The Role of DHMC as an ST Elevation Myocardial Infarction Receiving Center in a Regional STEMI Care Network:
|
|
|
- Jayson Austen Hines
- 5 years ago
- Views:
Transcription
1 The Role of DHMC as an ST Elevation Myocardial Infarction Receiving Center in a Regional STEMI Care Network: Nathaniel Niles, MD CREST Symposium November 7th, 28

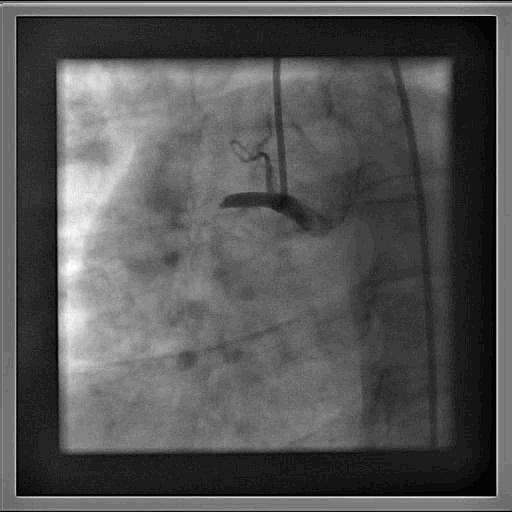
2 STEMI = Acute Coronary Thrombosis

3 STEMI (ST elevation Myocardial Infarction) Relatively common Multiple treatment strategy options Requires coordination Multidisciplinary EMS Emergency Medicine Cardiology Interhospital Must be managed quickly Time ~ Muscle
4 Pre-Hospital Delay The Golden early hours: Meta-analysis analysis on 5,246 patients in thrombolytic trials Boersma E. et al. Lancet. 1996:348:771
5 Thrombolytic Therapy is Inferior to PCI for Treating STEMI 23 study systematic review: short-term term outcomes 3 Frequency (%) 2 1 p= Death Primary PCI Thrombolytic Therapy p= Non-fatal reinfarction p= Total stroke p= Recurrent ischemia p= Death, reinfarction, stroke Lancet 23;361:13-2
6 Transfer for PCI vs On-site Thrombolytic 5 study systematic review: Frequency (%) Death o 1 PCI (n=1466) TTx (n=1443) Average Transfer Time 39 minutes p=.57 p= Non-fatal reinfarction p= p= p=.1 15 Total stroke ICH Death, reinfarction, stroke 8 Lancet 23;361:13-2
7 Absolute Risk Difference in Death (%) 1 o PCI Benefit also time dependent Mortality benefit with primary PCI as function of PCI-related time delay Circle sizes = P = sample size of the individual study. Solid line = weighted meta-regression. 62 min Benefit Favors PCI PCI-Related Time Delay (door-to-balloon - door-to-needle) Harm Favors Lysis Nallamothu BK, Bates ER. Am J Cardiol. 23;92:824-6
8 I IIa IIb III STEMI Guidelines (27) STEMI patients presenting to a hospital with PCI capability should be treated with primary PCI within 9 minutes of first medical contact as a systems goal (Level of Evidence: A) STEMI patients presenting to a hospital without PCI capability and who cannot be transferred to a PCI center and undergo PCI within 9 minutes of first medical contact should be treated with fibrinolytic therapy within 3 minutes of hospital presentation as a systems goal unless contraindicated. (Level of Evidence: B)
9 Regional STEMI Care Network Rationale PCI is > thrombolytic therapy Transfer for PCI > on-site fibrinolytic therapy Death during transfer rare US Guidelines: D2B 9 minutes Only ~ 25% acute care hospitals in the US are PCI capable and even en fewer have 24/7 cath labs Hospital specialization on primary PCI faster treatment and lower mortality So What once could be treated locally (Ttx( can be given at any hospital) now requires a regional network around a PCI Center to diagnose STEMI get the patient rapidly to PCI Moreover Trauma center systems have been successful Formalization of regional networks will better enable payers to track quality (treatment times) and structure incentives
10 DHMC Position in the System STEMI Patient ED 16% STEMI Patient EMS Primary PCI-Capable Capable Hospital DHMC ~4% 8% Zone 1 Zone 2 Local Non PCI-Capable Capable Hospital STEMI Referral Hospital Remote Non PCI-Capable Capable Hospital STEMI Referral Hospital STEMI Patient STEMI Patient
11 Reperfusion Strategy DHMC ED Primary PCI-Capable Capable Hospital 1 o PCI STEMI Patient Zone 1 Non PCI-Capable Capable Hospital (STEMI Referral Hospital) PCI avail within 9 Trf 1 o PCI Pharmaco-invasive Zone 2 Non PCI-Capable Capable Hospital (STEMI Referral Hospital) PCI not avail within 9 1 o Lytic Tx or ½ dose Lytic plus GP 2b3a Inh Trf for immediate PCI
12 CARESS Trial Outcome Death/re-MI/ refractory ischemia at 3 days Pharmaco invasive strategy (½ dose Lytic +Abciximab +PCI for all) (%) Thrombolysis alone (½ dose Lytic +Abciximab +rescue PCI only) (%) p Di Mario C. European Society of Cardiology Congress 27; September 3, 27; Vienna, Austria.

13 How has DHMC really performed as a STEMI Receiving Center?
14 The Region Upper CT Valley, ~6 m N and 45 m S on I91 and 3-4 m NW or SE on I89. 2 Referral Hospitals Zone 1 = the local area, APD and VAMC Zone 2 = everything else ~4 Ambulance services 2 Helicopters based at DHMC
15 DHMC STEMI Registry 94 total registry patients from 21 mid STEMI patients 13 NSTEMI patients 742 Presented to regional referral hospitals 149 Presented to DHMC 145 admitted with STEMI from DHMC ER 4 DHMC inpatients 34 Zone 1 (VAMC or APD) 33 transferred emergently to DHMC with STEMI 1 Admitted to initial hospital or initially tfxd elsewhere 78 Zone 2 (Other referral hospitals) 53 Admitted to 655 initial hospital transferred or initially tfxd emergently to elsewhere DHMC with STEMI 9 Managed conservatively 1 Managed conservatively 12 Managed conservatively 136 to cath lab emergently 5 post lytic 131 no lytic to cath lab late post lytic 32 to cath lab emergently 3 post lytic 29 no lytic to cath lab late post lytic 596 to cath lab emergently 47 post lytic 124 no lytic 47 to cath lab late post lytic
16 Median Times Over Time DHMC ED STEMI Patients minutes Door-to-tabletop Tabletop-to-balloon Door-to-balloon % of patients 9 minutes
17 Bradley E et al. N Engl J Med 26;355: MEDIAN DOOR-TO TO-BALLOON TIMES Distribution among 365 hospitals studied Median 1.4 SD April to September 25
18 DHMC ED STEMI Patients n= Actual 3 day mortality (%) ns TIMI score predicted 3 day mortality (%) 15 ns Years
19 DHMC ED & Zone 1 STEMI Patients n= Actual 3 day mortality (%) ns TIMI score predicted 3 day mortality (%) 15 ns Years
20 Zone 2 Patients (STEMI Patients Transferred from Remote Referral Hospitals)
21 Median Times Over Time Zone 2 STEMI Patients Ideal (Weekdays 7 AM to 5 PM) Door-to-tabletop Tabletop-to-balloon Door-to-balloon Suboptimal (After hours and Weekends) Door-to-tabletop Tabletop-to-balloon Door-to-balloon)
22 Circulation. 25;111: Initial Door-to-balloon times in Transfer Patients Undergoing 1 PCI in the US NRMI-3/4 Analysis ( ) n= % >24 minutes 4% < 9 minutes 12% 9-12 minutes 56% minutes 5% had door-to to-balloon time > 3 hours
23 Zone 2 STEMI Emergent Transfers: Zone 2 STEMI Emergent Transfers: Median Door-to to-table table time Q1(1)-Q2(7) Q2(7) Door-to-table table time (min) APD WRJVA Mt Ascutney New London VRH Gifford Springfield Cottage Grace Cottage NVRH Rutland CVH Speare Brattleboro Littleton Cheshire Weeks NCH Androscoggin UCVH Hospital
24 UCVH Zone 2 Transfers: Helicopter vs Ground Transport Median Door-to to-table table time Q1(1)-Q2(7) Q2(7) Helicopter (44%) Ground (56%) Mean of Median differences = 69 min Door-to-table table time (min) APD WRJVA Mt Ascutney New London VRH Gifford Springfield Cottage Grace Cottage NVRH Rutland CVH Speare Brattleboro Littleton Cheshire Weeks NCH Androscoggin Hospital
25 Q4(6) Q1(7) Q2(7) STEMI Emergent Transfer Volumes Q1(1)-Q2(7) Q2(7) Half Dose Full Dose No Lytic Given Ukn Percent of STEMI Patients Percent of STEMI Patients Q1(1) Q2(1) Q3(1) Q4(1) Q1(2) Q2(2) Q3(2) Q4(2) Q1(3) Q2(3) Q3(3) Q4(3) Q1(4) Q2(4) Q3(4) Q4(4) Q1(5) Q2(5) Q3(5) Q4(5) Q1(6) Q2(6) Q3(6)
