Resynchronization Therapy
 The Role of Ventricular Electrical Delay to Predict Left Ventricular Remodeling With Cardiac Resynchronization Therapy Results from the SMART-AV Trial Michael R. Gold, MD, PhD, Ulrika Birgersdotter-Green,
The Role of Ventricular Electrical Delay to Predict Left Ventricular Remodeling With Cardiac Resynchronization Therapy Results from the SMART-AV Trial Michael R. Gold, MD, PhD, Ulrika Birgersdotter-Green,
Treatment of Atrial Fibrillation in Heart Failure
 Stockholm, September 1st 2010 Treatment of Atrial Fibrillation in Heart Failure Rhythm control: Which drugs? Stefan H. Hohnloser J.W. Goethe University Frankfurt, Germany Presenter disclosure information:
Stockholm, September 1st 2010 Treatment of Atrial Fibrillation in Heart Failure Rhythm control: Which drugs? Stefan H. Hohnloser J.W. Goethe University Frankfurt, Germany Presenter disclosure information:
Disclosures. Advances in Chronic Heart Failure Management 6/12/2017. Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017
 Advances in Chronic Heart Failure Management Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017 I have nothing to disclose Disclosures 1 Goal statement To review recently-approved therapies
Advances in Chronic Heart Failure Management Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017 I have nothing to disclose Disclosures 1 Goal statement To review recently-approved therapies
How do I convert my CRT Non Responder into Responder?
 How do I convert my CRT Non Responder into Responder? Michael R Gold, MD, PhD Medical University of South Carolina Charleston, SC Disclosures: Clinical Trials and Consulting Boston Scientific, Medtronic
How do I convert my CRT Non Responder into Responder? Michael R Gold, MD, PhD Medical University of South Carolina Charleston, SC Disclosures: Clinical Trials and Consulting Boston Scientific, Medtronic
CRT response: definition and handling of non-responders
 CRT response: definition and handling of non-responders Maurizio Gasparini Chief of Electrophysiology and Pacing Unit IRCCS, Istituto Clinico Humanitas, Rozzano- Italy Definition of non-responders First
CRT response: definition and handling of non-responders Maurizio Gasparini Chief of Electrophysiology and Pacing Unit IRCCS, Istituto Clinico Humanitas, Rozzano- Italy Definition of non-responders First
ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure
 Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
ESC Guidelines. ESC Guidelines Update For internal training purpose. European Heart Journal, doi: /eurheart/ehn309
 ESC Guidelines Update 2008 ESC Guidelines Heart failure update 2008 For internal training purpose. 0 Agenda Introduction Classes of recommendations Level of evidence Treatment algorithm Changes to ESC
ESC Guidelines Update 2008 ESC Guidelines Heart failure update 2008 For internal training purpose. 0 Agenda Introduction Classes of recommendations Level of evidence Treatment algorithm Changes to ESC
A Square Peg in a Round Hole: CRT IN PAEDIATRICS AND CONGENITAL HEART DISEASE
 A Square Peg in a Round Hole: CRT IN PAEDIATRICS AND CONGENITAL HEART DISEASE Adele Greyling Dora Nginza Hospital, Port Elizabeth SA Heart November 2017 What are the guidelines based on? MADIT-II Size:
A Square Peg in a Round Hole: CRT IN PAEDIATRICS AND CONGENITAL HEART DISEASE Adele Greyling Dora Nginza Hospital, Port Elizabeth SA Heart November 2017 What are the guidelines based on? MADIT-II Size:
Cardiac resynchronization therapy for heart failure: state of the art
 Cardiac resynchronization therapy for heart failure: state of the art Béla Merkely MD, PhD, DSc, FESC, FACC Vice president of the European Society of Cardiology Honorary president of the Hungarian Society
Cardiac resynchronization therapy for heart failure: state of the art Béla Merkely MD, PhD, DSc, FESC, FACC Vice president of the European Society of Cardiology Honorary president of the Hungarian Society
Heart Failure Treatments
 Heart Failure Treatments Past & Present www.philippelefevre.com Background Background Chronic heart failure Drugs Mechanical Electrical Background Chronic heart failure Drugs Mechanical Electrical Sudden
Heart Failure Treatments Past & Present www.philippelefevre.com Background Background Chronic heart failure Drugs Mechanical Electrical Background Chronic heart failure Drugs Mechanical Electrical Sudden
Heart Failure. Jay Shavadia
 Heart Failure Jay Shavadia Definition Clinical syndrome characterized by: Symptoms: breathlessness at rest or on exercise, fatigue, tiredness or ankle swelling AND Signs: tachycardia, tachypnea, pulmonary
