Heart failure: Local solutions for a growing problem
|
|
|
- Silvia Matthews
- 5 years ago
- Views:
Transcription
1 Heart failure: Local solutions for a growing problem Dr Andrew Hannah Consultant Cardiologist ARI
2 What is heart failure? A clinical syndrome comprising of dyspnoea, fatigue or fluid retention due to cardiac dysfunction, either at rest or on exertion, with accompanying neurohormonal activation. Braunwald E. heart failure is NOT a final diagnosis and the term should be qualified by the underlying structural abnormality and cause heart failure due to severe aortic stenosis heart failure due to LV systolic dysfunction... due to IHD or due to inherited dilated cardiomyopathy etc etc
3 The size of the problem Prevalence of heart failure 1 2% of adult population and asymptomatic LVSD 0.4 2% Prevalence and incidence increase with age mean age of HF patient 74years prevalence approx. 8 10% in over 75s have heart failure Approximately cases in Scotland or 8000 in Grampian prevalence and incidence are increasing ageing pop, better survival post MI/CHF

4
5 Projected HF prevalence in Scotland
6 Prognosis: Heart Failure vs Cancer Mortality Pancreas Lung Oesophagus Stomach Leukaemia Kidney Ovarian Heart failure Colon NHL Prostate Bladder Uterus Breast Melanoma One year survival rate (%) The one-year survival rate for heart failure is worse than that for cancer of the breast, uterus, prostate & bladder Coronary heart disease statistics: heart failure supplement., BHF 2002, accessed Based on Quinn M et al. ONS 2001 & Cowie MR et al. Heart 2000; 83: NHL= Non-Hodgkins lymphoma
7 Heart failure: What are we trying to achieve? Improved quality and length of life for patients Reduced hospitalisations and re admissions
8 How might we achieve this? Make an accurate diagnosis in a timely fashion Perform appropriate investigations: to determine aetiology and prognosis Education: patients, relatives and healthcare professionals Evidence based drug therapy for all Appropriate selection for device therapy (CRT / ICD) or surgery or cardiac transplantation



9 Heart failure can be easy to diagnose
10 .but usually it is difficult to diagnose on clinical grounds alone Studies show diagnosis incorrect in approx % of cases * Chest crepitations, oedema, tachycardia not specific S3, JVP, displaced apex insensitive, poor inter observer agreement Many patients have symptoms only dyspnoea, fatigue are non specific Therefore objective evidence of cardiac dysfunction mandatory...usually by echo initially But we cannot cope with the volume of echo referrals 600/month at ARI alone *Wheeldon et al QJMed 1993:86:17 24
11 Are screening tests the answer? 12 Lead ECG LVSD unlikely if ECG normal (85 90% sensitive) Problems with confidence of interpretation in primary care, must be entirely normal or else loses reliability. Low specificity May be normal in other causes of HF BNP (brain (B type) natriuretic peptide) Simple blood test no subjective interpretation difficulties (cw ECG) LVSD virtually excluded if normal / low Much better specificity than the ECG Real world cost approx. 20 per test
12 Grampian BNP pilot NT pro BNP: more stable than BNP with equally good evidence base Different (higher) normal range Pilot commencing in Grampian Dec 2011 linking the test with the open access echo service Future funding will be dependent on proving cost effectiveness and /or improved patient care
13
14 LV systolic dysfunction: not a final diagnosis IHD related LVSD: infarcted, stunned, hibernating?? Dilated cardiomyopathy (LVSD with normal coronary arteries) Inherited: dilated, hypertrophic, ARVC, isolated non compaction Toxins: drugs, alcohol, Infections: prior and acute Immune mediated: viral, peripartum, autoimmune Endocrine: thyroid, phaeochomocytoma Metabolic/infiltrative: amyloid, haemachromatosis, sarcoid, mitochondrial disease muscular dystrophy related Obesity related, diabetic, ESRF Tachycardia related cardiomyopathy: AF/flutter, ventricular ectopic related, PJRT type SVTs Valvular heart disease related LVSD





15 Improving prognosis in LVSD heart failure

16 Grading of heart failure
17 Pharmacological treatment of chronic heart failure (due to LV systolic dysfunction) ACE inhibitors: uptitrated to max tolerated dose Betablockers: bisoprolol or carvedilol.max tolerated dose Aldosterone receptor blockers: spironolactone, eplerenone ARBs: if ACE I inolerant. Candesartan/valsartan Stop agents that exacerbate HF: NSAIDs, verapamil, diltiazem, doxazosin, dronedarone, class I AADs, glitizones Loop diuretics: as low a dose as possible to achieve euvolaemia Warfarin if AF Ivabradine: for some patients in SR if HR>70 despite max tolerated BB Hydralazine / ISDN if ACEI/ARB intolerant Digoxin: sometimes in AF rarely in SR
18 Betablockers in Heart failure US carvedilol trials NYHA I III (IV) n=1094, 4 separate trials, 65% RRR in mortality CIBIS II bisoprolol NYHA II III n=2647, mortality 11.8% v 17.3% (p<0.0001) MERIT metoprolol CR/XL NYHA II III improved mortality, morbidity and LVEF Betablockers reduce ABSOLUTE annual mortality by 6 8%
19 Probability of event-free survival Carvedilol reduces risk of death or cardiovascular hospitalisation 38% reduction in death or hospitalisation p<0.001 Carvedilol Placebo Duration of therapy (days) 400 Packer et al, NEJM 1996
20 Aldosterone receptor blockade Spironolactone 25mg or eplerenone 25 50mg
21 Spironolactone in NYHA III IV RALES: All Cause Mortality Probability of survival Placebo + ACE inhibitor + loop diuretic ± digitalis Risk reduction 30% 95% CI (18%-40%) p < Aldosterone receptor antagonist + ACE inhibitor + loop diuretic ± digitalis Months Pitt B et al, N Engl J Med 1999; 341:
22 EMPHASIS HF: Eplerenone in NYHA II heart failure NYHA II LVEF <30% (severe) LVEF 30 35% if QRS>130ms Outcome Eplerenone (%) Placebo (%) Adjusted hazard ratio (95% CI) p Cardiovascular death/heart-failure hospitalization ( ) <0.001 Cardiovascular death ( ) 0.01 Heart-failure hospitalization ( ) <0.001 Hospitalization for hyperkalemia ( ) 0.85