26 Zone 2 STEMI Emergent Transfer Patients: By Intended Dose 3 Day Mortality % Mortality ns p< None Given Full Dose Half Dose Lytic Dose Strategy p=.8 N=136 N=171 N=339
27 Zone 2 STEMI Emergent Transfer Patients: By Intended Dose Neuro Complications (ICH, Total Stroke) 4 ns 3.5 ns ns % ICH Total Stroke None Given Full Dose Half Dose Lytic Dose Strategy
28 Zone 2 Transfer Patients n= Actual 3 day mortality (%) ns TIMI Score predicted 3 day mortality (%) 15 ns Years
29 Door-to to-balloon Times Non- transfers (PPCI) (min) Transfers Zone 1 Zone 2 No lytic (PPCI) (min) No Lytic (PPCI) (min) ½ Dose Lytic (min) Full Dose Lytic (min) DHMC ANW Not reported 12 - Mayo Not reported
30 3 day Mortality DHMC n=395 ANW N=1345 Mayo N=597 Non- transfers (PPCI) No lytic (PPCI) Transfers ½ Dose Lytic Full Dose Lytic Overall * * *Facilitated PCI Primary Ttx with rescue PCI if necessary Late presenters only Early presenters only
31 DHMC ED & Zone 1-1 PCI Patients Early and Late Door-to to-balloon Times vs : 3 Day Mortality (%) TIMI Risk Predicted 3 Day Mortality (%) Pre-Cath Shock or Intubation 2 ns ns hours >2 hours -2 hours >2 hours Door-to-Balloon Time -2 hours >2 hours
32 Zone 2 PCI Patients Door-to to-balloon Time 3 Day Mortality (%) TIMI Risk Predicted 3 Day Mortality (%) Pre-Cath Shock or Intubation ns hours hours >4 hours -2 hours 2-4 hours >4 hours Door-to-Balloon Time -2 hours 2-4 hours > 4 hours
33 Can we be satisfied No! In- house D2B times are too slow We can see a relationship between D2B time and 3 day outcome in our overall data Less than 2% of our patients are offered 1º 1 PCI ICH risk of ½ dose lytic protocol (1.5%- in our hands too high?) A STEMI Center Certification Program is in the works (Criteria for eligibility will likely be based on treatment times and volumes as well as quality outcomes) Pay-for for-performance reimbursement strategies are here or coming
34 STEP 1 - Get Organized ST Elevation MI Process Upgrade STEP UP Project Obtain commitment of DHMC Senior management Form a multidisciplinary group with members from Cardiology, Emergency medicine, EMS, Communications, CCU, Cardiac Cath Lab, DHMC administration and Quality management Identify/develop and implement strategies which improve the process of care, treatment times and outcomes of STEMI patients within our hospital and within our region
35 STEP UP Project: Goals 1. Implement proven strategies for reducing Doorto-balloon time to < 9 min in > 75% of STEMI patients 2. Design a STEMI pre-hospital triage network for the purpose of providing timely primary angioplasty to STEMI patients from an enlarged geographic area around DHMC 3. Critically assess our current inter-hospital transfer system including the current facilitated PCI program in order to identify process/protocol improvements
36 STEP 2 - Improve In-house D2B D2B: An Alliance for Quality Evidence-based Strategies for reducing Doorto-balloon time to < 9 min in > 75% of STEMI patients 1. ED physician activates the cath lab 2. One call activates the cath lab 3. Cath lab team ready in 2-3 minutes 4. Prompt data feedback 5. Team-based approach 6. Pre-hospital ECG to activate the cath lab*
37 STEMI Patients Presenting to DHMC ED QC Chart D2B Individual Measurements 21-28(Q3) 28(Q3) May 1 st
38 STEMI Patients Presenting to DHMC ED % D2B 9 min by Quarter 1 >75% 9 min Target! % 75 5 On line with D2B Strategies May 1 st st '1 2nd '1 3rd '1 4th '1 1st '2 2nd '2 3rd '2 4th '2 1st '3 2nd '3 3rd '3 4th '3 1st '4 2nd '4 3rd '4 4th '4 1st '5 2nd '5 3rd '5 4th '5 1st '6 2nd '6 3rd '6 4th '6 1st '7 2nd '7 3rd '7 4th '7 1st '8 2nd '8 3rd '8
39 STEP 3 Expanding EMS DHMC system Strategies EMS 12 lead ECG capability (Medtronic grant) EMS checklist to establish candidacy for 1º PCI and collect QI data Cath Lab activation based on ECG in the field (automated reading) Destination protocols for local ED bypass and transport directly to DHMC Cath Lab Goal = 35 miles up and down I91 and I89




40 STEP 4 Expanding Zone 1 Strategy Shorten in-door-out-door time at presenting hospital ECG within 1 minutes of arrival for all Suspected STEMI patients EMS transported patients remain on stretcher for ECG and transfer decision Doc, Nurse, Scribe Checklists to allow parallel workflow and QI data feedback system Zone 1 ED Physician activates cath lab if transport is immediately available. Response to interhospital STEMI transfer based on system rather than next available ambulance Goal = min. Zone 1 Option Zone 1

41

42

43
44 STEP 5 Rethink the Zone 2 Strategy Continue the Facilitated PCI option? Selected patients only? Change lytic regimen? Yes No Yes
45 The Pharmaco-invasive Option for Zone 2 Patients Alternative Regimens ½ dose Lytic plus GP 2b3a inhibitor plus low dose heparin infusion followed by PCI ASAP Pros Superior to Stand-alone lytic Tx in CARESS Trial Benefits early presenters We have good mortality track record Cons Increased bleeding/ich in our hands Not guideline compliant Complex and time consuming Full dose lytic and clopidogrel plus low dose heparin bolus followed by PCI ASAP Pros Superior to Stand-alone lytic Tx in TRANSFER AMI and CAPITAL AMI Trials Benefits early presenters Simpler / Quicker Cons More Bleeding / ICH risk

46 Questions?
The Window for Fibrinolysis. Frans Van de Werf, MD, PhD Leuven, Belgium
 The Window for Fibrinolysis Frans Van de Werf, MD, PhD Leuven, Belgium ESC STEMI Guidelines : December 2008 Reperfusion Therapy: Fibrinolytic Therapy Recommendations Class LOE In the absence of contraindications
The Window for Fibrinolysis Frans Van de Werf, MD, PhD Leuven, Belgium ESC STEMI Guidelines : December 2008 Reperfusion Therapy: Fibrinolytic Therapy Recommendations Class LOE In the absence of contraindications
Facilitated Percutaneous Coronary Intervention in Acute Myocardial Infarction. Is it beneficial to patients?
 Facilitated Percutaneous Coronary Intervention in Acute Myocardial Infarction Is it beneficial to patients? Seung-Jea Tahk, MD. PhD. Suwon, Korea Facilitated PCI.. background Degree of coronary flow at
Facilitated Percutaneous Coronary Intervention in Acute Myocardial Infarction Is it beneficial to patients? Seung-Jea Tahk, MD. PhD. Suwon, Korea Facilitated PCI.. background Degree of coronary flow at
NEBRASKA STEMI CONFERENCE 2015 Dr. Doug Kosmicki. 2013, American Heart Association
 NEBRASKA STEMI CONFERENCE 2015 Dr. Doug Kosmicki 2013, American Heart Association 1 Dr. Doug Kosmicki Reperfusion Strategies Disclosure Information Report any disclosure information of conflicts of interest.
NEBRASKA STEMI CONFERENCE 2015 Dr. Doug Kosmicki 2013, American Heart Association 1 Dr. Doug Kosmicki Reperfusion Strategies Disclosure Information Report any disclosure information of conflicts of interest.