Heart Failure Jay Shavadia Definition Clinical syndrome characterized by: Symptoms: breathlessness at rest or on exercise, fatigue, tiredness or ankle swelling AND Signs: tachycardia, tachypnea, pulmonary
Follow-up of CRT patients ESC Munich Clinical and biological follow-up of CRT patients
 Follow-up of CRT patients ESC Munich 12-08-26 Clinical and biological follow-up of CRT patients Frieder Braunschweig MD PhD FESC Associate Professor of Cardiology Karolinska University Hospital Stockholm,
Follow-up of CRT patients ESC Munich 12-08-26 Clinical and biological follow-up of CRT patients Frieder Braunschweig MD PhD FESC Associate Professor of Cardiology Karolinska University Hospital Stockholm,
Heart Failure Management. Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist
 Heart Failure Management Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist Heart failure prevalence is expected to continue to increase¹ 21 MILLION ADULTS WORLDWIDE
Heart Failure Management Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist Heart failure prevalence is expected to continue to increase¹ 21 MILLION ADULTS WORLDWIDE
Implantable Cardioverter Defibrillator Therapy in MADIT II Patients with Signs and Symptoms of Heart Failure
 Implantable Cardioverter Defibrillator Therapy in MADIT II Patients with Signs and Symptoms of Heart Failure Wojciech Zareba Postinfarction patients with left ventricular dysfunction are at increased risk
Implantable Cardioverter Defibrillator Therapy in MADIT II Patients with Signs and Symptoms of Heart Failure Wojciech Zareba Postinfarction patients with left ventricular dysfunction are at increased risk
Gender and cardiac resynchronization therapy. Chairs: David Heaven & Belinda Green. Gender and Cardiac Resynchronisation Therapy
 Electrophysiology Gender and cardiac resynchronization therapy Dean Boddington Chairs: David Heaven & Belinda Green Gender and Cardiac Resynchronisation Therapy Dean Boddington Tauranga Hospital 1 Disclosure/Warning
Electrophysiology Gender and cardiac resynchronization therapy Dean Boddington Chairs: David Heaven & Belinda Green Gender and Cardiac Resynchronisation Therapy Dean Boddington Tauranga Hospital 1 Disclosure/Warning
ICD Guidelines: who benefits from an ICD?
 ICD Guidelines: who benefits from an ICD? Matthew Bennett Cardiac Electrophysiologist Vancouver Coastal Health, Device Lead Associate Professor, UBC Matthew.bennett@vch.ca Disclosures I have research collaborations
ICD Guidelines: who benefits from an ICD? Matthew Bennett Cardiac Electrophysiologist Vancouver Coastal Health, Device Lead Associate Professor, UBC Matthew.bennett@vch.ca Disclosures I have research collaborations
ESC Paris, August 2011
 Controversial Issues in CRT: Is The Optimisation of AV & VV Delays Useful? ESC Paris, August 2011 D Gras, MD, Nantes, France DECLARATION OF CONFLICT OF INTEREST Consultancy Minor Medtronic Saint Jude Medical
Controversial Issues in CRT: Is The Optimisation of AV & VV Delays Useful? ESC Paris, August 2011 D Gras, MD, Nantes, France DECLARATION OF CONFLICT OF INTEREST Consultancy Minor Medtronic Saint Jude Medical
Arrhythmias and Heart Failure Dr Chris Lang Consultant Cardiologist and Electrophysiologist Royal Infirmary of Edinburgh
 Arrhythmias and Heart Failure Dr Chris Lang Consultant Cardiologist and Electrophysiologist Royal Infirmary of Edinburgh Arrhythmias and Heart Failure Ventricular Supraventricular VT/VF Primary prevention
Arrhythmias and Heart Failure Dr Chris Lang Consultant Cardiologist and Electrophysiologist Royal Infirmary of Edinburgh Arrhythmias and Heart Failure Ventricular Supraventricular VT/VF Primary prevention
Thoranis Chantrarat MD
 Device Therapy in Heart Failure Thoranis Chantrarat MD 1 Scope of presentation Natural history of heart failure Primary and secondary prevention ICD and its indication CRT and its indication 2 Severity
Device Therapy in Heart Failure Thoranis Chantrarat MD 1 Scope of presentation Natural history of heart failure Primary and secondary prevention ICD and its indication CRT and its indication 2 Severity
The road to successful CRT implantation: The role of echo
 The road to successful CRT implantation: The role of echo Tae-Ho Park Dong-A University Hospital, Busan, Korea Terminology Cardiac Resynchronization Therapy (CRT) = Biventricular pacing (BiV) = Left ventricular
The road to successful CRT implantation: The role of echo Tae-Ho Park Dong-A University Hospital, Busan, Korea Terminology Cardiac Resynchronization Therapy (CRT) = Biventricular pacing (BiV) = Left ventricular
Epidemiology of Symptomatic Heart Failure in the U.S.