23 Safely prescribing spironolactone /eplerenone: avoiding hyperkalaemia Check renal function and potassium before starting Repeat U+Es after 1 week, then 1 month (2 weeks if renal dysfunction or K+>5) Check U+Es 3 monthly Reduce/withold if K+ >5.5, reintroduce at ½dose Advise patients to temporarily stop spiro/epler if intercurrent illness such as D+V / N+V / reduced fluid intake and inform GP/HFSN: must check U+Es
24 A well treated LVSD patient in 2011.in Grampian. Diuretic BFZ or loop: as low a dose as required ACE I NYHA I IV, max. tolerated dose BB NYHA I IV: carvedilol, bisoprolol stable, compensated HF, start low, go slow: aim for 25mg BD (50mgbd if >85kg) or 10mgOD respectively Spironolactone 25mg NYHA III IV, watch potassium/renal function Spironolactone or eplerenone NYHA II with severe LVSD esp if LBBB Candasartan/valsartan good alternatives to ACE I if ACE I intolerant. Hydralazine/nitrate if ACE I/ARB intolerant (usually renal failure) Ivabradine: if HR >70bpm despite max tolerated BB, and particularly consider in asthmatic patients
25 Beyond pharmacological therapy CRTs and ICDs
26 Cardiac resynchronisation therapy (CRT) the theory In patients with CHF and LBBB not only is there poor LV contraction but dyssynchronous contraction LBBB patients have a poorer prognosis: increased rate of HF and sudden arrhythmic deaths Cardiac resynchronisation therapy can improve these factors and increase cardiac performance Biventricular pacing +/ ICD


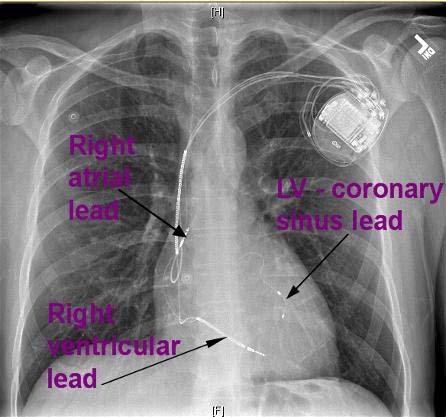
27 CRT (cardiac resynchronisation therapy): Biventricular pacemaker
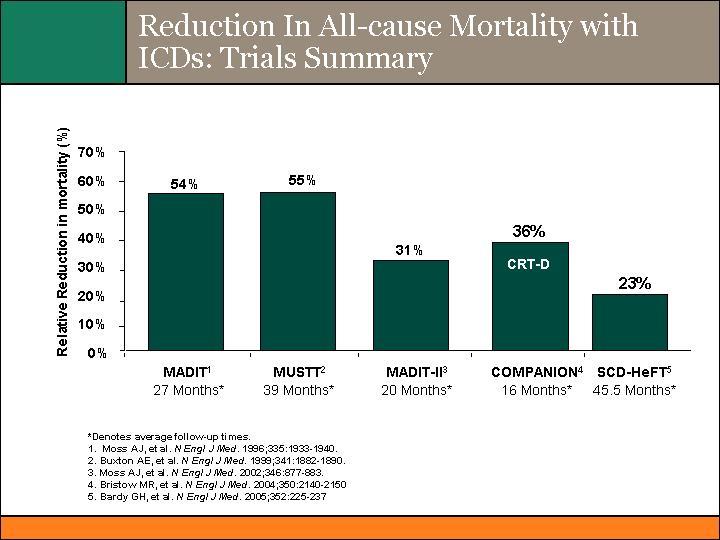
28 CARE HF n=813, NYHA III IV LVSD and LBBB Death/hosp for MACE: 224 (55%) in medical and 159 (39%) in CRT (HR 0.63, p<0.001) Death: 120 (30%) in medical and 82 (20%) in CRT (HR 0.64, ) Death and HF hosp: 191 (47%) in medical group vs 118 (29%) in CRT (HR 0.54, p<0.01)
29 Which patients should be considered for CRT? NYHA III IV despite maximum (tolerated) medical therapy No major co morbidity likely to be fatal in next 6 12 months or likely to be major contributor to poor QOL/SOB Evidence of conduction abnormalities (ideally LBBB) Age is not a contraindication

30 Mechanisms of death in CHF
31 Implantable cardioverter defibrillators: ICDs Implanted as per a pacemaker: local anaesthesia and sedation RV lead has a shocking coil and generator has defibrillator capacity Once inserted VF induced and device tested Secondary prevention well established: what about primary prevention?
32
33 What does NICE recommend? Ischaemic cardiomyopathies, >4 weeks post MI, NYHA < IV LVEF <35 % and NSVT on holter and inducible VT on EP testing LVEF<30% and QRS>120ms
34 Reducing HF admissions: why and how?

35 Hospitalisation for decompensated HF: an important event c10% in hospital mortality Mean days in hospital stay c30% readmission rate by 3 months c15% 3 month mortality
36 Healthcare Improvement Scotland (QIS) and SPSP recommendations for in patients with HF 1.Evidence based drug therapies 2.HF specialist nurse review 3.HF specialist review: treat acute decompensation/consider precipitating factors/ consider specialist investigation, drug therapy optimisation and consider CRT device if appropriate
 in usual care and nurse intervention groups Blue et al BMJ 2001;")
37 HF Specialist Nurse Intervention Time to first event (death from any cause or hospital admission for heart failure) in usual care and nurse intervention groups Blue et al BMJ 2001; 323: 715 8
38 The role of the heart failure specialist nurse Patient education Compliance, fluid balance awareness, daily weights, exercise, reduced anxiety Optimisation of drug therapy Contact point for patients All these contribute to less decompensations and earlier presentation: results in fewer hospitalisations and shorter admissions



39 Scottish National HF Audit 2008: n=1235
40 Scottish National HF Audit 2008 Table 9 Age adjusted in hospital mortality rates by specialty Specialty N Mean age (years) Deaths (% dead) Odds ratio (95% CI) p value Cardiology % Reference Care of the elderly % General %
41 Grampian strategy to reducing readmissions Starting point: 30% re admission rate for decompensated HF at 3 months 17.7% in hospital mortality rate (national audit) HFSN review during admission and early post discharge Inpatient review /management by cardiologist / HF specialist Avoid stopping important drugs during decompensations esp betablockers Accurate, informative (and legible) interim DC letters GP review early post discharge Good patient education: self management, daily weight Optimise drug therapy post discharge Early cardiology clinic review for most Consider CRT devices in timely fashion
42 Trial trends in 1 year mortality in NYHA III/IV CHF placebo therapy CONSENSUS RALES COPERNICUS CARE-HF
43 HFSN referrals 2011 Patient Referrals Number of individuals Jan Feb Mar Apr May Jun 2011
44 Reasons for optimism in Grampian? Improved diagnostic pathway with BNP Fastrack HF clinic for those at high risk HFSN referrals are up dramatically, hopefully leading to improved early post discharge care and fewer re admissions Renewed focus on HF in primary care: QOF pathway for HF finalised yesterday Active CRT service in ARI: improving pathways of care will result in higher referral rates

45
Advanced Heart Failure Management. Dr Andrew Hannah Consultant Cardiologist Aberdeen Royal Infirmary
 Advanced Heart Failure Management Dr Andrew Hannah Consultant Cardiologist Aberdeen Royal Infirmary Grading of heart failure Mr WY age 73 3/12 dyspnoea, fatigue and some ankle oedema PMH: hypertension
Advanced Heart Failure Management Dr Andrew Hannah Consultant Cardiologist Aberdeen Royal Infirmary Grading of heart failure Mr WY age 73 3/12 dyspnoea, fatigue and some ankle oedema PMH: hypertension
A patient with decompensated HF
 A patient with decompensated HF Professor Michel KOMAJDA University Pierre & Marie Curie Pitie Salpetriere Hospital Department of Cardiology Paris (France) Declaration Of Interest 2010 Speaker : Servier,
A patient with decompensated HF Professor Michel KOMAJDA University Pierre & Marie Curie Pitie Salpetriere Hospital Department of Cardiology Paris (France) Declaration Of Interest 2010 Speaker : Servier,
Heart Failure from a GP perspective