Regional STEMI Transfer Systems: the Mayo and NC RACE Experiences
 Regional STEMI Transfer Systems: the Mayo and NC RACE Experiences Dr. Henry H. Ting, Mayo Clinic College of Medicine Dr. James G. Jollis,, Duke University Medical Center Mayo Clinic STEMI System for Transferred
Regional STEMI Transfer Systems: the Mayo and NC RACE Experiences Dr. Henry H. Ting, Mayo Clinic College of Medicine Dr. James G. Jollis,, Duke University Medical Center Mayo Clinic STEMI System for Transferred
Management of STEMI in era of Reperfusion. Eagles Peter Moyer, MD, MPH Medical Director Boston EMS, Fire and Police
 Management of STEMI in era of Reperfusion Eagles 2007 Peter Moyer, MD, MPH Medical Director Boston EMS, Fire and Police STEMI in US ST Segment Elevation Myocardial Infarction (STEMI) ~500 K per year Thrombolysis
Management of STEMI in era of Reperfusion Eagles 2007 Peter Moyer, MD, MPH Medical Director Boston EMS, Fire and Police STEMI in US ST Segment Elevation Myocardial Infarction (STEMI) ~500 K per year Thrombolysis
Current Advances and Best Practices in Acute STEMI Management A pharmacoinvasive approach
 Current Advances and Best Practices in Acute STEMI Management A pharmacoinvasive approach Frans Van de Werf, MD, PhD University Hospitals, Leuven, Belgium Frans Van de Werf: Disclosures Research grants
Current Advances and Best Practices in Acute STEMI Management A pharmacoinvasive approach Frans Van de Werf, MD, PhD University Hospitals, Leuven, Belgium Frans Van de Werf: Disclosures Research grants
Transfer in D2B. Scott D Friedman, MD FACC Medical Director, Cardiology Services Shore Health System of Maryland. The Problem
 Transfer in D2B Scott D Friedman, MD FACC Medical Director, Cardiology Services Shore Health System of Maryland The Problem NRMI-5: North Carolina, July 2003- June 2004 NC Nation Guidelines N 2,738 79,927
Transfer in D2B Scott D Friedman, MD FACC Medical Director, Cardiology Services Shore Health System of Maryland The Problem NRMI-5: North Carolina, July 2003- June 2004 NC Nation Guidelines N 2,738 79,927
Recommendations for criteria for STEMI systems of care: A focus on pharmacoinvasive strategies
 Recommendations for criteria for STEMI systems of care: A focus on pharmacoinvasive strategies Mohammad Zubaid, MB, ChB, FRCPC, FACC Professor of Medicine, Kuwait University Chairman, Faculty of Cardiology,
Recommendations for criteria for STEMI systems of care: A focus on pharmacoinvasive strategies Mohammad Zubaid, MB, ChB, FRCPC, FACC Professor of Medicine, Kuwait University Chairman, Faculty of Cardiology,
Controversies on Primary angioplasty in STEMI
 Controversies on Primary angioplasty in STEMI 원주의대이승환 Case ( 51/M) CC C.C: ongoing squeezing chest pain D : for 2 hours Risk factors Current smoker ( 40 PYs) Hypercholesterolemia (+) Case ( 51/M) Physical
Controversies on Primary angioplasty in STEMI 원주의대이승환 Case ( 51/M) CC C.C: ongoing squeezing chest pain D : for 2 hours Risk factors Current smoker ( 40 PYs) Hypercholesterolemia (+) Case ( 51/M) Physical
Mark C. Bieniarz, MD Andrew Harrell, MD Peter Berger, MD
 Mark C. Bieniarz, MD Andrew Harrell, MD Peter Berger, MD Should PCI center activate the cathlab off EMS field interpretation of ECG? Is this happening consistently in New Mexico? What is acceptable rate
Mark C. Bieniarz, MD Andrew Harrell, MD Peter Berger, MD Should PCI center activate the cathlab off EMS field interpretation of ECG? Is this happening consistently in New Mexico? What is acceptable rate
STREAM - ONE YEAR MORTALITY STRATEGIC REPERFUSION EARLY AFTER MYOCARDIAL INFARCTION. STREAM 1Y AHA 2013 P Sinnaeve
 STREAM - ONE YEAR MORTALITY STRATEGIC REPERFUSION EARLY AFTER MYOCARDIAL INFARCTION PCI Hospital Ambulance/ER STREAM design STEMI
STREAM - ONE YEAR MORTALITY STRATEGIC REPERFUSION EARLY AFTER MYOCARDIAL INFARCTION PCI Hospital Ambulance/ER STREAM design STEMI
REFERRAL HOSPITAL. The Importance of Door In Door Out Time DIDO
 REFERRAL HOSPITAL The Importance of Door In Door Out Time DIDO Jean Skonhovd,RN,BSN,MSAS Emergency Department Director Avera Heart Hospital of South Dakota Time to Treatment is critical for STEMI patients
REFERRAL HOSPITAL The Importance of Door In Door Out Time DIDO Jean Skonhovd,RN,BSN,MSAS Emergency Department Director Avera Heart Hospital of South Dakota Time to Treatment is critical for STEMI patients
Level One STEMI Connecting the Dots changing Points of Care into Systems of Care
 Level One STEMI Connecting the Dots changing Points of Care into Systems of Care Myron Bloom MD MMM Medical Director Rural Healthcare Quality Network RHQN.org drmbloom@msn.com The Eastern Washington Level
Level One STEMI Connecting the Dots changing Points of Care into Systems of Care Myron Bloom MD MMM Medical Director Rural Healthcare Quality Network RHQN.org drmbloom@msn.com The Eastern Washington Level
Pharmaco-Invasive Approach for STEMI
 Pharmaco-Invasive Approach for STEMI Michael C. Kontos, MD Medical Director, Coronary Intensive Care Unit Director, Chest Pain Evaluation Center Associate Professor Departments of Internal Medicine (Cardiology),
Pharmaco-Invasive Approach for STEMI Michael C. Kontos, MD Medical Director, Coronary Intensive Care Unit Director, Chest Pain Evaluation Center Associate Professor Departments of Internal Medicine (Cardiology),
Sanford Chest Pain Network: Improving Rural STEMI Outcomes
 Sanford Chest Pain Network: Improving Rural STEMI Outcomes Naveen Rajpurohit, MD Cardiovascular Fellow Sanford Cardiovascular Institute Sanford Heart Hospital The University of South Dakota Sioux Falls,
Sanford Chest Pain Network: Improving Rural STEMI Outcomes Naveen Rajpurohit, MD Cardiovascular Fellow Sanford Cardiovascular Institute Sanford Heart Hospital The University of South Dakota Sioux Falls,
Treatment of ST-elevation myocardial infarction in China: Where are we?