 William T. Abraham, MD, FACP, FACC, FAHA, FESC Professor of Medicine, Physiology, and Cell Biology Director, Division of Cardiovascular Medicine Deputy Director Davis Heart and Lung Research Institute
William T. Abraham, MD, FACP, FACC, FAHA, FESC Professor of Medicine, Physiology, and Cell Biology Director, Division of Cardiovascular Medicine Deputy Director Davis Heart and Lung Research Institute
Device Based Therapy for the Failing Heart: ICD and Cardiac Resynchronization Rx
 Device Based Therapy for the Failing Heart: ICD and Cardiac Resynchronization Rx Charles Gottlieb, MD Director of Electrophysiology Abington Memorial Hospital Heart Failure Mortality Mechanism of death
Device Based Therapy for the Failing Heart: ICD and Cardiac Resynchronization Rx Charles Gottlieb, MD Director of Electrophysiology Abington Memorial Hospital Heart Failure Mortality Mechanism of death
This is What I do to Improve CRT Response for CRT Non-Responders
 This is What I do to Improve CRT Response for CRT Non-Responders Michael R Gold, MD, PhD Medical University of South Carolina Charleston, SC Disclosures: Steering Committees (unpaid) and Clinical Trials,
This is What I do to Improve CRT Response for CRT Non-Responders Michael R Gold, MD, PhD Medical University of South Carolina Charleston, SC Disclosures: Steering Committees (unpaid) and Clinical Trials,
Heart Failure. Guillaume Jondeau Hôpital Bichat, Paris, France
 Heart Failure Guillaume Jondeau Hôpital Bichat, Paris, France Epidemiology Importance of PEF Europe I-PREFER study. Abstract: 2835 Prevalence of HF Preserved LV systolic Function older (65 vs 62 y, p
Heart Failure Guillaume Jondeau Hôpital Bichat, Paris, France Epidemiology Importance of PEF Europe I-PREFER study. Abstract: 2835 Prevalence of HF Preserved LV systolic Function older (65 vs 62 y, p
Device therapy in heartfailure Update of the ESC guidelines. Karl Swedberg
 Device therapy in heartfailure Update of the ESC guidelines Karl Swedberg Professor of Medicine Department of emergency and cardiovascular medicine Sahlgrenska Academy University of Gothenburg, Sweden
Device therapy in heartfailure Update of the ESC guidelines Karl Swedberg Professor of Medicine Department of emergency and cardiovascular medicine Sahlgrenska Academy University of Gothenburg, Sweden
ICD Therapy. Disclaimers
 ICD Therapy Rodney Horton, MD Texas Cardiac Arrhythmia Institute Texas Cardiovascular, PA Austin, TX Speaker s Bureau St. Jude Medical Medtronic Boston Scientific Disclaimers Clinical Advisory Panel St.
ICD Therapy Rodney Horton, MD Texas Cardiac Arrhythmia Institute Texas Cardiovascular, PA Austin, TX Speaker s Bureau St. Jude Medical Medtronic Boston Scientific Disclaimers Clinical Advisory Panel St.