 Heart Failure from a GP perspective Jane Gilmour, Alison Wright Clinical Nurse Specialists for Heart Failure The Heart failure Team Dr Ganesan Kumar- Consultant Cardiologist Dr D Maras- Staff Grade Cardiology
Heart Failure from a GP perspective Jane Gilmour, Alison Wright Clinical Nurse Specialists for Heart Failure The Heart failure Team Dr Ganesan Kumar- Consultant Cardiologist Dr D Maras- Staff Grade Cardiology
Heart Failure. Jay Shavadia
 Heart Failure Jay Shavadia Definition Clinical syndrome characterized by: Symptoms: breathlessness at rest or on exercise, fatigue, tiredness or ankle swelling AND Signs: tachycardia, tachypnea, pulmonary
Heart Failure Jay Shavadia Definition Clinical syndrome characterized by: Symptoms: breathlessness at rest or on exercise, fatigue, tiredness or ankle swelling AND Signs: tachycardia, tachypnea, pulmonary
Heart Failure in 2012 with reference to NICE Guidance Dr Maurice Pye Consultant Cardiologist York District Hospital
 Heart Failure in 2012 with reference to NICE Guidance 2010 Dr Maurice Pye Consultant Cardiologist York District Hospital A little over elaborate,do not include ECG or CXR If clinical suspicion is high
Heart Failure in 2012 with reference to NICE Guidance 2010 Dr Maurice Pye Consultant Cardiologist York District Hospital A little over elaborate,do not include ECG or CXR If clinical suspicion is high
Inverclyde CHP Protected Learning Event- Heart Failure
 Inverclyde CHP Protected Learning Event- Heart Failure 14:00 14:05 14:05 14:20 14:20 14:30 14:30 15:10 15:10 15:30 15:30 15:50 15:50 16:05 16:05 16:35 Welcome & Introduction Paul Forsyth (HF Pharmacist)
Inverclyde CHP Protected Learning Event- Heart Failure 14:00 14:05 14:05 14:20 14:20 14:30 14:30 15:10 15:10 15:30 15:30 15:50 15:50 16:05 16:05 16:35 Welcome & Introduction Paul Forsyth (HF Pharmacist)
Understanding and Development of New Therapies for Heart Failure - Lessons from Recent Clinical Trials -
 Understanding and Development of New Therapies for Heart Failure - Lessons from Recent Clinical Trials - Clinical trials Evidence-based medicine, clinical practice Impact upon Understanding pathophysiology
Understanding and Development of New Therapies for Heart Failure - Lessons from Recent Clinical Trials - Clinical trials Evidence-based medicine, clinical practice Impact upon Understanding pathophysiology
8:30-10:30 WS #4: Cardiology :00-13:00 WS #11: Cardiology 101 (Repeated)
") Professor Ralph Stewart Cardiologist Auckland City Hospital Green Lane Cardiovascular Research Unit Auckland Heart Group Fiona Stewart Cardiologist Green Lane Hospital National Women's Hospital Professor
Professor Ralph Stewart Cardiologist Auckland City Hospital Green Lane Cardiovascular Research Unit Auckland Heart Group Fiona Stewart Cardiologist Green Lane Hospital National Women's Hospital Professor
1000 Lives Key Components of Reliable, Evidence-Based Chronic Heart Failure Care how do we compare?
 1000 Lives Key Components of Reliable, Evidence-Based Chronic Heart Failure Care how do we compare? Dr Nerys Davies, GPST Ms B. Davies, Specialist Nurse (Heart Failure) Dr J. Taylor, Consultant Cardiologist
1000 Lives Key Components of Reliable, Evidence-Based Chronic Heart Failure Care how do we compare? Dr Nerys Davies, GPST Ms B. Davies, Specialist Nurse (Heart Failure) Dr J. Taylor, Consultant Cardiologist
ESC Guidelines for the Diagnosis and Treatment of Chronic Heart Failure
 ESC Guidelines for the Diagnosis and Treatment of Chronic Heart Failure - 2005 Karl Swedberg Professor of Medicine Department of Medicine Sahlgrenska University Hospital/Östra Göteborg University Göteborg
ESC Guidelines for the Diagnosis and Treatment of Chronic Heart Failure - 2005 Karl Swedberg Professor of Medicine Department of Medicine Sahlgrenska University Hospital/Östra Göteborg University Göteborg
Heart Failure Treatments
 Heart Failure Treatments Past & Present www.philippelefevre.com Background Background Chronic heart failure Drugs Mechanical Electrical Background Chronic heart failure Drugs Mechanical Electrical Sudden
Heart Failure Treatments Past & Present www.philippelefevre.com Background Background Chronic heart failure Drugs Mechanical Electrical Background Chronic heart failure Drugs Mechanical Electrical Sudden
Cardiology. Presented by: Dr Paul Bethell GP Lead for Planned Care
 Cardiology Presented by: Dr Paul Bethell GP Lead for Planned Care 16 th April 2015 Integrated Cardiology Service for Ipswich and East Suffolk CCG IHT 6 consultants - all with specialist areas PCI CoW rapid
Cardiology Presented by: Dr Paul Bethell GP Lead for Planned Care 16 th April 2015 Integrated Cardiology Service for Ipswich and East Suffolk CCG IHT 6 consultants - all with specialist areas PCI CoW rapid
ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure
 Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Diagnosis and management of Chronic Heart Failure in 2018: What does NICE say? PCCS Meeting Issues and Answers Conference Nottingham
 Diagnosis and management of Chronic Heart Failure in 2018: What does NICE say? PCCS Meeting Issues and Answers Conference Nottingham NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Chronic heart failure
Diagnosis and management of Chronic Heart Failure in 2018: What does NICE say? PCCS Meeting Issues and Answers Conference Nottingham NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Chronic heart failure
Guideline-Directed Medical Therapy
 Guideline-Directed Medical Therapy Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation OPTIMAL THERAPY (As defined in
Guideline-Directed Medical Therapy Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation OPTIMAL THERAPY (As defined in
The Failing Heart in Primary Care
 The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
Congestive Heart Failure or Heart Failure
 Congestive Heart Failure or Heart Failure Dr Hitesh Patel Ascot Cardiology Group Heart Failure Workshop April, 2014 Question One What is the difference between congestive heart failure and heart failure?
Congestive Heart Failure or Heart Failure Dr Hitesh Patel Ascot Cardiology Group Heart Failure Workshop April, 2014 Question One What is the difference between congestive heart failure and heart failure?