 Treatment of ST-elevation myocardial infarction in China: Where are we? Associate Professor, Yihong Sun, MD Peking University People s Hospital Beijing, China Disclosure conflict of Interest The Challenges
Treatment of ST-elevation myocardial infarction in China: Where are we? Associate Professor, Yihong Sun, MD Peking University People s Hospital Beijing, China Disclosure conflict of Interest The Challenges
Critics of Thrombolytics: Is Pre-Hospital Clot-busting Actually a Bad Thing? David Persse, MD Houston Fire Department EMS
 Critics of Thrombolytics: Is Pre-Hospital Clot-busting Actually a Bad Thing? David Persse, MD Houston Fire Department EMS STEMI Stuff New or Recurrent MI s in U.S.: 865,000 Acute STEMI s: 500,000 Sooner
Critics of Thrombolytics: Is Pre-Hospital Clot-busting Actually a Bad Thing? David Persse, MD Houston Fire Department EMS STEMI Stuff New or Recurrent MI s in U.S.: 865,000 Acute STEMI s: 500,000 Sooner
Myocardial Infarction In Dr.Yahya Kiwan
 Myocardial Infarction In 2007 Dr.Yahya Kiwan New Definition Of Acute Myocardial Infarction The term of myocardial infarction should be used when there is evidence of myocardial necrosis in a clinical setting
Myocardial Infarction In 2007 Dr.Yahya Kiwan New Definition Of Acute Myocardial Infarction The term of myocardial infarction should be used when there is evidence of myocardial necrosis in a clinical setting
PPCI in STEMI. ESC at the 22nd Annual Conference of the Saudi Heart Association February 21th, 2011
 PPCI in STEMI Dr Hassan Mhish Interventional Cardiology Consultant Cardiology Fellowship Program Director Prince Salman Heart Center King Fahd Medical City Riyadh, KSA ESC at the 22nd Annual Conference
PPCI in STEMI Dr Hassan Mhish Interventional Cardiology Consultant Cardiology Fellowship Program Director Prince Salman Heart Center King Fahd Medical City Riyadh, KSA ESC at the 22nd Annual Conference
ST-elevation myocardial infarctions (STEMIs)
") Guidelines for Treating STEMI: Case-Based Questions As many as 25% of eligible patients presenting with STEMI do not receive any form of reperfusion therapy. The ACC/AHA guidelines highlight steps to improve
Guidelines for Treating STEMI: Case-Based Questions As many as 25% of eligible patients presenting with STEMI do not receive any form of reperfusion therapy. The ACC/AHA guidelines highlight steps to improve
Patient and System Time Delay
 Quality Indicators in the Management of ST-elevation Myocardial Infarction Patient and System Time Delay Jacob Thorsted Sorensen, MD, PhD Department of Cardiology Aarhus University Hospital, Denmark Disclosures
Quality Indicators in the Management of ST-elevation Myocardial Infarction Patient and System Time Delay Jacob Thorsted Sorensen, MD, PhD Department of Cardiology Aarhus University Hospital, Denmark Disclosures
Mission: Lifeline Addressing the System of STEMI Care
 Mission: Lifeline Addressing the System of STEMI Care Alice K. Jacobs, M.D. Boston University Medical Center Boston, MA, USA ACC West Virginia Chapter, April 2017 Disclosure Information FINANCIAL DISCLOSURE:
Mission: Lifeline Addressing the System of STEMI Care Alice K. Jacobs, M.D. Boston University Medical Center Boston, MA, USA ACC West Virginia Chapter, April 2017 Disclosure Information FINANCIAL DISCLOSURE:
Management of Acute Myocardial Infarction
 Management of Acute Myocardial Infarction Prof. Hossam Kandil Professor of Cardiology Cairo University ST Elevation Acute Myocardial Infarction Aims Of Management Emergency care (Pre-hospital) Early care
Management of Acute Myocardial Infarction Prof. Hossam Kandil Professor of Cardiology Cairo University ST Elevation Acute Myocardial Infarction Aims Of Management Emergency care (Pre-hospital) Early care
Decision for fibrinolysis or primary PCI in the prehospital phase
 Decision for fibrinolysis or primary PCI in the prehospital phase Nicolas Danchin, Hôpital Européen Georges Pompidou, Paris, France Disclosures Research grants: Astrazeneca, Eli-Lilly, GSK, Merck, Novartis,
Decision for fibrinolysis or primary PCI in the prehospital phase Nicolas Danchin, Hôpital Européen Georges Pompidou, Paris, France Disclosures Research grants: Astrazeneca, Eli-Lilly, GSK, Merck, Novartis,
Dashboard and Outcomes Report with Case Studies
 Dashboard and Outcomes Report with Case Studies Kim Hustler Clinical Quality Consultant, American College of Cardiology The following relationships exist: Kim Hustler: No Disclosures Section F- Procedures
Dashboard and Outcomes Report with Case Studies Kim Hustler Clinical Quality Consultant, American College of Cardiology The following relationships exist: Kim Hustler: No Disclosures Section F- Procedures
Patient Transfer. Mark de Belder The James Cook University Hospital Middlesbrough
 Patient Transfer Mark de Belder The James Cook University Hospital Middlesbrough Current Management Strategies for ACS ACS No ST Elevation ST ST Elevation Elevation Early Invasive Early Conservative Fibrinolysis
Patient Transfer Mark de Belder The James Cook University Hospital Middlesbrough Current Management Strategies for ACS ACS No ST Elevation ST ST Elevation Elevation Early Invasive Early Conservative Fibrinolysis
William D. Salerno, M.D. Director, Coronary Care Unit Hackensack University Medical Center Clinical Associate Professor of Medicine, UMDNJ
 William D. Salerno, M.D. Director, Coronary Care Unit Hackensack University Medical Center Clinical Associate Professor of Medicine, UMDNJ PROBLEM: blood supply to the heart has been compromised and heart
William D. Salerno, M.D. Director, Coronary Care Unit Hackensack University Medical Center Clinical Associate Professor of Medicine, UMDNJ PROBLEM: blood supply to the heart has been compromised and heart
Acute Coronary Syndromes
 Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
2017 AHA/ACC Clinical Performance and Quality Measures for Adults With ST-Elevation and Non ST-Elevation Myocardial Infarction
 2017 AHA/ACC Clinical Performance and Quality Measures for Adults With ST-Elevation and Non ST-Elevation Myocardial Infarction Ramzi Khalil MD FACC Assistant Professor Allegheny Gen.Hospital AHN Speakers
2017 AHA/ACC Clinical Performance and Quality Measures for Adults With ST-Elevation and Non ST-Elevation Myocardial Infarction Ramzi Khalil MD FACC Assistant Professor Allegheny Gen.Hospital AHN Speakers
Presenters: Disclaimer. Definitions. Deanna Jones, RN, CCRN. Annmarie Keck, RN, CEN
 Presenters: Deanna Jones, RN, CCRN Cardiac Level 1 Coordinator, Providence Sacred Heart Medical Center and Children s Hospital, Spokane, WA Annmarie Keck, RN, CEN Clinical Outreach Educator Northwest MedStar,
Presenters: Deanna Jones, RN, CCRN Cardiac Level 1 Coordinator, Providence Sacred Heart Medical Center and Children s Hospital, Spokane, WA Annmarie Keck, RN, CEN Clinical Outreach Educator Northwest MedStar,
I have no financial relationships to disclose
 I have no financial relationships to disclose Networking decreases mortality Vasil Velchev,MD,PhD UH St. Anna Sofia time = myocardium = life Transfer for angioplasty vs. Immediate Thrombolysis (hospital
I have no financial relationships to disclose Networking decreases mortality Vasil Velchev,MD,PhD UH St. Anna Sofia time = myocardium = life Transfer for angioplasty vs. Immediate Thrombolysis (hospital
Daily practice of ACS management in the Gulf: Data from Gulf COAST
 Daily practice of ACS management in the Gulf: Data from Gulf COAST Mohammad Zubaid, MB, ChB, FRCPC, FACC Professor of Medicine, Kuwait University Head, Division of Cardiology Mubarak Alkabeer Hospital
Daily practice of ACS management in the Gulf: Data from Gulf COAST Mohammad Zubaid, MB, ChB, FRCPC, FACC Professor of Medicine, Kuwait University Head, Division of Cardiology Mubarak Alkabeer Hospital
Hot Topics in Cardiac Arrest. Should the patient go To the Cath Lab?
 Hot Topics in Cardiac Arrest Should the patient go To the Cath Lab? Tim Russert 1950-2008 Host of NBC s Meet the Press Sudden Cardiac Arrest : Autopsy showed plaque rupture in his LAD ( per LA Times,
Hot Topics in Cardiac Arrest Should the patient go To the Cath Lab? Tim Russert 1950-2008 Host of NBC s Meet the Press Sudden Cardiac Arrest : Autopsy showed plaque rupture in his LAD ( per LA Times,
1 a) Please confirm or deny whether your Trust has admitted patients for acute myocardial infarction in 2008/09, 2009/10 or 2010/11
 Please confirm or deny whether your Trust has admitted patients for acute myocardial infarction in 2008/09, 2009/10 or 2010/11") May 2011 1 a) Please confirm or deny whether your Trust has admitted patients for acute myocardial infarction in 2008/09, 2009/10 or 2010/11 Yes b) If confirmed please provide details on the number of
May 2011 1 a) Please confirm or deny whether your Trust has admitted patients for acute myocardial infarction in 2008/09, 2009/10 or 2010/11 Yes b) If confirmed please provide details on the number of
DISCUSSION QUESTION - 1
 CASE PRESENTATION 87 year old male No past history of diabetes, HTN, dyslipidemia or smoking Very active Medications: omeprazole for heart burn Admitted because of increasing retrosternal chest pressure
CASE PRESENTATION 87 year old male No past history of diabetes, HTN, dyslipidemia or smoking Very active Medications: omeprazole for heart burn Admitted because of increasing retrosternal chest pressure
Rural Minnesota STEMI Systems of Care
 CARDIOVASCULAR HEALTH UNIT Rural Minnesota STEMI Systems of Care Almost 250,000 Americans experience ST-elevation Myocardial Infarction (STEMI), the deadliest form of heart attack, each year. Of approximately
CARDIOVASCULAR HEALTH UNIT Rural Minnesota STEMI Systems of Care Almost 250,000 Americans experience ST-elevation Myocardial Infarction (STEMI), the deadliest form of heart attack, each year. Of approximately
STEMI update. Vijay Krishnamoorthy M.D. Interventional Cardiology
 STEMI update Vijay Krishnamoorthy M.D. Interventional Cardiology OVERVIEW Current Standard of Care in Management of STEMI Update in management of STEMI Pre-Cath Lab In the ED/Office/EMS. Cath Lab Post
STEMI update Vijay Krishnamoorthy M.D. Interventional Cardiology OVERVIEW Current Standard of Care in Management of STEMI Update in management of STEMI Pre-Cath Lab In the ED/Office/EMS. Cath Lab Post
SHOULD A REGIONAL STEMI CENTRE ONLY OFFER PRIMARY PCI?