Left Ventricular Ejection Fraction >35%
 Controversies in Cardiac Resynchronisation Therapy Left Ventricular Ejection Fraction >35% Professor John GF Cleland University of Hull Kingston-upon-Hull United Kingdom Conflict of Interest: I have received
Controversies in Cardiac Resynchronisation Therapy Left Ventricular Ejection Fraction >35% Professor John GF Cleland University of Hull Kingston-upon-Hull United Kingdom Conflict of Interest: I have received
Optimal blockade of the Renin- Angiotensin-Aldosterone. in chronic heart failure
 Optimal blockade of the Renin- Angiotensin-Aldosterone Aldosterone- (RAA)-System in chronic heart failure Jan Östergren Department of Medicine Karolinska University Hospital Stockholm, Sweden Key Issues
Optimal blockade of the Renin- Angiotensin-Aldosterone Aldosterone- (RAA)-System in chronic heart failure Jan Östergren Department of Medicine Karolinska University Hospital Stockholm, Sweden Key Issues
Therapeutic Targets and Interventions
 Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
Scompenso cardiaco e F A : ruolo della ablazione transcatetere. Prof. Fiorenzo Gaita
 Scompenso cardiaco e F A : ruolo della ablazione transcatetere Prof. Fiorenzo Gaita Patients with atrial fibrillation (%) Prevalence of AF in HF Trials 60 50 30% NYHA III-IV NYHA IV 40 NYHA II-III 30 20
Scompenso cardiaco e F A : ruolo della ablazione transcatetere Prof. Fiorenzo Gaita Patients with atrial fibrillation (%) Prevalence of AF in HF Trials 60 50 30% NYHA III-IV NYHA IV 40 NYHA II-III 30 20
Sliwa et al. JACC 2004;44:
 TREATMENT OF ADVANCED HEART FAILURE HEART DISEASE IN KENTUCKY Navin Rajagopalan, MD Assistant Professor of Medicine University of Kentucky Director, Congestive Heart Failure Medical Director of Cardiac
TREATMENT OF ADVANCED HEART FAILURE HEART DISEASE IN KENTUCKY Navin Rajagopalan, MD Assistant Professor of Medicine University of Kentucky Director, Congestive Heart Failure Medical Director of Cardiac
TRATTAMENTO INTERVENTISTICO. Dr. Antonio Sagone
 TRATTAMENTO INTERVENTISTICO Dr. Antonio Sagone 1 Heart Failure Prevalence & Prognosis Over 26 million people worldwide suffer from heart failure, a chronic, progressive condition in which the heart muscle
TRATTAMENTO INTERVENTISTICO Dr. Antonio Sagone 1 Heart Failure Prevalence & Prognosis Over 26 million people worldwide suffer from heart failure, a chronic, progressive condition in which the heart muscle
Resynchronization/Defibrillation
 Resynchronization/Defibrillation for Ambulatory Heart Failure Trial Cardiac Resynchronization Therapy for Mild to Moderate Heart Failure George Wells University of Ottawa Heart Institute Department of
Resynchronization/Defibrillation for Ambulatory Heart Failure Trial Cardiac Resynchronization Therapy for Mild to Moderate Heart Failure George Wells University of Ottawa Heart Institute Department of
THE ROLE OF ICD THERAPY FOR PRIMARY PREVENTION Leonard Ganz, M.D. Pittsburgh, PA
 THE ROLE OF ICD THERAPY FOR PRIMARY PREVENTION Leonard Ganz, M.D. Pittsburgh, PA Speakers Bureau: Zoll / Lifecore, Sanofi Aventis, Cardionet Consultant: Boston Scientific, St. Jude Medical, Biotronik,
THE ROLE OF ICD THERAPY FOR PRIMARY PREVENTION Leonard Ganz, M.D. Pittsburgh, PA Speakers Bureau: Zoll / Lifecore, Sanofi Aventis, Cardionet Consultant: Boston Scientific, St. Jude Medical, Biotronik,
Is QRS width predictive of the clinical and echocardiographic response to chronic CRT in mildly symptomatic HF patients?