State-of-the-Art Management of Chronic Systolic Heart Failure
 State-of-the-Art Management of Chronic Systolic Heart Failure Michael McCulloch, MD 17 th Annual Cardiovascular Update Intermountain Medical Center December 16, 2017 Disclosures: I have no financial disclosures
State-of-the-Art Management of Chronic Systolic Heart Failure Michael McCulloch, MD 17 th Annual Cardiovascular Update Intermountain Medical Center December 16, 2017 Disclosures: I have no financial disclosures
Update on pharmacological treatment of heart failure. Aldo Pietro Maggioni, MD, FESC ANMCO Research Center Firenze, Italy
 Update on pharmacological treatment of heart failure Aldo Pietro Maggioni, MD, FESC ANMCO Research Center Firenze, Italy Presenter Disclosures Dr. Maggioni : Serving in Committees of studies sponsored
Update on pharmacological treatment of heart failure Aldo Pietro Maggioni, MD, FESC ANMCO Research Center Firenze, Italy Presenter Disclosures Dr. Maggioni : Serving in Committees of studies sponsored
Heart Failure (HF) - Primary Care Flow Charts. Pre diagnosis Symptoms or signs suggestive of HF
 - Primary Care Flow Charts. Pre diagnosis Symptoms or signs suggestive of HF") Heart Failure (HF) - Primary Care Flow Charts Pre diagnosis Symptoms or signs suggestive of HF 12 lead ECG Normal examination and 12 lead ECG HF highly unlikely Abnormal 12 lead ECG HF Possible Arrange
Heart Failure (HF) - Primary Care Flow Charts Pre diagnosis Symptoms or signs suggestive of HF 12 lead ECG Normal examination and 12 lead ECG HF highly unlikely Abnormal 12 lead ECG HF Possible Arrange
Heart Failure (HF) - Primary Care Flow Charts. Symptoms or signs suggestive of HF. Pre diagnosis. Refer to the Heart Failure Clinic at VHK for
 - Primary Care Flow Charts. Symptoms or signs suggestive of HF. Pre diagnosis. Refer to the Heart Failure Clinic at VHK for") Heart Failure (HF) - Primary Care Flow Charts Pre diagnosis Symptoms or signs suggestive of HF 12 lead ECG Normal examination and 12 lead ECG HF highly unlikely Abnormal 12 lead ECG HF Possible Arrange
Heart Failure (HF) - Primary Care Flow Charts Pre diagnosis Symptoms or signs suggestive of HF 12 lead ECG Normal examination and 12 lead ECG HF highly unlikely Abnormal 12 lead ECG HF Possible Arrange
Diagnosis & Management of Heart Failure. Abena A. Osei-Wusu, M.D. Medical Fiesta
 Diagnosis & Management of Heart Failure Abena A. Osei-Wusu, M.D. Medical Fiesta Learning Objectives: 1) Become familiar with pathogenesis of congestive heart failure. 2) Discuss clinical manifestations
Diagnosis & Management of Heart Failure Abena A. Osei-Wusu, M.D. Medical Fiesta Learning Objectives: 1) Become familiar with pathogenesis of congestive heart failure. 2) Discuss clinical manifestations
Heart Failure. GP Update Refresher 18 th January 2018
 GP Update Refresher 18 th January 2018 Heart Failure Dr. Alexander Lyon Senior Lecturer and Consultant Cardiologist Clinical Lead in Cardio-Oncology Royal Brompton Hospital, London UK President of British
GP Update Refresher 18 th January 2018 Heart Failure Dr. Alexander Lyon Senior Lecturer and Consultant Cardiologist Clinical Lead in Cardio-Oncology Royal Brompton Hospital, London UK President of British
Arrhythmias and Heart Failure Dr Chris Lang Consultant Cardiologist and Electrophysiologist Royal Infirmary of Edinburgh
 Arrhythmias and Heart Failure Dr Chris Lang Consultant Cardiologist and Electrophysiologist Royal Infirmary of Edinburgh Arrhythmias and Heart Failure Ventricular Supraventricular VT/VF Primary prevention
Arrhythmias and Heart Failure Dr Chris Lang Consultant Cardiologist and Electrophysiologist Royal Infirmary of Edinburgh Arrhythmias and Heart Failure Ventricular Supraventricular VT/VF Primary prevention
The NEW Heart Failure Guidelines
 The NEW Heart Failure Guidelines Daily Practice HF scenario of the Case Presentations HF as a complex and heterogeneous syndrome Several proposed pathophysiological mechanisms involving the heart and the
The NEW Heart Failure Guidelines Daily Practice HF scenario of the Case Presentations HF as a complex and heterogeneous syndrome Several proposed pathophysiological mechanisms involving the heart and the
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Heart Failure Management. Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist
 Heart Failure Management Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist Heart failure prevalence is expected to continue to increase¹ 21 MILLION ADULTS WORLDWIDE
Heart Failure Management Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist Heart failure prevalence is expected to continue to increase¹ 21 MILLION ADULTS WORLDWIDE
NCAP NATIONAL CARDIAC AUDIT PROGR AMME NATIONAL HEART FAILURE AUDIT 2016/17 SUMMARY REPORT
 NCAP NATIONAL CARDIAC AUDIT PROGR AMME NATIONAL HEART FAILURE AUDIT 2016/17 SUMMARY REPORT CONTENTS PATIENTS ADMITTED WITH HEART FAILURE...4 Demographics... 4 Trends in Symptoms... 4 Causes and Comorbidities
NCAP NATIONAL CARDIAC AUDIT PROGR AMME NATIONAL HEART FAILURE AUDIT 2016/17 SUMMARY REPORT CONTENTS PATIENTS ADMITTED WITH HEART FAILURE...4 Demographics... 4 Trends in Symptoms... 4 Causes and Comorbidities
Cardiac resynchronisation therapy (biventricular pacing) for the treatment of heart failure
 for the treatment of heart failure") NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Health Technology Appraisal for the treatment of heart failure Final scope Appraisal objective To appraise the clinical and cost effectiveness of cardiac
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Health Technology Appraisal for the treatment of heart failure Final scope Appraisal objective To appraise the clinical and cost effectiveness of cardiac
Checklist for Treating Heart Failure. Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute
 Checklist for Treating Heart Failure Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute Novartis Disclosure Heart Failure (HF) a complex clinical syndrome that arises secondary to abnormalities
Checklist for Treating Heart Failure Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute Novartis Disclosure Heart Failure (HF) a complex clinical syndrome that arises secondary to abnormalities
DISCLOSURES ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION NONE
 ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION Lori M. Tam, MD Providence Heart Institute DISCLOSURES NONE 1 OUTLINE Systolic vs. Diastolic Heart Failure New
ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION Lori M. Tam, MD Providence Heart Institute DISCLOSURES NONE 1 OUTLINE Systolic vs. Diastolic Heart Failure New
Pharmacological Treatment for Chronic Heart Failure. Dr Elaine Chau HK Sanatorium & Hospital, Hong Kong 3 August 2014
 Pharmacological Treatment for Chronic Heart Failure Dr Elaine Chau HK Sanatorium & Hospital, Hong Kong 3 August 2014 1 ACC/AHA 2005 guideline update for Diagnosis & management of CHF in the Adult -SA Hunt
Pharmacological Treatment for Chronic Heart Failure Dr Elaine Chau HK Sanatorium & Hospital, Hong Kong 3 August 2014 1 ACC/AHA 2005 guideline update for Diagnosis & management of CHF in the Adult -SA Hunt
ESC Guidelines. ESC Guidelines Update For internal training purpose. European Heart Journal, doi: /eurheart/ehn309