 SHOULD A REGIONAL STEMI CENTRE ONLY OFFER PRIMARY PCI? Kurt Huber, MD 3 Department of Internal Medicine, Cardiology and Intensive Care Medicine, Wilhelminenhospital, Vienna, Austria Disclosures DISCLOSURE
SHOULD A REGIONAL STEMI CENTRE ONLY OFFER PRIMARY PCI? Kurt Huber, MD 3 Department of Internal Medicine, Cardiology and Intensive Care Medicine, Wilhelminenhospital, Vienna, Austria Disclosures DISCLOSURE
The Strategic Reperfusion Early After STEMI study Implications for clinical practice
 The Strategic Reperfusion Early After STEMI study Implications for clinical practice Robert C. Welsh, MD, FRCPC Associate Professor of Medicine Director, Adult Cardiac Catheterization and Interventional
The Strategic Reperfusion Early After STEMI study Implications for clinical practice Robert C. Welsh, MD, FRCPC Associate Professor of Medicine Director, Adult Cardiac Catheterization and Interventional
Thrombolysis in Cardiology to whom? Professor Steen D. Kristensen, MD, DMSc, FESC Department of Cardiology
 Thrombolysis in Cardiology to whom? Professor Steen D. Kristensen, MD, DMSc, FESC Department of Cardiology UNIVERSITY OF AARHUS 1 COI Speakers fee: Aspen, AZ, Bayer, BMS/Pfizer Departmental research grant:
Thrombolysis in Cardiology to whom? Professor Steen D. Kristensen, MD, DMSc, FESC Department of Cardiology UNIVERSITY OF AARHUS 1 COI Speakers fee: Aspen, AZ, Bayer, BMS/Pfizer Departmental research grant:
Continuing Medical Education Post-Test
 Continuing Medical Education Post-Test Based on the information presented in this monograph, please choose one correct response for each of the following questions or statements. Record your answers on
Continuing Medical Education Post-Test Based on the information presented in this monograph, please choose one correct response for each of the following questions or statements. Record your answers on
Improving STEMI outcomes in Denmark. Michael Rahbek Schmidt, MD, PhD. Aarhus University Hospital Skejby Denmark
 Improving STEMI outcomes in Denmark Michael Rahbek Schmidt, MD, PhD. Aarhus University Hospital Skejby Denmark Presenter Disclosure Information Study funded by Fondation Leducq Michael Rahbek Schmidt The
Improving STEMI outcomes in Denmark Michael Rahbek Schmidt, MD, PhD. Aarhus University Hospital Skejby Denmark Presenter Disclosure Information Study funded by Fondation Leducq Michael Rahbek Schmidt The
Acute Coronary Syndrome
 Acute Coronary Syndrome Clinical Manifestation of CAD Silent Ischemia/asymptomatic Stable Angina Acute Coronary Syndrome (Non- STEMI/UA and STEMI) Arrhythmias Heart Failure Sudden Death Pain patterns with
Acute Coronary Syndrome Clinical Manifestation of CAD Silent Ischemia/asymptomatic Stable Angina Acute Coronary Syndrome (Non- STEMI/UA and STEMI) Arrhythmias Heart Failure Sudden Death Pain patterns with
The role of pre hospital thrombolysis. Aaron Frimerman Hillel Yaffe Medical Center Hadera Israel
 The role of pre hospital thrombolysis Aaron Frimerman Hillel Yaffe Medical Center Hadera Israel Is thrombolysis still valid? Disclosure I am an Interventional Cardiologist STEMI is mainly a thrombotic
The role of pre hospital thrombolysis Aaron Frimerman Hillel Yaffe Medical Center Hadera Israel Is thrombolysis still valid? Disclosure I am an Interventional Cardiologist STEMI is mainly a thrombotic
Disclosure Information
 Disclosure Information Speaker: G Simkus Title: Cardiac Sciences Program Medical Director Fraser Health AFFILIATION/FINANCIAL INTEREST DISCLOSURE Grants/Research Support: Grants/Research Support: Speakers
Disclosure Information Speaker: G Simkus Title: Cardiac Sciences Program Medical Director Fraser Health AFFILIATION/FINANCIAL INTEREST DISCLOSURE Grants/Research Support: Grants/Research Support: Speakers
Improving the Outcomes of
 Improving the Outcomes of STEMI Shelley Valaire, ACP; and Robert Welsh, MD, FRCPC Presented at the University of Alberta s 6th Annual Cardiology Update for General Practitioners and Internists, Edmonton,
Improving the Outcomes of STEMI Shelley Valaire, ACP; and Robert Welsh, MD, FRCPC Presented at the University of Alberta s 6th Annual Cardiology Update for General Practitioners and Internists, Edmonton,
ST Elevated Myocardial Infarction- Latest AHA recommendations
 ST Elevated Myocardial Infarction- Latest AHA recommendations Sherry Turner, DO, MPH, FACOEP Medical Director Emergency Services Wesley Medical Center The Problem 250,000 Americans each year 30% fail to
ST Elevated Myocardial Infarction- Latest AHA recommendations Sherry Turner, DO, MPH, FACOEP Medical Director Emergency Services Wesley Medical Center The Problem 250,000 Americans each year 30% fail to
Facilitated Percutaneous Coronary Intervention in STEMI Patients: Does It Work in Asian Patients?