 Is QRS width predictive of the clinical and echocardiographic response to chronic CRT in mildly symptomatic HF patients? Data from REVERSE C Thébault 1, M Gold 2, C Linde 3, WT Abraham 4, C Leclercq 1,
Is QRS width predictive of the clinical and echocardiographic response to chronic CRT in mildly symptomatic HF patients? Data from REVERSE C Thébault 1, M Gold 2, C Linde 3, WT Abraham 4, C Leclercq 1,
Imaging in dilated cardiomyopathy : factors associated with a poor outcome
 Imaging in dilated cardiomyopathy : factors associated with a poor outcome Johan De Sutter, MD, PhD, FESC AZ Maria Middelares Gent and University Gent - Belgium Dilated cardiomyopathy Cardiomyopathy with
Imaging in dilated cardiomyopathy : factors associated with a poor outcome Johan De Sutter, MD, PhD, FESC AZ Maria Middelares Gent and University Gent - Belgium Dilated cardiomyopathy Cardiomyopathy with
Cardiac devices beyond pacemaker and ICD Prof. Dr. Martin Borggrefe
 Cardiac devices beyond pacemaker and ICD Prof. Dr. Martin Borggrefe Mannheim CRT studies Patient selection CRT: NYHA III-IV, EF 35%, SR, QRS 120ms, LVEDD>55mm (25-45)% Non-Responder The Concept: Cardiac
Cardiac devices beyond pacemaker and ICD Prof. Dr. Martin Borggrefe Mannheim CRT studies Patient selection CRT: NYHA III-IV, EF 35%, SR, QRS 120ms, LVEDD>55mm (25-45)% Non-Responder The Concept: Cardiac
Why to use digoxin in heart failure?
 Why to use digoxin in heart failure? Yves Juillière, Cardiology, ILCV, CHU Nancy-Brabois, France Digitalis purpurea Representation of the extracellular loops and the transmembrane domain regions of the
Why to use digoxin in heart failure? Yves Juillière, Cardiology, ILCV, CHU Nancy-Brabois, France Digitalis purpurea Representation of the extracellular loops and the transmembrane domain regions of the
The SEPTAL CRT study (NCT: )
") Comparison of right ventricular septal pacing and right ventricular apical pacing in patients receiving cardiac resynchronization therapy defibrillators The SEPTAL CRT study (NCT: 00833352) Christophe
Comparison of right ventricular septal pacing and right ventricular apical pacing in patients receiving cardiac resynchronization therapy defibrillators The SEPTAL CRT study (NCT: 00833352) Christophe
Who does not need a primary preventive ICD?
 Who does not need a primary preventive ICD? Hildegard Tanner, Bern Universitätsklinik für Kardiologie Disclosure of potential conflicts of interest Travel grants for educational purposes from: Biosense
Who does not need a primary preventive ICD? Hildegard Tanner, Bern Universitätsklinik für Kardiologie Disclosure of potential conflicts of interest Travel grants for educational purposes from: Biosense
Fibrillazione atriale e scompenso: come interrompere il circolo vizioso.