 ESC Guidelines Update 2008 ESC Guidelines Heart failure update 2008 For internal training purpose. 0 Agenda Introduction Classes of recommendations Level of evidence Treatment algorithm Changes to ESC
ESC Guidelines Update 2008 ESC Guidelines Heart failure update 2008 For internal training purpose. 0 Agenda Introduction Classes of recommendations Level of evidence Treatment algorithm Changes to ESC
BSH Heart Failure Day for Revalidation and Training 2017
 BSH Heart Failure Day for Revalidation and Training 2017 Presentation title: Case Presentation cardio-oncology Speaker: Mark Drury-Smith Conflicts of interest: None British Society of Heart Failure 2017
BSH Heart Failure Day for Revalidation and Training 2017 Presentation title: Case Presentation cardio-oncology Speaker: Mark Drury-Smith Conflicts of interest: None British Society of Heart Failure 2017
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Position Statement on ALDOSTERONE ANTAGONIST THERAPY IN CHRONIC HEART FAILURE
 Position Statement on ALDOSTERONE ANTAGONIST THERAPY IN CHRONIC HEART FAILURE Over 8,000 patients have been studied in two well-designed placebo-controlled outcome-driven clinical trials to evaluate the
Position Statement on ALDOSTERONE ANTAGONIST THERAPY IN CHRONIC HEART FAILURE Over 8,000 patients have been studied in two well-designed placebo-controlled outcome-driven clinical trials to evaluate the
CT Academy of Family Physicians Scientific Symposium October 2012 Amit Pursnani, MD
 CT Academy of Family Physicians Scientific Symposium October 2012 Amit Pursnani, MD Clinical syndrome resulting from a structural or functional cardiac disorder that impairs the ability of the heart to
CT Academy of Family Physicians Scientific Symposium October 2012 Amit Pursnani, MD Clinical syndrome resulting from a structural or functional cardiac disorder that impairs the ability of the heart to
Combination of renin-angiotensinaldosterone. how to choose?
 Combination of renin-angiotensinaldosterone system inhibitors how to choose? Karl Swedberg Professor of Medicine Sahlgrenska Academy University of Gothenburg karl.swedberg@gu.se Disclosures Research grants
Combination of renin-angiotensinaldosterone system inhibitors how to choose? Karl Swedberg Professor of Medicine Sahlgrenska Academy University of Gothenburg karl.swedberg@gu.se Disclosures Research grants
Aldosterone Antagonism in Heart Failure: Now for all Patients?
 Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Antialdosterone treatment in heart failure
 Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
Chronic heart failure: management of chronic heart failure in adults in primary and secondary care (partial update)
") Chronic heart failure: management of chronic heart failure in adults in primary and secondary care (partial update) NICE guideline Apendix C The algorithms Draft for consultation, January 2010 Chronic
Chronic heart failure: management of chronic heart failure in adults in primary and secondary care (partial update) NICE guideline Apendix C The algorithms Draft for consultation, January 2010 Chronic
Heart Failure Acute and Chronic
 Heart Failure Acute and Chronic Cardiac Services in Wales Acute Heart Failure standards Chronic Heart Failure standards NWIS admissions/readmission data NHFA data 2016-17 Echo accessibility BNP availability
Heart Failure Acute and Chronic Cardiac Services in Wales Acute Heart Failure standards Chronic Heart Failure standards NWIS admissions/readmission data NHFA data 2016-17 Echo accessibility BNP availability
Optimal blockade of the Renin- Angiotensin-Aldosterone. in chronic heart failure
 Optimal blockade of the Renin- Angiotensin-Aldosterone Aldosterone- (RAA)-System in chronic heart failure Jan Östergren Department of Medicine Karolinska University Hospital Stockholm, Sweden Key Issues
Optimal blockade of the Renin- Angiotensin-Aldosterone Aldosterone- (RAA)-System in chronic heart failure Jan Östergren Department of Medicine Karolinska University Hospital Stockholm, Sweden Key Issues
eplerenone 25, 50mg film-coated tablets (Inspra ) SMC No. (793/12) Pfizer Ltd
 SMC No. (793/12) Pfizer Ltd") eplerenone 25, 50mg film-coated tablets (Inspra ) SMC No. (793/12) Pfizer Ltd 08 June 2012 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product and advises NHS Boards
eplerenone 25, 50mg film-coated tablets (Inspra ) SMC No. (793/12) Pfizer Ltd 08 June 2012 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product and advises NHS Boards
Chronic. Outline. Congestive^ Heart Failure: Update on Effective Monitoring and Treatment. Heart Failure Epidemiology. Michael G.
 Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Heart Failure A Disease for the Internist?
 Heart Failure A Disease for the Internist? Dr Chris Davidson Sussex Cardiac Centre BRIGHTON UK Hot Topics in Heart Failure Drug treatments Valsartan / neprilysin inhib Investigations BNP and others Devices
Heart Failure A Disease for the Internist? Dr Chris Davidson Sussex Cardiac Centre BRIGHTON UK Hot Topics in Heart Failure Drug treatments Valsartan / neprilysin inhib Investigations BNP and others Devices
What s new in 2016 Guidelines of the European Society of Cardiology? HEART FAILURE. Marc Ferrini (Lyon Fr)
") What s new in 2016 Guidelines of the European Society of Cardiology? HEART FAILURE Marc Ferrini (Lyon Fr) Palermo (I) 1 04 2017 Consulting Fees, Honoraria: BAYER PHARMA BOEHRINGER INGELHEIM BRISTOL MEYERS
What s new in 2016 Guidelines of the European Society of Cardiology? HEART FAILURE Marc Ferrini (Lyon Fr) Palermo (I) 1 04 2017 Consulting Fees, Honoraria: BAYER PHARMA BOEHRINGER INGELHEIM BRISTOL MEYERS
Therapeutic Targets and Interventions
 Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
Charles Spencer MD, FRCP Consultant Cardiologist Mid Staffs NHSFT
 Charles Spencer MD, FRCP Consultant Cardiologist Mid Staffs NHSFT Key Messages Heart Failure is Common Heart failure is complex Heart Failure is a major issue for the NHS Heart Failure has a worse prognosis
Charles Spencer MD, FRCP Consultant Cardiologist Mid Staffs NHSFT Key Messages Heart Failure is Common Heart failure is complex Heart Failure is a major issue for the NHS Heart Failure has a worse prognosis
Heart Failure Background, recognition, diagnosis and management
 Heart Failure Background, recognition, diagnosis and management Speaker bureau: Novartis At the conclusion of this activity, participants will be able to: Recognize signs and symptoms of heart failure
Heart Failure Background, recognition, diagnosis and management Speaker bureau: Novartis At the conclusion of this activity, participants will be able to: Recognize signs and symptoms of heart failure
Heart Failure A Team Approach Background, recognition, diagnosis and management
 Heart Failure A Team Approach Background, recognition, diagnosis and management Speaker bureau: Novartis At the conclusion of this activity, participants will be able to: Recognize signs and symptoms of
Heart Failure A Team Approach Background, recognition, diagnosis and management Speaker bureau: Novartis At the conclusion of this activity, participants will be able to: Recognize signs and symptoms of
HFpEF. April 26, 2018
 HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
HEART FAILURE SUMMARY. and is associated with significant morbidity and mortality. the cornerstone of heart failure treatment.