 Editorial Comment Acta Cardiol Sin 2014;30:292 297 Facilitated Percutaneous Coronary Intervention in STEMI Patients: Does It Work in Asian Patients? Wei-Chun Huang, 1,2,3 Cheng-Hung Chiang 1,2 and Chun-Peng
Editorial Comment Acta Cardiol Sin 2014;30:292 297 Facilitated Percutaneous Coronary Intervention in STEMI Patients: Does It Work in Asian Patients? Wei-Chun Huang, 1,2,3 Cheng-Hung Chiang 1,2 and Chun-Peng
Update Guidelines in STEMI Management: Focus on Logistic and System Approach to Reperfusion Therapy
 March 14 th, 2018 The First Asia Forum in Emergency Medicine BNH Hospital, Bangkok, Thailand Update Guidelines in STEMI Management: Focus on Logistic and System Approach to Reperfusion Therapy Wacin Buddhari,
March 14 th, 2018 The First Asia Forum in Emergency Medicine BNH Hospital, Bangkok, Thailand Update Guidelines in STEMI Management: Focus on Logistic and System Approach to Reperfusion Therapy Wacin Buddhari,
The Burden & Management of Ischaemic Heart Disease in Kenya
 The Burden & Management of Ischaemic Heart Disease in Kenya Dr Harun A Otieno FACC Tuesday, October 6th: Session X PASCAR & CSM Joint Congress 2015, Mauritius Disclosures With regards to this presentation,
The Burden & Management of Ischaemic Heart Disease in Kenya Dr Harun A Otieno FACC Tuesday, October 6th: Session X PASCAR & CSM Joint Congress 2015, Mauritius Disclosures With regards to this presentation,
ACTION Registry GWTG Research and Publications Update
 ACTION Registry GWTG Research and Publications Update Dr. Michael Kontos Director, Coronary Intensive Care Unit Pauley Heart Center, Virginia Commonwealth University The following relationships exist:
ACTION Registry GWTG Research and Publications Update Dr. Michael Kontos Director, Coronary Intensive Care Unit Pauley Heart Center, Virginia Commonwealth University The following relationships exist:
STEMI 2014 YAHYA KIWAN. Consultant Cardiologist Head Of Cardiology Belhoul Specialty Hospital
 STEMI 2014 YAHYA KIWAN Consultant Cardiologist Head Of Cardiology Belhoul Specialty Hospital Aspiration Thrombectomy Manual aspiration thrombectomy is reasonable for patients undergoing primary PCI. I
STEMI 2014 YAHYA KIWAN Consultant Cardiologist Head Of Cardiology Belhoul Specialty Hospital Aspiration Thrombectomy Manual aspiration thrombectomy is reasonable for patients undergoing primary PCI. I
Chapter 3 for 12 Lead Training -Precourse-
 ONTARIO BASE HOSPITAL GROUP Chapter 3 for 12 Lead Training -Precourse- Ontario Base Hospital Group Education Subcommittee 2008 TIME IS MUSCLE ONTARIO BASE HOSPITAL GROUP Introduction and Purpose Introduction
ONTARIO BASE HOSPITAL GROUP Chapter 3 for 12 Lead Training -Precourse- Ontario Base Hospital Group Education Subcommittee 2008 TIME IS MUSCLE ONTARIO BASE HOSPITAL GROUP Introduction and Purpose Introduction
Critical Review Form Therapy Objectives: Methods:
 Critical Review Form Therapy Clinical Trial Comparing Primary Coronary Angioplasty with Tissue-Plasminogen Activator for Acute Myocardial Infarction (GUSTO-IIb), NEJM 1997; 336: 1621-1628 Objectives: To
Critical Review Form Therapy Clinical Trial Comparing Primary Coronary Angioplasty with Tissue-Plasminogen Activator for Acute Myocardial Infarction (GUSTO-IIb), NEJM 1997; 336: 1621-1628 Objectives: To
The restoration of coronary flow after an
 Pharmacological Reperfusion in Acute Myicardial Infarction after ASSENT 3 and GUSTO V [81] DANIEL FERREIRA, MD, FESC Serviço de Cardiologia, Hospital Fernando Fonseca, Amadora, Portugal Rev Port Cardiol
Pharmacological Reperfusion in Acute Myicardial Infarction after ASSENT 3 and GUSTO V [81] DANIEL FERREIRA, MD, FESC Serviço de Cardiologia, Hospital Fernando Fonseca, Amadora, Portugal Rev Port Cardiol
Baseline Data Collection Tool
 Endorsed by the Vanderbilt Department of Emergency Medicine Research Partner of the ED Benchmarking Alliance Baseline Data Collection Tool The data collected via this form is the baseline member data for
Endorsed by the Vanderbilt Department of Emergency Medicine Research Partner of the ED Benchmarking Alliance Baseline Data Collection Tool The data collected via this form is the baseline member data for
Effect of upstream clopidogrel treatment in patients with ST-segment elevation myocardial infarction undergoing primary PCI
 Effect of upstream clopidogrel treatment in patients with ST-segment elevation myocardial infarction undergoing primary PCI Dr Sasha Koul, MD Dept of Cardiology, Lund University Hospital, Lund, Sweden
Effect of upstream clopidogrel treatment in patients with ST-segment elevation myocardial infarction undergoing primary PCI Dr Sasha Koul, MD Dept of Cardiology, Lund University Hospital, Lund, Sweden
TAB 7: SUB TAB: AMI/CHEST PAIN Specifications & Paper Tools
 TAB 7: SUB TAB: AMI/CHEST PAIN Specifications & Paper Tools Material inside brackets ([and]) is new to this Specifications Manual version. Hospital Outpatient Quality Measures Acute Myocardial Infarction
TAB 7: SUB TAB: AMI/CHEST PAIN Specifications & Paper Tools Material inside brackets ([and]) is new to this Specifications Manual version. Hospital Outpatient Quality Measures Acute Myocardial Infarction
Cardiology Department. Clinical Governance
 Cardiology Department Clinical Governance Background Cardiology department has a high throughput of emergency and elective patients Two acute sites CAH and DHH Cardiac investigation department provides
Cardiology Department Clinical Governance Background Cardiology department has a high throughput of emergency and elective patients Two acute sites CAH and DHH Cardiac investigation department provides
12/18/2009 Resting and Maxi Resting and Max mal Coronary Blood Flow 2
 Coronary Artery Pathophysiology ACS / AMI LeRoy E. Rabbani, MD Director, Cardiac Inpatient Services Director, Cardiac Intensive Care Unit Professor of Clinical Medicine Major Determinants of Myocardial
Coronary Artery Pathophysiology ACS / AMI LeRoy E. Rabbani, MD Director, Cardiac Inpatient Services Director, Cardiac Intensive Care Unit Professor of Clinical Medicine Major Determinants of Myocardial
Primary Percutaneous Coronary Intervention
 The big 5 in PCI Primary Percutaneous Coronary Intervention W. Wijns (Aalst, BE) Disclosures Consulting Fees: on my behalf go to the Cardiovascular Research Center Aalst Contracted Research between the
The big 5 in PCI Primary Percutaneous Coronary Intervention W. Wijns (Aalst, BE) Disclosures Consulting Fees: on my behalf go to the Cardiovascular Research Center Aalst Contracted Research between the
Door to Balloon : The Big Deal. Shaiful Azmi Yahaya,, M.D. Consultant Cardiologist Institut Jantung Negara
 Door to Balloon : The Big Deal Shaiful Azmi Yahaya,, M.D. Consultant Cardiologist Institut Jantung Negara Lecture Outline Pathophysiology of ACS History Door to balloon -? The big deal Myocardial ischaemia
Door to Balloon : The Big Deal Shaiful Azmi Yahaya,, M.D. Consultant Cardiologist Institut Jantung Negara Lecture Outline Pathophysiology of ACS History Door to balloon -? The big deal Myocardial ischaemia
Thrombolysis in Acute Myocardial Infarction
 CHAPTER 70 Thrombolysis in Acute Myocardial Infarction J. S. Hiremath Introduction Reperfusion of the occluded coronary artery at the earliest is the most important aim of management of STEMI. Once a flow
CHAPTER 70 Thrombolysis in Acute Myocardial Infarction J. S. Hiremath Introduction Reperfusion of the occluded coronary artery at the earliest is the most important aim of management of STEMI. Once a flow
Frans Van de Werf, MD, PhD Leuven, Belgium
 STEMI Cases and the ESC STEMI Guidelines Frans Van de Werf, MD, PhD Leuven, Belgium The Easy Case 2/21/2011 History and Risk Factors 50-year old male patient Past medical history: Teratoma right testis
STEMI Cases and the ESC STEMI Guidelines Frans Van de Werf, MD, PhD Leuven, Belgium The Easy Case 2/21/2011 History and Risk Factors 50-year old male patient Past medical history: Teratoma right testis
PHARMACO-INVASIVE STRATEGY COMPARED WITH PPCI: DESIGN AND MAIN OUTCOMES OF THE STREAM TRIAL
 PHARMACO-INVASIVE STRATEGY COMPARED WITH PPCI: DESIGN AND MAIN OUTCOMES OF THE STREAM TRIAL Frans Van de Werf Leuven, Belgium Disclosures Study grant from Boehringer Ingelheim to perform the STREAM trial,
PHARMACO-INVASIVE STRATEGY COMPARED WITH PPCI: DESIGN AND MAIN OUTCOMES OF THE STREAM TRIAL Frans Van de Werf Leuven, Belgium Disclosures Study grant from Boehringer Ingelheim to perform the STREAM trial,
Identification and pre-notification using 12-Lead. Why this so important to our STEMI System
 Identification and pre-notification using 12-Lead Why this so important to our STEMI System Jim Smith, MD Great Plains Health, North Platte Chair, NE State EMS Board Medical Director, Emergency Services,
Identification and pre-notification using 12-Lead Why this so important to our STEMI System Jim Smith, MD Great Plains Health, North Platte Chair, NE State EMS Board Medical Director, Emergency Services,
Eagles 2007 Focused Quality in EMS The Five Required Actions
 Eagles 2007 Focused Quality in EMS The Five Required Actions Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Prior
Eagles 2007 Focused Quality in EMS The Five Required Actions Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Prior
STEMI Presentation and Case Discussion. Case #1
 STEMI Presentation and Case Discussion Scott M Lilly MD PhD, Interventional Cardiology The Ohio State University Contemporary Multidisciplinary Cardiovascular Conference Orlando, Florida September 17 th,
STEMI Presentation and Case Discussion Scott M Lilly MD PhD, Interventional Cardiology The Ohio State University Contemporary Multidisciplinary Cardiovascular Conference Orlando, Florida September 17 th,
STEMI, Non-STEMI, Chest Pain?