 Alessandria, September 23 th 2017 Fibrillazione atriale e scompenso: come interrompere il circolo vizioso. Professor Fiorenzo Gaita Chief of the Cardiovascular Department Città della Salute e della Scienza
Alessandria, September 23 th 2017 Fibrillazione atriale e scompenso: come interrompere il circolo vizioso. Professor Fiorenzo Gaita Chief of the Cardiovascular Department Città della Salute e della Scienza
Heart Failure Dr Eric Klug Sunninghill, Sunward Park, CM Johannesburg Academic Hospital
 Heart Failure 2012 Dr Eric Klug Sunninghill, Sunward Park, CM Johannesburg Academic Hospital PRELOAD COWS Reduction in milk production INOTROPY & HEART RATE AFTERLOAD DISTRIBUTION NETWORK THE CLASSIC APPROACH
Heart Failure 2012 Dr Eric Klug Sunninghill, Sunward Park, CM Johannesburg Academic Hospital PRELOAD COWS Reduction in milk production INOTROPY & HEART RATE AFTERLOAD DISTRIBUTION NETWORK THE CLASSIC APPROACH
Nonpharmacologic Treatment of Ventricular Heart Failure
 Nonpharmacologic Treatment of Ventricular Heart Failure Hong Ryang Kil, MD, PhD Department of Pediatrics, College of Medicine, Chungnam National University 2001 AHA Guideline for CHF - Symptomatic LV dysfunction
Nonpharmacologic Treatment of Ventricular Heart Failure Hong Ryang Kil, MD, PhD Department of Pediatrics, College of Medicine, Chungnam National University 2001 AHA Guideline for CHF - Symptomatic LV dysfunction
Pharmacological Treatment for Chronic Heart Failure. Dr Elaine Chau HK Sanatorium & Hospital, Hong Kong 3 August 2014
 Pharmacological Treatment for Chronic Heart Failure Dr Elaine Chau HK Sanatorium & Hospital, Hong Kong 3 August 2014 1 ACC/AHA 2005 guideline update for Diagnosis & management of CHF in the Adult -SA Hunt
Pharmacological Treatment for Chronic Heart Failure Dr Elaine Chau HK Sanatorium & Hospital, Hong Kong 3 August 2014 1 ACC/AHA 2005 guideline update for Diagnosis & management of CHF in the Adult -SA Hunt
The Hearth Rate modulators. How to optimise treatment
 The Hearth Rate modulators How to optimise treatment Munich, ESC Congress 2012 Prof. Luigi Tavazzi GVM Care&Research E.S. Health Science Foundation Cotignola, IT Disclosure Cooperation with: Servier, Medtronic,
The Hearth Rate modulators How to optimise treatment Munich, ESC Congress 2012 Prof. Luigi Tavazzi GVM Care&Research E.S. Health Science Foundation Cotignola, IT Disclosure Cooperation with: Servier, Medtronic,
Interventional solutions for atrial fibrillation in patients with heart failure
 Interventional solutions for atrial fibrillation in patients with heart failure Advances in Cardiovascular Arrhythmias Great Innovations in Cardiology Matteo Anselmino, MD PhD Division of Cardiology Department
Interventional solutions for atrial fibrillation in patients with heart failure Advances in Cardiovascular Arrhythmias Great Innovations in Cardiology Matteo Anselmino, MD PhD Division of Cardiology Department
Online Appendix (JACC )
") Beta blockers in Heart Failure Collaborative Group Online Appendix (JACC013117-0413) Heart rate, heart rhythm and prognostic effect of beta-blockers in heart failure: individual-patient data meta-analysis
Beta blockers in Heart Failure Collaborative Group Online Appendix (JACC013117-0413) Heart rate, heart rhythm and prognostic effect of beta-blockers in heart failure: individual-patient data meta-analysis
Disclosures: Drs. Bristow, Saxon, Boehmer, Kass, and Feldman are consultants to Guidant (sponsor) HFSA Late-Breaker September 24, 2003
 HFSA Late-Breaker September 24, 2003") Cardiac Resynchronization Therapy (CRT) Reduces Hospitalizations, and CRT with Implantable Defibrillator (CRT-D) Reduces Mortality in Chronic Heart Failure: The COMPANION Trial Bristow MR,(Co-Ch) Feldman
Cardiac Resynchronization Therapy (CRT) Reduces Hospitalizations, and CRT with Implantable Defibrillator (CRT-D) Reduces Mortality in Chronic Heart Failure: The COMPANION Trial Bristow MR,(Co-Ch) Feldman
Dipartimento di Scienze Cardiovascolari Università Campus Bio-Medico di Roma Dott. Vito Calabrese
 Dipartimento di Scienze Cardiovascolari Università Campus Bio-Medico di Roma Dott. Vito Calabrese Because the primary objective was cure symptomatic bradicardya due to syncope Because this is the common
Dipartimento di Scienze Cardiovascolari Università Campus Bio-Medico di Roma Dott. Vito Calabrese Because the primary objective was cure symptomatic bradicardya due to syncope Because this is the common
State-of-the-Art Management of Chronic Systolic Heart Failure
 State-of-the-Art Management of Chronic Systolic Heart Failure Michael McCulloch, MD 17 th Annual Cardiovascular Update Intermountain Medical Center December 16, 2017 Disclosures: I have no financial disclosures
State-of-the-Art Management of Chronic Systolic Heart Failure Michael McCulloch, MD 17 th Annual Cardiovascular Update Intermountain Medical Center December 16, 2017 Disclosures: I have no financial disclosures
CRT: whom does it benefit?