 HEART FAILURE SUMMARY + Heart Failure is a condition affecting a large number of Irish people and is associated with significant morbidity and mortality. + ACE inhibitors, in combination with diuretics,
HEART FAILURE SUMMARY + Heart Failure is a condition affecting a large number of Irish people and is associated with significant morbidity and mortality. + ACE inhibitors, in combination with diuretics,
Chronic. Outline. Congestive^ Heart Failure: Update on Effective Monitoring and Treatment. Heart Failure Epidemiology
 Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Heart Failure. Dr. William Vosik. January, 2012
 Heart Failure Dr. William Vosik January, 2012 Questions for clinicians to ask Is this heart failure? What is the underlying cause? What are the associated disease processes? Which evidence-based treatment
Heart Failure Dr. William Vosik January, 2012 Questions for clinicians to ask Is this heart failure? What is the underlying cause? What are the associated disease processes? Which evidence-based treatment
Congestive Heart Failure: Outpatient Management
 The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
I know the trials in heart failure but how do I manage my patient? Dosing of neurohormones antagonists
 I know the trials in heart failure but how do I manage my patient? Dosing of neurohormones antagonists Alessandro Fucili (Ferrara, IT) Massimo F Piepoli (Piacenza, IT) Clinical Case: 82 year old woman
I know the trials in heart failure but how do I manage my patient? Dosing of neurohormones antagonists Alessandro Fucili (Ferrara, IT) Massimo F Piepoli (Piacenza, IT) Clinical Case: 82 year old woman
The CCS Heart Failure Companion: Bridging Guidelines to your Practice
 The CCS Heart Failure Companion: Bridging Guidelines to your Practice Looking for practical answers concerning optimal heart failure care? The CCS Heart Failure Guidelines Companion can help. The Canadian
The CCS Heart Failure Companion: Bridging Guidelines to your Practice Looking for practical answers concerning optimal heart failure care? The CCS Heart Failure Guidelines Companion can help. The Canadian
Heart Failure Dr Eric Klug Sunninghill, Sunward Park, CM Johannesburg Academic Hospital
 Heart Failure 2012 Dr Eric Klug Sunninghill, Sunward Park, CM Johannesburg Academic Hospital PRELOAD COWS Reduction in milk production INOTROPY & HEART RATE AFTERLOAD DISTRIBUTION NETWORK THE CLASSIC APPROACH
Heart Failure 2012 Dr Eric Klug Sunninghill, Sunward Park, CM Johannesburg Academic Hospital PRELOAD COWS Reduction in milk production INOTROPY & HEART RATE AFTERLOAD DISTRIBUTION NETWORK THE CLASSIC APPROACH
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Heart Failure Medical and Surgical Treatment
 Heart Failure Medical and Surgical Treatment Daniel S. Yip, M.D. Medical Director, Heart Failure and Transplantation Mayo Clinic Second Annual Lakeland Regional Health Cardiovascular Symposium February
Heart Failure Medical and Surgical Treatment Daniel S. Yip, M.D. Medical Director, Heart Failure and Transplantation Mayo Clinic Second Annual Lakeland Regional Health Cardiovascular Symposium February
LITERATURE REVIEW: HEART FAILURE. Chief Residents
 LITERATURE REVIEW: HEART FAILURE Chief Residents Heart Failure EF 40% HFrEF Problem with contractility EF 40-50% HFmrEF EF > 50% HFpEF Problem with filling/relaxation RISK FACTORS Post MI HTN DM Obesity
LITERATURE REVIEW: HEART FAILURE Chief Residents Heart Failure EF 40% HFrEF Problem with contractility EF 40-50% HFmrEF EF > 50% HFpEF Problem with filling/relaxation RISK FACTORS Post MI HTN DM Obesity
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST TAKE HOME MESSAGES FROM RECENT HEART FAILURE CLINICAL TRIALS How to use aldosterone blockers? Faiez Zannad INSERM, U961 and Clinical Investigation Center CHU, Heart
DECLARATION OF CONFLICT OF INTEREST TAKE HOME MESSAGES FROM RECENT HEART FAILURE CLINICAL TRIALS How to use aldosterone blockers? Faiez Zannad INSERM, U961 and Clinical Investigation Center CHU, Heart
Ventricular Assist Device: Are Early Interventions Superior? Hamang Patel, MD Section of Cardiomyopathy & Heart Transplantation
 Ventricular Assist Device: Are Early Interventions Superior? Hamang Patel, MD Section of Cardiomyopathy & Heart Transplantation Objectives Current rationale behind use of MCS Patient Selection Earlier?
Ventricular Assist Device: Are Early Interventions Superior? Hamang Patel, MD Section of Cardiomyopathy & Heart Transplantation Objectives Current rationale behind use of MCS Patient Selection Earlier?
Performance and Quality Measures 1. NQF Measure Number. Coronary Artery Disease Measure Set
 Unless indicated, the PINNACLE Registry measures are endorsed by the American College of Cardiology Foundation and the American Heart Association and may be used for purposes of health care insurance payer
Unless indicated, the PINNACLE Registry measures are endorsed by the American College of Cardiology Foundation and the American Heart Association and may be used for purposes of health care insurance payer
HEART FAILURE. A/Prof Nadarajah Kangaharan, FRACP, FCSANZ. Medical Director & Cardiologist Division of Medicine Royal Darwin Hospital
 HEART FAILURE A/Prof Nadarajah Kangaharan, FRACP, FCSANZ Medical Director & Cardiologist Division of Medicine Royal Darwin Hospital Cardiac Care in the NT Annual Workshop 2017 is proudly supported by:
HEART FAILURE A/Prof Nadarajah Kangaharan, FRACP, FCSANZ Medical Director & Cardiologist Division of Medicine Royal Darwin Hospital Cardiac Care in the NT Annual Workshop 2017 is proudly supported by:
Management of Heart Failure and Cardiomyopathies in Pregnancy
 Management of Heart Failure and Cardiomyopathies in Pregnancy Professor Sanjay Sharma Disclosures: None Epidemiology of Cardiac Disease In Pregnancy Cardiovascular disease in pregnancy is increasing in
Management of Heart Failure and Cardiomyopathies in Pregnancy Professor Sanjay Sharma Disclosures: None Epidemiology of Cardiac Disease In Pregnancy Cardiovascular disease in pregnancy is increasing in
Implantation of a CRT-Pacemaker Rather than CRT-Defibrillator is Usually Preferred
 Implantation of a CRT-Pacemaker Rather than CRT-Defibrillator is Usually Preferred Professor John GF Cleland University of Hull Kingston-upon-Hull United Kingdom Conflict of Interest: Funding or Speakers
Implantation of a CRT-Pacemaker Rather than CRT-Defibrillator is Usually Preferred Professor John GF Cleland University of Hull Kingston-upon-Hull United Kingdom Conflict of Interest: Funding or Speakers
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Implantable cardioverter defibrillators for the treatment of arrhythmias and cardiac resynchronisation therapy for the treatment of heart failure (review
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Implantable cardioverter defibrillators for the treatment of arrhythmias and cardiac resynchronisation therapy for the treatment of heart failure (review
Chronic. Outline. Congestive^ Heart Failure: Update on Effective Monitoring and Treatment. Heart Failure Epidemiology. Michael G.
 Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
New Strategies For Treating Patients With Chronic Heart Failure
 New Strategies For Treating Patients With Chronic Heart Failure Barry Greenberg MD Professor of Medicine Director, Advanced Heart Failure Treatment Program University of California, San Diego Disclosures
New Strategies For Treating Patients With Chronic Heart Failure Barry Greenberg MD Professor of Medicine Director, Advanced Heart Failure Treatment Program University of California, San Diego Disclosures
Diagnosis and management of chronic heart failure
 Quick reference guide for health professionals Diagnosis and management of chronic heart failure Updated October 2011 This quick reference guide is derived from the National Heart Foundation of Australia
Quick reference guide for health professionals Diagnosis and management of chronic heart failure Updated October 2011 This quick reference guide is derived from the National Heart Foundation of Australia
Chronic. Congestive^ Heart Failure: Update on Effective Monitoring and Treatment. Michael G. Shlipak, MD, MPH
 Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
CKD Satellite Symposium
 CKD Satellite Symposium Recommended Therapy by Heart Failure Stage AHA/ACC Task Force on Practice Guideline 2001 Natural History of Heart Failure Patients surviving % Mechanism of death Sudden death 40%
CKD Satellite Symposium Recommended Therapy by Heart Failure Stage AHA/ACC Task Force on Practice Guideline 2001 Natural History of Heart Failure Patients surviving % Mechanism of death Sudden death 40%
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
The ACC Heart Failure Guidelines
 The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
2/3/2017. Objectives. Effective Heart Failure Management through Evidence Based Practice and Innovation
 Effective Heart Failure Management through Evidence Based Practice and Innovation Jennifer Bauerly RN, CHFN, APRN-BC CentraCare Heart and Vascular Center Objectives Describe the scope and impact of heart
Effective Heart Failure Management through Evidence Based Practice and Innovation Jennifer Bauerly RN, CHFN, APRN-BC CentraCare Heart and Vascular Center Objectives Describe the scope and impact of heart
Faiez Zannad. Institut Lorrain du Coeur et des Vaisseaux. CIC - Inserm
 Faiez Zannad Institut Lorrain du Coeur et des Vaisseaux CIC - Inserm Disclosure Faiez Zannad Grants BG Medicine, Roche Diagnostics. Consultant/Steering committees/event committees/ Data safety Monitoring
Faiez Zannad Institut Lorrain du Coeur et des Vaisseaux CIC - Inserm Disclosure Faiez Zannad Grants BG Medicine, Roche Diagnostics. Consultant/Steering committees/event committees/ Data safety Monitoring
ESC Guidelines for diagnosis and management of HF 2012: What s new? John Parissis, MD Athens, GR
 ESC Guidelines for diagnosis and management of HF 2012: What s new? John Parissis, MD Athens, GR Disclosures ALARM INVESTIGATOR RESEARCH GRANTS BY ABBOTT USA AND ORION PHARMA The principal changes from
ESC Guidelines for diagnosis and management of HF 2012: What s new? John Parissis, MD Athens, GR Disclosures ALARM INVESTIGATOR RESEARCH GRANTS BY ABBOTT USA AND ORION PHARMA The principal changes from
Beta-blockers in heart failure: evidence put into practice
 Beta-blockers in heart failure: evidence put into practice John McMurray Professor of Medical Cardiology, University of Glasgow & Consultant Cardiologist,Western Infirmary, Glasgow, UK Eugene Braunwald
Beta-blockers in heart failure: evidence put into practice John McMurray Professor of Medical Cardiology, University of Glasgow & Consultant Cardiologist,Western Infirmary, Glasgow, UK Eugene Braunwald
Polypharmacy - arrhythmic risks in patients with heart failure
 Influencing sudden cardiac death by pharmacotherapy Polypharmacy - arrhythmic risks in patients with heart failure Professor Dan Atar Head, Dept. of Cardiology Oslo University Hospital Ullevål Norway 27.8.2012
Influencing sudden cardiac death by pharmacotherapy Polypharmacy - arrhythmic risks in patients with heart failure Professor Dan Atar Head, Dept. of Cardiology Oslo University Hospital Ullevål Norway 27.8.2012
Nora Goldschlager, M.D. SFGH Division of Cardiology UCSF
 CLASSIFICATION OF HEART FAILURE Nora Goldschlager, M.D. SFGH Division of Cardiology UCSF DISCLOSURES: NONE CLASSIFICATION C OF HEART FAILURE NYHA I IV New paradigm Stage A: Pts at high risk of developing
CLASSIFICATION OF HEART FAILURE Nora Goldschlager, M.D. SFGH Division of Cardiology UCSF DISCLOSURES: NONE CLASSIFICATION C OF HEART FAILURE NYHA I IV New paradigm Stage A: Pts at high risk of developing
Where Does the Wearable Cardioverter Defibrillator (WCD) Fit In?