 Minnesota Chest Pain / Acute Coronary Syndrome Tool-Kit Patient with Chest Pain Or Potential Acute Coronary Syndrome STEMI, n-stemi, Chest Pain? Follow MN STEMI Guideline Follow MN n-stemi Guideline Follow
Minnesota Chest Pain / Acute Coronary Syndrome Tool-Kit Patient with Chest Pain Or Potential Acute Coronary Syndrome STEMI, n-stemi, Chest Pain? Follow MN STEMI Guideline Follow MN n-stemi Guideline Follow
Know the Quality of our Care at Every Step. Kansas City ACS Summit BI-State Cardiovascular Education Consortium
 Know the Quality of our Care at Every Step Kansas City ACS Summit BI-State Cardiovascular Education Consortium Welcome to the Kansas City ACS Summit Objectives: Follow the flow and care of an ACS patient
Know the Quality of our Care at Every Step Kansas City ACS Summit BI-State Cardiovascular Education Consortium Welcome to the Kansas City ACS Summit Objectives: Follow the flow and care of an ACS patient
2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction
 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction Developed in Collaboration with American College of Emergency Physicians and Society for Cardiovascular Angiography and
2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction Developed in Collaboration with American College of Emergency Physicians and Society for Cardiovascular Angiography and
presenters 2010 Sameh Sabet Ain Shams University
 Guidelines for PCI in late STEMI presenters 2010 Sameh Sabet Assistant Professor of Cardiology Ain Shams University 29% of MI patients have STEMI. NRMI 4 (Fourth National Registry of Myocardial Infarction),
Guidelines for PCI in late STEMI presenters 2010 Sameh Sabet Assistant Professor of Cardiology Ain Shams University 29% of MI patients have STEMI. NRMI 4 (Fourth National Registry of Myocardial Infarction),
Guideline for STEMI. Reperfusion at a PCI-Capable Hospital
 MANSOURA. 2015 Guideline for STEMI Reperfusion at a PCI-Capable Hospital Mahmoud Yossof MANSOURA 2015 Reperfusion Therapy for Patients with STEMI *Patients with cardiogenic shock or severe heart failure
MANSOURA. 2015 Guideline for STEMI Reperfusion at a PCI-Capable Hospital Mahmoud Yossof MANSOURA 2015 Reperfusion Therapy for Patients with STEMI *Patients with cardiogenic shock or severe heart failure
4. Which survey program does your facility use to get your program designated by the state?
 STEMI SURVEY Please complete one survey for each TCD designation you have in your facility. There would be a maximum of three surveys completed if your facility was designated as a trauma, stroke and STEMI
STEMI SURVEY Please complete one survey for each TCD designation you have in your facility. There would be a maximum of three surveys completed if your facility was designated as a trauma, stroke and STEMI
STEMI Care 2014 at the Crossroads: Taking the right road
 STEMI Care 2014 at the Crossroads: Taking the right road Robert C. Welsh, MD, FRCPC, FESC, FAHA, FACC Professor of Medicine Vice President, The Canadian Association of Interventional Cardiology Director,
STEMI Care 2014 at the Crossroads: Taking the right road Robert C. Welsh, MD, FRCPC, FESC, FAHA, FACC Professor of Medicine Vice President, The Canadian Association of Interventional Cardiology Director,
Earlier reperfusion in patients with ST-elevation Myocardial infarction by use of helicopter
 Knudsen et al. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine 2012, 20:70 ORIGINAL RESEARCH Open Access Earlier reperfusion in patients with ST-elevation Myocardial infarction by
Knudsen et al. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine 2012, 20:70 ORIGINAL RESEARCH Open Access Earlier reperfusion in patients with ST-elevation Myocardial infarction by
Washington s Emergency Cardiac and Stroke System. Kathleen Jobe, MD FACEP Chair, Emergency Cardiac and Stroke Technical Advisory Committee
 Washington s Emergency Cardiac and Stroke System Kathleen Jobe, MD FACEP Chair, Emergency Cardiac and Stroke Technical Advisory Committee Emergency Cardiac and Stroke Care in Washington Problem: Effective
Washington s Emergency Cardiac and Stroke System Kathleen Jobe, MD FACEP Chair, Emergency Cardiac and Stroke Technical Advisory Committee Emergency Cardiac and Stroke Care in Washington Problem: Effective
ACUTE CORONARY SYNDROME PCI IN THE ELDERLY
 ACUTE CORONARY SYNDROME PCI IN THE ELDERLY G.KARABELA MD.PhD ATHENS NAVAL HOSPITAL INTERVENTIONAL CARDIOLOGY DEPARTMENT NO CONFLICT OF INTEREST TO DECLAIRE Risk stratification in Αcute Coronary Syndrome.
ACUTE CORONARY SYNDROME PCI IN THE ELDERLY G.KARABELA MD.PhD ATHENS NAVAL HOSPITAL INTERVENTIONAL CARDIOLOGY DEPARTMENT NO CONFLICT OF INTEREST TO DECLAIRE Risk stratification in Αcute Coronary Syndrome.
Trauma Service Area - B (BRAC) Regional Cardiac Plan
 Regional Cardiac Plan") Trauma Service Area - B (BRAC) Regional Cardiac Plan Trauma Service Area- B (BRAC) P.O. Box 53597 Lubbock, Texas 79453 806.791.2582 (office) BRAC serves the counties of Bailey, Borden, Castro, Cochran,
Trauma Service Area - B (BRAC) Regional Cardiac Plan Trauma Service Area- B (BRAC) P.O. Box 53597 Lubbock, Texas 79453 806.791.2582 (office) BRAC serves the counties of Bailey, Borden, Castro, Cochran,
This clinical study synopsis is provided in line with Boehringer Ingelheim s Policy on Transparency and Publication of Clinical Study Data.
 abcd Clinical Study Synopsis for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the
abcd Clinical Study Synopsis for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the
STEMI Linee guida ESC Maddalena Lettino, Italy
 STEMI Linee guida ESC 2017 Maddalena Lettino, Italy Disclosure Speaker fee: Aspen, Astra Zeneca, BMS, Boehringer, Eli Lilly, DaichiiSankio, Bayer, Pfizer, Sanofi Advisory board member: Astra Zeneca, Eli
STEMI Linee guida ESC 2017 Maddalena Lettino, Italy Disclosure Speaker fee: Aspen, Astra Zeneca, BMS, Boehringer, Eli Lilly, DaichiiSankio, Bayer, Pfizer, Sanofi Advisory board member: Astra Zeneca, Eli
Literature Review and Recommendations Prehospital Fibrinolytics Administration for Acute Myocardial Infarction
 Literature Review and Recommendations Prehospital Fibrinolytics Administration for Acute Myocardial Infarction EMS Bureau Protocol Review Steering Committee Background In 2009, approximately 683,000 Americans
Literature Review and Recommendations Prehospital Fibrinolytics Administration for Acute Myocardial Infarction EMS Bureau Protocol Review Steering Committee Background In 2009, approximately 683,000 Americans
ST-SEGMENT ELEVATION MYOCARDIAL INFARCTION (STEMI): DECREASING THE TIME TO TREATMENT IN THE ED
: DECREASING THE TIME TO TREATMENT IN THE ED") ST-SEGMENT ELEVATION MYOCARDIAL INFARCTION (STEMI): DECREASING THE TIME TO TREATMENT IN THE ED W. Brian Gibler, MD Professor and Chairman; Department of Emergency Medicine, University of Cincinnati College
ST-SEGMENT ELEVATION MYOCARDIAL INFARCTION (STEMI): DECREASING THE TIME TO TREATMENT IN THE ED W. Brian Gibler, MD Professor and Chairman; Department of Emergency Medicine, University of Cincinnati College
Acute Coronary Syndrome (ACS) is the consequence of
 is the consequence of") Clinical Practice Pharmaco-invasive Therapy for STEMI; The Most Suitable STEMI Reperfusion Therapy for Transferred Patients in Thailand Pradub Sukhum, MD. 1 1 Division of Cardiovascular Medicine, Bangkok
Clinical Practice Pharmaco-invasive Therapy for STEMI; The Most Suitable STEMI Reperfusion Therapy for Transferred Patients in Thailand Pradub Sukhum, MD. 1 1 Division of Cardiovascular Medicine, Bangkok
Management of ST-elevation myocardial infarction Update 2009 Late comers: which options?