 CRT: whom does it benefit? Francisco Leyva BSH Revalidation and Training 2018 Queen Elizabeth Hospital NICE guidelines for CRT LVEF 35% NYHA class I II III IV QRS
CRT: whom does it benefit? Francisco Leyva BSH Revalidation and Training 2018 Queen Elizabeth Hospital NICE guidelines for CRT LVEF 35% NYHA class I II III IV QRS
The Failing Heart in Primary Care
 The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
Contemporary Advanced Heart Failure Therapy
 Contemporary Advanced Heart Failure Therapy Andrew Boyle, MD Professor of Medicine Medical Director of Advanced Heart Failure Thomas Jefferson University Philadelphia, PA Audience Response Question 40
Contemporary Advanced Heart Failure Therapy Andrew Boyle, MD Professor of Medicine Medical Director of Advanced Heart Failure Thomas Jefferson University Philadelphia, PA Audience Response Question 40
12 th Annual Biomarkers in Heart Failure and Acute Coronary Syndromes: Diagnosis, Treatment and Devices. Heart Rate as a Cardiovascular Biomarker
 12 th Annual Biomarkers in Heart Failure and Acute Coronary Syndromes: Diagnosis, Treatment and Devices Heart Rate as a Cardiovascular Biomarker Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine,
12 th Annual Biomarkers in Heart Failure and Acute Coronary Syndromes: Diagnosis, Treatment and Devices Heart Rate as a Cardiovascular Biomarker Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine,
Heart Failure Medical and Surgical Treatment
 Heart Failure Medical and Surgical Treatment Daniel S. Yip, M.D. Medical Director, Heart Failure and Transplantation Mayo Clinic Second Annual Lakeland Regional Health Cardiovascular Symposium February
Heart Failure Medical and Surgical Treatment Daniel S. Yip, M.D. Medical Director, Heart Failure and Transplantation Mayo Clinic Second Annual Lakeland Regional Health Cardiovascular Symposium February
BENEFIT OF CRT IN MILDLY SYMPTOMATIC HEART FAILURE RECENT DATA FROM MADIT-CRT AND RAFT
 BENEFIT OF CRT IN MILDLY SYMPTOMATIC HEART FAILURE RECENT DATA FROM MADIT-CRT AND RAFT Ilan Goldenberg MD Professor of Cardiology Sheba Medical Center and Tel Aviv University, Israel University of Rochester
BENEFIT OF CRT IN MILDLY SYMPTOMATIC HEART FAILURE RECENT DATA FROM MADIT-CRT AND RAFT Ilan Goldenberg MD Professor of Cardiology Sheba Medical Center and Tel Aviv University, Israel University of Rochester
Advanced Heart Failure Management. Dr Andrew Hannah Consultant Cardiologist Aberdeen Royal Infirmary
 Advanced Heart Failure Management Dr Andrew Hannah Consultant Cardiologist Aberdeen Royal Infirmary Grading of heart failure Mr WY age 73 3/12 dyspnoea, fatigue and some ankle oedema PMH: hypertension
Advanced Heart Failure Management Dr Andrew Hannah Consultant Cardiologist Aberdeen Royal Infirmary Grading of heart failure Mr WY age 73 3/12 dyspnoea, fatigue and some ankle oedema PMH: hypertension
Medical management of LV aneurysm and subsequent cardiac remodeling: is it enough? J. Parissis Attikon University Hospital Athens, Greece
 Medical management of LV aneurysm and subsequent cardiac remodeling: is it enough? J. Parissis Attikon University Hospital Athens, Greece Disclosures Grants: ALARM investigator received research grants
Medical management of LV aneurysm and subsequent cardiac remodeling: is it enough? J. Parissis Attikon University Hospital Athens, Greece Disclosures Grants: ALARM investigator received research grants