 Fit In?") Where Does the Wearable Cardioverter Defibrillator (WCD) Fit In? 24 th Annual San Diego Heart Failure Symposium June 1-2, 2018 La Jolla, CA Barry Greenberg, MD Distinguished Professor of Medicine Director,
Where Does the Wearable Cardioverter Defibrillator (WCD) Fit In? 24 th Annual San Diego Heart Failure Symposium June 1-2, 2018 La Jolla, CA Barry Greenberg, MD Distinguished Professor of Medicine Director,
National Horizon Scanning Centre. Irbesartan (Aprovel) for heart failure with preserved systolic function. August 2008
 for heart failure with preserved systolic function. August 2008") Irbesartan (Aprovel) for heart failure with preserved systolic function August 2008 This technology summary is based on information available at the time of research and a limited literature search. It
Irbesartan (Aprovel) for heart failure with preserved systolic function August 2008 This technology summary is based on information available at the time of research and a limited literature search. It
NT-proBNP: Evidence-based application in primary care
 NT-proBNP: Evidence-based application in primary care Associate Professor Rob Doughty The University of Auckland, Auckland City Hospital, Auckland Heart Group NT-proBNP: Evidence in Primary Care The problem
NT-proBNP: Evidence-based application in primary care Associate Professor Rob Doughty The University of Auckland, Auckland City Hospital, Auckland Heart Group NT-proBNP: Evidence in Primary Care The problem
Heart Failure 101 The Basic Principles of Diagnosis & Management
 Heart Failure 101 The Basic Principles of Diagnosis & Management Bill Tran, MD Non Invasive Cardiologist February 24, 2018 What the eye does not see and the mind does not know, does not exist. DH Lawrence
Heart Failure 101 The Basic Principles of Diagnosis & Management Bill Tran, MD Non Invasive Cardiologist February 24, 2018 What the eye does not see and the mind does not know, does not exist. DH Lawrence
Cardiovascular Clinical Practice Guideline Pilot Implementation
 Cardiovascular Clinical Practice Guideline Pilot Implementation Pharmacologic Management of Chronic Heart Failure Sept 15, 2004 Angela Allerman, PharmD, BCPS DoD Pharmacoeconomic Center Promoting high
Cardiovascular Clinical Practice Guideline Pilot Implementation Pharmacologic Management of Chronic Heart Failure Sept 15, 2004 Angela Allerman, PharmD, BCPS DoD Pharmacoeconomic Center Promoting high
ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication Initiation and Titration
![ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication Initiation and Titration](/thumbs/77/76069192.jpg "ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication Initiation and Titration") ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication and Symptomatic HF despite ACEI/ARB and B-blocker therapy Bilateral renal artery stenosis Moderate/Severe
ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication and Symptomatic HF despite ACEI/ARB and B-blocker therapy Bilateral renal artery stenosis Moderate/Severe
Contemporary Advanced Heart Failure Therapy
 Contemporary Advanced Heart Failure Therapy Andrew Boyle, MD Professor of Medicine Medical Director of Advanced Heart Failure Thomas Jefferson University Philadelphia, PA Audience Response Question 40
Contemporary Advanced Heart Failure Therapy Andrew Boyle, MD Professor of Medicine Medical Director of Advanced Heart Failure Thomas Jefferson University Philadelphia, PA Audience Response Question 40
Heart Failure: Combination Treatment Strategies
 Heart Failure: Combination Treatment Strategies M. McDonald MD, FRCP State of the Heart Symposium May 28, 2011 None Disclosures Case 69 F, prior MIs (LV ejection fraction 25%), HTN No demonstrable ischemia
Heart Failure: Combination Treatment Strategies M. McDonald MD, FRCP State of the Heart Symposium May 28, 2011 None Disclosures Case 69 F, prior MIs (LV ejection fraction 25%), HTN No demonstrable ischemia
Heart Failure New Drugs- Updated Guidelines
 Heart Failure New Drugs- Updated Guidelines Eileen Handberg, PhD, ANP-BC, FAHA, FACC Professor of Medicine Division of Cardiovascular Medicine University of Florida Disclosures 1. 3 2. 6 3. 8 4. 11 Dunlay
Heart Failure New Drugs- Updated Guidelines Eileen Handberg, PhD, ANP-BC, FAHA, FACC Professor of Medicine Division of Cardiovascular Medicine University of Florida Disclosures 1. 3 2. 6 3. 8 4. 11 Dunlay
8. Pharmacological Management
 8. Pharmacological Management Neurohormonal deactivation 1. Adrenaline Beta Blockers Dose Side Effects Monitoring Neurohormonal Deactivation 2. Angiotensin II ACE Inhibition Dose Side Effects Monitoring
8. Pharmacological Management Neurohormonal deactivation 1. Adrenaline Beta Blockers Dose Side Effects Monitoring Neurohormonal Deactivation 2. Angiotensin II ACE Inhibition Dose Side Effects Monitoring
Drugs acting on the reninangiotensin-aldosterone
 Drugs acting on the reninangiotensin-aldosterone system John McMurray Eugene Braunwald Scholar in Cardiovascular Diseases, Brigham and Women s Hospital, Boston & Visiting Professor, Harvard Medical School
Drugs acting on the reninangiotensin-aldosterone system John McMurray Eugene Braunwald Scholar in Cardiovascular Diseases, Brigham and Women s Hospital, Boston & Visiting Professor, Harvard Medical School
Heart Failure Management: Continuum of Care
 Healthy Kingsport Conference Heart Failure Management: Continuum of Care Robin Harris PhD, ANP-BC, ACNS-BC Clinical Assistant Professor University of Tennessee College of Nursing Important Info I, Robin
Healthy Kingsport Conference Heart Failure Management: Continuum of Care Robin Harris PhD, ANP-BC, ACNS-BC Clinical Assistant Professor University of Tennessee College of Nursing Important Info I, Robin
Outline. Chronic Heart Failure: Update on Effective Monitoring and Treatment. Heart Failure Epidemiology. Michael G.
 Chronic Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center Scientific
Chronic Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center Scientific
HEART FAILURE. Study day November 2018 Sarah Briggs
 HEART FAILURE Study day November 2018 Sarah Briggs Overview and Introduction This course is an introduction and overview of heart failure. Normal heart function and basic pathophysiology of heart failure
HEART FAILURE Study day November 2018 Sarah Briggs Overview and Introduction This course is an introduction and overview of heart failure. Normal heart function and basic pathophysiology of heart failure
Behandlungsalgorithmus bei Herzinsuffizienz mit reduzierter Auswurffraktion
 Behandlungsalgorithmus bei Herzinsuffizienz mit reduzierter Auswurffraktion Professor Dr. med. Roger Hullin Leiter Programm für Schwere Herzinsuffizienz, VAD & Herztransplantation Suisse Romande Klinik
Behandlungsalgorithmus bei Herzinsuffizienz mit reduzierter Auswurffraktion Professor Dr. med. Roger Hullin Leiter Programm für Schwere Herzinsuffizienz, VAD & Herztransplantation Suisse Romande Klinik
heart failure John McMurray University of Glasgow.
 A to Z of RAAS blockade in heart failure John McMurray BHF Cardiovascular Research Centre University of Glasgow. RAAS inhibition in CHF ACE inhibition in patients with low LVEF CHF CONSENSUS Enalapril
A to Z of RAAS blockade in heart failure John McMurray BHF Cardiovascular Research Centre University of Glasgow. RAAS inhibition in CHF ACE inhibition in patients with low LVEF CHF CONSENSUS Enalapril
All in the Past? Win K. Shen, MD Mayo Clinic Arizona Controversies and Advances in CV Diseases Cedars-Sinai Heart Institute, MFMER
 ICD for NICM All in the Past? Win K. Shen, MD Mayo Clinic Arizona Controversies and Advances in CV Diseases Cedars-Sinai Heart Institute, 2017 2017 MFMER 3686275-1 DISCLOSURE Relevant Financial Relationship(s)
ICD for NICM All in the Past? Win K. Shen, MD Mayo Clinic Arizona Controversies and Advances in CV Diseases Cedars-Sinai Heart Institute, 2017 2017 MFMER 3686275-1 DISCLOSURE Relevant Financial Relationship(s)
NHS QIS National Measurement of Audit Acute Coronary Syndrome
 NHS QIS National Measurement of Audit Acute Coronary Syndrome Things have changed based on the experience and feedback from the first cycle of measurement and, for the better we think! The Acute Coronary
NHS QIS National Measurement of Audit Acute Coronary Syndrome Things have changed based on the experience and feedback from the first cycle of measurement and, for the better we think! The Acute Coronary