 European Society of Cardiology Annual Session 2009 Management of ST-elevation myocardial infarction Update 2009 Late comers: which options? Antonio Abbate, MD Assistant Professor of Medicine Virginia Commonwealth
European Society of Cardiology Annual Session 2009 Management of ST-elevation myocardial infarction Update 2009 Late comers: which options? Antonio Abbate, MD Assistant Professor of Medicine Virginia Commonwealth
New Insights on Reperfusion Choices Implications of STREAM. Paul W Armstrong MD
 New Insights on Reperfusion Choices Implications of STREAM ESC STEMI Satellite Symposium August 31 2014 Aligning Optimal Care to Time Place and Person Paul W Armstrong MD Disclosure Statement Paul W. Armstrong
New Insights on Reperfusion Choices Implications of STREAM ESC STEMI Satellite Symposium August 31 2014 Aligning Optimal Care to Time Place and Person Paul W Armstrong MD Disclosure Statement Paul W. Armstrong
Prasugrel vs. Ticagrelor in ACS/PCI Which one to choose? V. Voudris MD FESC FACC 2 nd Cardiology Division Onassis Cardiac Surgery Center
 Prasugrel vs. Ticagrelor in ACS/PCI Which one to choose? V. Voudris MD FESC FACC 2 nd Cardiology Division Onassis Cardiac Surgery Center Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes
Prasugrel vs. Ticagrelor in ACS/PCI Which one to choose? V. Voudris MD FESC FACC 2 nd Cardiology Division Onassis Cardiac Surgery Center Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes
Acute Coronary Syndrome: Interventional Strategy
 2005 Acute Coronary Syndrome: Interventional Strategy Youngkeun Ahn, MD, PhD, FACC, FSCAI Department of Cardiology Program in Gene and Cell Therapy, The Heart Center of Chonnam National University, GwangJu,,
2005 Acute Coronary Syndrome: Interventional Strategy Youngkeun Ahn, MD, PhD, FACC, FSCAI Department of Cardiology Program in Gene and Cell Therapy, The Heart Center of Chonnam National University, GwangJu,,
Optimal System Specification by Point of Care Operations Manual
 Optimal System Specification by Point of Care Operations Manual The Steering Committee of the Reperfusion of Acute Myocardial Infarction in Carolina Emergency Departments (RACE) Project Version 2.1 April
Optimal System Specification by Point of Care Operations Manual The Steering Committee of the Reperfusion of Acute Myocardial Infarction in Carolina Emergency Departments (RACE) Project Version 2.1 April
Thrombus Aspiration before PCI: Routine Mandatory. Professor Clinical Cardiology Academic Medical Center University of Amsterdam
 Seoul, 27 April TCT AP 2010 Thrombus Aspiration before PCI: Routine Mandatory Robbert J de Winter MD PhD FESC Professor Clinical Cardiology Academic Medical Center University of Amsterdam AMC Amsterdam
Seoul, 27 April TCT AP 2010 Thrombus Aspiration before PCI: Routine Mandatory Robbert J de Winter MD PhD FESC Professor Clinical Cardiology Academic Medical Center University of Amsterdam AMC Amsterdam
The Evolving ACC-NCDR Programs: What you need to know for your practice
 The Evolving ACC-NCDR Programs: What you need to know for your practice John S. Rumsfeld, MD PhD FACC Chief Science Officer and Chair, American College of Cardiology National Cardiovascular Data Registry
The Evolving ACC-NCDR Programs: What you need to know for your practice John S. Rumsfeld, MD PhD FACC Chief Science Officer and Chair, American College of Cardiology National Cardiovascular Data Registry
Prof. Adel El Etriby Ain Shams Faculty of Medicine
 Prof. Adel El Etriby Ain Shams Faculty of Medicine Reperfusion Options for STEMI Patients Step One: Assess Time and Risk. Time Since Symptom Onset Risk of STEMI Risk of Fibrinolysisi i Time Required for
Prof. Adel El Etriby Ain Shams Faculty of Medicine Reperfusion Options for STEMI Patients Step One: Assess Time and Risk. Time Since Symptom Onset Risk of STEMI Risk of Fibrinolysisi i Time Required for
STEMI in the State of Jefferson ASSET - 5 Years Later. Brian W. Gross, MD, FACC Mary Barnum, RN, BSN Karen Bales, RN, BSN Rogue Valley Medical Center
 STEMI in the State of Jefferson ASSET - 5 Years Later Brian W. Gross, MD, FACC Mary Barnum, RN, BSN Karen Bales, RN, BSN Rogue Valley Medical Center Sept 22, 2008 Percent # Procedures Performed Coronary
STEMI in the State of Jefferson ASSET - 5 Years Later Brian W. Gross, MD, FACC Mary Barnum, RN, BSN Karen Bales, RN, BSN Rogue Valley Medical Center Sept 22, 2008 Percent # Procedures Performed Coronary
Systems of Care to Improve Timeliness of Reperfusion Therapy for ST-Segment Elevation Myocardial Infarction During Off Hours
 JACC: CARDIOVASCULAR INTERVENTIONS VOL. 1, NO. 1, 2008 2008 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 1936-8798/08/$34.00 PUBLISHED BY ELSEVIER DOI: 10.1016/j.jcin.2007.10.002 Systems of Care
JACC: CARDIOVASCULAR INTERVENTIONS VOL. 1, NO. 1, 2008 2008 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 1936-8798/08/$34.00 PUBLISHED BY ELSEVIER DOI: 10.1016/j.jcin.2007.10.002 Systems of Care
Cover Page. The handle holds various files of this Leiden University dissertation
 Cover Page The handle http://hdl.handle.net/1887/21543 holds various files of this Leiden University dissertation Author: Dharma, Surya Title: Perspectives in the treatment of cardiovascular disease :
Cover Page The handle http://hdl.handle.net/1887/21543 holds various files of this Leiden University dissertation Author: Dharma, Surya Title: Perspectives in the treatment of cardiovascular disease :
Policy Register No: Status: Public. Contributes to Care Quality Commission Outcome 4
 Operational Policy for Transfer of ST Elevation MI (STEMI) patients to Essex Cardiothoracic Centre (ECTC) for Primary Percutaneous Coronary Intervention Policy Register No: 09122 Status: Public Developed
Operational Policy for Transfer of ST Elevation MI (STEMI) patients to Essex Cardiothoracic Centre (ECTC) for Primary Percutaneous Coronary Intervention Policy Register No: 09122 Status: Public Developed
A Report From the Second National Registry of Myocardial Infarction (NRMI-2)
") 1240 JACC Vol. 31, No. 6 Clinical Experience With Primary Percutaneous Transluminal Coronary Angioplasty Compared With Alteplase (Recombinant Tissue-Type Plasminogen Activator) in Patients With Acute Myocardial
1240 JACC Vol. 31, No. 6 Clinical Experience With Primary Percutaneous Transluminal Coronary Angioplasty Compared With Alteplase (Recombinant Tissue-Type Plasminogen Activator) in Patients With Acute Myocardial
ACC/AHA Guidelines for the Management of Patients With ST-Elevation Acute Myocardial Infarction- Focus Emergency Care
 ACC/AHA Guidelines for the Management of Patients With ST-Elevation Acute Myocardial Infarction- Focus Emergency Care A Report of the American College of Cardiology/American Heart Association Task Force
ACC/AHA Guidelines for the Management of Patients With ST-Elevation Acute Myocardial Infarction- Focus Emergency Care A Report of the American College of Cardiology/American Heart Association Task Force
Update on the management of STEMI. Elliot Rapaport, M.D. San Francisco, CA December 14, 2007
 Update on the management of STEMI Elliot Rapaport, M.D. San Francisco, CA December 14, 2007 Universal MI Definition Committee 2007 Recommendations Type 1 Spontaneous MI associated with ischemia and due
Update on the management of STEMI Elliot Rapaport, M.D. San Francisco, CA December 14, 2007 Universal MI Definition Committee 2007 Recommendations Type 1 Spontaneous MI associated with ischemia and due
KPNC Stroke EXPRESS EXpediting the PRocess of Evaluating & Stopping Stroke
 KPNC Stroke EXPRESS EXpediting the PRocess of Evaluating & Stopping Stroke Jeffrey G. Klingman, MD 1 Disclosures None 75% DTN < 60 50% DTN < 45 Why should we care about DTN?: Time is brain 2 million nerve
KPNC Stroke EXPRESS EXpediting the PRocess of Evaluating & Stopping Stroke Jeffrey G. Klingman, MD 1 Disclosures None 75% DTN < 60 50% DTN < 45 Why should we care about DTN?: Time is brain 2 million nerve